Paramedische en psychologische behandeling van FNS
Uitgangsvraag
Wat is de plaats van paramedische en psychologische behandeling bij patiënten met een functioneel-neurologisch-symptoomstoornis/functionele neurologische stoornis (FNS)?
Aanbeveling
Geef educatie over FNS na het stellen van de diagnose. Benoem expliciet de diagnose, en demonstreer of bespreek de positieve klinische kenmerken op basis waarvan de diagnose is gesteld. Wijs de patiënt op schriftelijke informatie over FNS, bijvoorbeeld de informatiefolder van de Nederlandse Vereniging voor Neurologie
Behandeling is afhankelijk van de aard van de symptomen:
- Verwijs patiënten met functionele motorische symptomen naar fysiotherapie
- Verwijs patiënten met FNS aanvallen voor psychologische behandeling
- Verwijs patiënten met functionele slik- en spraakstoornissen naar logopedie
- Overweeg “off-label” CGT of ACT voor patiënten met functionele cognitieve klachten
Overweeg hypnotherapie en katalepsie-inductie als onderdeel van een klachtgerichte behandeling van FNS, zoals fysiotherapie of CGT.
Overweeg “off-label” EMDR voor FNS bij patiënten die onvoldoende effect hebben van bovenstaande interventies.
Verwijs patiënten naar de ggz of revalidatie voor beschrijvende diagnostiek en behandeling volgens het biopsychosociale model als er bij indicatiestelling vermoeden is op belangrijke (andere) beïnvloedende factoren, zoals interfererende psychiatrische comorbiditeit, of wanneer klachtgerichte behandeling onvoldoende effect heeft. Zie ook submodule Geestelijke gezondheidszorg en module Multidisciplinaire behandeling.
Overwegingen
In de DSM-5(-TR) wordt de functionele neurologische stoornis geclassificeerd als 'functioneel-neurologisch-symptoomstoornis'. Hiernaast worden er in de wetenschappelijke literatuur ander termen gebruikt, zoals ‘conversion disorder en ‘dissociative neurological symptoms disorder’, ‘functional motor disorder’ (voor het motorische subtype), en ‘psychogenic non-epileptic seizures (PNES)’, ‘non-epileptic attacks (NEA)’ of ‘dissociative seizures’ (voor functionele aanvallen). In de neurologie, fysiotherapie en logopedie wordt de aanduiding 'functionele neurologische stoornis' gebruikt voor exact dezelfde stoornis als de functioneel-neurologisch-symptoomstoornis in de DSM-5. De term functionele neurologische stoornis is in lijn met gebruikte terminologie in recente wetenschappelijke literatuur en de voorkeur van patiënten (Ding, 2017). In deze module, die zich ook richt op klachtgerichte behandeling buiten de ggz, spreken we dan ook van de functionele neurologische stoornis (FNS) in plaats van de functioneel-neurologisch-symptoomstoornis.
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is een literatuuronderzoek verricht naar de effectiviteit van paramedische en psychologische behandelingen voor mensen met FNS. In totaal zijn er één systematische review (met daarin negen relevante RCTs) en twee RCTs gevonden die een vorm van paramedische of psychologische behandeling hebben onderzocht bij volwassenen FNS. De cruciale uitkomstmaten lichamelijke klachten, functioneren, psychologische klachten (angst, depressie) en kwaliteit van leven werden gerapporteerd door respectievelijk tien, vijf, acht, negen, en vier studies. Er werden klinisch relevante effecten gevonden in het voordeel van paramedische en psychologische behandeling voor de uitkomstmaten lichamelijke klachten en kwaliteit van leven. De overall bewijskracht werd beoordeeld als laag tot zeer laag. Dit betekent dat we (zeer) onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten. Er is afgewaardeerd vanwege (zeer) ernstige:
- Risk of Bias: methodologische beperkingen (gebrek aan blindering, hoog risico op selectiebias en detectiebias, ontbrekende uitkomstdata, selectieve uitkomst rapportage, en ontbrekende informatie voor meerdere domeinen).
- Imprecisie: onnauwkeurigheid, door brede betrouwbaarheidsintervallen en kleine studiepopulaties.
De bewijskracht van geselecteerde studies uit de literatuursearch voor deze module is beoordeeld als zeer laag. Echter is de behandeling van FNS een veld in ontwikkeling. Er is internationaal toenemende klinisch en wetenschappelijke aandacht voor de aandoening. Naast relevante experimentele en observationele studies zijn er aanbevelingen voor paramedische behandeling op basis van expert opinion gepubliceerd in de afgelopen jaren. De werkgroep heeft haar aanbevelingen derhalve niet alleen gebaseerd op de resultaten van de literatuurstudie, maar ook op de aanvullende wetenschappelijke evidentie, expert opinie en klinische ervaring.
In onderstaande tekst wordt onderscheid gemaakt tussen klachtgerichte behandeling en behandeling gericht op beïnvloedende factoren bij FNS. Met klachtgerichte behandeling bedoelen wij behandelingen die zich rechtstreeks op de functionele neurologische klachten richten, en als doel hebben deze klachten te verminderen of te herstellen. Bij behandeling gericht op beïnvloedende factoren wordt niet rechtstreeks aan de functionele neurologische klachten gewerkt, maar wordt de behandeling gericht op biopsychosociale factoren die de klachten in stand zouden kunnen houden of de patiënt kwetsbaar maken voor een terugval. In de tekst hieronder bespreken wij de klachtgerichte behandeling en behandeling gericht op beïnvloedende factoren separaat. Let wel: de eerste stap in iedere behandeling is educatie. Voor adviezen hierover verwijzen wij naar de Communicatie rondom diagnostiek van de functioneel-neurologisch-symptoomstoornis in submodule Medisch-specialistische zorg.
Klachtgerichte behandeling: paramedische behandeling
Bij het literatuuronderzoek naar paramedische behandeling voor FNS werden drie onderzoeken naar fysiotherapie geïncludeerd (Jordbru, 2014; Nielsen, 2017; Nielsen, 2024).
Fysiotherapeutische behandeling
Onze literatuurstudie toont aan dat fysiotherapie positieve effecten kan hebben op lichamelijke klachten, waaronder functionele motorische symptomen (Nielsen, 2017; Nielsen, 2024), functioneren (Jordbru, 2014; Nielsen, 2017; Nielsen, 2024) en kwaliteit van leven (Jordbru, 2014) bij mensen met FNS. De grootste studie, de RCT van Nielsen (2024), vergeleek gespecialiseerde fysiotherapie met reguliere fysiotherapie. Hoewel hier geen verschil tussen de groepen werd gevonden op de primaire uitkomstmaat (fysiek functioneren), was er wel een significant verschil op subjectieve verbetering van de symptomen. Daarnaast was er ten opzichte van het natuurlijk beloop (Gelauff, 2014) een verbetering in beide groepen van zowel fysiek functioneren als subjectieve ernst van de symptomen.
Een systematische review die naast RCTs ook observationele studies includeerde onderschrijft eveneens de positieve effecten van fysiotherapie (Nielsen, 2013). (Inter)nationale experts bevelen gespecialiseerde fysiotherapie aan, mede gebaseerd op nieuwe inzichten in pathofysiologische mechanismen waar fysiotherapie op kan aangrijpen, zoals veranderde aandachtsprocessen en verstoorde controle over beweging (Aybek, 2022). Ook in Nederland bestaat positieve en uitgebreide klinische ervaring met het effect van gespecialiseerde fysiotherapie op motorische symptomen bij FNS. Op basis van de wetenschappelijke evidentie en positieve klinische ervaringen beveelt de werkgroep fysiotherapie aan als eerste stap in de therapie van FNS met motorische symptomen.
Logopedie
In onze literatuurstudie werden geen studies naar de effecten van logopedie geïncludeerd. Een case serie (Goldstein, 2023) en case reports in een scoping review (Barnett, 2018) laten zien dat logopedie een zinvolle interventie kan zijn bij spraak- en slikproblemen bij FNS. Er is dus zeer beperkt onderzoek verricht naar logopedie voor FNS. De principes van de behandeling (Baker, 2021) zijn echter overeenkomstig met die van fysiotherapie voor FNS. Daarnaast is logopedie bij andere neurologische aandoeningen met spraak- en taalstoornissen de belangrijkste interventie.
Internationale experts onderschrijven dat logopedie een sleutelrol heeft in de behandeling van patiënten met functionele spraak- en taalstoornissen (Baker, 2021), en ook in Nederland zijn er positieve klinische ervaringen met de behandeling van FNS met logopedie. Daarom adviseert de werkgroep om logopedie te overwegen voor FNS met spraak-, taal- en slikstoornissen.
Klachtgerichte behandeling: psychologische behandeling
Bij het literatuuronderzoek naar psychologische behandeling voor FNS werden onderzoeken naar CGT (Aamir, 2012; Goldstein, 2010; 2020; 2022; Khattak, 2006), psychologische behandeling gebaseerd op CGT (LaFrance, 2014), kortdurende psychodynamische interpersoonlijke therapie (Hubschmid, 2015) en hypnose en katalepsie-inductie (Moene, 2003) geïncludeerd.
(Cognitieve) gedragstherapie:
CGT grijpt aan op diverse mechanismen die verondersteld worden een rol te spelen bij functionele aanvallen, waaronder aandachtsprocessen, emotieregulatie en interoceptie (Ertan, 2020). CGT blijkt in vergelijking met standaardzorg te kunnen leiden tot een afname van lichamelijke klachten, waaronder functionele aanvallen, angst en depressieve klachten, en tot verbetering van sociaal functioneren en patiënttevredenheid (Aamir, 2012; Goldstein 2010; 2020; 2022; Khattak, 2006). Psychologische behandeling gebaseerd op CGT (LaFrance, 2014) laat eveneens een grotere afname van lichamelijke klachten zien, hoewel het effect op sociaal functioneren beperkt is. Er is in Nederland positieve ervaring met de behandeling van aanvalsgewijze functionele neurologische symptomen met CGT. Op basis van deze resultaten en de positieve klinische ervaring beveelt de werkgroep CGT aan voor patiënten met FNS met aanvallen.
Kortdurende psychodynamische interpersoonlijke therapie:
In een onderzoek naar de effecten van kortdurende psychodynamische interpersoonlijke therapie in combinatie met gezamenlijke consultatie door neuroloog en psychiater namen lichamelijke en psychische klachten af bij patiënten met motorische symptomen of aanvallen (Hubschmid, 2015). Het effect op kwaliteit van leven was beperkt. Hoewel de resultaten van dit onderzoek veelbelovend zijn, wordt deze zorg in Nederland nog niet geboden, vermoedelijk vanwege financiële en praktische barrières. Om deze reden heeft de werkgroep deze niet opgenomen in de aanbevelingen.
Hypnose en katalepsie-inductie:
Onderzoek naar behandeling met hypnose en katalepsie-inductie suggereert dat deze behandeling leidt tot een grotere afname van motorische symptomen in vergelijking tot een wachtlijst bij mensen met FNS (Moene, 2003). Deze bevindingen worden ondersteund door een review van Connors en collega’s (2024) en een recente pilotstudie waarin behandeling met hypnose en katalepsie vergeleken werd met een within-subject wachtlijst controlegroep bevestigd deze bevinding (Tibben 2024). Hypnose en katalepsie-inductie worden in Nederland toegepast door verschillende zorgverleners in het kader van de behandeling van FNS, waaronder psychologen, psychiaters, psychomotorisch therapeuten, fysio- en oefentherapeuten. De werkgroep adviseert deze interventies in te zetten als onderdeel van een bredere behandeling, met bijvoorbeeld CGT of fysiotherapie, vanwege de beperkte evidentie voor behandeling met enkel hypnose, al dan niet in combinatie met katalepsie-inductie.
Andere vormen van psychotherapie:
Er is onderzoek gaande naar de veiligheid, haalbaarheid en effectiviteit van andere vormen van psychologische behandeling. Een recente pilotstudie van Cope (2025) laat zien dat EMDR voor FNS niet alleen veilig en haalbaar is, maar suggereert ook dat dit kan leiden tot afname van diverse functionele neurologische symptomen en psychische klachten. Er zijn tevens pilotstudies verricht naar de effecten van CGT, acceptance and commitment therapy (ACT), cognitieve revalidatie en online zelfhulp gericht op FNS met primair functionele cognitieve klachten, ook wel functionele cognitieve stoornis genoemd. Online groeps-ACT is veilig en haalbaar, en laat een matig effect zien op tevredenheid met het geheugen en psychische klachten (Poole, 2025). Rioux en collega’s (2024) vergeleken in een pilotstudie de effecten van CGT met cognitieve revalidatie (i.e. compensatiestrategieën voor geheugenproblemen) op functionele cognitieve klachten na een hersenschudding. Zowel CGT als cognitieve revalidatie waren aanvaardbaar en haalbaar, en lieten positieve effecten op subjectief cognitief functioneren zien. Een pilotstudie naar de zelfhulp-app Mementum (Cabreira, 2025) toonde aan dat gebruik van de app haalbaar en aanvaardbaar was voor patiënten, en suggereert dat dit kan bijdragen aan afname van de functionele cognitieve klachten en verbetering van ziekteperceptie, depressieve symptomen en kwaliteit van leven. Deze app bevat, naast educatie over functionele cognitieve stoornissen, strategieën uit de CGT, mindfulness en cognitieve revalidatie.
Hoewel uit bovenstaande pilotstudies duidelijk wordt dat EMDR voor FNS, en CGT, ACT en cognitieve revalidatie voor functionele cognitieve stoornissen veilig, aanvaardbaar en haalbaar zijn, is er gerandomiseerd, gecontroleerd onderzoek in een groter aantal onderzoeksdeelnemers nodig om de effecten van deze psychologische behandelingen vast te stellen. Bijwerkingen van psychologische behandeling lijken beperkt: in het onderzoek van Goldstein (2020) werden geen klinisch significante verschillen in complicaties gevonden tussen behandel- en controlegroep, en de opgetreden complicaties werden door onafhankelijke beoordelaars niet toegeschreven aan CGT. Algemene risico’s van psychologische behandeling, zoals tijdelijke toename van klachten of afhankelijkheid van de therapeut, blijven wel relevant (Berk, 2009).
Behandeling gericht op beïnvloedende factoren
Behandeling volgens het biopsychosociaal model is de norm binnen de gehele geneeskunde, en dus voor alle aandoeningen relevant. Gezien de veronderstelde multifactoriële etiologie van FNS (Hallett, 2022) wordt het belang hiervan bij de indicatiestelling en behandeling van FNS benadrukt door internationale experts (Aybek, 2022; Perez, 2021; Gasparini, 2019; Goldstein, 2024). Hoewel de neuroloog ook volgens het biopsychosociale model werkt, en dus aandacht zal hebben voor evidente beïnvloedende factoren zoals somatische of psychiatrische comorbiditeit, is deze in de dagelijkse praktijk beperkt in tijd. Uitgebreidere beschrijvende diagnostiek naar beïnvloedende factoren conform het biopsychosociaal model wordt derhalve vaak pas gedaan als de patiënt naar de ggz of een revalidatiesetting is verwezen.
De werkgroep adviseert verwijzing naar de ggz of revalidatiesetting voor uitgebreider beschrijvende diagnostiek volgens het biopsychosociale model wanneer klachtgerichte interventies onvoldoende effect hebben, of wanneer er bij de indicatiestelling al een vermoeden is op belangrijke beïnvloedende factoren of interfererende psychiatrische comorbiditeit. Bij beschrijvende diagnostiek wordt samen met de patiënt op gestructureerde wijze onderzoek gedaan naar de kwetsbaarheids-, uitlokkende en beïnvloedende factoren op biologisch, psychologisch en sociaal gebied die (hypothetisch) van invloed kunnen zijn op de klachten. Voor uitgebreidere uitleg over beschrijvende diagnostiek verwijzen wij naar submodule Geestelijke gezondheidszorg. Beïnvloedende factoren die mogelijk relevant zijn voor FNS worden beschreven in het overzichtsartikel van Hallett en collega’s (2022). Beschrijvende diagnostiek maakt inzichtelijk welke factoren de klachten of het functioneren beïnvloeden of het risico op een terugval vergroten, en daarmee ook waar de behandeling zich op kan richten; zie hiervoor ook de submodule Medisch specialistische zorg. Note bene, multidisciplinaire zorg voor FNS patiënten kan vaak ook in de eerste lijn georganiseerd worden, bijvoorbeeld door verwijzing naar psycholoog, fysiotherapeut en/of ergotherapeut.
Hoewel er bij patiënten met FNS is geen wetenschappelijk onderzoek verricht naar psychologische en paramedische behandeling gericht op biopsychosociale beïnvloedende factoren, wordt dit in Nederland veelvuldig toegepast. Hierbij is de ervaring dat behandeling van somatische of psychiatrische comorbiditeit, verschillende vormen van psychotherapie, vaktherapie, (psychosomatische) fysiotherapie, ergotherapie en ondersteuning vanuit het sociaal domein allen kunnen bijdragen aan een afname van functionele neurologische symptomen, andere lichamelijke klachten, verbetering van psychisch welzijn en kwaliteit van leven.
Tenslotte dient opgemerkt te worden dat een patiënt met FNS in principe altijd voor een klachtgerichte behandeling wordt verwezen. Wanneer de klachtgerichte interventies onvoldoende effect hebben of er is bij de indicatiestelling al een vermoeden van belangrijke factoren die de behandeling of het herstel negatief kunnen beïnvloeden, zoals comorbiditeit, dient behandeling gericht op deze factoren overwogen te worden. Hierbij heeft het de voorkeur om deze behandelingen parallel aan elkaar te bieden, idealiter in een multidisciplinaire behandelsetting. Indien dit echter niet haalbaar is vanwege praktische barrières of beperkte belastbaarheid van de patiënt, kan in overleg met de patiënt gezamenlijk gekozen worden om klachtgerichte behandeling of behandeling gericht op beïnvloedende factoren te prioriteren.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
De werkgroep adviseert om middels gezamenlijke besluitvorming met de patiënt tot een passende keuze voor behandeling te komen. Wanneer behandeling op beïnvloedende factoren wordt geadviseerd, moet de patiënt worden betrokken bij de vertaalslag naar behandeladviezen en helder worden uitgelegd welke behandelmogelijkheden er zijn. Uitleg dient altijd afgestemd te worden op het begripsniveau van de patiënt. De diagnose FNS gaat nog in veel gevallen gepaard met stigma. Zorgverleners hebben een belangrijke rol in het tegengaan van dit stigma. Allereerst hebben patiënten behoefte aan een duidelijke diagnose en uitleg over de geadviseerde behandeling. De bereidheid om paramedische of psychologische therapie te ondergaan, en de effectiviteit ervan, is groter als de neuroloog heeft uitgelegd waarom die therapieën zinvol zijn.
In het proces van gezamenlijke besluitvorming dienen ook andere relevante factoren meegewogen te worden, zoals beschikbaarheid van het zorgaanbod in de regio, effecten van eventuele eerdere behandeling, de eventuele aanwezigheid van comorbiditeit, prioritering in relatie tot de gestelde behandeldoelen, en haalbaarheid met het oog op belasting en belastbaarheid.
Kosten (middelenbeslag)
Onderzoek toont aan dat educatie over FNS kan leiden tot een afname van zorgkosten (Lagrand, 2023). Ook is aangetoond dat het uitblijven van diagnose en behandeling bijdraagt aan hogere zorg- en maatschappelijke kosten (Watson, 2023). Een economische analyse van bovengenoemde gerandomiseerde studie van Nielsen (2024) naar de behandeling van FNS met fysiotherapie, laat zien dat FNS geassocieerd is met hoge zorgkosten en hoge kosten voor de maatschappij en dat er een hoge waarschijnlijkheid is dat fysiotherapie een kosteneffectieve interventie is (Hunter, 2025).
Voor overige paramedische en psychologische interventies zijn geen kosteneffectiviteitsstudies gedaan.
Aanvaardbaarheid, haalbaarheid en implementatie
Er is geen kwantitatief of kwalitatief onderzoek naar de aanvaardbaarheid en haalbaarheid van paramedische en psychologische behandeling van patiënten met FNS verricht in Nederland.
Onderzoeken uit onze literatuurstudie die verricht zijn in het Verenigd Koninkrijk laten zien dat fysiotherapie voor FNS van het motorische subtype veilig, haalbaar en aanvaardbaar is (Nielsen, 2017) en dat patiënten met functionele aanvallen tevreden waren over behandeling met CGT (Goldstein 2020; 2022). Pilotstudies naar de effecten van EMDR voor FNS en ACT, CGT, cognitieve revalidatie en de zelfhulp-app Mementum toonden eveneens aan dat deze behandelingen aanvaardbaar en haalbaar zijn voor mensen met FNS (Cabreira, 2025; Cope, 2025; Poole 2025; Rioux, 2024). Implementatie van de zelfhulp-app is nog niet mogelijk omdat hier nog geen Nederlandse versie van beschikbaar is.
Kwalitatief onderzoek naar (niet-gespecialiseerde) psychologische behandeling in het Verenigd Koninkrijk (Staton, 2024) laat zien dat patiënten vaak een gebrek aan samenhang ervaren tussen verschillende zorgverleners, maar ook tussen de behandeldoelen en de geboden interventie. Ook hadden zij soms het gevoel dat hun psycholoog onvoldoende kennis had over FNS of hun klachten niet geloofde, wat een negatieve invloed had op het vertrouwen en de therapietrouw.
Op basis van bovenstaande studies kan dus verondersteld worden dat patiënten tevreden zijn over psychologische behandeling mits deze geboden wordt door een ggz zorgverlener die kennis van en ervaring met de behandeling van FNS heeft.
Dit is in lijn met de oplossingen die experts adviseren voor de gevonden problemen: betere scholing van zorgverleners over FNS en betere integratie tussen de betrokken disciplines (Staton, 2024). De klinische praktijk leert dat deze adviezen ook relevant zijn voor de Nederlandse situatie. Het onderwijs over FNS in de opleidingen voor de betrokken zorgverleners, zoals artsen, fysiotherapeuten en andere paramedici en psychologen, is beperkt, waardoor niet iedere zorgverlener voldoende kennis heeft om deze patiënten passende educatie en behandeling te bieden. Ook wordt in Nederland, net zoals in het Verenigd Koninkrijk, de samenwerking tussen de verschillende disciplines die betrokken zijn bij de diagnostiek en behandeling van mensen met FNS bemoeilijkt doordat verschillen in visie op de aandoening en terminologie, en beperkte kennis van de werkwijze van andere zorgverleners. Voor adviezen om dit te verbeteren verwijzen wij naar de module Samenwerking.
Klinische ervaring leert dat samenwerking en integratie van zorg het beste vormgegeven kan worden in een multidisciplinaire behandeling binnen één zorgsetting. In sommige Nederlandse ggz en revalidatie-instellingen wordt multidisciplinaire klinische of ambulante tweedelijnszorg geboden (zie module Multidisciplinaire behandeling).
De toegang tot psychologische en paramedische behandelingen voor FNS is suboptimaal. Omdat scholing over behandeling van FNS niet of nauwelijks aan bod komt in de opleiding van de betrokken zorgverleners, is het aantal behandelaren met kennis over de aandoening beperkter dan voor andere aandoeningen. De afgelopen jaren zijn er in toenemende mate geschoolde fysio- en oefentherapeuten die patiënten met functionele motorische symptomen kunnen behandelen. Er zijn nog weinig logopedisten geschoold op het gebied van FNS. Expertise van FNS bij zorgverleners werkzaam binnen de ggz is beperkter dan voor andere aandoeningen.
Een belangrijke belemmering voor de toegankelijkheid van fysiotherapie is de vergoeding; fysiotherapie voor FNS wordt niet vergoed vanuit de basisverzekering. In de ggz belemmeren de wachtlijsten snelle toegang tot behandeling.
Onderzoek laat zien dat de haalbaarheid en aanvaardbaarheid van gespecialiseerde, geprotocolleerde psychologische behandelingen voor FNS, zoals CGT voor functionele aanvallen, goed is (Goldstein 2020; 2022). Desalniettemin benadrukken experts dat de (psychologische) behandeling van FNS maatwerk is (Goldstein, 2024), gezien de diversiteit in presentatie, comorbiditeit, levensloop en behandelwensen en -doelen. Zij adviseren dan ook behandeling op maat (“matched care”) voor patiënten met FNS. Dit sluit aan bij het advies van onze werkgroep om op indicatie uitgebreide beschrijvende diagnostiek te verrichten, om in kaart te brengen welke biologische, psychologische en sociale factoren aandacht behoeven in de behandeling van de individuele patiënt met FNS die onvoldoende profiteert van klachtgerichte behandeling, of bij wie er sterke aanwijzingen zijn voor relevante beïnvloedende factoren.
Psychologische en paramedische behandeling van FNS zou ook toegankelijk aangeboden moeten worden aan mensen die de Nederlandse taal onvoldoende beheersen en mensen met een lager niveau van algemeen functioneren, zoals mensen met een licht verstandelijke beperking of ernstige fysieke beperkingen. In de praktijk zien wij echter dat deze doelgroepen niet altijd zorg geboden krijgen door praktische bezwaren: het aanpassen van de interventies aan intellectuele beperkingen of taal vraagt extra tijd en inspanning die in de klinische praktijk vaak niet geïnvesteerd wordt.
Ook zijn er in Nederland vrijwel geen klinische behandelmogelijkheden voor mensen met FNS die door ernstige fysieke beperkingen veel zorg of ADL-ondersteuning nodig hebben.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
De eerste stap in iedere behandeling is educatie over FNS. Goede uitleg door de neuroloog verbetert begrip, tevredenheid en behandeluitkomst. In de informatiefolder van de Nederlandse Vereniging voor Neurologie staan - naast uitleg over FNS en behandeling - links naar uitgebreidere online informatie.
In principe wordt er gestart met klachtgerichte behandeling, waarbij de aard van de symptomen richtinggevend is. Onderzoek naar het effect van fysiotherapie op functionele motorische symptomen laat verbetering zien van de symptomen zelf, fysiek functioneren en kwaliteit van leven; dit is met hoge mate van waarschijnlijkheid kosteneffectief. (Inter)nationale experts bevelen gespecialiseerde fysiotherapie aan en in Nederland zijn er positieve ervaringen met fysiotherapie voor FNS. Er zijn steeds meer fysiotherapeuten met expertise op dit gebied, waardoor er over het algemeen geen lange wachttijden zijn. De werkgroep beveelt fysiotherapie dan ook aan als eerste stap in de behandeling van functionele motorische symptomen.
Hoewel er zeer beperkt onderzoek is verricht naar logopedie voor FNS, zijn de principes van de behandeling overeenkomstig met die van fysiotherapie voor FNS - een behandeling waar meer onderzoek naar is verricht. Logopedie is bij andere neurologische aandoeningen met spraak- en taalstoornissen de belangrijkste interventie. Ook in Nederland is er positieve klinische ervaring met logopedische behandeling van FNS. Daarom adviseert de werkgroep behandeling met logopedie voor aan voor spraak-, taal- en slikstoornissen bij FNS. CGT kan leiden tot een afname van lichamelijke klachten, angst- en depressieve klachten, en verbetering van het sociaal functioneren en patiënten zijn tevreden zijn met deze behandeling. Dit komt overeen met de klinische ervaring met CGT in Nederland. Derhalve beveelt de werkgroep behandeling met CGT aan als behandeling van eerste keuze voor patiënten met FNS met aanvallen.
Voor de functionele cognitieve stoornis zijn alleen nog maar resultaten van pilotstudies beschreven zijn. Deze laten zien dat ACT, CGT, cognitieve revalidatie of de zelfhulp-app Mementum veilig, aanvaardbaar en haalbaar zijn. Er is echter gerandomiseerd, gecontroleerd onderzoek in grotere patiëntengroepen nodig om de effectiviteit van deze interventies voldoende aan te tonen. In de klinische praktijk vragen patiënten met functionele cognitieve stoornissen echter wel om behandeladvies, zeker omdat bij uitleg van de diagnose benoemd wordt dat de klachten potentieel reversibel zijn. Onder internationale experts is er consensus dat ACT en CGT aan te bevelen zijn voor deze klachten (Cabreira, 2025). De werkgroep heeft ervoor gekozen deze als “off-label” behandeling in de aanbevelingen op te nemen. De term “off-label” verwijst naar het gegeven dat de effectiviteit nog verder onderzocht dient te worden, maar dat onderzoek wel heeft aangetoond dat CGT en ACT veilig en haalbaar, en potentieel effectief, zijn voor mensen met een functionele cognitieve stoornis.
Hypnose (eventueel in combinatie met katalepsie-inductie) kan eveneens positieve effecten hebben op functionele neurologische symptomen, waarbij de effecten op motorische symptomen het best onderzocht zijn. In Nederland worden deze behandelvormen veel ingezet door verschillende zorgverleners binnen het kader van een andere behandeling zoals fysiotherapie, psychotherapie of psychomotorische therapie. De werkgroep adviseert om hypnose, eventueel in combinatie met katalepsie-inductie, te overwegen als interventie(s) binnen een bredere klachtgerichte behandeling van FNS met bijvoorbeeld fysiotherapie of CGT.
Ondanks de beperkte wetenschappelijke evidentie van EMDR voor FNS, is er in de klinische praktijk een duidelijke behoefte aan behandelopties voor patiënten die ondanks behandeling klachten houden. Omdat haalbaarheidsonderzoek laat zien dat EMDR mogelijk een positief effect op functionele neurologische klachten kan hebben en bovendien aanvaardbaar en veilig is, heeft de werkgroep ook deze behandeling als “off-label” optie in de aanbevelingen opgenomen.
Gezamenlijke neurologische en psychiatrische consultatie in combinatie met kortdurende psychodynamische interpersoonlijke therapie kan positieve effecten hebben op diverse functionele neurologische symptomen. In de praktijk zal dit echter lastiger te implementeren zijn; gecombineerde neurologische en psychiatrische consultatie én interpersoonlijke psychodynamische psychotherapie worden in Nederland momenteel zelden binnen dezelfde zorgsetting geboden. Om deze reden heeft de werkgroep ervoor gekozen deze vorm van zorg niet op te nemen in de aanbevelingen. Indien wel beschikbaar, kan deze interventie echter overwogen worden voor mensen met diverse functionele neurologische symptomen.
Wanneer er bij de indicatiestelling al een vermoeden is op belangrijke beïnvloedende factoren of interfererende psychiatrische comorbiditeit, of als klachtgerichte interventies onvoldoende effect hebben, moet verwijzing naar de ggz of revalidatiesetting overwogen worden voor uitgebreider beschrijvende diagnostiek volgens het biopsychosociale model, eventueel gevolgd door (multidisciplinaire) behandeling gericht op beïnvloedende factoren.
Onderbouwing
Functional neurological disorder (FND) is a common and often disabling condition. Without appropriate treatment, long–term outcomes are generally poor, with persistently reduced quality of life and ongoing symptom burden. Effective treatment is therefore essential. FND is understood as a disorder involving abnormalities within and between brain networks, influenced by biological, psychological and social factors. This multifactorial conceptualization underpins the use of several therapeutic approaches - including psychological treatment, physiotherapy and other paramedical interventions - that aim to restore movement and sensory functions, reduce symptom-related distress, and improve daily functioning. Although the evidence base is still developing, an increasing number of trials and systematic reviews have evaluated the effectiveness of these interventions. The available evidence, together with international expert consensus and clinical experience, is summarized in this module.
PICO 1 – Paramedical treatment for FND
1. Physical complaints
|
Very low GRADE |
Paramedical treatment may improve physical complaints when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Nielsen, 2017; Nielsen, 2024. |
2. Functioning
|
Very low GRADE |
Paramedical treatment may improve functioning when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Jordbru, 2014; Nielsen, 2017, Nielsen, 2024. |
3. Psychological complaints
3.1 Anxiety
|
Very low GRADE |
Paramedical treatment may worsen anxiety when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Nielsen, 2017; Nielsen, 2024. |
3.2 Depressive symptoms
|
Very low GRADE |
Paramedical treatment may improve depressive symptoms when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Nielsen, 2017; Nielsen, 2024. |
4. Fatigue
|
Very low GRADE |
Paramedical treatment may result in little to no difference when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Nielsen, 2024. |
5. Pain
|
Very low GRADE |
Paramedical treatment may worsen pain when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Nielsen, 2024. |
6. Quality of life
|
Very low GRADE |
Paramedical treatment may improve quality of life on the physical domain when compared with treatment as usual but the evidence is very uncertain.
Source: Jordbru, 2014 |
7. Patient satisfaction
|
No GRADE |
No evidence was found regarding the effect of paramedical treatment on patient satisfaction when compared with waitlist or treatment as usual in patients with a functional neurological disorder.
Source: -. |
8. Complications
|
Low GRADE |
Paramedical treatment may result in little to no difference in complications when compared with waitlist or treatment as usual in patients with a functional neurological disorder.
Source: Nielsen, 2024. |
PICO 2 – Psychological treatment for FND
1. Physical complaints
|
Very low GRADE |
Psychological treatment may improve physical complaints when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Aamir, 2012; Goldstein, 2010; Goldstein, 2020, 2022; Hubschmid, 2015; Khattak, 2006; LaFrance, 2014; Moene, 2003. |
2. Functioning
|
Low GRADE |
Psychological treatment may result in little to no difference in functioning when compared with waitlist or treatment as usual in patients with a functional neurological disorder.
Source: Goldstein, 2010; Goldstein, 2020, 2022; LaFrance, 2014. |
3. Psychological complaints
3.1 Anxiety
|
Very low GRADE |
Psychological treatment may improve anxiety when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Aamir, 2012; Goldstein, 2010; Goldstein, 2020, 2022; Khattak, 2006; LaFrance, 2014. |
3.1 Depressive symptoms
|
Very low GRADE |
Psychological treatment may improve depressive symptoms when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Aamir, 2012; Goldstein, 2010; Goldstein, 2020, 2022; Hubschmid, 2015; Khattak, 2006; LaFrance, 2014. |
4. Fatigue
|
no GRADE |
No evidence was found regarding the effect of psychological treatment on fatigue when compared with waitlist or treatment as usual in patients with a functional neurological disorder.
Source: - |
5. Pain
|
no GRADE |
No evidence was found regarding the effect of psychological treatment on pain when compared with waitlist or treatment as usual in patients with a functional neurological disorder.
Source: - |
6. Quality of life
|
Very low GRADE |
Psychological treatment may improve quality of life when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Goldstein, 2020, 2022; Hubschmid, 2015; LaFrance, 2014. |
7. Patient satisfaction
|
Low GRADE |
Psychological treatment may improve patient satisfaction when compared with waitlist or treatment as usual in patients with a functional neurological disorder.
Source: Goldstein 2020, 2022. |
8. Complications
|
Very low GRADE |
Psychological treatment may result in little to no difference in complications when compared with waitlist or treatment as usual in patients with a functional neurological disorder but the evidence is very uncertain.
Source: Goldstein 2020. |
Summary of literature
A total of four studies was included in the analysis of the literature, of which two (Goldstein, 2020; Goldstein, 2022) describe the results of the same RCT. The assessment of the risk of bias is summarized in the risk of bias tables (under ‘Evidence tabellen’).
Description of studies
Ganslev (2020) performed a systematic review and meta-analysis to assess the beneficial and harmful effects of psychosocial interventions for adults with conversion and dissociative disorders, i.e. FND. The international databases CENTRAL, Medline, CINAHL, Embase, PsycINFO, and Web of Science were searched until 16 July 2019, and the electronic database ERIC until 16 August 2019. Additionally, reference checking, citation searching, and contact with study authors were used to identify additional studies. RCTs that compared psychosocial interventions for FND with standard care, wait list or other interventions (pharmaceutical, somatic or psychosocial) were included. Quality assessment of the included studies was performed by using the criteria sent out in the Cochrane Handbook for Systematic Reviews of Interventions. The review included 17 RCTs with a total of 894 participants. Eventually, nine studies were included in the current literature analysis, because five studies did not have a control group receiving usual care or waitlist treatment (Ataoglu, 2003; Dallochio, 2016; Moene, 2002; Mousavi, 2008; Pleizier, 2017). Characteristics of the included studies can be found in table 1.
Nielsen (2024) performed a RCT -the Physio4FMD trial- to assess the clinical effectiveness of a specialist physiotherapy intervention for functional motor disorder, i.e. the motor subtype of FND, compared with treatment as usual. Adults (≥18 years) attending outpatient neurology clinics and inpatients who had a diagnosis of functional motor disorder were considered eligible. Consultant neurologists – collaborating in the trial – made the clinically definite diagnosis of functional motor disorder, according to the Gupta and Lang diagnostic criteria. Additional inclusion criteria were: 1) diagnostic investigations had been completed, 2) the individual was accepting of receiving the trial interventions, and 3) motor symptoms were causing substantial distress or impairment in social, occupational, or other important areas of functioning, independent of other comorbidities. Individuals with severe psychiatric comorbidity, with another diagnosis that could account for the majority of the symptoms or disability, with pain, fatigue or dissociative seizures or who had disability to the extent that they require assistance for toileting were excluded. Symptoms such as pain, fatigue, dissociative seizures, anxiety, or depressive symptoms were only considered exclusion criteria if they were judged to be severe enough to hinder the patients' ability to participate in the physiotherapy intervention. A total of 247 participants were included, who were randomly assigned to either the specialist physiotherapy group (n=141) or the treatment as usual group (n=106). Additional study characteristics are shown in table 2.
Goldstein (2020) conducted a RCT - the CODES trial - to compare the effectiveness of cognitive behavioral therapy (CBT) plus standardized medical care with standardized medical care alone for the reduction of dissociative seizure frequency. Individuals were considered eligible when they were aged ≥18 years, had dissociative seizures in the previous 8 weeks, and had no documented history of intellectual disabilities. Diagnosis of dissociative seizures, i.e. the seizure subtype of FND, was preferably confirmed by video-electroencephalogram (VEEG) or clinical consensus. Patients with comorbid epilepsy could only participate if they had been free of epileptic seizures for 12 months, and patients who met DSM-IV criteria for current drug or alcohol dependence were excluded. In total, 368 participants were included, who were randomized to either the CBT plus standardized medical care group (n=186) or the standardized medical care alone group (n=182). Additional study characteristics are displayed in table 2.
Goldstein (2022) performed a secondary analysis of the CODES trial to evaluate the effectiveness of CBT plus standardized medical care compared to standardized medical care alone at six months post-randomization. Additional characteristics are shown in table 2.
Table 1: Characteristics of the studies included in Ganslev (2020)
|
Author, year |
Diagnosis |
Intervention |
Control |
Duration of the study |
Risk of bias |
||
|
Characteristics |
Type |
Characteristics |
Type |
||||
|
Ganslev, 2020 |
|||||||
|
Aamir, 2012 RCT |
Conversion disorder (having pseudo seizures only) as per ICD-10 criteria. |
n=9 Mean age (SD): 22.2 (2.7) years* Sex (% female): 83.3%* |
Behavioral therapy, 15 sessions + training of carers for 1 week 9 weeks |
n=9 Mean age (SD): 22.2 (2.7) years* Sex (% female): 83.3%* |
Routine treatment (pharmacotherapy) and observation by the psychiatrist |
9 weeks |
Some concernsa |
|
Goldstein, 2010 RCT |
Psychogenic non-epileptic seizures primarily confirmed by VEEG telemetry. |
n=33 Mean age (SD): 37.4 (12.6) years Sex (% female): 72.7% Duration of symptoms (mean): 5.9 years |
CBT plus standardized medical care Up to 12 weekly/every 2 weeks for 1-hour outpatient sessions of CBT with a CBT- trained nurse therapist with experience in working with people with PNES. 4 months |
n=31 Mean age (SD): 35.9 (15.1) years Sex (% female): 83.9% Duration of symptoms (mean): 6.8 years |
Standardized medical care |
June 2001 to April 2007 |
Highb |
|
Hubschmid, 2015 RCT |
Conversion disorder according to DSM-IV-TR criteria with motor symptom or NEA, as assessed by experienced neurologists. |
n=11 Mean age (SD): 37.6 (4.0) years Sex (% female): 60% |
Joint neurological and psychiatric consultation followed by brief psychotherapeutic intervention Therapy was based on a psychodynamic interpersonal treatment approach 4-6 sessions for 2 months |
n=12 Mean age (SD): 31.5 (3.2) years Sex (% female): 90.9% |
Standard care |
November 2010 to January 2013 |
Highc |
|
Jordbru, 2014 RCT |
Disabling walking disturbance resembling psychogenic gait with no organic explanation after neurological examination. |
n=31 Mean age (SD): 38.8 (12.2) years Sex (% female): 81% Duration of symptoms (mean, SD): 8.4 (10.9) months |
Inpatient rehabilitation programme. The intervention consisted of adapted physical activity with an educational and cognitive behavioral frame of reference 3 weeks |
n=29 Mean age (SD): 36.3 (9.7) years Sex (% female): 79% Duration of symptoms (mean, SD): 10.9 (13.3) months |
Wait list |
May 2007 to October 2010 |
Some concernsa |
|
Khattak, 2006 RCT |
Dissociative convulsion disorder according to ICD-10 criteria. |
n=50 Mean age (SD): 24.3 (8.8) years* Sex (% female): 88%* |
Behavior therapy sessions daily 5 weeks |
n=50 Mean age (SD): 24.3 (8.8) years* Sex (% female): 88%* |
RCC, defined as all the measures taken for controlling symptoms, which includes drug treatment, reassurance and explanation given to patients and their relatives about the illness. |
April 2004 to September 2004 |
Highb,c,e |
|
LaFrance, 2014 RCT |
Psychogenic non-epileptic seizures confirmed by VEEG and ≥ 1 event in the month prior. |
n=9 Mean age (SD): 37.9 (11.5) years Sex (% female): 77.8% |
Cognitive behavioral therapy-informed psychotherapy treatment 12 weekly, 1-hour sessions |
n=7 Mean age (SD): 41.6 (8.3) years Sex (% female): 100% |
Treatment as usual Participants followed up with their treating neurologist and were seen biweekly for assessments. |
September 2008 to February 2012 |
Highb |
|
Moene, 2003 RCT |
Conversion disorder, motor type, or a diagnosis of somatisation disorder with conversion symptoms, motor type, according to DSM-III-R criteria. |
n=24 Mean age (SD): 36.6 (11.0) years* Sex (% female): 75%* Duration of symptoms (mean): 3.7 years* |
Hypnotic treatment 10 weekly 1-hour sessions |
n=25 Mean age (SD): 36.6 (11.0) years* Sex (% female): 75%* Duration of symptoms (mean): 3.7 years* |
Wait list |
1991-1996 |
Highb,d |
|
Nielsen, 2017 RCT |
Functional motor symptoms according to Fahn-Williams criteria. |
n=30 Mean age (SD): 44.0 (13.1) years Sex (% female): 73% Duration of symptoms (mean, SD): 5.9 (8.3) years |
Specialized physiotherapy-led intervention 8 sessions over 5 consecutive days, each lasting 45-90 minutes |
n=30 Mean age (SD): 41.0 (13.1) years Sex (% female): 70% Duration of symptoms (mean, SD): 5.6 (6.2) years |
Treatment as usual |
8 September 2014 to 4 June 2015 |
Highb,c,d |
|
Thompson, 2013 RCT |
PNES established by a neurologist using history, examination and VEEG capturing ≥ 1 of their typical events. |
n=19* Mean age: 33 years* Sex (% female): 60%* |
Brief educational intervention while the participants were still in the hospital for VEEG diagnostic testing |
n=19* Mean age: 33 years* Sex (% female): 60%* |
Standard care |
6 weeks |
Highd |
|
Abbreviations: CBT = Cognitive Behavioral Therapy; DSM = Diagnostic and Statistical Manual of Mental Disorders; NEA = Nonepileptic attacks; PNES = Psychogenic non-epileptic seizures; SD = Standard deviation; VEEG = Video-Electroencephalography. *Value is reported for the total study population only a Due to missing information for multiple domains b Due to high risk of performance bias (lack of blinding) c Due to high risk of detection bias (no blind outcome assessment) d Due to high risk of attrition bias (incomplete outcome data) e Due to high risk of reporting bias (selective outcome reporting) |
|||||||
Table 2: Characteristics of the individual included studies.
|
Author, year |
Diagnosis |
Participants (number, age, other important characteristics) |
Comparison |
Outcome measure |
Comments |
Risk of bias* |
|
Nielsen, 2024 Physio4FMD trial England, Scotland
|
Functional motor disorder confirmed by a consultant neurologist according to Gupta and Lang diagnostic classification criteria. |
N at baseline Intervention: 141 Control: 106
Age (mean, SD) Intervention: 45.0 (14.3) years Control: 44.4 (14.9) years
Sex (%female) Intervention: 74 Control: 75
Symptom duration (mean, SD) Intervention: 5.2 (7.2) years Control: 4.4 (4.9) years |
Intervention: Specialist physiotherapy
Control: Treatment as usual
|
Physical complaints (SF-36) Social functioning (SF-36) Psychological complaints, anxiety and depressive symptoms (HADS) Fatigue Pain (SF-36) Patient satisfaction (CGI-I) Complications |
The study was funded by the National Institute for Health and Care Research and Health Technology Assessment Programme. The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Potential conflicts of interest are reported. |
Some concerns |
|
Goldstein, 2020 Goldstein, 2022 CODES trial England, Scotland, Wales
|
Dissociative seizures as confirmed by VEEG or, if not available, clinical consensus provided by two consultants involved in the patient’s care or by expert review of the clinical records and relevant investigations by one of two neurologists in the research team. |
N at baseline Intervention: 186 Control: 182
Age (mean, SD) Intervention: 37.3 (14.2) years Control: 37.7 (14.5) years
Sex (%female) Intervention: 75 Control: 69
Duration of dissociative seizure symptoms (mean, SD) Intervention: 5.9 (7.8) years Control: 6.5 (9.7) years |
Intervention: Cognitive behavioral therapy plus standardized medical care
Control: Standardized medical care
|
Physical functioning (SF-12v2) Psychosocial functioning (WSAS) Psychological complaints, anxiety (GAD-7) and depressive symptoms (PHQ-9) Quality of life (EQ-5D-5L) Patient satisfaction Complications
|
The study was funded by the National Institute for Health Research, Health Technology Assessment programme. The funder had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had access to all study data and had final responsibility for the decision to submit for publication.
Potential conflicts of interest are reported. |
High |
|
Abbreviations: CGI-I = Clinical Global Impression Improvement scale; DSM = Diagnostic and Statistical Manual of mental Disorders; GAD-7 = Generalized Anxiety Disorder-7; HADS = Hospital Anxiety and Depression Scale; NR = not reported; PHQ-9 = Patient Health Questionnaire-9; SD = standard deviation; SF-12v2 = Short Form Health Survey-12 version 2; SF-36 = Short Form Health Survey-36; VEEG = Video-Electroencephalography; WSAS = Work and Social Adjustment Scale. *For further details, see risk of bias table in the appendix |
||||||
Results
PICO 1 – Paramedical treatment for FND
1. Physical complaints
One study included in Ganslev (2020) reported on the outcome measure physical complaints, defined as reduction in physical signs (Nielsen, 2017). Additionally, Nielsen (2024) reported on the outcome measure physical complaints, assessed by the Short Form Health Survey 36 (SF-36) (higher scores on the SF indicate fewer physical complaints).
Data was converted before pooling the data. The pooled data show mean difference of -4.91 (95%CI -14.00 to 4.18) in favor of paramedical interventions (Figure 1). This difference is considered not clinically relevant.

Figure 1: The effect of paramedical interventions on physical complaints in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
Nielsen (2024) also assessed the outcome measure physical complaints, i.e. functional neurological symptoms, by the clinical global impression of improvement (CGI-I) scale. The authors reported on the number of participants who rated their symptoms as ‘’much improved’’, twelve months post randomization. In total 26% (36/138) of participants in the specialist physiotherapy group rated their symptoms as ‘’much improved’’ compared to 14% (14/102) of participants in the treatment as usual group. Risk ratio is 1.90 (95%CI 1.08 to 3.33) in favor of specialist physiotherapy. This difference is considered clinically relevant.
2. Functioning
Two studies included in Ganslev (2020) reported on the outcome measure functioning (Jordbru, 2014; Nielsen, 2017). In addition, Nielsen (2024) reported on functioning. Nielsen (2024) defined the outcome measure as social functioning, assessed by the SF-36.
Data of Nielsen (2024) and Jordbru (2014) was converted before pooling the data. The pooled data show a SMD of -0.63 (95%CI -1.36 to 0.11) in favor of paramedical interventions (Figure 2). This difference is considered clinically relevant. SMD was used because different instruments were used to assess functioning.
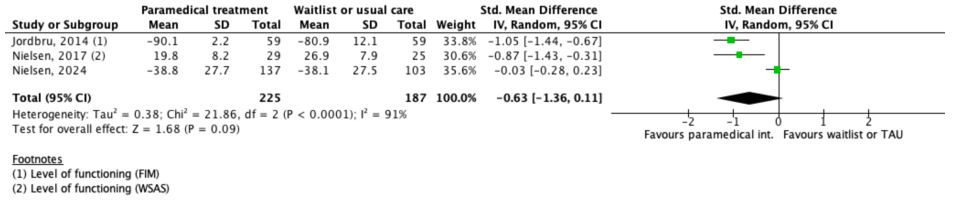
Figure 2: The effect of paramedical interventions on functioning in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
3. Psychological complaints
3.1 Anxiety
One study included in Ganslev (2020) reported on the outcome measure anxiety (Nielsen, 2017). Nielsen (2024) also reported on anxiety, assessed by the Hospital Anxiety and Depressive symptoms Scale (HADS). Higher scores indicate more severe anxiety.
The pooled data show a mean difference of 0.33 (95%CI -0.82 to 1.49) in favor of waitlist or usual care (Figure 3). This difference is considered not clinically relevant.

Figure 3: The effect of paramedical interventions on anxiety in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
3.2 Depressive symptoms
One study included in Ganslev (2020) reported on the outcome measure depressive symptoms (Nielsen, 2017). Nielsen (2024) also reported on depressive symptoms, assessed by the HADS. Higher scores indicate more severe depressive symptoms.
The pooled data show a mean difference of -1.29 (95%CI -5.04 to 2.47) in favor of paramedical interventions (Figure 4). This difference is considered not clinically relevant.

Figure 4: The effect of paramedical interventions on depressive symptoms in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
4. Fatigue
One study reported on the outcome measure fatigue (Nielsen, 2024). The outcome measure was defined as the number of participants with no, slight or moderate and severe or extreme fatigue, twelve months after randomization. The authors reported that 49% (67/136) of participants in the specialist physiotherapy group had no, slight or moderate fatigue, and 49% (48/97) of participants in the treatment as usual group. In addition, 51% (69/136) of participants in the specialist physiotherapy group reported to have severe or extreme fatigue, compared to 50% (53/106) of participants in the treatment as usual group. Risk ratio is 1.01 (95%CI 0.79 to 1.31) in favor of treatment as usual. This difference is considered not clinically relevant.
5. Pain
Nielsen (2024) reported on the outcome measure pain, assessed by the Short Form Health Survey-36 (SF-36) domain bodily pain, twelve months after randomization. SF36 subdomain scores range from 0 to 100, with a maximum score of 100 indicating optimal health. The authors reported a mean (SD) SF-36 bodily pain score of 35.4 (26.4) for the specialist physiotherapy group (n=138) and 37.1 (25.6) for the treatment as usual group (n=103). Mean difference is 1.70 (95%CI -8.32 to 4.92) in favor of treatment as usual. This difference is considered not clinically relevant.
6. Quality of life
One study included in Ganslev (2020) reported on the outcome measure quality of life (Jordbru, 2014). This was assessed by self-report using SF-12, which is a down-sized version of the Short-Form Health Survey (SF-36). It described that the model showed significant treatment effects, but the carry-over effect was significant only for SF-12 physical.
7. Patient satisfaction
None of the studies reported on the outcome measure patient satisfaction.
8. Complications
The outcome measure complications was reported by one study.
Nielsen (2024) reported on the number of participants with at least one adverse event. Adverse events were defined as any untoward medical occurrence, regardless of causal relationship with treatment. The authors reported at least one adverse event in 29% (41/141) of participants in the specialist physiotherapy group, and in 25% (26/106) of participants in the treatment as usual group. Risk ratio is 1.19 (95%CI 0.78 to 1.81) in favor of treatment as usual. This difference is considered not clinically relevant.
PICO 2 – Psychological treatment for FND
1. Physical complaints
Six studies included in Ganslev (2020) reported on the outcome measure physical complaints, defined as reduction in physical signs (Aamir, 2012; Goldstein, 2010; Hubschmid, 2015; Khattak, 2006; LaFrance, 2014; Moene, 2003). Additionally, Goldstein (2020, 2022) reported on the outcome measure physical complaints, assessed by the SF-12v2 (higher scores on the SF indicate fewer physical complaints).
Data of Goldstein (2020, 2022) and Moene (2003) was converted before pooling the data. The pooled data show a standardized mean difference (SMD) of -1.09 (95%CI -1.76 to -0.42) in favor of psychological interventions (Figure 1). This difference is considered clinically relevant. SMD was used because different instruments at different timepoints were used to assess physical complaints.
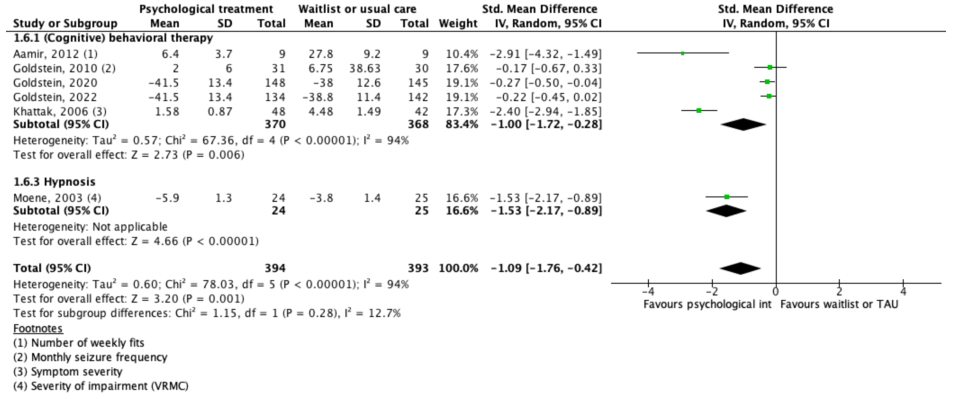
Figure 1: The effect of psychological interventions on physical complaints in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
Data of two studies could not be pooled due to the variability in reporting of the outcome measure (LaFrance, 2014; Hubschmid, 2015). LaFrance (2014) reported on the percentage of participants with seizure freedom. 33.3% (3/9) of participants in the CBT-informed psychotherapy treatment group had seizure freedom compared to 14.3% (1/7) of participants in the treatment as usual group. Risk ratio is 2.33 (95%CI 0.30 to 17.88) in favor of CBT-informed psychotherapy. This difference is considered clinically relevant.
Hubschmid (2015) reported on the percentage of participants with conversion symptoms, as assessed by the Somatoform Dissociation Questionnaire (SDQ-20). The authors reported conversion symptoms in 0% (0/9) of participants in the group that received joint neurological and psychiatric consultation followed by a psychotherapeutic intervention compared to 40% (4/10) of participants in the standard care group. Risk ratio is 0.12 (95%CI 0.01 to 2.00) in favor of the intervention. This difference is considered clinically relevant.
2. Functioning
Two studies included in Ganslev (2020) reported on the outcome measure functioning (Goldstein, 2010; LaFrance, 2014). In addition, Goldstein (2020, 2022) reported on functioning. Goldstein (2020, 2022) defined the outcome measure as psychosocial functioning, assessed by the Work and Social Adjustment Scale (WSAS).
The pooled data show a SMD of -0.35 (95%CI -0.68 to -0.01) in favor of psychological interventions (Figure 2). This difference is considered not clinically relevant. SMD was used because different instruments at different timepoints were used to assess physical complaints.
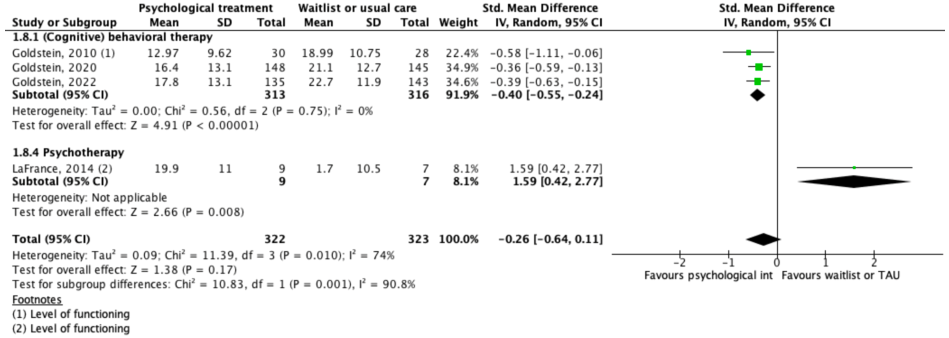
Figure 2: The effect of psychological interventions on functioning in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
3. Psychological complaints
3.1 Anxiety
Four studies included in Ganslev (2020) reported on the outcome measure anxiety (Aamir, 2012; Goldstein, 2010; Khattak, 2006; LaFrance, 2014). Goldstein (2020, 2022) also reported on anxiety, assessed by the Generalized Anxiety Disorder-7 (GAD-7), respectively. Higher scores indicate more severe anxiety.
Data of LaFrance (2014) was converted before pooling the data. The pooled data show a SMD of -0.68 (95%CI -1.13 to -0.22) in favor of psychological interventions (Figure 3). This difference is considered clinically relevant. SMD was used because different instruments at different timepoints were used to assess anxiety.
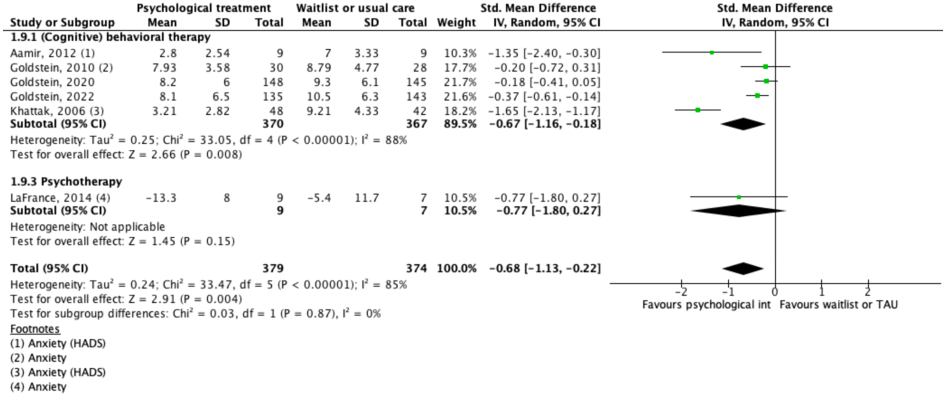
Figure 3: The effect of psychological interventions on anxiety in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
3.2 Depressive symptoms
Five studies included in Ganslev (2020) reported on the outcome measure psychological complaints (Aamir, 2012; Goldstein, 2010; Hubschmid, 2015; Khattak, 2006; LaFrance, 2014). Goldstein (2020, 2022) also reported on depressive symptoms, assessed by the Patient Health Questionnaire-9 (PHQ-9). Higher scores indicate more severe depressive symptoms.
Data of LaFrance (2014) was converted before pooling the data. The pooled data show a SMD of -0.56 (95%CI -0.97 to -0.16) in favor of psychological interventions (Figure 4). This difference is considered clinically relevant. SMD was used because different instruments at different timepoints were used to assess physical complaints.
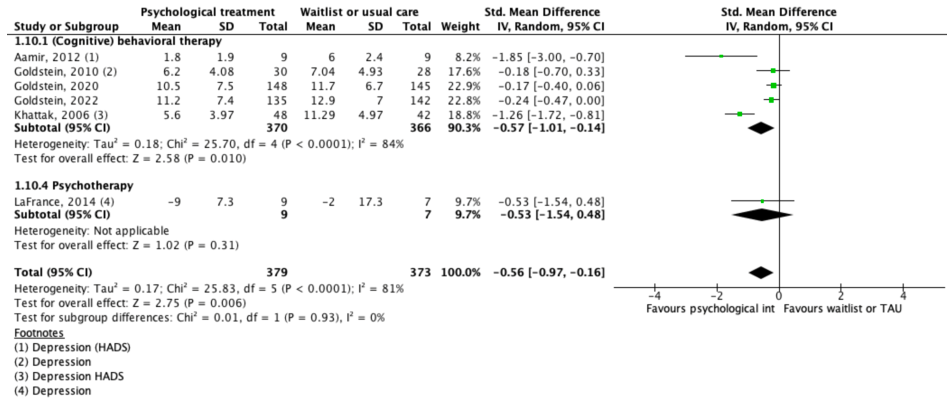
Figure 4: The effect of psychological interventions on depressive symptoms in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
Data of Hubschmid (2015) could not be pooled due to the variability in reporting of the outcome measure. The authors reported on the percentage of participants with depressive symptoms, assessed by the Beck Depressive symptoms Inventory-II (BDI-II). Higher scores on the BDI-II indicate more severe depressive symptoms. 1 out of 7 participants (14.3%) in the psychotherapeutic intervention group were reported to have a depressive symptoms, compared to 1 out of 9 participants (11.1%) in the standard care group. Risk ratio is 1.29 (95%CI 0.10 to 17.14) in favor of standard care. This difference is considered clinically relevant.
4. Fatigue
None of the studies reported on the outcome measure fatigue.
5. Pain
None of the studies reported on the outcome measure pain.
6. Quality of life
Two studies included in Ganslev (2020) reported on the outcome measure quality of life (Hubschmid, 2015; LaFrance, 2014). Additionally, Goldstein (2020, 2022) reported on the outcome measure quality of life, assessed by the EQ-5D-5L visual analogue scale (VAS). Higher scores indicate higher quality of life.
Data of Goldstein (2020, 2022) was converted before pooling the data. The pooled data show a SMD of -0.58 (95%CI -1.79 to 0.63) in favor of psychological interventions (Figure 5). This difference is considered clinically relevant. SMD was used because different instruments at different timepoints were used to assess physical complaints.
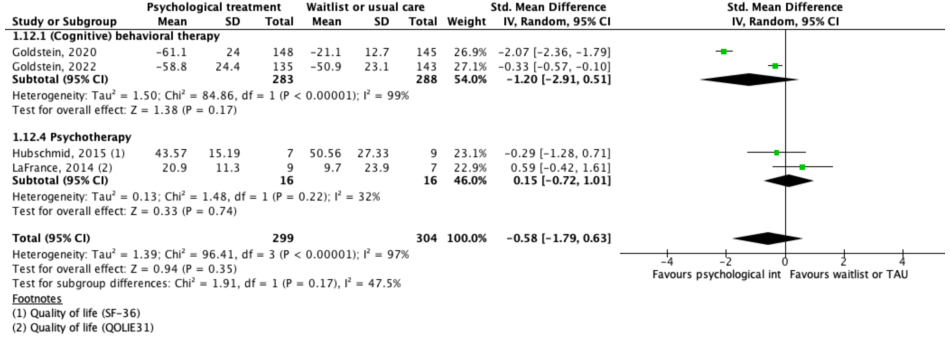
Figure 5: The effect of psychological interventions on quality of life in participants with functional neurological disorder.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
7. Patient satisfaction
One study reported on the outcome measure patient satisfaction (Goldstein 2020, 2022).
Goldstein (2020, 2022) reported a satisfaction score which was measured on a 7-point scale (0=very dissatisfied; 6=very satisfied), six and twelve months after randomization.
- At six months post randomization, the authors reported a mean (SD) satisfaction score of 5.1 (1.3) for the CBT group (n=135), and 3.8 (2.0) for the standard medical care group (n=140). Mean difference is 1.30 (95%CI 0.90 to 1.70) in favor of CBT. This difference is considered clinically relevant.
- At twelve months post randomization, a mean (SD) satisfaction score of 5.2 (1.4) for the CBT group (n=148), and 4.2 (2.0) for the standard medical care group (n=145). Mean difference is 1.00 (95%CI 0.60 to 1.40) in favor of CBT. This difference is considered clinically relevant.
8. Complications
The outcome measure complications was reported by one study (Goldstein, 2020).
Goldstein (2020) reported on the number of participants with serious adverse events. Serious adverse events were defined as any adverse event that resulted in death; was life-threatening; required hospital admission or prolongation of existing hospital stay; resulted in a new persistent or new significant disability or incapacity; was any other important medical condition that might jeopardize the participant and might require medical or surgical intervention to prevent one of the outcomes listed; or any new episode of deliberate self-harm. The authors reported serious adverse events in 13% (25/186) of participants in the CBT group, and in 13% (24/182) of participants in the standard medical care group. Psychological events (e.g., deteriorations in mood) were the most common type of adverse event in the CBT group, and musculoskeletal events (e.g., reports of injuries from dissociative seizures) were the most common type of adverse event in the standard medical care group. Risk ratio is 1.02 (95%CI 0.61 to 1.72) in favor of standard medical care. This difference is considered not clinically relevant.
Level of evidence of the literature
PICO 1 – Paramedical treatment for FND
1. Physical complaints
The level of evidence regarding the outcome measure physical complaints was downgraded by three levels to very low because of study limitations (lack of blinding, high risk of attrition bias and detection bias) (risk of bias: -2), and overlap of confidence interval with border of clinical relevance (imprecision: -1).
2. Functioning
The level of evidence regarding the outcome measure functioning was downgraded by three levels to very low because of study limitations (missing information on multiple domains, lack of blinding, high risk of attrition bias and detection bias) (risk of bias: -2), and overlap of confidence interval with border of clinical relevance (imprecision: -1).
3. Psychological complaints
3.1 Anxiety
The level of evidence regarding the outcome measure anxiety was downgraded by three levels to very low because of study limitations (lack of blinding, high risk of attrition bias and detection bias) (risk of bias: -2), and wide confidence intervals of individual studies (imprecision: -1).
3.2 Depressive symptoms
The level of evidence regarding the outcome measure depressive symptoms was downgraded by three levels to very low because of study limitations (lack of blinding, high risk of attrition bias and detection bias) (risk of bias: -2), and overlap of confidence interval with border of clinical relevance (imprecision: -1).
4. Fatigue
The level of evidence regarding the outcome measure fatigue was downgraded by four levels to very low because of study limitations (lack of blinding, high risk of detection bias and attrition bias) (risk of bias: -2), and overlap of confidence interval with both borders of clinical relevance (imprecision: -2).
5. Pain
The level of evidence regarding the outcome measure pain was downgraded by three levels to very low because of study limitations (lack of blinding, high risk of detection bias and attrition bias) (risk of bias: -2), and the low number of patients (imprecision: -1).
6. Quality of life
The level of evidence regarding the outcome measure quality of life could not be assessed.
7. Patient satisfaction
The level of evidence regarding the outcome measure patient satisfaction could not be assessed.
8. Complications
The level of evidence regarding the outcome measure complications was downgraded by four levels to low because of study limitations (lack of blinding) (risk of bias: -1), and overlap of confidence intervals with border of clinical relevance (imprecision: -1).
PICO 2 – Psychological treatment for FND
1. Physical complaints
The level of evidence regarding the outcome measure physical complaints was downgraded by three levels to very low because of study limitations (missing information on multiple domains, lack of blinding, high risk of attrition bias, detection bias, and reporting bias) (risk of bias: -2), and overlap of confidence interval with border of clinical relevance (imprecision: -1).
2. Functioning
The level of evidence regarding the outcome measure functioning was downgraded by three levels to low because of study limitations (lack of blinding) (risk of bias: -1), and overlap of confidence interval with border of clinical relevance (imprecision: -1).
3. Psychological complaints
3.1 Anxiety
The level of evidence regarding the outcome measure anxiety was downgraded by three levels to very low because of study limitations (missing information on multiple domains, lack of blinding, high risk of detection bias and reporting bias) (risk of bias: -2), and overlap of confidence interval with border of clinical relevance (imprecision: -1).
3.2 Depressive symptoms
The level of evidence regarding the outcome measure depressive symptoms was downgraded by three levels to very low because of study limitations (missing information on multiple domains, lack of blinding, high risk of detection bias and reporting bias) (risk of bias: -2), and overlap of confidence interval with border of clinical relevance (imprecision: -1).
4. Fatigue
The level of evidence regarding the outcome measure fatigue could not be assessed.
5. Pain
The level of evidence regarding the outcome measure pain could not be assessed.
6. Quality of life
The level of evidence regarding the outcome measure quality of life was downgraded by three levels to very low because of study limitations (lack of blinding, high risk of detection bias) (risk of bias: -1), and overlap of confidence interval with both borders of clinical relevance (imprecision: -2).
7. Patient satisfaction
The level of evidence regarding the outcome measure patient satisfaction was downgraded by two levels to low because of study limitations (lack of blinding) (risk of bias: -1), and overlap of confidence intervals with border of clinical relevance (imprecision: -1).
8. Complications
The level of evidence regarding the outcome measure complications was downgraded by four levels to very low because of study limitations (lack of blinding) (risk of bias: -1), and overlap of confidence intervals with both borders of clinical relevance (imprecision: -2).
A systematic review of the literature was performed to answer the following question:
What are the benefits and risks of paramedical and psychological treatment when compared to waitlist or usual care among patients with functional neurological disorder (FND)?
| P: | Patients with a diagnosis of functional neurological symptom disorder (DSM-5) or conversion disorder (DSM-IV), or patients diagnosed with FND by a neurologist based on positive clinical signs during neurological examination |
| I1: | Paramedical treatment (e.g., physical therapy, psychosomatic ergotherapy, education) |
| I2: | Psychological treatment |
| C: | Waitlist or usual care |
| O: | Physical complaints, functioning (including work participation), psychological complaints (e.g., anxiety, stress, mood), fatigue, pain, quality of life, patient satisfaction, complications |
Relevant outcome measures
The guideline development group considered physical complaints, psychological complaints, functioning, and quality of life as critical outcome measures for decision making, and fatigue, pain, patient satisfaction, and complications as important outcome measures for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
For all outcome measures, the working group defined a 25% difference for dichotomous outcomes (0.8 ≤ RR ≥ 1.25) and 0.5 SD for continuous outcomes as a minimal clinically (patient) important difference. If studies use different instruments to assess the same outcome measure, the standardized mean difference (SMD) is calculated. For SMDs, results were clinically relevant if they were smaller than -0.5 or larger than 0.5.
Search and select (Methods)
The databases Medline (via OVID), PsycINFO (via OVID), and Embase (via Embase.com) were searched with relevant search terms from 2010 until 2 July 2024. The detailed search strategy is available upon request. The systematic literature search resulted in 699 hits. Studies were selected based on the following criteria:
- Systematic review, RCTs or other comparative studies;
- Full-text English language publication;
- Studies according to the PICO.
In total, 27 studies were initially selected based on title and abstract screening. After reading the full text, 23 studies were excluded (see the table with reasons for exclusion under the tab ‘Evidence tabellen’) and four studies were selected for inclusion.
- Aybek S, Perez DL. Diagnosis and management of functional neurological disorder. BMJ. 2022 Jan 24;376:o64. doi: 10.1136/bmj.o64. PMID: 35074803.
- Baker J, Barnett C, Cavalli L, Dietrich M, Dixon L, Duffy JR, Elias A, Fraser DE, Freeburn JL, Gregory C, McKenzie K, Miller N, Patterson J, Roth C, Roy N, Short J, Utianski R, van Mersbergen M, Vertigan A, Carson A, Stone J, McWhirter L. Management of functional communication, swallowing, cough and related disorders: consensus recommendations for speech and language therapy. J Neurol Neurosurg Psychiatry. 2021 Oct;92(10):1112-1125. doi: 10.1136/jnnp-2021-326767. Epub 2021 Jul 1. PMID: 34210802.
- Barnett C, Armes J, Smith C. Speech, language and swallowing impairments in functional neurological disorder: a scoping review. Int J Lang Commun Disord. 2019 May;54(3):309-320. doi: 10.1111/1460-6984.12448. Epub 2018 Dec 27. PMID: 30592118.
- Berk M, Parker G. The elephant on the couch: side-effects of psychotherapy. Aust N Z J Psychiatry. 2009 Sep;43(9):787-94. doi: 10.1080/00048670903107559. PMID: 19670051.
- Cabreira V, Alty J, Antic S, Araújo R, Aybek S, Ball HA, Baslet G, Bhome R, Coebergh J, Dubois B, Edwards M, Filipović SR, Frederiksen KS, Harbo T, Hayhow B, Howard R, Huntley J, Isaacs J, LaFrance WC Jr, Larner AJ, Di Lorenzo F, Main J, Mallam E, Marra C, Massano J, McGrath ER, McWhirter L, Moreira IP, Nobili F, Pennington C, Tábuas-Pereira M, Perez DL, Popkirov S, Rayment D, Rossor M, Russo M, Santana I, Schott J, Scott EP, Taipa R, Tinazzi M, Tomic S, Toniolo S, Tørring CW, Wilkinson T, Frostholm L, Stone J, Carson A. Perspectives on the diagnosis and management of functional cognitive disorder: An international Delphi study. Eur J Neurol. 2025 Jan;32(1):e16318. doi: 10.1111/ene.16318. Epub 2024 May 3. PMID: 38700361; PMCID: PMC11617961.
- Cabreira V, Frostholm L, Stone J, Carson A. Feasibility trial of a self-help digital intervention for functional cognitive disorder. Brain Commun. 2025 Jun 19;7(4):fcaf248. doi: 10.1093/braincomms/fcaf248. PMID: 40641596; PMCID: PMC12241858.
- Connors MH, Quinto L, Deeley Q, Halligan PW, Oakley DA, Kanaan RA. Hypnosis and suggestion as interventions for functional neurological disorder: A systematic review. Gen Hosp Psychiatry. 2024 Jan-Feb;86:92-102. doi: 10.1016/j.genhosppsych.2023.12.006. Epub 2023 Dec 14. PMID: 38154334.
- Connors MH, Quinto L, Deeley Q, Halligan PW, Oakley DA, Kanaan RA. Hypnosis and suggestion as interventions for functional neurological disorder: A systematic review. Gen Hosp Psychiatry. 2024 Jan-Feb;86:92-102. doi: 10.1016/j.genhosppsych.2023.12.006. Epub 2023 Dec 14. PMID: 38154334
- Cope SR, Smith JG, El-Leithy S, Vanzan S, Hogwood P, Golder D, Turner KJ, Crowley M, Billings J, Pick S, Pentland C, Edwards MJ. Randomised feasibility study evaluating eye movement desensitisation and reprocessing therapy for functional neurological disorder (MODIFI). J Neurol. 2025 Jul 8;272(8):493. doi: 10.1007/s00415-025-13219-5. PMID: 40627223; PMCID: PMC12238153.
- Ding JM, Kanaan RA. Conversion disorder: A systematic review of current terminology. Gen Hosp Psychiatry. 2017 Mar-Apr;45:51-55. doi: 10.1016/j.genhosppsych.2016.12.009. Epub 2016 Dec 24. PMID: 28274339.
- Duncan R, Razvi S, Mulhern S. Newly presenting psychogenic nonepileptic seizures: incidence, population characteristics, and early outcome from a prospective audit of a first seizure clinic. Epilepsy Behav. 2011 Feb;20(2):308-11. doi: 10.1016/j.yebeh.2010.10.022. Epub 2010 Dec 30. PMID: 21195031.
- Ertan, D., Aybek, S., LaFrance Jr, W. C., Kanemoto, K., Tarrada, A., Maillard, L., ... & Hingray, C. (2022). Functional (psychogenic non-epileptic/dissociative) seizures: why and how?. Journal of Neurology, Neurosurgery & Psychiatry, 93(2), 144-157.
- Jordbru AA, Smedstad LM, Klungsøyr O, Martinsen EW. Psychogenic gait disorder: a randomized controlled trial of physical rehabilitation with one-year follow-up. J Rehabil Med. 2014 Feb;46(2):181-7. doi: 10.2340/16501977-1246. PMID: 24248149.
- Ganslev CA, Storebø OJ, Callesen HE, Ruddy R, Søgaard U. Psychosocial interventions for conversion and dissociative disorders in adults. Cochrane Database Syst Rev. 2020 Jul 17;7(7):CD005331. doi: 10.1002/14651858.CD005331.pub3. PMID: 32681745; PMCID: PMC7388313.
- Gasparini S, Beghi E, Ferlazzo E, Beghi M, Belcastro V, Biermann KP, Bottini G, Capovilla G, Cervellione RA, Cianci V, Coppola G, Cornaggia CM, De Fazio P, De Masi S, De Sarro G, Elia M, Erba G, Fusco L, Gambardella A, Gentile V, Giallonardo AT, Guerrini R, Ingravallo F, Iudice A, Labate A, Lucenteforte E, Magaudda A, Mumoli L, Papagno C, Pesce GB, Pucci E, Ricci P, Romeo A, Quintas R, Sueri C, Vitaliti G, Zoia R, Aguglia U. Management of psychogenic non-epileptic seizures: a multidisciplinary approach. Eur J Neurol. 2019 Feb;26(2):205-e15. doi: 10.1111/ene.13818. Epub 2018 Nov 29. PMID: 30300463.
- Gelauff JM, Rosmalen JGM, Carson A, Dijk JM, Ekkel M, Nielsen G, Stone J, Tijssen MAJ. Internet-based self-help randomized trial for motor functional neurologic disorder (SHIFT). Neurology. 2020 Sep 29;95(13):e1883-e1896. doi: 10.1212/WNL.0000000000010381. Epub 2020 Jul 20. PMID: 32690783.
- Gelauff J, Stone J, Edwards M, Carson A. The prognosis of functional (psychogenic) motor symptoms: a systematic review. J Neurol Neurosurg Psychiatry. 2014 Feb;85(2):220-6. doi: 10.1136/jnnp-2013-305321. Epub 2013 Sep 12. PMID: 24029543.
- Goldstein LH, Robinson EJ, Mellers JDC, Stone J, Carson A, Reuber M, Medford N, McCrone P, Murray J, Richardson MP, Pilecka I, Eastwood C, Moore M, Mosweu I, Perdue I, Landau S, Chalder T; CODES study group. Cognitive behavioural therapy for adults with dissociative seizures (CODES): a pragmatic, multicentre, randomised controlled trial. Lancet Psychiatry. 2020 Jun;7(6):491-505. doi: 10.1016/S2215-0366(20)30128-0. Epub 2020 May 20. PMID: 32445688; PMCID: PMC7242906.
- Goldstein LH, Robinson EJ, Chalder T, Reuber M, Medford N, Stone J, Carson A, Moore M, Landau S. Six-month outcomes of the CODES randomised controlled trial of cognitive behavioural therapy for dissociative seizures: A secondary analysis. Seizure. 2022 Mar;96:128-136. doi: 10.1016/j.seizure.2022.01.016. Epub 2022 Jan 25. PMID: 35228117; PMCID: PMC8970049.
- Goldstein AN, Paredes-Echeverri S, Finkelstein SA, Guthrie AJ, Perez DL, Freeburn JL. Speech and language therapy: A treatment case series of 20 patients with functional speech disorder. NeuroRehabilitation. 2023;53(2):227-238. doi: 10.3233/NRE-220182. PMID: 37599546.
- Goldstein LH, Stone J, Reuber M, Landau S, Robinson EJ, Carson A, Medford N, Chalder T. Reflections on the CODES trial for adults with dissociative seizures: what we found and considerations for future studies. BMJ Neurol Open. 2024 Jun 5;6(1):e000659. doi: 10.1136/bmjno-2024-000659. PMID: 38860230; PMCID: PMC11163627.
- Hallett M, Aybek S, Dworetzky BA, McWhirter L, Staab JP, Stone J. Functional neurological disorder: new subtypes and shared mechanisms. Lancet Neurol. 2022 Jun;21(6):537-550. doi: 10.1016/S1474-4422(21)00422-1. Epub 2022 Apr 14. Erratum in: Lancet Neurol. 2022 Jun;21(6):e6. doi: 10.1016/S1474-4422(22)00179-X. PMID: 35430029; PMCID: PMC9107510.
- Hunter RM, Nielsen G, Le Novere M, Marston L, Lee TC, Stone J, Goldstein LH, Carson A, Holt K, Marsden J, Nazareth I, Noble H, Reuber M, Strudwick AM, Santana Suarez B, Edwards MJ. Cost Utility of Specialist Physiotherapy for Functional Motor Disorder (Physio4FMD): Economic Analysis of a Pragmatic Randomized Controlled Trial. Neurol Clin Pract. 2025 Jun;15(3):e200465. doi: 10.1212/CPJ.0000000000200465. Epub 2025 Apr 1. PMID: 40190588; PMCID: PMC11970929.
- Lagrand TJ, Jones M, Bernard A, Lehn AC. Health Care Utilization in Functional Neurologic Disorders: Impact of Explaining the Diagnosis of Functional Seizures on Health Care Costs. Neurol Clin Pract. 2023 Feb;13(1):e200111. doi: 10.1212/CPJ.0000000000200111. Epub 2023 Jan 11. PMID: 36865642; PMCID: PMC9973286.
- Nielsen G, Stone J, Edwards MJ. Physiotherapy for functional (psychogenic) motor symptoms: a systematic review. J Psychosom Res. 2013 Aug;75(2):93-102. doi: 10.1016/j.jpsychores.2013.05.006. Epub 2013 Jun 12. PMID: 23915764.
- Nielsen G, Stone J, Matthews A, Brown M, Sparkes C, Farmer R, Masterton L, Duncan L, Winters A, Daniell L, Lumsden C, Carson A, David AS, Edwards M. Physiotherapy for functional motor disorders: a consensus recommendation. J Neurol Neurosurg Psychiatry. 2015 Oct;86(10):1113-9. doi: 10.1136/jnnp-2014-309255. Epub 2014 Nov 28. PMID: 25433033; PMCID: PMC4602268.
- Nielsen G, Stone J, Lee TC, Goldstein LH, Marston L, Hunter RM, Carson A, Holt K, Marsden J, Le Novere M, Nazareth I, Noble H, Reuber M, Strudwick AM, Santana Suarez B, Edwards MJ; Physio4FMD study group. Specialist physiotherapy for functional motor disorder in England and Scotland (Physio4FMD): a pragmatic, multicentre, phase 3 randomised controlled trial. Lancet Neurol. 2024 Jul;23(7):675-686. doi: 10.1016/S1474-4422(24)00135-2. Epub 2024 May 17. PMID: 38768621.
- Perez DL, Aybek S, Popkirov S, Kozlowska K, Stephen CD, Anderson J, Shura R, Ducharme S, Carson A, Hallett M, Nicholson TR, Stone J, LaFrance WC Jr, Voon V; (On behalf of the American Neuropsychiatric Association Committee for Research. A Review and Expert Opinion on the Neuropsychiatric Assessment of Motor Functional Neurological Disorders. J Neuropsychiatry Clin Neurosci. 2021 Winter;33(1):14-26. doi: 10.1176/appi.neuropsych.19120357. Epub 2020 Aug 11. PMID: 32778007.
- Poole N, Cope S, Vanzan S, Duffus A, Williams T, Mantovani N, Smith JG, Barrett B, Scicluna M, Beardmore S, Edwards MJ, Howard R. Randomised controlled feasibility trial of online group acceptance and commitment therapy for functional cognitive disorder. BJPsych Open. 2025 May 2;11(3):e91. doi: 10.1192/bjo.2025.33. PMID: 40314156; PMCID: PMC12089801.
- Rioux M, Mamman R, Byworth MT, Panenka WJ, Howard AK, Perez DL, Schmidt J, Courchesne C, LeMoult J, Heran MK, Silverberg ND. Pilot feasibility randomised controlled trial of cognitive-behavioural therapy for functional cognitive disorder after concussion. BMJ Neurol Open. 2024 Oct 11;6(2):e000666. doi: 10.1136/bmjno-2024-000666. PMID: 39410977; PMCID: PMC11474702.
- Staton A, Dawson D, Merdian H, Tickle A, Walker T. Functional neurological disorder: A qualitative study exploring individuals' experiences of psychological services. Psychol Psychother. 2024 Mar;97(1):138-156. doi: 10.1111/papt.12504. Epub 2023 Oct 6. PMID: 37800641.
- Stone J, Carson A, Hallett M. Explanation as treatment for functional neurologic disorders. Handb Clin Neurol. 2016;139:543-553. doi: 10.1016/B978-0-12-801772-2.00044-8. PMID: 27719870.
- Tibben MI, van Opdorp A, Bialek W, Schaap J, Tijssen MAJ, Merkx MJM. Efficacy of Hypnosis and Catalepsy Induction in Functional Neurological Disorders. Mov Disord Clin Pract. 2024 Feb;11(2):129-135. doi: 10.1002/mdc3.13934. Epub 2023 Dec 18. PMID: 38386488; PMCID: PMC10883405.
- Watson M, Woodward J, Strom LA. The Financial Burden of Functional Neurological Disorders. Curr Neurol Neurosci Rep. 2023 Oct;23(10):637-643. doi: 10.1007/s11910-023-01298-8. Epub 2023 Sep 11. PMID: 37695443.
Risk of bias table
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented? Were patients, healthcare providers, data collectors, outcome assessors, data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Nielsen, 2024 |
Definitely yes;
Reason: The randomization sequence was computer generated and programmed by an independent statistician. Block randomization was done with random block sizes. |
Definitely yes;
Reason: Randomization was web-based. |
Probably no;
Reason: Researchers, statisticians, and health economists were masked to treatment allocation, and participants were asked not to reveal their group allocation to research workers. Due to the nature of the intervention, it was not possible to mask the trial manager, participants, or treating clinicians. |
Probably yes;
Reason: 14 participants (8%) from the intervention group and 11 participants (6%) from the control group were lost to follow-up. Missing outcome data is balanced across both groups. |
Definitely yes;
Reason: Trial is registered at ISRCTN (ISRCTN56136713). Primary and secondary outcomes are reported as prespecified.
|
Definitely yes;
Reason: No other problems noted. |
Some concerns |
|
Goldstein, 2020/2022 |
Definitely yes;
Reason: Web-based randomization was used. Block randomization was done with random block sizes. |
Definitely yes;
Reason: Randomization was web-based. |
Definitely no;
Reason: The trial manager, chief investigator, all treating clinicians, and patients were aware of treatment allocation, but outcome data collectors and trial statisticians were unaware of treatment allocation. |
Probably yes
Reason: 30 participants (21%) from the intervention group and 25 participants (14%) from the control group were lost to follow-up. Missing outcome data is unbalanced across both groups. ITT analyses are performed. Multiple imputation was used to adjust for missing data. |
Definitely yes
Reason: Trial is registered at ClinicalTrials.gov (NCT02325544). Primary and secondary outcomes are reported as prespecified. |
Definitely yes;
Reason: No other problems noted. |
High |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Bartl M, Kewitsch R, Hallett M, Tegenthoff M, Paulus W. Diagnosis and therapy of functional tremor a systematic review illustrated by a case report. Neurol Res Pract. 2020 Dec 3;2:35. doi: 10.1186/s42466-020-00073-1. PMID: 33324935; PMCID: PMC7713151. |
Results are descriptively reported, no raw data presented. |
|
Connors MH, Quinto L, Deeley Q, Halligan PW, Oakley DA, Kanaan RA. Hypnosis and suggestion as interventions for functional neurological disorder: A systematic review. Gen Hosp Psychiatry. 2024 Jan-Feb;86:92-102. doi: 10.1016/j.genhosppsych.2023.12.006. Epub 2023 Dec 14. PMID: 38154334. |
Results are descriptively reported, no raw data presented. |
|
Gaskell C, Power N, Novakova B, Simmonds-Buckley M, Kerr WT, Reuber M, Kellett S, Rawlings GH. A meta-analytic evaluation of the effectiveness and durability of psychotherapy for adults presenting with functional dissociative seizures. Seizure. 2024 Jul;119:98-109. doi: 10.1016/j.seizure.2024.05.016. Epub 2024 May 25. PMID: 38824867. |
Wrong outcomes (seizure frequency, intensity, severity, bothersomeness, duration, clusters), results are descriptively reported, no raw data presented. |
|
Gonsalvez I, Spagnolo P, Dworetzky B, Baslet G. Neurostimulation for the treatment of functional neurological disorder: A systematic review. Epilepsy Behav Rep. 2021 Nov 9;16:100501. doi: 10.1016/j.ebr.2021.100501. PMID: 34950864; PMCID: PMC8671519. |
Wrong comparison (2x sham TMS, 1x root magnetic stimulation, 1x low-intensity stimulation). |
|
Nielsen G, Stone J, Edwards MJ. Physiotherapy for functional (psychogenic) motor symptoms: a systematic review. J Psychosom Res. 2013 Aug;75(2):93-102. doi: 10.1016/j.jpsychores.2013.05.006. Epub 2013 Jun 12. PMID: 23915764. |
Includes only one relevant RCT (Moene, 2002), which is included in Ganslev (2020) which is a more recent SR. |
|
Molero-Mateo P, Molina-Rueda F. Physiotherapy for patients with functional movement disorder: a systematic review. Neurologia (Engl Ed). 2024 Jul-Aug;39(6):505-514. doi: 10.1016/j.nrleng.2022.01.008. Epub 2023 Apr 27. PMID: 37116691. |
Results are descriptively reported, no raw data presented. |
|
Martlew J, Pulman J, Marson AG. Psychological and behavioural treatments for adults with non-epileptic attack disorder. Cochrane Database Syst Rev. 2014 Feb 11;2014(2):CD006370. doi: 10.1002/14651858.CD006370.pub2. PMID: 24519702; PMCID: PMC11032749. |
Includes four relevant RCTs (Moene, 2002; Moene, 2003; Goldstein, 2010; Ataoglu, 2003), which are included in Ganslev (2020) which is a more recent SR. |
|
Carlson P, Nicholson Perry K. Psychological interventions for psychogenic non-epileptic seizures: A meta-analysis. Seizure. 2017 Feb;45:142-150. doi: 10.1016/j.seizure.2016.12.007. Epub 2016 Dec 21. PMID: 28063373. |
Includes two relevant RCTs (Ataoglu, 2003; LaFrance, 2014), which are included in Ganslev (2020) which is a more recent SR. |
|
Gutkin M, McLean L, Brown R, Kanaan RA. Systematic review of psychotherapy for adults with functional neurological disorder. J Neurol Neurosurg Psychiatry. 2020 Nov 5:jnnp-2019-321926. doi: 10.1136/jnnp-2019-321926. Epub ahead of print. PMID: 33154184. |
No raw data presented (only effect sizes), no meta-analysis. |
|
Goldstein LH, Robinson EJ, Pilecka I, Perdue I, Mosweu I, Read J, Jordan H, Wilkinson M, Rawlings G, Feehan SJ, Callaghan H, Day E, Purnell J, Baldellou Lopez M, Brockington A, Burness C, Poole NA, Eastwood C, Moore M, Mellers JD, Stone J, Carson A, Medford N, Reuber M, McCrone P, Murray J, Richardson MP, Landau S, Chalder T. Cognitive-behavioural therapy compared with standardised medical care for adults with dissociative non-epileptic seizures: the CODES RCT. Health Technol Assess. 2021 Jun;25(43):1-144. doi: 10.3310/hta25430. PMID: 34196269; PMCID: PMC8273679. |
Health technology assessment of the CODES trial, which is included in the literature summary. |
|
Hubschmid M, Aybek S, Maccaferri GE, Chocron O, Gholamrezaee MM, Rossetti AO, Vingerhoets F, Berney A. Efficacy of brief interdisciplinary psychotherapeutic intervention for motor conversion disorder and nonepileptic attacks. Gen Hosp Psychiatry. 2015 Sep-Oct;37(5):448-55. doi: 10.1016/j.genhosppsych.2015.05.007. Epub 2015 May 29. PMID: 26099544. |
Included in Ganslev (2020). |
|
Libbon R, Gadbaw J, Watson M, Rothberg B, Sillau S, Heru A, Strom L. The feasibility of a multidisciplinary group therapy clinic for the treatment of nonepileptic seizures. Epilepsy Behav. 2019 Sep;98(Pt A):117-123. doi: 10.1016/j.yebeh.2019.06.032. Epub 2019 Jul 29. PMID: 31369968. |
Wrong outcomes (feasibility outcomes), wrong comparison (5-week programme versus 12-week programme). |
|
Velani H, Gledhill J. The effectiveness of psychological interventions for children and adolescents with non-epileptic seizures. Seizure. 2021 Dec;93:20-31. doi: 10.1016/j.seizure.2021.09.006. Epub 2021 Sep 14. PMID: 34656015. |
Wrong population (children and adolescents). |
|
FitzGerald TL, Southby AK, Haines TP, Hough JP, Skinner EH. Is physiotherapy effective in the management of child and adolescent conversion disorder? A systematic review. J Paediatr Child Health. 2015 Feb;51(2):159-67. doi: 10.1111/jpc.12630. Epub 2014 Jun 13. PMID: 24923418. |
Includes no RCTs. |
|
Duncan R, Berlowitz DJ, Mullen S, Bondarenko J, Winton-Brown TT, O'Brien TJ, Zaloumis S, Braat S, Oliver G, Kanaan RA. Breathing control training for functional seizures: A multi-site, open-label pilot study. Epilepsy Behav. 2024 May;154:109745. doi: 10.1016/j.yebeh.2024.109745. Epub 2024 Mar 22. PMID: 38521027. |
Observational non-comparative design. |
|
Chen DK, Maheshwari A, Franks R, Trolley GC, Robinson JS, Hrachovy RA. Brief group psychoeducation for psychogenic nonepileptic seizures: a neurologist-initiated program in an epilepsy center. Epilepsia. 2014 Jan;55(1):156-66. doi: 10.1111/epi.12481. Epub 2013 Dec 20. PMID: 24446955. |
Included in Ganslev (2020). |
|
Gelauff JM, Rosmalen JGM, Carson A, Dijk JM, Ekkel M, Nielsen G, Stone J, Tijssen MAJ. Internet-based self-help randomized trial for motor functional neurologic disorder (SHIFT). Neurology. 2020 Sep 29;95(13):e1883-e1896. doi: 10.1212/WNL.0000000000010381. Epub 2020 Jul 20. PMID: 32690783. |
Results are descriptively reported (self-reported). |
|
Abbass A, Lumley MA, Town J, Holmes H, Luyten P, Cooper A, Russell L, Schubiner H, De Meulemeester C, Kisely S. Short-term psychodynamic psychotherapy for functional somatic disorders: A systematic review and meta-analysis of within-treatment effects. J Psychosom Res. 2021 Jun;145:110473. doi: 10.1016/j.jpsychores.2021.110473. Epub 2021 Mar 26. PMID: 33814192. |
Includes no RCTs that are conform the PICO of this module. |
|
LaFrance WC Jr, Baird GL, Barry JJ, Blum AS, Frank Webb A, Keitner GI, Machan JT, Miller I, Szaflarski JP; NES Treatment Trial (NEST-T) Consortium. Multicenter pilot treatment trial for psychogenic nonepileptic seizures: a randomized clinical trial. JAMA Psychiatry. 2014 Sep;71(9):997-1005. doi: 10.1001/jamapsychiatry.2014.817. PMID: 24989152. |
Included in Ganslev (2020). |
|
Thompson N, Connelly L, Peltzer J, Nowack WJ, Hamera E, Hunter EE. Psychogenic nonepileptic seizures: a pilot study of a brief educational intervention. Perspect Psychiatr Care. 2013 Apr;49(2):78-83. doi: 10.1111/j.1744-6163.2012.00353.x. Epub 2012 Sep 20. PMID: 23557450. |
Included in Ganslev (2020). |
|
Tibben MI, van Opdorp A, Bialek W, Schaap J, Tijssen MAJ, Merkx MJM. Efficacy of Hypnosis and Catalepsy Induction in Functional Neurological Disorders. Mov Disord Clin Pract. 2024 Feb;11(2):129-135. doi: 10.1002/mdc3.13934. Epub 2023 Dec 18. PMID: 38386488; PMCID: PMC10883405. |
Non-randomized observational design. |
|
Dallocchio C, Tinazzi M, Bombieri F, Arnó N, Erro R. Cognitive Behavioural Therapy and Adjunctive Physical Activity for Functional Movement Disorders (Conversion Disorder): A Pilot, Single-Blinded, Randomized Study. Psychother Psychosom. 2016;85(6):381-383. doi: 10.1159/000446660. Epub 2016 Oct 15. PMID: 27744440. |
Included in Ganslev (2020). |
|
Goldstein LH, Chalder T, Chigwedere C, Khondoker MR, Moriarty J, Toone BK, Mellers JD. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology. 2010 Jun 15;74(24):1986-94. doi: 10.1212/WNL.0b013e3181e39658. PMID: 20548043; PMCID: PMC2905892. |
Included in Ganslev (2020). |
Beoordelingsdatum en geldigheid
Publicatiedatum : 09-07-2026
Beoordeeld op geldigheid : 09-07-2026
Algemene gegevens
Er is een verklaring van geen bezwaar afgegeven door:
- Ergotherapie Nederland
- Nederlandse Vereniging voor Neurologie
- Nederlands Huisartsen Genootschap
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor mensen met een somatisch-symptoomstoornis of functioneel-neurologisch-symptoomstoornis.
Werkgroep
- dr. E. (Ella) Bekhuis, psychiater, namens de NVvP
- D. (Door) Boxhoorn, patiëntvertegenwoordiger, namens het NALK (tot mei 2025)
- K. (Karin) Bruynesteyn, patiëntvertegenwoordiger, namens het NALK (tot april 2024)
- dr. E.M.J. (Elisabeth) Foncke, neuroloog, namens de NVN
- S. (Sem) Foreman, patiëntvertegenwoordiger, namens het NALK
- dr. J. (Jeannette) Gelauff, AIOS neurologie, namens de NVN (vanaf maart 2025)
- dr. D.J.C. (Denise) Hanssen, klinisch psycholoog/psychotherapeut, namens het NIP
- dr. H. (Hanneke) Kalisvaart, psychomotorisch therapeut, namens Vaktherapie Nederland
- drs. M. (Manouk) van de Klundert, patiëntvertegenwoordiger, namens het NALK
- prof. dr. R.C. (Richard) Oude Voshaar, psychiater, namens de NVvP
- prof. dr. J.G.M. (Judith) Rosmalen, hoogleraar, persoonlijke titel
- dr. S. (Sonja) Rutten, psychiater, namens de NVvP
- drs. C.A. (Lot) Spiertz, klinisch psycholoog/psychotherapeut, namens het NIP
- dr. L.M. (Lineke) Tak (voorzitter), psychiater, namens de NVvP
- dr. P.E. (Els) van Westrienen, docent-senior onderzoeker, namens het KNGF
- prof. dr. A.P. (André) Wolff, anesthesioloog-pijnspecialist, namens de NVA
- dr. L.N.L. (Lyonne) Zonneveld, klinisch psycholoog/psychotherapeut, namens het NIP
Klankbordgroep
- drs. M. (Marieke) van Beugen, revalidatiearts, namens de Nederlandse Vereniging van Revalidatieartsen (VRA)
- drs. B.F. (Bart) van Buchem, fysiotherapeut, namens het KNGF
- drs. W.B. (Wouter) Doorn, klinisch geriater, namens de Nederlandse Vereniging voor Klinische Geriatrie (NVKG)
- H.W.P.C. (Henk) van de Meerendonk, bedrijfsarts, namens de Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (NVAB)
- dr. A.F. (Alex) Muller, internist-endocrinoloog, namens Nederlandse Internisten Vereniging (NIV)
- dr. S.L. (Sonja) van Ockenburg, internist, namens de NIV
- dr. T.C. (Tim) Olde Hartman, huisarts(-onderzoeker), namens het Nederlands Huisartsen Genootschap (NHG)
- drs. R.F.A. (René) Oosterwijk, revalidatiearts, namens de VRA
- E.M. (Ilse) Otten, ergotherapeut, namens Ergotherapie Nederland (EN)
- drs. F. (Felice) Tauer, vaktherapeut, namens de Vaktherapie Nederland
- dr. K.H.N. (Kristel) Weerdesteijn, verzekeringsarts, namens de Nederlandse Vereniging voor Verzekeringsgeneeskunde (NVVG)
- dr. M.S.H. (Margreet) Wortman, senior onderzoeker, namens de Vereniging van Oefentherapeuten Cesar en Mensendieck (VvOCM)
Met ondersteuning van
- dr. M.L. (Marja) Molag, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- drs. L.C. (Laura) van Wijngaarden, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel 1. Gemelde (neven)functies en belangen werkgroep
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
E. (Ella) Bekhuis |
Psychiater, Dimence, Alkura |
Geen |
Geen |
Geen restricties |
|
D. (Door) Boxhoorn (tot mei 2025) |
Ervaringsdeskundige, Dimence Alkura |
Geen |
Geen |
Geen restricties |
|
K. (Karin) Bruynesteyn (tot april 2024) |
Lid patiëntenpanel NALK |
Geen |
Geen |
Geen restricties |
|
E.M.J. (Elisabeth) Foncke |
Neuroloog, Acibadem International Medical Center, Amsterdam |
Geen |
Geen |
Geen restricties |
|
S. (Sem) Foreman |
Lid patiëntenpanel NALK |
* Investment manager, Graduate Entrepreneur Fund |
Geen |
Geen restricties |
|
J. (Jeannette) Gelauff (vanaf maart 2025) |
AIOS neurologie, Amsterdam UMC |
* Voorzitter landelijke werkgroep FNS van de Nederlandse Vereniging voor Neurologie. * Deelname werkgroep zorgstandaard FNS (Akwa GGZ). |
Extern gefinancierd onderzoek: Zonmw; National Plan Hoofdzaken: BEGRIP studie naar educatie over FNS. ProjectLeidersrol, nee |
Geen restricties |
|
D.J.C. (Denise) Hanssen |
* Klinisch psycholoog/psychotherapeut, UMC Groningen * Senior wetenschappelijk onderzoeker ouderenpsychiatrie, UMC Groningen |
* Hoofddocent somatiek binnen de GZ-opleiding |
Extern gefinancierd onderzoek: * ZonMW, Haalbaarheidsstudie Acceptance and Commitment Therapy bij kwetsbare ouderen EU, Horizon 2020 * Kennis vergroten over Functionele Stoornissen (labeling, multidisciplinaire samenwerking) |
Geen restricties |
|
H. (Hanneke) Kalisvaart |
Psychomotorisch therapeut, vrijgevestigd |
* Trainer/supervisor in sensorimotor psychotherapy. * Freelance senior onderzoeker (Tilburg University) * Gast-docent Master PMT Hogeschool Windesheim. * Deelname werkgroep zorgstandaard FNS (Akwa GGZ). |
Extern gefinancierd onderzoek: * Stichting tot steun VCVGZ. Het effect van sensorimotor psychotherapie bij cliënten met persoonlijkheidsstoornissen. |
Geen restricties |
|
M. (Manouk) van de Klundert |
Lid patiëntenpanel NALK |
* Office manager NALK * Project manager/junior consultant Ftrprf |
Geen |
Geen restricties |
|
R.C. (Richard) Oude Voshaar |
* Psychiater, UMC Groningen * Hoogleraar ouderenpsychiatrie, Rijksuniversiteit Groningen |
Geen |
Geen |
Geen restricties |
|
J.G.M. (Judith) Rosmalen |
Hoogleraar Psychosomatiek, UMC Groningen, Rijksuniversiteit Groningen |
* Voorzitter Netwerk Aanhoudende Lichamelijke Klachten (NALK) tot okt 2024. * Vice-president European Association of Psychosomatic Medicine (EAPM) tot September 2025 |
Persoonlijke belangen: Ontwikkelaar van een eLearning op het gebied van ALK. Deelnemen aan de elearning is betaald voor sommige groepen; inkomsten gaan naar het UMCG en hiervan wordt de accreditatie betaald. Ontwikkelaar van Grip, een eHealth systeem dat zich richt op ALK. Momenteel is Grip niet beschikbaar buiten studiedoeleinden. Ik heb en had nooit persoonlijke financiële belangen bij Grip.
Extern gefinancierd onderzoek: * ZonMw: ME/CFS Lines – A multidisciplinary consortium and biobank for unravelling ME/CFS aetiology in Lifelines, projectleider * EU: Decision support for prediction and management of Long Covid Syndrome, geen projectleider * NIMH: An Integrative Approach to the Etiology of Internalizing Disorders in the Lifelines Cohort, geen projectleider * ZonMw: Persistent symptoms after COVID-19: perspective from the population, the patient, and the care system, projectleider * SBOH Innovatiefonds Huisartsopleiding: Ontwikkeling, implementatie en evaluatie van onderwijsprogramma voor somatisch onvoldoende verklaarde lichamelijke klachten (SOLK) in de huisartsopleiding, geen projectleider * NIMH: An Integrative Approach to the Etiology of Internal Sex and gender inequalities in COVID * Regionaal ALK netwerk Salland. Sex and gender inequalities in medical trajectories of patients with common somatic symptoms. Master Your symptoms: personalized e-health for Self-management of somatic symptom disorder (MYSelf), projectleider * EU: Encompassing Training in functional Disorders across Europe (ETUDE), projectleider * EU: Towards evidence-based tailored implementation strategies for eHealth (ImpleMentAll), geen projectleider |
Geen restricties |
|
S. (Sonja) Rutten |
* Psychiater, Amsterdam UMC * Senior-onderzoeker, Amsterdam UMC |
Geen |
Extern gefinancierd onderzoek: ZonMW: Meer BEkendheid en GRIP voor mensen met FNS middels een online educatiemodule (BEGRIP) |
Geen restricties |
|
C.A. (Lot) Spiertz |
Klinisch-psycholoog, behandelcoördinator en teamleider, Dimence, Deventer |
* Gastdocent Psychology master, Universiteit Twente (t/m 2024). * Gastdocentschap Psychology master, Radboud Universiteit (t/m 2025). |
Geen |
Geen restricties |
|
L.M. (Lineke) Tak |
Psychiater, Dimence, Deventer |
* Bestuurslid NALK, sinds okt 2024 voorzitter * Kernredactielid Tijdschrift voor Psychiatrie |
* EU: Encompassing Training in functional Disorders across Europe (ETUDE), * Collaborative care networks for Functional Disorders |
Geen restricties |
|
P.E. (Els) van Westrienen |
* Docent-senior onderzoeker, Fontys Hogeschool * Docent, Hogeschool Utrecht |
Geen |
* SIA RAAK publiek - PARASOL studie * SIA RAAK top-up - vervolg PARASOL studie * SIA RAAK MKB - van sensoren naar zorg * SIA RAAK publiek Evaluatie van een proactief interventie ter preventie van chroniciteit bij mensen met matige SOLK * SIA RAAK MKB Het toepassen van stressmetingen met wearables in de praktijk |
Geen restricties |
|
A.P. (André) Wolff |
* Anesthesioloog-pijnspecialist, UMC Groningen * Hoogleraar Rijksuniversiteit Groningen |
* Medisch hoofd UCG pijncentrum |
Extern gefinancierd onderzoek: * Philips, DANI studie, geen projectleider * KWR, Chordotomie studie, projectleider * Interreg, Chronische pijn in Noord-Nederland/Niedersachsen * QPS, verrichtingen voor derden, geen projectleider * Grunenthal, Prince studie, projectleider |
Geen restricties |
|
L.N.L. (Lyonne) Zonneveld |
Klinisch-psycholoog, Amsterdam UMC |
Geen |
* ZonMW Stimuleringssubsidie * Doelmatigheidsonderzoek |
Geen restricties |
Tabel 2. Gemelde (neven)functies en belangen klankbordgroep
|
Klankbordgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
M. (Marieke) van Beugen |
Revalidatiearts bij Heliomare Wijk aan Zee |
Geen |
Geen |
Geen restricties |
|
B.F. (Bart) van Buchem |
Eigenaar praktijk voor fysiotherapie Praktijk Noorder Spaarne |
Geen |
Nascholing voor fysiotherapeuten, het organiseren en doseren van cursussen. Aandeel in Noigroup Publications (Australia) Royalties van het boek Begrijp de Pijn (Explain Pain) |
Geen restricties |
|
W.B. (Wouter) Doorn |
Klinisch Geriater te Altrecht |
Secretaris en vice-voorzitter Stichting Buddho, onbetaald. |
Geen |
Geen restricties |
|
H.W.P.C. (Henk) van de Meerendonk |
VDM Medisch Consult: zelfstandig bedrijfsarts. |
Lid CROW NVAB |
Geen |
Geen restricties |
|
A.F. (Alex) Muller |
Internist Diakonessenziekenhuis Utrecht 1.0 fte |
Geen |
Geen |
Geen restricties |
|
S.L. (Sonja) van Ockenburg |
Internist-endocrinoloog in het UMCG (bezoldigd 1.0 fte) |
Geen |
Ja, Lifelines long covid studie ZonMw Pathofysiologisch onderzoek naar 'long covid' in de Lifelines populatie (werkpakket 2). Geen hoofdonderzoeker. |
Geen restricties |
|
T.C. (Tim) Olde Hartman |
Huisarts-onderzoeker, hoofd van de onderzoeksgroep Huisartsgeneeskunde Afdeling Eerstelijnsgeneeskunde Radboudumc (afgevaardigde vanuit het Nederlands Huisartsen Genootschap - NHG) |
Praktijkhoudend huisarts |
ZonMw Mental Health Verbindt - digitaal platform voor zoeken juiste zorg EU (Horizon ITN) ETUDE: Encompassing Training in fUnctional Disorders across Europe - Stigma - symptom diagnoses ZonMw GRIP3: General practice Research Infrastructure Pandemic Preparedness Program ZonMw ACTION: Aanhoudende Klachten na COVID-19: perspectief vanuit de populatie, patiënt, en zorg ZonMw Inzicht in aanhoudende klachten na Covid-19 besmetting: Een mixed methods benadering. |
Geen restricties |
|
R.F.A. (René) Oosterwijk |
Revalidatiearts-medisch directeur, CIR , Clinics In Revalidatie. Loondienstverband. Het betreft 0.6 fte patiëntenzorg voor patiënten met chronische pijn en 0.4 fte medisch manager. |
Onbezoldigd lid van het bestuur van het NALK |
Geen |
Geen restricties |
|
E.M. (Ilse) Otten |
Ergotherapeut in dienst bij Klimmendaal revalidatie. 24 uur/w |
Ergotherapeut ZZP bij Care2change 2-6 uur/w |
Geen |
Geen restricties |
|
F. (Felice) Tauer |
1. Beeldend therapeut bij Altrecht GGZ (16u), behandeling van patiënten met psychosomatische klachten in een multidisciplinair team, betaald 2. docent beeldende therapie bij Hogeschool van Arnhem en Nijmegen (20u), methodieklessen, onderzoek coördinatie bacheloronderzoek, docentonderzoeker lectoraat. betaald |
Geen |
Geen |
Geen restricties |
|
K. (Kristel) Weerdesteijn |
Verzekeringsarts en opleider bij UWV |
Betaald docent |
Gepromoveerd in 2022 KCVG Work-related functioning among long-term sick-listed workers with persistent subjective health complaints |
Geen restricties |
|
M.S.H. (Margreet) Wortman |
Senior onderzoeker Hogeschool van Amsterdam, 0.5 fte, betaald |
Curriculum ontwikkelaar en docent Hogeschool Windesheim, 0.5 fte, betaald |
ZonMw Oefentherapie voor gezond beweeggedrag in de leefomgeving van cliënten |
Geen restricties |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door afgevaardigden van het patiëntenpanel NALK te betrekken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen (zie kop ‘Waarden en voorkeuren van patiënten’). De conceptrichtlijn is tevens voor commentaar voorgelegd aan NALK en MIND en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
Module |
Uitkomst raming |
Toelichting |
|
Module Paramedische en psychologische behandeling van FNS |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Literature search strategy
|
Cluster/richtlijn: NVVP Akwa GGZ Somatisch-symptoomstoornis en Functioneel-neurologisch-symptoomstoornis |
|
|
Uitgangsvraag/modules: Wat is de plaats van paramedische en psychologische behandeling bij de functionele neurologische stoornis? |
|
|
Database(s): Embase.com, Ovid/Medline, Ovid/PsycInfo |
Datum: 2 juli 2024 |
|
Periode: 2010 |
Talen: geen restrictie |
|
Literatuurspecialist: Alies Oost |
Rayyan review: https://rayyan.ai/reviews/1081832 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen:
Onderstaande sleutelartikelen worden op zich gevonden, maar voldoen niet aan het gevraagde studie design: -Treatment of Psychogenic Nonepileptic Seizures/ Lopez M.R., et al. Current Neurology and Neuroscience Reports 2022 22:8 (467-474) -Management of functional communication, swallowing, cough and related disorders: Consensus recommendations for speech and language therapy/ Baker J., et al. Journal of Neurology, Neurosurgery and Psychiatry 2021 92:10 (1112-1125) |
|
|
Te gebruiken voor richtlijntekst: In de databases Embase.com, Ovid/Medline en Ovid/PsycInfo is op 2 juli 2024 systematisch gezocht naar systematische reviews, RCTs en observationele studies over paramedische en psychologische behandeling bij de functionele neurologische stoornis. De literatuurzoekactie leverde 699 unieke treffers op. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
OVID/PSYCINFO |
Ontdubbeld |
|
SR |
89 |
45 |
63 |
135 |
|
RCT |
141 |
100 |
40 |
180 |
|
Observationele studies |
365 |
134 |
54 |
384 |
|
Totaal |
595 |
279 |
157 |
699* |
*in Rayyan
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
'conversion disorder'/exp OR ((conversion NEAR/3 (disorder* OR syndrome*)):ti,ab,kw) OR 'functional neurological disorder'/exp OR 'functional movement disorder'/exp OR 'functional motor disorder'/exp OR ((('functional neurologic*' OR 'functional movement' OR 'functional motor' OR 'functional cognitive') NEAR/3 disorder*):ti,ab,kw) OR 'functional dizziness':ti,ab,kw OR 'nonepileptic seizure'/exp OR (((nonepileptic OR 'non epileptic' OR conversion OR dissociative OR hysteri* OR psychogenic OR functional) NEAR/3 seizure*):ti,ab,kw) OR pnes:ti,ab,kw |
12238 |
|
#2 |
'psychotherapy'/de OR 'psychodynamic psychotherapy'/exp OR psychotherap*:ti,ab,kw OR 'body psychotherapy'/exp OR ((somatic NEAR/3 experiencing):ti,ab,kw) OR (((body OR psychosomatic) NEAR/3 (therap* OR intervention* OR treat*)):ti,ab,kw) OR 'physiotherapy'/exp OR physiotherap*:ti,ab,kw OR 'physio therap*':ti,ab,kw OR 'physical therap*':ti,ab,kw OR 'kinesiotherapy'/exp OR kinesiotherap*:ti,ab,kw OR kinesitherapeutic*:ti,ab,kw OR 'occupational therapy'/exp OR 'occupation* therap*':ti,ab,kw OR ergotherap*:ti,ab,kw OR 'graded exposure':ti,ab,kw OR 'graded activit*':ti,ab,kw OR 'graded physical activit*':ti,ab,kw OR 'graded exercis*':ti,ab,kw OR 'hypnosis'/exp OR 'hypnotherapy'/exp OR hypnos*:ti,ab,kw OR hypnot*:ti,ab,kw OR hypnogenesis:ti,ab,kw OR mesmerism:ti,ab,kw OR 'catalepsy'/exp OR ((induc* NEAR/3 cataleps*):ti,ab,kw) OR 'cognitive behavioral therapy'/exp OR 'cognitive behavior*':ti,ab,kw OR 'cognitive behaviour*':ti,ab,kw OR cbt:ti,ab,kw OR ccbt:ti,ab,kw OR cbsm:ti,ab,kw OR 'rehabilitation'/exp OR rehabilitat*:ti,ab,kw OR 'patient education'/exp OR 'health education'/de OR 'psychoeducation'/exp OR 'psycho education':ti,ab,kw OR psychoeducation:ti,ab,kw OR ((patient* NEAR/3 educat*):ti,ab,kw) OR 'speech and language rehabilitation'/exp OR 'speech language pathologist'/exp OR logoped*:ti,ab,kw OR (((speech OR voice OR vocal OR language) NEAR/3 (therap* OR rehabilit* OR reeducat* OR train*)):ti,ab,kw) |
1419273 |
|
#3 |
#1 AND #2 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab,kw OR child*:ti,ab,kw OR schoolchild*:ti,ab,kw OR infant*:ti,ab,kw OR girl*:ti,ab,kw OR boy*:ti,ab,kw OR teen:ti,ab,kw OR teens:ti,ab,kw OR teenager*:ti,ab,kw OR youth*:ti,ab,kw OR pediatr*:ti,ab,kw OR paediatr*:ti,ab,kw OR puber*:ti,ab,kw) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab,kw OR man:ti,ab,kw OR men:ti,ab,kw OR woman:ti,ab,kw OR women:ti,ab,kw)) |
1540 |
|
#4 |
#3 AND [2010-2024]/py |
1135 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1041707 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4061567 |
|
#7 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8299631 |
|
#8 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
15207176 |
|
#9 |
#4 AND #5 - SR |
89 |
|
#10 |
#4 AND #6 NOT #9 - RCT |
141 |
|
#11 |
#4 AND (#7 OR #8) NOT (#9 OR #10) - observationeel |
365 |
|
#12 |
#9 OR #10 OR #11 |
595 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Conversion Disorder/ or (conversion adj3 (disorder* or syndrome*)).ti,ab,kf. or (('functional neurologic*' or 'functional movement' or 'functional motor' or 'functional cognitive') adj3 disorder*).ti,ab,kf. or 'functional dizziness'.ti,ab,kf. or exp Psychogenic Nonepileptic Seizures/ or ((nonepileptic or 'non epileptic' or conversion or dissociative or hysteri* or psychogenic or functional) adj3 seizure*).ti,ab,kf. or pnes.ti,ab,kf. |
7665 |
|
2 |
Psychotherapy/ or exp Psychotherapy, Psychodynamic/ or psychotherap*.ti,ab,kf. or (somatic adj3 experiencing).ti,ab,kf. or ((body or psychosomatic) adj3 (therap* or intervention* or treat*)).ti,ab,kf. or exp Physical Therapy Modalities/ or exp Occupational Therapy/ or physiotherap*.ti,ab,kf. or 'physio therap*'.ti,ab,kf. or 'physical therap*'.ti,ab,kf. or kinesiotherap*.ti,ab,kf. or kinesitherapeutic*.ti,ab,kf. or 'occupation* therap*'.ti,ab,kf. or ergotherap*.ti,ab,kf. or 'graded exposure'.ti,ab,kf. or 'graded activit*'.ti,ab,kf. or 'graded physical activit*'.ti,ab,kf. or 'graded exercis*'.ti,ab,kf. or exp Hypnosis/ or hypnos*.ti,ab,kf. or hypnot*.ti,ab,kf. or hypnogenesis.ti,ab,kf. or mesmerism.ti,ab,kf. or exp Catalepsy/ or (induc* adj3 cataleps*).ti,ab,kf. or exp Cognitive Behavioral Therapy/ or (cognitive behavior* or cognitive behaviour* or CBT or CCBT or CBSM).ti,ab,kf. or exp Rehabilitation/ or rehabilitat*.ti,ab,kf. or "Patient Education as Topic"/ or Health Education/ or 'psycho education'.ti,ab,kf. or psychoeducation.ti,ab,kf. or (patient* adj3 educat*).ti,ab,kf. or exp "Rehabilitation of Speech and Language Disorders"/ or logoped*.ti,ab,kf. or ((speech or voice or vocal or language) adj3 (therap* or rehabilit* or reeducat* or train* or intervention*)).ti,ab,kf. |
936899 |
|
3 |
(1 and 2) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) not ((Adolescent/ or Child/ or Infant/ or adolescen*.ti,ab,kf. or child*.ti,ab,kf. or schoolchild*.ti,ab,kf. or infant*.ti,ab,kf. or girl*.ti,ab,kf. or boy*.ti,ab,kf. or teen.ti,ab,kf. or teens.ti,ab,kf. or teenager*.ti,ab,kf. or youth*.ti,ab,kf. or pediatr*.ti,ab,kf. or paediatr*.ti,ab,kf. or puber*.ti,ab,kf.) not (Adult/ or adult*.ti,ab,kf. or man.ti,ab,kf. or men.ti,ab,kf. or woman.ti,ab,kf. or women.ti,ab,kf.)) |
1006 |
|
4 |
limit 3 to yr="2010 -Current" |
597 |
|
5 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
757521 |
|
6 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2745782 |
|
7 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4765974 |
|
8 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5727424 |
|
9 |
4 and 5 - SR |
45 |
|
10 |
(4 and 6) not 9 - RCT |
100 |
|
11 |
(4 and (7 or 8)) not (9 or 10) - observationeel |
134 |
|
12 |
9 or 10 or 11 |
279 |
Ovid/PsycInfo
|
# |
Searches |
Results |
|
1 |
exp Conversion Disorder/ or (conversion adj3 (disorder* or syndrome*)).ti,ab,id. or exp Functional Neurological Disorder/ or (('functional neurologic*' or 'functional movement' or 'functional motor' or 'functional cognitive') adj3 disorder*).ti,ab,id. or 'functional dizziness'.ti,ab,id. or ((nonepileptic or 'non epileptic' or conversion or dissociative or hysteri* or psychogenic or functional) adj3 seizure*).ti,ab,id. or pnes.ti,ab,id. |
4082 |
|
2 |
Psychotherapy/ or exp Psychodynamic Psychotherapy/ or psychotherap*.ti,ab,id. or (somatic adj3 experiencing).ti,ab,id. or ((body or psychosomatic) adj3 (therap* or intervention* or treat*)).ti,ab,id. or exp Physical Therapy/ or exp Occupational Therapy/ or physiotherap*.ti,ab,id. or 'physio therap*'.ti,ab,id. or 'physical therap*'.ti,ab,id. or kinesiotherap*.ti,ab,id. or kinesitherapeutic*.ti,ab,id. or 'occupation* therap*'.ti,ab,id. or ergotherap*.ti,ab,id. or 'graded exposure'.ti,ab,id. or 'graded activit*'.ti,ab,id. or 'graded physical activit*'.ti,ab,id. or 'graded exercis*'.ti,ab,id. or Hypnosis/ or exp Hypnotherapy/ or hypnos*.ti,ab,id. or hypnot*.ti,ab,id. or hypnogenesis.ti,ab,id. or mesmerism.ti,ab,id. or exp Catalepsy/ or (induc* adj3 cataleps*).ti,ab,id. or exp Cognitive Behavior Therapy/ or (cognitive behavior* or cognitive behaviour* or CBT or CCBT or CBSM).ti,ab,id. or exp Rehabilitation/ or rehabilitat*.ti,ab,id. or exp Patient Education/ or Health Education/ or Mental Health Education/ or 'psycho education'.ti,ab,id. or psychoeducation.ti,ab,id. or (patient* adj3 educat*).ti,ab,id. or exp Speech Therapy/ or exp "Speech and Language Pathology"/ or exp Speech Language Pathology/ or logoped*.ti,ab,id. or ((speech or voice or vocal or language) adj3 (therap* or rehabilit* or reeducat* or train* or intervention*)).ti,ab,id. |
377605 |
|
3 |
1 and 2 |
699 |
|
4 |
limit 3 to yr="2010 -Current" |
394 |
|
5 |
((literature review or systematic review or meta analysis).md. or "literature review"/ or meta analysis/ or (((meta adj2 analy*) or metaanaly* or (synthes* adj2 (literature* or research* or studies or data)) or (pooled and analys*) or ((data adj1 pool*) and studies) or medline or medlars or embase or cinahl or scisearch or psychlit or psyclit or cinhal or cancerlit or cochrane or bids or pubmed or ovid or ((hand or manual or database* or computer*) adj1 search*) or (electronic adj1 (database* or data base or data bases))).ti,ab,id. or (review* or overview).ti. or (bibliograph* or relevant journals or ((review* or overview*) adj9 (systematic* or methodologic* or quantitativ* or research* or literature* or studies or trial* or effective*))).ab.)) not (((retrospective* or record* or case* or patient*) adj1 review*) or ((patient* or review*) adj1 chart*)).ti,ab,id. |
497477 |
|
6 |
exp clinical trial/ or randomized controlled trial/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
304051 |
|
7 |
Epidemiologic studies/ or case control studies/ or exp Cohort Analysis/ or Controlled Before-After Studies/ or Case control.tw. or cohort*.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ |
487505 |
|
8 |
4 and 5 - SR |
63 |
|
9 |
(4 and 6) not 8 - RCT |
40 |
|
10 |
(4 and 7) not (8 or 9) - observationeel |
54 |
|
11 |
8 or 9 or 10 |
157 |