Laboratoriumonderzoek bij alcoholmisbruik
Uitgangsvraag
Wat is de diagnostische waarde en accuratesse van biomarkers bij het aantonen van alcoholmisbruik in het kader van onderzoek naar rijgeschiktheid en wat zijn de te hanteren beslisgrenzen?
Aanbeveling
Deelvraag 1. Diagnostische waarde biomarkers alcoholmisbruik (vanuit de wettelijke kaders)
CDT en in mindere mate GGT zijn de meest geschikte laboratoriumparameters voor onderzoek naar alcoholmisbruik in het kader van rijgeschiktheidskeuringen.
Het meten van CDT is geschikt om met hoge mate van zekerheid alcoholmisbruik aan te tonen in het kader van onderzoek naar rijgeschiktheid. Voor kwantitatief onderzoek en bij hogere prevalentie, zoals bij onderzoek naar rijgeschiktheid, scoort CDT in vergelijking met andere algemeen gebruikte laboratoriumtesten het beste voor het opsporen van alcoholmisbruik. Aan de CDT-uitslag moet daarom de meeste bewijswaarde worden toegekend.
Gebruik geen CDT bij personen met een transferrine variant. Bij een variant kan soms op basis van een HPLC uitslag een geschatte CDT-waarde worden gemaakt, maar een geschatte waarde is onvoldoende betrouwbaar voor juridisch/forensisch gebruik.
De werkgroep is van mening dat het meten van GGT bijdraagt aan het opsporen van alcoholmisbruik bij onderzoek naar rijgeschiktheid. Een solitair verhoogde GGT (boven het afkappunt) vormt alleen een aanwijzing voor alcoholmisbruik als andere mogelijke oorzaken, waaronder leverpathologie of enzyminductie, aannemelijk zijn uitgesloten.
Deelvraag 2. Beslisgrenzen (afkappunten) voor CDT en GGT
CDT
Een CDT uitslag moet als CDTIFCC gerapporteerd worden. Op deze wijze krijgt de aanvrager een uitslag die gestandaardiseerd is op de officiële IFCC referentie methode.
Een CDT-uitslag groter dan 2,0% (het afkappunt), als enkelvoudige uitslag verkregen met een conform IFCC gestandaardiseerde methode of met de IFCC-referentiemethode, betekent een niet meer normale waarde, rekening houdend met de meetonzekerheid. Mits andere oorzaken aantoonbaar zijn uitgesloten kan een dergelijke CDT-uitslag dienen als bewijs voor alcoholmisbruik in de laatste weken.
Een uitslag hoger dan de bovengrens van het referentie interval (1,7%), maar lager of gelijk aan het afkappunt (2,0%) geldt niet als directe aanwijzing of bewijs voor alcoholmisbruik in de laatste weken.
GGT
Een GGT-uitslag groter dan 74 U/L voor mannen en groter dan 44 U/L voor vrouwen (de afkappunten), als enkelvoudige uitslag verkregen met de IFCC-methode bij 37°C of een daarop gestandaardiseerde methode, betekent een niet meer normale waarde, rekening houdend met de meetonzekerheid. Mits andere oorzaken aantoonbaar zijn uitgesloten, kan een dergelijke GGT-uitslag dienen als aanwijzing voor alcoholmisbruik.
Een uitslag hoger dan de bovengrens van het referentie interval (68 U/L voor mannen en 40 U/L voor vrouwen), maar lager of gelijk aan het afkappunt (74 U/L voor mannen en 44 U/L voor vrouwen) geldt niet als aanwijzing voor alcoholmisbruik in de laatste weken.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Bij de herziening van 2025 is een systematische literatuursearch uitgevoerd. Net als in 2020 is de kwaliteit van de gevonden evidence zeer laag, vooral door grote variatie in studieopzet (inclusiecriteria, populaties, zelfgerapporteerde referentiestandaarden en afkappunten). De werkgroep concludeert dat er geen doorslaggevend nieuw bewijs is en baseert de aanbevelingen voornamelijk op eerdere literatuur en expert opinion. Belangrijk is dat in 2024 de Joint Committee for Traceability in Laboratory Medicine (JCTLM) de IFCC_HPLC_referentiemethode voor CDT formeel erkend heeft. Resultaten die hiernaar zijn gestandaardiseerd worden gerapporteerd als CDTIFCC, met een bovengrens van 1,7 % en een afkappunt van 2,0 (Wielders, 2024).
De nieuw toegevoegde aanbevelingen (m.b.t. transferrine variant) zijn geformuleerd op basis van expert opinie.
Literatuursamenvatting 2020
Vier studies die geïncludeerd werden in de literatuursamenvatting van 2020 rapporteerden een of meerdere diagnostische accuratesse uitkomstmaten voor CDT en GGT. Zowel CDT als GGT hadden een matig tot hoge AUC en een hoge specificiteit. De sensitiviteit was CDT was laag, en de sensitiviteit van GGT was laag tot matig (tabel 1). Zie voor meer details de richtlijn Alcoholmisbruik in het kader van rijgeschiktheidskeuringen 2020, opvraagbaar bij de Nederlandse Vereniging voor Psychiatrie.
Tabel 1. Resultaten literatuuranalyse 2019
|
|
AUC |
Specificiteit |
Sensitiviteit |
|
CDT |
0.75 tot 0.831, 2, 3, 4 (matig tot hoog) |
0.91 tot 0.961, 4 |
0.36 tot 0.511, 4 |
|
GGT |
0.61 tot 0.831, 2, 3, 4 (matig tot hoog) |
0.80 tot 0.813, 4 |
0.30 ot 0.663, 4 |
|
|||
Literatuursamenvatting 2025
Drie studies uit de systematische search uitgevoerd in 2025 rapporteerden de diagnostische accuratesse van CDT: O’Flaherty (2022), Aboutara (2022), en Archer (2019), zie voor meer details bij onderdeel Zoeken en selecteren en Samenvatting van de literatuur. O’Flaherty gebruikte CE CDT met een afkappunt van 1.6%, Aboutara (2022) gebruikte CDT-HPLC met een afkapwaarde van 1.7%, en Archer (2019) gebruikte N-Latex CDT met een afkappunt van 2.5%. O’Flaherty (2022) en Archer (2019) bepaalden daarnaast de diagnostische acuratesse van GGT. De gebruikte afkappunten waren 73 IU/L voor mannen en 38 IU/L voor vrouwen (O’Flaherty, 2022), en 60 IU/L voor mannen en 40 IU/L voor vrouwen (Archer, 2019). Voor alle bepalingen werd zelf-gerapporteerde alcoholconsumptie als referentiestandaard gebruikt. In de studies werden de volgende waarden gevonden voor de diagnostische accuratesse uitkomstmaten:
- Specificiteit: 45.7% tot 99.5% (laag tot hoog) voor CDT en 91% voor GGT (hoog).
- AUC: 0.65 tot 0.71 voor CDT (matig) en 0.66 tot 0.75 voor GGT (matig).
- Sensitiviteit: 8.0% tot 87.5% voor CDT (laag tot hoog) en 18.2% tot 40.0% voor GGT (laag).
- Positief voorspellende waarde: 35.9% tot 55.2% voor CDT (laag) en 18.8% tot 35.1% voor GGT (laag).
- Negatief voorspellende waarde: 82.7% tot 94.5% voor CDT (hoog) en 80.6% tot 95.5% voor GGT (hoog).
- LR+: 1.6 tot 15.8 voor CDT (laag tot hoog) en 2.0 tot 3.7 voor GGT (matig).
- LR-: 0.9 tot 0.3 voor CDT (laag tot matig) en 0.9 tot 0.8 voor GGT (laag)
Deelvraag 1 - Diagnostische waarde biomarkers alcoholmisbruik
Area Under the Curve (AUC)
De gevonden AUC-waardes in de geïncludeerde studies in de literatuursamenvatting van 2020 ((Bergström, 2008; Kharbouche, 2012; McDonald, 2013; Pirro, 2011)) varieerden. Dit komt mede door verschillen in het uitgevoerde labonderzoek, populatie verschillen (populaties met continue verdeling versus bimodale of trimodale populaties), referentiemethode zoals een interview of alcoholdagboekje en gehanteerde definities van drinkgedrag. Ook is zelf-gerapporteerd drinkgedrag gevoelig voor het geven van sociaal wenselijke antwoorden wat leidt tot rapportagebias. Toch wordt ervan uitgegaan dat ondanks een onderrapportage er wel onderscheid te maken is tussen mensen die heel veel drinken en mensen die weinig drinken.
Een AUC rond 0,6 of lager betekent ongeschiktheid van de marker, indien de studie correct is opgezet.
CDT bleek na literatuuronderzoek in de Richtlijn uit 2020 binnen de groep CDT, MCV, GGT, ASAT, ALAT het meest geschikt om recidieven te voorspellen van alcoholgebruik door automobilisten (Maenhout, 2014). De overige parameters scoorden nauwelijks beter dan willekeurig positief/negatief. In de algemene populatie en vergelijkende studies (op basis van ROC) met de traditionele biomarker GGT (en MCV of ASAT en ALAT) scoort CDT het beste, zoals onder meer uit de AUC-waarden blijkt (zie tabel 6.1). Vanaf 2008 is bij de standaardisatie van de methode nadrukkelijk gekozen voor de meting van de disialo- transferrine fractie. Die keuze en inzet van modernere methodes sindsdien verhoogde ook de specificiteit.
Het gebruik van CDT metingen bij personen met een transferrinevariant wordt afgeraden, omdat het percentage CDT (%CDT) niet nauwkeurig bepaald kan worden met behulp van HPLC of CE. Bij het gebruik van de N-Latex-methode voor het bepalen van %CDT is de juistheid bij transferrinevarianten nog onvoldoende onderzocht en schattingen volstaan juridisch niet.
Aangezien er een gebrek is aan studies bij personen met een transferrinevariant, waarin CDT wordt gemeten met zowel CE, HPLC én N-Latex, wordt aanbevolen om in deze gevallen gebruik te maken van directe biomarkers zoals EtG (korte termijn alcoholgebruik) of PEth (lange termijn alcoholgebruik) met dien verstande dat hiervoor nog geen universeel geaccepteerde afkappunten beschikbaar zijn.
Comorbiditeit
De ideale biomarker wordt niet of nauwelijks beïnvloed door comorbiditeit. Vaak worden bij studies van biomarkers voor alcoholisme de populaties opgeschoond voor andere pathologie zoals diabetes, hetgeen ten opzichte van de algemene populaties de resultaten kan beïnvloeden.
Comorbiditeit CDT
Een licht verhoogde waarde van CDT kan ook voorkomen bij ‘endstage’ leverziekten, bij sterk verlaagde transferrineconcentraties (Latex methode), bij een levercarcinoom (Arndt, 2001; Fleming, 2004; Bortolotti, 2006; Bergström CCA, 2008) en in de tweede helft van de zwangerschap (Kenan, 2011; Gottgens, 2024). Bij de tweede helft van de zwangerschap gelden hogere referentiewaarden voor CDT en dus ook een hoger afkappunt. Raadpleeg de laboratoriumspecialist. Bij studies met de N-Latex methode werd door sommigen een verminderde respons voor CDT gemeld bij vrouwen (Whitfield, 2008, Kok, 2015), dat kan ook te maken hebben met onderrapportage van het alcoholgebruik. Leeftijd is ook genoemd als factor (jongere mensen verwerken alcohol sneller) of geslacht (vrouwen hebben een lagere respons dan mannen), echter in een uitgebreide studie met de HPLC-methode was er geen significant verschil aantoonbaar voor geslacht, leeftijd, roken of BMI (Bergström, 2008) (zie ook bijlage Achtergronden bij de waarde van GGT als biomarker (2025)). Het voedingspatroon, frequent voorkomende ziektebeelden en het gebruik van de meest voorkomende geneesmiddelen in de huisartsenpraktijk blijken geen effect op de CDT-bepaling te hebben (Meerkerk, 1998; Fleming, 2004).
Comorbiditeit GGT
De waarde van GGT in het bloed kan ook verhoogd zijn door andere oorzaken. Er is een breed scala van klinische aandoeningen, die leiden tot een significant verhoogde GGT-waarde. Daarnaast geven leefstijl of omgevingsfactoren als roken of contact met xenobiotica verhoogde GGT-waarden terwijl ruim gebruik van koffie de GGT-waarde weer aanzienlijk kan doen dalen (zie ook bijlage Achtergronden bij de waarde van GGT als biomarker (2025)). Tabel 6.3 biedt een overzicht van voornaamste oorzaken van een verhoogde GGT-waarde.
Tabel 6.3 Voornaamste oorzaken verhoogd GGT
|
Galweg obstructie (galstenen, leververvetting) |
|
Enzym inductie (alcohol, geneesmiddelen en xenobiotica, zie onderaan deze tabel) |
|
Hepatitis (viraal, toxisch, alcoholisch), mononucleosis infectiosa |
|
Lever pathologie (cirrhose, tumor) |
|
Pancreas pathologie |
|
Chronische nierziekten |
|
Cardiovasculaire ziekten (leverstuwing/hartfalen, post AMI, hypertensie) |
|
Kanker (borst, prostaat, longen etc) |
|
Diabetes |
|
Colitis |
|
Hemochromatose |
|
Hodgkin & Non-Hodgkin |
|
Orale anticonceptie |
Enzyminductie leidt tot een maximaal twee a drievoudige GGT-verhoging ten opzichte van bovengrens normaal, naast alcohol moeten genoemd worden:
- Geneesmiddelen, waaronder barbituraten, psychofarmaca, statines, antidepressiva, fenytoïne, carbamazepine, rifampicine, antireumatica, MAO-remmers, anabole steroïden, thiazide diuretica, cytostatica, streptokinase, hoge paracetamol doses, NSAIDs, antibiotica, antifungica (voor een uitgebreide lijst raadpleeg Wu, 2006).
- Xenobiotica, waaronder oplosmiddelen als tetra, pesticiden.
Populatie
Studies worden idealiter uitgevoerd in de algemene populatie of bij mensen die worden uitgenodigd voor onderzoek naar rijgeschiktheid. Bergström en McDonald komen met hun selectie uit de algemene populatie het dichtste bij de werkelijke populatie in het kader van onderzoek naar rijgeschiktheid. Waar mogelijk is gekeken naar de discriminatie tussen ‘normaal’ en ‘at risk’ gebruik.
Aanvullend zijn ook effecten bekend van kunstmatige bimodale of trimodale populatie mixen, die door de eigenschappen van de subpopulatie het discriminerend vermogen van de biomarkers onjuist kunnen beïnvloeden (Wolff; Wielders, 2024).
Nieuwe biomarkers
Naast de oude indirecte biomarkers als MCV, GGT, ASAT en ALAT (indirecte verhoging door cel schade of metabolisme storing na alcoholmisbruik) en de relatief nieuwe marker CDT trekken vooral de nieuwe directe biomarkers (alcohol metabolieten) in bloed, urine en haar-monsters de aandacht.
Voorbeelden van directe biomarkers zijn ethylglucuronide (EtG) in bloed en urine, fosfatidylethanol (PEth) in bloed en EtG of vetzure ethylesters (FAEES) in haar. Een technische belemmering is dat het meten van de nieuwste biomarkers gecompliceerd is en daardoor buiten het bereik van veel laboratoria valt. Eveneens belangrijk is dat voor onderzoek naar alcoholmisbruik in het kader van rijgeschiktheidskeuringen (dus voor forensisch gebruik) naast een goed gevalideerde methode ook terdege onderbouwde en geaccepteerde grenzen aanwezig moeten zijn. Aangezien dit nog niet het geval is, worden PEth, EtG in urine of haaranalyse buiten beschouwing gelaten in deze Richtlijn (een korte toelichting wordt gegeven in bijlage PEth en andere nieuwe biomarkers voor overmatig alcoholgebruik (2025)). EtG in urine kan aanvullend bewijs opleveren voor alcoholgebruik in de voorafgaande 1-3 dagen. Dat is vooral forensisch van belang maar past niet direct bij het huidige CBR beleid van toetsen op voortduren van chronisch gebruik. Haaranalyse is nog helemaal niet gestandaardiseerd en kan alleen werken voor inzichten over gebruik over langere perioden van weken-maanden. Voor PEth analyse in volbloed zijn er wel voorstellen maar nog geen consensus. Het meten van alcohol in bloed of in adem wordt niet ingezet bij onderzoek naar alcoholmisbruik in het kader van rijgeschiktheidskeuringen en valt daarmee buiten het bestek van deze Richtlijn.
Deelvraag 2 - Beslisgrenzen (afkappunten) voor CDT en GGT
Overwegingen bij CDT
Sinds 2020 zijn de resultaten van alle in Nederland toegelaten methoden gestandaardiseerd, dat wil zeggen herleidbaar naar de IFCC HPLC referentiemethode en leveren daardoor, voor hetzelfde monster, vergelijkbare resultaten. De NVKC hanteert de aanbevolen IFCC-bovengrens van het 95% referentiegebied (Schellenberg, 2017) van 1,7% voor de HPLC-referentiemethode, de meetonzekerheid van 0,3 procentpunt en het afkappunt (beslisgrens) van 2,0% voor forensisch gebruik, waaronder begrepen onderzoek naar rijgeschiktheid. Het afkappunt 2,0% is dus de hoogste waarde die nog voor kan komen bij de normale populatie, rekening houdend met de meetonzekerheid.
Bij twijfel of bij dispuut van een uitslag gevonden met een commerciële methode, moet de IFCC-referentiemethode (HPLC volgens Helander, 2003) worden ingezet. De uitslag van de referentiemethode is doorslaggevend. Rapportage van CDT-resultaten met de IFCC-referentiemethode of met een daarop gestandaardiseerde commerciële methode is herkenbaar door gebruik van de aanduiding CDTIFCC. Met de introductie van de CDTIFCC is het gebruiken van methode afhankelijke bovengrenzen en afkappunten verleden tijd geworden. De IFCC-standaardisatie, de bijbehorende bovengrens en het afkappunt zijn met ingang van 2019 overgenomen door het CBR (zie brief CBR aan laboratoria d.d. 14 december 2018). Daarmee ligt vast dat sensitiviteit, specificiteit en diagnostische accuratesse gekoppeld moet zijn aan een CDTIFCC afkappunt van 2,0%. Het hoogste internationale orgaan voor referentiemethoden en methode standaardisatie JCTLM heeft begin 2024 de IFCC HPLC methode als referentie methode erkend.
Overwegingen bij GGT
De GGT-activiteit in serum of plasma wordt gemeten met een colorimetrische methode en glutamyl-carboxy p-nitroanalide als substraat. Aanbevolen wordt de IFCC-methode bij 37°C, dan wel een methode die hiertegen is gestandaardiseerd. Ingevroren monsters zijn een jaar stabiel bij -20°C.
Wat betreft beslisgrenzen wordt voor GGT uitgegaan van de bovengrens van normaal volgens internationaal IFCC-referentiegebieden onderzoek. Daar bovenop komt voor forensisch gebruik, waaronder inbegrepen onderzoek naar rijgeschiktheid, een gepubliceerde marge voor de meetonzekerheid. Voor de IFCC-methode, uitgevoerd bij 37°C is uitgegaan van internationaal referentie-interval onderzoek (Ceriotti, 2010) plus de meetonzekerheid (9% volgens Zhou, 2018). Ceriotti (2010) vond een referentie interval van 12-68 U/L voor mannen, met 9% meetonzekerheid erbij wordt het afkappunt dan 74 U/L. Voor vrouwen werd een referentie interval van 6-40 U/L gevonden, met 9% meetonzekerheid erbij opgeteld wordt het afkappunt dan 44 U/L.
Deelvraag 3 - Wat is de diagnostische accuratesse van de biomarkers CDT en GGT?
Doel bij onderzoek naar rijgeschiktheid is om met grote mate van zekerheid chronisch overmatig gebruik aan te tonen of uit te sluiten. Bij dergelijke forensische metingen is het van belang om het aantal fout-positieven laag te houden. Zowel voor GGT als voor CDT zijn de diagnostische prestaties bij de in deze richtlijn aanbevolen afkappunten zodanig dat er sprake is van een hoge specificiteit en een lage sensitiviteit(1).
1. De sensitiviteit van een test is het percentage terecht positieve uitslagen onder personen die alcohol misbruiken. De specificiteit van een test is het percentage terecht negatieve testuitslagen onder de personen die geen alcohol misbruiken. Hoe hoger de specificiteit is, hoe beter de test mensen die geen alcohol misbruiken als negatief aanwijst. Een test met lage specificiteit geeft aan veel gezonde/normale deelnemers een afwijkende/te hoge uitslag. Bij onderzoek naar rijgeschiktheid zou dat betekenen dat veel verkeersdeelnemers onterecht de conclusie alcoholmisbruik zouden krijgen, hetgeen ongewenst is. Daarom is het afkappunt verhoogd om de kans op dergelijke fout positieve uitslagen laag te houden.
(Evidence to decision framework)
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Het type laboratoriumonderzoek wat wordt uitgevoerd betreft geen voorkeursgevoelige beslissing. Dit onderdeel van het evidence to decision framwork is daarmee niet van toepassing binnen dit hoofdstuk.
Kostenaspecten
Kostenaspecten spelen bij laboratoriumonderzoek naar alcoholmisbruik in het kader van rijgeschiktheid geen rol die van invloed op de aanbevolen testen. De kosten van het laboratoriumonderzoek met testen zoals GGT en CDT zijn daarnaast verwaarloosbaar ten opzichte van de overige kosten bij rijgeschiktheidskeuringen. PEth wordt wegens gebrek aan standaardisering niet aanbevolen door de werkgroep, ook merkt de werkgroep op dat de kosten voor PEth significant hoger zijn.
Aanvaardbaarheid: Ethische aanvaardbaarheid en duurzaamheid
Ethische aspecten en duurzaamheid spelen bij laboratoriumonderzoek naar alcoholmisbruik in het kader van rijgeschiktheid geen rol die van invloed is op de aanbevolen testen.
Haalbaarheid
Het is niet de verwachting dat de aanbevelingen tot een toename van het aantal jaarlijkse testen zal leiden. Het beslag op middelen en menskracht lijkt gezien de verwachte gezondheidswinst aanvaardbaar. De diagnostiek is over het algemeen al standaard zorg in de praktijk. De werkgroep voorziet daarom geen belemmeringen rondom praktische, technische, juridische en logistieke aspecten.
Onderbouwing
Volgens de Nederlandse regelgeving wordt laboratoriumonderzoek dat deel uitmaakt van de rijgeschiktheidsonderzoeken die door het Centraal Bureau Rijvaardigheidsbewijzen (CBR) worden voorgeschreven, aangevraagd door een psychiater en uitgevoerd in medische laboratoria die ISO 15189-accreditatie hebben (of een gelijkwaardig internationaal erkend kwaliteitssysteem) en deelnemen aan externe kwaliteitsbeoordelingsprogramma’s (EQAS). Dergelijk onderzoek is bedoeld om chronisch overmatig alcoholgebruik te bevestigen of uit te sluiten en om objectief bewijs te leveren wanneer een klinisch interview of zelfrapportage mogelijk onbetrouwbaar is; het is niet ontworpen om zeer recent alcoholgebruik aan te tonen.
De serumbiomarkers die in deze context momenteel bewezen diagnostische waarde hebben, zijn carbohydrate-deficient transferrin (CDTIFCC) en gamma-glutamyltransferase (GGT).
In 2020 zijn mean corpuscular volume (MCV), aspartaataminotransferase (AST), alanineaminotransferase (ALT) en de bijbehorende hematologie-indices (hemoglobine, hematocriet, erytrocyten) uit het protocol verwijderd: zij leveren geen aanvullende diagnostische informatie bovenop CDT en GGT en vertonen een lage sensitiviteit en specificiteit voor chronisch alcoholmisbruik.
Inleiding deelvraag 1 - Diagnostische waarde biomarkers alcoholmisbruik
Bij een vergelijking van biomarkers naar alcoholmisbruik wordt gekeken naar besliskundige parameters als sensitiviteit en specificiteit, bij voorkeur met gebruik van ROC curves. Het niveau van de biomarker in het bloed wordt meestal vergeleken met zelf-gerapporteerde alcoholinname. Er zijn te weinig studies bekend waarbij aan grotere groepen gedocumenteerd verschillende hoeveelheden alcohol werd toegediend en vervolgens de respons werd gemeten.
Naar aanleiding van een systematische search in 2018 is naar voren gekomen dat CDT en in mindere mate GGT de meest geschikte laboratoriumparameters zijn voor een beoordeling van alcoholmisbruik in het kader van onderzoek naar rijgeschiktheid (zie ‘Literatuursamenvatting module ‘Laboratoriumonderzoek’ uit de Richtlijn 2020, opvraagbaar bij de Nederlandse Vereniging voor Psychiatrie). Hier gaan we nader in op de diagnostische accuratesse van deze biomarkers bij de in deze Richtlijn voorgestelde afkappunten. MCV, ASAT en ALAT hebben een te lage diagnostische accuratesse en zijn daarom niet meer toegelaten in het kader van CBR keuringen. Hiervoor verwijst de werkgroep naar de literatuursamenvatting en Richtlijntekst uit 2020 (zie Richtlijn Alcoholmisbruik in het kader van rijgeschiktheidskeuringen 2020, opvraagbaar bij de Nederlandse Vereniging voor Psychiatrie).
Zelfgerapporteerde alcoholinname is onderhevig aan verschillende vormen van bias. In het kader van de literatuursamenvatting heeft de werkgroep echter moeten kiezen voor zelfgerapporteerde alcoholinname als referentiestandaard bij het beoordelen van de diagnostische accuratesse. Er is naar gestreefd om studies van voldoende power te includeren die zo dicht mogelijk bij de doelpopulatie komen.
Inleiding deelvraag 2 - Beslisgrenzen (afkappunten) voor CDT en GGT
Bij het gebruik van biomarkers is het noodzakelijk om klinische ijkpunten te definiëren. De psychiatrische criteria t.a.v. alcoholmisbruik zijn echter niet direct te vertalen naar een corresponderend niveau van een biomarker. Als alternatief wordt daarom gekozen om de normale populatie vast te stellen plus de meetfout om met zekerheid vast te kunnen stellen wanneer iemand daarbuiten valt. Rekening houden met de meetfout gebeurt eveneens bij onderzoek naar aanwezigheid van alcohol of drugs in bloed.
Bij de medische interpretatie van laboratoriumonderzoek wordt een uitslag doorgaans vergeleken met een grenswaarde zoals de bovengrens van een 'referentiegebied'. Een referentie gebied (of referentie interval) werd vroeger ook het normaalwaarde gebied genoemd. Het referentiegebied wordt gedefinieerd als de centrale waarden die met 95% van de gezonde populatie corresponderen, d.w.z. 2,5% van de gezonden valt boven de bovengrens en 2,5% van de gezonden valt beneden de ondergrens.
Gebruik van deze 95%-referentiegebied bovengrens, zonder rekening te houden met de meetfout, leidt tot een significant percentage fout positieven, hetgeen ongewenst is voor juridische of forensische zaken. Verder is de bovengrens van een normale populatie zeker niet hetzelfde als de ondergrens van een bewezen stoornis.
Daarom wordt gewerkt met een afkappunt waarboven afwijkend alcoholgebruik zeer waarschijnlijk is. Dit afkappunt is afgeleid op basis van wetenschappelijk onderzoek en corrigeert voor zowel analytische als biologische variatie. Voor CDT is dit afkappunt vastgesteld op 2,0 %; bij een enkelvoudige meting boven deze waarde kan met 95 % zekerheid worden gesteld dat de uitslag niet uit de normale populatie afkomstig is.
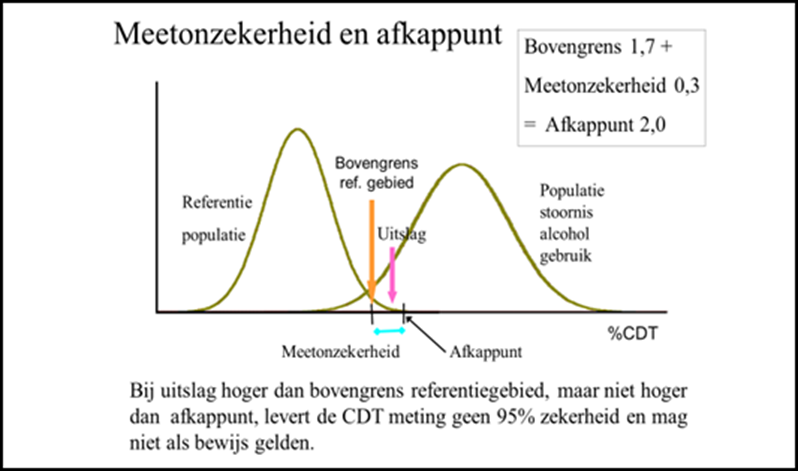
Figuur 6.1 Meetonzekerheid en afkappunt CDT
Bij interpretatie moet naast de biomarkerwaarde altijd rekening worden gehouden met eventuele verstorende comorbiditeit (zie overwegingen onder deelvraag 1), alsook met monstertransport‑ en opslagcondities.
Het doel van het laboratoriumonderzoek in het kader van rijgeschiktheid is het met hoge mate van zekerheid aantonen of uitsluiten van chronisch overmatig alcoholgebruik; het onderzoek is niet bedoeld voor het aantonen van recent alcoholgebruik.
Summary of Findings
Diagnostic accuracy of CDT and GGT
Population: Individuals referred to psychiatry due to suspected alcohol abuse in traffic/driving under influence (DUI)
Index and comparator test: CDT (CDT-HPLC, CE CDT, N-Latex CDT), GGT
Reference test: Actual reported alcohol intake based on self-report/audit
|
Outcome |
Study results and measurements
|
Certainty of the Evidence (Quality of Evidence) |
Summary |
|||
|
|
CDT |
GGT |
CDT |
GGT |
CDT |
GGT |
|
Specificity (critical) |
Aboutara, 2022: 45.7% (95% CI 30.9 to 61.0%)
O’Flaherty, 2022: 99.5% (95% CI 98.7 to 99.9%)1
O’Flaherty, 2022: 94.4% (95% CI 92.1 to 96.2%)2
Range: 45.7% to 99.5%
Prevalence (range): 6% to 26%
Based on data from 1578 participants in 2 studies |
O’Flaherty, 2022: 91.2% (95% CI 89.1 to 93.1%)1
O’Flaherty, 2022: 91.0% (95% CI 88.3 to 93.3%)2
Prevalence (range): 6% to 21%
Based on data from 1516 participants in 1 study |
Very low |
Very low
|
The evidence is very uncertain regarding the specificity of CDT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Aboutara, 2022; O’Flaherty, 2022) |
The evidence is very uncertain regarding the specificity of GGT (determined using self-reported alcohol consumption as reference standard) in the study population.
(O’Flaherty, 2022) |
|
AUC (critical) |
Archer, 2019: 0.68
O’Flaherty, 2022: 0.65 (95% CI 0.56 to 0.74)1
O’Flaherty, 2022: 0.71 (95% CI 0.66 to 0.76)2
Range: 0.65 to 0.71
6% to 20%
Based on data from 1718 participants in 2 studies |
Archer, 2019: 0.66
O’Flaherty, 2022: 0.75 (95% CI 0.68 to 0.82)1
O’Flaherty, 2022: 0.70 (95% CI 0.65 to 0.75)2
Range: 0.66 to 0.75
Prevalence (range): 6% to 20%
Based on data from 1718 participants in 2 studies |
Very low Due to very serious risk of bias, due to serious imprecision, due to indirectness5 |
Very low Due to very serious risk of bias, due to serious imprecision, due to indirectness6 |
The evidence is very uncertain regarding the AUC of CDT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Archer, 2019; O’Flaherty, 2022)
|
The evidence is very uncertain regarding the AUC of GGT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Archer, 2019; O’Flaherty, 2022)
|
|
Sensitivity (important) |
Aboutara, 2022: 87.5% (95% CI 61.7 to 98.5%)
Archer, 2019: 16.0%
O’Flaherty, 2022: 8.0% (95% CI 2.2 to 19.2%)1
O’Flaherty, 2022: 25.9% (95% CI 18.9 to 33.9%)2
Range: 8.0% to 87.5%
Prevalence (range): 6% to 26%
Based on data from 1780 participants in 3 studies |
Archer, 2019: 40.0%
O’Flaherty, 2022: 32.0% (95% CI 19.5 to 46.7%)1
O’Flaherty, 2022: 18.2% (95% CI 12.2 to 25.5%)2
Range: 18.2% to 40.0%
Prevalence (range): 6% to 20%
Based on data from 1718 participants in 2 studies |
Very low |
Very low Due to very serious risk of bias, due to indirectness8 |
The evidence is very uncertain regarding the sensitivity of CDT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Aboutara, 2022; Archer, 2019; O’Flaherty, 2022) |
The evidence is very uncertain regarding the sensitivity of GGT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Archer, 2019; O’Flaherty, 2022)
|
|
Positive predictive value (important) |
Aboutara, 2022: 35.9% (95% CI 28.8 to 43.6%)
O’Flaherty, 2022: 50.0% (95% CI 20.5 to 79.5%)1
O’Flaherty, 2022: 55.2% (95% CI 44.2 to 65.8%)2
Range: 35.9% to 55.2%
Prevalence (range): 6% to 26%
Based on data from 1578 participants in 2 studies |
O’Flaherty, 2022: 18.8% (95% CI 12.7 to 26.9%)1
O’Flaherty, 2022: 35.1% (95% CI 25.9 to 45.7%)2
Prevalence (range): 6% to 21%
Based on data from 1516 participants in 1 study |
Very low |
Very low |
The evidence is very uncertain regarding the positive predictive value of CDT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Aboutara, 2022; O’Flaherty, 2022) |
The evidence is very uncertain regarding the positive predictive value of GGT (determined using self-reported alcohol consumption as reference standard) in the study population.
(O’Flaherty, 2022) |
|
Negative predictive value (important) |
Aboutara, 2022: 91.3% (95% CI 73.4 to 97.6%)A
O’Flaherty, 2022: 94.5% (95% CI 94.0 to 94.9%)1
O’Flaherty, 2022: 82.7% (95% CI 81.2 to 84.0%)2
Range: 82.7% to 94.5%
Prevalence (range): 6% to 26%
Based on data from 1578 participants in 2 studies |
O’Flaherty, 2022: 95.5% (95% CI 94.6 to 96.2%)1
O’Flaherty, 2022: 80.6% (95% CI 79.3 to 81.9%)2
Prevalence (range): 6% to 21%
Based on data from 1516 participants in 1 study |
Very low |
Very low |
The evidence is very uncertain regarding the negative predictive value of CDT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Aboutara, 2022; O’Flaherty, 2022) |
The evidence is very uncertain regarding the negative predictive value of GGT (determined using self-reported alcohol consumption as reference standard) in the study population.
(O’Flaherty, 2022) |
|
LR+ (important) |
Aboutara, 2022: 1.6 (95% CI 1.2 to 2.2)
O’Flaherty, 2022: 15.8 (95% CI 4.1 to 61.2)1
O’Flaherty, 2022: 4.6 (95% CI 3.0 to 7.2)2
Range: 1.6 to 15.8
Prevalence (range): 6% to 26%
Based on data from 1578 participants in 2 studies |
O’Flaherty, 2022: 3.7 (95% CI 2.3 to 5.8)1
O’Flaherty, 2022: 2.0 (95% CI 1.3 to 3.2)2
Prevalence (range): 6% to 21%
Based on data from 1516 participants in 1 study |
Very low |
Very low |
The evidence is very uncertain regarding the LR+ of CDT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Aboutara, 2022; O’Flaherty, 2022)
|
The evidence is very uncertain regarding the LR+ of GGT (determined using self-reported alcohol consumption as reference standard) in the study population.
(O’Flaherty, 2022) |
|
LR- (important) |
Aboutara, 2022: 0.3 (95% CI 0.1 to 1.0)
O’Flaherty, 2022: 0.9 (95% CI 0.9 to 1.0)1
O’Flaherty, 2022: 0.8 (95% CI 0.7 to 0.9)2
Range: 0.9 to 0.3
Prevalence (range): 6% to 26%
Based on data from 1578 participants in 2 studies |
O’Flaherty, 2022: 0.8 (95% CI 0.6 to 0.9)1
O’Flaherty, 2022: 0.9 (95% CI 0.8 to 1.0)2
Prevalence (range): 6% to 21%
Based on data from 1516 participants in 1 study |
Very low |
Very low |
The evidence is very uncertain regarding the LR- of CDT (determined using self-reported alcohol consumption as reference standard) in the respective study populations.
(Aboutara, 2022; O’Flaherty, 2022)
|
The evidence is very uncertain regarding the LR- of GGT (determined using self-reported alcohol consumption as reference standard) in the study population.
(O’Flaherty, 2022) |
|
Summary of literature written in 2019 |
||||||
|
AUC |
Bergström, 2008: 0.832
Bergström, 2008: 0.821
Kharbouche, 2012: 0.80
McDonald, 2013: 0.75
Pirro, 2011: 0.77
Range: 0.75 to 0.83
Prevalence (range): 24% to 34%
Based on data from 2710 participants in 4 studies |
Bergström, 2008: 0.69
Kharbouche, 2012: 0.76
McDonald, 2013: 0.61
Pirro, 2011: 0.83
Range: 0.61 to 0.83
Prevalence (range): 24% to 34%
Based on data from 2710 participants in 4 studies |
Low Due to serious risk of bias, due to indirectness17 |
Low Due to serious risk of bias, due to indirectness18 |
The AUC of CDT may be moderate to high in the respective study populations.
(Bergström, 2008; Kharbouche, 2012; McDonald, 2013; Pirro, 2011) |
The AUC of GGT may be moderate to high in the respective study populations.
(Bergström, 2008; Kharbouche, 2012; McDonald, 2013; Pirro, 2011) |
|
Specificity |
Bergström, 2008: 96%
Pirro, 2011: 91%
Range: 91% to 96%
Prevalence (range): 24% to 34%
Based on data from 1562 participants in 2 studies |
McDonald, 2013: 80%
Pirro, 2011: 81%
Range: 80% to 81%
Prevalence (range): 34% (only reported for Pirro, 2011)
Based on data from 1198 participants in 2 studies |
Low Due to serious risk of bias, due to indirectness19 |
Low Due to serious risk of bias, due to indirectness20 |
The specificity of CDT may be high in the respective study populations.
(Bergström, 2008; Pirro, 2011) |
The specificity of GGT may be high in the respective study populations.
(McDonald, 2013; Pirro, 2011) |
|
Sensitivity |
Bergström, 2008: 36%
Pirro, 2011: 51%
Range: 36% to 51%
Prevalence (range): 24% to 34%
Based on data from 1562 participants in 2 studies |
McDonald, 2013: 30%
Pirro, 2011: 66%
Range: 30% to 66%
Prevalence (range): 34% (only reported for Pirro, 2011)
Based on data from 1198 participants in 2 studies |
Low Due to serious risk of bias, due to indirectness21 |
Very low Due to serious risk of bias, due to inconsistency, due to indirectness22 |
The sensitivity of CDT may be low in the respective study populations.
(Bergström, 2008; Pirro, 2011)
|
The evidence is very uncertain regarding the sensitivity of GGT in the respective study populations.
(McDonald, 2013; Pirro, 2011) |
1. Value in women
2. Value in men
3. Risk of bias: very serious (-2 levels). It is unclear whether the results of the index test and reference test were interpreted independently. The reference test (self-reported alcohol consumption) poses high risk of bias. Inconsistency: serious (-1 level). The difference between the results of the studies is large. Indirectness: serious (-1 level). Population is different from the DUI context.
4, 8, 10, 11, 12, 14, 16. Risk of bias: very serious (-2 levels). It is unclear whether the results of the index test and reference test were interpreted independently. The reference test (self-reported alcohol consumption) poses high risk of bias. Indirectness: serious (-1 level). Population is different from the DUI context.
5, 6, 9. Risk of bias: very serious (-2 levels). It is unclear whether the results of the index test and reference test were interpreted independently. The reference test (self-reported alcohol consumption) poses high risk of bias. Imprecision: serious (-1 level). Confidence intervals are wide. Indirectness: serious (-1 level). Population is different from the DUI context.
7, 13, 15. Risk of bias: very serious (-2 levels). It is unclear whether the results of the index test and reference test were interpreted independently. The reference test (self-reported alcohol consumption) poses high risk of bias. Inconsistency: serious (-1 level). Difference between results of the studies is large. Imprecision: serious (-1 level). Confidence intervals are wide. Indirectness: serious (-1 level). Population is different from the DUI context.
17,18, 19, 20, 21. Risk of bias: serious (-1 level). The reference test poses high risk of bias. Indirectness: serious (-1 level). Population is different from the DUI context.
22. Risk of bias: serious (-1 level). The reference test poses high risk of bias. Inconsistency: serious (-1 level). There is a large difference between the results. Indirectness: serious (-1 level). Population is different from the DUI context.
Description of studies
Four cross-sectional studies (Bergström, 2008; Kharbouche, 2012; McDonald, 2013; Pirro, 2011) were included in the analysis of the literature conducted in 2019. A total of three studies (O’Flaherty, 2022; Aboutara, 2022; Archer, 2019) were included in the updated analysis of the literature in 2025. An elaborate description of these studies can be found in Appendix 6 of this guideline.
Important study characteristics are summarized in Table 5. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’). For the characteristics of the studies analyzed in 2018, please refer to Appendix 6.
O’Flaherty (2022) conducted a cross-sectional study comparing the diagnostic accuracy of CE CDT and GGT. Participants were included from a random sample of the adult population (age >18 years) drawn from Spain’s National Health System Registry. Exclusion criteria were showing evidence of acute illness, fever and undue stress, being unable to give informed consent, being pregnant, having dementia, terminal cancer, allergy to adhesives, or any concomitant medical condition that would likely affect the evaluation of device performance.
Aboutara (2022) conducted a cross-sectional study evaluating the diagnostic accuracy of CDT-HPLC. Participants without permanent residency but with access to specialized medical practices, lodging houses or shelters, were included in this study. Participants without blood samples were excluded.
Archer (2019) conducted a cross-sectional study comparing the diagnostic accuracy of N-Latex CDT and GGT in patients with major depressive disorder. Moderately or severely depressed individuals (scoring ≥17 on the Beck Depression Inventory) were included in this study. Exclusion criteria were primary psychotic disorders (ICD-10 codes F20-29) and organic brain disease or damage.
Results are depicted under the tab “results” and in tables 5 to 10.
Table 5. Characteristics of included studies
|
Study |
Participants |
Comparison |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
O’Flaherty, 2022 |
N at baseline Indextest: 1516 Comparator test: 1516
Age (median (IQR)) Non-risk drinkers (men): 53 (38-68) years Risk drinkers (men): 48 (37-59) years Non-risk drinkers (women): 53 (39-68) years Risk drinkers (women): 50 (42-58) years
Sex 55% female
Prevalence of disease with reference test (%) Overall: 13% Men: 21.0% Women: 5.9% |
Index test (cut-off point(s)): CE CDT (cut-off point >1.6%)
Comparator test (cut-off point(s)): GGT (cut-off point >73 IU/L for men and >38 IU/L for women)
Reference test (cut-off point(s)): Alcohol Use Disorders Identification Test (AUDIT) questionnaire (cut-off point for risk drinking: >5 points for women and >7 points for men) |
Diagnostic accuracy outcome measures for risk drinking:
|
Carlos III, PI16/01404, PI13/2594, and PI20/01069), the Spanish Network for Addictive Disorders (Red de Trastornos Adictivos, RD16/0017/0018, Spanish Ministry of Health) the Spanish Network for Preventive Activity and Health Promotion Research in Primary Care (Red de Actividades Preventivas y de Promocion de Salud en Atención Primaria, RD16/0007/0006), and the European Regional Development Fund (FEDER, “A way to make Europe”).
|
Very high (for all outcome measures)
Reason: It is unclear whether the results of the index test and reference tekst were interpreted independently and the reference test (self-reported alcohol consumption) poses high risk of bias. |
|
Aboutara, 2022 |
N at baseline Indextest: 1151 Comparator test: 1151
Age (median (range)) 47 years (20-86 years)
Sex 21% female
Prevalence of disease with reference test (%) 26% |
Index test (cut-off point(s)): CDT-HPLC (cut-off point >1.7% for suspiciously excessive consumption)
Comparator test (cut-off point(s)): Not applicable
Reference test (cut-off point(s)): Questionnaire 26% (cut-off point for regular-high consumption: ≥ eight drinks per week) |
Diagnostic accuracy outcome measures for regular high consumption:
|
|
Very high (for all outcome measures)
Reason: It is unclear whether the results of the index test and reference tekst were interpreted independently and the reference test (self-reported alcohol consumption) poses high risk of bias. |
|
Archer, 2019 |
N at baseline 2722
Age (mean, SD) Abstainers (men): 38.9 (10.7) years Abstainers (women): 39.5 (12.3) years Low to moderate alcohol intake (men): 41.3 (10.6) years Low to moderate alcohol intake (women): 37.8 (12.4) years High risk alcohol intake (men): 41.9 (11.1) years High risk alcohol intake (women): 33.7 (13.3) years Alcohol abusers (men): 41.4 (10.0) years Alcohol abusers (women): 35.9 (13.5) years
Sex 54% female
Prevalence of disease with reference test (%) 20.2% |
Index test (cut-off point(s)): N-Latex CDT (cut-off point > 2.5%)
Comparator test (cut-off point(s)): GGT (cut-off point: >60 IU/L for men and >40 IU/L for women
Reference test (cut-off point(s)): AUDIT (cut-off point for high risk drinking: more than 14 drinks (men) or over 7 drinks (women) per week) |
Diagnostic accuracy outcome measures for high risk drinking:
|
|
Very high (for all outcome measures)
Reason: It is unclear whether the results of the index test and reference test were interpreted independently and the reference test (self-reported alcohol consumption) poses high risk of bias. |
1.Reference standard was only available for 62 participants
2.Laboratory data were only available for 202 participants
*For further details, see risk of bias table in the appendix
Results
Table 6 summarizes the most important results described in the literature summary written in 2018. The results were derived from the studies of Bergström (2008), Kharbouche (2012), McDonald (2013) and Pirro (2011).
Table 6. Diagnostic accuracy CDT and GGT as described in literature summary 2018
|
Method |
Sensitivity |
Specificity |
AUC |
|
CDT |
36% to 51% |
81% to 96% |
0.75 to 0.93 |
|
GGT |
30% to 66% |
80% to 81% |
0.61 to 0.83 |
"For further details, the 2020 guideline on alcohol misuse in the context of fitness-to-drive assessments may be requested from the Dutch Association for Psychiatry"
1. CDT
1.1 CDT-HPLC
Aboutara (2022) compared CDT-HPLC values with self-reported alcohol consumption as reference test and used a cut-off value of ≥ eight drinks per week to define regular-high alcohol consumption. Based on the results, the 2x2-table below (Table 7) can be constructed.
Table 7. 2x2-table CDT-HPLC versus self-reported alcohol consumption
|
|
Result reference standard |
|||||
|
Result CDT-HPLC |
Positive |
n |
Negative |
n |
||
|
Positive |
True positive |
14 |
False positive |
25 |
||
|
Negative |
False negative |
2 |
True negative |
21 |
||
This leads to the following diagnostic accuracy results with a cut-off value of >1.7% for CDT-HPLC (Table 8).
Table 8. Diagnostic accuracy CDT-HPLC
|
Diagnostic accuracy measure |
Value (95% CI) |
Interpretation |
|
Sensitivity |
87.5% (61.7% to 98.5%) |
High |
|
Specificity |
45.7% (30.9% to 61.0%) |
Low |
|
AUC |
Not reported |
- |
|
Positive predictive value |
35.9% (28.8% to 43.6%) |
Low |
|
Negative predictive value |
91.3% (73.4% to 97.6%) |
High |
|
LR+ |
1.6 (1.2 to 2.2) |
Low |
|
LR- |
0.3 (0.1 to 1.0) |
Moderate |
1.2 N-Latex CDT
Archer (2019) compared N-Latex CDT with self-reported alcohol consumption (AUDIT questionnaire) and used a cut-off value of more than 14 drinks per week for men or over seven drinks for women (high-risk drinkers). Regarding diagnostic accuracy, the results shown in Table 9 were found, using >2.5% as cut-off value for N-Latex CDT.
Table 9. Diagnostic accuracy N-Latex CDT
|
Diagnostic accuracy measure |
Value (95% CI)1 |
Interpretation |
|
Sensitivity |
16.0% |
Low |
|
Specificity |
Not reported2 |
- |
|
AUC |
0.68 |
Moderate |
|
Positive predictive value |
Not reported2 |
- |
|
Negative predictive value |
Not reported2 |
- |
|
LR+ |
Not reported2 |
- |
|
LR- |
Not reported2 |
- |
1. Confidence intervals were not reported by Archer (2019) and could not be calculated based on the available data
2. Not reported and could not be calculated using the available data
1.3 CE CDT
O’Flaherty (2022) compared CE CDT with self-reported alcohol consumption (AUDIT questionnaire) and used a cut-off value of greater than 40 g/day or AUDIT score greater than 7 points for men, and greater than 20 g/day or AUDIT score greater than 5 points for women to define risk drinkers. Regarding diagnostic accuracy, the results shown in Table 10 were found, using >1.6% as cut-off value for CE CDT.
Table 10. Diagnostic accuracy CE CDT
|
Diagnostic accuracy measure |
Women |
Men |
||
|
Value (95% CI) |
Interpretation |
Value (95% CI) |
Interpretation |
|
|
Sensitivity |
8.0% (2.2% to 19.2%) |
Low |
25.9% (18.9% to 33.9%) |
Low |
|
Specificity |
99.5% (98.7% to 99.9%) |
High |
94.4% (92.1% to 96.2%) |
High |
|
AUC |
0.65 (0.56 to 0.74) |
Moderate |
0.71 (0.66 to 0.76) |
Moderate |
|
Positive predictive value |
50.0% (20.5% to 79.5%) |
Low |
55.2% (44.2% to 65.8%) |
Low |
|
Negative predictive value |
94.5% (94.0% to 94.9%) |
High |
82.7% (81.2% to 84.0%) |
High |
|
LR+ |
15.8 (4.1 to 61.2) |
High |
4.6 (3.0 to 7.2) |
Moderate |
|
LR- |
0.9 (0.9 to 1.0) |
Low |
0.8 (0.7 to 0.9) |
Low |
2. GGT
Archer (2019) compared GGT with self-reported alcohol consumption (AUDIT questionnaire) and used a cut-off value of more than 14 drinks per week for men or over seven drinks for women to define high-risk drinkers. Regarding diagnostic accuracy, the results shown in Table 11 were found, using 60 IU/L and 40 IU/L as cut-off values for GGT for men and women, respectively.
O’Flaherty (2022) compared GGT with self-reported alcohol consumption (AUDIT questionnaire) and used a cut-off value of greater than 40 g/day or AUDIT score greater than 7 points for men, and greater than 20 g/day or AUDIT score greater than 5 points for women to define risk drinkers. Regarding diagnostic accuracy, the results shown in Table 11 were found, using 38 IU/L (women) and 73 IU/L (men) as cut-off values for GGT.
Table 11. Diagnostic accuracy GGT
|
Diagnostic accuracy measure |
Value (95% CI)1 (Archer, 2019) |
Interpretation (Archer, 2019) |
Value for women (95% CI) (O’Flaherty, 2022) |
Value for men (95% CI) (O’Flaherty, 2022) |
Interpretation (O’Flaherty, 2022) |
|
Sensitivity |
40.0% |
Low |
32.0% (19.5% to 46.7%) |
18.2% (12.2% to 25.5%) |
Low |
|
Specificity |
Not reported2 |
- |
91.2% (89.1% to 93.1%) |
91.0% (88.3% to 93.3%) |
High |
|
AUC |
0.66 |
Poor |
0.75 (0.68 to 0.82) |
0.70 (0.65 to 0.75) |
Moderate |
|
Positive predictive value |
Not reported2 |
- |
18.8% (12.7% to 26.9%) |
35.1% (25.9% to 45.7%) |
Low
|
|
Negative predictive value |
Not reported2 |
- |
95.5% (94.6% to 96.2%) |
80.6% (79.3% to 81.9%) |
High |
|
LR+ |
Not reported2 |
- |
3.65 (2.30 to 5.80) |
2.0 (1.3 to 3.2) |
Moderate |
|
LR- |
Not reported2 |
- |
0.75 (0.62 to 0.90) |
0.9 (0.8 to 1.0) |
Low |
1. Confidence intervals were not reported by Archer (2019) and could not be calculated based on the available data
2. Not reported and could not be calculated using the available data
A systematic review of the literature was performed to answer the following question(s):
What is the diagnostic accuracy of [index test] compared to [reference standard] in individuals referred to psychiatry due to suspected alcohol abuse in traffic/driving under influence (DUI)?
Table 2. PIC(R)O’s
| Patients | Individuals referred to psychiatry due to suspected alcohol abuse in traffic/driving under influence (DUI) |
| Index test |
|
| Comparator test | See index test |
| Reference test | Actual reported alcohol intake based on self-report/audit |
| Outcomes | Sensitivity, specificity, AUC, positive predictive value, negative predictive value, positive likelihood ratio (LR+), negative likelihood ratio (LR-) |
| Other selection criteria | Study design: systematic reviews, diagnostic test accuracy studies (with single-gate design, cross-sectional study) |
Relevant outcome measures
The guideline panel considered specificity and AUC as critical outcome measures for decision making; and sensitivity, positive predictive value, negative predictive value, LR+ and LR- as important outcome measures for decision making.
Table 3. Consequences of diagnostic test characteristics
|
Outcome |
Consequences |
Relevance |
|
True positives (TP) |
Individuals are justifiably diagnosed with DUI |
Important |
|
True negatives (TN) |
Individuals are justifiably not diagnosed with DUI |
Critical |
|
False positives (FP) |
Individuals are unjustifiably diagnosed with DUI |
Critical |
|
False negatives (FN) |
Patients are unjustifiably not diagnosed with DUI |
Important |
The guideline panel defined used the following cut-off values mentioned in Table 4 to score sensitivity, specificity, AUC, positive predictive value, negative predictive value, positive likelihood ratio (LR+) and negative likelihood ratio (LR-).
Table 4. Cut-off values diagnostic accuracy outcome measures
|
Outcome measure |
Interpretation |
Value |
|
Low |
<0.60 |
|
Moderate |
60% to 80% |
|
|
High |
>80% |
|
|
LR+ |
Low |
1-2 |
|
Moderate |
2-5 |
|
|
High |
>5 |
|
|
LR- |
Low |
1-0.5 |
|
Moderate |
0.5-0.2 |
|
|
High |
<0.2 |
Search and select (Methods)
An updated systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2018 to 25 March 2025 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) alcohol abuse; (2) biomarkers. Duplicates were removed using EndNote software. After deduplication a total of 631 records were imported for title/abstract screening. Initially, 25 studies were selected based on title and abstract screening. After reading the full text, 22 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and three studies were included.
- Aboutara N, Müller A, Jungen H, Szewczyk A, van Rüth V, Bertram F, Püschel K, Heinrich F, Iwersen-Bergmann S. Investigating the use of PEth, CDT and MCV to evaluate alcohol consumption in a cohort of homeless individuals- A comparison of different alcohol biomarkers. Forensic Sci Int. 2022 Feb;331:111147. doi: 10.1016/j.forsciint.2021.111147. Epub 2021 Dec 10. PMID: 34920332.
- Aboutara N, Jungen H, Szewczyk A, Müller A, Iwersen-Bergmann S. PEth 16:0/18:1 and 16:0/18:2 after consumption of low doses of alcohol-A contribution to cutoff discussion. Drug Test Anal. 2023 Jan;15(1):104-114. doi: 10.1002/dta.3376. Epub 2022 Oct 18. PMID: 36181234.
- Alatalo PI, Koivisto HM, Hietala JP, Puukka KS, Bloigu R, Niemelä OJ. Effect of moderate alcohol consumption on liver enzymes increases with increasing body mass index. Am J Clin Nutr. 2008 Oct;88(4):1097-103.
- Arndt T. Carbohydrate-deficient transferrin as a marker of chronic alcohol abuse: a critical review of preanalysis, analysis, and interpretation. Clin Chem. 2001 Jan;4fberf.
- Archer M, Kampman O, Bloigu A, Bloigu R, Luoto K, Kultti J, Hämäläinen M, Moilanen E, Leinonen E, Niemelä O. Assessment of alcohol consumption in depression follow-up using self-reports and blood measures including inflammatory biomarkers. Alcohol Alcohol. 2019 May 1;54(3):243-250. doi: 10.1093/alcalc/agz002. PMID: 30809628.
- Bianchi V, Premaschi S, Raspagni A, Secco S, Vidali M. A comparison between serum carbohydrate-deficient transferrin and hair ethyl glucuronide in detecting chronic alcohol consumption in routine. Alcohol Alcohol. 2015 May;50(3):266-70. doi: 10.1093/alcalc/agv005.
- Bergström JP, Helander A. Clinical characteristics of carbohydrate-deficient transferrin (%disialotransferrin) measured by HPLC: sensitivity, specificity, gender effects, and relationship with other alcohol biomarkers. Alcohol Alcohol. 2008 Jul-Aug;43(4):436-41. doi: 10.1093/alcalc/agn017. Epub 2008 Apr 14. PMID: 18411243.
- Bortolotti F, De Paoli G, Tagliaro F. Carbohydrate-deficient transferrin (CDT) as a marker of alcohol abuse: a critical review of the literature 2001-2005. J Chromatogr B Analyt Technol Biomed Life Sci. 2006 Sep 1;841(1-2):96-109.
- Breitling LP, Arndt V, Drath C, Brenner H. Liver enzymes: interaction analysis of smoking with alcohol consumption or BMI, comparing AST and ALT to γ-GT. PLoS One. 2011;6(11): e27951. doi: 10.1371/journal.pone.0027951. Epub 2011 Nov 22. PubMed PMID: 22132177.
- Breitling LP, Claessen H, Drath C, Arndt V, Brenner H (2011) Gamma-glutamyltransferase, general and cause-specific mortality in 19,000 construction workers followed over 20 years. J Hepatol 2011; 55:594–601. DOI: 10.1016/j.jhep.2010.12.029.
- Ceriotti F, Henny J, Queraltó J, Ziyu S, Özarda Y, Chen B, Boyd JC, Panteghini M; IFCC Committee on Reference Intervals and Decision Limits (C-RIDL); Committee on Reference Systems for Enzymes (C-RSE). Common reference intervals for aspartate aminotransferase (AST), alanine aminotransferase (ALT) and γ-glutamyl transferase (GGT) in serum: results from an IFCC multicenter study. Clin Chem Lab Med. 2010 Nov;48(11):1593-601.
- Chrostek L, Cylwik B, Szmitkowski M, Korcz W. The diagnostic accuracy of carbohydrate-deficient transferrin, sialic acid and commonly used markers of alcohol abuse during abstinence. Clin Chim Acta. 2006 Feb;364(1-2):167-71. doi: 10.1016/j.cccn.2005.06.020. Epub 2005 Aug 8. PMID: 16087169.
- Crunelle CL, Yegles M, De Doncker M, Dom G, Cappelle D, Maudens KE, van Nuijs AL, Covaci A, Neels H. Influence of repeated permanent coloring and bleaching on ethyl glucuronide concentrations in hair from alcohol-dependent patients. Forensic Sci Int. 2015 Feb;247: 18-22. doi: 10.1016/j.forsciint.2014.11.023.
- Danielsson J, Kangastupa P, Laatikainen T, Aalto M, Niemelä O. Individual and joint impacts of ethanol use, BMI, age and gender on serum gamma-glutamyltransferase levels in healthy volunteers. Int J Mol Sci. 2013 Jun 4;14(6):11929-41. doi: 10.3390/ijms140611929.
- Danielsson J, Kangastupa P, Laatikainen T, Aalto M, Niemelä O. Impacts of common factors of lifestyle on serum liver enzymes. World J Gastroenterol. 2014 Sep 7;20(33):11743-52.
- Fleming MF, Anton RF, Spies CD. A review of genetic, biological, pharmacological, and clinical factors that affect carbohydrate-deficient transferrin levels. Alcohol Clin Exp Res. 2004 Sep;28(9):1347-55.
- Fortman CS, Witte DL. Serum 5'-nucleotidase in patients receiving anti-epileptic drugs. Am J Clin Pathol. 1985 Aug;84(2):197-201. PubMed PMID: 2862788.
- Giroud M, Dumas R (1986) New developments in the diagnosis and therapy of epilepsy. J Neurol 1986;233:378. DOI: 10.1007/BF00313928.
- Göttgens EL, Haverkate L, Langelaan M, Lunshof S, Joosen AMCP, van Gammeren AJ, Remijn JA, Ermens AAM, Jacobs LHJ. Defining trimester-specific reference intervals for carbohydrate deficient transferrin in pregnant women. Clin Chim Acta. 2024 Feb 1;554:117748. doi: 10.1016/j.cca.2023.117748. Epub 2023 Dec 28. PMID: 38158004.
- Hastedt M, Büchner M, Rothe M, Gapert R, Herre S, Krumbiegel F, Tsokos M, Kienast T, Heinz A, Hartwig S. Detecting alcohol abuse: traditional blood alcohol markers compared to ethyl glucuronide (EtG) and fatty acid ethyl esters (FAEEs) measurement in hair. Forensic Sci Med Pathol. 2013 Dec;9(4):471-7. doi: 10.1007/s12024-013-9416-8.
- Helander A, Husa A, Jeppsson JO. Improved HPLC method for carbohydrate-deficient transferrin in serum. Clin Chem. 2003 Nov;49(11):1881-90. doi: 10.1373/clinchem.2003.023341. PMID: 14578320.
- Helander A, Zheng Y. Molecular species of the alcohol biomarker phosphatidylethanol in human blood measured by LC-MS. Clin Chem. 2009 Jul;55(7):1395-405.
- Helander A, Wielders J, Anton R, Arndt T, Bianchi V, Deenmamode J, Jeppsson JO, Whitfield JB, Weykamp C, Schellenberg F; International Federation of Clinical Chemistry and Laboratory Medicine Working Group on Standardisation of Carbohydrate-Deficient Transferrin (IFCC WG-CDT). Standardisation and use of the alcohol biomarker carbohydrate-deficient transferrin (CDT). Clin Chim Acta. 2016 Aug 1;459:19-24. doi: 10.1016/j.cca.2016.05.016. Epub 2016 May 21. PMID: 27221205.
- Helander A, Hermansson U, Beck O. Dose-Response Characteristics of the Alcohol Biomarker Phosphatidylethanol (PEth)-A Study of Outpatients in Treatment for Reduced Drinking. Alcohol Alcohol. 2019 Dec 1;54(6):567-573. doi: 10.1093/alcalc/agz064. PMID: 31529064.
- Helander A, Hansson T (2023) The alcohol biomarker phosphatidylethanol (PEth) - test performance and experiences from routine analysis and external quality assessment. Scand J Clin Lab Invest 2023;83:424-431. DOI: 10.1080/00365513.2023.2253734.
- Husen PO, Ahmed RA, Ahmed KM, Abdulla ID, Ayub HM, Hamad S (2015) Cigarette smoking risks on blood indices and liver enzymes of male and female smokers in Kurdistan Iraq. JJBS 2013; 8: 227-230.
- Jeppsson JO, Arndt T, Schellenberg F, Wielders JPM, Anton RF, Whitfield JB, Helander A. Toward standardization of carbohydrate-deficient transferrin (CDT) measurements: I. Analyte definition and proposal of a candidate reference method. Clin. Chem. Lab. Med. 2007; 45: 558–562. DOI: 10.1515/CCLM.2007.107.
- Keeffe EB, Sunderland MC, Gabourel JD. Serum gamma-glutamyl transpeptidase activity in patients receiving chronic phenytoin therapy. Dig Dis Sci. 1986 Oct;31(10):1056-61.
- Kenan N, Larsson A, Axelsson O, Helander A. Changes in transferrin glycosylation during pregnancy may lead to false-positive carbohydrate-deficient transferrin (CDT) results in testing for riskful alcohol consumption. Clin Chim Acta. 2011 Jan 14;412(1-2):129-33.
- Kharbouche H, Faouzi M, Sanchez N, Daeppen JB, Augsburger M, Mangin P, Staub C, Sporkert F. Diagnostic performance of ethyl glucuronide in hair for the investigation of alcohol drinking behavior: a comparison with traditional biomarkers. Int J Legal Med. 2012 Mar;126(2):243-50. doi: 10.1007/s00414-011-0619-9. Epub 2011 Sep 11. PMID: 21910015.
- Koenig G, Seneff S. Gamma-Glutamyltransferase: A Predictive Biomarker of Cellular Antioxidant Inadequacy and Disease Risk. Dis Markers. 2015; 2015:818570.
- Kok EE, Wielders JPM, Pasker-de Jong P, Defoury H, Rondes SJA en van de Wiel A. Biomarkers of excessive alcohol intake in alcohol addicts with a normal nutritional status. Ned Tijdschr Klin Chem Labgeneesk 2014; 39: 185-188.
- Lee D, Kang LH, Kim Y (2019) Association between Cigarette Smoking and Serum Gamma-Glutamyl Transferase Level. Int J Respir Pulm Med 2019; 6:125. DOI: 10.23937/2378-3516/1410125.
- Limdi JK, Hyde GM (2003) Evaluation of abnormal liver function tests. PMJ 2003; 79: 307-312. doi.org/10.1136/pmj.79.932.307.
- Luginbuhl M, Stoth F, Schrock A, Gaugler S, Weinmann W (2021) Quantitative determination of phosphatidylethanol in dried blood spots for monitoring alcohol abstnance. Nat Protoc 2021; 16: 283-308. DOI: 10.1038/s41596-020-00416-x.
- Luginbühl M, Wurst FM, Stöth F, Weinmann W, Stove CP, Van Uytfanghe K. Consensus for the use of the alcohol biomarker phosphatidylethanol (PEth) for the assessment of abstinence and alcohol consumption in clinical and forensic practice (2022 Consensus of Basel). Drug Test Anal. 2022 Oct;14(10):1800-1802. doi: 10.1002/dta.3340. Epub 2022 Jul 18. PMID: 35851997.
- Luginbuhl M, Wurst FM, Stoth F, Weinmann W, Stove CP, Van Uytfanghe K (2022) Consensus for the use of the alcohol biomarker phosphatidylethanol (PEth) for the assessment of abstinence and alcohol consumption in clinical and forensic practice. Drug Test. Anal. 2022;14:1800–1802. DOI: 10.1002/dta.3340.
- Luginbühl, M., Van Uytfanghe, K., Stöth, F., Wurst, F. M., & Stove, C. P. (2022). Current evolutions, applications, and challenges of phosphatidylethanol analysis for clinical and forensic purposes. Wiley Interdisciplinary Reviews: Forensic Science, 4(5), e1456.
- McDonald H, Borinskya S, Kiryanov N, Gil A, Helander A, Leon DA. Comparative performance of biomarkers of alcohol consumption in a population sample of working-aged men in Russia: the Izhevsk Family Study. Addiction. 2013 Sep;108(9):1579-89. doi: 10.1111/add.12251. Epub 2013 Jul 5. PMID: 23692391; PMCID: PMC3992900.
- McDonell MG, Skalisky J, Leickly E, McPherson S, Battalio S, Nepom JR, Srebnik D, Roll J, Ries RK (2023) Using ethyl glucuronide in urine to detect light and heavy drinking in alcohol dependent outpatients. Drug Alcohol Depend 2015: 157; 184-7. DOI: 10.1016/j.drugalcdep.2015.10.004.
- Meerkerk GJ, Njoo KH, Bongers IM, Trienekens P, van Oers JA. The specificity of the CDT assay in general practice: the influence of common chronic diseases and medication on the serum CDT concentration. Alcohol Clin Exp Res. 1998 Jun;22(4):908-13.
- Musshoff F, Böttcher M, Graw M, Skopp G, Neumann J,Hoiseth G, Helander A (2023) Comment on the upper cutoff level for the alcohol biomarker phosphatidylethanol (PEth) for the assessment of alcohol consumption in forensic practice. Drug Test Anal. 2023; 15: 791–792. DOI: 10.1002/dta.3432.
- Nanau RM, Neuman MG. (2015) Biomolecules and Biomarkers Used in Diagnosis of Alcohol Drinking and in Monitoring Therapeutic Interventions. Biomolecules. 2015; 5: 1339–1385. DOI: 10.3390/biom5031339.
- O'Flaherty R, Simon Á, Alonso-Sampedro M, Sánchez-Batán S, Fernández-Merino C, Gude F, Saldova R, González-Quintela A. Changes in Serum N-Glycome for Risk Drinkers: A Comparison with Standard Markers for Alcohol Abuse in Men and Women. Biomolecules. 2022 Feb 1;12(2):241. doi: 10.3390/biom12020241. PMID: 35204742; PMCID: PMC8961540.
- Perilli M, Toselli F, Franceschetto L, Cinquetti A, Ceretta A, Cecchetto G, Viel G. Phosphatidylethanol (PEth) in Blood as a Marker of Unhealthy Alcohol Use: A Systematic Review with Novel Molecular Insights. Int J Mol Sci. 2023 Jul 29;24(15):12175. doi: 10.3390/ijms241512175. PMID: 37569551; PMCID: PMC10418704.
- Pirro V, Valente V, Oliveri P, De Bernardis A, Salomone A, Vincenti M. Chemometric evaluation of nine alcohol biomarkers in a large population of clinically-classified subjects: pre-eminence of ethyl glucuronide concentration in hair for confirmatory classification. Anal Bioanal Chem. 2011 Oct;401(7):2153-64. doi: 10.1007/s00216-011-5314-7. Epub 2011 Sep 4. PMID: 21901464.
- Poikolainen K. Biased cohort studies on alcohol abuse and mortality. Addiction. 1997 Jul;92(7):903-4. PubMed PMID: 9293048.
- Pragst F, Rothe M, Moench B, Hastedt M, Herre S, Simmert D. Combined use of fatty acid ethyl esters and ethyl glucuronide in hair for diagnosis of alcohol abuse: interpretation and advantages. Forensic Sci Int. 2010 Mar 20;196(1-3):101-10.
- Schellenberg F, Schwan R, Mennetrey L, Loiseaux MN, Pagès JC, Reynaud M. Dose-effect relation between daily ethanol intake in the range 0-70 grams and %CDT value: validation of a cut-off value. Alcohol Alcohol. 2005 Nov-Dec;40(6):531-4. doi: 10.1093/alcalc/agh194. Epub 2005 Aug 15. PMID: 16103033.
- Schellenberg F, Wielders J, Anton R, Bianchi V, Deenmamode J, Weykamp C, Whitfield J, Jeppsson JO, Helander A. IFCC approved HPLC reference measurement procedure for the alcohol consumption biomarker carbohydrate-deficient transferrin (CDT): Its validation and use. Clin Chim Acta. 2017 Feb;465:91-100. doi: 10.1016/j.cca.2016.12.022. Epub 2016 Dec 23. PMID: 28025028.
- Sharpe PC. Biochemical detection and monitoring of alcohol abuse and abstinence. Ann Clin Biochem. 2001 Nov;38(Pt 6):652-64. doi: 10.1258/0004563011901064. PMID: 11732647.
- Sillanaukee P, Massot N, Jousilahti P, Vartiainen E, Sundvall J, Olsson U, Poikolainen K, Pönniö M, Allen JP, Alho H. Dose response of laboratory markers to alcohol consumption in a general population. Am J Epidemiol. 2000 Oct 15;152(8):747-51.
- Targher G. Elevated serum gamma-glutamyltransferase activity is associated with increased risk of mortality, incident type 2 diabetes, cardiovascular events, chronic kidney disease and cancer - a narrative review. Clin Chem Lab Med. 2010 Feb;48(2):147-57.
- van Beek JHDA, de Moor MHM, Geels LM, Sinke MRT, de Geus EJC, Lubke GH, Kluft C, Neuteboom J, Vink JM, Willemsen G, Boomsma DI. The association of alcohol intake with γ-glutamyl transferase (GGT) levels: evidence for correlated genetic effects. Drug Alcohol Depend. 2014 Jan 1; 134:99-105.
- Whitfield JB. Gamma glutamyl transferase. Crit Rev Clin Lab Sci. 2001 Aug;38(4):263-355. Review. PubMed PMID: 11563810.
- Whitefield JB, Heath AC, Madden PAF, Pergadia ML, Montgomery GW, Martin NG (2012) Metabolic and biochemical effects of low to moderate alcohol consumption. Alcohol Clin Exp Res 2012;37: 575-586. DOI: 10.1111/acer.12015.
- Whitfield JB, Heath AC, Madden PA, Pergadia ML, Montgomery GW, Martin NG. Metabolic and biochemical effects of low-to-moderate alcohol consumption. Alcohol Clin Exp Res. 2013 Apr;37(4):575-86. PubMed PMID: 23134229.
- Whitfield JB, Zhu G, Madden PAF, Montgomery GW, Heath AC, Martin NG. Biomarker and Genomic Risk Factors for Liver Function Test Abnormality in Hazardous Drinkers. Alcohol Clin Exp Res. 2019 Mar;43(3):473-482.
- Wielders J, Helander A, Deenmamode J, Weykamp C, Schellenberg F; IFCC Working Group CDT (December 2024). Biomarkers for Harmful Alcohol Use should be Reliable, Standardised, and Traceable: Only the CDT reference method has been approved by JCTLM and IFCC. EJIFCC. 2025 Feb 28;36(1):3-6. PMID: 40061061; PMCID: PMC11886621.
- Wielders JPM, Porpiglia NM, Schellenberg F, Deenamode J, Delanghe J, Anton RF, Bortolotti F, Siebelder C, Tagliaro F, Weykamp C, Helander (2024) Recommendations on the measurement and use of the alcohol consumption biomarker CDT. A position paper from the IFCC Working Group on CDT standardization. Clin Chem Acta 2024; 555: 1-11. DOI: 10.1016/j.cca.2024.117800.
- Wolff K, Gross S, Marshall EJ, Walsham NE. Robson N, Keaney F, Sherwood RA (2019) Carbohydrate deficient transferrin (CDT) as a biomarker to assess drinking in high-risk drink drivers Adv Clin Toxicol 2019; 4: 1-11 DOI: 10.23880/act-16000160.
- Wu, A.H.B. Tietz Clinical Guide to Laboratory Tests Fourth Edition 4th Edition. Druk: 4th. 2006. ISBN 9781437719871.
- Zhou R, Qin Y, Yin H, Yang Y, Wang Q (2018) Measurement uncertainty of γ-glutamyltransferase (GGT) in human serum by four approaches using different quality assessment data. Clin Chem Lab Med. 2018 Jan 26;56(2):242-248. DOI: 10.1515/cclm-2017-0511.
Risk of bias tables
Risk of bias assessment diagnostic accuracy studies (QUADAS II, 2011)
|
Study reference |
Patient selection
|
Index test |
Reference standard |
Flow and timing |
Comments with respect to applicability |
|
Aboutara, 2022 |
Was a consecutive or random sample of patients enrolled? Unclear
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
|
Were the index test results interpreted without knowledge of the results of the reference standard? Unclear
If a threshold was used, was it pre-specified? Yes
|
Is the reference standard likely to correctly classify the target condition? No
Were the reference standard results interpreted without knowledge of the results of the index test? Unclear
|
Was there an appropriate interval between index test(s) and reference standard? Unclear
Did all patients receive a reference standard? Yes
Did patients receive the same reference standard? Yes
Were all patients included in the analysis? No |
Are there concerns that the included patients do not match the review question? Unclear
Are there concerns that the index test, its conduct, or interpretation differ from the review question? Yes
Are there concerns that the target condition as defined by the reference standard does not match the review question? No
|
|
CONCLUSION: Could the selection of patients have introduced bias?
RISK: UNCLEAR Reason: insufficient information regarding enrolment of participants |
CONCLUSION: Could the conduct or interpretation of the index test have introduced bias?
RISK: UNCLEAR Reason: it is unclear whether the index test results were interpreted without knowledge of the results of the reference standard
|
CONCLUSION: Could the reference standard, its conduct, or its interpretation have introduced bias?
RISK: HIGH Reason: self-reported alcohol consumption is the best available reference standard, but risk of bias is high. It is unclear whether the reference standard results were interpreted without knowledge of the results of the index test |
CONCLUSION Could the patient flow have introduced bias?
RISK: LOW Reason: low number of excluded patients and no other significant problems were noted |
|
|
|
Archer, 2019 |
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
|
Were the index test results interpreted without knowledge of the results of the reference standard? Unclear
If a threshold was used, was it pre-specified? Yes
|
Is the reference standard likely to correctly classify the target condition? No
Were the reference standard results interpreted without knowledge of the results of the index test? Unclear
|
Was there an appropriate interval between index test(s) and reference standard? Unclear
Did all patients receive a reference standard? Yes
Did patients receive the same reference standard? Yes
Were all patients included in the analysis? Yes |
Are there concerns that the included patients do not match the review question? Unclear
Are there concerns that the index test, its conduct, or interpretation differ from the review question? Yes
Are there concerns that the target condition as defined by the reference standard does not match the review question? No
|
|
|
CONCLUSION: Could the selection of patients have introduced bias?
RISK: LOW |
CONCLUSION: Could the conduct or interpretation of the index test have introduced bias?
RISK: UNCLEAR Reason: it is unclear whether the index test results were interpreted without knowledge of the results of the reference standard
|
CONCLUSION: Could the reference standard, its conduct, or its interpretation have introduced bias?
RISK: HIGH Reason: self-reported alcohol consumption is the best available reference standard, but risk of bias is high. It is unclear whether the reference standard results were interpreted without knowledge of the results of the index test |
CONCLUSION Could the patient flow have introduced bias?
RISK: LOW |
Reason: it is unclear whether the index test results were interpreted without knowledge of the results of the reference standard. Population in DUI context might be different, but it is difficult to assess if this difference is reflected in the study results. |
|
O’Flaherty, 2022 |
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
|
Were the index test results interpreted without knowledge of the results of the reference standard? Unclear
If a threshold was used, was it pre-specified? Yes
|
Is the reference standard likely to correctly classify the target condition? No
Were the reference standard results interpreted without knowledge of the results of the index test? Unclear
|
Was there an appropriate interval between index test(s) and reference standard? Unclear
Did all patients receive a reference standard? Yes
Did patients receive the same reference standard? Yes
Were all patients included in the analysis? Yes
|
Are there concerns that the included patients do not match the review question? Unclear
Are there concerns that the index test, its conduct, or interpretation differ from the review question? Yes
Are there concerns that the target condition as defined by the reference standard does not match the review question? No
|
|
|
CONCLUSION: Could the selection of patients have introduced bias?
RISK: LOW |
CONCLUSION: Could the conduct or interpretation of the index test have introduced bias?
RISK: UNCLEAR Reason: it is unclear whether the index test results were interpreted without knowledge of the results of the reference standard
|
CONCLUSION: Could the reference standard, its conduct, or its interpretation have introduced bias?
RISK: HIGH Reason: self-reported alcohol consumption is the best available reference standard, but risk of bias is high. It is unclear whether the reference standard results were interpreted without knowledge of the results of the index test |
CONCLUSION Could the patient flow have introduced bias?
RISK: LOW |
Reason: it is unclear whether the index test results were interpreted without knowledge of the results of the reference standard. Population in DUI context might be different, but it is difficult to assess if this difference is reflected in the study results. |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Andresen-Streichert H, Müller A, Glahn A, Skopp G, Sterneck M. Alcohol Biomarkers in Clinical and Forensic Contexts. Dtsch Arztebl Int. 2018 May 4;115(18):309-315. doi: 10.3238/arztebl.2018.0309. PMID: 29807559; PMCID: PMC5987059. |
Selective review |
|
Bortolotti F, Sorio D, Bertaso A, Tagliaro F. Analytical and diagnostic aspects of carbohydrate deficient transferrin (CDT): A critical review over years 2007-2017. J Pharm Biomed Anal. 2018 Jan 5;147:2-12. doi: 10.1016/j.jpba.2017.09.006. Epub 2017 Sep 6. PMID: 28912047. |
Narrative review |
|
Skopp, G. and Muβhoff, F.Current topics on biomarkers in the forensic and clinical context of alcohol use disorders |
Narrative review |
|
Arnts J, Vanlerberghe BTK, Roozen S, Crunelle CL, Masclee AAM, Olde-Damink SWM, Heeren RMA, van Nuijs A, Neels H, Nevens F, Verbeek J. Diagnostic Accuracy of Biomarkers of Alcohol Use in Patients With Liver Disease: A Systematic Review. Alcohol Clin Exp Res. 2021 Jan;45(1):25-37. doi: 10.1111/acer.14512. Epub 2020 Dec 25. PMID: 33190239; PMCID: PMC7898850. |
Patients with liver disease |
|
Årving A, Høiseth G, Hilberg T, Trydal T, Husa A, Djordjevic A, Kabashi S, Vindenes V, Bogstrand ST. Comparison of the Diagnostic Value of Phosphatidylethanol and Carbohydrate-Deficient Transferrin as Biomarkers of Alcohol Consumption. Alcohol Clin Exp Res. 2021 Jan;45(1):153-162. doi: 10.1111/acer.14503. Epub 2020 Nov 21. PMID: 33164220. |
No reference standard |
|
Afshar M, Baker K, Corral J, Ross E, Lowery E, Gonzalez R, Burnham EL, Callcut RA, Kornblith LZ, Hendrickson C, Kovacs EJ, Joyce C. Internal and External Validation of an Alcohol Biomarker for Screening in Trauma. Ann Surg. 2022 Dec 1;276(6):e961-e968. doi: 10.1097/SLA.0000000000004770. Epub 2021 Feb 1. PMID: 33534233; PMCID: PMC8429522. |
CDT and GGT only described in combination with Peth |
|
Suzuki T, Eguchi A, Shigefuku R, Nagao S, Morikawa M, Sugimoto K, Iwasa M, Takei Y. Accuracy of carbohydrate-deficient transferrin as a biomarker of chronic alcohol abuse during treatment for alcoholism. Hepatol Res. 2022 Jan;52(1):120-127. doi: 10.1111/hepr.13642. Epub 2021 Apr 13. PMID: 33797850. |
Population already diagnosed with drinking problems, wrong and not pre-defined cut-off used for CDT |
|
Magzoub, Mohamed, et al. "Evaluation of Gamma-Glutamine Transferase (γ-GT) as a Marker of Alcohol Abuse." Biomedical and Pharmacology Journal 17.4 (2024): 2709-2715. |
No diagnostic accuracy outcome measures |
|
Tavaglione F, Amangurbanova M, Yang AH, Tincopa MA, Ajmera V, Richards L, Butcher C, Hernandez C, Madamba E, Singh S, Bettencourt R, Sirlin CB, Loomba R. Head-to-Head Comparison Between Phosphatidylethanol Versus Indirect Alcohol Biomarkers for Diagnosis of MetALD Versus MASLD: A Prospective Study. Aliment Pharmacol Ther. 2025 Mar;61(6):1043-1054. doi: 10.1111/apt.18506. Epub 2025 Jan 17. PMID: 39825487; PMCID: PMC11870800. |
Diagnostic outcome measures are provided for diagnosis of liver diseases instead of alcohol use |
|
Deas D, Johnson N, Thomas S. Carbohydrate deficient transferrin (CDT) predicts heavy drinking in adolescents with alcohol dependence. Alcohol. 2019 Dec;81:27-30. doi: 10.1016/j.alcohol.2019.06.002. Epub 2019 Jun 21. PMID: 31233805. |
Population already diagnosed with drinking problems |
|
van de Luitgaarden IAT, Beulens JWJ, Schrieks IC, Kieneker LM, Touw DJ, van Ballegooijen AJ, van Oort S, Grobbee DE, Bakker SJL. Urinary Ethyl Glucuronide Can Be Used as a Biomarker of Habitual Alcohol Consumption in the General Population. J Nutr. 2019 Dec 1;149(12):2199-2205. doi: 10.1093/jn/nxz146. PMID: 31268139; PMCID: PMC6887922. |
Only EtG is described |
|
Cherrier MM, Shireman LM, Wicklander K, Yeung W, Kooner P, Saxon AJ, Simpson T, Terman G, Shen D. Relationship of Phosphatidylethanol Biomarker to Self-Reported Alcohol Drinking Patterns in Older and Middle-Age Adults. Alcohol Clin Exp Res. 2020 Dec;44(12):2449-2456. doi: 10.1111/acer.14475. Epub 2020 Nov 9. PMID: 33038267; PMCID: PMC8476046. |
No diagnostic accuracy outcome measures and only PEth is described |
|
Liang SS, He Y, Huang ZG, Jia CY, Gan W. Evaluation of the diagnostic utility of carbohydrate-deficient transferrin in chronic alcoholism: Results from Southwest China. Medicine (Baltimore). 2021 Jan 29;100(4):e24467. doi: 10.1097/MD.0000000000024467. PMID: 33530257; PMCID: PMC7850677. |
Population consisting largerly of individuals with diagnosed drinking problems or liver disease |
|
Tsanaclis L, Davies M, Bevan S, Nutt J, Bagley K, Wicks J. Testing venous carbohydrate-deficient transferrin or capillary phosphatidylethanol with concurrent ethyl glucuronide and ethyl palmitate hair tests to assess historical and recent alcohol use. Drug Test Anal. 2021 Jan;13(1):203-207. doi: 10.1002/dta.2939. Epub 2020 Oct 26. PMID: 33025638. |
No diagnostic accuracy outcome measures |
|
Aboutara N, Szewczyk A, Jungen H, Mosebach A, Rodriguez Lago M, Vettorazzi E, Iwersen-Bergmann S, Müller A, Sterneck M. Phosphatidylethanol in patients with liver diseases of different etiologies: Analysis of six homologues and comparison with other alcohol markers. Clin Chim Acta. 2022 Jan 1;524:171-178. doi: 10.1016/j.cca.2021.11.013. Epub 2021 Nov 19. PMID: 34801484. |
Only EtG and PEth are described and patients with liver disease |
|
Ikonnikova, Karolina Andreevna, et al. "Clinical and diagnostic value of alcohol biomarkers." Experimental and clinical gastroenterology 7 (203) (2022): 211-223. |
Narrative review, only available in Russian |
|
Morinaga M, Kon K, Uchiyama A, Fukada H, Fukuhara K, Yaginuma R, Nakadera E, Yamashina S, Ikejima K. Carbohydrate-deficient transferrin is a sensitive marker of alcohol consumption in fatty liver disease. Hepatol Int. 2022 Apr;16(2):348-358. doi: 10.1007/s12072-022-10298-8. Epub 2022 Jan 20. PMID: 35060066. |
Patients with liver disease |
|
Cinquetti A, Terranova C, Aprile A, Favretto D. Driving license regranting: Hair EtG, serum CDT, and the role of sociodemographic and medicolegal variables. Drug Test Anal. 2023 Sep;15(9):953-961. doi: 10.1002/dta.3426. Epub 2022 Dec 25. PMID: 36525282. |
No diagnostic accuracy outcome measures |
|
Ghosh S, Jain R, Rao R, Mishra AK, Jhanjee S. Does ethyl glucuronide in hair correlate with alcohol consumption? A comparative study with other traditional biomarkers among individuals with alcohol dependence syndrome. Alcohol. 2023 Feb;106:55-60. doi: 10.1016/j.alcohol.2022.10.005. Epub 2022 Nov 14. PMID: 36395967. |
Population already diagnosed with drinking problems |
|
Cerioni A, Buratti E, Mietti G, Ribeiro ILA, Cippitelli M, Tassoni G, Cingolani M, Froldi R, Scendoni R. Comparative analysis between CDT in serum and Ethyl glucuronide in hair to define the best reliable tool for the diagnosis of alcohol abuse. Drug Alcohol Depend. 2024 Apr 1;257:111128. doi: 10.1016/j.drugalcdep.2024.111128. Epub 2024 Feb 14. PMID: 38394813. |
Incorrect reference standard (biomarkers used as reference) |
|
Cylwik B, Gruszewska E, Janicka K, Olanski W, Chrostek L. Diagnostic Usefulness of Disialotransferrin as an Indicator of Binge Drinking in Children and Adolescents. J Clin Med. 2024 Jun 29;13(13):3833. doi: 10.3390/jcm13133833. PMID: 38999399; PMCID: PMC11242074. |
Population is not an at-risk population because it consists of patients reported to emergency department due to alcohol poisoning |
|
Wielders JPM, Porpiglia NM, Schellenberg F, Deenmamode J, Delanghe J, Anton RF, Bortolotti F, Siebelder C, Tagliaro F, Weykamp C, Helander A. Recommendations on the measurement and use of the alcohol consumption biomarker CDT. A position paper from the IFCC Working Group on CDT standardisation. Clin Chim Acta. 2024 Mar 1;555:117800. doi: 10.1016/j.cca.2024.117800. Epub 2024 Feb 2. PMID: 38309557. |
Position paper |
Beoordelingsdatum en geldigheid
Publicatiedatum : 13-07-2026
Beoordeeld op geldigheid : 13-07-2026
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2024 een multidisciplinaire cluster ingesteld. Het cluster Psychiatrie en Diagnostiek bestaat uit meerdere richtlijnen, bekijk hier de actuele clusterindeling. De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden geven hun expertise in, indien nodig. De volgende personen uit het cluster zijn betrokken geweest bij de herziening van deze module:
Clusterstuurgroepleden
- Prof. dr. A.T.F. Beekman, psychiater, Amsterdam UMC, Amsterdam (NVvP)
- Dr. D.P. Ravelli, psychiater (NVvP)
- Dr. N.D. Veen, psychiater, ggz-Delftland, Delft (NVvP)
- Dr. T.J.M. Ingenhoven, psychiater (NVvP)
- Dr. S.M.P. van Veen, psychiater, Amsterdam UMC, Amsterdam (NVvP)
- Dr. S.J. Roza, psychiater, Erasmus Medisch Centrum, Rotterdam (NVvP)
Betrokken clusterexpertisegroepleden
- Dr. D.P. Ravelli, psychiater (NVvP) (coördinerend stuurgroeplid)
- Drs. F.J.M. Bergkamp, klinisch chemicus, Atalmedial (NVKC)
- Dr. J.P.M. Wielders, klinisch chemicus (senior lid, NVKC)
Met dank aan
- Dr. L.H.J. Jacobs, klinisch chemicus, Meander Medisch Centrum (NVKC)
- Dr. J.M.W. van den Ouweland, klinisch chemicus, Dicoon (NVKC)
- Mr. E. van Pernis, manager bezwaar en beroep divisie rijgeschiktheid CBR
- R.A. Bredewoud, arts, hoofd medische zaken CBR
Met ondersteuning van
- Dr. L.C. Houtepen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. B. Vogelaar, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. M. Lenaers, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- E. (Esther) van der Bijl, informatiespecialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van de clusterleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Gemelde (neven)functies en belangen stuurgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Datum |
Restrictie |
|
Sisco van Veen |
Psychiater bij ggz ingeest en postdoctoraal onderzoeker bij het Amsterdam UMC en 113 zelfmoordpreventie. |
* Bestuurslid ThaNet. * Podcastmaker bij Prelum uitgevers. * Dagvoorzitter bij BSL uitgevers. |
Geen |
Geen |
Mijn onderzoek wordt mede gefinancierd door de NVVE en stichting VCVGZ. Voor de bestuursfunctie bij ThaNet ontvang het Amsterdam UMC vacatiegelden via het UMC Groningen vanuit min VWS. *NVVE: Persisterende doodswensen, projectleider. *Suicidaliteit bij mensen met een psychiatrische eutheanasiewens, projectleider |
Geen |
04-06-2024 |
Alle moduleteksten en aanbevelingen werden besproken in de stuurgroep onder voorzitterschap van Aartjan Beekman, alvorens ze zijn vastgesteld. |
|
Natalie Veen |
psychiater, opleider, GGZ Delfland |
commissie lid geschillen commissie (onbezoldigd) |
Geen |
Geen |
Geen |
Geen |
11-06-2024 |
Geen restricties |
|
Theo Ingenhoven |
Arkin, NPI, Amsterdam |
ZZPer en docent bij RINO |
Geen |
Geen |
Geen |
Geen |
22-11-2024 |
Geen restricties |
|
Aartjan Beekman (voorzitter) |
Amsterdam UMC hoogleraar psychiatrie |
Raad van Toezicht Informatie Voorziening Zorg Raad van Toezicht NIVEL Stuurgroep landelijke agenda Suicidepreventie Diverse onderzoeksconsortia en gerelateerde stuurgroepn Referee voor diverse wetenschapopelijke bladen en onderzoeksorganisaties. |
Geen |
Geen |
De afgelopen drie jaar geen onderzoek gefinancierd door de farmaceutische industrie of door andere commerciële partijen. |
Ik heb in het verleden verschillende functies gehad bij de NVvP – o.a. voorzitter geweest tussen 2012 en 2016. |
22-07-2024 |
Geen restricties |
|
Dick Ravelli |
Directeur behandeling Max Ernst GGZ (2006) 0,4 fte. Lector Academie Beleidspsychiatrie(1999) 0,1 fte. Lid klachtencommissie GGZ Centraal (2020) 0,1 fte. Keurend specialist voor CBR (1999) 0,2 fte. |
Geen |
Geen |
Geen |
Geen |
Geen |
06-10-2025 |
Geen restricties |
|
Sabine Roza |
Universitair Hoofddocent Forensische Psychiatrie bij Erasmus MC: 8 uur per week (betaald) Universitair Hoofddocent Forensische Psychiatrie bij Erasmus MC: 8 uur per week (betaald) Psychiater en directeur Pieter Baan Centrum bij Nederlands Instituut voor Forensische Psychiatrie (onderdeel van Dienst Justitiële Inrichtingen, bij Ministerie van Justitie & Veiligheid): 32 uur / week (betaald). |
Gerechtelijk deskundige in strafzaken Jeugd en strafzaken Volwassenen (binnen dienstverband NIFP en als zzp (betaald).
Lid Adviescollege Verloftoetsing tbs (betaald). Toetser Nederland Register voor Gerechtelijk Deskundigen (betaald). |
Geen |
Geen |
Financier 1: Stichting tot Steun VCVGZ: Niet-aangeboren hersenletsel bij forensisch-psychiatrische patienten.
Financier 2: Stichting tot Steun VCVGZ: Sekseverschillen in delictgedrag, projectleider. raakt slechts indirect aan de richtlijn Psychiatrisch onderzoek en rapportage in strafzaken. Financier 3: ZonMW: Regionale kenniswerkplaats Onbegrepen Gedrag rotterdam-Rijnmond. |
Uitsluitend t.a.v. de richtlijn Psychiatrisch onderzoek en rapportage in strafzaken is vanwege mijn forensisch-psychiatrische expertise en reputatie hiervan enig voordeel te verwachten. |
15-08-2024 |
Geen restricties |
Gemelde (neven)functies en belangen expertisegroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Datum |
Restrictie |
|
Jos Wielders |
Geen werkgever meer wegens pensioen. Laatste functie van medisch manager lab Klinische Chemie, Meander Medisch Centrum, Amersfoort |
Voorzitter WG CDT standaardisatie van de Int. Federation Clinical Chemistry. Onbetaalde wetenschappelijke nevenfunctie voor opgeteld ca 2 weken per jaar. |
Geen financieel belang bij het effect van de Richtlijn op het gebruik van biomarkers CDT en GGT door laboratoria of opdrachtgevers (Psychiaters / CBR) |
Geen familie of vrienden, collega's die een financieel belang hebben, |
Niet van toepassing |
Uitkomst richtlijn heeft geen effect. |
Niet van toepassing |
30-04-2025 |
Geen restricties |
|
Ferry Bergkamp |
Klinisch chemicus Atalmedail Amsterdam (betaald hoofdwerkzaamheden) |
Voorzitter WG CDT van de NVKC. Onbetaalde wetenschappelijke nevenfunctie voor opgeteld ca 1 week per jaar. |
Geen |
Geen |
Geen |
Geen |
Geen |
06-06-2024 |
Geen restricties |
Inbreng patiëntenperspectief
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
|
Module |
Uitkomst raming |
Toelichting |
|
Laboratoriumonderzoek bij alcoholmisbruik |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Zoekstrategie - 25 maart 2025
Embase.com
|
No. |
Query |
Results |
|
#1 |
'alcohol consumption'/exp OR 'alcohol abuse'/exp OR 'drinking behavior'/exp OR 'alcohol blood level'/exp OR 'driver licence'/exp OR 'driving ability'/exp OR (('alcoholism'/exp OR alcoholism:ti,ab,kw) AND ('licensing'/exp OR 'drive'/exp OR 'driver'/exp OR drive*:ti,ab,kw OR driving*:ti,ab,kw OR licenc*:ti,ab,kw OR licens*:ti,ab,kw)) OR (((drive* OR driving*) NEAR/2 (licenc* OR licens* OR behavior* OR behaviour* OR ability OR abilities OR fitness OR skill* OR intox*)):ti,ab,kw) OR (((alcohol* OR ethanol*) NEAR/3 (consumption* OR consume OR consuming* OR intake* OR 'mis us*' OR abus* OR misus*)):ti,ab,kw) OR (((drink* OR drunk*) NEAR/3 (problem* OR heavy OR chronic* OR binge OR excessive OR hazardous OR severe OR blackout* OR 'black out*' OR college OR driving* OR behavior* OR behaviour* OR habit* OR pattern* OR drive*)):ti,ab,kw) OR 'alcohol* blood':ti,ab,kw OR 'blood alcohol*':ti,ab,kw OR alcoholemia:ti,ab,kw OR 'blood ethanol*':ti,ab,kw OR 'ethanol* blood':ti,ab,kw OR 'serum alcohol*':ti,ab,kw OR 'serum ethanol*':ti,ab,kw OR 'driving* under the influence*':ti,ab,kw OR 'driving* under influence*':ti,ab,kw OR 'drive* under the influence*':ti,ab,kw OR 'drive* under influence*':ti,ab,kw OR dui:ti,ab,kw OR duis:ti,ab,kw OR owi:ti,ab,kw |
359942 |
|
#2 |
'carbohydrate deficient transferrin'/exp OR 'carbohydrate* deficient transferrin*':ti,ab,kw OR cdt:ti,ab,kw OR 'cdt hplc*':ti,ab,kw OR 'capillary electrophoresis'/exp OR 'capillary electrophoresis':ti,ab,kw OR 'hpce':ti,ab,kw OR 'latex'/de OR 'latex':ti,ab,kw OR 'gamma glutamyltransferase'/exp OR 'gamma glutamyl transferase':ti,ab,kw OR 'gamma gt':ti,ab,kw OR 'glutamic transferase':ti,ab,kw OR 'glutamyl transferase':ti,ab,kw OR 'glutamyl transpeptidase':ti,ab,kw OR 'glutamyltransferase':ti,ab,kw OR 'glutamyltranspeptidase':ti,ab,kw OR 'transpeptidase':ti,ab,kw OR ggt:ti,ab,kw |
150765 |
|
#3 |
'sensitivity and specificity'/de OR sensitivity:ab,ti OR specificity:ab,ti OR predict*:ab,ti OR 'roc curve':ab,ti OR 'receiver operator':ab,ti OR 'receiver operators':ab,ti OR likelihood:ab,ti OR 'diagnostic error'/exp OR 'diagnostic accuracy'/exp OR 'diagnostic test accuracy study'/exp OR 'inter observer':ab,ti OR 'intra observer':ab,ti OR interobserver:ab,ti OR intraobserver:ab,ti OR validity:ab,ti OR kappa:ab,ti OR reliability:ab,ti OR reproducibility:ab,ti OR ((test NEAR/2 're-test'):ab,ti) OR ((test NEAR/2 'retest'):ab,ti) OR 'reproducibility'/exp OR accuracy:ab,ti OR 'differential diagnosis'/exp OR 'validation study'/de OR 'measurement precision'/exp OR 'diagnostic value'/exp OR 'reliability'/exp OR 'predictive value'/exp OR ppv:ti,ab,kw OR npv:ti,ab,kw OR (((false OR true) NEAR/3 (negative OR positive)):ti,ab) |
6796469 |
|
#4 |
#1 AND #2 AND #3 |
2283 |
|
#5 |
#4 AND [2018-2025]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
674 |
|
#6 |
'meta analysis'/exp OR 'systematic review'/exp OR 'scoping review'/exp OR 'rapid review'/exp OR 'umbrella review'/exp OR 'cochrane database of systematic reviews'/jt OR 'network meta-analysis'/exp OR 'networkmeta analy*':ti,ab,kw OR 'networkmetaanaly*':ti,ab,kw OR metaanaly*:ti,ab,kw OR 'meta analy*':ti,ab,kw OR metanaly*:ti,ab,kw OR prisma:ti,ab,kw OR prospero:ti,ab,kw OR metaanali*:ti,ab,kw OR 'meta anali*':ti,ab,kw OR metanali*:ti,ab,kw OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab,kw) OR (((structured OR systemic*) NEAR/3 (review* OR overview* OR synth*) NEAR/3 literature):ti,ab,kw) OR ((systemic* NEAR/1 review*):ti,ab,kw) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab,kw) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab,kw) OR (((literature NEAR/3 (review* OR overview*)):ti,ab,kw) AND (search*:ti,ab,kw OR database*:ti,ab,kw OR 'data base*':ti,ab,kw)) OR (('data extraction*':ti,ab,kw OR 'data source*':ti,ab,kw) AND ('study selection*':ti,ab,kw OR 'studies selection*':ti,ab,kw)) OR ('search strateg*':ti,ab,kw AND 'selection criteria*':ti,ab,kw) OR ('data source*':ti,ab,kw AND 'data synth*':ti,ab,kw) OR medline*:ti,ab,kw OR pubmed*:ti,ab,kw OR 'pub med*':ti,ab,kw OR embase:ti,ab,kw OR cochrane*:ti,ab,kw OR (((critical* OR rapid*) NEAR/2 (review* OR overview* OR synth*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synth*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynth*:ti,ab,kw OR 'meta synth*':ti,ab,kw OR 'review* of review*':ti,ab,kw |
1093584 |
|
#7 |
'randomized controlled trial'/exp OR 'clinical trial'/exp OR 'randomization'/de OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'triple blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ti,ab OR ((random* NEAR/2 (trial OR study)):ti,ab) OR ((random* NEAR/7 (trial OR trail OR 'clinical trial' OR 'clinical trail' OR 'clinical study' OR 'multicenter study' OR crossover OR 'cross over')):ti) OR (((randomised OR randomized) NEXT/6 study):ti) OR 'random* control* clinical trial':ti,ab OR 'random* control* clinical trail':ti,ab OR 'random* control* clinical study':ti,ab OR ((('single blind*' OR 'double blind*' OR 'triple blind*' OR 'quadruple blind*') NEAR/4 (study OR trial OR trail OR design)):ti,ab) OR placebo*:ti,ab OR ((randomly NEAR/1 assign*):ti,ab) OR ((random* NEAR/3 distribut* NEAR/7 group*):ti,ab) OR (((pragmatic OR practical) NEXT/1 ('clinical trial' OR 'clinical trail')):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEXT/3 (trial OR trail)):ti,ab) OR ((random* NEAR/4 ('cross over*' OR crossover*) NEAR/4 (trial OR trail OR study OR design)):ti,ab) OR ((phase NEAR/5 ('clinical trial' OR 'clinical trail' OR randomized OR randomised)):ti) OR ((random* NEAR/3 phase NEAR/3 (trial OR trail OR study)):ti,ab) |
3299215 |
|
#8 |
'major clinical study'/de OR 'clinical study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'cohort analysis'/de OR 'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
17932163 |
|
#9 |
#5 AND #6 - SR |
22 |
|
#10 |
#5 AND #7 NOT #9 - RCT |
143 |
|
#11 |
#5 AND #8 NOT (#9 OR #10) - Observationeel |
447 |
|
#12 |
#9 OR #10 OR #11 - Totaal |
612 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp "Driving Under the Influence"/ or exp Alcohol Drinking/ or exp Alcoholism/ or Drinking Behavior/ or exp Blood Alcohol Content/ or exp Automobile Driving/ or Licensure/ or ((drive* or driving*) adj2 (licenc* or licens* or behavior* or behaviour* or ability or abilities or fitness or skill* or intox*)).ti,ab,kf. or ((alcohol* or ethanol*) adj3 (consumption* or consume or consuming* or intake* or mis us* or abus* or misus*)).ti,ab,kf. or ((drink* or drunk*) adj3 (problem* or heavy or chronic* or binge or excessive or hazardous or severe or blackout* or black out* or college or driving* or behavior* or behaviour* or habit* or pattern* or drive*)).ti,ab,kf. or alcohol* blood.ti,ab,kf. or blood alcohol*.ti,ab,kf. or alcoholemia.ti,ab,kf. or blood ethanol*.ti,ab,kf. or ethanol* blood.ti,ab,kf. or serum alcohol*.ti,ab,kf. or serum ethanol*.ti,ab,kf. or driving* under the influence*.ti,ab,kf. or driving* under influence*.ti,ab,kf. or drive* under the influence*.ti,ab,kf. or drive* under influence*.ti,ab,kf. or dui.ti,ab,kf. or duis.ti,ab,kf. or owi.ti,ab,kf. |
266293 |
|
2 |
exp Electrophoresis, Capillary/ or exp gamma-Glutamyltransferase/ or exp Latex/ or carbohydrate* deficient transferrin*.ti,ab,kf. or cdt.ti,ab,kf. or cdt hplc*.ti,ab,kf. or capillary electrophoresis.ti,ab,kf. or hpce.ti,ab,kf. or latex.ti,ab,kf. or gamma glutamyl transferase.ti,ab,kf. or gamma gt.ti,ab,kf. or glutamic transferase.ti,ab,kf. or glutamyl transferase.ti,ab,kf. or glutamyl transpeptidase.ti,ab,kf. or glutamyltransferase.ti,ab,kf. or glutamyltranspeptidase.ti,ab,kf. or transpeptidase.ti,ab,kf. or ggt.ti,ab,kf. |
87000 |
|
3 |
exp "Sensitivity and Specificity"/ or (sensitivity or specificity).ti,ab. or (predict* or ROC-curve or receiver-operator*).ti,ab. or (likelihood or LR*).ti,ab. or exp Diagnostic Errors/ or (inter-observer or intra-observer or interobserver or intraobserver or validity or kappa or reliability).ti,ab. or reproducibility.ti,ab. or (test adj2 (re-test or retest)).ti,ab. or "Reproducibility of Results"/ or accuracy.ti,ab. or Diagnosis, Differential/ or Validation Study/ or ((false or true) adj3 (negative or positive)).ti,ab. |
5381940 |
|
4 |
1 and 2 and 3 |
1085 |
|
5 |
limit 4 to yr="2018 -Current" |
149 |
|
6 |
5 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
148 |
|
7 |
exp Meta-Analysis/ or exp Network Meta-Analysis/ or exp Systematic Review/ or (networkmeta analy* or networkmetaanaly* or metaanaly* or meta analy* or metanaly* or prisma or prospero or metaanali* or meta anali* or metanali*).ti,ab,kf. or ((systemati* or scoping or umbrella or structured literature) adj3 (review* or overview*)).ti,ab,kf. or ((structured or systemic*) adj3 (review* or overview* or synth*) adj3 literature).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 (review* or overview*)) and (search* or database* or data base*)).ti,ab,kf. or ((data extraction* or data source*) and (study selection* or studies selection*)).ti,ab,kf. or (search strateg* and selection criteria*).ti,ab,kf. or (data source* and data synth*).ti,ab,kf. or (medline* or pubmed* or pub med* or embase or cochrane*).ti,ab,kf. or cochrane.jw. or ((critical* or rapid*) adj2 (review* or overview* or synth*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synth*)) and (search* or database* or data base*)).ab. or metasynth*.ti,ab,kf. or meta synth*.ti,ab,kf. |
819634 |
|
8 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2868106 |
|
9 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or exp cohort studies/ or epidemiologic studies/ or ((multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ |
7982625 |
|
10 |
6 and 7 - SR |
4 |
|
11 |
(6 and 8) not 10 - RCT |
21 |
|
12 |
(6 and 9) not (10 or 11) - Observationeel |
92 |
|
13 |
10 or 11 or 12 - Totaal |
117 |