ART
Uitgangsvraag
Welke ART is geïndiceerd bij paren met mannelijke subfertiliteit?
De uitgangsvraag omvat de volgende deelvragen die deels op basis van expert opinion in de overwegingen aan bod komen:
- Wat is het afkappunt van semenkwaliteit voor IUI, IVF of ICSI? Wat is de ondergrens van de semenkwalilteit na opwerken, om te spreken van een zinvolle IUI-poging?
- Wat zijn de adviezen ten aanzien van abstinentietijd bij mannen met een extreme OAT, die behandeld worden met ART?
- Wanneer moet semen cryopreservatie voor toekomstig gebruik met ART overwogen worden?
Aanbeveling
Aanbeveling-1a
Adviseer een expectatief beleid voor de duur van tenminste 6 maanden bij paren met subfertiliteit op basis van een mannelijke factor met een VCM tussen 3-10 miljoen en een Hunault score ≥ 30% .
Aanbeveling-1b
Overweeg 6 IUI-behandeling in de natuurlijke cyclus bij paren met subfertiliteit op basis van een mannelijke factor met een VCM tussen 3-10 miljoen en na opwerken een VCM >1 miljoen en een Hunault score < 30%, of bij een score > 30% na een expectatieve periode van tenminste 6 maanden.
Aanbeveling-1c
Overweeg 6 IUI-behandeling bij paren met subfertiliteit op basis van een mannelijke factor en na opwerken een VCM >1 miljoen. Neem in deze overweging ook andere fertiliteitsbepalende factoren mee.
Aanbeveling-1d
Adviseer een ICSI-behandeling bij paren met subfertiliteit op basis van een mannelijke factor met een VCM <1 miljoen voor of na opwerken.
Aanbeveling-2
Overweeg IVF bij het uitblijven van een zwangerschap (na IUI-behandeling) bij paren met subfertiliteit op basis van een mannelijke factor met een concentratie 5–15 × 10⁶ per mL en/of progressieve motiliteit 10-32% voor opwerken.
Aanbeveling-3
Adviseer voor een ICSI-behandelingen een abstinentie periode tussen de 1 en 2 dagen.
Aanbeveling-4
Overweeg semenpreservatie in de volgende gevallen:
- Bij ejaculatieproblemen om te voorkomen dat er geen zaadcellen beschikbaar zijn op de dag van follikelpunctie.
- Na vasovasostomie met nadien:
- cryptozoöspermie (zaadcel concentratie < 1x106/ml);
- extreme oligozoöspermie (zaadcel concentratie < 5x106/ml) en/of
- ernstige asthenozoöspemie (progressieve motiliteit < 20%) en/of
- een VCM ≤ 3.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Indien er sprake is van verminderde semenkwaliteit bij paren met subfertiliteit kan er een afweging gemaakt worden of en zo ja welke geassisteerde voortplantingstechniek het meest passend is. Hierbij kan gedacht worden aan de prognose voor natuurlijke conceptie van het paar, de semenkwaliteit, zwangerschapskansen per behandeling, de veiligheid en kosten van de verschillende behandelingen. In de klinische praktijk wordt meestal de VCM vóór opwerking van het semen gebruikt om een afkappunt te definiëren, maar in de literatuur worden vaak verschillende definities gebruikt met verschillende afkapwaarden van semen parameters om onderscheid te maken tussen milde, matige en ernstige mannelijke subfertiliteit. Daarnaast de semenanalyse een multi parametrische test waarbij niet alleen de VCM beoordeeld dient te worden maar ook het percentage progressief motiele spermatozoa, morfologie, pH en volume. Voor de beoordeling van de semenanalyse verwijzen we naar de WHO laboratory manual for the examination and processing of human semen (WHO, 2021).
Gezien de beperkte beschikbare literatuur is een deel van de aanbevelingen geformuleerd op basis van expert opinion. Deze aanbevelingen zijn bedoeld als handvatten voor de behandeling van paren met subfertiliteit op basis van een mannelijke factor. Echter per laboratorium kunnen andere afwegingen gemaakt worden op basis van validatie van eigen data.
VCM vóór opwerken 3-10 miljoen
Bij een milde mannelijke factor (VCM 3-10 miljoen) kan er onderscheid gemaakt worden in paren met een goede kans op zwangerschap in de eerstvolgende 12 maanden en paren met een minder goede kans op zwangerschap. Deze kans kan berekend worden m.b.v. de Hunault score zoals deze ook geadviseerd wordt in de richtlijn onverklaarde subfertiliteit, waarbij er een behandelindicatie bestaat bij een prognose op natuurlijke conceptie onder de 30%.
IUI versus IVF
De beschikbare studies laten zien dat IVF bij paren met een milde mannelijke factor waarschijnlijk niet zal leiden tot meer zwangerschappen vergeleken met IUI. Ook leidde IUI niet tot meer meerlingzwangerschappen, indien strikte cancel criteria werden gebruikt voor het aantal preovulatoire follikels bij ovariële stimulatie. Derhalve heeft het de voorkeur om eerst te starten met IUI. De review van Cissen et al. laat tevens zien dat er onvoldoende bewijs is om gecontroleerde hyperstimulatie voor de indicatie mannelijke subfertiliteit toe te passen bij IUI, hoewel de kwaliteit van de evidence zeer laag was.
IVF versus ICSI
De studie van Wang (2024) laat zien dat ICSI niet tot meer zwangerschappen zal leiden in vergelijking met IVF bij een milde mannelijke factor. Milde mannelijke subfertiliteit werd in deze studie gedefinieerd als oligoasthenozoospermie (concentratie 5–15 × 10⁶ per mL en progressieve motiliteit 10–32%), oligozoospermie (concentratie 5–15 × 10⁶ per mL en progressieve motiliteit van ≥32%), of asthenozoospermie (concentratie ≥15 × 10⁶ mL en progressieve motiliteit 10–32%). Het aantal total fertilization failures in deze studie verschilt niet significant tussen de ICSI- en IVF-groep. Het nadeel van een ICSI-behandeling is dat dit meer apparatuurskosten en meer personele inzet met zich meebrengt voor het laboratorium. Ook brengt een ICSI behandeling potentieel meer risico’s met zich mee omdat het een invasieve behandeling is en meer stappen met zich meebrengt.
VCM 1-3 miljoen
Bij mannelijke subfertiliteit en een semenanalyse met een VCM tussen 1 en 3 miljoen voor opwerking wordt in de praktijk behandeling met IUI of IVF/ICSI aangeraden omdat dit waarschijnlijk een hogere kans geeft op een zwangerschap dan expectatief beleid. Welke behandeling de voorkeur heeft is op basis van de beschikbare literatuur niet duidelijk. De risico’s van IVF/ICSI dienen dan afgewogen te worden tegen de lagere risico’s en kosten van een IUI-behandeling zonder stimulatie.
Hoewel er geen studies bekend zijn die aangeven wanneer er een semenopwerkingstest (SOT) gedaan moet worden, kan het toch helpen in de besluitvorming of een IUI-behandeling zinvol zou kunnen zijn. Bij VCM-waarden na opwerking tussen de 1 x 106 en 9 x 106 is er een graduele stijging in de kansen op een zwangerschap na IUI, variërend van 7.45% bij een waarde tussen de 1.00-1.99 x 106 tot 16.70% kans bij een waarde ³9 x 106. Vanaf 2 x 106 is de kans op een zwangerschap boven de 10% per cyclus Muthigi (2021). Bij een VCM na opwerking <1x106 progressief beweeglijke zaadcellen is de kans op een zwangerschap <5% en daarmee lijkt een IVF of ICSI-behandeling de voorkeur te hebben (Ombelet, 2014; Muthigi, 2021). Bij een VCM na opwerking <1x106 progressief beweeglijke zaadcellen lijkt IVF geen goed alternatief voor IUI, gezien het risico op een TFF waarschijnlijk hoger dan 25% is (Rhemrev 2001), Echter kan op basis van het eicellen ook de afweging gemaakt worden om bij high responders (>15 follikels) een IVF behandeling uit te voeren aangezien daarbij de kans op een TFF lager ligt (kans op TFF <25 % bij 0.35 x 10^6 progressief motiele spermatozoa). Andersom kan bij een low responder (<4 follikels) de kans op een TFF hoger komen te liggen bij een lage opwerking (kans op TFF <25% bij 2.2 x 10^6 progressief motiele spermatozoa). Elk laboratorium kan op basis van eigen data een ander afkappunt hanteren.
Er zijn voor zover bekend geen studies die het optimale aantal IUI-behandelingen hebben onderzocht bij paren met mannelijke subfertiliteit. Custers (2008) heeft in een retrospectieve cohortstudie onderzocht wat de cumulatieve kansen zijn bij IUI-behandeling bij paren met mannelijke en onbegrepen subfertiliteit. Na 3 cycli was 18% van de vrouwen zwanger en dit nam toe naar 30% en 41% na respectievelijk 6 en 9 behandelcycli. Bij de afweging wanneer over te stappen naar IVF/ICSI kan de leeftijd van de vrouw en de opwerkresultaten van het semen meehelpen in deze keuze.
VCM < 1 miljoen
In de regel lijkt het uitvoeren van een SOT bij een VCM <1x106 niet nodig en is een ICSI-behandeling gerechtvaardigd (Rhemrev 2001). Wel dient er het semenonderzoek herhaalt te worden, bij voorkeur met een tussenperiode van 3 maanden. Indien bij herhaling een azoöspermie gevonden wordt, dient het paar verwezen de worden naar een TESE centrum. Voor behandeling NOA, zie module Niet Obstructieve azoöspermie (NOA). Ook dient er genetisch onderzoek ingezet te worden, zie module Genetisch onderzoek.
Ejaculatie abstinentie-advies
Het WHO-handboek voor semenanalyse hanteert een abstinentieperiode van 2-7 dagen voor een semenanalyse. Voor IUI-behandelingen zijn er voor zover bekend geen studies die een optimale abstinentieperiode hebben onderzocht. Voor ICSI-behandelingen zijn er steeds meer aanwijzingen dat een kortere abstinentie periode (variërend van één dag tot één uur) leidt tot betere sperma motiliteit, blastocyst vorming, hogere euploïdie ratio en meer klinische zwangerschappen (Ayad, 2018; Scarselli, 2019), zie module Aanvullende tests: Sperma DNA fragmentatie. Dit is echter nog niet aangetoond in een RCT.
Cryopreservatie semen
Er is met name veel literatuur over cryopreservaite van semen bij postpuberale jongens en mannen voorafgaand aan een oncologische behandeling. Er kunnen echter ook andere oorzaken zijn waarbij overwogen kan worden om semen in te vriezen, denk hierbij aan status na torsio testis of bij extreme OAT met in de toekomst kinderwens. De werkgroep is van mening dat hier terughoudend mee omgegaan moet worden. Het is onbekend om hoeveel mannen het gaat die niet spontaan of middels ART met ejaculaat een zwangerschap tot stand kunnen brengen en uiteindelijk een TESE-behandeling moeten ondergaan of kinderloos blijven.
Een indicatie waarbij wel semen preservatie overwogen kan worden is bij mannen na een vasovasotomie. De werkgroep stelt op basis van expert opinion en praktijkervaring vast, dat het risico op re-stenose in deze groep ongeveer 10% is. De indruk bestaat dat bij ernstige oligospermie in het eerste postoperatieve spermaonderzoek, het risico op re-stenose aanzienlijk hoger is, dan wanneer sprake is van normospermie of milde oligospermie. Zie richtlijn obstructieve azoöspermie.
Bij ejaculatieproblemen kan het helpen om vooraf semen in te vriezen om de druk op de dag van de punctie te verlagen.
Kwaliteit van bewijs
De overall kwaliteit van bewijs voor PICO 1 (ICSI of IVF versus IUI) is zeer laag. De overall kwaliteit van bewijs voor PICO 2 (ICSI versus IVF) is laag. Dit betekent dat we (zeer) onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege (zeer) ernstige:
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grens/beide grenzen van klinische relevantie overschrijdt, vanwege het niet bereiken van de optimale steekproefgrootte, vanwege een zeer klein aantal events bij een kleine steekproefgrootte.
Waarden en voorkeuren van patiënten (en eventueel hun partner)
Voor het bereiken van een zo gewenste zwangerschap, kan bij een mannelijke factor ART gewenst zijn. ART behandelingen brengen echter ook risico’s met zich mee, waarbij met name bij IVF/ICSI behandeling complicaties kunnen optreden, zoals een bloeding na punctie en OHSS. Hoewel sommige patiënten terughoudend zijn om ART te starten, zijn er ook patiënten die zo snel mogelijk een IVF/ICSI behandeling willen ondergaan, hoewel hier bij een nog gunstige prognose of milde mannelijke factor geen indicatie voor is. Hier zijn soms de verlangens van de patiënt niet in lijn met de aanbeveling in deze richtlijn.
Bij een VCM tussen de 3-10 x 10^6 kan de afweging gemaakt worden om een semenopwerkings test uit te voeren of direct te starten met een IUI-behandeling. In dat geval dient met patiënt en partner besproken te worden dat er een kans bestaat dat bij 2-maal een VCM na opwerken <1 x 10^6 er alsnog een indicatie is voor een IVF/ICSI behandeling. Wel dienen andere factoren meegewogen te worden zoals een koorts episode.
Kostenaspecten
Een ART behandeling brengt altijd meer kosten met zich mee dan een expectatief beleid. Als er wel een indicatie voor ART behandeling is, dan zijn de kosten van IVF hoger dan IUI met dezelfde zwangerschapskansen bij een milde mannelijke factor. Echter na meerdere IUI-behandelingen in de natuurlijke cyclus dient de VCM na opwerking meegewogen te worden in de beslissing om door te gaan met IUI behandelingen of over te stappen op een IVF/ICSI behandeling. Indien de semenopwerking bij herhaling tussen de 1-2 x 10^6 is, dan is het de vraag of IVF/ICSI niet kosten-effectiever. Bij een opwerking van >2 x 10^6 kan men doorgaan tot 6 IUI behandeling, indien dan geen zwangerschap is ontstaan is het advies om over te stappen op een IVF/ICSI behandeling.
Gelijkheid ((health) equity/equitable)
Niet van toepassing.
Aanvaardbaarheid
De werkgroep voorziet geen ethische bezwaren.
Duurzaamheid
Er is geen onderzoek gedaan of een serie IUI-behandelingen duurzamer is dan IVF ten aanzien van medicatiegebruik en afval. Wel kan elk centrum nagaan hoe men duurzamer kan werken zoals minder medicatie verspilling, geen gebruik maken van plastic specula, reduceren van afval.
Haalbaarheid
De interventies zijn al gangbare behandelingen.
Rationale van aanbeveling-1: weging van argumenten voor en tegen de interventies
Bij een milde mannelijke factor (VCM 3-10 miljoen) kan er op basis van de Hunault score onderscheid gemaakt worden in paren met een goede kans op een spontane zwangerschap in de eerstvolgende 12 maanden en paren met een minder goede kans op zwangerschap waarbij er een indicatie is voor een IUI behandeling.
De beschikbare studies laten zien dat IVF bij paren met een milde mannelijke factor waarschijnlijk niet zal leiden tot meer zwangerschappen vergeleken met IUI. Op basis van bewijs van lage kwaliteit lijkt gecontroleerde hyperstimulatie voor de indicatie mannelijke subfertiliteit niet van meerwaarde.
Bij een VCM na opwerking <1x106 progressief beweeglijke zaadcellen lijkt IVF geen goed alternatief voor IUI, gezien het risico op een TFF waarschijnlijk hoger dan 25% is. Indien er meer dan 15 follikels aanwezig zijn, kan deze cut-off mogelijk lager liggen. Er is echter onvoldoende data om een advies te geven wat die ondergrens is en of percentage type A motiliteit hierin meegenomen dient te worden.
Eindoordeel:
Zwakke aanbeveling voor afwegen van verschillende behandelopties.
Rationale van aanbeveling-2: weging van argumenten voor en tegen de interventies
Indien er geen zwangerschap is ontstaan na meerdere IUI behandelingen of als er direct gekozen wordt voor IVF/ICSI op basis van andere factoren, dan kan er bij een milde mannelijke factor gedefinieerd als oligoasthenozoospermie (concentratie 5–15 × 10⁶ per mL en progressieve motiliteit 10–32%), oligozoospermie (concentratie 5–15 × 10⁶ per mL en progressieve motiliteit van ≥32%), of asthenozoospermie (concentratie ≥15 × 10⁶ mL en progressieve motiliteit 10–32%) gekozen worden voor een IVF behandeling. Indien op de dag van de punctie na opwerken <1 miljoen progressief bewegende spermatozoa aanwezig zijn dient een ICSI behandeling overwogen te worden afhankelijk van het aantal verkregen eicellen.
Eindoordeel:
Zwakke aanbeveling voor overstappen naar IVF.
Rationale van aanbeveling-3: weging van argumenten voor en tegen de interventies
Voor ICSI-behandelingen zijn er steeds meer aanwijzingen dat een kortere abstinentie periode (variërend van één dag tot één uur) leidt tot minder oxidatieve schade en derhalve betere sperma motiliteit, blastocyst vorming, hogere euploïdie ratio en meer klinische zwangerschappen. Dit is echter nog niet aangetoond in een RCT, derhalve is het expert opinion om een abstinentie periode van 1-2 dagen te hanteren. Als er op de dag van productie geen/niet genoeg zaadcellen worden gevonden, vraag de man om nogmaals te produceren.
Eindoordeel:
Zwakke aanbeveling voor abstinentie periode van 1 tot 2 dagen.
Rationale van aanbeveling-4: weging van argumenten voor en tegen de interventies
Semenpreservatie voor niet-oncologische indicaties is niet gebruikelijk. Voor enkele indicaties kan dit echter overwogen worden.
Eindoordeel:
Zwakke aanbeveling voor semenpreservatie.
Onderbouwing
IUI, IVF, and ICSI treatments aim to increase the likelihood of a live birth in couples dealing with male subfertility. However, it is still unclear at what threshold of the total number of progressively motile spermatozoa (i.e. Total Motal Sperm Count: TMSC) before or after processing one should opt for expectant management, IUI (with or without stimulation), IVF, or ICSI. In addition to TMSC, other findings may also influence treatment recommendations, such as the Hunault score, sperm morphological characteristics, or sperm DNA fragmentation.
Summary of Findings
The effect of different assisted reproductive technologies compared to each other on the chance of pregnancy in couples with male subfertility.
PICO 1
Population: Couples with diagnosis subfertility
Intervention: ICSI or IVF
Comparison: IUI
|
Outcome
|
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Conclusion |
|
|
IUI in natural cycles |
IVF |
||||
|
Live birth rate (critical) |
Relative risk: 0.85 (CI 95% 0.42 - 1.71) Based on data from 53 participants in 1 study
|
407 per 1000 |
346 per 1000 |
Very low Due to very serious imprecision1 |
The evidence is very uncertain about the effect of IVF compared to IUI in natural cycles on live birth rate in couples with mild male subfertility.
(Goverde, 2000). |
|
Difference: 61 fewer per 1000 (CI 95% 236 fewer - 289 more) |
|||||
|
Pregnancy rate, miscarriage rate, multiple pregnancy, OHSS, total fertilization failure (important) |
- |
- |
No GRADE |
Not enough information was given regarding the effect of IVF compared to IUI in natural cycles on pregnancy rate, miscarriage rate, multiple pregnancy, OHSS, total fertilization failure in couples with male subfertility. Therefore, GRADE was not determined. |
|
Outcome
|
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Conclusion |
|
|
IUI in cycles with ovarian hyperstimulation |
IVF |
||||
|
Live birth rate (critical) |
Relative risk: 1.03 (CI 95% 0.66 - 1.61) Based on data from 86 participants in 2 studies
|
452 per 1000 |
466 per 1000 |
Very low Due to very serious imprecision2 |
The evidence is very uncertain about the effect of IVF compared to IUI in cycles with ovarian hyperstimulation on live birth rate in couples with mild male subfertility.
(Bensdorp, 2015 & Goverde, 2000). |
|
Pregnancy rate (critical) |
Relative risk: 1.09 (CI 95% 0.67 - 1.79) Based on data from 36 participants in 1 studies
|
611 per 1000 |
666 per 1000 |
Very low Due to very serious imprecision3 |
The evidence is very uncertain about the effect of IVF compared to IUI in cycles with ovarian hyperstimulation on pregnancy rate in couples with mild male subfertility. (Bensdorp, 2015)
|
|
Difference: 55 more per 1000 (CI 95% 202 fewer - 483 more) |
|||||
|
Miscarriage rate, multiple pregnancy, OHSS, total fertilization failure (important) |
- |
- |
No GRADE |
Not enough information was given regarding the effect of IVF compared to IUI in cycles with ovarian hyperstimulation on miscarriage rate, multiple pregnancy, OHSS, total fertilization failure in couples with male subfertility. Therefore, GRADE was not determined. |
1. Imprecision: very serious. Wide confidence interval that crosses the borders for clinical relevance on both sides, only data from one study, low number of patients;
2. Imprecision: very serious. Wide 95% confidence interval that crosses the borders for clinical relevance on both sides, low number of patients;
3. Imprecision: very serious. Wide 95% confidence interval that crosses the borders for clinical relevance on both sides, only data from one study, low number of patients.
PICO 2
Population: Couples with diagnosis subfertility
Intervention: ICSI
Comparison: IVF
|
Outcome
|
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Conclusion |
|
|
IVF |
ICSI |
||||
|
Pregnancy rate (critical) |
Relative risk: 0.95 (CI 95% 0.86 - 1.04) Based on data from 2329 participants in 1 study
|
424 per 1000 |
403 per 1000 |
Low Due to serious imprecision4 |
ART with ICSI may result in little to no difference in pregnancy rate when compared to IVF in couples with mild male subfertility.
(Wang, 2024) |
|
Difference: 21 fewer per 1000 (CI 95% 59 fewer - 17 more) |
|||||
|
Live birth rate (critical) |
Relative risk: 0.92 (CI 95% 0.83 - 1.03) Based on data from 2329 participants in 1 study
|
366 per 1000 |
337 per 1000 |
Low Due to serious imprecision5 |
ART with ICSI may slightly reduce live birth rate when compared to IVF in couples with mild male subfertility.
(Wang, 2024) |
|
Difference: 29 fewer per 1000 (CI 95% 62 fewer - 11 more) |
|||||
|
Multiple pregnancy (important) |
Relative risk: 0.85 (CI 95% 0.66 - 1.08) Based on data from 2329 participants in 1 study
|
106 per 1000 |
90 per 1000 |
Low Due to serious imprecision6 |
ART with ICSI may result in little to no difference in multiple pregnancies when compared to IVF in couples with mild male subfertility. (Wang, 2024) |
|
Difference: 16 fewer per 1000 (CI 95% 36 fewer - 8 more) |
|||||
|
OHSS (important) |
Relative risk: 0.9 (CI 95% 0.45 - 1.79) Based on data from 2329 participants in 1 study
|
14 per 1000 |
13 per 1000 |
Very low Due to very serious imprecision7 |
The evidence is very uncertain about the effect of ICSI on OHSS when compared to IVF in couples with mild male subfertility. (Wang, 2024) |
|
Difference: 1 fewer per 1000 (CI 95% 8 fewer - 11 more) |
|||||
|
Total fertilization failure (important) |
Relative risk: 0.76 (CI 95% 0.52 - 1.13) Based on data from 2329 participants in 1 study
|
48 per 1000 |
36 per 1000 |
Very low Due to very serious imprecision8 |
The evidence is very uncertain about the effect of ICSI on total fertilization failure when compared to IVF in couples with mild male subfertility.
(Wang, 2024) |
|
Difference: 12 fewer per 1000 (CI 95% 23 fewer - 6 more) |
|||||
|
Miscarriage rate (important) |
- |
- |
No GRADE |
No evidence was found regarding the effect of ICSI compared to IVF on miscarriage rate in couples with mild male subfertility. |
4. Imprecision: serious. Lower limit of 95% confidence interval crosses the border for clinical relevance;
5. Imprecision: serious. Lower limit of 95% confidence interval crosses the border for clinical relevance
6. Imprecision: serious. Low number of patients, Low number of events;
7. Imprecision: very serious. Wide 95% confidence intervals, Low number of events;
8. Imprecision: very serious. Wide 95% confidence intervals, Low number of events.
Description of studies
Two studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
The selected Cochrane review (Cissen, 2016) assessed the effectiveness and safety of different fertility treatments for couples whose subfertility appears to be due to abnormal sperm parameters. The systematic review (SR) included ten RCTs covering data from 757 participants. Inclusion criteria of the review were couples with male subfertility who had been trying to conceive for at least one year. Thirteen comparisons were assessed in the review. However, for the current PICO only two comparisons, IVF vs IUI in natural cycles and IVF vs IUI in stimulated cycles, were considered relevant. These comparisons were reported in two RCTs (Bensdorp, 2015; Goverde, 2000) covering data of 86 participants. Outcome measures were live birth rate, clinical pregnancy rate, miscarriage rate, incidence of OHSS and total fertilization failure rates. All interventions that couples received within 12 months after randomization were included (Bensdorp, 2015) or outcomes were reported after follow-up of a maximum of six treatment cycles of IUI or IVF, couples with a viable pregnancy at 12 weeks of gestation were excluded from further treatment within the study, irrespective of the outcome of pregnancy (Goverde, 2000). The SR included RCTs or cross-over trials (then only the first-phase data were included) from inception until April 2015.
Wang (2024) performed an RCT in ten medical centers to compare the efficacy and safety of ICSI versus IVF in couples with infertility with non-severe male factor. Non-severe male factor was defined as oligoasthenozoospermia (sperm concentration 5–15 × 10⁶ sperm per mL and progressive motility 10–32%), oligozoospermia (sperm concentration 5–15 × 10⁶ sperm per mL and progressive motility ≥32%), or asthenozoospermia (sperm concentration ≥15 × 10⁶ sperm per mL and progressive motility 10–32%), according to the fifth edition of WHO’s laboratory manual for the examination and processing of human semen.
Couples were eligible if they were scheduled for their first or second IVF or ICSI cycle following a gonadotropin-releasing hormone (GnRH) agonist or antagonist protocol as controlled ovarian hyperstimulation treatment, and if the male partner showed non-severe male factor during initial evaluation. Exclusion criteria were treatment with donor sperm or eggs, preimplantation genetic testing, treatment with frozen-thawed semen or poor fertilization in a previous IVF cycle (<25%). In addition, couples in whom no oocytes were retrieved and couples with a total progressive motile sperm count for insemination of less than 0.1x106 sperm/mL on the day of oocyte retrieval were excluded. Cumulative fertility and pregnancy outcomes were reported with a follow-up of 12 months after randomisation.
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
PICO 1 – ICSI or IVF versus IUI Included in systematic review, Cissen 2016 |
||||||
|
Bensdorp, 2015 |
*N at baseline Intervention: 18 Control: 18
^Age of female partner (mean, SD) Intervention: 33 ± 3.4 Control: 34 ± 3.7
^Data on couples with male subfertility not reported. Data shown are from the full sample. |
Intervention: IVF Control: IUI + ovarian hyperstimulation |
12 months |
Live birth rate, ongoing pregnancy, OHSS |
*Data on couples with male subfertility were not reported by Bensdorp (2015). The author supplied this data for use by Cissen (2016). |
Low risk (all outcomes) |
|
Goverde, 2000 |
*N at baseline Intervention 1: 27 Intervention 2: 24 Control: 26
^Age of female partner (mean, SD) Intervention 1: 31.6 ± 3.7 Intervention 2: 31.7 ± 3.9 Control: 32.0 ± 4.2
^Data on couples with male subfertility not reported. Data shown are from the full sample. |
Intervention 1: IUI alone Intervention 2: IUI plus stimulation Control: IVF
|
Not reported |
Live birth rate, OHSS |
*77 couples with male subfertility were included in the trial and 179 with unexplained subfertility. Data from the couples with male subfertility are reported in the current summary. |
Low risk (all outcomes) |
|
PICO 2 – ICSI versus IVF Individual study (RCT) |
||||||
|
Wang, 2024 |
N at baseline Intervention: 1154 Control: 1175
Age of female partner (median, IQR) Intervention: 34 (31-37) Control: 33 (30-37)
|
Intervention: ICSI Control: conventional IVF |
Primary and secondary outcomes observed for the first embryo transfer within 6 months of oocyte retrieval. Collection of maternal and neonatal information completed within 6 weeks of delivery. |
Live birth rate, ongoing pregnancy, multiple pregnancy, OHSS, total fertilization failure
|
|
Low risk (all outcomes) |
*For further details, see risk of bias table in the appendix
Results
PICO 1 – ICSI or IVF versus IUI
One Cochrane review (Cissen, 2016) was included for PICO 1.
1. Live birth rate (critical outcome)
One study included in Cissen (2016) reported live birth rate for the comparison IVF versus IUI in natural cycles. Subfertility was diagnosed if three out of five semenanalysis showed fewer than 20 million progressively motile spermatozoa in the ejaculate and a minimum of 1 million progressively motile spermatozoa at least once (Goverde, 2000). The study included 53 couples, and live birth was reported in 9/26 (34.6%) and 11/27 (40.7%) in the IVF and IUI group respectively (RR 0.85, 95%CI 0.42 to 1.71). This difference is considered clinically relevant, in favor of IUI. However, the confidence interval is wide and crosses the borders for clinical relevance on both sides.
Two studies reported live birth rate for the comparison IVF versus IUI in cycles with ovarian hyperstimulation (Bensdorp, 2015; Goverde, 2000). In total 86 couples were included. Live birth was reported in 20/44 (45.5%) and 19/42 (42.2%) in the IVF and IUI group respectively (RR 1.03, 95%CI 0.66 to 1.61). This difference is not considered clinically relevant (Figure 1).
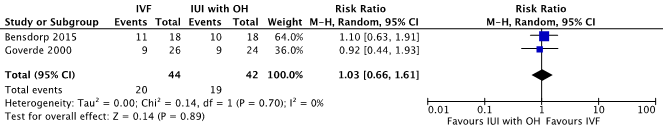
Figure 1. Forest plot for the outcome live birth rate per couple, comparison in vitro fertilization (IVF) versus intrauterine insemination (IUI) in cycles with ovarian hyperstimulation (OH)
2. Pregnancy rate (critical outcome)
One study reported pregnancy rate per couple for the comparison IVF versus IUI in cycles with ovarian hyperstimulation (Bensdorp, 2015). Pregnancy was reported in 12/18 (66.7%) women in the IVF group and 11/18 (61.1%) women in the IUI + OH group (RR 1.09, 95%CI 0.67 to 1.79). This difference is not considered clinically relevant.
3. Miscarriage rate (important outcome)
Bensdorp (2015) reported two miscarriages, one in the IUI with OH group, and one in the IVF with single embryo transfer group.
4. Multiple pregnancy (important outcome)
Bensdorp (2015) reported two twins, one in the IUI with OH group, and one in the IVF with single transfer group.
Goverde (2000) reported a multiple pregnancy rate of 29% of the viable pregnancies in the group assigned lUI with OH (nine pairs of twins) and 21 % in the IVF group (one group of triplets, six pair of twins).
5. OHSS (important outcome)
The outcome OHSS was reported by Goverde (2000) and Bensdorp (2015).
For the comparison IVF versus IUI in natural cycles (Goverde, 2000) three cases of severe ovarian hyperstimulation occurred in the IVF group. However, it is unclear how many of these cases occurred in couples with mild male subfertility and how many of the cases in the unexplained subfertility group.
For the comparison IVF versus IUI in cycles with ovarian hyperstimulation no cases of OHSS were reported (Bensdorp, 2015).
PICO 2 – ICSI versus IVF
One RCT (Wang, 2024) was included for PICO 2, comparison ICSI versus conventional IVF.
1. Live birth rate (critical outcome)
Wang (2024) reported live birth after first embryo transfer in 390/1154 (33.8%) couples in the ICSI group compared to 430/1175 (36.6%) couples in the IVF group (RR 0.92, 95% CI 0.83 to 1.03). This is considered clinically relevant in favor of conventional IVF. However, the confidence interval crosses the lower border for clinical relevance.
2. Pregnancy rate (critical outcome)
Clinical pregnancy was reported in 463/1154 (40.1%) couples in the ICSI group compared to 498/1175 (42.4%) couples in the IVF group (RR 0.95, 95% CI 0.86 to 1.04). This difference is not considered clinically relevant.
3. Miscarriage rate (important outcome)
There was no data available for this outcome measure.
4. Multiple pregnancy (important outcome)
Multiple pregnancy was reported in 103/1154 (8.9%) couples in the ICSI group compared to 124/1175 (10.6%) in the IVF group (RR 0.85, 95% CI 0.66 to 1.08). This difference is not considered clinically relevant.
5. OHSS (important outcome)
Moderate or severe OHSS was reported in 15/1154 (1.3%) couples in the ICSI group compared to 17/1175 (1.4%) in the IVF group (RR 0.90, 95% CI 0.45 to 1.79). This difference is not considered clinically relevant.
6. Total fertilization failure (important outcome)
Total fertilization failure was reported in 42/1154 (3.6%) couples in the ICSI group compared to 56/1175 (4.8%) in the IVF group (RR 0.77, 95% CI 0.52 to 1.14). This difference is considered clinically relevant in favor of ICSI. However, the confidence interval is wide and crosses the lower border for clinical relevance.
A systematic review of the literature was performed to answer the following question:
What is the effect of different assisted reproductive technologies compared to each other on the chance of pregnancy in couples with male subfertility?
Table 1. PICO's
PICO 1
| Patients | Couples with diagnosis male subfertility |
| Intervention | ICSI or IVF |
| Control | IUI |
| Outcomes | Live birth rate, pregnancy rate, miscarriage rate, multiple pregnancy, OHSS, total fertilization failure |
PICO 2
| Patients | Couples with diagnosis male subfertility |
| Intervention | ICSI |
| Control | IVF |
| Outcomes | Live birth rate, pregnancy rate, miscarriage rate, multiple pregnancy, OHSS, total fertilization failure |
| Other selection criteria |
Study design: systematic reviews, randomized controlled trials and observational studies. From 2000 onwards |
Relevant outcome measures
The guideline panel considered live birth rate and pregnancy rate as critical outcome measures for decision making; and miscarriage rate, multiple pregnancy, OHSS, total fertilization failure as important outcome measures for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
The guideline panel defined a 5% difference (RR <0.95 or >1.05) for live birth rate and pregnancy rate as minimal clinically (patient) important difference. For other outcomes, the default boundaries as defined by GRADE were used: a 25% difference for dichotomous outcomes (RR< 0.8 or >1.25) and 0.5 SD for continuous outcomes as minimal clinically (patient) important difference.
Search and select (Methods)
A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2000 to April 3, 2024, for systematic reviews (SRs), randomized controlled trials (RCTs) and observational studies. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 10782 hits. Due to the large number of studies, initially only SRs (1114) were screened based on the PICO criteria. The Cochrane SR by Cissen (2016) was selected as a key article. Then RCTs from 2015 onward were screened based on the PICO criteria. Initially, nine studies were selected based on title and abstract screening. After reading the full text, eight studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and one study, in addition to the SR was included.
- Ayad BM, Horst GV, Plessis SSD. Revisiting The Relationship between The Ejaculatory Abstinence Period and Semen Characteristics. Int J Fertil Steril. 2018 Jan;11(4):238-246. doi: 10.22074/ijfs.2018.5192. Epub 2017 Oct 12. PMID: 29043697; PMCID: PMC5641453.
- Bensdorp AJ, Tjon-Kon-Fat RI, Bossuyt PM, Koks CA, Oosterhuis GJ, Hoek A, Hompes PG, Broekmans FJ, Verhoeve HR, de Bruin JP, van Golde R, Repping S, Cohlen BJ, Lambers MD, van Bommel PF, Slappendel E, Perquin D, Smeenk JM, Pelinck MJ, Gianotten J, Hoozemans DA, Maas JW, Eijkemans MJ, van der Veen F, Mol BW, van Wely M. Prevention of multiple pregnancies in couples with unexplained or mild male subfertility: randomised controlled trial of in vitro fertilisation with single embryo transfer or in vitro fertilisation in modified natural cycle compared with intrauterine insemination with controlled ovarian hyperstimulation. BMJ. 2015 Jan 9;350:g7771. doi: 10.1136/bmj.g7771. PMID: 25576320; PMCID: PMC4288434.
- Cissen M, Bensdorp A, Cohlen BJ, Repping S, de Bruin JP, van Wely M. Assisted reproductive technologies for male subfertility. Cochrane Database Syst Rev. 2016 Feb 26;2(2):CD000360. doi: 10.1002/14651858.CD000360.pub5. PMID: 26915339; PMCID: PMC10335364.
- Cissen M, Wely MV, Scholten I, Mansell S, Bruin JP, Mol BW, Braat D, Repping S, Hamer G. Measuring Sperm DNA Fragmentation and Clinical Outcomes of Medically Assisted Reproduction: A Systematic Review and Meta-Analysis. PLoS One. 2016 Nov 10;11(11):e0165125. doi: 10.1371/journal.pone.0165125. PMID: 27832085; PMCID: PMC5104467.
- Custers IM, Steures P, Hompes P, Flierman P, van Kasteren Y, van Dop PA, van der Veen F, Mol BW. Intrauterine insemination: how many cycles should we perform? Hum Reprod. 2008 Apr;23(4):885-8. doi: 10.1093/humrep/den008. Epub 2008 Feb 8. PMID: 18263638.
- Goverde AJ, McDonnell J, Vermeiden JP, Schats R, Rutten FF, Schoemaker J. Intrauterine insemination or in-vitro fertilisation in idiopathic subfertility and male subfertility: a randomised trial and cost-effectiveness analysis. Lancet. 2000 Jan 1;355(9197):13-8. doi: 10.1016/S0140-6736(99)04002-7. PMID: 10615885.
- Muthigi A, Jahandideh S, Bishop LA, Naeemi FK, Shipley SK, O'Brien JE, Shin PR, Devine K, Tanrikut C. Clarifying the relationship between total motile sperm counts and intrauterine insemination pregnancy rates. Fertil Steril. 2021 Jun;115(6):1454-1460. doi: 10.1016/j.fertnstert.2021.01.014. Epub 2021 Feb 18. PMID: 33610321.
- Wang Y, Li R, Yang R, Zheng D, Zeng L, Lian Y, Zhu Y, Zhao J, Liang X, Li W, Liu J, Tang L, Cao Y, Hao G, Wang H, Zhang H, Wang R, Mol BW, Huang H, Qiao J. Intracytoplasmic sperm injection versus conventional in-vitro fertilisation for couples with infertility with non-severe male factor: a multicentre, open-label, randomised controlled trial. Lancet. 2024 Mar 9;403(10430):924-934. doi: 10.1016/S0140-6736(23)02416-9. Epub 2024 Feb 5. PMID: 38330980.
- Ombelet W, Dhont N, Thijssen A, Bosmans E, Kruger T. Semen quality and prediction of IUI success in male subfertility: a systematic review. Reprod Biomed Online. 2014 Mar;28(3):300-9. doi: 10.1016/j.rbmo.2013.10.023. Epub 2013 Nov 15. PMID: 24456701.
- Rhemrev JP, Lens JW, McDonnell J, Schoemaker J, Vermeiden JP. The postwash total progressively motile sperm cell count is a reliable predictor of total fertilization failure during in vitro fertilization treatment. Fertil Steril. 2001 Nov;76(5):884-91. doi: 10.1016/s0015-0282(01)02826-6. PMID: 11704106.
- Scarselli F, Cursio E, Muzzì S, Casciani V, Ruberti A, Gatti S, Greco P, Varricchio MT, Minasi MG, Greco E. How 1 h of abstinence improves sperm quality and increases embryo euploidy rate after PGT-A: a study on 106 sibling biopsied blastocysts. J Assist Reprod Genet. 2019 Aug;36(8):1591-1597. doi: 10.1007/s10815-019-01533-7. Epub 2019 Jul 19. PMID: 31325068; PMCID: PMC6708030.
- WHO laboratory manual for the examination and processing of human semen, sixth edition. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
Risk of Bias tables
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Wang, 2024 |
Definitely yes;
Reason: Randomization was done immediately after oocyte retrieval through an online trial system with a computer-generated randomisation list, by use of permuted blocks of varying size (4 or 6) stratified by centre. |
Probably yes;
Reason: a web-based allocation system was used. It is unclear how the randomization procedure was overseen. |
Definitely no;
Reason: participants, clinicians, investigators assessing outcomes, and investigators analyzing the data were not masked to intervention allocation. |
Probably yes;
Reason: Loss to follow-up was infrequent in intervention and control group. |
Probably yes;
Reason: All relevant outcomes were reported |
Probably yes;
Reason: No other problems noted |
LOW |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Bensdorp AJ, Tjon-Kon-Fat RI, Bossuyt PM, Koks CA, Oosterhuis GJ, Hoek A, Hompes PG, Broekmans FJ, Verhoeve HR, de Bruin JP, van Golde R, Repping S, Cohlen BJ, Lambers MD, van Bommel PF, Slappendel E, Perquin D, Smeenk JM, Pelinck MJ, Gianotten J, Hoozemans DA, Maas JW, Eijkemans MJ, van der Veen F, Mol BW, van Wely M. Prevention of multiple pregnancies in couples with unexplained or mild male subfertility: randomised controlled trial of in vitro fertilisation with single embryo transfer or in vitro fertilisation in modified natural cycle compared with intrauterine insemination with controlled ovarian hyperstimulation. BMJ. 2015 Jan 9;350:g7771. doi: 10.1136/bmj.g7771. PMID: 25576320; PMCID: PMC4288434. |
Included in SR Cissen (2016) |
|
Shuai HL, Ye Q, Huang YH, Xie BG. Comparison of conventional in vitro fertilisation and intracytoplasmic sperm injection outcomes in patients with moderate oligoasthenozoospermia. Andrologia. 2015 Jun;47(5):499-504. doi: 10.1111/and.12291. Epub 2014 May 9. PMID: 24811903. |
Doubts about study quality |
|
Tournaye H, Verheyen G, Albano C, Camus M, Van Landuyt L, Devroey P, Van Steirteghem A. Intracytoplasmic sperm injection versus in vitro fertilization: a randomized controlled trial and a meta-analysis of the literature. Fertil Steril. 2002 Nov;78(5):1030-7. doi: 10.1016/s0015-0282(02)03377-0. PMID: 12413989. |
Wrong method, randomized occytes instead of patients |
|
Xie BG, Huang YH, Zhu WJ, Jin S. Comparison of the outcome of conventional in vitro fertilization and intracytoplasmic sperm injection in moderate male infertility from ejaculate. Urol Int. 2015;94(1):111-6. doi: 10.1159/000353975. Epub 2013 Nov 13. PMID: 24246711. |
Seems a duplicate of Shuai (2015), which was excluded based on doubts about study quality |
|
Xu J, Yu Y, Xue M, Lv X. Intracytoplasmic Sperm Injection Improves Normal Fertilization Rate and Clinical Pregnancy Rate in Male Infertility. Contrast Media Mol Imaging. 2022 Jul 31;2022:1522636. doi: 10.1155/2022/1522636. PMID: 35965625; PMCID: PMC9357718. |
Doubts about study quality |
|
Younes G, Tannus S, Son WY, Dahan MH. When to do intracytoplasmic sperm injection: a prospective comparison. Arch Gynecol Obstet. 2019 Nov;300(5):1461-1471. doi: 10.1007/s00404-019-05324-4. Epub 2019 Oct 20. PMID: 31631246. |
Wrong P |
Beoordelingsdatum en geldigheid
Publicatiedatum : 30-04-2026
Beoordeeld op geldigheid : 30-04-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met mannelijke subfertiliteit.
Werkgroep
- Cantineau A.E.P. (Astrid), gynaecoloog, subspecialist voortplantingsgeneeskunde Universitair Medisch Centrum Groningen te Groningen, NVOG
- Dinkelman-Smit M. (Marij), uroloog-androloog, Erasmus Medisch Centrum te Rotterdam, NVU
- Verberg M.F.G. (Marieke), gynaecoloog, Medisch Spectrum Twente te Enschede, NVOG
- Heida K.Y. (Karst), gynaecoloog, Dijklander ziekenhuisbte Purmerend, NVOG
- van der Houwen L.E.E. (Lisette), gynaecoloog, Radboud universitair medisch centrum te Nijmegen, NVOG
- de Bruin J.P. (Jan Peter), gynaecoloog, Jeroen Bosch Ziekenhuis te ’s Hertogenbosch, NVOG
- van Breda H.M.K. (Jetske), uroloog-androloog, Universitair Medisch Centrum Utrecht te Utrecht, NVU
- van Roijen J.H. (Herman), uroloog-androloog, voorheen ETZ Tilburg – nu gepensioneerd
- D’Hauwers K.W.M. (Kathleen), uroloog-androloog, Radboud universitair medisch centrum te Nijmegen, NVU
- Meißner A. (Andreas), uroloog-androloog, Amsterdam Universitair Medisch Centrum te Amsterdam, NVU
- Bailleux B.B.E.P. (Bart), laboratoriumspecialist Klinische Chemie en Endocrinologie, Leids Universitair Medisch Centrum te Leiden, NVKC
- Kempers M.J.E. (Marlies), klinisch geneticus, Radboud universitair medisch centrum te Nijmegen, VKGN
- van der Kevie-Kersemaekers A.M.F. (Anne-Marie), laboratoriumspecialist klinische genetica, Universitair Medisch Centrum Utrecht te Utrecht, VKGL
- Westra D. (Dineke), laboratoriumspecialist klinische genetica, Radboud universitair medisch centrum te Nijmegen, VKGL
- Ramos L. (Liliana), klinisch embryoloog, Radboud universitair medisch centrum te Nijmegen, KLEM
- Grolle R.L. (Rosanne), fertiliteitsarts, Erasmus Medisch Centrum te Rotterdam, VVF
- Sinjorgo S. (Simone), medewerker medewerker patientenperspectief wetenschappelijk onderzoek en richtlijnen, Freya (vanaf december 2024)
- Vermeulen M. (Marloes), medewerker patientenperspectief wetenschappelijk onderzoek en richtlijnen, Freya (tot december 2024)
Met ondersteuning van
- Mostovaya I.M. (Irina), senior-adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- van der Lee J.H. (Hanneke), senior-adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Middelhuis D. (Danique), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Van Bommel M. (Majke), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Schultink J.M. (Janneke), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- E. (Esther) van der Bijl, informatiespecialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel Gemelde (neven)functies en belangen werkgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaam-heden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Datum |
Restrictie |
|
Astrid Cantineau (voorzitter) |
Gynaecoloog. UMCG, 1.0 FTE |
auteur Up to date Hyperthecosis |
Geen |
Geen |
Geen |
Voorzitter SIG andrologie NVOG aanvrager subsidie ZonMw over leefstijl en mannelijke subfertiliteit |
Geen |
13/11/2022 |
Geen restricties. |
|
Marij Dinkelman-Smit (vice voorzitter) |
Staflid Uroloog-Androloog Voorzitter Voortplantingscentrum Erasmus MC Plaatsvervangend afdelingshoofd Urologie Erasmus MC Erasmus MC Universitair Medisch Centrum |
Bestuurslid Nederlandse Vereniging voor Urologie (NVU) (onbetaald) Bestuurslid multidisciplenaire Special Interest Group (SIG) Andrologie, Nederlandse Verening voor Obstetrie en Gynaecologie (NVOG) (onbetaald) Bestuurslid European Association of Urology (EAU) section for Andrological Urology (ESAU) (onbetaald) Medical director European Academy of Andrology (EAA) training center Andrology Erasmus MC (onbetaald) Lid Commissie Kwaliteitvisitatie NVU (onbetaald) Medische adviesraad Klinefelter Vereniging (onbetaald) Medische adviesraad Stichting Lichen Sclerosus (onbetaald) |
Geen |
Geen |
Geen |
Geen |
Geen |
12/12/2022 |
Geen restricties. |
|
Marieke Verberg |
Gynaecoloog, Medisch Spectrum Twente 0.5 FTE betaalde functie Gynaecoloog en statutair directeur Fertiliteitskliniek Twente 0.5 FTE betaalde functie |
Geen relevante |
Geen |
Geen |
Geen |
Geen |
Geen |
19/11/2022 |
Geen restricties. |
|
Karst Heida |
Gynaecoloog bij het Dijklander ziekenhuis - betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
7/12/2022 |
Geen restricties. |
|
Lisette van der Houwen |
Gynaecoloog - fellow voortplantingsgeneeskunde Radboudumc |
Bestuurslid SIG endometriose NVOG algemeen lid SIG ART en SIG fertiliteitspreservatie van de NVOG |
Geen |
Geen |
Merck / Impect study - improving patient-centeredness in endometriosis care. / Ja |
Geen |
Geen |
02/12/2022 |
Geen restricties, extern gefinancierd onderzoek heeft geen betrekking op richtlijn onderwerp. |
|
Jan Peter de Bruin |
Gynaecoloog Jeroen Bosch Ziekenhuis, betaald |
Waarnemend gynaecoloog Radboudumc, betaald |
Medical Advisory Board Ferring BV - De medical advisory board komt op verzoek van Ferring ongeveer eens per jaar samen. Daarbij worden ontwikkelingen in het veld en relevant studie uitkomsten bediscussieerd. Ferring gebruikt de uitkomsten van deze besprekingen als input voor hun strategie. |
- |
Ja - Het gaat om eigen onderzoek op gebied voortplantingsgeneeksunde waarvoor mijn afdeling een unrestricted research grant kreeg. Dit onderzoek bestaat uit de volgende lijnen: • het ontwikkelen en evalueren van toepassingen voor online fertilteitszorg (geen raakvlak met uit te werken modules voor deze richtlijn). • het effect van gebruik van supplementen op de zwangerschapskans bij paren met mannelijke subfertiliteit (raakvlak met module over supplementen waar de Bruin bij betrokken is als locale hoofdonderzoeker, tweede auteur van de nog te publiceren paper) Gefinincierd door Goodlife pharma |
- |
- |
26/11/2022 |
Vanwege deelname aan een adviesraad aan de start van het traject is de richtlijn tijdens de commentaarfase ook aan de Commissie Kwaliteitsdocumenten van de NVOG voorgelegd. Verder is dit lid uitgesloten van besluitvorming bij onderwerpen die raken aan de adviesraad. |
|
Jetske van Breda |
Uroloog/ Androloog UMCUtrecht |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
18/11/2022 |
Geen restricties. |
|
Kathleen D' Hauwers |
Uroloog, staflid Radboudumc: betaald |
Lid Cie Kwaliteit NVU: onbetaald Lid Cie Andrologie NVU: onbetaald Board memeber Klinefelter Vereniging Nederland: onbeteaald Cie Keuzehulp ED: vergoed |
Geen |
Geen |
Geen |
Inbrengen van expertise. Geen specifieke, persoonlijke baat bij één of ander: het gaat om de patiënt / klant. |
Geen |
28/09/2022 |
Geen restricties. |
|
Andreas Meißner |
Uroloog - Androloog Staflid Centrum voor Voortplantingsgeneeskunde, locatie AMC, en afdeling Urologie, locatie VUMC, van het Amsterdam UMC betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
24/11/2022 |
Geen restricties. |
|
Herman van Roijen |
Uroloog ETZ Tilburg |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
13/11/2022 |
Geen restricties. |
|
Bart Ballieux |
Laboratoriumspecialist Klinische Chemie en Endocrinologie Afdeling KCL, LUMC, Leiden |
Geen |
geen persoonlijke financiele belangen |
Geen relevante persoonlijke relaties die van invloed kunnen zijn op mijn adviezen |
geen |
Geen intellectuele belangen bij mijn adviezen |
Geen overige belangen |
10/01/2023 |
Geen restricties. |
|
Marlies Kempers |
Klinisch Geneticus (Radboudumc) |
Voorzitter subcommissie Richtlijnen, onderdeel van Kwaliteitscommissie VKGN |
Geen |
Geen |
Aytu Pharma / Prevent studie (effect Enzastaurin bij vasculair EDS) Studie is nog niet gestart, financiering on hold / Tijdelijk, ter vervanging verlof projectleider |
Geen |
Geen |
10/11/2022 |
Geen restricties. De studie waar mw. Kempers bij betrokken was is nooit gestart. Inhoudelijk had deze studie niet met mannelijke infertiliteit te maken. |
|
Anne-Marie van der Kevie - Kersemaekers |
laboratoriumspecialist klinische genetica UMC Utrecht |
Vakdeskundige Raad van Accreditatie |
Geen |
Geen |
Geen |
Geen |
Geen |
28/03/2023 |
Geen restricties. |
|
Manon Oud |
Laboratoriumspecialist Klinische Genetica in opleiding, Radboudumc Betaalde functie (hoofdberoep) |
Geen |
Geen |
Geen |
Deelname aan onderzoeksproject als PhD student De novo mutations in male infertility (NWO VICI van prof. Joris Veltman) van 2015-2020 Travel Grant van de Catherine van Tussenbroek Foundation voor bezoek van 3 maanden aan Monash University (2019) |
Geen |
Geen |
8/11/2022 |
Geen restricties, niet actief geweest in de werkgroep. |
|
Dineke Westra |
Laboratoriumspecialist Klinische Genetica (1.0 FTE, betaald) Afd. Genetica, sectie Genoomdiagnostiek Radboudumc, Nijmegen Werkzaamheden: Genetische diagnostiek |
Technical Assessor ISO15189 Raad van Accreditatie betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
16/02/2023 |
Geen restricties. |
|
Liliana Ramos |
Klinisch embryoloog Radboudumc |
Geen |
Geen |
Geen |
Geen |
Boegbeeldfunctie bij patiënten en beroepsorganisatie |
Geen |
10/08/2023 |
Geen restricties. |
|
Rosanne Grolle |
Fertiliteitsarts, Erasmus MC. Het begeleiden en behandelen van paren met een kinderwens. Functie is betaald. |
Lid van de symposiumcommissie van de VVF Onder andere het opstellen van het wetenschappelijk programma, het vragen van sprekers, het regelen van een symposiumlocatie en buffet, het versturen van de uitnodigingen en het aanvragen van accreditatie en sponsoring. Functie is onbetaald. |
Geen |
Geen |
Geen |
Geen |
Geen |
3/11/2022 |
Geen restricties. |
|
Marloes Vermeulen |
Freya, medewerker externe relaties |
Verloskundige 1e lijn. |
Geen |
Geen |
Geen |
Geen |
Geen |
27/09/2022 |
Geen restricties. |
|
José Knijnenburg |
Directeur bij Freya, vereniging voor mensen met vruchtbaarheidsproblemen - 32u p/wk Medewerker communicatie en marketing bij van der Pol-consulting b.v. - 8u p/wk |
Geen |
Dienstverband bij de (onafhankelijke) landelijke patiëntenvereniging voor mensen met vruchtbaarheidsproblemen. |
Geen |
ZonMW / Alife2 en T4Life / nee ZonMW / Antarctica2 / nee ZonMW / Cosy - Zin en zwanger / nee ZonMW / FOAM / nee ZonMW / Scratch-OFO / nee ZonMW / TOF (3 or 5) / nee ZonMW / H2Olie / nee ZonMW / H2OlieFlush / nee ZonMW / MYPP - myo-inositol bij PCOS / nee ZonMW / PSIDER Embryonic checkpoints - releasing the brakes on IVF /nee RadboudUMC/Goodlife / Summer - voedingssupplement man / nee ZonMW / Divine - dosiscalculator / nee Amsterdam UMC / ANDES / nee ZonMW / PSIDER - Hip gametes / nee ZonMW / COPIE - - endometriose en IVF / nee |
Belangenbehartiger bij patiëntenorganisatie |
Radboud/MUMC / Hmove sporten en afweersysteem bij miskramen / nee ZonMW / Medium2 kweekvloeistof IVF / nee ZonMW / Selectimo timelapse / nee MUMC+ / Murlm hhmk en ril / nee ZonMw / LUMO luteal phase support / nee ZonMw / PSIDER SteMBlast / nee ZonMw / SEGa veiligheid vp-technieken / nee ZonMw / Covid-19 Impact endometriose/fertiliteitspatiënten / nee ZonMw / PREMI / nee ZonMw / HyFosy-HSG stugie / nee ZonMw / REMI III / nee |
20/07/2023 |
Geen restricties, mevrouw was tijdelijke inval tijdens zwangerschapsverlof. In rol van patientvertegenwoordiger betrokken bij onderzoek. |
|
Simone Sinjorgo |
Parttime medewerker patientenperspectief en -participatie bij Freya (vereniging voor mensen met vruchtbaarheidsproblemen) - betaald 14 uur https://www.freya.nl/over-freya/wie-we-zijn/de-werknemers. Ter info: door mijn functie bij Freya ben ik betrokken bij diverse richtlijnontwikkeling en/of onderzoeken op het gebied van fertiliteit. In de vorm van toelichten, belichten en/of vertegenwoordigen van alleen het patiëntenperspectief tav het bepaalde onderwerp, zoals bij deze 3 richtlijnen OFO, OHSS en mannelijke subfertiliteit. |
Lichaamsgericht psychosociaal therapeut - zzp eigen praktijk in Dongen-Vaart - geregistreerd therapeut RBCZ incl. AGB-codes. www.praktijkdediamant.nl
- Psychosociaal docent Bijscholing Instituut voor therapeuten - betaling via praktijk https://bivt.nl/?s=lichaamsgericht+coachen
- Psychosociaal docent vrouwencoach opleiding - betaling via praktijk https://www.devrouwencoach.nl/vrouwencoach-opleiding/ |
Geen |
Geen |
Geen |
Geen |
Geen |
03/12/2024 |
Geen restricties. |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door uitnodigen van Freya en de Patientenfederatie Nederland voor de invitational conference. Daarnaast zat namens Freya een afgevaardigde in de werkgroep. Het verslag van de invitational conference is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen (zie kop waarden en voorkeuren van patiënten). De conceptrichtlijn is tevens voor commentaar voorgelegd aan Freya en de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
ART
|
Geen financiele gevolgen. |
Uit de toetsing volgt dat de aanbevelingen niet breed toepasbaar zijn (<5.000 patiënten) en daarom naar verwachting geen substantiële financiële gevolgen zullen hebben voor de collectieve uitgaven. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Mannelijke subfertiliteit – UV14 ART |
|
|
Uitgangsvraag/modules: Welke ART is geïndiceerd? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 3 april 2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
Rayyan review: https://rayyan.ai/reviews/985655 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen mannelijke subfertiliteit EN assisted reproduction techniques.
→ De sleutelartikelen worden gevonden met deze search:
Vanwege de grote opbrengst worden in eerste instantie alleen de SR’s aangeboden in Rayyan. |
|
|
Te gebruiken voor richtlijntekst: In de databases Embase.com en Ovid/Medline is op 3 april 2024 systematisch gezocht naar systematische reviews, RCTs en observationele studies over het effect van ART bij paren met de diagnose mannelijke subfertiliteit. De literatuurzoekactie leverde 1114 unieke treffers op. |
|
Zoekopbrengst - 3 april 2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
932 |
727 |
1114* |
|
RCT |
1755 |
1261 |
2424 |
|
Observationeel |
6063 |
4233 |
7244 |
|
Totaal |
8750 |
6221 |
10782 |
*in Rayyan
Zoekstrategie - 3 april 2024
Embase.com
|
No. |
Query |
Results |
|
#1 |
'male infertility'/exp OR 'male fertility'/exp OR (('subfertility'/de OR 'childlessness'/exp) AND 'male'/exp) OR (((male* OR men OR man) NEAR/3 (infertil* OR hypofertil* OR 'fertil*' OR subfertil* OR infecund* OR childless* OR reproduct*)):ti,ab,kw) OR (((spermatogen* OR spermiation OR spermiogen*) NEAR/3 failure):ti,ab,kw) OR ((spermatozoon NEAR/3 (abnormalit* OR anomal*)):ti,ab,kw) OR (((semen OR sperm) NEAR/3 (qualit* OR quantit* OR parameter* OR dna)):ti,ab,kw) OR asperm*:ti,ab,kw OR asthenazoosperm*:ti,ab,kw OR asthenosperm*:ti,ab,kw OR asthenozoosperm*:ti,ab,kw OR azoosperm*:ti,ab,kw OR cryptosperm*:ti,ab,kw OR cryptozoosperm*:ti,ab,kw OR hyposperm*:ti,ab,kw OR oligoasthenosperm*:ti,ab,kw OR oligosperm*:ti,ab,kw OR oligozoosperm*:ti,ab,kw OR 'retrograde ejaculat*':ti,ab,kw OR 'sco syndrome*':ti,ab,kw OR 'sertoli cell only syndrome*':ti,ab,kw OR teratozoosperm*:ti,ab,kw OR 'thermosensitive genic male steril*':ti,ab,kw OR globozoosperm*:ti,ab,kw OR macrozoosperm*:ti,ab,kw |
114384 |
|
#2 |
'infertility therapy'/exp OR 'intracytoplasmic sperm injection'/exp OR 'in vitro fertilization'/exp OR 'artificial insemination'/exp OR (((fertil* OR reproduct*) NEAR/3 (technique* OR technolog* OR therap* OR treatment* OR assist* OR extracorporeal OR 'in vitro')):ti,ab,kw) OR ((('intracytoplasm*' OR 'intra cytoplasm*') NEAR/3 'sperm* inject*'):ti,ab,kw) OR ((testtube* NEAR/3 bab*):ti,ab,kw) OR (((artificial* OR oviduct*) NEAR/3 inseminat*):ti,ab,kw) OR 'icsi':ti,ab,kw OR ivf:ti,ab,kw |
200727 |
|
#3 |
#1 AND #2 |
31493 |
|
#4 |
#3 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
13898 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1016264 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4005117 |
|
#7 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8157287 |
|
#8 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
14966536 |
|
#9 |
#4 AND #5 – SR’s |
932 |
|
#10 |
#4 AND #6 NOT #9 – RCT’s |
1755 |
|
#11 |
#4 AND (#7 OR #8) NOT (#9 OR #10) – Observationele studies |
6063 |
|
#12 |
#9 OR #10 OR #11 |
8750 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Infertility, Male/ or ((exp Infertility/ or Fertility/) and exp Male/) or ((male* or men or man) adj3 (infertil* or hypofertil* or fertil* or subfertil* or infecund* or childless* or reproduct*)).ti,ab,kf. or ((spermatogen* or spermiation or spermiogen*) adj3 failure).ti,ab,kf. or (spermatozoon adj3 (abnormalit* or anomal*)).ti,ab,kf. or ((semen or sperm) adj3 (qualit* or quantit* or parameter* or dna)).ti,ab,kf. or asperm*.ti,ab,kf. or asthenazoosperm*.ti,ab,kf. or asthenosperm*.ti,ab,kf. or asthenozoosperm*.ti,ab,kf. or azoosperm*.ti,ab,kf. or cryptosperm*.ti,ab,kf. or cryptozoosperm*.ti,ab,kf. or hyposperm*.ti,ab,kf. or oligoasthenosperm*.ti,ab,kf. or oligosperm*.ti,ab,kf. or oligozoosperm*.ti,ab,kf. or retrograde ejaculat*.ti,ab,kf. or sco syndrome*.ti,ab,kf. or sertoli cell only syndrome*.ti,ab,kf. or teratozoosperm*.ti,ab,kf. or thermosensitive genic male steril*.ti,ab,kf. or globozoosperm*.ti,ab,kf. or macrozoosperm*.ti,ab,kf. |
102646 |
|
2 |
exp Sperm Injections, Intracytoplasmic/ or exp Fertilization in Vitro/ or exp Reproductive Techniques, Assisted/ or exp Insemination, Artificial/ or ((fertil* or reproduct*) adj3 (technique* or technolog* or therap* or treatment* or assist* or extracorporeal or in vitro)).ti,ab,kf. or ((intracytoplasm* or intra cytoplasm*) adj3 sperm* inject*).ti,ab,kf. or (testtube* adj3 bab*).ti,ab,kf. or ((artificial* or oviduct*) adj3 inseminat*).ti,ab,kf. or icsi.ti,ab,kf. or ivf.ti,ab,kf. |
117565 |
|
3 |
1 and 2 |
20832 |
|
4 |
limit 3 to yr="2000 -Current" |
15678 |
|
5 |
4 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
12270 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
737147 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2709295 |
|
8 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4692361 |
|
9 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5659051 |
|
10 |
5 and 6 – SR’s |
727 |
|
11 |
(5 and 7) not 10 – RCT’s |
1261 |
|
12 |
(5 and (8 or 9)) not (10 or 11) – Observationele studies |
4233 |
|
13 |
10 or 11 or 12 |
6221 |