Heruitgifte van medicatie
Uitgangsvraag
In hoeverre kan het heruitgeven van medicatie de milieu-impact verminderen?
Aanbeveling
Pas heruitgifte van medicatie toe vanuit duurzaamheidsoogpunt voor medicatie waarbij dit wettelijk is toegestaan en volg het Standpunt Heruitgifte van orale oncolytica.
Apotheker
- Betrek de voorschrijver bij heruitgifte van medicatie. Zorg voor eenduidige communicatie tussen de voorschrijver en apotheek richting de patiënt.
- Informeer de patiënt om ongebruikte medicatie in te leveren bij de apotheek waar deze is verstrekt, en dat er mogelijkheid bestaat dat zij heruitgegeven medicatie ontvangen.
- Geef de patiënt een keuze om wel/niet aan heruitgifte mee te doen.
- Zorg voor goede instructies zodat de patiënt de ongebruikte medicatie inlevert bij de apotheek.
Voorschrijver
- Instrueer patiënten om ongebruikte medicatie terug te brengen naar de apotheek.
- Ondersteun deelname aan heruitgifte.
Overwegingen
Definitie heruitgifte
Heruitgifte van medicatie is het opnieuw ter handstellen van medicatie aan een patiënt door een (poliklinische) apotheek voor gebruik in de thuissituatie. Deze medicatie is eerder ter hand gesteld en ongebruikt teruggebracht naar de apotheek.
Onder heruitgifte valt niet het herdistribueren* van medicatie binnen een ziekenhuis, zie hiervoor submodule Medicatiedistributiesystemen.
*Medicatie die vanuit de ziekenhuisapotheek reeds naar een zorgafdeling is verplaatst en retour is gekomen naar de apotheek voor inzet elders, wordt in de praktijk weleens heruitgifte van medicatie genoemd. Echter, er is geen terhandstelling geweest en dus valt het niet onder heruitgifte maar onder herdistributie. Herdistributie kent geen juridische restricties.
Kwaliteit van bewijs
Op basis van de beschikbare literatuur is gekeken naar de milieu-impact van heruitgifte van medicatie in vergelijking met het regulier verstrekken van medicatie aan een patiënt voor thuisgebruik en de verwerking van ongebruikte medicatie in deze situatie. Er zijn twee studies gevonden conform de PICO (Smale, 2024a; Smale, 2024b), waarbij de cruciale uitkomstmaat ‘climate change’ (uitgedrukt in CO2-emissie) en belangrijke uitkomstmaat ‘waste’ zijn gerapporteerd. Deze studies maakten gebruik van dezelfde dataset. Er werden geen studies gevonden voor de uitkomstmaten ‘eco-toxicity’, ‘human toxicity’, ‘water use’, ‘land use’, ‘acidification’ en ‘eutrophication’.
De overall kwaliteit van bewijs is laag. Dit betekent dat we onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten. Er is afgewaardeerd vanwege imprecisie. Op basis van deze GRADE beoordeling van de literatuur kunnen geen sterke conclusies geformuleerd worden over de precieze mate van milieu-impact van heruitgifte van medicatie. Echter, ondanks de methodologische beperkingen van beide studies, wijzen de resultaten wel dezelfde richting op: beide studies stellen dat heruitgifte van medicatie kan leiden tot een lagere milieu-impact wanneer kwaliteitscontroles (met name de materialen nodig hiervoor) beperkt dan wel doelmatig wordt ingezet.
Balans tussen gewenste en ongewenste effecten
Heruitgifte van ongebruikte medicatie die patiënten in de thuissituatie overhouden heeft meerdere gewenste effecten. Allereerst wordt het weggooien van medicatie die van goede kwaliteit is tegengegaan, hetgeen de milieu-impact door onnodige productie van medicatie die niet worden gebruikt en verbranding van medicatieverspilling vermindert. Heruitgifte kan naast de genoemde midpoint indicatoren voor climate change (CO2) ook positieve impact hebben op zogenoemde endpoint indicatoren, met potentiële gevolgen van milieubelasting voor human health damage (disability-adjusted life-years) en ecosystems damage (species × year; Smale, 2024b).
Daarnaast heeft heruitgifte de potentie om te leiden tot kostenbesparingen, in ieder geval bij dure medicatie en, in geval van schaarste, tot minder tekorten. Zowel patiënten als stakeholders zijn vóór heruitgifte, mits de kwaliteit van de medicatie geborgd wordt (Alhamad, 2018; Donyai, 2021; Hui, 2020; de Jong, 2018; Lam, 2021; McRae, 2021). Beperkingen zijn een hogere milieu-impact door het gebruik van de materialen om de kwaliteit van de medicatie te borgen, zoals de temperatuurloggers. Deze nadelen kunnen voorkomen worden door de materialen doelgerichter, oftewel alleen bij temperatuurafhankelijke medicatie, in te zetten.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Literatuur laat zien dat patiënten bereid zijn om teruggebrachte medicatie van een andere patiënt te gebruiken, mits de kwaliteit gewaarborgd is (Smale, 2022; Smale, 2024a). Deelname aan heruitgifte wordt vooral gedreven door de wens om een positieve maatschappelijke impact te hebben, met name op het gebied van betaalbaarheid en duurzaamheid van de zorg. Vertrouwen in de kwaliteit van het heruitgegeven medicijn is daarbij een voorwaarde. Een belangrijke bevorderende factor is het ontvangen van voldoende informatie over onder andere het heruitgifteproces. Tot slot is een gebruiksvriendelijk retourproces bij de apotheek gewenst.
In overleg met de patiënt kunnen overwegingen voor heruitgifte van medicatie aan bod komen en de keuzemogelijkheden besproken worden. Patiënten dienen de keuze te krijgen om aan heruitgifte mee te doen. Indien de patiënt dit weigert, ontvangt het de verstrekte medicatie zoals gebruikelijk.
Kostenaspecten
Heruitgifte van medicatie levert een kostenbesparing (minimaal €575 per patiënt per jaar) vergeleken met reguliere uitgifte en verwerking van ongebruikte medicatie, in ieder geval bij dure medicatie (Smale, 2024a). Dit zijn de netto besparingen gecorrigeerd voor de geleverde tijdsinvestering en benodigde materialen voor kwaliteitsborging. De doelmatigheidswinst bij goedkope (generieke) medicatie is onvoldoende onderzocht.
Gezondheidsgelijkheid
Heruitgifte kan leiden tot een toename in gezondheidsgelijkheid, omdat de potentiele vermindering van de milieu-impact van medicatie indirect kan bijdragen aan gezondheidsgelijkheid, aangezien negatieve milieueffecten wereldwijd relatief zwaar drukken op regio’s met een lagere sociaal-economische status (Chancel, 2022; The Lancet Public Health Editorial Board, 2022; Wilkinson, 2022). Heruitgegeven medicatie worden gecrediteerd bij de patiënt die het medicijn heeft teruggebracht. Kostenbesparingen kunnen uiteindelijk leiden tot een vermindering van het eigen risico waarmee de zorg toegankelijk blijft. Hierbij is het belangrijk dat het inleveren van ongebruikte medicatie zo toegankelijk mogelijk wordt ingericht, tijdens reguliere ziekenhuizbezoeken.
Aanvaardbaarheid:
Ethische aanvaardbaarheid
De interventie lijkt aanvaardbaar voor de betrokkenen (Smale, 2024c). Verspilling van medicatie wordt door alle stakeholders als onacceptabel geacht (Bekker, 2017; Smale, 2022). Er zijn geen ethische bezwaren, wanneer heruitgegeven medicatie verrekend wordt met de betalende verzekeraar. Er wordt de patiënt geen extra handeling opgelegd bij heruitgifte. Medicatie kan tijdens een regulier apotheekbezoek worden ingeleverd. Patiënten willen geïnformeerd worden over de aanpak en hoe kwaliteitsborging plaatsvindt. Hiermee kan een negatieve perceptie op heruitgegeven medicatie worden ondervangen.
Duurzaamheid
Deze module is volledig gericht op het verlagen van milieu-impact, derhalve speelt duurzaamheid een doorslaggevende- en hoofdrol bij de beschreven vergelijkingen.
Haalbaarheid
De interventie lijkt haalbaar, al kan de interventie alleen als standaardzorg in de praktijk worden toegepast mits dit juridisch is toegestaan. De haalbaarheid van de beschreven interventie hangt af van de wettelijke mogelijkheden. Op dit moment worden de juridische kaders voor heruitgifte in Nederland geschetst. Daarbij wordt er gekeken naar de verdere toepassing zoals eerder beschreven in het NVZA Standpunt Heruitgifte van orale oncolytica. De werkwijze in dit standpunt zal leidend gaan zijn voor de toepassing van heruitgifte, indien ook mogelijk voor andere medicatie.
Bij deze module is een implementatieplan opgesteld, dat ondersteuning biedt bij het (verder) in de praktijk brengen van de aanbevelingen.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Beschikbare literatuur met een lage bewijskracht laat zien dat heruitgifte van ongebruikte medicatie van patiënten in de thuissituatie potentie heeft om een positieve milieu-impact te bewerkstelligen. Daarnaast is de werkgroep van mening dat heruitgifte kosten kan besparen en dat patiënten bereid zijn om hieraan deel te nemen. Daarom beveelt de werkgroep aan om heruitgifte toe te passen voor alle daarvoor in aanmerking komende medicatie.
Onderbouwing
Patients frequently stop treatment earlier than intended, due to, for instance, treatment modifications, overprescribing, excessive supplies or insufficient effectiveness. As a result, they may be left with unused medications, leading to considerable waste. This waste carries substantial environmental consequences, from production to disposal. A part of these unused medications remains in unopened packaging. Redistributing unused medications could yield meaningful environmental benefits. Additionally, these unused medications represent significant financial value and redispensing them offers an opportunity to significantly reduce pharmaceutical expenses, at least for expensive medications, and help maintain the accessibility of healthcare. There is a strong demand from pharmaceutical supply chain stakeholders, driven by ongoing research into redistribution and a commitment to reducing medication waste, for clear guidance on the redistribution of unused medications. If proven effective, redistribution aligns with the Framework for Appropriate Care (emphasizing the efficient use of people, resources, and materials), as outlined in the Integrated Care Agreement. Furthermore, it is referenced under Article 6 of the Green Deal 3.0.
1. Climate change (critical)
|
Low GRADE |
The evidence suggests that redispensing unused oral (anticancer) medication with an optimized quality assurance process may reduce climate change when compared with standard dispensing practice and disposal of unused medication.
Source: (Smale, 2024b) |
2. Waste (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of redispensing of unused oral (anticancer) medication on waste in patients taking medications.
Source: (Smale, 2024a) |
3. Eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
|
No GRADE |
Outcome measures ‘eco-toxicity’, ‘human toxicity’, ‘water use’, ‘land use’, ‘acidification’, and ‘eutrophication’ were not reported.
Source: - |
Description of studies
Two studies were included in the analysis of the literature. Important study characteristics and results are summarized in the Evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Smale (2024a) conducted a prospective, single-group multicenter intervention study in outpatient pharmacies across four hospitals in the Netherlands (Redispensing Oral Anticancer Drugs (ROAD) study), including two academic medical centers to evaluate waste reduction by redispensing oral anticancer drugs (OADs) that remain unused by patients compared with the standard practice of disposing unused medication. The study period was from February 1, 2021 till February 1, 2023. Patients were eligible if they were aged ≥18 years with a clinical diagnosis of cancer and a current prescription for any oral anticancer drug (OAD) that could be stored at room temperature. The reported environmental outcome measure was waste reduction, which was defined as the percentage of returned OAD packages that was redispensed and the number of participants needed to prevent waste for one patient.
Smale (2024b) assessed the environmental impacts of redispensing quality assured OADs using a life cycle assessment (LCA) framework on the same dataset as Smale (2024a). A cradle-to grave LCA was performed, incorporating pharmaceutical production, formulation, packaging, distribution, quality control, redispensing logistics, and disposal (including disposal of disapproved packages). Each input within the defined scope was matched with the corresponding unit process and cumulative LCI from the Ecoinvent 3.8 LCI database (ecoinvent, Zurich, Switzerland). The reported environmental outcome measure was climate change, which was reported as kg of CO2e.
Results
1. Climate change (CO2 footprint/Global Warming Potential (GWP)) (critical)
Smale (2024b) reported on the outcome measure of climate change. An overview of the climate impact of redispensing in kg of CO2e per scenario is provided in Table 1. For the base case quality assurance procedure, the avoided emissions (1.9 kg CO2e per patient per year) of redispensing did not outweigh the emissions related to the quality assurance process burden (3.9 kg CO2e), resulting in a net climate impact of +2.1 kg CO2e per patient per year. In this scenario, time-temperature indicators (TTIs) were the main driver of climate impact in the quality assurance process and accounted for ~87% of quality assurance-related CO2e emissions. Production of APIs (active pharmaceutical ingredients) showed large variability and ranged from 57.6 kg CO2e/kg API (hydroxycarbamide) to 1910.9 kg CO2e/kg API (temozolomide) per patient per year. After optimization of the quality assurance process, redispensing of OADs resulted in a net benefit of 1.7 kg CO2e per patient per year. When only visual quality checks were performed, redispensing of OADs resulted in a net benefit of 2.4 kg CO2e per patient per year. Assuming that the optimized scenario and scenario with visual inspection only are both feasible, the guideline panel considered the difference in kgCO2e as relevant in favor of redispensing.
Table 1. Climate change impact summary of redispensing per quality assurance scenario
|
Scenario |
Quality assurance materials used |
Avoided emissions (kg CO2e) via redispensing, per patient per year |
Quality assurance process burden (kg CO2e), per patient per year |
Net climate impact (kg CO2e), per patient per year |
|
Base Case |
TTIs for all OADs, seal bag, leaflet |
1.9 (95% CI: 1.3–2.4) |
3.9 (95% CI: 3.8–4.1) |
+2.1 |
|
Optimized |
TTIs only for temp-sensitive OADs (≤25 °C) |
1.9 (95% CI: 1.4–2.6) |
~0.2 |
–1.7 |
|
Visual |
No TTIs; visual inspection only |
2.4 (95% CI: 1.8–3.0) |
≈ 0 |
–2.4 |
OAD, oral anticancer drugs; TTI, time-temperature indicator
2. Waste (important)
Smale (2024a) reported on the outcome measure of waste reduction. Overall, 171 patients (16.0%; 95% CI, 13.8%–18.3%) returned 335 unused OAD packages, representing 2.6% (95% CI, 2.4%–2.7%) of the dispensed packages. Following quality assurance procedures, 228 OAD packages from 128 patients were redispensed, resulting in a waste reduction of 68.1% (95% CI, 67.7%–68.5%) compared to standard care (disposal). The guideline panel considered this difference in waste as relevant in favor of redispensing.
3. Eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
No studies reported on important outcome measures eco-toxicity, human toxicity, water use, land use, acidification, and eutrophication.
Level of evidence of the literature
1. Climate change (critical)
The level of evidence regarding the outcome measure climate change was downgraded with two levels to low due to imprecision (-2; limited generalizability as only one study is included, heterogeneity of interventions).
2. Waste (important)
The level of evidence regarding the outcome measure waste was downgraded with three levels to very low due to risk of bias (-2; selection of participants, lack of adequate adjustment for confounders, lack of confounding analysis, lack of information on co-interventions), indirectness (-1; the outcomes were presented through economic impact or units, but not in weight).
3. Eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
Outcomes were not reported, thus could not be graded.
A systematic review of the literature was performed to answer the following question:
In patients receiving medication, what is the difference in environmental impact between standard care plus redispensing and standard care without redispensing of medication?
Table PICO
| Patients | Patients receiving medications |
| Intervention | Redispensing medication that has left the pharmacy and remains unused by a patient |
| Control | Standard dispensing practice of medication and disposal of unused medication by the pharmacy |
| Outcomes | Climate change (CO2 footprint/Global Warming Potential (GWP)), waste, eco-toxicity, human toxicity, water use, land use, acidification, eutrophication |
| Other selection criteria |
Study design: systematic reviews, randomized controlled trials, comparative observational studies (cohort studies, case-control studies), life cycle assessments Period: from 2023 |
Relevant outcome measures
This module focuses specifically on environmental outcomes. Currently, there is no standardized or acknowledged core outcome set available in the field of environmental impact. Therefore, the guideline panel focused on outcomes used in environmental assessments such as life cycle assessments, material flow analyses, waste audits, and footprinting.
The guideline panel considered climate change (CO2 footprint/Global Warming Potential) as critical outcome measures for decision making; and waste, eco-toxicity, human toxicity, water use, land use, acidification, and eutrophication as important outcome measures for decision making.
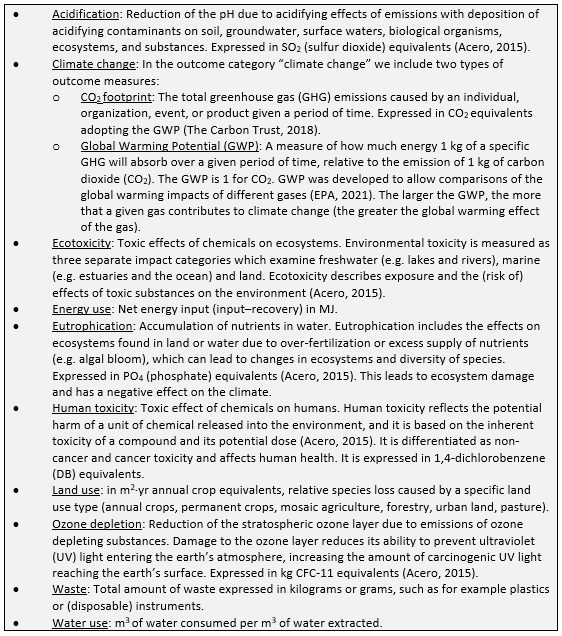
A priori, the guideline panel defined the outcome measures listed above according to the glossary provided in Box 1, which is adapted from leidraad Duurzaamheid in richtlijnen.
Given the variety in scopes and methods of performing and reporting in studies, the guideline panel did not define a priori the minimal important difference. Differences between the interventions were evaluated by the guideline panel after data extraction.
Box 1. Glossary
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2023 until 8 April 2025. The current search is an update of the systematic literature search performed in Standpunt Heruitgifte van orale oncolytica, which was published in 2023. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 245 unique results.
Studies were selected based on the following criteria:
- Systematic reviews in which searches were performed in at least two databases, with a detailed search strategy, risk of bias assessment and results of individual studies available, randomized controlled trials, (observational) comparative studies, LCA.
- Full-text English or Dutch language publication and
- Studies according to the PICO.
Initially, seven studies were selected based on the title and abstract screening. After reading the full text, five studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’) and two studies reporting on the same dataset were included (Smale, 2024a; Smale, 2024b).
- Alhamad H, Patel N, Donyai P. How do people conceptualise the reuse of medicines? An interview study. Int J Pharm Pract. 2018 Jun;26(3):232-241. doi: 10.1111/ijpp.12391. Epub 2017 Aug 9. PMID: 28795460; PMCID: PMC5969265.
- Bekker CL, Gardarsdottir H, Egberts TC, Bouvy ML, van den Bemt BJ. Redispensing of medicines unused by patients: a qualitative study among stakeholders. Int J Clin Pharm. 2017 Feb;39(1):196-204. doi: 10.1007/s11096-017-0424-8. Epub 2017 Jan 9. PMID: 28070689.
- Chancel L. Global carbon inequality over 1990–2019. Nat Sustain. 2022 Sep;5:931–938. doi: 10.1038/s41893-022-00955-z.
- Donyai P, McCrindle R, Hui TKL, Sherratt RS. Stakeholder Views on the Idea of Medicines Reuse in the UK. Pharmacy (Basel). 2021 Apr 16;9(2):85. doi: 10.3390/pharmacy9020085. PMID: 33923745; PMCID: PMC8167662.
- Hui TKL, Mohammed B, Donyai P, McCrindle R, Sherratt RS. Enhancing Pharmaceutical Packaging through a Technology Ecosystem to Facilitate the Reuse of Medicines and Reduce Medicinal Waste. Pharmacy (Basel). 2020 Mar 31;8(2):58. doi: 10.3390/pharmacy8020058. PMID: 32244551; PMCID: PMC7355753.
- de Jong MJ, Pierik MJ, Peters A, Roemers M, Hilhorst V, van Tubergen A. Exploring conditions for redistribution of anti-tumor necrosis factors to reduce spillage: A study on the quality of anti-tumor necrosis factor home storage. J Gastroenterol Hepatol. 2018 Feb;33(2):426-430. doi: 10.1111/jgh.13920. PMID: 28800384.
- Lam Y, McCrindle R, Hui TKL, Sherratt RS, Donyai P. The Effect of Quality Indicators on Beliefs about Medicines Reuse: An Experimental Study. Pharmacy (Basel). 2021 Jul 21;9(3):128. doi: 10.3390/pharmacy9030128. PMID: 34449720; PMCID: PMC8396184.
- McRae D, Gould A, Price-Davies R, Tagoe J, Evans A, James DH. Public Attitudes towards Medicinal Waste and Medicines Reuse in a 'Free Prescription' Healthcare System. Pharmacy (Basel). 2021 Apr 8;9(2):77. doi: 10.3390/pharmacy9020077. PMID: 33917990; PMCID: PMC8167727.
- The Lancet Public Health Editorial Board. No public health without planetary health. Lancet Public Health. 2022 Apr;7(4):e291. doi: 10.1016/S2468-2667(22)00068-8.
- Smale EM, Egberts TCG, Heerdink ER, van den Bemt BJF, Bekker CL. Key factors underlying the willingness of patients with cancer to participate in medication redispensing. Res Social Adm Pharm. 2022 Aug;18(8):3329-3337. doi: 10.1016/j.sapharm.2021.12.004. Epub 2021 Dec 25. PMID: 34973931.
- Smale EM, van den Bemt BJF, Heerdink ER, Desar IME, Egberts TCG, Bekker CL; ROAD Study Group. Cost Savings and Waste Reduction Through Redispensing Unused Oral Anticancer Drugs: The ROAD Study. JAMA Oncol. 2024a Jan 1;10(1):87-94. doi: 10.1001/jamaoncol.2023.4865. Erratum in: JAMA Oncol. 2025 Feb 1;11(2):189. doi: 10.1001/jamaoncol.2024.6289. PMID: 37971730; PMCID: PMC10654927.
- Smale EM, Ottenbros AB, van den Bemt BJF, Heerdink ER, Verploegen J, van Zelm R, Egberts TCG, Bekker CL. Environmental Outcomes of Reducing Medication Waste by Redispensing Unused Oral Anticancer Drugs. JAMA Netw Open. 2024b Oct 1;7(10):e2438677. doi: 10.1001/jamanetworkopen.2024.38677. PMID: 39388180; PMCID: PMC11581632.
- Smale EM, Verkerk EW, Heerdink ER, Egberts TCG, van den Bemt BJF, Bekker CL. Barriers and facilitators to implement the redispensing of unused oral anticancer drugs in clinical care: A hybrid-effectiveness type I study. Explor Res Clin Soc Pharm. 2024c Aug 17;15:100493. doi: 10.1016/j.rcsop.2024.100493. PMID: 39263193; PMCID: PMC11388756.
- Wilkinson JL, Boxall ABA, Kolpin DW, Leung KMY, Lai RWS, Galbán-Malagón C, Adell AD, Mondon J, Metian M, Marchant RA, Bouzas-Monroy A, Cuni-Sanchez A, Coors A, Carriquiriborde P, Rojo M, Gordon C, Cara M, Moermond M, Luarte T, Petrosyan V, Perikhanyan Y, Mahon CS, McGurk CJ, Hofmann T, Kormoker T, Iniguez V, Guzman-Otazo J, Tavares JL, Gildasio De Figueiredo F, Razzolini MTP, Dougnon V, Gbaguidi G, Traoré O, Blais JM, Kimpe LE, Wong M, Wong D, Ntchantcho R, Pizarro J, Ying GG, Chen CE, Páez M, Martínez-Lara J, Otamonga JP, Poté J, Ifo SA, Wilson P, Echeverría-Sáenz S, Udikovic-Kolic N, Milakovic M, Fatta-Kassinos D, Ioannou-Ttofa L, Belušová V, Vymazal J, Cárdenas-Bustamante M, Kassa BA, Garric J, Chaumot A, Gibba P, Kunchulia I, Seidensticker S, Lyberatos G, Halldórsson HP, Melling M, Shashidhar T, Lamba M, Nastiti A, Supriatin A, Pourang N, Abedini A, Abdullah O, Gharbia SS, Pilla F, Chefetz B, Topaz T, Yao KM, Aubakirova B, Beisenova R, Olaka L, Mulu JK, Chatanga P, Ntuli V, Blama NT, Sherif S, Aris AZ, Looi LJ, Niang M, Traore ST, Oldenkamp R, Ogunbanwo O, Ashfaq M, Iqbal M, Abdeen Z, O'Dea A, Morales-Saldaña JM, Custodio M, de la Cruz H, Navarrete I, Carvalho F, Gogra AB, Koroma BM, Cerkvenik-Flajs V, Gombač M, Thwala M, Choi K, Kang H, Ladu JLC, Rico A, Amerasinghe P, Sobek A, Horlitz G, Zenker AK, King AC, Jiang JJ, Kariuki R, Tumbo M, Tezel U, Onay TT, Lejju JB, Vystavna Y, Vergeles Y, Heinzen H, Pérez-Parada A, Sims DB, Figy M, Good D, Teta C. Pharmaceutical pollution of the world's rivers. Proc Natl Acad Sci U S A. 2022 Feb 22;119(8):e2113947119. doi: 10.1073/pnas.2113947119. PMID: 35165193; PMCID: PMC8872717.
Evidence table for LCA studies
|
Study reference |
Journal |
Study characteristics |
Methods |
Data collection |
Outcomes |
Interpretation |
Comments |
||||||||||||||||||||
|
Smale, 2024 |
JAMA Network Open
Journal information: International, peer-reviewed, open access, general medical journal that publishes research on clinical care, innovation in health care, health policy, and global health across all health disciplines and countries for clinicians, investigators, and policy makers.
Critical review: Peer reviewed article. Not in specific LCA journal. |
Type of study: LCA
Objective: To assess the environmental impact of redispensing quality-assured unused oral anticancer drugs (OADs), and to explore environmentally optimized approaches.
LCA-method: ISO14040-compliant; conducted in SimaPro v9.4.0.2 using ReCiPe 2016 (H), v1.07 method
Setting and country: Outpatient pharmacies in four hospitals in the Netherlands
Facility: Outpatient pharmacy departments
Years of data collection: February 2021 – February 2023
Surgical discipline(s): Oncology – treatment with oral anticancer agents
Funding and conflicts of interest: Funded by the Netherlands Organization for Health Research and Development (ZonMw), grant #848018008. No conflicts of interest reported. |
Goal and scope1: To evaluate waste reduction and environmental sustainability via redispensing unused OADs. The scope of the LCA included API synthesis, formulation, packaging, transport, incineration, and quality assurance process.
Functional unit(s)2: Treatment of one patient with oral anticancer drugs for one year
System boundaries: Cradle-to-grave
Included stages: API production, formulation, packaging, distribution, redispensing logistics, quality control, disposal
Stated excluded components: Not reported
Inventory database: Ecoinvent v3.8.
Allocation: No
Normalization & Weighting: Yes
Impacts reported: Human health (DALYs), ecosystem damage (species·year), climate change (kg CO₂-eq).
Contribution analysis: Yes
Scenario analysis: Yes
Comparative analysis: No
Sensitivity analysis: Yes
Uncertainty analysis: Yes
Variance analysis: No |
Quality assurance materials (ie, patient leaflet, seal bag, and TTI) were separated into components containing single materials and weighed. Background data on these components were taken from ecoinvent, version 3.8 (ecoinvent). It was assumed that paper (from the patient leaflet and secondary packaging materials) and plastic (from the seal bag) were recycled, following Dutch waste management protocols. The TTIs were collected in the pharmacy for reuse, and, if reuse was not possible, batteries were recycled.
A sample of 6 OADs was selected to calculate the estimates of the environmental outcomes of all redispensed OADs: hydroxycarbamide, lenalidomide, olaparib, pomalidomide, sunitinib, and temozolomide. Inventory data were gathered for production, distribution, and incineration of OAD packages. First, the production processes of the active pharmaceutical ingredients (APIs) were modeled based on chemical reaction pathways found via Reaxys. All modeled chemical reactions were scaled up to industrial scale, and background processes were taken from ecoinvent, version 3.8.19 The second step encompassed galenic formulation: the addition of excipients to APIs and the mixing processes to create unit doses (ie, tablets or capsules). Third, medication packaging processes, consisting of primary packaging material (ie, blisters or jars) and secondary packaging material (ie, Summary of Product Characteristics and carton box), were modeled. The transportation between manufacturing sides, wholesalers, and pharmacies were included. Disposal of OADs and other waste was assumed to take place in the Netherlands through incineration as chemical hazardous waste. |
Climate change Avoided emissions and QA process burden of redispensing per quality assurance scenario
Climate change impact summary of redispensing per quality assurance scenario
a TTIs for all OADs, seal bag, leaflet b TTIs only for temp-sensitive OADs (≤25 °C) c No TTIs; visual inspection only |
Redispensing unused OADs is climate beneficial only if:
|
Comments: The study found large variation in impact between different OADs, mainly due to the complexity of API molecules and differences in dosage strength and number of units per package. These differences may influence the generalizability of results to other drug classes.
Limitations:
Authors’ conclusion: Redispensing unused OADs is environmentally beneficial after QA process optimization and could support sustainable cancer care. |
API, active pharmaceutical ingredients; OAD, oral anticancer drugs; QA, quality assurance; TTI, time-temperature indicator.
1 Goals and scope: ‘Phase of life cycle assessment in which the aim of the study, and in relation to that, the breadth and depth of the study is established’
2 Functional unit: Quantified description of the function of a product or process that serves as the reference basis for all calculations regarding impact assessment.
Evidence table for intervention studies (RCTs and non-randomized observational studies)
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention |
Comparison/ control |
Follow-up |
Outcome measures and effect size |
Comments |
|
Smale, 2024a
|
Type of study: Observational study
Setting and country: Outpatient pharmacies of 4 hospitals in the Netherlands, 2 academic medical centers and 2 teaching hospitals
Funding and conflicts of interest: This study was supported by the Netherlands Organization for Health Research and Development (ZonMw grant No. 848018008) reported. Authors declared no competing interests. |
1071 patients
Median age 70 years (IQR 62-75 years)
42% women 58% men |
Participants received prescribed oral anticancer drugs with additional qualityassurance materials, so the pharmacy could redispense quality-assured drugs based on authenticity, appearance, remaining shelf life, and/or adequate storage. |
standard care (disposal) |
12 months |
171 patients (16.0%; 95% CI, 13.8%–18.3%) returned 335 unused OAD packages, representing 2.6% (95% CI, 2.4%–2.7%) of the dispensed packages. Following quality assurance procedures, 228 OAD packages from 128 patients were redispensed, resulting in a waste reduction of 68.1% (95% CI, 67.7%–68.5%) compared to standard care (disposal).
|
Limitations
Authors’ conclusions This study indicates that redispensing unused drugs has the potential to improve sustainability and affordability in cancer treatment.
|
Risk of Bias tables
Critical appraisal of LCAs (based on Drew, 2021)
Drew (2021) developed a critical appraisal pro forma, based on Weidema’s guidelines for critical review of LCA (Weidema, 1997). This scoring system consists of 16 appraisal criteria, which are divided between the different phases of an LCA. It addresses a range of study quality indicators, such as internal validity, external validity, consistency, transparency, and bias. The percentage score provides an indication of the overall study quality. A higher score indicates a higher overall study quality. The points that can be obtained are displayed in the column labeled "appraisal criteria".
|
Appraisal criteria |
Indicator(s) |
Key effect modifiers |
Smale (2024b) |
|
Phase 1: Goal & Scope (13 points) |
|
|
|
|
Study goal is clearly stated, including the study's rationale (1), intended application (1), and intended audience (1) |
Transparency |
|
3 |
|
Lifecycle assessment method is clearly stated (1) |
Transparency |
Process-based life-cycle assessment, which is well suited to product-level analysis, may underestimate environmental impacts (i.e. from truncation error); economic input-output lifecycle assessment (EIO-LCA), which uses aggregate data and is well-suited to sector-level analysis, may overestimate environmental impacts |
1 |
|
Functional unit is clearly defined and measurable (1), justified (1), and consistent with the study's intended application (1) |
Consistency |
|
2 |
|
The system to be studied is adequately described with clearly stated system boundaries (1), lifecycle stages (1), and appropriate justification of any omitted stages (1) |
Transparency; bias |
Assessments with narrow system boundaries that exclude a number of lifecycle stages are prone to underestimating life-cycle environmental impacts |
1 |
|
The system covers production (1), use/reuse (1) and disposal (1) of materials and energy (half mark if only for energy and vice versa) |
Internal Validity; completeness |
|
3 |
|
Phase 2: Inventory analysis (7 points) |
|
|
|
|
The data collection process is clearly explained, including the source(s) of foreground material weights and energy values (1); the source(s) of reference data (e.g. inventory database; 1); and what data are included (e.g. production and disposal of unit processes; 1) |
Transparency, internal Validity |
|
3 |
|
Representativeness of the data is discussed (1), differences in electricity generating mix are accounted for (1), and the potential significance of exclusions or assumptions is addressed (1) |
Internal validity; external validity |
|
1 |
|
Allocation procedures, where necessary, are described and appropriately justified (1; mark given if no allocation used) |
Transparency; bias |
|
1 |
|
Phase 3: Impact assessment (6 points) |
|
|
|
|
Impact categories (1), characterization method (1), and software used (1) are documented transparently |
Transparency |
|
3 |
|
Results are clearly reported in the context of the functional unit (1) (0.5 if graphically, 0 if only normalized results reported) |
Consistency; transparency |
|
1 |
|
A contribution analysis is performed and clearly reported (1), and hotspots are identified (1) |
|
|
2 |
|
Phase 4: Interpretation (9 points) |
|
|
|
|
Conclusions are consistent with the goal and scope (1) and supported by the impact assessment results (1) |
Internal Validity; consistency |
|
2 |
|
Results are contextualized through the use of sensitivity analysis (1) and uncertainty analysis (1) |
Internal Validity |
|
2 |
|
Limitations are adequately discussed (1), and the potential impact of omissions or assumptions on the study's outcomes are described (1) |
Bias |
|
2 |
|
The assessment has been critically appraised (i.e. peer review if journal article or independent, external critical review if report/thesis; 1) |
Bias |
|
1 |
|
Source(s) of funding and any potential conflict(s) of interest are disclosed (1), and are unlikely to be a source of bias (1) |
Bias |
|
2 |
|
|
Total (/35) |
|
30 |
|
|
Percentage score |
|
86% |
Smale (2024a, cross-sectional, observational, and retrospective studies)
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors?
|
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables?
|
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed?
|
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Low, Some concerns, High |
|
|
Smale, 2024a |
Probably no
Reason. Only those who consented and had unused drugs are included. |
Definitely yes
Reason: Exposure was systemetically assessed and well-described. |
Definitely no
Not reported |
Definitely no
Not reported |
Definitely no
Not reported |
Probably yes
Reason: outcome assessment is objective. |
Probably yes
Reason: Incomplete data due to not return unused drugs |
Definitely no
Not reported |
HIGH |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Alnsour M, Moqbel S. Enhancing environmental sustainability through a household pharmaceuticals take-back program in Jordan. Environmental Monitoring and Assessment [Internet]. 2023 Nov 7;195(12). Available from: https://doi.org/10.1007/s10661-023-12050-7 |
Wrong intervention |
|
Gianino MM, Cotugno V, Scattaglia M, Colasanto I, Scaldaferri M, Cattel F. Medicine recovery and reuse in a hospital setting: a lesson from Italy. Int J Pharm Pract. 2022 Dec 31;30(6):554-558. doi: 10.1093/ijpp/riac056. PMID: 35808979. |
Wrong intervention |
|
Mohammed AM, Al-Hamadani F. Assessment of general population knowledge, attitude, and practice on safe unused and expired drugs disposal: a cross-sectional study. F1000Res. 2023 Oct 16;12:1333. doi: 10.12688/f1000research.142146.1. PMID: 38515859; PMCID: PMC10955187. |
Wrong intervention |
|
Monestime S, Magallon T, Jenkins L, Page R. Guidance on Implementing an Oral Chemotherapy Drug Repository Program in a Medically Integrated Pharmacy Setting. JCO Oncol Pract. 2021 Jul;17(7):e448-e453. doi: 10.1200/OP.20.00959. Epub 2021 Apr 26. PMID: 33900790. |
Wrong intervention |
|
Yu X, Lyu S, Zhao W, Guo C, Xu J, Sui Q. A picture of pharmaceutical pollution in landfill leachates: Occurrence, regional differences and influencing factors. Waste Manag. 2024 Jul 15;184:20-27. doi: 10.1016/j.wasman.2024.05.019. Epub 2024 May 24. PMID: 38788499. |
Wrong intervention
|
Beoordelingsdatum en geldigheid
Publicatiedatum : 07-05-2026
Beoordeeld op geldigheid : 07-05-2026
Algemene gegevens
De ontwikkeling/herziening van deze module werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS).
De financier heeft geen enkele invloed gehad op de inhoud van de leidraad.
Samenstelling werkgroep
Voor het ontwikkelen van de leidraad is in 2024 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij farmaceutisch specialistische zorg.
Werkgroep Inhoud
- Dr. L.J.M. (Loes) van Herpen – Meeuwissen (voorzitter), ziekenhuisapotheker, Radboudumc, NVZA
- Dr. M.E. (Milly) Attema – de Jonge, ziekenhuisapotheker, Meander MC, NVZA
- Dr. C. (Charlotte) Bekker, universitair docent, Radboudumc, persoonlijke titel
- Drs. V. (Vivienne) de Smet, AIOS spoedeisende geneeskunde, Diakonessenhuis, NVSHA
- Dr. N.G.M. (Nicole) Hunfeld, ziekenhuisapotheker, universitair hoofddocent, Erasmus MC, NVIC
- Dr. B.J.A. (Ben) Janssen, farmacoloog, universitair hoofddocent, Maastricht UMC, persoonlijke titel
- Dr. B. (Berber) Kapitein, kinderarts-intensivist, Amsterdam UMC, NVK
- Drs. R. (Remco) Minkhorst, anesthesioloog, UMC Utrecht, NVA
- Drs. J.D. (Joost) Piët, arts-docent en promovendus farmacotherapie, Amsterdam UMC, NVKFB
- Y.H.M. (Yvonne) van Grinsven – Ariaans, (regie)verpleegkundige, Radboudumc, V&VN
- M. (Marga) van Timmeren, kwaliteitsfunctionaris, BModesto, NVFZ
Werkgroep Implementatie
- B.A.P. (Bart) Cramers, apotheker, programmamanager dure geneesmiddelen, NVZ
- Drs. M. (Maarten) Loof, programmamanager dure geneesmiddelen, ZN
- P. (Peter) Roos, adviseur, UMCNL (voorheen NFU; tot december 2024)
- Prof. dr. E.L. (Noortje) Swart, ziekenhuisapother, hoogleraar Klinische Farmacologie en Apotheek, hoofd adeling klinische farmacologie en apotheek, Amsterdam UMC, UMCNL (vanaf maart 2025)
Klankbordgroep
- Dr. P.H.P (Pascal) de Jong, reumatoloog, universitair hoofddocent, Erasmus MC, NVR
- Dr. F. (Femme) Dirksmeier – Harinck, MDL-arts, Franciscus, NVMDL
- Prof. dr. W.J.K. (Wouter) Hehenkamp, gynaecoloog, hoogleraar gynaecologie gericht op doelmatige en duurzame zorg, Amsterdam UMC, NVOG
- Drs. A. (Annemieke) Horikx, apotheker, KNMP
- Dr. J.J.W.M. (Jeroen) Janssen, internist-hematoloog, Radboudumc, NIV
- Dr. P.H.C. (Philip) Kremer, neuroloog, Leids Universitair Medisch Centrum, NVN
- Dr. M. (Maartje) Los, internist-oncoloog, St. Antonius Ziekenhuis, NIV
- Prof. dr. F.M.A.C. (Fabrice) Martens, cardioloog, hoogleraar Preventieve cardiologie, Amsterdam UMC, NVVC
- Drs. N.M.F. (Nikki) Noorda, klinisch geriater, Dijklander Ziekenhuis, NVKG
- Dr. S. (Sam) Schoenmakers, gynaecoloog, Erasmus MC, NVOG
- Drs. D.C. (Dorothée) van Trier, traumachirurg, Diakonessenhuis, NVvH
- P. (Paula) Warmerdam, verpleegkundig specialist, Alrijne Ziekenhuis, V&VN
Met ondersteuning van
- Dr. R. (Renee) Bolijn, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. T. (Thibaut) Dederen, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. C.T.J. (Charlotte) Michels, senior adviseur, Kennisinstituut van de Federatie Medisch Speclisten
- E. (Esther) van der Bijl, Informatiespecialist, Kennisinstituut van de Federatie Medisch Speclisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Gemelde belangen |
Ondernomen actie |
|
Werkgroep Inhoud |
||||
|
Van Herpen – Meeuwissen (voorzitter) |
Ziekenhuisapotheker, Radboudumc, Nijmegen |
NVZA: lid commissie Duurzaamheid |
* ZonMW, Medicatie in eigen beheer 848022007. * Auteur: |
Geen restricties |
|
Attema – de Jonge |
Ziekenhuis apotheker, Meander Medisch Centrum, Amersfoort |
Lid Commissie Duurzaamheid NVZA |
Geen |
Geen restricties |
|
Bekker |
Senior onderzoeker, Radboudumc, Nijmegen |
Voorzitter NFU werkgroep Green deal duurzame zorg thema 5 'medicijnen' |
* ZonMw Heruitgifte orale oncolytica 848018008 * ZonMw RODEO trial 10140021910501 * Transformatieovereenkomst heruitgifte orale oncolytica * VWS Green Deal duurzame zorg thema 5 'medicijnen' * Senior onderzoeker duurzaam geneesmiddelgebruik |
Geen restricties |
|
De Smet |
AIOS SEH, Diakonessenhuis, Utrecht |
* Lid commissie Groene SEH |
Geen |
Geen restricties |
|
Hunfeld |
* Ziekenhuisapotheker, Erasmus MC, Rotterdam (betaald) * Projectleider onderzoek duurzame zorg, Erasmus MC, Rotterdam (betaald) |
* Vice voorzitter en penningmeester KNMP (betaald) * Voorzitter Groene IC NVIC (onbetaald) vVoorzitter commissie ATG (LCG) (betaald) * Toezichthouder VVT Het Maanderzand (betaald) * Lid Commissie Duurzaamheid NVZA |
NWO (geen onderzoek over medicijnen) |
Geen restricties |
|
Janssen (Ben) |
Universitair Hoofddocent Farmacologie, Vakgroep Farmacologie & Toxicologie, Faculty of Health Medicines and Life Sciences Maastricht University. Werk op afdeling Beeldvorming van het Maastrichts Universitair Medisch Centrum. |
Geen |
Geen |
Geen restricties |
|
Kapitein |
Kinderarts-intensivist, Emma Kinderziekenhuis Amsterdam UMC, Amsterdam |
* Lid Groene Kinderarts * NVK Lid wetenschapscommissie |
* MACU-PICU Stichting CJ Vaillant. Multisystem phenotyping of severe ACUte asthma at the Pediatric Intensive Care Unit (macu-pico). Postdoc (geen PI). * AUMC Medewerkersberaad innovatie subsidie "Het AUMC medewerkersberaad: op weg naar duurzaam woon-werkverkeer (studie reeds afgerond). |
Geen restricties |
|
Minkhorst |
Anesthesioloog UMC Utrecht |
Geen |
Geen |
Geen restricties |
|
Piët |
*Fulltime arts-docent en -onderzoeker Farmacotherapie in het AmsterdamUMC (locatie VUmc). *Al het onderwijs betreffende het voorschrijven van medicatie verzorgen voor de opleidingen geneeskunde, tandheelkunde en masteropleidingen voor verpleegkundigen. *Promovendus op gebied van het integreren van milieu-impact door medicatie in het medisch onderwijs. Deze werkzaamheden zijn allen betaald vanuit mijn aanstelling. |
* Klinisch farmacoloog in opleiding * Projectcoördinator Erasmus+ projecten CP4T en PlanED Prescribing |
Erasmus+ projecten: * Planetary Health Education in Prescribing (PlanED Prescribing) * Clinical Pharmacology and Therapeutics Teach The Teacher (CP4T)
Auteur NTvG artikel "Vermindering van de milieu-impact van medicatie; De rol van de voorschrijver" (D7985) (Toekomstige) Uitkomsten (wetenschappelijk) van Erasmus+ project PlanED Prescribing en van eigen PhD. PMID 39303730 |
Geen restricties |
|
Van Grinsven – Ariaans |
* Verpleegkundige Orthopedie Radboudumc (contract 12 uur, betaald) * Kwaliteitsfunctionaris afdeling Orthopedie/KNO/MKA/PCH/Trauma Radboudumc (contract 12 uur, betaald) |
Geen |
Geen |
Geen restricties |
|
Van Timmeren |
Sr Quality Officer, Bmodesto, Lelystad |
Geen |
Geen |
Geen restricties |
|
Werkgroep Implementatie |
||||
|
Cramers |
Programmamanager Dure Geneesmiddelen NVZ Belangenbehartiging ziekenhuizen op dure geneesmiddelen gebied. Gaat over kwaliteit, beschikbaarheid en betaalbaarheid. |
Geen |
Geen |
Geen restricties |
|
Loof |
Programmamanager Dure Geneesmiddelen bij ZN |
Geen |
Geen |
Geen restricties |
|
Roos |
Adviseur binnen NFU |
Geen |
Geen |
Geen restricties |
|
Swart |
Hoofd Afdeling Apotheek en Klinische Farmacologie, AmsterdamUMC |
* Voorzitter Wetenschappelijke Adviesraad Commissie Farmacotherapeutisch Kompas (WAR CFK), Zorginstituut Nederland * Voorzitter NVKFB. * Lid bestuur KNMP |
Echtgenoot werkt bij Pfizer in een niet commerciële functie. Geen relatie met werkgroep
Medicijn voor de Maatschappij: Bereidingen voor zeldzame metabole ziekten. |
Geen restricties |
|
Klankbordgroep |
||||
|
De Jong |
Reumatoloog, Erasmus MC, Rotterdam |
* Lid adviesraad voor Abbvie; AstraZeneca; Bristol-Myers Squibb; Galapagos; Lilly; Novartis; Pfizer; Sanofi Genzyme; UCB * Verzorging van onderwijs voor Abbvie; Galapagos; Lilly; Novartis; Pfizer |
Subsidies voor investigated initiated studies van Abbvie; Dutch Arthritis Foundation; Galapagos; Lilly; Pfizer. 1. Abbvie, ontwikkelen tool voor zorg op afstand, projectleider. 2. Dutch Arthitis Foudation, gecombineerde leefstijlinterventie trial, projectleider. 3. Galapagos: trial naar belandeling op maat. 4. Pfizer: Toediening van medicatie obv chronobiologie, projectleider. 5. Lilly: Implementatieonderzoek gericht op persoonsgerichte zorg, projectleider. |
Geen restricties |
|
Dirksmeier – Harinck |
MDL-arts, Franciscus, Rotterdam |
Geen |
Geen |
Geen restricties |
|
Hehenkamp |
Gynaecoloog, AmsterdamUMC, Amsterdam |
Allen onbetaald: -lid pijlerbestuur gynaecologie -voorzitter Gynae Goes Green (landelijke groen commissie GYN) -lid bestuur SIG anticonceptie -Bestuur Hector Treub stichting |
1. ZonMW: Substitutie van zorg Covid, projectleider. 2. ZonMW: Ulipristal bij myomen., projectleider. 3. Merit Medical: QUESTA trial (adenomyose en hysterectomie danwel embolisatie). 4. ZonMW: Keuzehulp Myomen, projectleider. |
Geen restricties |
|
Horikx |
Apotheker, teamleider Geneesmiddel Informatie Centrum KNMP |
* Bestuurslid Stichting Farmaceutisch Erfgoed. * Commissielid interacterende medicatie VKA's. * Werkgroeplid kritische en kwetsbare geneesmiddelenlijst-NVZA. * Praktijkteamlid palliatieve zorg |
Geen |
Geen restricties |
|
Janssen (Jeroen) |
internist-hematoloog, Afdeling Hematologie, Radboud UMC, Nijmegen, betaald |
* Voorzitter, St. Apps for Care and Science, betaald. * Bestuurslid en penningmeester, Nederlandse Vereniging voor Hematologie, onbetaald |
De St. Apps for Care and Science ontwikkelt de HematologyApp, een smartphone-, tablet- en binnenkort ook web-based applicatie die als doel heeft het werk van hematologen te verbeteren, de kwaliteit van de zorg voor hematologische patienten te verbeteren en klinisch wetenschappelijk onderzoek te bevorderen. Deze stichting zoekt ondersteuning voor het behalen van haar doelen bij farmaceutische bedrijven die initatieven van de stichting kunnen sponsoren. De volgende bedrijven zijn sponsor/donateur van de stichting: Daiichi-Sankyo, Johnson & Johnson, SERB, Sanofi, SOBI, Novo-Nordisk, MSD, Biomea, AstraZeneca, BristolMyersSquibb, Alexion, Kite-Gilead, Pfizer, Abbvie, Astellas,Novartis, Amgen, Takeda en Servier. |
Geen restricties |
|
Kremer |
*Research Director Neurology bij The Centre for Human Drug Research, Leiden * Neuroloog bij het Leids Universitair Medisch Centrum, Leiden |
Geen |
In het CHDR ben ik verantwoordelijk voor ongeveer 10 vroege fase medicijnstudies gefinancierd door veelal Amerikaanse biotech of grote farma. De onderzoeksmiddelen zitten dermate vroeg in het ontwikkeltraject dat er geen belangenverstrengeling is. |
Geen restricties |
|
Los |
internist oncoloog in het St Antonius Ziekenhuis Utrecht/ Nieuwegein |
Geen |
Geen |
Geen restricties |
|
Martens |
Cardioloog, hoogleraar Preventieve Cardiologie bij het Amsterdam UMC, Amsterdam. Namens de NVVC vertegenwoordigend. |
* Adviseur CVRM en medicatie NVVC. * Voorzitter Werkgroep Geneesmiddelen NVVC * Voorzitter DCVA Commissie Preventie * Clinical Valorization Officer Amsterdam UMC *Voorzitter Hartstichting Hart-Vaatagenda-project 'Op tijd ontdekken' Wetenschappelijk nog wel verbonden aan het HartVaatCentrumSalland |
Sprekersvergoeding zonder belangenverstrengeling gezien altijd naar Amsterdam UMC.
Sponsoring GOLDEN-studie: Novartis, Amarin, Novo Nordisk en een Europese IHI-grant. Sponsoring 2-DECIDE-studie: ZoNMW en ZE&GG Sponsoring EUROASPIRE: Hartstichting |
Geen restricties |
|
Noorda |
Klinisch geriater in het Dijklanderziekenhuis |
Geen |
Geen |
Geen restricties |
|
Schoenmakers |
Gynaecoloog, Erasmus MC Universtair Medisch Centrum, Rotterdam |
* Wetenschap-commissielid Strong Babies (onbetaald) * Gezondheidsraad - algemeen / commissie vaccinatie (vacatiegelden) |
ZonMW Open Competitie (2019-2024) - ondewerp Obesitas, microbioom en zwangerschap |
Geen restricties |
|
Van Trier |
(Trauma) Chirurg OLVG en BovenIJ Ziekenhuis |
* Werkgroep Groen OK NVVH. * Tevens lid van de werkgroep Plastic en Circulair van het Landelijk Netwerk Groene OK, onbetaald. |
Geen |
Geen restricties |
|
Warmerdam |
Verpleegkundig specialist werkzaam bij Alrijne |
Presentaties geven aan POH en Huisartsen |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland (PFN) voor deelname aan de werkgroep Inhoud en aan twee invitational conferences. Op advies van de PFN heeft de werkgroep de uitkomsten uit het rapport Verduurzaming van de zorg geïntergreerd in de modules. Daarnaast is module 6 Communicatie over milieubewust medicatiegebruik specifiek gericht op communicatie over milieubewust medicatiegebruik met patiënten. De conceptleidraad is tevens voor commentaar voorgelegd aan de PFN en de aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de leidraad voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de leidraad per module op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Heruitgifte van medicatie |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten), volgt uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte methodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze leidraad is hieronder weergegeven.
Zoekverantwoording
Zoekstrategie - 8 april 2025
Embase.com
|
No. |
Query |
|
#1 |
redispens*:ti,ab,kw OR 're dispens*':ti,ab,kw OR (((reus* OR 're us*' OR redistribut* OR 're distribut*' OR reallocat* OR 're allocat*' OR reissu* OR 're issu*' OR 're utili*' OR reutili* OR recycl* OR 're cycl*' OR unus* OR 'un us*') NEAR/4 (medication OR drug OR drugs OR pharmaceutical* OR oncologic* OR medicine OR antineoplast* OR 'anti cancer*' OR chemotherapeutic*)):ti,ab,kw) |
|
#2 |
'drug'/exp OR 'drug therapy'/exp OR medication:ti,ab,kw OR drug:ti,ab,kw OR drugs:ti,ab,kw OR pharmaceutical*:ti,ab,kw OR oncologics:ti,ab,kw OR medicine*:ti,ab,kw OR antineoplastics:ti,ab,kw OR 'anti cancers':ti,ab,kw OR chemotheraupeutics:ti,ab,kw OR 'anti cancer agent*':ti,ab,kw |
|
#3 |
'biodegradable plastic'/exp OR 'biodiversity'/de OR 'climate change'/exp OR 'climate resilience'/exp OR 'disposable equipment'/exp OR 'ecological diversity'/exp OR 'energy conservation'/exp OR 'environmental aspects and related phenomena'/exp OR 'environmental footprint'/exp OR 'environmental protection'/exp OR 'eutrophication'/exp OR 'life cycle assessment'/exp OR 'pollution and pollution related phenomena'/exp OR 'species diversity'/exp OR 'waste and waste related phenomena'/exp OR 'wastewater'/exp OR 'water management'/exp OR 'water pollution'/exp OR 'global warming potential'/exp OR acidification:ti,ab,kw OR (((water OR land) NEXT/1 use):ti,ab,kw) OR (((air OR organic OR soil OR water OR plastic* OR liquid*) NEAR/4 (pollut* OR contamina* OR wast*)):ti,ab,kw) OR biodivers*:ti,ab,kw OR 'biological divers*':ti,ab,kw OR (((co2 OR 'co 2' OR carbon OR 'nitrous oxide') NEAR/3 (emission* OR footprint OR equival* OR reduct*)):ti,ab,kw) OR (((nature OR environment* OR climat*) NEAR/3 (impact* OR pollut* OR conservat* OR protect* OR preserv* OR effect* OR benefit* OR chang* OR exposure* OR resilien*)):ti,ab,kw) OR disposable*:ti,ab,kw OR ((eco* NEAR/3 (toxic* OR efficien* OR damage)):ti,ab,kw) OR ecotoxic*:ti,ab,kw OR ecoefficien*:ti,ab,kw OR (((emission OR waste) NEAR/3 reduc*):ti,ab,kw) OR environmental*:ti OR (((equipment* OR product* OR waste*) NEAR/3 reus*):ti,ab,kw) OR recycl*:ti,ab,kw OR 'resource recover*':ti,ab,kw OR eutrophicat*:ti,ab,kw OR (((global OR climate) NEAR/2 warming):ti,ab,kw) OR ((green* NEAR/2 (deal OR surger* OR effect* OR gas* OR resource*)):ti,ab,kw) OR (((hospital OR medical OR zero OR product* OR byproduct* OR 'by product*' OR avoid* OR energy OR management OR nuclear OR biomass) NEAR/3 waste*):ti,ab,kw) OR ((('life cycle' OR lifecycle) NEAR/2 (assess* OR inventor*)):ti,ab,kw) OR lca:ti,ab,kw OR lcas:ti,ab,kw OR 'human toxicity potential*':ti,ab,kw OR (((ep OR h+ OR gwp OR faetp OR fatp OR ap OR cfc OR 'kg n' OR 'nox' OR '2.4' OR '2,4' OR pocp OR so2 OR dichlorobenzen* OR ethan* OR po4 OR dcb) NEAR/3 equival*):ti,ab,kw) OR ((ozone NEAR/3 (deplet* OR hole*)):ti,ab,kw) OR (((plastic* OR microplastic* OR 'micro plastic*') NEAR/3 (overuse OR soup OR pollut* OR contaminat*)):ti,ab,kw) OR recycle*:ti,ab,kw OR recycling:ti,ab,kw OR (((refuse OR waste) NEAR/3 disposal):ti,ab,kw) OR reusable*:ti,ab,kw OR reuse*:ti,kw OR reusing:ti,kw OR 'rising sea level*':ti,ab,kw OR 'sea level ris*':ti,ab,kw OR smog:ti,ab,kw OR sustainab*:ti,kw OR ((sustainab* NEAR/3 (development* OR cycle* OR management OR effect* OR environment*)):ti,ab,kw) OR ((water NEAR/3 (purificat* OR sanitat* OR treatment)):ti,ab,kw) OR wastewater:ti,ab,kw OR ((hydrogen NEAR/3 moles NEAR/3 equival*):ti,ab,kw) OR 'circular econom*':ti,ab,kw OR biodegradab*:ti,ab,kw OR (((ecological OR environmental OR water OR energy OR climate OR global) NEAR/2 footprint*):ti,ab,kw) OR waste:ti,ab,kw OR wastes:ti,ab,kw OR reuse:ti,ab,kw OR reusab*:ti,ab,kw OR reprocess*:ti,ab,kw OR pollut*:ti,ab,kw OR greening:ti,ab,kw OR spillage:ti,ab,kw OR spilling:ti,ab,kw OR spoilage:ti,ab,kw OR salinization:ti,ab,kw OR 'cradle to cradle':ti,ab,kw OR 'carbon neutral*':ti,ab,kw OR wastage*:ti,ab,kw |
|
#4 |
#1 AND #2 AND #3 |
|
#5 |
#4 AND [1-1-2023]/sd - Totaal |
Ovid/Medline
|
# |
Searches |
|
1 |
(redispens* or re dispens* or ((reus* or re us* or redistribut* or re distribut* or reallocat* or re allocat* or reissu* or re issu* or re utili* or reutili* or recycl* or re cycl* or unus* or un us*) adj4 (medication or drug or drugs or pharmaceutical* or oncologic* or medicine or antineoplast* or anti cancer* or chemotherapeutic*))).ti,ab,kf. |
|
2 |
exp Pharmaceutical Preparations/ or exp Drug Therapy/ or medication.ti,ab,kf. or drug.ti,ab,kf. or drugs.ti,ab,kf. or pharmaceutical*.ti,ab,kf. or oncologics.ti,ab,kf. or medicine*.ti,ab,kf. or antineoplastics.ti,ab,kf. or anti cancers.ti,ab,kf. or chemotheraupeutics.ti,ab,kf. or anti cancer agent*.ti,ab,kf. |
|
3 |
Biodegradable Plastics/ or exp Biodiversity/ or exp Carbon Footprint/ or exp Environmental Pollution/ or exp Climate Change/ or Disposable Equipment/ or Environment/ or Equipment Reuse/ or exp Eutrophication/ or Greenhouse Gases/ or Greenhouse Effect/ or exp Hazardous Waste/ or exp Medical Waste/ or Ozone Depletion/ or Recycling/ or exp Refuse Disposal/ or Smog/ or Waste Products/ or exp Waste Water/ or acidification.ti,ab,kf. or ((air or organic or soil or water or plastic* or liquid*) adj4 (pollut* or contamina* or wast*)).ti,ab,kf. or (biodivers* or "biological divers*").ti,ab,kf. or ((co2 or "co 2" or carbon) adj3 (emission* or footprint or equival* or reduct*)).ti,ab,kf. or ((nature or environment* or climat*) adj3 (impact* or pollut* or conservat* or protect* or preserv* or effect* or benefit* or chang* or exposure* or resilien*)).ti,ab,kf. or disposable*.ti,ab,kf. or (eco* adj3 (toxic* or efficien* or damage)).ti,ab,kf. or ecotoxic*.ti,ab,kf. or ecoefficien*.ti,ab,kf. or ((waste or emission*) adj3 reduc*).ti,ab,kf. or environmental*.ti. or ((equipment* or product* or waste*) adj3 reus*).ti,ab,kf. or recycl*.ti,ab,kf. or resource recover*.ti,ab,kf. or eutrophicat*.ti,ab,kf. or ((global or climate) adj2 warming).ti,ab,kf. or (("life cycle" or lifecycle) adj2 (assess* or inventor*)).ti,ab,kf. or LCA.ti,ab,kf. or LCAs.ti,ab,kf. or (("life cycle" or lifecycle) adj2 (assess* or inventor* or analys*)).ti,ab,kf. or (green* adj2 (deal or surger* or effect* or gas* or resource*)).ti,ab,kf. or greening.ti,ab,kf. or ((hospital or medical or zero or product* or byproduct* or "by product*" or avoid* or energy or management or nuclear or biomass) adj3 waste*).ti,ab,kf. or "human toxicity potential*".ti,ab,kf. or ((EP or H+ or GWP or FAETP or FATP or AP or CFC or "kg N" or "NOx" or "2.4" or "2,4" or POCP or SO2 or dichlorobenzen* or ethan* or PO4 or DCB) adj3 equival*).ti,ab,kf. or (ozone adj3 (deplet* or hole*)).ti,ab,kf. or ((plastic* or microplastic* or "micro plastic*") adj3 (overuse or soup or pollut* or contaminat*)).ti,ab,kf. or recycle*.ti,ab,kf. or recycling.ti,ab,kf. or ((refuse or waste) adj3 disposal).ti,ab,kf. or reusable*.ti,ab,kf. or reuse*.ti,kf. or reusing.ti,kf. or "rising sea level*".ti,ab,kf. or "sea level ris*".ti,ab,kf. or smog.ti,ab,kf. or sustainab*.ti,kf. or (sustainab* adj3 (development* or cycle* or management or effect* or environment*)).ti,ab,kf. or (water adj3 (purificat* or sanitat* or treatment)).ti,ab,kf. or wastewater.ti,ab,kf. or (hydrogen adj3 moles adj3 equival*).ti,ab,kf. or "circular econom*".ti,ab,kf. or biodegradab*.ti,ab,kf. or ((ecological or environmental or water or energy or global or climat*) adj2 footprint*).ti,ab,kf. or (waste adj3 by product*).ti,ab,kf. or waste.ti,ab,kf. or wastes.ti,ab,kf. or reuse.ti,ab,kf. or reusab*.ti,ab,kf. or reprocess*.ti,ab,kf. or pollut*.ti,ab,kf. or (microplastic* and pollut*).ti,ab,kf. or greening.ti,ab,kf. or spillage.ti,ab,kf. or spoilage.ti,ab,kf. or salinization.ti,ab,kf. or "cradle to cradle".ti,ab,kf. or 'compostable plastic*'.ti,ab,kf. or desertification.ti,ab,kf. or deforestation.ti,ab,kf. or 'algal bloom*'.ti,ab,kf. or eco-friendly.ti,ab,kf. or ecofriendly.ti,ab,kf. or 'global change'.ti,ab,kf. or 'climate change'.ti,ab,kf. or "carbon neutral*".ti,ab,kf. or wastage*.ti,ab,kf. |
|
4 |
1 and 2 and 3 |
|
5 |
limit 4 to yr="2023 -Current" - Totaal |