Corticosteroïden
Uitgangsvraag
Wat is de plaats van corticosteroïd-injecties bij de behandeling bij patiënten met fasciopathie plantaris?
Aanbeveling
Wees terughoudend met lokale corticosteroïd injecties, deze zijn te overwegen indien eerdere conservatieve behandelingen en pijnstilling niet de gewenste uitkomst hebben.
Bespreek samen met de patiënt de volgende mogelijke effecten van een lokale corticosteroïd injectie:
- Mogelijk vermindert pijn op de korte termijn, het effect op functie is onbekend.
- Op de lange termijn is het effect onduidelijk voor zowel pijn als functie.
- De risico’s op ernstige complicaties lijken laag, maar hebben wel een negatieve impact indien deze ontstaan: ruptuur van de fascia plantaris, infectie en huid- en vet atrofie.
Pas corticosteroïd injecties enkel toe in combinatie met krachtoefeningen, en injecteer bij voorkeur echogeleid.
Wees terughoudend met het herhalen van corticosteroïd injectie bij ineffectiviteit na eerste injectie. Indien toch besloten wordt corticosteroïd injectie te herhalen, overweeg dit dan na ten minste 3 maanden te doen.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Op de lange termijn is het effect van een lokale corticosteroïd-injectie voor zowel pijn als functie onduidelijk, tussen de interventiegroep (corticosteroïden) en controlegroep zijn door de werkgroep geen klinisch relevante verschillen gevonden. Op de korte termijn kan een lokale corticosteroïd-injectie wel verlichting van pijn bieden (zie figuur 1.), maar is het onzeker of dit ook leidt tot verbetering van functie (David, 2017; Elizondo-Rodríguez, 2021; McMillan, 2012). Tegelijk is de bewijskracht hiervoor laag. Er is geen evidentie gevonden voor de bijdrage van een corticosteroïd injectie in vergelijking tot een placebo op return to sport en/of kwaliteit van leven.
Aanbeveling:
Mocht er gekozen worden voor een corticosteroïden injectie, adviseer dit dan in combinatie met krachtraining (Johannsen, 2019).
Bijwerkingen:
Bespreek altijd de mogelijke bijwerkingen met de patiënt. Mogelijke bijwerkingen zijn:
- lokale pijn op de injectie plek (Whittaker, 2019);
- beschadiging van collageenweefsel (Li, 2019);
- huid- vetkussen atrofie (Li, 2019);
- peesruptuur en infecties (McMillan, 2012).
Patiënten met diabetes mellitus kunnen ervaren dat de bloedglucosewaarden stijgt, dit kan van enkele dagen tot weken aanhouden. Diabetespatiënten die slecht ingesteld zijn dienen dit scherp in de gaten te houden.
Kwaliteit van bewijs
Uit de systematische search kwam één systematische review en drie RCT’s naar voren waar injecteren van corticosteroïden is vergeleken met placebo-injectie, bij patiënten met fasciopathie plantaris. Alle meegenomen studies beschrijven de cruciale uitkomstmaat pijn, de helft van de studies (Elizondo-Rodriguez, 2021; Abdihakin, 2012; McMillan, 2012) rapporteerden over de cruciale uitkomstmaat functie.
Er is geen klinisch relevant verschil gevonden in functie tussen het injecteren van corticosteroïden ten opzichte van placebo. Er lijkt wel een klinisch relevante verbetering te zijn op pijn bij het injecteren van corticosteroïden, ten opzichte van placebo. De kracht van het bewijs voor deze bevindingen is echter laag door een beperkt aantal studies met kleine patiëntaantallen (functie en pijn) en door inconsistente uitkomsten (functie) of studiebeperkingen (pijn). Hier is duidelijk nog nood aan het vergroten van bewijslast door meerdere, grotere studies en beter uitgevoerde studies.
Er konden geen conclusies worden getrokken over het effect van corticosteroïde injecties op bijwerkingen ten opzichte van placebo. Dit komt door het inconsistent rapporteren van bijwerkingen. Geen van de gevonden studies rapporteerde over de gedefinieerde belangrijke uitkomstmaten terugkeer naar sport en kwaliteit van leven. Er is dus duidelijk een kennislacune voor deze uitkomstmaten.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Bespreek met de patiënt dat de gewenste effecten op patiëntrelevante uitkomstmaten onzeker zijn. Op de korte termijn kan het zijn dat de patiënt na de injectie minder pijnklachten ervaart (David, 2017; Elizondo-Rodríguez, 2021). Er is in de literatuursamenvatting geen evidentie gevonden dat hiermee de functie ook verbetert. De ongewenste effecten op patiëntrelevante uitkomstmaten zijn onvoldoende gerapporteerd (Whittaker, 2019), maar kunnen een grote impact hebben vooral wanneer meerdere injecties gegeven worden (McMillan, 2012). Zie hiervoor de paragraaf Balans tussen gewenste en ongewenste effecten.
Kostenaspecten
Er zijn geen studies uitgevoerd naar hoe de (kosten)effectiviteit van corticosteroïde injecties zich verhoudt tot de controlebehandeling. De kosten, zowel direct als indirect, van de interventie zijn afhankelijk van de persoon die de interventie uitvoert (huisarts, medisch specialist, physician assistent of op basis van taak- delegatie/herschikking). Voor zover de werkgroep weet is het onbekend of de effectiviteit van de injectie afhangt van de kwalificaties of ervaring van de zorgverlener. Ook is het onbekend of er meer of ernstigere bijwerkingen optreden op basis van de kwalificaties of ervaring.
Gezondheidsgelijkheid
Er zijn bij de werkgroep geen studies bekend die gekeken hebben naar gezondheidsgelijkheid. De interventie is al standaardzorg in de praktijk en wordt uitgevoerd doormedisch specialisten en physician assistants. De werkgroep ziet daarom geen redenen om aan te nemen dat de interventie leidt tot een verandering van de gezondheidsgelijkheid.
Aanvaardbaarheid
De interventie lijkt wel aanvaardbaar voor de betrokkenen. De werkgroep voorziet geen ethische bezwaren. Wel is het van belang dat de gezondheidsvaardigheden en geletterdheid van de patiënt meegenomen worden.
Aangezien de effectiviteit van corticosteroïden injectie op de lange termijn op zowel pijn als functie beperkt is, moet worden overwogen of het ethisch verantwoord is om deze behandeling aan te bieden als er mogelijk nog veiligere alternatieven beschikbaar zijn.
Duurzaamheid
Bij de interventie spelen de volgende duurzaamheidsaspecten een rol: de impact van corticosteroïden-injectie heeft een beperkte impact op het milieu, maar op grotere schaal of bij herhaald gebruik kan dit oplopen. Het is belangrijk om hiermee rekening te houden om zo de impact op het milieu te beperken. Er kan worden overwogen om andere, minder milieubelastende alternatieven met vergelijkbare resultaten voor te schrijven. Denk aan oefentherapie, leefstijladvies maar bijvoorbeeld ook aan plaatjesrijk plasma wat als lichaamseigen stof makkelijker afbreekbaar is.
Haalbaarheid
De haalbaarheid van de beschreven interventie hangt af van verschillende factoren, waaronder beschikbaarheid en getraind personeel, infrastructuur zorginstelling, financiële dekking zorgverzekeraar. De interventie is over het algemeen al standaardzorg in de praktijk, die door huisartsen, medisch specialisten en physician assistants wordt uitgevoerd. Dit houdt dus in dat er voldoende kennis voorhanden is. De werkgroep acht bij terughoudendheid met corticosteroïden zoals aanbevolen in deze module geen capaciteitsproblemen.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Bij de behandeling van fasciopathie plantaris wordt eerst de voorkeur gegeven voor niet-invasieve conservatieve therapie (zie modules ‘Educatie’, ‘Oefentherapie’, ‘Op maat gemaakte zolen’ en ‘Shockwavetherapie’), en dienen dus alleen wanneer conservatieve therapie onvoldoende effect heeft gehad of wanneer de patiënt geen oefentherapie kan uitvoeren vanwege de ernst van de klacht. Dit advies is gebaseerd op de beschikbare evidentie waarin de voordelen vermoedelijk niet opwegen tegen de risico’s van corticosteroïden injecties (Lee, 2014; Morrissey, 2021; Mosca, 2022).
Eindoordeel
Op basis van bovenstaande overwegingen wordt een zwakke aanbeveling tegen het gebruik van corticosteroïd-injecties voor de behandeling van fasciopathie plantaris gegeven. Hoewel deze injecties op de korte termijn pijnverlichting kunnen geven dienen zij alleen als conservatieve therapie onvoldoende effect heeft gehad overwogen te worden of wanneer de patiënt geen oefentherapie kan uitvoeren vanwege de ernst van de klacht.
Onderbouwing
Corticosteroid injections have been used for a long time as a treatment for patients with plantar fasciopathy (Seth, 2023; Whittaker, 2019). Local corticosteroid injections are sometimes reported to be potentially harmful, but the literature does not provide clear evidence for this. However, repeated use of corticosteroid injections is reported to lead to side-effects such as post-injection pain (Whittaker, 2019), damage to collagen tissue (Li, 2019), skin atrophy (Li, 2019), tendon rupture and infection (McMillan, 2012). Partly due to these side effects, corticosteroid injections are under debate. Additionally, the effect of these injections in tendon-related conditions seems to last only 3 to 4 months but no longer (Johannsen, 2019). It is unknown if this effect is similar in plantar fasciopathy. This leads to variability in clinical practice. In this module, the working group evaluates the effectiveness of corticosteroid injections as a treatment for patients with plantar fasciopathy.
Summary of findings table
|
Outcome |
Term |
Study results and measurements |
Absolute effect estimates* |
Certainty |
Conclusions |
|
|
Corticosteroids |
placebo |
|||||
|
Function (crucial)
|
Short term (3 months) |
Function was measured with the maryland Foot Scale (MFS), foot function index (FFI) (0-100), foot function subscale of the Foot Health Status Questionnaire (0-100) and the AOFAS score |
Narrative summary, see result-paragraph |
Low Due to serious inconsistency and serious imprecision1 |
Corticosteroid injections may result in little to no difference in function when compared with placebo in patients with plantar fasciopathy.
Source: David (2017) (Abdihakin, 2012; McMillan, 2012) , Elizondo-Rodriguez (2021) |
|
|
Long term (6 months) |
||||||
|
Pain (crucial)
|
Short term (1 months) |
Pain was measured with the VAS scale (0-10 or 0-100) and foot pain subscale of the Foot Health Status Questionnaire (0-100) |
Mean difference was -13.61 [-32.66 to 5.44] favoring corticosteroid injection |
Low Due to serious risk of bias and serious imprecision2 |
Corticosteroid injections may result in a reduction of pain when compared with placebo in patients with plantar fasciopathy.
Source: David (2017), Elizondo-Rodriguez (2021), Digra (2023), Mahindra (2016) |
|
|
Long term (6 months) |
Pain was measured with the VAS scale (0-10 or 0-100) and foot pain subscale of the Foot Health Status Questionnaire (0-100) |
Mean difference was -17.40 [-37.29 to 2.50] favoring corticosteroid injection |
||||
|
Adverse events (crucial) |
|
- |
Narrative summary, see result-paragraph |
Very low GRADE Due to very serious risk of bias and serious imprecision3 |
The evidence is very uncertain about the effect of corticosteroid injections on adverse events compared to placebo in patients with plantar fasciopathy.
Source: David (2017), Elizondo-Rodriguez (2021) |
|
|
Return to sport (important) |
|
No studies |
-
|
No GRADE
|
No evidence was found regarding the effect of PRP injections on quality of life when compared with placebo in patients with plantar fasciopathy. |
|
|
Quality of life (important) |
|
No studies |
-
|
No GRADE
|
No evidence was found regarding the effect of PRP injections on return to sport when compared with placebo in patients with plantar fasciopathy. |
|
1. because of conflicting results (inconsistency -1) and a low number of included studies and participants (imprecision -1)
2. because of study limitations (risk of bias due to missing baseline characteristics -1) and the confidence interval crossing the border of clinical relevance (imprecision -1).
3. because of study limitations (high risk of reporting bias -2), and a low number of included studies and participants (imprecision -1).
Description of studies
David (2017) performed a systematic review on the effectiveness of corticosteroid injection in adult patients with plantar heel pain due to plantar fasciitis. They included RCTs with patients >16 years of age with plantar fasciitis. The comparison intervention was not specified before analysis, but they do perform a separate analysis on studies that use no intervention or a placebo intervention as a comparison. Primary outcomes reported were heel pain, function and serious adverse events. They also reported on return to activity or work and health-related quality of life. However, these outcome measures were not reported by the studies included in this review. They reported on these outcome measures in short (<1month), medium (1-6 months) and long term (>6 month) follow up.
For this module we excluded studies from David (2017) that did not use a placebo as control, and studies published before 2000 from our analysis. This resulted in 3 RCTs that could be considered for this review (Abdihakin, 2012; Ball, 2013 and McMillan, 2012).
Additionally, we extended the analysis of David (2017) with the 3 RCTs from our search that were published after the search date of David (2017) and that adhered to our PICO. Characteristics of these studies are summarized in Table 2.
All 3 additional RCTs contained 3 arms of which two were corticosteroid injection and a saline injection (placebo). The third arm consisted of autologous whole blood injection (Digra, 2023), Plasma injection (Elizondo-Rodriguez, 2021) or palpation guided steroid injection (Mahindra, 2016) using a peppering technique. respectively. Peppering technique is after insertion the needle is withdrawn and redirected and reinserted multiple times. We only took the arms with corticosteroid injection and with placebo in consideration for this review.
Studies were conducted in Australia (McMillan,2012), the United Kingdom (Ball,2013), Kenya (Abdihakim, 2012), India (Digra, 2023; Mahindra, 2016) and Mexico (Elizondo-Rodriguez, 2012). Follow-up period ranged from 2 months to 24 weeks. Mean age ranged from 34 (Mahindra, 2016) to 54 years (McMillan,2012). All studies reported on pain and four out of six reported on function (Elizondo-Rodriquez, 2012; Mahindra, 2016; Abdihakin, 2012 and McMillan, 2012). Adverse events were not reported in detail by any study. No studies reported on return to sport or quality of life.
Table 2. Characteristics of the included studies
|
Study (year) Study type |
Intervention (n) |
Characteristics |
Control (n) |
Characteristics |
Outcomes of interest reported |
FU |
ROB |
Considerations |
|
Abdihakin (2012) RCT from David(2017) |
Palpation-guided steroid injection and conservative management (47) |
Age: 41.0±9.6 %male: 49 VAS (0-10): 8.6±1.3 |
Saline injection and conservative management (41) |
Age: 45.1±8.2 %male: 46 VAS (0-10): 8.74±1.5 |
Pain (VAS ) Function; foot-function index |
2 months |
High risk of reporting bias – no adverse events reported |
|
|
Ball (2013) RCT from David(2017) |
Ultrasound guided steroid injection (22) |
Age: 49.0±12.9 % male: 45 VAS (0-100): 62.0±19.2 |
Ultrasound guided placebo injection (22) |
Age: 50.1±10.6 %male: 52 VAS (0-100): 56.0(27.9) |
Pain (VAS) Adverse events
|
|
High risk of incomplete outcome data reporting, high risk of selective reporting bias. |
Frequent loss to follow up/ dropouts |
|
McMillan (2012) RCT from David(2017) |
Intrafascial steroid injection - (41) |
Age: 51.7±11.9 % male: 46 FHS – pain: 36.8±19.9 FHS- function 53.4±25.5 |
Intrafascial injection – saline (41) |
Age: 53.6±9.0 % male: 58 FHS – pain: 35.9±20.4 FHS- function 60.2±25.3 |
Pain (foot health status questionnaire), function(foot health status questionnaire, Adverse events, first step pain |
12 weeks |
Low risk of bias |
12 pt. In each arm had a bilateral injection which was treated as one injection. |
|
Digra (2023) RCT (group B and C) |
Palpation guided injection with methylprednisolone acetate at 0 and 2 weeks (20) |
Mean age: 45.0 (SD not reported) |
Palpation guided Injection with saline at 0 and 2 weeks (20) |
Mean age: 42.2 (SD not reported) |
Pain (VAS) |
12 weeks |
High |
Very little description of group demographics. No adverse events, no clear blinding procedure |
|
Mahindra (2016) RCT (group B and C) |
Steroid injection (methylprednisolone) peppering technique (30)
physical therapy (stretching) |
Age: 33.9±8.6 % male: 48 VAS: 7.7 |
Saline injection (30)
physical therapy (stretching) |
Age: 35.5±9.5 % male: 44 VAS: 7.6 |
Pain (VAS) Foot and Ankle Society Function: (AOFAS) |
3 months |
Some concerns (adverse events) |
No information on adverse events |
|
Elizondo-Rodriguez (2021) |
Steroid injection (25) |
Age: 46.4±11.0 %male: 24 VAS (0-10): 7.7±1.9 MFS: 83.9±13.4 |
Anesthetic injection (23) |
Age: 49.3±10.6 %male: 24 VAS (0-10): 7.9±1.2 MFS: 84.6±12.1 |
Pain (VAS) Function (MFS) Side effects |
24 weeks |
Low risk |
|
|
Abbreviations: AOFAS: Ankle and Hindfoot score, MFS: Maryland Foot Score, SD: standard deviation, VAS: visual analogue scale for pain |
||||||||
Results
1. Function (crucial)
Elizondo-Rodriguez (2021) reported on function with the Maryland Foot Scale (MFS) with a maximum of 100 points based on pain and function criteria. The higher the score the better the function. A score above 90 represents an excellent outcome. They report a mean MFS (SD) at 4 weeks post intervention of 94.3 (1.30) in the intervention group compared to 90.3 in the placebo group resulting in a difference (95%CI) of 4.0 (2.60 to 5.40) points in favor of the steroid group. However, at 24 weeks post intervention they report an MFS(SD) of 96.1 (1.78) in the group receiving steroid injection compared to 99.4 in the placebo group resulting in a difference (95%CI) of -3.3 (-4.35 to -2.25) points in favor of the placebo group. Both differences are not clinically relevant.
Abdihakin (2012) reported on function with the foot function index (FFI) (0-100). The lower the score the better the function. They report a FFI (SD) at 2 months post-intervention of 42.3 (17.2) in the group receiving the steroid injection compared to 40.5(13.3) in the placebo group resulting in a mean difference (95%CI) of 1.8(-4.83 to 8.39) in favor of the placebo group. This difference is not clinically relevant.
McMillan (2012) reported the foot function subscale of the Foot Health Status Questionnaire (0-100) in which a higher score represents better function. They report a difference (95%CI) at 12 weeks post-intervention of 4.1(-3.8 to 11.9) points in favor of the steroid group. This difference is not clinically relevant.
Although Mahindra (2016) reports on function with the AOFAS score, they do not provide scores for the placebo group, therefore we could not take them into account for this analysis.
2. Pain (crucial)
All studies reported on pain. They all defined pain with the VAS scale (0-10 or 0-100; higher score represents more pain), except for McMillan (2012) who reported the foot pain subscale of the Foot Health Status Questionnaire (0-100) in which a higher score represents less pain. To pool results the VAS 0-10 was multiplied by 10 and the FHSQ score was multiplied by -1. Pooled results show that both in the short term <1 month and in the medium term 1 <6 months, participants experience less pain in the steroid group (Figure 1). Mean difference was -13.61 [-32.66 to 5.44] and -17.40 [-37.29 to 2.50] respectively in favor of the steroid group. This difference is clinically relevant (>10%). No data are available for a follow-up after 6 months.
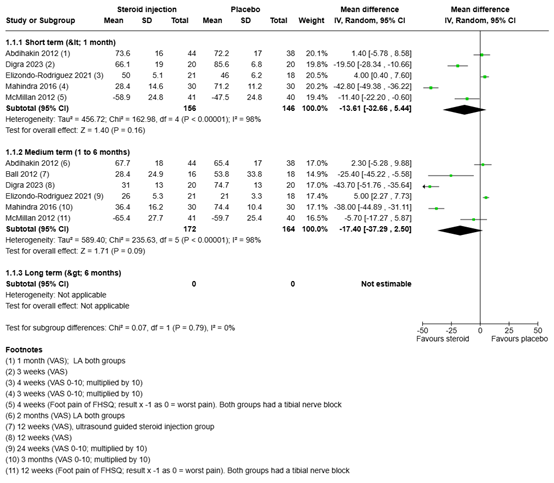
Figure 1
Pooled results of the pain scores
3. Adverse events (important)
None of the studies report on any (serious) adverse events. Elizondo (2021), Ball (2013) and McMillan (2012) explicitly state this. The other studies do not report on adverse events.
Ball (2013) also reported on repeat ultrasound injection. After the intervention participants were offered a repeat injection if treatment failed. One patient (5%) in the corticosteroid group needed a repeat injection at 12 weeks compared to 11 (52%) patients in the placebo group. An important note is that six patients in the steroid group were lost to follow-up at 12 weeks, with two of them withdrawing due to heel pain. This might have led to a more favorable result for the intervention than what actually occurred.
4. Return to sport (important)
No studies reported on the effect of steroid injections on return to sport in patients with plantar fasciopathy.
5.Quality of Life (important)
No studies reported on the effect of steroid injections on quality of life in patients with plantar fasciopathy.
A systematic review of the literature was performed to answer the following question:
What is de efficacy of corticosteroid-injections in patients with plantar fasciopathy compared to placebo?
Table 1. PICO
| Patients | Patients with plantar fasciopathy |
| Intervention | Corticosteroid-injection |
| Control | Placebo or placebo as add-on to physical therapy |
| Outcomes | Function, pain, adverse events, return to sport and quality of life |
| Other selection criteria | Study design: systematic reviews, meta-analyses and randomized controlled trials |
Relevant outcome measures
The guideline development group considered function, pain and adverse events as a crucial outcome measure for decision making; and return to sport and quality of life as an important outcome measure for decision making.
A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies. Important adverse events are infection, rupture, atrophy and pain.
The working group defined a 10% difference for both continuous outcome measures and
dichotomous outcome measures informing on relative risk (RR ≤ 0.91 and ≥ 1.1).
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until March 28th, 2024. The detailed search strategy is available upon request. The systematic literature search resulted in 238 hits.
Studies were selected based on the following criteria:
- randomized controlled trials (RCTs), systematic review and/or meta-analysis;
- studies on patients with plantar fasciopathy;
- described corticosteroid injection as intervention;
- described placebo or placebo as add-on to physical therapy as control;
- described at least one of the critical outcome measures as described in the PICO;
- minimum of 10 patients per arm.
In case of a systematic review:
- minimum of two databases searched;
- detailed search strategy with search date;
- in- and exclusion criteria;
- exclusion table;
- evidence table for included studies;
- risk of bias assessment per study.
33 studies were initially selected based on title and abstract screening. After reading the full text, 29 studies were excluded (see the table with reasons for exclusion under the tab Methods), and 4 studies were included.
Results
Four studies were included in the analysis of the literature. The assessment of the risk of bias is summarized in the risk of bias tables.
- David, J. A., Sankarapandian, V., Christopher, P. R. H., Chatterjee, A., & Macaden, A. S. (2017). Injected corticosteroids for treating plantar heel pain in adults. Cochrane Database of Systematic Reviews, 2017(6). https://doi.org/10.1002/14651858.CD009348.pub2.
- Digra N, Beri A, Sharma S, Verma R. Autologous Whole-Blood Versus Corticosteroid Local Injection in Treatment of Plantar Fasciitis: A Randomized Single Blind Placebo-Controlled Study. Cureus. 2023 Sep 20;15(9):e45588. doi: 10.7759/cureus.45588. PMID: 37868394; PMCID: PMC10587858.
- Elizondo-Rodríguez, J., Simental-Mendía, M., Peña-Martínez, V., Vilchez-Cavazos, F., Tamez-Mata, Y., & Acosta-Olivo, C. (2021). Comparison of Botulinum Toxin A, Corticosteroid, and Anesthetic Injection for Plantar Fasciitis. Foot and Ankle International, 42(3), 305–313. https://doi.org/10.1177/1071100720961093.
- Johannsen, F. E., Herzog, R. B., Malmgaard-Clausen, N. M., Hoegberget-Kalisz, M., Magnusson, S. P., & Kjaer, M. (2019). Corticosteroid injection is the best treatment in plantar fasciitis if combined with controlled training. Knee Surgery, Sports Traumatology, Arthroscopy, 27(1), 5–12. https://doi.org/10.1007/s00167-018-5234-6.
- Lee, H. S., Choi, Y. R., Kim, S. W., Lee, J. Y., Seo, J. H., & Jeong, J. J. (2014). Risk factors affecting chronic rupture of the plantar fascia. Foot and Ankle International, 35(3), 258–263. https://doi.org/10.1177/1071100713514564.
- Mahindra, P., Yamin, M., Selhi, H. S., Singla, S., & Soni, A. (2016). Chronic plantar fasciitis: Effect of platelet- rich plasma, corticosteroid, and placebo. Orthopedics, 39(2), e285–e289. https://doi.org/10.3928/01477447-20160222-01.
- McMillan, A. M., Landorf, K. B., Gilheany, M. F., Bird, A. R., Morrow, A. D., & Menz, H. B. (2012). Ultrasound guided corticosteroid injection for plantar fasciitis: Randomised controlled trial. BMJ (Online), 344(7859), 1–12. https://doi.org/10.1136/bmj.e3260.
- Morrissey, D., Cotchett, M., Said J’bari, A., Prior, T., Griffiths, I. B., Rathleff, M. S., Gulle, H., Vicenzino, B., & Barton, C. J. (2021). Management of plantar heel pain: A best practice guide informed by a systematic review, expert clinical reasoning and patient values. British Journal of Sports Medicine, 55(19), 1106–1118. https://doi.org/10.1136/bjsports-2019-101970.
- Mosca, M., Fuiano, M., Massimi, S., Censoni, D., Catanese, G., Grassi, A., Caravelli, S., & Zaffagnini, S. (2022). Ruptures of the Plantar Fascia: A Systematic Review of the Literature. Foot and Ankle Specialist, 15(3), 272–282. https://doi.org/10.1177/1938640020974889.
- Sconfienza, L. M., Adriaensen, M., Albano, D., Alcala-Galiano, A., Allen, G., Aparisi Gómez, M. P., Aringhieri, G., Bazzocchi, A., Beggs, I., Chianca, V., Corazza, A., Dalili, D., De Dea, M., del Cura, J. L., Di Pietto, F., Drakonaki, E., Facal de Castro, F., Filippiadis, D., Gitto, S., … Obradov, M. (2021). Clinical indications for image-guided interventional procedures in the musculoskeletal system: a Delphi-based consensus paper from the European Society of Musculoskeletal Radiology (ESSR)—part VI, foot and ankle. European Radiology. https://doi.org/10.1007/s00330-021-08125-z.
- Whittaker, G. A., Munteanu, S. E., Menz, H. B., Bonanno, D. R., Gerrard, J. M., & Landorf, K. B. (2019). Corticosteroid injection for plantar heel pain: A systematic review and meta-analysis. BMC Musculoskeletal Disorders, 20(1). https://doi.org/10.1186/s12891-019-2749-z.
Risk of bias table for intervention studies (randomized controlled trials; based on Cochrane risk of bias tool and suggestions by the CLARITY Group at McMaster University)
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
|
Was the allocation adequately concealed?
|
Blinding: Was knowledge of the allocated interventions adequately prevented? |Were all involved blinded? |
Was loss to follow-up (missing outcome data) infrequent?
|
Are reports of the study free of selective outcome reporting? |
Was the study apparently free of other problems that could put it at a risk of bias?
|
Overall risk of bias If applicable/necessary, per outcome measure
LOW/Some concerns/ HIGH
|
|
Digra, 2023 |
Probably no
Reason: “patients were divided into three groups by simple randomization” No further clarification |
No information
Reason: no description of allocation |
No information
Reason: no description of blinding |
No information
Reason: no mention of loss to follow up |
Probably no
Reason: All outcomes in the methods are reported. However these are minimal and no baseline characteristics are reported. |
Probably no:
Reason: no baseline characteristics reported for main outcome measures. No adverse events reported. |
HIGH (all outcome measures)
Reason: Unclear blinding procedure, missing baseline characteristics, missing demographics. |
|
Mahindra, 2016 |
Definitely yes
Reason: Central randomization with computer programming |
No information
Reason: no description of allocation |
Probably yes
Reason: Patients were blinded, outcome assessor was blinded. (blinding of analysts not reported) |
No information
Reason: no mention of loss to follow up |
Probably yes
Reason: No protocol available. Alle measures in introduction are reported. |
Probably no:
Reason: No information on adverse events reported. |
Some concerns
Reason: No information on adverse events. Missing information om some points regarding risk of bias |
|
Elizondo-Rodriguez, 2021 |
Definitely yes
Reason: Central randomization with computer programming |
No information
Reason: no description of allocation |
Probably yes
Reason: patients were blinded. Data collectors/outcome assessors were blinded. (blinding of analysts not reported) |
Probably yes
Missing data was infrequent and multiple imputation was used to hand missing data. Sensitivity analysis was performed with ITT analysis. |
Probably yes
Reason: No protocol available. Alle measures in introduction are reported. |
Probably yes
Reason: no other problems noted |
Low ; |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Al-Boloushi Z, López-Royo MP, Arian M, Gómez-Trullén EM, Herrero P. Minimally invasive non-surgical management of plantar fasciitis: A systematic review. J Bodyw Mov Ther. 2019 Jan;23(1):122-137. doi: 10.1016/j.jbmt.2018.05.002. Epub 2018 Jun 1. PMID: 30691739. |
Systematic review of insufficient quality |
|
Ang TW. The effectiveness of corticosteroid injection in the treatment of plantar fasciitis. Singapore Med J. 2015 Aug;56(8):423-32. doi: 10.11622/smedj.2015118. PMID: 26311907; PMCID: PMC4545130. |
Systematic review including only 2 relevant RCTs that are already in literature search. |
|
Arnold MJ, Gruber J. Injected Corticosteroids for Plantar Heel Pain. Am Fam Physician. 2018 Feb 1;97(3):169-170. PMID: 29431981. |
Wrong article type: clinical summary |
|
Assad S, Ahmad A, Kiani I, Ghani U, Wadhera V, Tom TN. Novel and Conservative Approaches Towards Effective Management of Plantar Fasciitis. Cureus. 2016 Dec 5;8(12):e913. doi: 10.7759/cureus.913. PMID: 28083457; PMCID: PMC5215813. |
Systematic review of insufficient quality |
|
Babatunde OO, Legha A, Littlewood C, Chesterton LS, Thomas MJ, Menz HB, van der Windt D, Roddy E. Comparative effectiveness of treatment options for plantar heel pain: a systematic review with network meta-analysis. Br J Sports Med. 2019 Feb;53(3):182-194. doi: 10.1136/bjsports-2017-098998. Epub 2018 Jun 28. PMID: 29954828. |
SYstematic review with fewer relevant outcome measures compared to David(2017) |
|
Ball EM, McKeeman HM, Patterson C, Burns J, Yau WH, Moore OA, Benson C, Foo J, Wright GD, Taggart AJ. Steroid injection for inferior heel pain: a randomised controlled trial. Ann Rheum Dis. 2013 Jun;72(6):996-1002. doi: 10.1136/annrheumdis-2012-201508. Epub 2012 Jun 27. PMID: 22739993. |
In David(2017) |
|
Celik D, Kuş G, Sırma SÖ. Joint Mobilization and Stretching Exercise vs Steroid Injection in the Treatment of Plantar Fasciitis: A Randomized Controlled Study. Foot Ankle Int. 2016 Feb;37(2):150-6. doi: 10.1177/1071100715607619. Epub 2015 Sep 23. PMID: 26400901. |
Wrong comparison: no placebo but stretching exercise.
|
|
Chen CM, Lee M, Lin CH, Chang CH, Lin CH. Comparative efficacy of corticosteroid injection and non-invasive treatments for plantar fasciitis: a systematic review and meta-analysis. Sci Rep. 2018 Mar 5;8(1):4033. doi: 10.1038/s41598-018-22402-w. PMID: 29507320; PMCID: PMC5838257. |
Does not include comparison to placebo |
|
Crawford F, Atkins D, Edwards J. Interventions for treating plantar heel pain. The Foot. 2001 Dec; 11(4);228-250. doi; /10.1054/foot.2002.0689. |
Wrong article type: citation |
|
Crawford F. Plantar heel pain (including plantar fasciitis). Clin Evid. 2002 Dec;(8):1238-49. Update in: Clin Evid. 2003 Dec;(10):1431-43. PMID: 12603938. |
Review with articles untill 1997 |
|
Crawford F, Thomson C. Interventions for treating plantar heel pain. Cochrane Database Syst Rev. 2003;(3):CD000416. doi: 10.1002/14651858.CD000416. |
Cochrane review untill 2002, no pooled data, focusses on different types of treatment |
|
Dev K, Meena AS, Meena M, Joshi M.A Randomized Control Study of Comparison of Standard Care versusUltrasonography Guided Single Dose of MethylprednisoloneAcetate Injection for Planar Fasciopathy. European Journal of Molecular and Clinical Medicine. 2022; 9(3). |
Wrong comparison: not placebo but physical therapy
|
|
Gao R, Sun J, Zhang L, Chen S, Dong W, Yu H, Han B, Tan M, Li X. Comparative Effectiveness of Minimally Invasive Nonsurgical Treatments for Plantar Fasciitis: A Network Meta-analysis of 30 Randomized Controlled Trials. Pain Physician. 2021 Nov;24(7):E955-E971. PMID: 34704707. |
tematic review of insufficient quality |
|
Hsiao MY, Hung CY, Chang KV, Chien KL, Tu YK, Wang TG. Comparative effectiveness of autologous blood-derived products, shock-wave therapy and corticosteroids for treatment of plantar fasciitis: a network meta-analysis. Rheumatology (Oxford). 2015 Sep;54(9):1735-43. doi: 10.1093/rheumatology/kev010. Epub 2015 Apr 6. PMID: 25848072. |
Does not include comparison to placebo |
|
Karimzadeh A, Raeissadat SA, Erfani Fam S, Sedighipour L, Babaei-Ghazani A. Autologous whole blood versus corticosteroid local injection in treatment of plantar fasciitis: A randomized, controlled multicenter clinical trial. Clin Rheumatol. 2017 Mar;36(3):661-669. doi: 10.1007/s10067-016-3484-6. Epub 2016 Dec 12. PMID: 27957618. |
Does not include comparison to placebo |
|
Kuldeep, S. and Gaur, R. and Jindal, R. Comparison of The Efficacy of Different Treatment Modalities in Use for Plantar Fasciitis: A Randomized Controlled Trial International Journal of Pharmaceutical and Clinical Research |
Full-text not available |
|
Kumar, V. A. and Khalid, K. M. and Vajrangi, A. and Sherikar, N. and Srinivas, R. and Rakshith, C. H. Y. and Kurupati, R. B. and Rajanna, P.A Comparative Study Between Platelet-Rich Plasma And Corticosteroid Injection For Plantar Fasciitis. 2024 |
Full-text not available |
|
Li H, Lv H, Lin T. Comparison of efficacy of eight treatments for plantar fasciitis: A network meta-analysis. J Cell Physiol. 2018 Jan;234(1):860-870. doi: 10.1002/jcp.26907. Epub 2018 Aug 4. PMID: 30078188. |
systematic review of insufficient quality |
|
Li Z, Yu A, Qi B, Zhao Y, Wang W, Li P, Ding J. Corticosteroid versus placebo injection for plantar fasciitis: A meta-analysis of randomized controlled trials. Exp Ther Med. 2015 Jun;9(6):2263-2268. doi: 10.3892/etm.2015.2384. Epub 2015 Mar 24. PMID: 26136971; PMCID: PMC4473350. |
All relevant studies in cluded in David(2017) |
|
McMillan AM, Landorf KB, Gilheany MF, Bird AR, Morrow AD, Menz HB. Ultrasound guided corticosteroid injection for plantar fasciitis: randomised controlled trial. BMJ. 2012 May 22;344:e3260. doi: 10.1136/bmj.e3260. PMID: 22619193. |
In David (2017) |
|
Orhan Ö, Ağır H, Sarıkaya B, Dolap MA, Altay MA. Pain relief and functional improvement provided by extracorporeal shock wave therapy in plantar fasciitis is better than corticosteroid injection and kinesio taping: A randomized trial. Turkish Journal of Physical Medicine and Rehabilitation. 2023 |
Does not include comparison to placebo |
|
Peña-Martínez VM, Acosta-Olivo C, Simental-Mendía LE, Sánchez-García A, Jamialahmadi T, Sahebkar A, Vilchez-Cavazos F, Simental-Mendía M. Effect of corticosteroids over plantar fascia thickness in plantar fasciitis: a systematic review and meta-analysis. Phys Sportsmed. 2023 Jun 13:1-12. doi: 10.1080/00913847.2023.2223673. Epub ahead of print. PMID: 37293970. |
Primary aim is to study plantar fascia thickness, secondary pain. Not only placebo as control
|
|
Riel H, Vicenzino B, Olesen JL, Bach Jensen M, Ehlers LH, Rathleff MS. Does a corticosteroid injection plus exercise or exercise alone add to the effect of patient advice and a heel cup for patients with plantar fasciopathy? A randomised clinical trial. Br J Sports Med. 2023 Sep;57(18):1180-1186. doi: 10.1136/bjsports-2023-106948. Epub 2023 Jul 6. PMID: 37414460; PMCID: PMC10579183. |
Does not include comparison to placebo |
|
Ryan M, Hartwell J, Fraser S, Newsham-West R, Taunton J. Comparison of a physiotherapy program versus dexamethasone injections for plantar fasciopathy in prolonged standing workers: a randomized clinical trial. Clin J Sport Med. 2014 May;24(3):211-7. doi: 10.1097/JSM.0000000000000021. PMID: 24172656. |
Does not include comparison to placebo |
|
Seth I, Bulloch G, Seth N, Lower K, Rodwell A, Rastogi A, Gibson D, Bedi H. The role of corticosteroid injections in treating plantar fasciitis: A systematic review and meta-analysis. Foot (Edinb). 2023 Mar;54:101970. doi: 10.1016/j.foot.2023.101970. Epub 2023 Feb 3. PMID: 36774828. |
No comparison to placebo but to other treatments
|
|
Shetty SH, Dhond A, Arora M, Deore S. Platelet-Rich Plasma Has Better Long-Term Results Than Corticosteroids or Placebo for Chronic Plantar Fasciitis: Randomized Control Trial. J Foot Ankle Surg. 2019 Jan;58(1):42-46. doi: 10.1053/j.jfas.2018.07.006. Epub 2018 Nov 15. PMID: 30448183. |
Incomplete reports on outcome data |
|
Tsikopoulos K, Vasiliadis HS, Mavridis D. Injection therapies for plantar fasciopathy ('plantar fasciitis'): a systematic review and network meta-analysis of 22 randomised controlled trials. Br J Sports Med. 2016 Nov;50(22):1367-1375. doi: 10.1136/bjsports-2015-095437. Epub 2016 May 3. PMID: 27143138. |
Less recent than David (2017), similar objective
|
|
Whittaker GA, Landorf KB, Munteanu SE, Menz HB. Predictors of response to foot orthoses and corticosteroid injection for plantar heel pain. J Foot Ankle Res. 2020 Sep 29;13(1):60. doi: 10.1186/s13047-020-00428-6. PMID: 32993721; PMCID: PMC7526364. |
Wrong study type: predictor study
|
|
Whittaker GA, Munteanu SE, Menz HB, Bonanno DR, Gerrard JM, Landorf KB. Corticosteroid injection for plantar heel pain: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2019 Aug 17;20(1):378. doi: 10.1186/s12891-019-2749-z. PMID: 31421688; PMCID: PMC6698340. |
Fewer relevant outcome measures reported compared to David (2017) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 17-02-2026
Beoordeeld op geldigheid : 17-02-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire werkgroep samengesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met fasciopathie plantaris.
Werkgroep
- Dhr. prof. dr. Fred Hartgens (voorzitter), sportarts, namens de Vereniging voor Sportgeneeskunde (VSG)
- Dhr. dr. Bernard te Boekhorst, sportarts, namens de VSG
- Dhr. drs. Daan Gelsing, extended scope specialist, echografist en manueel therapeut, namens de Nederlandse Vereniging voor Manuele Therapie en het Koninklijk Nederlands Genootschap voor Fysiotherapie (NVMT/KNGF)
- Dhr. drs. David Hanff, radioloog, namens de Nederlandse Vereniging voor Radiologie (NVvR)
- Dhr. dr. Eric Bakker, fysiotherapeut en klinisch epidemioloog, namens het Koninklijk Nederlands Genootschap voor Fysiotherapie (KNGF)
- Mevr. drs. Eva Hoefnagels, orthopedisch chirurg, namens de Nederlandse Orthopaedische Vereniging (NOV)
- Mevr. drs. Inge Koetser, radioloog, namens de NVvR
- Mevr. drs. Kayleigh van Amelsfort, podotherapeut en gezondheidswetenschapper, namens de Nederlandse Vereniging voor Podotherapeuten (NVvP)
- Dhr. drs. Niek Vink, fysiotherapeut en fysiotherapiewetenschapper, namens de KNGF
- Dhr. dr. Robert-Jan de Vos, sportarts, namens de VSG
- Dhr. drs. Thomas Eggen, orthopedisch chirurg, namens de NOV
Klankbordgroep
- Dhr. dr. Dorus Fennis, neuroloog, namens de Nederlandse Vereniging voor Neurologie (NVN)
- Dhr. dr. Florus van der Giesen, physician assistant reumatologie, namens de Nederlandse Vereniging voor Reumatologie (NVR)
- Mevr. drs. Juliette Starmans, AIOS bedrijfsgeneeskunde en orthopedisch chirurg, namens de Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (NVAB)
- Mevr. drs. Lisette de Graauw, register podoloog, namens Stichting LOOP
Met ondersteuning van
- Mevr. drs. Beatrix Vogelaar, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. drs. Isabelle Laseur, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel Gemelde (neven)functies en belangen werkgroep
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Fred Hartgens (voorzitter) |
Hoofd Afdeling Sportgeneeskunde en Hoogleraar Klinische Sportgeneeskunde in UMC Utrecht (0,8 fte) |
Op free lance basis praktiserend sportarts in Zuid-Limburg en sportarts-docent voor andere organisaties (in totaal 10-15 uur per maand) VSG vertegenwoordiger bij FMS Raad Wetenschap & Innovatie Lid van Werkgroep Herziening Kennisagenda VSG VSG vertegenwoordiger in SKMS Beweeg Alliantie |
UTC lmaging B.V: The effects of tendinopathy and reliability of hamstrings Ultrasiund Tissue Characterisation (UTC) echo types - geen projectleidersrol BioActor B.V. : The Effect of a Citrus and Pomegranate Complex on Physical Fitness and Mental Well-Being in Healthy Elde a Randomized Placebo controlled Trial - geen projectleidersrol
Allebei afgerond |
Geen restricties |
|
Bernard te Boekhorst |
SMA sportarts middennederland |
- |
- |
Geen restricties |
|
Daan Gelsing |
Echo On The Spot - eigenaar, MSK-echografist Rembrandt fysiotherapie - echografist en manueel therapeut Echo On The Spot - het uitvoeren van echografisch diagnostisch onderzoek in de eerstelijns zorg. Rembrandt fysiotherapie - fysiotherapeutische zorg. |
Geven van mini-klinieken en examinator aan de SOMT University |
|
Geen restricties |
|
Eric Bakker |
Epidemioloog(B) master EBPiHC, Amsterdam UMC locatie AMC, Amsterdam 0,3 FtE. Onderwijs en begeleidingen onderzoek van de studenten epidemiologie. Betaald
|
Eigenaar wetenschappelijk adviesbureau KOKD.nl. Betaald. Niet over onderwerpen in de richtlijn |
|
Geen restricties |
|
Eva Hoefnagels
|
Sint maartenskliniek orthopedisch chirurg betaald |
Voorzitter nederlandse voet en enkel vereniging (onbetaald) |
Promotie onderzoek fasciitis plantaris, onderzoek is afgerond en data al verwerkt, dit onderzoek heeft geen invloed op de data Bestuur Nederlandse voet en enkelvereniging. Uitkomst onderzoek heeft geen invloed op mijn functie daar. Promotieonderzoek lopend, geen financier. Publicaties sinds 2019: - PAPPI: Personalized analysis of plantar pressure images using statistical modelling and parametric mapping - The effect of lengthening the gastrocnemius muscle in chronic therapy resistant plantar fasciitis
Promotie onderzoek over operatieve behandeling bij chronische fasciitis plantaris. Is al begonnen in 2017 en data zijn al verzameld tot 2020. Voor de start van deze richtlijn. De data van mijn onderzoek is niet van invloed voor de richtlijn en de uitkomst van de richtlijn niet voor het onderzoek. Mijn onderzoeks data zijn niet gebruikt voor de richtlijn. |
Geen restricties |
|
Inge Koetser
|
Radioloog, Reade |
GAIA commissie
|
- |
Geen restricties |
|
Kayleigh van Amelsfort
|
Podotherapeut, Podotherapie Inka (betaald, 20 uur) |
Bestuurslid Wetenschap & Vakinhoud, Nederlandse Vereniging van Podotherapeuten (betaald, 10 uur) |
- |
Geen restricties |
|
Niek Vink |
Manager en docent Nationaal Trainingscentrum voor echografie (NT-e) |
Manager van het opleidingscentrum NT-e. Hier worden post-HBO opleidingen gegeven in echografie, shockwave therapie en percutane electrolyse (ook bij plantaire hielpijnklachten). Ik geef een dag in de week les binnen de opleidingen voor echografie. Het NT-e is onderdeel van Fyzzio International BV. Fyzzio verkoopt apparatuur voor bovenvermelde activiteiten. Ik ben bij het NT-e in loondienst, heb geen aandelen in het bedrijf en krijg ook geen bonussen. Ik heb geen financiële belangen bij een bepaalde uitkomst van de richtlijn. |
- |
Geen restricties |
|
Robert-Jan de Vos |
Sportarts en Universitair Hoofddocent, Erasmus MC Universitair Medisch Centrum Rotterdam (0.8 fte) |
Consulent SBV Excelsior Rotterdam (onbetaald). Associate editor British Journal of Sports Medicine (onbetaald). Voorzitter multidisciplinaire richtlijn achilles tendinopathie (onbetaald). Werkgroeplid multidisciplinaire richtlijn achillespeesruptuur (onbetaald). Werkgroeplid Kennisagenda VSG 2023 (onbetaald). Werkgroeplid SKMS richtlijnen commissie (betaald). |
In de afgelopen 5 jaar zijn er onderzoeksprojecten uitgevoerd onder mijn supervisie die zijn gefinancierd door ReumaNederland, Annafonds, ZonMw, GE Healthcare, de National Basketball Association (NBA), het Trustfonds en de Erasmus MC Foundation. Deze financiers hebben echter geen belangen bij de aanbevelingen die zullen worden gedaan in deze richtlijn. Ik heb een consultancy functie voor een project naar nieuwe injectie behandeling voor Achilles tendinopathie, gesponsord door Novartis (2021), dit raakt niet aan het onderwerp van de richtlijn. Tevens is deze injectie behandeling nog niet ontwikkeld voor de huidige klinische zorg en daardoor zal deze ook niet in de richtlijn kunnen worden behandeld. Daarnaast is de consultancy functie eenmalig geweest en niet meer actief, en inkomsten zijn voor de instelling waarin ik werk en niet voor persoonlijke doeleinden). Op dit moment is er geen commercieel gefinancieerd onderzoek dat loopt onder mijn leiding. Ik ben aan het oriënteren met Causeway Therapeutics of we een onderzoek gaan opstarten met een nieuwe injectable voor epicondylaire tendinopthie, maar ook daarvoor geldt dat het niet direct zal zijn gerelateerd aan fasciopathie plantaris. Het is niet mijn verwachting dat dit leidt tot belangenverstrengeling.
In de afgelopen 5 jaar zijn er onderzoeksprojecten uitgevoerd onder mijn supervisie die zijn gefinancierd door HORIZON MSCA, ReumaNederland, Annafonds, ZonMw, GE Healthcare, de National Basketball Association (NBA), het Trustfonds en de Erasmus MC Foundation. Deze financiers hebben echter geen belangen bij de aanbevelingen die worden gedaan in deze richtlijn. Ik heb een consultancy functie gehad voor een project naar nieuwe injectie behandeling voor Achilles tendinopathie (Novartis, 2021) en laterale epicondylaire tendinopathie (Causeway therapeutics. 2025). Dit raakt niet aan het onderwerp van de richtlijn. Tevens zijn deze injectie behandelingen nog niet ontwikkeld voor de huidige klinische zorg en daardoor worden deze behandelingen ook niet in de richtlijn behandeld. Daarnaast zijn deze consultancy functies eenmalig geweest en niet meer actief, en inkomsten zijn voor de instelling waarin ik werk en niet voor persoonlijke doeleinden).
Op dit moment is er geen commercieel gefinancierd onderzoek dat loopt onder mijn leiding. HORIZON MSCA Postdoctoral Fellowship – Identifying Predictive factors for the Recovery of Achilles Tendinopathy (PReAcT trial) NWO / ReumaNederland – The State of the Cartilage (START project) ReumaNederland / Annafonds – High-Volume injectie Achilles tendinopathie (HAT trial) ZonMW – Preventie hardloopblessures (INSPIRE trial en SPRINT trial) GE Healthcare / NBA – Oefentherapie Patella tendinopathie (JUMPER trial) Trustfonds / Erasmus MC Foundation – Normwaarden echografie achillespezen (REVEAL trial) Causeway therapeutics – Consultancy voor trial nieuwe injectable laterale epicondylaire tendinopathie Novartis – Consultancy voor trial nieuwe injectable achilles tendinopathie |
Geen restricties |
|
Thomas Eggen |
Orthopedisch chirurg Canisius Wilhelmina Ziekenhuis |
Dagvoorzitter NOV en LVO congressen Orthopedisch consultant op KNMG carriere beurs Mede-oprichter BotCast orthopedische podcast (educatief/informatief). Mogelijke tegemoetkoming vanuit Orlymedia BV (sponsor kan farmaceut zijn). |
- |
Geen restricties |
|
David Hanff |
Voorzitter van de MSK sectie Nederlandse Vereniging voor Radiologie |
Nederlandse Vereniging voor Radiologie |
- |
Geen restricties |
|
Dorus Fennis (klankbordgroep) |
Geen werkgever maar vrijgevestigd meidsch specialist bij Cooperatie Medische Staf St Jansdal UA |
- |
- |
Geen restricties |
|
Juliëtte Starmans (klankbordgroep) |
AIOS bedrijfsgeneeskunde. Ik werk als ZZP’er en ben aldus aangesloten bij Immediator. Tijdens mijn opleiding ben ik werkzaam bij een klant, waar ik betaalde werkzaamheden verricht. |
Naast AIOS bedrijfsgeneeskunde ben ik werkzaam als orthopedisch chirurg. In deze hoedanigheid werk ik eveneens als ZZP’er in mijn éénmansbedrijf: Starmans orthopedische expertises. Via dit bedrijf verricht ik orthopedische expertises voor verzekeringen. Tevens ben ik via dit bedrijf als medisch adviseur werkzaam voor Medisch Advies Bureau. Alle werkzaamheden voor Starmans orthopedische expertises zijn betaalde werkzaamheden. |
- |
Geen restricties |
|
Florus van der Giesen (klankbordgroep) |
Physician assistant reumatologie |
- |
- |
Geen restricties |
|
Lisette de Graauw (klankbordgroep) |
Zorgverlener in zowel de eerste als tweede lijngezondheidszorg.
|
- |
Ik werk in de voetzorg, dus ja, als blijkt dat de uitkomsten van de richtlijn laten zien dat de door mijn beroepsgroep geleverde zorg werkt, dan heb ik (en mijn beroepsgroep) daar voordeel bij. |
Geen restricties |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door de Patiëntenfederatie Nederland te betrekken in de klankbordgroep-fase. De verkregen input is meegenomen bij het opstellen van de overwegingen (zie kop “Waarden en voorkeuren van patiënten”). De conceptrichtlijn is tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Corticosteroïden - Fasciopathie Plantaris |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (5.000- 40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Fasciopathie Plantaris – UV7 Corticosteroïden |
|
|
Uitgangsvraag/modules: Wat is de plaats van corticosteroïd-injecties bij de behandeling bij patiënten met fasciopathie plantaris? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 28-3-2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
Rayyan review: https://rayyan.ai/reviews/980292 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen corticosteroïden EN fasciopathie plantaris.
→ De sleutelartikelen worden gevonden met deze search.
|
|
|
Te gebruiken voor richtlijntekst: In de databases Embase.com en Ovid/Medline is op 28 maart 2024 systematisch gezocht naar systematische reviews en RCTs over de plaats van corticosteroïd-injecties bij de behandeling bij patiënten met fasciopathie plantaris. De literatuurzoekactie leverde 238 unieke treffers op. |
|
Zoekopbrengst - 28 maart 2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
91 |
61 |
100 |
|
RCT |
129 |
81 |
138 |
|
Observationeel |
|
|
|
|
Totaal |
220 |
142 |
238* |
*in Rayyan
Zoekstrategie - 28 maart 2024
Embase.com
|
No. |
Query |
Results |
|
#1 |
'plantar fasciitis'/exp OR 'plantar fasciopathy'/exp OR 'heel spur'/exp OR 'policeman heel'/exp OR (((calcane* OR heel* OR subcalcane*) NEAR/3 (spur* OR exostos* OR pain* OR policeman* OR jogger*)):ti,ab,kw) OR ((plant* NEAR/3 (fasciitis OR fasciopath* OR fascios* OR inflam*)):ti,ab,kw) OR (((baxter* OR plant* OR calcane* OR heel) NEAR/3 neuropath*):ti,ab,kw) OR calcaneodyn*:ti,ab,kw OR 'calcane* periostitis':ti,ab,kw |
6372 |
|
#2 |
'corticosteroid'/exp OR 'corticosteroid therapy'/exp OR corticosteroid*:ti,ab,kw OR glucocortico*:ti,ab,kw OR 'adrenal cortex hormone*':ti,ab,kw OR 'adrenal steroid*':ti,ab,kw OR corticoid*:ti,ab,kw OR corticotherap*:ti,ab,kw |
1281681 |
|
#3 |
#1 AND #2 |
824 |
|
#4 |
#3 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
575 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1014761 |
|
#6 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
2178974 |
|
#7 |
#4 AND #5 – SR’s |
91 |
|
#8 |
#4 AND #6 NOT #7 – RCT’s |
129 |
|
#9 |
#7 OR #8 |
220 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Fasciitis, Plantar/ or exp Heel Spur/ or ((calcane* or heel* or subcalcane*) adj3 (spur* or exostos* or pain* or policeman* or jogger*)).ti,ab,kf. or (plant* adj3 (fasciitis or fasciopath* or fascios* or inflam*)).ti,ab,kf. or ((baxter* or plant* or calcane* or heel) adj3 neuropath*).ti,ab,kf. or calcaneodyn*.ti,ab,kf. or calcane* periostitis.ti,ab,kf. |
4416 |
|
2 |
exp Adrenal Cortex Hormones/ or corticosteroid*.ti,ab,kf. or glucocortico*.ti,ab,kf. or 'adrenal cortex hormone*'.ti,ab,kf. or 'adrenal steroid*'.ti,ab,kf. or corticoid*.ti,ab,kf. or corticotherap*.ti,ab,kf. |
530831 |
|
3 |
1 and 2 |
324 |
|
4 |
limit 3 to yr="2000 -Current" |
279 |
|
5 |
4 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
259 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
735289 |
|
7 |
exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf. |
1700385 |
|
8 |
5 and 6 – SR’s |
61 |
|
9 |
(5 and 7) not 8 – RCT’s |
81 |
|
10 |
8 or 9 |
142 |