Shockwave therapie
Uitgangsvraag
Wat is de plaats van shockwavetherapie bij de behandeling bij patiënten met fasciopathie plantaris?
Aanbeveling
Overweeg shockwave therapie (ESWT) in samenspraak met de patiënt als aanvullende behandeling voor patiënten met fasciopathie plantaris, mits:
- De patiënt minimaal 12 weken adequaat wordt behandeld via educatie (zie module Educatie) en oefentherapie (zie module Oefentherapie) zonder effect.
- De patiënt niet eerder is behandeld met shockwave therapie binnen deze ziekte-episode.
Overweeg maximaal 3 sessies toe te passen. Zowel radiaal als gefocusseerde shockwave kunnen 1x per week worden toegepast.
Overweeg shockwave therapie (ESWT) te combineren met oefentherapie.
Overwegingen
Balans tussen gewenste en ongewenste effecten
In de literatuursamenvatting zijn 15 studies samengevat die het effect van ESWT met sham-ESWT vergelijken op de uitkomstmaten pijn, functie, bijwerkingen en kwaliteit van leven.
Uit de geselecteerde literatuur kwam naar voren dat ESWT waarschijnlijk pijn en functie verbetert na 12 weken follow-up (middellange termijn) ten opzichte van placebo met een moderate GRADE. Voor korte (3-6 weken) en lange (1 jaar) termijn kan ESWT mogelijk leiden tot een verbetering van pijn en functie (low GRADE). Alle effecten gemeten op pijn en functie waren in het voordeel van ESWT en klinisch relevante verschillen. Echter kan ESWT mogelijk ook leiden tot meer korte-termijn bijwerkingen zoals zwelling, roodheid, en pijn en/of ongemak ten opzichte van sham-ESWT, met een klinisch relevant verschil. ESWT heeft waarschijnlijk weinig tot geen effect op kwaliteit van leven. De uitkomstmaat terugkeer naar sport werd in geen van de geïncludeerde studies gerapporteerd.
Recent werd er een studie gepubliceerd die geen effectiviteit van radiale ESWT liet zien boven op de behandeling met advies en aangepaste inlays voor de aanpak van fasciopathie plantaris (Heide, 2024). Deze werd zowel vanwege zeer recente publicatie als vanwege afwijking van de tevoren opgestelde PICO niet geïncludeerd in de analyse.
Vergroting van ziekte-inzicht vergroot de mate van therapietrouw en toepassing van nuttige coping strategieën ten aanzien van genezing. Daarom is de richtlijncommissie van mening dat educatie als eerste toegepast moet worden in geval van fasciopathie plantaris. Om een metafoor te gebruiken: het is niet nuttig te gaan dweilen terwijl de kraan open staat. Daarom is het belangrijk de educatie ten aanzien van load management allereerst toe te passen en zo doende de kraan dicht te draaien. Het dweilen, dat wil zeggen ESWT ten aanzien van het peesweefsel, pas toe te passen als de belasting voor voldoende lange tijd aangepast is. Een actieve participatie van de patiënt vanaf het begin van de behandeling helpt ook de therapietrouw te bevorderen. Vandaar dat de richtlijncommissie van mening is het zelfstandig uitvoeren van rekoefeningen van de fascia plantaris door de patiënt samen met educatie eerst dient plaats te vinden.
De werkgroep baseert het doseringsadvies voor ESWT op de doseringen die in de geïncludeerde studies zijn gebruikt. Hierin dient wel onderscheid te worden gemaakt tussen gefocusseerde en radiale shockwave therapie:
- Voor gefocusseerde ESWT adviseert de werkgroep een dosis tussen de 0.08 mJ/mm2 tot 0.60 mJ/mm2, resulterend in een cumulatieve dosis tot 1000 mJ/mm2 bij 1000-3500 shocks.
- Voor radiale ESWT adviseert de werkgroep een dosis tussen de 0.05 mJ/mm2 tot 0.320 mJ/mm2, resulterend in een cumulatieve dosis tot 400 mJ/mm2 bij 1000-2000 shocks.
Gezien de literatuursamenvatting concludeert tot een waarschijnlijke verbetering in pijn en functie 12 weken na afronding van gemiddeld 3 ESWT-sessies, beveelt de werkgroep aan om 3 ESWT sessies toe te passen 1x per week.
Uit een systematic review van Roerdink et al in 2017, bleek na analyse van 39 studies (2493 patiënten, follow up 24 uur tot 6 jaar) dat er nauwelijks complicaties tijdens of na ESWT optreden. Dit kwam slechts twee keer voor: één patiënt had precordiale pijn en één patiënt had een oppervlakkige huidinfectie na regionale anesthesie. Daarnaast worden pijn tijdens de behandeling en tijdelijk lokaal erytheem beschreven na de behandeling als bijwerking. Andere gerapporteerde bijwerkingen waren tijdelijke pijn na de behandeling, dysesthesie, zwelling, ecchymose en/of petechiën, ernstige hoofdpijn, blauwe plekken en een bonzend gevoel.
ESWT lijkt een veilige behandeling voor fasciopathie plantaris te zijn, waarbij geen complicaties worden verwacht na een follow-up van één jaar. Lange termijn complicaties zijn echter onbekend op basis van de huidige literatuur.
Bij bepaalde patiëntcategorieën, zoals patiënten met hypersensitiviteit of verhoogde pijnbeleving of verminderde verstandelijke vermogens, waarbij het voorbereiden op de te verwachten pijn lastig wordt, zal ESWT als behandelingsoptie mogelijk minder gewenst zijn.
Kwaliteit van bewijs
De overall kwaliteit van bewijs is laag. Dit betekent dat we terughoudend zijn over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege ernstige:
- Risk of Bias: methodologische beperkingen zoals onder andere onvoldoende blindering van toewijzing tijdens het randomisatie proces, ontbreken van blindering van uitkomstmaatbeoordelaars en ontbrekende intention-to-treat analyses.
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grens van klinische relevantie overschrijdt.
Publicatiebias was niet beoordeeld.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
ESWT kan pijnklachten, roodheid en zwelling geven op het moment van en korte tijd na de behandeling. Dit kan door veel patiënten als zeer onprettig ervaren worden. Ook al zijn dit zeker hinderlijke bijwerkingen van de behandeling, toch denken we dat de nadelen hiervan ruimschoots gecompenseerd worden door de voordelen van werkzaamheid van de behandeling. Het is belangrijk de patiënt goed in te lichten over het te verwachten effect van de behandeling en de mogelijke bijwerkingen. Bij patiënten met hypersensitiviteit of verhoogde pijnbeleving of verminderde verstandelijke vermogens, waarbij het voorbereiden op de te verwachten pijn lastig wordt, dient het optreden van bijwerkingen goed besproken te worden met de patiënt.
Gewenste effecten:
De vermindering van de oorspronkelijke pijnklacht passend bij fasciopathie plantaris zal in de meeste gevallen ruimschoots opwegen tegen de nadelen van pijnklachten op het moment van de behandeling en korte tijd erna.
Ongewenste effecten:
Een ongewenst effect kan naast de veroorzaakte pijn, ook het verminderd vertrouwen van de patiënt in de behandelaar zijn, zeker als de patiënt tot een van de eerdere patiëntcategorieën, als patiënten met verhoogde sensitiviteit, pijnbeleving of verminderde verstandelijke vermogens, behoort.
Kostenaspecten
Momenteel worden voor de kosten van behandeling met ESWT alleen de kosten voor het spreekuur bij de fysiotherapeut in rekening gebracht. In het verleden kwamen daar ook nog kosten voor gebruik van het apparaat bij, maar dat is inmiddels niet meer het geval. Dit zorgt ervoor dat het net zo duur/goedkoop is als het geven van advies en of het voordoen van oefeningen of verrichten van manuele handelingen in de fysiotherapiepraktijk. Het is wel zo dat er sprake is van 3 behandelingssessies.
Gelijkheid ((health) equity/equitable)
Gezien er qua kosten geen evident verschil is met de gebruikelijke therapie zoals uitleg en voordoen van oefeningen in het spreekuur en follow-up, en voldoende beschikbaarheid van ESWT-apparatuur in fysiotherapiepraktijken in Nederland, zou er geen toename van ongelijkheid in gezondheid verwacht worden. Echter dient er rekening te worden gehouden met de verzekerde zorg en aantal vergoede behandelingen, wat wanneer overschreden wel kan leiden tot gezondheidsongelijkheid.
Aanvaardbaarheid
Ethische aanvaardbaarheid
De interventie lijkt aanvaardbaar voor de betrokkenen. Er zijn geen ethische bezwaren, mits eventuele bijwerkingen van de behandeling goed uitgelegd kunnen worden.
Duurzaamheid
Duurzaamheid heeft geen invloed op de keuze tussen shockwave therapie of andere conservatieve behandelingen.
Haalbaarheid
De interventie met ESWT is over het algemeen al standaardzorg in de praktijk. Er zijn voldoende fysiotherapiepraktijken in NL met de beschikbaarheid over ESWT-apparatuur. Ook lijken er geen financiële obstakels aanwezig om ESWT toe te passen zoals voorgesteld in de richtlijn.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Er is enig bewijs om shockwave als behandeling toe te voegen o.b.v. middellange termijneffect (twaalf weken) voor pijn en functie. Effectiviteit is veelal bepaald bij patiënten met chronische klachten en/of patiënten die niet reageren op conservatieve behandelingen. Daarom wordt shockwave enkel in deze selectie patiënten aanbevolen.
Eindoordeel:
Zwakke aanbeveling voor shockwave therapie.
Onderbouwing
Shockwave therapy (ESWT) is applied in secondary care in the Netherlands as a treatment for plantar fasciopathy, but there is undesirable practice variation. It is not known how frequently shockwave is applied or referred to in hospitals.
The goal of this module is to determine the role of shockwave therapy in relation to first-line treatments in secondary care (exercise therapy; education).
Summary of Findings
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
sham-ESWT |
ESWT |
||||
|
Short-term pain 3-6 weeks |
Measured by: VAS Scale: 0 - 10 Lower better
Based on data from 1013 participants in 9 studies Follow up 3-6 weken |
Difference: MD 1.93 lower (CI 95% 3.19 lower - 0.61 lower) |
Low Due to serious risk of bias, Due to serious imprecision2 |
Extracorporale shockwave therapy may reduce short-term pain when compared with placebo in patients with plantar fasciopathy. |
|
|
Mid-term pain 12 weeks |
Measured by: VAS Scale: 0 - 10 Lower better
Based on data from 1559 participants in 10 studies Follow up 12 weeks |
Difference: MD 2.13 lower (CI 95% 3.38 lower - 0.95 lower) |
Moderate Due to serious imprecision3 |
Extracorporale shockwave therapy probably reduces pain at 12 weeks when compared with placebo in patients with plantar fasciopathy |
|
|
Long-term pain 1 year
|
Measured by: Scale: - High better
Based on data from 357 participants in 4 studies Follow up 1 year |
Difference: MD 5.61 lower (CI 95% 10.00 lower - 0.89 lower) |
Low Due to serious risk of bias, Due to serious imprecision4 |
Extracorporale shockwave therapy may reduce long-term pain when compared with placebo in patients with plantar fasciopathy. |
|
|
Short-term function
|
Measured by: Roles & Maudsley score Scale: 1 - 4 Lower better
Based on data from 358 participants in 5 studies Follow up 3-6 weeks |
Difference: MD 0.95 lower (CI 95% 1.60 lower - 0.18 lower) |
Low GRADE Due to serious risk of bias, Due to serious imprecision5 |
Extracorporale shockwave therapy may improve short-term function when compared with placebo in patients with plantar fasciopathy. |
|
|
Mid-term function
|
Measured by: Roles & Maudsley score Scale: 1 - 4 Lower better
Based on data from 567 participants in 4 studies Follow up 12 weeks |
Difference: MD 0.75 lower (CI 95% 1.39 lower - 0.11 lower) |
Moderate GRADE Due to serious imprecision6 |
Extracorporale shockwave therapy probably slightly improves function at 12 weeks when compared with placebo in patients with plantar fasciopathy |
|
|
Long-term function
|
Measured by: Roles & Maudsley score Scale: 1 - 4 Lower better
Based on data from 80 participants in 2 studies Follow up 1 year |
Difference: MD 5.61 lower (CI 95% 10.0 lower - 0.89 lower) |
Low GRADE Due to serious risk of bias, Due to serious imprecision7 |
Extracorporale shockwave therapy may improve long-term function when compared with placebo in patients with plantar fasciopathy. |
|
|
Side effects
|
Relative risk: 3.32 (CI 95% 1.89 - 5.85)
Based on data from 1260 participants in 7 studies Follow up during /post treatment |
1 per 1000 |
3 per 1000 |
Low GRADE Due to very serious risk of bias1 |
Extracorporale shockwave therapy may lead to more short-term adverse events (pain, discomfort, swelling, redness) when compared with placebo in patients with plantar fasciopathy. |
|
Difference: 2 more per 1000 (CI 95% 1 more - 5 more) |
|||||
|
Quality of life- physical
|
Measured by: SF-36 (physical domain) Scale: 0 - 100 High better
Based on data from 508 participants in 3 studies Follow up 12 weeks |
Difference: MD 2.91 lower (CI 95% 9.96 lower - 4.13 higher) |
Moderate GRADE Due to serious inconsistency8 |
Extracorporale shockwave therapy probably has little or no difference on physical quality of life when compared with placebo in patients with plantar fasciopathy |
|
|
Quality of life- Mental
|
Measured by: SF-36 (mental domain) Scale: 0 - 100 High better
Based on data from 508 participants in 3 studies Follow up 12 weeks |
Difference: MD 0.92 lower (CI 95% 5.05 lower - 3.21 higher) |
Moderate GRADE Due to serious inconsistency9 |
Extracorporale shockwave therapy probably has little or no difference on mental quality of life when compared with placebo in patients with plantar fasciopathy |
|
|
Return to sport
|
|
|
No GRADE
|
No evidence was found regarding the effect of extracorporale shockwave therapy on return to sport when compared with placebo in patients with plantar fasciopathy. |
|
1. Risk of Bias: very serious. Selective outcome reporting, Trials stopping earlier than scheduled, resulting in potential for overestimating benefits, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Incomplete data and/or large loss to follow up, due to [reason].
2. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias, Incomplete data and/or large loss to follow up, Missing intention-to-treat analysis; Imprecision: serious. Wide confidence intervals.
3. Imprecision: serious. Wide confidence intervals.
4. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias, Incomplete data and/or large loss to follow up, Missing intention-to-treat analysis; Imprecision: serious. Wide confidence intervals.
5. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias, Incomplete data and/or large loss to follow up, Missing intention-to-treat analysis; Imprecision: serious. Wide confidence intervals.
6. Imprecision: serious. Wide confidence intervals.
7. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias, Incomplete data and/or large loss to follow up, Missing intention-to-treat analysis; Imprecision: serious. Wide confidence intervals, Low number of patients.
8. Inconsistency: serious. The direction of the effect is not consistent between the included studies; Point estimates vary widely.
9. Inconsistency: serious. Point estimates vary widely; The direction of the effect is not consistent between the included studies.
Description of studies
A total of 15 studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
Buchbinder 2002, Australia |
N at baseline ESWT: 80 Placebo: 81
Age (mean ± SD) ESWT 52.2 ± 12.81 Placebo: 54.2 ± 12.05
Sex (% female) ESWT: 57.5 Placebo: 58.0
Baseline overall pain (mean VAS ± SD) ESWT: 71.5 ± 21.7 Placebo: 68.6 ±23.3
Baseline function (mean Maryland Foot Score ± SD) ESWT: 54.6 ± 16.0 Placebo: 53.4 ± 17.0
Inclusion: Patients had plantar heel pain for at least 6 weeks and clinical diagnosis, including thickened plantar fascia on ultrasound. |
f-ESWT: 3 sessions of 2000/2500 shock waves per treatment for 3 weeks. Total cumulative dose 1000 mJ/mm2. Ultrasound gel used.
sham ESWT: 3 sessions of 100 shock waves per treatment, for 3 weeks. Total dose 6.0 mJ/mm2. |
6 weeks, 12 weeks |
Pain (100 VAS) Function (Maryland Foot Score) Quality of life (SF-36 domains) Side effects |
As-treated analysis (5 drop-outs in total).
Conflicts of interest not reported.
|
LOW |
|
Haake, 2003 Germany |
N at baseline ESWT: 135 placebo: 136
Age (mean ± SD) ESWT 53.1 ± 10.8 Placebo: 52.9 ± 10.8
Sex (% female) ESWT: 73 Placebo: 78
Baseline pain at rest (mean VAS ± SD) ESWT: 3.9 ± 2.5 Placebo: 3.7 ± 2.3
Inclusion: Patients had plantar medial heel pain for at least 6 months and clinical diagnosis, and radiologically proven calcaneal spur |
f-ESWT: 4000 impulses of a positive energy flux density (0.08 mJ/mm2) under local anaesthesia with 2 ml mepivacaine 1%. Therapy was applied every two weeks plus or minus two days (3 × 4000 impulses).
Sham-ESWT: Patients received the same regimen of therapy under local anaesthesia. A foil filled with air was fixed with ultrasound gel in front of the coupling cushion to reflect the shock waves
|
6 weeks, 12 weeks |
Pain (10-point VAS) Function (dichotomized Roles and Maudsley score) Side effects |
Authors declared no conflicts of interest.
|
LOW |
|
Speed, 2003 United Kingdom |
N at baseline ESWT:46 Placebo: 42
Age (mean ± SD) ESWT: 51.7± NR Placebo:52.5± NR
Sex (% female) ESWT: 56% Placebo: 59.5%
Baseline VAS (mean ± SD) ESWT: 73.6 (20.1) Placebo: 70.0 (20.1)
Inclusion: Adult subjects with a clinical diagnosis of plantar fasciitis and at least 3 months of plantar heel pain |
f-ESWT: 3 applications of Electromagnetic 1500 pulses at 0.12 mJ/mm2 over 8 weeks.
Placebo: 3 applications of Sham ESWT with deflated treatment minimal energy pulses (0.04 mJ/mm2 ) over 8 wks. |
4 weeks (12 weeks from baseline) |
Pain (100 point VAS) |
No conflicts of interest reported.
|
some concerns |
|
Rompe, 2003 Germany |
N at baseline ESWT: 22 Placebo: 23
Age (mean ± SD) ESWT: 43±NR Placebo: 40±NR
Sex (% female) not reported (no significant difference between groups)
Baseline VAS first walking pain (mean ± SD) ESWT: 6.9 ± 1.3 Placebo: 7.0 ± 1.3
Inclusion: Patients were long-distance runners (recreational athletes) with at least 12 months of symptoms |
Low energy f-ESWT: 3 applications of 2 100 impulses of 0.16mJ/mm2, 4Hz radius 1.5-2cm over 3 wks
Placebo: 3 applications of Sham ESWT over 3 wks with sound reflecting pad, no coupling gel. |
6 months, 1 year |
Pain (10 point VAS)
|
Conflicts of interest not reported. |
Some concerns |
|
Theodore, 2004 United States |
N at baseline ESWT: 76 Placebo: 74
Age (mean ± SD) ESWT: 50±NR Placebo: 53±NR
Sex (% female) ESWT: 81.6% Placebo: 63.5%*
Baseline VAS first walking pain (mean ± SD) ESWT: 7.7 ± 1.4 Placebo: 7.7 ± 1.5
Inclusion: Patients had plantar medial heel pain for at least 6 months and clinical diagnosis, and participated in stretching program 6 months prior start of trial. |
f-ESWT: 1 session with 3800 shocks (3500 at 0.36 mJ/mm2) for a total of 1300 mJ/mm2 (generated using the Epos Ultradevice. Medial calcaneal nerve block using 5 mL of 1% xylocaine 15–20 minutes prior to the procedure).
Placebo: sham ESWT. With thin air cushion on the therapy head. |
6 weeks, 12 weeks |
Pain (10-point VAS), Function (dichotomized Roles and Maudsley), QoL (SF-12) |
Study was industry sponsored.
|
some concerns |
|
Kudo, 2006 Canada |
N at baseline ESWT: 58 Placebo: 56
Age (mean ± SD) ESWT: 51.1 ± 10.6 Placebo: 48.8 ± 9.8
Sex (% female) ESWT: 69.0% Placebo: 59.0%
Baseline VAS first walking pain (mean ± SD) ESWT: 7.5 ± 1.5 Placebo: 7.9 ± 1.5
Inclusion: Patients had plantar medial heel pain for at least 6 months and clinical diagnosis, and participated in stretching program 6 months prior (similar to Theodore, 2004) |
f-ESWT: 1 session of 3800 shockwaves, total energy delivery of 1,300 mJ/mm2 (ED+) or 2,330 mJ/mm2 (ED).
Placebo: sham ESWT with thin foam cushion and ultrasound gel. |
6 weeks, 12 weeks |
Pain (10-point VAS), Function (dichotomized Roles and Maudsley), QoL (SF-12), Side effects |
Study was industry sponsored.
|
Some concerns |
|
Malay, 2006 United States |
N at baseline ESWT: 115 Placebo: 57
Age (mean ± SD) ESWT: 50.8 ± 10.1 Placebo: 52.1 ± 11.1
Sex (% female) ESWT: 68.7% Placebo: 63.2%
Inclusion: Included patients with chronic proximal plantar fasciitis. |
f-ESWT: 3800 shockwave impulses, 150/minute for 25 minutes. Dose not reported, but variable (from level 1 up to 7 of the Orthospec device)
Placebo ESWT: Same procedure as ESWT group, but with foam-insulated membrane |
4 weeks, 12 weeks |
Pain (10-point VAS) Side effects |
Study was industry sponsored. |
Some concerns |
|
Chow, 2007 Hong-Kong |
n at baseline ESWT: 19 Placebo: 19
Age (mean ± SD) ESWT fixed dose: 51.9 ± 11.7 Placebo: 50.6 ± 9.8
Sex (% female) ESWT: 63.2% Placebo: 52.6%
Inclusion: Included patients with plantar heel pain for at least 3 months |
r-ESWT: rESWT in 3 sessions (1 per wk) of 1000 shock wave impulses, 3 Hz. Dose 0.05 mJ/ mm2, gradually increasing to highest possible tolerable pain level.
Placebo ESWT: 3 sessions (1 per wk) of 30 shock wave impulses, 3 Hz. Dose 0.03 mJ/ mm2.
|
3 weeks |
Pain (VAS) function (FFI) |
Conflicts of interest not reported
|
HIGH |
|
Gerdesmeyer, 2008 United States, Europe |
n at baseline ESWT: 125 Placebo: 118
Age (mean ± SD) ESWT: 52.4 ± 12.0 Placebo: 52.0± 10.5
Sex (% female) ESWT: 69.6% Placebo: 67.9%
Baseline VAS first walking pain (mean ± SD) ESWT: 7.5 ± 1.5 Placebo: 7.5 ± 1.6
Inclusion: Patients with clinical diagnosis and at least 6 months of chronic plantar heel pain that proved resistant to conservative treatments. |
r-ESWT: 3 applications of radial ESWT with 2000 impulses at 0.16 mJ/mm2 over 6 weeks
Control: Placebo: Sham ESWT. 3 sessions over 6 weeks |
12 weeks |
Pain (10-point VAS) function (dichotomized roles and Maudsley) QoL (SF-36) Side effects |
The study was sponsored by the manufacturer
|
LOW |
|
Ibrahim 2010, ibrahim 2017
United States |
n at baseline ESWT: 25 Placebo: 25
Age (mean ± SD) ESWT: 56.6 ± 13.5 Placebo: 49.10± 12.8
Sex (% female) ESWT: 72% Placebo: 56%
Baseline VAS first walking pain (mean ± SD) ESWT: 8.5 ± 1.7 Placebo: 8.9 ± 1.0
Inclusion: Patients with clinical diagnosis and at least 6 months of chronic plantar heel pain that proved resistant to conservative treatments. |
r-ESWT: 2 sessions 2,000 impulses (Air pressure of device at 3.5 bar) Dose =0.16 mJ/mm2; 15 mm applicator at frequency of 8 Hz.
Placebo: 2 sessions of sham ESWT performed with clasp on heel to prevent transmission of impulses from applicator to skin |
4 weeks, 12 weeks, 1 year |
Pain (10 point VAS), Function (Modified Roles and Maudsley) Side effects
|
One of the authors served as consultant for manufacturer, authors declared no other conflicts of interest.
|
LOW |
|
Saxena, 2012
|
n at baseline ESWT: 11 Placebo: 14
Age (mean ± SD) ESWT: 47.9 ± 12.6 Placebo: 47.6 ± 9.9
Sex (% female) ESWT: 36% Placebo: 42%
Baseline VAS first walking pain (mean ± SD) ESWT: 8.7 ± 1.4 Placebo: 8.0 ± 1.1
Inclusion: Patients were athletes. Patients with clinical diagnosis and at least 6 months of chronic plantar heel pain that proved resistant to conservative treatments |
f-ESWT: 3 sessions, once per week with 2000 impulses and dose of 0.24 mJ/mm2 at frequency of 4 Hz.
Placebo: 3 sessions (once per week) of sham ESWT performed with blocking head to prevent transmission of impulses from applicator to skin |
1 year |
Pain (10-point VAS) Function (roles and Maudsley)
|
Study also included surgical study arm, which is not included in this analysis.
|
HIGH |
|
Gollwitzer, 2015 United States |
n at baseline ESWT: 125 Placebo: 121
Age (mean ± SD) ESWT: 50.0 ± 11.2 Placebo: 47.4 ± 10.6
Sex (% female) ESWT: 68% Placebo: 72.7%
Baseline VAS first walking pain (mean ± SD) ESWT: 7.9 ± 1.6 Placebo: 8.0 ± 1.6
Inclusion: Patients with clinical diagnosis and at least 6 months of chronic plantar heel pain that proved resistant to conservative treatments |
f-ESWT: 3 applications of ESWT 2000 waves to the point of maximal tenderness at 0.25 mJ/mm2 over 3 weeks.
placebo: Sham ESWT with airfilled standoff preventing transmission. 3 sessions over 3 weeks |
12 weeks |
Pain (10-point VAS) Function (Roles and Maudsley) Side effects |
Funded by manufacturer, but they had no active role.
|
LOW |
|
Hawamdeh, 2016 Jordan |
n at baseline ESWT: 12 Placebo: 12
Age (mean ± SD) Not reported
Sex (% female) ESWT: 66% Placebo: 86%
Baseline VAS first walking pain (mean ± SD) ESWT: 6.2 ± 2.3 Placebo: 6.6± 2.3
Inclusion: Adults with diagnosis of plantar fasciitis |
f-ESWT: 3 sessions (over 3 wks) of 2000 shockwaves Dose: 0.25mj/mm2. ESWT was followed by 10-min ice application and 3 times 30 second plantar stretching exercises
Placebo: sham-ESWT identical to ESWT group with clasp on heel to prevent transmission. 3 sessions for 3 weeks |
3 weeks |
Pain (10-point VAS) Function (Roles and Maudsley) |
Conflicts of interest not reported
|
HIGH |
|
Şah, 2023 Turkey |
n at baseline f-ESWT group: 30 r-ESWT group: 33 placebo: 29
Age (mean ± SD) f-ESWT group: 46 ± 11.3 r-ESWT group: 48.7 ± 10.6 placebo: 52.2 ± 10.5
Sex (% female) f-ESWT group: 50% r-ESWT group: 51% placebo: 55%
Baseline FFI pain (mean ± SD) f-ESWT group: 60 .0± 7.5 r-ESWT group: 62.8 ± 11.7 placebo: 59.2 ± 12.3
Inclusion: Patients with clinical diagnosis of plantar fasciitis as well as calcaneal spur present
|
f-ESWT: 5 minutes of focused ESWT with 500 pulses at 5Hz for 1.40 minutes and 1800 pulses at 10 Hz for 3 minutes. Dosage was 0.02–0.60 mJ/mm2.
r-ESWT: radial ESWT for 5 minutes with 500 pulses at 5Hz for 1.40 10 Hz with 1800 pulses for 3 minutes. All with a dosage of 0.204 mJ/mm2
- sham ESWT (0 Joule), with same frequency and pressure values as radial ESWT group
All ESWT groups applied in three sessions, with 2-4 day intervals, for 1 week total |
4 weeks, 12 weeks |
Pain and function (both via FFI) |
Compared focused, radial and sham ESWT.
Authors declared no conflicts of interest.
|
LOW |
*For further details, see risk of bias table in the appendix
Results
1. Pain (crucial)
Pain was reported by all studies. 14 studies assessed pain with the visual analogue scale of either 10 or 100 points (VAS; scale of 0 to 10 or 100 with 0 representing no pain and 10 or 100 the worst pain imaginable). Haake (2003) and Chow (2007) assessed pain on palpation instead of overall pain. Theodore (2004) assessed pain at first walking in the morning.
Sah (2023) reported on pain using the pain subcategory of the Foot function index (FFI) which consists of 9 items (resulting in a score of 0-90) assessing pain in different situations.
The results on pain were pooled for three follow-up periods: short term pain, assessed between 3-6 weeks after last treatment; mid-term pain, assessed at 12 weeks after last treatment; and long-term pain, assessed at one year after treatment.
As different scales were used for assessment, the results were pooled using the standardized mean difference (SMD).
Nine studies assessed short-term pain (figure 1). When pooling the results of 1009 patients, this resulted in an SMD of -0.70 (95% CI -1.18 to -0.22) in favor of ESWT. To assess the clinical relevance on the found effect, the SMD was transformed back to a 10-point VAS, resulting in a mean difference (MD) of -1.93 (95% CI -3.19 to -0.60). This is a clinically relevant difference.
Pain at 12 weeks (mid-term) was assessed in ten studies with in total 1559 patients, off which the pooled results lead to an SMD of -0.56 (95% CI -0.89 to -0.24). After transforming this back to the VAS this results in an MD of -2.13 (95% CI -3.38 to -0.95) in favour of ESWT. This is also a clinically relevant difference.
Four studies (n=357) assessed long-term pain at one year after last intervention. This resulted in an SMD of -1.26 (95% CI -2.32 to -0.20), which transformed to the VAS equaled an MD of -5,61 (95% CI -10,00 to -0.89) in favour of ESWT. This is also a clinically relevant difference.
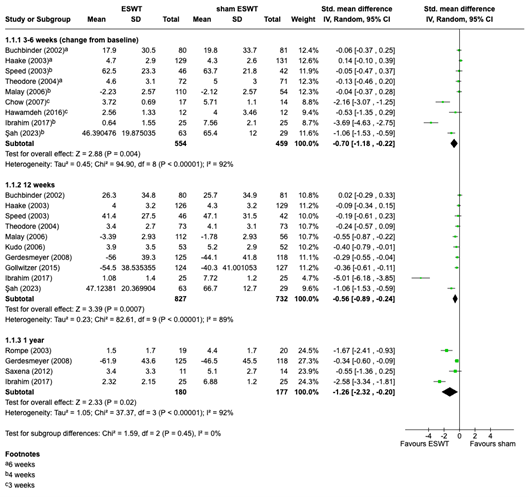
Figure 1. Meta-analysis of the effect of ESWT on pain (continuous scales)
2. Function (crucial)
Eleven of the included studies reported on function. Haake (2003), Theodore (2004), Kudo (2006), Gerdesmeyer, (2008), Saxena (2012), Gollwitzer ( 2015), Hawamdeh (2016) and Ibrahim (2010, 2017) used the Roles and Maudsley (R&M) score to assess function (score of 1 to 4, ranging from full movement and no pain to severe limitation of movement with pain).
Chow (2007) and Sah (2023) reported on function using the disability subcategory of the Foot function index (FFI) which consists of nine items (rated on a 10-point VAS, resulting in a score between 0 and 90) assessing disability in different daily tasks.
Buchbinder (2002) assessed function using the Maryland Foot Score, a disability index that derives a score from 0 to 100 points, measuring pain and function of the foot.
For short term function (3-6) weeks, the continuous score of the R&M (Hawamdeh 2016 & Ibrahim 2010/2017) was pooled together with the FFI disability subcategory and the Maryland Foot score, resulting in an SMD of -1.58 (95% CI -2.86 to -0.30). Transforming this back the R&M this results in an MD of -0.95 (95% CI -1.60 to -0.18) in favour of ESWT. This is a clinically relevant difference.
For mid-term function, which was reported by four studies (n = 547), the SMD of -0.77 (95% CI -1.43 to -0.11) was transformed to an MD of -0.75 (95% -1.39 to -0.11) in favour of ESWT on the R&M score. This was also a clinically relevant difference.
Long-term function was assessed by Saxena (2012) and Ibrahim (2010/2017) and was pooled to an SMD of -0.73 (95% CI -1.20 to -0.26). This was transformed back to an R&M MD of -5.61 (95% CI -10.00 to -0.89). This was also a clinically relevant difference.
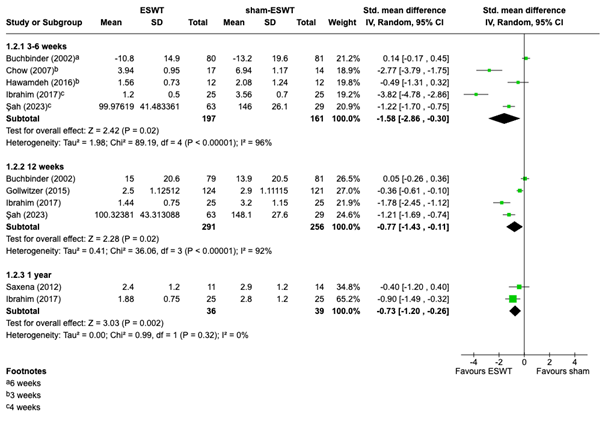
Figure 2. Meta-analysis of function on continuous scale. Divided in subgroups for short-term, mid-term and long-term effects
Four studies (n= 750 patients) assessed the R&M score as a dichotomous outcome, in which patients with the scores 1 and 2 (Excellent, good) were scored as successful events, and the scores 3 and 4 (fair, poor) as unsuccessful. Results for mid-term (12 weeks) function are displayed in figure 3. The meta-analysis resulted in an RR of 1.34 (95% CI 1.15 to 1.57).

Figure 3. Meta analysis of function (12 weeks, dichotomized, shows RR for excellent to good score on the Roles and Maudsley score)
3. Side effects (crucial)
Seven studies (n = 1260) assessed side effects as a pre-specified outcome measure. Common reported side effects were redness, swelling, heat, numbness and pain or discomfort shortly after intervention. The incidence of these and similar side effects are pooled in figure 4, which resulted in an RR of 3.32 (95% CI 1.89 to 5.85) in favour of ESWT, meaning there was a higher risk in the ESWT group. The risk difference between groups was 0.18 (95% CI -0.04 to 0.40) and was also in favour of ESWT. This was a clinically relevant effect.
None of the studies reported any serious adverse events.
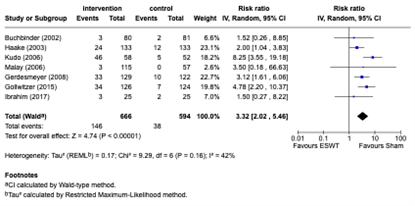
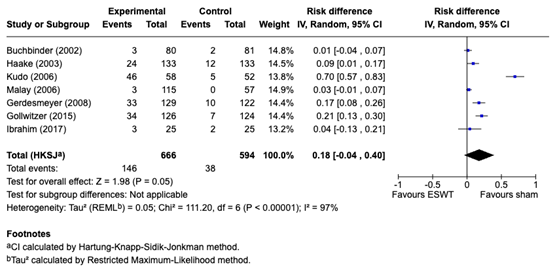
Figure 4. adverse events during or immediately post-intervention
4. Quality of life (important)
Four of the included studies assessed quality of life. Buchbinder (2002) and Gerdesmeyer (2008) used the physical and mental subscales of Short Form-36 Health Survey (SF-36) and Theodore (2004) and Kudo (2006) used the subscales of Short Form-12 Health Survey (SF-12), which is a shortened form of the SF-36 with fewer items. The subscales of both instruments range from 0 to 100, yet due to construct and unit differences an SMD was needed to pool the results. Theodore (2004) did not report the results (mean and SD) of the SF-12 questionnaire but stated solely that no statistically significant changes were found.
The other three studies (n= 508) were pooled in a meta-analysis (figure 5), resulting in an SMD of -0.12 (95% CI -0.41 to 0.17) for the physical subscale and -0.06 (95% CI -0.33 to 0.21) for the mental subscale. When transforming these back to the sf-36 this resulted in an MD of -2.91 (95% CI -9.96 to 4.13) and -0.92 (95% CI -5.05 to 3.21) respectively. Both of these differences were not clinically relevant.
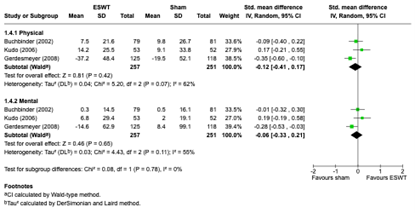
Figure 5.
5. Return to sport (important)
No studies reported on return to sport.
A systematic review of the literature was performed to answer the following question(s):
What is the effectiveness of shockwavetherapy in comparison to placebo (with add on exercise therapy) in patients with plantar fasciopathy?
Table 1. PICO
| Patients | Patients with plantar fasciopathy |
| Intervention | Radial extracorporeal shockwave therapy, focused extracorporeal shockwave therapy |
| Control | Placebo (with exercise therapy add-on) |
| Outcomes |
Pain (critical), function (critical), side effects (important), return to sport (important), quality of life (important) |
| Other selection criteria | Study design: systematic reviews, meta-analyses and randomized controlled trials |
Relevant outcome measures
The guideline panel considered pain, function and side effects as a crucial outcome measure for decision making; and return to sport and quality of life as an important outcome measure for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
The guideline panel defined 10% as a minimal clinically important difference for both continuous as well as dichotomous outcome measures. This includes a 10% difference on the outcome measurement on a continuous scale or an increase/decrease of relative risk (RRR) of 10% or more.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2000 until 28th of March 2024. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 278 hits.
Studies were selected based on the following criteria:
- Randomized controlled trials (RCTs), systematic reviews and/or meta-analyses.
- Studies according to the PICO.
- Studies including a minimum of 20 patients (10 patients per study arm).
- Full text English language publication.
Initially, 92 studies were selected based on title and abstract screening. After reading the full text, 77 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and 15 studies were included.
- Buchbinder R, Ptasznik R, Gordon J, Buchanan J, Prabaharan V, Forbes A. Ultrasound-guided extracorporeal shock wave therapy for plantar fasciitis: a randomized controlled trial. JAMA. 2002 Sep 18;288(11):1364-72. doi: 10.1001/jama.288.11.1364. PMID: 12234230.
- Chow IH, Cheing GL. Comparison of different energy densities of extracorporeal shock wave therapy (ESWT) for the management of chronic heel pain. Clin Rehabil. 2007 Feb;21(2):131-41. doi: 10.1177/0269215506069244. PMID: 17264107.
- Gerdesmeyer L, Frey C, Vester J, Maier M, Weil L Jr, Weil L Sr, Russlies M, Stienstra J, Scurran B, Fedder K, Diehl P, Lohrer H, Henne M, Gollwitzer H. Radial extracorporeal shock wave therapy is safe and effective in the treatment of chronic recalcitrant plantar fasciitis: results of a confirmatory randomized placebo-controlled multicenter study. Am J Sports Med. 2008 Nov;36(11):2100-9. doi: 10.1177/0363546508324176. Epub 2008 Oct 1. PMID: 18832341.
- Gollwitzer H, Saxena A, DiDomenico LA, Galli L, Bouché RT, Caminear DS, Fullem B, Vester JC, Horn C, Banke IJ, Burgkart R, Gerdesmeyer L. Clinically relevant effectiveness of focused extracorporeal shock wave therapy in the treatment of chronic plantar fasciitis: a randomized, controlled multicenter study. J Bone Joint Surg Am. 2015 May 6;97(9):701-8. doi: 10.2106/JBJS.M.01331. PMID: 25948515.
- Haake M, Buch M, Schoellner C, Goebel F, Vogel M, Mueller I, Hausdorf J, Zamzow K, Schade-Brittinger C, Mueller HH. Extracorporeal shock wave therapy for plantar fasciitis: randomised controlled multicentre trial. BMJ. 2003 Jul 12;327(7406):75. doi: 10.1136/bmj.327.7406.75. PMID: 12855524; PMCID: PMC164919.
- Hawamdeh, Ziad & Alghwiri, Alia & Nassar, Aseel. (2016). The Short-Term Effect of Extracorporeal Shock Wave in Treating Plantar Fasciitis: RCT. Jordan Medical Journal. 50. 1-11. 10.12816/0025979.
- Heide M, Røe C, Mørk M, Myhre K, Brunborg C, Brox JI, Hoksrud AF. Is radial extracorporeal shock wave therapy (rESWT), sham-rESWT or a standardised exercise programme in combination with advice plus customised foot orthoses more effective than advice plus customised foot orthoses alone in the treatment of plantar fasci. Br J Sports Med. 2024 Jul 31;58(16):910-918.
- Ibrahim MI, Donatelli RA, Schmitz C, Hellman MA, Buxbaum F. Chronic plantar fasciitis treated with two sessions of radial extracorporeal shock wave therapy. Foot Ankle Int. 2010 May;31(5):391-7. doi: 10.3113/FAI.2010.0391. PMID: 20460065.
- Ibrahim MI, Donatelli RA, Hellman M, Hussein AZ, Furia JP, Schmitz C. Long-term results of radial extracorporeal shock wave treatment for chronic plantar fasciopathy: A prospective, randomized, placebo-controlled trial with two years follow-up. J Orthop Res. 2017 Jul;35(7):1532-1538. doi: 10.1002/jor.23403. Epub 2016 Sep 16. PMID: 27567022.
- Kudo P, Dainty K, Clarfield M, Coughlin L, Lavoie P, Lebrun C. Randomized, placebo-controlled, double-blind clinical trial evaluating the treatment of plantar fasciitis with an extracoporeal shockwave therapy (ESWT) device: a North American confirmatory study. J Orthop Res. 2006 Feb;24(2):115-23. doi: 10.1002/jor.20008. PMID: 16435344.
- Malay DS, Pressman MM, Assili A, Kline JT, York S, Buren B, Heyman ER, Borowsky P, LeMay C. Extracorporeal shockwave therapy versus placebo for the treatment of chronic proximal plantar fasciitis: results of a randomized, placebo-controlled, double-blinded, multicenter intervention trial. J Foot Ankle Surg. 2006 Jul-Aug;45(4):196-210. doi: 10.1053/j.jfas.2006.04.007. PMID: 16818146.
- Roerdink RL, Dietvorst M, van der Zwaard B, van der Worp H, Zwerver J. Complications of extracorporeal shockwave therapy in plantar fasciitis: Systematic review. Int J Surg. 2017 Oct;46:133-145. doi: 10.1016/j.ijsu.2017.08.587. Epub 2017 Sep 7. PMID: 28890412.
- Rompe JD, Decking J, Schoellner C, Nafe B. Shock wave application for chronic plantar fasciitis in running athletes. A prospective, randomized, placebo-controlled trial. Am J Sports Med. 2003 Mar-Apr;31(2):268-75. doi: 10.1177/03635465030310021901. PMID: 12642264.
- Şah V, Kaplan Ş, Özkan S, Adanaş C, Toprak M. Comparison between radial and focused types of extracorporeal shock-wave therapy in plantar calcaneal spur: A randomized sham-controlled trial. Phys Sportsmed. 2023 Feb;51(1):82-87. doi: 10.1080/00913847.2022.2091413. Epub 2022 Jun 21. PMID: 35713119.
- Saxena A, Fournier M, Gerdesmeyer L, Gollwitzer H. Comparison between extracorporeal shockwave therapy, placebo ESWT and endoscopic plantar fasciotomy for the treatment of chronic plantar heel pain in the athlete. Muscles Ligaments Tendons J. 2013 Jan 21;2(4):312-6. PMID: 23738317; PMCID: PMC3666533.
- Speed CA, Nichols D, Wies J, Humphreys H, Richards C, Burnet S, Hazleman BL. Extracorporeal shock wave therapy for plantar fasciitis. A double blind randomised controlled trial. J Orthop Res. 2003 Sep;21(5):937-40. doi: 10.1016/S0736-0266(03)00048-2. PMID: 12919884.
- Theodore GH, Buch M, Amendola A, Bachmann C, Fleming LL, Zingas C. Extracorporeal shock wave therapy for the treatment of plantar fasciitis. Foot Ankle Int. 2004 May;25(5):290-7. doi: 10.1177/107110070402500503. PMID: 15134608.
Risk of Bias table
|
Study reference
|
Was the allocation sequence adequately generated?
|
Was the allocation adequately concealed?
|
Blinding: Was knowledge of the allocated interventions adequately prevented? |
Was loss to follow-up (missing outcome data) infrequent?
|
Are reports of the study free of selective outcome reporting?
|
Was the study apparently free of other problems that could put it at a risk of bias?
|
Overall risk of bias If applicable/necessary, per outcome measure
|
|
Buchbinder, 2002
|
Definitely yes
Patients were randomized and stratified by treatment center (3 treatment sites) in blocks of 4 to receive either active treatment or placebo regimens according to a computer-generated random numbers list created by the study biostatistician |
definitely yes,
treatments were given by a single extracorporeal shock wave (ESW) therapist who was informed of treatment allocation (by central telephone) just prior to commencement of treatment according to the participant’s identification number. Care was taken to ensure that study participants did not meet, and individual study participants were asked to wait in separate waiting areas. |
Probably yes
Patients and the single outcome assessor were blinded; healthcare provider and data analyst were not |
Probably no,
4/85 (<5%) withdrew from placebo group, and 1/81 withdrew from ESWT group so LTFU was low, however as-treated analysis was done
|
Definitely yes,
All outcomes reported |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Haake, 2003 |
Definitely yes
Random permuted blocks of sizes six and four were used to provide each centre with a separate computer generated list of random treatment assignments |
definitely yes,
The study doctor was told by telephone what treatment had been allocated to his or her patient when the patient turned up for the first intervention
|
Probably yes
Patients and outcome assessors were blinded, study doctor and caregiver performing intervention were not |
Probably no,
8/137 (5%) withdrew from placebo group, and 8/135 withdrew from ESWT group ,so LTFU was low, however how protocol violations (receiving other treatment) were handled. Also as-treated analysis was done
|
Definitely yes,
All outcomes reported |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Speed, 2003 |
Probably yes,
Subjects were randomised using randomisation tables |
Not reported |
Probably yes
Patients and outcome assessors were blinded |
Probably yes,
4/46 ESWT group and 8/42 placebo group withdrew. Intention to treat analysis was done. |
Not reported |
Definitely yes;
Reason: No other problems noted |
Some concerns? |
|
Rompe, 2003 |
Not reported |
Probably yes,
Randomization by use of identical sealed envelopes
|
Probably yes
Patients and outcome assessors were blinded, physican performing intervention was not |
Definitely no,
High loss to follow up due to self-reported ineffective intervention in both groups. No intention to treat protocol, power not reached |
Not reported |
Probably no;
Baseline characteristics not reported |
Some concerns |
|
Theodore, 2004 |
Not reported |
Not reported |
Probably yes
Patients and outcome assessors were blinded, |
Probably yes,
Low loss to follow up but no intention to treat analysis |
Not reported |
Definitely no;
Baseline not equal between groups (gender) |
Some concerns |
|
Kudo, 2006 |
Definitely yes,
randomization scheme was generated by Biostat International, Inc., Tampa, Florida. |
Definitely yes,
Sealed, opaque, tamper-proof envelopes containing individual randomization assignments
|
Probably no,
Even though patients and outcome assessors were blinded, comparing of blinding showed a significant difference between groups (related to experienced pain) |
Probably yes,
Low loss to follow up but no intention to treat analysis |
Not reported |
Definitely yes;
Reason: No other problems noted |
Some concerns |
|
Malay, 2006 |
Definitely yes,
Randomization was determined by computer- generated random numbers separately for each study center. |
|
Probably yes
Patients and outcome assessors were blinded, physician performing intervention was not |
Probably yes,
Loss to follow up +/- 10% in both groups, but intention to treat analysis with LOCF |
Definitely yes,
All outcomes reported |
Probably no,
|
Some concerns |
|
Chow, 2007 |
Not reported |
Not reported |
Probably no,
Patients were blinded, all others not reported |
Definitely no,
LTFU was higher in control group (26%), with as treated analysis |
Not reported |
Definitely yes;
Reason: No other problems noted |
HIGH |
|
Gerdesmeyer 2008 |
Definitely yes,
allocation in permuted blocks of 4 to 8, stratified by treatment center with the use of a computer-generated random list |
Definitely yes,
Concealment of randomization was guaranteed by nontransparent envelopes. |
Probably yes,
Both patients and assessing physicians were blinded to randomization as well as to the evaluating physician. Others not reported |
definitely yes,
Loss to follow up low in both groups, and intention to treat analysis with LOCF |
Definitely yes,
All outcomes reported |
Probably no,
The study was sponsored by the manufacturer |
LOW |
|
Ibrahim, 2010/2017 |
Definitely yes,
Randomization was performed by a computerized random number generator created by an independent biostatistician |
Definitely yes,
An administrative assistant distributed interventions via opaque, sealed envelopes |
Probably yes,
Both patients and study investigators were blinded to randomization or patient records. Others not reported |
Definitely yes,
No loss to follow up |
Definitely yes,
All outcomes reported |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Saxena, 2012 |
Definitely yes,
Randomization was done by a computerized program |
Definitely yes,
Numbering was placed in sealed envelopes. A non-blinded investigator recorded the subjects’ category. |
Probably no,
Patients blinded, others not reported |
Not reported |
Not reported |
Probably no,
Potential selection bias due to surgery option |
HIGH |
|
Gollwitzer 2015 |
Definitely yes,
Randomization via permuted blocks of four to eight, stratified by treatment center, with the use of a computer-generated random list |
Definitely yes,
Concealed allocation with non-transparent envelopes |
Probably yes,
participants and evaluating physicians were blinded, treating physicians were not |
Probably yes,
Loss to follow up +/- 10% in both groups, but intention to treat analysis with LOCF |
Definitely yes,
All outcomes reported |
Probably yes,
The study was sponsored by the manufacturer, but they were not involved actively |
LOW |
|
Hawamdeh, 2016 |
Not reported |
Not reported |
Probably no,
Patients blinded, others not reported |
Definitely no,
Higher loss-to follow up in placebo group, as treated analysis |
Not reported |
Definitely yes;
Reason: No other problems noted |
HIGH |
|
Sah, 2023 |
Probably yes,
Random allocation software randomized patients in three groups by a block randomization method. Size of blocks unknown |
Not reported |
Probably yes,
participants and assessors were blinded, others not reported |
Probably yes,
Loss to follow-up was low and equal among groups, but as treated analysis |
Definitely yes,
All outcomes reported |
Definitely yes;
Reason: No other problems noted |
LOW |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Abt T, Hopfenmüller W, Mellerowicz H. Stosswellentherapie bei therapieresistenter Plantarfasziitis mit Fersensporn: eine prospektiv randomisiert plazebokontrollierte Doppelblindstudie [Shock wave therapy for recalcitrant plantar fasciitis with heel spur: a prospective randomized placebo-controlled double-blind study]. Z Orthop Ihre Grenzgeb. 2002 Sep-Oct;140(5):548-54. German. doi: 10.1055/s-2002-34001. PMID: 12226782. |
German language |
|
Akınoğlu B, Köse N. A comparison of the acute effects of radial extracorporeal shockwave therapy, ultrasound therapy, and exercise therapy in plantar fasciitis. J Exerc Rehabil. 2018 Apr 26;14(2):306-312. doi: 10.12965/jer.1836048.024. PMID: 29740568; PMCID: PMC5931170. |
Wrong control, no placebo |
|
Akinoglu B, Köse N, Kirdi N, Yakut Y. Comparison of the Acute Effect of Radial Shock Wave Therapy and Ultrasound Therapy in the Treatment of Plantar Fasciitis: A Randomized Controlled Study. Pain Med. 2017 Dec 1;18(12):2443-2452. doi: 10.1093/pm/pnx113. PMID: 28575496. |
Double study |
|
Alvarez RG, Ogden JA, Jaakkola J, Cross GL. Symptom duration of plantar fasciitis and the effectiveness of Orthotripsy. Foot Ankle Int. 2003 Dec;24(12):916-21. doi: 10.1177/107110070302401208. PMID: 14733347. |
study limitations, unblinded FDA study
|
|
Aqil A, Siddiqui MR, Solan M, Redfern DJ, Gulati V, Cobb JP. Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: a meta-analysis of RCTs. Clin Orthop Relat Res. 2013 Nov;471(11):3645-52. doi: 10.1007/s11999-013-3132-2. Epub 2013 Jun 28. PMID: 23813184; PMCID: PMC3792262. |
Too few studies included |
|
Babatunde OO, Legha A, Littlewood C, Chesterton LS, Thomas MJ, Menz HB, van der Windt D, Roddy E. Comparative effectiveness of treatment options for plantar heel pain: a systematic review with network meta-analysis. Br J Sports Med. 2019 Feb;53(3):182-194. doi: 10.1136/bjsports-2017-098998. Epub 2018 Jun 28. PMID: 29954828. |
Reporting of search strategy insufficient |
|
Böddeker R, Schäfer H, Haake M. Extracorporeal shockwave therapy (ESWT) in the treatment of plantar fasciitis--a biometrical review. Clin Rheumatol. 2001;20(5):324-30. doi: 10.1007/pl00011207. PMID: 11642513. |
Only includes risk of bias analysis |
|
Boob MA Jr, Phansopkar P, Somaiya KJ. Physiotherapeutic Interventions for Individuals Suffering From Plantar Fasciitis: A Systematic Review. Cureus. 2023 Jul 31;15(7):e42740. doi: 10.7759/cureus.42740. PMID: 37654968; PMCID: PMC10467524. |
Wrong intervention |
|
Buch M, Knorr U, Fleming L, Theodore G, Amendola A, Bachmann C, Zingas C, Siebert WE. Extrakorporale Stosswellentherapie beim symptomatischen Fersensporn. Eine Ubersicht [Extracorporeal shockwave therapy in symptomatic heel spurs. An overview]. Orthopade. 2002 Jul;31(7):637-44. German. doi: 10.1007/s00132-002-0323-z. PMID: 12219661. |
German language |
|
Caglar Okur, Sibel & Aydın, Abdulkadir. (2019). Comparison of extracorporeal shock wave therapy with custom foot orthotics in plantar fasciitis treatment: A prospective randomized one-year follow-up study. Journal of musculoskeletal & neuronal interactions. 19. 178-186. |
Wrong comparison |
|
Chang KV, Chen SY, Chen WS, Tu YK, Chien KL. Comparative effectiveness of focused shock wave therapy of different intensity levels and radial shock wave therapy for treating plantar fasciitis: a systematic review and network meta-analysis. Arch Phys Med Rehabil. 2012 Jul;93(7):1259-68. doi: 10.1016/j.apmr.2012.02.023. Epub 2012 Mar 12. PMID: 22421623. |
Search strategy insufficient |
|
Charles R, Fang L, Zhu R, Wang J. The effectiveness of shockwave therapy on patellar tendinopathy, Achilles tendinopathy, and plantar fasciitis: a systematic review and meta-analysis. Front Immunol. 2023 Aug 16;14:1193835. doi: 10.3389/fimmu.2023.1193835. PMID: 37662911; PMCID: PMC10468604. |
Reporting of search strategy insufficient |
|
Chen CM, Lee M, Lin CH, Chang CH, Lin CH. Comparative efficacy of corticosteroid injection and non-invasive treatments for plantar fasciitis: a systematic review and meta-analysis. Sci Rep. 2018 Mar 5;8(1):4033. doi: 10.1038/s41598-018-22402-w. PMID: 29507320; PMCID: PMC5838257. |
Wrong comparison |
|
Chew KT, Leong D, Lin CY, Lim KK, Tan B. Comparison of autologous conditioned plasma injection, extracorporeal shockwave therapy, and conventional treatment for plantar fasciitis: a randomized trial. PM R. 2013 Dec;5(12):1035-43. doi: 10.1016/j.pmrj.2013.08.590. Epub 2013 Aug 22. PMID: 23973504. |
No placebo as control, solely conventional treatment, thus wrong control |
|
Cinar E, Saxena S, Akkurt HE, Uygur F. Extracorporeal shockwave therapy in the management of plantar fasciitis: A randomized controlled trial. Foot (Edinb). 2020 Sep;44:101679. doi: 10.1016/j.foot.2020.101679. Epub 2020 Jul 13. PMID: 32674009. |
Wrong comparison |
|
Cinar E, Saxena S, Uygur F. Combination Therapy Versus Exercise and Orthotic Support in the Management of Pain in Plantar Fasciitis: A Randomized Controlled Trial. Foot Ankle Int. 2018 Apr;39(4):406-414. doi: 10.1177/1071100717747590. Epub 2018 Jan 12. PMID: 29327602. |
Same study population as Cinar 2020 |
|
Cosentino R, Falsetti P, Manca S, De Stefano R, Frati E, Frediani B, Baldi F, Selvi E, Marcolongo R. Efficacy of extracorporeal shock wave treatment in calcaneal enthesophytosis. Ann Rheum Dis. 2001 Nov;60(11):1064-7. doi: 10.1136/ard.60.11.1064. PMID: 11602481; PMCID: PMC1753417. |
study limitations: no limiting of-or correction for other concurrent interventions |
|
Crawford F, Thomson C. Interventions for treating plantar heel pain. Cochrane Database Syst Rev. 2003;(3):CD000416. doi: 10.1002/14651858.CD000416. Update in: Cochrane Database Syst Rev. 2010 Jan 20;(1):CD000416. doi: 10.1002/14651858.CD000416.pub2. PMID: 12917892. |
More interventions, no meta-analysis |
|
Díaz López AM, Guzmán Carrasco P. Efectividad de distintas terapias físicas en el tratamiento conservador de la fascitis plantar: revisión sistemática [Effectiveness of different physical therapy in conservative treatment of plantar fasciitis: systematic review]. Rev Esp Salud Publica. 2014 Jan-Feb;88(1):157-78. Spanish. doi: 10.4321/S1135-57272014000100010. PMID: 24728397. |
Spanish language |
|
Dizon JN, Gonzalez-Suarez C, Zamora MT, Gambito ED. Effectiveness of extracorporeal shock wave therapy in chronic plantar fasciitis: a meta-analysis. Am J Phys Med Rehabil. 2013 Jul;92(7):606-20. doi: 10.1097/PHM.0b013e31828cd42b. PMID: 23552334. |
Reporting of search strategy insufficient |
|
|
|
|
Gollwitzer H, Diehl P, von Korff A, Rahlfs VW, Gerdesmeyer L. Extracorporeal shock wave therapy for chronic painful heel syndrome: a prospective, double blind, randomized trial assessing the efficacy of a new electromagnetic shock wave device. J Foot Ankle Surg. 2007 Sep-Oct;46(5):348-57. doi: 10.1053/j.jfas.2007.05.011. PMID: 17761319. |
Due to lack of reporting of results |
|
Grecco MV, Brech GC, Greve JM. One-year treatment follow-up of plantar fasciitis: radial shockwaves vs. conventional physiotherapy. Clinics (Sao Paulo). 2013;68(8):1089-95. doi: 10.6061/clinics/2013(08)05. PMID: 24037003; PMCID: PMC3752632. |
Wrong comparison |
|
Greve JM, Grecco MV, Santos-Silva PR. Comparison of radial shockwaves and conventional physiotherapy for treating plantar fasciitis. Clinics (Sao Paulo). 2009;64(2):97-103. doi: 10.1590/s1807-59322009000200006. PMID: 19219314; PMCID: PMC2666476. |
Wrong comparison |
|
Guimarães JS, Arcanjo FL, Leporace G, Metsavaht LF, Conceição CS, Moreno MVMG, Vieira TEM, Moraes CC, Gomes Neto M. Effects of therapeutic interventions on pain due to plantar fasciitis: A systematic review and meta-analysis. Clin Rehabil. 2023 Jun;37(6):727-746. doi: 10.1177/02692155221143865. Epub 2022 Dec 26. PMID: 36571559. |
Reporting of search strategy insufficient |
|
Badil Güloğlu S, Yalçın Ü. Comparison of effects of low-level laser therapy and extracorporeal shock wave therapy in calcaneal spur treatment: A prospective, randomized, clinical study. Turk J Phys Med Rehabil. 2021 May 25;67(2):218-224. doi: 10.5606/tftrd.2021.5260. PMID: 34396073; PMCID: PMC8343161. |
Wrong comparison |
|
Hammer DS, Rupp S, Kreutz A, Pape D, Kohn D, Seil R. Extracorporeal shockwave therapy (ESWT) in patients with chronic proximal plantar fasciitis. Foot Ankle Int. 2002 Apr;23(4):309-13. doi: 10.1177/107110070202300403. PMID: 11991475. |
Wrong comparison |
|
Hammer DS, Adam F, Kreutz A, Kohn D, Seil R. Extracorporeal shock wave therapy (ESWT) in patients with chronic proximal plantar fasciitis: a 2-year follow-up. Foot Ankle Int. 2003 Nov;24(11):823-8. doi: 10.1177/107110070302401103. PMID: 14655885. |
Wrong comparison |
|
Ho C. Extracorporeal shock wave treatment for chronic plantar fasciitis (heel pain). Issues Emerg Health Technol. 2007 Jan;(96 (part 1)):1-4. PMID: 17302019. |
Wrong study design |
|
Hsiao MY, Hung CY, Chang KV, Chien KL, Tu YK, Wang TG. Comparative effectiveness of autologous blood-derived products, shock-wave therapy and corticosteroids for treatment of plantar fasciitis: a network meta-analysis. Rheumatology (Oxford). 2015 Sep;54(9):1735-43. doi: 10.1093/rheumatology/kev010. Epub 2015 Apr 6. PMID: 25848072. |
Wrong intervention |
|
Küçükakkaş, Okan & Öz, Beyzanur & Koçyiğit, H.. (2017). Efficacy of different doses of radial extracorporeal shock wave therapy in patients with painful calcaneal spur. Turkiye Fiziksel Tip ve Rehabilitasyon Dergisi. 63. 31-41. 10.5606/tftrd.2017.23590. |
Turkish language |
|
Landorf KB. Plantar heel pain and plantar fasciitis. BMJ Clin Evid. 2015 Nov 25;2015:1111. PMID: 26609884; PMCID: PMC4661045. |
No risk of bias analysis |
|
Landorf KB, Menz HB. Plantar heel pain and fasciitis. BMJ Clin Evid. 2008 Feb 5;2008:1111. PMID: 19450330; PMCID: PMC2907928. |
Old version of Landorf 2015 |
|
Pisirici P, Cil ET, Coskunsu DK, Saylı U, Subasi F. Extracorporeal Shockwave Therapy Versus Graston Instrument-Assisted Soft-Tissue Mobilization in Chronic Plantar Heel Pain: A Randomized Controlled Trial. J Am Podiatr Med Assoc. 2022 Nov-Dec;112(6):21-036. doi: 10.7547/21-036. PMID: 36125974. |
Wrong control, no placebo |
|
Vahdatpour B, Sajadieh S, Bateni V, Karami M, Sajjadieh H. Extracorporeal shock wave therapy in patients with plantar fasciitis. A randomized, placebo-controlled trial with ultrasonographic and subjective outcome assessments. J Res Med Sci. 2012 Sep;17(9):834-8. PMID: 23826009; PMCID: PMC3697207. |
Conflicting results reported within article |
|
Zhiyun L, Tao J, Zengwu S. Meta-analysis of high-energy extracorporeal shock wave therapy in recalcitrant plantar fasciitis. Swiss Med Wkly. 2013 Jul 7;143:w13825. doi: 10.4414/smw.2013.13825. PMID: 23832373. |
No search strategy reported |
Beoordelingsdatum en geldigheid
Publicatiedatum : 17-02-2026
Beoordeeld op geldigheid : 17-02-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire werkgroep samengesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met fasciopathie plantaris.
Werkgroep
- Dhr. prof. dr. Fred Hartgens (voorzitter), sportarts, namens de Vereniging voor Sportgeneeskunde (VSG)
- Dhr. dr. Bernard te Boekhorst, sportarts, namens de VSG
- Dhr. drs. Daan Gelsing, extended scope specialist, echografist en manueel therapeut, namens de Nederlandse Vereniging voor Manuele Therapie en het Koninklijk Nederlands Genootschap voor Fysiotherapie (NVMT/KNGF)
- Dhr. drs. David Hanff, radioloog, namens de Nederlandse Vereniging voor Radiologie (NVvR)
- Dhr. dr. Eric Bakker, fysiotherapeut en klinisch epidemioloog, namens het Koninklijk Nederlands Genootschap voor Fysiotherapie (KNGF)
- Mevr. drs. Eva Hoefnagels, orthopedisch chirurg, namens de Nederlandse Orthopaedische Vereniging (NOV)
- Mevr. drs. Inge Koetser, radioloog, namens de NVvR
- Mevr. drs. Kayleigh van Amelsfort, podotherapeut en gezondheidswetenschapper, namens de Nederlandse Vereniging voor Podotherapeuten (NVvP)
- Dhr. drs. Niek Vink, fysiotherapeut en fysiotherapiewetenschapper, namens de KNGF
- Dhr. dr. Robert-Jan de Vos, sportarts, namens de VSG
- Dhr. drs. Thomas Eggen, orthopedisch chirurg, namens de NOV
Klankbordgroep
- Dhr. dr. Dorus Fennis, neuroloog, namens de Nederlandse Vereniging voor Neurologie (NVN)
- Dhr. dr. Florus van der Giesen, physician assistant reumatologie, namens de Nederlandse Vereniging voor Reumatologie (NVR)
- Mevr. drs. Juliette Starmans, AIOS bedrijfsgeneeskunde en orthopedisch chirurg, namens de Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (NVAB)
- Mevr. drs. Lisette de Graauw, register podoloog, namens Stichting LOOP
Met ondersteuning van
- Mevr. drs. Beatrix Vogelaar, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. drs. Isabelle Laseur, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel Gemelde (neven)functies en belangen werkgroep
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Fred Hartgens (voorzitter) |
Hoofd Afdeling Sportgeneeskunde en Hoogleraar Klinische Sportgeneeskunde in UMC Utrecht (0,8 fte) |
Op free lance basis praktiserend sportarts in Zuid-Limburg en sportarts-docent voor andere organisaties (in totaal 10-15 uur per maand) VSG vertegenwoordiger bij FMS Raad Wetenschap & Innovatie Lid van Werkgroep Herziening Kennisagenda VSG VSG vertegenwoordiger in SKMS Beweeg Alliantie |
UTC lmaging B.V: The effects of tendinopathy and reliability of hamstrings Ultrasiund Tissue Characterisation (UTC) echo types - geen projectleidersrol BioActor B.V. : The Effect of a Citrus and Pomegranate Complex on Physical Fitness and Mental Well-Being in Healthy Elde a Randomized Placebo controlled Trial - geen projectleidersrol
Allebei afgerond |
Geen restricties |
|
Bernard te Boekhorst |
SMA sportarts middennederland |
- |
- |
Geen restricties |
|
Daan Gelsing |
Echo On The Spot - eigenaar, MSK-echografist Rembrandt fysiotherapie - echografist en manueel therapeut Echo On The Spot - het uitvoeren van echografisch diagnostisch onderzoek in de eerstelijns zorg. Rembrandt fysiotherapie - fysiotherapeutische zorg. |
Geven van mini-klinieken en examinator aan de SOMT University |
|
Geen restricties |
|
Eric Bakker |
Epidemioloog(B) master EBPiHC, Amsterdam UMC locatie AMC, Amsterdam 0,3 FtE. Onderwijs en begeleidingen onderzoek van de studenten epidemiologie. Betaald
|
Eigenaar wetenschappelijk adviesbureau KOKD.nl. Betaald. Niet over onderwerpen in de richtlijn |
|
Geen restricties |
|
Eva Hoefnagels
|
Sint maartenskliniek orthopedisch chirurg betaald |
Voorzitter nederlandse voet en enkel vereniging (onbetaald) |
Promotie onderzoek fasciitis plantaris, onderzoek is afgerond en data al verwerkt, dit onderzoek heeft geen invloed op de data Bestuur Nederlandse voet en enkelvereniging. Uitkomst onderzoek heeft geen invloed op mijn functie daar. Promotieonderzoek lopend, geen financier. Publicaties sinds 2019: - PAPPI: Personalized analysis of plantar pressure images using statistical modelling and parametric mapping - The effect of lengthening the gastrocnemius muscle in chronic therapy resistant plantar fasciitis
Promotie onderzoek over operatieve behandeling bij chronische fasciitis plantaris. Is al begonnen in 2017 en data zijn al verzameld tot 2020. Voor de start van deze richtlijn. De data van mijn onderzoek is niet van invloed voor de richtlijn en de uitkomst van de richtlijn niet voor het onderzoek. Mijn onderzoeks data zijn niet gebruikt voor de richtlijn. |
Geen restricties |
|
Inge Koetser
|
Radioloog, Reade |
GAIA commissie
|
- |
Geen restricties |
|
Kayleigh van Amelsfort
|
Podotherapeut, Podotherapie Inka (betaald, 20 uur) |
Bestuurslid Wetenschap & Vakinhoud, Nederlandse Vereniging van Podotherapeuten (betaald, 10 uur) |
- |
Geen restricties |
|
Niek Vink |
Manager en docent Nationaal Trainingscentrum voor echografie (NT-e) |
Manager van het opleidingscentrum NT-e. Hier worden post-HBO opleidingen gegeven in echografie, shockwave therapie en percutane electrolyse (ook bij plantaire hielpijnklachten). Ik geef een dag in de week les binnen de opleidingen voor echografie. Het NT-e is onderdeel van Fyzzio International BV. Fyzzio verkoopt apparatuur voor bovenvermelde activiteiten. Ik ben bij het NT-e in loondienst, heb geen aandelen in het bedrijf en krijg ook geen bonussen. Ik heb geen financiële belangen bij een bepaalde uitkomst van de richtlijn. |
- |
Geen restricties |
|
Robert-Jan de Vos |
Sportarts en Universitair Hoofddocent, Erasmus MC Universitair Medisch Centrum Rotterdam (0.8 fte) |
Consulent SBV Excelsior Rotterdam (onbetaald). Associate editor British Journal of Sports Medicine (onbetaald). Voorzitter multidisciplinaire richtlijn achilles tendinopathie (onbetaald). Werkgroeplid multidisciplinaire richtlijn achillespeesruptuur (onbetaald). Werkgroeplid Kennisagenda VSG 2023 (onbetaald). Werkgroeplid SKMS richtlijnen commissie (betaald). |
In de afgelopen 5 jaar zijn er onderzoeksprojecten uitgevoerd onder mijn supervisie die zijn gefinancierd door ReumaNederland, Annafonds, ZonMw, GE Healthcare, de National Basketball Association (NBA), het Trustfonds en de Erasmus MC Foundation. Deze financiers hebben echter geen belangen bij de aanbevelingen die zullen worden gedaan in deze richtlijn. Ik heb een consultancy functie voor een project naar nieuwe injectie behandeling voor Achilles tendinopathie, gesponsord door Novartis (2021), dit raakt niet aan het onderwerp van de richtlijn. Tevens is deze injectie behandeling nog niet ontwikkeld voor de huidige klinische zorg en daardoor zal deze ook niet in de richtlijn kunnen worden behandeld. Daarnaast is de consultancy functie eenmalig geweest en niet meer actief, en inkomsten zijn voor de instelling waarin ik werk en niet voor persoonlijke doeleinden). Op dit moment is er geen commercieel gefinancieerd onderzoek dat loopt onder mijn leiding. Ik ben aan het oriënteren met Causeway Therapeutics of we een onderzoek gaan opstarten met een nieuwe injectable voor epicondylaire tendinopthie, maar ook daarvoor geldt dat het niet direct zal zijn gerelateerd aan fasciopathie plantaris. Het is niet mijn verwachting dat dit leidt tot belangenverstrengeling.
In de afgelopen 5 jaar zijn er onderzoeksprojecten uitgevoerd onder mijn supervisie die zijn gefinancierd door HORIZON MSCA, ReumaNederland, Annafonds, ZonMw, GE Healthcare, de National Basketball Association (NBA), het Trustfonds en de Erasmus MC Foundation. Deze financiers hebben echter geen belangen bij de aanbevelingen die worden gedaan in deze richtlijn. Ik heb een consultancy functie gehad voor een project naar nieuwe injectie behandeling voor Achilles tendinopathie (Novartis, 2021) en laterale epicondylaire tendinopathie (Causeway therapeutics. 2025). Dit raakt niet aan het onderwerp van de richtlijn. Tevens zijn deze injectie behandelingen nog niet ontwikkeld voor de huidige klinische zorg en daardoor worden deze behandelingen ook niet in de richtlijn behandeld. Daarnaast zijn deze consultancy functies eenmalig geweest en niet meer actief, en inkomsten zijn voor de instelling waarin ik werk en niet voor persoonlijke doeleinden).
Op dit moment is er geen commercieel gefinancierd onderzoek dat loopt onder mijn leiding. HORIZON MSCA Postdoctoral Fellowship – Identifying Predictive factors for the Recovery of Achilles Tendinopathy (PReAcT trial) NWO / ReumaNederland – The State of the Cartilage (START project) ReumaNederland / Annafonds – High-Volume injectie Achilles tendinopathie (HAT trial) ZonMW – Preventie hardloopblessures (INSPIRE trial en SPRINT trial) GE Healthcare / NBA – Oefentherapie Patella tendinopathie (JUMPER trial) Trustfonds / Erasmus MC Foundation – Normwaarden echografie achillespezen (REVEAL trial) Causeway therapeutics – Consultancy voor trial nieuwe injectable laterale epicondylaire tendinopathie Novartis – Consultancy voor trial nieuwe injectable achilles tendinopathie |
Geen restricties |
|
Thomas Eggen |
Orthopedisch chirurg Canisius Wilhelmina Ziekenhuis |
Dagvoorzitter NOV en LVO congressen Orthopedisch consultant op KNMG carriere beurs Mede-oprichter BotCast orthopedische podcast (educatief/informatief). Mogelijke tegemoetkoming vanuit Orlymedia BV (sponsor kan farmaceut zijn). |
- |
Geen restricties |
|
David Hanff |
Voorzitter van de MSK sectie Nederlandse Vereniging voor Radiologie |
Nederlandse Vereniging voor Radiologie |
- |
Geen restricties |
|
Dorus Fennis (klankbordgroep) |
Geen werkgever maar vrijgevestigd meidsch specialist bij Cooperatie Medische Staf St Jansdal UA |
- |
- |
Geen restricties |
|
Juliëtte Starmans (klankbordgroep) |
AIOS bedrijfsgeneeskunde. Ik werk als ZZP’er en ben aldus aangesloten bij Immediator. Tijdens mijn opleiding ben ik werkzaam bij een klant, waar ik betaalde werkzaamheden verricht. |
Naast AIOS bedrijfsgeneeskunde ben ik werkzaam als orthopedisch chirurg. In deze hoedanigheid werk ik eveneens als ZZP’er in mijn éénmansbedrijf: Starmans orthopedische expertises. Via dit bedrijf verricht ik orthopedische expertises voor verzekeringen. Tevens ben ik via dit bedrijf als medisch adviseur werkzaam voor Medisch Advies Bureau. Alle werkzaamheden voor Starmans orthopedische expertises zijn betaalde werkzaamheden. |
- |
Geen restricties |
|
Florus van der Giesen (klankbordgroep) |
Physician assistant reumatologie |
- |
- |
Geen restricties |
|
Lisette de Graauw (klankbordgroep) |
Zorgverlener in zowel de eerste als tweede lijngezondheidszorg.
|
- |
Ik werk in de voetzorg, dus ja, als blijkt dat de uitkomsten van de richtlijn laten zien dat de door mijn beroepsgroep geleverde zorg werkt, dan heb ik (en mijn beroepsgroep) daar voordeel bij. |
Geen restricties |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door de Patiëntenfederatie Nederland te betrekken in de klankbordgroep-fase. De verkregen input is meegenomen bij het opstellen van de overwegingen (zie kop “Waarden en voorkeuren van patiënten”). De conceptrichtlijn is tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Shockwave therapie |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (5.000- 40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Fasciopathie Plantaris - UV6 Shockwavetherapie |
|
|
Uitgangsvraag/modules: Wat is de plaats van shockwavetherapie bij de behandeling bij patiënten met fasciopathie plantaris? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 28-3-2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
Rayyan review: https://rayyan.ai/reviews/979942 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen fasciopathie plantaris EN shockwavetherapie.
→ De volgende sleutelartikelen worden gevonden met deze search:
|
|
|
Te gebruiken voor richtlijntekst: In de databases Embase.com en Ovid/Medline is op 28 maart 2024 systematisch gezocht naar systematische reviews en RCTs over de plaats van shockwavetherapie bij de behandeling bij patiënten met fasciopathie plantaris. De literatuurzoekactie leverde 278 unieke treffers op. |
|
Zoekopbrengst - 28 maart 2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
89 |
74 |
104 |
|
RCT |
164 |
123 |
174 |
|
|
|
|
|
|
Totaal |
253 |
197 |
278* |
*in Rayyan
Zoekstrategie - 28 maart 2024
Embase.com
|
No. |
Query |
Results |
|
#1 |
'plantar fasciitis'/exp OR 'plantar fasciopathy'/exp OR 'heel spur'/exp OR 'policeman heel'/exp OR (((calcane* OR heel* OR subcalcane*) NEAR/3 (spur* OR exostos* OR pain* OR policeman* OR jogger*)):ti,ab,kw) OR ((plant* NEAR/3 (fasciitis OR fasciopath* OR fascios* OR inflam*)):ti,ab,kw) OR (((baxter* OR plant* OR calcane* OR heel) NEAR/3 neuropath*):ti,ab,kw) OR calcaneodyn*:ti,ab,kw OR 'calcane* periostitis':ti,ab,kw |
6372 |
|
#2 |
'shock wave'/exp OR 'shock wave therapy'/exp OR 'ultrasound therapy'/exp OR 'radiation'/exp OR ((('non ioniz*' OR 'nonioniz*') NEAR/3 radiat*):ti,ab,kw) OR (((extracorporeal OR radial) NEAR/3 shock*):ti,ab,kw) OR 'shock wave*':ti,ab,kw OR 'shockwave*':ti,ab,kw OR eswt:ti,ab,kw OR hesw:ti,ab,kw OR ecst:ti,ab,kw OR ecsw:ti,ab,kw |
857465 |
|
#3 |
#1 AND #2 |
790 |
|
#4 |
#3 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
543 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1014761 |
|
#6 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
2178974 |
|
#7 |
#4 AND #5 – SR’s |
89 |
|
#8 |
#4 AND #6 NOT #7 – SR’s |
164 |
|
#9 |
#7 OR #8 |
253 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Fasciitis, Plantar/ or exp Heel Spur/ or ((calcane* or heel* or subcalcane*) adj3 (spur* or exostos* or pain* or policeman* or jogger*)).ti,ab,kf. or (plant* adj3 (fasciitis or fasciopath* or fascios* or inflam*)).ti,ab,kf. or ((baxter* or plant* or calcane* or heel) adj3 neuropath*).ti,ab,kf. or calcaneodyn*.ti,ab,kf. or calcane* periostitis.ti,ab,kf. |
4416 |
|
2 |
exp Extracorporeal Shockwave Therapy/ or exp Radiation, Nonionizing/ or exp Ultrasonic Therapy/ or ((non ioniz* or nonioniz*) adj3 radiat*).ti,ab,kf. or ((extracorporeal or radial) adj3 shock*).ti,ab,kf. or shock wave*.ti,ab,kf. or shockwave*.ti,ab,kf. or eswt.ti,ab,kf. or hesw.ti,ab,kf. or ecst.ti,ab,kf. or ecsw.ti,ab,kf. |
338029 |
|
3 |
1 and 2 |
440 |
|
4 |
limit 3 to yr="2000 -Current" |
419 |
|
5 |
4 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
377 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
735289 |
|
7 |
exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf. |
1700385 |
|
8 |
5 and 6 – SR’s |
74 |
|
9 |
(5 and 7) not 8 – RCT’s |
123 |
|
10 |
8 or 9 |
197 |