Preventie verplichte zorg in de ggz
Uitgangsvraag
Welke preventiestrategie is effectief in het voorkomen van verplichte zorg?
Aanbeveling
- Maak een duidelijke keuze voor een preventiestrategie en zorg dat deze in alle lagen van de organisatie wordt onderschreven.
- Zorg voor een gedegen implementatie van de gekozen preventiestrategie. Tijdens de implementatie moeten centrale en decentrale verandering van de organisatiecultuur, attitude van het personeel en de werkwijze bij crisissituaties centraal staan. Borging van preventie ontstaat alleen doordat een strategie intensief wordt gebruikt en door alle lagen van de organisatie wordt onderschreven. Bij implementatie is het belangrijk om aandacht te hebben voor (kwetsbare) minderheidsgroepen.
- Betrek, naast alle betrokken zorgprofessionals en ketenpartners uit het sociaal domein, cliëntenraden, naastbetrokkenenraden, patiënten en hun naasten actief bij het selecteren, implementeren en uitvoeren van preventiestrategieën voor verplichte zorg op team-, afdelings- of organisatieniveau.
- Faciliteer educatie en/of training voor alle zorgprofessionals die in aanraking komen met crisissituaties in de-escalerend werken, herstelondersteunende zorg en vroegsignalering van (dreigende) escalatie.
- Overweeg om ten behoeve van preventie van verplichte opnames één of meerdere van de volgende strategieën toe te passen:
- Geïntegreerde, intensieve ambulante zorg bij patiënten in een (dreigende) psychiatrische crisis, zoals door middel van bemoeizorg, Intensive Home Treatment en Peer Supported Open Dialogue;
- Optimaal en intensief gebruik van de beschikbare (al dan niet verplichte) eigen regie instrumenten, zoals WRAP, het crisisplan, de crisiskaart, het signaleringsplan en de wettelijke instrumenten de zorgkaart, het eigen plan van aanpak en de zelfbindingsverklaring;
- Interventies gericht op het gedrag van de patiënt, zoals psycho-educatie, motiverende gespreksvoering, inzet van (familie-)ervaringsdeskundigen en intensief triadisch werken.
- Overweeg om ten behoeve van preventie van verplichte zorg in de intramurale setting om één of meerdere van de volgende strategieën toe te passen:
- Interventiemodellen die gericht zijn op cultuur- en organisatieverandering, waarbij contact maken met patiënten, gelijkwaardigheid en een herstelgerichte benadering centraal staan, zoals High Intensive Care, Herstelondersteunende Zorg, Safewards, Six Core Strategies en Open Door Policy;
- Kortdurende, gestructureerde vroegsignalering van ongewenst of gevaarlijk gedrag, bijvoorbeeld door middel van START of de Crisismonitor.
Overwegingen
De overwegingen en aanbevelingen in deze module zijn gebaseerd op twee afzonderlijk uitgewerkte uitgangsvragen (met bijbehorende PICO’s), die ieder ondersteund worden door een systematische literatuursearch (zie Samenvatting literatuur). Omdat de inhoudelijke overwegingen grotendeels overlappen, zijn deze in de tekst geïntegreerd en niet strikt per uitgangsvraag gescheiden weergegeven.
Kwaliteit van bewijs
Deze module evalueert de effectiviteit van preventiestrategieën in het voorkomen van verplichte zorg. Er is systematisch gezocht in de literatuur om de effectiviteit van preventiestrategieën te evalueren. Er werden in totaal vier systematische reviews en zes RCT’s opgenomen in de literatuursamenvatting.
De overall kwaliteit van bewijs is zeer laag. Dit betekent dat we zeer onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten. Er is afgewaardeerd vanwege (zeer) ernstige:
- Risk of Bias: methodologische beperkingen (ontbrekende informatie over de randomisatie procedure, ontoereikende randomisatie, ontbrekende uitkomstdata, onduidelijk risico op bias door gebrek aan blindering en selectieve rapportage van uitkomstdata).
- Inconsistentie: inconsistentie van de resultaten.
- Indirectheid: indirectheid van het bewijs, door verschillen in populatie.
- Imprecisie: onnauwkeurigheid (brede betrouwbaarheidsintervallen), en het ontbreken van spreidingsmaten waardoor het niet mogelijk is om effectmaten te berekenen.
Balans tussen gewenste en ongewenste effecten
Het Verdiepingsonderzoek Uitvoering Wvggz: goede voorbeelden uit de praktijk (Plomp, 2024, hierna: Verdiepingsonderzoek)) biedt een gedetailleerd overzicht van preventieve interventies voor de praktijk. Naast een juridische evaluatie geeft het handvatten in de vorm van best practices uit de GGZ in Nederland. De focus van het verdiepingsonderzoek ligt daarbij niet op klinisch bewezen effectiviteit, maar op positieve ervaringen in de praktijk. Het stimuleert daarbij dat organisaties leren van elkaar en successen delen. Er bestaan diverse parellellen tussen de interventies die worden genoemd in het Verdiepingsonderzoek en de interventies die worden genoemd in de wetenschappelijke literatuur. Zo pleiten de auteurs van het Verdiepingsonderzoek onder andere voor het gebruik van bemoeizorg en drang ter preventie van verplichte zorg. Hoewel deze termen vaak niet expliciet in de internationale literatuur worden genoemd, hebben modellen voor intensieve en geïntegreerde ambulante zorg veel elementen in zich die in de Nederlandse situatie als bemoeizorg, outreachende zorg of drang worden gedefinieerd.
Veel patiënten die te maken krijgen met een psychiatrische crisis ervaren ook problemen in het sociaal domein, zoals schuldenproblematiek of gebrek aan huisvesting. Hoewel er geen wetenschappelijk bewijs hiervoor is gevonden, wijst de praktijk uit dat het oplossen of verlichten van dergelijke problemen een substantiële bijdrage kunnen leveren aan het voorkomen van verplichte zorg. Eigen regie instrumenten kunnen hier ook een waardevolle rol in spelen. Dit pleit voor een geïntegreerde benadering van de GGZ met partners uit het sociaal domein om patiënten te ondersteunen in alle levensgebieden om verplichte zorg te voorkomen.
Het resultaat van het literatuuronderzoek beweegt langs twee lijnen, namelijk interventies om gedwongen opname te voorkomen en interventies om verplichte zorg tijdens gedwongen opname te voorkomen, zoals insluiting, fixatie en gedwongen medicatietoediening. Hoewel er enige overlap bestaat tussen de interventies beschrijft de werkgroep de resultaten op basis van die twee categorieën.
Verplichte opname
Ten aanzien van verplichte opname keek de werkgroep naar de invloed van preventiestrategieën voor verplichte opname en de duur van verplichte opnames. In de literatuur worden diverse interventies genoemd, namelijk eigen regie instrumenten (advance directives, crisisplannen, signaleringsplannen etc.), community treatment orders (CTO, ambulante verplichte zorg volgens Brits model), intensieve ambulante zorg (zoals intensive home treatment), financiële incentives, geïntegreerde zorg (een multimodale interventie gebaseerd op het ACT-model), ondersteuning bij therapietrouw en psycho-educatie. Verplichte medicatie in de ambulante setting wordt door de werkgroep niet beschreven in relatie tot preventie van verplichte opname. Dit valt binnen de kaders van de uitvoering en evaluatie van ambulante verplichte zorg, zoals beschreven in module Ambulant verplichte zorg.
Eigen regie instrumenten blijken voor een klinisch relevante afname te zorgen van het aantal verplichte opnames. Over de invloed op de duur van verplichte opnames wordt door een beperkt aantal studies wisselend gerapporteerd (i.e. een afname van de duur versus geen noemenswaardig effect). Er zijn diverse eigen regie instrumenten beschikbaar, waarvan het eigen plan van aanpak, de zorgkaart en de zelfbindingsverklaring in de Wvggz zijn opgenomen. Voorbeelden van eigen regie instrumenten die niet in de wet staan vermeld, maar die in de praktijk veel gebruikt worden zijn het signaleringsplan, het crisisplan (al of niet in combinatie met de crisiskaart) en het Wellness and Recovery Action Plan (WRAP). Deze instrumenten zijn onderwerp van een kwaliteitsverbeteringsproject van de Stichting PVP en MIND om het gebruik hiervan te bevorderen en verbeteren (Molenaar, 2025):
•Eigen plan van aanpak
Het eigen plan van aanpak geeft patiënten de mogelijkheid om tijdens de aanvraagprocedure van een zorgmachtiging te komen met een eigen plan om het (vermeende) ernstig nadeel af te wenden zonder een zorgmachtiging. Ook de rechter kan de patiënt nog de gelegenheid geven een eigen plan van aanpak te maken. Als de geneesheer-directeur akkoord gaat met de inhoud van het eigen plan van aanpak wordt de aanvraag zorgmachtiging beëindigd.
•Zorgkaart
In de zorgkaart worden wensen en voorkeuren van de patiënt vastgelegd over (al dan niet verplichte) zorg. De zorgverlener is verplicht in het zorgplan te vermelden op welke manier rekening wordt gehouden met de wensen en voorkeuren van de patiënt. Hiermee wordt niet alleen preventie van verplichte opname beoogd, maar ook preventie van verplichte zorg in de intramurale setting.
•Zelfbindingsverklaring
In een zelfbindingsverklaring maakt de patiënt met diens behandelaar bindende afspraken over de omstandigheden waarbij (al dan niet verplicht) gehandeld kan worden om ernstig nadeel te voorkomen. Wanneer de geneesheer-directeur deze bekrachtigt kan, als dat nodig is, verplichte zorg in een versnelde procedure worden aangevraagd bij de rechter. De zelfbindingsverklaring komt het dichtst in de buurt van wat de Engelstalige literatuur definieert als een "advance directive".
•Signaleringsplan
In het signaleringsplan legt de patiënt, samen met diens naasten en behandelaren, vast hoe het met de patiënt gaat in goeden doen en wat signalen en symptomen zijn van verslechtering. Daarnaast wordt vastgelegd wat de patiënt zelf kan doen om in goeden doen te blijven en hoe de patiënt kan handelen bij verslechtering. Dergelijke acties door naasten en behandelaren worden ook vastgelegd. Hiervoor wordt vaak het stoplichtmodel gebruikt, met een groene, oranje en rode fase. Het signaleringsplan kan worden toegepast in de langdurige (ambulante) zorg, maar is ook onderdeel van het Toetsingskader Terugdringen insluiting (IGJ, 2025) om verplichte zorg (met name insluiting) in de intramurale setting te voorkomen.
•Crisisplan
Het crisisplan lijkt op de zorgkaart en is een overzicht van wensen en behoeften van patiënten in een crisissituatie. Een crisisplan kan worden samengevat in een crisiskaart, die de patiënt bij zich kan dragen in de vorm van een zakkaartje (www.crisiskaart.nl).
•Wellness and Recovery Action Plan (WRAP)
Een WRAP is een zelfhulpinstrument dat patiënten helpt om weer grip te krijgen op het leven, na een ontregeling door ingrijpende gebeurtenissen. Hoewel preventie van verplichte zorg niet het primaire doel is van een WRAP is dit wel een vorm om de eigen regie van de patiënt te versterken en toekomstige ontregeling te voorkomen.
Er is geen wetenschappelijke literatuur die de (in Nederland beschikbare) eigen regie instrumenten qua effectiviteit met elkaar vergelijkt. De werkgroep is van mening dat zorgprofessionals zich moeten verdiepen in de beschikbare instrumenten, om zo samen met de patiënt en diens naasten, een keuze te maken om eigen regie instrumenten optimaal in te zetten ter preventie van verplichte zorg. Hierbij moet worden benadrukt dat de Wvggz in sommige situaties, zoals bij de aanvraag van een zorgmachtiging, de zorgprofessional verplicht om een patiënt te ondersteunen bij het invullen van een zorgkaart en de informatie uit de zorgkaart mee te nemen in het zorgplan.
Ambulante verplichte zorg, in de vorm van CTO’s, heeft geen relevant effect op verplichte opnames of de duur van verplichte opnames. De literatuur is niet eenduidig over het effect op verplichte heropname nadat de ambulante verplichte zorg volgt op een verplichte opname.
Intensieve ambulante zorg wordt in de literatuur besproken in de vorm van intensive home treatment (IHT) en crisisinterventie teams. Laatstgenoemde zijn teams voor snelle interventie bij psychiatrische crisis, volgens een methode die de basis heeft gevormd voor het ontstaan van het IHT-model (Prinsen, 2016). IHT leidt niet tot een relevante afname van (verplichte) opnames, maar wel tot een relevante afname in aantal (verplichte) opnamedagen. De inzet van crisisinterventie teams zorgt voor zowel een relevante afname van aantal (verplichte) opnames, als voor een relevante afname van de hoeveelheid (verplichte) opnamedagen. Een andere vorm van laagdrempelige intensieve ambulante zorg is Peer Supported Open Dialogue. Hoewel deze methode (nog) niet onderworpen is aan gerandomiseerde studies zijn de resultaten van diverse implementaties en praktijkervaringen veelbelovend (Kinane, 2022).
Daarnaast beschrijven we hier enkele overige interventies, financiële incentives, ondersteuning bij therapietrouw, geïntegreerde zorg en psycho-educatie, in relatie tot verplichte opnames en de duur van verplichte opnames. Financiële incentives om ambulante zorg te accepteren hebben geen klinisch relevant effect op verplichte opnames. Geïntegreerde zorg heeft geen klinisch relevant effect op het aantal verplichte opnames. Psycho-educatie en ondersteuning bij de therapietrouw laten wel (beide in een enkele studie) een klinisch relevant effect zien bij de preventie van verplichte opnames. Psycho-educatie leidt ook tot een kleine, doch klinisch relevante afname van het aantal verplichte opnamedagen.
In de literatuur zijn geen aanwijzingen voor ongewenste effecten van de hier beschreven interventies ter voorkoming van verplichte opnames gevonden. Al moet daarbij worden opgetekend dat hier nauwelijks empirisch onderzoek naar is verricht. Bij preventie van verplichte zorg is een mogelijk ongewenst effect dat er te lang gewacht wordt met ingrijpen in een (snel) verslechterende situatie. Hierdoor kunnen patiënten langer aan hun lot worden overgelaten dan de werkgroep verstandig acht. Dit is geen argument tegen preventie, maar wel een argument voor het zorgvuldig blijven maken van een risicoafweging of preventieve maatregelen nog afdoende zijn om ernstig nadeel af te wenden.
Verplichte zorg in de intramurale setting
Ten aanzien van verplichte zorg binnen de intramurale setting keek de werkgroep naar de invloed van preventiestrategieën voor insluiting, fysieke en mechanische fixatie, de duur van deze interventies en ook naar de duur van verplichte opnames. Er is internationaal variatie in welke interventie als laatste redmiddel wordt gebruikt. Sommige landen hebben de traditie om fixatie te gebruiken en andere landen hebben de voorkeur voor insluiting. De besluitvormingsmechanismen zijn echter vergelijkbaar (Doedens, 2020). Daarom bespreekt de werkgroep de onderzoeksresultaten voor beide eindpunten samen, tenzij er verschillende effecten voor verschillende vormen van verplichte zorg rondom een interventie worden gerapporteerd.
In de literatuur worden diverse interventies genoemd, namelijk training van zorgprofessionals in de-escalatie en veiligheidsmanagement, kortdurende vroegsignalering van gevaarlijk gedrag (START en de Crisismonitor), modellen voor cultuur- en organisatieverandering (Safewards, Six Core Strategies, geïntegreerde zorg, Open Door Policy) en shared decision making. Daarnaast is het High Intensive Care (HIC) model momenteel de gouden standaard voor acute intramurale psychiatrische zorg in Nederland (Voskes, 2026). Hoewel dit model niet is getoetst in gerandomiseerde studies zijn de ervaringen ermee dermate positief dat het HIC-model ook in de toekomst als kwaliteitsstandaard wordt aanbevolen.
Training van zorgprofessionals in de-escalatie en veiligheidsmanagement lijkt in algemene zin effectief om verplichte zorg in de intramurale setting te voorkomen, al zijn de gevonden effecten wisselend qua klinische relevantie. Er zijn geen trainingsprogramma’s die in meerdere studies zijn onderzocht. Ook zijn er geen studies gevonden die de programma’s onderling vergelijken. Om adequaat te kunnen werken binnen de context van een HIC is het essentieel om te kunnen werken vanuit een herstelgerichte benadering. Herstelondersteunende zorg is daarom naast de-escalatie en veiligheidsmanagement een essentieel onderwerp om aan zorgprofessionals te trainen (Lim, 2017).
Kortdurende vroegsignalering van gevaarlijk gedrag heeft een klinisch relevant effect op de incidentie (START) en de duur van intramurale verplichte zorg (Crisismonitor). De twee modellen die in de literatuur worden beschreven zijn niet onderling met elkaar vergeleken. Het gebruik van de Crisismonitor wordt ook aangeraden door het HIC-werkboek (Voskes, 2026). Gebruik van alleen de Brøset Violence Checklist (BVC, ook onderdeel van de Crisismonitor) heeft (op basis van één studie) geen klinisch relevant effect op de hoeveelheid toepassingen van intramurale verplichte zorg (Abderhalden, 2008).
Er bestaan diverse modellen voor cultuur- en organisatieveranderingen die uit de literatuur naar voren komen. Deze modellen hebben gemeen dat daarin contact maken met patiënten, gelijkwaardigheid en een herstelgerichte benadering centraal staan. In het Europese Compendium report: Good practices to promote Voluntary Measures in Mental Health Services (Gooding, 2021) wordt een aanzienlijke hoeveelheid modellen uitgebreid besproken, zowel ter preventie van verplichte opname als ter preventie van verplichte zorg binnen de instelling. Het compendium bespreekt onder andere modellen die gedegen onderzocht zijn en die ook in de literatuursearch van de richtlijn naar voren komen, zoals Safewards en Six Core Strategies. Daarnaast wordt een groot aantal best practices besproken die (nog) niet zijn onderworpen aan gerandomiseerde studies. Toch beschouwt de werkgroep deze best practices wel als relevante opties om preventie van verplichte zorg verder te brengen. Safewards heeft een klinisch relevant effect op intramurale verplichte zorg, naast een klinisch relevant effect op het aantal conflicten. Six Core Strategies heeft ook een klinisch relevant effect op de hoeveelheid toepassingen van intramurale verplichte zorg.
Geïntegreerde zorg leidt niet tot een lagere incidentie van mechanische fixatie, maar heeft wel een klinisch relevant effect op de incidentie van insluiting en de duur van mechanische fixatie. Echter, beide effecten zijn gebaseerd op een zeer klein incidentiepercentage. Open Door Policy heeft een klinisch relevant effect op mechanische en fysieke fixatie, maar geen effect op insluiting.
Shared decision making heeft geen klinisch relevant effect op intramurale verplichte zorg. Er werd een effect gevonden ten faveure van de controleconditie, op basis van zeer kleine incidentiepercentages. Gezien de kleine sample sizes en lage GRADE-waardering is de werkgroep van mening dat dit tegengesteld effect van shared decision making een toevalsbevinding is en daarmee geen invloed heeft op de aanbevelingen.
Ongewenste effecten
In de literatuur zijn geen aanwijzingen voor ongewenste effecten van de hierboven beschreven interventies, al moet daarbij worden opgetekend dat hier nauwelijks empirisch onderzoek naar is verricht.
Waarden en voorkeuren van patiënten en naasten
Verplichte zorg heeft, naast de beoogde positieve effecten, meestal ook negatieve effecten voor patiënten en ook voor hun naasten en moet ook daarom echt een ultimum remedium zijn. Indien mogelijk heeft hulp en ondersteuning op vrijwillige basis de voorkeur. Een belangrijk doel van de Wvggz is de preventie van verplichte zorg en daar kunnen naasten bij helpen. Zij kunnen de patiënt bijvoorbeeld ondersteunen bij het maken en uitvoeren van een eigen plan van aanpak, een zorgplan, de zorgkaart, een zelfbindingsverklaring en de crisiskaart. Triadisch werken is hiervoor een voorwaarde en hier moet vanaf het eerste contact mee gestart worden. De patiënt bepaalt of, en zo ja, met wie naast de hulpverlener wordt samengewerkt. Ook de inzet van (familie-)ervaringsdeskundigen kan leiden tot voorkomen en verminderen van verplichte zorg.
De zorgverantwoordelijke moet bij een voornemen om verplichte zorg toe te passen tijdig vooroverleg plegen met de patiënt. In dit overleg kan de zorgverantwoordelijke de overwegingen delen en kan de patiënt een beroep doen op bijvoorbeeld de patiëntenvertrouwenspersoon. Het is essentieel om tijdig en bij voorkeur niet pas als verplichte zorg (opnieuw) wordt overwogen, het belang van een zelfbindingsverklaring en andere eigen regie instrumenten te bespreken met de patiënt en diens naasten. Daarnaast blijft het gedurende het hele zorgtraject belangrijk om preventie van verplichte zorg een gespreksonderwerp te laten zijn met de patiënt en diens naasten, evenals het minder ingrijpend maken van de uitvoering van verplichte zorg, als deze toch nog noodzakelijk blijkt. Hierbij valt te denken aan het opstellen en nauwkeurig bijhouden van een signaleringsplan en crisiskaart. Geef ook naasten genoeg handvatten om staande te blijven en de patiënt tot steun te kunnen zijn. Wijs de patiënt erop dat deze zich kan laten bijstaan door de patiëntenvertrouwenspersoon. Wijs naasten erop dat zij in het kader van de Wvggz recht hebben op ondersteuning van een familievertrouwenspersoon.
Wanneer verplichte zorg heeft plaatsgevonden is evaluatie van deze verplichte zorg met de patiënt en diens naasten essentieel. De zorgverantwoordelijke dient de resultaten van deze evaluatie te gebruiken om verplichte zorg in de toekomst te voorkomen.
Om verplichte zorg te voorkomen is het van belang dat er een soepele overgang (en overdracht) tussen ambulant en klinische zorg is. De onderlinge communicatie tussen de betrokken partijen is essentieel om terugval kort na ontslag uit de klinische setting te voorkomen. Zorg in de intramurale omgeving voor een healing environment, een comfortroom en rooming in, een gastvrije sfeer, en liefdevolle aandacht voor elke patiënt. Daar passen de traditionele separeer- en afzonderingsruimten niet bij. Die zouden buiten gebruik moeten worden gesteld, of omgebouwd tot Extra Beveiligde Kamer, binnen een Intensive Care omgeving (Voskes, 2026).
Er zijn diverse landelijke initiatieven om de ggz te verbeteren en meer hulp te kunnen bieden op vrijwillige basis, zoals Ecosystemen Mentale Gezondheid (zie https://denieuweggz.nl/nl en https://www.dejuistezorgopdejuisteplek.nl/praktijkvoorbeelden/gem-een-nieuwe-beweging-binnen-de-ggz/) en Radicale vernieuwing in de langdurige ggz (zie https://www.radicalevernieuwing.nl/ggz/). De werkgroep roept organisaties op om zich aan te sluiten bij dergelijke initiatieven om gezamenlijk preventie van verplichte zorg tot kernthema te maken.
De werkgroep acht het essentieel dat patiënten en naasten actief worden betrokken bij de selectie, implementatie en uitvoering van preventiestrategieën en interventies. Door hun inbreng in alle fasen mee te nemen, worden waarden, wensen en voorkeuren van patiënten structureel gewogen en vertaald naar passende zorg.
Kostenaspecten
De interventie levert onbekende kosten op ten opzichte van de controle behandeling. Dit weegt wel op tegen het verschil in effectiviteit.
Er zijn weinig kosten-effectiviteitsstudies verricht naar de beschreven preventiestrategieën. Uitzonderingen daarop zijn gezamenlijke crisisplannen (“joint crisis plans”, JCP’s, een vorm van crisisplannen die door de patiënt in gezamenlijkheid met de hulpverlener en/of naaste wordt samengesteld) en ambulante verplichte zorg. Gezamenlijke crisisplannen werden door Barrett et al (2013) onderzocht, onder andere op kosteneffectiviteit. Deze auteurs vonden iets lagere kosten voor de groep met een gezamenlijk crisisplan op organisatieniveau en geen verschil op maatschappelijk niveau. Qua kosteneffectiviteit op organisatieniveau bleken gezamenlijke crisisplannen te prefereren boven standaardbehandeling (Barrett, 2013). Ambulante verplichte zorg (“community treatment orders”, CTO’s) werden door Simon et al (2020) onderzocht op kosteneffectiviteit. De kosten van CTO’s waren grotendeels gelijk aan de controlegroep (Simon, 2021). Doordat de studie geen positieve effecten vond van CTO’s op kwaliteit van leven concludeerden de auteurs dat CTO’s hoogstwaarschijnlijk niet kosteneffectief waren.
In algemene zin vergen alle genoemde interventies capaciteit van organisaties voor implementatie, training van zorgprofessionals en (waar nodig) het aanpassen van de omgeving. Dit kan aanzienlijke kosten met zich meebrengen. Daarentegen kan inzetten van verplichte zorg ook forse maatschappelijke kosten met zich meebrengen, zeker wanneer de potentiële gezondheidsschade daarin wordt meegenomen (Tseng, 2022). Mogelijk wegen de aanzienlijke kosten voor preventie op tegen de maatschappelijke kosten van schade van inzet van verplichte zorg.
Gezondheidsgelijkheid
De toegang tot vrijwillige zorg is niet voor iedereen gelijk. Groepen waarvoor vrijwillige zorg minder toegankelijk is, lopen meer risico om geconfronteerd te worden met verplichte zorg. De impact van adequate preventie van verplichte zorg is daarom mogelijk groter voor kwetsbare groepen, waardoor de gezondheidsgelijkheid door deze interventies (mogelijk) toeneemt. Deze groepen verdienen dus extra aandacht van zorgverleners.
Patiënten met een lage sociaaleconomische status (SES) hebben een groter risico op verplichte opnames, mogelijk doordat zij minder sociaal vangnet hebben (Walker, 2019). Daarnaast hebben patiënten met een lage SES mogelijk minder kennis van het zorgsysteem en is informatie hierover voor hen vaak in te moeilijke taal geschreven. Diverse internationale studies rapporteren daarnaast dat patiënten met een donkere huidskleur vaker met verplichte opnames te maken krijgen dan patiënten met een lichte huidskleur. Er zijn ook aanwijzingen dat het behoren tot een minderheid an sich een groter risico geeft op verplichte opnames (Ali, 2025; Barnett, 2019; Shea, 2022). Vergelijkbare resultaten zijn gevonden in onderzoek naar de relatie tussen etniciteit en ambulante verplichte zorg (Moss, 2019).
Dit heeft gevolgen voor het implementeren van preventiestrategieën. De kosteneffectiviteit van gezamenlijke crisisplannen bleek bijvoorbeeld veel groter voor patiënten met een donkere huidskleur dan voor patiënten met een lichte huidskleur in relatie tot het voorkomen van verplichte opnames (Barret, 2013).
Internationale studies naar diversiteit, gelijkheid en inclusie (of: DEI) zijn niet per definitie generaliseerbaar naar de Nederlandse maatschappij. Tegelijkertijd is het goed voor te stellen dat dergelijke verschillen in gezondheid en behandeling ook in Nederland een rol spelen. Preventiestrategieën kunnen dus voor patiënten uit minderheidsgroepen een extra grote impact hebben en daarmee bijdragen aan een toename van gezondheidsgelijkheid. Het lijkt hierbij een voorwaarde dat er aandacht is voor minderheidsgroepen bij de implementatie van preventiestrategieën.
Aanvaardbaarheid
Ethische aanvaardbaarheid
De interventie lijkt wel aanvaardbaar voor de betrokkenen. De werkgroep voorziet geen ethische bezwaren.
Verplichte zorg heeft diverse potentieel schadelijke componenten, met name vormen van verplichte zorg die alleen als veiligheidsmaatregel kunnen worden gebruikt door het ontbreken van positieve effecten voor de patiënt, zoals insluiting en fixatie. Deze interventies worden geassocieerd met allerhande fysieke en psychologische ongewenste effecten (Aragonés-Calleja, 2024. Er zijn geen aanwijzingen voor ongewenste effecten van de meeste preventiestrategieën. Inzet van preventie strategieën kan bijdragen aan voorkomen van verplichte zorg en daarmee verminderen van ongewenste effecten. Inzet van preventiestrategieën wordt daarom ethisch verantwoord geacht.
De meeste preventiestrategieën worden ingezet om verplichte zorg te voorkomen of de duur daarvan te verminderen. Ze zijn dus gericht op het voorkomen van nadeel voor de patiënt. Een punt van aandacht hierbij is altijd het risico op een fenomeen dat in de Engelstalige literatuur “informal coercion” (of: informele dwang) wordt genoemd. In het Nederlands zouden we dit definiëren als stevige drang, waarbij de patiënt mogelijk de verplichting ervaart om mee te werken aan een voorgestelde interventie om verplichte zorg te voorkomen, terwijl dat niet als verplichte zorg wordt beschouwd en waarbij dus geen sprake is van de bescherming van de rechten van de patiënt. Dit is een onwenselijke situatie, omdat vanwege de rechtsbescherming van de patiënt het de voorkeur heeft om zorg met stevige drang laagdrempelig als verplichte zorg te beschouwen (zie module Onderscheid definities vrijwillige zorg en verplichte zorg). Het risico van informele dwang is wel een ethisch aspect dat bij het inzetten van preventieve interventies een duidelijke plaats moet hebben. Patiënten en naasten moeten in elk geval goed geïnformeerd worden over de voor- en nadelen van verplichte zorg enerzijds en anderzijds van het meewerken aan een interventie zonder verzet, maar eigenlijk met gemengde gevoelens of zelfs met tegenzin, meewerken aan een interventie. Voordeel van vrijwillige zorg voor de patiënt is dat deze zelf de regie in handen houdt, uiteraard in overleg met de zorgverlener.
Duurzaamheid
Bij de interventies spelen de duurzaamheidsaspecten geen specifieke rol van betekenis.
Haalbaarheid
De haalbaarheid van de beschreven interventies hangt af van diverse capaciteitsaspecten. De interventies lijken wel haalbaar.
Er zijn diverse verschillen tussen de beschreven interventies in de literatuur en de Nederlandse situatie. Zo zijn bijvoorbeeld de eigen regie instrumenten die in de literatuur beschreven worden niet identiek aan de beschikbare instrumenten in Wvggz. Dit maakt de interventies niet per se onhaalbaar, maar betekent wel dat de verwachte effecten anders kunnen zijn dan we kennen uit onderzoek.
Het project Eigen regie in de Wvggz (Molenaar, 2025) laat zien dat kleine aanpassingen in de werkwijze van zorgteams kan zorgen voor een sterke verbetering van het gebruik van eigen regie instrumenten. In ieder geval zijn heldere communicatie tussen patiënten, naasten en zorgprofessionals en structurele evaluatie essentieel voor goed gebruik van eigen regie instrumenten. De zorgorganisatie moet zich inspannen om ervoor te zorgen dat gemaakte afspraken tussen patiënten, naasten en zorgprofessionals voor iedereen inzichtelijk en terug te vinden zijn, zeker in momenten van crisis.
Alle preventiestrategieën vragen capaciteit van zorgorganisaties en zorgprofessionals. Dit is problematisch, gezien de ernstige tekorten aan zorgprofessionals in alle deelsectoren van Nederlandse gezondheidszorg. Om minimale capaciteit te waarborgen is al niet altijd voldoende personeel beschikbaar, laat staan om te innoveren, implementeren en investeren in het voorkomen van verplichte zorg. Toch zijn er diverse best practices in Nederland beschikbaar waar met dezelfde capaciteitsproblemen toch verplichte zorg sterk is teruggedrongen (Plomp, 2024). Om de preventiestrategieën haalbaar te maken in de praktijk is een sterke interprofessionele samenwerking nodig binnen en tussen zorgorganisaties, waarbij leren van elkaar en een kritische blik op de eigen context centraal staan.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Er zijn meer dan voldoende preventiestrategieën beschikbaar om te implementeren ter preventie van verplichte zorg. Sommige van deze strategieën zijn slechts zeer lokaal toepasbaar en ze bevatten veel onderlinge overlap. Daarnaast zijn geen van deze strategieën vergeleken met elkaar in gerandomiseerde studies. Inhoudelijk focussen veel van deze strategieën op vergelijkbare thema’s; een duidelijke visie die terugkomt in alle lagen van de organisatie ten aanzien van verplichte zorg, zorgdragen voor cultuurverandering, aandacht voor ethiek en/of inzetten op een adequate kwantitatieve en kwalitatieve personeelsbezetting (zowel qua aantal als qua attitude, competenties en disciplinemix).
Er is daarom geen specifieke preventiestrategie aan te bevelen (Voskes, 2026). Onderzoek en klinische ervaring suggereren dat een combinatie van strategieën de meeste kans geeft op verandering (Daguman, 2024). De werkgroep adviseert organisaties een keuze te maken voor één, maar bij voorkeur meerdere (complementaire) preventiestrategieën en ervoor te zorgen dat deze zeer goed geïmplementeerd worden. Hiervoor is toewijding van alle lagen van de organisatie noodzakelijk. Professionals in de directe patiëntenzorg, zoals verpleegkundigen, groepsbegeleiders en behandelaren, zijn hierbij de meest bepalende factoren onder andere doordat een algemeen goedkeurende attitude ten opzichte van verplichte zorg geassocieerd is met meer gebruik van verplichte zorg (Efkemann, 2022). Daarnaast is de inzet en betrokkenheid van patiënten en hun naasten bij het maken van preventiebeleid, naar de mening van de werkgroep, strikt noodzakelijk. De input en inzet van (familie-)ervaringsdeskundigheid is passend in elke fase van het selecteren, implementeren en uitvoeren van een preventiestrategie voor verplichte zorg.
Om verplichte zorg adequaat te voorkomen is het een voorwaarde dat de betrokken zorgprofessionals bevoegd en bekwaam zijn en in voldoende mate aanwezig om preventieve zorg te leveren. Hiervoor is aanvullende training, specifiek voor het voorkomen van verplichte zorg, noodzakelijk. In de literatuur wordt met name gesproken over training op het gebied van de-escalerend werken en vroegsignalering van (dreigende) escalatie. Er zijn geen vergelijkende studies van goede kwaliteit bekend die verschillende vormen of modellen van training met elkaar vergelijken. Educatieve interventies behandelen grotendeels dezelfde thema’s, zoals contact maken, communicatie in crisis, herstelondersteunend werken, vroegsignalering en (vervolgens) tijdig niet-verplichte interventies initiëren. Een voorbeeld hiervan zijn de trainingen van het Britse Restraint Reduction Network. Er is geen duidelijk bewijs dat laat zien dat een specifieke training of model te prefereren is boven anderen. De werkgroep is daarom van mening dat training essentieel is, maar dat organisaties een vorm en model moeten kiezen die passen bij de behoeften van de organisatie en deze vervolgens ruimhartig te faciliteren.
Veelomvattende preventiestrategieën, zoals High Intensive Care en Six Core Strategies, focussen op de intramurale setting en zijn daarom hooguit in die setting onderzocht op effectiviteit. Trainingen op het gebied van de-escalatie en vroegsignalering zijn ook vooral in de intramurale setting onderzocht. De werkgroep is van mening dat dergelijke preventiestrategieën en het trainen van zorgprofessionals essentieel zijn voor preventie van verplichte zorg, ongeacht de setting.
Voor de preventie van verplichte opnames kunnen in de literatuur en praktijk drie categorieën van interventies worden geïdentificeerd.
De eerste categorie zijn modellen voor intensieve ambulante zorg, zoals intensive home treatment (IHT). Er zijn aanwijzingen in de literatuur dat deze interventies effectief zijn. Specifiek voor de Nederlandse situatie is gebleken dat IHT zorgt voor significant minder opnamedagen dan conventionele psychiatrische crisiszorg. Niet alleen kan intensieve ambulante zorg verplichte opname voorkomen, het kan ook helpen om opnames te verkorten of na ontslag heropname te voorkomen. Hoewel intensieve behandeling thuis voor veel patiënten en naasten een optie van eerste voorkeur zal zijn, moeten behandelaren in de crisiszorg alert zijn op situaties waarbij deze voorkeur negatieve gevolgen kan hebben (bijv. een overbelasting van het netwerk waardoor een beschermende factor op de lange duur wegvalt).
De tweede categorie is het gebruik van eigen regie instrumenten, zoals het signaleringsplan of de crisiskaart en de wettelijk vastgelegde instrumenten plan van aanpak, zorgkaart en zelfbindingsverklaring. Het gebruik van de zorgkaart is, indien de patiënt dit wil, in de aanvraagprocedure voor een zorgmachtiging zelfs een verplichting voor de zorgverantwoordelijke (artikel 5:12). In de internationale literatuur worden deze instrumenten op verschillende manieren aangeduid. Voorbeelden daarvan zijn advance statements of advance directives, waarvoor waardevolle effecten worden gevonden ten aanzien van de preventie van verplichte opnames. De Wvggz biedt de drie bovengenoemde mogelijkheden voor het gebruik van eigen regie instrumenten, die in de praktijk nog niet allemaal voldoende geïmplementeerd zijn (Plomp, 2024). In deze context wordt internationaal ook vaak de community treatment order (CTO) genoemd, een vorm van ambulante dwang die men vindt in Engelssprekende landen. Uit meerdere, weliswaar kleine, studies blijkt dat de CTO niet bijdraagt aan het verminderen of verkorten van verplichte opnames.
De derde categorie zijn interventies die gericht zijn op het gedrag van de patiënt, zoals psycho-educatie en motiverende gespreksvoering. Deze interventies worden in een ideale situatie ingezet op basis van de behoefte en voorkeur van de patiënt, gecombineerd met intensieve ambulante zorg en/of eigen regie instrumenten.
Voor de preventie van verplichte zorg in de intramurale setting kunnen in de literatuur en praktijk twee categorieën van interventies worden geïdentificeerd.
De eerste categorie zijn interventiemodellen gericht op attitude-, cultuur- en organisatieveranderingen, zoals High Intensive Care, Six Core Strategies en Safewards. Van sommige van deze interventies, zoals Safewards en Open Door Policy, zijn ook in de wetenschappelijke literatuur gunstige effecten bekend. Hoewel er veel overlap bestaat tussen deze modellen en elke lokale context zijn eigen uitdagingen kent adviseert de werkgroep organisaties om zich te laten inspireren door het werk van collega’s in binnen- en buitenland om de organisatie in beweging te zetten.
De tweede categorie is kortdurende, gestructureerde vroegsignalering van ongewenst of gevaarlijk gedrag, met bijvoorbeeld START of de Crisismonitor. Door verslechtering vroegtijdig op te sporen is het mogelijk om vroegtijdig in de escalatie (niet-verplichte) interventies in te zetten. Het geeft professionals houvast om gevaar in kaart te brengen en dit kan, mits goed ingezet, helpen om het contact met de patiënt aan te gaan over een verslechterende situatie. START is met name onderzocht in een forensische populatie, maar in het buitenland is ook enige ervaring opgedaan hiermee in acute psychiatrische voorzieningen. Met name de Crisismonitor is bewezen effectief om escalaties en verplichte zorg te voorkomen, mits ingebed in een werkwijze waarin ook daadwerkelijk naar aanleiding van de Crisismonitor niet-verplichte interventies beschikbaar zijn.
Eindoordeel: Sterke aanbeveling voor
Onderbouwing
De Wvggz beoogt verplichte zorg zoveel mogelijk te voorkomen. Uit de eerste evaluatie van de Wvggz is echter gebleken dat het toepassen van verplichte zorg onvoldoende daalt. Momenteel heerst onduidelijkheid in de praktijk over de rol van preventiestrategieën en welke aanpak het meest effectief is met betrekking tot de preventie van verplichte zorg. Mede hierdoor is er sprake van praktijkvariatie. Deze module heeft als doel om effectieve strategieën te evalueren om verplichte zorg te voorkomen en/of te verminderen.
PICO 1 - Summary of Findings
Summary of Findings table: Prevention strategies compared to standard care or not applying a prevention strategy in patients with mental illness
Population: Patients with mental illness
Intervention: Prevention strategy
Comparator: Standard care or not applying a prevention strategy
|
Outcome |
Study results and measurements |
Absolute effect estimates |
Certainty of the Evidence (Quality of evidence) |
Summary |
|
|
Prevention strategy |
Standard care or no prevention strategy |
||||
|
Compulsory admission (crucial) |
Relative risk: 0.84 (95%CI 0.75 to 0.94) Based on data from 3575 participants in 15 studies. |
26 per 100 |
31 per 100 |
Very low Due to serious risk of bias*, indirectness, and imprecision1 |
The evidence is very uncertain about the effect of prevention strategies on compulsory admission when compared with standard care or not applying a prevention strategy in patients with mental illness.
(Burns, 2013; Henderson, 2004; Johnson, 2005; Lay, 2015; Lay, 2018; Ohlenschlaeger, 2008; Papageorgiou, 2002; Priebe, 2013; Ruchlewska, 2014; Staring, 2010; Steadman, 2001; Swartz, 1999; Thornicroft, 2013; Cornelis, 2022; Tinland, 2022) |
|
Difference: 5 fewer per 100 (95%CI 8 fewer - 2 fewer) |
|||||
|
Physical and mechanical restraint (crucial) |
Based on data from 12717 participants in 7 studies·. |
Results could not be pooled due to heterogeneity in interventions and reporting of the outcome measure. For more details, see Results section. |
Very low Due to serious risk of bias*, inconsistency, and indirectness2 |
The evidence is very uncertain about the effect of prevention strategies on physical and mechanical restraint when compared with standard care or not applying a prevention strategy in patients with mental illness.
(Celofiega, 2022; Hvidhjelm, 2022; Kontio, 2014; Ohlenschlaeger, 2008; Indregard, 2024; Valimaki, 2022; Hamann, 2020) |
|
|
Seclusion (crucial) |
Based on data from 9523 participants in 5 studies·. |
Results could not be pooled due to heterogeneity in interventions and reporting of the outcome measure. For more details, see Results section. |
Very low Due to serious risk of bias*, inconsistency, and indirectness3 |
The evidence is very uncertain about the effect of prevention strategies on seclusion when compared with standard care or not applying a prevention strategy in patients with mental illness.
(Kontio, 2014; Ohlenschlaeger, 2008; van de Sande, 2011; Indregard, 2024; Valimaki, 2022) |
|
|
Duration of compulsory admission (important) |
Based on data from 1795 participants in 6 studies. |
Difference: SMD 0.13 lower (95% CI 0.48 lower - 0.22 lower) |
Very low Due to serious risk of bias*, indirectness, and imprecision4 |
The evidence is very uncertain about the effect of prevention strategies on duration of compulsory admission when compared with standard care or not applying a prevention strategy in patients with mental illness.
(Burns, 2013; Johnson, 2005; Lay, 2015; Lay, 2018; Thornicroft, 2013; Cornelis, 2022) |
|
|
Duration of physical and mechanical restraint (important) |
Based on data from 464 participants in 3 studies·. |
Results could not be pooled due to variability in reporting of the outcome measure. For more details, see Results section. |
Very low Due to serious risk of bias*, indirectness, and imprecision5 |
The evidence is very uncertain about the effect of prevention strategies on duration of physical and mechanical restraint when compared with standard care or not applying a prevention strategy in patients with mental illness.
(Hvidhjelm, 2022; Kontio, 2014; Ohlenschlaeger, 2008) |
|
|
Compulsory care (important) |
Based on data from 6 studies. |
Results could not be pooled due to variability in reporting of the outcome measure. For more details, see Results section. |
Very low Due to serious risk of bias*, indirectness, and imprecision6 |
The evidence is very uncertain about the effect of prevention strategies on compulsory care when compared with standard care or not applying a prevention strategy in patients with mental illness.
(Abderhalden, 2008; Hvidhjelm, 2022; Ohlenschlaeger, 2008; Putkonen, 2013; Indregard, 2024; Steinert, 2023) |
|
|
Duration of seclusion (important) |
Based on data from 3 studies. |
Results could not be pooled due to variability in reporting of the outcome measure. For more details, see Results section. |
Very low Due to serious risk of bias*, Due to very serious imprecision7 |
The evidence is very uncertain about the effect of prevention strategies on duration of seclusion when compared with standard care or not applying a prevention strategy in patients with mental illness.
(Kontio, 2014; van de Sande, 2011; Valimaki, 2022) |
|
|
Isolation (important) |
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of prevention strategies on isolation when compared with standard care or not applying a prevention strategy in patients with mental illness. |
|
|
Care authorization (important) |
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of prevention strategies on care authorization when compared with standard care or not applying a prevention strategy in patients with mental illness. |
|
1 Risk of Bias: serious. Due to missing information about randomization procedure, baseline differences between groups, missing outcome data, unclear risk of bias due to selective outcome reporting, unclear risk of bias due to lack of blinding. Indirectness: serious. Due to heterogeneity in study populations. Imprecision: serious. Due to wide confidence intervals of individual studies.
2 Risk of Bias: serious. Due to missing information about randomization procedure, unclear risk of bias due to lack of blinding. Inconsistency: serious. Due to conflicting results. Indirectness: serious. Due to heterogeneity in study populations.
3 Risk of Bias: serious. Due to missing information about/insufficient randomization procedure, unclear risk of bias due to lack of blinding, missing information about loss to follow-up. Inconsistency: serious. Due to conflicting results. Indirectness: serious. Due to heterogeneity in study populations.
4 Risk of Bias: serious. Due to missing information about randomization procedure, missing outcome data, unclear risk of bias due to selective outcome reporting, unclear risk of bias due to lack of blinding. Indirectness: serious. Due to heterogeneity in study populations. Imprecision: serious. Due to wide confidence intervals of individual studies.
5 Risk of Bias: serious. Due to missing information about randomization procedure, unclear risk of bias due to lack of blinding. Indirectness: serious. Due to heterogeneity in study populations. Imprecision: serious. Due to wide confidence intervals of individual studies.
6 Risk of Bias: serious. Due to missing information about randomization procedure, missing outcome data, unclear risk of bias due to lack of blinding. Indirectness: serious. Due to heterogeneity in study populations. Imprecision: serious. Due to wide confidence intervals of individual studies.
7 Risk of Bias: serious. Due to missing information about/insufficient randomization procedure, unclear risk of bias due to lack of blinding, missing information about loss to follow-up. Imprecision: very serious. Due to missing dispersion measures and the inability to calculate effect measures.
*For further details, see risk of bias table in the appendix; · The number of participants included in Kontio (2014) is unclear.
PICO 2 - Summary of findings
No studies were included and could therefore not be graded.
Summary of literature
PICO 1 - Description of studies
A total of four systematic reviews and six RCTs were included in the analysis of the literature. Important characteristics of the included systematic reviews are summarized in table 2. Table 3 presents important study characteristics of the included RCTs. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Indregard (2024) performed a RCT to compare coercive practices in open-door policy and treatment as usual wards in an urban hospital setting. All patients (≥18 years) referred to the acute psychiatric ward at Lovisenberg Diaconal Hospital (Oslo, Norway) were screened for eligibility. Patients were excluded if 1) they were legally prohibited from admission in an open-door facility due to being under active criminal justice custody or serving a sentence, or 2) they had a documented history of persistent violence. Patients referred for acute psychiatric ward care from the admission ward were allocated to either an open-door policy ward (n=245) or a treatment as usual ward (n=311). In the open-door policy wards, the main doors were open from 9:00 to 21:00 every day of the week but could be locked if it was the only solution to ensure safety. Patients in the control wards received treatment as usual in which the main doors were always locked and patients’ freedom to leave the ward would depend on the staff’s availability and individual risk assessment. Staff on all wards underwent de-escalation and harm minimization training every three to six months. Additional study characteristics can be found in table 3.
Pedersen (2024) aimed to examine evaluated evidence-based interventions that seek to reduce the incidence of and/or time in mechanical restraint (restrictive practice in mental health to immobilize or restrict people’s movement in response to violent and aggressive behavior, defined as the use of equipment, such as belts, straps or cuffs, by trained staff) in adult mental health inpatient settings. To identify relevant studies, a two-phased approach was used. First, the review by Baker (2021) was reviewed to identify relevant studies between 1999 and April 2019. Second, an updated systematic search was performed from 1 January 2019 to 4 July 2023 based on the search strategy adopted in Baker (2021). The international databases CINAHL, Embase, and PubMed were searched. Inclusion criteria were: 1) peer-reviewed primary research literature, 2) evaluation of interventions that seek to reduce the incidence of and/or time in mechanical restraint (or seclusion/mechanical restraint reported simultaneously), and 3) English full-text available. Studies that also included findings for children or adolescents or other types of restraint, but which were not reported independently, were excluded. In total, 41 studies were included in the review. Of these, five studies were controlled trials (Celofiega, 2022; Hamann, 2020; Hvidhjelm, 2022; Kontio, 2014; Putkonen, 2013) and were included in the current analysis.
Steinert (2023) performed a RCT to investigate whether the number of coercive measures used in psychiatric wards could be reduced by implementation of recommendations of the PreVCo (prevention of violence and coercion) program. Wards were eligible to participate in the study if they: 1) admitted involuntary patients regardless of their diagnoses, 2) routinely recorded data on coercive measures and incidents of aggression, and 3) had the support of both medical and nursing management for the study's objectives. A total of 54 wards were considered eligible and randomized to either an intervention (n=27 wards) or a control condition (n=27 wards) (waiting list). The intervention consisted of the implementation of three out of 12 suggested recommendations or at least one complex intervention program drawn from the guidelines (tailored approach). Workshops were conducted with the ward teams for implementation. Additional study characteristics can be found in table 3.
Cornelis (2022) conducted a RCT to evaluate the potential of intensive home treatment to reduce bed-days and its clinical effectiveness compared with treatment as usual. Participants were recruited at the psychiatric emergency service in Amsterdam and from emergency wards of two major mental health institutions Arkin and GGZ inGeest. Inclusion criteria were: 1) a diagnosis of at least one DSM-IV-TR or DSM-5 disorder (not primarily a substance use disorder), 2) age 18-65 years, and 3) experiencing an acute severe psychiatric crisis for which a psychiatrist indicated or executed a clinical admission. Participants that were receiving Flexible Assertive Community Treatment (FACT) with integrated crisis care or participants that received previous intensive home treatment were excluded. Eligible participants were randomly assigned to either the intensive home treatment group (n=183), or the treatment as usual group (n=63). Intensive home treatment provided intensive outpatient care and functioned as a gatekeeper for hospital admissions. Treatment plans were tailored to the patient and included for example pharmacotherapy, structuring the daytime, psychoeducation, cognitive behavioral therapy, and social care. Participants in the treatment as usual group received a combination of highly intensive inpatient treatment in the first phase, and low frequency outpatient treatment in the second phase. Treatment settings included hospital wards, acute treatment teams, and outpatient clinics (no home treatment). Additional study characteristics are presented in table 3.
Tinland (2022) conducted a RCT to determine the efficacy of psychiatric advance directives (PADs) facilitated by peer workers in people with mental disorders. Participants were included if they 1) were aged older than 18 years, 2) had a diagnosis of schizophrenia, bipolar disorder, or schizoaffective disorder according to the DSM-5, 3) were involuntary admitted to the hospital within the past 12 months, and 4) had decision-making capacity according to the MacArthur Competence Assessment Tool for Clinical Research. Eligible participants were randomized to either the peer-worker psychiatric advance directives (PW-PAD) group (n=196), or the control group (n=198). Participants in the PW-PAD group could, depending on their preferences, meet a peer worker in a place of their choice, be supported by this peer worker in drafting the PAD document, and/or be supported by the peer worker during the sharing of PADs with the health care agent and the psychiatrist. Participants assigned to the control group were followed up as usual. Additional study characteristics can be found in table 3.
Välimäki (2022) performed a cluster-RCT to examine whether an evidence-based educational intervention for nurses decreases the use of seclusion rooms in psychiatric hospitals compared with usual practice. Hospitals with at least one adult psychiatric ward that used coercive measures as defined in the Finnish Mental Health Act were eligible. Hospital wards that specialized solely in child and adolescent psychiatric care, psychogeriatric care, or forensic psychiatry were excluded. All nurses working on the study wards were invited to join the study, without any in- or exclusion criteria. For patients, inclusion criteria were: 1) admission to the study ward, 2) aged ≥18 years, and 3) fluency in Finnish. Hospitals were randomly assigned to the evidence-based educational intervention (VIOLIN) group (n=13 wards) or the usual practice group (n=15 wards). VIOLIN is an 18-month intervention aimed to reduce coercive practices in psychiatric wards. Eight months of intervention were followed by a 10-month maintenance period. Usual practice wards continued with their normal activities. Additional study characteristics are displayed in table 3.
Baker (2021) conducted a systematic review to provide an overview of non-pharmacological interventions to reduce restrictive practices in adult mental health inpatient settings. The following databases were searched from 1999 to April 2019: British Nursing Index (BNI), CINAHL, Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Database of Systematic Reviews (CDSR), Database of Abstracts of Reviews of Effects (DARE), Embase, Health Technology Assessment (HTA) database, HTA Canadian and International, Medline, NHS Economic Evaluation Database (NHS EED), PsycINFO, and PubMed. Additionally, a grey literature search was performed. Inclusion criteria were: 1) evaluation of interventions aimed at changing the behavior of inpatient adult mental health service staff to reduce restrictive practices, 2) reporting on the outcome reduction of restrictive practices, and 3) English full-text available. Studies that included findings regarding children and adolescent mental health services, learning disability and organic conditions or studies that evaluated pharmacological interventions were excluded. In total, 175 studies were included in the review of which six studies used a RCT design. Eventually, two RCTs were included in the current analysis (van de Sande, 2011; Abderhalden, 2008). Two RCTs were excluded because they were included in Pedersen (2024) (Kontio, 2014; Putkonen, 2013), one because no relevant outcomes -according to the PICO- were reported (Bowers, 2015), and one because no full-text was available (Parasurum, 2011).
Hamann (2020) performed a post-hoc analysis with data from the cluster-randomized SDM-plus trial to investigate whether shared decision making (SDM) reduces the number of patients with incidents of aggression and the use of coercive measures compared to treatment as usual. The study was conducted in 12 acute psychiatric wards of 4 psychiatric hospitals in Germany. Inclusion criteria were: 1) inpatient status of participating ward, 2) age 18-65 years, and 3) diagnosis of schizophrenia or schizoaffective disorder. Patients with intellectual disabilities were excluded. Pairs of comparable wards were determined, after which one ward of each pair was randomized to the intervention group (n=154) and the other to the control group (n=151). In the intervention group, staff, and patients both received training in SDM-plus, which aims to empower health care staff and patients regarding SDM-specific communication techniques. Staff and patients from the control wards acted under treatment as usual conditions. They were offered SDM-plus training after the end of the study. Additional study characteristics are presented in table 3.
Molyneaux (2019) aimed to synthesize evidence on the effectiveness of crisis-planning interventions in reducing rates of compulsory hospital admissions for people with psychotic illness or bipolar disorder, compared with usual care. The international databases CENTRAL, CINAHL, Medline, Embase, PsycINFO, and the international Standard Randomized Controlled Trial Number (ISRCTN) registry were searched from inception to 16 October 2018. Inclusion criteria were: 1) RCTs, 2) adults (≥16 years) with a diagnosis of a psychotic illness or bipolar disorder with or without psychotic symptoms, 3) examination any form of crisis-planning intervention, and 3) comparison group was treatment as usual. There were no exclusion criteria based on language or date of publication. A total of five RCTs were included in the review, which were all included in the current analysis (Papageorgiou, 2002; Henderson, 2004; Thornicroft, 2013; Ruchlewska, 2014; Lay, 2018).
De Jong (2016) performed a systematic review to establish which interventions effectively reduce compulsory admissions in adult psychiatric patients in outpatient settings. The international databases Embase, Medline, Web of Science, PsycINFO, CINAHL, and CENTRAL were searched from inception to 30 April 2015. Studies were eligible if: 1) they were RCTs, 2) they investigated interventions of any kind that were designed to reduce compulsory admission rates in adult psychiatric patients in outpatient settings, 3) they reported on compulsory admission as primary or secondary outcome measure. Studies with compulsory admission as an intervention or any intervention during hospitalization were not eligible. A total of thirteen RCTs were included in the review, of which eight were included in the current analysis (Swartz, 1999; Steadman, 2001; Burns, 2013; Staring, 2010; Priebe, 2013; Johnson, 2005; Ohlenschlaeger, 2008; Lay, 2015). Four RCTs were excluded because they were included in Molyneaux (2019) (Papageorgiou, 2002; Henderson, 2004; Thornicroft, 2013; Ruchlewska, 2014), and one because of its long follow-up of 12 years (Sigrunarson, 2013).
Table 2. Characteristics of included systematic reviews
|
Study |
Main inclusion criteria |
Participant/ward characteristics |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias* |
|
Included in systematic review Pedersen (2024) |
|||||||
|
Celofiega, 2022 Cluster-RCT, Slovenia |
Acute psychiatric wards that provide inpatient psychiatric treatment in six psychiatric hospitals |
Participant N at baseline I: 1251 | C: 1939
Age (mean, SD) I: 48.4 (17.0) years C: 49.2 (19.1) years
Sex (% male) I: 55.1 | C: 52.2
Hospitalization length (mean, SD) I: 11.8 (14.2) days C: 8.3 (12.7) days
Involuntary hospitalization (n, %) I: 116 (9.3) | C: 430 (22.2)
Ward Number of beds (mean, SD) I: 20.3 (3.6) | C: 18.3 (3.0)
Nursing staff (mean, SD) I: 14.2 (1.0) | C: 15.2 (2.5) |
Intervention: De-escalation education
Control: Treatment as usual |
Baseline period of 5 months followed by an intervention period of 5 months. |
Physical and mechanical restraint |
The study was conducted as part of a research project of the University Medical Center Maribor.
The authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
|
High |
|
Hvidhjelm, 2022 Cluster-RCT, Denmark |
Forensic male patients who displayed ≥1 basic aggressive episode(s) |
Participant N at baseline I: 42 | C: 94
Age (n, %) <27 years I: 11 (26.2) | C: 26 (27.7) 28-35 years I: 9 (21.4) | C: 19 (20.2) 36-45 years I: 12 (28.6) | C: 28 (29.8) >45 years I: 10 (23.8) | C: 21 (22.3)
Sex (% male): NR
Hospitalization length <1 year (n, %) I: 13 (31.0) | C: 51 (54.3) |
Intervention: Short-term Assessment of Risk and Treatability (START)
Control: No START |
6 months |
Physical and mechanical restraint Duration of physical and mechanical restraint Compulsory care |
Nothing is reported about funding of the study, except that all forensic psychiatric facilities in Denmark are publicly funded and subject to public health authorities.
The authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. |
Some concerns |
|
Kontio, 2014+ Cluster-RCT, Finland |
Acute, closed, adult inpatient wards practising seclusion and restraint |
Ward N at baseline I: 5 | C: 5
Number of beds 2007-2008 I: 88 | C: 78 2009-2010 I: 91 | C: 91
Nursing staff (n) 2007-2008 I: 96 | C: 87 2009-2010 I: 92 | C: 87 |
Intervention: E-learning course
Control: Treatment as usual |
4 years (data is collected for 24 months over 4 years) |
Physical and mechanical restraint Duration of physical and mechanical restraint Seclusion Duration of seclusion |
The study was supported by the European Commission, the University of Turku, the Finnish Cultural Foundation, the Hospital District of Helsinki and Uusimaa, and he Hyvinkää Hospital Region.
The authors alone are responsible for the content and writing of the paper.
The authors report no conflicts of interest. |
High |
|
Putkonen, 2013+ Cluster-RCT, Finland |
State-run secured hospital for criminal and civil patients with psychotic disorders and violent behavioral problems |
Participant Age (mean, SD) I: 40.2 (10.6) years C: 38.4 (10.6) years
Sex (% male) I: 100 | C: 100
Ward Number of beds I: 50 | C: 38 |
Intervention: Six Core Strategies
Control: Treatment as usual |
1 year (6 months of training followed by 6 months of supervised intervention) |
Compulsory care |
The study was funded by the Finnish Ministry of Health through the developmental fund for Niuvanniemi Hospital.
Potential conflicts of interest are reported for dr. Tiihonen. The other authors report no conflicts of interest.
|
High |
|
Included in systematic review Baker (2021) |
|||||||
|
Bowers, 2015 Cluster-RCT, UK |
Acute, psychiatric wards for adults of any gender |
Ward N at baseline I: 16 | C: 15
Number of beds (mean, SD) 19 (4.0)
Sex (n) Mixed gender: 16 Men only: 10 Women only: 5 |
Intervention: Safewards
Control: Physical health intervention |
24 weeks (8 weeks baseline period, 8 weeks of implementation, and 8 weeks of intervention) |
Compulsory care |
Funding was obtained by the National Institute of Health Research.
The authors declared no conflicts of interest. |
Some concerns |
|
Van de Sande, 2011 Cluster-RCT, the Netherlands |
Four acute psychiatric wards in Rotterdam |
Participant N at baseline I: 80 | C: 90
Age (mean, SD) I: 38 (13) years C: 40 (11) years
Sex (% male) I: 66 | C: 60
Involuntary admitted (n, %) I: 70 (88) | C: 39 (43)
Ward Number of beds I: 20 | C: 16
Aggression incidents I: 49 | C: 35
Seclusion incidents I: 49 | 33 |
Intervention: Structured short-term risk assessment (Brøset Violence Checklist, Crisis Monitor, Kennedy–Axis V scale, Brief Psychiatric Rating Scale, Dangerousness Scale, Social Dysfunction and Aggression Scale)
Control: Treatment as usual |
40 weeks (10-week baseline period followed by a 30-week intervention period) |
Seclusion Duration of seclusion |
The study was funded by the Dutch Ministry of Health to investigate interventions that might contribute to the reduction of use of seclusion in The Netherlands.
The authors declared no conflicts of interest. |
High |
|
Abderhalden, 2008 Cluster-RCT, Switzerland |
Psychiatric wards treating patients with any acute psychiatric disorder. |
Participant Age (mean, SD) I: 39.0 (13.1) years C: 38.0 (14.3) years
Sex (% male) I: 54.4 | C: 55.2
Ward Number of beds (mean, SD) I: 17.5 (1.3) | C: 18.0 (1.2)
Nursing staff per bed (mean, SD) I: 0.67 (0.24) | C: 0.73 (0.08)
Length of stay (mean, SD) I: 20.7 (29.9) days C: 18.1 (26.5) days
Involuntary admissions (%) I: 41.4 | C: 38.4 |
Intervention: Structured short-term risk assessment (Brøset Violence Checklist) for every patient admission
Control: Treatment as usual |
6 months (3-month baseline period followed by a 3-month intervention period) |
Compulsory care |
The study was supported by grant 3251B0-100710 from the Swiss National Science Foundation.
The authors declared no conflicts of interest. |
High |
|
Included in systematic review Molyneaux (2019) |
|||||||
|
Papageorgiou, 2002· RCT, UK |
Inpatient compulsory treatment |
N at baseline I: 79 | C: 77
Age (mean, SD) I: 35.5 (11.3) years C: 36.3 (12.6) years
Sex (% male) I: 53 | C: 66
Number of days in hospital (grouped median, [min-max]) I: 94 (13-545) | C: 123 (13-1546)
Number of admissions in previous 5 years (grouped median, [min-max]) I: 1.3 (0-17) | C: 1.4 (0-10) |
Intervention: Advance statement
Control: Treatment as usual |
12 months |
Compulsory admission |
This work was funded by the National Health Service (NHS) Executive, London Research and Development Programme. The views expressed are those of the authors and not necessarily those of the NHS Executive or the Department of Health.
The authors declared no conflicts of interest. |
Low |
|
Henderson, 2004· RCT, UK
|
Severe mental illness and ≥1 admission in last 2 years |
N at baseline I: 80 | C: 80
Age (mean, SD) I: 39.5 (12.1) years C: 38.6 (10.6) years
Sex (% male) I: 59 | C: 59
Number of previous psychiatric admissions (median) I: 5 | C: 5 |
Intervention: Joint crisis plan
Control: Treatment as usual and information leaflet |
15 months |
Compulsory admission |
One author was supported by a Medical Research Council training fellowship in health services research, and one other author was supported by a South London and Maudsley Trust health services research committee grant.
The authors declared no conflicts of interest. |
Low |
|
Thornicroft, 2013· RCT, UK |
Relapsing psychotic disorder and ≥1 admission in last 2 years |
N at baseline I: 286 | C: 284
Age (mean, SD) I: 40.0 (11.8) years C: 39.6 (12.1) years
Sex (% male) I: 49 | C: 51
Number of admissions in previous 2 years (mean, SD) I: 1.54 (0.99) | C: 1.44 (0.88)
Total duration of admissions in previous 2 years (median, IQR) I: 66 (30-132) | C: 55 (31-123) |
Intervention: Joint crisis plan
Control: Treatment as usual |
18 months |
Compulsory admission Duration of compulsory admission
|
The study was funded by the Medical Research Council UK and the National Institute for Health Research. The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the manuscript.
The authors declared no conflicts of interest. |
Low |
|
Ruchlewska, 2014· RCT, the Netherlands |
Outpatient, psychotic/bipolar disorder, ≥1 crisis admission in last 2 years |
N at baseline I (PACP): 69 I (CCP): 70 C: 73
Age (mean, SD) I (PACP): 40.3 (10.9) years I (CCP): 40.6 (11.6) years C: 39.4 (11.6) years
Sex (% male) I (PACP): 72.5 I (CCP): 65.7 C: 67.1 |
Intervention: Two types of joint crisis plan 1) Patient advocate crisis plan (PACP) 2) Clinician facilitated crisis plan (CCP)
Control: Treatment as usual |
18 months |
Compulsory admission |
The trial was funded by the Dutch organization for health research and development (ZonMw) and BavoEuropoort. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declared no conflicts of interest. |
High |
|
Lay, 2018 RCT, Switzerland |
≥1 compulsory admissions to psychiatry during the past 2 years |
N at baseline I: 119 | C: 119
Age (mean, SD) I: 41.5 (12.3) years C: 43.4 (11.3) years
Sex (% male) I: 40.3 | C: 47.9
Psychiatric hospital admissions (mean, SD) I: 8.5 (12.1) | C: 9.3 (14.4)
Compulsory psychiatric admissions (mean, SD) I: 3.8 (5.2) | C: 4.8 (8.5) |
Intervention: Crisis plan with intensive monitoring
Control: Treatment as usual |
24 months |
Compulsory admission Duration of compulsory admission |
The study was funded by a private donation. The donator had no role in the study design or the collection, analysis, and interpretation of the data.
The authors declared no conflicts of interest. |
Some concerns |
|
Included in systematic review de Jong (2016) |
|||||||
|
Swartz, 1999 RCT, USA |
Severe mental illness > 1 year, decreasing Global Assessment of Functioning (GAF) score, intensive treatment for 2 years |
N at baseline I: 129 | C: 135
Age (mean, SD) I: 39.6 (10.4) years C: 39.8 (11.1) years
Sex (% male) I: 50.4 C: 49.6 |
Intervention: Community treatment order
Control: Case management |
12 months |
Compulsory admission
|
The study was supported by grants from NIMH.
Nothing is reported about potential conflicts of interest. |
High |
|
Steadman, 2001 RCT, USA
|
Referral to outpatient commitment program |
N at baseline I: 78 | C: 65
Age (mean, SD) I: 41 (11) years C: 41 (12) years
Sex (% male) I: 69 | C: 40
Length of stay for the index hospitalization (median) I: 53 days | C: 51 days |
Intervention: Community treatment order
Control: Standard care |
11 months |
Compulsory admission
|
Nothing is reported about potential funding source or conflicts of interest. |
Some concerns |
|
Burns, 2013 RCT, UK |
Currently detained with psychosis |
N at baseline I: 167 | C: 169
Age (mean, SD) I: 39.8 (11.2) years C: 39.5 (11.7) years
Sex (% male) I: 66 | C: 67
Past psychiatric hospital admissions (median, IQR) I: 6 (3-8) | C: 5 (3-9)
Past involuntary hospital admissions (median, IQR) I: 4 (2-7) | C: 3 (2-8) |
Intervention: Community treatment order
Control: Standard outpatient care |
12 months |
Compulsory admission Duration of compulsory admission |
The study was funded by the National Institute of Health Research. The sponsor of the trial had no role in trial design, data collection, data analysis, interpretation, or writing of the report.
The authors declared no conflicts of interest.
|
Low |
|
Staring, 2010 RCT, the Netherlands |
Outpatient, severe mental illness, problems with service engagement |
N at baseline I: 54 | C: 55
Age (mean, SD) 39.0 (11.6) years
Sex (% male) 71 |
Intervention: Treatment adherence
Control: Standard community mental health care |
12 months |
Compulsory admission |
Funding was provided by the Dutch Ministry of Health, Welfare, and Sports.
The authors declared no conflicts of interest. |
Some concerns |
|
Priebe, 2013 Cluster-RCT, UK |
Severe mental illness, receiving ≤75% of prescribed depot |
N at baseline I: 78 | C: 63
Age (mean, SD) I: 44.4 (9.6) years C: 42.7 (10.2) years
Sex (% male) I: 76 | C: 73
≥1 hospital admission in past year (n, %) I: 20 (26) | C: 12 (20)
CTO at time of randomization (n, %) I: 3 (4) | C: 4 (7) |
Intervention: Financial incentives
Control: Treatment as usual |
12 months |
Compulsory admission |
The study was funded by the National Institute for Health Research Health Technology Assessment program. The funder had no role in study design, data collection, data analysis, interpretation, writing of the report, or decision to submit for publication.
Potential conflicts of interest are reported. |
Low |
|
Johnson, 2005 RCT, UK |
Crisis severe enough to consider admission |
N at baseline I: 135 | C: 125
Age (mean, SD) I: 38.0 (11.9) years C: 37.8 (11.7) years
Sex (% male) I: 48 | C: 54
Previous psychiatric admission (n, %) I: 93 (69) | C: 89 (71) |
Intervention: Crisis resolution teams
Control: Standard care from inpatient services and community mental health teams |
6 months |
Compulsory admission Duration of compulsory admission |
The study was funded by the Camden and Islington Health Authority and the Department of Health.
The authors declared no conflicts of interest. |
Some concerns |
|
Ohlenschlaeger, 2008 RCT, Denmark |
First-episode schizophrenia spectrum disorder |
N at baseline I: 167 | C: 161 |
Intervention: Integrated care
Control: Standard care |
12 months |
Compulsory admission Physical and mechanical restraint Duration of physical and mechanical restraint Compulsory care Seclusion |
The trial was funded by grants from the Danish Ministry of Health and the Danish Medical Research Council. The Copenhagen Hospital Corporation funded the first author during the research period.
Nothing is reported about potential conflicts of interest. |
Some concerns |
|
Lay, 2015 RCT, Switzerland |
≥1 compulsory admission in last 2 years |
N at baseline I: 119 | C: 119
Age (mean, SD) I: 41.5 (12.3) years C: 43.4 (11.3) years
Sex (% male) I: 40 | C: 48
Psychiatric hospital admissions (mean, SD) I: 8.5 (12.1) | C: 9.3 (14.4)
Compulsory psychiatric admissions (mean, SD) I: 3.8 (5.2) | C: 4.8 (8.5) |
Intervention: Psychoeducation plus focused monitoring
Control: Treatment as usual |
12 months |
Compulsory admission Duration of compulsory admission |
The study is implemented as a sub-project within the framework of the Zurich Programme for Sustainable Development of Mental Health Services (ZInEP). ZInEP is funded by a private donation. The donator had no role in the study design or the collection, analysis, and interpretation of data.
The authors declared no conflicts of interest. |
High |
*For further details, see risk of bias table in the appendix.
+ Studies were included in Baker (2021) as well.
· Studies were included in de Jong (2016) as well.
Table 3. Characteristics of included RCTs
|
Study |
Main inclusion criteria |
Participant/ward characteristics |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias* |
|
Indregard, 2024 RCT, Norway |
Patients referred for acute psychiatric ward care |
N at baseline I: 245 | C: 311
Age (mean, SD) I: 41.6 (14.5) years C: 41.6 (14.3) years
Sex (% male) I: 49 | C: 55
Involuntary admission (n, %) I: 180 (73) | C: 234 (75)
Admission in previous 2 years (n, %) 0: I: 103 (42) | C: 149 (48) 1: I: 60 (24) | C: 60 (19) 2: I: 29 (12) | C: 42 (14) ≥3: I: 53 (22) | C: 60 (19) |
Intervention: Open-door policy
Control: Treatment as usual |
12 months |
Physical and mechanical restraint Seclusion Compulsory care |
The study was funded by public grants from the Research Council of Norway and the South-Eastern Norway Regional Health Authority. The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
The authors declared no competing interests. |
Some concerns |
|
Steinert, 2023 RCT, Germany |
Wards that admitted involuntary patients regardless of their diagnoses, routinely recorded data on coercive measures and incidents of aggression and had the support of personnel for the study's objectives. |
Ward N at baseline I: 27 | C: 27
Number of coercive measures used per month and occupied bed (median, IQR) I: 0.96 (1.34) C: 0.98 (1.71)
Number of assaults per month and occupied bed (median, IQR) I: 0.23 (0.57) C: 0.34 (0.57) |
Intervention: Implementation of recommendations of the PreVCo program
Control: Waiting list |
12 months |
Compulsory care |
The study was funded by the German Innovationsfonds beim Gemeinsamen Bundesausschuss. The funder had no role in study design or data collection.
Potential conflicts of interest are reported.
|
Some concerns |
|
Cornelis, 2022 RCT, the Netherlands |
Adults (18-65 years) with a diagnosis of at least one DSM-IV-TR or DSM-5 disorder who are experiencing an acute severe psychiatric crisis for which a psychiatrist indicated or executed a clinical admission |
N at baseline I: 183 | C: 63
Age (mean, SD) I: 40.0 (12.7) years C: 43.9 (12.2) years
Sex (% male) I: 43 | C: 52
Participants admitted in hospital (n, %) I: 18 (10) | C: 8 (13)
Participants admitted involuntary in hospital 1 year before initial crisis (n, %) I: 5 (28) | 1 (13)
Bed days of admitted participants (mean, SD) I: 28.1 (39.7) | C: 31.4 (35.1) |
Intervention: Intensive home treatment
Control: Treatment as usual |
12 months |
Compulsory admission Duration of compulsory admission
|
The study was funded by De Stichting tot Steun Vereniging voor Christelijke Verzorging van Geestes- en Zenuwzieken. The funder of the study had no role in the study design, data collection, data analysis, data interpretation, report writing, or the decision to submit the paper.
The authors declared no competing interests.
|
Some concerns |
|
Tinland, 2022 RCT, France |
Adults (>18 years) with a diagnosis of schizophrenia, bipolar disorder, or schizoaffective disorder according to the DSM-5 who were involuntary admitted to the hospital within the past 12 months |
N at baseline I: 196 | C: 198
Age (mean, SD) I: 37.4 (11.7) years C: 41.0 (12.7) years
Sex (% male) I: 65 | C: 57
Number of admissions in previous 1 year (mean, SD) I: 1.5 (0.9) | C: 1.4 (0.8)
Patients with admissions in previous 1 year (n, %) 1: I: 132 (67.3) | C: 148 (75.5) 2: I: 45 (23.0) | C: 37 (18.9) ≥3: I: 17 (8.7) | C: 11 (5.6) |
Intervention: Peer-worker psychiatric advance directives (PW-PAD)
Control: Treatment as usual |
12 months |
Compulsory admission |
This study was supported by an institutional grant from the French National Program of Health Services Research. The Clinical Research Direction of Assistance Publique Hôpitaux de Marseille was the sponsor of this trial. The funding sources had no role in the design or conduct of the study, collection, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Potential conflicts of interest are reported. |
Some concerns |
|
Valimaki, 2022 Cluster-RCT, Finland |
Hospitals with at least one adult psychiatric ward that used coercive measures as defined in the Finnish Mental Health Act |
Participant N at baseline I: 4163 | C: 4186
Age (mean, SD) I: 41.5 (6.5) years C: 40.0 (5.1) years
Sex (% male) I: 49 | C: 56
Patients involuntary admitted (n, %) I: 1146 (27.5) | C: 1488 (42.2)
Ward N at baseline I: 13 | C: 15
Number of beds I: 238 | C: 235
Number of nurses I: 335 | C: 313
Length of stay (mean, SD) I: 23.2 (20.4) days C: 31.8 (16.7) days |
Intervention: Evidence-based educational intervention (VIOLIN)
Control: Treatment as usual |
18 months |
Physical restraint Seclusion Duration of seclusion
|
This study was funded by grants from the Academy of Finland, the Turku University Hospital and the University of Turku. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Potential conflicts of interest are reported.
|
Some concerns |
|
Hamann, 2020 Cluster-RCT, Germany |
Adult (18-65 years) inpatients of participating acute psychiatric wards with a diagnosis of schizophrenia or schizoaffective disorder |
N at baseline I: 154 | C: 151
Age (mean, SD) I: 42.4 (12.9) years C: 41.2 (13.3) years
Sex (% male) I: 47 | C: 52
Patients involuntary admitted (n, %) I: 61 (40) | C: 42 (27) |
Intervention: SDM-plus training
Control: Treatment as usual |
12 months |
Mechanical restraint |
Janssen Cilag supported the trial with an unrestricted grant. The company had no influence on the design of the trial, the collection, analysis, and interpretation of the data.
Potential conflicts of interest are reported. |
Some concerns |
PICO 2 - Description of studies
No studies were included in the literature analysis.
PICO 1 - Results
1. Compulsory admission
Fifteen studies reported on the outcome measure compulsory admissions, defined as the number of compulsorily admitted patients (Burns, 2013; Henderson, 2004; Johnson, 2005; Lay, 2015; Lay, 2018; Ohlenschlaeger, 2008; Papageorgiou, 2002; Priebe, 2013; Ruchlewska, 2014; Staring, 2010; Steadman, 2001; Swartz, 1999; Thornicroft, 2013; Cornelis, 2022; Tinland, 2022).
The results were pooled using four subgroups based on the kind of prevention strategy that was studied (advance statements, community treatment orders, compliance enhancement, and intensive home treatment) (figure 1). Results of Johnson (2005), Lay (2015), and Ohlenschlaeger (2008) could not be pooled due to heterogeneity in the interventions studied.
The pooled data of RCTs studying advance statements show a risk ratio of 0.73 (95%CI 0.61 to 0.86) in favor of advance statements. The risk of compulsory admission had been reduced by 27%. This difference was considered clinically relevant. The pooled data of RCTs studying community treatment orders show a risk ratio of 0.95 (95%CI 0.81 to 1.10) favoring community treatment orders. This difference was considered not clinically relevant. The pooled data of RCTs studying compliance enhancement show a risk ratio of 0.52 (95%CI 0.11 to 2.37) in favor of compliance enhancement. The risk of compulsory admission had been reduced by 48%, which was considered a clinically relevant difference.
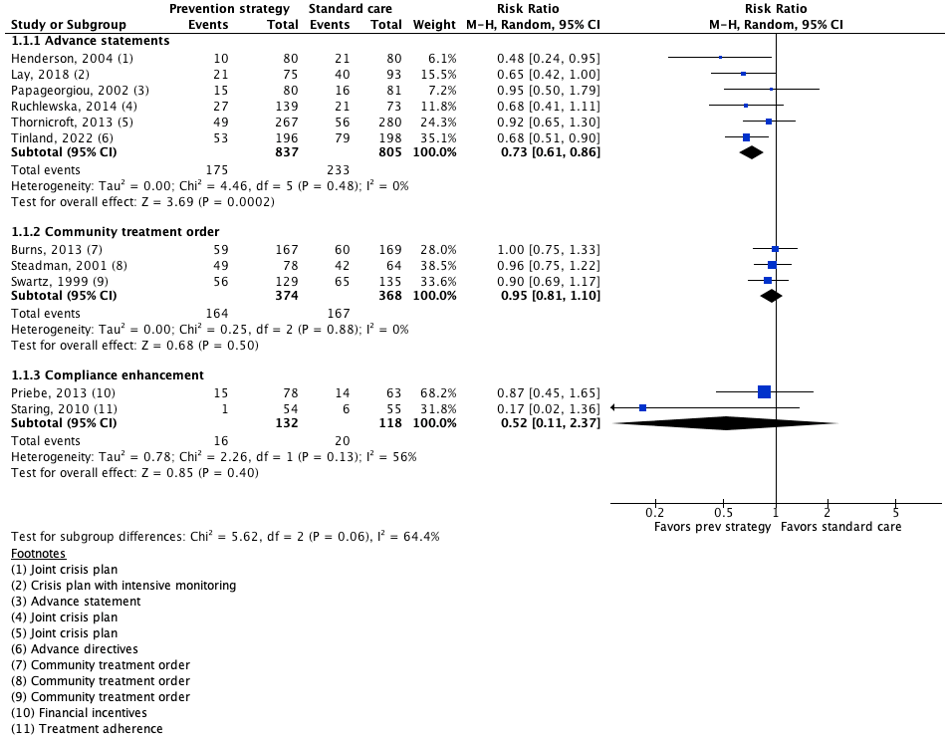
Figure 1: The effect of prevention strategies compared with standard care on compulsory admissions.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
Cornelis (2022) studied intensive home treatment reported that 62.3% (114/183) of participants in the intervention group (intensive home treatment) was compulsory admitted, compared to 73.0% (46/63) of participants in the control group (standard care). Risk ratio was 0.85 (95%CI 0.71 to 1.03), in favor of intensive home treatment. This difference is considered clinically relevant.
Johnson (2005) reported that 17.8% (24/135) of participants in the intervention group (crisis resolution) was compulsorily admitted, compared to 25.6% (32/125) of participants in the control group (standard care). Risk ratio was 0.69 (95%CI 0.43 to 1.11) in favor of crisis resolution. This difference is considered clinically relevant.
Lay (2015) found that 18 out of 80 (22.5%) participants in the intervention group (psychoeducation) were compulsorily admitted, compared to 36 out of 102 (35.3%) participants in the control group (treatment as usual). Risk ratio was 0.64 (95%CI 0.39 to 1.03) in favor of psychoeducation. This difference is considered clinically relevant.
Ohlenschlaeger (2008) reported that 16.8% (28/167) of participants in the intervention group (integrated care) was compulsorily admitted, compared to 14.3% (23/161) of participants in the control group (standard care). Risk ratio was 1.17 (95%CI 0.71 to 1.95) in favor of standard care. This difference is considered clinically relevant.
2. Physical and mechanical restraint
Seven studies reported on the incidence of physical and mechanical restraint (Celofiega, 2022; Hvidhjelm, 2022; Kontio, 2014; Ohlenschlaeger, 2008; Indregard, 2024; Valimaki, 2022; Hamann, 2020). Results could not be pooled due to heterogeneity in interventions and reporting of the outcome measure. For one study (Kontio, 2014), effect sizes ([standardized] mean difference/risk ratio) could not be calculated, because mean change values were reported.
Celofiega (2022) reported on the incidence of mechanical restraint (with belts) during the intervention period. The authors reported the use of mechanical restraint in 7.4% (100/1347) of patients in the de-escalation education group, and in 11.4% (213/1864) of patients in the treatment as usual group. Risk ratio was 0.65 (95%CI 0.52 to 0.82) in favor of de-escalation education (figure 2). This difference is considered clinically relevant.
Hvidhjelm (2022) reported on the mean incidence rate (number/month) of mechanical restraint. The mean (SD) rate of mechanical restraint use within the intervention period was 0.03 (0.10) for the START group (n=42) and 0.18 (0.39) for the control group (n=94). Mean difference was 0.15 (95%CI -0.23 to -0.07) in favor of START. This difference is considered clinically relevant.
Kontio (2014) reported mean (SD) changes in rates (incidents per 1000 occupied bed days) of mechanical restraint. The authors reported a mean change in the rates of mechanical restraint incidents of 2.9 (3.7) for the e-learning course wards, and 0.9 (1.0) for the treatment as usual wards.
Ohlenschlaeger (2008) reported on the number of patients mechanically restrained (use of a leather belt) and the number of patients physically restrained (use of force). The authors reported mechanical restraint in 7% (11/167) of patients in the integrated care group, and in 5% (8/161) of patients in the standard care group. Risk ratio was 1.33 (95%CI 0.55 to 3.21) in favor of standard care (figure 2). This difference is considered clinically relevant. Additionally, the authors reported physical restraint in 5% (9/167) of patients in the integrated care group, and in 3% (5/161) of patients in the standard care group. Risk ratio was 1.74 (95%CI 0.59 to 5.07) favoring standard care (figure 2). This difference is also considered clinically relevant.
Indregard (2024) reported on the number of patients mechanically restrained. The authors reported mechanical restraint in 3.3% (8/245) of patients in the open-door policy wards, and in 4.8% (15/311) of patients in the treatment as usual wards. Risk ratio was 0.68 (95%CI 0.29 to 1.57) favoring open-door policy (figure 2). This difference is considered clinically relevant. In addition, the authors also reported on physical restraint: 10.2% (25/245) in the open-door policy wards, and 12.9% (40/311) in the treatment as usual wards. Risk ratio was 0.79 (95%CI 0.50 to 1.27) in favor of open-door policy (figure 2). This difference is considered clinically relevant.
Valimaki (2022) reported on the number of patients physically restrained. Use of physical restraint was reported for 70 out of 4089 (1.7%) patients in the intervention group (VIOLIN) compared to 14 out of 4092 (0.3%) patients in the treatment as usual group. Risk ratio was 5.00 (95%CI 2.82 to 8.87) favoring treatment as usual, which was considered clinically relevant.
Hamann (2020) reported on the number of patients being mechanically restrained at least once during the intervention phase. Mechanical restraint was reported in 5% (7/154) of patients in the SDM-plus training group, and in 3% (4/151) of patients in the treatment as usual group. Risk ratio was 1.72 (95%CI 0.51 to 5.74) in favor of treatment as usual (figure 2). This difference was considered clinically relevant.
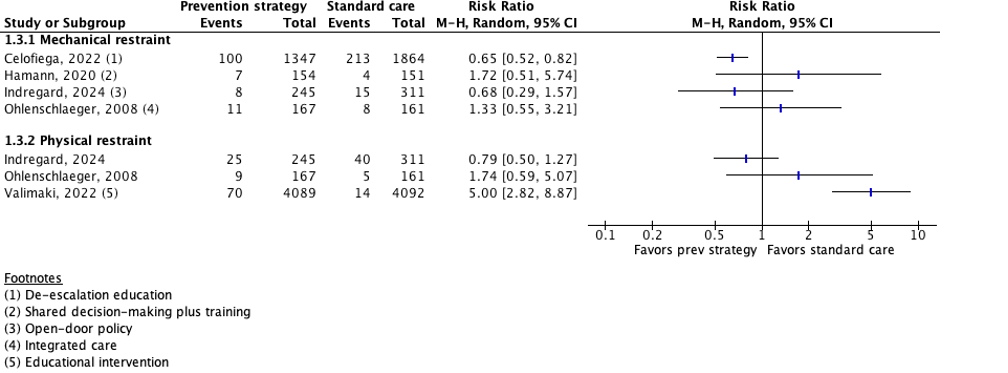
Figure 2: The effect of prevention strategies compared with standard care on physical and mechanical restraint.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
3. Seclusion
Five studies reported on the outcome measure seclusion (Kontio, 2014; Ohlenschlaeger, 2008; van de Sande, 2011; Indregard, 2024; Valimaki, 2022). Results could not be pooled due to heterogeneity in interventions and reporting of the outcome measures. Effect sizes ([standardized] mean difference/risk ratio) could not be calculated for Kontio (2014), because mean change values were reported.
Kontio (2014) reported mean (SD) changes in rates (incidents per 1000 occupied bed days) of seclusion. The authors reported a mean change in the rates of seclusion of 15.6 (9.2) for the e-learning course wards, and 8.7 (4.4) for the treatment as usual wards.
Ohlenschlaeger (2008) reported on the number of patients that were secluded (locked door). The authors reported that none of the patients in the integrated treatment group (n=167) were secluded, compared to three patients (2%) in the standard treatment group (n=161). Risk ratio was 0.14 (95%CI 0.01 to 2.65) favoring integrated treatment. This difference was considered clinically relevant.
Van de Sande (2011) reported on the number of patients that were secluded. The authors reported that 29% (60/207) of patients in the intervention wards (structured short-term risk assessment) were secluded compared to 17% (42/251) of patients in the control wards (treatment as usual). Risk ratio was 1.73 (95%CI 1.22 to 2.46) favoring treatment as usual. This difference was considered clinically relevant.
Indregard (2024) reported on the number of secluded patients. 5.3% (13/245) of patients in the open-door policy wards were secluded compared to 5.5% (17/311) of patients in the treatment as usual wards. Risk ratio was 0.97 (95%CI 0.48 to 1.96) favoring open-door policy. This difference was considered not clinically relevant.
Valimaki (2022) reported on the number of patients that were secluded. The authors reported that 437 out of 4089 (10.7%) of patients in the educational intervention group were secluded, and 512 out of 4092 (12.5%) of patients in the treatment as usual group. Risk ratio was 0.85 (95%CI 0.76 to 0.96), in favor of the educational intervention. This difference was considered clinically relevant.
4. Duration of compulsory admission
Six studies reported on the outcome measure duration of compulsory admission (Burns, 2013; Johnson, 2005; Lay, 2015; Lay, 2018; Thornicroft, 2013; Cornelis, 2022). Thornicroft (2013), Lay (2015) and Lay (2018) reported on the mean duration of compulsory admissions in days. Burns (2013) reported on the mean total duration of all psychiatric hospitalizations in nights. Johnson (2005) and Cornelis (2022) reported on mean bed days in hospitals/crisis house.
Results of Lay (2018) and Thornicroft (2013) were pooled (figure 3). Results of Johnson (2005) and Lay (2015) could not be pooled due to heterogeneity in the interventions studied. Results of Burns (2013) and Cornelis (2022) could not be pooled due to results of one study only.
The pooled data of RCTs studying advance statements show a standardized mean difference (SMD) of -0.13 (95%CI -0.48 to 0.22) in favor of advance statements. This difference was considered not clinically relevant.
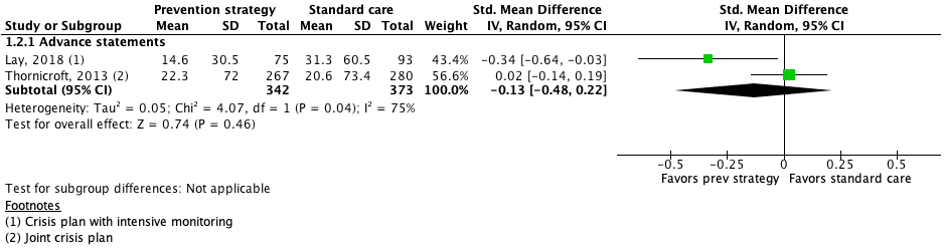
Figure 3: The effect of prevention strategies compared with standard care on the duration of compulsory admission.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval.
Johnson (2005) reported 21.3 (37.9) mean (SD) bed days in a hospital/crisis house for patients the intervention group (crisis resolution) compared to 38.6 (47) days for patients in the control group (standard care). Mean difference was 17.30 (95%CI -27.73 to -6.87) in favor of crisis resolution. This difference is considered clinically relevant.
Lay (2015) reported a mean (SD) duration of compulsory admission of 9.1 (21.8) days for the intervention group (psychoeducation) compared to 14.8 (31.2) days for the control group (treatment as usual). Mean difference was 5.70 (95%CI -13.41 to 2.01) in favor of psychoeducation. This difference is considered clinically relevant.
Burns (2013) reported a mean (SD) total duration of all psychiatric hospitalizations of 82.2 (102) nights for the intervention group (community treatment order) compared to 90.9 (104.5) nights for the control group (standard outpatient care). Mean difference was 8.70 (95%CI -30.88 to 13.48) in favor of community treatment order. This difference is considered not clinically relevant.
Cornelis (2022) reported on mean (SD) bed days in hospital. The authors reported 18.1 (17.7) mean bed days in hospital for the intervention group (intensive home treatment) and 24.2 (17.5) mean bed days in hospital for the control group (treatment as usual). Mean difference was 6.10 (95%CI -11.12 to -1.08) in favor of intensive home treatment. This difference is considered clinically relevant.
5. Duration of physical and mechanical restraint
Three studies reported on the duration of mechanical restraint (Hvidhjelm, 2022; Kontio, 2014; Ohlenschlaeger, 2008). Results could not be pooled due to variability in reporting of the outcome measure. For one study (Kontio, 2014), effect sizes ([standardized] mean difference/risk ratio) could not be calculated, because mean change values were reported.
Hvidhjelm (2022) reported on the mean (SD) duration of mechanical restraint. A mean mechanical restraint duration of 274 (1652) minutes was reported for the START group (n=42) compared to 609 (1950) minutes for the control group (n=94). Mean difference was 335 (95%CI -971.40 to 301.40) favoring START. This difference was considered not clinically relevant.
Kontio (2014) reported mean (SD) changes in time patient spent in mechanical restraint. The authors reported a mean change in time patient spent in mechanical restraint of 27.4 (67.2) for the e-learning course wards, and 26.7 (34.9) for the treatment as usual wards.
Ohlenschlaeger (2008) reported on the mean (SD) duration of mechanical restraint with the leather belt. They reported a mean duration of 19.4 (24.2) hours for the integrated care group (n=167), and 37.4 (50.3) hours in the standard care group (n=161). Mean difference was 18.0 (95%CI -26.59 to -9.41) in favor of integrated care. This difference was considered clinically relevant.
6. Compulsory care
Six studies reported on the outcome measure compulsory care, using different definitions (Abderhalden, 2008; Hvidhjelm, 2022; Ohlenschlaeger, 2008; Putkonen, 2013; Indregard, 2024; Steinert, 2023). Results could not be pooled due to variability in reporting of the outcome measure. For three studies (Abderhalden, 2008; Putkonen, 2013; Steinert, 2023), effect sizes ([standardized] mean difference/risk ratio) could not be calculated, because incidence rate(s) (ratio’s) or median (IQR) values were reported.
Abderhalden (2008) reported on compulsory care, defined as the overall incidence rate of coercion during the intervention period. The overall incidence rate of coercion was 1.75 (95%CI 1.47 to 2.07) per 100 hospitalization days in the intervention group (structured short-term risk assessment) (135 incidents involving 390 patients), and 1.20 (95%CI 1.00 to 1.43) per 100 hospitalization days in the control group (126 incidents involving 583 patients).
Bowers (2015) did not report sufficient results for GRADE evaluation; these results were therefore not graded.
Hvidhjelm (2022) reported on total coercive episodes, defined as the number of physical restraint episodes, episodes of acute forced medication, episodes of one-to-one observation, and mechanical restraint episodes. The mean (SD) rate of total use of coercion was 0.12 (0.32) for the START group (n=42), and 0.39 (0.94) for the control group (n=94). Mean difference was 0.27 (95%CI -0.48 to -0.06) in favor of START. This difference was considered clinically relevant.
Putkonen (2013) reported on compulsory care, defined as rates of seclusion, restraints, and room observation. The authors reported an incidence rate ratio of 0.88 (95%CI 0.86 to 0.90) for six core strategies wards, and 0.97 (95%CI 0.93 to 1.01) for control wards.
Ohlenschlaeger (2008) reported on the total number of patients subjected to coercive measure(s). 19% (31/167) of patients in the integrated care group were subjected to coercive measure(s) compared to 16% (25/161) of patients in the standard care group. Risk ratio was 1.20 (95%CI 0.74 to 1.93) favoring standard care. This difference was considered clinically relevant.
Indregard (2024) reported on the total number of patients subjected to one or more coercive measures during admission. The authors reported that 65 out of 245 (26.5%) of patients in the open-door policy wards were subjected to one or more coercive measures compared to 104 out of 311 (33.4%) of patients in the treatment as usual wards. Risk ratio was 0.79 (95%CI 0.61 to 1.03) in favor of open-door policy. This difference was considered clinically relevant.
Steinert (2023) reported on the median (IQR) number of coercive measures used per month and occupied bed. The authors reported a value of 0.53 (0.59) for the intervention wards (n=27) and 0.71 (1.08) for the waiting list wards (n=27).
7. Duration of seclusion
Three studies reported on duration of seclusion (Kontio, 2014; van de Sande, 2011; Valimaki, 2022). Effect sizes ([standardized] mean difference/risk ratio) could not be calculated, because mean change values were reported (Kontio, 2014) or due to missing dispersion measures (SD/SE) (van de Sande, 2011; Valimaki, 2022).
Kontio (2014) reported on mean (SD) changes in time patient spent in seclusion. A mean change of 42.8 (86.9) was reported for patients in the e-learning course wards, and 27.4 (67.2) for patients in the treatment as usual wards.
Van de Sande (2011) reported on seclusion duration. The authors reported a seclusion duration of 1624 hours during the intervention period for the structured short-term risk assessment wards and 2149 hours for the treatment as usual wards.
Valimaki (2022) reported on the length per seclusion event on ward level, expressed as geometric mean. The authors reported a seclusion length of 1762 minutes for the educational intervention group and 1614 minutes for the treatment as usual group.
8. Isolation (prevention, duration), 9. Care authorization
None of the studies reported on the outcome measures isolation and care authorization.
PICO 2 - Results
No studies were included in the literature analysis
Search and select
A systematic review of the literature was performed to answer the following question(s):
- What is the effectiveness of a prevention strategy compared to not applying a prevention strategy or standard care (‘treatment as usual’) in preventing compulsory care for patients with mental illness?
- What is the most effective prevention strategy to prevent compulsory care for patients with mental illness?
Table 1. PICO
|
Patients |
Patients with mental illness |
|
Intervention |
Prevention strategy to prevent compulsory care |
|
Control 1 |
Not applying a prevention strategy, standard care |
|
Control 2 |
Comparison between prevention strategies |
|
Outcomes |
Compulsory admission, physical and mechanical restraint, seclusion, duration of compulsory admission, duration of physical and mechanical restraint, compulsory care, duration of seclusion, isolation, care authorization |
|
Other selection criteria |
Study design: systematic reviews Published after 2005 |
Relevant outcome measures
The guideline panel considered compulsory admission, physical and mechanical restraint, and seclusion as critical outcome measures for decision making; and duration of compulsory admission, duration of physical and mechanical restraint, compulsory care, duration of seclusion, isolation, and care authorization as important outcome measures for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
For all outcome measures the guideline panel defined a 10% difference for dichotomous outcomes (0.9 ≥ RR ≥ 1.1) and 0.2 SD or -0.2 ≥ SMD ≥ 0.2 for continuous outcomes as a minimal clinically (patient) important difference.
Search and select (Methods)
The databases Medline (via OVID), Embase (via Embase.com), and PsycINFO (via OVID) were searched with relevant search terms from 2005 until 9 September 2024. The detailed search strategy is listed under the tab ‘Literature search strategy.’ The systematic literature search resulted in 405 hits. Studies were selected based on the following criteria:
- Systematic reviews in which searches were performed in at least two databases, with a detailed search strategy, risk of bias assessment and results of individual studies available;
- Full-text English or Dutch language publication; and
- Studies according to the PICO.
Initially, 29 systematic reviews were selected based on title and abstract screening. After reading the full text, 25 systematic reviews were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and four were selected for inclusion. Additionally, RCTs with a publication date of 2018 or more recent (based upon the last search date of the systematic review performed by Molyneaux, 2019) were screened. Twenty RCTs were selected based on title and abstract screening. After reading the full text, fourteen RCTs were excluded (see the exclusion table), and six were selected for inclusion.
All included studies compared a prevention strategy to standard care or not applying a prevention strategy (comparison 1), no studies were included that compared two different prevention strategies (comparison 2). Thus, the literature summary focuses specifically on comparison 1.
- Abderhalden C, Needham I, Dassen T, Halfens R, Haug HJ, Fischer JE. Structured risk assessment and violence in acute psychiatric wards: randomised controlled trial. Br J Psychiatry. 2008 Jul;193(1):44-50. doi: 10.1192/bjp.bp.107.045534. PMID: 18700217.
- Ali R, Walker S, Nyikavaranda P, Downs J, Patel R, Khondoker M, Bhui K, Hayes RD, de Freitas DF. Ethnicity and involuntary hospitalisation: a study of intersectional effects. Soc Psychiatry Psychiatr Epidemiol. 2025 Sep;60(9):2061-2075. doi: 10.1007/s00127-025-02898-0. Epub 2025 Apr 16. PMID: 40240693; PMCID: PMC12378639.
- Aragonés-Calleja M, Sánchez-Martínez V. Evidence synthesis on coercion in mental health: An umbrella review. Int J Ment Health Nurs. 2024 Apr;33(2):259-280. doi: 10.1111/inm.13248. Epub 2023 Oct 31. PMID: 37908175.
- Barnett P, Mackay E, Matthews H, Gate R, Greenwood H, Ariyo K, Bhui K, Halvorsrud K, Pilling S, Smith S. Ethnic variations in compulsory detention under the Mental Health Act: a systematic review and meta-analysis of international data. Lancet Psychiatry. 2019 Apr;6(4):305-317. doi: 10.1016/S2215-0366(19)30027-6. Epub 2019 Mar 4. PMID: 30846354; PMCID: PMC6494977.
- Barrett B, Waheed W, Farrelly S, Birchwood M, Dunn G, Flach C, Henderson C, Leese M, Lester H, Marshall M, Rose D, Sutherby K, Szmukler G, Thornicroft G, Byford S. Randomised controlled trial of joint crisis plans to reduce compulsory treatment for people with psychosis: economic outcomes. PLoS One. 2013 Nov 25;8(11):e74210. doi: 10.1371/journal.pone.0074210. PMID: 24282495; PMCID: PMC3839936.
- Burns T, Rugkåsa J, Molodynski A, Dawson J, Yeeles K, Vazquez-Montes M, Voysey M, Sinclair J, Priebe S. Community treatment orders for patients with psychosis (OCTET): a randomised controlled trial. Lancet. 2013 May 11;381(9878):1627-33. doi: 10.1016/S0140-6736(13)60107-5. Epub 2013 Mar 26. PMID: 23537605.
- Celofiga A, Kores Plesnicar B, Koprivsek J, Moskon M, Benkovic D, Gregoric Kumperscak H. Effectiveness of De-Escalation in Reducing Aggression and Coercion in Acute Psychiatric Units. A Cluster Randomized Study. Front Psychiatry. 2022 Apr 7;13:856153. doi: 10.3389/fpsyt.2022.856153. PMID: 35463507; PMCID: PMC9021532.
- Cornelis J, Barakat A, Blankers M, Peen J, Lommerse N, Eikelenboom M, Zoeteman J, Van H, Beekman ATF, Dekker J. The effectiveness of intensive home treatment as a substitute for hospital admission in acute psychiatric crisis resolution in the Netherlands: a two-centre Zelen double-consent randomised controlled trial. Lancet Psychiatry. 2022 Aug;9(8):625-635. doi: 10.1016/S2215-0366(22)00187-0. Epub 2022 Jun 30. PMID: 35779532.
- Daguman EI, Hutchinson M, Lakeman R. Uncovering Complexities in Reducing Aggression, Conflict and Restrictive Practices in Acute Mental Healthcare Settings: An Overview of Reviews. Int J Ment Health Nurs. 2024 Dec;33(6):1666-1686. doi: 10.1111/inm.13376. Epub 2024 Jun 17. PMID: 38886873.
- Doedens P, Vermeulen J, Boyette LL, Latour C, de Haan L. Influence of nursing staff attitudes and characteristics on the use of coercive measures in acute mental health services-A systematic review. J Psychiatr Ment Health Nurs. 2020 Aug;27(4):446-459. doi: 10.1111/jpm.12586. Epub 2020 Jan 14. PMID: 31876970; PMCID: PMC7508163.
- Efkemann SA, Scholten M, Bottlender R, Juckel G, Gather J. Influence of mental health professionals' attitudes and personality traits on decision-making around coercion: Results from an experimental quantitative survey using case vignettes. Acta Psychiatr Scand. 2022 Aug;146(2):151-164. doi: 10.1111/acps.13429. Epub 2022 Apr 4. PMID: 35322402.
- Gooding P. Compendium report - Good practices to promote Voluntary Measures in Mental Health Services. 2021. Council of Europe. Beschikbaar via: https://rm.coe.int/inf-2021-9-compendium-final-e/1680b11f60, geraadpleegd op 9 september 2025
- Hamann J, John M, Holzhüter F, Siafis S, Brieger P, Heres S. Shared decision making, aggression, and coercion in inpatients with schizophrenia. Eur Psychiatry. 2020 Sep 28;63(1):e90. doi: 10.1192/j.eurpsy.2020.88. PMID: 32981554; PMCID: PMC7576528.
- Henderson C, Flood C, Leese M, Thornicroft G, Sutherby K, Szmukler G. Effect of joint crisis plans on use of compulsory treatment in psychiatry: single blind randomised controlled trial. BMJ. 2004 Jul 17;329(7458):136. doi: 10.1136/bmj.38155.585046.63. Epub 2004 Jul 7. PMID: 15240438; PMCID: PMC478218.
- Hvidhjelm J, Brandt-Christensen M, Delcomyn C, Møllerhøj J, Siersma V, Bak J. Effects of Implementing the Short-Term Assessment of Risk and Treatability for Mechanical Restraint in a Forensic Male Population: A Stepped-Wedge, Cluster-Randomized Design. Front Psychiatry. 2022 Feb 24;13:822295. doi: 10.3389/fpsyt.2022.822295. PMID: 35280154; PMCID: PMC8907583.
- Indregard AR, Nussle HM, Hagen M, Vandvik PO, Tesli M, Gather J, Kunøe N. Open-door policy versus treatment-as-usual in urban psychiatric inpatient wards: a pragmatic, randomised controlled, non-inferiority trial in Norway. Lancet Psychiatry. 2024 May;11(5):330-338. doi: 10.1016/S2215-0366(24)00039-7. Epub 2024 Mar 6. PMID: 38460529.
- Inspectie voor Gezondheidszorg en Jeugd. Toetsingskader terugdringen insluiting. 2025. Beschikbaar via: https://www.igj.nl/documenten/2025/03/05/toetsingskader-terugdringen-insluiting, geraadpleegd op 14 november 2025
- Johnson S, Nolan F, Pilling S, Sandor A, Hoult J, McKenzie N, White IR, Thompson M, Bebbington P. Randomised controlled trial of acute mental health care by a crisis resolution team: the north Islington crisis study. BMJ. 2005 Sep 17;331(7517):599. doi: 10.1136/bmj.38519.678148.8F. Epub 2005 Aug 15. PMID: 16103032; PMCID: PMC1215550.
- Kinane C, Osborne J, Ishaq Y, Colman M, MacInnes D. Peer supported Open Dialogue in the National Health Service: implementing and evaluating a new approach to Mental Health Care. BMC Psychiatry. 2022 Feb 22;22(1):138. doi: 10.1186/s12888-022-03731-7. PMID: 35193551; PMCID: PMC8862567.
- Kontio R, Pitkänen A, Joffe G, Katajisto J, Välimäki M. eLearning course may shorten the duration of mechanical restraint among psychiatric inpatients: a cluster-randomized trial. Nord J Psychiatry. 2014 Oct;68(7):443-9. doi: 10.3109/08039488.2013.855254. Epub 2013 Nov 25. PMID: 24274836.
- Lay B, Blank C, Lengler S, Drack T, Bleiker M, Rössler W. Preventing compulsory admission to psychiatric inpatient care using psycho-education and monitoring: feasibility and outcomes after 12 months. Eur Arch Psychiatry Clin Neurosci. 2015 Apr;265(3):209-17. doi: 10.1007/s00406-014-0553-1. Epub 2014 Nov 1. PMID: 25361537.
- Lay B, Kawohl W, Rössler W. Outcomes of a psycho-education and monitoring programme to prevent compulsory admission to psychiatric inpatient care: a randomised controlled trial. Psychol Med. 2018 Apr;48(5):849-860. doi: 10.1017/S0033291717002239. Epub 2017 Aug 14. PMID: 28805175.
- Lim E, Wynaden D, Heslop K. Recovery-focussed care: How it can be utilized to reduce aggression in the acute mental health setting. Int J Ment Health Nurs. 2017 Oct;26(5):445-460. doi: 10.1111/inm.12378. PMID: 28960737.
- Molenaar H, Roode R.P. de, Attema S.J. Eigen regie en de Wvggz. JGGZR+. 2025 Sept;3:20-24.
- Moss K, Wyder M, Braddock V, Arroyo D, Kisely S. Compulsory community treatment and ethnicity: Findings from a culturally and linguistically diverse area of Queensland. Int J Law Psychiatry. 2019 Jan-Feb;62:154-159. doi: 10.1016/j.ijlp.2018.09.007. Epub 2018 Sep 28. PMID: 30274852.
- Ohlenschlaeger J, Nordentoft M, Thorup A, Jeppesen P, Petersen L, Christensen TØ, Krarup G, Jørgensen P. Effect of integrated treatment on the use of coercive measures in first-episode schizophrenia-spectrum disorder. A randomized clinical trial. Int J Law Psychiatry. 2008 Jan-Feb;31(1):72-6. doi: 10.1016/j.ijlp.2007.11.003. Epub 2008 Jan 9. PMID: 18191455.
- Papageorgiou A, King M, Janmohamed A, Davidson O, Dawson J. Advance directives for patients compulsorily admitted to hospital with serious mental illness. Randomised controlled trial. Br J Psychiatry. 2002 Dec;181:513-9. doi: 10.1192/bjp.181.6.513. PMID: 12456522.
- Plomp E. Legemaate J. Verdiepingsonderzoek Uitvoering Wvggz: goede voorbeelden uit de praktijk. 2024. ZonMW, Den Haag. Beschikbaar via Eindrapport-Verdiepingsonderzoek-Uitvoering-Wvggz-def.pdf. Geraadpleegd op 9 september 2025.
- Priebe S, Yeeles K, Bremner S, Lauber C, Eldridge S, Ashby D, David AS, O'Connell N, Forrest A, Burns T. Effectiveness of financial incentives to improve adherence to maintenance treatment with antipsychotics: cluster randomised controlled trial. BMJ. 2013 Oct 7;347:f5847. doi: 10.1136/bmj.f5847. PMID: 24100934; PMCID: PMC3805491.
- Prinsen E, Wel B van, Mulder N, Koning N de. Handboek IHT – Intensive Home Treatment (eerste druk). 2016. De Tijdstroom, Utrecht. ISBN: 9789058983053
- Putkonen A, Kuivalainen S, Louheranta O, Repo-Tiihonen E, Ryynänen OP, Kautiainen H, Tiihonen J. Cluster-randomized controlled trial of reducing seclusion and restraint in secured care of men with schizophrenia. Psychiatr Serv. 2013 Sep 1;64(9):850-5. doi: 10.1176/appi.ps.201200393. PMID: 23771480.
- Ruchlewska A, Wierdsma AI, Kamperman AM, van der Gaag M, Smulders R, Roosenschoon BJ, Mulder CL. Effect of crisis plans on admissions and emergency visits: a randomized controlled trial. PLoS One. 2014 Mar 19;9(3):e91882. doi: 10.1371/journal.pone.0091882. PMID: 24647274; PMCID: PMC3960137.
- Shea T, Dotson S, Tyree G, Ogbu-Nwobodo L, Beck S, Shtasel D. Racial and Ethnic Inequities in Inpatient Psychiatric Civil Commitment. Psychiatr Serv. 2022 Dec 1;73(12):1322-1329. doi: 10.1176/appi.ps.202100342. Epub 2022 Aug 12. PMID: 35959533.
- Simon J, Mayer S, Łaszewska A, Rugkåsa J, Yeeles K, Burns T, Gray A. Cost and quality-of-life impacts of community treatment orders (CTOs) for patients with psychosis: economic evaluation of the OCTET trial. Soc Psychiatry Psychiatr Epidemiol. 2021 Jan;56(1):85-95. doi: 10.1007/s00127-020-01919-4. Epub 2020 Jul 27. PMID: 32719905; PMCID: PMC7847440.
- Staring AB, Van der Gaag M, Koopmans GT, Selten JP, Van Beveren JM, Hengeveld MW, Loonen AJ, Mulder CL. Treatment adherence therapy in people with psychotic disorders: randomised controlled trial. Br J Psychiatry. 2010 Dec;197(6):448-55. doi: 10.1192/bjp.bp.110.077289. PMID: 21119150.
- Steadman HJ, Gounis K, Dennis D, Hopper K, Roche B, Swartz M, Robbins PC. Assessing the New York City involuntary outpatient commitment pilot program. Psychiatr Serv. 2001 Mar;52(3):330-6. doi: 10.1176/appi.ps.52.3.330. PMID: 11239100.
- Steinert T, Baumgardt J, Bechdolf A, Bühling-Schindowski F, Cole C, Flammer E, Jaeger S, Junghanss J, Kampmann M, Mahler L, Muche R, Sauter D, Vandamme A, Hirsch S. Implementation of guidelines on prevention of coercion and violence (PreVCo) in psychiatry: a multicentre randomised controlled trial. Lancet Reg Health Eur. 2023 Nov 20;35:100770. doi: 10.1016/j.lanepe.2023.100770. PMID: 38058297; PMCID: PMC10696231.
- Swartz MS, Swanson JW, Wagner HR, Burns BJ, Hiday VA, Borum R. Can involuntary outpatient commitment reduce hospital recidivism?: Findings from a randomized trial with severely mentally ill individuals. Am J Psychiatry. 1999 Dec;156(12):1968-75. doi: 10.1176/ajp.156.12.1968. PMID: 10588412.
- Thornicroft G, Farrelly S, Szmukler G, Birchwood M, Waheed W, Flach C, Barrett B, Byford S, Henderson C, Sutherby K, Lester H, Rose D, Dunn G, Leese M, Marshall M. Clinical outcomes of Joint Crisis Plans to reduce compulsory treatment for people with psychosis: a randomised controlled trial. Lancet. 2013 May 11;381(9878):1634-41. doi: 10.1016/S0140-6736(13)60105-1. Epub 2013 Mar 26. PMID: 23537606.
- Tinland A, Loubière S, Mougeot F, Jouet E, Pontier M, Baumstarck K, Loundou A, Franck N, Lançon C, Auquier P; DAiP Group. Effect of Psychiatric Advance Directives Facilitated by Peer Workers on Compulsory Admission Among People With Mental Illness: A Randomized Clinical Trial. JAMA Psychiatry. 2022 Aug 1;79(8):752-759. doi: 10.1001/jamapsychiatry.2022.1627. PMID: 35662314; PMCID: PMC9171654.
- Tseng PY, Xie XY, Hsu CC, Chien SH, Chen JD, Wang JY. Investigating Medical Cost and Mortality Among Psychiatric Patients Involuntary Admissions: A Nationwide Propensity Score-Matched Study. Psychiatry Investig. 2022 Jul;19(7):527-537. doi: 10.30773/pi.2021.0219. Epub 2022 Jul 21. PMID: 35903055; PMCID: PMC9334811.
- Välimäki M, Lantta T, Anttila M, Vahlberg T, Normand SL, Yang M. An Evidence-Based Educational Intervention for Reducing Coercive Measures in Psychiatric Hospitals: A Randomized Clinical Trial. JAMA Netw Open. 2022 Aug 1;5(8):e2229076. doi: 10.1001/jamanetworkopen.2022.29076. PMID: 36040740; PMCID: PMC9428738.
- van de Sande R, Nijman HL, Noorthoorn EO, Wierdsma AI, Hellendoorn E, van der Staak C, Mulder CL. Aggression and seclusion on acute psychiatric wards: effect of short-term risk assessment. Br J Psychiatry. 2011 Dec;199(6):473-8. doi: 10.1192/bjp.bp.111.095141. Epub 2011 Oct 20. PMID: 22016437.
- Voskes Y, van Melle L, Jehoel-van As M, Mulder N, van Mierlo T. Werkboek HIC. 2026. Boom, Amsterdam. ISBN: 9789024476633.
- Walker S, Mackay E, Barnett P, Sheridan Rains L, Leverton M, Dalton-Locke C, Trevillion K, Lloyd-Evans B, Johnson S. Clinical and social factors associated with increased risk for involuntary psychiatric hospitalisation: a systematic review, meta-analysis, and narrative synthesis. Lancet Psychiatry. 2019 Dec;6(12):1039-1053. doi: 10.1016/S2215-0366(19)30406-7. PMID: 31777340; PMCID: PMC7029280
Risk of Bias tables
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated? |
Was the allocation adequately concealed? |
Blinding: Was knowledge of the allocated interventions adequately prevented? |
Was loss to follow-up (missing outcome data) infrequent? |
Are reports of the study free of selective outcome reporting? |
Was the study apparently free of other problems that could put it at a risk of bias? |
Overall risk of bias If applicable/necessary, per outcome measure |
|
Celofiega, 2022 |
No information |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: No hospitals were lost to follow-up. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably no
Reason: Randomization was performed at hospital level instead of individual ward level. This reduced the power of the study. |
High |
|
Hvidhjelm, 2022 |
Definitely yes
Reason: A random number generator in the statistics software was used. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: Not reported. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Kontio, 2014 |
Definitely no
Reason: Wards were randomly assigned by tossing a coin. However, bot wards with difficult-to-manage patients fell into the intervention group while both acute-subacute wards fell into the control group. |
Probably no
Reason: Wards were aware of their allocation arm. |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: Not reported. |
Definitely yes
Reason: Outcomes are reported as prespecified in aims and hypothesis. |
Probably yes
Reason: No other problems reported. |
High |
|
Putkonen, 2013 |
Probably no
Reason: Allocation of participants was based on treatment ward (place-based allocation). But intervention and control wards were stratified by use of seclusion and restraint to avoid the possibility of unbalanced comparisons. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: Not reported. |
Definitely yes
Reason: Outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
High |
|
Bowers, 2015 |
Probably yes
Reason: Simple randomization was used to assign wards to the experimental or control condition. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably no
Reason: No wards dropped out from the study. But the large quantity of missing data is reported as a study limitation. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Van de Sande, 2011 |
Definitely no
Reason: Randomization was not completely successful due to significant differences between groups at baseline. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
No information |
Definitely yes
Reason: Outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
High |
|
Abderhalden, 2008 |
Probably yes
Reason: Randomization was carried out based on a computer-generated random number list. There still were some baseline differences. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
No information |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
High |
|
Papageorgiou, 2002 |
Definitely yes
Reason: Block-design was used with blocks of twelve random combinations. |
Definitely yes
Reason: Sealed envelopes were used. |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Definitely yes
Reason: Missing outcome data is balanced in numbers across both groups. Missing data has been imputed by LOCF analyses. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Low |
|
Henderson, 2004 |
Definitely yes
Reason: Participants were randomized by using minimization, stratified by team and by severity of the patients’ condition to ensure even distributions. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Definitely yes
Reason: Missing outcome data is balanced in numbers across both groups. Not related to intervention. ITT analyses. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Low |
|
Thornicroft, 2013 |
Definitely yes
Reason: Patients were randomized using permuted blocks of randomly varying block size, with equal allocation to both groups. |
Definitely yes
Reason: Web-based allocation. |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Definitely yes
Reason: 46/285 participants were lost to follow-up in intervention group compared to 19/284 in control group. ITT analyses were performed. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Low |
|
Ruchlewska, 2014 |
No information |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably no
Reason: A lot of patients did not complete the crisis plan (30% and 43%) compared to no dropouts in the control group. ITT analyses were performed. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
High |
|
Lay, 2018 |
Probably yes
Reason: Block-random allocation within centres was used. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably no
Reason: 37% of patients in the intervention compared to 22% in the control group were lost to follow-up. ITT analyses were performed. Retrospective imputation approach was used. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Swartz, 1999 |
No information |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: Attrition from the study was 18% and did not differ significantly across study groups (control subjects, 16%; subjects in outpatient commitment, 21%). |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
High |
|
Steadman, 2001 |
Definitely yes
Reason: Randomization was performed by using a random number list. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: Not reported. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Burns, 2013 |
Definitely yes
Reason: Randomization used random permuted blocks with lengths of two, four, and six, and stratified for sex, schizophrenic diagnosis, and duration of illness. |
Definitely yes
Reason: Sequentially numbered, opaque, sealed envelopes were used. |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Definitely yes
Reason: Missing outcome data is balanced in numbers across both groups. Imputation methods were used.
|
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Low |
|
Staring, 2010 |
Definitely yes
Reason: Randomization was performed by using a lottery system. |
Definitely no
Reason: Allocation was not concealed from the participants, therapists or researchers. |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Definitely yes
Reason: Missing outcome data is balanced in numbers across both groups. ITT analyses were performed. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Priebe, 2013 |
Definitely yes
Reason: Block randomization was used with blocks of random length. Stata was used. |
Probably yes
Reason: A researcher informed the participants of their allocation. |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Definitely yes
Reason: Very few patients were lost to follow up (n=0 in intervention group, and n=3 in control group). |
No information |
Probably yes
Reason: No other problems reported. |
Low |
|
Johnson, 2005 |
No information |
Probably yes
Reason: The health services research unit of the University of Aberdeen allocated participants at random to the experimental or control group. |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Definitely yes
Reason: Few missing data (n=1 for both groups for admission, and n=1 (I) and n=2 (C) for bed use. |
No information |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Ohlenschlaeger, 2008 |
Definitely yes
Reason: Central randomization was used. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: Not reported. |
Definitely yes
Reason: Primary and secondary outcomes are reported as prespecified in methods section. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Lay, 2015 |
No information
|
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
No information |
Definitely yes
Reason: Outcomes are reported as prespecified in aims and hypothesis. |
Probably yes
Reason: No other problems reported. |
High |
|
Indregard, 2024 |
Definitely yes
Reason: Allocation sequence was a simple binomial list allocating participants to either group in a 2:3 ratio. A random number generator was used (random.org). |
Definitely no
Reason: Open-label continuous allocation sequence. |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Definitely yes
Reason: 4 participants (1.6%) discontinued the intervention, and 5 participants (1.6%) discontinued treatment as usual. ITT analyses were performed. |
Definitely yes
Reason: Trial is registered (ISRCTN16876467). Primary and secondary outcomes are reported as prespecified. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Steinert, 2023 |
Probably yes
Reason: Wards were randomized to intervention or control group by a 1:1 matched randomization. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
No information |
Definitely yes
Reason: Trial is registered (ISRCTN71467851). Primary and secondary outcomes are reported as prespecified. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Cornelis, 2022 |
Probably yes
Reason: A seeded pseudo-random number generator was used. The seed was based on patient characteristics. Allocation took place in a 2:1 ratio. (groups were not comparable at baseline) |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: A lot of participants in both groups declined participation, but multiple imputations using chained equations were used for missing data. |
Definitely yes
Reason: Trial is registered (NL6020, NTR-6151). Primary and secondary outcomes are reported as prespecified. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Tinland, 2022 |
Definitely yes
Reason: Participants were randomly assigned using a web-based system in a 1:1 ratio. The randomization list used a permuted block design and was stratified by center. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: Interviews at the 12-month follow-up were completed for 127 (65%) in the PW-PAD group and 139 (70%) in the control group. Missing data were addressed using multiple imputations. |
Definitely yes
Reason: Trial is registered (NCT03630822). Primary and secondary outcomes are reported as prespecified. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Valimaki, 2022 |
Definitely yes
Reason: Randomization was centralized, concealed and computer generated by an independent statistician. Randomization was stratified by the number of nursing staff vacancies and beds on each study ward. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: Of 28 psychiatric wards screened, 27 completed the study. One ward was closed during the study period, and 16 nurses were lost to follow-up. |
Definitely yes
Reason: Trial is registered (NCT02724748). Primary and secondary outcomes are reported as prespecified. |
Probably yes
Reason: No other problems reported. |
Some concerns |
|
Hamann, 2020 |
Definitely yes
Reason: A blinded member of the statistical department generated binary random variables using the statistical software R. |
No information |
Probably yes
Reason: In this research field, it is impossible to blind participants and health care professionals, but it remains unclear whether this awareness led to bias. |
Probably yes
Reason: No wards were lost to follow-up, but 34 (21%) and 31 (19%) patients were lost. ITT analyses were performed. |
Probably yes
Reason: Trial is registered at Deutsches Register Klinischer Studien (DRKS00010880). There is no reason to doubt that the study is free of selective outcome reporting. |
Probably yes
Reason: No other problems reported. |
Some concerns |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Dahm KT, Steiro AK, Leiknes KA, Husum TL, Kirkehei I, Dalsbø TK, Brurberg KG. Interventions for Reducing Seclusion and Restraint in Mental Health Care for Adults: A Systematic Review [Internet]. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Dec 19. Report from the Norwegian Institute of Public Health No. 2017-26. PMID: 29553686. |
Excerpt from the full report, which is written in Norwegian, describes only descriptive results. |
|
Goulet, M.-H., Larue, C., & Dumais, A. (2017). Evaluation of seclusion and restraint reduction programs in mental health: A systematic review. Aggression and Violent Behavior, 34, 139–146. https://doi.org/10.1016/j.avb.2017.01.019 |
Includes only two possibly relevant RCTs, but is less recent and complete compared to Pedersen (2024). |
|
Ye J, Xiao A, Yu L, Guo J, Lei H, Wei H, Luo W. Staff Training Reduces the Use of Physical Restraint in Mental Health Service, Evidence-based Reflection for China. Arch Psychiatr Nurs. 2018 Jun;32(3):488-494. doi: 10.1016/j.apnu.2017.11.028. Epub 2017 Nov 22. PMID: 29784235. |
Includes only two relevant RCTs (Kotio, 2014; Putkonen, 2013), which are also included in Pedersen (2024) and Baker (2021) which are more recent. |
|
Oostermeijer S, Brasier C, Harvey C, Hamilton B, Roper C, Martel A, Fletcher J, Brophy L. Design features that reduce the use of seclusion and restraint in mental health facilities: a rapid systematic review. BMJ Open. 2021 Jul 7;11(7):e046647. doi: 10.1136/bmjopen-2020-046647. PMID: 34233981; PMCID: PMC8264870. |
Includes no RCTs. |
|
Kisely S, Hall K. An updated meta-analysis of randomized controlled evidence for the effectiveness of community treatment orders. Can J Psychiatry. 2014 Oct;59(10):561-4. doi: 10.1177/070674371405901010. Erratum in: Can J Psychiatry. 2017 May;62(5):357. doi: 10.1177/0706743717708348. PMID: 25565690; PMCID: PMC4197791. |
Included studies are not extensively described. Relevant included studies are included in de Jong (2016) which is a more recent SR. |
|
Lam EHY, Lai ESK, Lai ECL, Lau E, Siu BWM, Tang DYY, Mok CCM, Lam M. Effect of Community Treatment Orders on Mental Health Service Usage, Emergency Visits, and Violence: a Systematic Review and Meta-Analysis. East Asian Arch Psychiatry. 2023 Jun;33(2):37-43. doi: 10.12809/eaap2246. PMID: 37400226. |
Includes no RCTs, describes no outcome measures that are conform the PICO of this module. |
|
Haig S, Hallett N. Use of sensory rooms in adult psychiatric inpatient settings: A systematic review and narrative synthesis. Int J Ment Health Nurs. 2023 Feb;32(1):54-75. doi: 10.1111/inm.13065. Epub 2022 Sep 9. PMID: 36082841. |
Includes pre-post studies and qualitative studies only. |
|
Barnett P, Matthews H, Lloyd-Evans B, Mackay E, Pilling S, Johnson S. Compulsory community treatment to reduce readmission to hospital and increase engagement with community care in people with mental illness: a systematic review and meta-analysis. Lancet Psychiatry. 2018 Dec;5(12):1013-1022. doi: 10.1016/S2215-0366(18)30382-1. Epub 2018 Nov 1. PMID: 30391280; PMCID: PMC6251967. |
Results are descriptively reported, no raw data presented. |
|
Quinn M, Jutkowitz E, Primack J, Lenger K, Rudolph J, Trikalinos T, Rickard T, Mai HJ, Balk E, Konnyu K. Protocols to reduce seclusion in inpatient mental health units. Int J Ment Health Nurs. 2024 Jun;33(3):600-615. doi: 10.1111/inm.13277. Epub 2024 Jan 9. PMID: 38193620. |
Results are descriptively reported, no raw data presented. |
|
Borckardt JJ, Grubaugh AL, Pelic CG, Danielson CK, Hardesty SJ, Frueh BC. Enhancing patient safety in psychiatric settings. J Psychiatr Pract. 2007 Nov;13(6):355-61. doi: 10.1097/01.pra.0000300121.99193.61. PMID: 18032980. |
Non-systematic literature review. |
|
Allen DE, Fetzer S, Siefken C, Nadler-Moodie M, Goodman K. Decreasing Physical Restraint in Acute Inpatient Psychiatric Hospitals: A Systematic Review. J Am Psychiatr Nurses Assoc. 2019 Sep/Oct;25(5):405-409. doi: 10.1177/1078390318817130. Epub 2018 Dec 20. Erratum in: J Am Psychiatr Nurses Assoc. 2020 Mar/Apr;26(2):219. doi: 10.1177/1078390319883630. PMID: 30569807. |
Includes no RCTs. Results are descriptively reported, no raw data presented. |
|
Bak J, Brandt-Christensen M, Sestoft DM, Zoffmann V. Mechanical restraint--which interventions prevent episodes of mechanical restraint?- a systematic review. Perspect Psychiatr Care. 2012 Apr;48(2):83-94. doi: 10.1111/j.1744-6163.2011.00307.x. Epub 2011 Apr 19. Erratum in: Perspect Psychiatr Care. 2012 Jul;48(3):183-4. PMID: 21967236. |
Methods are unclear. (Old) SR of insufficient quality. |
|
Gaynes BN, Brown CL, Lux LJ, Brownley KA, Van Dorn RA, Edlund MJ, Coker-Schwimmer E, Weber RP, Sheitman B, Zarzar T, Viswanathan M, Lohr KN. Preventing and De-escalating Aggressive Behavior Among Adult Psychiatric Patients: A Systematic Review of the Evidence. Psychiatr Serv. 2017 Aug 1;68(8):819-831. doi: 10.1176/appi.ps.201600314. Epub 2017 Apr 17. PMID: 28412887. |
Results are descriptively reported, no raw data presented. |
|
Carpenter RA, Falkenburg J, White TP, Tracy DK. Crisis teams: systematic review of their effectiveness in practice. The Psychiatrist. 2013;37(7):232-237. doi:10.1192/pb.bp.112.039933 |
Results are descriptively reported, no raw data presented. Included only one RCT. |
|
Maughan D, Molodynski A, Rugkåsa J, Burns T. A systematic review of the effect of community treatment orders on service use. Soc Psychiatry Psychiatr Epidemiol. 2014 Apr;49(4):651-63. doi: 10.1007/s00127-013-0781-0. Epub 2013 Oct 18. PMID: 24136002. |
Included only one RCT (Burns, 2013) which is included in de Jong (2016), which is more recent. |
|
Brenig, D., Gade, P. & Voellm, B. Is mental health staff training in de-escalation techniques effective in reducing violent incidents in forensic psychiatric settings? – A systematic review of the literature. BMC Psychiatry 23, 246 (2023). https://doi.org/10.1186/s12888-023-04714-y |
Includes four studies without control group and one study with a post-test-only design. |
|
Kisely S. Canadian Studies on the Effectiveness of Community Treatment Orders. Can J Psychiatry. 2016 Jan;61(1):7-14. doi: 10.1177/0706743715620414. PMID: 27582448; PMCID: PMC4756603. |
Includes no RCTs, describes no outcome measures that are conform the PICO of this module. |
|
Muralidharan S, Fenton M. Containment strategies for people with serious mental illness. Cochrane Database Syst Rev. 2006 Jul 19;2006(3):CD002084. doi: 10.1002/14651858.CD002084.pub2. PMID: 16855984; PMCID: PMC11384505. |
Includes no studies, describes no outcome measures that are conform the PICO of this module. |
|
Lantta T, Duxbury J, Haines-Delmont A, Björkdahl A, Husum TL, Lickiewicz J, Douzenis A, Craig E, Goodall K, Bora C, Whyte R, Whittington R. Models, frameworks and theories in the implementation of programs targeted to reduce formal coercion in mental health settings: a systematic review. Front Psychiatry. 2023 Jun 15;14:1158145. doi: 10.3389/fpsyt.2023.1158145. PMID: 37398581; PMCID: PMC10311067. |
Describes no outcome measures that are conform the PICO of this module (focuses on implementation). |
|
McDonnell AA, O'Shea MC, Bews-Pugh SJ, McAulliffe H, Deveau R. Staff training in physical interventions: a literature review. Front Psychiatry. 2023 Jul 26;14:1129039. doi: 10.3389/fpsyt.2023.1129039. PMID: 37564241; PMCID: PMC10411725. |
Includes only one possibly relevant RCT. |
|
Price O, Papastavrou Brooks C, Johnston I, McPherson P, Goodman H, Grundy A, Cree L, Motala Z, Robinson J, Doyle M, Stokes N, Armitage CJ, Barley E, Brooks H, Callaghan P, Carter LA, Davies LM, Drake RJ, Lovell K, Bee P. Development and evaluation of a de-escalation training intervention in adult acute and forensic units: the EDITION systematic review and feasibility trial. Health Technol Assess. 2024 Jan;28(3):1-120. doi: 10.3310/FGGW6874. PMID: 38343036; PMCID: PMC11017147. |
Includes no RCTs. |
|
Stephenson L, Gieselmann A, Gergel T, Owen G, Gather J, Scholten M. Self-binding directives in psychiatric practice: a systematic review of reasons. Lancet Psychiatry. 2023 Nov;10(11):887-895. doi: 10.1016/S2215-0366(23)00221-3. Epub 2023 Sep 12. PMID: 37714174. |
Wrong publication type (systematic review of reasons for and against the use of self-binding directives in psychiatric practice). |
|
Strand M, von Hausswolff-Juhlin Y. Patient-controlled hospital admission in psychiatry: A systematic review. Nord J Psychiatry. 2015;69(8):574-86. doi: 10.3109/08039488.2015.1025835. Epub 2015 Apr 2. PMID: 25832757. |
Includes no RCTs. |
|
Gaillard AS, Braun E, Vollmann J, Gather J, Scholten M. The Content of Psychiatric Advance Directives: A Systematic Review. Psychiatr Serv. 2023 Jan 1;74(1):44-55. doi: 10.1176/appi.ps.202200002. Epub 2022 Aug 30. PMID: 36039553. |
Descriptive review on psychiatric advance directives. No focus on prevention. |
|
Gaynes BN, Brown C, Lux LJ, Brownley K, Van Dorn R, Edlund M, Coker-Schwimmer E, Zarzar T, Sheitman B, Weber RP, Viswanathan M, Lohr KN. Strategies To De-escalate Aggressive Behavior in Psychiatric Patients [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Jul. Report No.: 16-EHC032-EF. PMID: 27536754. |
Update available (Gaynes, 2017). |
|
Thomsen CT, Benros ME, Maltesen T, Hastrup LH, Andersen PK, Giacco D, Nordentoft M. Patient-controlled hospital admission for patients with severe mental disorders: a nationwide prospective multicentre study. Acta Psychiatr Scand. 2018 Apr;137(4):355-363. doi: 10.1111/acps.12868. Epub 2018 Mar 4. PMID: 29504127. |
Non-randomized study design. |
|
Schreiber LK, Metzger FG, Flammer E, Rinke H, Fallgatter AJ, Steinert T. Open Doors by Fair Means: a quasi-experimental controlled study on the effects of an open-door policy on acute psychiatric wards. BMC Health Serv Res. 2022 Jul 22;22(1):941. doi: 10.1186/s12913-022-08322-6. PMID: 35869551; PMCID: PMC9308253. |
Non-randomized study design. |
|
Celofiga A, Kores Plesnicar B, Koprivsek J, Moskon M, Benkovic D, Gregoric Kumperscak H. Effectiveness of De-Escalation in Reducing Aggression and Coercion in Acute Psychiatric Units. A Cluster Randomized Study. Front Psychiatry. 2022 Apr 7;13:856153. doi: 10.3389/fpsyt.2022.856153. PMID: 35463507; PMCID: PMC9021532. |
Included in Pedersen (2024). |
|
Schöttle D, Ruppelt F, Schimmelmann BG, Karow A, Bussopulos A, Gallinat J, Wiedemann K, Luedecke D, Rohenkohl AC, Huber CG, Bock T, Lambert M. Reduction of Involuntary Admissions in Patients With Severe Psychotic Disorders Treated in the ACCESS Integrated Care Model Including Therapeutic Assertive Community Treatment. Front Psychiatry. 2019 Oct 24;10:736. doi: 10.3389/fpsyt.2019.00736. PMID: 31708810; PMCID: PMC6822062. |
Non-randomized study design. |
|
Ye J, Xia Z, Wang C, Liao Y, Xu Y, Zhang Y, Yu L, Li S, Lin J, Xiao A. Effectiveness of CRSCE-Based De-escalation Training on Reducing Physical Restraint in Psychiatric Hospitals: A Cluster Randomized Controlled Trial. Front Psychiatry. 2021 Feb 16;12:576662. doi: 10.3389/fpsyt.2021.576662. PMID: 33679467; PMCID: PMC7928340. |
Presents no useful results for the literature summary of this module (trends only). |
|
Griffith JJ, Meyer D, Maguire T, Ogloff JRP, Daffern M. A Clinical Decision Support System to Prevent Aggression and Reduce Restrictive Practices in a Forensic Mental Health Service. Psychiatric Services. 2021;72(8):885-890. doi:10.1176/appi.ps.202000315 |
Focus on aggression, studied a decision support system, wrong outcomes. |
|
Lay B, Kawohl W, Rössler W. Outcomes of a psycho-education and monitoring programme to prevent compulsory admission to psychiatric inpatient care: a randomised controlled trial. Psychol Med. 2018 Apr;48(5):849-860. doi: 10.1017/S0033291717002239. Epub 2017 Aug 14. PMID: 28805175. |
Included in Molyneaux (2019). |
|
McDade Y. Effectiveness of the Mandt System aggression management training in an inpatient behavioral health program. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2018. |
Wrong publication type (dissertation, not published in a peer reviewed journal). |
|
Badouin J, Bechdolf A, Bermpohl F, Baumgardt J, Weinmann S. Preventing, reducing, and attenuating restraint: A prospective controlled trial of the implementation of peer support in acute psychiatry. Front Psychiatry. 2023 Feb 7;14:1089484. doi: 10.3389/fpsyt.2023.1089484. PMID: 36824670; PMCID: PMC9941159. |
Wrong design (pre-post study). |
|
Wullschleger A, Berg J, Bermpohl F, Montag C. Can "Model Projects of Need-Adapted Care" Reduce Involuntary Hospital Treatment and the Use of Coercive Measures? Front Psychiatry. 2018 May 1;9:168. doi: 10.3389/fpsyt.2018.00168. PMID: 29765339; PMCID: PMC5939233. |
Non-randomized study design. |
|
Duxbury J, Baker J, Downe S, Jones F, Greenwood P, Thygesen H, McKeown M, Price O, Scholes A, Thomson G, Whittington R. Minimising the use of physical restraint in acute mental health services: The outcome of a restraint reduction programme ('REsTRAIN YOURSELF'). Int J Nurs Stud. 2019 Jul;95:40-48. doi: 10.1016/j.ijnurstu.2019.03.016. Epub 2019 Mar 28. PMID: 31009823. |
Non-randomized study design. |
|
Schöttle D, Schimmelmann BG, Ruppelt F, Bussopulos A, Frieling M, Nika E, Nawara LA, Golks D, Kerstan A, Lange M, Schödlbauer M, Daubmann A, Wegscheider K, Rohenkohl A, Sarikaya G, Sengutta M, Luedecke D, Wittmann L, Ohm G, Meigel-Schleiff C, Gallinat J, Wiedemann K, Bock T, Karow A, Lambert M. Effectiveness of integrated care including therapeutic assertive community treatment in severe schizophrenia-spectrum and bipolar I disorders: Four-year follow-up of the ACCESS II study. PLoS One. 2018 Feb 27;13(2):e0192929. doi: 10.1371/journal.pone.0192929. PMID: 29485988; PMCID: PMC5828355. |
Non-randomized study design. |
|
Geoffrion S, Goncalves J, Giguère CÉ, Guay S. Impact of a Program for the Management of Aggressive Behaviors on Seclusion and Restraint Use in Two High-Risk Units of a Mental Health Institute. Psychiatr Q. 2018 Mar;89(1):95-102. doi: 10.1007/s11126-017-9519-6. PMID: 28500477. |
Non-randomized study design. |
|
Heres S, Holzhüter F, Hamann J. Shared Decision Making in an acute psychiatric setting. Nervenheilkunde, 2021;40(6), 436–446. https://doi.org/10.1055/a-1401-3586 |
No English full text available. |
Beoordelingsdatum en geldigheid
Publicatiedatum : 02-07-2026
Beoordeeld op geldigheid : 02-07-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de ‘Samenstelling van de werkgroep’) die betrokken zijn bij de preventie van, de besluitvorming over en de toepassing van verplichte zorg in de psychiatrie en de verslavingszorg in Nederland.
Werkgroep
- Dhr. E.J.D. (Elnathan) Prinsen (voorzitter), psychiater, namens de NVvP
- Mevr. C. (Carolien) Bakker, jurist, namens de Nederlandse ggz
- Dhr. C.J. (Chris) Bavinck, psychiater en geneesheer-directeur, namens de NVvP
- Dhr. P. (Paul) Doedens, verpleegkundige, onderzoeker en docent, namens V&VN
- Dhr. M.U. (Maarten) van Grevenstein, psychiater en geneesheer-directeur, namens de NVvP
- Dhr. A.G. (Rob) Havermans, psychiater en geneesheer-directeur, namens de NVvP
- Mevr. M. (Margot) Klooster, juridisch beleidsadviseur, namens de NVvP (per januari 2025)
- Mevr. K.M. (Kathelijne) Koorengevel, psychiater en geneesheer-directeur, namens de NVvP (per januari 2025)
- Dhr. A. (Arjen) Neven, psychiater, namens de NVvP
- Mevr. E. (Evi) Peters Rit, klinisch geriater, namens de NVKG (tot juni 2024)
- Mevr. M. (Maaike) Philippi, klinisch psycholoog, namens het NIP
- Dhr. P. (Peter) Pierik, patiëntvertegenwoordiging, namens MIND (tot juli 2024)
- Mevr. H. (Heleen) Schaffels, psychiater en geneesheer-directeur, namens de NVvP
- Dhr. E.P.K. (Erik) Sikkens, psychiater en geneesheer-directeur, namens de NVvP
- Mevr. M. (Mirjam) van Til, verpleegkundig specialist, namens V&VN
- Mevr. G.L. (Laura) Treurniet, patiëntvertegenwoordiger, namens MIND (per november 2024)
- Mevr. Y. (Yolande) Voskes, universitair docent medische ethiek, op persoonlijke titel
- Mevr. M.C.G. (Marja) van der Zanden, patiëntvertegenwoordiger, namens MIND
Klankbordgroep
- Dhr. J.W. (Jan Willem) de Boer, medisch manager ambulancezorg/ ziekenhuispsychiater, namens Ambulance zorg Nederland
- Dhr. D. (David) Baden, spoedeisendehulparts, namens de NVSHA
- Mevr. A. (Anneke) Huson, beleidsadviseur, namens Landelijke Stichting Familievertrouwenspersonen
- Mevr. M. (Marjo) Markx, naastenvertegenwoordiger, namens MIND
- Dhr. H. (Hans) Mollen, patiëntvertegenwoordiger, namens MIND
- Mevr. R.P. (Robinetta) de Roode, senior-jurist, namens Stichting PVP (patiëntenvertrouwenspersonen in de ggz)
- Dhr. H. (Hans) Slijpen, accountmanager gezondheidszorg, namens de Nederlandse Politie (tot oktober 2025)
- Mevr. M. (Marieke) Zeeman, internist, namens de NIV
Met ondersteuning van
- Mevr. C.T.J. (Charlotte) Michels, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. B. (Beatrix) Vogelaar, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. L.C. (Laura) van Wijngaarden, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel 1. Gemelde (neven)functies en belangen werkgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Datum |
Restrictie |
|
Prinsen, Elnathan |
Psychiater en lid raad van het bestuur, Parnassia groep |
*Lid kamer psychiatrie van de Stichting BOLS. *Voorzitter Opleidings- en Onderwijsregio Den Haag/Leiden. *Lid winning team Verkennend Gesprek/ Mentale gezondheidscentra dNggz. *Psychiater Leo Kannerhuis (onderdeel PG), Oosterbeek. * OVV Begeleidingscommissie (sept 2024). Onderzoek naar de veiligheid van mensen met ernstige psychiatrische aandoeningen, een vervolg op: Zorg voor veiligheid - Veiligheid van mensen met een ernstige psychische aandoening en hun omgeving - Onderzoeksraad voor Veiligheid. |
Hoofdstukken geschreven over psychiatrie en recht en specifiek de Wvggz in verschillende boeken, waar er bij één een kleine vergoeding is betaald.
|
Geen |
Geen |
*Veel gepubliceerd en gepresenteerd (en doe dat nog) over gedwongen zorg, dwangbehandeling en dan zowel de juridische- als de ethische aspecten. *Als voorzitter van de commissie wet- en regelgeving en later van de NVvP betrokken geweest bij de totstandkoming van de wet verplichte GGZ. Vanuit deze positie ook deelgenomen aan rondetafelbijeenkosmten in de 2e kamer en ook aan een expertmeeting in de 1e kamer. Ook heb ik in de media frequent kritiek geuit op de wet. *Momenteel bestuurder van een grote GGZ-instelling waar ook gedwongen zorg geleverd wordt. |
Geen |
08-04-2024 |
Geen restrictie |
|
Bakker, Carolien |
Juridisch adviseur, de Nederlandse ggz |
Lid redactie JGGZR (onbetaald). |
Geen |
Geen |
Geen |
Geen |
Geen |
12-03-2024 |
Geen restrictie |
|
Bavinck, Chris |
Psychiater en geneesheer-directeur, GGz Centraal, Amersfoort |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
21-02-2024 |
Geen restrictie |
|
Doedens, Paul |
* Verpleegkundige, postdoc onderzoeker & principal nurse educator, Amsterdam UMC (0.8 fte) * Docent-onderzoeker, Hogeschool van Amsterdam (0.2 fte) |
Sarcina Hortis: Eigenaar eenmanszaak (KvK: 61018953). Betaalde opdrachten op het gebied van onderwijs, advies en training in de gezondheidszorg sinds 2014 bij: - Arkin - Bohn Stafleu van Loghum - Cordaan - GGZ Oostbrabant - NCOI Groep - Noordhoff Health - Vereniging van Nederlandse Reflexzonetherapeuten - Hogeschool van Amsterdam - SDU Nurse Academy: Redactielid (betaald) V&VN: Commissielid, V&V Rookvrij (onbetaald) Stichting Vakantiespelen: * Bestuurslid (onbetaald) * Vereniging Beheer mandelig terrein Paktuinen gelegen achter nummer 27 t/m 35 (oneven nummers) * Voorzitter (onbetaald) Pointer: Spreker (eenmalig) in uitzending van Pointer over separaties in de GGZ. |
Geen |
Geen |
Ik neem geen deel aan extern gefinancierd onderzoek, alleen heb ik een beurs ontvangen van mijn werkgever om postdoctoraal onderzoek mee te doen. |
Geen |
Geen |
05-02-2024 |
Geen restrictie |
|
van Grevenstein, Maarten |
* Kinder- en jeugdpsychiater en geneesheer directeur, Karakter (betaald) * Lid van de NVVP, afdeling geneesheer directeuren, afdeling kinder- en jeugdpsychiatrie, platform digitalisering (onbetaald). * Lid van de commissie wet- en regelgeving (CWER) (onbetaald). |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
31-01-2024 |
Geen restrictie |
|
Havermans, Rob |
Geneesheer-directeur, Mondriaan |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
30-01-2024 |
Geen restrictie |
|
Klooster, Margot (per januari 2025) |
Juridisch beleidsadviseur NVvP |
Gastdocent Recht en Ethiek aan Radboud Centrum voor Sociale Wetenschappen (enkele keren per jaar). |
Geen |
Geen |
Geen |
Geen |
Geen |
04-02-2025 |
Geen restrictie |
|
Koorengevel, Kathelijne (per januari 2025) |
Psychiater en geneesheer-directeur, Erasmus MC, afdeling Psychiatrie |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
03-04-2025 |
Geen restrictie |
|
Neven, Arjen |
Psychiater, Fivoor FPA Utrecht |
*Prelum *NVvP Leidraad over verplichte zorg bij verslaving (lid commissie, onbetaald) |
Geen |
Geen |
Geen |
Ik geef verschillende presentaties over verplichte zorg bij verslaving, o.a. bij verslavingsartsen in opleiding, het leertraject verslavingspsychiatrie van het Radboud MC, rechters en Officieren van Justitie en de afd. geneesheren-directeur van de NVvP. |
Geen |
30-01-2024 |
Geen restrictie |
|
Peters Rit, Evi (tot juni 2024) |
Klinisch Geriater, Reinier de Graaf Gasthuis (betaald). Klinisch, poliklinisch en consulterend werk in het ziekenhuis. |
Lid werkgroep Wet Zorg en Dwang, NVKG (onbetaald) |
Geen |
Geen |
Geen |
Geen |
Geen |
31-01-2024 |
Geen restrictie |
|
Philippi, Maaike |
Directeur behandeling, CTP Veldzicht |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
06-03-2024 |
Geen restrictie |
|
Pierik, Peter (tot juli 2024) |
*Mediant 36u p/w Ervaringswerker *Saxion 8u p/w Docent Ad Ervaringsdeskundigheid *Patiëntvertegenwoordiger MIND |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
10-03-2024
|
Geen restrictie |
|
Schaffels, Heleen |
Psychiater en geneesheer-directeur, GGZinGeest, Amsterdam |
Lid van klachtencommissie Zuid Holland noord |
Geen |
Geen |
Geen |
Geen |
Geen |
14-02-2024 |
Geen restrictie |
|
Sikkens, Erik |
Psychiater, Arkin GGZ (24 uur) en FPC Oostvaarderskliniek (16 uur) |
Eigen praktijk via 1nP (2-4 uur) *Docent SSR *Docent OSR *Docent St. PVP |
Geen |
Geen |
Geen |
Geen |
Geen |
11-03-2024 |
Geen restrictie |
|
van Til, Mirjam |
Verpleegkundig Specialist, Geestelijke Gezondheidszorg Stichting Arkin |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
12-02-2024 |
Geen restrictie |
|
Treurniet, Laura (per november 2024) |
Patiëntvertegen woordiger MIND |
Onderzoeksstagair WKZ Utrecht |
Geen |
Geen |
Geen |
Geen |
Geen |
25-10-2024 |
Geen restrictie |
|
Voskes, Yolande |
*Universitairs docent te Amsterdam UMC; *Senior onderzoeker GGZ Breburg |
Voorzitter Stichting HIC&ART |
Geen |
Geen |
Geen |
Geen |
Geen |
02-04-2024
|
Geen restrictie |
|
van der Zanden, Marja |
Patiëntvertegen woordiger MIND |
Lid redactieraad Journaal GGZ en Recht Plus |
Geen |
Geen |
Geen |
Geen |
Geen |
05-03-2024 |
Geen restrictie |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiënten- en naastenperspectief door afgevaardigden van de patiëntvereniging MIND te betrekken in de werkgroep en klankbordgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en het opstellen van de overwegingen (zie kop ‘Waarden en voorkeuren van patiënten’). De conceptrichtlijn is tevens voor commentaar voorgelegd aan MIND, Stichting Patiëntenvertrouwenspersonen (PVP) en Landelijke Stichting Familievertrouwenspersonen en de eventueel aangeleverde commentaren zijn bekeken en verwerkt door de werkgroep.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Module |
Uitkomst raming |
Toelichting |
|
Module Preventie verplichte zorg in de ggz |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Literature search strategy
Embase.com
|
No. |
Query |
Results |
|
#1 |
'mental disease'/exp OR 'mental health'/exp OR 'mental health care'/exp OR 'mental patient'/exp OR 'psychiatry'/exp OR 'psychology'/exp OR 'psychiatrist'/exp OR 'psychologist'/exp OR ((mental* NEAR/3 (disease* OR disorder* OR ill* OR problem* OR health* OR patient*)):ti,ab,kw) OR psychot*:ti,ab,kw OR psychos*:ti,ab,kw OR psychiatr*:ti,ab,kw |
3814969 |
|
#2 |
'involuntary commitment'/exp OR 'mandatory program'/de OR 'coercion'/exp OR 'physical restraint'/exp OR coersion:ti,ab,kw OR restraint*:ti,ab,kw OR (((involunta* OR 'in volunta*' OR mandator* OR coerc* OR compuls* OR forced OR enforced OR restrictive OR 'against the will') NEAR/3 (commit* OR inpatient* OR stay* OR admiss* OR readmiss* OR admit* OR treatment* OR interven* OR measure* OR medication* OR drug* OR injection* OR care OR healthcare OR hospitaliz* OR hospitalis* OR detain* OR seclusion OR segregation OR isolation OR 'solitary confinement' OR psychiatr* OR mental OR program* OR practice*)):ti,ab,kw) OR 'community treatment order*':ti,ab,kw OR cto:ti,ab,kw OR ctos:ti,ab,kw |
81334 |
|
#3 |
'prevention'/de OR 'primary prevention'/exp OR 'secondary prevention'/exp OR 'tertiary prevention'/exp OR (((prevent* OR reduc* OR decreas* OR eliminat* OR avoid* OR limit*) NEAR/4 (involunta* OR 'in volunta*' OR mandator* OR coerc* OR compuls* OR cto OR ctos OR restraint* OR seclusion* OR segregation OR isolation OR 'solitary confinement' OR forced OR enforced OR restrictive OR 'against the will')):ti,ab,kw) OR 'de escalat*':ti,ab,kw OR 'deescalat*':ti,ab,kw OR ((prevent*:ti OR reduc*:ti OR decreas*:ti OR eliminat*:ti OR avoid*:ti OR limit*:ti) AND (involunta*:ti OR 'in volunta*':ti OR mandator*:ti OR coerc*:ti OR compuls*:ti OR cto:ti OR ctos:ti OR restraint*:ti OR seclusion*:ti OR segregation:ti OR isolation:ti OR 'solitary confinement':ti OR forced:ti OR enforced:ti OR restrictive:ti OR 'against the will':ti OR crisis:ti OR crises:ti) NOT 'obsessive compulsive':ti) OR (((advance* OR 'self binding') NEAR/3 (directive* OR statement* OR 'care plan*')):ti,ab,kw) OR (((crisis OR crises) NEAR/3 (plan OR resolut* OR monitor*)):ti,ab,kw) OR 'wellness recovery action plan*':ti,ab,kw OR 'open door':ti,ab,kw OR 'open dialogue*':ti,ab,kw OR psychoeducat*:ti,ab,kw OR 'compliance enhanc*':ti,ab,kw OR 'treatment adherence therap*':ti,ab,kw OR (((aggression OR arousal) NEAR/3 management):ti,ab,kw) OR (((sensory OR comfort) NEAR/3 room*):ti,ab,kw) OR 'shared decision':ti,ab,kw OR 'six core strateg*':ti,ab,kw OR '6 core strateg*':ti,ab,kw OR safeward*:ti,ab,kw OR (('trauma informed' NEAR/3 (care OR approach*)):ti,ab,kw) OR 'no force first':ti,ab,kw OR (((weddinger OR trieste OR tidal OR engagement OR 'high and intensive care' OR hic) NEAR/3 model*):ti,ab,kw) OR (((peer OR circle) NEAR/3 support):ti,ab,kw) OR 'circle of care':ti,ab,kw |
507419 |
|
#4 |
#1 AND #2 AND #3 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) AND [2005-2024]/py |
2062 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1059608 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4102390 |
|
#7 |
#4 AND #5 - SR |
202 |
|
#8 |
#4 AND #6 NOT #7 - RCT |
326 |
|
#9 |
#7 OR #8 |
528 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Mental Disorders/ or exp Mental Health/ or exp Mental Health Services/ or exp Mentally Ill Persons/ or exp Psychiatry/ or exp Psychology/ or exp Psychiatrists/ or (mental* adj3 (disease* or disorder* or ill* or problem* or health* or patient*)).ti,ab,kf. or psychot*.ti,ab,kf. or psychos*.ti,ab,kf. or psychiatr*.ti,ab,kf. |
2102609 |
|
2 |
exp Involuntary Commitment/ or exp Mandatory Programs/ or exp Coercion/ or exp Restraint, Physical/ or coersion.ti,ab,kf. or restraint*.ti,ab,kf. or ((involunta* or 'in volunta*' or mandator* or coerc* or compuls* or forced or enforced or restrictive or 'against the will') adj3 (commit* or inpatient* or stay* or admiss* or readmiss* or admit* or treatment* or interven* or measure* or medication* or drug* or injection* or care or healthcare or hospitaliz* or hospitalis* or detain* or seclusion or segregation or isolation or 'solitary confinement' or psychiatr* or mental or program* or practice*)).ti,ab,kf. or 'community treatment order*'.ti,ab,kf. or cto.ti,ab,kf. or ctos.ti,ab,kf. |
79738 |
|
3 |
Primary Prevention/ or Secondary Prevention/ or Tertiary Prevention/ or ((prevent* or reduc* or decreas* or eliminat* or avoid* or limit*) adj4 (involunta* or 'in volunta*' or mandator* or coerc* or compuls* or cto or ctos or restraint* or seclusion* or segregation or isolation or 'solitary confinement' or forced or enforced or restrictive or 'against the will')).ti,ab,kf. or 'de escalat*'.ti,ab,kf. or 'deescalat*'.ti,ab,kf. or (((prevent* or reduc* or decreas* or eliminat* or avoid* or limit*) and (involunta* or 'in volunta*' or mandator* or coerc* or compuls* or cto or ctos or restraint* or seclusion* or segregation or isolation or 'solitary confinement' or forced or enforced or restrictive or 'against the will' or crisis or crises)) not 'obsessive compulsive').ti. or ((advance* or 'self binding') adj3 (directive* or statement* or 'care plan*')).ti,ab,kf. or ((crisis or crises) adj3 (plan or resolut* or monitor*)).ti,ab,kf. or 'wellness recovery action plan*'.ti,ab,kf. or 'open door'.ti,ab,kf. or 'open dialogue*'.ti,ab,kf. or psychoeducat*.ti,ab,kf. or 'compliance enhanc*'.ti,ab,kf. or 'treatment adherence therap*'.ti,ab,kf. or ((aggression or arousal) adj3 management).ti,ab,kf. or ((sensory or comfort) adj3 room*).ti,ab,kf. or 'shared decision'.ti,ab,kf. or 'six core strateg*'.ti,ab,kf. or '6 core strateg*'.ti,ab,kf. or safeward*.ti,ab,kf. or ('trauma informed' adj3 (care or approach*)).ti,ab,kf. or 'no force first'.ti,ab,kf. or ((((weddinger or trieste or tidal or engagement or 'high) and intensive care') or hic) adj3 model*).ti,ab,kf. or ((peer or circle) adj3 support).ti,ab,kf. or 'circle of care'.ti,ab,kf. |
126936 |
|
4 |
(1 and 2 and 3) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
2252 |
|
5 |
limit 4 to yr="2005 -Current" |
1881 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
773076 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2775106 |
|
8 |
5 and 6 - SR |
188 |
|
9 |
(5 and 7) not 8 - RCT |
263 |
|
10 |
8 or 9 |
451 |
Ovid/PsycINFO
|
# |
Searches |
Results |
|
1 |
exp Mental Disorders/ or exp Mental Health/ or exp Mental Health Services/ or exp Psychiatry/ or exp Psychology/ or exp Psychiatrists/ or exp Psychologists/ or (mental* adj3 (disease* or disorder* or ill* or problem* or health* or patient*)).ti,ab,id. or psychot*.ti,ab,id. or psychos*.ti,ab,id. or psychiatr*.ti,ab,id. |
1820335 |
|
2 |
exp Involuntary Treatment/ or exp Coercion/ or exp Physical Restraint/ or exp Patient Seclusion/ or coersion.ti,ab,id. or restraint*.ti,ab,id. or ((involunta* or 'in volunta*' or mandator* or coerc* or compuls* or forced or enforced or restrictive or 'against the will') adj3 (commit* or inpatient* or stay* or admiss* or readmiss* or admit* or treatment* or interven* or measure* or medication* or drug* or injection* or care or healthcare or hospitaliz* or hospitalis* or detain* or seclusion or segregation or isolation or 'solitary confinement' or psychiatr* or mental or program* or practice*)).ti,ab,id. or 'community treatment order*'.ti,ab,id. or cto.ti,ab,id. or ctos.ti,ab,id. |
31340 |
|
3 |
Prevention/ or ((prevent* or reduc* or decreas* or eliminat* or avoid* or limit*) adj4 (involunta* or 'in volunta*' or mandator* or coerc* or compuls* or cto or ctos or restraint* or seclusion* or segregation or isolation or 'solitary confinement' or forced or enforced or restrictive or 'against the will')).ti,ab,id. or 'de escalat*'.ti,ab,id. or 'deescalat*'.ti,ab,id. or (((prevent* or reduc* or decreas* or eliminat* or avoid* or limit*) and (involunta* or 'in volunta*' or mandator* or coerc* or compuls* or cto or ctos or restraint* or seclusion* or segregation or isolation or 'solitary confinement' or forced or enforced or restrictive or 'against the will' or crisis or crises)) not 'obsessive compulsive').ti. or ((advance* or 'self binding') adj3 (directive* or statement* or 'care plan*')).ti,ab,id. or ((crisis or crises) adj3 (plan or resolut* or monitor*)).ti,ab,id. or 'wellness recovery action plan*'.ti,ab,id. or 'open door'.ti,ab,id. or 'open dialogue*'.ti,ab,id. or psychoeducat*.ti,ab,id. or 'compliance enhanc*'.ti,ab,id. or 'treatment adherence therap*'.ti,ab,id. or ((aggression or arousal) adj3 management).ti,ab,id. or ((sensory or comfort) adj3 room*).ti,ab,id. or 'shared decision'.ti,ab,id. or 'six core strateg*'.ti,ab,id. or '6 core strateg*'.ti,ab,id. or safeward*.ti,ab,id. or ('trauma informed' adj3 (care or approach*)).ti,ab,id. or 'no force first'.ti,ab,id. or ((((weddinger or trieste or tidal or engagement or 'high) and intensive care') or hic) adj3 model*).ti,ab,id. or ((peer or circle) adj3 support).ti,ab,id. or 'circle of care'.ti,ab,id. |
81985 |
|
4 |
1 and 2 and 3 |
2564 |
|
5 |
limit 4 to yr="2005 -Current" |
2071 |
|
6 |
((literature review or systematic review or meta analysis).md. or "literature review"/ or meta analysis/ or (((meta adj2 analy*) or metaanaly* or (synthes* adj2 (literature* or research* or studies or data)) or (pooled and analys*) or ((data adj1 pool*) and studies) or medline or medlars or embase or cinahl or scisearch or psychlit or psyclit or cinhal or cancerlit or cochrane or bids or pubmed or ovid or ((hand or manual or database* or computer*) adj1 search*) or (electronic adj1 (database* or data base or data bases))).ti,ab,id. or (review* or overview).ti. or (bibliograph* or relevant journals or ((review* or overview*) adj9 (systematic* or methodologic* or quantitativ* or research* or literature* or studies or trial* or effective*))).ab.)) not (((retrospective* or record* or case* or patient*) adj1 review*) or ((patient* or review*) adj1 chart*)).ti,ab,id. |
501519 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
306998 |
|
8 |
5 and 6 - SR |
287 |
|
9 |
(5 and 7) not 8 - RCT |
214 |
|
10 |
8 or 9 |
501 |