Sliktrainingsprogramma's bij dysfagie
Uitgangsvraag
Wat is de effectiviteit van intensieve sliktrainingsprogramma’s en welke patiënten komen hiervoor in aanmerking?
Aanbeveling
Aanbeveling-1
Bied bij orofaryngeale dysfagie standaard logopedische behandeling aan bestaande uit compensatiestrategieën (aanpassing van houding, aanpassen van voedselconsistentie). Bepaal de compensatiestrategieën altijd in overleg met de patiënt en houdt rekening met diens fysieke en cognitieve mogelijkheden.
Aanbeveling-2
Bied bij naar verwachting herstellende orofaryngeale dysfagie, naast compensatiestrategieën, ook een actief functiegericht sliktrainingsprogramma aan. Houdt hierbij rekening met fysieke en cognitieve mogelijkheden van patiënt.
Aanbeveling-3
Bespreek bij naar verwachting niet herstellende of progressieve orofaryngeale dysfagie, naast compensatiestrategieën, de mogelijkheid voor een actief, functiegericht sliktrainingsprogramma, mits dit haalbaar is en in overeenstemming met de wensen van de patiënt en diens fysieke en cognitieve mogelijkheden. Betrek hierin laagdrempelig mantelzorger(s)- en check met regelmaat wens en haalbaarheid van sliktrainingsprogramma bij betrokkenen.
Bespreek bij naar verwachting langzaam herstellende orofaryngeale dysfagie, naast compensatiestrategieën, de mogelijkheid voor een actief, functiegericht sliktrainingsprogramma, mits dit haalbaar is en aansluit bij de voorkeuren van de patiënt en diens fysieke en cognitieve mogelijkheden.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Er is literatuuronderzoek verricht naar het effect van (additionele) sliktrainingsprogramma’s in patiënten met orofaryngeale dysfagie (OD). Voor de patiëntengroepen na doorgemaakt CVA, hoofd-halskanker, ziekte van Parkinson, Muliple Sclerosis, post-intubatie en in een heterogene groep inclusief ouderen met OD is literatuur gevonden. In de analyse werden een systematische literatuuranalyse en vijfafzonderlijke studies geïncludeerd.
Onder additionele sliktrainingsprogramma’s wordt het toevoegen van een extra sliktrainingsprogramma aan de interventiegroep bedoeld.
Standaardzorg wordt verschillend in de artikelen gedefinieerd, maar omvatten voornamelijk compensatie strategieën, dieetadvies, supervisie en educatie.
Klinisch relevante verschillen voor de cruciale uitkomstmaat functionele orale voedselinname werden gezien bij CVA patiënten in het voordeel van additionele sliktrainingsprogramma’s. Deze verschillen werden ook gezien bij hoofdhals kankerpatiënten, MS-patiënten en post-intubatie patiënten wanneer sliktrainingsprogramma’s werd vergeleken met standaardzorg.
De kwaliteit van het bewijs van de geïncludeerde artikelen voor de cruciale uitkomstmaat functionele orale voedselinname was (zeer) laag met name op de brede betrouwbaarheidsintervallen en kleine studiepopulatie.
Voor de cruciale uitkomstmaat slik gerelateerde kwaliteit van leven werd een klinisch relevant verschil gevonden in het voordeel van sliktrainingsprogramma’s ten opzichte van standaardzorg in hoofdhalskanker patiënten. De kwaliteit van bewijs was laag door de kleine studiepopulatie en methodologische opzet van de studie.
Voor de belangrijke uitkomstmaat functioneel slikvermogen werd een klinisch relevant verschil gevonden in het voordeel van additionele sliktrainingsprogramma’s ten opzichte van standaard sliktrainingsprogramma’s in patiënten die een CVA hadden gehad. De kwaliteit van bewijs was laag door de kleine studiepopulatie en methodologische opzet van de studie.
Klinisch relevante verschillen voor de belangrijke uitkomstmaat aspiratie werden gezien in CVA patiënten in het voordeel van additionele sliktrainingsprogramma’s. Deze verschillen werden ook gezien bij patiënten met de ziekte van Parkinson wanneer sliktrainingsprogramma’s werden vergeleken met standaardzorg.
De kwaliteit van het bewijs van de geïncludeerde artikelen was (zeer) laag met name op de brede betrouwbaarheidsintervallen en methodologische opzet van de studie.
Voor de belangrijke uitkomstmaat aantal of percentage van de patiënten dat terugkeert naar een normaal dieet zijn geen artikelen gevonden die deze uitkomstmaat hadden gerapporteerd.
Uit de search zijn ook artikelen naar voren gekomen die niet voldoen aan de opstelde PICO, maar die de werkgroep wel relevant vonden om te beschrijven.
Banda (2020) voerde een systematische review en meta-analyse uit om de effectiviteit van sliktherapie-oefeningen te beoordelen bij patiënten met hoofdhalskanker. De review omvatte 19 gerandomiseerde gecontroleerde onderzoeken met in totaal ongeveer 1.100 volwassenen die verschillende behandelingen voor hoofdhalskanker ondergingen. De interventies richtten zich op orofaryngeale oefeningen—zoals tongversterking, slikmanoeuvres en kaakmobiliteit—die werden toegepast tijdens of na de kankerbehandeling.
De bevindingen toonden kleine maar statistisch significante verbeteringen in de slikfunctie direct na de interventie (gestandaardiseerd gemiddeld verschil [SMD] ≈ 0,33) en na zes maanden (SMD ≈ 0,46). Er werden ook matige verbeteringen in mondopening (trismus) waargenomen (SMD ≈ 0,60). De interventies hadden echter geen significant effect op het risico op aspiratie, de algemene prestaties of de kwaliteit van leven. De auteurs concludeerden dat sliktherapie-oefeningen bescheiden functionele voordelen bieden en opgenomen moeten worden in de standaardzorg voor hoofdhalskanker patiënten, bij voorkeur ondersteund door gestructureerde gedragsstrategieën om de therapietrouw te bevorderen.
Kwaliteit van bewijs
De overall kwaliteit van bewijs is (zeer) laag. Dit betekent dat we (zeer) onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege (zeer)ernstige:
- Risk of Bias: methodologische beperkingen binnen het randomizatieproces.
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grens van klinische relevantie overschrijdt en vanwege het niet bereiken van de optimale steekproefgrootte.
Hoewel het gevonden bewijs als methodologisch (zeer) laag wordt afgegeven, zijn er ook enkele positieve punten te benoemen. Het aantal RCT’s waarbij verschillende sliktrainingsmethodes met standaard zorg of compensatie strategieën worden vergeleken is toegenomen en er is een netwerk meta-analyse verricht, die zowel voor verbeteren van slikfunctie als voor het verminderen van verslikken een positief effect laat zien in het voordeel van sliktrainingsprogramma’s. Dit geldt met name voor CVA en hoofdhalskanker patiënten. Voor patiënten met orofaryngeale dysfagie bij (spier)zwakte blijft het aantal studies zeer beperkt.
Hoewel het bewijs, gezien onvolkomenheden in de studies, laag blijft, is zowel het aantal studies toegenomen en is in het algeheel de methodologische kwaliteit de afgelopen jaren verbeterd, wat zeker een factor is om mee te wegen bij het bespreken en afwegen om wel/geen sliktraining te geven aan een patiënt met orofaryngeale dysfagie.
Een belangrijk aandachtspunt is dat de langetermijneffecten van sliktrainingsprogramma’s nog onbekend zijn, omdat de follow-up in de huidige studies beperkt bleef tot drie maanden. Daarnaast is er in de uitgevoerde literatuur search niet gekeken naar uitvoerbaarheid van de trainingsprogramma’s, belastbaarheid van patiënten, en mogelijk (ongewenste) uitval bij patiënten. Er zijn wel aanwijzingen (Lee, 2024) dat bij toenemend aantal sessie van een sliktrainingsprogramma, het positieve effect op de slikfunctie toeneemt. Tenslotte is er voor de Nederlandse setting geen beraming van kosten versus effectiviteit gedaan.
Het mogelijke positieve effect van sliktrainingsprogramma’s — zoals het verbeteren van de slikfunctie en het verminderen van verslikken — vormt een belangrijk voordeel voor de patiënt. Deze baten moeten echter worden afgewogen tegen de bijbehorende kosten, zoals de inspanning en tijdsinvestering voor zowel patiënt als logopedist, het ontbreken van langetermijnresultaten en de mogelijke toename in zorgkosten.
Binnen een samen-beslis-model zou bij orofaryngeale dysfagie compensatie strategieën aangeboden moeten worden, gericht op de aanpassing van houding, en indien nodig, het aanpassen van voedselconsistenties.
Bij patiënten met naar verwachting herstellende dysfagie, zoals na CVA en bij hoofdhalskanker, en met de aanname dat de patiënt voldoende belastbaar is, is het de aanbeveling om daarnaast ook een actief, functiegericht sliktrainingsprogramma aan te bieden.
Bij patiënten met een verminderde cognitieve en/of fysieke belastbaarheid en leerbaarheid moet het specifieke doel en intensiteit van de training worden aangepast door de logopedist.
Bij patiënten met naar verwachting progressieve, niet herstellende, of langzaam herstellende orofaryngeale dysfagie, zoals bij neurodegeneratieve aandoeningen (zoals bij patiënten met de ziekte van Parkinson, dementie, Multiple sSlerose) of ten gevolge van (spier)zwakte en/of frailty (zwakte, kwetsbaarheid, post-intubatie/post-IC opname) kan, naast het standaard aanbieden van compensatie strategieën, ook het aanbieden van een actief, functiegericht sliktrainingsprogramma overwogen worden. Ook in deze situaties dienen de wensen, belastbaarheid en zowel de fysieke als cognitieve mogelijkheden van de patiënt te worden meegewogen. Voor patiënten met de ziekte van Parkinson kan ook de NVLF richtlijn “Logopedie bij de ziekte van Parkinson” geraadpleegd worden.
In het algemeen is het raadzaam om laagdrempelig een diëtist bij de zorg te betrekken (zie ook de module Diëtetische behandeling bij dysfagie en de paramedische richtlijn Parkinson).
De invulling van een sliktrainingsprogramma (welke oefeningen en in welke intensiteit) wordt bepaald door de logopedist op basis van zowel de presentatie van orofaryngeale dysfagie als patiënten kenmerken. Er zijn meerdere oefeningen zoals kaak- en tongoefeningen, chin tuck against resistance (CTAR), Shaker oefeningen, “effortful swallowing” sliktraining (EST), en ademhalingsspiertraining (IMST en EMST).
Gewenste effecten zijn verbetering van kwaliteit van leven; op functie niveau (afname aspiratie, verbetering passage, afname residu), op activiteiten niveau (mogelijkheid tot (volledige) voedsel inname, zonder gewichtsverlies), en op participatie niveau (deelname aan eetmomenten, sociale context). Daarnaast zou er een gewenst effect op zorgkosten kunnen zijn, zoals minder gebruik bijvoeding en/of sondevoeding, minder ondersteuning door thuiszorg, afname van ligdagen/ziekhuisopnames bij aspiratiepneumonie. Deze kosteneffecten zijn niet meegenomen in deze literatuur search, maar zouden aannemelijk kunnen zijn (Dyreborg, 2023; Jansen, 2021; Baijens, 2016).
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
In de literatuur search en uitwerking is rekening gehouden met gelijk(waardig)heid van specifieke doelgroepen, door verschillende subgroepen te includeren. Of de gewenste effecten gelden voor een individuele patiënt is moeilijk in te schatten, mede door lage GRADE van bewijs, met grote spreiding in uitkomsten en kleine aantallen per studie.
Mogelijke ongewenste effecten van sliktrainingsprogramma’s zijn overbelasting fysiek en mentaal van patiënt, (voortijdig) stoppen van het sliktrainingsprogramma, afwezigheid van blijvend effect, onnodige zorgkosten zonder behalen van klinisch relevante verbetering bij patiënt, onnodige kosten mantelzorger (afwezigheid van werk, transport).
Het oordeel ten aanzien van bovengenoemde ongewenste effecten; deze zijn allen onbekend en moeten dus meegewogen worden bij de keuze wel/geen sliktrainingsprogramma te starten.
Kostenaspecten
Het kosteneffectiviteit aspect voor de Nederlandse situatie is niet bekend. Een recent uitgevoerde Deense CEA analyse uit 2023 waarbij verschillende vormen van dysfagie geïncludeerd waren en waarbij standaard zorg -bestaande uit twee bezoeken van een ergotherapeut en een diëtist om voorlichting te geven over dysfagie, een optimale zitpositie, viscositeiten en calorie- en eiwitinname- vergeleken werd met standaard zorg aangevuld met CTAR, (chin tuck against resistance)- een veel toegepaste vorm sliktraining. De CEA viel uit ten gunste van de behandeling met toegevoegde sliktraining met minder kosten en grotere effectiviteit. Een vergelijkbare studie zou voor de Nederlandse populatie, met inzet van de (paramedische) zorg in Nederlandse situatie en bijbehorende kosten, verricht kunnen worden om zicht te krijgen hierop.
Gelijkheid ((health) equity/equitable)
Op dit moment is het niet bekend of de interventie, zijnde sliktrainingsprogramma’s toevoegen aan standaard (logopedische) zorg kan leiden tot een mogelijke toename van gezondheidsongelijkheid. Dit zal in de toekomst vervolgd moeten worden.
Aanvaardbaarheid
Ethische aanvaardbaarheid
Er zijn geen ethische bezwaren. De kans dat een patiënt fysieke, emotionele, of sociale schade wordt toegebracht bij het uitvoeren van sliktrainingstherapieën is uiterst gering, ervan uitgaande dat belastbaarheid van patiënt gemonitord wordt en zo nodig doel en uitvoer van therapie hierop aangepast worden.
Duurzaamheid
Overwogen kan worden om fysieke controles (groten)deels te vervangen door online consulten en geïndividualiseerde trainingsschema’s voor de patiënt online of per app aan te bieden. Hiermee kunnen aantal reisbewegingen, als ook noodzaak tot inzet van mantelzorgers verminderd worden. Dit beperkt op meerdere fronten de CO2 uitstoot. Voorwaarde is wel dat patiënt vaardig is om online consulten en digitaal aangeboden sliktrainingen te volgen.
Haalbaarheid
De interventie lijkt haalbaar. Sliktrainingsprogramma’s zijn reeds bestaande behandelingen in de logopedische praktijk. Mogelijk zal het aantal slikgespecialiseerde logopedisten in de toekomst niet toereikend zijn, maar een mogelijke oplossing hiervoor ziet de werkgroep in de reeds hierboven benoemde mogelijkheid tot het toepassen van online sliktrainingen.
Rationale van aanbeveling-1: weging van argumenten voor en tegen de interventies
Compensatiestrategieën (aanpassing van houding, aanpassen van voedselconsistentie) zijn van toegevoegde waarde bij (langzaam) herstellende, niet herstellende, als ook progressieve dysfagie. Deze toepassing van logopedie bestaande uit slik- en voedingsadviezen als ook aanpassingen van voedsel inname kunnen bij alle vormen van dysfagie toegepast worden.
De logopedist kan dysfagie op twee manieren behandelen: door compensatiestrategieën toe te passen of door stoornisgerichte therapie te geven door middel van sliktrainingsprogramma's of slikrevalidatie.
Een compensatiestrategie houdt in dat een specifieke aanpassing consequent wordt toegepast (zoals een andere hoofdhouding, een veranderde voedselconsistentie en/of een andere slikmethode) (Glynn, 1999; Shaker, 2013). Compensatiestrategieën zijn met name effectief bij niet-herstellende of langzaam herstellende dysfagie, evenals bij progressieve dysfagie (zoals bij neurodegeneratieve aandoeningen en neuromusculaire aandoeningen). Intensieve sliktrainingsprogramma's, met of zonder instrumentele ondersteuning zoals biofeedback (zie de module 'Biofeedback bij dysfagie') of neuromusculaire elektrostimulatie (zie de module Elektrostimulatie bij dysfagie), zijn daarentegen geschikter voor dysfagie waarbij functioneel herstel wordt verwacht, bijvoorbeeld na een CVA, operatie of radiotherapie.
Eindoordeel:
Sterke aanbeveling voor (Doen).
Rationale van aanbeveling-2: weging van argumenten voor en tegen de interventies
Op basis van huidig bewijs, dient het te aanbeveling om bij patiënten met naar verwachting herstellende dysfagie, zoals na CVA en bij hoofdhalskanker, een actief, functiegericht sliktrainingsprogramma aan te bieden. Op geleiden van de belastbaarheid van de patiënt wordt het doel en de intensiteit van de training aangepast door de logopedist.
Eindoordeel:
Sterke aanbeveling voor (Doen).
Rationale van aanbeveling-3: weging van argumenten voor en tegen de interventies
Bij patiënten met orofaryngeale dysfagie, ongeacht de prognose van de onderliggende aandoeningen en/of slikklachten, kan het aanbieden van een actief, functiegericht sliktrainingsprogramma worden overwogen. Ook hier dienen de wensen, belastbaarheid en zowel de fysieke als cognitieve mogelijkheden van de patiënt te worden meegewogen.
Eindoordeel:
Zwakke aanbeveling voor (Doen).
Onderbouwing
The speech-language therapist can treat dysphagia in two ways: by compensating for the disorder (applying compensation strategies) or by attempting to resolve the disorder through swallowing training programs or swallowing rehabilitation.
A compensation strategy involves consistently applying a specific adjustment (such as a different head posture, altered food consistency, and/or a different method of swallowing) (Glynn, 1999; Shaker, 2013). Compensation strategies are particularly effective for non-recovering or slowly recovering, as well as progressive dysphagia (such as in neurodegenerative conditions and neuromuscular diseases). Intensive swallowing training programs, with or without instrumental support such as biofeedback (see the module 'Biofeedback in Dysphagia') or electrical stimulation (see the module 'Electrical Stimulation in Dysphagia'), are instead more appropriate for dysphagia where functional recovery is expected, for example after a stroke, surgery, radiotherapy, etc.
However, the results of such training are generally only seen after a period of practice, in contrast to compensation strategies, whose effects are usually immediately observable. Therefore, the focus of the guiding question is on swallowing rehabilitation techniques and not on compensation strategies.
Swallowing training programs aim, among other things, to improve quality of life. This means:
- At the functional level: less frequent or absent aspiration, nasal regurgitation, or bothersome residue (food that remains stuck in the oral or pharyngeal cavity).
- At the activity level: being able to eat and drink regular foods and liquids (while maintaining weight).
- At the participation level: being able to participate as normally as possible in daily meals, dining, coffee breaks, and so on in any social context (family, work, etc.).
Summary of Findings
Stroke
PICO (1.1)
Population: Stroke patients
Intervention: Additional swallowing training
Comparator: standard swallowing training or other additional training
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
Standard/other additional swallowing training |
Additional swallowing training |
||||
|
Number/percentage of patients who return to a normal diet
|
-
|
-
|
No GRADE (no evidence was found)
|
No evidence was found regarding the effect of additional swallowing training compared to standard swallowing training in stroke patients. |
|
|
Functional oral intake of food experienced by the patient |
Measured by: FOIS Scale: 1-7, higher is better Based on data from 212 participants in 6 studies
|
|
|
Very low Due to serious risk of bias, due to serious inconsistency, due to serious imprecision1 |
The evidence is very uncertain about the effect of additional swallowing training on the FOIS when compared with standard swallowing training in stroke patients.
(Park, 2016; Park, 2020; Choi, 2017; Kim and Park, 2019a; Liaw, 2020; Liu, 2025)
|
|
Difference: MD 1.27 higher (CI 95% 0.83 higher - 1.70 higher) |
|||||
|
Measured by: FOIS Scale: 1-7, higher is better Based on data from 38 participants in 1 studies |
|
|
Very low Due to serious risk of bias, due to serious imprecision2 |
The evidence is very uncertain about the effect of additional CTAR on functional oral intake compared to additional shaker in stroke patients.
(Park, 2019b) |
|
|
Difference: MD 0.40 higher (CI 95% 0.20 lower - 1.0 higher) |
|||||
|
Measured by: MASA Scale: 0-200, higher is better Based on data from 16 participants in 1 studies
|
|
|
Low due to serious imprecision3 |
Additional swallowing training may result in little to no difference in MASA scores when compared with standard swallowing training in stroke patients.
(Moon, 2018) |
|
|
Difference: MD 4.5 higher (CI 95% 2.23 lower - 11.23 higher) |
|||||
|
Measured by: ASHA-NOMS Scale: 0-7, higher is better Based on data from 36 participants in 1 studies
|
|
|
Very low Due to serious risk of bias, due to serious imprecision4 |
The evidence is very uncertain about the effect of additional swallowing training on the ASHA-NOMS when compared with standard swallowing training in stroke patients.
(Jang, 2019) |
|
|
Difference: MD 0.40 higher (CI 95% 0.34 lower - 1.14 higher) |
|||||
|
Swallowing-related quality of life
|
Measured by: SWAL-QOL Scale: 0-100, higher is better Based on data from 16 participants in 1 studies
|
|
|
Low due to serious imprecision5 |
Additional swallowing training may result in little to no difference in swallowing-related quality of life when compared with standard swallowing training in stroke patients.
(Moon, 2018) |
|
Difference: MD 6.5 higher (CI 95% 3.93 lower - 16.93 higher) |
|||||
|
Functional swallowing ability
|
Measured by: FDS Scale: 0-100, lower is better Based on data from 94 participants in 2 studies
|
|
|
Low Due to serious risk of bias, due to serious imprecision6 |
Additional swallowing training may improve the functional swallowing ability when compared with standard swallowing training in stroke patients.
(Jang, 2019; Liu, 2025) |
|
Difference: MD 11.12 lower (CI 95% 11.76 lower - 10.47 lower) |
|||||
|
Aspiration
|
Measured by: PAS Scale: 1-8, lower is better Based on data from 351 participants in 11 studies
|
|
|
Very low Due to serious risk of bias, due to serious inconsistency, due to serious imprecision7 |
The evidence is very uncertain about the effect of additional swallowing training on aspiration when compared with standard swallowing training in stroke patients.
(Park, 2016; Park, 2017; Park, 2018; Park, 2019a; Park, 2020; Choi, 2017; Kim and Park, 2019; Liu, 2025; Eom, 2017; Jang, 2019; Kim, 2017) |
|
Difference: MD 0.87 lower (CI 95% 1.37 lower - 0.36 lower) |
|||||
|
Measured by: PAS Scale: 1-8, lower is better Based on data from 38 participants in 1 studies |
|
|
Very low Due to serious risk of bias, due to serious imprecision8 |
The evidence is very uncertain about the effect of additional CTAR on aspiration compared to additional shaker in stroke patients.
(Park, 2019b) |
|
|
Difference: MD 0.25 lower (CI 95% 0.80 lower - 0.30 higher) |
|||||
1. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Inconsistency: serious. Statistical heterogeneity (I²) was high (>60%)
Imprecision: serious. Average number of patients (100–300), Wide confidence intervals;
2. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals;
3. Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals;
4. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals;
5. Imprecision: serious. Low number of patients (<100), Wide confidence intervals;
6. Risk of Bias: serious Inadequate generation of sequences or comparable groups
Imprecision: serious. Low number of patients (<100), Wide confidence intervals;
7. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Inconsistency: serious. Statistical heterogeneity (I²) was high (>60%)
Imprecision: serious. Wide confidence intervals;
8. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals.
HNC
PICO (1.2)
Population: HNC patients
Intervention: (additional) Swallowing training
Comparator: standard care or swallowing training
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
standard care / swallowing training |
Swallowing training |
||||
|
Number/percentage of patients who return to a normal diet
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in HNC patients. |
|
|
Functional oral intake of food experienced by the patient
|
Measured by: FOIS Scale: 1-7, higher is better Based on data from 56 participants in 2 studies
|
Difference: MD 3.0 higher (CI 95% 2.41 higher - 3.59 higher) |
Low Due to serious risk of bias, due to serious imprecision1 |
Swallowing training may result increase the functional oral intake when compared with standard care in HNC patients. (Balbinot, 2020; Kotz, 2012) |
|
|
Swallowing-related quality of life
|
Measured by: MDADI Scale: 20-100, higher is better Based on data from 95 participants in 1 study
|
Difference: MD 10.76 higher (CI 95% 6.19 higher - 15.33 higher) |
Low due to serious imprecision2 |
Swallowing training may increase the swallowing-related quality of life when compared with standard care in HNC patients. (Zhang, 2025) |
|
|
Measured by: EAT-10 Scale: 0-40, lower is better Based on data from 95 participants in 1 study
|
Difference: MD 3.88 lower (CI 95% 6.06 lower - 1.70 lower) |
Low due to serious imprecision3 |
Swallowing training may result in little to no difference in the swallowing-related quality of life when compared with standard care in HNC patients. (Zhang, 2025) |
||
|
Measured by: EAT-10 Scale: 0-40, lower is better Based on data from 47 participants in 1 study
|
Difference: MD 2.60 lower (CI 95% 4.97 lower - 0.23 lower) |
Low due to serious imprecision4 |
Additional swallowing training may result in little to no difference in the swallowing-related quality of life when compared with standard swallowing training in HNC patients. (Dotevall, 2023) |
||
|
Functional swallowing ability
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of (additional) swallowing training compared to standard care/swallowing training in HNC patients. |
|
|
Aspiration
|
Measured by: PAS Scale: 1-8, lower is better Based on data from 40 participants in 1 study
|
Difference: MD 0.35 lower (CI 95% 0.68 lower - 0.02 lower) |
Very low Due to serious risk of bias, due to serious imprecision5 |
The evidence is very uncertain about the effect of swallowing training on aspiration compared to standard care in HNC patients. (Hsiang, 2019) |
|
|
Measured by: PAS Scale: 1-8, lower is better Based on data from 99 participants in 2 studies
|
Difference: MD 0.01 higher (CI 95% 0.75 lower - 0.77 higher) |
Moderate due to serious imprecision6 |
Additional swallowing training likley result in little to no difference in aspiration when compared with standard swallowing training in HNC patients. (Dotevall, 2023; Tuomi, 2022) |
||
1. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Imprecision: serious.Low number of patients (<100)
2. Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals;
3. Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals;
4. Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals;
5. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals;
6. Imprecision: serious. Low number of patients (<100), Wide confidence intervals.
Patients with Parkinson’s Disease
PICO (1.3)
Population: patients with Parkinson’s Disease
Intervention: Expiratory muscle training or additional swallowing training
Comparator: standard care or standard swallowing training
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
Standard care / swallowing training |
Expiratory muscle training/ additional swallowing training |
||||
|
Number/percentage of patients who return to a normal diet
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of expiratory muscle training compared to standard care or additional swallowing training compared with standard swallowing training in patients with Parkinson’s Disease. |
|
|
Functional oral intake of food experienced by the patient
|
Measured by: FOIS Scale: 1-7, higher is better Based on data from 60 participants in 1 study
|
Difference: MD 0.27 higher (CI 95% 0.05 lower - 0.59 higher) |
Low Due to serious risk of bias, due to serious imprecision1 |
Additional swallowing training may result in little to no difference in the functional swallowing ability when compared with standard swallowing training in patients with Parkinson’s Disease. (Plaza, 2022) |
|
|
Swallowing-related quality of life
|
Measured by: SWAL-QOL Scale: 44-220, higher is better Based on data from 50 participants in 1 study
|
Difference: MD 11.40 higher (CI 95% 4.47 lower – 27.27 higher)
|
LOW due to serious imprecision2 |
Expiratory muscle training may improve the swallowing-related quality of life when compared with standard care in patients with Parkinson’s Disease. (Claus, 2021) |
|
|
Functional swallowing ability
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of expiratory muscle training compared to standard care or additional swallowing training compared with standard swallowing training in patients with Parkinson’s Disease. |
|
|
Aspiration
|
Measured by: PAS Scale: 1-8, lower is better Based on data from 60 participants in 1 study |
Difference: MD 1.04 lower (CI 95% 1.69 lower - 0.39 lower) |
Low due to serious imprecision3 |
Expiratory muscle training may decrease the aspiration when compared with standard care in patients with Parkinson’s Disease. (Troche, 2010) |
|
1. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Imprecision: serious. Low number of patients (<100), Data from only one study
2. Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals;
3. Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals.
Patients with Multiple Sclerosis
PICO (1.4)
Population: MS patients
Intervention: Swallowing training
Comparator: standard care
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
Standard care |
Swallowing training |
||||
|
Number/percentage of patients who return to a normal diet
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in MS patients. |
|
|
Functional oral intake of food experienced by the patient
|
Measured by: MASA Scale: 0-200, higher is better Based on data from 20 participants in 1 study |
Difference: MD 24.0 higher (CI 95% 14.40 higher - 33.60 higher) |
Low due to serious imprecision1 |
Swallowing training may increase the functional oral intake when compared with standard care in MS patients. (Tarameshlu, 2019) |
|
|
Swallowing-related quality of life
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in MS patients. |
|
|
Functional swallowing ability
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in MS patients. |
|
|
Aspiration
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in MS patients. |
|
1. Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals.
Post-intubation
PICO (1.5)
Population: post-intubation patients
Intervention: Swallowing training
Comparator: standard care
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
Standard care |
Swallowing training |
||||
|
Number/percentage of patients who return to a normal diet
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in post-intubation patients. |
|
|
Functional oral intake of food experienced by the patient
|
Measured by: FOIS Scale: 1-7, higher is better Based on data from 32 participants in 1 study
|
Difference: MD 1.56 higher (CI 95% 0.57 higher - 2.55 higher) |
Very low Due to serious risk of bias, due to serious imprecision1 |
The evidence is very uncertain about the effect of swallowing training on functional oral intake compared to standard care in post-intubation patients. (Turra, 2021) |
|
|
Swallowing-related quality of life
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in post-intubation patients. |
|
|
Functional swallowing ability
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in post-intubation patients. |
|
|
Aspiration
|
-
|
-
|
No GRADE (no evidence was found) |
No evidence was found regarding the effect of swallowing training compared to standard care in post-intubation patients. |
|
1. Risk of Bias: serious. Inadequate generation of sequences or comparable groups
Imprecision: very serious. Low number of patients (<100), Data from only one study, Wide confidence intervals.
Heterogenous including elderly with OD
PICO (1.6)
Population: heterogenous including elderly with OD
Intervention: Swallowing training
Comparator: Standard care
A Summary of Findings table could not be created due to lack of data.
Description of studies
A total of six studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Wakabayahi (2018) conducted a cluster-randomized controlled trial to evaluate the effects of resistance training of swallowing muscles on dysphagia in older adults. A total of 104 community-dwelling individuals aged ≥65 years with dysphagia (EAT-10 score ≥3) were enrolled from 19 care facilities and randomized by cluster into an intervention group (8 clusters, 43 participants completing follow-up) and a control group (11 clusters, 48 participants). The intervention consisted of tongue-press and head-flexion resistance exercises; both groups received educational materials on dysphagia.
Claus (2021) conducted a double-blind, randomized, placebo-controlled trial to evaluate the effects of expiratory muscle strength training (EMST) on pharyngeal dysphagia in patients with Parkinson’s Disease (PD). Fifty individuals with PD and FEES-confirmed dysphagia participated in a 4-week home-based training program.
Participants were randomly assigned to either an active EMST intervention, using a threshold device set at 75% of individual maximum expiratory pressure, or a sham training condition with minimal resistance. Both groups followed the same training schedule (5 days per week, 5 sets of 5 repetitions per session).
The primary outcome measure was change in overall FEES-based dysphagia severity after the intervention. Secondary outcomes included FEES subscores (such as pharyngeal residue and penetration/aspiration), patient-reported swallowing function and swallowing-related quality of life, and the persistence of effects at 3-month follow-up. In a subgroup, changes in swallowing-related cortical activation were additionally assessed using magnetoencephalography.
Jensen (2022) conducted a cluster randomized controlled trial to evaluate the effect of Chin Tuck Against Resistance (CTAR) exercises on oropharyngeal dysphagia in older adults. The median age of the participants was 78 years, with an interquartile range (IQR) of 71 to 84 years. Ninety-two community-dwelling participants with dysphagia, confirmed by the Volume-Viscosity Swallow Test and/or the Minimal Eating Observation Form-II, were randomized to either standard care (n = 46) or standard care plus a 6-week CTAR training program (n = 46).
Lee (2024) conducted a network meta-analysis and evaluated the comparative efficacy of various swallowing rehabilitative therapies for adults with dysphagia. The mean age ranged from 39.9 to 83.1 years. The study aimed to identify which interventions most effectively improve swallowing function and reduce aspiration risk. A systematic search was conducted across five databases (Web of Science, Embase, CINAHL, Cochrane Library, and PubMed) up to September 2024. Eligible studies were randomized controlled trials (RCTs) involving adults with diagnosed dysphagia and reporting outcomes on swallowing function and/or aspiration. Out of 7,697 screened records, 24 RCTs with a total of 953 participants (post-stroke, neurodegenerative diseases [Parkinson’s Disease and Multiple Sclerosis], head and neck cancer, traumatic brain injury and older adults) met the inclusion criteria. The interventions assessed included jaw and tongue exercises, chin tuck against resistance (CTAR), Shaker exercises, effortful swallow training (EST), traditional dysphagia therapy (TDT), and respiratory muscle training (IMST and EMST). Both standalone and combination therapies were analyzed.
Liu (2025) conducted a single-center randomized controlled trial to evaluate the efficacy of inspiratory muscle training on aspiration symptoms in patients with dysphagia following ischemic stroke. Inclusion criteria encompassed adult inpatients with a confirmed diagnosis of ischemic stroke complicated by dysphagia-associated aspiration, who were deemed capable of participating in the intervention protocols.
A total of 58 participants were randomized into two groups: a control group receiving conventional swallowing therapy and an intervention group receiving conventional therapy supplemented with inspiratory muscle training using the POWERbreathe device. The intervention was administered twice daily over a two-week period.
Zhang (2025) conducted a randomized controlled trial at a single center, the Shanghai Proton and Heavy Ion Center, between March and October 2023. The trial aimed to evaluate the efficacy of combined swallowing training and feeding management in improving swallowing function, swallowing-related quality of life, and nutritional status in patients with head and neck cancer undergoing particle therapy.
The inclusion criteria consisted of adult patients aged 18 years or older with histologically confirmed head and neck cancer who were undergoing particle therapy, with or without concurrent chemotherapy. Patients with dysphagia due solely to cancer-related factors were eligible, whereas those with dysphagia caused by non-cancerous conditions were excluded.
A total of 96 patients were enrolled and randomized equally into intervention (n=48) and control (n=48) groups.
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
Included in systematic review Lee, 2024 see Table 1 in article (Balbinot, 2020; Chen, 2018; Kotz, 2012; Tarameshlu, 2019; Turra, 2021; Hsiang, 2019; Troche, 2010; Park, 2019a; Choi, 2017; Dotevall, 2023; Park, 2017; Tuomi, 2022; Kim and Park, 2019; Park, 2018; Park, 2020; Kim, 2017; Moon, 2018; Plaza 2022; Jang, 2019; Liaw, 2020; Eom, 2017; Park, 2016; Gao& Huang, 2014; Park, 2019b) |
||||||
|
Individual studies |
||||||
|
Wakabayashi, 2018 |
N at baseline Intervention: 43 Control: 48
Age (mean, SD) Intervention: 79.6, 7.2 Control: 80.2, 6.6
Sex (M/F) Intervention: 17/26 Control: 20/28 |
Intervention: Resistance training of swallowing muscles (tongue-press + head-flexion) Control: usual care with educational brochure only |
Post-intervention (duration not clearly specified; intervention described as 2 sessions/week for several weeks) |
EAT-10 score |
No funding from industry declared; nutritional status was associated with better outcomes in secondary analysis |
Some concerns (lack of blinding) |
|
Claus, 2021 |
N at baseline |
Intervention: Expiratory Muscle Strength Training (EMST) using a threshold device set at 75% of individual maximum expiratory pressure; home-based training, 5 days/week, 5 sets of 5 repetitions, for 4 weeks |
Post-intervention (4 weeks) and 3-month follow-up |
Patient-reported swallowing function (Swallowing Disturbance Questionnaire, SDQ) |
No industry funding reported |
Low |
|
Jensen, 2022 |
N at baseline Intervention: 48 Control: 42
Age (median) Intervention: 79 Control: 77.1
Sex (M/F) Intervention: 24/24 Control: 24/18 |
Intervention: CTAR training + standard care Control: standard care only (dietary advice, supervision, posture) |
12 weeks |
DHI-DK |
No industry funding reported; some heterogeneity in diagnoses (e.g., stroke, Parkinson’s Disease); no instrumental swallowing assessments used |
High (unclear allocation concealment, blinding loss to follow-up) |
|
Liu, 2025 |
N at baseline Intervention: 29 Control: 29
Age (mean, SD) Intervention: 59.66, 8.90 Control: 62.44, 8.60
Sex (M/F) Intervention: 21/8 Control: 21/8 |
Intervention: conventional swallowing therapy plus inspiratory muscle training
Control: conventional swallowing therapy
(Both groups received conventional swallowing function training, including oral sensory training, oral motor training, airway safety protection training, and neuromuscular electrical stimulation therapy for 10–20 min per session, twice daily for 2 weeks. The treatment group additionally received inspiratory muscle resistance training using the POWERbreathe device for 20 min per session, twice daily for 2 weeks.) |
2 weeks |
FOIS FDS PAS |
This research was supported by Fujian Provincial Natural Science Foundation of China (Grant No. 2023 J011858), the National Natural Science Foundation of China (Grant No. 82172531) and the Joint Funds for the Innovation of Science and Technology, Fujian Provinc (No.2021Y9105).
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Patients: post ischemic stroke |
High (randomization, allocation concealment, blinding) |
|
Zhang (2025) |
N at baseline Intervention: 48 Control: 48
Age (mean, SD) Intervention: 58.2 (±8.7) Control: 59.1 (±9.2)
Sex M/F Intervention: 35/13 Control: 34/14 |
Intervention: Combined swallowing training + nutritional management
Control: Standard care (no swallowing or feeding intervention) |
3 months |
EAT-10 MDADI |
No major funding bias reported.Study conducted at single specialized cancer center.No conflicts of interest reported.
Patients: head neck cancer |
Some concern (lack of blinding) |
*For further details, see risk of bias table in the appendix
Results
Stroke patients
Thirteen studies evaluated the impact of additional swallowing training (Choi, 2017; Eom, 2017; Jang, 2019; Kim, 2017; Kim and Park, 2019; Liaw, 2020; Liu, 2025; Moon, 2018; Park, 2016; Park, 2017; Park, 2018; Park, 2019a; Park, 2020) and one study compared Chin Tuck Against Resistance (CTAR) combined with swallowing training to the Shaker exercise combined with swallowing training (Park, 2019b), assessing the effects on outcome measures in patients with stroke.
Functional oral intake of food as experienced by the patient (crucial)
Nine studies reported the outcome measure functional oral intake of food as experienced by the patient.
Six studies reported the outcome with the use of the Functional Oral Intake Scale (FOIS) up to six weeks (scale 1-7, higher is better) (Choi, 2017; Kim and Park, 2019; Liaw, 2020; Liu, 2025; Park, 2016; Park, 2020). In total 106 patients received additional swallowing training, and 106 patients received standard swallowing training (Figure 1). The mean difference was 1.27 points (95% CI 0.83 to 1.70), in favor of the patients receiving additional swallowing training. This difference is considered clinically relevant.
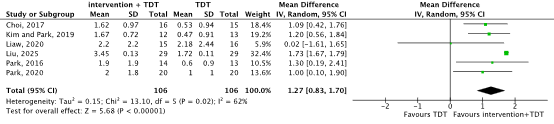
Figure 1. Functional oral intake in stroke patients receiving additional swallowing training versus standard swallowing training
One study reported the outcome with the use of the Mann Assessment of Swallowing Ability (MASA) up to 8 weeks (scale 0-200, higher is better) (Moon, 2018). In total 8 patients received additional swallowing training (tongue exercises), and 8 patients received standard swallowing training. The mean difference was 4.50 points (95% CI -2.23 to 11.23), in favor of the patients receiving additional swallowing training. The difference is not considered clinically relevant.
One study reported the outcome with the use of the American Speech-Language-Hearing Association National Outcome Measurement System (ASHA-NOMS) up to 2 weeks (scale 0-7, higher is better) (Jang, 2019). In total 18 patients received additional swallowing training (Respiratory Muscle Training), and 18 patients received standard swallowing training. The mean difference was 0.40 points (95% CI -0.34 to 1.14), in favor of the patients receiving additional swallowing training. The difference is not considered clinically relevant.
One study reported the outcome measure functional oral intake of food as experienced by the patients with the use of the FOIS up to 4 weeks (scale 1-7, higher is better) (Park, 2019b).
In total 19 patients received CTAR and swallowing training, and 19 patients received Shaker and swallowing training. The mean differences was 0.40 points (95% CI -0.20 to 1.00), in favor of the patients receiving CTAR and swallowing training. The difference is not considered clinically relevant.
Swallowing-related quality of life (crucial)
One study reported the outcome swallowing-related quality of life with the use of the Swallowing Quality of Life Questionnaire (SWAL-QOL) up to 8 weeks (scale 0-100, higher is better) (Moon, 2018). In total 8 patients received additional swallowing training (tongue exercises), and 8 patients received standard swallowing training. The mean differences was 6.50 points (95% CI -3.93 to 16.93), in favor of the patients receiving additional swallowing training. The difference is not considered clinically relevant.
Functional swallowing ability (important)
Two studies reported the outcome measure functional swallowing ability with the use of the Functional Dysphagia Scale (FDS) up to 2 weeks (scale 0-100, lower is better) (Jang, 2019; Liu, 2025).
Jang: In total 18 patients received additional swallowing training (Respiratory Muscle Training), and 18 patients received standard swallowing training. The mean difference was –2.09 points (95% CI -5.35 to 1.17), in favor of the patients receiving additional swallowing training. The difference is not considered clinically relevant.
Liu: In total 29 patients received additional swallowing training (inspiratory muscle training), and 29 patients received standard swallowing training. The mean difference was -11.48 points (95% CI -10.82 to -12.14), in favor of the patients receiving additional swallowing training. The difference is considered clinically relevant.
Number or percentage of patients who return to a normal diet (important)
The outcome measure number or percentage of patients who return to a normal diet was not reported.
Aspiration (important)
Twelve studies reported the outcome measure aspiration (Choi, 2017; Eom, 2017; Jang, 2019; Kim, 2017; Kim and Park, 2019; Liu, 2025; Park, 2016; Park, 2017; Park, 2018; Park, 2019a; Park, 2019b; Park, 2020.
Eleven studies reported the outcome measure aspiration with the use of the Penetration Aspiration Scale (PAS) up to six weeks (scale 1-8, lower is better) (Choi, 2017; Eom, 2017; Jang, 2019; Kim, 2017; Kim and Park, 2019; Liu, 2025; Park, 2016; Park, 2017; Park, 2018; Park, 2019a; Park, 2020). In total 176 patients received additional swallowing training, and 175 patients received standard swallowing training (Figure 2). The mean difference was -0.87 points (95% CI -1.37 to -0.36), in favor of the patients receiving additional swallowing training. This difference is considered clinically relevant.

Figure 2. Aspiration in stroke patients receiving additional swallowing training versus standard swallowing training
One study reported the outcome measure aspiration with the use of the PAS up to 4 weeks (scale 1-8, lower is better) (Park, 2019b). In total 19 patients received CTAR and swallowing training, and 19 patients received Shaker and swallowing training. The mean difference was -0.25 points (95% CI -0.80 to 0.30), in favor of the patients receiving CTAR and swallowing training. This difference is not considered clinically relevant.
HNC-patients
Four studies compared swallowing training to standard care (Balbinot, 2020; Hsiang, 2019; Kotz, 2012; Zhang, 2025) and two studies evaluated the impact of additional shaker training (Dotevall, 2023; Tuomi, 2022), assessing their effects on outcome measures in patients with head and neck cancer.
Furthermore, a systemic review with meta-analysis has been performed on the effect of swallowing exercises for head and neck cancer patients (Banda 2020).
Functional oral intake of food as experienced by the patient (crucial)
Two studies reported the outcome measure functional oral intake of food as experienced by the patient with the use of the FOIS up to twelve weeks (scale 1-7, higher is better) (Balbinot, 2020; Kotz, 2012).
Balbinot: In total 15 patients received swallowing training, and 15 patients received standard care. The mean difference was 3.00 points (95% CI 2.41 to 3.59), in favor of the patients receiving swallowing training. This difference is considered clinically relevant.
Kotz: In total 13 patients received swallowing training, and 13 patients received standard care. Mean difference could not be calculated as only median and ranges were reported.
Swallowing training group median score, 3 (range, 1-7), vs median standard care score, 4 (range, 1-6) However, swallowing training group had significantly better scores at months 3 and 6 (median 3-month intervention score, 7(range, 5-7), vs median control score, 5 (range, 3-7); median 6-month intervention score, 7 (range,6-7), vs median control score, 6 (range, 3-7)). There was no significant difference in scores at months 9 and 12.
Swallowing-related quality of life (crucial)
Two studies reported the outcome measure swallowing-related quality of life (Dotevall, 2023; Zhang, 2025).
One study reported the outcome measure swallowing-related quality of life with the use of the M.D. Anderson Dysphagia Inventory (MDADI) up to 12 weeks (scale 20-100, higher is better) and Eating Assessment Tool- 10 (EAT- 10) up to 12 weeks (scale 0-40, lower is better) (Zhang, 2025). In total 47 patients received swallowing training, and 48 patients received standard care. For the MDADI the mean difference was 10.76 points (95% CI 6.19 to 15.33), in favor of the patients receiving swallowing training. The difference is considered clinically relevant.
For the EAT-10 the mean differences was -3.88 points (95% CI -6.06 to -1.70), in favor of the patients receiving swallowing training. The difference is not considered clinically relevant
One study reported the outcome measure swallowing-related quality of life with the use of the EAT- 10 up to 8 weeks (scale 0-40, lower is better) (Dotevall, 2023). In total 23 patients received additional shaker, and 24 patients received standard swallowing training. The mean difference was -2.60 points (95% CI -4.97 to -0.23), in favor of the patients receiving additional shaker. The difference is not considered clinically relevant.
Functional swallowing ability (important)
The outcome measure functional swallowing ability was not reported.
Number or percentage of patients who return to a normal diet (important)
The outcome measure number or percentage of patients who return to a normal diet was not reported.
Aspiration (important)
Three studies reported the outcome measure aspiration (Dotevall, 2023; Hsiang, 2019; Tuomi, 2022).
One study reported the outcome measure aspiration with the use of the PAS up to 12 weeks (scale 1-8, lower is better) (Hsiang, 2019). In total 20 patients received swallowing training, and 20 patients received standard care. The mean difference was -0.35 points (95% CI -0.68 to 0.02), in favor of the patients receiving swallowing training. This difference is not considered clinically relevant.
Dotevall (2023) reported that in total 23 patients received additional shaker, and 24 patients received standard swallowing training. The mean difference was -0.30 points (95% CI -1.70 to 1.00), in favor of the patients receiving additional shaker. This difference is not considered clinically relevant.
Tuomi (2022) reported that in total 25 patients received additional shaker, and 27 patients received standard swallowing training. The mean difference was -0.40 points (95% CI -1.58 to 0.78), in favor of the patients receiving additional shaker. This difference is not considered clinically relevant.
Neurodegenerative diseases
Patients with Parkinson’s Disease
Two studies compared expiratory muscle training to a sham intervention (Troche, 2010; Claus, 2021) and one study evaluated the impact of additional tongue exercises (Plaza, 2022), assessing the effects on outcome measures in patients with Parkinson’s Disease.
Functional oral intake of food as experienced by the patient (crucial)
One study reported the outcome measure functional oral intake of food as experienced by the patients with the use of the FOIS up to 8 weeks (scale 1-7, higher is better) (Plaza, 2022).
In total 30 patients received additional swallowing training (tongue exercises), and 30 patients received standard swallowing training. The mean differences was 0.27 points (95% CI -0.05 to 0.59), in favor of the patients receiving additional swallowing training. The difference is not considered clinically relevant.
Swallowing-related quality of life (crucial)
Two studies reported the outcome swallowing-related quality of life (Plaza, 2022; Claus, 2021)
One study reported the outcome swallowing-related quality of life with the use of the SWAL-QOL up to 8 weeks (scale 0-100, higher is better) (Plaza, 2022). Mean difference could not be calculated due to lack of reporting. In summary, before the intervention, there were no significant differences between the groups in the SWAL-QOL items: food selection, symptom frequency, eating duration, and eating desire. After the intervention, significant differences between groups were found for all these items, with notable effect sizes.
Claus (2021) reported the outcome up to 12 weeks with the use of the SWAL-QOL total score (44-220, higher is better). In total 25 patients received swallowing training (expiratory muscle training), and 25 patients received a sham intervention. The mean difference was 11.40 points (95% CI -4.47 to 27.27), in favor of the patients receiving swallowing training. This difference is not considered clinically relevant.
Functional swallowing ability (important)
The outcome measure functional swallowing ability was not reported.
Number or percentage of patients who return to a normal diet (important)
The outcome measure number or percentage of patients who return to a normal diet was not reported.
Aspiration (important)
One study reported the outcome measure aspiration with the use of the PAS up to 4 weeks (scale 1-8, lower is better) (Troche, 2010). In total 30 patients received swallowing training (expiratory muscle training), and 30 patients received a sham intervention. The mean difference was -1.04 points (95% CI -1.69 to -0.39), in favor of the patients receiving swallowing training. This difference is considered clinically relevant.
Patients with Multiple Sclerosis
One study compared swallowing training to standard care, assessing the effects on outcome measures in patients with Multiple Sclerosis.
Functional oral intake of food as experienced by the patient (crucial)
One study reported the outcome with the use of the MASA up to 6 weeks (scale 0-200, higher is better) (Tarameshlu, 2019). In total 10 patients received swallowing training, and 10 patients received standard care. The mean differences was 24 points (95% CI 14.40 to 33.60), in favor of the patients receiving swallowing training. The difference is considered clinically relevant.
Swallowing-related quality of life (crucial)
The outcome measure swallowing-related quality of life was not reported.
Functional swallowing ability (important)
The outcome measure functional swallowing ability was not reported.
Number or percentage of patients who return to a normal diet (important)
The outcome measure number or percentage of patients who return to a normal diet was not reported.
Aspiration (important)
One study reported the outcome measure aspiration with the use of the PAS up to 6 weeks (scale 1-8, lower is better) (Taramashlu, 2019). In total 10 patients received swallowing training, and 10 patients received standard care. Mean difference could not be calculated due to lack of reporting. In summary, the PAS scores improved across the time in both groups. They were different between groups after treatment in favor of the swallowing training group.
Frailty/general weakness
Post-intubation patients
One study compared swallowing training to standard care, assessing the effects on outcome measures in post-intubation patients.
Functional oral intake of food as experienced by the patient (crucial)
One study reported the outcome measure functional oral intake of food as experienced by the patients with the use of the FOIS up to 2 weeks (scale 1-7, higher is better) (Turra, 2021).
In total 17 patients received swallowing training, and 15 patients received standard care. The mean differences was 1.56 points (95% CI 0.57 to 2.55), in favor of the patients receiving swallowing training. The difference is considered clinically relevant.
Swallowing-related quality of life (crucial)
The outcome measure swallowing-related quality of life was not reported.
Functional swallowing ability (important)
The outcome measure functional swallowing ability was not reported.
Number or percentage of patients who return to a normal diet (important)
The outcome measure number or percentage of patients who return to a normal diet was not reported.
Aspiration (important)
The outcome measure aspiration was not reported.
Heterogenous including elderly with OD
Two studies evaluated the impact of additional swallowing training on outcome measures in heterogenous patients including elderly with OD.
Functional oral intake of food as experienced by the patient (crucial)
The outcome measure functional oral intake of food as experienced by the patient was not reported.
Swallowing-related quality of life (crucial)
Two studies reported the outcome measure swallowing-related quality of life (Wakabayashi, 2018; Jensen, 2022).
Wakabayashi (2018) reported the outcome measure swallowing-related quality of life with the use of the EAT- 10 (scale 0-40, lower is better). In total 43 patients received swallowing training, and 48 patients received standard care. Only median and interquartile ranges were reported. Before intervention the swallowing training and standard care group had a median score of 7 (5-13) and 8 (4-11) respectively. After the intervention the swallowing training and standard care group had also a median score of 7 (5-14) and 8 (4-12), respectively.
Jensen (2022) reported the outcome measure swallowing-related quality of life with the use of the Dysphagia Handicap Index—Danish version (DHI-DK) up to 12 weeks (scale 0-100, lower is better). In total 40 patients received additional swallowing training (CTAR), and 35 patients received standard swallowing training. Only median and interquartile ranges were reported. Before intervention the additional swallowing training and standard swallowing training group had a median score of 32 (22-43) and 24 (16-32) respectively. After the intervention the additional swallowing training and standard swallowing training group had a median score of 19 (12-37) and 18 (8-34), respectively.
Functional swallowing ability (important)
The outcome measure functional swallowing ability was not reported.
Number or percentage of patients who return to a normal diet (important)
The outcome measure number or percentage of patients who return to a normal diet was not reported.
Aspiration (important)
The outcome measure aspiration was not reported.
A systematic review of the literature was performed to answer the following question(s):
What is the effectiveness of intensive swallowing training programs, and which patients are eligible for them?
Table 1. PICO
| Patients | Patients with oropharyngeal dysphagia |
| Intervention | Swallowing rehabilitation/ swallowing training program |
| Control | Standard treatment or no treatment |
| Outcomes | The functional oral intake of food as experienced by the patient (measured with FOIS or FOAMS), swallowing-related quality of life (measured with the Swal-QoL, Visual Analogue Scale (VAS), MD Anderson Dysphagia Inventory(MDADI), and other questionnaires with a dysphagia domain), functional swallowing ability; the number or percentage of patients who return to a normal diet, aspiration |
| Other selection criteria | Study design: systematic reviews and randomized controlled trials |
Relevant outcome measures
The guideline panel considered the functional oral intake of food as experienced by the patient and swallowing-related quality of life as a critical outcome measure for decision making; and functional swallowing ability, the number or percentage of patients who return to a normal diet and aspiration as an important outcome measure for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
The guideline panel used the GRADE standard limits of 25% (a relative risk (RR) of <0.80 and >1.25) for dichotomous outcomes and 10% for continuous outcomes as a minimal clinically (patient) important difference. For dichotomous outcomes with very few events, a risk difference of 25% was used as a minimal clinically (patient) important difference.
Search and select (Methods)
A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2015 to 1st April 2025 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) dysphagia; (2) swallowing training. Duplicates were removed using EndNote software. After deduplication a total of 2515 records were imported for title/abstract screening. Studies were selected based on the criteria described in Table 1. Titles and abstracts were screened using the ASReview software version 1.6.2. The settings TF-IDF and Naïve bayes were used. Five studies were used as prior knowledge for inclusion (Balou, 2019; Wakabayashi, 2018; Furuya, 2020; Sayaca, 2020; Gandhi, 2021). One study was used as prior knowledge for exclusions (Ambrocio, 2023).
The first 10% of references were screened by the working group and the guideline methodologist. The remaining articles were subsequently screened by the guideline methodologist, using the following stopping rule: stop after 200 subsequent exclusions.
Initially, 43 studies were selected based on title and abstract screening. After reading the full text, 37 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and six studies, including a network meta-analysis, were included.
The included studies are described separately per disease category in the results section. These categories comprise patients after suffering from stroke, patients with head and neck cancer (HNC), patients with neurodegenerative diseases (including Parkinson’s Disease and Multiple Sclerosis), post-intubation patients, and heterogeneous patient populations, including elderly with oropharyngeal dysphagia (OD).
- Ambrocio KR, Garand KLF, Roy B, Bhutada AM, Malandraki GA. Diagnosing and managing dysphagia in inclusion body myositis: a systematic review. Rheumatology (Oxford). 2023 Oct 3;62(10):3227-3244. doi: 10.1093/rheumatology/kead194. PMID: 37115631.
- Baijens LW, Clavé P, Cras P, Ekberg O, Forster A, Kolb GF, Leners JC, Masiero S, Mateos-Nozal J, Ortega O, Smithard DG, Speyer R, Walshe M. European Society for Swallowing Disorders - European Union Geriatric Medicine Society white paper: oropharyngeal dysphagia as a geriatric syndrome. Clin Interv Aging. 2016 Oct 7;11:1403-1428. doi: 10.2147/CIA.S107750. PMID: 27785002; PMCID: PMC5063605.
- Balou M, Herzberg EG, Kamelhar D, Molfenter SM. An intensive swallowing exercise protocol for improving swallowing physiology in older adults with radiographically confirmed dysphagia. Clin Interv Aging. 2019 Feb 11;14:283-288. doi: 10.2147/CIA.S194723. PMID: 30804667; PMCID: PMC6375531.
- Claus I, Muhle P, Czechowski J, Ahring S, Labeit B, Suntrup-Krueger S, Wiendl H, Dziewas R, Warnecke T. Expiratory Muscle Strength Training for Therapy of Pharyngeal Dysphagia in Parkinson's Disease. Mov Disord. 2021 Aug;36(8):1815-1824. doi: 10.1002/mds.28552. Epub 2021 Mar 2. PMID: 33650729.
- Dyreborg L, Raunbak SM, Sørensen SS, Melgaard D, Westmark S. The Cost-Effectiveness of Chin Tuck Against Resistance Compared to Usual Care in Citizens with Oropharyngeal Dysphagia - An Economic Evaluation. Clinicoecon Outcomes Res. 2023 Dec 20;15:787-797. doi: 10.2147/CEOR.S431380. PMID: 38143783; PMCID: PMC10749109.
- Furuya H, Kikutani T, Igarashi K, Sagawa K, Yajima Y, Machida R, Tohara T, Takahashi N, Tamura F. Effect of dysphagia rehabilitation in patients receiving enteral nutrition at home nursing care: A retrospective cohort study. J Oral Rehabil. 2020 Aug;47(8):977-982. doi: 10.1111/joor.13030. Epub 2020 Jul 13. PMID: 32506544; PMCID: PMC7496106.
- Gandhi P, Steele CM. Effectiveness of Interventions for Dysphagia in Parkinson Disease: A Systematic Review. Am J Speech Lang Pathol. 2022 Jan 18;31(1):463-485. doi: 10.1044/2021_AJSLP-21-00145. Epub 2021 Dec 10. PMID: 34890260; PMCID: PMC9159671.
- Glynn, M. (1999). Management of Adult Neurogenic Dysphagia Maggie Lee Huckabee, Cathy A. Pelletier, Singular Publishing Group Inc., 1998. ISBN 1 56593 731 7. Price: £38.00. pp 300. The Journal of Laryngology & Otology, 113(7), 698–698. doi:10.1017/S0022215100144937.
- Jansen F, Coupé VMH, Eerenstein SEJ, Cnossen IC, van Uden-Kraan CF, de Bree R, Doornaert P, Halmos GB, Hardillo JAU, van Hinte G, Honings J, Leemans CR, Verdonck-de Leeuw IM. Cost-utility and cost-effectiveness of a guided self-help head and neck exercise program for patients treated with total laryngectomy: Results of a multi-center randomized controlled trial. Oral Oncol. 2021 Jun;117:105306. doi: 10.1016/j.oraloncology.2021.105306. Epub 2021 Apr 24. PMID: 33905913.
- Jensen D, Bendsen BB, Westmark S, Riis J, Krarup AL, Westergren A, Melgaard D. Effect of Chin Tuck against Resistance Exercise in Citizens with Oropharyngeal Dysphagia-A Randomised Controlled Study. Geriatrics (Basel). 2022 Nov 18;7(6):129. doi: 10.3390/geriatrics7060129. PMID: 36412618; PMCID: PMC9680398.
- Lee CL, Banda KJ, Chu YH, Liu D, Lee CK, Sung CM, Arifin H, Chou KR. Efficacy of swallowing rehabilitative therapies for adults with dysphagia: a network meta-analysis of randomized controlled trials. Geroscience. 2025 Apr;47(2):2047-2065. doi: 10.1007/s11357-024-01389-5. Epub 2024 Oct 23. PMID: 39438392; PMCID: PMC11979051.
- Liu S, Fan Z, Fu M, Cheng K, Zhang X, Ni J, Wang Z. Impact of inspiratory muscle training on aspiration symptoms in patients with dysphagia following ischemic stroke. Brain Res. 2025 Mar 1;1850:149396. doi: 10.1016/j.brainres.2024.149396. Epub 2024 Dec 9. PMID: 39662789.
- Sayaca C, Serel-Arslan S, Sayaca N, Demir N, Somay G, Kaya D, Karaduman A. Is the proprioceptive neuromuscular facilitation technique superior to Shaker exercises in swallowing rehabilitation? Eur Arch Otorhinolaryngol. 2020 Feb;277(2):497-504. doi: 10.1007/s00405-019-05772-3. Epub 2019 Dec 23. PMID: 31873776.
- Shaker, R., Easterling, C., Belafsky, P. C., & Postma, G. N. (Eds.). (2013). Manual of diagnostic and therapeutic techniques for disorders of deglutition (1st ed.). Springer. https://doi.org/10.1007/978-1-4614-3779-6
- Turra GS, Schwartz IVD, Almeida ST, Martinez CC, Bridi M, Barreto SSM. Efficacy of speech therapy in post-intubation patients with oropharyngeal dysphagia: a randomized controlled trial. Codas. 2021 Apr 26;33(2):e20190246. doi: 10.1590/2317-1782/20202019246. PMID: 33909759.
- Wakabayashi H, Matsushima M, Momosaki R, Yoshida S, Mutai R, Yodoshi T, Murayama S, Hayashi T, Horiguchi R, Ichikawa H. The effects of resistance training of swallowing muscles on dysphagia in older people: A cluster, randomized, controlled trial. Nutrition. 2018 Apr;48:111-116. doi: 10.1016/j.nut.2017.11.009. Epub 2017 Nov 27. PMID: 29469011.
Risk of Bias tables
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Wakabayashi, 2018 |
Probably yes
|
Probably yes
|
Probably no
Reason: Intervention was not blinded due to nature of physical training; blinding of assessors not clearly described. |
Definitely yes
|
Probably yes
|
Probably yes Reason: No major conflicts of interest or industry funding reported; cluster design may introduce contamination risk but was justified. |
Some concerns
Reason: Lack of blinding and incomplete reporting of allocation concealment |
|
Claus, 2021 |
Probably yes
Reason: The study is described as randomized, although the exact method of sequence generation is not reported. |
Probably yes
Reason: Use of an identical sham device suggests adequate concealment, but the specific concealment procedure is not explicitly described. |
Definitely yes
Reason: The trial is explicitly described as double-blind; participants were unaware of group allocation. |
Definitely yes
Reason: Drop-out was minimal and comparable between groups. |
Probably yes
Reason: All pre-specified primary and secondary outcomes were reported. |
Probably yes
Reason: No major baseline imbalances or conflicts of interest reported; small sample size and short intervention duration noted. |
LOW |
|
Jensen, 2022 |
Probably yes
Reason: Participants were randomized. Although the exact method (e.g. computer‑generated sequence) isn't described |
Probably no
Reason: No details on allocation concealment (e.g. sealed opaque envelopes, centralized randomization) were reported. |
Probably no
Reason: The paper does not specify whether patients, providers, outcome assessors or data analysts were blinded. No explicit statements on assessor blinding |
Probably no
Reason: Ninety‑two participants were initially included; retention and complete‑case results are reported. The numbers remaining at 12 weeks (31 intervention, 33 control) |
Probably yes
Reason; All primary and secondary outcomes described in methods (e.g. V‑VST, MEOF‑II, dysphagia frequency) are reported in results. No evidence of omitted pre‑specified outcomes. |
Probably yes
Reason: No major competing interests declared; multicentre across municipalities; standardized training; no obvious other issues detected |
HIGH
Reason: unclear allocation concealment, blinding loss to follow-up |
|
Liu, 2025 |
Probably no;
Reason: randomization process not stated |
Probably no;
Reason: allocation process not stated |
Probably no;
Reason: blinding process not stated |
Definitely yes;
Reason: no loss to follow-up |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
HIGH
Reason: randomization, allocation concealment, blinding |
|
Zhang, 2025 |
Definitely yes;
Reason: Central randomization with computer generated random numbers |
Definitely yes;
Reason: Opaque, sealed envelopes were used and opened by an independent researcher. |
Definitely yes;
Reason: Due to the inability to blind patients and intervention implementers to the content of the feeding management and swallowing training combined programme, blinding was only applied to data col- lectors and analysts. Assessment results for all patients were collected by a clinical nurse not involved in the intervention process. Similarly, data analysis was performed by dedicated members of the research team, as per blinding requirements for data analysts. |
Probably no;
Reason: large loss to follow-up in both groups. No imputation methods were used. |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
Some concerns (loss to follow-up) |
|
The risk of bias for the other articles can be found in the supplementary materials of Lee (2024) |
|||||||
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Tsou YA, Meng NH, Chang WD, Hua CH. Does swallow rehabilitation improve recovery of swallow function after treatment for advanced head and neck cancer. Sci Rep. 2025 Mar 10;15(1):8300. doi: 10.1038/s41598-025-87877-w. PMID: 40064906; PMCID: PMC11894089. |
Retrospective study |
|
Eliküçük Ç, Esen Aydinli F, Has Selmi N, Uzunoğlu C, Köksal M, Öter V, Akan B, Bostanci EB, Argun G. Can invasive interventions be avoided with a holistic swallowing therapy program in older patients in intensive care units: percutaneous endoscopic gastrostomy tubes or oral intake? Front Neurol. 2025 Jan 22;16:1484493. doi: 10.3389/fneur.2025.1484493. PMID: 39911454; PMCID: PMC11794108. |
Does not meet PICO criteria |
|
Kim HH, Park JS. Effects of effortful swallowing against kinesiology taping resistance on the swallowing function in patients with poststroke dysphagia: A randomized controlled trial. Medicine (Baltimore). 2024 May 24;103(21):e38344. doi: 10.1097/MD.0000000000038344. PMID: 38788044; PMCID: PMC11124620. |
Does not meet PICO criteria |
|
Ni BY, Jin HP, Wu W. Therapeutic effects of deep pharyngeal electrical stimulation combined with modified masako maneuver on aspiration in patients with stroke. NeuroRehabilitation. 2024;54(3):391-398. doi: 10.3233/NRE-240005. PMID: 38607771. |
Does not meet PICO criteria |
|
Ni B, Jin H, Wu W. Therapeutic effect of proprioceptive neuromuscular facilitation combined with muscle energy technique on post-stroke dysphagia. Technol Health Care. 2024;32(6):4331-4342. doi: 10.3233/THC-240220. PMID: 39520172; PMCID: PMC11613027. |
Does not meet PICO criteria |
|
Yang C, Zhao F, Xie C, Zhang Y, Dou Z, Wei X. Community-based group rehabilitation program for stroke patients with dysphagia on quality of life, depression symptoms, and swallowing function: a randomized controlled trial. BMC Geriatr. 2023 Dec 20;23(1):876. doi: 10.1186/s12877-023-04555-0. PMID: 38124046; PMCID: PMC10731687. |
Does not meet PICO criteria |
|
Dotevall H, Tuomi L, Petersson K, Löfhede H, Bergquist H, Finizia C. Treatment with head-lift exercise in head and neck cancer patients with dysphagia: results from a randomized, controlled trial with flexible endoscopic evaluation of swallowing (FEES). Support Care Cancer. 2022 Dec 17;31(1):56. doi: 10.1007/s00520-022-07462-z. PMID: 36526734; PMCID: PMC9758100. |
Included in the review by Lee (2024) |
|
Krekeler BN, Yee J, Kurosu A, Osman F, Peña-Chávez R, Leverson G, Young B, Sattin J, Knigge M, Thibeault S, Rogus-Pulia N. Effects of Device-Facilitated Lingual Strengthening Therapy on Dysphagia Related Outcomes in Patients Post-Stroke: A Randomized Controlled Trial. Dysphagia. 2023 Dec;38(6):1551-1567. doi: 10.1007/s00455-023-10583-0. Epub 2023 May 17. PMID: 37195518; PMCID: PMC10615659. |
Does not meet PICO criteria |
|
Petersson K, Finizia C, Pauli N, Dotevall H, Tuomi L. A randomized controlled study evaluating the head-lift exercise in head and neck cancer patients with radiation-induced dysphagia: effect on swallowing function and health-related quality of life over 12 months. Eur Arch Otorhinolaryngol. 2023 Dec;280(12):5445-5457. doi: 10.1007/s00405-023-08183-7. Epub 2023 Aug 16. PMID: 37584752; PMCID: PMC10620310. |
Does not meet PICO criteria |
|
Gao M, Xu L, Wang X, Yang X, Wang Y, Wang H, Song J, Zhou F. Efficacy and safety of oropharyngeal muscle strength training on poststroke oropharyngeal dysphagia: a systematic review and meta-analysis. BMJ Open. 2023 Sep 27;13(9):e072638. doi: 10.1136/bmjopen-2023-072638. PMID: 37758672; PMCID: PMC10537832. |
All studies are also included in the review by Lee (2024) |
|
Gandhi P, Steele CM. Effectiveness of Interventions for Dysphagia in Parkinson Disease: A Systematic Review. Am J Speech Lang Pathol. 2022 Jan 18;31(1):463-485. doi: 10.1044/2021_AJSLP-21-00145. Epub 2021 Dec 10. PMID: 34890260; PMCID: PMC9159671. |
Does not meet PICO criteria |
|
Liu J, Wang Q, Tian J, Zhou W, Gao Y, Chen X, Zhang W, Gao Y, Zhou L. Effects of chin tuck against resistance exercise on post-stroke dysphagia rehabilitation: A systematic review and meta-analysis. Front Neurol. 2023 Jan 9;13:1109140. doi: 10.3389/fneur.2022.1109140. PMID: 36698882; PMCID: PMC9868925. |
Part of the studies are also included in the review by Lee (2024) |
|
Wang T, Tai J, Hu R, Fan S, Li H, Zhu Y, Wu Y, Wu J. Effect of Tongue-Pressure Resistance Training in Poststroke Dysphagia Patients With Oral Motor Dysfunction: A Randomized Controlled Trial. Am J Phys Med Rehabil. 2022 Dec 1;101(12):1134-1138. doi: 10.1097/PHM.0000000000001998. Epub 2022 Mar 22. PMID: 35320813. |
Not available |
|
Tuomi L, Dotevall H, Bergquist H, Petersson K, Andersson M, Finizia C. The effect of the Shaker head-lift exercise on swallowing function following treatment for head and neck cancer: Results from a randomized, controlled trial with videofluoroscopic evaluation. Head Neck. 2022 Apr;44(4):862-875. doi: 10.1002/hed.26982. Epub 2022 Jan 23. PMID: 35068016; PMCID: PMC9306707. |
Included in the review by Lee (2024) |
|
Hajdú SF, Wessel I, Dalton SO, Eskildsen SJ, Johansen C. Swallowing Exercise During Head and Neck Cancer Treatment: Results of a Randomized Trial. Dysphagia. 2022 Aug;37(4):749-762. doi: 10.1007/s00455-021-10320-5. Epub 2021 Jun 11. PMID: 34117531; PMCID: PMC9345844. |
Does not meet PICO criteria |
|
Park JS, Hwang NK. Chin tuck against resistance exercise for dysphagia rehabilitation: A systematic review. J Oral Rehabil. 2021 Aug;48(8):968-977. doi: 10.1111/joor.13181. Epub 2021 Jun 12. PMID: 33973284. |
Included in the review by Lee (2024) |
|
Banda KJ, Chu H, Kao CC, Voss J, Chiu HL, Chang PC, Chen R, Chou KR. Swallowing exercises for head and neck cancer patients: A systematic review and meta-analysis of randomized control trials. Int J Nurs Stud. 2021 Feb;114:103827. doi: 10.1016/j.ijnurstu.2020.103827. Epub 2020 Nov 11. PMID: 33352439. |
Patient group included in Lee (2024), older studies included in meta-analysis |
|
Sayaca C, Serel-Arslan S, Sayaca N, Demir N, Somay G, Kaya D, Karaduman A. Is the proprioceptive neuromuscular facilitation technique superior to Shaker exercises in swallowing rehabilitation? Eur Arch Otorhinolaryngol. 2020 Feb;277(2):497-504. doi: 10.1007/s00405-019-05772-3. Epub 2019 Dec 23. PMID: 31873776. |
Does not meet PICO criteria |
|
Furuya H, Kikutani T, Igarashi K, Sagawa K, Yajima Y, Machida R, Tohara T, Takahashi N, Tamura F. Effect of dysphagia rehabilitation in patients receiving enteral nutrition at home nursing care: A retrospective cohort study. J Oral Rehabil. 2020 Aug;47(8):977-982. doi: 10.1111/joor.13030. Epub 2020 Jul 13. PMID: 32506544; PMCID: PMC7496106. |
Cohort study |
|
Balou M, Herzberg EG, Kamelhar D, Molfenter SM. An intensive swallowing exercise protocol for improving swallowing physiology in older adults with radiographically confirmed dysphagia. Clin Interv Aging. 2019 Feb 11;14:283-288. doi: 10.2147/CIA.S194723. PMID: 30804667; PMCID: PMC6375531. |
Cohort study |
|
Hägglund P, Hägg M, Wester P, Levring Jäghagen E. Effects of oral neuromuscular training on swallowing dysfunction among older people in intermediate care-a cluster randomised, controlled trial. Age Ageing. 2019 Jul 1;48(4):533-540. doi: 10.1093/ageing/afz042. PMID: 31062842; PMCID: PMC6593320. |
Does not meet PICO criteria |
|
Kim HH, Park JS. Efficacy of modified chin tuck against resistance exercise using hand-free device for dysphagia in stroke survivors: A randomised controlled trial. J Oral Rehabil. 2019 Nov;46(11):1042-1046. doi: 10.1111/joor.12837. Epub 2019 Jul 2. PMID: 31206210. |
Included in the review by Lee (2024) |
|
Park JS, Lee G, Jung YJ. Effects of game-based chin tuck against resistance exercise vs head-lift exercise in patients with dysphagia after stroke: An assessor-blind, randomized controlled trial. J Rehabil Med. 2019 Oct 29;51(10):749-754. doi: 10.2340/16501977-2603. PMID: 31515567. |
Included in the review by Lee (2024) |
|
Park HS, Oh DH, Yoon T, Park JS. Effect of effortful swallowing training on tongue strength and oropharyngeal swallowing function in stroke patients with dysphagia: a double-blind, randomized controlled trial. Int J Lang Commun Disord. 2019 May;54(3):479-484. doi: 10.1111/1460-6984.12453. Epub 2019 Jan 28. PMID: 30693627. |
Included in the review by Lee (2024) |
|
Tarameshlu M, Ghelichi L, Azimi AR, Ansari NN, Khatoonabadi AR. The effect of traditional dysphagia therapy on the swallowing function in patients with Multiple Sclerosis: A pilot double-blinded randomized controlled trial. J Bodyw Mov Ther. 2019 Jan;23(1):171-176. doi: 10.1016/j.jbmt.2018.01.016. Epub 2018 Jan 31. PMID: 30691748. |
Included in the review by Lee (2024) |
|
Hashemian M, Khorasani B, Tarameshlu M, Haghani H, Ghelichi L, Nakhostin Ansari N. Effects of Dysphagia Therapy on Swallowing Dysfunction after Total Thyroidectomy. Iran J Otorhinolaryngol. 2019 Nov;31(107):329-334. doi: 10.22038/ijorl.2019.36233.2193. PMID: 31857976; PMCID: PMC6914318. |
Does not meet PICO criteria |
|
Park JS, An DH, Oh DH, Chang MY. Effect of chin tuck against resistance exercise on patients with dysphagia following stroke: A randomized pilot study. NeuroRehabilitation. 2018;42(2):191-197. doi: 10.3233/NRE-172250. PMID: 29562558. |
Included in the review by Lee (2024) |
|
Babu S, Balasubramaniam RK, Varghese A. Effect of Modified Shaker Exercise on the Amplitude and Duration of Swallowing Sounds: Evidence from Cervical Auscultation. Rehabil Res Pract. 2017;2017:6526214. doi: 10.1155/2017/6526214. Epub 2017 Sep 7. PMID: 29082044; PMCID: PMC5610851. |
Does not meet PICO criteria |
|
Choi JB, Shim SH, Yang JE, Kim HD, Lee DH, Park JS. Effects of Shaker exercise in stroke survivors with oropharyngeal dysphagia. NeuroRehabilitation. 2017;41(4):753-757. doi: 10.3233/NRE-172145. PMID: 28946582. |
Included in the review by Lee (2024) |
|
Gao J, Zhang HJ. Effects of chin tuck against resistance exercise versus Shaker exercise on dysphagia and psychological state after cerebral infarction. Eur J Phys Rehabil Med. 2017 Jun;53(3):426-432. doi: 10.23736/S1973-9087.16.04346-X. Epub 2016 Nov 10. PMID: 27830923. |
Included in the review by Lee (2024) |
|
Eom MJ, Chang MY, Oh DH, Kim HD, Han NM, Park JS. Effects of resistance expiratory muscle strength training in elderly patients with dysphagic stroke. NeuroRehabilitation. 2017;41(4):747-752. doi: 10.3233/NRE-172192. PMID: 29254116. |
Included in the review by Lee (2024) |
|
Moon JH, Jung JH, Won YS, Cho HY, Cho K. Effects of expiratory muscle strength training on swallowing function in acute stroke patients with dysphagia. J Phys Ther Sci. 2017 Apr;29(4):609-612. doi: 10.1589/jpts.29.609. Epub 2017 Apr 20. PMID: 28533594; PMCID: PMC5430257. |
Included in the review by Lee (2024) |
|
Kim HD, Choi JB, Yoo SJ, Chang MY, Lee SW, Park JS. Tongue-to-palate resistance training improves tongue strength and oropharyngeal swallowing function in subacute stroke survivors with dysphagia. J Oral Rehabil. 2017 Jan;44(1):59-64. doi: 10.1111/joor.12461. PMID: 27883209. |
Included in the review by Lee (2024) |
|
Hajdú SF, Wessel I, Johansen C, Kristensen CA, Kadkhoda ZT, Plaschke CC, Dalton SO. Swallowing therapy and progressive resistance training in head and neck cancer patients undergoing radiotherapy treatment: randomized control trial protocol and preliminary data. Acta Oncol. 2017 Feb;56(2):354-359. doi: 10.1080/0284186X.2016.1269193. PMID: 28206871. |
Protocol |
|
Don Kim K, Lee HJ, Lee MH, Ryu HJ. Effects of neck exercises on swallowing function of patients with stroke. J Phys Ther Sci. 2015 Apr;27(4):1005-8. doi: 10.1589/jpts.27.1005. Epub 2015 Apr 30. PMID: 25995543; PMCID: PMC4433964. |
Does not meet PICO criteria |
|
Park JS, Kim HJ, Oh DH. Effect of tongue strength training using the Iowa Oral Performance Instrument in stroke patients with dysphagia. J Phys Ther Sci. 2015 Dec;27(12):3631-4. doi: 10.1589/jpts.27.3631. Epub 2015 Dec 28. PMID: 26834320; PMCID: PMC4713759. |
Does not meet PICO criteria |
|
Zhang B, Wong KP, Guo C, Chen SC, Fu S, Kang R, Xiao Q, Qin J. Effects of Non-Pharmacological Interventions on the Swallowing Function of Patients With Post-Stroke Dysphagia: A Systematic Review and Network Meta-Analysis. J Oral Rehabil. 2025 Jan;52(1):109-120. doi: 10.1111/joor.13901. Epub 2024 Nov 12. PMID: 39532528; PMCID: PMC11680505. |
All studies included in Zhang (2024) overlap with those in Lee (2024), and the non-overlapping studies do not fulfill the eligibility criteria defined by our PICO. |
Beoordelingsdatum en geldigheid
Publicatiedatum : 12-03-2026
Beoordeeld op geldigheid : 12-03-2026
Algemene gegevens
De ontwikkeling van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire cluster ingesteld. Dit cluster bestaat uit vertegenwoordigers van alle relevante organisaties die betrekking hebben op de zorg voor patiënten met stem- en slikklachten.
Het cluster Laryngologie bestaat uit meerdere richtlijnen, zie hier voor de actuele clusterindeling. De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden worden indien nodig gevraagd om hun expertise in te zetten voor een specifieke richtlijnmodule. Het cluster Laryngologie bestaat uit de volgende personen:
Clusterstuurgroep
- Dhr. drs. R.N.P.M. (Rico) Rinkel
- Mevr. drs. M.M.G.E.C. (Margaret) de Jong
- Mevr. dr. E.M.J.M. (Emke) van den Broek
- Dhr. dr. D.A. (Derrek) Heuveling
- Mevr. drs. M.J. (Marieke) Hazewinkel
Clusterexpertisegroep
- Mevr. drs. M. (Maya) Kemps
- Mevr. C. (Carine) Roos
- Mevr. Y.G.J. (Yvonne) Hendrick
- Mevr. drs. M.M. (Masja) van het Hoofd
- Mevr. P.S. (Petra) Verdouw
Met ondersteuning van
- Mevr. drs. B.L. (Babette) Gal-de Geest, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. dr. A.C. (Anniek) van ‘t Veld, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. E. (Esther) van der Bijl, informatiespecialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle clusterstuurgroepleden en actief betrokken expertisegroepsleden (fungerend als schrijver en/of meelezer bij tenminste één van de geprioriteerde richtlijnmodules) hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een richtlijnmodule worden wijzigingen in belangen aan de projectleider doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase. Een overzicht van de belangen van de clusterleden en betrokken expertisegroepsleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
Clusterstuurgroep
Tabel Gemelde (neven)functies en belangen stuurgroep
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Rico Rinkel (voorzitter) |
KNO-arts laryngoloog Amsterdam UMC |
Plv Regionaal Tuchtcollege |
Geen |
Geen restricties |
|
Emke van den Broek |
Laryngoloog UMC Utrecht |
Voorzitter kerngroep laryngologie, lid werkgroep chronische hoest, MAR larynxpapillomatose, bezoekend docent/KNO-arts opleiding logopedie Hogeschool Utrecht |
Geen |
Geen restricties |
|
Marieke Hazewinkel |
Radioloog bij MRON (Maatschap Radiologie Oost Nederland)
|
MRI trekker radioloog MST (Medisch Spectrum Twente) |
Geen |
Geen restricties |
|
Derrek Heuveling
|
KNO-arts Meander Medisch Centrum |
Lid Kerngroep Laryngologie Lid werkgroep Standpuntnota benigne speekselklierpathologie |
Geen |
Geen restricties |
|
Margaret de Jong
|
HumanCapitalCare arbodienst verlener
|
Lid klachtencommissie Sexuele Intimidatie en Geweld sociale werkvoorziening; onkostenvergoeding per zitting |
Geen |
Geen restricties |
Clusterexpertisegroep
Tabel Gemelde (neven)functies en belangen expertisegroep
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Maya Kemps
|
Klinisch geriater in Slingeland Ziekenhuis |
Geen |
Geen |
Geen restricties |
|
Carine Roos |
Logopedist slikteam, De Hoogstraat Revalidatie |
Axon docent slikproblematiek |
Geen |
Geen restricties |
|
Yvonne Hendrick |
Logopedist slikteam, De Hoogstraat Revalidatie |
Geen |
Geen |
Geen restricties |
|
Masja van het Hoofd |
Beleidsmedewerker Parkinson Vereniging |
Redacteur bij het parkinsonplatform in oprichting (informatieplatform vergelijkbaar met bijv ms.nl, diabetes.nl) |
Geen |
Geen restricties |
|
Petra Verdouw |
Patiëntenvereniging |
Geen |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door deelname van relevante patiëntenorganisaties aan de need-for-update en/of prioritering. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijnmodule is tevens ter commentaar voorgelegd aan alle relevante patiëntenorganisaties in de stuur- en expertisegroep (zie ‘Samenstelling cluster’ onder ‘Verantwoording’). De eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
| Module |
Uitkomst raming |
Toelichting |
|
Sliktrainingsprogramma’s bij dysfagie |
Geen financiële gevolgen |
Uitkomst 2 |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 3.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Need-for-update, prioritering en uitgangsvragen
Tijdens de need-for-update fase (november, 2023) inventariseerde het cluster de geldigheid van de richtlijnmodules binnen het cluster. Naast de partijen die deelnemen aan de stuur- en expertisegroep zijn hier ook andere stakeholders voor benaderd. Per richtlijnmodule is aangegeven of deze geldig is, herzien moet worden, kan vervallen of moet worden samengevoegd. Ook was er de mogelijkheid om nieuwe onderwerpen aan te dragen die aansluiten bij één (of meerdere) richtlijn(en) behorend tot het cluster. De richtlijnmodules waarbij door één of meerdere partijen werd aangegeven herzien te worden, werden doorgezet naar de prioriteringsronde. Ook suggesties voor nieuwe richtlijnmodules werden doorgezet naar de prioriteringsronde. Afgevaardigden vanuit de partijen in de stuur- en expertisegroep werden gevraagd om te prioriteren (zie ‘Samenstelling cluster’ onder ‘Verantwoording’). Hiervoor werd de RE-weighted Priority-Setting (REPS) – tool gebruikt. De uitkomsten (ranklijst) werd gebruikt als uitgangspunt voor de discussie. Voor de geprioriteerde richtlijnmodules zijn door de het cluster concept-uitgangsvragen herzien of opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde het cluster welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. Het cluster waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde het cluster tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd indien mogelijk gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding). GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
Tabel Gradaties voor de kwaliteit van wetenschappelijk bewijs
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in een richtlijnmodule volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door het cluster wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. Het cluster heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
Tabel Sterkte van de aanbevelingen
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
Bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de richtlijnmodule Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd voorgelegd aan alle partijen die benaderd zijn voor de need-for-update fase. De commentaren werden verzameld en besproken met het cluster. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door het cluster. De definitieve richtlijnmodule werd ter autorisatie of goedkeuring voorgelegd aan de partijen die beschreven staan bij ‘Initiatief en autorisatie’ onder ‘Verantwoording’.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 3.0 (2023). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html.
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Laryngologie - Module sliktraining |
|
|
Uitgangsvraag/modules: Wat is de effectiviteit van intensieve sliktrainingsprogramma’s en welke patiënten komen hiervoor in aanmerking? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 1 april 2025 |
|
Periode: vanaf 2015 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
|
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl:9777/ |
|
|
Toelichting:
De sleutelartikelen worden gevonden met deze search. Tevens worden onderstaande vier reviews en twee RCTs uit de huidige Richtlijn gevonden in de P en de I:
Vanwege de grote opbrengst wordt de search in AS Review uitgevoerd. |
|
|
Te gebruiken voor richtlijntekst: A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2015 to the 1st of April 2025 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) dysphagia; (2) swallowing training. Duplicates were removed using EndNote software. After deduplication a total of 2515 records were imported for title/abstract screening. |
|
Zoekopbrengst - 1 april 2025
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
360 |
273 |
|
|
RCT |
743 |
515 |
|
|
Observationele studies |
1052 |
757 |
|
|
Totaal |
2155 |
1545 |
2515* |
*voor AS Review
Zoekstrategie - 1 april 2025
Embase.com
|
No. |
Query |
Results |
|
#1 |
'dysphagia'/exp OR 'oropharyngeal dysphagia'/exp OR 'regurgitation'/exp OR 'swallowing'/exp OR 'cricopharyngeal dysfunction'/exp OR aphagopraxia:ti,ab,kw OR dysphag*:ti,ab,kw OR disphag*:ti,ab,kw OR dysfag*:ti,ab,kw OR disfag*:ti,ab,kw OR regurgitat*:ti,ab,kw OR swallow*:ti,ab,kw |
247473 |
|
#2 |
'kinesiotherapy'/exp OR 'exercise'/de OR 'muscle training'/exp OR 'resistance training'/de OR 'tongue strength'/exp OR 'muscle exercise'/exp OR (((muscle* OR myofunction* OR swallow* OR deglutit*) NEAR/3 (strength* OR training* OR therap* OR rehabilitat* OR improvement*)):ti,ab,kw) OR ((exercis* NEAR/3 (correcti* OR technique* OR therap* OR treatment*)):ti,ab,kw) OR ((resist* NEAR/3 (exercis* OR training*)):ti,ab,kw) OR ((tongue NEAR/3 (exercis* OR strengthen*)):ti,ab,kw) OR (((physical* OR speech*) NEAR/3 (therap* OR stimulat* OR rehabilitat*)):ti,ab,kw) OR kinesiotherap*:ti,ab,kw OR kinesitherap*:ti,ab,kw |
643540 |
|
#3 |
#1 AND #2 |
11067 |
|
#4 |
#3 AND [2015-2025]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
3465 |
|
#5 |
'meta analysis'/exp OR 'systematic review'/exp OR 'scoping review'/exp OR 'rapid review'/exp OR 'umbrella review'/exp OR 'cochrane database of systematic reviews'/jt OR 'network meta-analysis'/exp OR 'networkmeta analy*':ti,ab,kw OR 'networkmetaanaly*':ti,ab,kw OR metaanaly*:ti,ab,kw OR 'meta analy*':ti,ab,kw OR metanaly*:ti,ab,kw OR prisma:ti,ab,kw OR prospero:ti,ab,kw OR metaanali*:ti,ab,kw OR 'meta anali*':ti,ab,kw OR metanali*:ti,ab,kw OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab,kw) OR (((structured OR systemic*) NEAR/3 (review* OR overview* OR synth*) NEAR/3 literature):ti,ab,kw) OR ((systemic* NEAR/1 review*):ti,ab,kw) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab,kw) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab,kw) OR (((literature NEAR/3 (review* OR overview*)):ti,ab,kw) AND (search*:ti,ab,kw OR database*:ti,ab,kw OR 'data base*':ti,ab,kw)) OR (('data extraction*':ti,ab,kw OR 'data source*':ti,ab,kw) AND ('study selection*':ti,ab,kw OR 'studies selection*':ti,ab,kw)) OR ('search strateg*':ti,ab,kw AND 'selection criteria*':ti,ab,kw) OR ('data source*':ti,ab,kw AND 'data synth*':ti,ab,kw) OR medline*:ti,ab,kw OR pubmed*:ti,ab,kw OR 'pub med*':ti,ab,kw OR embase:ti,ab,kw OR cochrane*:ti,ab,kw OR (((critical* OR rapid*) NEAR/2 (review* OR overview* OR synth*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synth*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynth*:ti,ab,kw OR 'meta synth*':ti,ab,kw OR 'review* of review*':ti,ab,kw |
1095859 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4242733 |
|
#7 |
'major clinical study'/de OR 'clinical study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'cohort analysis'/de OR 'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
17958585 |
|
#8 |
#4 AND #5 - SR |
360 |
|
#9 |
#4 AND #6 NOT #8 - RCT |
743 |
|
#10 |
#4 AND #7 NOT (#8 OR #9) - Observationeel |
1052 |
|
#11 |
#8 OR #9 OR #10 - Totaal |
2155 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Deglutition Disorders/ or exp Deglutition/ or aphagopraxia.ti,ab,kf. or dysphag*.ti,ab,kf. or disphag*.ti,ab,kf. or dysfag*.ti,ab,kf. or disfag*.ti,ab,kf. or regurgitat*.ti,ab,kf. or swallow*.ti,ab,kf. |
160353 |
|
2 |
exp Physical Therapy Modalities/ or exp Exercise Therapy/ or ((muscle* or myofunction* or swallow* or deglutit*) adj3 (strength* or training* or therap* or rehabilitat* or improvement*)).ti,ab,kf. or (exercis* adj3 (correcti* or technique* or therap* or treatment*)).ti,ab,kf. or (resist* adj3 (exercis* or training*)).ti,ab,kf. or (tongue adj3 (exercis* or strengthen*)).ti,ab,kf. or ((physical* or speech*) adj3 (therap* or stimulat* or rehabilitat*)).ti,ab,kf. or kinesiotherap*.ti,ab,kf. or kinesitherap*.ti,ab,kf. |
300149 |
|
3 |
1 and 2 |
4624 |
|
4 |
limit 3 to yr="2015 -Current" |
2642 |
|
5 |
4 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
2581 |
|
6 |
exp Meta-Analysis/ or exp Network Meta-Analysis/ or exp Systematic Review/ or (networkmeta analy* or networkmetaanaly* or metaanaly* or meta analy* or metanaly* or prisma or prospero or metaanali* or meta anali* or metanali*).ti,ab,kf. or ((systemati* or scoping or umbrella or structured literature) adj3 (review* or overview*)).ti,ab,kf. or ((structured or systemic*) adj3 (review* or overview* or synth*) adj3 literature).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 (review* or overview*)) and (search* or database* or data base*)).ti,ab,kf. or ((data extraction* or data source*) and (study selection* or studies selection*)).ti,ab,kf. or (search strateg* and selection criteria*).ti,ab,kf. or (data source* and data synth*).ti,ab,kf. or (medline* or pubmed* or pub med* or embase or cochrane*).ti,ab,kf. or cochrane.jw. or ((critical* or rapid*) adj2 (review* or overview* or synth*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synth*)) and (search* or database* or data base*)).ab. or metasynth*.ti,ab,kf. or meta synth*.ti,ab,kf. |
815497 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2862164 |
|
8 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or exp cohort studies/ or epidemiologic studies/ or ((multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ |
7963356 |
|
9 |
5 and 6 - SR |
273 |
|
10 |
(5 and 7) not 9 - RCT |
515 |
|
11 |
(5 and 8) not (9 or 10) - Observationeel |
757 |
|
12 |
9 or 10 or 11 - Totaal |
1545 |