Niet-operatieve behandeling
Uitgangsvraag
Wat is de rol van oefentherapie bij de niet-operatieve behandeling van schouderinstabiliteit?
Aanbeveling
Overweeg in samenspraak met de patiënt en de individuele wensen de inzet van oefentherapie bij schouderinstabiliteit indien de recidiefkans laag is.
Adviseer de oefentherapie bij aanvang te richten op het verbeteren van neuromusculaire controle en spieruithoudingsvermogen.
Overweeg bij aanwezige angst voor reluxatie een gespecialiseerde fysio-/oefentherapeut in te schakelen voor een multifactoriële aanpak. Indien deze angst leidt tot persisterende belemmeringen in adl-, werk- of sporthervatting, overweeg dan in samenspraak met de patiënt de inzet van een interdisciplinair eerstelijnstraject in samenwerking met een psycholoog.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Er is literatuuronderzoek gedaan naar de rol van oefentherapie bij de niet-operatieve behandeling van schouderinstabiliteit. Hierbij wordt standaardtherapie gezien als fysio-/ oefentherapie volgens een vastgesteld protocol, met evaluatiemomenten na 6 weken, 3 maanden, 6 maanden en 12 maanden, gericht op herstel van mobiliteit, spierkracht en coördinatie. Er werden drie gerandomiseerde onderzoeken gevonden waarin niet-operatieve behandeling met uitgebreide oefentherapie (inclusief neuromusculaire training en advies) werd vergeleken met de standaard zorg. Standaard zorg betrof in deze studies klassieke krachttraining en range of motion oefeningen. De cruciale uitkomstmaat reluxatie werd in twee onderzoeken gerapporteerd (Eshoj, 2020; Kearney, 2024). In beide studies was het aantal patiënten met een reluxatie laag. Dit kan mogelijk worden verklaard door de (korte) follow-up periode. Vanwege het zeer lage aantal patiënten met een reluxatie in beide groepen en heterogeniteit tussen de studies, was de bewijskracht voor het gevonden effect zeer laag (GRADE very low). Dit betekent dat er veel onzekerheid bestaat rond het effect van niet-operatieve behandeling met oefentherapie op de uitkomstmaat reluxatie. Door deze zeer lage bewijskracht konden geen conclusies worden getrokken over het risico op reluxatie na niet-operatieve behandeling met oefentherapie, vergeleken met standaard zorg. Patiënt-gerapporteerde uitkomstmaten (PROMs) pijn en range of motion werden als belangrijke uitkomstmaten gedefinieerd. In de drie geïncludeerde studies werden diverse PROMs gerapporteerd, o.a. voor functie en voor mate van ervaren instabiliteit. Er wordt bij een meerderheid van de PROMs resultaten gevonden die in het voordeel zijn van de interventiegroep, maar er worden ook op een tweetal PROMS, uitkomsten gerapporteerd die in het voordeel zijn van de standaard zorg. De resultaten zijn dus tegenstrijdig. Bovendien is belangrijk om te vermelden dat alle resultaten op de PROMs (met uitzondering van de Patient Specific Function Scale in Eshoj, 2020), niet de klinisch relevante grens halen. Ook voor pijn en range of motion lijken er geen klinisch relevante verschillen te zijn. Voor de effecten op de belangrijke uitkomstmaten geldt dat deze met veel zorg moeten worden geïnterpreteerd. Onder andere vanwege het risico op bias en omdat de 95% betrouwbaarheidsintervallen de grenzen van klinische relevantie overschrijden waardoor er onduidelijkheid bestaat over het daadwerkelijke effect.
Hoewel de studie van Kearney (2024) vergeleken met Eshoj (2020) en Pulido (2023) verreweg het grootste aantal patiënten includeert, zijn er een aantal factoren waar rekening mee moet worden gehouden bij het interpreteren van de resultaten. Ten eerste het feit dat in de patiëntenpopulatie alleen patiënten met primaire traumatische luxaties zijn geïncludeerd, en de recidiverende luxaties niet zijn meegenomen. De studie van Kearney (2024) suggereert dat een begeleid fysiotherapeutisch programma voor vier maanden niet leidt tot betere uitkomsten op het gebied van recidiverende instabiliteit, functie en pijn, vergeleken met een eenmalig adviserend consult. Echter is 54% van de geïncludeerde populatie in deze studie ouder dan 40 jaar. In deze oudere populatie worden überhaupt minder recidieven gezien en vanwege een hogere kans op rotator cuff letsel vindt herstel ook trager plaats. Slechts 36% van de in de studie van Kearney (2024) omschreven populatie, heeft een luxatie opgelopen tijdens een sportactiviteit. Dit is een lager percentage dan wordt vermeld in andere studies (Robinson, 2006). Het feit dat er géén significante verandering van de Oxford Shoulder Instability Score (OSIS) werd gevonden in de jonge interventie groep, kan mogelijk verklaard worden door het lage aantal geïncludeerde jonge patiënten met een sportspecifieke luxatie. Verder is er een recidief aantal van 3,5% (10/284) gemeten in de hele groep. Dit is aanzienlijk minder dan in andere literatuur (36-100% in het eerste jaar na de eerste luxatie (Olds, 1992; Marans, 1992). Deze bevindingen zouden kunnen worden verklaard doordat de gegevens zijn verzameld in COVID tijd, waardoor wellicht de sport uitdagingen zijn beïnvloed binnen de populatie. Daarmee zouden de uitkomsten niet representatief kunnen zijn voor de normale populatie. Het interventie programma van Kearney (2024) was voornamelijk gericht op verbeteren van mobiliteit en versterken van de posterieure cuff. Bij een anterieure schouderluxatie zou ook meer aandacht uit moeten gaan naar de anterieure cuff en de proprioceptieve vaardigheden. Aandacht voor bewegingsangst reducerende handelingen zijn niet beschreven (Olds 2024). Vanwege deze beperkingen dienen de resultaten uit de studie van Kearney (2024) met zorg te worden geïnterpreteerd.
Kwaliteit van bewijs
De overall kwaliteit van bewijs is (zeer) laag. Dit betekent dat we (zeer) onzeker zijn over het gevonden geschatte effect van niet-operatieve behandeling met oefentherapie op de cruciale en belangrijke uitkomstmaten. Er is afgewaardeerd vanwege (zeer) ernstige:
- Risk of Bias: methodologische beperkingen waaronder een gebrek aan blindering.
- Inconsistentie: inconsistentie van de resultaten.
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grens/grenzen van klinische relevantie overschrijdt, en vanwege een zeer klein aantal events.
Samengevat kan er op basis van het gevonden bewijs geen conclusie worden getrokken over de effecten van niet-operatieve behandeling met oefentherapie vergeleken met standaard zorg. De aanbevelingen zijn daarom gebaseerd op basis van expert opinie.
Wel of geen niet-operatieve behandeling?
De keuze voor wel of geen niet-operatieve behandeling (met oefentherapie) hangt af van verschillende factoren, waaronder de kans op een recidief. Het bepalen van de recidiefkans is niet eenvoudig. Er zijn twee predictietools te gebruiken om richting te geven aan wie er minder kans heeft op een recidief en wellicht geschikt is voor niet-operatieve behandeling.
- Predicting Recurrent Instability of the Shoulder (PRIS; Olds, 2019).
- Nonoperative Instability Severity Index Score (NISIS; Tokish, 2020).
Indien er een lage kans op recidief bestaat, lijkt een niet-operatief traject meer gerechtvaardigd. Indien er een sportwens is, kan de haalbaarheid van ‘return to play’ worden bepaald middels de Shoulder Instabilty Return to Sport after Injury (SIRSI; Olds, 2021) vragenlijst. Op basis van de uitkomsten van deze vragenlijst kan een sportspecifiek interventieprogramma worden opgestart.
Na het doormaken van een eerste traumatische anterieure schouderluxatie, wordt aanbevolen dat patiënten die een risicoprofiel hebben om recidiverende instabiliteit te ontwikkelen een eenmalig consult hebben met een medisch specialist gespecialiseerd in schouder stabiliserende chirurgie (mannelijk geslacht, jonger dan 40 jaar, contactsporter, significant botverlies; zie richtlijn acute, primaire schouderluxaties). Afhankelijk van de risicofactoren en recidiefkans wordt in samenspraak met de patiënt de behandelkeuze gemaakt.
Indien er een recidief heeft plaatsgevonden en de voorkeur voor behandeling vanuit de patiënt nog steeds niet-operatief blijft, zal de fysio-/oefentherapeut opnieuw (net als na een eerste luxatie) in kaart moeten brengen welke functionele aspecten een relatie hebben met de instabiliteit. Op basis van deze bevindingen kan wederom worden overwogen of een niet-operatieve behandeling kans van slagen heeft. De functionele aspecten die een relatie hebben met instabiliteit worden in de volgende alinea’s toegelicht.
Sport
De impact van de gewenste sport bepaalt mede het risico op reluxatie. Bij bovenhandse contact-impactsporten, zoals rugby, handbal, waterpolo etc., kan pas een return to play fase worden ingegaan als alle noodzakelijke aspecten van een specifieke sport in de oefentherapie zijn getraind en gemeten. Tijd na de eerste luxatie, mag hierbij niet de leidende factor zijn. Het schetsen van een return to sport tijdspad is een van de onderwerpen die een fysio-/oefentherapeut samen met de patiënt bij aanvang van de niet-operatieve behandeling doorneemt. Voor de terugkeer naar sporttraining en wedstrijden dient in overleg met de trainer/ coach een opbouwend programma te worden gemaakt. (Schwank, 2022). In de module Terugkeer naar functie en sport staan de verschillende fasen voor terugkeer naar sport beschreven.
Range of motion en mate van laxiteit
De mate van trauma/impact die nodig is voor een “traumatisch anterieure schouderluxatie” verschilt per patiënt. Patiënten met meer laxiteit zijn kwetsbaarder en hebben minder impact nodig. De fysio-/oefentherapeut zal beoordelen of er sprake is van enige gewrichtslaxiteit, lokaal of gegeneraliseerd. Bij laxiteit is een stabiliserend trainingsprogramma aan te bevelen, eventueel in aanvulling op een noodzakelijke chirurgische behandeling.
Aan de andere kant wordt een endorotatie bewegingsbeperking (GIRD) ook in verband gebracht met schouderinstabiliteit, vooral bij bovenhandse sporters en zal moeten worden geïdentificeerd als risicofactor (Kun-yu Chou, 2025). Patiënten die volleybal spelen worden daarom beschouwd als een specifieke subgroep binnen deze richtlijn.
Angst voor reluxatie
Angst voor reluxatie wordt veel gezien bij schouderinstabiliteit (Olds, 2021). Omdat de literatuur naar de rol van psychologische impact bij schouderinstabiliteit groeiend maar nog zeer beperkt is, is dit niet meegenomen in het literatuuronderzoek, toch is het een factor waar rekening mee moet worden gehouden. Patiënten geven in een kwalitatieve studie aan graag erkenning te krijgen voor deze angst (van Iersel 2023). Bovendien wordt angst voor re-injury gezien als een belangrijke indicator voor het niet terugkeren naar sport (Broekmans, 2024). Beschermende motoriek leidt tot beperkingen in het bewegingsbereik (ROM) van het schoudergewricht, het vermijden van risicovolle bewegingen en het aanleren van een compensatoir beweegpatroon. Dit heeft een negatieve impact op de rotator cuff functie, zeker in het bewegingstraject dat wordt vermeden. Deze vicieuze cirkel vergroot het risico op recidiverende instabiliteit (Brindisino, 2023). Langdurig of overmatige angst, waarbij op fMRI aangetoonde cerebrale veranderingen (Ladderman, 2015) op diverse locaties zijn aangetoond, kan leiden tot uitgebreidere bewegingsangst zoals kinesiofobie.
Vermijdend bewegingsgedrag doorbreken
Het fysio-/oefentherapeutische doel is deze vicieuze cirkel te doorbreken. De behandeling vereist een benadering die zich, naast de focus op fysieke oefentherapie, ook richt op het reduceren van kinesiofobie (Sole, 2024; Brindisino, 2023; van Gastel 2024). Een beproefd middel is graded exposure; het graduele blootstellen aan risicovolle bewegingen en het verminderen van apprehension. Het erkennen van deze angst voor recidieven en alle gevolgen binnen het psychosociale domein zouden een onderdeel moeten zijn van de behandeling als er sprake is van angst voor reluxatie. Indien een meer overmatige bewegingsangst zoals kinesiofobie zich heeft gemanifesteerd, kan een multidisciplinaire aanpak worden overwogen met psychologische interventies zoals cognitieve gedragstherapie (Sole, 2024).
Neuromusculaire functie
Laesies in het capsulolabrale complex na een schouderluxatie kunnen leiden tot verstoringen van de proprioceptieve feedbackloop en neuromusculaire disfunctie van de rotator cuff. (Woo Sung Do, 2023). Het identificeren van trainbare neuromusculaire disfunctie is essentieel voor het beoordelen of er verbetering te verwachten valt met fysio-/oefentherapeutische behandeling.
Het trainen van coördinatie, proprioceptie en snelheid van aanspannen is in de primaire fase na een luxatie belangrijker dan het trainen op kracht. De rotator cuff heeft een primair stabiliserende functie en de snelheid waarmee het kan reageren op een externe impact, ten behoeve van het stabiliseren van de humeruskop, is de essentie van zijn functie (Jan, 2012; Roach 2013). Bij standaard zorg ligt de aandacht doorgaans meer op kracht en mobiliteit, waar bij neuromusculaire training de focus ligt op coördinatie, uithoudingsvermogen en snelheid van reageren.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
De geïncludeerde studies rapporteren verschillende PROMs. Er werden geen klinisch relevante verschillen gevonden tussen niet-operatieve behandeling met oefentherapie en standaardzorg. Op basis van deze uitkomsten kan niet worden geconcludeerd welke vorm van niet-operatieve behandeling de beste resultaten geeft op patiënt-gerapporteerde functie, pijn en instabiliteit. Voor de patiënt is een snel en pijnloos herstel het belangrijkste doel van de behandeling. Vaak wordt gekozen voor fysio-/oefentherapeutische begeleiding, vooral als er sprake is van de wens snel terug te keren op sportniveau. Een niet-operatieve behandeling is logischerwijs minder ingrijpend dan een chirurgische behandeling. Echter, compliance en geduld van de patiënt om de opbouw van oefentherapie geleidelijk uit te voeren van neuromusculaire controle tot sportspecifieke kracht en uithoudingsvermogen is essentieel voor een optimaal resultaat. Deze compliance en dit geduld is in de praktijk variabel bij patiënten.
Een van de belangrijkste voordelen van het niet-operatief starten met behandelen is dat bij teleurstellende resultaten of een recidiverende luxatie, alsnog gekozen kan worden voor een operatieve stabilisatie.
Het is belangrijk om de patiënt goed te informeren over een niet-operatieve behandeling met oefentherapie en de verwachtingen ten aanzien van de uiteindelijke terugkeer naar activiteit en/of sport. De keuze voor behandeling moet in overleg met de patiënt worden gemaakt en hierbij dienen de principes van samen beslissen te worden gehanteerd.
Kostenaspecten
Een uitgebreide, begeleide vorm van oefentherapie door een gespecialiseerde oefen- of fysio-/oefentherapeut is naar verwachting duurder en tijdsintensiever dan standaard niet-operatieve behandeling of wanneer een patiënt eenmalig advies krijgt en zelfstandig verder gaat trainen. Echter wanneer dankzij deze begeleiding een juiste opbouw van oefentherapie plaatsvindt en zodoende operatief ingrijpen bespaard kan blijven, wegen deze kosten wel op tegen het verschil in (beperkte) effectiviteit. Fysio-/oefentherapeutische behandeling na een luxatie wordt niet volledig vergoed vanuit de basis zorgverzekering. In het samen beslissen hoe het traject vorm te geven, komen de kosten daarom ook aan bod. Deze invulling is voor iedere patiënt anders.
Gelijkheid ((health) equity/equitable)
Aangezien fysio-/oefentherapeutische sessies niet volledig worden vergoed, kan dit voor patiënten een barrière zijn om niet-operatieve behandeling (met oefentherapie) te ondergaan. Indien iemand niet over de middelen beschikt om behandeling te bekostigen, kan ook dit een barrière vormen om het traject met de gewenste intensiteit en frequentie te ondergaan.
Aanvaardbaarheid
De interventie lijkt aanvaardbaar voor de betrokkenen. Er zijn geen ethische bezwaren.
Duurzaamheid
Duurzaamheidsoverwegingen spelen geen rol bij de behandelbeslissing.
Haalbaarheid
De keuze voor oefen- of fysiotherapie wordt met de patiënt besproken in de spreekkamer van de medisch specialist. Indien er onduidelijkheid is over welke interventie het meest passend is voor de patiënt, kan een eenmalig functionele beoordeling door een in schouderklachten gespecialiseerde fysio-/oefentherapeut worden ingezet. Bij een keuze voor niet-operatieve behandeling, bepaalt de fysio-/oefentherapeut vervolgens in samenspraak met de patiënt hoe de niet-operatieve behandeling verder wordt vormgegeven. Gezien het belang van het verminderen van angst voor reluxatie, kan er in de behandeling mogelijk ook een rol weggelegd zijn voor een psycholoog.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Op basis van de resultaten uit de literatuur kan geen conclusie worden getrokken over de effectiviteit van oefentherapie bij de niet-operatieve behandeling van schouderinstabiliteit. De aanbevelingen zijn daarom gebaseerd op basis van expert opinie. Wanneer de recidiefkans laag is, kan niet-operatieve behandeling met oefentherapie worden overwogen. Mogelijk kan door de inzet hiervan een ingrijpende en duurdere schouderoperatie bespaard blijven. De behandelbeslissing dient samen met de patiënt te worden gemaakt. Wanneer er gekozen wordt voor oefentherapie bij een niet-operatieve behandeling, dient de bij aanvang de focus te liggen op neuromusculaire controle en spieruithoudingsvermogen. Gerichte oefentherapie adresseert deze principes. Daarnaast is het belangrijk om aandacht te hebben voor het verminderen van angst, indien aanwezig. Dit vraagt om een multifactoriële aanpak. Indien de angst persisteert en zorgt voor een belemmering in het hervatten van adl-, werk- of sportactiviteiten, kan er worden overwogen een interdisciplinair eerstelijns traject op te starten in samenwerking met een psycholoog. De inzet van een psycholoog kan zinvol zijn omdat angst ook andere onderliggende oorzaken kan hebben dan enkel het fysieke trauma. Een psycholoog kan helpen om dit te onderzoeken en eventueel te behandelen.
Eindoordeel:
Zwakke aanbeveling voor gerichte oefentherapie bij de niet-operatieve behandeling van (recidiverende) schouderinstabiliteit.
Onderbouwing
It is uncertain whether physiotherapy in a broad sense is effective in the treatment of recurrent anterior shoulder instability. Standard non-operative treatment involves protocol-based physiotherapy, with assessments at 6 weeks, 3 months, 6 months and 12 months, with focus on mobililty, strength and coordination. Specific physiotherapy interventions, such as neuromuscular, motor control and strength training, have demonstrated significant effect in the short term, but demonstrate hardly any clinically relevant effect. Recently literature is presenting the psychological impact after anterior shoulder instability and treatment options to incorporate within the exercise program. Fear for re-injury influences return to play and sports, which might also influence treatment outcome for exercise therapy. In this module we will systematically review the literature on the effect of exercise therapy in the conservative treatment of traumatic anterior shoulder instability, which will lead to a recommendation. This will be complemented with a broader new insight regarding conservative treatment.
Summary of Findings
What is are the (un)favorable effects of exercise therapy (including neuromuscular training) in the conservative treatment of traumatic shoulder instability?
Population: Patients with traumatic shoulder instability
Intervention: Stability training/exercise therapy (especially neuromuscular training)
Comparison: Wait and see/ conservative policy/regular exercise therapy (without supervision/one-time instruction)
Click here to see this table in a document.
|
Outcome |
Study results and measurements |
Absolute effect estimates |
Certainty of the Evidence (Quality of evidence) |
Summary |
|
|
Control |
Intervention |
||||
|
Redislocation (crucial) |
Results were not pooled
Based on data of 538 participants in 2 studies |
- |
- |
Very low Due to serious inconsistency and very serious imprecision1 |
The evidence is very uncertain about the effect of exercise therapy on redislocation when compared with other conservative policy in patients with traumatic shoulder instability.
(Eshoj 2020, Kearney 2024) |
|
|
|||||
|
PROMs (important) |
Results were not pooled
WOSI-score,Patient-Specific Functional Scale, QuickDASH, Oxford Shoulder Instability Score, UQYBT
Based on data of 563 participants in 3 studies |
On the WOSI-score, Oxford Shoulder Instability Score and UQYBT no clinically relevant difference were reported. |
Low Due to serious risk of bias and serious imprecision2 |
Exercise therapy may result in little to no difference in patient reported function when compared with other conservative policy in patients with traumatic shoulder instability.
(Eshoj 2020, Kearney 2024, Pulido 2023) |
|
|
Pain (important) |
Measured by NRS Lower is better
Based on data of 56 participants in 1 study |
Current pain and pain in the last 24 hours did not differ between groups. Pain over the last 24 hours increased more in the intervention group. |
Very low Due to extremely serious imprecision3 |
The evidence is very uncertain about the effect of exercise therapy on pain when compared with other conservative policy in patients with traumatic shoulder instability.
(Eshoj 2020) |
|
|
Range of motion (important) |
Measured by CMS Lower is better
Based on data of 56 participants in 1 study |
Mean CFB: -7.3 (95% CI -10.0 to -4.6) |
Mean CFB: -3.5 (95% CI -6.2 to -0.8) |
Very low Due to serious indirectness and very serious imprecision5 |
The evidence is very uncertain about the effect of exercise therapy on range of motion when compared with conservative policy in patients with traumatic shoulder instability.
(Eshoj 2020) |
|
Difference: 3.8 (95% CI -0.1 to 7.7) |
|||||
Abbreviations: NRS, numerical rating scale. CMS, Constant-Murley Score. CFB, change from baseline. WOSI, Western Ontario Shoulder Instability Index.
1 Inconsistency: serious. Due to conflicting results.
Imprecision: very serious. Due to low number of participants and events and overlap of both limits of the 95% confidence interval with the minimal clinically important difference.
2 Risk of bias: serious. Due to limitation in study designs.
Imprecision: serious. Due to overlap of the lower limit of the 95% confidence interval with the minimal clinically important difference.
3 Imprecision: extremely serious. Due to low number of participants in only one study and overlap of the lower limit of the 95% confidence interval with the minimal clinically important difference.
4 Risk of bias: serious. Due to limitation in study designs.
Inconsistency: serious. Due to conflicting results.
Imprecision: serious. Due to overlap of the lower limit of the 95% confidence interval with the minimal clinically important difference.
5 Indirectness: serious. Due to indirect measurement of the outcome measure.
Imprecision: very serious. Due to low number of participants in only one study.
Description of studies
A total of 3 studies reported in 4 papers were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Eshoj (2020) performed a multicenter, randomized, assessor-blind, controlled, superiority trial in three orthopedic shoulder units in Denmark. They evaluated the efficacy and safety of a nonsurgical, supervised, progressive shoulder instability neuromuscular exercise program compared with a self-managed, home-based, standard care shoulder exercise program in patients with traumatic anterior shoulder dislocation. In this study, 56 participants with radiographically verified, trauma-initiated primary or recurrent anterior shoulder dislocation and self-reported decreased shoulder function were randomized into neuromuscular exercise program (n=28) or standard care (n=28). Duration of follow-up was 12 weeks. The primary outcome was Western Ontario Shoulder Instability Index (WOSI) score. The risk of bias for this study was considered moderate for the outcome measures redislocation and range of motion as there was a low complicate rate with the exercise program. For the other outcomes measures, the risk of bias was considered high as there was no blinding.
Kearney (2024) published in two papers about a multicenter, randomized, controlled, superiority trial in 41 hospitals in the United Kingdom (both papers are referred to as Kearney 2024). They assessed the effects of a physiotherapy program in participants with a first-time traumatic shoulder dislocation compared with a single session of advice, supporting materials, and option to self-refer to physiotherapy. In this study, 482 participants with radiographically confirmed first time traumatic anterior shoulder dislocation were randomized into advice plus physiotherapy program (n=242) or advice (n=240). Duration of follow-up was six months. The primary outcome was the Oxford shoulder instability score at six months. The risk of bias for this study was considered low for the outcome measures redislocation and range of motion. For the outcome measures, the risk of bias was considered moderate as there was no blinding.
Pulido (2023) performed a randomized, controlled longitudinal trial in five community colleges in Canada. They compared three exercise protocols for shoulder rehabilitation on athletes with traumatic anterior shoulder instability. In this study, 37 participants with traumatic anterior shoulder instability were randomized into a Bodyblade protocol (n=13), a traditional training protocol (n=12) or a mixed training protocol (n=12). The latter group is not included in this summary of literature. Duration of follow-up was three months. The primary outcome was the Western Ontario Shoulder Instability Index score. The risk of bias for this study was considered high as the randomization process was not described, no funding source was reported, and no blinding was performed.
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
|
Eshoj, 2020 |
N at baseline: 56 Intervention: 28 Control: 28
Age (mean (SD)) I: 26.2 (6.4) C: 25.8 (5.8)
Sex (% male) I: 93 C: 82
First dislocation (%) I: 64 C: 67
All participants had radiographically verified, trauma-initiated primary or recurrent anterior shoulder dislocation and self-reported decreased shoulder function. |
Intervention: Neuromuscular exercises: strength, coordination, balance, and proprioception, Integrated simultaneously into various body positions, enhancing compensatory functional shoulder stability for 12 weeks 3 times weekly + daily exercises. Half of all session were supervised.
Control: Active exercises for the rotator cuff and scapular muscles using elastic bands and an exercise for mobility/coactivation of the scapular and core stability muscles for 12 weeks, 3 times weekly. Home based, at first, there was 1 supervised session. |
|
Kearney, 2024 (2 papers) |
N at baseline: 482 Intervention: 242 Control: 240
Age (mean (SD)) I: 44.7 (19) C: 45 (20)
Sex (% male) I: 66 C: 66
All participants had radiographically verified, traumatic shoulder dislocation. |
Intervention: Advice session including progressive exercises plus physiotherapy sessions for maximal 4 months to supervise the core set of exercises.
Control: Advice session including progressive exercises. |
|
Pulido, 2023 |
N at baseline: 37 Intervention: 13 Control: 12 (12 in arm not of interest)
Age (mean (SD)) I: 19.8 (1.6) C: 19.9 (2.2)
Sex (% male) I: 77 C: 58
All participants had traumatic anterior shoulder instability in the last 12 months and were student-athletes.
|
Intervention: Bodyblade exercise protocol with internal and external rotation, flexion and abduction progressively adding resistance, repetitions, or increasing time and intensity; for 8 weeks, 3 times weekly under guidance of a trainer. The Bodyblade provided verbal and tactile cues to maintain a neutral pelvis, athletic position, and shoulder retraction throughout the exercises.
Control: Traditional exercise protocol with elastic resistance band exercises for ad- and abduction, extension, and bilateral row and progressively adding resistance, repetitions, or increasing time and intensity; for 8 weeks, 3 times weekly under guidance of a trainer.
A third group had a mixed protocol of the traditional and bodyblade protocols. |
*For further details, see risk of bias table in the appendix
Abbreviations: WOSI, Western Ontario Shoulder Instability Index. QuickDASH, shortened version of the disabilities of the arm, shoulder and hand questionnaire. UQYBT, Upper Quarter Y-Balance test
Results
1. Redislocation (crucial outcome)
Two studies reported on the recurrence of a dislocation (Eshoj 2020, Kearney 2024). Due to heterogeneity in the intervention type and follow-up duration, the results were not pooled.
Eshoj (2020) reported at three months follow-up 3/28 (10.7%) patients with redislocation in the intervention group, compared to 2/28 (7.1%) in the control group. The RR was 1.50 (95% CI 0.27 to 8.30), the RD was 0.04 (95% CI: -0.11 to 0.18), see Figure 1.
Kearney (2024) reported at six months follow-up 3/242 (1.2%) patients with redislocation in intervention group compared to 7/240 (2.9%) patients in control group. The RR was 0.43 (95% CI: 0.11 to 1.62), the RD was -0.02 (95% CI: -0.04 to 0.01), see Figure 1.
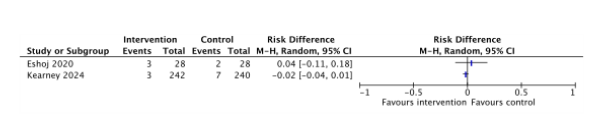

Figure 1. Forest plots of recurrent dislocation among participants with a traumatic shoulder dislocation
Risk Ratio and Risk difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; SD: standard deviation; I2; statistical heterogeneity; CI: confidence interval
2. Patient Reported Outcome Measures (important outcome)
In the included studies, various patient reported outcome measures were used (see Table 3).
Eshoj (2020) used the WOSI score, the Patient-Specific Functional Scale, and the Global Perceived Effect scale to measure function after 3 months and reported mean changes from baseline.
- The WOSI score consist of 21 items and each item results in a score ranging from 0 to 100 (total score is 2100). A higher score indicates worse shoulder-related quality of life. The mean change from baseline (at 3 months follow-up) was 655.3 (457.5 to 853.0) in the intervention group and 427.2 (245.9 to 608.6) in the control group. The difference in change from baseline was –228.1 (–430.5 to –25.6).
- The Patient-Specific Functional Scale ranges from 0 to 10 and a higher score reflects better function. The intervention group had a change from baseline of -2.5 (95% CI -3.6 to 1.4) and the control group -1.3 (95% CI -2.5 to -0.2). The difference between treatment arms in change from baseline was 1.2 (95% CI -0.3 to 2.7).
Kearney (2024) used the QuickDASH to measure function after 6 months.
- The QuickDASH ranges from 0 to 100 and a higher score means greater disability. The advice plus physiotherapy group had a score of 12.7 (SD 16.9) and the advice group had a score of 14.4 (SD 17.5), which was reported to not be statistically significantly different. The mean difference was -1.70 (95 CI -4.77 to 1.37).
- Kearney (2024) used the Oxford Shoulder instability score. The scores ranges from 0 to 48 and a higher score reflects better function. The score was 38.4 (SD 9.2) in the advice plus physiotherapy group and 36.2 (SD 10.7) in the advice group, which was reported to not be statistically significantly different. The mean difference was 2.20 (95% CI 0.42 to 3.98).
Pulido (2023) used the WOSI-score and Upper Quarter Y-Balance after 3 months.
- The WOSI score consist of 21 items and each item results in a score ranging from 0 to 100 (total score is 2100). Pulido (2023) converted the score to a 0-100 scale, with a higher score indicates a worse status. The score was 16.4 (SD 17.3) in the Bodyblade group and 13.4 (SD 17.3) in the traditional exercise group. The mean difference was 3.00 (95% CI -10.57 to 16.57).
- The UQYBT composite score identify upper extremity and trunk mobility in the reaching limb’s open kinetic chain as well as midrange limitations, asymmetries, core stability in the closed kinetic chain on the stabilizing limb. Each direction’s maximum score was extracted to represent the end range of performance; thus a higher score is better. Ranges of normal values were not reported. The Bodyblade group had a score of 95.8 (SD 9.7) and the traditional exercise group 91.0 (SD 14.9), this was reported to not be statistically significantly different. The mean difference was 4.80 (95% CI -5.14 to 14.74).
Table 3. overview of the results on PROMs reported in the included studies
|
Study |
Measure |
Results |
|||
|
|
|
Intervention |
Control |
Difference |
In favour of |
|
Eshoj, 2020 |
WOSI score; shoulder-related quality of life total score (0-2100; higher score = worse = status) |
CFB: 655.3 (457.5 to 853.0)
|
CFB: 427.2 (245.9 to 608.6)
|
CFB: –228.1 (–430.5 to –25.6)
|
Intervention group, not clinically relevant |
|
Patient-Specific Functional Scale; Function (0-10; higher score = worse status |
CFB: -2.5 (95% CI -3.6 to 1.4) |
CFB: -1.3 (95% CI -2.5 to -0.2) |
CFB: 1.2 (95% CI -0.3 to 2.7) |
Control group, Clinically relevant |
|
|
Kearney, 2024 |
QuickDASH; function (0-100; higher score = greater disability) |
12.7 (SD 16.9) |
14.4 (SD 17.5) |
-1.70 (95 CI -4.77 to 1.37) |
Intervention group, not clinically relevant |
|
|
Oxford Shoulder Instability score; function (0-48, higher score = better function) |
38.4 (SD 9.2) |
36.2 (SD 10.7) |
2.20 (95% CI 0.42 to 3.98). |
Intervention group, not clinically relevant |
|
Pulido, 2023 |
WOSI-score; quality of life (0-100; higher score = more complaints) |
16.4 (SD 17.3)
|
13.4 (SD 19.3)
|
3.00 (95% CI -10.57 to 16.57). |
Control group not clinically relevant |
|
|
Upper Quarter Y-Balance test; |
95.8 (SD 9.7) |
91.0 (SD 14.9) |
4.80 (95% CI -5.14 to 14.74) |
Intervention group, not clinically relevant |
CFB = change from baseline; SD = standard deviation; 95% CI = 95% confidence interval
3. Pain (important outcome)
One study reported on pain (Eshoj 2020). The Numeric Pain Rating Scale (NRS) was used to measure pain intensity now, in the past 24 hours and the previous seven days. The scale ranges from 0 to 10 and a higher score indicates more pain.
- Current pain intensity had a 0.5 (95% CI -1.4 to 0.5) difference between treatment arms which was reported to not be statistically significantly different. This result is not considered clinically relevant.
- The mean pain in the last 24 hours had a difference between groups of -0.4 (95% CI -1.5 to 0.6) which was reported to not be statistically significantly different. This result is not considered clinically relevant.
- The mean pain in the last seven days had a difference between groups of -1.1 (95% CI -2.1 to -0.9) with more increase in pain in the neuromuscular exercise group which was reported to be statistically significantly different. This result is considered clinically relevant.
4. Range of motion (important outcome)
Range of motion was reported by Eshoj (2020). The Constant-Murley score was used to measure range of motion, in this score a lower score indicates better status and scores can range from 0 to 100. The neuromuscular exercise group had a mean change from baseline of -7.3 (95% CI -10.0 to -4.6) and the traditional exercise group -3.5 (95% CI -6.2 to -0.8). The difference between groups was 3.8 (95% CI -0.1 to 7.7) in favor of the neuromuscular exercise group. This change from baseline is not considered clinically relevant.
A systematic review of the literature was performed to answer the following question:
What is are the (un)favorable effects of exercise therapy (including neuromuscular training) in the conservative treatment of traumatic shoulder instability?
Table 1. PICO
| Patients | Patients with traumatic shoulder instability |
| Intervention | Stability training/exercise therapy (especially neuromuscular training) |
| Control | Wait and see/conservative policy/regular exercise therapy (without supervision/one-time instruction) |
| Outcomes | Redislocation, patient reported outcome measures (PROMs, a.o. WOSI-score, Oxford Shoulder Instability Score, QuickDash), pain, range of motion |
| Other selection criteria |
Study design: systematic reviews and randomized controlled trials. From 2000 |
Relevant outcome measures
The guideline panel considered redislocation, as a critical outcome measure for decision making; and PROMS and range of motion as an important outcome measure for decision making.
If a study reported more than two PROMs, the two PROMs that the guideline development panel considered most relevant, were selected for the summary of literature.
The guideline development panel defined the following thresholds as a minimal clinically (patient) important difference:
- For dichotomous outcomes (redislocation), a relative risk of <0.80 and >1.25 was considered as a minimal clinically (patient) important difference.
- For continuous outcomes (PROMs, pain, and range of motion), a difference of 10% for the PROM WOSI-score, a difference of 250 points (on a 2100-point scale) was considered clinically relevant (Eshoj, 2020).
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until the 26th of August 2024. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 675 hits. Studies were selected based on the PICO criteria. 24 studies were initially selected based on title and abstract screening. After reading the full text, 20 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and 4 papers were included that described 3 studies.
- Brindisino, F., et al. (2023). "Shoulder proprioception and motor control: Implications for rehabilitation of shoulder instability." Journal of Shoulder and Elbow Surgery, 32(3), 506-515. DOI: 10.1016/j.jse.2023.01.009.
- Eshoj H, Rasmussen S, Frich LH, Jensen SL, Søgaard K, Juul-Kristensen B. Patients with non-operated traumatic primary or recurrent anterior shoulder dislocation have equally poor self-reported and measured shoulder function: a cross-sectional study. BMC Musculoskelet Disord. 2019 Feb 8;20(1):59. doi: 10.1186/s12891-019-2444-0. PMID: 30736761; PMCID: PMC6368725.
- Eshoj HR, Rasmussen S, Frich LH, Hvass I, Christensen R, Boyle E, Jensen SL, Søndergaard J, Søgaard K, Juul-Kristensen B. Neuromuscular Exercises Improve Shoulder Function More Than Standard Care Exercises in Patients With a Traumatic Anterior Shoulder Dislocation: A Randomized Controlled Trial. Orthop J Sports Med. 2020 Jan 30;8(1):2325967119896102. doi: 10.1177/2325967119896102. PMID: 32064291; PMCID: PMC6993151.
- Jan J, Benkalfate T, Rochcongar P. The impact of recurrent dislocation on shoulder rotator muscle balance (a prospective study of 102 male patients). Ann Phys Rehabil Med. 2012 Sep;55(6):404-14. doi: 10.1016/j.rehab.2012.05.004. Epub 2012 Jun 20. PMID: 22835451.
- Kearney R, Ellard D, Parsons H, Haque A, Mason J, Nwankwo H, Bradley H, Drew S, Modi C, Bush H, Torgerson D, Underwood M; ARTISAN collaborators. Advice only versus advice and a physiotherapy programme for acute traumatic anterior shoulder dislocation: the ARTISAN RCT. Health Technol Assess. 2024 Apr;28(22):1-94. doi: 10.3310/CMYW9226. PMID: 38695098; PMCID: PMC11089447.
- Kearney RS, Ellard DR, Parsons H, Haque A, Mason J, Nwankwo H, Bradley H, Drew S, Modi C, Bush H, Torgerson D, Underwood M; The ARTISAN collaborators; ARTISAN collaborators. Acute rehabilitation following traumatic anterior shoulder dislocation (ARTISAN): pragmatic, multicentre, randomised controlled trial. BMJ. 2024 Jan 17;384:e076925. doi: 10.1136/bmj-2023-076925. Erratum in: BMJ. 2024 Mar 15;384:q662. doi: 10.1136/bmj.q662. PMID: 38233068; PMCID: PMC10792684.
- Marans HJJ, Angel KRR, Schemitsch EHH, Wedge JHH. The fate of traumatic anterior dislocation of the shoulder in children. J Bone Joint Surg Am 1992;74:-4. doi: 10.2106/00004623-199274080-00015 pmid: 1400553.
- Olds M, Ellis R, Parmar P, Kersten P. Who will redislocate his/her shoulder? Predicting recurrent instability following a first traumatic anterior shoulder dislocation. Br Med J Open Sport Exerc 2019;5:e000447.
- Olds M, Ellis R, Parmar P, Kersten P. The immediate and subsequent impact of a first-time traumatic anterior shoulder dislocation in people aged 16-40: results from a national cohort study. Shoulder Elb 2021;13:-232. doi: 10.1177/1758573220921484. pmid: 33897854.
- Pulido V, Alvar B, Behm D. Bodyblade™ Training in Athletes with Traumatic Anterior Shoulder Instability. Int J Sports Phys Ther. 2023 Feb 1;18(1):188-198. doi: 10.26603/001c.65900. PMID: 36793570; PMCID: PMC9897004.
- Robinson CM, Howes J, Murdoch H, Will E, Graham C. Functional outcome and risk of recurrent instability after primary traumatic anterior shoulder dislocation in young patients. J Bone Joint Surg Am 2006;88:-36. doi: 10.2106/JBJS.E.01327 pmid: 17079387.
- Tokish JM, Thigpen CA, Kissenberth MJ, Tolan SJ, Lonergan KT, Tokish JM Jr, Dickens JF, Hawkins RJ, Shanley E. The Nonoperative Instability Severity Index Score (NISIS): A Simple Tool to Guide Operative Versus Nonoperative Treatment of the Unstable Shoulder. Sports Health. 2020 Nov/Dec;12(6):598-602. doi: 10.1177/1941738120925738. Epub 2020 Jul 1. PMID: 32609577; PMCID: PMC7785891.
- Woo-Sung Do, et al. (2023). "Negative Apprehension Test and Recidivism of Shoulder Instability: A Clinical Case Study." Journal of Shoulder and Elbow Surgery, 32(7), 1505-1513.
- Ariane Schwank, Paul Blazey, Martin Asker, Merete Møller, Martin Hägglund, Suzanne Gard, Christopher Skazalski, Stig Haugsbø Andersson, Ian Horsley, Rod Whiteley, Ann M Cools, Mario Bizzini, Clare L Ardern. Bern Consensus Statement on Shoulder Injury Prevention, Rehabilitation, and Return to Sport for Athletes at All Participation Levels J Orthop Sports Phys Ther. 2022 Jan;52(1):11-28. doi: 10.2519/jospt.2022.10952.
- Kun-Yu Chou Wan-Ling Wu Chun-Wen Chiu Shih-Chung Cheng , Hsiao-Yun Chang Adaptation Characteristics in the Range of Motion of the Shoulder Among Young Male Volleyball Players. J Funct Morphol Kinesiol. 2025 Feb 15;10(1):67 doi: 10.3390/jfmk10010067.
Risk of bias table for intervention studies (randomized controlled trials; based on Cochrane risk of bias tool and suggestions by the CLARITY Group at McMaster University)
|
Study reference |
Was the allocation sequence adequately generated? |
Was the allocation adequately concealed? |
Blinding: |
Was loss to follow-up (missing outcome data) infrequent? |
Are reports of the study free of selective outcome reporting? |
Was the study apparently free of other problems that could put it at a risk of bias? |
Overall risk of bias |
|
Eshoj, 2020 |
Definitely yes
Reason: Authors used computer-generated randomization. |
Definitely yes
Reason: List with randomization was sequentially numbered in opaque, concealed envelopes. |
Definitely no
Reason: Blinding of outcomes assessors, not of participants. |
Definitely yes
Reason: 6 of 28 lost to follow-up in intervention arm and 2 of 28 in control arm. |
Definitely yes
Reason: The study was performed according to the published protocol. |
Probably no
Reason: No conflict of interest, registered trial, no funding source reported. Compliance rate was 43% and 54%. |
High risk of bias
Reason: No blinding (not possible), low compliance rate.
|
|
Kearney, 2024 |
Definitely yes
Reason: Authors used a secured web-based system. |
Definitely yes
Reason: by an independent team that had no role in recruitment. |
Definitely no
Reason: Blinding of outcomes assessors, and of participants until after the advice session. |
Definitely yes
Reason: 27% was loss to follow-up (n=75 and 63). |
Definitely yes
Reason: The study was performed according to the published protocol. |
Probably yes
Reason: Registered trial. The funder had no role in any part of the study. Completing interest are described. Complicate rate was 69% and 81%. |
Some concerns
Reason: No blinding (not possible). |
|
Pulido, 2023 |
Probably yes
Reason: Authors used ‘controlled randomization’, no further information provided. |
Probably no
Reason: No information provided. |
Definitely no
Reason: Blinding of outcomes assessors, not of participants. |
Definitely no
Reason: 1 missing due to shoulder surgery (in mixed group). |
Probably yes
Reason: Outcomes measured reported in the Methods are reported in the Results section. |
Reason: No conflict of interest, no funding source reported, but there is a high suspicion of sponsoring. Complicate rate was 97.3%. |
High risk of bias
Reason: Unclear randomization, no blinding (not possible). |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Ager AL, Borms D, Bernaert M, Brusselle V, Claessens M, Roy JS, Cools A. Can a Conservative Rehabilitation Strategy Improve Shoulder Proprioception? A Systematic Review. J Sport Rehabil. 2020 Jul 31;30(1):136-151. doi: 10.1123/jsr.2019-0400. PMID: 32736342. |
Wrong population and wrong outcome. |
|
Avila Lafuente JL, Moros Marco S, García Pequerul JM. Controversies in the Management of the First Time Shoulder Dislocation. Open Orthop J. 2017 Aug 31;11:1001-1010. doi: 10.2174/1874325001711011001. PMID: 29430264; PMCID: PMC5789581. |
Wrong design: review, not systematic. |
|
Bateman M, Osborne S, Smith B. Physiotherapy treatment for atraumatic recurrent shoulder instability: updated results of the Derby Shoulder Instability Rehabilitation Programme. J Arthrosc Jt Surg 2019;6:35–41. doi: 10.1016/j.jajs.2019.01.002 |
Wrong population: patients with atraumatic shoulder instability. |
|
Buss DD, Lynch GP, Meyer CP, Huber SM, Freehill MQ. Nonoperative management for in-season athletes with anterior shoulder instability. Am J Sports Med. 2004 Sep;32(6):1430-3. doi: 10.1177/0363546503262069. Epub 2004 Jul 20. Erratum in: Am J Sports Med. 2004 Oct-Nov;32(7):1780. PMID: 15310567. |
No comparison, descriptive study. |
|
Coyle M, Jaggi A, Weatherburn L, DanielI H, Chester R. Post-operative rehabilitation following traumatic anterior shoulder dislocation: A systematic scoping review. Shoulder Elbow. 2023 Oct;15(5):554-565. doi: 10.1177/17585732221089636. Epub 2022 Mar 31. PMID: 37811389; PMCID: PMC10557935. |
No intervention and comparison defined, wrong design: scoping review. |
|
Donohue MA, Brelin AM, LeClere LE. Management of First-Time Shoulder Dislocation in the Contact Athlete. Operative Techniques in Sports Medicine. 2016; Aug. DOI: 10.1053/j.otsm.2016.09.001 |
No intervention and comparison defined, wrong desig. |
|
Eljabu W, Klinger HM, von Knoch M. The natural course of shoulder instability and treatment trends: a systematic review. J Orthop Traumatol. 2017 Mar;18(1):1-8. doi: 10.1007/s10195-016-0424-9. Epub 2016 Aug 17. PMID: 27535060; PMCID: PMC5311001. |
No intervention and comparison, wrong outcome. |
|
Eshoj H, Rasmussen S, Frich LH, Hvass I, Christensen R, Jensen SL, Søndergaard J, Søgaard K, Juul-Kristensen B. A neuromuscular exercise programme versus standard care for patients with traumatic anterior shoulder instability: study protocol for a randomised controlled trial (the SINEX study). Trials. 2017 Feb 28;18(1):90. doi: 10.1186/s13063-017-1830-x. PMID: 28245853; PMCID: PMC5331774. |
wrong design: study protocol. |
|
Gibson K, Growse A, Korda L, Wray E, MacDermid JC. The effectiveness of rehabilitation for nonoperative management of shoulder instability: a systematic review. J Hand Ther. 2004 Apr-Jun;17(2):229-42. doi: 10.1197/j.jht.2004.02.010. PMID: 15162108. |
No/wrong comparisons made. |
|
Griffin J, Jaggi A, Daniell H, Chester R. A systematic review to compare physiotherapy treatment programmes for atraumatic shoulder instability. Shoulder Elbow. 2023 Aug;15(4):448-460. doi: 10.1177/17585732221080730. Epub 2022 Feb 18. PMID: 37538527; PMCID: PMC10395403. |
Wrong design and population: scoping review. |
|
Hagesæter AN, Løvold T, Juul-Kristensen B, Blomquist J, Hole R, Eshoj H, Magnussen LH. Feasibility of the SINEX program for patients with traumatic anterior shoulder instability. Pilot Feasibility Stud. 2020 Oct 6;6:148. doi: 10.1186/s40814-020-00679-x. PMID: 33042568; PMCID: PMC7541274. |
No comparison, wrong outcome. |
|
Hanchard NC, Goodchild LM, Kottam L. Conservative management following closed reduction of traumatic anterior dislocation of the shoulder. Cochrane Database Syst Rev. 2014 Apr 30;(4):CD004962. doi: 10.1002/14651858.CD004962.pub3. Update in: Cochrane Database Syst Rev. 2019 May 10;5:CD004962. doi: 10.1002/14651858.CD004962.pub4. PMID: 24782346. |
Cochrane update, but not the most recent Cochrane. Also does Cochrane regard the wrong intervention. |
|
Handoll HH, Hanchard NC, Goodchild L, Feary J. Conservative management following closed reduction of traumatic anterior dislocation of the shoulder. Cochrane Database Syst Rev. 2006 Jan 25;(1):CD004962. doi: 10.1002/14651858.CD004962.pub2. Update in: Cochrane Database Syst Rev. 2014 Apr 30;(4):CD004962. doi: 10.1002/14651858.CD004962.pub3. PMID: 16437506. |
Not the most recent Cochrane. |
|
Kavaja L, Lähdeoja T, Malmivaara A, Paavola M. Treatment after traumatic shoulder dislocation: a systematic review with a network meta-analysis. Br J Sports Med. 2018 Dec;52(23):1498-1506. doi: 10.1136/bjsports-2017-098539. Epub 2018 Jun 23. PMID: 29936432; PMCID: PMC6241619. |
Meets PICO, but only one study meets our PICO. |
|
Kearney RS, Dhanjal G, Parsons N, Ellard D, Parsons H, Haque A, Karasouli E, Mason J, Nwankwo H, Brown J, Liew Z, Drew S, Modi C, Bush H, Torgerson D, Underwood M. Acute Rehabilitation following Traumatic anterior shoulder dISlocAtioN (ARTISAN): protocol for a multicentre randomised controlled trial. BMJ Open. 2020 Nov 19;10(11):e040623. doi: 10.1136/bmjopen-2020-040623. PMID: 33444204; PMCID: PMC7678365. |
Wrong design: study protocol. |
|
Lafrance S, Ouellet P, Alaoui R, Roy JS, Lewis J, Christiansen DH, Dubois B, Langevin P, Desmeules F. Motor Control Exercises Compared to Strengthening Exercises for Upper- and Lower-Extremity Musculoskeletal Disorders: A Systematic Review With Meta-Analyses of Randomized Controlled Trials. Phys Ther. 2021 Jul 1;101(7):pzab072. doi: 10.1093/ptj/pzab072. PMID: 33609357. |
Meets PICO, but only one study meets our PICO. |
|
Liew Z, Mazuquin B, Ellard DR, Karasouli E, Drew S, Modi C, Bush H, Underwood M, Kearney RS. Development of a single-session physiotherapy and self-management intervention for the treatment of primary traumatic anterior shoulder dislocation for the 'Acute Rehabilitation following Traumatic anterior shoulder dISlocAtioN (ARTISAN)' multi centre RCT. Physiotherapy. 2021 Dec;113:80-87. doi: 10.1016/j.physio.2021.06.002. Epub 2021 Jun 17. PMID: 34607077; PMCID: PMC8612274. |
Wrong design. |
|
Olds M, Ellis R, Donaldson K, Parmar P, Kersten P. Risk factors which predispose first-time traumatic anterior shoulder dislocations to recurrent instability in adults: a systematic review and meta-analysis. Br J Sports Med. 2015 Jul;49(14):913-22. doi: 10.1136/bjsports-2014-094342. Epub 2015 Apr 21. PMID: 25900943; PMCID: PMC4687692. |
No intervention and comparison. |
|
Stokes DJ, McCarthy TP, Frank RM. Physical Therapy for the Treatment of Shoulder Instability. Phys Med Rehabil Clin N Am. 2023 May;34(2):393-408. doi: 10.1016/j.pmr.2022.12.006. Epub 2023 Feb 26. PMID: 37003660. |
Wrong design. |
|
Struyf F, Cagnie B, Cools A, Baert I, Brempt JV, Struyf P, Meeus M. Scapulothoracic muscle activity and recruitment timing in patients with shoulder impingement symptoms and glenohumeral instability. J Electromyogr Kinesiol. 2014 Apr;24(2):277-84. doi: 10.1016/j.jelekin.2013.12.002. Epub 2013 Dec 18. PMID: 24389333. |
No intervention and comparison. |
Beoordelingsdatum en geldigheid
Publicatiedatum : 17-02-2026
Beoordeeld op geldigheid : 17-02-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodules is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met schouderinstabiliteit.
Werkgroep richtlijn schouderinstabiliteit
- Prof. Dr. M.P.J (Michel) Bekerom, orthopedisch chirurg OLVG en MC Jan van Gooijen, NOV – voorzitter richtlijnwerkgroep
- Dr. J.J.A.M. (Jos) van Raaij, orthopedisch chirurg, niet praktiserend, NOV
- Dr. O.A.J. (Olivier) van der Meijden, orthopedisch chirurg Albert Schweitzer Ziekenhuis, NOV
- Dr. A.R. (Alex) Poublon, orthopedisch chirurg Ziekenhuis Gelderse Vallei, NOV
- Dr. T.D.W. (Tjarco) Alta, orthopedisch chirurg Spaarne Gasthuis, NOV
- Dr. R.J. (Robert Jan) Derksen, traumachirurg, Zaans Medisch Centrum, NVvH
- MSc. F. (Femke) Boon, fysio-, manueel therapeut, extended scope specialist Schoudercentrum IBC, KNGF
- MSc. K.M.C. (Karin) Hekman, fysio-, manueel therapeut, extended scope specialist, Schoudercentrum IBC, KNGF
- Dr. I.D. (Iris) Kilsdonk, radioloog Deventer Ziekenhuis, NVvR
- Dr. H.J. (Henk-Jan) van der Woude, radioloog OLVG, NVvR
- Drs. H.K. (Rik) van der Kolk, sportarts OLVG, VSG
- Mevr. drs. G. (Gerardine) Willemsen-de Mey, patiëntvertegenwoordiger Nationale Vereniging ReumaZorg Nederland
Met ondersteuning van
- Dr. J. (Jacqueline) Jennen, adviseur Kennisinstituut van de Federatie Medisch Specialisten (tot december 2023)
- Dr. F. (Floor) Willeboordse, senior adviseur Kennisinstituut van de Federatie Medisch Speciaisten (tot januari 2025)
- Dr. M.S. (Matthijs) Ruiter, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten (vanaf januari 2025)
- MSc. D.G. (Dian) Ossendrijver, adviseur kennisinstituut van de Federatie Medisch Specialisten (vanaf december 2023)
- Dr. M. (Michiel) Oerbekke, adviseur Kennisinstituut van de Federatie Medisch Specialisten
- Dr. J. (Jing) de Haan-Du, adviseur Kennisinstituut van de Federatie Medisch Specialisten
- E. (Esther) van Bijl, medisch informatiespecialist, kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Gemelde (neven)functies en belangen werkgroep
|
Naam |
Hoofdfunctie |
Neven werkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Datum |
Restrictie |
|
Michel van den Bekerom (voorzitter) |
Orthopedisch chirurg, OLVG, Amsterdam |
Betaald onderwijs geven bij/voor: |
Geen |
Geen |
Onderzoek gesteund door: SECEC (European Society for surgery of the shoulder an the elbow), ZonMW, SNN (Smith and Nephew). Het OLVG ontvangt financiële support voor een shoulder and elbow clinical and research fellowship van van Smith en Nephew. Dit fellowship wordt mede (financieel) ondersteund door een firma die materiaal maakt dat gebruikt wordt voor schouderstabilisaties. Het betreft een overeenkomst tussen het OLVG en de firma vanwege educatieve doeleinden. |
Geen |
Het OLVG is voornemens om een consultancy contract met zimmer/biomet op te stellen zodat ik op vraag elders kan opereren. |
19-10-2022 |
Geen restricties
|
|
Jos van Raaij |
Orthopedisch chirurg, Martini ziekenhuis Groningen |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
11-07-2022 |
Geen restricties |
|
Olivier van der Meijden |
Orthopedisch chirurg |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
28-09-2023 |
Geen restricties |
|
Alexander Poublon |
Orthopedisch chirurg met aandachtsgebied schouder |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
06-10-2023 |
Geen restricties |
|
Tjarco Alta |
Orthopedisch Chirurg |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
28-09-2023 |
Geen restricties |
|
Karin Hekman |
Fysiotherapeut bij Schoudercentrum IBC |
Voorzitter Schoudernetwerk Nederland; onkostenvergoeding |
Ik behandel patiënten die schouderinstabiliteit hebben binnen het schoudercentrum en binnen MC Jan van Goyen, dit is de reden voor het plaatsnemen in deze expertise groep. |
Geen |
Geen |
Het enige voordeel dat deelname aan deze richtlijn oplevert is nog meer persoonlijke expertise wat mogelijk leidt tot een verdieping van de fysiotherapeutische toepassingen bij schouderinstabiliteit. Dit is voor het SchouderNetwerk Nederland van primair belang en kan leiden tot uitdragen van kennis naar de regionale netwerken. Als voorzitter van deze stichting voel ik mij hier verantwoordelijk voor. |
Geen |
09-10-2023 |
Geen restricties |
|
Femke Boon |
Fysio- manueel therapeut en Extended Scope specialist bij Schoudercentrum IBC locatie Amstelland |
- 2x/ maand elleboog-schouder orthopedie poli bij Medisch Centrum Jan van Goyen (betaald, gedetacheerd vanuit IBC) |
Werkzaam bij Schoudercentrum IBC Amstelland |
Geen |
Richtlijn ontwikkeling FMS primaire anterieure schouderluxaties |
Geen |
Geen |
4-10-2023 |
Geen restricties |
|
Iris Kilsdonk |
Deventer Ziekenhuis |
Bestuurslid NVvR, sectie muskuloskeletale radiologie |
Geen |
Geen |
Geen |
Geen |
Geen |
2-10-2023 |
Geen restricties |
|
Robert Jan Derksen |
Traumachirurg Zaans Medisch Centrum |
Bestuurslid NVT |
Geen |
Geen |
Geen |
Geen |
Geen |
28-08-2022 |
Geen restricties |
|
Rik van der Kolk |
Sportarts, OLVG |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
10-08-2022 |
Geen restricties |
|
Henk-Jan van der Woude |
Radioloog Onze Lieve Vrouwe Gasthuis Amsterdam |
Consulent Commissie voor Beentumoren, onbezoldigd |
Geen |
Geen |
Geen |
Geen |
Geen |
07-02-2023 |
Geen restricties |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland en de Nationale Vereniging ReumaZorg Nederland voor de knelpunteninventarisatie. Daarnaast nam een patiëntvertegenwoordiger van ReumaZorg Nederland deel aan de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan Patiëntenfederatie Nederland en ReumaZorg Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Niet-operatieve behandeling |
Geen financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5.000 patiënten) en zal daarom naar verwachting geen substantiële financiële gevolgen hebben voor de collectieve uitgaven.
|
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling van deze richtlijn is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Schouderinstabiliteit - Module 3 en 5.2 Conservatieve behandeling |
|
|
Uitgangsvraag/modules:
|
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 26 augustus 2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
Rayyan review: https://rayyan.ai/reviews/1134284 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl:9777/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen schouderinstabiliteit EN (oefentherapie OF conservatieve therapie).
De sleutelartikelen worden gevonden met deze search. |
|
|
Te gebruiken voor richtlijntekst: In de databases Embase.com en Ovid/Medline is op 26 augustus 2024 systematisch gezocht naar systematische reviews en RCTs over de plaats van oefentherapie/ conservatieve therapie bij patiënten met schouderinstabiliteit. De literatuurzoekactie leverde 675 unieke treffers op. |
|
Zoekopbrengst - 28 augustus 2024
|
SR |
159 |
128 |
201 |
|
RCT |
377 |
230 |
474 |
|
Observationele studies |
827 |
578 |
|
|
Totaal |
536 |
358 |
675* |
*in Rayyan
Zoekstrategie - 26 augustus 2024
Embase.com
|
No. |
Query |
Results |
|
#1 |
'shoulder dislocation'/exp OR 'recurrent shoulder dislocation'/exp OR ('shoulder'/exp AND ('dislocation'/de OR 'recurrent dislocation'/exp OR 'subluxation'/exp OR 'joint dislocation'/exp OR 'bone erosion'/exp OR 'joint instability'/de)) OR ((('shoulder*' OR 'gleno-humeral*' OR 'humer*' OR 'scapulohumer*') NEAR/3 ('dislocat*' OR 'diastasis' OR 'instabil*' OR 'luxat*' OR 'subluxat*')):ti,ab,kw) OR ('shoulder*':ti,ab,kw AND (('bon*' NEAR/3 ('resorption' OR 'loss' OR 'erosion*')):ti,ab,kw)) OR 'bankart lesion'/exp OR (('bankart' NEAR/3 ('fracture*' OR 'lesion*' OR 'tear*')):ti,ab,kw) OR (('hill-sachs' NEAR/3 'lesion*'):ti,ab,kw) OR ((('on track' OR 'off track') NEAR/6 ('hill sachs' OR 'bone loss' OR 'shoulder*' OR 'lesion*')):ti,ab,kw) |
19245 |
|
#2 |
'physiotherapy'/exp OR 'kinesiotherapy'/exp OR 'occupational therapy'/exp OR 'exercise'/exp OR 'proprioception'/exp OR 'proprioceptive exercise'/exp OR 'rehabilitation'/exp OR 'neuromuscular exercise'/exp OR 'motor control exercise'/exp OR 'apprehension'/exp OR (((kinaesthetic OR kinesio* OR kinesthetic OR kinetic* OR 'rotator cuff') NEAR/3 (discrimination* OR perception* OR perceptual)):ti,ab,kw) OR (((neuromuscular OR resistance OR strength OR 'motor control' OR coordination OR stability) NEAR/3 (exercise* OR training*)):ti,ab,kw) OR 'proprioception*':ti,ab,kw OR physiotherap*:ti,ab,kw OR 'physio therap*':ti,ab,kw OR 'physical therap*':ti,ab,kw OR kinesiotherap*:ti,ab,kw OR kinesitherapeutic*:ti,ab,kw OR 'occupation* therap*':ti,ab,kw OR ergotherap*:ti,ab,kw OR rehabilit*:ti,ab,kw OR revalidat*:ti,ab,kw OR 'kinetic chain*':ti,ab,kw OR propriocepsis:ti,ab,kw OR proprioceptive*:ti,ab,kw OR 'apprehension':ti,ab,kw OR 'postoperative management':ti,ab,kw |
1303348 |
|
#3 |
#1 AND #2 |
3595 |
|
#4 |
#3 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
2640 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1056009 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4094350 |
|
#7 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8376239 |
|
#8 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
15339755 |
|
#9 |
#4 AND #5 - SR |
159 |
|
#10 |
#4 AND #6 NOT #9 - RCT |
377 |
|
#11 |
#4 AND (#7 OR #8) NOT (#9 OR #10) - Observationeel |
827 |
|
#12 |
#9 OR #10 OR #11 - Totaal |
536 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Shoulder Dislocation/ or exp Bankart Lesions/ or ((shoulder* or gleno-humer* or glenoid* or humer* or scapulohumer* or glenohumer*) adj3 (dislocat* or diastasis or instabil* or luxat* or subluxat* or defect*)).ti,ab,kf. or ((shoulder* or glenoid* or gleno-humer* or humer* or scapulohumer* or glenohumer*) and (bon* adj3 (loss* or erosion*))).ti,ab,kf. or ((bankart or hill-sachs) adj3 (fracture* or lesion* or tear*)).ti,ab,kf. or ((on track or off track) adj3 (hill sachs or bone loss* or shoulder* or lesion*)).ti,ab,kf. |
14152 |
|
2 |
exp Conservative Treatment/ or exp Physical Therapy Modalities/ or exp Occupational Therapy/ or exp Exercise/ or exp Exercise Therapy/ or exp Rehabilitation/ or ((kinaesthetic or kinesio* or kinesthetic or kinetic* or rotator cuff) adj3 (discrimination* or perception* or perceptual)).ti,ab,kf. or ((neuromuscular or resistance or strength or motor control or coordination or stability) adj3 (exercise* or training*)).ti,ab,kf. or proprioception*.ti,ab,kf. or physiotherap*.ti,ab,kf. or physio therap*.ti,ab,kf. or physical therap*.ti,ab,kf. or kinesiotherap*.ti,ab,kf. or kinesitherapeutic*.ti,ab,kf. or occupation* therap*.ti,ab,kf. or ergotherap*.ti,ab,kf. or rehabilit*.ti,ab,kf. or revalidat*.ti,ab,kf. or kinetic chain*.ti,ab,kf. or propriocepsis.ti,ab,kf. or proprioceptive*.ti,ab,kf. or apprehension.ti,ab,kf. or postoperative management.ti,ab,kf. |
831252 |
|
3 |
1 and 2 |
2172 |
|
4 |
limit 3 to yr="2000 -Current" |
1662 |
|
5 |
4 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
1606 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
769650 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2768340 |
|
8 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4809539 |
|
9 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5768007 |
|
10 |
5 and 6 - SR |
128 |
|
11 |
(5 and 7) not 10 - RCT |
230 |
|
12 |
(5 and (8 or 9)) not (10 or 11) - Observationeel |
578 |
|
13 |
10 or 11 or 12 - Totaal |
358 |