Varicocèle
Uitgangsvraag
Wat is de rol van de behandeling van een varicocèle bij mannen met subfertiliteit?
Aanbeveling
Aanbeveling-1
Overweeg het (chirurgisch of radiologisch) behandelen van een vacicocèle indien er sprake is van de drie volgende criteria, hoewel het effect op verbetering van kwaliteit van het semen en dientengevolge de kans op zwangerschap onzeker is.
- Een klinische aanwezige vacicocèle.
- Afwijkende concentratie/totaal aantal zaadcellen en/of motiliteit. (Geïsoleerde teratozoospermie is geen indicatie voor vacicocèle behandeling ter verbetering van de kwaliteit van het semen).
- Subfertiliteit, waarbij een eventuele fertiliteitsbeperkende oorzaak bij de vrouw niet- of slechts beperkt bijdraagt
Aanbeveling-2
Counsel de patiënt waarbij de mogelijkheid om een klinisch aanwezige vacicocèle te behandelen wordt afgezet tegen:
- De aanwezigheid van klachten van de vacicocèle.
- De zeer lage kans op bijwerkingen en complicaties van chirurgische of radiologische behandeling.
- Het mogelijke positieve effect op de kwaliteit van het semen.
- De onzekerheid of dit bijdraagt aan de kans op zwangerschap.
Neem in deze afweging eveneens mee, de eventuele aanwezige fertiliteit belemmerende oorzaken van de vrouwelijke partner.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
De werkgroep verwijst naar module Lichamelijk onderzoek voor de diagnose van een klinische varicocele. Geconcludeerd kan worden dat door chirurgische of radiologische behandeling van een klinisch aanwezige vacicocèle slechts een geringe, niet significante, verbetering optreedt van de verschillende parameters van de kwaliteit van het semen (concentratie, motiliteit en morfologie). Er is sprake van een zeer lage bewijskracht, waarbij tevens moet worden opgemerkt dat niet vastgelegd is wat een klinisch relevant verschil zou zijn voor de drie verschillende parameters van semen kwaliteit.
Aangezien kwaliteit van het semen in de gezonde populatie zeer wisselend kan zijn, zijn herhaalde metingen geïndiceerd en zou in geval van een fertiliteitsstoornis een verandering in ART behandelmodaliteit klinische consequenties kunnen hebben. Verbetering in concentratie van een zeer ernstige ICSI met slechts enkele spermatozoa naar een eenvoudig uit te voeren ICSI met een miljoen spermatozoa, of van ICSI geschikt semen naar kwaliteit geschikt voor IUI, kan zeker een positieve consequentie zijn voor de vrouwelijke partner. Helaas zijn hier geen prospectief gerandomiseerde data over in de huidige literatuur, er zijn wel observationele studies die “upgrading” van ART techniek na varicocele behandeling van de man mogelijk maken. (Samplaski, 2017) Bovendien zijn er meta-analyses van observationele studies, die suggereren dat de uitkomst van ICSI bij mannen met ernstige oligospermie en azoospermie met een gecorrigeerde varicocele beter is, dan bij mannen bij wie de varicocele onbehandeld bleef (Kirby, 2016; Palani, 2024).
Een niet significante verbetering in de overall kans op een spontane zwangerschap (RR 1,38, 95%CI 0,86-2,22) maakt dat niet zondermeer geconcludeerd kan worden dat een chirurgische of radiologische behandeling van een klinische vacicocèle verricht moet worden ter verbetering van de kans op zwangerschap. Echter, in de gerandomiseerde studies zijn tevens mannen met afwezigheid van afwijkende semenparameters geïncludeerd, waardoor het effect van de vacicocèle behandeling potentieel onderschat kan zijn. De lage bewijskracht op basis van risico op bias, conflicterende uitkomsten en het lage aantal events, maakt dat geen harde conclusies getrokken kunnen worden in het al dan niet behandelen van een klinische vacicocèle. Helaas kunnen op basis van de literatuur geen uitspraken gedaan worden over kans op doorgaande zwangerschap of levendgeborene.
De werkgroep volgt de aanbevelingen van de EAU en AUA/ASRM guidelines, die stellen dat geïsoleerde teratozoospermie geen behandelindicatie is voor een klinisch vastgestelde vacicocèle.
Bijwerkingen en complicaties van de chirurgische of radiologische behandeling van de vacicocèle waren geen uitkomst van onze literatuuranalyse. Risico’s zijn in het algemeen laag, en complicaties mild, waaronder wondinfectie, scrotale pijn, ontstaan van een hydrocèle, persisterende of recidief vacicocèle, en zeer zelden testiculaire atrofie. Er is geen systematisch literatuuronderzoek gedaan naar de doelmatigheid van embolisatie van de vena spermatica versus chirurgische of microchirurgische behandeling. De internationale richtlijnen suggereren dat microchirurgische beahndeling het laagste risico en recidief geeft. Emobilisatie is wellicht de meest doelmatige eerte vorm van beahndeling, aangezien microchirurgische behandeling in slechts enkele centra wordt aangeboden.
Rationale van aanbeveling-1: weging van argumenten voor en tegen de interventies
Indien zowel sprake is van een klinische vacicocèle, een afwijkende semenanalyse, als subfertiliteit kan overwogen worden deze vacicocèle chirurgisch dan wel radiologisch te behandelen, hoewel het effect op de verbetering van de kwaliteit van het semen en dientengevolge de kans op zwangerschap onzeker is (zwakke aanbeveling, geconcludeerd op basis van het beoordelen van gerandomiseerde studies). In de internationale richtlijnen wordt dezelfde aanbeveling gedaan met een grotere stelligheid, waarbij de bewijskracht is gebaseerd op (retrospectieve) observationele studies. Vanwege een laag risico op complicaties en potentiële individuele voordelen kan een afweging gemaakt worden dat het behandelen van de vacicocèle van meerwaarde kan zijn.
Een eventuele beperkte, hoewel klinisch relevante verbetering van de kwaliteit van het semen kan ervoor zorgen dat er een adaptatie van behandelmodaliteit mogelijk is (i.e. van marginaal ICSI naar ICSI geschikt, van ICSI geschikt naar geringe oligospermie, waarvoor slechts IUI nodig is, van geringe oligospermie naar normospermie). Een dergelijke geringe verbetering heeft vervolgens directe consequenties voor de vrouwelijke partner, die dientengevolge mogelijk wordt blootgesteld aan een minder invasieve behandeling. Hoewel de kwaliteit van het semen in absolute zin een niet-significante, geringe verbetering laat zien na chirurgische of radiologische behandeling van een vacicocèle, geeft de literatuur ons geen informatie over deze klinische relevante uitkomstmaat. Voorafgaand aan het aanbieden van geassisteerde voortplanting wordt geadviseerd counseling van man en vrouw te laten plaatsvinden, waarbij feiten en controverse van de associatie tussen de varicocele en kans op een kind, verbetering van zaadkwaliteit na behandeling en overbodig worden van ART moeten worden afgewogen.
Eindoordeel:
Zwakke aanbeveling voor het behandelen van een vacicocèle.
Rationale van aanbeveling-2: weging van argumenten voor en tegen de interventies
Eindoordeel:
Zwakke aanbeveling voor counselen van de patiënt op mogelijkheid tot behandelen van een varicocèle.
Onderbouwing
A varicocele can negatively influence spermatogenesis and therefore, semen quality and is associated with increased levels of sperm DNA fragmentation (SDF) that potentially reduces fertility. Literature suggests that treatment of the varicocele can improve semen quality, may reduce SDF and enhance natural conception or outcome of assisted reproduction technologies. Currently, it is unknown whether this regards all types of abnormal semen analyses, including azoospermic cases. The European Association of Urology Guideline on sexual and Reproductive Health recommends treatment of infertile men with a clinical varicocele, abnormal semen parameters and otherwise unexplained infertility in couples where the female partner has good ovarian reserve to improve fertility rates (Strong strength rating) (Salonia, 2024). The American Urological Association with the American Society of Reproductive Medicine recommends that clinician should consider surgical varicocelectomy in males attempting to conceive who have palpable varicocele, infertility, and abnormal semen parameters, except for azoospermic males. (Moderate recommendation; Evidence Level: Grade B) (Schlegel, 2021). Despite these international guideline recommendations, varicocele treatment still remains controversial. Low recruitment in randomized controlled trials and observational study designs and conflicting meta-analysis have led to the continuation of the controversy that it is unclear whether treatment of a varicocele improves pregnancy rates.
Summary of Findings table: Clinical varicocele in males with subfertility: treatment or observation
Population: Men with clinical varicocele and subfertility
Intervention: Surgical or radiological treatment of varicocele
Comparison: Observation, no treatment
|
Outcome |
Study results and measurements |
Absolute effect estimates |
Certainty of the Evidence (Quality of evidence) |
Summary |
|
|
Observation |
Treatment |
||||
|
Sperm concentration (x10^6/ml) |
Higher better Based on data from 577 participants in 6 studies Follow up 12 months |
Difference: MD 9.34 higher (CI 95% 3.86 lower - 22.54 higher) |
Very low Due to serious risk of bias, due to serious inconsistency, due to serious imprecision1 |
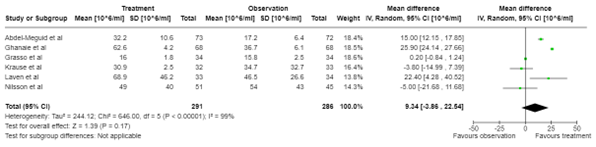
The evidence is very uncertain about the effect of varicocele treatment on sperm concentration when compared with observation in males with subfertility and a clinical varicocele.
(Nilsson 1979, Laven 1992, Grasso 2000, Krause 2002, Abdel-Meguid 2011, Ghanaie 2012) |
|
|
Sperm progressive motility (%) |
Higher better Based on data from 713 participants in 7 studies Follow up 12 months |
Difference: MD 6.86 higher (CI 95% 4.66 lower - 18.38 higher)
|
Very low Due to serious risk of bias, due to serious inconsistency, due to serious imprecision1 |
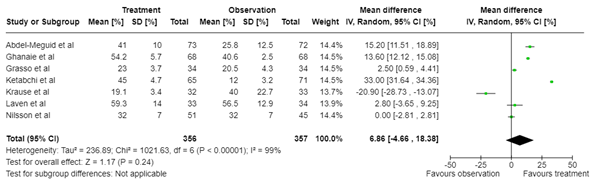
The evidence is very uncertain about the effect of varicocele treatment on sperm progressive motility when compared with observation in males with subfertility and a clinical varicocele.
(Nilsson 1979, Laven 1992, Grasso 2000, Krause 2002, Abdel-Meguid 2011, Ghanaie 2012, Ketabchi 2018) |
|
|
Sperm morphology (%) |
Higher better Based on data from 713 participants in 7 studies |
Difference: MD 2.75 higher (CI 95% 2.82 lower - 8.33 higher) |
Very low Due to serious risk of bias, due to serious inconsistency, due to serious imprecision1 |
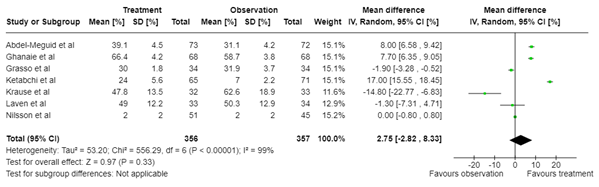
The evidence is very uncertain about the effect of varicocele treatment on sperm morphology when compared with observation in males with subfertility and a clinical varicocele.
(Nilsson 1979, Laven 1992, Grasso 2000, Krause 2002, Abdel-Meguid 2011, Ghanaie 2012, Ketabchi 2018) |
|
|
Pregnancy rate |
Relative risk: 1.38 (CI 95% 0.86 - 2.22) Based on data from 612 participants in 6 studies Follow up 12 months |
24 per 100 |
33 per 100 |
Very low Due to serious risk of bias, due to serious inconsistency, due to very serious imprecision2 |
The evidence is very uncertain about the effect of varicocele treatment on pregnancy rate when compared with observation in males with subfertility and a clinical varicocele.
(Nilsson 1979, Madgar 1995, Nieschlag 1998, Krause 2002, Abdel-Meguid 2011, Ketabchi 2018) |
|
Difference: 9 more per 100 (CI 95% 3 fewer - 29 more) |
|||||
1. Risk of Bias: serious, due to lack of blinding
Inconsistency: serious, due to conflicting results
Imprecision: serious, due to overlap of the upper limit of the 95% confidence interval with the minimal clinically important difference.
2. Risk of Bias: serious, due to lack of blinding
Inconsistency: serious, due to conflicting results
Imprecision: very serious, due to overlap of both limits of the 95% confidence interval with the minimal clinically important difference and due to low number of events
To answer our question, we excluded three out of these twelve studies of the review of Fallara (2023): two were excluded due to a non-randomized design and one was excluded as the population did not match PICO. One study was replaced with an updated version of the particular study. One study included couples with recurrent pregnancy loss, this study was included in the analyses of semen quality, but not in the analysis of pregnancy rate (Ghanaie, 2012). Thus, our analyses for semen quality are based on nine studies and for pregnancy rate on eight studies. It is important to highlight that the methodology for the current analyses differed to the EAU and AUA/ASRM guidelines that included studies with non-randomized designs and selective outcome reporting for the generation of recommendations in favor of varicocele correction. The Cochrane Meta-Analysis from 2021 concluded that based on limited evidence, it remains unclear whether surgical or radiological treatment compared to no treatment in subfertile men may be of benefit on live birth rate, but treatment may improve the chances of pregnancy. (Persad, 2021) Although the evidence was insufficient to determine whether surgical or radiological treatment was superior, microscopic subinguinal surgical treatment probably improves chances of pregnancy (Persad, 2021).
Results
The systematic review included twelve studies with a total of 1357 patients. Inclusion criteria of the systematic review were (a) primary infertile males aged ≥18 years old, (b) diagnoses of a clinically significant varicocele with or without semen abnormalities, (c) no evidence of any cause of infertility in the female partner of the couple, and (d) prospective studies comparing treatment (either surgical or radiological) to no treatment (observation). Studies were excluded if pretreatment varicocele assessment (semenanalysis) was not reported. Important study characteristics and results per study are summarized in the evidence table. The assessment of the risk of bias is summarized in the risk of bias table. The systematic review included studies up until November 26, 2021.
The nine studies that we included in our analyses all had a randomized controlled design and included patients with an abnormal semen analysis. All studies compared treatment to observation. Duration of follow-up after treatment was twelve months in eight studies and 74 months in one study (Nilsson, 1979). The number of included participants per study and treatment arm are depicted in the forest plots below.
Surgical treatment was investigated in six studies: three studies performed the supra-inguinal approach (van Nilsson, 1979; Madgar, 1995; Grasso, 2000), two performed subinguinal microsurgery (Abdel-Meguid, 2011; Ketabchi, 2018) and one performed inguinal microsurgery (Ghanaie, 2012). Radiological treatment was assessed in two studies: Laven (1992) performed anterograde embolization and Krause (2002) performed antegrade or retrograde sclerotherapy. Nieschlag (1998) investigated both surgical and radiological treatment: high retroperitoneal ligation and anterograde sclerotization.
1. Semen quality (critical)
Sperm concentration was investigated in six studies with data of 577 participants. The mean difference in sperm concentration (106/ml) when comparing treatment to observation was 9.34 (95% CI -3.86 to 22.54) in favor of treatment (figure 1A). The difference in weighted mean sperm concentration before and after treatment was 14.56, whereas this difference was 1.69 before and after observation.
Sperm progressive motility was assessed in seven studies with data of 713 participants and showed a mean difference of 6.86 (95% CI -4.66 to 18.38) favoring treatment compared to observation, although the confidence intervals were wide (figure 1B). The difference in weighted mean sperm progressive motility before and after treatment was 12.58, whereas this difference was 1.30 before and after observation.
The percentage of cells with normal sperm morphology (figure 1C) was reported in seven studies, providing data on 713 participants. Meta-analysis revealed a mean difference of 2.75 (95%CI -2.82 to 8.33) in favor of treatment when compared to observation, although the confidence intervals were wide. When investigating before and after differences, the difference in weighted mean percentage of cells with normal sperm morphology before and after treatment was 7.94, whereas this difference was 1.19 before and after observation.
A
B
C
Figure 1. Forest plot of sperm quality
(A sperm concentration, B sperm progressive motility, C normal sperm morphology) after treatment versus observation in males with subfertility and a clinical varicocele
2. Pregnancy rate (important)
Pregnancy rate was assessed in six studies providing data on 612 participants. All studies investigated spontaneous pregnancy rate, thus without the use of assisted reproductive technology. Overall, the relative risk to become pregnant after treatment was 1.38 (95% CI 0.86 to 2.22) compared to observation.
A sensitivity analysis on treatment modality revealed that the relative risk to become pregnant after surgical treatment was 1.62 (95% CI 0.78 to 3.38) compared to observation, whereas for radiological treatment this risk was 0.86 (95% CI 0.29 to 2.64), though the latter analysis regards one study only (figure 2).
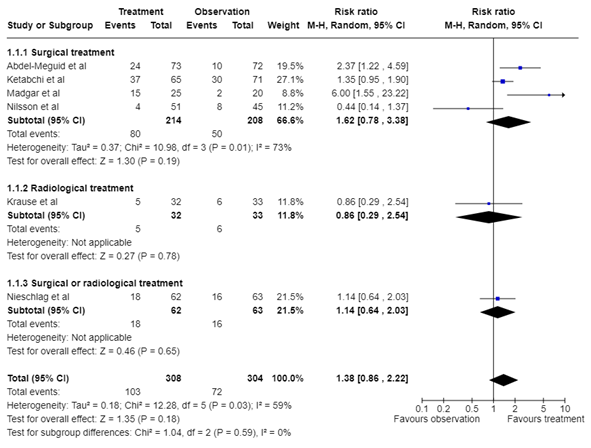
Figure 2. Forest plot of pregnancy rate after treatment versus observation in males with subfertility and a clinical varicocele
3. Sperm DNA fragmentation (SDF), pregnancy rate with ART, ongoing pregnancy, live birth (important)
No studies that complied with our PICO reported these outcome measures.
A systematic review of the literature was performed to answer the following question:
‘what is the additional value of surgical or radiological treatment of a varicocele in subfertile males to improve semen quality and the chance of an ongoing pregnancy?
| P: patients | Men with clinical varicocele and subfertility/infertility, oligospermia, azoospermia |
| I: intervention | Surgical or microsurgical treatment of varicocele, radiological treatment of varicocele (retrograde sclerotherapy or embolization) |
| C: control | Observation, no treatment |
| O: outcome measure |
1. Semen quality and DNA fragmentation 2. Pregnancy: chance of pregnancy (with and without ART), ongoing pregnancy, live birth rate |
Relevant outcome measures
The guideline panel considered semen quality as a critical outcome measures for decision making; and chance of pregnancy, ongoing pregnancy, live birth and DNA fragmentation as important outcome measures for decision making.
The guideline panel defined a 25% difference for dichotomous outcomes (RR< 0.8 or >1.25) and 0.5 SD for continuous outcomes (default boundaries as defined by GRADE) as minimal clinically (patient) important difference.
Search and select (Methods)
The databases OVID/Medline and Embase were searched for systematic reviews and RCTs with relevant search terms from 2000 until February 22, 2024. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 259 hits. Studies were selected based on the criteria as stated in de PICO. Studies were initially selected based on title and abstract screening. Twenty-six studies were screened on full text. After reading the full text, 25 studies were excluded (see the table with reasons for exclusion under the tab Methods), and one study was included. The included study was a systematic review based on twelve studies (Fallara, 2023).
- Abdel-Meguid TA, Al-Sayyad A, Tayib A, Farsi HM. Does varicocele repair improve male infertility? An evidence-based perspective from a randomized, controlled trial. Eur Urol. 2011 Mar;59(3):455-61. doi: 10.1016/j.eururo.2010.12.008. Epub 2010 Dec 21. PMID: 21196073.
- Fallara G, Capogrosso P, Pozzi E, Belladelli F, Corsini C, Boeri L, Candela L, Schifano N, Dehò F, Castiglione F, Muneer A, Montorsi F, Salonia A. The Effect of Varicocele Treatment on Fertility in Adults: A Systematic Review and Meta-analysis of Published Prospective Trials. Eur Urol Focus. 2023 Jan;9(1):154-161. doi: 10.1016/j.euf.2022.08.014. Epub 2022 Sep 20. PMID: 36151030.
- Grasso M, Lania C, Castelli M, Galli L, Franzoso F, Rigatti P. Low-grade left varicocele in patients over 30 years old:the effect of spermatic vein ligation on fertility. BJU Int. 2000 Feb;85(3):305-7. doi: 10.1046/j.1464-410x.2000.00437.x. PMID: 10671887.
- Ketabchi A, Salehi S, Shirin Salajghah. The Effect of Varicocelectomy on Assisted Reproductive Technique Indications and Outcomes based on Kruger Strict Morphology Test: a Randomized Clinical Trial. Journal of Kerman University of Medical Sciences, 2018; 25 (6): 519-527.
- Kirby EW, Wiener LE, Rajanahally S, et al. Undergoing varicocele repair before assisted reproduction improves pregnancy rates and live birth rate in azoospermic and oligospermic man with a varicocele: a systematic review and meta-analysis. Fertil Steril. 2016;160:1338-1343.
- Krause W, Müller HH, Schäfer H, Weidner W. Does treatment of varicocele improve male fertility? results of the 'Deutsche Varikozelenstudie', a multicentre study of 14 collaborating centres. Andrologia. 2002 Jun;34(3):164-71. doi: 10.1046/j.1439-0272.2002.00494.x. PMID: 12059812.
- Laven JS, Haans LC, Mali WP, te Velde ER, Wensing CJ, Eimers JM. Effects of varicocele treatment in adolescents: a randomized study. Fertil Steril. 1992 Oct;58(4):756-62. doi: 10.1016/s0015-0282(16)55324-2. PMID: 1426322.
- Madgar I, Weissenberg R, Lunenfeld B, Karasik A, Goldwasser B. Controlled trial of high spermatic vein ligation for varicocele in infertile men. Fertil Steril. 1995 Jan;63(1):120-4. doi: 10.1016/s0015-0282(16)57306-3. PMID: 7805900.
- Nieschlag E, Hertle L, Fischedick A, Abshagen K, Behre HM. Update on treatment of varicocele: counselling as effective as occlusion of the vena spermatica. Hum Reprod. 1998 Aug;13(8):2147-50. doi: 10.1093/humrep/13.8.2147. PMID: 9756286.
- Nilsson S, Edvinsson A, Nilsson B. Improvement of semen and pregnancy rate after ligation and division of the internal spermatic vein: fact or fiction? Br J Urol. 1979 Dec;51(6):591-6. doi: 10.1111/j.1464-410x.1979.tb03609.x. PMID: 534846.
- Palani A, Cannarella R, Saleh R, et al. Impact of Varicocele repair on assisted reproductive technique outcomes in infertile men: a systematic review and meta-analysis. World J Mens Health. 2024;42:e80.
- Salonia A, Bettocchi A, et al. EAU Guideline on Sexual and Reproductive Health. Chapter 11. Male infertility. 2024.
- Samplaski M, Lo KC, Grober ED, et al. Varicocelectomy to “upgrade” semen quality to allow couples to use less invasive forms of assisted reproductive technology. Fertil Steril. 2017;108:609-612.
- Schlegel PN, Sigman M, Collura B et al. Diagnosis and treatment of infertility in men: UAU/ASRM guideline part I. Fertil Steril. 2021;115:54-61.
- Schlegel PN, Sigman M, Collura B, et al. Diagnosis and treatment of infertility in men: AUA/ASRM guideline part II. Fertil Steril. 2021;115:62-69.
- Persad E, O’Loughlin CA, Kaur S, et al. Surgical or radiological treatment for varicoceles in subfertile men.
Evidence table for systematic review of RCTs and observational studies (intervention studies)
Risk of Bias table
|
Study reference |
Appropriate and clearly focused question?1 |
Comprehensive and systematic literature search?2 |
Description of included and excluded studies?3 |
Description of relevant characteristics of included studies?4 |
Assessment of scientific quality of included studies?5 |
Enough similarities between studies to make combining them reasonable?6 |
Potential risk of publication bias taken into account?7 |
Potential conflicts of interest reported?8
|
|
Fallara, 2023 |
Yes |
Yes |
Yes |
Yes |
Yes |
No |
Yes |
No |
1. Research question (PICO) and inclusion criteria should be appropriate (in relation to the research question to be answered in the clinical guideline) and predefined
2. Search period and strategy should be described; at least Medline searched
3. Potentially relevant studies that are excluded at final selection (after reading the full text) should be referenced with reasons
4. Characteristics of individual studies relevant to the research question (PICO) should be reported
5. Quality of individual studies should be assessed using a quality scoring tool or checklist (preferably QUADAS-2; COSMIN checklist for measuring instruments) and taken into account in the evidence synthesis
6. Clinical and statistical heterogeneity should be assessed; clinical: enough similarities in patient characteristics, diagnostic tests (strategy) to allow pooling? For pooled data: at least 5 studies available for pooling; assessment of statistical heterogeneity and, more importantly (see Note), assessment of the reasons for heterogeneity (if present)? Note: sensitivity and specificity depend on the situation in which the test is being used and the thresholds that have been set, and sensitivity and specificity are correlated; therefore, the use of heterogeneity statistics (p-values; I2) is problematic, and rather than testing whether heterogeneity is present, heterogeneity should be assessed by eye-balling (degree of overlap of confidence intervals in Forest plot), and the reasons for heterogeneity should be examined.
7. There is no clear evidence for publication bias in diagnostic studies, and an ongoing discussion on which statistical method should be used. Tests to identify publication bias are likely to give false-positive results, among available tests, Deeks’ test is most valid. Irrespective of the use of statistical methods, you may score “Yes” if the authors discuss the potential risk of publication bias.
8. Sources of support (including commercial co-authorship) should be reported in both the systematic review and the included studies. Note: To get a “yes,” source of funding or support must be indicated for the systematic review AND for each of the included studies.
Table of Excluded studies after reading full text
|
|
Reference |
Reason for exclusion |
|
1 |
Zini A, Dohle G. Are varicoceles associated with increased deoxyribonucleic acid fragmentation? Fertil Steril. 2011 Dec;96(6):1283-7. doi: 10.1016/j.fertnstert.2011.10.016. Epub 2011 Oct 28. PMID: 22035729. |
Wrong comparison: before/after study |
|
2 |
Evers JL, Collins JA. Assessment of efficacy of varicocele repair for male subfertility: a systematic review. Lancet. 2003 May 31;361(9372):1849-52. doi: 10.1016/S0140-6736(03)13503-9. PMID: 12788571. |
Population unclearly described, also not the most recent review |
|
3 |
Birowo P, Tendi W, Widyahening IS, Atmoko W, Rasyid N. The benefits of varicocele repair for achieving pregnancy in male infertility: A systematic review and meta-analysis. Heliyon. 2020 Nov 5;6(11):e05439. doi: 10.1016/j.heliyon.2020.e05439. PMID: 33204888; PMCID: PMC7648199. |
Wrong population: also patients with subclinical varicocele |
|
4 |
Wang X, Chen T, Qiu J, Wu H, Chen X, Xuan X. Effects of Primary Varicocele and Related Surgery in Male Infertility: A Meta-Analysis. Front Surg. 2020 Oct 30;7:586153. doi: 10.3389/fsurg.2020.586153. PMID: 33330606; PMCID: PMC7673405. |
Wrong population: also patients with subclinical varicocele, also not the most recent review |
|
5 |
Birowo P, Rahendra Wijaya J, Atmoko W, Rasyid N. The effects of varicocelectomy on the DNA fragmentation index and other sperm parameters: a meta-analysis. Basic Clin Androl. 2020 Sep 10;30:15. doi: 10.1186/s12610-020-00112-6. PMID: 32944248; PMCID: PMC7488296. |
Wrong comparison: before/after study |
|
6 |
Qiu D, Shi Q, Pan L. Efficacy of varicocelectomy for sperm DNA integrity improvement: A meta-analysis. Andrologia. 2021 Feb;53(1):e13885. doi: 10.1111/and.13885. Epub 2020 Oct 28. PMID: 33118219. |
Comparison of interest not reported: either before/after varicocelectomy, or patients with/without varicocele repair. |
|
7 |
Kim KH, Lee JY, Kang DH, Lee H, Seo JT, Cho KS. Impact of surgical varicocele repair on pregnancy rate in subfertile men with clinical varicocele and impaired semen quality: a meta-analysis of randomized clinical trials. Korean J Urol. 2013 Oct;54(10):703-9. doi: 10.4111/kju.2013.54.10.703. Epub 2013 Oct 15. PMID: 24175046; PMCID: PMC3806996. |
Wrong population: also patients with subclinical varicocele, |
|
8 |
Agarwal A, Cannarella R, Saleh R, Boitrelle F, Gül M, Toprak T, Salvio G, Arafa M, Russo GI, Harraz AM, Singh R, Garrido N, Hamoda TAA, Rambhatla A, Kavoussi P, Kuroda S, Çalik G, Saini P, Ceyhan E, Dimitriadis F, Henkel R, Crafa A, Palani A, Duran MB, Maziotis E, Saïs É, Bendayan M, Darbandi M, Le TV, Gunes S, Tsioulou P, Sengupta P, Hazir B, Çeker G, Darbandi S, Durairajanayagam D, Aghamajidi A, Alkhalidi N, Sogutdelen E, Leisegang K, Alarbid A, Ho CCK, Malhotra V, Finocchi F, Crisóstomo L, Kosgi R, ElBardisi H, Zini A, Birowo P, Colpi G, Park HJ, Serefoglu EC, Nguyen Q, Ko E, de la Rosette J, Pinggera GM, Nguyen HVP, Kandil H, Shah R. Impact of Varicocele Repair on Semen Parameters in Infertile Men: A Systematic Review and Meta-Analysis. World J Mens Health. 2023 Apr;41(2):289-310. doi: 10.5534/wjmh.220142. Epub 2022 Oct 28. PMID: 36326166; PMCID: PMC10042659. |
Not the most recent review |
|
9 |
Esteves SC, Roque M, Agarwal A. Outcome of assisted reproductive technology in men with treated and untreated varicocele: systematic review and meta-analysis. Asian J Androl. 2016 Mar-Apr;18(2):254-8. doi: 10.4103/1008-682X.163269. PMID: 26510504; PMCID: PMC4770495. |
Not the most recent review |
|
10 |
Marmar JL, Agarwal A, Prabakaran S, Agarwal R, Short RA, Benoff S, Thomas AJ Jr. Reassessing the value of varicocelectomy as a treatment for male subfertility with a new meta-analysis. Fertil Steril. 2007 Sep;88(3):639-48. doi: 10.1016/j.fertnstert.2006.12.008. Epub 2007 Apr 16. PMID: 17434508. |
Wrong comparison: either no treatment, or medical treatment. Not defined what medical treatment entails. |
|
11 |
Evers JL, Collins JA. Surgery or embolisation for varicocele in subfertile men. Cochrane Database Syst Rev. 2004;(3):CD000479. doi: 10.1002/14651858.CD000479.pub2. |
Not the most recent Cochrane |
|
12 |
Evers JL, Collins JA, Vandekerckhove P. Surgery or embolisation for varicocele in subfertile men. Cochrane Database Syst Rev. 2001;(1):CD000479. doi: 10.1002/14651858.CD000479. |
Not the most recent Cochrane |
|
13 |
Evers JH, Collins J, Clarke J. Surgery or embolisation for varicoceles in subfertile men. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD000479. doi: 10.1002/14651858.CD000479.pub4. |
Not the most recent Cochrane |
|
14 |
Kroese AC, de Lange NM, Collins J, Evers JL. Surgery or embolization for varicoceles in subfertile men. Cochrane Database Syst Rev. 2012 Oct 17;10:CD000479. doi: 10.1002/14651858.CD000479.pub5. |
Not the most recent Cochrane |
|
15 |
Persad E, O'Loughlin CA, Kaur S, Wagner G, Matyas N, Hassler-Di Fratta MR, Nussbaumer-Streit B. Surgical or radiological treatment for varicoceles in subfertile men. Cochrane Database Syst Rev. 2021 Apr 23;4(4):CD000479. doi: 10.1002/14651858.CD000479.pub6. PMID: 33890288; PMCID: PMC8408310. |
The included studies had either a correct population but incorrect comparison, or vice versa therefore none of the studies matched our PICO |
|
16 |
Biyani CS, Cartledge J, Janetschek G. Varicocele. BMJ Clin Evid. 2009 Jan 6;2009:1806. PMID: 19445764; PMCID: PMC2907779. |
Incorrect article type: guideline paper |
|
17 |
Macleod R, Biyani CS, Cartledge J, Eardley I. Varicocele. BMJ Clin Evid. 2015 Jul 13;2015:1806. PMID: 26168774; PMCID: PMC4500994. |
Incorrect article type: guideline paper |
|
18 |
Baazeem A, Belzile E, Ciampi A, Dohle G, Jarvi K, Salonia A, Weidner W, Zini A. Varicocele and male factor infertility treatment: a new meta-analysis and review of the role of varicocele repair. Eur Urol. 2011 Oct;60(4):796-808. doi: 10.1016/j.eururo.2011.06.018. Epub 2011 Jul 5. PMID: 21733620. |
Population, intervention, and comparison poorly described. Not the most recent review |
|
19 |
Krause W, Müller HH, Schäfer H, Weidner W. Does treatment of varicocele improve male fertility? results of the 'Deutsche Varikozelenstudie', a multicentre study of 14 collaborating centres. Andrologia. 2002 Jun;34(3):164-71. doi: 10.1046/j.1439-0272.2002.00494.x. PMID: 12059812. |
Included in our included review |
|
20 |
Abdel-Meguid TA, Al-Sayyad A, Tayib A, Farsi HM. Does varicocele repair improve male infertility? An evidence-based perspective from a randomized, controlled trial. Eur Urol. 2011 Mar;59(3):455-61. doi: 10.1016/j.eururo.2010.12.008. Epub 2010 Dec 21. PMID: 21196073. |
Included in our included review |
|
21 |
Richardson I, Grotas AB, Nagler HM. Outcomes of varicocelectomy treatment: an updated critical analysis. Urol Clin North Am. 2008 May;35(2):191-209, viii. doi: 10.1016/j.ucl.2008.01.007. PMID: 18423240. |
No systematic review |
|
22 |
Huyghe E, Methorst C, Faix A. Varicocèle et infertilité masculine [Varicocele and male infertility]. Prog Urol. 2023 Nov;33(13):624-635. French. doi: 10.1016/j.purol.2023.09.003. PMID: 38012908. |
Full text in French |
|
23 |
Ficarra V, Crestani A, Novara G, Mirone V. Varicocele repair for infertility: what is the evidence? Curr Opin Urol. 2012 Nov;22(6):489-94. doi: 10.1097/MOU.0b013e328358e115. PMID: 23026895. |
No systematic review |
|
24 |
Bozhedomov VA, Shomarufov AB, Bozhedomova GE, D OA, Kamalov DM, Sorokin NI, Kamalov AA. [Varicocele and reproductive function: pathozoospermia treatment (a prospective comparative study)]. Urologiia. 2021 May;(2):62-68. Russian. PMID: 33960159. |
Full text in Russian |
|
25 |
Adams Y, Amidu N, Afoko AA. Changes in testicular arterial hemodynamic, gonadotropin levels, and semen parameters among varicocele patients randomized to varicocelectomy or observed in Tamale, Ghana. Urologia. 2023 May;90(2):286-294. doi: 10.1177/03915603221127116. Epub 2022 Oct 13. PMID: 36227064. |
Wrong comparison in the subpopulation of patients (includes healthy controls as well) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 30-04-2026
Beoordeeld op geldigheid : 30-04-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met mannelijke subfertiliteit.
Werkgroep
- Cantineau A.E.P. (Astrid), gynaecoloog, subspecialist voortplantingsgeneeskunde Universitair Medisch Centrum Groningen te Groningen, NVOG
- Dinkelman-Smit M. (Marij), uroloog-androloog, Erasmus Medisch Centrum te Rotterdam, NVU
- Verberg M.F.G. (Marieke), gynaecoloog, Medisch Spectrum Twente te Enschede, NVOG
- Heida K.Y. (Karst), gynaecoloog, Dijklander ziekenhuisbte Purmerend, NVOG
- van der Houwen L.E.E. (Lisette), gynaecoloog, Radboud universitair medisch centrum te Nijmegen, NVOG
- de Bruin J.P. (Jan Peter), gynaecoloog, Jeroen Bosch Ziekenhuis te ’s Hertogenbosch, NVOG
- van Breda H.M.K. (Jetske), uroloog-androloog, Universitair Medisch Centrum Utrecht te Utrecht, NVU
- van Roijen J.H. (Herman), uroloog-androloog, voorheen ETZ Tilburg – nu gepensioneerd
- D’Hauwers K.W.M. (Kathleen), uroloog-androloog, Radboud universitair medisch centrum te Nijmegen, NVU
- Meißner A. (Andreas), uroloog-androloog, Amsterdam Universitair Medisch Centrum te Amsterdam, NVU
- Bailleux B.B.E.P. (Bart), laboratoriumspecialist Klinische Chemie en Endocrinologie, Leids Universitair Medisch Centrum te Leiden, NVKC
- Kempers M.J.E. (Marlies), klinisch geneticus, Radboud universitair medisch centrum te Nijmegen, VKGN
- van der Kevie-Kersemaekers A.M.F. (Anne-Marie), laboratoriumspecialist klinische genetica, Universitair Medisch Centrum Utrecht te Utrecht, VKGL
- Westra D. (Dineke), laboratoriumspecialist klinische genetica, Radboud universitair medisch centrum te Nijmegen, VKGL
- Ramos L. (Liliana), klinisch embryoloog, Radboud universitair medisch centrum te Nijmegen, KLEM
- Grolle R.L. (Rosanne), fertiliteitsarts, Erasmus Medisch Centrum te Rotterdam, VVF
- Sinjorgo S. (Simone), medewerker medewerker patientenperspectief wetenschappelijk onderzoek en richtlijnen, Freya (vanaf december 2024)
- Vermeulen M. (Marloes), medewerker patientenperspectief wetenschappelijk onderzoek en richtlijnen, Freya (tot december 2024)
Met ondersteuning van
- Mostovaya I.M. (Irina), senior-adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- van der Lee J.H. (Hanneke), senior-adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Middelhuis D. (Danique), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Van Bommel M. (Majke), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Schultink J.M. (Janneke), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- E. (Esther) van der Bijl, informatiespecialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel Gemelde (neven)functies en belangen werkgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaam-heden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Datum |
Restrictie |
|
Astrid Cantineau (voorzitter) |
Gynaecoloog. UMCG, 1.0 FTE |
auteur Up to date Hyperthecosis |
Geen |
Geen |
Geen |
Voorzitter SIG andrologie NVOG aanvrager subsidie ZonMw over leefstijl en mannelijke subfertiliteit |
Geen |
13/11/2022 |
Geen restricties. |
|
Marij Dinkelman-Smit (vice voorzitter) |
Staflid Uroloog-Androloog Voorzitter Voortplantingscentrum Erasmus MC Plaatsvervangend afdelingshoofd Urologie Erasmus MC Erasmus MC Universitair Medisch Centrum |
Bestuurslid Nederlandse Vereniging voor Urologie (NVU) (onbetaald) Bestuurslid multidisciplenaire Special Interest Group (SIG) Andrologie, Nederlandse Verening voor Obstetrie en Gynaecologie (NVOG) (onbetaald) Bestuurslid European Association of Urology (EAU) section for Andrological Urology (ESAU) (onbetaald) Medical director European Academy of Andrology (EAA) training center Andrology Erasmus MC (onbetaald) Lid Commissie Kwaliteitvisitatie NVU (onbetaald) Medische adviesraad Klinefelter Vereniging (onbetaald) Medische adviesraad Stichting Lichen Sclerosus (onbetaald) |
Geen |
Geen |
Geen |
Geen |
Geen |
12/12/2022 |
Geen restricties. |
|
Marieke Verberg |
Gynaecoloog, Medisch Spectrum Twente 0.5 FTE betaalde functie Gynaecoloog en statutair directeur Fertiliteitskliniek Twente 0.5 FTE betaalde functie |
Geen relevante |
Geen |
Geen |
Geen |
Geen |
Geen |
19/11/2022 |
Geen restricties. |
|
Karst Heida |
Gynaecoloog bij het Dijklander ziekenhuis - betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
7/12/2022 |
Geen restricties. |
|
Lisette van der Houwen |
Gynaecoloog - fellow voortplantingsgeneeskunde Radboudumc |
Bestuurslid SIG endometriose NVOG algemeen lid SIG ART en SIG fertiliteitspreservatie van de NVOG |
Geen |
Geen |
Merck / Impect study - improving patient-centeredness in endometriosis care. / Ja |
Geen |
Geen |
02/12/2022 |
Geen restricties, extern gefinancierd onderzoek heeft geen betrekking op richtlijn onderwerp. |
|
Jan Peter de Bruin |
Gynaecoloog Jeroen Bosch Ziekenhuis, betaald |
Waarnemend gynaecoloog Radboudumc, betaald |
Medical Advisory Board Ferring BV - De medical advisory board komt op verzoek van Ferring ongeveer eens per jaar samen. Daarbij worden ontwikkelingen in het veld en relevant studie uitkomsten bediscussieerd. Ferring gebruikt de uitkomsten van deze besprekingen als input voor hun strategie. |
- |
Ja - Het gaat om eigen onderzoek op gebied voortplantingsgeneeksunde waarvoor mijn afdeling een unrestricted research grant kreeg. Dit onderzoek bestaat uit de volgende lijnen: • het ontwikkelen en evalueren van toepassingen voor online fertilteitszorg (geen raakvlak met uit te werken modules voor deze richtlijn). • het effect van gebruik van supplementen op de zwangerschapskans bij paren met mannelijke subfertiliteit (raakvlak met module over supplementen waar de Bruin bij betrokken is als locale hoofdonderzoeker, tweede auteur van de nog te publiceren paper) Gefinincierd door Goodlife pharma |
- |
- |
26/11/2022 |
Vanwege deelname aan een adviesraad aan de start van het traject is de richtlijn tijdens de commentaarfase ook aan de Commissie Kwaliteitsdocumenten van de NVOG voorgelegd. Verder is dit lid uitgesloten van besluitvorming bij onderwerpen die raken aan de adviesraad. |
|
Jetske van Breda |
Uroloog/ Androloog UMCUtrecht |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
18/11/2022 |
Geen restricties. |
|
Kathleen D' Hauwers |
Uroloog, staflid Radboudumc: betaald |
Lid Cie Kwaliteit NVU: onbetaald Lid Cie Andrologie NVU: onbetaald Board memeber Klinefelter Vereniging Nederland: onbeteaald Cie Keuzehulp ED: vergoed |
Geen |
Geen |
Geen |
Inbrengen van expertise. Geen specifieke, persoonlijke baat bij één of ander: het gaat om de patiënt / klant. |
Geen |
28/09/2022 |
Geen restricties. |
|
Andreas Meißner |
Uroloog - Androloog Staflid Centrum voor Voortplantingsgeneeskunde, locatie AMC, en afdeling Urologie, locatie VUMC, van het Amsterdam UMC betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
24/11/2022 |
Geen restricties. |
|
Herman van Roijen |
Uroloog ETZ Tilburg |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
13/11/2022 |
Geen restricties. |
|
Bart Ballieux |
Laboratoriumspecialist Klinische Chemie en Endocrinologie Afdeling KCL, LUMC, Leiden |
Geen |
geen persoonlijke financiele belangen |
Geen relevante persoonlijke relaties die van invloed kunnen zijn op mijn adviezen |
geen |
Geen intellectuele belangen bij mijn adviezen |
Geen overige belangen |
10/01/2023 |
Geen restricties. |
|
Marlies Kempers |
Klinisch Geneticus (Radboudumc) |
Voorzitter subcommissie Richtlijnen, onderdeel van Kwaliteitscommissie VKGN |
Geen |
Geen |
Aytu Pharma / Prevent studie (effect Enzastaurin bij vasculair EDS) Studie is nog niet gestart, financiering on hold / Tijdelijk, ter vervanging verlof projectleider |
Geen |
Geen |
10/11/2022 |
Geen restricties. De studie waar mw. Kempers bij betrokken was is nooit gestart. Inhoudelijk had deze studie niet met mannelijke infertiliteit te maken. |
|
Anne-Marie van der Kevie - Kersemaekers |
laboratoriumspecialist klinische genetica UMC Utrecht |
Vakdeskundige Raad van Accreditatie |
Geen |
Geen |
Geen |
Geen |
Geen |
28/03/2023 |
Geen restricties. |
|
Manon Oud |
Laboratoriumspecialist Klinische Genetica in opleiding, Radboudumc Betaalde functie (hoofdberoep) |
Geen |
Geen |
Geen |
Deelname aan onderzoeksproject als PhD student De novo mutations in male infertility (NWO VICI van prof. Joris Veltman) van 2015-2020 Travel Grant van de Catherine van Tussenbroek Foundation voor bezoek van 3 maanden aan Monash University (2019) |
Geen |
Geen |
8/11/2022 |
Geen restricties, niet actief geweest in de werkgroep. |
|
Dineke Westra |
Laboratoriumspecialist Klinische Genetica (1.0 FTE, betaald) Afd. Genetica, sectie Genoomdiagnostiek Radboudumc, Nijmegen Werkzaamheden: Genetische diagnostiek |
Technical Assessor ISO15189 Raad van Accreditatie betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
16/02/2023 |
Geen restricties. |
|
Liliana Ramos |
Klinisch embryoloog Radboudumc |
Geen |
Geen |
Geen |
Geen |
Boegbeeldfunctie bij patiënten en beroepsorganisatie |
Geen |
10/08/2023 |
Geen restricties. |
|
Rosanne Grolle |
Fertiliteitsarts, Erasmus MC. Het begeleiden en behandelen van paren met een kinderwens. Functie is betaald. |
Lid van de symposiumcommissie van de VVF Onder andere het opstellen van het wetenschappelijk programma, het vragen van sprekers, het regelen van een symposiumlocatie en buffet, het versturen van de uitnodigingen en het aanvragen van accreditatie en sponsoring. Functie is onbetaald. |
Geen |
Geen |
Geen |
Geen |
Geen |
3/11/2022 |
Geen restricties. |
|
Marloes Vermeulen |
Freya, medewerker externe relaties |
Verloskundige 1e lijn. |
Geen |
Geen |
Geen |
Geen |
Geen |
27/09/2022 |
Geen restricties. |
|
José Knijnenburg |
Directeur bij Freya, vereniging voor mensen met vruchtbaarheidsproblemen - 32u p/wk Medewerker communicatie en marketing bij van der Pol-consulting b.v. - 8u p/wk |
Geen |
Dienstverband bij de (onafhankelijke) landelijke patiëntenvereniging voor mensen met vruchtbaarheidsproblemen. |
Geen |
ZonMW / Alife2 en T4Life / nee ZonMW / Antarctica2 / nee ZonMW / Cosy - Zin en zwanger / nee ZonMW / FOAM / nee ZonMW / Scratch-OFO / nee ZonMW / TOF (3 or 5) / nee ZonMW / H2Olie / nee ZonMW / H2OlieFlush / nee ZonMW / MYPP - myo-inositol bij PCOS / nee ZonMW / PSIDER Embryonic checkpoints - releasing the brakes on IVF /nee RadboudUMC/Goodlife / Summer - voedingssupplement man / nee ZonMW / Divine - dosiscalculator / nee Amsterdam UMC / ANDES / nee ZonMW / PSIDER - Hip gametes / nee ZonMW / COPIE - - endometriose en IVF / nee |
Belangenbehartiger bij patiëntenorganisatie |
Radboud/MUMC / Hmove sporten en afweersysteem bij miskramen / nee ZonMW / Medium2 kweekvloeistof IVF / nee ZonMW / Selectimo timelapse / nee MUMC+ / Murlm hhmk en ril / nee ZonMw / LUMO luteal phase support / nee ZonMw / PSIDER SteMBlast / nee ZonMw / SEGa veiligheid vp-technieken / nee ZonMw / Covid-19 Impact endometriose/fertiliteitspatiënten / nee ZonMw / PREMI / nee ZonMw / HyFosy-HSG stugie / nee ZonMw / REMI III / nee |
20/07/2023 |
Geen restricties, mevrouw was tijdelijke inval tijdens zwangerschapsverlof. In rol van patientvertegenwoordiger betrokken bij onderzoek. |
|
Simone Sinjorgo |
Parttime medewerker patientenperspectief en -participatie bij Freya (vereniging voor mensen met vruchtbaarheidsproblemen) - betaald 14 uur https://www.freya.nl/over-freya/wie-we-zijn/de-werknemers. Ter info: door mijn functie bij Freya ben ik betrokken bij diverse richtlijnontwikkeling en/of onderzoeken op het gebied van fertiliteit. In de vorm van toelichten, belichten en/of vertegenwoordigen van alleen het patiëntenperspectief tav het bepaalde onderwerp, zoals bij deze 3 richtlijnen OFO, OHSS en mannelijke subfertiliteit. |
Lichaamsgericht psychosociaal therapeut - zzp eigen praktijk in Dongen-Vaart - geregistreerd therapeut RBCZ incl. AGB-codes. www.praktijkdediamant.nl
- Psychosociaal docent Bijscholing Instituut voor therapeuten - betaling via praktijk https://bivt.nl/?s=lichaamsgericht+coachen
- Psychosociaal docent vrouwencoach opleiding - betaling via praktijk https://www.devrouwencoach.nl/vrouwencoach-opleiding/ |
Geen |
Geen |
Geen |
Geen |
Geen |
03/12/2024 |
Geen restricties. |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door uitnodigen van Freya en de Patientenfederatie Nederland voor de invitational conference. Daarnaast zat namens Freya een afgevaardigde in de werkgroep. Het verslag van de invitational conference is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen (zie kop waarden en voorkeuren van patiënten). De conceptrichtlijn is tevens voor commentaar voorgelegd aan Freya en de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Varicocèle
|
Geen financiele gevolgen. |
Uit de toetsing volgt dat de aanbevelingen niet breed toepasbaar zijn (<5.000 patiënten) en daarom naar verwachting geen substantiële financiële gevolgen zullen hebben voor de collectieve uitgaven. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Zoekopbrengst - 22 februari 2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
136 |
114 |
152 |
|
RCT |
100 |
80 |
107 |
|
Totaal |
236 |
194 |
259 |
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
'male infertility'/exp OR 'male fertility'/exp OR (('subfertility'/de OR 'childlessness'/exp) AND 'male'/exp) OR (((male* OR men OR man) NEAR/3 (infertil* OR hypofertil* OR 'fertil*' OR subfertil* OR infecund* OR childless* OR reproduct*)):ti,ab,kw) OR (((spermatogen* OR spermiation OR spermiogen*) NEAR/3 failure):ti,ab,kw) OR ((spermatozoon NEAR/3 (abnormalit* OR anomal*)):ti,ab,kw) OR (((semen OR sperm) NEAR/3 (qualit* OR quantit*)):ti,ab,kw) OR asperm*:ti,ab,kw OR asthenazoosperm*:ti,ab,kw OR asthenosperm*:ti,ab,kw OR asthenozoosperm*:ti,ab,kw OR azoosperm*:ti,ab,kw OR cryptosperm*:ti,ab,kw OR cryptozoosperm*:ti,ab,kw OR hyposperm*:ti,ab,kw OR oligoasthenosperm*:ti,ab,kw OR oligosperm*:ti,ab,kw OR oligozoosperm*:ti,ab,kw OR 'retrograde ejaculat*':ti,ab,kw OR 'sco syndrome*':ti,ab,kw OR 'sertoli cell only syndrome*':ti,ab,kw OR teratozoosperm*:ti,ab,kw OR 'thermosensitive genic male steril*':ti,ab,kw OR globozoosperm*:ti,ab,kw OR macrozoosperm*:ti,ab,kw |
106669 |
|
#2 |
'varicocele'/exp OR varicocele*:ti,ab,kw OR varicocoele*:ti,ab,kw |
10192 |
|
#3 |
'surgical approach'/exp OR 'microsurgery'/exp OR 'inguinal surgery'/exp OR 'radiological procedures'/exp OR 'palomo technique'/exp OR (((surgical* OR surger* OR radiological*) NEAR/3 (approach* OR management* OR treatment* OR procedure* OR technique* OR repair*)):ti,ab,kw) OR (((micro* OR inguinal* OR 'minimal* invasive') NEAR/3 surger*):ti,ab,kw) OR (('spermatic vein' NEAR/3 (embolization OR embolisation)):ti,ab,kw) OR microsurg*:ti,ab,kw OR palomo:ti,ab,kw |
1929593 |
|
#4 |
#2 AND #3 |
2457 |
|
#5 |
'varicocelectomy'/exp OR 'subinguinal varicocelectomy'/exp OR varicocelectom*:ti,ab,kw OR varicocoelectom*:ti,ab,kw OR 'varicocele* repair*':ti,ab,kw OR 'varicocoele* repair*':ti,ab,kw |
2972 |
|
#6 |
#4 OR #5 |
4079 |
|
#7 |
#1 AND #6 |
2147 |
|
#8 |
#7 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
1165 |
|
#9 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1002104 |
|
#10 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
2159478 |
|
#11 |
#8 AND #9 – SR’s |
136 |
|
#12 |
#8 AND #10 NOT #11 – RCT’s |
100 |
|
#13 |
#11 OR #12 |
236 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Infertility, Male/ or ((exp Infertility/ or Fertility/) and exp Male/) or ((male* or men or man) adj3 (infertil* or hypofertil* or fertil* or subfertil* or infecund* or childless* or reproduct*)).ti,ab,kf. or ((spermatogen* or spermiation or spermiogen*) adj3 failure).ti,ab,kf. or (spermatozoon adj3 (abnormalit* or anomal*)).ti,ab,kf. or ((semen or sperm) adj3 (qualit* or quantit*)).ti,ab,kf. or asperm*.ti,ab,kf. or asthenazoosperm*.ti,ab,kf. or asthenosperm*.ti,ab,kf. or asthenozoosperm*.ti,ab,kf. or azoosperm*.ti,ab,kf. or cryptosperm*.ti,ab,kf. or cryptozoosperm*.ti,ab,kf. or hyposperm*.ti,ab,kf. or oligoasthenosperm*.ti,ab,kf. or oligosperm*.ti,ab,kf. or oligozoosperm*.ti,ab,kf. or retrograde ejaculat*.ti,ab,kf. or sco syndrome*.ti,ab,kf. or sertoli cell only syndrome*.ti,ab,kf. or teratozoosperm*.ti,ab,kf. or thermosensitive genic male steril*.ti,ab,kf. or globozoosperm*.ti,ab,kf. or macrozoosperm*.ti,ab,kf. |
97161 |
|
2 |
exp Varicocele/ or varicocele*.ti,ab,kf. or varicocoele*.ti,ab,kf. |
6506 |
|
3 |
exp Microsurgery/ or exp General Surgery/ or Urologic Surgical Procedures, Male/ or ((surgical* or surger* or radiological*) adj3 (approach* or management* or treatment* or procedure* or technique* or repair*)).ti,ab,kf. or ((micro* or inguinal* or minimal* invasive) adj3 surger*).ti,ab,kf. or (spermatic vein adj3 (embolization or embolisation)).ti,ab,kf. or microsurg*.ti,ab,kf. or palomo.ti,ab,kf. |
691417 |
|
4 |
2 and 3 |
1540 |
|
5 |
(varicocelectom* or varicocoelectom* or varicocele* repair* or varicocoele* repair*).ti,ab,kf. |
1634 |
|
6 |
4 or 5 |
2321 |
|
7 |
1 and 6 |
1228 |
|
8 |
limit 7 to yr="2000 -Current" |
935 |
|
9 |
8 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
880 |
|
10 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
727461 |
|
11 |
exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf. |
1690178 |
|
12 |
9 and 10 – SR’s |
114 |
|
13 |
(9 and 11) not 12 – RCT’s |
80 |
|
14 |
12 or 13 |
194 |