Hypogonadisme
Uitgangsvraag
Wat is de rol van behandeling van hypogonadisme bij subfertiele mannen?
De volgende onderwerpen worden behandeld in de overwegingen van deze module:
- Fysiologie van testosteronproductie
- Hypogonadisme
- Invloed exogeen testosteron
- Symptomatisch hypogonadisme behandelen zonder negatieve invloed op de fertiliteit
- Leefstijladviezen
- Medicamenteus
- Hypogonadotroop hypogonadisme en spermatogenese inductie
- Kinderwens bij gebruik van testosterontherapie ivm symptomatisch hypogonadisme
- Kinderwens bij gebruik van testosterontherapie en Klinefelter Syndroom
- Kinderwens na androgene anabole steroiden misbruik
- Kinderwens bij mannen met afwijkende semenanalyse en hormonale stimulatie
Aanbeveling
Aanbeveling-1
Gebruik geen testosterontherapie bij mannen met een actieve kinderwens.
Aanbeveling-2
Induceer spermatogenese bij congenitaal of idiopathisch hypogonadotroop hypogonadisme door middel van HCG/r-HCG injecties gecombineerd met FSH-injecties.
Aanbeveling-3
Bespreek met de patiënt dat het staken van testosteron therapie bij het merendeel van de mannen herstel van spermatogenese geeft zonder hormonale stimulatie.
Aanbeveling-4
Staak testosterontherapie minimaal 6 maanden bij een kinderwens bij patiënten met Klinefelter syndroom en staak testosterontherapie alvorens er een mTESE verricht wordt bij persisterende azoöspermie.
Aanbeveling-5
Stop het gebruik van androgene anabole steroïden bij kinderwens voor minimaal 12 maanden om na te gaan of de spermatogenese op gang komt en natuurlijke conceptie afgewacht kan worden.
Indien na 12 maanden staken van de androgene anabole steroïden oligo- of azoöspermie persisteert wordt geadviseerd de patiënt te verwijzen voor andrologisch onderzoek door een deskundig specialist.
Aanbeveling-6
Bied niet standaard hormonale stimulatie aan bij mannen met oligospermie of non obstructieve azoöspermie, met als doel de spermakwaliteit te verbeteren.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
De werkgroep heeft een literatuurstudie verricht om te achterhalen wat de rol is van behandeling van hypogonadisme bij subfertiele mannen. Er werd een systematische zoekopdracht uitgevoerd, maar deze leverde geen resultaten op die voldeden aan de selectiecriteria. Dit voornamelijk vanwege de studiepopulatie. Er was een studie die leek te voldoen aan de PICO (Wiehle 2014), maar deze bleek niet geschikt vanwege de vraagstelling. Met de opgestelde PICO beoogde de werkgroep te onderzoeken of de behandeling van laag testosteron/hypogonadisme de zaadkwaliteit kan verbeteren, echter onderzocht Wiehle (2014) of hypogonadisme te behandelen is zonder de zaadkwaliteit te verslechteren.
De onderstaande tekst is opgesteld op basis van een oriënterende zoekopdracht die is uitgevoerd door de werkgroep. De formulering en adviezen zijn tot stand gekomen in samenspraak met de gehele richtlijnwerkgroep.
Hypogonadisme bij mannen is een klinisch én biochemisch syndroom, dat wordt veroorzaakt door testosterondeficiëntie in combinatie met symptomen van testosterongebrek, zoals verminderd(e) seksueel verlangen en sexdrive (“libido”) en erecties, verlies van spiermassa en kracht, moeheid, depressieve stemming, osteoporose en een veranderd metabolisme. Op den duur kunnen daarbij ook verminderde kwaliteit van leven en schadelijke gevolgen voor multiple orgaansystemen optreden (Khera, 2016).
1. De fysiologie van testosteronproductie
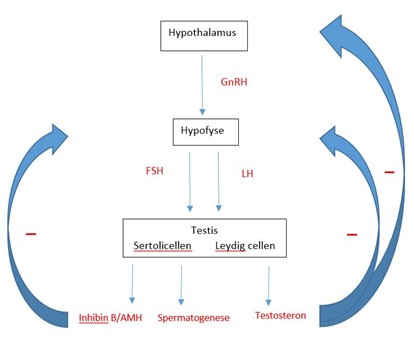
Endogene testosteronproductie wordt aangestuurd door de hypothalame-hypofysaire-gonadale as (HHG-as) (figuur 1).
De hypothalamus geeft pulsatiel gonadotrofine-releasing hormoon (GnRH) af en stimuleert daarmee de hypofysevoorkwab om de gonadotrofinen luteïniserend hormoon (LH) en follikelstimulerend hormoon (FSH) af te geven. LH stimuleert de Leydig-cellen in de testis om testosteron aan te maken. Testosteron wordt uitgescheiden in de systemische circulatie en verspreidt zich in de testikel. In de testis is de concentratie testosteron 50–100 × hoger dan in het serum. Deze hoge intratesticulaire concentratie is nodig voor de spermatogenese. Als de serum-testosteronspiegel stijgt, heeft testosteron een remmende werking (er is sprake van negatieve feedback) op zowel de hypothalamus als de hypofyse waardoor de afgifte van GnRH, LH en FSH geremd worden.
FSH stimuleert de Sertoli-cellen. Deze cellen begeleiden de kiemcellen tijdens het proces van spermatogenese en scheiden anti-Müllerian hormone (AMH) en inhibine B uit. Inhibine B heeft een remmende werking op de uitscheiding van FSH door de hypofyse (Neto, 2016). AMH beïnvloed lokale processen in de testis, zoals rijping en gevoeligheid van cellen voor andere hormonen. Er zijn aanwijzingen dat AMH via de lokale effecten in Sertoli cellen en interactie met Inhibine B indirect bijdragen aan de negatieve feedback van FSH-uitscheiding door de hypofyse.
Figuur 1. Hypothalame hypofysaire-gonadale as (HHG-as) (nTVU)
2. Hypogonadisme
Hypogonadisme komt voor in drie verschillende vormen.
- Primair hypogonadisme. Deze vorm wordt veroorzaakt door testiculaire disfunctie. De hypofyse probeert deze testiculaire disfunctie te compenseren door meer LH en FSH uit te scheiden: hypergonadotroop hypogonadisme genoemd.
- Secundair hypogonadisme. De oorzaak hiervan ligt bij de centrale aansturing. De testes worden niet adequaat gestimuleerd, wat resulteert in een hypogonadotroop hypogonadisme. Hierbij ziet men lage of laag-normale LH/FSH.
- Symptomatisch hypogonadisme door androgeen resistentie en verminderd bioactief testosteron bij androgeenreceptordefecten. Dit is een zeer zeldzame variant.
Hypogonadisme wordt beschreven in 40% van mannen die analyse ondergaan ivm subfertiliteit. In Nederland hanteert elk klinisch chemisch laboratorium een methode-specifiek referentie-interval. Sommige laboratoria hanteren ook leeftijd-specifieke referentie-intervallen. We spreken van een te laag testosteron als het totaal testosteron / vrij testosteron concentratie onder de referentie-interval van de gebruikte assay liggen.
De werkgroep verwijst naar module Endocrinologische diagnostiek voor de diagnose hypogonadisme bij de man met subfertiliteit. Hypogonadisme wordt in de context van de richtlijn mannelijke subfertiliteit gedefinieerd als totaal serum testosteron gemeten tussen 7.00 en 10.00 uur, 2 maal bepaald en beiden onder de lokale referentiewaarde.
De gouden standaard voor behandeling van hypogonadisme is testosterontherapie (TT). Exogeen testosteron heeft een negatieve invloed op de endogene testosteronproductie en spermatogenese, met subfertiliteit of onvruchtbaarheid tot gevolg. Na staken kan het 6 tot 24 maanden duren vooraleer de spermatogenese hersteld is, bij 10% van de patiënten herstelt deze zich niet. (Mulhall, 2018 & WHO, 1996)
3. De invloed van exogeen testosteron op de fertiliteit
Als exogeen testosteron toegediend wordt, stijgt het testosterongehalte in het serum en treedt er een remming op van zowel hypothalamus als hypofyse, wat resulteert in een remmend effect op de endogene aanmaak van testosteron en de spermatogenese (figuur 1).
4. Symptomatisch Hypogonadisme behandelen zonder negatieve invloed op de fertiliteit
Naast leefstijladviezen kan ook medicamenteus behandeld worden. Het enige geregistreerde middel zijn HCG-injecties. Hiernaast worden ook off label recombinant humaan choriongonadotropine (r-HCG), selectieve oestrogeenreceptor modulatoren (SERM’s = Selective Estrogen Receptor Modulators) en aromataseremmers (AI’s = aromatase inhibitors) gebruikt om endogene testosteron productie te stimuleren en spermatogenese te behouden. Ook is er onderzoek gedaan naar pulsatiele GnRH-behandeling, echter wordt dit hedendaags niet gebruikt.
Leefstijladviezen
Leefstijl aanpassingen die een positief effect op de testosteronproductie kunnen hebben zijn:
-
- Dieet en lichamelijke oefening, inclusief krachttraining
- Betere bloedsuiker controle
- Gewichtsverlies, reductie vetmassa
- Slaap
- Stressreductie
Medicamenteus
Pulsatiele GnRH-behandeling
In het verleden is onderzoek gedaan naar het gebruik van pulsatiele GnRH-behandeling. Omdat GnRH pulsatiel wordt uitgescheiden, leidt het gebruik van continue toediening van GnRH tot desensitisatie van de hypofyse met een daling van de LH- en FSH-uitscheiding. Pulsatiele GnRH-therapie kan goed werken. Deze behandeling is echter duur en kan alleen toegediend worden met een speciale pulsatiele pomp. Om deze reden wordt pulsatiele behandeling bij de man niet langer routinematig gebruikt in de klinische praktijk (Dwyer, 2015).
Human chorionic gonadotrophine / recombinant Human chorionic gonadotrophine
HCG en r-HCG imiteert de werking van LH. Met de toediening van HCG/r-HCG worden de testes gestimuleerd om testosteron te maken. HCG/r-HCG wordt 1–3 per week subcutaan of intramusculair geïnjecteerd worden met een dosis van 500–5.000 IU per keer (Nieschlag, 1997). Afhankelijk van het testosterongehalte wordt de dosering aangepast.
Momenteel is alleen humaan choriongonadotrofine (HCG) geregistreerd voor behandeling van hypogonadotroop hypogonadisme. Het wordt echter niet meer in Nederland geproduceerd en is het ook in Europa beperkt beschikbaar (Gonasi, geproduceerd in Italie, Brectavid, geproduceerd in Duitsland). Recombinant HCG is niet geregistreerd voor spermatogenese inductie of behoud en behandeling van hypogonadisme maar wordt off-label gebruikt voor deze indicatie.
Selectieve oestrogeenreceptormodulatoren (SERM’s) en aromatase inhibitors (AI’s)
De werking van SERM’s en AI’s zijn gebaseerd op het verhogen van de LH. LH stimuleert de testosteronproductie van de testes. Vaak gebruikte SERM’s zijn Clomifeencitraat en Tamoxifen, een vaak gebruikte aromatase inhibitor is Anastrozole. Testosteron wordt in perifeer vetweefsel door aromatisering omgezet in oestradiol. 10–20% van het circulerende oestradiol wordt direct geproduceerd door de Leydig-cellen in de testes. Zowel testosteron als oestradiol hebben een remmende werking op de hypothalamus en de hypofyse (figuur 2). SERM’s bezetten de oestrogeenreceptoren in de hypothalamus en de hypofyse, wat zorgt voor een verhoogde uitscheiding van LH en FSH en zo voor een verhoogde testosteronaanmaak. AI’s remmen de omzetting van testosteron in oestradiol. Hierdoor daalt de oestradiolspiegel en wordt de remmende werking op de hypothalamus en hypofyse verminderd en stijgt de LH- en FSH-uitscheiding. (Nieschlag, 1997).

Figuur 2. Het werkingsmechanisme van SERMs en AI’s. (nTVU)
5. Hypogonadotroop hypogonadisme Spermatogenese inductie
Kallmann syndroom, is een x-linked recessieve afwijking en geassocieerd met anosmie en het gebrek aan endogene GnRH-secretie door een ANOS1 mutatie. Daarnaast bestaat er ook een idiopatische hypogonadotroop hypogonadisme (IHH) variant, veroorzaakt door verscheidene genetische afwijkingen met verschillende overervingspatronen, maar vaak zonder anosmie. Genetische diagnostiek door middel van een specifiek genpanel is geïndiceerd bij hypogonadotroop hypogonadisme en kan bij ~50% verklarende varianten voor secundair hypogonadisme opleveren.
Spermatogeneseinductie bij mannen met hypogonadotroop hypogonadisme vindt plaats via HCG/r-HCG injecties 500-5000IU 1-3x per week om de testosteronproductie op gang te brengen (Nieschlag 1997), gevolgd door FSH-injecties 75-150IU 3x per week. Ook kan er gekozen worden om HCG en FSH tegelijkertijd te starten. Er wordt geen verschil gezien in het gebruik van HCG of rHCG (Neto, 2016). Bij sommige patiënten is alleen HCG/r-HCG toediening afdoende om de spermatogenese op gang te brengen, voor de meeste patiënten leidt combinatie therapie tot de kortste tijd tot spermatogenese inductie (Pozzi, 2025).
Het testisvolume bij aanvang van de therapie is een positieve prognostische factor voor spermatogenese inductie. Langdurig TT gebruik in het verleden kan mogelijk een negatief effect op herstel van spermatogenese hebben.
De werkgroep stelt vast dat in de Nederlandse praktijk voor spermatogenese inductie door een deskundig specialist eerst gestart wordt met HCG 3x 1500IU. Afhankelijk van het testosterongehalte wordt deze dosering aangepast. Na het bereiken van een adequaat testosteron wordt FSH toegevoegd 3x per week 150IE. Voor de eerste semenanalyse wordt minimaal 3 maanden gestimuleerd met FSH.
De kans op een succesvolle spermatogenese inductie is 75%, (Rastrelli, 2014) na gemiddeld 11 maanden gonadotrofinen suppletie.
Indien er azoöspermie persisteert bij een adequaat testosterongehalte en FSH-suppletie kan een microscopische Testiculaire Sperma Extractie (TESE) verricht worden. Het advies is minimaal 12-24 maanden te stimuleren alvorens een TESE te verrichten.
In Nederland is puberteitsinductie van jongens met pubertas tarda of uitblijvende puberteit omschreven door middel van testosteron of gonadotrofinen die na inductie wordt omgezet naar testosteronsuppletie. Het is onduidelijk of de behandeling in de puberteit met HCG en FSH tot een hogere kans op fertiliteit leidt op volwassen leeftijd dan direct testosteronbehandeling. Het voordeel van de gonadotrofinen behandeling is wel dat de testis groeien in volume en dat de tijd tot spermatogenese inductie bij hervatten van gonadotrofinen suppletie bij kinderwens verkort wordt.
6. Kinderwens bij gebruik van testosterontherapie in verband met symptomatisch hypogonadisme
Bij mannen die TT gebruiken en een kinderwens hebben zal de testosterontherapie gestopt moeten worden. Bij het merendeel van de mannen zal de spermatogenese herstellen in 6-12 maanden na staken TT. Bij sommige mannen zal dit herstel langer op zich laten wachten of in 10% zelfs niet optreden. Een hoger leeftijd van de patiënt en de duur van TT-therapie kan een negatief effect hebben op het herstel van spermatogenese.
Studies waar testosteron als een anticonceptie gebruikt werd, toonden aan dat de zaadcelconcentratie gemiddeld na 4,6 maanden hersteld. Velen hadden echter een langere tijd nodig tot herstel; in 67% van deze mannen herstelde de zaadcelconcentratie na 6 maanden, 90% na 12 maanden en 100% na 24 maanden (Liu, 2006). Deze studie bevatte mannen die bewezen fertiel waren zonder hypogonadisme. De vraag is dan ook of deze getallen naar een populatie van mannen met symptomatisch hypogonadisme en TT vertaald kunnen worden.
Ten tijde van het stoppen van TT of om klachten van symptomatisch hypogonadisme op te vangen kunnen patiënten eventueel ondersteund worden door het off-label toedienen van een SERM of AI met als doel om het herstel van endogene testosteronproductie te versnellen. De werkgroep stelt vast dat er geen gerandomiseerd onderzoek is verricht naar de effectiviteit van deze strategie, maar dat dit bij mannen die TT staken i.v.m. kinderwens in de Nederlandse en internationale praktijk toegepast wordt.
Behandeling met HCG om klachten van hypogonadisme op te vangen zijn controversieel, mede derhalve beveelt de werkgroep de behandeling middels HCG niet aan.
Indien de spermatogenese na 6-12 maanden staken niet op gang komt wordt geadviseerd verder onderzoek te doen.
7. Kinderwens bij gebruik van testosterontherapie en Klinefelter Syndroom
Mannen met Klinefelter Syndroom en kinderwens of de wens tot fertiliteit preservatie die TT gebruiken, kunnen onder begeleiding van een deskundige op dit gebied staken met TT. De werkgroep is van mening dat de begeleiding van deze patiënten het meest op zijn plaats is in een TESE-centrum. De kans op vinden van zaadcellen in het ejaculaat bij mannen met KS die geen TT gebruiken is hooguit 8% (Selice, 2010).
De werkgroep beveelt aan om TT tenminste 6 maanden te staken bij mannen met KS. Als er geen zaadcellen in het ejaculaat gevonden worden, stelt de werkgroep microTESE voor na tenminste 6 maanden staken TT.
In sommige studies wordt hypogonadisme in verband gebracht met lagere Sperm Retrieval Rate (SRR) bij mannen met KS (Rohayem, 2015). In veel landen wordt hormonale stimulatie met HCG of SERM gestart zowel na staken van TT als in KS-mannen die TT naief zijn. Er is geen gerandomiseerd onderzoek dat bewijst dat de SRR verbetert oiv hormonale stimulatie en endogene Totaal testosteron titratie. Er zijn ook studies die geen associatie vinden tussen SRR en endogene T levels of voorgaande TT-behandeling (Pozzi, 2020).
Een mogelijke verklaring voor ontbreken van effect van hormonale stimulatie is dat focale spermatogenese bij KS afhankelijk is van testiculair mozaicisme van spermatogoniale stamcellen en Sertoli cellen (Deebel, 2020). Dit zou een gevonden positief verband tussen AMH en SRR bij KS patienten kunnen verklaren (Renault, 2022). Anderzijds zou het ook kunnen dat de gevoeligheid van somatische cellen in de testis van mannen met KS voor exogene hormonale stimulatie individueel bepaald is (Liu, 2023).
8. Kinderwens na androgene anabole steroiden misbruik
Het fysiologische herstel van de HHG-as en dus de endogene testosteron productie en spermatogenese inductie na het staken van androgene anabole steroiden (AAS) misbruik is variabel en hangt af van de leeftijd van de patiënt, de duur en ernst van AAS misbruik (Solanki, 2023 & Vilar Neto, 2021) Er is discrepantie in studie uitkomsten van compleet herstel in korte tijd, versus geen herstel na langere tijd. Uit onderzoek lijkt ook dat herstel van de fertiliteit en het herstel van de testosteronaanmaak niet altijd gelijk is (Vilar Neto, 2021).
Na een periode van AAS misbruik wordt er vaak gesproken van “post exposure therapie” met een SERM of HCG-injecties om het herstel van spermatogenese te verspoedigen, echter is er hier geen wetenschappelijk bewijs voor (Smit, 2021).
Ondanks het ontbreken van bewijs voor kortere tijd tot herstel van symptomen of terugkeer van spermatogenese beschrijft de “Leidraad diagnostiek en behandeling van gezondheidsschade als gevolg van misbruik van androgene anabole steroïden” (Gonaden - Nederlandse Vereniging voor Endocrinologie) stimulatie van de endogene testosteronproductie door middel van Tamoxifen 20mg of Clomifeen 50mg dagelijks voor enkele weken bij mannen die symptomen van staken van anabolen niet goed verdragen. Indien na 6-12 maanden staken van de AAS azoöspermie of extreme oligospermie persisteert wordt geadviseerd verder onderzoek te doen door een deskundig specialist op dit gebied (Leidraad diagnostiek en behandeling van gezondheidsschade als gevolg van misbruik van androgene anabole steroïden (AAS), 2021).
Voor hulp bij staken van anabolen misbruik en klachten reductie kan een patiënt doorverwezen worden naar een gespecialiseerde anabolen kliniek.
9. Kinderwens bij mannen met afwijkende semenanalyse en hormonale stimulatie
Ondanks het ontbreken van prospectief gerandomiseerd onderzoek, wordt nationaal en internationaal bij mannen met oligospermie of niet-obstructieve azoöspermie empirisch hormonale stimulatie aangeboden (HCG, SERM, AI) met als doel de endogene testosteron productie te verhogen en spermatogenese te stimuleren of de kans op het vinden van zaadcellen bij TESE te verhogen. Echter weten we dat de intratesticulaire testosteronspiegel niet correleert met de serum testosteronconcentraties.
Sommige studies laten een mogelijk positief effect op de semenkwaliteit zien. (Huijben, 2023) andere studies geen verbetering of niet significant (Al Wattar, 2024) Daarnaast is er geen bewijs dat het een positief effect heeft op de zwangerschapskans (Khashaba, 2025).
Een dataset van 1644 mannen met NOA en biochemisch hypogonadisme toont dat in deze groep hormonale stimulatie met Clomifeencitraat of HCG, AI of combinatie therapie in respectievelijk 30%, 37% en 17% te overwegen zou zijn op basis van hun hormonale profiel (Pozzi, 2025).
Met de huidige bewijslast adviseert de werkgroep geen standaard hormonale stimulatie met als doel de spermatogenese te stimuleren of de kans op het vinden van zaadcellen bij TESE te verhogen.
Waarden en voorkeuren van patiënten (en eventueel hun partner)
Vertel de patiënt met een symptomatisch hypogonadisme én een actieve kinderwens waarom er geen testosterontherapie gestart wordt. Of dat de therapie moet worden gestopt omdat het een remmend effect heeft op de endogene aanmaak van testosteron en de spermatogenese. Leg uit dat eventueel wel HCG-therapie gestart kan worden, of off label een SERM of AI en wat deze therapie inhoudt. Benoem dat na het stoppen met testosterontherapie in verband met een actieve kinderwens, de patiënt hypogonadale klachten kan ervaren zoals verminderd seksueel verlangen (“libido”), gebrek aan energie of stemmingswisselingen.
Kostenaspecten
Niet van toepassing.
Gelijkheid ((health) equity/equitable)
Door hypogonadisme te behandelen ervaren mannen met hypogonadisme minder klachten en een betere kwaliteit van leven.
Aanvaardbaarheid
Niet van toepassing.
Duurzaamheid
Niet van toepassing.
Haalbaarheid
Niet van toepassing.
Rationale van aanbeveling-1: weging van argumenten voor en tegen de interventies
Testosteron therapie heeft een remmend effect heeft op de endogene aanmaak van testosteron en de spermatogenese.
Eindoordeel:
Sterke aanbeveling tegen testosterontherapie bij mannen met een actieve kinderwens.
Rationale van aanbeveling-2: weging van argumenten voor en tegen de interventies
Spermatogenese inductie bij congenitaal of idiopathisch hypogonadotroop hypogonadisme heeft een hoge kans van slagen, ook wanneer dit wordt ingezet na staken van testosteron therapie.
Eindoordeel:
Sterke aanbeveling voor het induceren van spermatogenese bij congenitaal of idiopatisch hypogonadotroop hypogonadisme door middel van HCG/r-HCG injecties gecombineerd met FSH-injecties.
Rationale van aanbeveling-3: weging van argumenten voor en tegen de interventies
Na staken van testosteron therapie voor andere indicaties dan hypogonadotroop hypogonadisme keert de spermatogenese bij het merendeel van de mannen terug. De duur van testosteron therapie en mate van testiculair falen kunnen herstel van spermatogenese negatief beïnvloeden.
Eindoordeel:
Zwakke aanbeveling voor bespreken van staken van testosteron therapie.
Rationale van aanbeveling-4: weging van argumenten voor en tegen de interventies
Patiënten met Klinefelter syndroom hebben zelden zaadcellen in het ejaculaat. Dit kan beoordeeld worden onderzocht als eventuele testosteron therapie tenminste 6 maanden gestaakt is.
Eindoordeel:
Sterke aanbeveling voor het staken van testosteron therapie bij patiënten met Klinefelter syndroom en een kinderwens.
Rationale van aanbeveling-5: weging van argumenten voor en tegen de interventies
Androgene anabole steroïden hebben een tijdelijk effect op de spermatogenese, maar de duur en intensiteit van anabolen gebruik kan de terugkeer van spermatogenese beïnvloeden. Ook kan onderliggend testiculair falen persisterende oligo- of azoöspermie verklaren.
Eindoordeel:
Sterke aanbeveling voor het stoppen met androgene anabolen steroïden.
Rationale van aanbeveling-6: weging van argumenten voor en tegen de interventies
Er is geen gerandomiseerd onderzoek dat bewijslast levert dat de kans op een kind hoger wordt bij mannen met oligospermie of de sperm retrieval rate verbeterd bij TESE bij NOA, na hormonale stimulatie.
Eindoordeel:
Zwakke aanbeveling tegen het gebruik van hormonale stimulatie bij mannen met oligospermie of non obstructieve azoöspermie.
Onderbouwing
In men with symptomatic hypogonadism, there is an indication to treat based on complaints. Testosterone supplementations deteriorates sperm production. Hormonal stimulation in asymptomatic men with low testosterone and oligo- or azoospermia might improve sperm quality or even induce spermatogenesis.
We conducted two PICOs to summarize evidence for hormonal treatment in subfertile men with hypogonadism. Unfortunately, the systematic search based on these PICOs did not yield any results that met the selection criteria.
Description of studies
A systematic search was conducted, but it did not yield any results that met the selection criteria.
A systematic review of the literature was performed to answer the following question:
What are the benefits of treatment of hypogonadism (through hormone stimulation) compared to no treatment for subfertile men with hypergonadotropic/normogonadotropic hypogonadism?
PICO 1
| P: | Subfertile men with hypergonadotropic/normogonadotropic hypogonadism and subfertility |
| I: | Treatment of hypogonadism, hormone stimulation |
| C: | No treatment |
| O: | Chance of ongoing pregnancy (with and without ART), sperm quality, less invasive assisted reproductive technology (ART), improvement in semen parameters |
PICO 2
| P: | Subfertile men with hypergonadotropic/normogonadotropic hypogonadism prior to TESE (testicular sperm extraction) |
| I: | Treatment of hypogonadism, hormone stimulation |
| C: | No treatment |
| O: | Sperm quality, chance of ongoing pregnancy (with and without ART) |
Relevant outcome measures
The guideline development group considered sperm quality as a critical outcome measure for decision making; and chance of ongoing pregnancy, less invasive assisted reproductive technology and improvement in semen parameters as important outcome measures for decision making.
A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
The guideline panel defined 25% difference (RR <0.8 to >1.25) for dichotomous and 0.5 SD for continuous outcomes as a minimal clinically (patient) important difference.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2000 until the 26th of February, 2024. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 430 hits. Studies were selected based on the following criteria:
- The study population had to meet the criteria as defined in the PICO.
- The intervention had to meet the criteria as defined in the PICO.
- Research type: systematic review, randomized-controlled trials or observational studies about treatment of hypogonadism compared to no treatment
- Articles written in English or Dutch.
One hundred and five studies were initially selected based on title and abstract screening. After reading eighteen studies in full text, eighteen studies were excluded (see the table with reasons for exclusion under the tab Methods), and no studies were included.
Results
None of the studies identified in the search matched the PICO. Therefore, no studies were included in the analysis of literature, and no evidence tables or risk-of-bias tables were created.
- Al Wattar BH, Rimmer MP, Teh JJ, Mackenzie SC, Ammar OF, Croucher C, Anastasiadis E, Gordon P, Pacey A, McEleny K, Sangster P. Pharmacological non-hormonal treatment options for male infertility: a systematic review and network meta-analysis. BMC Urol. 2024 Jul 29;24(1):158. doi: 10.1186/s12894-024-01545-1. Erratum in: BMC Urol. 2025 Jul 18;25(1):174. doi: 10.1186/s12894-025-01874-9. PMID: 39075435; PMCID: PMC11285325.
- Deebel NA, Bradshaw AW, Sadri-Ardekani H. Infertility considerations in klinefelter syndrome: From origin to management. Best Pract Res Clin Endocrinol Metab. 2020 Dec;34(6):101480. doi: 10.1016/j.beem.2020.101480. Epub 2020 Dec 15. PMID: 33358481.
- Dwyer AA, Raivio T, Pitteloud N. Gonadotrophin replacement for induction of fertility in hypogonadal men. Best Pract Res Clin Endocrinol Metab. 2015 Jan;29(1):91-103. doi: 10.1016/j.beem.2014.10.005. Epub 2014 Oct 27. PMID: 25617175.
- Huijben M, Huijsmans RLN, Lock MTWT, de Kemp VF, de Kort LMO, van Breda JHMK. Clomiphene citrate for male infertility: A systematic review and meta-analysis. Andrology. 2023 Sep;11(6):987-996. doi: 10.1111/andr.13388. Epub 2023 Jan 29. PMID: 36680549.
- Khashaba S, Khashaba S, Krishan A, Bruce A, Almaghlouth A, Huang J, Mima M, Niederberger C. Efficacy of clomiphene citrate and tamoxifen on pregnancy rates in idiopathic male subfertility: A systematic review and meta-analysis. Asian J Urol. 2025 Jan;12(1):15-22. doi: 10.1016/j.ajur.2024.09.001. Epub 2024 Sep 17. PMID: 39990067; PMCID: PMC11840313.
- Liu H, Zhang Z, Gao Y, Lin H, Zhu Z, Zheng H, Ye W, Luo Z, Qing Z, Xiao X, Hu L, Zhou Y, Zhang X. Leydig cell metabolic disorder act as a new mechanism affecting for focal spermatogenesis in Klinefelter syndrome patients: a real world cross-sectional study base on the age. Front Endocrinol (Lausanne). 2023 Nov 1;14:1266730. doi: 10.3389/fendo.2023.1266730. PMID: 38027184; PMCID: PMC10650597.
- Liu PY, Swerdloff RS, Christenson PD, Handelsman DJ, Wang C, Hormonal Male Contraception Summit G. Rate, extent, and modifiers of spermatogenic recovery after hormonal male contraception: an integrated analysis. Lancet. 2006;367(9520):1412-20.
- Khera M, Adaikan G, Buvat J, Carrier S, El-Meliegy A, Hatzimouratidis K, McCullough A, Morgentaler A, Torres LO, Salonia A. Diagnosis and Treatment of Testosterone Deficiency: Recommendations From the Fourth International Consultation for Sexual Medicine (ICSM 2015). J Sex Med. 2016 Dec;13(12):1787-1804. doi: 10.1016/j.jsxm.2016.10.009. PMID: 27914560.
- Mulhall JP, Trost LW, Brannigan RE, Kurtz EG, Redmon JB, Chiles KA, Lightner DJ, Miner MM, Murad MH, Nelson CJ, Platz EA, Ramanathan LV, Lewis RW. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018 Aug;200(2):423-432. doi: 10.1016/j.juro.2018.03.115. Epub 2018 Mar 28. PMID: 29601923.
- Neto FT, Bach PV, Najari BB, Li PS, Goldstein M. Spermatogenesis in humans and its affecting factors. Semin Cell Dev Biol. 2016 Nov;59:10-26. doi: 10.1016/j.semcdb.2016.04.009. Epub 2016 Apr 30. PMID: 27143445.
- Nieschlag E, Behre HM. Andrology. Berlin: Springer; 1997.
- Pozzi E, Boeri L, Capogrosso P, Palmisano F, Preto M, Sibona M, Franceschelli A, Ruiz-Castañé E, Sarquella-Geli J, Bassas-Arnau L, Scroppo FI, Gentile G, Falcone M, Timpano M, Ceruti C, Gadda F, Colombo F, Rolle L, Gontero P, Montorsi F, Sánchez-Curbelo J, Montanari E, Salonia A. Rates of hypogonadism forms in Klinefelter patients undergoing testicular sperm extraction: A multicenter cross-sectional study. Andrology. 2020 Nov;8(6):1705-1711. doi: 10.1111/andr.12843. Epub 2020 Jul 3. PMID: 32558292.
- Pozzi E, Venigalla G, Raymo A, Ila V, Achermann APP, Esteves SC, Salonia A, Ramasamy R. Eligibility for the medical therapy among men with non-obstructive azoospermia-Findings from a multi-centric cross-sectional study. Andrology. 2025 Feb;13(2):234-242. doi: 10.1111/andr.13670. Epub 2024 May 28. PMID: 38804793.
- Rastrelli G, Corona G, Mannucci E, Maggi M. Factors affecting spermatogenesis upon gonadotropin-replacement therapy: a meta-analytic study. Andrology. 2014 Nov;2(6):794-808. doi: 10.1111/andr.262. Epub 2014 Oct 1. PMID: 25271205.
- Renault L, Labrune E, Giscard d'Estaing S, Cuzin B, Lapoirie M, Benchaib M, Lornage J, Soignon G, de Souza A, Dijoud F, Fraison E, Pral-Chatillon L, Bordes A, Sanlaville D, Schluth-Bolard C, Salle B, Ecochard R, Lejeune H, Plotton I. Delaying testicular sperm extraction in 47,XXY Klinefelter patients does not impair the sperm retrieval rate, and AMH levels are higher when TESE is positive. Hum Reprod. 2022 Oct 31;37(11):2518-2531. doi: 10.1093/humrep/deac203. PMID: 36112034; PMCID: PMC9627253.
- Rohayem J, Fricke R, Czeloth K, Mallidis C, Wistuba J, Krallmann C, Zitzmann M, Kliesch S. Age and markers of Leydig cell function, but not of Sertoli cell function predict the success of sperm retrieval in adolescents and adults with Klinefelter's syndrome. Andrology. 2015 Sep;3(5):868-75. doi: 10.1111/andr.12067. Epub 2015 Jul 31. PMID: 26235799.
- Selice R, Di Mambro A, Garolla A, Ficarra V, Iafrate M, Ferlin A, Foresta C. Spermatogenesis in Klinefelter syndrome. J Endocrinol Invest. 2010 Dec;33(11):789-93. doi: 10.1007/BF03350343. Epub 2010 Mar 22. PMID: 20332707.
- Smit DL, Buijs MM, de Hon O, den Heijer M, de Ronde W. Disruption and recovery of testicular function during and after androgen abuse: the HAARLEM study. Hum Reprod. 2021 Mar 18;36(4):880-890. doi: 10.1093/humrep/deaa366. PMID: 33550376.
- Solanki P, Eu B, Smith J, Allan C, Lee K. Physical, psychological and biochemical recovery from anabolic steroid-induced hypogonadism: a scoping review. Endocr Connect. 2023 Oct 19;12(12):e230358. doi: 10.1530/EC-23-0358. PMID: 37855241; PMCID: PMC10620455.
- Vilar Neto JO, da Silva CA, Bruno da Silva CA, Pinto DV, Caminha JSR, de Matos RS, Nunes Filho JCC, Alves FR, Magalhães SC, De Francesco Daher E. Anabolic androgenic steroid-induced hypogonadism, a reversible condition in male individuals? A systematic review. Andrologia. 2021 Aug;53(7):e14062. doi: 10.1111/and.14062. Epub 2021 Apr 22. PMID: 33887077.
- World Health Organization Task Force on Methods for the Regulation of Male Fertility. Contraceptive efficacy of testosterone-induced azoospermia and oligozoospermia in normal men. Fertil Steril. 1996 Apr;65(4):821-9. Erratum in: Fertil Steril 1996 Jun;65(6):1267. PMID: 8654646.
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Abbasi H, Dadkhah A, Moshtaghi D, Hamiditabar MA. Gonadotropins in infertile men with idiopathic hypogonadotropic hypogonadism. International Journal of Fertility and Sterility. 2008 Nov 1;2(3):113-4. |
No comparison |
|
Adamopoulos DA, Pappa A, Billa E, Nicopoulou S, Koukkou E, Michopoulos J. Effectiveness of combined tamoxifen citrate and testosterone undecanoate treatment in men with idiopathic oligozoospermia. Fertil Steril. 2003 Oct;80(4):914-20. doi: 10.1016/s0015-0282(03)01123-3. PMID: 14556812. |
Does not match with PICO: no distinction is made between hypogonadism or not |
|
Ahmadi-Asrbadr Y, Hemmati-Ghavshough M, Khanzadeh N, Ansari F, Mohammad-Rahimi M. Comparison of the effect of combined therapy of HCG ampule and letrozole tablet with each method separately on the spermogram parameters in the obese men with idiopathic infertility: a clinical trial. Am J Clin Exp Urol. 2022 Aug 15;10(4):258-265. PMID: 36051612; PMCID: PMC9428570. |
Wrong comparison: comparison between Letrozole, HCG or combination of both |
|
Alder NJ, Keihani S, Stoddard GJ, Myers JB, Hotaling JM. Combination therapy with clomiphene citrate and anastrozole is a safe and effective alternative for hypoandrogenic subfertile men. BJU Int. 2018 Oct;122(4):688-694. doi: 10.1111/bju.14390. Epub 2018 Jun 6. PMID: 29873446. |
No comparison |
|
Alkandari MH, Zini A. Medical management of non-obstructive azoospermia: A systematic review. Arab J Urol. 2021 Jul 24;19(3):215-220. doi: 10.1080/2090598X.2021.1956233. PMID: 34552772; PMCID: PMC8451648. |
No comparison |
|
Alrabeeah K, Addar A, Alothman A, Melha SA, Alkhayal A. Effect of hormonal manipulation using clomiphene citrate prior to microdissection testicular sperm retrieval. Urol Ann. 2021 Jul-Sep;13(3):254-257. doi: 10.4103/UA.UA_129_20. Epub 2021 Jul 14. PMID: 34421260; PMCID: PMC8343278. |
No hypogonadism |
|
Andrabi SW, Saini P, Joshi M, Mehta P, Makker GC, Mishra G, Rajender S. HCG therapy in azoospermic men with lower or borderline testosterone levels and the prognostic value of Y-deletion analysis in its outcome. Andrologia. 2022 Feb;54(1):e14251. doi: 10.1111/and.14251. Epub 2021 Oct 6. PMID: 34617300. |
Wrong comparison: pre- and post-treatment HCG therapy |
|
Bakircioglu ME, Erden HF, Ciray HN, Bayazit N, Bahçeci M. Gonadotrophin therapy in combination with ICSI in men with hypogonadotrophic hypogonadism. Reprod Biomed Online. 2007 Aug;15(2):156-60. doi: 10.1016/s1472-6483(10)60703-1. PMID: 17697490. |
No comparison |
|
Behre HM. Clinical Use of FSH in Male Infertility. Front Endocrinol (Lausanne). 2019 May 24;10:322. doi: 10.3389/fendo.2019.00322. PMID: 31178827; PMCID: PMC6543808. |
Wrong study design: narrative review |
|
Bajoria R, Chatterjee R. Hypogonadotrophic hypogonadism and diminished gonadal reserve accounts for dysfunctional gametogenesis in thalassaemia patients with iron overload presenting with infertility. Hemoglobin. 2011;35(5-6):636-42. doi: 10.3109/03630269.2011.623809. Epub 2011 Oct 28. PMID: 22035015. |
No comparison |
|
Bo SO, QIAN WP. Effectiveness of combined testosterone undecanoate with tamoxifen citrate treatment in men with idiopathic azoospermia or serious oligozoospermia. Journal of Reproduction and Contraception. 2012 Dec 1;23(4):254-8. |
No comparison |
|
Bouloux PM, Handelsman DJ, Jockenhövel F, Nieschlag E, Rabinovici J, Frasa WL, de Bie JJ, Voortman G, Itskovitz-Eldor J; FSH-CTP study group. First human exposure to FSH-CTP in hypogonadotrophic hypogonadal males. Hum Reprod. 2001 Aug;16(8):1592-7. doi: 10.1093/humrep/16.8.1592. Erratum in: Hum Reprod 2001 Dec;16(12):2727. PMID: 11473948. |
No comparison |
|
Bouloux PM, Nieschlag E, Burger HG, Skakkebaek NE, Wu FC, Handelsman DJ, Baker GH, Ochsenkuehn R, Syska A, McLachlan RI, Giwercman A, Conway AJ, Turner L, van Kuijk JH, Voortman G. Induction of spermatogenesis by recombinant follicle-stimulating hormone (puregon) in hypogonadotropic azoospermic men who failed to respond to human chorionic gonadotropin alone. J Androl. 2003 Jul-Aug;24(4):604-11. doi: 10.1002/j.1939-4640.2003.tb02712.x. PMID: 12826700. |
Wrong comparison: two treatment schemes of recFSH |
|
Bouloux P, Warne DW, Loumaye E; FSH Study Group in Men's Infertility. Efficacy and safety of recombinant human follicle-stimulating hormone in men with isolated hypogonadotropic hypogonadism. Fertil Steril. 2002 Feb;77(2):270-3. doi: 10.1016/s0015-0282(01)02973-9. PMID: 11821082. |
No comparison |
|
Cakan M, Aldemir M, Topcuoglu M, Altuğ U. Role of testosterone/estradiol ratio in predicting the efficacy of tamoxifen citrate treatment in idiopathic oligoasthenoteratozoospermic men. Urol Int. 2009;83(4):446-51. doi: 10.1159/000251186. Epub 2009 Dec 8. PMID: 19996653. |
Not matching with PICO: about ratio; no cut-off value for progesterone |
|
Cannarella R, Condorelli RA, Mongioì LM, Barbagallo F, Calogero AE, La Vignera S. Effects of the selective estrogen receptor modulators for the treatment of male infertility: a systematic review and meta-analysis. Expert Opin Pharmacother. 2019 Aug;20(12):1517-1525. doi: 10.1080/14656566.2019.1615057. Epub 2019 May 23. PMID: 31120775. |
No comparison |
|
Cavallini G, Biagiotti G, Bolzon E. Multivariate analysis to predict letrozole efficacy in improving sperm count of non-obstructive azoospermic and cryptozoospermic patients: a pilot study. Asian J Androl. 2013 Nov;15(6):806-11. doi: 10.1038/aja.2013.99. Epub 2013 Oct 14. PMID: 24121976; PMCID: PMC3854065. |
No hypogonadism |
|
Chua ME, Escusa KG, Luna S, Tapia LC, Dofitas B, Morales M. Revisiting oestrogen antagonists (clomiphene or tamoxifen) as medical empiric therapy for idiopathic male infertility: a meta-analysis. Andrology. 2013 Sep;1(5):749-57. doi: 10.1111/j.2047-2927.2013.00107.x. PMID: 23970453. |
No hypogonadism; focused on the semen analysis abnormality |
|
Colpi GM, Francavilla S, Haidl G, Link K, Behre HM, Goulis DG, Krausz C, Giwercman A. European Academy of Andrology guideline Management of oligo-astheno-teratozoospermia. Andrology. 2018 Jul;6(4):513-524. doi: 10.1111/andr.12502. PMID: 30134082. |
Wrong study design: guideline |
|
Crosnoe-Shipley LE, Elkelany OO, Rahnema CD, Kim ED. Treatment of hypogonadotropic male hypogonadism: Case-based scenarios. World J Nephrol. 2015 May 6;4(2):245-53. doi: 10.5527/wjn.v4.i2.245. PMID: 25949938; PMCID: PMC4419134. |
No comparison |
|
Del Giudice F, Busetto GM, De Berardinis E, Sperduti I, Ferro M, Maggi M, Gross MS, Sciarra A, Eisenberg ML. A systematic review and meta-analysis of clinical trials implementing aromatase inhibitors to treat male infertility. Asian J Androl. 2020 Jul-Aug;22(4):360-367. doi: 10.4103/aja.aja_101_19. PMID: 31621654; PMCID: PMC7406101. |
Only 1 study matching with PICO which was also found in search |
|
Delu A, Kiltz RJ, Kuznetsov VA, Trussell JC. Clomiphene citrate improved testosterone and sperm concentration in hypogonadal males. Syst Biol Reprod Med. 2020 Dec;66(6):364-369. doi: 10.1080/19396368.2020.1822457. Epub 2020 Oct 12. PMID: 33043679. |
Wrong comparison: before and after clomiphene citrate treatment |
|
de Silva NL, Dissanayake H, Suarez C, Wickramarachchi RE, Ramasamy R, Dhillo WS, Minhas S, Corona G, Jayasena CN. Effect of oestrogen modulation on semen parameters in men with secondary hypogonadism: Systematic review and meta-analysis. Andrology. 2024 Feb;12(2):259-276. doi: 10.1111/andr.13480. Epub 2023 Jun 28. PMID: 37306109. |
No comparison |
|
Earl JA, Kim ED. Enclomiphene citrate: A treatment that maintains fertility in men with secondary hypogonadism. Expert Rev Endocrinol Metab. 2019 May;14(3):157-165. doi: 10.1080/17446651.2019.1612239. Epub 2019 May 7. PMID: 31063005. |
Wrong study design: narrative review |
|
El Meliegy A, Motawi A, El Salam MAA. Systematic review of hormone replacement therapy in the infertile man. Arab J Urol. 2017 Dec 30;16(1):140-147. doi: 10.1016/j.aju.2017.11.011. PMID: 29713545; PMCID: PMC5922183. |
Wrong study design: narrative review |
|
ElSheikh MG, Hosny MB, Elshenoufy A, Elghamrawi H, Fayad A, Abdelrahman S. Combination of vitamin E and clomiphene citrate in treating patients with idiopathic oligoasthenozoospermia: A prospective, randomized trial. Andrology. 2015 Sep;3(5):864-7. doi: 10.1111/andr.12086. Epub 2015 Jul 31. PMID: 26235968. |
Wrong comparison: comparison between vitamin E, clomiphene citrate or combination of both drugs |
|
Farmakiotis D, Farmakis C, Rousso D, Kourtis A, Katsikis I, Panidis D. The beneficial effects of toremifene administration on the hypothalamic-pituitary-testicular axis and sperm parameters in men with idiopathic oligozoospermia. Fertil Steril. 2007 Oct;88(4):847-53. doi: 10.1016/j.fertnstert.2006.12.038. Epub 2007 Apr 6. PMID: 17412336. |
Wrong comparison: before and after toremifene treatment |
|
Fink J, Schoenfeld BJ, Hackney AC, Maekawa T, Horie S. Human chorionic gonadotropin treatment: a viable option for management of secondary hypogonadism and male infertility. Expert Rev Endocrinol Metab. 2021 Jan;16(1):1-8. doi: 10.1080/17446651.2021.1863783. Epub 2020 Dec 21. PMID: 33345656. |
Wrong study design: narrative review |
|
Foresta C, Selice R, Moretti A, Pati MA, Carraro M, Engl B, Garolla A. Gonadotropin administration after gonadotropin-releasing-hormone agonist: a therapeutic option in severe testiculopathies. Fertil Steril. 2009 Oct;92(4):1326-1332. doi: 10.1016/j.fertnstert.2008.07.1766. Epub 2008 Oct 1. PMID: 18829015. |
Wrong population: severe testiculopathy |
|
Giagulli VA, Triggiani V, Corona G, Carbone MD, Tafaro E, Licchelli B, Resta F, Sabbà C, Maggi M, Guastamacchia E. Effectiveness of gonadotropin administration for spermatogenesis induction in hypogonadotropic hypogonadism: a possible role of androgen receptor CAG repeat polymorphism and therapeutic measures. Endocr Metab Immune Disord Drug Targets. 2012 Sep;12(3):236-42. doi: 10.2174/187153012802002866. PMID: 22385118. |
No comparison |
|
Gül Ü, Turunç T. The Effect of Human Chorionic Gonadotropin Treatment Before Testicular Sperm Extraction in Non-Obstructive Azoospermia Non-Obstruktif Azoospermide Testiküler Sperm Ekstraksiyonu Öncesi Human Koryonik Gonadotropin Tedavisinin Etkisi. |
Does not match with PICO: unclear if population consists of hypogonadism (no distinction in testosterone values) |
|
Gregoriou O, Bakas P, Grigoriadis C, Creatsa M, Hassiakos D, Creatsas G. Changes in hormonal profile and seminal parameters with use of aromatase inhibitors in management of infertile men with low testosterone to estradiol ratios. Fertil Steril. 2012 Jul;98(1):48-51. doi: 10.1016/j.fertnstert.2012.04.005. Epub 2012 May 11. PMID: 22579129. |
Wrong comparison: letrozole versus anastrozole |
|
Gundewar T, Kuchakulla M, Ramasamy R. A paradoxical decline in semen parameters in men treated with clomiphene citrate: A systematic review. Andrologia. 2021 Feb;53(1):e13848. doi: 10.1111/and.13848. Epub 2020 Oct 27. PMID: 33108678. |
No comparison |
|
Guo F, Fang A, Fan Y, Fu X, Lan Y, Liu M, Cao S, An G. Role of treatment with human chorionic gonadotropin and clinical parameters on testicular sperm recovery with microdissection testicular sperm extraction and intracytoplasmic sperm injection outcomes in 184 Klinefelter syndrome patients. Fertil Steril. 2020 Nov;114(5):997-1005. doi: 10.1016/j.fertnstert.2020.05.043. Epub 2020 Aug 28. PMID: 32868102. |
Wrong population: Klinefelter syndrome |
|
Guo B, Li JJ, Ma YL, Zhao YT, Liu JG. Efficacy and safety of letrozole or anastrozole in the treatment of male infertility with low testosterone-estradiol ratio: A meta-analysis and systematic review. Andrology. 2022 Jul;10(5):894-909. doi: 10.1111/andr.13185. Epub 2022 Apr 26. PMID: 35438843. |
Wrong comparison: letrozole or anastrozole versus selective estrogen receptor modulators or HCG |
|
Habous M, Giona S, Tealab A, Aziz M, Williamson B, Nassar M, Abdelrahman Z, Remeah A, Abdelkader M, Binsaleh S, Muir G. Clomiphene citrate and human chorionic gonadotropin are both effective in restoring testosterone in hypogonadism: a short-course randomized study. BJU Int. 2018 Nov;122(5):889-897. doi: 10.1111/bju.14401. Epub 2018 Jun 14. PMID: 29772111. |
Wrong comparison: clomiphene citrate versus human chorionic gonadotropin or combination of both therapies |
|
Helo S, Ellen J, Mechlin C, Feustel P, Grossman M, Ditkoff E, McCullough A. A randomized prospective double‐blind comparison trial of clomiphene citrate and anastrozole in raising testosterone in hypogonadal infertile men. The journal of sexual medicine. 2015 Aug;12(8):1761-9. |
Wrong comparison: clomiphene citrate versus anastrozole |
|
Ho CC, Tan HM. Treatment of the Hypogonadal Infertile Male-A Review. Sex Med Rev. 2013 May;1(1):42-49. doi: 10.1002/smrj.4. Epub 2015 Oct 21. PMID: 27784559. |
Wrong study design: narrative review |
|
Huijben M, Huijsmans RLN, Lock MTWT, de Kemp VF, de Kort LMO, van Breda JHMK. Clomiphene citrate for male infertility: A systematic review and meta-analysis. Andrology. 2023 Sep;11(6):987-996. doi: 10.1111/andr.13388. Epub 2023 Jan 29. PMID: 36680549. |
Wrong comparison: before versus during clomiphene citrate |
|
Huijben MM, Lock MT, de Kemp VV, de Kort LL, van Breda HJ. Clomiphene Citrate a First Step to Improve Idiopathic Male Infertility: A Retrospective Analysis. Andrologia. 2023;2023(1):8743882. |
No comparison |
|
Hussein A, Ozgok Y, Ross L, Niederberger C. Clomiphene administration for cases of nonobstructive azoospermia: a multicenter study. J Androl. 2005 Nov-Dec;26(6):787-91; discussion 792-3. doi: 10.2164/jandrol.04180. PMID: 16291975. |
No comparison |
|
Jahanshahi A, Kheradmand A, Zakerkish M, Rashidi H, Goudarzian Khozani N. Success of gonadotropin replacement therapy in men with hypogonadotropin hypogonadism in urology and endocrinology clinics of Golestan Hospital in Ahvaz. Tehran University of Medical Sciences Journal. 2023 Jan 10;80(10):780-8. |
Article in Persian |
|
Jiang T, Osadchiy V, Santamaria A, Zheng MH, Modiri N, Sigalos JT, Regets KV, Mills JN, Eleswarapu SV. Initial gonadotropin levels and sperm parameters differentiate the response to clomiphene citrate in subfertile men. Transl Androl Urol. 2022 Feb;11(2):116-123. doi: 10.21037/tau-21-987. PMID: 35280658; PMCID: PMC8899152. |
No comparison |
|
Jiang T, Sigalos JT, Osadchiy V, Santamaria A, Zheng MH, Modiri N, Regets KV, Mills JN, Eleswarapu SV. Temporal Changes of Clomiphene on Testosterone Levels and Semen Parameters in Subfertile Men. World J Mens Health. 2023 Jan;41(1):198-203. doi: 10.5534/wjmh.220010. Epub 2022 Jun 13. PMID: 35791301; PMCID: PMC9826904. |
No comparison |
|
Jin X, Man C, Gong D, Fan Y. Adjuvant Treatment with Qilin Pill for Men with Oligoasthenospermia: A Meta-Analysis of Randomized Controlled Trials. Phytother Res. 2017 Sep;31(9):1291-1297. doi: 10.1002/ptr.5854. Epub 2017 Jun 21. PMID: 28635070. |
Wrong comparison: adjuvant therapy with Qilin Pill versus other treatment |
|
Jones TH, Dobs AS, Randeva H, Moore W, Parkin JM. Leflutrozole in male obesity-associated hypogonadotropic hypogonadism: Ph 2b double-blind randomised controlled trial. Eur J Endocrinol. 2023 Sep 1;189(3):297-308. doi: 10.1093/ejendo/lvad099. PMID: 37579053. |
Wrong population: Men with Obesity-associated Hypogonadotropic Hypogonadism |
|
Jungwirth A, Giwercman A, Tournaye H, Diemer T, Kopa Z, Dohle G, Krausz C; European Association of Urology Working Group on Male Infertility. European Association of Urology guidelines on Male Infertility: the 2012 update. Eur Urol. 2012 Aug;62(2):324-32. doi: 10.1016/j.eururo.2012.04.048. Epub 2012 May 3. PMID: 22591628. |
Wrong study design: guideline |
|
Kadioglu TC. Oral tamoxifen citrate treatment is more effective in normogonadotropic patients who have follicle-stimulating hormone levels within the lower half of normal. Int Urol Nephrol. 2009 Dec;41(4):773-6. doi: 10.1007/s11255-009-9568-3. Epub 2009 Apr 21. PMID: 19381855. |
Wrong comparison: before and after tamoxifen citrate |
|
Kalkanli A, Akdere H, Cevik G, Salabas E, Cilesiz NC, Kadioglu A. Hypergonadotropic Hypogonadism: Management of Infertility. Curr Pharm Des. 2021;27(24):2790-2795. doi: 10.2174/1381612826666201102110456. PMID: 33138760. |
Wrong study design: narrative review |
|
Kaminetsky J, Hemani ML. Clomiphene citrate and enclomiphene for the treatment of hypogonadal androgen deficiency. Expert Opin Investig Drugs. 2009 Dec;18(12):1947-55. doi: 10.1517/13543780903405608. PMID: 19938905. |
Wrong study design: narrative review |
|
Keihani S, Alder NJ, Cheng PJ, Stoddard GJ, Pastuszak AW, Hotaling JM. Obesity and Baseline Estradiol Levels Are Independent Predictors for Initiation of Anastrozole in Hypogonadal Men on Clomiphene Citrate. World J Mens Health. 2020 Oct;38(4):582-590. doi: 10.5534/wjmh.190160. Epub 2020 Feb 24. PMID: 32202084; PMCID: PMC7502320. |
Wrong comparison: conversion rate from clomiphene citrate to clomiphene citrate plus anastrozole |
|
Khodamoradi K, Khosravizadeh Z, Parmar M, Kuchakulla M, Ramasamy R, Arora H. Exogenous testosterone replacement therapy versus raising endogenous testosterone levels: current and future prospects. F S Rev. 2021 Jan;2(1):32-42. doi: 10.1016/j.xfnr.2020.11.001. Epub 2020 Nov 17. PMID: 33615283; PMCID: PMC7894643. |
Wrong study design: narrative review |
|
Kim ED, Crosnoe L, Bar-Chama N, Khera M, Lipshultz LI. The treatment of hypogonadism in men of reproductive age. Fertil Steril. 2013 Mar 1;99(3):718-24. doi: 10.1016/j.fertnstert.2012.10.052. Epub 2012 Dec 7. PMID: 23219010. |
Wrong study design: narrative review |
|
Kooshesh L, Bahmanpour S, Zeighami S, Nasr-Esfahani MH. Effect of Letrozole on sperm parameters, chromatin status and ROS level in idiopathic Oligo/Astheno/Teratozoospermia. Reprod Biol Endocrinol. 2020 May 13;18(1):47. doi: 10.1186/s12958-020-00591-2. PMID: 32404173; PMCID: PMC7218838. |
Wrong comparison: before and after letrozole |
|
Korani M. Aromatase inhibitors in male: A literature review. Medicina Clínica Práctica. 2023 Jan 1;6(1):100356. |
Wrong study design: narrative review |
|
La Vignera S, Condorelli RA, Duca Y, Mongioi LM, Cannarella R, Giacone F, Calogero AE. FSH therapy for idiopathic male infertility: four schemes are better than one. Aging Male. 2020 Dec;23(5):750-755. doi: 10.1080/13685538.2019.1590696. Epub 2019 Apr 3. PMID: 30942139. |
No comparison |
|
Liao Y, Chang YK, Wang SM, Chang HC. Ceiling effect of clomiphene citrate on the testosterone to estradiol ratio in eugonadal infertile men. PLoS One. 2022 Jan 31;17(1):e0262924. doi: 10.1371/journal.pone.0262924. PMID: 35100304; PMCID: PMC8803167. |
Wrong comparison: before and after clomiphene use |
|
Liu Z, Mao J, Wu X, Xu H, Wang X, Huang B, Zheng J, Nie M, Zhang H. Efficacy and Outcome Predictors of Gonadotropin Treatment for Male Congenital Hypogonadotropic Hypogonadism: A Retrospective Study of 223 Patients. Medicine (Baltimore). 2016 Mar;95(9):e2867. doi: 10.1097/MD.0000000000002867. PMID: 26945370; PMCID: PMC4782854. |
No comparison |
|
Matsumoto AM, Snyder PJ, Bhasin S, Martin K, Weber T, Winters S, Spratt D, Brentzel J, O'Dea L. Stimulation of spermatogenesis with recombinant human follicle-stimulating hormone (follitropin alfa; GONAL-f): long-term treatment in azoospermic men with hypogonadotropic hypogonadism. Fertil Steril. 2009 Sep;92(3):979-990. doi: 10.1016/j.fertnstert.2008.07.1742. Epub 2008 Oct 18. PMID: 18930190. |
No comparison |
|
Morgado A, Tsampoukas G, Sokolakis I, Schoentgen N, Urkmez A, Sarikaya S. Do "testosterone boosters" really increase serum total testosterone? A systematic review. Int J Impot Res. 2024 Jun;36(4):348-364. doi: 10.1038/s41443-023-00763-9. Epub 2023 Sep 11. PMID: 37697053. |
Wrong comparison: Eurycoma longifolia, a blend of Punica granatum fruit rind and Theobroma cacao seed extracts (Tesnor TM) and purified Shilajit extract (PrimaVie TM) |
|
Morris GC, Lloyd-Evans E, Cahill DJ. Induction of spermatogenesis in men with hypogonadotropic hypogonadism. J Assist Reprod Genet. 2021 Apr;38(4):803-807. doi: 10.1007/s10815-020-02058-0. Epub 2021 Jan 11. PMID: 33432424; PMCID: PMC8079531. |
No comparison |
|
Ortac M, Hidir M, Salabas E, Boyuk A, Bese C, Pazir Y, Kadioglu A. Evaluation of gonadotropin-replacement therapy in male patients with hypogonadotropic hypogonadism. Asian J Androl. 2019 Nov-Dec;21(6):623-627. doi: 10.4103/aja.aja_6_19. PMID: 31062720; PMCID: PMC6859661. |
No comparison |
|
Paffenholz P, Votteler S, Nazari S, Nestler T, Salem J, Grabbert M, von Brandenstein M, Loosen SH, Zey S, Heidenreich A, Herden J, Denil J. Efficacy of the Oestrogen Antagonist Tamoxifen on Sperm Parameters in Patients with Idiopathic Oligoathenoteratozoospermia. Urol Int. 2019;103(1):108-115. doi: 10.1159/000500301. Epub 2019 May 8. PMID: 31067562. |
Wrong comparison: before and after treatment with tamoxifen |
|
Panidis D, Koliakos G, Kourtis A, Rousso D, Mavromatidis G, Triantos A, Kalahanis I. Short-term human chorionic gonadotropin-induced testosterone rise does not modify leptin levels in eugonadal men. Gynecol Endocrinol. 2002 Feb;16(1):75-81. PMID: 11915586. |
No comparison |
|
Panner Selvam MK, Baskaran S, Tannenbaum J, Greenberg J, Shalaby HY, Hellstrom WJG, Sikka SC. Clomiphene Citrate in the Management of Infertility in Oligospermic Obese Men with Hypogonadism: Retrospective Pilot Study. Medicina (Kaunas). 2023 Oct 26;59(11):1902. doi: 10.3390/medicina59111902. PMID: 38003951; PMCID: PMC10673313. |
No comparison |
|
Patankar SS, Kaore SB, Sawane MV, Mishra NV, Deshkar AM. Effect of clomiphene citrate on sperm density in male partners of infertile couples. Indian J Physiol Pharmacol. 2007 Apr-Jun;51(2):195-8. PMID: 18175667. |
No comparison |
|
Patel DP, Brant WO, Myers JB, Presson AP, Johnstone EB, Dorais JA, Aston KI, Carrell DT, Hotaling JM. The safety and efficacy of clomiphene citrate in hypoandrogenic and subfertile men. Int J Impot Res. 2015 Nov-Dec;27(6):221-4. doi: 10.1038/ijir.2015.21. Epub 2015 Aug 20. PMID: 26289907. |
Wrong comparison: pre- and posttreatment clomiphene citrate |
|
Pavlovich CP, King P, Goldstein M, Schlegel PN. Evidence of a treatable endocrinopathy in infertile men. J Urol. 2001 Mar;165(3):837-41. PMID: 11176482. |
Wrong comparison: fertile control reference group |
|
Peivandi S, Jafarpour H, Abbaspour M, Ebadi A. Effect of letrozole on spermogram parameters and hormonal profile in infertile men: A clinical trial study. Endocr Regul. 2019 Oct 1;53(4):231-236. doi: 10.2478/enr-2019-0023. PMID: 31734656. |
Wrong comparison: before and after letrozole |
|
Pitteloud N, Dwyer A. Hormonal control of spermatogenesis in men: therapeutic aspects in hypogonadotropic hypogonadism. Ann Endocrinol (Paris). 2014 May;75(2):98-100. doi: 10.1016/j.ando.2014.04.002. Epub 2014 Apr 29. PMID: 24793994. |
No comparison |
|
Rahnema CD, Lipshultz LI, Crosnoe LE, Kovac JR, Kim ED. Anabolic steroid-induced hypogonadism: diagnosis and treatment. Fertil Steril. 2014 May;101(5):1271-9. doi: 10.1016/j.fertnstert.2014.02.002. Epub 2014 Mar 14. PMID: 24636400. |
No comparison |
|
Raman JD, Schlegel PN. Aromatase inhibitors for male infertility. J Urol. 2002 Feb;167(2 Pt 1):624-9. doi: 10.1016/S0022-5347(01)69099-2. PMID: 11792932. |
Wrong comparison: treatment with testolactone or anastrozole |
|
Rastrelli G, Corona G, Mannucci E, Maggi M. Factors affecting spermatogenesis upon gonadotropin-replacement therapy: a meta-analytic study. Andrology. 2014 Nov;2(6):794-808. doi: 10.1111/andr.262. Epub 2014 Oct 1. PMID: 25271205. |
No comparison |
|
Ribeiro MA, Gameiro LF, Scarano WR, Briton-Jones C, Kapoor A, Rosa MB, El Dib R. Aromatase inhibitors in the treatment of oligozoospermic or azoospermic men: a systematic review of randomized controlled trials. JBRA Assist Reprod. 2016 May 1;20(2):82-8. doi: 10.5935/1518-0557.20160019. PMID: 27244767. |
Only 1 study matching with PICO which was also found in search |
|
Rodriguez KM, Pastuszak AW, Lipshultz LI. Enclomiphene citrate for the treatment of secondary male hypogonadism. Expert Opin Pharmacother. 2016 Aug;17(11):1561-7. doi: 10.1080/14656566.2016.1204294. Epub 2016 Jul 4. PMID: 27337642; PMCID: PMC5009465. |
Wrong study design: narrative review |
|
Samli MM, Demirbas M, Guler C. Induction of spermatogenesis in idiopathic hypogonadotropic hypogonadism with gonadotropins in older men. Arch Androl. 2004 Jul-Aug;50(4):267-71. doi: 10.1080/01485010490448732. PMID: 15277005. |
No comparison |
|
Schlegel PN. Aromatase inhibitors for male infertility. Fertil Steril. 2012 Dec;98(6):1359-62. doi: 10.1016/j.fertnstert.2012.10.023. Epub 2012 Oct 25. PMID: 23103016. |
Wrong study design: narrative review |
|
Shah T, Nyirenda T, Shin D. Efficacy of anastrozole in the treatment of hypogonadal, subfertile men with body mass index ≥25 kg/m2. Transl Androl Urol. 2021 Mar;10(3):1222-1228. doi: 10.21037/tau-20-919. PMID: 33850757; PMCID: PMC8039603. |
Wrong comparison: hormonal measurements and semen analysis prior to and after treatment with anastrozole |
|
Shahid MN, Khan TM, Neoh CF, Lean QY, Bukhsh A, Karuppannan M. Effectiveness of Pharmacological Intervention Among Men with Infertility: A Systematic Review and Network Meta-Analysis. Front Pharmacol. 2021 Aug 16;12:638628. doi: 10.3389/fphar.2021.638628. PMID: 34483894; PMCID: PMC8415454. |
No studies matching with PICO |
|
Sharma D, Zillioux J, Khourdaji I, Reines K, Wheeler K, Costabile R, Kavoussi P, Smith R. Improvements in semen parameters in men treated with clomiphene citrate-A retrospective analysis. Andrologia. 2019 Jun;51(5):e13257. doi: 10.1111/and.13257. Epub 2019 Feb 18. PMID: 30779195. |
Wrong comparison: pre- and post-treatment clomiphene citrate |
|
Shinjo E, Shiraishi K, Matsuyama H. The effect of human chorionic gonadotropin-based hormonal therapy on intratesticular testosterone levels and spermatogonial DNA synthesis in men with non-obstructive azoospermia. Andrology. 2013 Nov;1(6):929-35. doi: 10.1111/j.2047-2927.2013.00141.x. Epub 2013 Oct 2. PMID: 24123916. |
Wrong comparison: before and after hCG treatment |
|
Shiraishi K, Ohmi C, Matsuyama H. Patient-reported outcomes and biochemical alterations during hormonal therapy in men with hypogonadotropic hypogonadism who have finished infertility treatment. Endocr J. 2021 Feb 28;68(2):221-229. doi: 10.1507/endocrj.EJ20-0365. Epub 2020 Oct 3. PMID: 33012744. |
Wrong comparison: hCG vs TRT treatment |
|
Shoshany O, Abhyankar N, Mufarreh N, Daniel G, Niederberger C. Outcomes of anastrozole in oligozoospermic hypoandrogenic subfertile men. Fertil Steril. 2017 Mar;107(3):589-594. doi: 10.1016/j.fertnstert.2016.11.021. Epub 2017 Jan 6. PMID: 28069178. |
Wrong comparison: pre- and posttreatment anastrozole |
|
Shuling L, Sie Kuei ML, Saffari SE, Jiayun Z, Yeun TT, Leng JPW, Viardot-Foucault V, Nadarajah S, Chan JKY, Hao TH. Do men with normal testosterone-oestradiol ratios benefit from letrozole for the treatment of male infertility? Reprod Biomed Online. 2019 Jan;38(1):39-45. doi: 10.1016/j.rbmo.2018.09.016. Epub 2018 Oct 30. PMID: 30449700. |
No comparison |
|
Sinisi AA, Esposito D, Bellastella G, Maione L, Palumbo V, Gandini L, Lombardo F, De Bellis A, Lenzi A, Bellastella A. Efficacy of recombinant human follicle stimulating hormone at low doses in inducing spermatogenesis and fertility in hypogonadotropic hypogonadism. J Endocrinol Invest. 2010 Oct;33(9):618-23. doi: 10.1007/BF03346659. Epub 2010 Apr 30. PMID: 20436264. |
Wrong comparison: rFSH versus highly purified urinary FSH |
|
Stephens SM, Polotsky AJ. Big enough for an aromatase inhibitor? How adiposity affects male fertility. Semin Reprod Med. 2013 Jul;31(4):251-7. doi: 10.1055/s-0033-1345272. Epub 2013 Jun 17. PMID: 23775380. |
Wrong study design: narrative review |
|
Surbone A, Vaucher L, Primi MP, Leyvraz C, Pitteloud N, Ballabeni P, Mathevet P, Vulliemoz N. Clomiphene citrate effect on testosterone level and semen parameters in 18 infertile men with low testosterone level and normal/low gonadotropines level. Eur J Obstet Gynecol Reprod Biol. 2019 Jul;238:104-109. doi: 10.1016/j.ejogrb.2019.05.011. Epub 2019 May 11. PMID: 31128532. |
No comparison |
|
Taylor F, Levine L. Clomiphene citrate and testosterone gel replacement therapy for male hypogonadism: efficacy and treatment cost. J Sex Med. 2010 Jan;7(1 Pt 1):269-76. doi: 10.1111/j.1743-6109.2009.01454.x. Epub 2009 Aug 17. PMID: 19694928. |
Wrong comparison: clomiphene citrate or testosterone gel replacement therapy |
|
Tharakan T, Corona G, Foran D, Salonia A, Sofikitis N, Giwercman A, Krausz C, Yap T, Jayasena CN, Minhas S. Does hormonal therapy improve sperm retrieval rates in men with non-obstructive azoospermia: a systematic review and meta-analysis. Hum Reprod Update. 2022 Aug 25;28(5):609-628. doi: 10.1093/humupd/dmac016. PMID: 35526153; PMCID: PMC9434299. |
No studies matching with PICO |
|
Thomas J, Suarez Arbelaez MC, Narasimman M, Weber AR, Blachman-Braun R, White JT, Ledesma B, Ghomeshi A, Jara-Palacios MA, Ramasamy R. Efficacy of Clomiphene Citrate Versus Enclomiphene Citrate for Male Infertility Treatment: A Retrospective Study. Cureus. 2023 Jul 6;15(7):e41476. doi: 10.7759/cureus.41476. PMID: 37546076; PMCID: PMC10404117. |
Wrong comparison: clomiphene citrate versus enclomiphene citrate |
|
Vahidi S, Abedinzadeh M, Rahavian A, Mirjalili A, Sadeghi A, Karami H, Abouei S. Does Clomiphene citrate administration increase the success rate of microdissection testicular sperm extraction in non-obstructive azoospermic men? A cross-sectional study. Int J Reprod Biomed. 2023 Dec 19;21(11):943-948. doi: 10.18502/ijrm.v21i11.14658. PMID: 38292509; PMCID: PMC10823115. |
Does not match with PICO: unclear if population consists of hypogonadism; not further described in article (no distinction in testosterone values) |
|
Vandekerckhove P, Lilford R, Vail A, Hughes E. Clomiphene or tamoxifen for idiopathic oligo/asthenospermia. Cochrane Database Syst Rev. 2000;1996(2):CD000151. doi: 10.1002/14651858.CD000151. Update in: Cochrane Database Syst Rev. 2007 Jul 18;(4):CD000151. doi: 10.1002/14651858.CD000151. PMID: 10796497; PMCID: PMC10865959. |
Withdrawal from publication |
|
Vandekerckhove P, Lilford R, Vail A, Hughes E. WITHDRAWN: Clomiphene or tamoxifen for idiopathic oligo/asthenospermia. Cochrane Database Syst Rev. 2007 Jul 18;(4):CD000151. doi: 10.1002/14651858.CD000151. PMID: 17636604. |
Withdrawal from publication |
|
Verdi A, Nasr-Esfahani MH, Forouzanfar M, Tavalaee M. The Effect of Recombinant Human Follicle-Stimulating Hormone on Sperm Quality, Chromatin Status and Clinical Outcomes of Infertile Oligozoospermic Men Candidate for Intracytoplasmic Sperm Injection: A Randomized Clinical Trial. Int J Fertil Steril. 2021 Jan;15(1):1-7. doi: 10.22074/ijfs.2021.6210. Epub 2021 Jan 19. PMID: 33497040; PMCID: PMC7838760. |
Does not match with PICO: inclusion based on FSH, no testosterone |
|
Vilar Neto JO, da Silva CA, Bruno da Silva CA, Pinto DV, Caminha JSR, de Matos RS, Nunes Filho JCC, Alves FR, Magalhães SC, De Francesco Daher E. Anabolic androgenic steroid-induced hypogonadism, a reversible condition in male individuals? A systematic review. Andrologia. 2021 Aug;53(7):e14062. doi: 10.1111/and.14062. Epub 2021 Apr 22. PMID: 33887077. |
No comparison |
|
Warne DW, Decosterd G, Okada H, Yano Y, Koide N, Howles CM. A combined analysis of data to identify predictive factors for spermatogenesis in men with hypogonadotropic hypogonadism treated with recombinant human follicle-stimulating hormone and human chorionic gonadotropin. Fertil Steril. 2009 Aug;92(2):594-604. doi: 10.1016/j.fertnstert.2008.07.1720. Epub 2008 Oct 18. PMID: 18930225. |
No comparison |
|
Wenker EP, Dupree JM, Langille GM, Kovac J, Ramasamy R, Lamb D, Mills JN, Lipshultz LI. The Use of HCG-Based Combination Therapy for Recovery of Spermatogenesis after Testosterone Use. J Sex Med. 2015 Jun;12(6):1334-7. doi: 10.1111/jsm.12890. Epub 2015 Apr 22. PMID: 25904023. |
No comparison |
|
Wheeler KM, Sharma D, Kavoussi PK, Smith RP, Costabile R. Clomiphene Citrate for the Treatment of Hypogonadism. Sex Med Rev. 2019 Apr;7(2):272-276. doi: 10.1016/j.sxmr.2018.10.001. Epub 2018 Dec 3. PMID: 30522888. |
Wrong study design: narrative review |
|
Whitten SJ, Nangia AK, Kolettis PN. Select patients with hypogonadotropic hypogonadism may respond to treatment with clomiphene citrate. Fertil Steril. 2006 Dec;86(6):1664-8. doi: 10.1016/j.fertnstert.2006.05.042. Epub 2006 Sep 27. PMID: 17007848. |
Wrong comparison: treated with either clomiphene citrate or injectable gonadotropins |
|
Yang Y, Chen S, Chen H, Guo Y, Teng X. The efficacy of anastrozole in subfertile men with and without abnormal testosterone to estradiol ratios. Transl Androl Urol. 2022 Sep;11(9):1262-1270. doi: 10.21037/tau-22-95. PMID: 36217397; PMCID: PMC9547167. |
No comparison |
|
Yang C, Li P, Li Z. Clinical application of aromatase inhibitors to treat male infertility. Hum Reprod Update. 2021 Dec 21;28(1):30-50. doi: 10.1093/humupd/dmab036. PMID: 34871401. |
Wrong study design: narrative review |
|
Yang MG, Zheng GD, Xu ZQ, Lin HL, Zhuang ZM, Zhang CX. [Qilin Pills combined with clomiphene for idiopathic oligoasthenozoospermia]. Zhonghua Nan Ke Xue. 2015 Jun;21(6):549-54. Chinese. PMID: 26242048. |
Article in Chinese |
|
Zhang L, Cai K, Wang Y, Ji W, Cheng Z, Chen G, Liao Z. The Pulsatile Gonadorelin Pump Induces Earlier Spermatogenesis Than Cyclical Gonadotropin Therapy in Congenital Hypogonadotropic Hypogonadism Men. Am J Mens Health. 2019 Jan-Feb;13(1):1557988318818280. doi: 10.1177/1557988318818280. Epub 2018 Dec 20. PMID: 30569789; PMCID: PMC6775549. |
Wrong comparison: pulsatile gonadorelin pump versus cyclical gonadotropin therapy |
|
Zhang J, Zhu Y, Zhang R, Liu H, Sun B, Zhang W, Wang X, Nie M, Mao J, Wu X. Pulsatile Gonadotropin-Releasing Hormone Therapy Is Associated With Better Spermatogenic Outcomes than Gonadotropin Therapy in Patients With Pituitary Stalk Interruption Syndrome. Endocr Pract. 2024 Feb;30(2):146-154. doi: 10.1016/j.eprac.2023.11.010. Epub 2023 Nov 28. PMID: 38029930. |
Wrong comparison: hMG/hCG and GnRH therapy |
Beoordelingsdatum en geldigheid
Publicatiedatum : 30-04-2026
Beoordeeld op geldigheid : 30-04-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met mannelijke subfertiliteit.
Werkgroep
- Cantineau A.E.P. (Astrid), gynaecoloog, subspecialist voortplantingsgeneeskunde Universitair Medisch Centrum Groningen te Groningen, NVOG
- Dinkelman-Smit M. (Marij), uroloog-androloog, Erasmus Medisch Centrum te Rotterdam, NVU
- Verberg M.F.G. (Marieke), gynaecoloog, Medisch Spectrum Twente te Enschede, NVOG
- Heida K.Y. (Karst), gynaecoloog, Dijklander ziekenhuisbte Purmerend, NVOG
- van der Houwen L.E.E. (Lisette), gynaecoloog, Radboud universitair medisch centrum te Nijmegen, NVOG
- de Bruin J.P. (Jan Peter), gynaecoloog, Jeroen Bosch Ziekenhuis te ’s Hertogenbosch, NVOG
- van Breda H.M.K. (Jetske), uroloog-androloog, Universitair Medisch Centrum Utrecht te Utrecht, NVU
- van Roijen J.H. (Herman), uroloog-androloog, voorheen ETZ Tilburg – nu gepensioneerd
- D’Hauwers K.W.M. (Kathleen), uroloog-androloog, Radboud universitair medisch centrum te Nijmegen, NVU
- Meißner A. (Andreas), uroloog-androloog, Amsterdam Universitair Medisch Centrum te Amsterdam, NVU
- Bailleux B.B.E.P. (Bart), laboratoriumspecialist Klinische Chemie en Endocrinologie, Leids Universitair Medisch Centrum te Leiden, NVKC
- Kempers M.J.E. (Marlies), klinisch geneticus, Radboud universitair medisch centrum te Nijmegen, VKGN
- van der Kevie-Kersemaekers A.M.F. (Anne-Marie), laboratoriumspecialist klinische genetica, Universitair Medisch Centrum Utrecht te Utrecht, VKGL
- Westra D. (Dineke), laboratoriumspecialist klinische genetica, Radboud universitair medisch centrum te Nijmegen, VKGL
- Ramos L. (Liliana), klinisch embryoloog, Radboud universitair medisch centrum te Nijmegen, KLEM
- Grolle R.L. (Rosanne), fertiliteitsarts, Erasmus Medisch Centrum te Rotterdam, VVF
- Sinjorgo S. (Simone), medewerker medewerker patientenperspectief wetenschappelijk onderzoek en richtlijnen, Freya (vanaf december 2024)
- Vermeulen M. (Marloes), medewerker patientenperspectief wetenschappelijk onderzoek en richtlijnen, Freya (tot december 2024)
Met ondersteuning van
- Mostovaya I.M. (Irina), senior-adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- van der Lee J.H. (Hanneke), senior-adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Middelhuis D. (Danique), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Van Bommel M. (Majke), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Schultink J.M. (Janneke), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- E. (Esther) van der Bijl, informatiespecialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel Gemelde (neven)functies en belangen werkgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaam-heden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Datum |
Restrictie |
|
Astrid Cantineau (voorzitter) |
Gynaecoloog. UMCG, 1.0 FTE |
auteur Up to date Hyperthecosis |
Geen |
Geen |
Geen |
Voorzitter SIG andrologie NVOG aanvrager subsidie ZonMw over leefstijl en mannelijke subfertiliteit |
Geen |
13/11/2022 |
Geen restricties. |
|
Marij Dinkelman-Smit (vice voorzitter) |
Staflid Uroloog-Androloog Voorzitter Voortplantingscentrum Erasmus MC Plaatsvervangend afdelingshoofd Urologie Erasmus MC Erasmus MC Universitair Medisch Centrum |
Bestuurslid Nederlandse Vereniging voor Urologie (NVU) (onbetaald) Bestuurslid multidisciplenaire Special Interest Group (SIG) Andrologie, Nederlandse Verening voor Obstetrie en Gynaecologie (NVOG) (onbetaald) Bestuurslid European Association of Urology (EAU) section for Andrological Urology (ESAU) (onbetaald) Medical director European Academy of Andrology (EAA) training center Andrology Erasmus MC (onbetaald) Lid Commissie Kwaliteitvisitatie NVU (onbetaald) Medische adviesraad Klinefelter Vereniging (onbetaald) Medische adviesraad Stichting Lichen Sclerosus (onbetaald) |
Geen |
Geen |
Geen |
Geen |
Geen |
12/12/2022 |
Geen restricties. |
|
Marieke Verberg |
Gynaecoloog, Medisch Spectrum Twente 0.5 FTE betaalde functie Gynaecoloog en statutair directeur Fertiliteitskliniek Twente 0.5 FTE betaalde functie |
Geen relevante |
Geen |
Geen |
Geen |
Geen |
Geen |
19/11/2022 |
Geen restricties. |
|
Karst Heida |
Gynaecoloog bij het Dijklander ziekenhuis - betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
7/12/2022 |
Geen restricties. |
|
Lisette van der Houwen |
Gynaecoloog - fellow voortplantingsgeneeskunde Radboudumc |
Bestuurslid SIG endometriose NVOG algemeen lid SIG ART en SIG fertiliteitspreservatie van de NVOG |
Geen |
Geen |
Merck / Impect study - improving patient-centeredness in endometriosis care. / Ja |
Geen |
Geen |
02/12/2022 |
Geen restricties, extern gefinancierd onderzoek heeft geen betrekking op richtlijn onderwerp. |
|
Jan Peter de Bruin |
Gynaecoloog Jeroen Bosch Ziekenhuis, betaald |
Waarnemend gynaecoloog Radboudumc, betaald |
Medical Advisory Board Ferring BV - De medical advisory board komt op verzoek van Ferring ongeveer eens per jaar samen. Daarbij worden ontwikkelingen in het veld en relevant studie uitkomsten bediscussieerd. Ferring gebruikt de uitkomsten van deze besprekingen als input voor hun strategie. |
- |
Ja - Het gaat om eigen onderzoek op gebied voortplantingsgeneeksunde waarvoor mijn afdeling een unrestricted research grant kreeg. Dit onderzoek bestaat uit de volgende lijnen: • het ontwikkelen en evalueren van toepassingen voor online fertilteitszorg (geen raakvlak met uit te werken modules voor deze richtlijn). • het effect van gebruik van supplementen op de zwangerschapskans bij paren met mannelijke subfertiliteit (raakvlak met module over supplementen waar de Bruin bij betrokken is als locale hoofdonderzoeker, tweede auteur van de nog te publiceren paper) Gefinincierd door Goodlife pharma |
- |
- |
26/11/2022 |
Vanwege deelname aan een adviesraad aan de start van het traject is de richtlijn tijdens de commentaarfase ook aan de Commissie Kwaliteitsdocumenten van de NVOG voorgelegd. Verder is dit lid uitgesloten van besluitvorming bij onderwerpen die raken aan de adviesraad. |
|
Jetske van Breda |
Uroloog/ Androloog UMCUtrecht |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
18/11/2022 |
Geen restricties. |
|
Kathleen D' Hauwers |
Uroloog, staflid Radboudumc: betaald |
Lid Cie Kwaliteit NVU: onbetaald Lid Cie Andrologie NVU: onbetaald Board memeber Klinefelter Vereniging Nederland: onbeteaald Cie Keuzehulp ED: vergoed |
Geen |
Geen |
Geen |
Inbrengen van expertise. Geen specifieke, persoonlijke baat bij één of ander: het gaat om de patiënt / klant. |
Geen |
28/09/2022 |
Geen restricties. |
|
Andreas Meißner |
Uroloog - Androloog Staflid Centrum voor Voortplantingsgeneeskunde, locatie AMC, en afdeling Urologie, locatie VUMC, van het Amsterdam UMC betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
24/11/2022 |
Geen restricties. |
|
Herman van Roijen |
Uroloog ETZ Tilburg |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
13/11/2022 |
Geen restricties. |
|
Bart Ballieux |
Laboratoriumspecialist Klinische Chemie en Endocrinologie Afdeling KCL, LUMC, Leiden |
Geen |
geen persoonlijke financiele belangen |
Geen relevante persoonlijke relaties die van invloed kunnen zijn op mijn adviezen |
geen |
Geen intellectuele belangen bij mijn adviezen |
Geen overige belangen |
10/01/2023 |
Geen restricties. |
|
Marlies Kempers |
Klinisch Geneticus (Radboudumc) |
Voorzitter subcommissie Richtlijnen, onderdeel van Kwaliteitscommissie VKGN |
Geen |
Geen |
Aytu Pharma / Prevent studie (effect Enzastaurin bij vasculair EDS) Studie is nog niet gestart, financiering on hold / Tijdelijk, ter vervanging verlof projectleider |
Geen |
Geen |
10/11/2022 |
Geen restricties. De studie waar mw. Kempers bij betrokken was is nooit gestart. Inhoudelijk had deze studie niet met mannelijke infertiliteit te maken. |
|
Anne-Marie van der Kevie - Kersemaekers |
laboratoriumspecialist klinische genetica UMC Utrecht |
Vakdeskundige Raad van Accreditatie |
Geen |
Geen |
Geen |
Geen |
Geen |
28/03/2023 |
Geen restricties. |
|
Manon Oud |
Laboratoriumspecialist Klinische Genetica in opleiding, Radboudumc Betaalde functie (hoofdberoep) |
Geen |
Geen |
Geen |
Deelname aan onderzoeksproject als PhD student De novo mutations in male infertility (NWO VICI van prof. Joris Veltman) van 2015-2020 Travel Grant van de Catherine van Tussenbroek Foundation voor bezoek van 3 maanden aan Monash University (2019) |
Geen |
Geen |
8/11/2022 |
Geen restricties, niet actief geweest in de werkgroep. |
|
Dineke Westra |
Laboratoriumspecialist Klinische Genetica (1.0 FTE, betaald) Afd. Genetica, sectie Genoomdiagnostiek Radboudumc, Nijmegen Werkzaamheden: Genetische diagnostiek |
Technical Assessor ISO15189 Raad van Accreditatie betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
16/02/2023 |
Geen restricties. |
|
Liliana Ramos |
Klinisch embryoloog Radboudumc |
Geen |
Geen |
Geen |
Geen |
Boegbeeldfunctie bij patiënten en beroepsorganisatie |
Geen |
10/08/2023 |
Geen restricties. |
|
Rosanne Grolle |
Fertiliteitsarts, Erasmus MC. Het begeleiden en behandelen van paren met een kinderwens. Functie is betaald. |
Lid van de symposiumcommissie van de VVF Onder andere het opstellen van het wetenschappelijk programma, het vragen van sprekers, het regelen van een symposiumlocatie en buffet, het versturen van de uitnodigingen en het aanvragen van accreditatie en sponsoring. Functie is onbetaald. |
Geen |
Geen |
Geen |
Geen |
Geen |
3/11/2022 |
Geen restricties. |
|
Marloes Vermeulen |
Freya, medewerker externe relaties |
Verloskundige 1e lijn. |
Geen |
Geen |
Geen |
Geen |
Geen |
27/09/2022 |
Geen restricties. |
|
José Knijnenburg |
Directeur bij Freya, vereniging voor mensen met vruchtbaarheidsproblemen - 32u p/wk Medewerker communicatie en marketing bij van der Pol-consulting b.v. - 8u p/wk |
Geen |
Dienstverband bij de (onafhankelijke) landelijke patiëntenvereniging voor mensen met vruchtbaarheidsproblemen. |
Geen |
ZonMW / Alife2 en T4Life / nee ZonMW / Antarctica2 / nee ZonMW / Cosy - Zin en zwanger / nee ZonMW / FOAM / nee ZonMW / Scratch-OFO / nee ZonMW / TOF (3 or 5) / nee ZonMW / H2Olie / nee ZonMW / H2OlieFlush / nee ZonMW / MYPP - myo-inositol bij PCOS / nee ZonMW / PSIDER Embryonic checkpoints - releasing the brakes on IVF /nee RadboudUMC/Goodlife / Summer - voedingssupplement man / nee ZonMW / Divine - dosiscalculator / nee Amsterdam UMC / ANDES / nee ZonMW / PSIDER - Hip gametes / nee ZonMW / COPIE - - endometriose en IVF / nee |
Belangenbehartiger bij patiëntenorganisatie |
Radboud/MUMC / Hmove sporten en afweersysteem bij miskramen / nee ZonMW / Medium2 kweekvloeistof IVF / nee ZonMW / Selectimo timelapse / nee MUMC+ / Murlm hhmk en ril / nee ZonMw / LUMO luteal phase support / nee ZonMw / PSIDER SteMBlast / nee ZonMw / SEGa veiligheid vp-technieken / nee ZonMw / Covid-19 Impact endometriose/fertiliteitspatiënten / nee ZonMw / PREMI / nee ZonMw / HyFosy-HSG stugie / nee ZonMw / REMI III / nee |
20/07/2023 |
Geen restricties, mevrouw was tijdelijke inval tijdens zwangerschapsverlof. In rol van patientvertegenwoordiger betrokken bij onderzoek. |
|
Simone Sinjorgo |
Parttime medewerker patientenperspectief en -participatie bij Freya (vereniging voor mensen met vruchtbaarheidsproblemen) - betaald 14 uur https://www.freya.nl/over-freya/wie-we-zijn/de-werknemers. Ter info: door mijn functie bij Freya ben ik betrokken bij diverse richtlijnontwikkeling en/of onderzoeken op het gebied van fertiliteit. In de vorm van toelichten, belichten en/of vertegenwoordigen van alleen het patiëntenperspectief tav het bepaalde onderwerp, zoals bij deze 3 richtlijnen OFO, OHSS en mannelijke subfertiliteit. |
Lichaamsgericht psychosociaal therapeut - zzp eigen praktijk in Dongen-Vaart - geregistreerd therapeut RBCZ incl. AGB-codes. www.praktijkdediamant.nl
- Psychosociaal docent Bijscholing Instituut voor therapeuten - betaling via praktijk https://bivt.nl/?s=lichaamsgericht+coachen
- Psychosociaal docent vrouwencoach opleiding - betaling via praktijk https://www.devrouwencoach.nl/vrouwencoach-opleiding/ |
Geen |
Geen |
Geen |
Geen |
Geen |
03/12/2024 |
Geen restricties. |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door uitnodigen van Freya en de Patientenfederatie Nederland voor de invitational conference. Daarnaast zat namens Freya een afgevaardigde in de werkgroep. Het verslag van de invitational conference is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen (zie kop waarden en voorkeuren van patiënten). De conceptrichtlijn is tevens voor commentaar voorgelegd aan Freya en de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Hypogonadisme
|
Geen financiele gevolgen. |
Uit de toetsing volgt dat de aanbevelingen niet breed toepasbaar zijn (<5.000 patiënten) en daarom naar verwachting geen substantiële financiële gevolgen zullen hebben voor de collectieve uitgaven. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Mannelijke subfertiliteit - UV11 Hypogonadisme |
|
|
Uitgangsvraag/modules: Wat is de rol van behandeling van hypogonadisme bij subfertiele mannen? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 26-2-2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
Rayyan review: https://rayyan.ai/reviews/943734 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen subfertiele mannen EN hypogonadisme EN behandeling.
→ De sleutelartikelen PMID36680549, PMID31621654 en PMID25271205 worden gevonden met deze search. |
|
|
Te gebruiken voor richtlijntekst: In de databases Embase.com en Ovid/Medline is op 26 februari 2024 systematisch gezocht naar systematische reviews, RCTs en observationele studies over de rol van behandeling van hypogonadisme bij subfertiele mannen. De literatuurzoekactie leverde 430 unieke treffers op. |
|
Zoekopbrengst - 26 februari 2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
74 |
38 |
80 |
|
RCT |
126 |
69 |
154 |
|
Observationeel |
183 |
103 |
196 |
|
Totaal |
383 |
210 |
430* |
*in Rayyan
Zoekstrategie - 26 februari 2024
Embase.com
|
No. |
Query |
Results |
|
#1 |
'male infertility'/exp OR 'male fertility'/exp OR (('subfertility'/de OR 'childlessness'/exp) AND 'male'/exp) OR (((male* OR men OR man) NEAR/3 (infertil* OR hypofertil* OR 'fertil*' OR subfertil* OR infecund* OR childless* OR reproduct*)):ti,ab,kw) OR (((spermatogen* OR spermiation OR spermiogen*) NEAR/3 failure):ti,ab,kw) OR ((spermatozoon NEAR/3 (abnormalit* OR anomal*)):ti,ab,kw) OR (((semen OR sperm) NEAR/3 (qualit* OR quantit*)):ti,ab,kw) OR asperm*:ti,ab,kw OR asthenazoosperm*:ti,ab,kw OR asthenosperm*:ti,ab,kw OR asthenozoosperm*:ti,ab,kw OR azoosperm*:ti,ab,kw OR cryptosperm*:ti,ab,kw OR cryptozoosperm*:ti,ab,kw OR hyposperm*:ti,ab,kw OR oligoasthenosperm*:ti,ab,kw OR oligosperm*:ti,ab,kw OR oligozoosperm*:ti,ab,kw OR 'retrograde ejaculat*':ti,ab,kw OR 'sco syndrome*':ti,ab,kw OR 'sertoli cell only syndrome*':ti,ab,kw OR teratozoosperm*:ti,ab,kw OR 'thermosensitive genic male steril*':ti,ab,kw OR globozoosperm*:ti,ab,kw OR macrozoosperm*:ti,ab,kw |
106746 |
|
#2 |
'hypogonadism'/exp OR 'hypergonadotropic hypogonadism'/exp OR 'hypergonadotropism'/exp OR 'klinefelter syndrome'/exp OR ((gonad* NEAR/3 (insufficien* OR failure*)):ti,ab,kw) OR ((hypergonadotroph* NEAR/3 (azoosperm* OR testi*)):ti,ab,kw) OR (((xxy OR xxyy) NEAR/3 (constitution OR syndrome* OR trisom*)):ti,ab,kw) OR testosterone:ti,ab,kw OR hypogenitalism:ti,ab,kw OR hypogonadism:ti,ab,kw OR hypergonadotrophism:ti,ab,kw OR hypergonadotropism:ti,ab,kw OR klinefelter*:ti,ab,kw |
147433 |
|
#3 |
'clomifene citrate'/exp OR 'selective estrogen receptor modulator'/exp OR 'aromatase inhibitor'/exp OR 'chorionic gonadotropin'/exp OR 'recombinant chorionic gonadotropin'/exp OR 'choriogonadotropin alfa (drug)'/exp OR 'tamoxifen'/exp OR 'anastrozole'/exp OR 'letrozole'/exp OR 'clomifene'/exp OR (((estrogen OR oestrogen) NEAR/3 'receptor modulator*'):ti,ab,kw) OR (((aromatase OR 'estrogen synthetase' OR 'oestrogen synthetase' OR 'steroid aromatase') NEAR/3 inhibitor*):ti,ab,kw) OR ((recombinant NEAR/3 gonadotropin):ti,ab,kw) OR anexin:ti,ab,kw OR blesifen:ti,ab,kw OR clomhexal:ti,ab,kw OR clomid:ti,ab,kw OR 'clomifene citrate':ti,ab,kw OR 'clomifene dihydrogen citrate':ti,ab,kw OR clomifil:ti,ab,kw OR 'clomiphene citrate':ti,ab,kw OR 'clomiphene serono':ti,ab,kw OR clomivid:ti,ab,kw OR clomoval:ti,ab,kw OR clonin:ti,ab,kw OR cloprezine:ti,ab,kw OR clostil:ti,ab,kw OR clostilbegyt:ti,ab,kw OR dufine:ti,ab,kw OR duinum:ti,ab,kw OR dyneric:ti,ab,kw OR fensipros:ti,ab,kw OR fertilan:ti,ab,kw OR fertilphen:ti,ab,kw OR fertin:ti,ab,kw OR fertomid:ti,ab,kw OR fertyl:ti,ab,kw OR genoclam:ti,ab,kw OR gravosan:ti,ab,kw OR ikaclomin:ti,ab,kw OR ikaklomin:ti,ab,kw OR indovar:ti,ab,kw OR mestrolin:ti,ab,kw OR milophene:ti,ab,kw OR nefimol:ti,ab,kw OR ofertil:ti,ab,kw OR omifin:ti,ab,kw OR 'ova mit':ti,ab,kw OR ovamit:ti,ab,kw OR ovipreg:ti,ab,kw OR pergotime:ti,ab,kw OR phemilon:ti,ab,kw OR pinfetil:ti,ab,kw OR profertil:ti,ab,kw OR provula:ti,ab,kw OR serofene:ti,ab,kw OR serophene:ti,ab,kw OR serpafar:ti,ab,kw OR zimaquin:ti,ab,kw OR serm:ti,ab,kw OR 'serms apl':ti,ab,kw OR brevactid:ti,ab,kw OR choragon:ti,ab,kw OR chorex:ti,ab,kw OR chorigon:ti,ab,kw OR choriogonadotrophi*:ti,ab,kw OR choriogonadotropin*:ti,ab,kw OR choriogonin:ti,ab,kw OR choriomon:ti,ab,kw OR 'chorion* gonadotrophi*':ti,ab,kw OR 'chorion* gonadotropi*':ti,ab,kw OR choriongonadotrophi*:ti,ab,kw OR choron:ti,ab,kw OR chorulon:ti,ab,kw OR coriantin:ti,ab,kw OR corion:ti,ab,kw OR endocorion:ti,ab,kw OR follutein:ti,ab,kw OR 'gestasol dry':ti,ab,kw OR gonabion:ti,ab,kw OR gonacor:ti,ab,kw OR gonadex:ti,ab,kw OR 'gonadotrophi* chorion*':ti,ab,kw OR gonadotrophon:ti,ab,kw OR gonatropin:ti,ab,kw OR h.c.g.:ti,ab,kw OR hcg:ti,ab,kw OR homosten:ti,ab,kw OR libigen:ti,ab,kw OR novarel:ti,ab,kw OR ovulgone:ti,ab,kw OR physex:ti,ab,kw OR praedyn:ti,ab,kw OR pranturon:ti,ab,kw OR predalon:ti,ab,kw OR pregnesin:ti,ab,kw OR pregnyl:ti,ab,kw OR primogonyl:ti,ab,kw OR profasi:ti,ab,kw OR promogonyl:ti,ab,kw OR prophasi:ti,ab,kw OR prymogonyl:ti,ab,kw OR pubergen:ti,ab,kw OR puberogen:ti,ab,kw OR riogon:ti,ab,kw OR synapoidin:ti,ab,kw OR zivafert:ti,ab,kw OR ovidrel:ti,ab,kw OR ovidrelle:ti,ab,kw OR ovitrelle:ti,ab,kw OR ebefen:ti,ab,kw OR kessar:ti,ab,kw OR tamoplac:ti,ab,kw OR tamoxasta:ti,ab,kw OR tamoxifen:ti,ab,kw OR tamoxifene:ti,ab,kw OR anastrazole:ti,ab,kw OR anastrozole:ti,ab,kw OR arimidex:ti,ab,kw OR femathina:ti,ab,kw OR trozolet:ti,ab,kw OR femar:ti,ab,kw OR femara:ti,ab,kw OR letrozole:ti,ab,kw OR loxifan:ti,ab,kw |
195197 |
|
#4 |
#1 AND #2 AND #3 |
1699 |
|
#5 |
#4 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
698 |
|
#6 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1003926 |
|
#7 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
3976736 |
|
#8 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8084646 |
|
#9 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
14842224 |
|
#10 |
#5 AND #6 – SR’s |
74 |
|
#11 |
#5 AND #7 NOT #10 – RCT’s |
126 |
|
#12 |
#5 AND (#8 OR #9) NOT (#10 OR #11) – Observationele studies |
183 |
|
#13 |
#10 OR #11 OR #12 |
383 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Infertility, Male/ or ((exp Infertility/ or Fertility/) and exp Male/) or ((male* or men or man) adj3 (infertil* or hypofertil* or fertil* or subfertil* or infecund* or childless* or reproduct*)).ti,ab,kf. or ((spermatogen* or spermiation or spermiogen*) adj3 failure).ti,ab,kf. or (spermatozoon adj3 (abnormalit* or anomal*)).ti,ab,kf. or ((semen or sperm) adj3 (qualit* or quantit*)).ti,ab,kf. or asperm*.ti,ab,kf. or asthenazoosperm*.ti,ab,kf. or asthenosperm*.ti,ab,kf. or asthenozoosperm*.ti,ab,kf. or azoosperm*.ti,ab,kf. or cryptosperm*.ti,ab,kf. or cryptozoosperm*.ti,ab,kf. or hyposperm*.ti,ab,kf. or oligoasthenosperm*.ti,ab,kf. or oligosperm*.ti,ab,kf. or oligozoosperm*.ti,ab,kf. or retrograde ejaculat*.ti,ab,kf. or sco syndrome*.ti,ab,kf. or sertoli cell only syndrome*.ti,ab,kf. or teratozoosperm*.ti,ab,kf. or thermosensitive genic male steril*.ti,ab,kf. or globozoosperm*.ti,ab,kf. or macrozoosperm*.ti,ab,kf. |
97204 |
|
2 |
exp Hypogonadism/ or exp Klinefelter Syndrome/ or (gonad* adj3 (insufficien* or failure*)).ti,ab,kf. or (hypergonadotroph* adj3 (azoosperm* or testi*)).ti,ab,kf. or ((xxy or xxyy) adj3 (constitution or syndrome* or trisom*)).ti,ab,kf. or testosterone.ti,ab,kf. or hypogenitalism.ti,ab,kf. or hypogonadism.ti,ab,kf. or hypergonadotrophism.ti,ab,kf. or hypergonadotropism.ti,ab,kf. or klinefelter*.ti,ab,kf. |
110539 |
|
3 |
exp Clomiphene/ or exp Selective Estrogen Receptor Modulators/ or exp Aromatase Inhibitors/ or exp Chorionic Gonadotropin/ or exp Tamoxifen/ or exp Anastrozole/ or exp Letrozole/ or exp Clomiphene/ or ((estrogen or oestrogen) adj3 receptor modulator*).ti,ab,kf. or ((aromatase or estrogen synthetase or oestrogen synthetase or steroid aromatase) adj3 inhibitor*).ti,ab,kf. or (recombinant adj3 gonadotropin).ti,ab,kf. or anexin.ti,ab,kf. or blesifen.ti,ab,kf. or clomhexal.ti,ab,kf. or clomid.ti,ab,kf. or clomifene citrate.ti,ab,kf. or clomifene dihydrogen citrate.ti,ab,kf. or clomifil.ti,ab,kf. or clomiphene citrate.ti,ab,kf. or clomiphene serono.ti,ab,kf. or clomivid.ti,ab,kf. or clomoval.ti,ab,kf. or clonin.ti,ab,kf. or cloprezine.ti,ab,kf. or clostil.ti,ab,kf. or clostilbegyt.ti,ab,kf. or dufine.ti,ab,kf. or duinum.ti,ab,kf. or dyneric.ti,ab,kf. or fensipros.ti,ab,kf. or fertilan.ti,ab,kf. or fertilphen.ti,ab,kf. or fertin.ti,ab,kf. or fertomid.ti,ab,kf. or fertyl.ti,ab,kf. or genoclam.ti,ab,kf. or gravosan.ti,ab,kf. or ikaclomin.ti,ab,kf. or ikaklomin.ti,ab,kf. or indovar.ti,ab,kf. or mestrolin.ti,ab,kf. or milophene.ti,ab,kf. or nefimol.ti,ab,kf. or ofertil.ti,ab,kf. or omifin.ti,ab,kf. or ova mit.ti,ab,kf. or ovamit.ti,ab,kf. or ovipreg.ti,ab,kf. or pergotime.ti,ab,kf. or phemilon.ti,ab,kf. or pinfetil.ti,ab,kf. or profertil.ti,ab,kf. or provula.ti,ab,kf. or serofene.ti,ab,kf. or serophene.ti,ab,kf. or serpafar.ti,ab,kf. or zimaquin.ti,ab,kf. or serm.ti,ab,kf. or serms apl.ti,ab,kf. or brevactid.ti,ab,kf. or choragon.ti,ab,kf. or chorex.ti,ab,kf. or chorigon.ti,ab,kf. or choriogonadotrophi*.ti,ab,kf. or choriogonadotropin*.ti,ab,kf. or choriogonin.ti,ab,kf. or choriomon.ti,ab,kf. or chorion* gonadotrophi*.ti,ab,kf. or chorion* gonadotropi*.ti,ab,kf. or choriongonadotrophi*.ti,ab,kf. or choron.ti,ab,kf. or chorulon.ti,ab,kf. or coriantin.ti,ab,kf. or corion.ti,ab,kf. or endocorion.ti,ab,kf. or follutein.ti,ab,kf. or gestasol dry.ti,ab,kf. or gonabion.ti,ab,kf. or gonacor.ti,ab,kf. or gonadex.ti,ab,kf. or gonadotrophi* chorion*.ti,ab,kf. or gonadotrophon.ti,ab,kf. or gonatropin.ti,ab,kf. or hcg.ti,ab,kf. or homosten.ti,ab,kf. or libigen.ti,ab,kf. or novarel.ti,ab,kf. or ovulgone.ti,ab,kf. or physex.ti,ab,kf. or praedyn.ti,ab,kf. or pranturon.ti,ab,kf. or predalon.ti,ab,kf. or pregnesin.ti,ab,kf. or pregnyl.ti,ab,kf. or primogonyl.ti,ab,kf. or profasi.ti,ab,kf. or promogonyl.ti,ab,kf. or prophasi.ti,ab,kf. or prymogonyl.ti,ab,kf. or pubergen.ti,ab,kf. or puberogen.ti,ab,kf. or riogon.ti,ab,kf. or synapoidin.ti,ab,kf. or zivafert.ti,ab,kf. or ovidrel.ti,ab,kf. or ovidrelle.ti,ab,kf. or ovitrelle.ti,ab,kf. or ebefen.ti,ab,kf. or kessar.ti,ab,kf. or tamoplac.ti,ab,kf. or tamoxasta.ti,ab,kf. or tamoxifen.ti,ab,kf. or tamoxifene.ti,ab,kf. or anastrazole.ti,ab,kf. or anastrozole.ti,ab,kf. or arimidex.ti,ab,kf. or femathina.ti,ab,kf. or trozolet.ti,ab,kf. or femar.ti,ab,kf. or femara.ti,ab,kf. or letrozole.ti,ab,kf. or loxifan.ti,ab,kf. |
98944 |
|
4 |
1 and 2 and 3 |
948 |
|
5 |
limit 4 to yr="2000 -Current" |
526 |
|
6 |
5 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
405 |
|
7 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
728276 |
|
8 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2694188 |
|
9 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4659587 |
|
10 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5629016 |
|
11 |
6 and 7 – SR’s |
38 |
|
12 |
(6 and 8) not 11 – RCT’s |
69 |
|
13 |
(6 and (9 or 10)) not (11 or 12) – Observationele studies |
103 |
|
14 |
11 or 12 or 13 |
210 |