Medicatiebibliotheken
Uitgangsvraag
- Wat is het aanbevolen type infuuspomp - met of zonder medicatiebibliotheek - voor het toedienen van een intraveneus geneesmiddel?
- Aan welke randvoorwaarden moet je voldoen om medicatiebibliotheken in infuuspompen effectief en veilig in te kunnen zetten?
Aanbeveling
Aanbeveling-1
Overweeg infuuspompen met een medicatiebibliotheek te gebruiken indien implementatie haalbaar is binnen de zorginstelling en voldaan kan worden aan randvoorwaarden om medicatiebibliotheken effectief en veilig in te zetten.
Aanbeveling-2
Richt onderstaande randvoorwaarden in om medicatiebibliotheken in infuuspompen effectief en veilig in te kunnen zetten:
- Beschikbaarheid van een medicatiebibliotheek die past bij de specifieke afdeling en patiënt.
- Beperking van het aantal medicatiebibliotheken in de zorginstelling om het gebruik en beheer voor en door alle stakeholders zo optimaal mogelijk te laten verlopen en standaard toedieningen te bevorderen.
- Gebruik van afdelingsspecifieke medicatiebibliotheken, om daarmee de betrokkenheid en compliantie per afdeling hoog te houden.
- Borging dat de toedieningsparameters per geneesmiddel in de medicatiebibliotheek overeenkomen met het vigerende protocol op de afdeling.
- Borging dat standaard doseringen en concentraties en de toedieningslimieten per geneesmiddel in de medicatiebibliotheek overeenkomen met het vigerende protocol op de afdeling.
- Borging dat geneesmiddelen op basis van dosering per tijdseenheid (mg/h of mg /kg/min) toegevoegd zijn aan de medicatiebibliotheek.
- Borging dat geneesmiddelen die middels complexe protocollen worden toegediend toegevoegd zijn aan de medicatiebibliotheek.
- Borging van een proces voor aanmaken, wijzigen, controleren, vrijgeven en uploaden van een medicatiebibliotheek dat nauw aansluit bij het gebruik van slimme infuuspompen middels een ingerichte plan-do-check-act (PDCA) cyclus.
- Beschikbaarheid van geschoold personeel in het gebruik van de medicatiebibliotheek.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Slimme infuuspompen zijn pompen met een medicatiebibliotheek. Traditionele infuuspompen maken hier geen gebruik van. Het niet gebruiken van een medicatiebibliotheek in een slimme infuuspomp maakt deze gelijk aan een traditionele infuuspomp (Pang, 2011). Met specifieke software kunnen zorginstellingen een medicatiebibliotheek maken en naar eigen behoefte inrichten en aanpassen op concentraties, doseringseenheden en doseringslimieten. Minimale en maximale zachte doseringslimieten geven waarschuwingsberichten aan de gebruiker. Minimale en maximale harde limieten kunnen door de gebruiker niet omzeild worden (Guerin, 2015). Met andere woorden: een medicatiebibliotheek is een database in een pomp die informatie bevat over mogelijk toe te dienen geneesmiddelen via de infuuspomp en de toedieningsparameters per geneesmiddel.
Slimme infuuspompen (hiermee wordt zowel een spuitenpomp als een volumetrische pomp bedoeld, met een medicatiebibliotheek) zijn ontworpen en op de markt gebracht om incidenten te verminderen en worden geacht medicatiefouten te voorkomen en te verminderen. Slimme infuuspompen kunnen zowel intramuraal als extramuraal ingezet worden.
Momenteel wordt een medicatiebibliotheek niet altijd gebruikt in infuuspompen. Ofwel omdat een medicatiebibliotheek niet is ingericht door een zorginstelling, ofwel omdat een zorgverlener de medicatiebibliotheek in een infuuspomp niet gebruikt. Gevolgen van het niet altijd gebruiken van een medicatiebibliotheek kunnen medicatie- en doseringsfouten zijn. Door te achterhalen wat de optimale inrichting van een medicatiebibliotheek is en welke aspecten in overweging genomen moeten worden als je buiten de medicatiebibliotheek om wilt werken, kunnen de risico's van medicatie- en doseringsfouten verlaagd worden (Guerin, 2015). Het gebruik maken van een aanwezige medicatiebibliotheek, oftewel hoge compliantie in de organisatie voor effectief gebruik van slimme infuuspompen, blijft daarbij uiteraard cruciaal (Escandell-Rico, 2024).
Wat is het aanbevolen type infuuspomp - met of zonder medicatiebibliotheek - voor het toedienen van een intraveneus geneesmiddel?
Er is systematisch literatuuronderzoek uitgevoerd naar het effect van het gebruik van infuuspompen met medicatiebibliotheken vergeleken met het gebruik van traditionele infuuspompen zonder medicatiebibliotheken. Er werden vijf observationele studies gevonden die dit onderzochten. Hoewel klinisch relevant minder medicatiefouten werden geobserveerd bij het gebruik van slimme infuuspompen vergeleken met traditionele infuuspompen, is de werkgroep zeer onzeker over het werkelijke effect van slimme infuuspompen op de cruciale uitkomstmaat medicatiefouten. Dit vanwege de zeer lage kwaliteit van het bewijs. Er kunnen geen conclusies worden getrokken over het effect van slimme infuuspompen op het aantal medicatiefouten.
Ten aanzien van de andere cruciale uitkomstmaat complicaties en de belangrijke uitkomstmaat werklastreductie bij het gebruik van slimme infuuspompen konden ook geen conclusies worden getrokken over de voor- en nadelen van het gebruik van slimme infuuspompen vanwege het gebrek aan studies die dit onderzochten.
Desalniettemin is de ervaring van de werkgroep dat het gebruik van slimme infuuspompen een duidelijke meerwaarde heeft ten opzichte van traditionele infuuspompen.
Enerzijds ten aanzien van een hogere kwaliteit van zorg door een eenduidige manier van werken op basis van een actuele en klinisch relevante medicatiebibliotheek. Door daarnaast gebruik te maken van standaard doseringen en concentraties als onderdeel van het totale medicatieproces wordt ook verdere foutreductie bereikt en kunnen voorgevulde spuiten (zie submodule Spuiten) eventueel ook gebruikt worden (Larsen, 2005; Pang, 2011). Dit versterkt de visualisatie en verkleint de kans op fouten.
Anderzijds doordat meer veiligheid wordt gegarandeerd door zichtbaarheid van het geneesmiddel op de infuuspomp en door gebruik te maken van zachte en harde limieten. Bovendien biedt een dosiscalculator in een slimme infuuspomp, als onderdeel van de medicatiebibliotheek, een verdere mogelijkheid tot foutreductie. Hierbij wordt niet de toedieningssnelheid ingevoerd, maar wordt deze door de pomp berekend op basis van gewenste dosis en gewicht van de patiënt.
Men dient zich er wel van bewust te zijn dat slimme infuuspompen ook nieuwe soorten fouten kunnen introduceren. Fouten kunnen worden geïntroduceerd in de volgende fases:
- de programmeerfase van de medicatiebibliotheek, wat kan leiden tot onbewust foutief gebruik van de geneesmiddelen in de medicatiebibliotheek met bijbehorende eventuele nadelige gevolgen;
- de VTGM (Voor Toediening Gereed Maken) fase van een geneesmiddel, waarbij de verkeerde concentratie kan worden voorbereid, niet overeenkomend met de concentratie in de medicatiebibliotheek, met als gevolg een foutieve toediening (Pang, 2011);
- de gebruiksfase van de slimme infuuspomp vereist dat de gebruiker het juiste geneesmiddel en de juiste concentratie in de medicatiebibliotheek selecteert en indien noodzakelijk het juiste gewicht van de patiënt invoert;
- de toedieningsfase door het ontbreken van een koppeling tussen de infuuspomp en het Elektronische Patiënten/Cliënten Dossier(EPD/ECD), waardoor het aantal gedupliceerde toedieningen kan toenemen (Howlett, 2020).
Momenteel wordt een medicatiebibliotheek niet altijd gebruikt in infuuspompen en de gevolgen daarvan kunnen zijn medicatie- en doseringsfouten. Inzet van een medicatiebibliotheek heeft naar mening van de werkgroep een duidelijke meerwaarde t.a.v. hogere kwaliteit en veiligheid van de zorg. Ook met het in ogenschouw nemen van de genoemde nieuwe soorten fouten die geïntroduceerd kunnen worden.
Kwaliteit van bewijs
De overall kwaliteit van bewijs is zeer laag. Dit betekent dat de werkgroep zeer onzeker is over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege (zeer) ernstige:
- Risk of Bias: Geen gerandomiseerde studies; verschillen in de populaties in de interventie en controlegroep; geen correctie voor vertekenende factoren.
- Inconsistentie: Verschillen in resultaten van de verschillende studies.
Aan welke randvoorwaarden moet je voldoen om medicatiebibliotheken effectief en veilig in te kunnen zetten?
Om medicatiebibliotheken effectief en veilig in te kunnen zetten, moet naar mening van de werkgroep aan een aantal randvoorwaarden voldaan worden. Enerzijds t.a.v. de inrichting van medicatiebibliotheken en anderzijds t.a.v. organisatorische aspecten.
Voor een optimale inrichting van de medicatiebibliotheek ziet de werkgroep de volgende overwegingen:
- Een optimale aansluiting van de medicatiebibliotheek op iedere afdeling en patiënt:
- intensieve en acute zorgafdelingen hebben veelal een uitgebreide medicatiebibliotheek nodig, algemene verpleegafdelingen veelal een beperkte medicatiebibliotheek;
- instellingen voor hetzelfde geneesmiddel kunnen verschillen tussen medicatiebibliotheken op basis van indicatie of patiëntcategorieën, om maximaal aan te sluiten bij het gewenste gebruik op de desbetreffende afdeling;
- er kan gekozen worden voor specifieke pijnbestrijdingspompen met een dedicated medicatiebibliotheek.
- Een beperkt aantal medicatiebibliotheken in de zorginstelling is nodig om het gebruik en beheer voor alle stakeholders zo optimaal mogelijk te laten verlopen en een gestandaardiseerde manier van toediening te bevorderen.
- Het gebruik van een afdelingsspecifieke medicatiebibliotheek, om daarmee de betrokkenheid en compliantie per afdeling hoog te houden.
- Er zijn meerdere technische mogelijkheden om dit veilig in te richten. Denk in de zorginstelling goed na hoe een afdelingsspecifieke medicatiebibliotheek ingericht wordt.
- Inrichting van standaard doseringen, concentraties en mogelijkheid tot bolustoediening.
- Inrichting van toedieningslimieten waar mogelijk voor concentratie, dosis, inloopsnelheid, gewicht en bolusdosering per geneesmiddel in de medicatiebibliotheek die overeen te komen met het vigerende protocol op de afdeling (ECRI (2020)) om de patiëntveiligheid te verhogen.
- Het toevoegen van geneesmiddelen aan de medicatiebibliotheek op basis van dosis per tijdseenheid (mg/h of mg /kg/min) en niet op basis van inloopsnelheid (ml/h), omdat inloopsnelheid van een infuuspomp een resultante is van omrekening en daarmee foutgevoelig:
- Om fouten bij omrekenen te voorkomen kan gebruikt gemaakt worden van de ingebouwde dosiscalculator in een infuuspomp.
- Toevoeging van geneesmiddelen die middels complexe protocollen (bijvoorbeeld TCI (Target-controlled infusion) of PIEB (Programmed Intermittent Epidural Boluses)) worden toegediend aan de medicatiebibliotheek, ter voorkoming van medicatie- en doseringsfouten.
- Inrichtingsaspecten van het display van een pomp hangen af van de mogelijkheden van de betreffende pomp. Denk na over het gebruik van ISO kleurlabels, afkortingen wanneer de tekst niet op de display past en tall man lettering (hoofdlettergebruik). Neem hierin mee in op welke manier het distributie- en controle proces van de medicatiebibliotheken plaatsvindt.
De werkgroep adviseert om een kortlopend geneesmiddel dat bijvoorbeeld via een bijspuitpunt of piggyback wordt toegediend niet toe te voegen aan de medicatiebibliotheek, omdat de gebruiker daar in de praktijk niet mee geholpen is.
Randvoorwaarden ten aanzien van organisatorische aspecten hebben naar mening van de werkgroep betrekking op:
- Betrokkenheid van stakeholders.
- Scholing in gebruik van de medicatiebibliotheek.
Betrokkenheid van stakeholders
De implementatie van slimme infuuspompen vereist een aanzienlijke inspanning en multidisciplinaire samenwerking van artsen, verpleegkundigen, (ziekenhuis)apothekers, klinisch fysici, biomedisch technologen, technici en andere belanghebbenden (Guerin, 2015). Deze stakeholders dienen een proces in te richten voor het aanmaken, wijzigen, controleren, vrijgeven en uploaden van medicatiebibliotheken om gebruik van correcte medicatiebibliotheken te borgen. Bovendien vereist de aanwezigheid van een medicatiebibliotheek regelmatige updates om klinische relevantie te garanderen en de acceptatie door gebruikers te optimaliseren (Pang, 2011). Dit dient niet onderschat te worden. Afhankelijk van de soort pompen en het aantal medicatiebibliotheken in de zorginstelling is dit een intensieve actie. Optimaal gebruik van een slimme infuuspomp is alleen mogelijk met een optimale inrichting van de medicatiebibliotheek. Onbewust foutief gebruik van een medicatiebibliotheek dient voorkomen te worden.
Scholing in gebruik van de medicatiebibliotheek
Het gebruik maken van een aanwezige medicatiebibliotheek in een infuuspomp, oftewel hoge compliantie op de afdeling in effectief gebruik van slimme infuuspompen, is cruciaal (Escandell-Rico, 2024). Noodzakelijk daarvoor is scholing over het gebruik van de medicatiebibliotheek om ervoor te zorgen dat de gebruiker:
- de juiste concentratie voorbereid;
- het juiste geneesmiddel en concentratie selecteert in de infuuspomp;
- weet heeft van het bestaan van toedieningslimieten per geneesmiddel;
- weet hoe de medicatiebibliotheek te gebruiken in de infuuspomp.
De rol van EPD integratie
Toenemend gebruik van informatietechnologie, zoals elektronisch voorschrijven of geautomatiseerde invoer van medicatie orders op slimme infuuspompen, wordt gezien als volgende stap om medicatiefouten te verminderen (Howlett, 2020) en om te komen tot een closed-loop medicatie management proces (Kuitunen, 2020) met focus op het reductie van werklast en workarounds (Ohashi, 2014). De definitie van een closed-loop medicatie proces is als volgt geformuleerd: systemen, maatregelen en procedures om het juiste geneesmiddel in de juiste dosering, met de juiste loopsnelheid, aan de juiste patiënt op het juiste moment en op de juiste manier toe te dienen; relevante data wordt real time vastgelegd in het EPD. Het sturen van een order tot in de juiste pomp bij de juiste patiënt biedt een closed-loop medicatie benadering, waarbij de zorgverlener op het scherm van de pomp de order ziet, deze controleert en de toediening accordeert en start. We zien hiervoor op dit moment diverse initiatieven. De implementatie van deze functionaliteit is in de praktijk echter nog beperkt, met name waar het de automatische overdracht van voor gedefinieerde medicatieopdrachten (VMO) naar infuuspompen betreft. Voor deze stap is het volgens de werkgroep belangrijk een aantal aspecten te realiseren:
- beschikbaarheid van een medicatie opdracht in een voorschrijfsysteem, die met eventueel aanvullende medicatie protocol informatie, omgezet kan worden in een order direct vanuit het EPD naar een slimme infuuspomp;
- beschikbaarheid van het geneesmiddel in de medicatiebibliotheek;
- toepassing van één unieke identifier waarmee ieder geneesmiddel in de juiste concentratie in alle relevante gekoppelde systemen herkend kan worden;
- ontwikkeling van een systeem en proces integratie waarbij medicatie voorschrift, spuit of infuuszak ID, patiënt ID en slimme infuuspomp ID gecombineerd gebruikt worden;
- bij uitval van een van de gekoppelde systemen dient geneesmiddeltoediening mogelijk te blijven door gebruik te maken van de aanwezige medicatiebibliotheek.
Werken buiten de medicatiebibliotheek om
Werken buiten de medicatiebibliotheek om maakt een slimme infuuspomp tot een traditionele infuuspomp. Dit kan in een basisconfiguratie van een infuuspomp niet geblokkeerd worden, zodat handmatige toediening van een geneesmiddel in acute situaties gegarandeerd blijft. Als in de praktijk blijkt dat de medicatiebibliotheek in een infuuspomp regelmatig niet gebruikt wordt om zo een harde limiet te omzeilen of een geneesmiddel via de infuuspomp toe te dienen die niet voorkomt in de medicatiebibliotheek, dient de medicatiebibliotheek aangepast te worden. Hiermee wordt het effectief gebruik van de medicatiebibliotheek in de zorginstelling bevorderd. Om dit te bewerkstelligen dient het proces voor beheer van een medicatiebibliotheek nauw aan te sluiten bij het gebruik van slimme infuuspompen middels een ingerichte plan-do-check-act (PDCA) cyclus.
Kwaliteit van bewijs
Voor deze uitgangsvraag is geen search uitgevoerd, omdat geen PICO kon worden opgesteld die aansluit bij de vraag. De kwaliteit van het bewijs kon daarom niet worden vastgesteld.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Voor de patiënt is het vooral belangrijk dat medicatie veilig en comfortabel, zonder complicaties, wordt toegediend. Een betere veiligheid wordt gegarandeerd door zichtbaarheid van het toegediende geneesmiddel op de infuuspomp, waarvoor een medicatiebibliotheek in een infuuspomp noodzakelijk is. Bovendien kan het meerwaarde hebben voor patiënten en naasten om uitleg te krijgen over hoe een infuuspomp met medicatiebibliotheek in het totale proces werkt.
Kostenaspecten
Inzet en gebruik van een actuele medicatiebibliotheek in een infuuspomp heeft een duidelijke meerwaarde. Randvoorwaardelijk daarvoor is een distributie- en controle proces van medicatiebibliotheken via het IT netwerk van de zorginstelling. Alternatief daarvoor is een handmatige distributie 1 keer per 1 of 2 jaar. Handmatige distributie vereist inzet van medisch technisch personeel, wat gezien de te verwachten tekorten op de arbeidsmarkt geen realistisch alternatief is. De kosten van IT-infrastructuur, inclusief netwerk, licenties en beheer, kunnen aanzienlijk zijn en in de praktijk vaak hoger uitvallen dan initieel geraamd. Naar mening van de werkgroep wegen deze extra kosten op tegen de effectiviteit van een complete en actuele medicatiebibliotheek in een infuuspomp.
Gelijkheid ((health) equity/equitable)
De werkgroep voorziet een verschil in gezondheidsgelijkheid ten aanzien van het wel/niet gebruiken van een medicatiebibliotheek in een infuuspomp. Een hogere kwaliteit en betere veiligheid van zorg wordt gegarandeerd door gebruik te maken van een medicatiebibliotheek in een infuuspomp wanneer voldaan kan worden aan de randvoorwaarden voor veilige toepassing. Het gebruik van medicatiebibliotheken en de mogelijkheid om aan randvoorwaarden te voldoen kan per zorginstelling verschillen.
Aanvaardbaarheid
Ethische aanvaardbaarheid
De werkgroep voorziet ten aanzien van het wel of niet gebruiken van een medicatiebibliotheek in een infuuspomp geen ethische bezwaren.
Duurzaamheid
Het gebruik van een medicatiebibliotheek in een infuuspomp en het inzetten van een distributieproces via het IT netwerk van de zorginstelling kan leiden tot extra verbruik van energie en hardware (WiFi modules en andere IT middelen). Handmatige distributie van een medicatiebibliotheek kan leiden tot extra belasting van medisch technisch zorgpersoneel.
Haalbaarheid
De werkgroep voorziet ten aanzien van het gebruik van een medicatiebibliotheek in een infuuspomp geen belemmeringen voor de uitvoerbaarheid. De expertise is over het algemeen al aanwezig in de Nederlandse ziekenhuizen. De werkgroep ziet geen belemmeringen in de multidisciplinaire samenwerking van alle stakeholders rondom de implementatie van slimme infuuspompen en het beheer van medicatiebibliotheken. De werkgroep ziet wel belemmeringen t.a.v. de kosten die gemoeid gaan met de inzet en gebruik van actuele medicatiebibliotheken.
Rationale van aanbeveling-1: weging van argumenten voor en tegen de interventies
Op basis van de literatuur kon geen conclusie getrokken worden over het effect van de inzet van een medicatiebibliotheek in een infuuspomp. Echter, de inzet van een medicatiebibliotheek in een infuuspomp heeft naar mening van de werkgroep een duidelijke meerwaarde ten aanzien van:
- een hogere kwaliteit van zorg door een eenduidige manier van werken op basis van een actuele en klinisch relevante medicatiebibliotheek;
- een betere veiligheid in de zorg door zichtbaarheid van het geneesmiddel op de infuuspomp en door gebruik te maken van zachte en harde limieten.
Deze meerwaarde ziet de werkgroep ook in het perspectief van de nieuwe soorten fouten die geïntroduceerd kunnen worden.
De werkgroep ziet wel belemmeringen ten aanzien van de kosten die gemoeid gaan met de inzet en het beheer van actuele medicatiebibliotheken en daarmee ten aanzien van de haalbaarheid. Daarnaast kan de beperkte mate van systeemintegratie tussen EPD en infuuspompen, met name voor automatische overdracht van medicatieopdrachten, in de praktijk een beperkende factor zijn voor implementatie.
Eindoordeel:
Conditionele aanbeveling voor het gebruik van infuuspompen met een medicatiebibliotheek.
Rationale van aanbeveling-2: weging van argumenten voor en tegen de interventies
De werkgroep heeft enkele randvoorwaarden geïdentificeerd die nodig zijn om veilige toepassing en inzet van medicatiebibliotheken in infuuspompen te garanderen.
Eindoordeel:
Sterke aanbeveling voor het inrichten van randvoorwaarden om medicatiebibliotheken in infuuspompen effectief en veilig in te kunnen zetten.
Onderbouwing
Currently, a medication library is not always used in infusion pumps. This could lead to medication and dosage errors. In this module, a. the aspects needed for an optimal design of a medication library are described and b. which aspects need to be taken into consideration to work outside the drug library are discussed. The aim of the given recommendations is to reduce the risks of possible consequences.
Summary of Findings
Population: Patients who are treated with medication infusion
Intervention: Use of infusion pumps with medication library
Comparator: Use of infusion pumps without medication library
|
Outcome
|
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
Traditional pumps |
Smart pumps |
||||
|
Medication errors (critical)
|
Relative risk: 0.63 (CI 95% 0.45 - 0.87)
Based on data from 3054 participants in 4 studies1
|
122 per 1000 |
77 per 1000 |
Very low Due to very serious risk of bias, Due to serious inconsistency2 |
The evidence is very uncertain about the effect of the use of smart pumps on medication errors compared with traditional pumps in patients treated with medication infusion.
(Guerrin, 2015; Hewlett, 2022; Lyons, 2018; Pang, 2011; Wiseman, 2018) |
|
Difference: 45 fewer per 1000 (CI 95% 67 fewer - 16 fewer) |
|||||
|
Complications (critical)
|
|
|
No GRADE No evidence was found |
No evidence was found regarding the effect of smart pumps on complications when compared with traditional pumps in patients with chronic migraine. |
|
|
Work load reduction (important)
|
|
|
No GRADE No evidence was found |
No evidence was found regarding the effect of smart pumps on work load reduction when compared with traditional pumps in patients with chronic migraine. |
|
1. One study (Guerrin, 2015) could not be included in the meta-analysis
2. Risk of Bias: very serious. Differences between populations traditional and smart pumps; no correction for confounding factors
Inconsistency: serious. Point estimates vary widely
Description of studies
Five studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Guerin (2015) retrospectively investigated the number of drug-related accidents and events before and after implementation of smart pumps with drug libraries in a mother child hospital.
Howlett (2020) retrospectively investigated the number of infusion related prescribing errors before and after implementation of a locally devised smart-pump drug library on syringe drivers and large-volume infusion pumps in a pediatric intensive care unit in an Irish tertiary pediatric hospital.
Lyons (2018) performed a cross-sectional study in sixteen hospitals on several wards. Errors and discrepancies were recorded and compared between smart pumps with drug libraries and/or dose reduction systems enabled and pumps without smart features enabled.
Pang (2011) prospectively investigated the number of Intravenous medication errors before and after the implementations of smart pumps with guardrails software in an acute teaching hospital.
Wiseman (2018) prospectively investigated the number of medication infusion errors before and after the implementation of smart pump technology in a tertiary referral metropolitan hospital.
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
Guerin, 2015 |
N not specified
Patient characteristics not further specified |
Intervention: Implementation of smart pumps (n=1045; about 60 % Infusomat and About 40 % Perfusor Space from B. Braun, Melsungen, Germany) with developed and approved libraries and limits. Training was provided in the month before go-live. Support 24/7 was offered throughout the first two weeks after implementation.
Control: Not specified – before implementation |
Before: from October 2010 to 5 November 2011
After: From 10 November 2011 to 5 November 2012 (0-1 year after implementation)
And From 6 November 2012 to 5 November 2013 (1-2 years after implementation) |
accidents and incidents related to intravenous drug administration |
Retrospective before-after study in a mother-child hospital with 500 beds.
Implementation was performed 9 November 2011. |
High |
|
Howlett, 2020 |
I: 246 infusions C: 138 infusions
Patient characteristics: Control:
Age: Control: |
Intervention: SCIs across four weight bands (5, >5– 10, >10– 20, and >20 kg) was uploaded onto “smart” syringe drivers and large-volume infusion pumps (B. Braun Space pumps, Melsungen, Germany)
Control: |
Before: |
Infusion related prescribing errors |
Retrospective before-after study in 23-bed PICU in an Irish tertiary pediatric hospital.
Implementation of smart pumps was performed in May 2012. |
High |
|
Lyons, 2018 |
N 1326 patients (2008 infusions)
I: 640 infusions (I1: with used drug library: 356 I2: drug library not used although relevant drug listed: 67 I3: drug library not used as relevant drug not listed: 215
C: 1202 infusions
Patient characteristics not further specified |
Intervention: Smart pumps (infusion pump with a drug library and/or dose error reduction software enabled)
Control: Pump with no smart features enabled |
April 2015 – December 2016 |
intravenous infusion administration deviations |
Cross-sectional study in 16 hospitals. 11 of these hospitals did (partly) use smart pumps |
High |
|
Pang, 2011 |
N 698 infusions I1: with guardrails: 165 infusions C: 432 infusions
Patient characteristics not further specified |
Intervention: Implementation of Alaris GP pumps with Guardrails software (CareFusion). 600 infusion protocols involving 89 medicines were developed to form the drug library. The drug library was approved by the hospital’s Drugs and Therapeutics Committee and programmed into the Guardrails software. Pumps were introduced to the wards in tandem with staff education and promotional activities to increase uptake of Guardrails.
Control: Before: IMED Gemini Volumetric Infusion Pumps |
Before: 41 days (November to December 2007) during weekday business hours
After: 27 working days from January to February 2010 (1.5 years after implementation) |
Intravenous medication administration errors |
Prospective before-after study in a 380–bed acute teaching hospital.
Implementation of Alaris GP pumps was performed in May 2008. |
High |
|
Wiseman, 2018 |
I1: April 2012: 658 infusions I2: June 2014: 701 infusions
C: 744 infusions |
I: implementation of smart pump technology (Carefusion Alaris PC Guardrails Suite MX, San Diego, CA, USA) including first data set Release
C: Before, not further specified |
Before: July 2011 |
intravenous medication infusion error |
Prospective before-after study in a 450-bed tertiary referral metropolitan hospital, across 15 general and critical care ward areas.
Implementation of smart pump technology was performed In November 2011.
Note that a pre-intervention ‘Clinical pharmacist annotation on medication charts’ was implemented before implementing smart pumps. Baseline data was collected after that intervention. |
High |
*For further details, see risk of bias table in the appendix
Results
Medication errors (critical)
Guerin (2015), Howlett (2020), Lyons (2018), Pang (2011) and Wiseman (2018) reported medication errors in traditional (without medication library) and smart pump (with medication libraries). A meta-analysis is shown in figure 1.
Guerin (2015) reported 1834 errors in the first year after implementation and 1389 errors in the second year after implementation of smart pumps compared to 1432 errors in the year before the implementation of smart pumps. The study could not be included in the meta-analysis as the total number of performed infusions was not reported.
The studies included in the meta-analysis reported 189 errors in 2538 infusions (7.3%) in the smart pump group compared to 306 errors in 2516 infusions (12.2%) in the traditional pump group (RR 0.63; 95%CI 0.45 to 0.87; RD at 12.2% baseline risk -0.05; 95%CI -0.07 to -0.02). The difference was clinically relevant in favor of smart pumps.
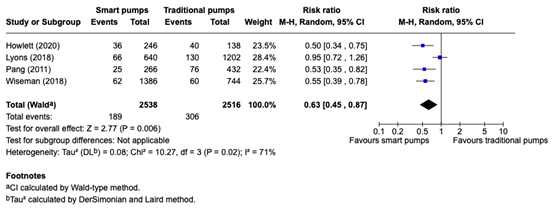
Figure 1. meta-analysis comparing medication errors between smart pumps (with medication library) to traditional pumps (without medication library)
Complications (critical)
Complications were not reported in the included studies.
Workload reduction (important)
Workload reduction was not reported in the included studies.
A systematic review of the literature was performed to answer the following question(s):
What is the effect of smart pumps (pumps with a medication library / dose error reduction system) compared to traditional pumps (no medication library/dose reduction error systems) in patients who are treated with medication infusion pumps?
Table 1. PICO
| Patients | Patients who are treated with medication infusion |
| Intervention | Use of smart pumps |
| Control | Use of traditional pumps |
| Outcomes | Medication errors, complications, workload reduction |
| Other selection criteria |
Study design: systematic reviews, randomized controlled trials, observational (comparing) studies Published ≥ year 2000 |
Relevant outcome measures
The guideline panel considered medication errors and complications as a critical outcome measure for decision making; and workload reduction as an important outcome measure for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
The guideline panel defined the following thresholds as a minimal clinically (patient) important difference:
- Medication error: Relative Risk (RR) 0.80≥RR≥1.25.
- Very serious complications (like mortality): 0.95≥RR≥1.05.
- Serious complications: 0.91≥RR≥1.10.
- Workload reduction: 10% of maximum score at a 1 to 100-scale.
Search and select (Methods)
A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 1 January 2000 to 5 September 2024 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) patients treated with medication infusion and (2) infusion pumps with medication library. Duplicates were removed using EndNote software. After deduplication a total of 138 records were imported for title/abstract screening. Initially, 31 studies were selected based on title and abstract screening. After reading the full text, 26 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and five studies were included.
- ECRI (2020) ISMP Guidelines for Optimizing Safe Implementation and Use of Smart Infusion Pumps.
- Guérin A, Tourel J, Delage E, Duval S, David MJ, Lebel D, Bussières JF. Accidents and Incidents Related to Intravenous Drug Administration: A Pre-Post Study Following Implementation of Smart Pumps in a Teaching Hospital. Drug Saf. 2015 Aug;38(8):729-36. doi: 10.1007/s40264-015-0308-6. PMID: 26108297.
- Howlett MM, Butler E, Lavelle KM, Cleary BJ, Breatnach CV. The Impact of Technology on Prescribing Errors in Pediatric Intensive Care: A Before and After Study. Appl Clin Inform. 2020 Mar;11(2):323-335. doi: 10.1055/s-0040-1709508. Epub 2020 May 6. PMID: 32375194; PMCID: PMC7202919.Lyons I, Furniss D, Blandford A, Chumbley G, Iacovides I, Wei L, Cox A, Mayer A, Vos J, Galal-Edeen GH, Schnock KO, Dykes PC, Bates DW, Franklin BD. Errors and discrepancies in the administration of intravenous infusions: a mixed methods multihospital observational study. BMJ Qual Saf. 2018 Nov;27(11):892-901. doi: 10.1136/bmjqs-2017-007476. Epub 2018 Apr 7. PMID: 29627799; PMCID: PMC6225796.
- Pang RKY, Kong DCM, deClifford JM, Lam SS, Leung BK. Smart infusion pumps reduce intravenous medication administration errors at an Australian teaching hospital. Journal of Pharmacy Practice and Research. 2011;41(3):192-5.
- Wiseman, M. L. and Poole, S. and Ahlin, A. and Dooley, M. J. Reducing intravenous infusion errors: an observational study of 16 866 patients over five years. Journal of Pharmacy Practice and Research. 2018; 48 (1) :49-55.
Risk of Bias tables
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors?
|
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables?
|
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed?
|
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Low, Some concerns, High |
|
|
Guerin (2015) |
Definitely no
Reason: different time frames |
Probably yes
Reason: Data extracted from local registry |
Definitely yes
Reason: Before-after study |
Probably no
Reason: No collection of confounding factors reported |
Definitely no
Reason: No matching or adjustments for confounding factors was reported |
Probably yes
Reason: Data extracted from local registry |
Probably yes
Reason: No missing data reported |
Probably yes
Reason: It is not described that other changes in care processes were implemented |
High |
|
Howlett (2020) |
Definitely no
Reason: different time frames |
Probably yes
Reason: Data extracted from databases |
Definitely yes
Reason: Before-after study |
Probably no
Reason: No collection of confounding factors reported |
Definitely no
Reason: No matching or adjustments for confounding factors was reported |
Probably yes
Reason: Data extracted from databases |
Definitely no:
Reason: 30% missing data reported in intervention group due to incomplete pharmacy records |
Probably yes
Reason: It is not described that other changes in care processes were implemented |
High |
|
Lyons (2018) |
Probably no
Reason: Patients treated with smart pumps were treated in other hospitals than patients treated with traditional pumps |
Probably yes Data collected by trained observers with standardized forms |
Probably yes Data collected by trained observers with standardized forms |
Probably no
Reason: No collection of confounding factors reported |
Definitely no
Reason: No matching or adjustments for confounding factors was reported |
Probably yes Data collected by trained observers with standardized forms |
Probably no
Reason: 15% missing data, not specified for different groups |
Probably no
Reason: Data collected for intervention and control group were collected in different hospitals |
High |
|
Pang (2011) |
Definitely no
Reason: different time frames |
Definitely yes Reason: data collected by independent observers |
Definitely yes
Reason: Before-after study |
Probably no
Reason: No collection of confounding factors reported |
Definitely no
Reason: No matching or adjustments for confounding factors was reported |
Definitely yes
Reason: data collected by independent observers |
Probably yes
Reason: No missing data reported |
Probably yes
Reason: It is not described that other changes in care processes were implemented |
High |
|
Wiseman (2018) |
Definitely no
Reason: different time frames |
Definitely yes
Reason: data collected by auditor |
Definitely yes
Reason: Before-after study |
Probably no
Reason: No collection of confounding factors reported |
Definitely no
Reason: No matching or adjustments for confounding factors was reported |
Definitely yes
Reason: data collected by auditor |
Probably yes
Reason: No missing data reported |
Probably yes
Reason: It is not described that other changes in care processes were implemented |
High |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Bates, D. W. Preventing medication errors: A summary. American Journal of Health-System Pharmacy. 2007; 64 (14) :S3-S9 |
Narrative review |
|
Blandford A, Furniss D, Galal-Edeen GH, Chumbley G, Wei L, Mayer A, Franklin BD. Intravenous infusion practices across England and their impact on patient safety: a mixed-methods observational study. Southampton (UK): NIHR Journals Library; 2020 Feb. PMID: 32040286. |
Same study as Lyons, 2018 |
|
Bowdle, T. A. and Jelacic, S. and Nair, B. and Togashi, K. and Caine, K. and Bussey, L. and Kruger, C. and Grieve, R. and Grieve, D. and Webster, C. S. and Merry, A. F. Facilitated self-reported anaesthetic medication errors before and after implementation of a safety bundle and barcode-based safety system. British Journal of Anaesthesia. 2018; 121 (6) :1338-1345 |
Does not fit PICO (wrong intervention: smart pumps as part of an safety bundle) |
|
Carayon, Pascale and Hundt, Ann Schoofs and Wetterneck, Tosha B. Nurses' acceptance of Smart IV pump technology. International journal of medical informatics. 2010; 79 (6) :401-11 |
Does not fit PICO (wrong outcome) |
|
Conroy, S. and Sweis, D. and Planner, C. and Yeung, V. and Collier, J. and Haines, L. and Wong, I. C. K. Interventions to reduce dosing errors in children: A systematic review of the literature. Drug Safety. 2007; 30 (12) :1111-1125 |
Scoping review |
|
Cour, M. and Hernu, R. and Bénet, T. and Robert, J. M. and Regad, D. and Chabert, B. and Malatray, A. and Conrozier, S. and Serra, P. and Lassaigne, M. and Vanhems, P. and Argaud, L. Benefits of smart pumps for automated changeovers of vasoactive drug infusion pumps: A quasi-experimental study. British Journal of Anaesthesia. 2013; 111 (5) :818-824 |
Other research question (prefilled syringe system compared) |
|
Escandell-Rico FM, Pérez-Fernández L. Analysis of medication errors in Neonatal Intensive Care: A systematic review. Med Intensiva (Engl Ed). 2024 Aug 16:S2173-5727(24)00221-2. doi: 10.1016/j.medine.2024.08.002. Epub ahead of print. PMID: 39153953. |
Systematic review not meeting quality criteria; potential relevant studies already included in search hits |
|
Giuliano, K. K. and Penoyer, D. and Mahuren, R. S. and Bennett, M. A descriptive comparison of primary and secondary infusion practices. Journal of Infusion Nursing. 2021; 44 (3) :128-136 |
Does not fit PICO (no comparison with traditional pump) |
|
Giuliano, K. K. IV Smart Pumps: The Impact of a Simplified User Interface on Clinical Use. Biomedical instrumentation & technology / Association for the Advancement of Medical Instrumentation. 2015; :13-21 |
Does not fit PICO (no comparison with traditional pump) |
|
Howlett, M. M. and Sutton, S. and McGrath, E. L. and Breatnach, C. V. Implementation of a national system for best practice delivery of paediatric infusions. International Journal of Clinical Pharmacy. 2024; 46 (1) :4-13 |
Does not fit PICO (no comparison with traditional pump) |
|
Joseph, R. and Lee, S. W. and Anderson, S. V. and Morrisette, M. J. Impact of interoperability of smart infusion pumps and an electronic medical record in critical care. American Journal of Health-System Pharmacy. 2020; 77 (15) :1231-1236 |
Does not fit PICO (smart pump interoperability compared to no interoperability) |
|
Kirkendall, E. S. and Timmons, K. and Huth, H. and Walsh, K. and Melton, K. Human-Based Errors Involving Smart Infusion Pumps: A Catalog of Error Types and Prevention Strategies. Drug Safety. 2020; 43 (11) :1073-1087 |
No comparison was made between conventional and smart pumps |
|
Kuitunen, S. K. and Niittynen, I. and Airaksinen, M. and Holmström, A. R. Systemic Defenses to Prevent Intravenous Medication Errors in Hospitals: A Systematic Review. Journal of patient safety. 2021; 17 (8) :e1669-e1680 |
Systematic review not meeting quality criteria; potential relevant studies already included in searchhits |
|
Larsen, G. Y. and Parker, H. B. and Cash, J. and O'Connell, M. and Grant, M. J. C. Standard drug concentrations and smart-pump technology reduce continuous-medication-infusion errors in pediatric patients. Pediatrics. 2005; 116 (1) :e21-e25 |
Does not fit PICO (wrong intervention: smart pumps as part of three interventions) |
|
Moreira, A. P. A. and Carvalho, M. F. and Silva, R. C. L. D. and Marta, C. B. and Fonseca, E. R. D. and Barbosa, M. T. S. Handling errors in conventional and smart pump infusions: A systematic review with meta-analysis. Revista da Escola de Enfermagem da U S P. 2020; 54 :e03562 |
Systematic review not meeting quality criteria; potential relevant studies already included in search hits |
|
Nuckols, T. K. and Bower, A. G. and Paddock, S. M. and Hilborne, L. H. and Wallace, P. and Rothschild, J. M. and Griffin, A. and Fairbanks, R. J. and Carlson, B. and Panzer, R. J. and Brook, R. H. Programmable infusion pumps in ICUS: An analysis of corresponding adverse drug events. Journal of General Internal Medicine. 2008; 23 (1) :41-45 |
Does not fit PICO (wrong outcome) |
|
Ohashi, K. and Dalleur, O. and Dykes, P. C. and Bates, D. W. Benefits and Risks of Using Smart Pumps to Reduce Medication Error Rates: A Systematic Review. Drug Safety. 2014; 37 (12) :1011-1020 |
Systematic review not meeting quality criteria; potential relevant studies already included in search hits or added to full-text selection (n=3) |
|
Orto, V. and Hendrix, C. C. and Griffith, B. and Shaikewitz, S. T. Implementation of a smart pump champions program to decrease potential patient harm. Journal of nursing care quality. 2015; 30 (2) :138-143 |
Does not fit PICO (no comparison with traditional pump) |
|
Palacios Rosas, E. and Soria-Cedillo, I. F. and Puértolas-Balint, F. and Ibarra-Pérez, R. and Zamora-Gómez, S. E. and Lozano-Cruz, E. and Amezcua-Gutiérrez, M. A. and Castro-Pastrana, L. I. Impact of Implementing Smart Infusion Pumps in an Intensive Care Unit in Mexico: A Pre-Post Cost Analysis Based on Intravenous Solutions Consumption. Hospital Pharmacy. 2019; 54 (3) :203-208 |
Does not fit PICO (wrong outcome) |
|
Paul JE, Bertram B, Antoni K, et al. Impact of a comprehensive safety initiative on patient-controlled analgesia errors. Anesthesiology. 2010;113(6):1427-32. |
Does not fit PICO (safety intervention) |
|
Perrigino, M. B. and Dunford, B. B. The unique effects of general and specific support in health care technology: An empirical examination of the principle of compatibility. Health care management review. 2016; 41 (4) :334-343 |
Does not fit PICO (no comparison with traditional pump) |
|
Prewitt, J. and Schneider, S. and Horvath, M. and Hammond, J. and Jackson, J. and Ginsberg, B. PCA safety data review after clinical decision support and smart pump technology implementation. Journal of patient safety. 2013; 9 (2) :103-109 |
Other research question (implementation of clinical support system and smart pumps) |
|
Rashed AN, Whittlesea C, Davies C, Forbes B, Tomlin S. Standardised concentrations of morphine infusions for nurse/patient-controlled analgesia use in children. BMC Anesthesiol. 2019 Feb 23;19(1):26. doi: 10.1186/s12871-019-0697-7. PMID: 30797229; PMCID: PMC6387512. |
Other research question (prefilled syringe system compared) |
|
Rosenkoetter, M. M. and Bowcutt, M. and Khasanshina, E. V. and Chernecky, C. C. and Wall, J. Perceptions of the impact of "Smart pumps" on nurses and nursing care provided. JAVA - Journal of the Association for Vascular Access. 2008; 13 (2) :60-70 |
Does not fit PICO (no comparison with traditional pump) |
|
Trbovich PL, Pinkney S, Cafazzo JA, Easty AC. The impact of traditional and smart pump infusion technology on nurse medication administration performance in a simulated inpatient unit. Qual Saf Health Care. 2010 Oct;19(5):430-4. doi: 10.1136/qshc.2009.032839. Epub 2010 Apr 27. PMID: 20427310; PMCID: PMC2975961. |
Does not fit PICO (mannequins were used instead of patients) |
|
Vitoux, R. R. and Lehr, J. and Chang, H. Eliminating Clinical Workarounds through Improved Smart Pump Drug Library Use. Biomedical instrumentation & technology / Association for the Advancement of Medical Instrumentation. 2015; :23-28 |
Does not fit PICO (no comparison with traditional pump) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 06-07-2026
Beoordeeld op geldigheid : 06-07-2026
Algemene gegevens
De ontwikkeling van deze leidraad werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de leidraad.
Samenstelling werkgroep
Voor het ontwikkelen van de leidraad is in 2023 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten die worden behandeld met infusietechnologie.
Werkgroep
- Dr. ir. A. M. D.E. (Annemoon) Timmerman (voorzitter), Klinisch Fysicus, UMC Utrecht, NVKF
- Ing. M.G.B.M. (Marc) Van Hauwe, Medisch Technoloog, Catharina Ziekenhuis, VZI
- Dr. ir. M.J.A. (Maurice) Janssen, Klinisch Fysicus, Zuyderland MC, NVKF
- Dr. V.C. (Verena) Mulder, Apotheker, Franciscus Gasthuis & Vlietland, NVZA
- Drs. K. (Kelly) Niggebrugge-Mentink, Ziekenhuisapotheker, HagaZiekenhuis, NVZA
- Ir. S.E. (Sanne) Vaartjes, Klinisch Fysicus, ZGT, NVKF
- L.H. (Linda) van de Werken, IC Verpleegkundige, UMC Utrecht, V&VN
- R. (Renze) Jongstra, IC Verpleegkundige, LUMC, V&VN (vanaf januari 2026)
Klankbordgroep
- Dr. M.J.L. (Martin) Bucx, Anesthesioloog, RadboudUMC, NVA
- Dr. H. (Hanneke) Buter, Intensivist, Frisius Ziekenhuis, NVIC
- Dr. ir. S.J.P.M. (Susanne) van Engelen, Adviseur Medische Technologie, LUMC, BMTZ
- Ir. ing. G.B.L. (Guido) Hendricks, Adviseur Medische Technologie, RadboudUMC, VZI
- B. (Britt) Ketelaars MSc, LLM, PF
- B. (Hugo) Versluis, Informatiemanager infuustechnologie, Erasmus MC, WIBAZ
- A. (Anne) ten Wolde, Biomedisch Technoloog, Prinses Máxima Centrum voor Kinderoncologie, BMTZ
Met ondersteuning van
- Drs. E. (Esther) van der Bijl, Informatiespecialist, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. P. (Phylisha) van Heemskerken, Junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. L.C. (Lotte) Houtepen, Adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. J.C. (José) Maas, Adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
|
Lid |
Functie |
Neven-werkzaamheden |
Gemelde belangen |
Ondernomen actie |
|
Janssen |
Zuyderland MC klinisch fysicus in dienstverband |
Geen |
Geen |
Geen restricties |
|
Jongstra |
IC verpleegkundige Volwassenen en Kinderen Circulation Practitioner Leiden Universitair Medisch Centrum |
*Voorzitter V&VN afdeling IC *IC verpleegkundige MICU ZuidWest Nederland |
Geen |
Geen restricties |
|
Mulder |
Apotheker Franciscus Gasthuis & Vlietland |
*Eigenaar Zicht op Kwaliteit; *Apotheker Ceban Clinic Services; *Deelnemer congres EAHP 2024, gedeeltelijk gefinancierd door Bayer (farmaceut) |
Geen |
Geen restricties |
|
Niggebrugge-Mentink |
Ziekenhuisapotheker, HagaZiekenhuis |
*NVZA (Nederlandse Vereniging voor Ziekenhuisapothekers): SIG Oncologie, voorzitter Expertgroep Arbo *Gastdocent Fontys Hogeschool (verpleegkundig specialist opleiding) |
* De richtlijn heeft betrekking op mijn werkveld (ziekenhuis), gedane kennis zal gebruikt kunnen worden om de processen in het HagaZiekenhuis te optimaliseren. Daarnaast gezien mandaat vanuit beroepsvereniging: kennis overdragen binnen de NVZA is denkbaar.Betrokken bij herziening WIP richtlijnen: SRI richtlijn intra-arteriele en veneuze katheters (als schrijver). Kennis kan over en weer toegepast worden. |
Geen restricties |
|
Timmerman |
Klinisch Fysicus - UMC Utrecht |
*Lid Raad van Advies School of Medical Physics Eindhoven (tot 31-01-2025) *Co-auteur position paper veilig gebruik infuuspompen t.b.v. BECTON, DICKINSON SWITZERLAND SÀRL *Gastdocent TU Eindhoven (infusie, ioniserende straling) *Lid NEN normcommissie infusie transfusie (tot 31-1-2025) |
* Vergoeding ontvangen in de 2022 en mrt 2023 (totaal €1416) t.b.v. Co-auteur position paper veilig gebruik infuuspompen van BECTON, DICKINSON SWITZERLAND SÀRL (BD). Bijbehorende raamovereenkomst voor consultancy van mei 2022 - mei 2024. Geen verdere lopende financiële contracten. Ik heb BD geïnformeerd de consultancy per direct te staken en een toezegging van BD dat deze raamovereenkomst z.s.m. wordt ontbonden. * EUROPEAN METROLOGY PROGRAMME FOR INNOVATION AND RESEARCH (EMPIR) 18HLT08 MeDDII Metrology for drug delivery II, €150000 (2019-2022) Geen belangenconflict op gebied van extern gefinancierd onderzoek van toepassing met betrekking tot het onderwerp medische technologie. Alle onderzoeksresultaten zijn Open Access en toegankelijk via Zenodo.org (toegevoegd per 27-11-2025: https://zenodo.org/communities/medd2/records?q=&l=list&p=1&s=10&sort=newest) * EU, EURAMET - Multi-infusie - Geen projectleider (toegevoegd per 27-11-2025) Wel verantwoordelijk voor een Work Package (Work Package Leader WP4) |
Geen restricties |
|
Vaartjes |
Klinisch Fysicus, ZGT |
Geen |
Geen |
Geen restricties |
|
Van de Werken |
UMC Utrecht, |
Geen |
Geen |
Geen restricties |
|
Van Hauwe |
Medisch Technoloog Catharina Ziekenhuis Eindhoven |
Regiocoördinator VZI Medisch Coördinator Kennedymars Someren
Per 24-11-2025: Geen |
*Operationeel, bekend bij de twee grootste leveranciers van infuuspompen. Er loopt op dit moment een oriëntatie vervanging infuuspompen. Ben ik onafhankelijk, ja, beide hebben een doordacht concept, integrale keuze noodzakelijk, ben hierin geen projectleider. * Onderzoek binnen CZE naar toepasbaarheid van Ready-to-Administer spuiten. Uitkomst: grote voordelen, maar niet altijd veilig toepasbaar. Plannen om CZE productie-apotheek te verzelfstandigen, waarbij ik binnen het CZE blijf - Geen projectleider
Per 1 april 2025 aanvulling op bovenstaande: * Samenwerkingsverband Catharina Ziekenhuis met PharmaHelder t.a.v. op de markt brengen van voorgevulde spuiten
Per 24-11-2025 herformulering belangen: *Onderzoek binnen Catharina Ziekenhuis naar toepasbaarheid van Ready-to-Administer spuiten. * M.b.t. samenwerkingsverband Catharina Ziekenhuis met PharmaHelder t.a.v. op de markt brengen van voorgevulde spuiten: reductie belangenbehartiging, impact is tijdens het schrijven al gereduceerd. De samenwerking met de apotheek heeft weinig vervolg meer gekregen. |
Gezien de potentiële belangen ten aanzien van voorgevulde spuiten worden de aanbevelingen van module spuiten kritisch nagelezen door de werkgroep. Daarnaast wordt in de commentaarfase de NVKF gevraagd om een onafhankelijk reviewer kritisch naar de module spuiten te laten kijken. |
|
Van Reijen (tot 19-12-2024) |
Technisch Thuiszorg Verpleegkundige, Stichting tanteLouise |
Bestuurslid bij de TTV van de V&VN |
Geen |
Geen restricties |
|
Bucx |
Anesthesioloog, Radboudumc |
Geen |
Geen |
Geen restricties |
|
Buter |
Intensivist Medisch Centrum Leeuwarden |
Bestuurslid NVIC |
Geen |
Geen restricties |
|
Hendricks |
Adviseur medische technologie - Radboudumc Nijmegen |
Geen
Aanvulling per 2-12-2025: *Gastdocent INTOP zorgsector - Elektriciteitsleer en Medische-elektrische apparatuur |
Geen |
Geen restricties |
|
Ketelaars |
Adviseur patiëntbelang bij Patiëntenfederatie Nederland, full time, betaald. |
Geen |
Geen |
Geen restricties |
|
Ten Wolde |
Biomedisch technoloog, Prinses Máxima Centrum voor Kinderoncologie |
Communicatiecommissie BMTZ |
*Innovatief karakter Prinses Máxima Centrum. Voortrekkersrol ziekenhuis op het gebied van stille alarmering, closed-loop medicatie. *Initiator kennisdeelsessies BMTZ-infusietechnologie. |
Geen restricties |
|
Van Engelen |
LUMC, adviseur medische technologie |
Geen |
Geen |
Geen restricties |
|
Versluis |
Informatiemanager Infuustechnologie Erasmus MC |
Geen |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door uitnodigen van Patiëntenfederatie Nederland voor de schriftelijke knelpuntenanalyse en door deelname van een afgevaardigde van deze patiëntenorganisatie in de klankbordgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, en bij het opstellen van de overwegingen van de modules. De conceptleidraad is tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de leidraad voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de leidraad per module op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Medicatiebibliotheken |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte methodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze leidraad is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Database(s): Embase.com, Ovid/Medline |
Datum: 5 september 2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
Zoekopbrengst - 5 september 2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
19 |
18 |
21 |
|
RCT |
33 |
26 |
41 |
|
Observationele studies |
68 |
59 |
76 |
|
Totaal |
120 |
103 |
138* |
*in Rayyan
Zoekstrategie - 5 september 2024
Embase.com
|
No. |
Query |
Results |
|
#1 |
'infusion pump'/exp OR 'infusion'/exp OR 'drug infusion'/exp OR (('drug administration'/exp OR 'drug delivery device'/exp OR ((drug* NEAR/3 (administrat* OR infiltrat* OR injecti*)):ti,ab,kw)) AND ('infusion'/exp OR infusion*:ti,ab,kw OR pump*:ti,ab,kw)) OR infusion*:ti,ab,kw OR 'alaris':ti,ab,kw OR 'asena':ti,ab,kw OR 'cadd solis vip':ti,ab,kw OR 'gemstar':ti,ab,kw OR 'graseby 3500':ti,ab,kw OR 'infu disk':ti,ab,kw OR 'medex c-fusor':ti,ab,kw OR 'mip':ti,ab,kw OR 'medfusion 4000':ti,ab,kw OR 'medstream':ti,ab,kw OR 'metriq':ti,ab,kw OR 'microinfusion pump':ti,ab,kw OR 'minimed quick-set':ti,ab,kw OR 'minimed silhouette':ti,ab,kw OR 'minimed sure-t':ti,ab,kw OR 'minimed mio':ti,ab,kw OR 'mio advance':ti,ab,kw OR 'neosyp':ti,ab,kw OR 'neofuser':ti,ab,kw OR 'on-q painbuster':ti,ab,kw OR 'plum 360':ti,ab,kw OR 'pompa infonde':ti,ab,kw OR 'renalguard':ti,ab,kw OR 'sigma spectrum':ti,ab,kw OR 'spectrum iq':ti,ab,kw OR 'statcorp':ti,ab,kw OR 'surefuser':ti,ab,kw OR 'terufusion':ti,ab,kw OR 'trusteel':ti,ab,kw OR 'z-800f':ti,ab,kw OR 'z-800w':ti,ab,kw OR 'z-800wf':ti,ab,kw OR 'iprecio':ti,ab,kw OR 'infusor*':ti,ab,kw OR 'inset 30':ti,ab,kw OR 'inset ii':ti,ab,kw OR 'intravenous pressure infusor*':ti,ab,kw OR 'perfusion pump*':ti,ab,kw |
504177 |
|
#2 |
'smart pump'/exp OR 'drug library'/exp OR (((pump* OR drug* OR medicat*) NEAR/3 librar*):ti,ab,kw) OR (ders:ti,ab,kw AND pump*:ti,ab,kw) OR ((smart NEAR/3 pump*):ti,ab,kw) OR 'dose error reduction system*':ti,ab,kw |
3209 |
|
#3 |
#1 AND #2 |
436 |
|
#4 |
#3 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
304 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1059097 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4101308 |
|
#7 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8393535 |
|
#8 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
15370224 |
|
#9 |
#4 AND #5 - SR |
19 |
|
#10 |
#4 AND #6 NOT #9 - RCT |
33 |
|
#11 |
#4 AND (#7 OR #8) NOT (#9 OR #10) - Observationeel |
68 |
|
#12 |
#9 OR #10 OR #11 - Totaal |
120 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Infusion Pumps/ or ((Drug Delivery Systems/ or exp Drug Administration Routes/ or (drug* adj3 (administrat* or infiltrat* or injecti*)).ti,ab,kf.) and (infusion* or pump*).ti,ab,kf.) or infusion*.ti,ab,kf. or alaris.ti,ab,kf. or asena.ti,ab,kf. or cadd solis vip.ti,ab,kf. or gemstar.ti,ab,kf. or graseby 3500.ti,ab,kf. or infu disk.ti,ab,kf. or medex c-fusor.ti,ab,kf. or mip.ti,ab,kf. or medfusion 4000.ti,ab,kf. or medstream.ti,ab,kf. or metriq.ti,ab,kf. or microinfusion pump.ti,ab,kf. or minimed quick-set.ti,ab,kf. or minimed silhouette.ti,ab,kf. or minimed sure-t.ti,ab,kf. or minimed mio.ti,ab,kf. or mio advance.ti,ab,kf. or neosyp.ti,ab,kf. or neofuser.ti,ab,kf. or on-q painbuster.ti,ab,kf. or plum 360.ti,ab,kf. or pompa infonde.ti,ab,kf. or renalguard.ti,ab,kf. or sigma spectrum.ti,ab,kf. or spectrum iq.ti,ab,kf. or statcorp.ti,ab,kf. or surefuser.ti,ab,kf. or terufusion.ti,ab,kf. or trusteel.ti,ab,kf. or z-800f.ti,ab,kf. or z-800w.ti,ab,kf. or z-800wf.ti,ab,kf. or iprecio.ti,ab,kf. or infusor*.ti,ab,kf. or inset 30.ti,ab,kf. or inset ii.ti,ab,kf. or intravenous pressure infusor*.ti,ab,kf. or perfusion pump*.ti,ab,kf. |
306678 |
|
2 |
(((pump* or drug* or medicat*) adj3 librar*) or (ders and pump*) or (smart adj3 pump*) or dose error reduction system*).ti,ab,kf. |
2165 |
|
3 |
1 and 2 |
283 |
|
4 |
limit 3 to yr="2000 -Current" |
279 |
|
5 |
4 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
271 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
772307 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2773875 |
|
8 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4819732 |
|
9 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5777673 |
|
10 |
5 and 6 - SR |
18 |
|
11 |
(5 and 7) not 10 - RCT |
26 |
|
12 |
(5 and (8 or 9)) not (10 or 11) - Observationeel |
59 |
|
13 |
10 or 11 or 12 - Totaal |
103 |