Doorgebruik van thuismedicatie
Uitgangsvraag
Hoe kan de inzet van doorgebruik van thuismedicatie (DGTM) in het ziekenhuis de milieu-impact verminderen?
Aanbeveling
Kies bij opname van een patiënt voor doorgebruiken van thuismedicatie, mits deze werkwijze past bij het distributiesysteem in het ziekenhuis en het adequaat wordt geïmplementeerd.
Combineer voor een maximaal effect op patiëntbetrokkenheid, doelmatigheid en medicatieveiligheid het doorgebruik van thuismedicatie met medicatie in eigen beheer, indien de klinische situatie dit toelaat.
Overwegingen
Kwaliteit van bewijs
Deze module evalueert de milieu-impact van doorgebruik van thuismedicatie (DGTM) tijdens opname in het ziekenhuis. Er is literatuuronderzoek uitgevoerd en hierbij is een studie gevonden conform de PICO (van Herpen-Meeuwissen, 2019), waarbij de uitkomstmaat verspilling (‘medicatiespillage’) is gerapporteerd. Medicatiespillage werd uitgedrukt in aantallen. Het prospectieve onderzoek evalueerde medicatiespillage gedurende een periode van twee maanden voor en na implementatie van DGTM en verrichte deze evaluatie op acht afdelingen verdeeld over zeven ziekenhuizen. Er werden geen studies gevonden voor de overige uitkomstmaten (i.e. ‘climate change’, ‘eco-toxicity’, ‘human toxicity’, ‘water use’, ‘land use’, ‘acidification’, ‘eutrophication’).
De kwaliteit van bewijs is zeer laag. Dit betekent dat we zeer onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten. Er is afgewaardeerd vanwege (zeer) ernstig risico op bias, indirectheid en imprecisie. Op basis van deze GRADE beoordeling van de literatuur kunnen geen sterke conclusies geformuleerd worden over de precieze mate van milieu-impact van DGTM in het ziekenhuis. Echter, ondanks de methodologische beperkingen van het onderzoek, wijzen de resultaten wel op een potentiële vermindering van medicatieverspilling als gevolg van DGTM.
Balans tussen gewenste en ongewenste effecten
Bij DGTM brengen patiënten hun eigen medicatie naar het ziekenhuis en worden deze medicatie vervolgens tijdens hun ziekenhuisverblijf door verpleegkundigen toegediend. Wanneer dit wordt gecombineerd met medicatie in eigen beheer (MIEB), beheren geschikte patiënten ook zelf hun medicatiegebruik tijdens ziekenhuisverblijf, waaronder de opslag en toediening van hun medicatie (Van Herpen-Meeuwissen, 2023a). In de literatuur en praktijk zijn beiden niet altijd goed van elkaar te onderscheiden en daarom wordt hieronder veelal gesproken over DGTM/MIEB.
Het doorgebruiken van thuismedicatie gedurende een ziekenhuisopname heeft meerdere gewenste effecten. Hoewel het onderzoek van Van Herpen-Meeuwissen (2019) geen directe milieueffecten beschrijft, lijkt het op de meeste afdelingen waar DGTM/MIEB geïmplementeerd is wel tot minder spillage van medicatie te leiden. Het verminderen van medicatie-afval draagt bij aan duurzaamheid, doordat minder afval vervoerd en verbrand hoeft te worden en daarmee ook de CO₂-uitstoot afneemt. Wanneer medicatie helemaal niet hoeft te worden weggegooid – bijvoorbeeld doordat deze zorgvuldig en volledig aan de patiënt wordt meegegeven – ontstaat er minder vraag naar productie, transport en opslag. Dit resulteert wederom in een lagere CO₂-uitstoot en een positieve impact op het milieu (Bekker, 2018). Kanttekening hierbij is dat in de studie van Van Herpen-Meeuwissen geen totale afname van de medicatiespillage werd gezien (Van Herpen-Meeuwissen, 2019). Dit is het gevolg van het onjuist implementeren van de werkwijze op een van de zes afdelingen. Hierdoor werd op deze afdeling juist meer medicatie verspild. Dat een goede implementatie bijdraagt aan mindere spillage van medicatie en daarmee een positief effect op de milieubelasting laten ook twee pilot onderzoeken in de Nederlandse setting zien. De werkgroep is bekend met gegevens uit het Elisabeth-Tweesteden ziekenhuis (ETZ) waar implementatie van DGTM gecombineerd met MIEB zorgde voor een afname van de medicatiespillage met 44% (data opvraagbaar bij ETZ, Tilburg). Ook in het UMCG zorgde de implementatie van DGTM met MIEB voor een afname van de medicatiespillage van ruim boven de 40% (Van den Bemt, 2024). Tevens wordt internationaal geconcludeerd dat DGTM met MIEB bijdraagt aan duurzaamheid (Lummis, 2006). De pilotstudie van Duyvendak en Sikking laat echter zien dat het gebruikte distributiesysteem en de gezondheidsvaardigheden van patiënten belangrijke randvoorwaarden voor implementatie zijn (Duyvendak, 2022). Hieruit concludeert de werkgroep dat DGTM/MIEB, indien adequaat geïmplementeerd, een positieve impact heeft op duurzaamheid. Mede op basis van ervaringen tijdens bovenstaande (pilot) onderzoeken hebben de NVZA, UMCNL en KNMP, in het kader van de Green Deal Duurzame Zorg 3.0, een toolkit ontwikkeld welke handvatten biedt voor een adequate implementatie van DGTM (al dan niet in combinatie met MIEB) (toolkit DoorGebruik ThuisMedicatie/Medicatie in Eigen Beheer (DGTM/MEB)). De werkgroep raadt aan om deze toolkit te gebruiken om een adequate implementatie te bewerkstelligen en daarmee de grootste impact te realiseren op het gebied van duurzaamheid.
Naast de positieve bijdrage die DGTM/MIEB levert op het gebied van duurzaamheid kent het voordelen op het gebied van medicatieveiligheid en therapietrouw, wat indirect een positeive bijdrage levert op duurzaamheid omdat het de zorgvraag doet verlagen. DGTM/MIEB lijkt bij te dragen aan het verbeteren van medicatieveiligheid, onder andere door de afname van medicatiefouten tijdens ziekenhuisopname (Kaday, 2020; Sørensen, 2020a; Sørensen, 2020b). DGTM/MIEB kan het foutpercentage reduceren met 24–100% en leidt tot 44% minder medicatieverschillen na ontslag (Sørensen, 2020a; Sørensen, 2020b). Daarnaast lijkt het een positief effect te hebben op therapietrouw (Hajialibeigloo, 2021; Kaday, 2020; Sørensen, 2020b), hoewel dit niet bevestigd werd in een onderzoek in de Nederlandse setting, mogelijk door verschillen in uitvoering en meetinstrumenten (Van Herpen-Meeuwissen, 2022c). Studies rapporteren ook dat bij patiënten meer inzicht en kennis over medicatie lijkt op te treden door DGTM/MIEB, wat het goed gebruik van de medicatie in de thuissituatie bevordert (Kaday, 2020; Sørensen, 2020a; Sørensen, 2020b). DGTM vergroot ook het zelfgerapporteerde kennisniveau over medicatie bij patiënten (Van Herpen-Meeuwissen, 2022c). Literatuur bevestigt kennisverbetering na MIEB-deelname (Beigloo, 2019; Kaday, 2020; Polito, 2022). Deze verhoogde kennis kan leiden tot betere therapietrouw en veiligheid (Náfrádi, 2017; Najjar, 2015; Okuyan, 2013; Salama, 2017; WHO, 2003). Als laatste zorgt DGTM/MIEB ook voor een verbetering in de perceptie van patiënt wat betreft veiligheid. Meer patiënten geven aan een veiliger gevoel te hebben wanneer zij hun thuismedicatie doorgebruiken (Van Herpen-Meeuwissen, 2022c).
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Een belangrijk voordeel van DGTM/MIEB is dat het patiëntparticipatie kan vergroten, wat mogelijk leidt tot hogere patiënttevredenheid. MIEB sluit aan bij de maatschappelijke trend waarin mensen meer betrokken willen zijn bij beslissingen in hun zorg (Canadian Institutes of Health Research, 2018; Patiëntenfederatie Nederland; The Joint Commission, 2021; World Health Assembly, 2016; WHO, 2013). Met MIEB, en deels met DGTM, krijgen patiënten meer regie over hun medicatie, wat hun zelfstandigheid en gevoel van controle versterkt (National Prescribing Centre, 2008). Uit onderzoek bleek dat 82% DGTM verkiest boven standaardzorg, en 62% ook zelf medicatie wil toedienen (Van Herpen-Meeuwissen, 2022c).
Belanghebbenden vanuit het zorgveld en patiënten bevestigden deze voordelen en benadrukten dat DGTM/MIEB patiënten beter voorbereidt op medicatiegebruik na ontslag (Van Herpen-Meeuwissen, 2022b; 2023b). Ook de internationale literatuur toont aan dat DGTM/MIEB tijdens ziekenhuisopname leidt tot hogere patiënttevredenheid (Beigloo, 2019; Deeks, 2000; Sørensen, 2020a; Sørensen, 2020b). Binnen de kindergeneeskunde zou DGTM/MIEB door mantelzorgers, veelal ouders, autonomie en gevoel van controle over hun vaak zorgcomplexe kind in een vaak oncontroleerbare (onzekere) setting kunnen geven. Dit is positieve ontwikkeling is voor de pediatrische patiëntenpopulatie en hun mantelzorgers.
De ongewenste effecten op patiëntrelevante uitkomstmaten zijn onbekend. Er zijn zorgen dat DGTM/MIEB mogelijk zou kunnen leiden tot medicatiefouten, bijvoorbeeld doordat de kwaliteit van de medicatie niet kan worden gegarandeerd (omdat het bij de patiënt thuis is geweest) of de verpakking van de medicatie er anders uit kan zien waardoor het niet als zodanig wordt herkend door de verpleging. Deze mogelijk geïntroduceerde risico’s dienen te worden ondervangen door adequate implementatie van DGTM/MIEB waarbij patiënten en zorgverleners goed worden geïnformeerd waarbij technische ondersteuning in het Elektronisch Patienten Dossier (EPD) wenselijk is. Met beheersbare risico’s en vele voordelen zoals het stimuleren van de continuïteit van zorg, het voorkomen van medicatiefouten en bevorderen van het gebruik van medicatie in de thuissituatie (Kaday, 2020; Polito, 2022; Sørensen, 2020a; Sørensen, 2020b) zal de implementatie positief zijn voor de patiënt. Samen beslissen over DGTM/MIEB is belangrijk, met name bij kwetsbare patiënten.
Kostenaspecten
Patiëntparticipatie draagt bij aan betaalbare zorg (World Health Assembly, 2016; WRR, 2021). Daarnaast lijkt DGTM/MIEB bij te dragen aan doelmatige zorg en realiseert het een afname in tijdsinvestering van ziekenhuismedewerkers op gebied van de medicatielogistiek (Van Herpen-Meeuwissen, 2023a) en daarmee een indirecte besparing. Tevens levert DGTM vergelijkbare medicatiekosten ten opzichte van medicatieverstrekking door de ziekenhuisapotheek voor het ziekenhuis (Verdijk, 2024). Momenteel wordt thuismedicatie gedurende ziekenhuisopname bekostigd in de DBC-structuur als algemene kosten tijdens een ziekenhuisopname. Voor de bekostiging van nieuw geleverde thuismedicatie dient het ziekenhuis afspraken te maken met de verzekeraar conform het advies van de Nederlandse Zorgautoriteit (NZa, 2019).
Hierbij is hervorming van de financiële structuur in de Nederlandse gezondheidszorg wenselijk om het tijdens ziekenhuisopname mogelijk te maken dat nieuwe thuismedicatie en bijbehorende zorg (onder andere prestatie eerste uitgifte gesprek) bekostigd worden.
Gezondheidsgelijkheid
De interventie leidt niet tot een verschil in gezondheidsgelijkheid. Immers, de medicatie is reeds in bezit van de patiënt en medicatie is vrijwel allemaal vergoede zorg via het Geneesmiddel Vergoedingssysteem (GVS). Deze vergoeding valt wel onder het eigen risico en kan dus voelen als zelf betaald. Echter, een ziekenhuisopname zal altijd zorgen dat een patiënt het volledige eigen risico zal moeten betalen.
Aanvaardbaarheid
Ethische aanvaardbaarheid
De interventie lijkt aanvaardbaar voor de betrokkenen. De werkgroep voorziet geen ethische bezwaren en deze zijn ook niet genoemd in de onderzoeken naar de implementatie van MIEB (Van Herpen-Meeuwissen, 2023b; Smale, 2025), die beiden keken naar onder andere de haalbaarheid van en vereiste voor implementatie van DGTM/MIEB in de Nederlandse setting. Er wordt de patiënt geen extra handeling opgelegd behoudens het zelf meenemen van de thuismedicatie (en indien geschikt zelf gebruiken van de medicatie). De patiënt zal mogelijk meer autonomie ervaren en meer controle hebben over de situatie (van Herpen-Meeuwissen, 2022b; van Herpen-Meeuwissen, 2023a). De ervaring leert dat ook zorgverleners positief zijn over deze nieuwe werkwijze. Wel zullen patiënten in staat moeten zijn om verantwoordelijkheid te nemen voor de eigen medicatie inname. Het is de gezamenlijke verantwoordelijkheid van het ziekenhuis en de patiënt om te borgen dat medicatie juist is opgeslagen (thuis en in het ziekenhuis), de medicatie nog houdbaar is en de medicatie correct wordt ingenomen. De continuïteit van thuismedicatie gebuik is belangrijk (vanuit eigen voorraad patiënt, danwel hetzelfde middel in het ziekenhuis – zie ook overwegingen leidraad Verantwoord Wisselen Medicijnen (Patiëntenfederatie Nederland, 2024). Eventuele aanpassingen vinden in overleg met de patiënt en/of initiële voorschrijver plaats.
Duurzaamheid
Deze module is volledig gericht op het verlagen van milieu-impact, derhalve speelt duurzaamheid een doorslaggevende- en hoofdrol bij de beschreven vergelijkingen.
Haalbaarheid
De haalbaarheid van DGTM/MIEB hangt af van de communicatie rondom het doorgebruik, de bereidheid van de zorgverlener om dit te doen en de veiligheid en controle op het gebruik van thuismedicatie. Het is belangrijk de administratie van DGTM/MIEB kritisch te beoordelen en te borgen dat de juiste medicatie correct en betrouwbaar in het EPD wordt geregistreerd. De toolkit DoorGebruik ThuisMedicatie/Medicatie in Eigen Beheer (DGTM/MEB) kan worden gebruikt om de implementatie te bevorderen. Momenteel wordt DGTM/MIEB al toegepast op een aantal ziekenhuisafdelingen in verschillende ziekenhuizen in Nederland.
Bij deze module is een implementatieplan opgesteld, dat ondersteuning biedt bij het (verder) in de praktijk brengen van de aanbevelingen.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Ondanks de zeer lage bewijskracht en beperkte beschikbare data, formuleert de werkgroep sterke richtinggevende aanbevelingen, gebaseerd op overige literatuur, praktijkervaringen en expert opinie van de werkgroepleden. Hiermee streeft de werkgroep naar meer bewustwording omtrent het milieu bij medicatiegebruik tijdens een ziekenhuisopname. De werkgroep is van mening dat redelijkerwijs kan worden aangenomen dat DGTM/MIEB leidt tot een reductie van medicatieafval mits de werkwijze goed geïmplementeerd is. Tevens lijken er positieve effecten van DGTM/MIEB te zijn op gebied van medicatieveiligheid, patiëntparticipatie en doelmatigheid. De werkgroep ziet noodzaak om meer onderzoek te doen naar de milieu-impact van DGTM/MIEB; hier ligt een kennislacune.
Onderbouwing
Currently, it is common practice for hospitals to provide all necessary medication during a patient’s hospitalization. However, continued use of the patient’s own medication (POM) in the hospital setting (in Dutch: “doorgebruik thuismedicatie”; DGTM) offers patients the opportunity to maintain more control over their treatment. Continued POM use implies that the patients bring their own medication, which is administered by healthcare staff, possibly in combination with self-administration of medication (SAM). Continued use of the POM during hospital admission may reduce medication waste and, consequently, lower environmental impact, by allowing uninterrupted use of existing medication during hospital admission and discharge. This is particularly relevant for medication with a short shelf life after opening, such as eye drops. SAM may further enhance adherence, helping to prevent unnecessary medication waste as nonadherence may increase medication waste. The aim of this module is to provide recommendations on continued use of POM during hospital admission, based on environmental considerations.
1. Climate change (critical)
|
No GRADE |
No outcomes on climate change were reported.
Source: - |
2. Waste (critical)
|
Very low GRADE |
The evidence is very uncertain about the effect of using patient’s own medication on waste in hospitalized patients.
Source: (van Herpen-Meeuwissen, 2019) |
3. Eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
|
No GRADE |
Outcome measures ‘eco-toxicity’, ‘human toxicity’, ‘water use’, ‘land use’, ‘acidification’, and ‘eutrophication’ were not reported.
Source: - |
Description of studies
One study was included in the analysis of the literature (van Herpen-Meeuwissen, 2019) Important study characteristics and results are summarized in the Evidence table. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Van Herpen-Meeuwissen (2019) aimed to evaluate the economic effects of allowing patients to use their own medications (patient’s own medication, POM) during hospitalization. The methodology involved a multicenter, prospective pre-post intervention design conducted across eight wards in seven Dutch hospitals. Data were collected over two distinct 2-month periods.
Before the implementation of POM, hospitals had to manage medications that were ordered but not used, leading to the disposal of unused medications. After implementing POM, patients brought their own medications to the hospital, which were then used instead of prescribing new ones. This practice reduced the need for the hospital to supply and dispose of excess medications that were often wasted. Medication waste was presented in this study through units.
Results
1. Climate change (critical)
No studies were found for the outcome climate change.
2. Waste (critical)
Van Herpen-Meeuwissen (2019) reported a total quantity of 1787 individual units of medication wasted per 100 patient days prior to implementation of POM and 2053 individual units of wasted medication post introduction of POM. This shows an average increase of 14.9% in medication units wasted. However, there was much variability between wards. Four wards found a reduction in medication wastage, as seen in Figure 1. As an explanation for this, it was suggested that one ward was not sufficiently prepared to implement the new strategy, leading to double orders of medication.
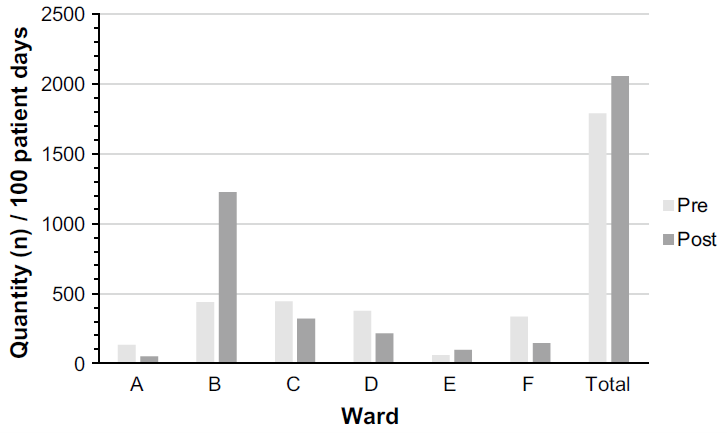
Figure 1. The quantity (n = individual units) of wasted medication per 100 patient days during the pre- and post-implementation of POM use during hospitalisation on the participating medical wards
Adopted from Van Herpen-Meeuwissen (2019)
3. Eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
No studies were found on important outcome measures eco-toxicity, human toxicity, water use, land use, acidification, and eutrophication.
Level of evidence of the literature
1. Climate change (critical)
The outcome measure climate change was not reported, thus could not be graded.
2. Waste (critical)
The level of evidence regarding the outcome measure medication waste was downgraded with three levels to very low due to risk of bias (-1; lack of adequate adjustment for confounders, short follow-up period), indirectness (-1; the outcomes were presented through units, but not in weight) and imprecision (-1; due to variability and inconsistency in the findings).
3. Eco-toxicity (important), human toxicity (important), water use (important), land use
Outcomes were not reported, thus could not be graded.
A systematic review of the literature was performed to answer the following question:
What is the difference in environmental impact between patient’s own medication use and medication dispensed from the hospital pharmacy during hospitalization?
Table PICO
| Patients | Hospitalized patients receiving pharmaceutical treatment |
| Intervention | Patient’s own medication (POM) use during hospitalization (possibly combined with self-administration of medication (SAM)) |
| Control | Medication dispensed from the hospital pharmacy during hospitalization |
| Outcomes | Climate change (CO2 footprint/Global Warming Potential (GWP)), waste, eco-toxicity, human toxicity, water use, land use, acidification, eutrophication |
| Other selection criteria |
Study design: systematic reviews, randomized controlled trials, comparative observational studies (cohort studies, case-control studies), life cycle assessments Period: from 2010 |
Relevant outcome measures
This module focuses specifically on environmental outcomes. Currently, there is no standardized or acknowledged core outcome set available in the field of environmental impact. Therefore, the guideline panel focused on outcomes used in environmental assessments, like life cycle assessments, material flow analyses, waste audits, or footprints.
The guideline panel considered climate change (CO2 footprint/Global Warming Potential) and waste as critical outcome measures for decision making; and eco-toxicity, human toxicity, water use, land use, acidification, and eutrophication as important outcome measures for decision making.
A priori, the guideline panel defined the outcome measures listed above according to the glossary provided in Box 1, which is adapted from leidraad Duurzaamheid in richtlijnen.
Given the variety in scopes and methods of performing and reporting in studies, the guideline panel did not define a priori the minimal important difference. Differences between the interventions were evaluated by the guideline panel after data extraction.
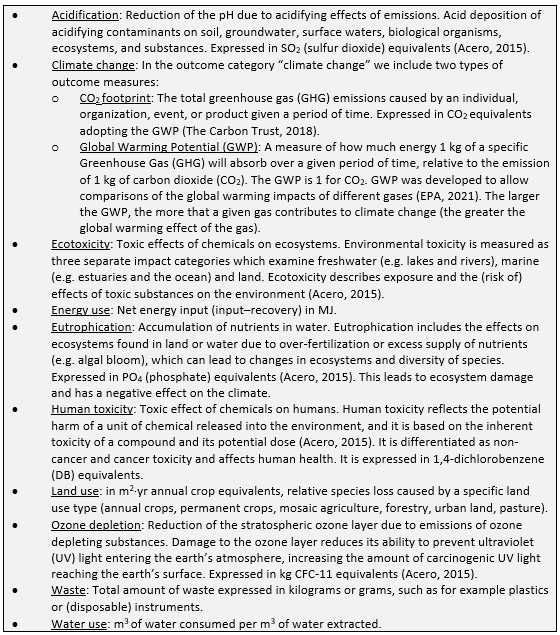
Box 1. Glossary
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2000 until 17 October 2024. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 601 unique results.
Studies were selected based on the following criteria:
- Systematic reviews in which searches were performed in at least two databases, with a detailed search strategy, available exclusion reasons for potentially relevant studies that were excluded after reading the full text, risk of bias assessment and results of individual studies available, randomized controlled trials, (observational) comparative studies, LCA.
- Full-text English or Dutch language publication and
- Studies according to the PICO.
Initially, twelve studies were selected based on the title and abstract screening. After reading the full text, eleven studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’) and one study was included (van Herpen-Meeuwissen, 2019).
- Beigloo RHA, Mohajer S, Eshraghi A, Mazlom SR. Self-administered medications in cardiovascular ward: a study on patients’ self-efficacy, knowledge and satisfaction. Evid Based Care J. 2019;9(1):16–25.
- Bekker CL. Sustainable use of medication: Medication waste and feasibility of redispensing [thesis]. Utrecht: Utrecht University; 2018. ISBN: 978‑90‑393‑7045‑2. Beschikbaar via: https://dspace.library.uu.nl/handle/1874/371914.
- Canadian Institutes of Health Research. Strategy for patient-oriented research: patient engagement framework [Internet]. Ottawa: CIHR; 2018 [cited 2025 Jul 21]. Available from: http://www.cihr-irsc.gc.ca/e/45851.html.
- Duyvendak M, Sikking C. Spillage in een perifeer ziekenhuis: inzet van geautomatiseerde systemen voor optimale medicatieveiligheid en duurzaamheid met aandacht voor doorgebruik thuismedicatie. Nederlands Platform voor Farmaceutisch Onderzoek. 2022;7:a1753
- Deeks PA, Byatt K. Are patients who self-administer their medicines in hospital more satisfied with their care? J Adv Nurs. 2000 Feb;31(2):395-400. doi: 10.1046/j.1365-2648.2000.01286.x. PMID: 10672098.
- Hajialibeigloo R, Mazlum SR, Mohajer S, Morisky DE. Effect of self-administration of medication programme on cardiovascular inpatients' medication adherence and nurses' satisfaction: A randomized clinical trial. Nurs Open. 2021 Jul;8(4):1947-1957. doi: 10.1002/nop2.870. Epub 2021 Apr 3. PMID: 33811803; PMCID: PMC8186674.
- Kaday R, Ratanajamit C. Inpatient self-administered medication under the supervision of a multidisciplinary team: a randomized, controlled, blinded parallel trial. Pharm Pract (Granada). 2020 Apr-Jun;18(2):1766. doi: 10.18549/PharmPract.2020.2.1766. Epub 2020 Apr 19. PMID: 32377277; PMCID: PMC7194043.
- Lummis H, Sketris I, Veldhuyzen van Zanten S. Systematic review of the use of patients' own medications in acute care institutions. J Clin Pharm Ther. 2006 Dec;31(6):541-63. doi: 10.1111/j.1365-2710.2006.00773.x. PMID: 17176360.
- Náfrádi L, Nakamoto K, Schulz PJ. Is patient empowerment the key to promote adherence? A systematic review of the relationship between self-efficacy, health locus of control and medication adherence. PLoS One. 2017 Oct 17;12(10):e0186458. doi: 10.1371/journal.pone.0186458. PMID: 29040335; PMCID: PMC5645121.
- Najjar A, Amro Y, Kitaneh I, Abu-Sharar S, Sawalha M, Jamous A, Qiq M, Makharzeh E, Subb Laban B, Amro W, Amro A. Knowledge and Adherence to Medications among Palestinian Geriatrics Living with Chronic Diseases in the West Bank and East Jerusalem. PLoS One. 2015 Jun 5;10(6):e0129240. doi: 10.1371/journal.pone.0129240. PMID: 26046771; PMCID: PMC4457851.
- National Prescribing Centre. Service improvement guide: self administration of medicines in mental health trusts. Grantham: National Prescribing Centre; 2008 Apr.
- Nederlandse Zorgautoriteit. Brief over doorgebruik van thuismedicatie in het ziekenhuis (DGTM) en tariefregulering NZa [Internet]. PUC_291466_22; versie 1 [gepubliceerd 14 okt 2019; beschikbaar vanaf 18 okt 2019; geraadpleegd 21 jul 2025]. Beschikbaar via: https://puc.overheid.nl/nza/doc/PUC_291466_22/1/.
- Okuyan B, Sancar M, Izzettin FV. Assessment of medication knowledge and adherence among patients under oral chronic medication treatment in community pharmacy settings. Pharmacoepidemiol Drug Saf. 2013 Feb;22(2):209-14. doi: 10.1002/pds.3275. Epub 2012 Apr 18. PMID: 22514147.
- Patiëntenfederatie Nederland, NHG, LHV, KNMP, FMS, Zorgverzekeraars Nederland. Leidraad verantwoord wisselen medicijnen. Versie 2024 [Internet]. Utrecht: Federatie Medisch Specialisten; 2024 [cited 2025 Jul 21]. Available from: https://demedischspecialist.nl/sites/default/files/2022-11/Leidraad_Verantwoord_Wisselen_Medicijnen_versie15nov2022.pdf.
- Patiëntenfederatie Nederland. Patiëntenparticipatie [Internet]. Utrecht: Patiëntenfederatie Nederland; [cited 2025 Jul 21]. Available from: https://www.patientenfederatie.nl/dit-doen-wij/patientenparticipatie.
- Polito S, Ho L, Pang I, Dara C, Viswabandya A. Evaluation of a patient self-medication program in allogeneic hematopoietic stem cell transplantation. J Oncol Pharm Pract. 2022 Dec;28(8):1790-1797. doi: 10.1177/10781552211043525. Epub 2021 Sep 27. PMID: 34569857; PMCID: PMC9623336.
- Salama A, Yasin AE-R, Elbarbary W. Medication knowledge as a determinant of medication adherence in geriatric patients, Serse Elian City, Menoufia Governorate, Egypt. Menoufia Medical Journal. 2017;30(1):63- 8.
- Smale EM, van den Berg J, Korporaal-Heijman J, Bekker CL, van den Bemt BJF. Barriers, facilitators and implementation strategies to implement 'patient's own medication' and 'self-administration of medication' in hospitals. Int J Qual Health Care. 2025 May 16;37(2):mzaf038. doi: 10.1093/intqhc/mzaf038. PMID: 40293863.
- Sørensen CA, Lisby M, Olesen C, Enemark U, Sørensen SB, de Thurah A. Self-administration of medication: a pragmatic randomized controlled trial of the impact on dispensing errors, perceptions, and satisfaction. Ther Adv Drug Saf. 2020a May 4;11:2042098620904616. doi: 10.1177/2042098620904616. PMID: 32435443; PMCID: PMC7225786.
- Sørensen CA, de Thurah A, Lisby M, Olesen C, Sørensen SB, Enemark U. Cost-consequence analysis of self-administration of medication during hospitalization: a pragmatic randomized controlled trial in a Danish hospital setting. Ther Adv Drug Saf. 2020b Aug 29;11:2042098620929921. doi: 10.1177/2042098620929921. PMID: 32922722; PMCID: PMC7457413.
- The Joint Commission. National patient safety goals effective January 2021 for the hospital program. Oakbrook Terrace (IL): The Joint Commission; 2021.
- van den Bemt PMLA, Oude Munnink TH. Green Team Clinical Pharmacy and Pharmacology of a university hospital in the Netherlands: Towards sustainable clinical pharmacy [poster]. Poster presented at: European Association of Hospital Pharmacists (EAHP) Congress, Sustainability topic; June 2024. Available via: https://eahp.eu/wp‑content/uploads/2024/05/cps13249.pdf
- van Herpen-Meeuwissen LJM, van den Bemt BJF, Derijks HJ, van den Bemt PMLA, de Vries F, Maat B, van Onzenoort HAW. Economic impact of Patient's Own Medication use during hospitalisation: a multicentre pre-post implementation study. Int J Clin Pharm. 2019 Dec;41(6):1658-1665. doi: 10.1007/s11096-019-00932-1. Epub 2019 Nov 8. PMID: 31705458.
- van Herpen-Meeuwissen LJM, van den Bemt BJF, Derijks HJ, van den Bemt PMLA, Maat B, van Onzenoort HAW. The effect of Patient's Own Medication use on patient's self-reported medication knowledge during hospitalisation: a pre-post intervention study. BMC Health Serv Res. 2022a Mar 30;22(1):423. doi: 10.1186/s12913-022-07752-6. PMID: 35354464; PMCID: PMC8969375.
- van Herpen-Meeuwissen LJM, Bekker CL, Cornelissen N, Maat B, van Onzenoort HAW, van den Bemt BJF. Patients' views on Self-administration of Medication during hospitalisation: a mixed-methods study. Ther Adv Drug Saf. 2022b Jul 28;13:20420986221107804. doi: 10.1177/20420986221107804. PMID: 35923715; PMCID: PMC9340381.
- van Herpen-Meeuwissen LJM, van Onzenoort HAW, van den Bemt PMLA, Maat B, van den Bemt BJF. The Effect of Self-Administration of Medication During Hospitalization on Patient's Self-Efficacy and Medication Adherence After Discharge. Patient Prefer Adherence. 2022c Sep 28;16:2683-2693. doi: 10.2147/PPA.S375295. PMID: 36196066; PMCID: PMC9527028.
- van Herpen‑Meeuwissen LJM. Patient participation in medication management during hospitalisation – Empower to sustain [thesis]. Nijmegen: Radboud University Nijmegen; 2023a. Beschikbaar via: : https://repository.ubn.ru.nl/handle/2066/286391.
- van Herpen-Meeuwissen LJM, Djodikromo MF, Maat B, van den Bemt BJF, Bekker CL, van Onzenoort HAW. Inpatients Self-Administration of Medication: Stakeholders' views and prerequisites. J Clin Nurs. 2023b Jun;32(11-12):2709-2721. doi: 10.1111/jocn.16369. Epub 2022 May 20. PMID: 35596267.
- Verdijk JC, van den Bemt BJF, Melis EJ, van Onzenoort HAW, van Seyen M, Derijks HJ. Het effect van verschillende afleverstrategieën op de mate van dubbele bekostiging bij patiënten die thuismedicatie doorgebruiken tijdens opname in het ziekenhuis. Nederlands Platform voor Farmaceutisch Onderzoek. 2024;9:a1777. Available from: https://www.npfo.nl/artikel/het-effect-van-verschillende-afleverstrategieën-op-de-mate-van-dubbele-bekostiging-bij-patiënten-die.
- Wetenschappelijke Raad voor het Regeringsbeleid (WRR). Kiezen voor houdbare zorg: mensen, middelen en maatschappelijk draagvlak. Den Haag: WRR; 2021.
- World Health Assembly. Framework on integrated, people-centred health services: report by the Secretariat. Geneva: World Health Organization; 2016.
- World Health Organization. Adherence to long-term therapies: evidence for action. Geneva: World Health Organization; 2003.
- World Health Organization. Exploring patient participation in reducing health-care-related safety risks. Copenhagen: WHO Regional Office for Europe; 2013.
Evidence table for intervention studies (RCTs and non-randomized observational studies)
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention |
Comparison/ control |
Follow-up |
Outcome measures and effect size |
Comments |
||||||||
|
Van Herpen-Meeuwissen (2019) |
Type of study: Prospective intervention study with a pre-post design
Setting and country: 8 different wards in 7 hospitals (3 university, 2 teaching, 1 general, 1 specialized) in the Netherlands
Funding: Dutch Ministry of Health, Welfare and Sport, the Hague
Conflicts of interest: Authors declared no competing interests. |
Patient characteristics were not reported |
POM use during hospitalization: patients were asked to bring their own medication in original packages to the hospital. In case of an acute hospitalization, patient’s relatives were asked to bring these within 24 hours. |
Pre-intervention: standard care |
In pre- and post-intervention period, data were collected for 2 months |
Wasted medication
|
Comment: -
Limitations: * Participating wards did not include all patients who were able to participate in POM schemes. Additionally, it was unclear what the proportion of included patients was. * The follow-up period was relatively short (2 months). * The post-implementation period started directly after the implementation, which may have resulted in unintended medication waste and additional time spent on the medication process as a consequence of limited habituation.
Authors conclusion: This study showed that the implementation of POM implementation may have a positive environmental impact, as the value of medication waste decreases. |
POM, patient’s own medication
Risk of Bias tables
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors?
|
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables? |
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed?
|
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
van Herpen-Meeuwissen, 2019 |
Definitely yes
Reason: Participants were drawn from the same hospital populations before and after POM implementation |
Definitely yes
Reason: Exposure status was based on clear implementation timeline and hospital documentation. |
Definitely no
Reason: Waste was present during whole study period. |
Definitely no
Reason: No statistical analysis regarding confidence intervals/ uncertainty, confounding was performed. |
Definitely no
Reason: See previous comment. |
Definitely yes
Reason: Outcomes were measured using validated hospital systems. |
Probably no
Reason: The follow-up period was relatively short (2 months) |
Probably yes,
Reason: There was no indication of other systematic differences other than POM use. |
High |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Abdul Nasir HH, Goh HP, Wee DVT, Goh KW, Lee KS, Hermansyah A, Al-Worafi YM, Ming LC. Economic Analysis of Patient's Own Medication, Unit-Use and Ward Stock Utilization: Results of the First Pilot Study. Int J Environ Res Public Health. 2022 Sep 9;19(18):11350. doi: 10.3390/ijerph191811350. PMID: 36141623; PMCID: PMC9517008. |
Wrong outcome |
|
Alhamad H, Patel N, Donyai P. Towards Medicines Reuse: A Narrative Review of the Different Therapeutic Classes and Dosage Forms of Medication Waste in Different Countries. Pharmacy (Basel). 2020 Dec 1;8(4):230. doi: 10.3390/pharmacy8040230. PMID: 33271889; PMCID: PMC7712270. |
Wrong intervention |
|
Almalki A, Jambi A, Elbehiry B, Albuti H. Improving Inpatient Medication Dispensing with an Automated System. Glob J Qual Saf Healthc. 2023 Nov 24;6(4):117-125. doi: 10.36401/JQSH-23-15. PMID: 38404460; PMCID: PMC10887473. |
Wrong intervention |
|
Gil-Candel M, Solana-Altabella A, Vicente-Escrig E, Puplá-Bartoll A, Bodega Azuara J, Pérez-Huertas P, Ferrando Piqueres R. Developing a telepharmacy programme with home medication dispensing and informed delivery in a tertiary hospital: description of the model and analysis of the results. Eur J Hosp Pharm. 2023 Mar;30(2):107-112. doi: 10.1136/ejhpharm-2021-003194. Epub 2022 Apr 20. PMID: 35444000; PMCID: PMC9986923. |
Wrong population |
|
Hoefgen ER, Jones Y, Courter J, Hare A, Garcia JAT, Simmons J. Leveraging the Outpatient Pharmacy to Reduce Medication Waste in Pediatric Asthma Hospitalizations. J Hosp Med. 2020 Jan 1;15(1):28-34. doi: 10.12788/jhm.3275. Epub 2019 Aug 16. PMID: 31433770; PMCID: PMC6932591. |
Wrong intervention |
|
Lim PC, Chung YY, Tan SJ, Wong TY, Permalu DD, Cheah TK, Lim SL, Lee CY. Comparing the cost, glycaemic control and medication adherence of utilizing patients' own medicines (POMs) versus usual dispensing among diabetic patients in an outpatient setting. Daru. 2021 Jun;29(1):125-132. doi: 10.1007/s40199-021-00389-6. Epub 2021 Feb 4. PMID: 33538999; PMCID: PMC8149523. |
Wrong population |
|
Lummis H, Sketris I, Veldhuyzen van Zanten S. Systematic review of the use of patients' own medications in acute care institutions. J Clin Pharm Ther. 2006 Dec;31(6):541-63. doi: 10.1111/j.1365-2710.2006.00773.x. PMID: 17176360. |
Outdated review |
|
Sánchez VLC, Bueno EV, Morales MA, Encinar MR, Jimenez CS, Catedra CL, Perez EA, Ambrosio AH. Green hospital pharmacy: A sustainable approach to the medication use process in a tertiary hospital. Farm Hosp. 2023 Sep-Oct;47(5):196-200. English, Spanish. doi: 10.1016/j.farma.2023.05.008. Epub 2023 Jul 12. PMID: 37451908. |
Wrong study design |
|
Siderov J. Utility of PhaSeal, a closed-system drug transfer device, in facilitating vial sharing to reduce waste and assist in medication cost savings. J Pharm Pract Res. 2019;49(5):421–5 |
Wrong intervention |
|
Verdijk JC, van den Bemt BJF, Melis EJ, van Onzenoort HAW, van Seyen M, Derijks HJ. The effect of different drug (re)supply strategies on the extent of double funding in patients who use their own medication during hospitalization. Pharm Weekbl. 2024. |
Wrong outcomes |
|
Wong GY. Cost impact of using patients' own multidose medications in hospital. Can J Hosp Pharm. 2014 Jan;67(1):9-16. doi: 10.4212/cjhp.v67i1.1316. PMID: 24634521; PMCID: PMC3952918. |
Wrong outcomes |
Beoordelingsdatum en geldigheid
Publicatiedatum : 07-05-2026
Beoordeeld op geldigheid : 07-05-2026
Algemene gegevens
De ontwikkeling/herziening van deze module werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS).
De financier heeft geen enkele invloed gehad op de inhoud van de leidraad.
Samenstelling werkgroep
Voor het ontwikkelen van de leidraad is in 2024 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij farmaceutisch specialistische zorg.
Werkgroep Inhoud
- Dr. L.J.M. (Loes) van Herpen – Meeuwissen (voorzitter), ziekenhuisapotheker, Radboudumc, NVZA
- Dr. M.E. (Milly) Attema – de Jonge, ziekenhuisapotheker, Meander MC, NVZA
- Dr. C. (Charlotte) Bekker, universitair docent, Radboudumc, persoonlijke titel
- Drs. V. (Vivienne) de Smet, AIOS spoedeisende geneeskunde, Diakonessenhuis, NVSHA
- Dr. N.G.M. (Nicole) Hunfeld, ziekenhuisapotheker, universitair hoofddocent, Erasmus MC, NVIC
- Dr. B.J.A. (Ben) Janssen, farmacoloog, universitair hoofddocent, Maastricht UMC, persoonlijke titel
- Dr. B. (Berber) Kapitein, kinderarts-intensivist, Amsterdam UMC, NVK
- Drs. R. (Remco) Minkhorst, anesthesioloog, UMC Utrecht, NVA
- Drs. J.D. (Joost) Piët, arts-docent en promovendus farmacotherapie, Amsterdam UMC, NVKFB
- Y.H.M. (Yvonne) van Grinsven – Ariaans, (regie)verpleegkundige, Radboudumc, V&VN
- M. (Marga) van Timmeren, kwaliteitsfunctionaris, BModesto, NVFZ
Werkgroep Implementatie
- B.A.P. (Bart) Cramers, apotheker, programmamanager dure geneesmiddelen, NVZ
- Drs. M. (Maarten) Loof, programmamanager dure geneesmiddelen, ZN
- P. (Peter) Roos, adviseur, UMCNL (voorheen NFU; tot december 2024)
- Prof. dr. E.L. (Noortje) Swart, ziekenhuisapother, hoogleraar Klinische Farmacologie en Apotheek, hoofd adeling klinische farmacologie en apotheek, Amsterdam UMC, UMCNL (vanaf maart 2025)
Klankbordgroep
- Dr. P.H.P (Pascal) de Jong, reumatoloog, universitair hoofddocent, Erasmus MC, NVR
- Dr. F. (Femme) Dirksmeier – Harinck, MDL-arts, Franciscus, NVMDL
- Prof. dr. W.J.K. (Wouter) Hehenkamp, gynaecoloog, hoogleraar gynaecologie gericht op doelmatige en duurzame zorg, Amsterdam UMC, NVOG
- Drs. A. (Annemieke) Horikx, apotheker, KNMP
- Dr. J.J.W.M. (Jeroen) Janssen, internist-hematoloog, Radboudumc, NIV
- Dr. P.H.C. (Philip) Kremer, neuroloog, Leids Universitair Medisch Centrum, NVN
- Dr. M. (Maartje) Los, internist-oncoloog, St. Antonius Ziekenhuis, NIV
- Prof. dr. F.M.A.C. (Fabrice) Martens, cardioloog, hoogleraar Preventieve cardiologie, Amsterdam UMC, NVVC
- Drs. N.M.F. (Nikki) Noorda, klinisch geriater, Dijklander Ziekenhuis, NVKG
- Dr. S. (Sam) Schoenmakers, gynaecoloog, Erasmus MC, NVOG
- Drs. D.C. (Dorothée) van Trier, traumachirurg, Diakonessenhuis, NVvH
- P. (Paula) Warmerdam, verpleegkundig specialist, Alrijne Ziekenhuis, V&VN
Met ondersteuning van
- Dr. R. (Renee) Bolijn, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. T. (Thibaut) Dederen, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. C.T.J. (Charlotte) Michels, senior adviseur, Kennisinstituut van de Federatie Medisch Speclisten
- E. (Esther) van der Bijl, Informatiespecialist, Kennisinstituut van de Federatie Medisch Speclisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Gemelde belangen |
Ondernomen actie |
|
Werkgroep Inhoud |
||||
|
Van Herpen – Meeuwissen (voorzitter) |
Ziekenhuisapotheker, Radboudumc, Nijmegen |
NVZA: lid commissie Duurzaamheid |
* ZonMW, Medicatie in eigen beheer 848022007. * Auteur: |
Geen restricties |
|
Attema – de Jonge |
Ziekenhuis apotheker, Meander Medisch Centrum, Amersfoort |
Lid Commissie Duurzaamheid NVZA |
Geen |
Geen restricties |
|
Bekker |
Senior onderzoeker, Radboudumc, Nijmegen |
Voorzitter NFU werkgroep Green deal duurzame zorg thema 5 'medicijnen' |
* ZonMw Heruitgifte orale oncolytica 848018008 * ZonMw RODEO trial 10140021910501 * Transformatieovereenkomst heruitgifte orale oncolytica * VWS Green Deal duurzame zorg thema 5 'medicijnen' * Senior onderzoeker duurzaam geneesmiddelgebruik |
Geen restricties |
|
De Smet |
AIOS SEH, Diakonessenhuis, Utrecht |
* Lid commissie Groene SEH |
Geen |
Geen restricties |
|
Hunfeld |
* Ziekenhuisapotheker, Erasmus MC, Rotterdam (betaald) * Projectleider onderzoek duurzame zorg, Erasmus MC, Rotterdam (betaald) |
* Vice voorzitter en penningmeester KNMP (betaald) * Voorzitter Groene IC NVIC (onbetaald) vVoorzitter commissie ATG (LCG) (betaald) * Toezichthouder VVT Het Maanderzand (betaald) * Lid Commissie Duurzaamheid NVZA |
NWO (geen onderzoek over medicijnen) |
Geen restricties |
|
Janssen (Ben) |
Universitair Hoofddocent Farmacologie, Vakgroep Farmacologie & Toxicologie, Faculty of Health Medicines and Life Sciences Maastricht University. Werk op afdeling Beeldvorming van het Maastrichts Universitair Medisch Centrum. |
Geen |
Geen |
Geen restricties |
|
Kapitein |
Kinderarts-intensivist, Emma Kinderziekenhuis Amsterdam UMC, Amsterdam |
* Lid Groene Kinderarts * NVK Lid wetenschapscommissie |
* MACU-PICU Stichting CJ Vaillant. Multisystem phenotyping of severe ACUte asthma at the Pediatric Intensive Care Unit (macu-pico). Postdoc (geen PI). * AUMC Medewerkersberaad innovatie subsidie "Het AUMC medewerkersberaad: op weg naar duurzaam woon-werkverkeer (studie reeds afgerond). |
Geen restricties |
|
Minkhorst |
Anesthesioloog UMC Utrecht |
Geen |
Geen |
Geen restricties |
|
Piët |
*Fulltime arts-docent en -onderzoeker Farmacotherapie in het AmsterdamUMC (locatie VUmc). *Al het onderwijs betreffende het voorschrijven van medicatie verzorgen voor de opleidingen geneeskunde, tandheelkunde en masteropleidingen voor verpleegkundigen. *Promovendus op gebied van het integreren van milieu-impact door medicatie in het medisch onderwijs. Deze werkzaamheden zijn allen betaald vanuit mijn aanstelling. |
* Klinisch farmacoloog in opleiding * Projectcoördinator Erasmus+ projecten CP4T en PlanED Prescribing |
Erasmus+ projecten: * Planetary Health Education in Prescribing (PlanED Prescribing) * Clinical Pharmacology and Therapeutics Teach The Teacher (CP4T)
Auteur NTvG artikel "Vermindering van de milieu-impact van medicatie; De rol van de voorschrijver" (D7985) (Toekomstige) Uitkomsten (wetenschappelijk) van Erasmus+ project PlanED Prescribing en van eigen PhD. PMID 39303730 |
Geen restricties |
|
Van Grinsven – Ariaans |
* Verpleegkundige Orthopedie Radboudumc (contract 12 uur, betaald) * Kwaliteitsfunctionaris afdeling Orthopedie/KNO/MKA/PCH/Trauma Radboudumc (contract 12 uur, betaald) |
Geen |
Geen |
Geen restricties |
|
Van Timmeren |
Sr Quality Officer, Bmodesto, Lelystad |
Geen |
Geen |
Geen restricties |
|
Werkgroep Implementatie |
||||
|
Cramers |
Programmamanager Dure Geneesmiddelen NVZ Belangenbehartiging ziekenhuizen op dure geneesmiddelen gebied. Gaat over kwaliteit, beschikbaarheid en betaalbaarheid. |
Geen |
Geen |
Geen restricties |
|
Loof |
Programmamanager Dure Geneesmiddelen bij ZN |
Geen |
Geen |
Geen restricties |
|
Roos |
Adviseur binnen NFU |
Geen |
Geen |
Geen restricties |
|
Swart |
Hoofd Afdeling Apotheek en Klinische Farmacologie, AmsterdamUMC |
* Voorzitter Wetenschappelijke Adviesraad Commissie Farmacotherapeutisch Kompas (WAR CFK), Zorginstituut Nederland * Voorzitter NVKFB. * Lid bestuur KNMP |
Echtgenoot werkt bij Pfizer in een niet commerciële functie. Geen relatie met werkgroep
Medicijn voor de Maatschappij: Bereidingen voor zeldzame metabole ziekten. |
Geen restricties |
|
Klankbordgroep |
||||
|
De Jong |
Reumatoloog, Erasmus MC, Rotterdam |
* Lid adviesraad voor Abbvie; AstraZeneca; Bristol-Myers Squibb; Galapagos; Lilly; Novartis; Pfizer; Sanofi Genzyme; UCB * Verzorging van onderwijs voor Abbvie; Galapagos; Lilly; Novartis; Pfizer |
Subsidies voor investigated initiated studies van Abbvie; Dutch Arthritis Foundation; Galapagos; Lilly; Pfizer. 1. Abbvie, ontwikkelen tool voor zorg op afstand, projectleider. 2. Dutch Arthitis Foudation, gecombineerde leefstijlinterventie trial, projectleider. 3. Galapagos: trial naar belandeling op maat. 4. Pfizer: Toediening van medicatie obv chronobiologie, projectleider. 5. Lilly: Implementatieonderzoek gericht op persoonsgerichte zorg, projectleider. |
Geen restricties |
|
Dirksmeier – Harinck |
MDL-arts, Franciscus, Rotterdam |
Geen |
Geen |
Geen restricties |
|
Hehenkamp |
Gynaecoloog, AmsterdamUMC, Amsterdam |
Allen onbetaald: -lid pijlerbestuur gynaecologie -voorzitter Gynae Goes Green (landelijke groen commissie GYN) -lid bestuur SIG anticonceptie -Bestuur Hector Treub stichting |
1. ZonMW: Substitutie van zorg Covid, projectleider. 2. ZonMW: Ulipristal bij myomen., projectleider. 3. Merit Medical: QUESTA trial (adenomyose en hysterectomie danwel embolisatie). 4. ZonMW: Keuzehulp Myomen, projectleider. |
Geen restricties |
|
Horikx |
Apotheker, teamleider Geneesmiddel Informatie Centrum KNMP |
* Bestuurslid Stichting Farmaceutisch Erfgoed. * Commissielid interacterende medicatie VKA's. * Werkgroeplid kritische en kwetsbare geneesmiddelenlijst-NVZA. * Praktijkteamlid palliatieve zorg |
Geen |
Geen restricties |
|
Janssen (Jeroen) |
internist-hematoloog, Afdeling Hematologie, Radboud UMC, Nijmegen, betaald |
* Voorzitter, St. Apps for Care and Science, betaald. * Bestuurslid en penningmeester, Nederlandse Vereniging voor Hematologie, onbetaald |
De St. Apps for Care and Science ontwikkelt de HematologyApp, een smartphone-, tablet- en binnenkort ook web-based applicatie die als doel heeft het werk van hematologen te verbeteren, de kwaliteit van de zorg voor hematologische patienten te verbeteren en klinisch wetenschappelijk onderzoek te bevorderen. Deze stichting zoekt ondersteuning voor het behalen van haar doelen bij farmaceutische bedrijven die initatieven van de stichting kunnen sponsoren. De volgende bedrijven zijn sponsor/donateur van de stichting: Daiichi-Sankyo, Johnson & Johnson, SERB, Sanofi, SOBI, Novo-Nordisk, MSD, Biomea, AstraZeneca, BristolMyersSquibb, Alexion, Kite-Gilead, Pfizer, Abbvie, Astellas,Novartis, Amgen, Takeda en Servier. |
Geen restricties |
|
Kremer |
*Research Director Neurology bij The Centre for Human Drug Research, Leiden * Neuroloog bij het Leids Universitair Medisch Centrum, Leiden |
Geen |
In het CHDR ben ik verantwoordelijk voor ongeveer 10 vroege fase medicijnstudies gefinancierd door veelal Amerikaanse biotech of grote farma. De onderzoeksmiddelen zitten dermate vroeg in het ontwikkeltraject dat er geen belangenverstrengeling is. |
Geen restricties |
|
Los |
internist oncoloog in het St Antonius Ziekenhuis Utrecht/ Nieuwegein |
Geen |
Geen |
Geen restricties |
|
Martens |
Cardioloog, hoogleraar Preventieve Cardiologie bij het Amsterdam UMC, Amsterdam. Namens de NVVC vertegenwoordigend. |
* Adviseur CVRM en medicatie NVVC. * Voorzitter Werkgroep Geneesmiddelen NVVC * Voorzitter DCVA Commissie Preventie * Clinical Valorization Officer Amsterdam UMC *Voorzitter Hartstichting Hart-Vaatagenda-project 'Op tijd ontdekken' Wetenschappelijk nog wel verbonden aan het HartVaatCentrumSalland |
Sprekersvergoeding zonder belangenverstrengeling gezien altijd naar Amsterdam UMC.
Sponsoring GOLDEN-studie: Novartis, Amarin, Novo Nordisk en een Europese IHI-grant. Sponsoring 2-DECIDE-studie: ZoNMW en ZE&GG Sponsoring EUROASPIRE: Hartstichting |
Geen restricties |
|
Noorda |
Klinisch geriater in het Dijklanderziekenhuis |
Geen |
Geen |
Geen restricties |
|
Schoenmakers |
Gynaecoloog, Erasmus MC Universtair Medisch Centrum, Rotterdam |
* Wetenschap-commissielid Strong Babies (onbetaald) * Gezondheidsraad - algemeen / commissie vaccinatie (vacatiegelden) |
ZonMW Open Competitie (2019-2024) - ondewerp Obesitas, microbioom en zwangerschap |
Geen restricties |
|
Van Trier |
(Trauma) Chirurg OLVG en BovenIJ Ziekenhuis |
* Werkgroep Groen OK NVVH. * Tevens lid van de werkgroep Plastic en Circulair van het Landelijk Netwerk Groene OK, onbetaald. |
Geen |
Geen restricties |
|
Warmerdam |
Verpleegkundig specialist werkzaam bij Alrijne |
Presentaties geven aan POH en Huisartsen |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland (PFN) voor deelname aan de werkgroep Inhoud en aan twee invitational conferences. Op advies van de PFN heeft de werkgroep de uitkomsten uit het rapport Verduurzaming van de zorg geïntergreerd in de modules. Daarnaast is module 6 Communicatie over milieubewust medicatiegebruik specifiek gericht op communicatie over milieubewust medicatiegebruik met patiënten. De conceptleidraad is tevens voor commentaar voorgelegd aan de PFN en de aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de leidraad voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de leidraad per module op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Medicatieverstrekking - Doorgebruik van thuismedicatie |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten), volgt uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte methodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze leidraad is hieronder weergegeven.
Zoekverantwoording
Zoekstrategie - 17 oktober 2024
Embase.com
|
No. |
Query |
|
#1 |
'hospital patient'/exp OR 'hospital care'/exp OR 'hospital management'/exp OR 'inpatient*':ti,ab,kw OR 'inhospital*':ti,ab,kw OR 'intramural care':ti,ab,kw OR hospital*:ti,ab,kw |
|
#2 |
'drug self administration'/exp OR 'pharmacy (shop)'/de OR 'pharmacist'/de OR 'community pharmacist'/exp OR ((('self-manag*' OR selfmanag* OR 'self administrat*' OR 'selfadministrat*') NEAR/3 (medicati* OR medicine* OR drug* OR 'drugtherap*' OR 'pharmac*')):ti,ab,kw) OR (((home OR 'outpatient*' OR 'out patient*') NEAR/3 (medicati* OR medicine* OR 'drug* therap*' OR 'drugtherap*' OR 'pharmac*' OR 'drug* treatment*')):ti,ab,kw) OR ((own NEXT/1 (medication* OR medicine* OR drug*)):ti,ab,kw) OR 'apothecar*':ti,ab,kw OR 'chemist* shop*':ti,ab,kw OR 'communit* pharmac*':ti,ab,kw OR 'pharmac* service*':ti,ab,kw |
|
#3 |
#1 AND #2 |
|
#4 |
'biodegradable plastic'/exp OR 'biodiversity'/de OR 'climate change'/exp OR 'climate resilience'/exp OR 'disposable equipment'/exp OR 'ecological diversity'/exp OR 'energy conservation'/exp OR 'environmental aspects and related phenomena'/exp OR 'environmental footprint'/exp OR 'environmental protection'/exp OR 'eutrophication'/exp OR 'life cycle assessment'/exp OR 'pollution and pollution related phenomena'/exp OR 'species diversity'/exp OR 'waste and waste related phenomena'/exp OR 'wastewater'/exp OR 'water management'/exp OR 'water pollution'/exp OR 'global warming potential'/exp OR acidification:ti,ab,kw OR (((water OR land) NEXT/1 use):ti,ab,kw) OR (((air OR organic OR soil OR water OR plastic* OR liquid*) NEAR/4 (pollut* OR contamina* OR wast*)):ti,ab,kw) OR biodivers*:ti,ab,kw OR 'biological divers*':ti,ab,kw OR (((co2 OR 'co 2' OR carbon OR 'nitrous oxide') NEAR/3 (emission* OR footprint OR equival* OR reduct*)):ti,ab,kw) OR (((nature OR environment* OR climat*) NEAR/3 (impact* OR pollut* OR conservat* OR protect* OR preserv* OR effect* OR benefit* OR chang* OR exposure* OR resilien*)):ti,ab,kw) OR disposable*:ti,ab,kw OR ((eco* NEAR/3 (toxic* OR efficien* OR damage)):ti,ab,kw) OR ecotoxic*:ti,ab,kw OR ecoefficien*:ti,ab,kw OR (((emission OR waste) NEAR/3 reduc*):ti,ab,kw) OR environmental*:ti OR (((equipment* OR product* OR waste*) NEAR/3 reus*):ti,ab,kw) OR recycl*:ti,ab,kw OR 'resource recover*':ti,ab,kw OR eutrophicat*:ti,ab,kw OR (((global OR climate) NEAR/2 warming):ti,ab,kw) OR ((green* NEAR/2 (deal OR surger* OR effect* OR gas* OR resource*)):ti,ab,kw) OR (((hospital OR medical OR zero OR product* OR byproduct* OR 'by product*' OR avoid* OR energy OR management OR nuclear OR biomass) NEAR/3 waste*):ti,ab,kw) OR ((('life cycle' OR lifecycle) NEAR/2 (assess* OR inventor*)):ti,ab,kw) OR lca:ti,ab,kw OR lcas:ti,ab,kw OR 'human toxicity potential*':ti,ab,kw OR (((ep OR h+ OR gwp OR faetp OR fatp OR ap OR cfc OR 'kg n' OR 'nox' OR '2.4' OR '2,4' OR pocp OR so2 OR dichlorobenzen* OR ethan* OR po4 OR dcb) NEAR/3 equival*):ti,ab,kw) OR ((ozone NEAR/3 (deplet* OR hole*)):ti,ab,kw) OR (((plastic* OR microplastic* OR 'micro plastic*') NEAR/3 (overuse OR soup OR pollut* OR contaminat*)):ti,ab,kw) OR recycle*:ti,ab,kw OR recycling:ti,ab,kw OR (((refuse OR waste) NEAR/3 disposal):ti,ab,kw) OR reusable*:ti,ab,kw OR reuse*:ti,kw OR reusing:ti,kw OR 'rising sea level*':ti,ab,kw OR 'sea level ris*':ti,ab,kw OR smog:ti,ab,kw OR sustainab*:ti,kw OR ((sustainab* NEAR/3 (development* OR cycle* OR management OR effect* OR environment*)):ti,ab,kw) OR ((water NEAR/3 (purificat* OR sanitat* OR treatment)):ti,ab,kw) OR wastewater:ti,ab,kw OR ((hydrogen NEAR/3 moles NEAR/3 equival*):ti,ab,kw) OR 'circular econom*':ti,ab,kw OR biodegradab*:ti,ab,kw OR (((ecological OR environmental OR water OR energy OR climate OR global) NEAR/2 footprint*):ti,ab,kw) OR waste:ti,ab,kw OR wastes:ti,ab,kw OR reuse:ti,ab,kw OR reusab*:ti,ab,kw OR reprocess*:ti,ab,kw OR pollut*:ti,ab,kw OR greening:ti,ab,kw OR spillage:ti,ab,kw OR spilling:ti,ab,kw OR spoilage:ti,ab,kw OR salinization:ti,ab,kw OR 'cradle to cradle':ti,ab,kw OR 'carbon neutral*':ti,ab,kw OR wastage*:ti,ab,kw |
|
#5 |
#3 AND #4 |
|
#6 |
#5 AND [2000-2025]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
|
#7 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
|
#8 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
|
#9 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
|
#10 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
|
#11 |
#6 AND #7 - SR |
|
#12 |
#6 AND #8 NOT #11 - RCT |
|
#13 |
#6 AND (#9 OR #10) NOT (#11 OR #12) - Observationeel |
|
#14 |
#11 OR #12 OR #13 - Totaal |
Ovid/Medline
|
# |
Searches |
|
1 |
exp Patients/ or exp Hospitalization/ or (within adj2 hospital*).ti,ab,kf. or (setting* adj2 hospital*).ti,ab,kf. or inpatient*.ti,ab,kf. or out patient*.ti,ab,kf. or outpatient*.ti,ab,kf. or outward patient*.ti,ab,kf. or inhospital*.ti,ab,kf. or intramural care.ti,ab,kf. or hospital*.ti,ab,kf. |
|
2 |
exp Self Administration/ or exp Community Pharmacy Services/ or Pharmacy/ or exp Pharmacists/ or ((self-manag* or selfmanag* or self administrat* or selfadministrat*) adj3 (medicati* or medicine* or drug* or drugtherap* or pharmac*)).ti,ab,kf. or ((home or outpatient* or out patient*) adj3 (medicati* or medicine* or drug* therap* or drugtherap* or pharmac* or drug* treatment*)).ti,ab,kf. or (own adj1 (medication* or medicine* or drug*)).ti,ab,kf. or apothecar*.ti,ab,kf. or chemist* shop*.ti,ab,kf. or communit* pharmac*.ti,ab,kf. or pharmac* service*.ti,ab,kf. |
|
3 |
Biodegradable Plastics/ or exp Biodiversity/ or exp Carbon Footprint/ or exp Environmental Pollution/ or exp Climate Change/ or Disposable Equipment/ or Environment/ or Equipment Reuse/ or exp Eutrophication/ or Greenhouse Gases/ or Greenhouse Effect/ or exp Hazardous Waste/ or exp Medical Waste/ or Ozone Depletion/ or Recycling/ or exp Refuse Disposal/ or Smog/ or Waste Products/ or exp Waste Water/ or acidification.ti,ab,kf. or ((air or organic or soil or water or plastic* or liquid*) adj4 (pollut* or contamina* or wast*)).ti,ab,kf. or (biodivers* or "biological divers*").ti,ab,kf. or ((co2 or "co 2" or carbon) adj3 (emission* or footprint or equival* or reduct*)).ti,ab,kf. or ((nature or environment* or climat*) adj3 (impact* or pollut* or conservat* or protect* or preserv* or effect* or benefit* or chang* or exposure* or resilien*)).ti,ab,kf. or disposable*.ti,ab,kf. or (eco* adj3 (toxic* or efficien* or damage)).ti,ab,kf. or ecotoxic*.ti,ab,kf. or ecoefficien*.ti,ab,kf. or ((waste or emission*) adj3 reduc*).ti,ab,kf. or environmental*.ti. or ((equipment* or product* or waste*) adj3 reus*).ti,ab,kf. or recycl*.ti,ab,kf. or resource recover*.ti,ab,kf. or eutrophicat*.ti,ab,kf. or ((global or climate) adj2 warming).ti,ab,kf. or (("life cycle" or lifecycle) adj2 (assess* or inventor*)).ti,ab,kf. or LCA.ti,ab,kf. or LCAs.ti,ab,kf. or (("life cycle" or lifecycle) adj2 (assess* or inventor* or analys*)).ti,ab,kf. or (green* adj2 (deal or surger* or effect* or gas* or resource*)).ti,ab,kf. or greening.ti,ab,kf. or ((hospital or medical or zero or product* or byproduct* or "by product*" or avoid* or energy or management or nuclear or biomass) adj3 waste*).ti,ab,kf. or "human toxicity potential*".ti,ab,kf. or ((EP or H+ or GWP or FAETP or FATP or AP or CFC or "kg N" or "NOx" or "2.4" or "2,4" or POCP or SO2 or dichlorobenzen* or ethan* or PO4 or DCB) adj3 equival*).ti,ab,kf. or (ozone adj3 (deplet* or hole*)).ti,ab,kf. or ((plastic* or microplastic* or "micro plastic*") adj3 (overuse or soup or pollut* or contaminat*)).ti,ab,kf. or recycle*.ti,ab,kf. or recycling.ti,ab,kf. or ((refuse or waste) adj3 disposal).ti,ab,kf. or reusable*.ti,ab,kf. or reuse*.ti,kf. or reusing.ti,kf. or "rising sea level*".ti,ab,kf. or "sea level ris*".ti,ab,kf. or smog.ti,ab,kf. or sustainab*.ti,kf. or (sustainab* adj3 (development* or cycle* or management or effect* or environment*)).ti,ab,kf. or (water adj3 (purificat* or sanitat* or treatment)).ti,ab,kf. or wastewater.ti,ab,kf. or (hydrogen adj3 moles adj3 equival*).ti,ab,kf. or "circular econom*".ti,ab,kf. or biodegradab*.ti,ab,kf. or ((ecological or environmental or water or energy or global or climat*) adj2 footprint*).ti,ab,kf. or (waste adj3 by product*).ti,ab,kf. or waste.ti,ab,kf. or wastes.ti,ab,kf. or reuse.ti,ab,kf. or reusab*.ti,ab,kf. or reprocess*.ti,ab,kf. or pollut*.ti,ab,kf. or (microplastic* and pollut*).ti,ab,kf. or greening.ti,ab,kf. or spillage.ti,ab,kf. or spoilage.ti,ab,kf. or salinization.ti,ab,kf. or "cradle to cradle".ti,ab,kf. or 'compostable plastic*'.ti,ab,kf. or desertification.ti,ab,kf. or deforestation.ti,ab,kf. or 'algal bloom*'.ti,ab,kf. or eco-friendly.ti,ab,kf. or ecofriendly.ti,ab,kf. or 'global change'.ti,ab,kf. or 'climate change'.ti,ab,kf. or "carbon neutral*".ti,ab,kf. or wastage*.ti,ab,kf. |
|
4 |
1 and 2 and 3 |
|
5 |
limit 4 to yr="2000 -Current" |
|
6 |
5 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
|
7 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
|
8 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
|
9 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
|
10 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
|
11 |
6 and 7 - SR |
|
12 |
(6 and 8) not 11 - RCT |
|
13 |
(6 and (9 or 10)) not (11 or 12) - Observationeel |
|
14 |
11 or 12 or 13 - Totaal |