Gebruik van ready-to-use/ready-to-administer preparaten
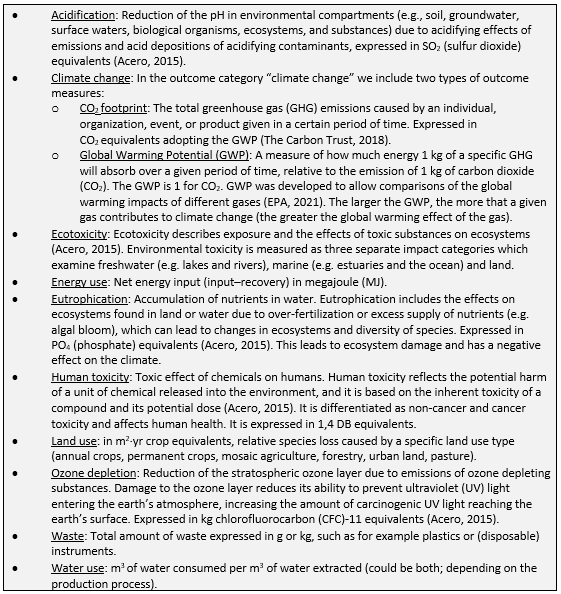
Uitgangsvraag
Hoe kan de inzet van steriele ready-to-use (RTU) en/of ready-to-administer (RTA) preparaten de milieu-impact verminderen?
Aanbeveling
Houd er rekening mee dat het gebruik van ready-to-use (RTU) en/of ready-to-administer (RTA) kan leiden tot een lagere milieu-impact, voornamelijk door minder afval, minder materialen en minder transport.
Pas het principe “op-is-stop” toe (alleen een nieuwe spuit of zak aanhangen als dit medisch nodig is).
Overwegingen
Kwaliteit van bewijs
Deze module evalueert of steriele ready-to-use (RTU) en/of ready-to-administer (RTA) preparaten de milieu-impact kunnen verminderen. Hiervoor zijn twee PICOs uitgezet in de literatuur, waarbij PICO1 resulteerde in geen beschikbaar bewijs gericht op milieu-impact van steriele RTU en/of RTA in vergelijking met conventioneel VTGM (voor toediening gereed maken) op de verpleegafdeling*.
Bij PICO2 werd één observationele studie uit de literatuursearch gevonden, welke is gericht op een vergelijking van steriele met aseptisch batchgewijs klaargemaakte RTA spuiten (Van Gelder, 2023). Conclusie uit deze studie is dat steriele RTA spuiten minder afval opleveren dan aseptisch batchgewijs klaargemaakte spuiten. De bewijskracht voor de cruciale uitkomstmaat ‘waste’ komt echter uit op zeer laag (risk of bias, imprecisie). Voor de overige uitkomstmaten (‘climate change’, ‘eco-toxicity’, ‘human toxicity’, ‘water use’, ‘land use’, ‘acidification’, ‘eutrophication’) zijn geen data gevonden. Wegens de zeer lage bewijskracht kunnen er op basis van de literatuur geen harde conclusies geformuleerd worden. Echter, erkent de werkgroep de urgentie om de milieu-impact te verminderen en kiest voor sterke aanbevelingen op basis van de huidige beschikbare literatuur en expert opinie van de werkgroepleden.
*dit is inclusief de operatiekamers.
Balans tussen gewenste en ongewenste effecten
Er is geen literatuur gevonden dat heeft aangetoond dat de milieu-impact lager is bij gebruik van steriele RTU en/of RTA ten opzichte van medicatie die voor toediening gereed gemaakt zijn op de verpleegafdeling (PICO 1). De werkgroep verwacht echter dat dit wel het geval is, wegens het gebruik van minder materialen en minder transport (in verband met de veelal Nederlandse productie van RTA Prefilled Sterilized Syringe (PFSS) spuiten van 50 ml). Specifiek geldt voor RTA PFSS dat deze tot 7 dagen houdbaar zijn na aanhangen, omdat de inhoud steriel is (zie GMP‑Z Z3 Aseptische handelingen, NVZA, 2022). Dit scheelt het weggooien van restant medicatie vergeleken met spuiten die, na handmatig optrekken op een werkblad, 32 uur houdbaar zijn en daardoor sneller de houdbaarheidsdatum zullen overschrijden (NVZA, 2022). Daarnaast scheelt het gebruik van RTA PFSS verpleegkundigen tijd. Ze hoeven minder handelingen uit te voeren tot aan het aanhangen van een spuit (NHS, 2022). Ook leidt dit tot minder medicatiefouten (Benhamou, 2023; Kelly, 2023) en minder besmettingen (Larmené-Beld, 2019), wat aanvullende zorg (met weer aanvullende milieu-impact) kan voorkomen. Er zijn ook standpunten die voorkeur geven aan RTA PFSS (Whitaker, 2024; EAHP, 2023), vanwege bijvoorbeeld minder handschoenen, spuiten, naalden en desinfectantia gebruik.
Daarnaast hebben Honkoop et al uitgezocht dat het gebruik van 50 ml RTA PFSS resulteert in minder afval (Honkoop, 2022). Dit sluit aan bij de conclusie van PICO 2 dat steriele RTA spuiten minder afval opleveren dan aseptisch batchgewijs klaargemaakte spuiten. De werkgroep voorziet dat de volgende duurzaamheidsaspecten voornamelijk een rol spelen bij het gebruik van PFSS/RTU flacons: minder gebruik van disposable producten (wat leidt tot minder afval) en minder transport in verband met productie van 50 ml RTA PFSS in Nederland (Honkoop, 2022).
Daarnaast mogen PFSS en RTA-infuuszakken maximaal 7 dagen aangehangen worden, waardoor minder verspilling optreedt dan bij iedere 24 uur wisselen. Daarnaast leidt het gebruik van PFSS tot minder besmette spuiten (NHS, 2022; Benhamou, 2023; Kelly, 2023; Larmené-Beld, 2019), hetgeen het infectierisico verlaagt.
Bij de werkgroep zijn enkele meldingen bekend van onbedoelde bolusinjecties met propofol en kalium voorgevulde PFSS (Peters, 2024). Deze meldingen zijn terug te voeren op het niet correct indraaien van de plunjer in de RTA PFSS. Hiervoor is een goede instructie nodig voor zorgverleners.
Naast de inzet van PFSS/RTU flacons zijn ook werkafspraken te maken die leiden tot minder gebruik van spuiten. Een voorbeeld hiervan is het “op-is-stop” principe (De Groene IC, 2025). Als een spuit op is, dan wordt alleen een nieuwe spuit aanhangen als dit medisch nodig is. De werkgroep adviseert zorgverleners zich hiervan bewust te zijn. Daarnaast adviseert de werkgroep om periodiek te evalueren (liefst dagelijks tijdens patiëntenronde) of de toediening per spuit gestopt kan worden in het kader van R2-Reduce (Hospital Pharmacy Recommendations).
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
De gewenste en ongewenste effecten op patiëntrelevante uitkomstmaten zijn bij de werkgroep onbekend. Voor de patiënt en zorgverlener is het van belang dat medicatie en producten veilig en effectief zijn, waarbij geldt dat gebruik van RTU/RTA niet ten koste mag gaan van maatwerk en doseernauwkeurigheid voor kwetsbare patiënten. Daarnaast heeft duurzaamheid van het product ook indirect een positief effect op de gezondheid van de mens (van Daalen, 2024; Romanello, 2023).
Kostenaspecten
Aanschafkosten van RTU en/of RTA zijn over het algemeen hoger dan van losse ampullen en benodigde materialen voor VTGM.
Bij de werkgroep zijn tot zover geen kosten-effectiviteitsstudies bekend. In het algemeen zijn de (aanschaf)kosten van PFSS hoger, in vergelijking met een losse ampul en benodigde materialen voor VGTM. Echter, als andere factoren (e.g. tijdsbesparing personeel, minder medicatiefouten, lagere milieu-impact) worden meegenomen dan laten verschillende business cases (e.g. Erasmus MC, UMCG; opvraagbaar bij werkgroep) zien dat de meerkosten weggestreept worden ten opzichte van andere factoren. De PFSS geven een kostenbesparing wanneer wordt doorgerekend voor heel Nederland met een sensitiviteitsanalyse, rekening houdend met reductie van medicatiefouten en contaminatie (Larmené-Beld, 2019). Deze studie toont dat minder medicatiefouten en minder besmettingen leiden tot kostenbesparing bij brede inzet van PFSS in Nederland.
Gezondheidsgelijkheid
Het gebruik van RTA- en RTU-preparaten leidt naar verwachting niet tot directe verschillen in gezondheidsgelijkheid. Wel geldt dat het verminderen van de milieu-impact van medicatie indirect kan bijdragen aan gezondheidsgelijkheid, aangezien negatieve milieueffecten wereldwijd relatief zwaar drukken op regio’s met een lagere sociaal-economische status (Chancel, 2022; The Lancet Public Health Editorial Board, 2022; Wilkinson, 2022). Het is daarbij belangrijk dat verduurzamingsmaatregelen, zoals de inzet van RTA- en RTU-preparaten, niet leiden tot hogere kosten of verminderde beschikbaarheid, zodat de toegankelijkheid van zorg voor alle patiëntengroepen behouden blijft.
Aanvaardbaarheid
Ethische aanvaardbaarheid
Het gebruik van RTU/RTA is veelal een keuze die een ziekenhuis en zorgverlener maakt en geen directe keuze die aan patiënten wordt voorgelegd. Uiteraard heeft duurzaamheid van een product ook indirect een positief effect op de gezondheid van de mens. De werkgroep voorziet geen ethische bezwaren.
Duurzaamheid
Deze module is volledig gericht op het verlagen van milieu-impact, derhalve speelt duurzaamheid een doorslaggevende- en hoofdrol bij de beschreven interventies.
Haalbaarheid
De haalbaarheid van RTA/RTU hangt af van de bereidwilligheid om als ziekenhuis de keuze te maken om RTA/RTU te gebruiken en de daarmee gepaard gaande hogere directe kosten te dragen. De werkgroep acht het gebruik in de dagelijkse klinische praktijk zeker haalbaar, gezien deze medicatie voldoende voorradig zijn. De interventie kan gezien worden als standaardzorg.
Een ziekenhuis moet financieel bereid zijn om PFSS/RTU flacons en zakken te gebruiken, waarbij minder medicatiefouten, minder besmettingen, minder handelingen en minder gebruik van producten, leidend tot minder afval, meegewogen dient te worden.
Bij deze module is een implementatieplan opgesteld, dat ondersteuning biedt bij het (verder) in de praktijk brengen van de aanbevelingen.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Deze module richt zich op de milieu-impact van RTU/RTA in ziekenhuizen. Voor de vergelijking met conventioneel VTGM op de verpleegafdeling werd geen literatuur gevonden (i.e. geen bewijskracht vastgesteld; PICO1). Voor onderlinge vergelijking tussen verschillende RTA typen is één studie gevonden (PICO2).
Ondanks beperkte beschikbare data worden richtinggevende aanbevelingen gedaan, gebaseerd op literatuur en expert opinie van de werkgroepleden, om bewustwording bij voorschrijvers te vergroten en milieu-impact te verminderen. De werkgroep ziet noodzaak om meer onderzoek te doen naar de milieu-impact van RTU/RTA.
Onderbouwing
Most medications administered parenterally require preparation before administration on the point of care. To skip this preparation-step, some medications are commercially available as sterile ready-to-use (RTU) or ready-to-administer (RTA) products. Examples of RTA product are prefilled syringes or prefilled infusion bags. An example of a RTU product is a vial with a medication-solution in the desired concentration, only requiring removing of the medication from the vial. Although RTU and RTA products are generally more expensive, they might offer advantages in requiring minimal preparation time and lowering infection rates. In addition, the use of these RTU and RTA preparations might potentially lead to a reduction in waste (since less materials are needed for preparation) and fewer medication errors (since preparation-errors are excluded). Another advantage is that sterilized RTA products can be administered during up to 7 days compared to a maximum of 24 hours for products prepared on the ward. However, it is currently unclear what the environmental impact is of RTU and/or RTA parenteral products when compared to conventional parenteral products requiring preparation or batch (=multiple syringes) preparation by the pharmacy. Therefore, this module evaluates the environmental impact of RTU and RTA.
Terminology & abbreviations
|
VTGM |
In Dutch ‘voor toediening gereed maken’. This involves the preparation of medication, often performed on the ward by nurses. Requires the use of products (e.g. gloves, needles, syringes, disinfection products) and the product itself has a relatively short expiry time (24h). |
|
Aseptic |
Using methods to keep free of pathological microorganisms (“no touch method”). |
|
RTU |
Ready To Use. E.g. a vial with a medication-solution in the desired concentration, requiring only removing of the medication from the vial (cf VTGM procedure). |
|
RTA |
Ready To Administer. Prefilled syringe or prefilled infusion bag with the desired concentration of a drug. |
|
PFSS |
Prefilled Sterilized Syringe. A syringe with the desired concentration of a drug, ready to administer. The medication solution in the syringe is sterilized, resulting in longer allowed administration duration (up to 7 days compared to a maximum of 24 hours after VTGM at the ward). |
Note: the terminology RTA is used in the Netherlands only. RTA refers to prefilled syringe of infusion bag
C1
Waste (critical), Climate change (critical), eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
|
No GRADE |
No evidence was found regarding environmental outcomes of RTA and RTU syringes and bags compared with preparation of conventional parenteral products on the ward in hospitalized patients.
Sources: - |
C2
1. Waste (critical)
|
Very low GRADE |
The evidence is very uncertain regarding ‘waste’ of RTA PFSSs compared with RTA aseptic syringes prepared by the hospital pharmacy in hospitalized patients.
Source: (Van Gelder, 2023) |
2. Climate change (critical), eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
|
No GRADE |
Outcome measures ‘climate change’, ‘eco-toxicity’, ‘human toxicity’, ‘water use’, ‘land use’, ‘acidification’, and ‘eutrophication’ were not reported.
Source: - |
Description of studies – C1
No studies were found.
Results – C1
No studies were found.
Level of evidence of the literature – C1
No studies could be graded.
Description of studies – C2
One observational study was included in the analysis of the literature (Van Gelder, 2023). Important study characteristics and results are summarized in the evidence table. The assessment of the risk of bias is summarized in the risk of bias table (under the tab ‘Evidence tabellen’).
Van Gelder (2023) performed an observational study, which evaluated the difference in drug waste between prefilled sterilized syringes (RTA PFSSs) and syringes that were prepared through aseptic batchwise filling by the pharmacy (RTA aseptic syringes) in the Intensive Care Unit (ICU). This study was performed in the 32-bed ICU of the University Medical Center Utrecht. Four different periods were defined within the 8-year study period (August 2015 to May 2023):
- August 2015 – September 2017 (no quarantine time).
- October 2017 – January 2019 (3-day quarantine; RTA aseptic syringes made available for use after preliminary results of TSB fills).
- February 2019 – June 2022 (7-day quarantine; RTA aseptic syringes made available for use after preliminary results of TSB fills and definitive results of TSA settle plate) and
- July 2022 – May 2023 (introduction of three RTA PFSS products; 7-day quarantine still in place for the control group).
Intervention-group = RTA PFSSs
The intervention group consisted of three drug products (potassium chloride 60mmol =60ml, midazolam 50mg =50ml and morphine 50mg =50ml) that were first prepared through aseptic batchwise filling by the hospital pharmacy and then replaced by sterile RTA PFSSs produced by ‘Apotheek A15’, a large-scale compounding pharmacy. These three PFSSs were chosen based on the product range of ‘Apotheek A15’ and product use in the ICU. All three PFSSs had a shelf-life of 18 months during the study period.
Control-group = RTA aseptic syringes
The control group consisted of five drug products (cefazolin, insulin (NovoRapid®), magnesium chloride, milrinone, norepinephrine) that were prepared through aseptic batchwise filling (RTA aseptic syringes). The hospital pharmacy prepared different RTA syringes by aseptic handling through batchwise filling for the ICU according to Dutch national guidelines for preparation under aseptic conditions. Batch sizes differed from 40 syringes (e.g. milrinone 10mg =50ml) to 200 syringes (e.g. norepinephrine 5mg = 50ml).
Outcome: waste (critical)
The primary endpoint of this study was the number of RTA syringes that was wasted, expressed as the percentage of the total number of syringes dispensed to the ICU per time period. Thus, for this literature analysis the reported environmental outcome measure was waste (critical).
Results – C2
1. Waste (critical)
Van Gelder (2023) reported on the outcome waste. The control group and intervention group showed a similar trend across all different time periods (p<0.001), see Table 2.
At the ‘no quarantine period’, the proportion of waste was 5% and 4% in the control group and intervention group, respectively. After introduction of RTA PFSSs, the proportion of waste was 16% in the control group and 5% intervention group. Of the three drug products in the intervention group, morphine had the highest waste percentages over time.
An interrupted time series analysis estimated a direct decrease in total waste percentage of 17.7% after the introduction of RTA PFSSs (p=0.083).
Authors concluded that drug waste percentage of RTA syringes for the ICU can be substantially
decreased by introducing RTA PFSSs, supporting hospitals to enhance environmental sustainability. The guideline panel considered the reported difference in waste between RTA PFSSs and RTA aseptic syringes as relevant.
Table 2. Waste percentage across different time periods (in %)§
|
|
No quarantine |
3-day quarantine |
7-day quarantine |
7-day quarantine |
|
|
Aug 2015 – Sep 2017 |
Oct 2017 – Jan 2019 |
Feb 2019 – June 2022 |
July 2022 – May 2023± |
|
Control group (RTA aseptic syringes) |
5% |
17% |
20% |
16% |
|
Intervention group (RTA PFSSs) |
4% |
27% |
31% |
5% |
±Control group: 7-day quarantine; intervention group: introduction PFSS.
§Waste was in this study defined as the number of RTA syringes that was wasted, expressed as the percentage of the total number of syringes dispensed to the ICU per period.
2. Climate change (critical), eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
No studies were found on critical outcome measure climate change and important outcome measures eco-toxicity, human toxicity, water use, land use, acidification, and eutrophication.
Level of evidence of the literature – C2
1. Waste (critical)
The level of evidence regarding the outcome measure ‘waste’ was downgraded with 3 levels to very low due to risk of bias (-2; lack of adequate adjustment for confounders, short follow-up) and imprecision (-1; lacking information on data distribution, limited generalizability as only one study is included).
2. Climate change (critical), eco-toxicity (important), human toxicity (important), water use (important), land use (important), acidification (important), eutrophication (important)
Outcomes were not reported, thus could not be graded.
Search and select
A systematic review of the literature was performed to answer the following question:
- PICO1: What is the difference in environmental impact between RTU and/or RTA products and conventional products in hospitalized patients receiving intravenous medication?
- PICO2: What is the difference in environmental impact between different RTU and/or RTA products in hospitalized patients receiving intravenous medication?
Table PICO
| Patients | Hospitalized patients receiving treatment with intravenous medications |
| Intervention | Sterile RTU and/or RTA products |
|
Control 1
Control 2 |
C1: Preparation of conventional parenteral products on the ward |
| Outcomes | Climate change (CO2 footprint/Global Warming Potential (GWP)), waste, eco-toxicity, human toxicity, water use, land use, acidification, eutrophication |
| Other selection criteria |
Study design: systematic reviews, randomized controlled trials, comparative observational studies (cohort studies, case-control studies), life cycle assessments, material flow analyses, waste audits, footprinting Period: from 2000 |
Relevant outcome measures
This module focuses specifically on environmental outcomes. Currently, there is no standardized or acknowledged core outcome set available in the field of environmental impact. Therefore, the guideline panel focused on outcomes used in environmental assessments, like life cycle assessments, material flow analyses, waste audits, or footprinting.
The guideline panel considered climate change (CO2 footprint/Global Warming Potential) and waste as critical outcome measures for decision making; and eco-toxicity, human toxicity, water use, land use, acidification, and eutrophication as important outcome measures for decision making.
A priori, the guideline panel defined the outcome measures listed above according to the glossary provided in Box 1, which is adapted from leidraad Duurzaamheid in richtlijnen.
Due to the variety of scopes and methods used in studies to perform and report results, the guideline panel did not define the minimal important difference a priori. Differences between the techniques were evaluated by the guideline panel after data extraction.
Box 1. Glossary
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 13 August 2024. The detailed search strategy is listed under the tab ‘Search strategy’. The systematic literature search resulted in 25 hits.
Studies were selected based on the following criteria:
- Systematic reviews in which searches were performed in at least two databases, with a detailed search strategy, risk of bias assessment and results of individual studies available, randomized controlled trials, (observational) comparative studies, life cycle assessments.
- Full-text English or Dutch language publication and
- Studies according to the PICO.
Initially, five studies were selected based on title and abstract screening. After reading the full text, four studies were excluded (see the Exclusion table under the tab ‘Evidence tabellen’), and one study was included (Van Gelder, 2023).
- Benhamou D, Weiss M, Borms M, Lucaci J, Girgis H, Frolet C, Baisley WT, Shoushi G, Cribbs KA, Wenk M. Assessing the Clinical, Economic, and Health Resource Utilization Impacts of Prefilled Syringes Versus Conventional Medication Administration Methods: Results From a Systematic Literature Review. Ann Pharmacother. 2024 Sep;58(9):921-934. doi: 10.1177/10600280231212890. Epub 2023 Nov 28. PMID: 38014840.
- Chancel L. Global carbon inequality over 1990–2019. Nat Sustain. 2022 Sep;5:931–938. doi: 10.1038/s41893-022-00955-z.
- van Daalen KR, Tonne C, Semenza JC, et al. The 2024 Europe report of the Lancet Countdown on health and climate change: unprecedented warming demands unprecedented action. Lancet Public Health. 2024 Jul;9(7):e495-e522. doi: 10.1016/S2468-2667(24)00055-0. Epub 2024 May 12. Erratum in: Lancet Public Health. 2024 Jul;9(7):e420. doi: 10.1016/S2468-2667(24)00129-4. PMID: 38749451; PMCID: PMC11209670.
- De Groene IC, 2025. Alle tips > Medicatie > Op = Stop principe. Geraadpleegd op: 6 februari 2025. Link: https://degroeneic.nl/aan-de-slag/medicatie/.
- EAHP, 2023. Report: Special Interest Group on the Use of Prefilled Syringes in Intensive Care Units and Operating Theatres. Link: sig_report_on_the_use_of_pfs_in_icus_and_operatign_theatres.pdf.
- Van Gelder TG, Lalmohamed A, Dorst-Mooiman KD, Dekker JC, Schinkel MJ, Sikma MA, Uijtendaal EV, Egberts TCG. Drug waste of ready-to-administer syringes in the intensive care unit: Aseptically prepared syringes versus prefilled sterilized syringes. Eur J Pharm Sci. 2023 Dec 1;191:106590. doi: 10.1016/j.ejps.2023.106590. Epub 2023 Sep 22. PMID: 37742987.
- Honkoop, Margot, et al. "Reducing the Environmental Impact of Syringes at the Intensive Care Unit." International Conference on Healthcare Systems Ergonomics and Patient Safety. Cham: Springer Nature Switzerland, 2022. Link: https://repository.tudelft.nl/record/uuid:6996ab9f-cc04-4ef7-92e5-4f9399afaf4f.
- Larmené-Beld KHM, Spronk JT, Luttjeboer J, Taxis K, Postma MJ. A Cost Minimization Analysis of Ready-to-Administer Prefilled Sterilized Syringes in a Dutch Hospital. Clin Ther. 2019 Jun;41(6):1139-1150. doi: 10.1016/j.clinthera.2019.04.024. Epub 2019 May 10. PMID: 31079861.
- Kelly FE, Frerk C. Prefilled syringes have significant human factors benefits and would improve anaesthetic medication safety. Anaesthesia. 2023 Jul;78(7):921. doi: 10.1111/anae.16023. Epub 2023 Apr 5. PMID: 37020326.
- Nederlandse Vereniging van Ziekenhuisapothekers (NVZA). GMP‑Z Z3: Herziening februari 2022 – Aseptische handelingen [Internet]. Utrecht: NVZA; 2022 [cited 2025 Jul 21]. Available from: https://nvza.nl/wp-content/uploads/Z3-GMPZ_Herziening-feb-2022-definitief.pdf
- NHS, 2022. Guidance - Transforming NHS pharmacy aseptic services in England. Published 29 October 2020. Accessed at 31-12-2024. Link: https://www.gov.uk/government/publications/transforming-nhs-pharmacy-aseptic-services-in-england/transforming-nhs-pharmacy-aseptic-services-in-england.
- Peters E, Fikkers B, de Sévaux R, ter Heine Rob. Case report: De kaliumverrassing; een onbedoeld hoge dosis zonder gevolgen. De intensivist. Editie 5 - september 2024, Volume 32. Link: h https://de-intensivist.nl/de-kaliumverrassing-een-onbedoeld-hoge-dosis-zonder-gevolgen/.
- Romanello M, Napoli CD, Green C, et al. The 2023 report of the Lancet Countdown on health and climate change: the imperative for a health-centred response in a world facing irreversible harms. Lancet. 2023 Dec 16;402(10419):2346-2394. doi: 10.1016/S0140-6736(23)01859-7. Epub 2023 Nov 14. PMID: 37977174.
- The Lancet Public Health Editorial Board. No public health without planetary health. Lancet Public Health. 2022 Apr;7(4):e291. doi: 10.1016/S2468-2667(22)00068-8.
- Whitaker DK, Lomas JP. Time for prefilled syringes - everywhere. Anaesthesia. 2024 Feb;79(2):119-122. doi: 10.1111/anae.16181. Epub 2023 Nov 16. PMID: 37971165.
- Wilkinson JL, Boxall ABA, Kolpin DW, Leung KMY, Lai RWS, Galbán-Malagón C, Adell AD, Mondon J, Metian M, Marchant RA, Bouzas-Monroy A, Cuni-Sanchez A, Coors A, Carriquiriborde P, Rojo M, Gordon C, Cara M, Moermond M, Luarte T, Petrosyan V, Perikhanyan Y, Mahon CS, McGurk CJ, Hofmann T, Kormoker T, Iniguez V, Guzman-Otazo J, Tavares JL, Gildasio De Figueiredo F, Razzolini MTP, Dougnon V, Gbaguidi G, Traoré O, Blais JM, Kimpe LE, Wong M, Wong D, Ntchantcho R, Pizarro J, Ying GG, Chen CE, Páez M, Martínez-Lara J, Otamonga JP, Poté J, Ifo SA, Wilson P, Echeverría-Sáenz S, Udikovic-Kolic N, Milakovic M, Fatta-Kassinos D, Ioannou-Ttofa L, Belušová V, Vymazal J, Cárdenas-Bustamante M, Kassa BA, Garric J, Chaumot A, Gibba P, Kunchulia I, Seidensticker S, Lyberatos G, Halldórsson HP, Melling M, Shashidhar T, Lamba M, Nastiti A, Supriatin A, Pourang N, Abedini A, Abdullah O, Gharbia SS, Pilla F, Chefetz B, Topaz T, Yao KM, Aubakirova B, Beisenova R, Olaka L, Mulu JK, Chatanga P, Ntuli V, Blama NT, Sherif S, Aris AZ, Looi LJ, Niang M, Traore ST, Oldenkamp R, Ogunbanwo O, Ashfaq M, Iqbal M, Abdeen Z, O'Dea A, Morales-Saldaña JM, Custodio M, de la Cruz H, Navarrete I, Carvalho F, Gogra AB, Koroma BM, Cerkvenik-Flajs V, Gombač M, Thwala M, Choi K, Kang H, Ladu JLC, Rico A, Amerasinghe P, Sobek A, Horlitz G, Zenker AK, King AC, Jiang JJ, Kariuki R, Tumbo M, Tezel U, Onay TT, Lejju JB, Vystavna Y, Vergeles Y, Heinzen H, Pérez-Parada A, Sims DB, Figy M, Good D, Teta C. Pharmaceutical pollution of the world's rivers. Proc Natl Acad Sci U S A. 2022 Feb 22;119(8):e2113947119. doi: 10.1073/pnas.2113947119. PMID: 35165193; PMCID: PMC8872717.
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
||||||||||||||||||||||||||||||||||
|
Van Gelder, 2023 |
Type of study: Observational study
Setting and country: ICU, the Netherlands
Funding and conflicts of interest: No information on funding was reported. Authors declared no competing interests. |
No patients involved |
RTA prefilled sterilized syringes (PFSS): commercially available RTA syringes prepared by a large-scale compounding pharmacy that were sterilized after production.
Three drug products: morphine, midazolam, potassium chloride. |
RTA aseptic syringes: RTA syringes prepared by the hospital pharmacy in the drug compounding facility of the ICU by aseptic handling through batchwise filling.
Five drug products: cefazolin, insulin novorapid, magnesium chloride, milrinone, norepinephrine.
|
Three different time periods were defined, based on quarantine time:
During quarantine, mandatory pharmaceutical quality control (QC) testing was performed. Quarantine time changed over the study period due to updates in national guidelines. |
Wastage of RTA syringes
Total waste percentages differed significantly across the four groups (p<0.001).
The 5% total waste after introduction of the RTA PFSS decreased significantly from the 7-day quarantine period (p<0.001). In an interrupted time series analysis, this was estimated at a direct absolute decrease of 17.7% (p=0.083). |
Comment: No direct comparisons in drug waste were made between the introduction of PFSS and use of aseptic syringes during the period without quarantine and period with 3-day quarantine.
Limitation: Study only looked at transaction data of the syringes and that no other data was included in the ITS model. Possible elements that could have impacted on drug waste over time were thus not taken into account.
Authors conclusion: Drug waste of RTA syringes for the ICU can be significantly decreased by introducing PFSSs, supporting hospitals to enhance environmental sustainability. The waste percentage of RTA syringes prepared through aseptic batchwise filling is significantly impacted by duration of quarantine time. |
||||||||||||||||||||||||||||||||||
Risk of Bias table
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors?
|
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables? |
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed?
|
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
Van Gelder, 2023 |
Not applicable
Reason: It applied RTA syringes versus RTA PFSSs.
|
Definitely yes
Reason: The two groups were compared in this observational study, a medication management system was used. |
Definitely no
Reason: Waste was present during whole study period.
|
Definitely no
Reason: No statistical analysis regarding confidence intervals/ uncertainty, confounding was performed.
|
Probably no
Reason: See previous comment. |
Probably yes
Reason: A medication management system was used to register every transaction, which seems a valid/ reliable method. On the other hand, only transaction data were considered. Possible elements that could have impacted on drug waste over time were not measured. |
Definitely no
Reason: The waste % of RTA PFSSs were only measured over a relatively short period of 10mo, within a total study period of 8y. This limited data on RTA PFSSs may contributed to lack of statistical significance. |
No information
Reason: Not reported. |
HIGH (waste)
|
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Benhamou D, Piriou V, De Vaumas C, Albaladejo P, Malinovsky JM, Doz M, Lafuma A, Bouaziz H. Ready-to-use pre-filled syringes of atropine for anaesthesia care in French hospitals - a budget impact analysis. Anaesth Crit Care Pain Med. 2017 Apr;36(2):115-121. doi: 10.1016/j.accpm.2016.03.009. Epub 2016 Jul 30. PMID: 27481691. |
Wrong outcome |
|
Ramesh S, Sivaranjani S, Hasmukhbhai NZ, Yadav D. Power of compounding intravitreal Bevacizumab - Experience from a tertiary eye care hospital. Indian J Ophthalmol. 2022 May;70(5):1869. doi: 10.4103/ijo.IJO_1016_22. PMID: 35502117; PMCID: PMC9332976. |
Wrong article type (video abstract) |
|
Vogl TJ, Wessling J, Buerke B. An observational study to evaluate the efficiency and safety of ioversol pre-filled syringes compared with ioversol bottles in contrast-enhanced examinations. Acta Radiol. 2012 Oct 1;53(8):914-20. doi: 10.1258/ar.2012.120303. Epub 2012 Sep 14. PMID: 22983259. |
Wrong comparison |
|
No authors listed. Study: use of prefilled syringes is faster, safer than bedside preparation of drug infusions. Health Devices. 2012 Nov;41(11):370. PMID: 23444728. |
Wrong article type (conference abstract) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 07-05-2026
Beoordeeld op geldigheid : 07-05-2026
Algemene gegevens
De ontwikkeling/herziening van deze module werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS).
De financier heeft geen enkele invloed gehad op de inhoud van de leidraad.
Samenstelling werkgroep
Voor het ontwikkelen van de leidraad is in 2024 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij farmaceutisch specialistische zorg.
Werkgroep Inhoud
- Dr. L.J.M. (Loes) van Herpen – Meeuwissen (voorzitter), ziekenhuisapotheker, Radboudumc, NVZA
- Dr. M.E. (Milly) Attema – de Jonge, ziekenhuisapotheker, Meander MC, NVZA
- Dr. C. (Charlotte) Bekker, universitair docent, Radboudumc, persoonlijke titel
- Drs. V. (Vivienne) de Smet, AIOS spoedeisende geneeskunde, Diakonessenhuis, NVSHA
- Dr. N.G.M. (Nicole) Hunfeld, ziekenhuisapotheker, universitair hoofddocent, Erasmus MC, NVIC
- Dr. B.J.A. (Ben) Janssen, farmacoloog, universitair hoofddocent, Maastricht UMC, persoonlijke titel
- Dr. B. (Berber) Kapitein, kinderarts-intensivist, Amsterdam UMC, NVK
- Drs. R. (Remco) Minkhorst, anesthesioloog, UMC Utrecht, NVA
- Drs. J.D. (Joost) Piët, arts-docent en promovendus farmacotherapie, Amsterdam UMC, NVKFB
- Y.H.M. (Yvonne) van Grinsven – Ariaans, (regie)verpleegkundige, Radboudumc, V&VN
- M. (Marga) van Timmeren, kwaliteitsfunctionaris, BModesto, NVFZ
Werkgroep Implementatie
- B.A.P. (Bart) Cramers, apotheker, programmamanager dure geneesmiddelen, NVZ
- Drs. M. (Maarten) Loof, programmamanager dure geneesmiddelen, ZN
- P. (Peter) Roos, adviseur, UMCNL (voorheen NFU; tot december 2024)
- Prof. dr. E.L. (Noortje) Swart, ziekenhuisapother, hoogleraar Klinische Farmacologie en Apotheek, hoofd adeling klinische farmacologie en apotheek, Amsterdam UMC, UMCNL (vanaf maart 2025)
Klankbordgroep
- Dr. P.H.P (Pascal) de Jong, reumatoloog, universitair hoofddocent, Erasmus MC, NVR
- Dr. F. (Femme) Dirksmeier – Harinck, MDL-arts, Franciscus, NVMDL
- Prof. dr. W.J.K. (Wouter) Hehenkamp, gynaecoloog, hoogleraar gynaecologie gericht op doelmatige en duurzame zorg, Amsterdam UMC, NVOG
- Drs. A. (Annemieke) Horikx, apotheker, KNMP
- Dr. J.J.W.M. (Jeroen) Janssen, internist-hematoloog, Radboudumc, NIV
- Dr. P.H.C. (Philip) Kremer, neuroloog, Leids Universitair Medisch Centrum, NVN
- Dr. M. (Maartje) Los, internist-oncoloog, St. Antonius Ziekenhuis, NIV
- Prof. dr. F.M.A.C. (Fabrice) Martens, cardioloog, hoogleraar Preventieve cardiologie, Amsterdam UMC, NVVC
- Drs. N.M.F. (Nikki) Noorda, klinisch geriater, Dijklander Ziekenhuis, NVKG
- Dr. S. (Sam) Schoenmakers, gynaecoloog, Erasmus MC, NVOG
- Drs. D.C. (Dorothée) van Trier, traumachirurg, Diakonessenhuis, NVvH
- P. (Paula) Warmerdam, verpleegkundig specialist, Alrijne Ziekenhuis, V&VN
Met ondersteuning van
- Dr. R. (Renee) Bolijn, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. T. (Thibaut) Dederen, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. C.T.J. (Charlotte) Michels, senior adviseur, Kennisinstituut van de Federatie Medisch Speclisten
- E. (Esther) van der Bijl, Informatiespecialist, Kennisinstituut van de Federatie Medisch Speclisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Gemelde belangen |
Ondernomen actie |
|
Werkgroep Inhoud |
||||
|
Van Herpen – Meeuwissen (voorzitter) |
Ziekenhuisapotheker, Radboudumc, Nijmegen |
NVZA: lid commissie Duurzaamheid |
* ZonMW, Medicatie in eigen beheer 848022007. * Auteur: |
Geen restricties |
|
Attema – de Jonge |
Ziekenhuis apotheker, Meander Medisch Centrum, Amersfoort |
Lid Commissie Duurzaamheid NVZA |
Geen |
Geen restricties |
|
Bekker |
Senior onderzoeker, Radboudumc, Nijmegen |
Voorzitter NFU werkgroep Green deal duurzame zorg thema 5 'medicijnen' |
* ZonMw Heruitgifte orale oncolytica 848018008 * ZonMw RODEO trial 10140021910501 * Transformatieovereenkomst heruitgifte orale oncolytica * VWS Green Deal duurzame zorg thema 5 'medicijnen' * Senior onderzoeker duurzaam geneesmiddelgebruik |
Geen restricties |
|
De Smet |
AIOS SEH, Diakonessenhuis, Utrecht |
* Lid commissie Groene SEH |
Geen |
Geen restricties |
|
Hunfeld |
* Ziekenhuisapotheker, Erasmus MC, Rotterdam (betaald) * Projectleider onderzoek duurzame zorg, Erasmus MC, Rotterdam (betaald) |
* Vice voorzitter en penningmeester KNMP (betaald) * Voorzitter Groene IC NVIC (onbetaald) vVoorzitter commissie ATG (LCG) (betaald) * Toezichthouder VVT Het Maanderzand (betaald) * Lid Commissie Duurzaamheid NVZA |
NWO (geen onderzoek over medicijnen) |
Geen restricties |
|
Janssen (Ben) |
Universitair Hoofddocent Farmacologie, Vakgroep Farmacologie & Toxicologie, Faculty of Health Medicines and Life Sciences Maastricht University. Werk op afdeling Beeldvorming van het Maastrichts Universitair Medisch Centrum. |
Geen |
Geen |
Geen restricties |
|
Kapitein |
Kinderarts-intensivist, Emma Kinderziekenhuis Amsterdam UMC, Amsterdam |
* Lid Groene Kinderarts * NVK Lid wetenschapscommissie |
* MACU-PICU Stichting CJ Vaillant. Multisystem phenotyping of severe ACUte asthma at the Pediatric Intensive Care Unit (macu-pico). Postdoc (geen PI). * AUMC Medewerkersberaad innovatie subsidie "Het AUMC medewerkersberaad: op weg naar duurzaam woon-werkverkeer (studie reeds afgerond). |
Geen restricties |
|
Minkhorst |
Anesthesioloog UMC Utrecht |
Geen |
Geen |
Geen restricties |
|
Piët |
*Fulltime arts-docent en -onderzoeker Farmacotherapie in het AmsterdamUMC (locatie VUmc). *Al het onderwijs betreffende het voorschrijven van medicatie verzorgen voor de opleidingen geneeskunde, tandheelkunde en masteropleidingen voor verpleegkundigen. *Promovendus op gebied van het integreren van milieu-impact door medicatie in het medisch onderwijs. Deze werkzaamheden zijn allen betaald vanuit mijn aanstelling. |
* Klinisch farmacoloog in opleiding * Projectcoördinator Erasmus+ projecten CP4T en PlanED Prescribing |
Erasmus+ projecten: * Planetary Health Education in Prescribing (PlanED Prescribing) * Clinical Pharmacology and Therapeutics Teach The Teacher (CP4T)
Auteur NTvG artikel "Vermindering van de milieu-impact van medicatie; De rol van de voorschrijver" (D7985) (Toekomstige) Uitkomsten (wetenschappelijk) van Erasmus+ project PlanED Prescribing en van eigen PhD. PMID 39303730 |
Geen restricties |
|
Van Grinsven – Ariaans |
* Verpleegkundige Orthopedie Radboudumc (contract 12 uur, betaald) * Kwaliteitsfunctionaris afdeling Orthopedie/KNO/MKA/PCH/Trauma Radboudumc (contract 12 uur, betaald) |
Geen |
Geen |
Geen restricties |
|
Van Timmeren |
Sr Quality Officer, Bmodesto, Lelystad |
Geen |
Geen |
Geen restricties |
|
Werkgroep Implementatie |
||||
|
Cramers |
Programmamanager Dure Geneesmiddelen NVZ Belangenbehartiging ziekenhuizen op dure geneesmiddelen gebied. Gaat over kwaliteit, beschikbaarheid en betaalbaarheid. |
Geen |
Geen |
Geen restricties |
|
Loof |
Programmamanager Dure Geneesmiddelen bij ZN |
Geen |
Geen |
Geen restricties |
|
Roos |
Adviseur binnen NFU |
Geen |
Geen |
Geen restricties |
|
Swart |
Hoofd Afdeling Apotheek en Klinische Farmacologie, AmsterdamUMC |
* Voorzitter Wetenschappelijke Adviesraad Commissie Farmacotherapeutisch Kompas (WAR CFK), Zorginstituut Nederland * Voorzitter NVKFB. * Lid bestuur KNMP |
Echtgenoot werkt bij Pfizer in een niet commerciële functie. Geen relatie met werkgroep
Medicijn voor de Maatschappij: Bereidingen voor zeldzame metabole ziekten. |
Geen restricties |
|
Klankbordgroep |
||||
|
De Jong |
Reumatoloog, Erasmus MC, Rotterdam |
* Lid adviesraad voor Abbvie; AstraZeneca; Bristol-Myers Squibb; Galapagos; Lilly; Novartis; Pfizer; Sanofi Genzyme; UCB * Verzorging van onderwijs voor Abbvie; Galapagos; Lilly; Novartis; Pfizer |
Subsidies voor investigated initiated studies van Abbvie; Dutch Arthritis Foundation; Galapagos; Lilly; Pfizer. 1. Abbvie, ontwikkelen tool voor zorg op afstand, projectleider. 2. Dutch Arthitis Foudation, gecombineerde leefstijlinterventie trial, projectleider. 3. Galapagos: trial naar belandeling op maat. 4. Pfizer: Toediening van medicatie obv chronobiologie, projectleider. 5. Lilly: Implementatieonderzoek gericht op persoonsgerichte zorg, projectleider. |
Geen restricties |
|
Dirksmeier – Harinck |
MDL-arts, Franciscus, Rotterdam |
Geen |
Geen |
Geen restricties |
|
Hehenkamp |
Gynaecoloog, AmsterdamUMC, Amsterdam |
Allen onbetaald: -lid pijlerbestuur gynaecologie -voorzitter Gynae Goes Green (landelijke groen commissie GYN) -lid bestuur SIG anticonceptie -Bestuur Hector Treub stichting |
1. ZonMW: Substitutie van zorg Covid, projectleider. 2. ZonMW: Ulipristal bij myomen., projectleider. 3. Merit Medical: QUESTA trial (adenomyose en hysterectomie danwel embolisatie). 4. ZonMW: Keuzehulp Myomen, projectleider. |
Geen restricties |
|
Horikx |
Apotheker, teamleider Geneesmiddel Informatie Centrum KNMP |
* Bestuurslid Stichting Farmaceutisch Erfgoed. * Commissielid interacterende medicatie VKA's. * Werkgroeplid kritische en kwetsbare geneesmiddelenlijst-NVZA. * Praktijkteamlid palliatieve zorg |
Geen |
Geen restricties |
|
Janssen (Jeroen) |
internist-hematoloog, Afdeling Hematologie, Radboud UMC, Nijmegen, betaald |
* Voorzitter, St. Apps for Care and Science, betaald. * Bestuurslid en penningmeester, Nederlandse Vereniging voor Hematologie, onbetaald |
De St. Apps for Care and Science ontwikkelt de HematologyApp, een smartphone-, tablet- en binnenkort ook web-based applicatie die als doel heeft het werk van hematologen te verbeteren, de kwaliteit van de zorg voor hematologische patienten te verbeteren en klinisch wetenschappelijk onderzoek te bevorderen. Deze stichting zoekt ondersteuning voor het behalen van haar doelen bij farmaceutische bedrijven die initatieven van de stichting kunnen sponsoren. De volgende bedrijven zijn sponsor/donateur van de stichting: Daiichi-Sankyo, Johnson & Johnson, SERB, Sanofi, SOBI, Novo-Nordisk, MSD, Biomea, AstraZeneca, BristolMyersSquibb, Alexion, Kite-Gilead, Pfizer, Abbvie, Astellas,Novartis, Amgen, Takeda en Servier. |
Geen restricties |
|
Kremer |
*Research Director Neurology bij The Centre for Human Drug Research, Leiden * Neuroloog bij het Leids Universitair Medisch Centrum, Leiden |
Geen |
In het CHDR ben ik verantwoordelijk voor ongeveer 10 vroege fase medicijnstudies gefinancierd door veelal Amerikaanse biotech of grote farma. De onderzoeksmiddelen zitten dermate vroeg in het ontwikkeltraject dat er geen belangenverstrengeling is. |
Geen restricties |
|
Los |
internist oncoloog in het St Antonius Ziekenhuis Utrecht/ Nieuwegein |
Geen |
Geen |
Geen restricties |
|
Martens |
Cardioloog, hoogleraar Preventieve Cardiologie bij het Amsterdam UMC, Amsterdam. Namens de NVVC vertegenwoordigend. |
* Adviseur CVRM en medicatie NVVC. * Voorzitter Werkgroep Geneesmiddelen NVVC * Voorzitter DCVA Commissie Preventie * Clinical Valorization Officer Amsterdam UMC *Voorzitter Hartstichting Hart-Vaatagenda-project 'Op tijd ontdekken' Wetenschappelijk nog wel verbonden aan het HartVaatCentrumSalland |
Sprekersvergoeding zonder belangenverstrengeling gezien altijd naar Amsterdam UMC.
Sponsoring GOLDEN-studie: Novartis, Amarin, Novo Nordisk en een Europese IHI-grant. Sponsoring 2-DECIDE-studie: ZoNMW en ZE&GG Sponsoring EUROASPIRE: Hartstichting |
Geen restricties |
|
Noorda |
Klinisch geriater in het Dijklanderziekenhuis |
Geen |
Geen |
Geen restricties |
|
Schoenmakers |
Gynaecoloog, Erasmus MC Universtair Medisch Centrum, Rotterdam |
* Wetenschap-commissielid Strong Babies (onbetaald) * Gezondheidsraad - algemeen / commissie vaccinatie (vacatiegelden) |
ZonMW Open Competitie (2019-2024) - ondewerp Obesitas, microbioom en zwangerschap |
Geen restricties |
|
Van Trier |
(Trauma) Chirurg OLVG en BovenIJ Ziekenhuis |
* Werkgroep Groen OK NVVH. * Tevens lid van de werkgroep Plastic en Circulair van het Landelijk Netwerk Groene OK, onbetaald. |
Geen |
Geen restricties |
|
Warmerdam |
Verpleegkundig specialist werkzaam bij Alrijne |
Presentaties geven aan POH en Huisartsen |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland (PFN) voor deelname aan de werkgroep Inhoud en aan twee invitational conferences. Op advies van de PFN heeft de werkgroep de uitkomsten uit het rapport Verduurzaming van de zorg geïntergreerd in de modules. Daarnaast is module 6 Communicatie over milieubewust medicatiegebruik specifiek gericht op communicatie over milieubewust medicatiegebruik met patiënten. De conceptleidraad is tevens voor commentaar voorgelegd aan de PFN en de aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de leidraad voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de leidraad per module op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Gebruik van ready-to-use/ready-to-administer preparaten |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten), volgt uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte methodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze leidraad is hieronder weergegeven.
Zoekverantwoording
Zoekstrategie - 13 augustus 2024
Embase.com
|
No. |
Query |
|
#1 |
'intravenous drug administration'/exp OR 'parenteral drug administration'/exp OR (((iv OR intravenous OR 'intra venous' OR parenteral*) NEAR/3 (drug* OR deliver* OR therap* OR medicat* OR administer* OR dos* OR drip* OR infusion* OR injection* OR therap* OR transfusion* OR infusion* OR treatment*)):ti,ab,kw) OR (((vein* OR venous) NEAR/2 (injection* OR drip* OR infusion* OR transfusion* OR administer*)):ti,ab,kw) OR 'drip* infusion*':ti,ab,kw |
|
#2 |
'prefilled syringe'/exp OR (((prefill* OR preload* OR 'pre fill*' OR 'pre load*') NEAR/3 (syringe* OR system* OR inject*)):ti,ab,kw) OR 'ready to use':ti,ab,kw OR 'ready to administ*':ti,ab,kw |
|
#3 |
((rtu OR rta) NEAR/3 (intravenous OR 'intra venous')):ti,ab,kw |
|
#4 |
'biodegradable plastic'/exp OR 'biodiversity'/de OR 'climate change'/exp OR 'climate resilience'/exp OR 'disposable equipment'/exp OR 'ecological diversity'/exp OR 'energy conservation'/exp OR 'environmental aspects and related phenomena'/exp OR 'environmental footprint'/exp OR 'environmental protection'/exp OR 'eutrophication'/exp OR 'life cycle assessment'/exp OR 'pollution and pollution related phenomena'/exp OR 'species diversity'/exp OR 'waste and waste related phenomena'/exp OR 'wastewater'/exp OR 'water management'/exp OR 'water pollution'/exp OR 'global warming potential'/exp OR acidification:ti,ab,kw OR (((water OR land) NEXT/1 use):ti,ab,kw) OR (((air OR organic OR soil OR water OR plastic* OR liquid*) NEAR/4 (pollut* OR contamina* OR wast*)):ti,ab,kw) OR biodivers*:ti,ab,kw OR 'biological divers*':ti,ab,kw OR (((co2 OR 'co 2' OR carbon OR 'nitrous oxide') NEAR/3 (emission* OR footprint OR equival* OR reduct*)):ti,ab,kw) OR (((nature OR environment* OR climat*) NEAR/3 (impact* OR pollut* OR conservat* OR protect* OR preserv* OR effect* OR benefit* OR chang* OR exposure* OR resilien*)):ti,ab,kw) OR disposable*:ti,ab,kw OR ((eco* NEAR/3 (toxic* OR efficien* OR damage)):ti,ab,kw) OR ecotoxic*:ti,ab,kw OR ecoefficien*:ti,ab,kw OR (((emission OR waste) NEAR/3 reduc*):ti,ab,kw) OR environmental*:ti OR (((equipment* OR product* OR waste*) NEAR/3 reus*):ti,ab,kw) OR recycl*:ti,ab,kw OR 'resource recover*':ti,ab,kw OR eutrophicat*:ti,ab,kw OR (((global OR climate) NEAR/2 warming):ti,ab,kw) OR ((green* NEAR/2 (deal OR surger* OR effect* OR gas* OR resource*)):ti,ab,kw) OR (((hospital OR medical OR zero OR product* OR byproduct* OR 'by product*' OR avoid* OR energy OR management OR nuclear OR biomass) NEAR/3 waste*):ti,ab,kw) OR ((('life cycle' OR lifecycle) NEAR/2 (assess* OR inventor*)):ti,ab,kw) OR lca:ti,ab,kw OR lcas:ti,ab,kw OR 'human toxicity potential*':ti,ab,kw OR (((ep OR h+ OR gwp OR faetp OR fatp OR ap OR cfc OR 'kg n' OR 'nox' OR '2.4' OR '2,4' OR pocp OR so2 OR dichlorobenzen* OR ethan* OR po4 OR dcb) NEAR/3 equival*):ti,ab,kw) OR ((ozone NEAR/3 (deplet* OR hole*)):ti,ab,kw) OR (((plastic* OR microplastic* OR 'micro plastic*') NEAR/3 (overuse OR soup OR pollut* OR contaminat*)):ti,ab,kw) OR recycle*:ti,ab,kw OR recycling:ti,ab,kw OR (((refuse OR waste) NEAR/3 disposal):ti,ab,kw) OR reusable*:ti,ab,kw OR reuse*:ti,kw OR reusing:ti,kw OR 'rising sea level*':ti,ab,kw OR 'sea level ris*':ti,ab,kw OR smog:ti,ab,kw OR sustainab*:ti,kw OR ((sustainab* NEAR/3 (development* OR cycle* OR management OR effect* OR environment*)):ti,ab,kw) OR ((water NEAR/3 (purificat* OR sanitat* OR treatment)):ti,ab,kw) OR wastewater:ti,ab,kw OR ((hydrogen NEAR/3 moles NEAR/3 equival*):ti,ab,kw) OR 'circular econom*':ti,ab,kw OR biodegradab*:ti,ab,kw OR (((ecological OR environmental OR water OR energy OR climate OR global) NEAR/2 footprint*):ti,ab,kw) OR waste:ti,ab,kw OR wastes:ti,ab,kw OR reuse:ti,ab,kw OR reusab*:ti,ab,kw OR reprocess*:ti,ab,kw OR pollut*:ti,ab,kw OR greening:ti,ab,kw OR spillage:ti,ab,kw OR spilling:ti,ab,kw OR spoilage:ti,ab,kw OR salinization:ti,ab,kw OR 'cradle to cradle':ti,ab,kw OR 'carbon neutral*':ti,ab,kw OR wastage*:ti,ab,kw |
|
#5 |
(#1 AND #2 OR #3) AND #4 |
|
#6 |
#5 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
|
#7 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
|
#8 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
|
#9 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
|
#10 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
|
#11 |
#6 AND #7 – SR’s |
|
#12 |
#6 AND #8 NOT #11 – RCT’s |
|
#13 |
#6 AND (#9 OR #10) NOT (#11 OR #12) – Observationeel |
|
#14 |
#6 NOT (#11 OR #12 OR #13) – Overig |
|
#15 |
#11 OR #12 OR #13 OR #14 |
Ovid/Medline
|
# |
Searches |
|
1 |
exp Administration, Intravenous/ or exp Infusions, Intravenous/ or exp Injections, Intravenous/ or ((iv or intravenous or intra venous or parenteral*) adj3 (drug* or deliver* or therap* or medicat* or administer* or dos* or drip* or infusion* or injection* or therap* or transfusion* or infusion* or treatment*)).ti,ab,kf. or ((vein* or venous) adj2 (injection* or drip* or infusion* or transfusion* or administer*)).ti,ab,kf. or drip* infusion*.ti,ab,kf. |
|
2 |
(((prefill* or preload* or pre fill* or pre load*) adj3 (syringe* or system* or inject*)) or 'ready to use' or 'ready to administ*').ti,ab,kf. |
|
3 |
((rtu or rta) adj3 (intravenous or intra venous)).ti,ab,kf. |
|
4 |
Biodegradable Plastics/ or exp Biodiversity/ or exp Carbon Footprint/ or exp Environmental Pollution/ or exp Climate Change/ or Disposable Equipment/ or Environment/ or Equipment Reuse/ or exp Eutrophication/ or Greenhouse Gases/ or Greenhouse Effect/ or exp Hazardous Waste/ or exp Medical Waste/ or Ozone Depletion/ or Recycling/ or exp Refuse Disposal/ or Smog/ or Waste Products/ or exp Waste Water/ or acidification.ti,ab,kf. or ((air or organic or soil or water or plastic* or liquid*) adj4 (pollut* or contamina* or wast*)).ti,ab,kf. or (biodivers* or "biological divers*").ti,ab,kf. or ((co2 or "co 2" or carbon) adj3 (emission* or footprint or equival* or reduct*)).ti,ab,kf. or ((nature or environment* or climat*) adj3 (impact* or pollut* or conservat* or protect* or preserv* or effect* or benefit* or chang* or exposure* or resilien*)).ti,ab,kf. or disposable*.ti,ab,kf. or (eco* adj3 (toxic* or efficien* or damage)).ti,ab,kf. or ecotoxic*.ti,ab,kf. or ecoefficien*.ti,ab,kf. or ((waste or emission*) adj3 reduc*).ti,ab,kf. or environmental*.ti. or ((equipment* or product* or waste*) adj3 reus*).ti,ab,kf. or recycl*.ti,ab,kf. or resource recover*.ti,ab,kf. or eutrophicat*.ti,ab,kf. or ((global or climate) adj2 warming).ti,ab,kf. or (("life cycle" or lifecycle) adj2 (assess* or inventor*)).ti,ab,kf. or LCA.ti,ab,kf. or LCAs.ti,ab,kf. or (("life cycle" or lifecycle) adj2 (assess* or inventor* or analys*)).ti,ab,kf. or (green* adj2 (deal or surger* or effect* or gas* or resource*)).ti,ab,kf. or greening.ti,ab,kf. or ((hospital or medical or zero or product* or byproduct* or "by product*" or avoid* or energy or management or nuclear or biomass) adj3 waste*).ti,ab,kf. or "human toxicity potential*".ti,ab,kf. or ((EP or H+ or GWP or FAETP or FATP or AP or CFC or "kg N" or "NOx" or "2.4" or "2,4" or POCP or SO2 or dichlorobenzen* or ethan* or PO4 or DCB) adj3 equival*).ti,ab,kf. or (ozone adj3 (deplet* or hole*)).ti,ab,kf. or ((plastic* or microplastic* or "micro plastic*") adj3 (overuse or soup or pollut* or contaminat*)).ti,ab,kf. or recycle*.ti,ab,kf. or recycling.ti,ab,kf. or ((refuse or waste) adj3 disposal).ti,ab,kf. or reusable*.ti,ab,kf. or reuse*.ti,kf. or reusing.ti,kf. or "rising sea level*".ti,ab,kf. or "sea level ris*".ti,ab,kf. or smog.ti,ab,kf. or sustainab*.ti,kf. or (sustainab* adj3 (development* or cycle* or management or effect* or environment*)).ti,ab,kf. or (water adj3 (purificat* or sanitat* or treatment)).ti,ab,kf. or wastewater.ti,ab,kf. or (hydrogen adj3 moles adj3 equival*).ti,ab,kf. or "circular econom*".ti,ab,kf. or biodegradab*.ti,ab,kf. or ((ecological or environmental or water or energy or global or climat*) adj2 footprint*).ti,ab,kf. or (waste adj3 by product*).ti,ab,kf. or waste.ti,ab,kf. or wastes.ti,ab,kf. or reuse.ti,ab,kf. or reusab*.ti,ab,kf. or reprocess*.ti,ab,kf. or pollut*.ti,ab,kf. or (microplastic* and pollut*).ti,ab,kf. or greening.ti,ab,kf. or spillage.ti,ab,kf. or spoilage.ti,ab,kf. or salinization.ti,ab,kf. or "cradle to cradle".ti,ab,kf. or 'compostable plastic*'.ti,ab,kf. or desertification.ti,ab,kf. or deforestation.ti,ab,kf. or 'algal bloom*'.ti,ab,kf. or eco-friendly.ti,ab,kf. or ecofriendly.ti,ab,kf. or 'global change'.ti,ab,kf. or 'climate change'.ti,ab,kf. or "carbon neutral*".ti,ab,kf. or wastage*.ti,ab,kf. |
|
5 |
((1 and 2) or 3) and 4 |
|
6 |
limit 5 to yr="2000 -Current" |
|
7 |
6 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
|
8 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
|
9 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
|
10 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
|
11 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
|
12 |
7 and 8 – SR’s |
|
13 |
(7 and 9) not 12 – RCT’s |
|
14 |
(7 and (10 or 11)) not (12 or 13) – Observationeel |
|
15 |
7 not (12 or 13 or 14) – Overig |
|
16 |
12 or 13 or 14 or 15 |