Antibioticagebruik bij acute cholecystitis
Uitgangsvraag
Wat is het aanbevolen perioperatieve antibioticabeleid bij patiënten met acute cholecystitis?
Aanbeveling
Aanbeveling-1
Dien bij patiënten met acute cholecystitis zonder tekenen van sepsis die een laparoscopische cholecystectomie ondergaan géén routinematige perioperatieve antibiotica toe.
Aanbeveling-2
Beperk het gebruik van antibiotica tot patiënten met acute cholecystitis met tekenen van sepsis. Raadpleeg daarbij de richtlijn Sepsis. Kies het antibioticum conform lokaal beleid en richt het op zowel aërobe als anaërobe bacteriën.
Aanbeveling-3
Overweeg antibiotische behandeling in patiënten met acute cholecystitis die een percutane/EUS-geleide galblaasdrainage ondergaan, als onderdeel van de behandeling gericht op het beperken van ziekteduur en ontwikkeling van sepsis.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Er is literatuuronderzoek verricht naar het effect van antibiotica versus geen antibiotica in patiënten met acute cholecystitis.
Er werd een systematische review geïncludeerd met daarin studies waarin patiënten operatief werden behandeld. Voor de cruciale uitkomstmaat complicaties (postoperatieve infectieuze complicaties, postoperatieve niet-infectieuze complicaties en infectie van de operatiewond) werd geen klinisch relevant verschil gevonden tussen de groep patiënten die antibiotica kreeg en de groep patiënten die geen antibiotica kreeg. De bewijskracht voor deze cruciale uitkomstmaat was laag tot matig. Voor de belangrijke uitkomstmaat verblijfsduur in het ziekenhuis werd een klinisch relevant verschil gevonden in het voordeel van patiënten die geen antibiotica ontvingen. Ook voor deze uitkomstmaat was de bewijskracht matig.
Eén studie behandelde patiënten in eerste instantie conservatief. Voor de belangrijke uitkomstmaat operatie/drainage werd een klinisch relevant verschil gevonden in het voordeel van patiënten die geen antibiotica ontvingen. De bewijskracht voor deze uitkomstmaat was laag. In deze studie werd ook de cruciale uitkomstmaat complicaties (postoperatieve niet-infectieuze complicaties) gerapporteerd. Er werd een klinisch relevant verschil gevonden in het voordeel van de patiënten die werden behandeld met antibiotica. De bewijskracht van deze uitkomstmaat was laag. Voor de belangrijke uitkomstmaat verblijfsduur in het ziekenhuis werd geen verschil gevonden.
Er werden geen studies gevonden waarin patiënten werden behandeld met drainage.
De uitkomstmaat kwaliteit van leven werden niet gerapporteerd in de geïncludeerde studies.
Kwaliteit van bewijs
De overall kwaliteit van bewijs is laag. Dit betekent dat we onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege ernstige:
- Risk of Bias: methodologische beperkingen: onduidelijke randomisatie, gebrek aan blindering en selectie van gerapporteerde resultaten.
- Inconsistentie: inconsistentie van de resultaten.
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grens van klinische relevantie overschrijdt.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Voor patiënten met acute cholecystitis zijn het voorkómen van complicaties, de duur van ziekenhuisopname en het behoud van kwaliteit van leven belangrijke factoren in de behandelkeuze. Veel patiënten hechten waarde aan een snel herstel en zo min mogelijk invasieve ingrepen. Bij conservatieve behandeling speelt ook het risico op recidief een rol, dat met name in de eerste 1-2 jaar na behandeling verhoogd lijkt (20–40%). Intraveneus antibiotica verlengt de opname duur. De voorkeuren voor een behandeling kunnen sterk verschillen per patiënt en hangen onder meer af van de ernst van de cholecystitis, leeftijd, comorbiditeit, en persoonlijke omstandigheden.
Kostenaspecten
Op basis van één kosteneffectiviteit analyse (Satheeskaran, 2023), uitgevoerd als secundaire analyse van de PEANUTS-II trial, zijn er aanwijzingen dat het gebruik van antibiotica bij acute cholecystitis leidt tot beperkte kostenbesparing. In deze studie waren de gemiddelde zorgkosten per patiënt £4026,71 in de groep die antibiotica kreeg, tegenover £4070,31 in de placebogroep. Dit komt neer op een verschil van £43,59 per patiënt in het voordeel van de antibioticagroep. Deze kosten omvatten ziekenhuisopname, medicatie en nazorg.
Maatschappelijke kosten, zoals werkverzuim, zijn in deze studie niet meegenomen en blijven daarmee onzeker. Gezien het kleine verschil en de lage bewijskracht moet het kostenaspect met terughoudendheid worden geïnterpreteerd en vormt het geen doorslaggevend argument voor of tegen antibioticagebruik.
Gelijkheid ((health) equity/equitable)
Het wel of niet voorschrijven van antibiotica bij acute cholecystitis heeft naar verwachting geen invloed op gezondheidsongelijkheid. Antibiotica die worden voorgeschreven in de ziekenhuissetting vallen binnen het basispakket van de zorgverzekering en worden doorgaans volledig vergoed. Nederlandse patiënten hebben geen aanvullende verzekering of eigen bijdrage nodig om toegang te krijgen tot deze behandeling.
Ook zijn er geen bijzondere vaardigheden vereist van patiënten om antibiotica te kunnen gebruiken, aangezien het in de meeste gevallen gaat om intraveneuze toediening tijdens opname of kortdurend oraal gebruik na ontslag. De therapietrouw is in deze acute setting doorgaans hoog en er zijn geen aanwijzingen dat bepaalde patiëntgroepen (zoals laaggeletterden of mensen met beperkte gezondheidsvaardigheden) belemmeringen ondervinden.
Aanvaardbaarheid:
Ethische aanvaardbaarheid
Het gebruik van antibiotica bij acute cholecystitis is over het algemeen aanvaardbaar voor patiënten en zorgverleners. Antibiotica worden in de acute zorg breed toegepast en worden door patiënten doorgaans geaccepteerd als onderdeel van de behandeling, zeker wanneer het gaat om infectiepreventie of -bestrijding. Er zijn geen ethische bezwaren gerapporteerd met betrekking tot het al dan niet geven van antibiotica in deze context.
Wel is er bij terughoudend gebruik van antibiotica (bijvoorbeeld bij milde cholecystitis zonder aanwijzingen voor infectieuze complicaties) ruimte voor een terughoudend beleid. Vanuit het perspectief van antibioticaresistentie is het zorgvuldig en terughoudend voorschrijven van antibiotica maatschappelijk wenselijk. Het niet-routinematig voorschrijven van antibiotica in patiënten met de diagnose acute cholecystitis, waar dit klinisch niet noodzakelijk is, is verantwoord.
Duurzaamheid
Er is geen literatuur beschikbaar over de levenscyclusanalyse van antibiotica specifiek in het kader van gebruik bij acute cholecystitis. Het is algemeen bekend dat de productie, distributie en het gebruik van antibiotica bijdraagt aan milieuvervuiling, onder andere via uitstoot bij productieprocessen, reststoffen in afvalwater en bevordering van antimicrobiële resistentie in het milieu. Deze effecten zijn echter sterk afhankelijk van het soort antibioticum, de dosering, de duur van gebruik. Bij het afwegen van antibioticagebruik dient de mogelijke milieubelasting (nog) niet meegenomen te worden als bijkomend argument om gebruik te beperken.
Haalbaarheid
Het al dan niet voorschrijven van antibiotica bij patiënten met acute cholecystitis vereist geen aanpassing van de huidige praktijk. De aanbevelingen sluiten aan bij het bestaande beleid in veel Nederlandse ziekenhuizen, waarin bij milde tot matige acute cholecystitis routinematig gebruik van antibiotica steeds kritischer wordt beoordeeld.
Uit de geïncludeerde studies blijkt dat het achterwege laten van antibiotica bij een geselecteerde patiëntengroep (milde tot matige acute cholecystitis) veilig en effectief kan zijn. Deze strategie vereist geen aanpassing van infrastructuur of aanvullende financiële middelen, maar wel goede klinische beoordeling van de ernst van de cholecystitis.
Voor de conservatieve behandeling zonder antibiotica is de haalbaarheid eveneens hoog, mits er heldere protocollen zijn voor monitoring en eventuele opschaling naar het starten van antibiotica.
Rationale van aanbeveling-1: weging van argumenten voor en tegen de interventies
Er is geen klinisch relevant verschil aangetoond in postoperatieve complicaties of mortaliteit tussen wel of niet toedienen van antibiotica. De bewijskracht is laag, maar het beperken van antibioticagebruik verkort opname duur en vermindert resistentie.
Eindoordeel:
Sterke aanbeveling tegen (Niet doen).
Rationale van aanbeveling-2: weging van argumenten voor en tegen de interventies
Antibioticagebruik biedt bij milde vormen van cholecystitis geen aantoonbaar relevant voordeel en draagt mogelijk bij aan resistentie-ontwikkeling. Een terughoudend voorschrijfbeleid is gerechtvaardigd, mits klinisch verantwoord.
Eindoordeel:
Sterke aanbeveling tegen (Niet doen).
Rationale van aanbeveling-3: weging van argumenten voor en tegen de interventies
Alleen een selectieve, vaak kwetsbare groep komt in aanmerking voor drainage, doorgaans vanwege hoge operatieve risico’s of comorbiditeit. Er is geen directe evidence beschikbaar over antibioticagebruik in deze subgroep, waardoor de bewijskracht laag is. Vanuit klinisch perspectief lijkt het gerechtvaardigd, met als doel het ziektebeloop te bekorten, infectieuze complicaties te beperken en de kans op klinisch herstel te vergroten.
Eindoordeel:
Zwakke aanbeveling voor.
Onderbouwing
Treatment options for acute cholecystitis includes conservative treatment (with antibiotic support), cholecystectomy (acute or delayed) or (percutaneous/endoscopic) gallbladder drainage. There is variation in practice in antibiotic use in conservatively treated patients and in perioperative and peri-interventional use if patients undergo surgery or gallbladder drainage. This module provides guidance on the timing, type and duration of antibiotic use in patients with acute cholecystitis.
Summary of Findings
Population: Patients with acute cholecystitis
Intervention: Antibiotics
Comparator: No antibiotics
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
No antibiotics |
Antibiotics |
||||
|
Postoperative infectious complications
|
Relative risk: 0.84 (CI 95% 0.63 - 1.12) Risk difference: -0.01 Based on data from 1747 participants in 7 studies
|
108 per 1000 |
91 per 1000 |
Moderate Due to serious risk of bias1 |
Treatment with antibiotics likely results in little to no difference in postoperative infectious complications when compared with no antibiotics in patients with acute cholecystitis |
|
Difference: 17 fewer per 1000 (CI 95% 40 fewer - 13 more) |
|||||
|
Postoperative non-infectious complications
|
Relative risk: 0.84 (CI 95% 0.64 - 1.11) Risk difference: -0.02 (CI 95% -0.04 - 0.01) Based on data from 1741 participants in 7 studies
|
110 per 1000 |
91 per 1000 |
Low Due to serious risk of bias, Due to serious inconsistency2 |
Treatment with antibiotics may result in little to no difference in postoperative non-infectious complications when compared with no antibiotics in patients with acute cholecystitis. |
|
Difference: 19 fewer per 1000 (CI 95% 41 fewer - 11 more) |
|||||
|
Surgical site infection
|
Relative risk: 0.81 (CI 95% 0.53 - 1.22) Risk difference: -0.01 (CI 95% -0.04 – 0.02) Based on data from 1657 participants in 6 studies
|
84 per 1000 |
68 per 1000 |
Moderate Due to serious risk of bias, Due to serious imprecision3 |
Treatment with antibiotics likely results in little to no difference in surgical site infections when compared with no antibiotics in patients with acute cholecystitis. |
|
Difference: 16 fewer per 1000 (CI 95% 39 fewer - 18 more) |
|||||
|
Surgery
|
Relative risk: 1.38 (CI 95% 1.06 - 1.81) Risk difference: 0.24 (CI 95% 0.06 – 0.42) Based on data from 84 participants in 1 studies
|
619 per 1000 |
854 per 1000 |
Moderate Due to serious risk of bias4 |
Treatment with antibiotics likely results in an increase in surgery when compared with no antibiotics in patients with acute cholecystitis. |
|
Difference: 235 more per 1000 (CI 95% 37 more - 501 more) |
|||||
|
Drainage
|
Relative risk: 2.20 (CI 95% 0.84 - 5.78) Risk difference: 0.14 (CI 95% -0.02 to 0.31) Based on data from 84 participants in 1 studies
|
119 per 1000 |
262 per 1000 |
Very low Due to serious risk of bias, Due to very serious imprecision5 |
The evidence is very uncertain about the effect of treatment with antibiotics on drainage when compared with no antibiotics in patients with acute cholecystitis. |
|
Difference: 143 more per 1000 (CI 95% 19 fewer - 569 more) |
|||||
|
Length of hospital stay
|
Measured by: Scale: - Lower better Based on data from 1243 participants in 5 studies
|
Mean |
Mean |
Low Due to serious imprecision, Due to serious inconsistency6 |
Treatment with antibiotics may increase length of hospital stay when compared with no antibiotics in patients with acute cholecystitis |
|
Difference: MD 1.01 higher (CI 95% 0.28 lower - 2.30 higher) |
|||||
|
Quality of life
|
|
None of the studies reported the outcome measure quality of life. |
|
|
|
1. Risk of Bias: serious. Selective outcome reporting, Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias;
2. Risk of Bias: serious. Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias; Inconsistency: serious. Differences in reported results.
3. Risk of Bias: serious. Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias;
4. Risk of Bias: serious. Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias;
5. Risk of Bias: serious. Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias; Imprecision: very serious. Due to overlap of the 95% confidence interval with both limits of the MCID;
6. Inconsistency: serious. Point estimates vary widely; Imprecision: serious. Due to overlap of the 95% confidence interval with the upper limit of the MCID.
Description of studies
A total of three studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Elkasaby (2024) performed a systematic review and meta-analysis. PubMed, Embase, Cochrane CENTRAL, Web of Science, and Scopus were searched up to June 14, 2023. Randomized controlled trials that involved patients diagnosed with mild to moderate acute cholecystitis who were undergoing emergency cholecystectomy and were administered preoperative and/or postoperative antibiotics (compared to a control placebo group), reporting outcome measure postoperative infectious complications (PIC), were included in the analysis. In total, seven studies were included.
Satheeskaran (2023) performed a secondary cost-effectiveness analysis of the PEANUTS-II trial. The trial was a multicenter (five), randomized trial.
Mazeh (2012) performed a single-center, prospective randomized controlled trial to evaluate the role of intravenous antibiotic therapy in patients with mild acute calculus cholecystitis. Patients who were eighteen to 70 years old, and who met the following criteria were eligible for trial participation: sonographic findings of cholecystolithiasis or sludge, wall thickening of at least four mm, a positive sonographic Murphy sign, and epigastric or right upper quadrant pain, fever higher than 38 degrees Celsius, or a white blood cell count of more than 10.000 per mm3.
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
Included in systematic review Elkasaby, 2024 |
||||||
|
Braak, 2022 PEANUTS-II trial |
N at baseline Intervention: 226 Control: 231
Age (mean, SD) Intervention: 58.0 ± 13.9 years Control: 57.5 ± 14.6 years
Sex (female) Intervention: 119 (52.7%) Control: 114 (49.4%)
BMI (mean ± SD): Intervention: 28.8 ± 5.2 kg/m2 Control: 28.7 ± 5.1 kg/m2
Treatment: cholecystectomy |
Intervention: Antibiotics (IV), preoperative Control: Placebo |
30 days after cholecystectomy |
Postoperative infectious complications
Surgical site infection
Distant infections
Post-operative non-infectious complications
Mortality
Readmission
Length of hospital stay |
NR |
LOW |
|
Jaafar, 2020 |
N at baseline Intervention: 42 Control: 48
Age (mean, SD) Intervention: 48.5 ± 24 years Control: 49 ± 25 years
Sex (female) Intervention: 24 (57.1%) Control: 25 (52.1%)
BMI (mean ± SD): Intervention: 27 ± 7 kg/m2 Control: 28 ± 6 kg/m2
Treatment: cholecystectomy |
Intervention: Antibiotics (IV), preoperative Control: Placebo |
30 days postoperatively |
Postoperative infectious complications
|
NR |
Some concerns (selection of reported results) |
|
Park, 2023 |
N at baseline Intervention: 125 Control: 122
Age (mean, SD) Intervention: 51.6 ± 15.51 years Control: 52.4 ± 13.71 years
Sex (female) Intervention: 62 (49.6%) Control: 75 (61.5%)
BMI (mean ± SD): Intervention: 25 ± 3.47 kg/m2 Control: 24.5 ± 3.79 kg/m2
Treatment: cholecystectomy |
Intervention: Antibiotics (IV), preoperative Control: Placebo |
4 weeks postoperatively |
Postoperative infectious complications
Surgical site infection
Distant infections
Postoperative non-infectious complications
Mortality
Readmission
Length of hospital stay |
NR |
LOW |
|
Kim, 2017 |
N at baseline Intervention: 93 Control: 95
Age (mean, SD) Intervention: 52.1 ± 15.3 years Control: 52 ± 15 years
Sex (female) Intervention: 44 (47.31%) Control: 49 (51.58%)
BMI (mean ± SD): Intervention: 24.8 ± 3.4 kg/m2 Control: 25 ± 4 kg/m2
Treatment: cholecystectomy |
Intervention: Antibiotics (IV), postoperative Control: Placebo |
30 days postoperatively |
Postoperative infectious complications
Surgical site infection
Distant infections
Postoperative non-infectious complications
Mortality
Length of hospital stay |
NR |
LOW |
|
Loozen, 2017 |
N at baseline Intervention: 77 Control: 73
Age (median, IQR) Intervention: 52 (IQR 66) years Control: 54 (IQR 58) years
Sex (female) Intervention: 45 (58.4%) Control: 35 (48%)
BMI (mean ± SD): Intervention: NR Control: NR
Treatment: cholecystectomy |
Intervention: Antibiotics (IV), postoperative Control: Placebo |
30 days after cholecystectomy |
Postoperative infectious complications
Surgical site infection
Distant infections
Postoperative non-infectious complications
Mortality
Readmission
Length of hospital stay |
NR |
Some concerns (randomization process) |
|
Regimbeau, 2014 |
N at baseline Intervention: 207 Control: 207
Age (median, IQR) Intervention: 55 (IQR 75) years Control: 56 (IQR 74) years
Sex (female) Intervention: 107 (51.7%) Control: 103 (49.8%)
BMI (mean ± SD): Intervention: NR Control: NR
Treatment: cholecystectomy |
Intervention: Antibiotics (IV), postoperative Control: Placebo |
4 weeks postoperatively |
Postoperative infectious complications
Surgical site infection
Distant infections
Postoperative non-infectious complications
Mortality
Readmission
Length of hospital stay |
NR |
Some concerns (randomization process, deviations from intended interventions) |
|
Santibanes, 2018 |
N at baseline Intervention: 96 Control: 105
Age (mean, SD) Intervention: 49.9 ± 14.7 years Control: 49.9 ± 14.3 years
Sex (female) Intervention: 44 (45.8%) Control: 57 (54.3%)
BMI (mean ± SD): Intervention: 28.6 ± 5.2 kg/m2 Control: 28.2 ± 4.3 kg/m2
Treatment: cholecystectomy |
Intervention: Antibiotics (oral), postoperative Control: Placebo |
30 days postoperative |
Postoperative infectious complications
Surgical site infection
Distant infections
Postoperative non-infectious complications
Mortality
Readmission
Length of hospital stay |
NR |
LOW |
|
Individual studies |
||||||
|
Satheeskaran, 2023 (secondary analysis of PEANUTS-II trial) |
N at baseline Intervention: 226 Control: 231
Age (mean, SD) Intervention: 58.0 ± 13.9 years Control: 57.5 ± 14.6 years
Sex (female) Intervention: 119 (52.7%) Control: 114 (49.4%)
BMI (mean ± SD): Intervention: 28.8 ± 5.2 kg/m2 Control: 28.7 ± 5.1 kg/m2
Treatment: cholecystectomy |
Intervention: Antibiotics (IV), preoperative Control: Placebo |
30 days after cholecystectomy |
Cost-effectiveness |
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. No competing interests declared. |
LOW |
|
Mazeh, 2012 |
N at baseline Intervention: 42 Control: 42
Age (mean, SD) Intervention: 46.8 (range 25-65) years Control: 44.3 (range 22-69) years
Sex (male) Intervention: 24 (57%) Control: 22 (52%)
BMI (mean ± SD): NR
Treatment: elective cholecystectomy after 6-8 weeks, conservative at first |
Intervention: IV antibiotics Control: supportive treatment |
Mean follow-up 17.1 months (range 4-28 months) |
Surgery
Drain placement
Complications
Length of hospital stay |
NR |
Some concerns |
*For further details, see risk of bias table in the appendix
Results
Complications (critical)
One systematic review and one study reported the outcome measure complications (Elkasaby, 2024; Mazeh, 2012).
Operative treatment
Postoperative infectious complications
Elkasaby (2024) reported postoperative infections complications. In total, 78 of the 866 patients (9.0%) who received antibiotics had a postoperative infectious complication, compared with 95 of the 881 patients (10.8%) who received placebo (Figure 1). The risk ratio was 0.84 (95% CI 0.63 to 1.12), in favor of the patients who received antibiotics. The risk difference was -0.01 (95% CI -0.03 to 0.02), in favor of the patients who received antibiotics. This difference is not considered clinically relevant.
Preoperative antibiotics
In total, 31 of the 393 patients (7.9%) who received preoperative antibiotics had a postoperative infectious complication, compared with 46 of the 401 patients (11.5%) who received placebo (Figure 1). The risk ratio was 0.70 (95% CI 0.43 to 1.16), in favor of the patients who received preoperative antibiotics. The risk difference was -0.03 (95% CI -0.08 to 0.02), in favor of the patients who received preoperative antibiotics. This difference is not considered clinically relevant.
Postoperative antibiotics
In total, 47 of the 473 patients (9.9%) who received postoperative antibiotics had a postoperative infectious complication, compared with 49 of the 480 patients (10.2%) who received placebo (Figure 1). The risk ratio was 0.96 (95% CI 0.66 to 1.40), in favor of the patients who received postoperative antibiotics. The risk difference was 0.01 (95% CI -0.02 to 0.04), in favor of the patients who received placebo. This difference is not considered clinically relevant.
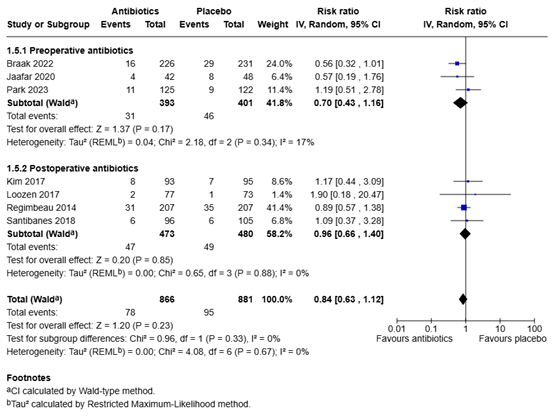
Figure 1. Postoperative infectious complications for antibiotics versus placebo in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Postoperative non-infectious complications
Elkasaby (2024) reported postoperative non-infections complications. In total, 78 of the 824 patients (9.5%) who received antibiotics had a postoperative non-infectious complication, compared with 94 of the 833 patients (11.3%) who received placebo (Figure 2). The risk ratio was 0.84 (95% CI 0.64 to 1.11), in favor of the patients who received antibiotics. The risk difference was -0.02 (95% CI -0.04 to 0.01), in favor of the patients who received antibiotics. This difference is not considered clinically relevant.
Preoperative antibiotics
In total, 57 of the 351 patients (16.2%) who received preoperative antibiotics had a postoperative non-infectious complication, compared with 68 of the 353 patients (19.3%) who received placebo (Figure 2). The risk ratio was 0.85 (95% CI 0.61 to 1.17), in favor of the patients who received preoperative antibiotics. The risk difference was -0.03 (95% CI -0.09 to 0.02), in favor of the patients who received preoperative antibiotics. This difference is not considered clinically relevant.
Postoperative antibiotics
In total, 21 of the 473 patients (4.4%) who received postoperative antibiotics had a postoperative non-infectious complication, compared with 26 of the 480 patients (5.4%) who received placebo (Figure 2). The risk ratio was 0.82 (95% CI 0.46 to 1.47), in favor of the patients who received postoperative antibiotics. The risk difference was -0.01 (95% CI -0.04 to 0.01), in favor of the patients who received postoperative antibiotics. This difference is not considered clinically relevant.
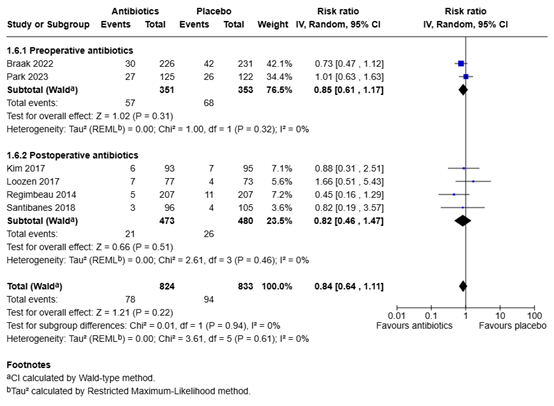
Figure 2. Postoperative infectious complications for antibiotics versus placebo in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Surgical site infection
Elkasaby (2024) reported surgical site infection. In total, 54 of the 824 patients (6.6%) who received antibiotics had a surgical site infection, compared with 70 of the 833 patients (8.4%) who received placebo (Figure 3). The risk ratio was 0.81 (95% CI 0.53 to 1.22), in favor of the patients who received antibiotics. The risk difference was -0.01 (95% CI -0.04 to 0.02), in favor of the patients who received antibiotics. This difference is not considered clinically relevant.
Preoperative antibiotics
In total, 22 of the 351 patients (6.3%) who received preoperative antibiotics had a surgical site infection, compared with 37 of the 353 patients (10.5%) who received placebo (Figure 3). The risk ratio was 0.66 (95% CI 0.27 to 1.59), in favor of the patients who received preoperative antibiotics. The risk difference was -0.03 (95% CI -0.11 to 0.04), in favor of the patients who received preoperative antibiotics. This difference is not considered clinically relevant.
Postoperative antibiotics
In total, 32 of the 473 patients (6.8%) who received postoperative antibiotics had a surgical site infection, compared with 33 of the 480 patients (6.9%) who received placebo (Figure 3). The risk ratio was 0.98 (95% CI 0.61 to 1.56), in favor of the patients who received postoperative antibiotics. The risk difference was 0.00 (95% CI -0.02 to 0.03). This difference is not considered clinically relevant.
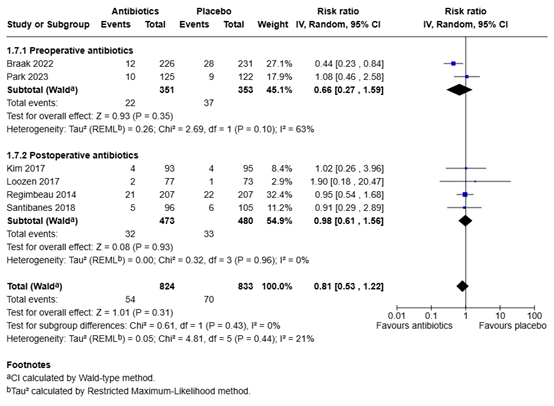
Figure 3. Surgical site infections for antibiotics versus placebo in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Conservative treatment
Mazeh (2012) reported postoperative non-infectious complications. In total, 0 of the 42 patients (0%) who received preoperative antibiotics had a postoperative non-infectious complication, compared with 2 of the 42 patients (4.8%) who received no antibiotics. The risk ratio was 0.20 (95% CI 0.01 to 4.04), in favor of the patients who received preoperative antibiotics. The risk difference was -0.05 (95% CI -0.12 to 0.03), in favor of the patients who received preoperative antibiotics. This difference is considered clinically relevant.
Length of hospital stay (important)
Operative treatment
One systematic review and one study reported the outcome measure length of hospital stay (Elkasaby, 2024; Mazeh, 2012). The mean difference in total length of hospital stay between the 617 patients who received antibiotics and the 626 patients who received placebo was 1.01 days (95% CI -0.28 to 2.30), in favor of the patients who received placebo (Figure 4). This difference is considered clinically relevant.
Preoperative antibiotics
The mean difference in total length of hospital stay between the 351 patients who received preoperative antibiotics and the 353 patients who received placebo was 3.67 days (95% CI -4.04 to 11.37), in favor of the patients who received placebo (Figure 4). This difference is considered clinically relevant.
Postoperative antibiotics
The mean difference in total length of hospital stay between the 266 patients who received postoperative antibiotics and the 273 patients who received placebo was 0.78 days (95% CI -0.45 to 2.01), in favor of the patients who received placebo (Figure 4). This difference is not considered clinically relevant.

Figure 4. Length of hospital stay for antibiotics versus placebo in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Conservative treatment
Mazeh (2012) reported length of hospital stay in days. Since a range was reported instead of the standard deviation, the results could not be pooled.
The patients who received antibiotics (n=42) had a mean length of hospital stay of 1.4 days (range 1 to 3 days), and the patients who received no antibiotics (n=42) had a mean length of hospital stay of 1.4 days (range 1 to 6 days). There was no difference in means between the two groups.
Surgery/drainage (important)
One study reported the outcome measure surgery/drainage (Mazeh, 2012).
Conservative treatment
Surgery
Mazeh (2012) reported the number of patients that underwent surgery. In total, 36 of the 42 patients (86%) who received antibiotics underwent surgery, compared with 26 of the 42 patients (62%) who received no antibiotics. The risk ratio was 1.38 (95% CI 1.06 to 1.81), in favor of the patients who received no antibiotics. The risk difference was 0.24 (95% CI 0.06 to 0.42), in favor of the patients who received no antibiotics. This difference is considered clinically relevant.
Drainage
Mazeh (2012) reported the number of patients that underwent drain placement. In total, 11 of the 42 patients (30%) who received antibiotics underwent drain placement, compared with 5 of the 42 patients (19%) who received no antibiotics. The risk ratio was 2.20 (95% CI 0.84 to 5.78), in favor of the patients who received no antibiotics. The risk difference was 0.14 (95% CI -0.02 to 0.31), in favor of the patients who received no antibiotics. This difference is considered clinically relevant.
Quality of life (important)
None of the studies reported the outcome measure quality of life.
A systematic review of the literature was performed to answer the following question(s):
What are the (un)favorable effects of the use of antibiotics in patients with acute cholecystitis?
Table 1. PICO
| Patients |
Patients with acute cholecystitis undergoing
|
| Intervention | Treatment with antibiotics |
| Control | No treatment with antibiotics |
| Outcomes | Percentage of interventions needed: surgery/drainage, length of hospital stay, complications (surgical), quality of life |
| Other selection criteria | Study design: systematic reviews and randomized controlled trials |
Relevant outcome measures
The guideline panel considered complications as a critical outcome measure for decision making; and length of hospital stay, surgery/drainage, and quality of life as an important outcome measure for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
The guideline panel defined the following as minimal clinically (patient) important differences:
- Complications (surgical): ARD 5%.
- (Total) Length of hospital stay: 1 day.
- Percentage of interventions needed: surgery/drainage: ARD 2%.
- Quality of life: 10% difference of the maximum score.
Search and select (Methods)
A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2000 to 18th of January 2025 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) acute cholecystitis; (2) antibiotics. Duplicates were removed using EndNote software. After deduplication a total of 860 records were imported for title/abstract screening. Initially, 26 studies were selected based on title and abstract screening. After reading the full text, 23 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and three studies were included.
- Elkasaby MH, Elsayed H, Charo DC, Rashed MA, Elkoumi O, Elhaddad IM, Gadallah A, Ramadan A. Antibiotic prophylaxis in emergency cholecystectomy for mild to moderate acute cholecystitis: a systematic review and meta-analysis of randomized controlled trials. Perioper Med (Lond). 2024 Aug 9;13(1):87. doi: 10.1186/s13741-024-00441-4. PMID: 39123238; PMCID: PMC11312388.
- Mazeh H, Mizrahi I, Dior U, Simanovsky N, Shapiro M, Freund HR, Eid A. Role of antibiotic therapy in mild acute calculus cholecystitis: a prospective randomized controlled trial. World J Surg. 2012 Aug;36(8):1750-9. doi:10.1007/s00268-012-1572-6. PMID:22456803.
- Satheeskaran M, Hussan A, Anto A, de Preux L. Cost-effectiveness analysis of antibiotic prophylaxis versus no antibiotic prophylaxis for acute cholecystectomy. BMJ Open Gastroenterol. 2023 Aug;10(1):e001162. doi:10.1136/bmjgast-2023-001162. PMID:37562856; PMCID: PMC10423775.
Risk of Bias tables
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Mazeh, 2012 |
Definitely yes
Reason: Randomization was stratified using a computerized random number generator list. |
Probably yes
Reason: Study number and group assignment were obtained by placing a telephone call to the study coordinator who was blinded to the patients details. |
Definitely no
Reason: After randomization, the patient and staff members were made aware of the assigned treatment group. |
Definitely yes
Reason: No loss-to-follow-up. |
Definitely yes
Reason: All relevant outcomes were reported. |
Definitely no
Reason: No patients with moderate or severe cholecystitis were included, decision for cholecystectomy tube were tailored to each patient’s status and depended on surgeon’s evaluation. |
Some concerns
|
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Bornscheuer T, Schmiedel S. Calculated Antibiosis of Acute Cholangitis and Cholecystitis. Viszeralmedizin. 2014 Oct;30(5):297-302. doi: 10.1159/000368335. Epub 2014 Oct 6. PMID: 26535043; PMCID: PMC4571718. |
Wrong study design: narrative review
|
|
Brazzelli M, Cruickshank M, Kilonzo M, Ahmed I, Stewart F, McNamee P, Elders A, Fraser C, Avenell A, Ramsay C. Clinical effectiveness and cost-effectiveness of cholecystectomy compared with observation/conservative management for preventing recurrent symptoms and complications in adults presenting with uncomplicated symptomatic gallstones or cholecystitis: a systematic review and economic evaluation. Health Technol Assess. 2014 Aug;18(55):1-101, v-vi. doi: 10.3310/hta18550. PMID: 25164349; PMCID: PMC4781329. |
Not conform PICO: wrong P: uncomplicated gallstones and cholecystitis, wrong comparison (surgical removal vs. conservative (possibly antibiotcis)
|
|
de Santibañes M, Glinka J, Pelegrini P, Alvarez FA, Elizondo C, Giunta D, Barcan L, Simoncini L, Dominguez NC, Ardiles V, Mazza O, Claria RS, de Santibañes E, Pekolj J. Extended antibiotic therapy versus placebo after laparoscopic cholecystectomy for mild and moderate acute calculous cholecystitis: A randomized double-blind clinical trial. Surgery. 2018 Mar 2:S0039-6060(18)30030-8. doi: 10.1016/j.surg.2018.01.014. Epub ahead of print. PMID: 29506881. |
Included in SR Elkasaby
|
|
Hajibandeh S, Popova P, Rehman S. Extended Postoperative Antibiotics Versus No Postoperative Antibiotics in Patients Undergoing Emergency Cholecystectomy for Acute Calculous Cholecystitis: A Systematic Review and Meta-Analysis. Surg Innov. 2019 Aug;26(4):485-496. doi: 10.1177/1553350619835347. Epub 2019 Mar 15. PMID: 30873901. |
Overlap met SR Elkasaby
|
|
Jaafar G, Sandblom G, Lundell L, Hammarqvist F. Antibiotic prophylaxis in acute cholecystectomy revisited: results of a double-blind randomised controlled trial. Langenbecks Arch Surg. 2020 Dec;405(8):1201-1207. doi: 10.1007/s00423-020-01977-x. Epub 2020 Aug 29. PMID: 32860109; PMCID: PMC7686002. |
Included in SR Elkasaby
|
|
Kim EY, Yoon YC, Choi HJ, Kim KH, Park JH, Hong TH. Is there a real role of postoperative antibiotic administration for mildmoderate acute cholecystitis? A prospective randomized controlled trial. J Hepatobiliary Pancreat Sci. 2017 Oct;24(10):550-558. doi: 10.1002/jhbp.495. Epub 2017 Sep 18. PMID: 28834296. |
Included in SR Elkasaby
|
|
Kivivuori A, Salminen P, Ukkonen M, Ilves I, Vihervaara H, Zalevskaja K, Pajari J, Paajanen H, Rantanen T. Laparoscopic cholecystectomy versus antibiotic therapy for acute cholecystitis in patients over 75 years: Randomized clinical trial and retrospective cohort study. Scand J Surg. 2023 Dec;112(4):219-226. doi: 10.1177/14574969231178650. Epub 2023 Aug 12. PMID: 37572012. |
Not conform PICO: wrong comparison (LC with preoperative IV cefuroxime + postoperative antibiotics for severe cases vs. IV cefuroxime + postoperative oral antibiotics)
|
|
La Regina D, Di Giuseppe M, Cafarotti S, Saporito A, Ceppi M, Mongelli F, Bihl F, Balzarotti Canger RC, Ferrario di Tor Vajana A. Antibiotic administration after cholecystectomy for acute mild-moderate cholecystitis: a PRISMA-compliant meta-analysis. Surg Endosc. 2019 Feb;33(2):377-383. doi: 10.1007/s00464-018-6498-0. Epub 2018 Oct 16. PMID: 30327917. |
Overlap met SR Elkasaby
|
|
Loozen CS, Kortram K, Kornmann VN, van Ramshorst B, Vlaminckx B, Knibbe CA, Kelder JC, Donkervoort SC, Nieuwenhuijzen GA, Ponten JE, van Geloven AA, van Duijvendijk P, Bos WJ, Besselink MG, Gouma DJ, van Santvoort HC, Boerma D. Randomized clinical trial of extended versus single-dose perioperative antibiotic prophylaxis for acute calculous cholecystitis. Br J Surg. 2017 Jan;104(2):e151-e157. doi: 10.1002/bjs.10406. PMID: 28121041. |
Included in SR Elkasaby
|
|
Loozen CS, Oor JE, van Ramshorst B, van Santvoort HC, Boerma D. Conservative treatment of acute cholecystitis: a systematic review and pooled analysis. Surg Endosc. 2017 Feb;31(2):504-515. doi: 10.1007/s00464-016-5011-x. Epub 2016 Jun 17. PMID: 27317033. |
Not conform PICO: no comparison in article (overlap met SR van Dijk, individuele studies geïncludeerd)
|
|
Matsui Y, Satoi S, Hirooka S, Kosaka H, Kawaura T, Kitawaki T. Reappraisal of previously reported meta-analyses on antibiotic prophylaxis for low-risk laparoscopic cholecystectomy: an overview of systematic reviews. BMJ Open. 2018 Mar 16;8(3):e016666. doi: 10.1136/bmjopen-2017-016666. PMID: 29549197; PMCID: PMC5857705. |
Not conform PICO: wrong P: patients undergoing low-risk laparoscopic cholecystectomies, no patients with acute cholecystitis
|
|
Park SE, Choi HJ, You YK, Hong TH. Clinical significance of preoperative antibiotic use in mild to moderate acute inflammatory gallbladder disease: A randomized controlled trial. J Hepatobiliary Pancreat Sci. 2023 Apr;30(4):482-492. doi: 10.1002/jhbp.1237. Epub 2022 Sep 15. PMID: 36050816. |
Included in SR Elkasaby
|
|
Pellegrini P, Campana JP, Dietrich A, Goransky J, Glinka J, Giunta D, Barcan L, Alvarez F, Mazza O, Sánchez Claria R, Palavecino M, Arbues G, Ardiles V, de Santibañes E, Pekolj J, de Santibañes M. Protocol for extended antibiotic therapy after laparoscopic cholecystectomy for acute calculous cholecystitis (Cholecystectomy Antibiotic Randomised Trial, CHART). BMJ Open. 2015 Nov 18;5(11):e009502. doi: 10.1136/bmjopen-2015-009502. PMID: 26582405; PMCID: PMC4654351. |
Protocol
|
|
Ramírez-Giraldo C, Van-Londoño I, Pesce A. Pre-operative antibiotics in patients with acute mild cholecystitis undergoing laparoscopic cholecystectomy: is it really useful? A systematic review. World J Emerg Surg. 2025 Jan 10;20(1):4. doi: 10.1186/s13017-025-00574-x. PMID: 39794804; PMCID: PMC11724567. |
Individual studies included in SR Elkasaby or included invidually (Mazeh)
|
|
Regimbeau JM, Fuks D, Pautrat K, Mauvais F, Haccart V, Msika S, Mathonnet M, Scotté M, Paquet JC, Vons C, Sielezneff I, Millat B, Chiche L, Dupont H, Duhaut P, Cossé C, Diouf M, Pocard M; FRENCH Study Group. Effect of postoperative antibiotic administration on postoperative infection following cholecystectomy for acute calculous cholecystitis: a randomized clinical trial. JAMA. 2014 Jul;312(2):145-54. doi: 10.1001/jama.2014.7586. PMID: 25005651. |
Included in SR Elkasaby
|
|
Sarkut P, Kilicturgay S, Aktas H, Ozen Y, Kaya E. Routine Use of Prophylactic Antibiotics during Laparoscopic Cholecystectomy Does Not Reduce the Risk of Surgical Site Infections. Surg Infect (Larchmt). 2017 Jul;18(5):603-609. doi: 10.1089/sur.2016.265. Epub 2017 Apr 4. PMID: 28375803. |
Not conform PICO: patients with gallstones (only a few patients with acute cholecystitis)
|
|
Singh A, Kaur M, Swaminathan C, Subramanian A, Singh KK, Sajid MS. Preoperative antibiotic prophylaxis in acute cholecystectomy: a systematic review and meta-analysis of randomised controlled trials. Transl Gastroenterol Hepatol. 2023 Oct 24;8:37. doi: 10.21037/tgh-23-48. PMID: 38021359; PMCID: PMC10643220. |
Overlap met SR Elkasaby
|
|
Sneider EB, Lewis J, Friedrich A, Baratta K, Whitman M, Li Y, Biswas M, Litwin DE, Cahan MA. Timing and choice of intervention influences outcome in acute cholecystitis: a prospective study. Surg Laparosc Endosc Percutan Tech. 2014 Oct;24(5):414-9. doi: 10.1097/SLE.0000000000000075. PMID: 25222712. |
Not conform PICO: wrong comparison (simple cholecystitis vs. complex cholecystitis)
|
|
Steinberg DI. In acute calculous cholecystitis, antibiotics after cholecystectomy did not reduce infection. Ann Intern Med. 2014 Dec 16;161(12):JC4. doi: 10.7326/0003-4819-161-12-201412160-02004. PMID: 25506876. |
No article available
|
|
Tazuma S, Igarashi Y, Inui K, Ohara H, Tsuyuguchi T, Ryozawa S; BTI Therapy Research Group. Clinical efficacy of i.v. doripenem, a new class of carbapenem, in patients with biliary tract infection: A multicenter trial. Hepatol Res. 2011 Apr;41(4):340-9. doi: 10.1111/j.1872-034X.2011.00783.x. PMID: 21426451. |
Not conform PICO: no comparison, all patients received antibiotics
|
|
van Braak WG, Ponten JEH, Loozen CS, Schots JPM, van Geloven AAW, Donkervoort SC, Nieuwenhuijzen GAP, Besselink MG, van Heek TNT, de Reuver PR, Vlaminckx B, Kelder JC, Knibbe CAJ, van Santvoort HC, Boerma D. Antibiotic prophylaxis for acute cholecystectomy: PEANUTS II multicentre randomized non-inferiority clinical trial. Br J Surg. 2022 Feb 24;109(3):267-273. doi: 10.1093/bjs/znab441. PMID: 35020797. |
Included in SR Elkasaby
|
|
van Dijk AH, de Reuver PR, Tasma TN, van Dieren S, Hugh TJ, Boermeester MA. Systematic review of antibiotic treatment for acute calculous cholecystitis. Br J Surg. 2016 Jun;103(7):797-811. doi: 10.1002/bjs.10146. Epub 2016 Mar 30. PMID: 27027851. |
Not conform PICO: no comparison (success rate of anitbiotics), one study with comparison, individually included. |
|
Weigand K, Köninger J, Encke J, Büchler MW, Stremmel W, Gutt CN. Acute cholecystitis - early laparoskopic surgery versus antibiotic therapy and delayed elective cholecystectomy: ACDC-study. Trials. 2007 Oct 4;8:29. doi: 10.1186/1745-6215-8-29. PMID: 17916243; PMCID: PMC2098782. |
Not conform PICO: wrong comparison (both groups received antibiotics)
|
Beoordelingsdatum en geldigheid
Publicatiedatum : 01-06-2026
Beoordeeld op geldigheid : 01-06-2026
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinair cluster ingesteld. Het cluster GE-chirurgie bestaat uit meerdere richtlijnen (zie hier de actuele clusterindeling). De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden brengen hun expertise in, indien nodig. De volgende personen uit het cluster zijn betrokken geweest bij de herziening van deze module:
Clusterstuurgroepleden
- Prof. dr. M.A. (Marja) Boermeester, voorzitter, chirurg (NVvH), Amsterdam UMC
- Dr. B.R. (Boudewijn) Toorenvliet, chirurg (NVvH), Ikazia, Rotterdam
- Dr. C.C. (Charles) van Rossem, chirurg (NVvH), Maasstad Ziekenhuis, Rotterdam
- Dr. I. (Ian) Faneyte, Chirurg (NVvH), ZGT, Almelo
- Prof. dr. M.W. (Markus) Hollmann, anesthesioloog (NVA), Amsterdam UMC
- Prof. dr. P.D. (Peter) Siersema, MDL-arts (NVMDL), Erasmus MC, Rotterdam
- Prof. dr. R.G.H. (Regina) Beets-Tan, radioloog (NVvR), Netherlands Cancer Insitute (NKI), Amsterdam
- Mevr. E.C. (Esen) Doganer, beleidsmedewerker, Stichting Kind & Ziekenhuis
Betrokken clusterexpertisegroepleden
- Dr. I. (Ian) Faneyte, chirurg (NVvH), ZGT, Almelo
- Dr. P. (Philip) de Reuver, chirurg (NVvH), Radboud UMC, Nijmegen
Met ondersteuning van
- Dr. M.S. (Matthijs) Ruiter, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. E.R.L. (Evie) Verweg, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- E. (Esther) van der Bijl, literatuurspecialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van de clusterleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Gemelde (neven)functies en belangen stuurgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen |
Overige belangen |
Datum |
Restrictie |
|
Boermeester |
Chirurg |
Medisch Ethische Commissie, Amsterdam UMC, locatie AMC |
Hieronder staan de beroepsmatige relaties met bedrijfsleven vermeld waarbij eventuele financiële belangen via de AMC Research B.V. lopen, dus institutionele en geen persoonlijke gelden zijn: |
Geen |
Institutionele grants van Solventum/3M, Johnson&Johnson
|
Ik maak me sterk voor een 100% evidence-based benadering van maken van aanbevelingen, volledig transparant en reproduceerbaar. Dat is mijn enige belang in deze; geen persoonlijk gewin.
|
Geen |
31-10-2024 |
Geen restricties |
|
Hollmann |
Afdelingshoofd Anesthesiologie Amsterdam UMC locatie AMC en afgevaardigde van NVA
|
Executive Section Editor Pharmacology Anesthesia & Analgesia |
Geen |
Geen |
ZonMw Doelmatigheid (onderzoeken hebben geen betrekking op het onderwerp GE-chirurgie, met name beademingsstudies) |
Geen |
Geen |
19-10-2022 |
Geen restricties |
|
Van Rossem |
Gastro-intestinaal chirurg, Maasstad Ziekenhuis Rotterdam |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
06-03-2021 |
Geen restricties |
|
Beets-Tan |
Hoofd Radiologie |
Scientific Director Eur Institute for Biomedical Research (onbetaald). Adviseur Eur Innovation Council |
Geen |
Geen |
Geen |
Geen |
Geen |
09-03-2021 |
Geen restricties |
|
Toorenvliet |
Chirurg, Maatschap Chirurgen en Plastisch Chirurgen Ikazia, Rotterdam |
Chirurg, Heelkunde instituut Nederland (betaald) |
Geen |
Geen |
Geen |
Geen |
Geen |
28-02-2021 |
Geen restricties |
|
Faneyte |
Chirurg Ziekenhuisgroep Twente (ZGT) / Chirurgen Cooperatie Oost-Nederland (ChirCON) |
Voorzitter ChirCON
|
Geen |
Geen |
Geen |
Geen |
Geen |
31-10-2024 |
Geen restricties |
|
Siersema |
Maag-Darm-Leverarts |
Editor in Chief Endoscopie betaald
|
Geen |
Geen |
FujiFilm, Pentax, Sanofi/Regeneron, Magentiq Eye
|
Geen |
Geen |
01-11-2024 |
Geen restricties |
|
Doganer |
Alle projecten van Rowy Uitzinger |
Stichting Kind en Ziekenhuis, Junior Projectmanager/beleidsmedewerker |
Geen |
Geen |
Geen |
Geen |
Geen |
16-06-2022 |
Geen restricties |
Gemelde (neven)functies en belangen expertisegroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen |
Overige belangen |
Datum |
Restrictie |
|
Faneyte |
Zie tabel 1 |
||||||||
|
De Reuver |
Chirurg, Radboud UMC |
Geen |
Geen |
Geen |
ZonMW, kosteneffectiviteit keuzehulpen bij oa galblaaschirurgie. MLDS, onderzoek naar verbeteren van zorg voor patienten met pijn in de bovenbuik |
Geen |
Geen |
22-09-2022 |
Geen restricties |
Inbreng patiëntenperspectief
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerden de clusterleden conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Antibioticagebruik bij acute cholecystitis |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: GE-chirurgie - Galsteenlijden - Module Antibioticagebruik bij acute cholecystitis |
|
|
Uitgangsvraag/modules: |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 18 januari 2025 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
Rayyan review: https://new.rayyan.ai/reviews/1293015/overview |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen acute cholecystitis EN antibiotics.
Het sleutelartikel wordt gevonden met deze search:
De volgende achtergrondartikelen worden gevonden met deze seach:
Het volgende achtergrondartikel valt uit op de I (antibiotics):
|
|
|
Te gebruiken voor richtlijntekst: A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2000 to 18th of Januari 2025 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) acute cholecystitis; (2) antibiotics. Duplicates were removed using EndNote software. After deduplication a total of 860 records were imported for title/abstract screening. |
|
Zoekopbrengst - 18 januari 2025
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
96 |
35 |
103 |
|
RCT |
267 |
52 |
274 |
|
Observationele studies |
446 |
148 |
483 |
|
Totaal |
809 |
235 |
860* |
*in Rayyan
Zoekstrategie - 18 januari 2025
Embase.com
|
No. |
Query |
Results |
|
#1 |
'acute cholecystitis'/exp OR (((acut* OR haemorrhag* OR hemorrhag*) NEAR/4 (cholecystit* OR colecystit* OR colecistit*)):ti,ab,kw) |
17023 |
|
#2 |
'antiinfective agent'/exp OR 'antibiotic agent'/exp OR 'antibiotic*':ti,ab,kw OR 'anti biotic*':ti,ab,kw |
5467978 |
|
#3 |
#1 AND #2 |
3242 |
|
#4 |
#3 AND [2000-2025]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
1895 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR 'systematic review'/exp OR 'systematic review (topic)'/exp OR 'scoping review'/exp OR 'rapid review'/exp OR 'umbrella review'/exp OR 'cochrane database of systematic reviews'/jt OR 'network meta-analysis'/exp OR 'networkmeta analy*':ti,ab,kw OR 'networkmetaanaly*':ti,ab,kw OR metaanaly*:ti,ab,kw OR 'meta analy*':ti,ab,kw OR metanaly*:ti,ab,kw OR prisma:ti,ab,kw OR prospero:ti,ab,kw OR metaanali*:ti,ab,kw OR 'meta anali*':ti,ab,kw OR metanali*:ti,ab,kw OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab,kw) OR (((structured OR systemic*) NEAR/3 (review* OR overview* OR synth*) NEAR/3 literature):ti,ab,kw) OR ((systemic* NEAR/1 review*):ti,ab,kw) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab,kw) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab,kw) OR (((literature NEAR/3 (review* OR overview*)):ti,ab,kw) AND (search*:ti,ab,kw OR database*:ti,ab,kw OR 'data base*':ti,ab,kw)) OR (('data extraction*':ti,ab,kw OR 'data source*':ti,ab,kw) AND ('study selection*':ti,ab,kw OR 'studies selection*':ti,ab,kw)) OR ('search strateg*':ti,ab,kw AND 'selection criteria*':ti,ab,kw) OR ('data source*':ti,ab,kw AND 'data synth*':ti,ab,kw) OR medline*:ti,ab,kw OR pubmed*:ti,ab,kw OR 'pub med*':ti,ab,kw OR embase:ti,ab,kw OR cochrane*:ti,ab,kw OR (((critical* OR rapid*) NEAR/2 (review* OR overview* OR synth*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synth*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynth*:ti,ab,kw OR 'meta synth*':ti,ab,kw OR 'review* of review*':ti,ab,kw |
1114430 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4189384 |
|
#7 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8605029 |
|
#8 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
15728549 |
|
#9 |
#4 AND #5 - SR |
96 |
|
#10 |
#4 AND #6 NOT #9 - RCT |
267 |
|
#11 |
#4 AND (#7 OR #8) NOT (#9 OR #10) - Observationeel |
446 |
|
#12 |
#9 OR #10 OR #11 - Totaal |
809 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Cholecystitis, Acute/ or ((acut* or haemorrhag* or hemorrhag*) adj4 (cholecystit* or colecystit* or colecistit*)).ti,ab,kf. |
10224 |
|
2 |
exp Anti-Bacterial Agents/ or exp Antibiotic Prophylaxis/ or antibiotic*.ti,ab,kf. or anti biotic*.ti,ab,kf. |
1074745 |
|
3 |
1 and 2 |
824 |
|
4 |
limit 3 to yr="2000 -Current" |
559 |
|
5 |
4 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
534 |
|
6 |
exp Meta-Analysis/ or exp "Meta-Analysis as Topic"/ or exp Network Meta-Analysis/ or exp Systematic Review/ or exp "Systematic Reviews as Topic"/ or (networkmeta analy* or networkmetaanaly* or metaanaly* or meta analy* or metanaly* or prisma or prospero or metaanali* or meta anali* or metanali*).ti,ab,kf. or ((systemati* or scoping or umbrella or structured literature) adj3 (review* or overview*)).ti,ab,kf. or ((structured or systemic*) adj3 (review* or overview* or synth*) adj3 literature).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 (review* or overview*)) and (search* or database* or data base*)).ti,ab,kf. or ((data extraction* or data source*) and (study selection* or studies selection*)).ti,ab,kf. or (search strateg* and selection criteria*).ti,ab,kf. or (data source* and data synth*).ti,ab,kf. or (medline* or pubmed* or pub med* or embase or cochrane*).ti,ab,kf. or cochrane.jw. or ((critical* or rapid*) adj2 (review* or overview* or synth*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synth*)) and (search* or database* or data base*)).ab. or metasynth*.ti,ab,kf. or meta synth*.ti,ab,kf. |
806871 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2832573 |
|
8 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4935535 |
|
9 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5884618 |
|
10 |
5 and 6 - SR |
35 |
|
11 |
(5 and 7) not 10 - RCT |
52 |
|
12 |
(5 and (8 or 9)) not (10 or 11) - Observationeel |
148 |
|
13 |
10 or 11 or 12 - Totaal |
235 |