Audiologische zorg bij unilaterale verliezen
Uitgangsvraag
Welke audiologische zorg (monitoring, technische revalidatie, vroegbehandeling) is geïndiceerd bij kinderen van 0-4 jaar met een unilateraal gehoorverlies?
Aanbeveling
Aanbeveling-1
Bepaal de keuze voor behandeling met een hoortoestel van kinderen met een blijvend unilateraal gehoorverlies in nauwe samenspraak met ouders/verzorgers:
- Bespreek dat kinderen met licht (20-35 dB) tot matig-ernstig (<65 dB gemiddeld bij .5-1-2-4 kHz) unilateraal gehoorverlies met een hoortoestel aantoonbaar een hogere kwaliteit van leven ervaren, en betere auditieve uitkomsten behalen.
- Bespreek de voor- en nadelen van een proef met een hoortoestel (of BCD bij atresie/microtie conform de Richtlijn BCD bij unilaterale geleidingsverliezen), bepaal samen op welk moment de kans op acceptatie van een hoortoestel het grootst is, en bepaal samen behandeldoelen.
- Als ouders/verzorgers kiezen voor een hoortoestel: start een hoortoestelproef en evalueer periodiek (na afloop van de proef en daarna minimaal jaarlijks, overweeg een herhaaltermijn van 6 maanden) of de behandeldoelen worden behaald.
- Als ouders/verzorgers vooralsnog niet kiezen voor een proef met hoortoestel: evalueer de behandeldoelen periodiek (minimaal jaarlijks, overweeg een herhaaltermijn van 6 maanden).
Monitor daarnaast de ontwikkeling op verschillende domeinen:
- Monitor de auditieve ontwikkeling zoals beschreven in module Monitoring van auditieve ontwikkeling.
- Monitor de spraaktaalontwikkeling zoals beschreven in module Monitoring van algehele en spraaktaalontwikkeling.
- Monitor de sociaal-emotionele lontwikkeling zoals beschreven in module Monitoring van algehele en spraaktaalontwikkeling.
- Monitor de non-verbale cognitieve ontwikkeling zoals beschreven in module Monitoring van algehele en spraaktaalontwikkeling.
Aanbeveling-2
Raad een interventie met een hoortoestel af als het aangedane oor een (zeer) ernstig gehoorverlies heeft of doof is.
- Bespreek dat kinderen met (zeer) ernstig (>65 dB gemiddeld bij .5-1-2-4 kHz) dB) unilateraal gehoorverlies geen bewezen baat hebben bij een hoortoestel, CROS of BCD.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
De meeste observationele studies suggereren een klinisch relevante verbetering in kwaliteit van leven, spraakperceptie, auditieve ontwikkeling en auditieve discriminatie met een hoortoestel bij jonge kinderen met unilateraal gehoorverlies.
Er waren geen studies die een positief effect van een CROS (Contraleral Routing of the Signal) - hoortoestel lieten zien. Ook vonden we geen studies over de inzet van FM-apparatuur bij de doelgroep 0-4 jaar.
Twee studies (Kenworthy, 1990, en Updike 1994) toonden tegengestelde resultaten (betere auditieve discriminatie bij geen gebruik van een hoortoestel in vergelijking met geen interventie of FM-systeem), waarvan de inconsistente resultaten konden worden verklaard door het gebruik van oudere (niet meer in gebruik zijnde) analoge hoortoestellen, geen gewenningsperiode en grote gehoorverliezen. Aangezien de inconsistente resultaten van Kenworthy (1990) en Updike (1994) konden worden verklaard, werd de GRADE voor de uitkomst auditieve discriminatie niet verder verlaagd. De meer recente gerandomiseerde studie van Benchetrit (2022) bevestigde een verbetering van de meeste van deze uitkomsten (auteurs gebruikten een gecombineerd eindpunt van onderzoeken naar kwaliteit van leven en luisterproblemen of uitdagingen met gehoorversterking). Hoewel uitkomsteffecten in de meeste onderzoeken klinisch relevant waren, hebben we de GRADE niet verder verhoogd, aangezien de totale steekproefomvang klein bleef, waardoor verschillende soorten, gradaties en configuraties van unilateraal gehoorverlies niet konden worden bestudeerd.
Er lijkt geen probleem van een placebo-effect te zijn omdat de effecten zeer groot zijn waardoor een uitkomst ten gevolge van een placebo-effect onwaarschijnlijk lijkt. Wel zijn de resultaten merendeels afkomstig van kinderen >4 jaar met unilateraal gehoorverlies. Ofschoon deze studieresultaten strikt genomen niet binnen de PICO vallen, zijn ze toch meegenomen omdat we verwachten dat de uitkomsten bij 0-4 jaar hetzelfde zijn. De reden waarom er zo weinig studies in de leeftijd van 0-4 jaar keken is onbekend, maar kan te maken hebben met dat het soort instrumenten om de uitkomst te evalueren makkelijker zijn af te nemen bij oudere kinderen.
Het effect van de leeftijd ten tijde van de start van de interventie blijft onduidelijk (de literatuursamenvatting gaf hier geen antwoord op) en valt daarom buiten de scope van de uitkomsten van de zoekvraag. Aan de ene kant verwacht je een positief effect op de ontwikkeling van zo vroeg mogelijk starten met een interventie (net als bij kinderen met een bilateraal gehoorverlies). Het effect van een unilateraal gehoorverlies is echter wat anders, en een hoortoestel heeft als doel het optimaal herstel van binaurale functies (naast detectie van geluid aan de aangedane zijde). Van wisselende middenoorproblemen is bekend dat dit een negatief effect heeft op de ontwikkeling van de binaurale functies, dat pleit voor een vroeg herstel van de binaurale functies. Aan de andere kant vergt het wel direct een inspanning van ouders om de interventie te laten accepteren terwijl de uitkomsten pas later in de ontwikkeling te evalueren zijn.
Deze opmerkingen in beschouwing nemende is de reden waarom de GRADE voor de uitkomsten kwaliteit van leven, spraakperceptie, auditieve ontwikkeling en auditieve discriminatie met een hoortoestel bij kinderen met unilateraal gehoorverlies neerkomen op zeer laag.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Doel van de interventie is om voor de patiënt de gevolgen van het gehoorverlies waar mogelijk te beperken.
De verwachte voordelen zijn een verbetering in spraakverstaan, hoorontwikkeling, auditieve discriminatie en kwaliteit van leven.
Nadelen zijn praktisch van aard (het kost veel moeite om een jong kind een hoortoestel consequent te laten dragen). Ook kan het bij zeer jonge kinderen moeilijk zijn om de meerwaarde van interventie vast te stellen. Ouders kunnen geen hoortoestel willen of terughoudendheid hebben bij jonge leeftijd. De motivatie kan ontbreken daar ze nu geen problemen zien of daar ze (zelf/in de familie) ervaring hebben met eenorigheid, waarmee ze enerzijds de uitdagingen goed kennen, maar ook de resultaten kennen zonder interventie en dat mogelijk verkiezen. Verder kan voor kinderen met bredere ontwikkelingsproblematiek gelden dat kwaliteit van leven in mindere mate samenhangt met spraakverstaan, hoorontwikkeling, en auditieve discriminatie.
Kosten (middelenbeslag)
In de analyse zijn geen kosteneffectiviteitsstudies meegenomen. De kosteneffectiviteit is moeilijk te bepalen. Een hoortoestel bij deze doelgroep valt echter al binnen de basiszorgverzekering, de kosten zijn beperkt en moeten worden afgezet tegen een winst op lange termijn: betere kwaliteit van leven en beter auditief functioneren.
Aanvaardbaarheid, haalbaarheid en implementatie
Een hoortoestel bij kinderen met unilateraal verlies gaat om een reeds bestaande interventie die bij jonge kinderen met een bilateraal gehoorverlies routinematig wordt ingezet. De interventie is veelal verzekerde zorg en wordt ouders optioneel aangeboden. Bij motivatie is dit praktisch zeker haalbaar.
Belemmerend bij de implementatie is dat de meerwaarde op individueel niveau van deze interventie op zeer jonge leeftijd lastig is vast te stellen met meetinstrumenten. Daarnaast is de indicatie voor vroegbehandeling (die een proef met hoortoestel op jonge leeftijd zouden kunnen begeleiden) nog niet afgestemd op kinderen met een unilateraal gehoorverlies. Bij kinderen met een bilateraal gehoorverlies is dit standaard zorg. De indicatie voor vroegbehandeling zou naar onze mening moeten worden verruimd om de interventie met een hoortoestel te begeleiden bij kinderen van 0-4 jaar met een unilateraal gehoorverlies.
Al met al is een hoortoestel bij kinderen met unilateraal verlies een aanvaardbare en haalbare interventie.
Rationale van aanbeveling-1
Voor een interventie met hoortoestelrevalidatie pleit dat op groepsniveau is beschreven dat kinderen met licht (20-35 dB) tot matig-ernstig (<65 dB gemiddeld bij .5-1-2-4 kHz) unilateraal gehoorverlies met een hoortoestel een hogere kwaliteit van leven ervaren, en betere auditieve uitkomsten behalen. Het ligt voor de hand dat dit de ontwikkeling van een jong kind met unilateraal gehoorverlies ten goede kan komen.
De nadelen van deze interventie zijn vooral praktisch van aard: het vereist inspanning en volharding om bij een jong kind te komen tot acceptatie en consistent gebruik van een hoortoestel. Ook is het effect van deze interventie lastig meetbaar te maken op jonge leeftijd, wat ten koste kan gaan van de motivatie bij ouders.
Als laatste is het niet zo, dat ouders direct een probleem observeren, en soms ook, gekoppeld daaraan niet zelf directe revalidatiedoelen hebben gesteld.
Omdat uit de literatuur nu geen sterke aanknopingspunten komen over het effect van de leeftijd bij start interventie, vereist de startleeftijd een gezamenlijke en gemotiveerde beslissing met ouders. De werkgroep acht het aanbieden van vroegbehandeling daarbij als standaard zorg op zijn plaats.
Ondanks de lage tot zeer lage bewijskracht van de GRADE is onze aanbeveling sterk geformuleerd omdat de studies een verbetering in kwaliteit van leven, spraakperceptie, auditieve ontwikkeling en auditieve discriminatie met een hoortoestel bij jongere kinderen met unilateraal gehoorverlies lieten zien.
Onafhankelijk van of wordt gestart met hoorrevalidatie adviseren we het kind te volgen in de ontwikkeling.
Rationale van aanbeveling-2: indien het aangedane oor een (zeer) ernstig gehoorverlies heeft of doof is
Voor deze groep is niet beschreven dat een interventie met hoortoestel, CROS of BCD een positief effect heeft. De nadelen blijven wel staan en zijn vooral praktisch van aard: het vereist soms inspanning en volharding om bij een jong kind te komen tot acceptatie en consistent gebruik van een hoortoestel. Dit is mogelijk belastend voor zowel ouders als het kind. Ook is het effect van deze interventie lastig meetbaar te maken op jonge leeftijd.
N.B.1 Deze afweging kan op latere leeftijd, als het kind zelf kan aangeven welke problemen het ervaart, opnieuw worden gemaakt. Zie hiervoor module Hoorzorg voor kinderen met een eenzijdig blijvend gehoorverlies van de Richtlijn Audiologische zorg 4-18 jaar.
N.B.2 Een interventie met een cochleair implantaat bij deze doelgroep wordt sinds kort in België wél toegepast, op basis van de uitkomsten van verschillende wetenschappelijke studies. Dit ligt buiten de scope van deze richtlijn, en valt binnen de veldnorm cochleaire implantatie in Nederland van het CI-ON.
Onderbouwing
Achtergrond
Jaarlijks worden vanuit de Neonatale Gehoorscreening in Nederland ca. 80 neonaten gediagnosticeerd met een unilateraal gehoorverlies. De huidige standaardzorg bestaat uit een aanbod van onderzoek naar de oorzaak van het gehoorverlies, en een periodieke audiologische controle. Het risico op verder progressief gehoorverlies (aan het slechte en/of goede oor), en problemen in de ontwikkeling is verhoogd bij deze groep (Bell, 2022; Fitzpatrick, 2023). Er is in het werkveld echter geen consensus over welke audiologische zorg (informatie, advies, monitoring, evt. revalidatie) deze populatie moet krijgen. Er is praktijkvariatie in informatievoorziening, advies, monitoring en de inzet van hoorrevalidatie bij kinderen met een unilateraal gehoorverlies. Deze zoekvraag moet leiden tot consensus over het te volgen beleid bij deze groep.
Conclusies / Summary of Findings
Quality of life (crucial outcome)
|
Low GRADE |
A hearing aid may result in a large increase in quality of life as compared with baseline accommodations alone
Briggs (2011), Benchetrit (2022) |
Auditory development (crucial outcome)
|
Very Low GRADE |
A hearing aid may increase auditory development but the evidence is very uncertain
Cywka (2021) |
Speech perception (crucial outcome)
|
Very Low GRADE |
A hearing aid may increase speech perception but the evidence is very uncertain
Briggs (2011) |
Auditory discrimination (crucial outcome)
|
Very Low GRADE |
A hearing aid may increase auditory discrimination as compared with baseline accommodations (i.e., watchful waiting) alone but the evidence is very uncertain
Briggs (2011), , Kenworthy (1990), Updike (1994) |
Language (crucial outcome)
|
- GRADE |
Due to the lack of data, it is not possible to draw a conclusion about the effect of a hearing aid as compared with baseline accommodations alone on language |
Hearing attention (crucial outcome)
|
- GRADE |
Due to the lack of data, it is not possible to draw a conclusion about the effect of a hearing aid as compared with baseline accommodations alone on hearing attention |
Outcomes related to the exposure of family centered early intervention
|
- GRADE |
Due to the lack of data, it is not possible to draw a conclusion about the effect of family centered early intervention as compared with baseline accommodations alone on hearing attention |
Samenvatting literatuur
Abbreviations used in the summary of literature
AC: Air conduction
BC: Bone conduction
BKB SIN: Bamford-Kowal-Bench Speech-in-Noise-Test
dB: Decibel
GFWTAD: Goldman-Frostoe-Woodcock test of Auditory Discriminatipn
HA: Hearing aide
NST: Nonsense Syllable Test
MD: Monaural direct
MI: Monaural indirect
MS/ON: Midline signal/omnidirectional noise
PICO: Patient, Intervention, Comparison, Outcome
SD: standard deviation
SNR: Single Number Rating
SPL: Sound Pressure Level
QoL: Quality of life
UHL: Unilateral hearing loss
One systematic review of observational studies (Appachi 2017) and 6 extra results from observational studies that were not included in the systematic review of Appachi, 2017 (i.e., Alexander 2021, Bagatto 2019, Bakkum 2023, Cywka 2021, Fitzpatrick 2019, Fitzpatrick,1 2019, Priwin 2007) and one clinical trial (Benchetrit 2022) were included by the reviewers. After reading the full text, the following studies were excluded as they were not part of the PICO: Alexander 2021 (no outcomes reported that were part of the PICO), Bagatto 2019 (narrative review based on expert opinion, no comparison), Fitzpatrick 2019 (qualitative analysis, no comparison), Fitzpatrick1 2019 (wrong comparator group; i.e., patients with bilateral hearing loss), Priwin 2007 (wrong outcome).
Three of the five studies of patients with unilateral hearing loss (UHL) who received a non-surgical hearing aid and that were included in the systematic review of Appachi (2017); i.e. Briggs 2011, Kenworthy 1990, Updike 1994 were also included in the present review, while Johnstone 2010 was excluded (wrong outcome). The other 7 studies included by Appachi 2017 did not fit the PICO (i.e., were patients with UHL who received a cochlear implant) and were therefore excluded.
Considering that confounding can play a role (i.e. bias) in observational studies where patients with aided UHL are compared with patients with unaided UHL, we decided to exclude observational studies that did not take confounding into account; either by statistical control, or by comparing patients with themselves (controlled before-and-after study; Suissa 1995). The following study was excluded for this reason: Bakkum 2023.
The following 5 studies were included for analysis:
Benchetrit 2022 (randomized crossover trial),
Briggs 2011 (controlled before-and-after study),
Cywka 2021 (controlled before-and-after study),
Kenworthy 1990 (controlled before-and-after study),
Updike 1994 (controlled before-and-after study).
Indirectness
Please note that the clinical trial of Benchetrit (2022) included patients aged 6-12 years with UHL, which does not fit the P of the PICO, but was still included as it was deemed unlikely by the working group that results would not be applicable for 0–4-year-old patients with UHL (this relates to indirectness, see Guyatt 2011). For similar reasons the controlled before-and-after studies of Briggs (2011), Kenworthy (1990), and Updike (1994) were included even though these studies included patients with UHL that were aged 7-12 years, 8-12 years, 8-12 years, respectively.
Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
Results
Outcome definitions
The trial of Benchetrit (2022) and the observational study of Briggs (2011) reported on quality of life (QOL)
The observational studies of Cywka (2021) reported on auditory development
The observational study of Briggs (2011) reported on speech perception
The observational studies of Briggs (2011), Kenworthy (1990), Updike (1994) reported on auditory discrimination
Definitions QOL:
Benchetrit (2022): An integrated outcome of the Hearing Environments and Reflection on Quality of Life (HEAR-QL), Children’s Home Inventory for Listening Difficulties (CHILD (child)), and Listening Inventory For Education-Revised (LIFE-R) Student and the LIFE-R Teacher surveys (primary outcome). Survey score analyses were averaged for each survey individually as well as for the integrated five surveys per treatment arm and timepoint. All individual scores were standardized on a scale of 0 to 100, with 0 indicating the worse outcomes and 100 indicating the best outcomes. Following standardization, all survey scores were combined by mean averaging.
Briggs (2011): The HEAR-QL (completed by the child) that measures how hearing loss affects the child’s QOL in three areas: environment, activities, and feelings.
Definitions auditory development:
Cywka (2021): Auditory development was assessed twice using the LittlEARS questionnaire– before and after use of the hearing aids.
Definitions of speech perception:
Briggs (2011): Subjective measures, completed by the child, included the CHILD (Children’s Home Inventory of Listening Difficulties), LIFE Student (Learning Inventory for Education). Teacher subjective measures included the LIFE Teacher and the SIFTER (Screening Instrument for Targeting Educational Risk). The parent subjective measure used was the CHILD Parent.
Definitions of auditory discrimination:
Briggs (2011): Bamford-Kowal-Bench Speech-in-Noise-Test.
(BKB-SIN) and the Nonsense Syllable Test (NST).
Kenworthy (1990): Bamford-Kowal-Bench Speech-in-Noise-Test.
(BKB-SIN) and the Nonsense Syllable Test (NST). NST and BKB-SIN were tested under three listening
conditions encountered in a classroom [monaural direct (MD), monaural indirect (MI), midline signal/omnidirectional noise (MS/ON)].
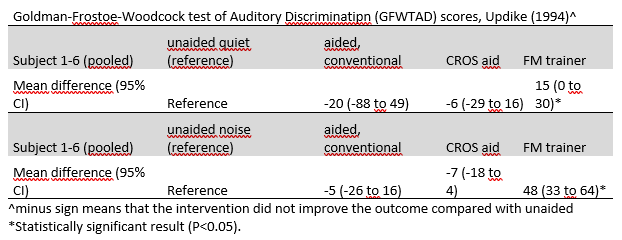
Updike (1994): The Goldman-Frostoe-Woodcock test of Auditory Discriminatipn (GFWTAD) under two listening conditions: in the absence of background noise and in a noise subtest.
Study characteristics
In the pooled data (of 5 studies in total), 76 participants with UHL were included. One study included children aged < 4 years: 21 participants (27%). The remaining 4 studies included children aged > 4 years (range 6-12 years). There were 3 studies that had a follow-up of 12-26 weeks, while the other 2 studies compared a hearing aid intervention to control on the same study day. Due to heterogeneity between exposures-, outcome definitions and populations it was decided to not pool the results.
1. Quality of life (crucial outcome)
Benchetrit (2022): Survey scores were higher with HA than during the baseline-only interval (P = .036). favouring the HA intervention over the control. SD or 95% CIs were not provided. Benchetrit (2022) defined a minimal clinically important difference as a ≥10% score improvement. In arm 1, 35% and in arm 2 41% of patients experienced a clinically meaningful score improvement during the HA intervals.
Briggs (2011): Survey scores were higher with HA than during the baseline-only interval (mean difference
20.1; 95%CI, 7.8 to 32.3), favouring the HA intervention over the control, with a 95% confident interval that exceeded the threshold of clinical relevance (0.5SD)
2. Auditory development (crucial outcome)
Cywka (2021): The LittlEARS survey score was 5.91 (95% CI, 1.27 to 10.55) points higher for the HA period, favoring the HA intervention over the control. The hearing age was 5.62 (95% CI, 2.47 to 8.77) months older for the HA period, favoring the HA intervention over the control. The point estimates exceeded the threshold of clinical relevance (0.5SD), but the 95% confidence intervals did not exceed the threshold of clinical relevance.
3. Speech (perception) (crucial outcome)
Briggs (2011): The LIFE Teacher, revealed that half of the subjects’ teachers found hearing aid use to be beneficial or highly beneficial. Three of the subjects’ teachers reported no change, none reported a negative change, and one subject’s questionnaire was not returned. The SIFTER results showed no significant change in average scores with the hearing aid.
Mean differences post-hearing aid scores were for
Child CHILD, 1.25 (95% CI, 0.53 to 1.97)
Parent CHILD, 1.18 (95% CI, 0.25 to 2.11)
Student LIFE Classroom Listening, 16.2 (95%CI, 1.18 to 31.2)
Student LIFE Additional Situations, 20.7 (95% CI, 10.4-31.0), all favoring the HA intervention over the control with 95% confidents intervals exceeding the thresholds of clinical relevance (0.5SD).
4. Auditory discrimination (crucial outcome)
Briggs (2011): Inspection of individual cases revealed that six of the eight children showed an
improvement in scores (i.e. lower SNR-50) on both the BKB-SIN MD and MI conditions
that ranged from 0.75 to 2.3 dB and 0.5 to 4.5 dB, respectively, i.e. favoring the HA intervention over the control.
Kenworthy (1990): The FM system was the only audiological recommendation to produce uniformly high speech recognition scores across all listening conditions with both types of speech materials, with point estimates, but not 95% confidence intervals, exceeding the thresholds of clinical relevance (0.5SD), i.e., favoring the control intervention over the HA.
Nonsense syllable test (NST) mean differences post-hearing aid scores as compared with unaided were
-25.3% (95%CI -37 to -13) for monoaural direct (MD)
34.8% (95%CI -22.6 to 47) for monoaural indirect (MI)
-10.8% (95CI -21 to -1.0) for midline signal/omnidirectional noise (MS/ON)
(minus sign means that the control intervention is favored over the HA)
NST mean differences post-hearing aid scores as compared with FM systems were
-32% (95%CI -40 to -24) for MD
-32% (95%CI -40 to -24) for MI
-23% (95CI -30 to -15) for MS/ON
(minus sign means that the control intervention is favored over the HA)
Bamford-Kowal-Bench Speech-in-Noise-Test (BKB-SIN) mean differences post-hearing aid scores as compared with unaided were
-49.6% (95%CI -75 to -24) for MD
61% (95%CI 47 to 74) for MI
-8% (95CI -19 to 3) for MS/ON
(minus sign means that the control intervention is favored over the HA)
BKB mean differences post-hearing aid scores as compared with FM systems were
-43% (95%CI -69 to -16) for MD
1% (95%CI -7 to -9) for MI
-23% (95CI -30 to -15) for MS/ON
(minus sign means that the control intervention is favored over the FM HA)
Updike (1994): Results were provided on a case-to-case basis. As shown in the table below, with the FM trainer, word recognition improved with point estimates, and 95% confidence intervals (for noise, but not for quiet), exceeding the threshold of clinical relevance (0.5SD), i.e., favoring the FM intervention over the control (no intervention). Word recognition in conventional hearing aids and CROS were diminished as compared to unaided, both in noise and quiet, but not exceeding the threshold of clinical relevance (0.5SD).
Level of evidence of the literature
Summary
The level of evidence (GRADE method) is determined per comparison and outcome measure and is based on results from 6 observational studies and starts at level “low”. Subsequently, the level of evidence was downgraded if there were relevant shortcomings in one of the several GRADE domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. We did not GRADE the Benchetrit (2022) trial, but used its results as external validation of the observational studies. Observational data evaluating hearing amplification in children with UHL were limited to 36 participants in total. Most observational studies do suggest a clinically relevant improvement in speech perception, auditory development, and auditory discrimination with a hearing aid. Two studies (Kenworthy, 1990, and Updike 1994) showed opposite results (better auditory discrimination when not using a hearing aid as compared with no intervention or FM system). These inconsistent results could be explained by use of older (no longer in use) analogue hearing aids or no acclimatization period (risk of bias). Since the inconsistent results of Kenworthy (1990) and Updike (1994) could be explained, the GRADE was not further downgraded for inconsistency. The trial of Benchetrit (2022) confirmed an improvement of most of these outcomes (authors used a combined endpoint of surveys of quality of life and listening difficulties or challenges with hearing amplification). Even though outcome effects were clinically relevant in most studies, we did not further upgrade the GRADE, given that the total sample size remained small for which reasons varied types, degrees, and configurations of unilateral hearing loss could not be studied.
The level of evidence regarding the outcome measure quality of life was not further downgraded.
The level of evidence regarding the outcome measure auditory development was downgraded by 1 level because of imprecision (only one study that reported on this outcome, low number of events, with large 95% CIs that did not exceed the threshold of clinical relevance).
The level of evidence regarding the outcome measure speech perception was downgraded by 1 level because of imprecision (only one study that reported on this outcome, low number of events)
The level of evidence regarding the outcome measure auditory discrimination was downgraded by 1 level because of imprecision (Three studies that reported on this outcome, but only one with up to date hearing system, low number of events)
The level of evidence regarding the outcome measure language was ungraded due to lack of data.
The level of evidence regarding the outcome measure hearing attention was ungraded due to lack of data.
The level of evidence regarding all outcomes related to early treatment (family centred care)
was ungraded due to lack of data.
Zoeken en selecteren
Wat is het effect van technische hoorrevalidatie en/of vroegbehandeling vergeleken met monitoring (watchful waiting) op de spraaktaalontwikkeling en de auditieve ontwikkeling bij kinderen van 0-4 jaar met een unilateraal gehoorverlies?
A systematic review of the literature was performed to answer the following question:
What is the effect of technical hearing rehabilitation and/or early treatment compared with monitoring (watchful waiting) on speech language development and auditory development in children aged 0-4 years with unilateral hearing loss (UHL)?
| P: | Children aged 0-4 years with (congenital) permanent unilateral hearing loss |
| I: | Technical hearing rehabilitation (hearing aid or remote microphone system), and/or early treatment (family centred care) |
| C: | No intervention or watchful waiting (i.e., periodic check-ups where hearing is measured) |
| O: | Quality of life, auditory development, speech (perception), auditory discrimination, language, hearing attention |
Relevant outcome measures
The guideline development group considered quality of life, auditory development, speech (perception), auditory discrimination as critical outcomes for decision making. The working group did not define the outcome measures listed above but used the definitions in the studies. The working group did not define a minimal clinically important difference for outcome measures. Therefore, default thresholds were used: 0.5SD for continuous outcomes and a 25% difference in relative risk (RR< 0.8 or RR>1.25) for dichotomous outcomes.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 3 March 2023. This search strategy can be found in the Methods section. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 309 hits, including 19 systematic reviews, 12 randomized controlled trials (RCTs) and 273 observational studies. Three reviewers independently performed data extraction. Studies (according to the abstract selection) were included when at least two authors agreed that the study could be included for data abstraction.
Referenties
- Alexander NL, Feng Z, Silva RC, Liu YC. Bone conduction hearing device adherence in relationship to age in pediatric unilateral congenital aural atresia. Int J Pediatr Otorhinolaryngol. 2021;141:110564. doi:10.1016/j.ijporl.2020.110564.
- Appachi S, Specht JL, Raol N, et al. Auditory Outcomes with Hearing Rehabilitation in Children with Unilateral Hearing Loss: A Systematic Review. Otolaryngol Head Neck Surg. 2017;157(4):565-571. doi:10.1177/0194599817726757.
- Bagatto M, DesGeorges J, King A, et al. Consensus practice parameter: audiological assessment and management of unilateral hearing loss in children. Int J Audiol. 2019;58(12):805-815. doi:10.1080/14992027.2019.1654620.
- Bakkum KHE, Teunissen EM, Janssen AM, Lieu JEC, Hol MKS. Subjective Fatigue in Children With Unaided and Aided Unilateral Hearing Loss. Laryngoscope. 2023;133(1):189-198. doi:10.1002/lary.30104.
- Benchetrit L, Stenerson M, Ronner EA, et al. Hearing Aid Use in Children With Unilateral Hearing Loss: A Randomized Crossover Clinical Trial. Laryngoscope. 2022;132(4):881-888. doi:10.1002/lary.29829.
- Bell R, Mouzourakis M, Wise SR. Impact of unilateral hearing loss in early development. Curr Opin Otolaryngol Head Neck Surg. 2022;30(5):344-350. doi:10.1097/MOO.0000000000000848.
- Briggs L, Davidson L, Lieu JEC. Outcomes of conventional amplification for pediatric unilateral hearing loss. Ann Otol Rhinol Laryngol. 2011;120:448-454.
- Cywka KB, Król B, Skar?y?ski PH. Effectiveness of Bone Conduction Hearing Aids in Young Children with Congenital Aural Atresia and Microtia. Med Sci Monit. 2021;27:e933915. Published 2021 Sep 25. doi:10.12659/MSM.933915.
- Fitzpatrick EM, Coyle D, Gaboury I, et al. Service Preferences of Parents of Children With Mild Bilateral or Unilateral Hearing Loss: A Conjoint Analysis Study. Ear Hear. 2019;40(3):671-679. doi:10.1097/AUD.0000000000000651.
- Fitzpatrick1 EM, Gaboury I, Durieux-Smith A, et al. Parent Report of Amplification Use in Children with Mild Bilateral or Unilateral Hearing Loss. J Am Acad Audiol. 2019;30(2):93-102. doi:10.3766/jaaa.17020.
- Fitzpatrick EM, Nassrallah F, Gaboury I, Whittingham J, Vos B, Coyle D, Durieux-Smith A, Pigeon M, Olds J. Trajectory of hearing loss in children with unilateral hearing loss. Front Pediatr. 2023 Apr 11;11:1149477. doi: 10.3389/fped.2023.1149477. PMID: 37114003; PMCID: PMC10126436.
- Kenworthy OT, Klee T, Tharpe AM. Speech recognition ability of children with unilateral sensorineural hearing loss as a function of amplification, speech stimuli and listening condition. Ear Hear. 1990;11(4):264-270. doi:10.1097/00003446-199008000-00003.
- Suissa S. The case-time-control design. Epidemiology. 1995;6(3):248-253. doi:10.1097/00001648-199505000-00010
- Updike CD. Comparison of FM auditory trainers, CROS aids, and personal amplification in unilaterally hearing impaired children. J Am Acad Audiol. 1994;5(3):204-209.
Evidence tabellen
Risk of bias table
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population? |
Exposure
Can we be confident in the assessment of exposure? |
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study? |
Confounding-assessment
Can we be confident in the assessment of confounding factors? |
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables? |
Assessment of outcome
Can we be confident in the assessment of outcome? |
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed? |
Co-interventions
Were co-interventions similar between groups? |
Overall Risk of bias |
|
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Low, Some concerns, High |
|
|
Cywka, 2021 |
Definitely yes
Reason: Participants were selected from one outpatient clinic |
Definitely yes
Reason: All children were provided with bone conduction hearing aids on a softband. |
Not applicable
Reason: this is controlled before-and-after study, where patients (by definition) could have the outcome of interest at start of study |
Probably yes
Reason: within individual comparisement |
Probably yes
Reason: within individual comparisement |
Definitely yes
Between 0- 6 months of hearing aid use, outcome questionnaire in children with unilateral defects |
Probably yes
After 6 months of hearing aid use, outcome questionnaire in children with unilateral defects |
Probably yes
Reason: within individual comparisement |
Low |
|
Briggs, 2011 |
Definitely yes
Reason: Participants were selected from one outpatient clinic |
Definitely yes
Reason: All children were fit with digital hearing aids using pediatric prescriptive targets. |
Not applicable
Reason: this is controlled before-and-after study, where patients (by definition) could have the outcome of interest at start of study |
Probably yes
Reason: within individual comparisement |
Probably yes
Reason: within individual comparisement |
Definitely yes
Between 0-3 months of hearing aid use, outcome questionnaires in children with unilateral defects were provided |
Probably yes
After 3 months of hearing aid use, outcome questionnaires in children with unilateral defects were provided |
Probably yes
Reason: within individual comparisement |
Low |
|
Kenworthy, 1990 |
Definitely yes
Reason: Participants were selected from one outpatient clinic |
Definitely yes
Reason: The patients fitted with hearing instruments were all fitted according to clinical standards. |
Not applicable
Reason: this is controlled before-and-after study, where patients (by definition) could have the outcome of interest at start of study |
Probably yes
Reason: within individual comparisement |
Probably yes
Reason: within individual comparisement |
Probably no
Immediate analysis of test measures in children with unilateral defects was provided (no acclimatization period) |
Probably yes
Immediate analysis test measures in children with unilateral defects was provided |
Probably yes
Reason: within individual comparisement |
Some (no acclimatization period) |
|
Updike, 1994 |
Definitely yes
Reason: Participants were selected from one outpatient clinic |
Definitely yes
Reason: The patients fitted with hearing instruments were all fitted according to clinical standards. |
Not applicable
Reason: this is controlled before-and-after study, where patients (by definition) could have the outcome of interest at start of study |
Probably yes
Reason: within individual comparisement |
Probably yes
Reason: within individual comparisement |
Probably no
Immediate analysis of auditory discrimination perception in children with unilateral defects was provided (no acclimatization period) |
Probably yes
Immediate analysis of auditory discrimination perception in children with unilateral defects was provided |
Probably yes
Reason: within individual comparisement |
Some (no acclimatization period) |
Risk of bias table
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Benchetrit, 2022 |
Definitely yes;
Reason: Central randomization with computer generated random numbers |
Definitely yes;
Reason: Central randomization with computer generated random numbers |
Definitely no;
Reason: Open label study |
Probably yes;
Reason: Loss to follow-up was infrequent in intervention and control group. |
Definitely yes;
Reason: All relevant outcomes were reported |
Definitely yes;
Reason: No other problems noted |
LOW |
Verantwoording
Beoordelingsdatum en geldigheid
Laatst beoordeeld : 15-01-2025
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de audiologische zorg voor slechthorende kinderen van 0 tot 4 jaar.
Werkgroep
- Dr. Y.J.W. Simis, voorzitter, klinisch fysicus audioloog, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- Ir. M.S. Toll, klinisch fysicus audioloog, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- Dr. Ir. W.J.A. Koopmans, klinisch fysicus audioloog, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- Ir. J.G. Kleinhuis, klinisch fysicus audioloog, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- Dr. D.C.P.B.M. Breukels, klinisch fysicus audioloog, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- Dr. Ir. R.A. Boerboom, klinisch fysicus audioloog, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- Dr. R.J.H. Ensink, KNO-arts, Nederlandse Vereniging voor Keel-Neus-Oorheelkunde en Heelkunde van het Hoofd-Halsgebied (NVKNO)
- Dr. E. Huysmans, klinisch-linguïst/master in audiologie, Vereniging voor Klinische Linguïstiek (VKL)
- Dr. E. Dirks, psycholoog, Nederlands Instituut van Psychologen (NIP)
- M.P. van der Heijden, audiologisch maatschappelijk werker, Landelijk Werkverband Maatschappelijk werkers in de Audiologie (LWMA)
Klankbordgroep
- C.P.W.M. van Daelen-Swinkels, logopedist, Nederlandse vereniging voor Logopedie en Foniatrie (NVLF)
- Dr. A.S. Smeijers, kinderarts, Nederlandse Vereniging voor Kindergeneeskunde (NVK)
- R. Glijsteen, huisarts, persoonlijke titel
- Dr. Ir. P. Brienesse, klinisch fysicus audioloog, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- C. ter Huurne, klinisch fysicus audioloog, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- J. Hoogeveen, Federatie van Ouders van Dove Kinderen (FODOK)
- L. Zwemmer, audioloog, Master Audiologen actief in Nederland (MAaN)
- B. van Malcot, audioloog, Master Audiologen actief in Nederland (MAaN)
Met ondersteuning van
- L.W.M. Boerboom, literatuurspecialist, Kennisinstituut van Federatie Medisch Specialisten
- L.H.M. Niesink-Boerboom, literatuurspecialist, Kennisinstituut van Federatie Medisch Specialisten
- Dr. N. van der Zwaluw, senior adviseur, Kennisinstituut van Federatie Medisch Specialisten
- Drs. A.E. Sussenbach, adviseur, Kennisinstituut van Federatie Medisch Specialisten
- Dr. W. Lijfering, senior adviseur, Kennisinstituut van Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Dr. Y.J.W. Simis |
klinisch fysicus -audioloog, Amsterdam UMC |
Extern lid van de klachtencommissie voor medewerkers, MOC 't Kabouterhuis, Amsterdam |
Geen |
Geen restricties |
|
Ir. M.S. Toll |
klinisch fysicus -audioloog, ErasmusMC |
Lid programmacommissie neonatale gehoorscreening |
Geen |
Geen restricties |
|
Dr. Ir. W.J.A. Koopmans |
klinisch fysicus -audioloog, Pento |
Geen |
Geen |
Geen restricties |
|
Ir. J.G. Kleinhuis |
klinisch fysicus -audioloog, Pento |
Geen |
Geen |
Geen restricties |
|
Dr. D.C.P.B.M. Breukels |
klinisch fysicus -audioloog, MUMC+ |
Geen |
Geen |
Geen restricties |
|
Dr. Ir. R.A. Boerboom |
klinisch fysicus -audioloog, UMC Utrecht |
Geen |
Extern gefinancierd onderzoek: Evaluating cochlear insertion trauma and hearing preservation after cochlear implantation (CIPRES) |
Restricties t.a.v. aanbevelingen m.b.t. cochleaire implantaten |
|
Dr. R.J.H. Ensink |
KNO-arts |
lid adviescommissie richtlijnen |
Geen |
Geen restricties |
|
Dr. E. Huysmans |
Klinisch linguïst, Amsterdam UMC |
Geen |
Geen |
Geen restricties |
|
Dr. E. Dirks |
Psycholoog, NSDSK |
Docent ontwikkelingspsychologie universiteit Utrecht (gedetacheerd vanuit NSDSK). Docent postmaster opleiding schoolpsycholoog (betaald 35 uur per jaar). bestuurslid sectie jeugd Nip (vrijwillig) |
Geen |
Geen restricties |
|
M.P. van der Heijden |
Maatschappelijk werker, Libra |
Bestuurslid LWMA |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het perspectief van ouders/verzorgers van patiënten door het uitnodigen van patiëntenfederaties FODOK en FOSS voor de invitational conference. Het verslag hiervan [zie aanverwante producten] is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan FODOK en FOSS en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz (wordt na de commentaarfase ingevuld)
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Module |
Uitkomst raming |
Toelichting |
|
Module Audiologische zorg voor unilaterale verliezen |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor slechthorende kinderen van 0-4 jaar. Tevens zijn er knelpunten aangedragen door verschillende partijen via een invitational conference. Een verslag hiervan is opgenomen onder aanverwante producten.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.