Selection of treatment modalities
Uitgangsvraag
Research questions
For which patient is which modality and in what order indicated for the treatment of spinal metastases, with the goals of palliation, achieving local control, and maintaining mobility in patients with spinal metastases?
Subquestions:
- How do you determine the phase the patient is in that indicates a particular treatment?
- Which treatment is indicated?
Aanbeveling
Recommendations
- Discuss whether the patient has a treatment preference or treatment wish.
- Assess the patient prior to initiating treatment systematically (using for example the NOMS framework$; see “Background”) in order to determine the preferred treatment, sequence, and priority. Discuss this preferably with the organ specialist with oncology expertise, an (interventional) radiologist, radiation oncologist, neurologist — if neurological deficits are present — and spinal surgeon).
- Before initiating therapy, consult in an ad-hoc multidisciplinary team meeting (MDO in Dutch) to discuss the impact that starting radiotherapy, surgery, or (delaying) systemic therapy may have on one another. Consider potential interactions between treatment modalities.
- Use the NOMS framework during MDO discussions of a patient; an alternative framework may also be used.
- Consider systemic therapy as first-line treatment for selected primary tumor types or a critical indication for systemic therapy (see module Systemic therapy), preferably after discussion in an MDO.
- For surgical interventions where radiotherapy is required, or for radiotherapy where surgical intervention cannot be excluded, see module Combination of surgery and radiotherapy.
- Depending on the disease stage, it is increasingly desirable to consult with a referral center in the region where 24/7 spinal surgery is available, and where - if in doubt -management decisions can be evaluated.
- Always consult a referral center immediately in patients with the following symptoms (derived from NOMS or otherwise):
- Any new neurological deficit, including bladder or bowel dysfunction
- Any MESCC grade 3 / spinal cord or cauda equina compression / absolute canal stenosis caused by tumor
- Any spinal instability with a SINS* score > 12
- For the following clinical presentations, refer to the respective modules described elsewhere:
- For patients with asymptomatic spinal metastases: see module Management of asymptomatic spinal metastases and module Systemic therapy.
- For patients with spinal metastases and pain but without instability (see module Evaluation of spinal stability): see module Systemic therapy and module Radiotherapy.
- For patients with instability:
- If there is no or minimal mechanical pain (= pain aggravated by walking or changes in posture and relieved by lying down), see module Radiotherapy.
- If surgical treatment is indicated, see module Surgery.
* Spinal Instability Neoplastic Score.
$ Neurologic, Oncologic, Mechanical, Systemic framework
Overwegingen
Considerations
Balance between desired and undesired effects
When selecting an appropriate treatment option for patients with spinal metastases it is imperative to have answers available to questions pertaining to the patient’s condition including: the presence of alarm symptoms (e.g. neurological deficits), (mechanical) back pain or radicular pain, oncological status and availability of treatment options, and overall performance status (Tsukamoto, 2021). As neurological alarm symptoms may be indicative of the development of serious and irreversible damage due to ongoing compression of the spinal cord or cauda equina, it is suggested that these symptoms receive the highest priority in terms of allocating time and resources for diagnosis, decision-making and treatment (van der Linden, 2015; Cole, 2008).
Neurological alarm symptoms can often be diagnosed by history taking combined with a relatively basic physical examination (van der Linden, 2015). Imaging studies have great value to indicate the location of the metastatic epidural spinal cord/cauda compression (MESCC) and may even visualize an imminent threat to neurological function in an, otherwise, asymptomatic patient (Cole, 2008; Switlyk, 2012). Once a high-grade MESCC (Bilsky 2/3, see chapter 1.2 pathofysiology) has been visualized in a patient with spinal metastasis, it is critical to record the presence of neurological symptoms (if any) and their progression over time. Rapidly progressing neurological deficits can lead to (irreversible) loss of function in the course of hours to days; while slowly progressing deficits may lead to minimal loss of function and remain stable for days to weeks (Vaishya,2024). As a rule of thumb, rapid progression of neurological deficits warrants an equally rapid response from caregivers to maintain or restore as much function as possible (van Tol, 2020). For patients who are fit for surgery, the presence of neurological symptoms in combination with a high-grade MESCC warrants urgent decompressive surgery, sometimes combined with stabilizing surgery and often followed by radiotherapy for long term tumor control (Amelink, 2025).
For patients with spinal metastasis not displaying alarm symptoms (e.g. neurological deficits and/or high-grade MESCC), it is important to balance the nature and severity of the complaints against the demands and complications of treatments offered. For some patients no specific treatment or intervention is needed due to minor symptoms or limited life expectancy. For other patients symptoms can be moderate to severe warranting further examination and treatment. It is currently believed that different forms of pain exist in patients with spinal metastases each with their optimal treatment modality (Pahuta, 2025). Inflammatory pain has been described as the pain caused by local secretion of inflammation mediators, cytokines etc. by the spinal metastasis (Takemura, 2023). Inflammatory pain typically responds well to palliative radiotherapy (Mercadante, 2007). This type of pain differs from the pain due to weakening of the bone by a locally destructive tumor. With the advent of the SINS score more information has become available on the topic of ‘mechanical instability’ (Versteeg, 2016). Many studies have shown pain caused by mechanical instability to respond best to a form of stabilization, mostly by surgically fixing vertebral segments together to restore stability (Versteeg, 2019). However, patients with pain caused by mechanical instability of spinal metastases should be carefully selected and declared to be fit for surgery, for example based on their performance status (Verlaan, 2016). If patients are not declared fit for surgery, patients with pain form unstable spinal metastases might still benefit from systemic and/or radiotherapy. Generally accepted criteria to briefly assess whether a patient is fit for surgery are a KPS > 50 and a life expectancy of more than 3 months. To select the best treatment for each patient, we advocate a treatment/referral scheme based on the amount of pain, neurological status and performance status of patient with painful spinal metastases. In this scheme we also advocate a timeline for referral for patients with different characteristics in pain and neurological status.
Values and preferences of patients (and possibly their relatives/caregivers)
Timely, systematically organized consultation and treatment within a multidisciplinary team meeting is expected to offer patients personalized, optimal care. During the process of creating a treatment plan, the recommended treatment will be communicated to the patient, including both the advantages and the risks. The values and preferences of patients, and possibly their relatives or caregivers, will be taken into consideration.
Cost aspects
The recommendations in this module are designed to provide patients with the best available and most effective treatment, which is expected to improve patient outcomes and reduce costs compared with less organized approaches.
Equity (health equity / equitable access)
Since the selection of treatment modality is applicable to every patient, the recommendations are not expected to affect health equity.
Acceptability
Ethical acceptability
Ethical acceptability does not play a role in this module.
Sustainability
Sustainability does not play a role in this module.
Feasibility
The working group believe that working through an multidisciplinairy team meeting approach using the NOMS framework is feasible. However, there should be regional consensus on which hospital serves as the referral center in cases of neurological involvement. Such a referral center should provide 24/7 coverage by a spinal surgeon (either an orthopedic surgeon or a neurosurgeon). Therefore, it is highly recommended to establish a clear protocol or care pathway for patients with spinal metastases, specifying which hospital acts as the referral center for spinal surgery. It should also be defined when immediate discussion with the referral center is mandatory and which cases can be discussed later, for example during a multidisciplinairy team meeting.
Onderbouwing
Background
In the old guideline in which this module was titled ‘Radiotherapie of chirurgie’, decisions are based on factors such as life expectancy or the tumor's sensitivity to chemotherapy. Estimating life expectancy is often difficult, as is assessing the tumor's sensitivity to chemotherapy. As a result, the recommendations are challenging to implement. The number of affected vertebrae is also no longer a mandatory criterion. Therefore, the old module is considered outdated.
Moreover, the old module operates on the assumption of isolated work by either the oncologist, radiation oncologist or the spine surgeon, rather than emphasizing strong collaboration between disciplines. In the past 10 years, multidisciplinary teamwork has become prevalent. There is increased awareness of the interplay and impact of initiating radiation therapy, surgery, or (delaying) systemic therapy on the patient and the various treatments.
Decisions regarding interventions are now more frequently made using conceptual frameworks such as the NOMS (see Figure 1.), to discuss cases in a multidisciplinary team (Laufer, 2013). The NOMS framework encompasses the four key components that systematically guide treatment decision-making.
- The Neurologic component (N) is determined by the severity of neurological deficits and/or the degree of spinal cord or cauda equina compression, the latter commonly assessed using the MESCC/Bilsky scale.
- The Oncologic component (O) is defined by the origin of the primary tumor and the availability of systemic therapy and/or radiotherapy options.
- The Mechanical component (M) is determined by the SINS score (Spinal Instability Neoplastic Score), in which the pain component may carry additional weight in treatment decision-making.
- The Systemic component (S) refers to the patient’s overall fitness for treatment and is typically expressed using the Karnofsky Performance Status or the ECOG/WHO performance scale.
This has also been incorporated into training and continuing education programs. Therefore, we updated this treatment module and changed the name for radiotherapy or surgery to selection of treatment modality to emphasize the importance of providing the preferred order of treatment modalities by a multidisciplinary team.
Whenever a radiologist is mentioned in the context of treatment, this also includes interventional radiologists.
Figure 1. Schematic depiction of the neurologic, oncologic, mechanical, and systemic (NOMS) decision framework
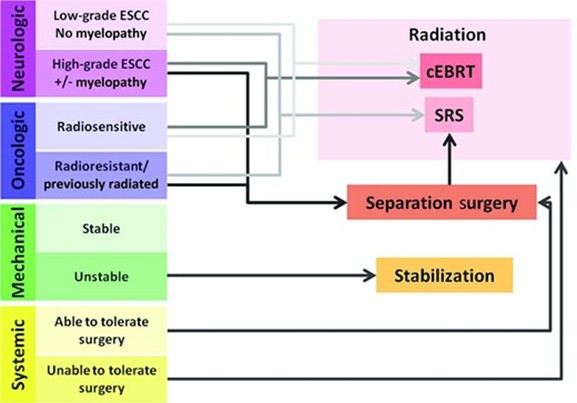
Comments:
- Radioresistant histologies include metastases from renal cell carcinoma, melanoma, or colon carcinoma
- Separation surgery includes decompressive surgery
Abbreviations: ESCC, epidural spinal cord compression; cEBRT, conventional external beam radiation; SRS, stereotactic radiosurgery.
Resource: Laufer 2013
Search and select
A search was not conducted because it was not anticipated that there would be research available to answer this key question. Therefore, the question has been addressed using expert opinion, the expertise of the working group, and existing agreements regarding the organization of care in the Netherlands.
- 1 - Amelink JJ, Bindels BJ, Kasperts N, MacDonald SM, Tobert DG, Verlaan JJ. Radiotherapy and surgery: can this combination be further optimized for patients with metastatic spine disease?. The Oncologist. 2025 Jan;30(1):oyae359.
- 2 - Cole JS, Patchell RA. Metastatic epidural spinal cord compression. The Lancet Neurology. 2008 May 1;7(5):459-66.
- 3 - Laufer I, Rubin DG, Lis E, Cox BW, Stubblefield MD, Yamada Y, Bilsky MH. The NOMS framework: approach to the treatment of spinal metastatic tumors. The oncologist. 2013 Jun 1;18(6):744-51.
- 4 - Mercadante S, Fulfaro F. Management of painful bone metastases. Current opinion in oncology. 2007 Jul 1;19(4):308-14.
- 5 - Pahuta M, Laufer I, Lo SF, Boriani S, Fisher C, Dea N, Weber MH, Chou D, Sahgal A, Rhines L, Reynolds J. Defining Spine Cancer Pain Syndromes: A Systematic Review and Proposed Terminology. Global spine journal. 2025 Jan;15(1_suppl):81S-92S.
- 6 - Switlyk MD, Hole KH, Skjeldal S, Hald JK, Knutstad K, Seierstad T, Zaikova O. MRI and neurological findings in patients with spinal metastases. Acta Radiologica. 2012 Dec;53(10):1164-72.
- 7 - Takemura M, Niki K, Okamoto Y, Tamura H, Kawamura T, Kohno M, Matsuda Y, Ikeda K. Differences in the analgesic effect of opioids on pain in cancer patients with spinal metastases. Palliative Medicine Reports. 2023 Aug 1;4(1):220-30.
- 8 - Tsukamoto S, Kido A, Tanaka Y, Facchini G, Peta G, Rossi G, Mavrogenis AF. Current overview of treatment for metastatic bone disease. Current Oncology. 2021 Aug 29;28(5):3347-72.
- 9 - Vaishya S, Gaonkar V, Bedi MS, Yaman O, Zileli M, Sharif S. Clinical evaluation, diagnosis, and decision-making for metastatic spine tumors: WFNS spine committee recommendations. Neurosurgical review. 2024 Dec 14;47(1):902.
- 10 - van der Linden YM, Rolf CA, de Graeff A, Dijkstra PD, Kuijlen JM, Taal W. Alarm symptoms of spinal metastases in patients with cancer. Nederlands Tijdschrift Voor Geneeskunde. 2015 Jan 1;159:A9256-.
- 11 - van Tol FR, Suijkerbuijk KP, Choi D, Verkooijen HM, Oner FC, Verlaan JJ. The importance of timely treatment for quality of life and survival in patients with symptomatic spinal metastases. European Spine Journal. 2020 Dec;29(12):3170-8.
- 12 - Verlaan JJ, Choi D, Versteeg A, Albert T, Arts M, Balabaud L, Bunger C, Buchowski JM, Chung CK, Coppes MH, Crockard HA. Characteristics of patients who survived< 3 months or> 2 years after surgery for spinal metastases: can we avoid inappropriate patient selection?. Journal of Clinical Oncology. 2016 Sep 1;34(25):3054-61.
- 13 - Versteeg AL, Verlaan JJ, Sahgal A, Mendel E, Quraishi NA, Fourney DR, Fisher CG. The spinal instability neoplastic score: impact on oncologic decision-making. Spine. 2016 Oct 15;41:S231-7.
- 14 - Versteeg AL, Sahgal A, Kawahara N, Rhines LD, Sciubba DM, Weber MH, Lazary Á, Fehlings MG, Schuster JM, Clarke MJ, Arnold PM. Patient satisfaction with treatment outcomes after surgery and/or radiotherapy for spinal metastases. Cancer. 2019 Dec 1;125(23):4269-77.
Beoordelingsdatum en geldigheid
Publicatiedatum : 05-06-2026
Beoordeeld op geldigheid : 05-06-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met wervelmetastasen.
Werkgroep
- dr. W. (Walter) Taal (voorzitter), neuroloog Erasmuc MC, Nederlandse Vereniging voor Neurologie
- drs. L. (Lena) van Iterson, AIOS-neuroloog Elisabeth-TweeSteden Ziekenhuis, Nederlandse Vereniging voor Neurologie
- drs. R.P.B. (Robin) Boltjes, neuroloog Antoni van Leeuwenhoek Ziekenhuis, Nederlandse Vereniging voor Neurologie
- Prof. dr. JJ. (Jorrit-Jan) Verlaan, Orthopedisch chirurg UMC Utrecht, Nederlandse Orthopaedische Vereniging
- dr. J. (Jasper) van Tiel, Orthopedisch chirurg UMC Utrecht, Nederlandse Orthopaedische Vereniging
- dr. V. (Vivian) Bongers, Nucleaire geneeskunde Diakonessenhuis Utretch, Nederlandse Vereniging voor Nucleaire Geneeskunde
- Prof. dr. R. (Ronald) Bartels, Neurochirurg Radboudumc, Nederlandse Vereniging voor Neurochirurgie
- dr. S.O. (Selma) Algra, Radioloog UMC Utrecht, Nederlandse Vereniging voor Radiologie
- drs. M.G.A. (Maaike) Schippers, radiotherapeut Instituut Verbeeten, Nederlandse Vereniging voor Radiotherapie en Oncologie
- dr. J.M. (Joanne) van der Velden, radiotherapeut UMC Utrecht, Nederlandse Vereniging voor Radiotherapie en Oncologie
- dr. M.S. (Marthe) Paats, longarts Erasmus MC, Nederlandse Vereniging voor Artsen voor Longziekten en TBC
- dr. P.F. (Paula) Ypma, Internist hematoloog Haga Ziekenhuis, Nederlandse Internisten Vereniging
- dr. F.Y.F.L. (Filip) de Vos, internist-oncoloog en kaderarts palliatieve zorg UMC Utrecht, Nederlandse Internisten Vereniging
- dr. M. (Marije) Vos- van der Hulst, revalidatiearts Sint Maartenskliniek, Nederlandse Vereniging van Revalidatieartsen (vanaf oktober 2025)
- Mevr. S (Silvie) Dronkers†, patiëntvertegenwoordiger, Stichting Darmkanker (tot oktober 2025)
- dr. T.A.R. (Tebbe) Sluis†, Revalidatiearts Rijndam, Nederlandse Vereniging van Revalidatieartsen (tot mei 2025)
Klankbordgroep
- Mevr. Manon Immerzeel, Verpleegkundig specialist Reinier de Graaf ziekenhuis, Verpleegkundigen en Verzorgenden Nederland
- drs. A. (Anita) Ophof, anesthesioloog Antoni van Leeuwenhoek Ziekenhuis, Nederlandse Vereniging voor Anesthesiologie
Met dank aan
- dr. J.H. (Jurgen) Runge, interventieradioloog, UMC Groningen, Nederlandse Vereniging voor Radiologie
Met ondersteuning van
- dr. J. (Josefien) Buddeke, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten (vanaf juli 2024)
- dr. L. (Linda) Oostendorp, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten (tot juli 2024)
- drs. B. (Beatrix) Vogelaar, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- dr. J. (Jing) de Haan-Du, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- drs. D. (Danique) Middelhuis, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- drs. A. (Alies) Oost, informatiespecialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Gemelde (neven)functies en belangen werkgroep
|
Naam WERKGROEP |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke Financiele_Belangen |
Persoonlijke Relaties |
Extern Gefinancierd Onderzoek |
Intellectuele Belangen Reputatie |
Overige Belangen |
Datum |
Acties |
|
Jasper van Tiel |
Orthopedisch chirurg UMC Utrecht en Acibadem IMC |
geen |
geen |
geen |
geen |
geen |
geen |
22-11-2023 |
Geen restrictie |
|
Joanne van der Velden |
Radiotherapeut bij het UMC Utrecht, betaald |
Bestuurslid bij het Landelijk Platform Palliatieve Radiotherapie (NVRO), onbetaald |
Geen |
Geen |
Deelname aan 2 extern gefinancierde onderzoeken, zie onder |
Verwerven van erkenning speelt mee aan mijn deelname aan de werkgroep richtlijn Wervelmetastasen |
Geen overige belangen |
28-12-2023 |
Geen restrictie |
|
Jorrit-Jan Verlaan |
Orthopedisch chirurg, UMC Utrecht (0.4 Fte) |
Lid steering committee AO Spine Knowledge Forum Tumor (onbetaald maar met onkosten vergoeding). |
Hoe de richtlijn wordt vormgegeven staat los van mijn persoonlijke financiële belangen. Er zijn ook geen belangen voor SentryX hoe de richtlijn wordt vormgegeven. |
geen |
Ja. |
Ik heb nationale/internationale expertise/reputatie en een leerstoel op het gebied van de behandeling van wervelmetastasen. Een goed uitgevoerde richtlijn kan helpen deze expertise/reputatie meer exposure te geven maar de impact en eventuele belangenverstrengeling zijn mij onduidelijk. |
geen |
22-11-2023 |
Geen restrictie. Geen penvoerder bij module 'Inschatten overleving'. |
|
Filip de Vos |
Internist-oncoloog en kaderarts palliatieve zorg |
geen |
geen |
geen |
ja |
geen |
BMS Advisory Board; Faculty member ESMO CNS tumors; Quality of Care commission Dutch Society of Medical Oncology; |
20-12-2023 |
Geen restrictie. (In de richtlijn worden geen systemische therapien aanbevolen.) |
|
Maaike Schippers |
Radiotherapeut |
geen |
geen |
geen |
geen |
geen |
geen |
3-12-2023 |
Geen restrictie |
|
Marthe Paats |
Longarts Erasmus MC |
geen |
Geen relevant voor huidige richtlijn. |
geen |
industrie gesponsorde studies lopend in het Erasmus MC waarbij ik lokale PI ben. |
geen |
geen |
26-02-2024 |
Geen restrictie. In de richtlijn worden geen systemische therapien aanbevolen. |
|
Robin Boltjes |
Neuroloog in Antoni van Leeuwenhoek/NKI |
geen |
geen |
nee |
geen |
geen |
nee |
22-11-2023 |
Geen restrictie |
|
Ronald Bartels |
Neurochirurg |
Medisch Adviseur |
geen |
nee |
geen |
net |
geen |
03-04-2024 |
Restrictie ten aanzien van besluitvorming betreffende 'Inschatten overleving'. Vanuit expertise wel meegediscussierd over inhoud van de module, niet betrokken bij het formuleren van de aanbevelingen. |
|
Tebbe Sluis |
revalidatiearts |
geen |
geen |
geen |
geen |
geen |
geen |
11-12-2023 |
Geen restrictie |
|
Vivian Bongers |
MSB Domstad, medisch specialist |
Uitgeverij Prelum, Redacteur tijdschrift IMAGO |
Geen |
Geen |
Geen |
Geen |
Geen |
23-11-2023 |
Geen restrictie |
|
Ypma |
internist hematoloog Hagaziekenhuis den Haag |
geen |
geen |
geen |
Alphabet trial |
geen |
nvt |
04-05-2024 |
Geen restrictie |
|
Van Iterson |
AIOS neurologie |
geen |
geen |
geen |
geen |
geen |
geen |
25-04-2024 |
Geen restrictie |
|
Selma Algra |
Radioloog,St Jansdal Ziekenhuis |
geen |
geen |
geen |
geen |
geen |
geen |
03-09-2024 |
Geen resctrictie |
|
Silvie Dronkers |
Stichting Darmkanker |
geen |
geen |
geen |
geen |
geen |
geen |
06-02-2025 |
Geen restrictie |
|
Walter Taal (voorzitter) |
Neuroloog, Erasmus MC, Rotterdam |
Geen |
Geen |
Geen |
Ja. Alleen op het gebied van neurofibromatose type 1 |
Geen |
Geen |
07-06-2023 |
Geen restrictie |
|
Marije Vos-van der Hulst |
Revalidatie arts, Sint Maartenskliniek Nijmegen |
Voorzitter werkgroep revalidatie artsen dwarslaesie (Nederlands Vlaams dwarslaesie genootschap= werkgroep van de vereniging revalidatieartsen nederland (VRA)) |
geen |
geen |
geen |
geen |
geen |
13-10-2025 |
Geen restrictie |
|
Naam KLANKBORDGROEP |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke Financiele_Belangen |
Persoonlijke Relaties |
Extern Gefinancierd Onderzoek |
Intellectuele Belangen Reputatie |
Overige Belangen |
Datum |
Acties |
|
Manon Immerzeel |
Deelnemer clusterstuurgroep |
Geen |
Geen |
Geen |
Geen |
Voorzitter in het bestuur van V&VN pijnverpleegkundigen |
Neen |
22-03-2022 |
Geen restrictie |
|
Anita Ophof |
Antoni van Leeuwenhoek Ziekenhuis |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
01-05-2025 |
Geen restrictie |
Inbreng patiëntenperspectief
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
De kwalitatieve raming is toegevoegd aan het einde van elke herziene module.
| Module | Uitkomst raming | Toelichting |
| Selection of treatment modalities | Geen substantiële financiële gevolgen | Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.