Techniek voor tracheacanule plaatsing
Uitgangsvraag
Welke techniek voor tracheacanule plaatsing heeft de voorkeur bij een volwassen patiënt die op de intensive care is opgenomen?
Aanbeveling
Gebruik standaard de percutane dilatatie techniek bij het verrichten van een tracheotomie.
Neem de chirurgische techniek in overweging bij de volgende indicaties:
- status na hoofd-halschirurgie of bestraling;
- struma of andere afwijkingen in de halsanatomie;
- voorliggende grote vaten (vasculaire afwijkingen);
- ernstige obesitas;
- stollingsstoornissen;
- onduidelijke of moeilijke anatomie op echografie;
- noodzaak tot langdurige tracheotomie (bijvoorbeeld bij oncologische patiënten).
Overwegingen
Balans tussen gewenste en ongewenste effecten
In de literatuur werd het verschil in succespercentage tussen de percutane dilatatie techniek (PDT) en chirurgische techniek bij een electieve tracheotomie niet beschreven. Er zijn twee systematische reviews verricht waarin gekeken werd naar de complicaties van een electieve tracheotomie. Bij de PDT werden minder wondinfecties vastgesteld dan bij de chirurgische techniek. Ook het aantal postoperatieve bloedingen, periodes van hypoxie en saturatiedalingen onder de 90% leken lager te zijn in de PDT-groep dan in de chirurgische groep. De overall bewijskracht voor deze cruciale uitkomstmaten is zeer laag doordat er sprake is van heterogeniteit tussen de geïncludeerde patiënten, het verschil in de hoeveelheid ervaring met de uitgevoerde techniek van de operateurs in de studies en kleine patiëntengroepen. Er werden geen verschillen gevonden tussen de technieken wat betreft het aantal levensbedreigende complicaties zoals excessief bloedverlies tijdens de procedure of obstructie van de canule door ingedikt slijm en/of bloed.
Gezien het feit dat intensivisten in Nederland de meeste ervaring hebben met de percutane dilatatie techniek, waarbij bijna altijd onder zicht door middel van flexibele tracheoscopie een canule wordt geplaatst, en het aantal complicaties met deze techniek lager lijkt dan bij de chirurgische techniek, is de werkgroep van mening dat de percutane dilatatie techniek de voorkeur heeft bij een electieve tracheotomie. Aangezien het aantal electieve tracheacanule plaatsingen op een IC gering kan zijn, kan het opdoen van individuele ervaring met het plaatsen van een canule in de praktijk lastig zijn. Daarom is het te overwegen om per IC een beperkt aantal dedicated intensivisten aan te wijzen voor het electief plaatsen van een tracheacanule. Daarnaast kan lokaal besloten worden de algemeen chirurg met expertise, MKA (mond-, kaak, aangezichts-,)chirurg of keel-, neus, oor (KNO)-arts in consult te vragen voor het plaatsen van een canule middels de chirurgische techniek, indien er te weinig expertise is wat betreft de percutane dilatatie techniek.
Uiteraard is het van belang om te beoordelen of een patiënt geschikt is voor de percutane dilatatie techniek. De tussenruimte tussen 1ste en 2de trachearing moet bij palpatie voelbaar zijn. Indien palpatie van de tussenruimte lastig is, kunnen palpatie van het thyroidkraakbeen en jugulum helpen: de tussenruimte tussen de 1ste en 2de trachearing bevindt zich in het midden van deze twee structuren. Echografie van de hals kan behulpzaam zijn in het identificeren van anatomische structuren zoals de schildklier, kraakbeen- en vaatstructuren.
Kwaliteit van bewijs
De bewijskrachten van de cruciale uitkomstmaten lopen zeer uiteen. Voor de cruciale uitkomstmaat infectie (onderdeel van complicaties) werd een redelijke bewijskracht gevonden, terwijl voor de andere cruciale uitkomstmaten zeer lage bewijskrachten werd gevonden. De overall kwaliteit van bewijs is daarom zeer laag. Dit betekent dat we zeer onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege (zeer) ernstige:
- Risico op bias: methodologische beperkingen
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grens/beide grenzen van klinische relevantie overschrijdt of vanwege het niet bereiken van de optimale steekproefgrootte.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Indien de beademing bij een patiënt langer lijkt te gaan duren dan twee weken, kan een tracheotomie overwogen worden. Vanuit het patiëntenperspectief kan het plaatsen van een tracheacanule het eten, drinken, en spreken mogelijk maken, het ophoesten vergemakkelijken, de bewegingsvrijheid vergroten, het ontwennen van de beademing bevorderen, en uiteindelijk overplaatsing naar de afdeling mogelijk maken. Uit de literatuur blijkt dat het plaatsen van een tracheacanule risico’s kent, zoals bloedverlies en infecties, en zelfs overlijden. Deze complicaties lijken minder vaak op te treden als de tracheacanule met de percutane dilatatie techniek wordt geplaatst dan wanneer dit met een chirurgische techniek gebeurt. Kanttekening hierbij is dat per patiënt moet worden ingeschat of de percutane dilatatie techniek mogelijk is en of er voldoende getraind personeel aanwezig is om de percutane dilatatie techniek veilig te kunnen uitvoeren. De afwegingen om te kiezen voor een bepaalde techniek en de kans op complicaties dienen met de patiënt en familie gedeeld te worden.
Houd bij alle afwegingen rekening met de aanbevelingen uit de richtlijn Nazorg en Revalidatie van intensive care patiënten (2022).
Kostenaspecten
Een inbrengset (conische dilatatietechniek) kost circa 320 euro. Bij de chirurgische techniek is een losse canule nodig (à circa 100 euro), maar zijn er ook significante kosten voor het gebruik van de OK, kosten van de chirurg en anesthesioloog, waardoor de totale kosten voor de chirurgische techniek altijd hoger zullen uitkomen dan voor een percutane dilatatie procedure op de IC.
Gelijkheid ((health) equity/equitable)
De interventie heeft geen invloed op de gezondheidsgelijkheid.
Aanvaardbaarheid, haalbaarheid en implementatie:
De interventie lijkt aanvaardbaar voor de betrokkenen. Er zijn geen ethische bezwaren. Bij de interventie spelen bij zowel de percutane dilatatie techniek als de chirurgische techniek de volgende duurzaamheidsaspecten een rol: er zijn een canule inbrengset, steriele doeken, een canule, kompressen, een fixatiebandje, desgewenst een spreekventiel en reinigingsmateriaal nodig. De interventie is over het algemeen al standaardzorg in de praktijk.
Bij het verrichten van een electieve tracheotomie bij volwassen patiënten op de IC gaat de voorkeur uit naar de percutane dilatatie techniek. Bij de percutane dilatatie techniek lijken minder wondinfecties op te treden dan bij de chirurgische techniek. Ook het aantal postoperatieve bloedingen, periodes van hypoxie en saturatiedalingen onder de 90% leken, hoewel niet significant, lager te zijn in de PDT-groep dan in de chirurgische groep. De bewijskracht voor deze uitkomstmaten is echter redelijk tot zeer laag.
Kanttekening hierbij is dat wel de juiste patiënt voor de percutane dilatatie techniek moet worden geselecteerd. Bij patiënten bij wie de anatomische referentiepunten zeer moeilijk te lokaliseren zijn, door bijvoorbeeld eerdere hoofd-halschirurgie of bestraling, struma, voorliggende grote vaten (vasculaire afwijkingen) of ernstige obesitas, en bij patiënten waarbij de intubatie in een eerder stadium zeer lastig was, is de chirurgische techniek te overwegen. In het geval van een eerdere moeilijke intubatie moet worden nagegaan wat de reden hiervoor was en kan in overleg met de (MKA)chirurg of KNO-arts besloten worden welke techniek de voorkeur heeft. Bij een moeilijke intubatie, bijvoorbeeld vanwege een beperkte mondopening of een laryngeaal probleem, kan bij een verder slanke patiënt mogelijk probleemloos een PDT worden uitgevoerd. In deze gevallen bestaat er een hoger risico om de luchtweg te verliezen wanneer de tube voor de procedure wordt teruggetrokken. Er kan overwogen worden om een anesthesioloog te betrekken.
Een chirurgische techniek is aan de orde indien de intensivist onvoldoende expertise heeft in het uitvoeren van de percutane dilatatie techniek.
Eindoordeel:
Sterke aanbeveling voor het gebruik van de percutane dilatatie techniek boven de chirurgische techniek bij het electief plaatsen van een tracheacanule op de IC. In het geval van afwijkende anatomie van de hals (status na hoofd-halschirurgie of bestraling, struma, voorliggende grote vaten of ernstige obesitas) zal overleg plaats vinden met een collega met expertise in het verrichten van een chirurgisch tracheotomie.
Onderbouwing
Placing a percutaneous tracheostomy is common practice in intensive care units (ICU) in the Netherlands. This procedure is almost always performed by intensivists themselves. The percutaneous technique has many practical advantages and has replaced the surgical technique. Several studies have shown that the percutaneous technique is faster, safer, and cheaper than the surgical technique. The exceptions are a difficult airway, unfavorable anatomy (including abnormal neck vascularization, enlarged thyroid gland, morbid obesity) and burns in the neck, for which the surgical technique must be considered.
Summary of Findings
Population: Adult patients admitted to the ICU who are going to have a tracheostomy placed and who are intubated
Intervention: Percutaneous dilatational tracheostomy
Comparator: Surgical tracheostomy
Click here to see this table in a document
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Conclusions |
||
|
Surgical tracheostomy |
Percutaneous dilatational tracheostomy |
|||||
|
Successful tracheostomy placement (critical)
|
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of percutaneous dilatational tracheostomy on successful tracheostomy placement when compared with surgical tracheostomy in adult patients admitted to the ICU who are going to have a tracheostomy placed and who are intubated. |
||
|
Major complications |
||||||
|
Intraoperative serious, life-threatening adverse events (critical)
|
Relative risk: 0.93 (CI 95% 0.57 - 1.53) Based on data from 1211 participants in 12 studies |
49 per 1000 |
46 per 1000 |
Very low Due to serious risk of bias, due to very serious imprecision1 |
The evidence is very uncertain about the effect of percutaneous dilatational tracheostomy on intraoperative serious, life threatening events when compared with surgical tracheostomy in adult patients admitted to the ICU who are going to have a tracheostomy placed and who are intubated. |
|
|
Difference: 3 fewer per 1000 |
||||||
|
Direct postoperative serious, life-threatening adverse events (critical) |
Relative risk: 0.72 (CI 95% 0.41 - 1.25) Based on data from 984 participants in 10 studies |
49 per 1000 |
35 per 1000 |
Very low Due to serious risk of bias, due to very serious imprecision1 |
The evidence is very uncertain about the effect of percutaneous dilatational tracheostomy on direct postoperative serious, life threatening events when compared with surgical tracheostomy in adult patients admitted to the ICU who are going to have a tracheostomy placed and who are intubated. |
|
|
Difference: 14 fewer per 1000 |
||||||
|
Significant infection (critical)
|
Relative risk: 0.29 (CI 95% 0.18 - 0.45) Based on data from 1096 participants in 15 studies
|
161 per 1000 |
47 per 1000 |
Moderate Due to serious risk of bias2
|
Percutaneous dilatational tracheostomy likely results in a reduction in infection when compared with surgical tracheostomy in adult patients admitted to the ICU who are going to have a tracheostomy placed and who are intubated. |
|
|
Difference: 114 fewer per 1000 (CI 95% 132 fewer - 89 fewer) |
||||||
|
Postoperative bleeding (critical)
|
Relative risk: 0.62 (CI 95% 0.31 - 1.23) Based on data from 1144 participants in 13 studies
|
79 per 1000 |
49 per 1000 |
Very low Due to serious risk of bias, due to serious inconsistency, due to serious imprecision3
|
The evidence is very uncertain about the effect of percutaneous dilatational tracheostomy on postoperative bleeding when compared with surgical tracheostomy in adult patients admitted to the ICU who are going to have a tracheostomy placed and who are intubated. |
|
|
Difference: 30 fewer per 1000 (CI 95% 55 fewer - 18 more) |
||||||
|
Procedural bleeding (critical) |
Based on data from 2 studies |
Kim (2023) reported a mean difference of 0.60 mL (95%CI -0.58 to 1.78) in procedure-related estimated blood loss in favor of surgical tracheostomy. Pandit (2023) reported a risk ratio of 0.91 (95%CI 0.55 to 1.50) for minimal peri-operative hemorrhage and a risk ratio of 1.20 (95%CI 0.46 to 3.15) for moderate peri-operative hemorrhage. |
Very low Due to serious risk of bias, due to very serious imprecision4 |
The evidence is very uncertain about the effect of percutaneous dilatational tracheostomy on procedural bleeding when compared with surgical tracheostomy in adult patients admitted to the ICU who are going to have a tracheostomy placed and who are intubated. |
||
|
Air leakage (critical) |
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of percutaneous dilatational tracheostomy on air leakage when compared with surgical tracheostomy. |
||
|
Airway loss (critical) |
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of percutaneous dilatational tracheostomy on airway loss when compared with surgical tracheostomy. |
||
|
|
||||||
|
Tracheomalacia (important) |
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of percutaneous dilatational tracheostomy on tracheomalacia when compared with surgical tracheostomy. |
||
|
Stenosis (important) |
Based on data from 1 study |
Pandit (2023) reported that 1 of the 16 patients (6.3%) who underwent percutaneous dilatational tracheostomy had a tracheal stenosis, while this did not occur in patients who underwent surgical tracheostomy. |
Very low Due to serious risk of bias, due to very serious imprecision4 |
The evidence is very uncertain about the effect of percutaneous dilatational tracheostomy on stenosis when compared with surgical tracheostomy in adult patients admitted to the ICU who are going to have a tracheostomy placed and who are intubated. |
||
1. Risk of Bias: serious. Due to study limitations.
Imprecision: very serious. Due to overlap of the upper and lower limit of the 95% confidence interval with the minimal clinically important difference.
2. Risk of Bias: serious. Due to study limitations.
3. Risk of Bias: serious. Due to study limitations.
Inconsistency: serious. Due to conflicting results and heterogeneity in the definition of the outcome measure.
Imprecision: serious. Due to overlap of the lower limit of the 95% confidence interval with the minimal clinically important difference.
4. Risk of Bias: serious. Due to study limitations.
Imprecision: very serious. Due to the optimal information size which was not achieved.
Description of studies
A total of five studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Battaglini (2022) performed a systematic review to assess the effect of surgical versus percutaneous tracheostomy in mechanically ventilated patients with COVID-19. PubMed, Embase, Scopus, and Cochrane were searched for all published observational studies between January 1, 2020 and January 10, 2022. Observational studies and randomized trials including 20 or more adult patients with suspected or confirmed SARS-CoV-2 infection who received a tracheostomy during their ICU course were included. In total, 47 observational studies were included.
The Cochrane review of Brass (2016) examined the effectiveness and safety of percutaneous techniques compared to surgical techniques for elective tracheostomy in critically ill adults and children. CENTRAL, MEDLINE, EMBASE, and CINAHL were searched until the 28th of May 2015 for randomized and quasi-randomized controlled trials comparing percutaneous techniques with surgical techniques. In addition, reference lists of articles, ’grey literature’, dissertations, intensive care and anaesthesia journals, abstracts, and proceedings of scientific meetings were searched. Unpublished or ongoing studies were identified by contacting manufacturers and expertise in the field and searching in trial registers. Twenty studies were included.
Katial (2024) performed a randomized controlled trial to compare percutaneous dilation tracheostomy (PDT) with open surgical tracheostomy (ST) in critically ill patients. Patients aged ≥18 years with indication for tracheostomy were included. Thirty patients received PDT and 30 patients received ST. Groups were comparable at baseline.
Kim (2023) performed a randomized controlled trial to assess the safety and efficacy of ultrasound-guided PDT as compared to ST. Adult patients who required prolonged intubation, pulmonary hygiene, airway protection due to neurologic disease or traumatic brain injury, or adjunct tracheostomy to major head and neck surgery or airway obstruction were included. In total, 33 patients underwent PDT and 35 patients received ST. Groups were comparable at baseline.
Pandit (2023) performed a randomized controlled trial to compare PDT to conventional ST. Critically ill adult patients admitted to intensive care unit and subjected to tracheostomy either for prolonged intubation, airway protection or facilitation of weaning from ventilator (ventilator support) or pulmonary hygiene were included. Sixteen patients underwent PDT and sixteen patients underwent ST. Groups were comparable at baseline.
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
Systematic review |
||||||
|
Battaglini, 2022 |
Adult patients with suspected or confirmed SARS-CoV-2 infection who received a tracheostomy during their ICU course
47 studies included (n=5268 patients; mean age=60.1 years) |
Intervention: percutaneous tracheostomy Control: surgical tracheostomy |
Unclear |
Major complications (bleeding) |
One author received consultancy fees. The other authors declare that they have no conflicts of interest. |
High |
|
Brass, 2016 |
Intubated and mechanically-ventilated critically ill participants (children and adults) who required an elective tracheostomy.
20 studies included (n=1652) |
Intervention: percutaneous technique for tracheotomy Control: surgical technique for elective tracheotomy |
Up to 2 years for wound infection
Up to 24 hours for major bleeding |
Major complications (wound infection/stomatitis; major bleeding)
|
No conflicts of interest. None of the studies were funded. |
Some concerns |
|
Individual studies |
||||||
|
Katial, 2024 |
N at baseline Intervention: 30 Control: 30
Age (mean, SD) Intervention: 41 (17.12) years Control: 45.67 (18.01)
Sex (males) Intervention: 16 (53.33%) Control: 17 (56.67%) |
Intervention: Percutaneous dilation tracheostomy, Control: Surgical tracheostomy |
Not exactly mentioned; till the patient was discharged, died or transferred to another facility. |
Major complications (bleeding, infection) |
No financial support/sponsorship. There are no conflicts of interest. |
Some concerns |
|
Kim, 2023 |
N at baseline Intervention: 33 Control: 35
Age (mean ± SD) Intervention: 65.6 ± 13.8 years Control: 67.7 ± 13.7 years
Sex (males) Intervention: 21 (60%) Control: 20 (60.1%) |
Intervention: Ultrasound-guided percutaneous dilation tracheostomy, Control: Surgical tracheostomy |
At least 3 months |
Major complications (bleeding, infection) |
This research was supported by the Soonchunhyang University Research Fund, the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (Grant no. 2017R1C1B5018147). No potential conflict of interest relevant to this article was reported. |
Some concerns |
|
Pandit, 2023 |
N at baseline Intervention: 16 Control: 16
Age (mean ± SD) Intervention: 48.2 ± 15.3 years Control: 50.6 ± 18.4 years
Sex (males) Intervention: 9 (56.25%) Control: 8 (50%) |
Intervention: Percutaneous dilation tracheostomy, Control: Surgical tracheostomy |
Unclear |
Major complications (bleeding, infection), stenosis |
This research did not receive any grants from funding agencies in the public, commercial or not-for-profit sector. There is no competing interest among the authors and are solely responsible for the content and writing of the paper. |
High (complications, stenosis) |
*For further details, see risk of bias table in the appendix
Results
1. Successful tracheostomy placement (critical)
Not reported.
2. Major complications (critical)
2.1. Intraoperative serious, life-threatening adverse events
Brass (2016) included twelve studies that reported intraoperative serious, life-threatening adverse events (Figure 1). This consisted of: major vascular injury or excessive bleeding (determined by the need for blood transfusion or an additional surgical procedure), tracheal or esophageal injury (detected by intraoperative bronchoscopy), loss of the airway (loss of the tube or tracheostomy cannula > 20 sec) or a misplaced airway (paratracheal insertion of the tube or the tracheostomy cannula), a severe hypoxic episode, or cardiac arrest. In total, 26 of the 634 patients (4.1%) who underwent percutaneous dilatational tracheostomy (PDT) had an intraoperative serious, life-threatening event as compared to 25 of the 577 patients (4.3%) who underwent surgical tracheostomy (ST) (RR=0.96, 95%CI 0.47 to 1.97). This difference is not clinically relevant.
2.2. Direct postoperative serious, life-threatening adverse events
Brass (2016) included ten studies that reported direct postoperative serious, life-threatening adverse events (Figure 1). This consisted of: major vascular injury or excessive bleeding (determined by the need for blood transfusion or an additional surgical procedure), a severe hypoxic episode, or saturation < 90%. In total, 19 of the 496 patients (3.8%) who underwent PDT had an intraoperative serious, life-threatening event as compared to 27 of the 488 patients (5.5%) who underwent ST (RR=0.66, 95%CI 0.30 to 1.45). This difference is clinically relevant favoring PDT.
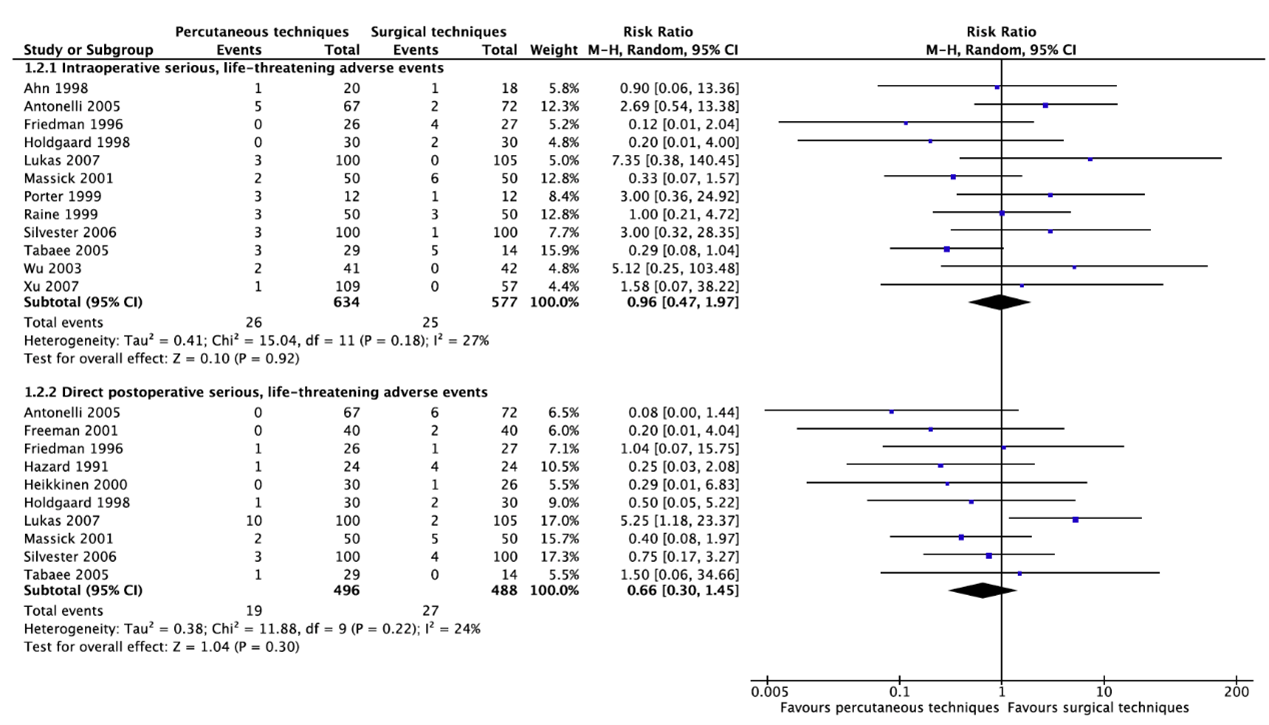
Figure 1. Intraoperative and direct postoperative serious life-threatening adverse events
2.3 Significant infection
Fifteen studies reported infection (Figure 2). Twenty-one of the 542 patients (3.9) who underwent PDT had an infection as compared to 89 of the 554 patients (16.1%) who underwent ST (RR=0.29, 95%CI 0.18 to 0.45). This difference is clinically relevant favoring PDT.
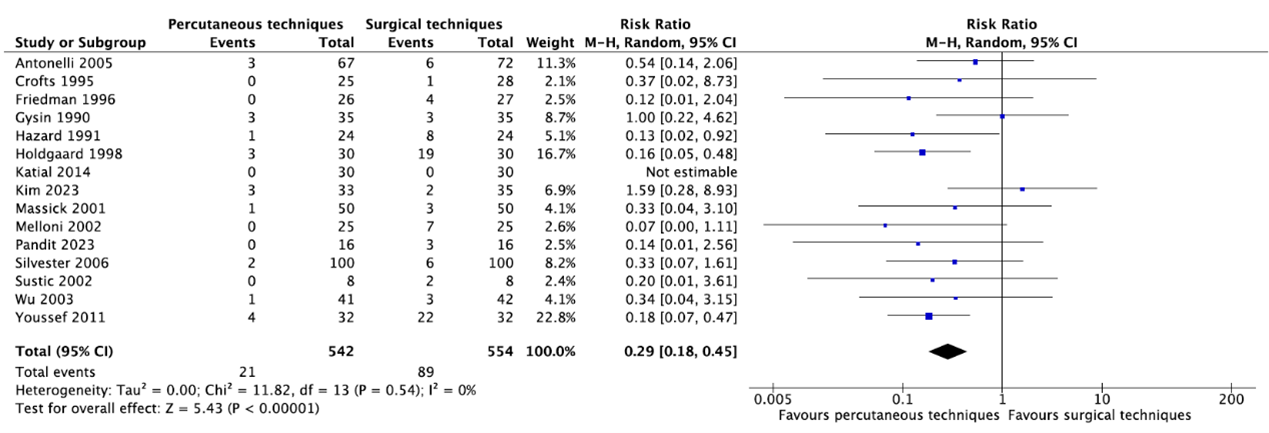
Figure 2. Infection
2.4 Postoperative bleeding
Fifteen studies reported postoperative bleeding (Figure 3). Thirty-two of the 575 patients (5.6%) who underwent PDT had postoperative bleeding as compared to 45 of the 569 patients (7.9%) who underwent ST (RR=0.62, 95%CI 0.31 to 1.23). This difference is clinically relevant favoring PDT.
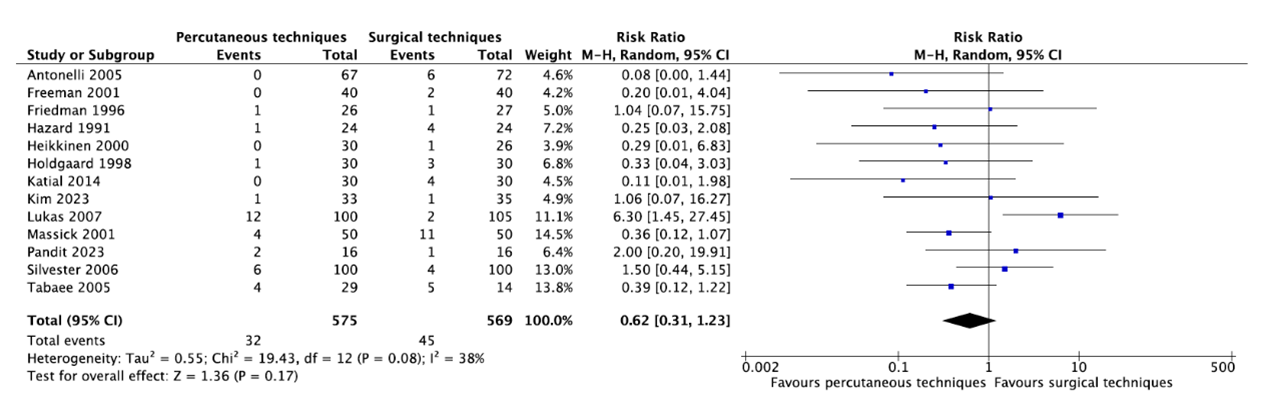
Figure 3. Postoperative bleeding
COVID-19
Battaglini (2022) reported no differences in bleeding between PDT and ST (5.6% [95%CI: 2.0 to 9.1] versus 6.9% [95%CI: -1.6 to 15.4]; P=0.83; OR=0.9 [95%CI: 0.6 to 1.4]) for patients with COVID-19. Since no data was available about the number of participants, no GRADE assessment could be performed.
2.5 Procedural bleeding
Kim (2023) reported procedure-related estimated blood loss. Patients who underwent ultrasound-guided PDT had an estimated blood loss of 2.7 mL (SD=2.8) as compared to 2.1 mL (SD=2.1) for patients who underwent ST (MD=0.60 mL; 95%CI -0.58 to 1.78). This difference is not clinically relevant.
Pandit (2023) reported minimal and moderate peri-operative hemorrhage (not defined). Ten of the 16 patients (62.5%) who underwent PDT had minimal peri-operative hemorrhage as compared to 11 of the 16 patients (68.8%) who underwent ST (RR=0.91, 95%CI 0.55 to 1.50). Six of the 16 patients (37.5%) who underwent PDT had moderate peri-operative hemorrhage as compared to 5 of the 16 patients (31.3%) who underwent ST (RR=1.20, 95%CI 0.46 to 3.15). These differences were not clinically relevant.
2.6 Air leakage
Not reported.
2.7Airway loss
Not reported.
3. Tracheomalacia (important)
Not reported.
4. Stenosis (important)
Pandit (2023) reported that 1 of the 16 patients (6.3%) who underwent PDT had a tracheal stenosis, while this did not occur in patients who underwent ST.
A systematic review of the literature was performed to answer the following question(s):
What are the effectiveness and complications of percutaneous tracheostomy placement in adult patients admitted to the ICU compared to surgical tracheostomy placement?
Table 1. PICO
| Patients | Adult patients admitted to the ICU who are intubated and who are going to have a tracheostomy placed |
|
Intervention |
Percutaneous dilatational tracheostomy (PDT) |
| Controle | Surgical tracheostomy (ST) |
| Outcomes | Successful tracheostomy placement, major complications, tracheomalacia, stenosis |
| Other selection criteria |
Study design: systematic reviews, randomized controlled trials and observational studies More than 10 patients per arm |
Relevant outcome measures
The guideline panel considered successful tracheostomy placement and major complications as critical outcome measures for decision making; and tracheomalacia and stenosis as important outcome measures for decision making.
The guideline panel defined the outcome measure ‘major complications’ as follows: airway loss, intraoperative and direct significant postoperative bleeding, significant hypoxia, a misplaced airway, pneumothorax, cardiac arrest, air leakage and significant infection. For the other outcomes, the guideline panel did not define the outcome measures but used the definitions used in the studies.
The guideline panel defined 25% difference (RR <0.8 to >1.25) for dichotomous and 0.5 SD for continuous outcomes as a minimal clinically (patient) important difference.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2000 until the 2nd of August 2024. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 636 hits. Studies were selected based on the following criteria:
- The study population had to meet the criteria as defined in the PICO
- The intervention had to meet the criteria as defined in the PICO
- Research type: systematic review, randomized-controlled trials or observational studies
- Articles written in English
- More than 10 patients per arm
Initially, 327 studies were selected based on title and abstract screening. First, the systematic reviews were screened. After reading thirteen systematic reviews in full text, eleven studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and two systematic reviews were included (Battaglini, 2022; Brass, 2016). Then, the randomized controlled trials were screened from the search date of Brass 2016. After reading three randomized controlled trials in full text, no study was excluded and three studies were included (Katial, 2024; Kim, 2023; Pandit, 2023).
- Battaglini D, Premraj L, White N, Sutt AL, Robba C, Cho SM, Di Giacinto I, Bressan F, Sorbello M, Cuthbertson BH, Bassi GL, Suen J, Fraser JF, Pelosi P. Tracheostomy outcomes in critically ill patients with COVID-19: a systematic review, meta-analysis, and meta-regression. Br J Anaesth. 2022 Nov;129(5):679-692. doi: 10.1016/j.bja.2022.07.032. Epub 2022 Aug 3. PMID: 36182551; PMCID: PMC9345907.
- Brass P, Hellmich M, Ladra A, Ladra J, Wrzosek A. Percutaneous techniques versus surgical techniques for tracheostomy. Cochrane Database Syst Rev. 2016 Jul 20;7(7):CD008045. doi: 10.1002/14651858.CD008045.pub2. PMID: 27437615; PMCID: PMC6458036.
- Katial T, Shree S, Mishra K, Mishra S, Mustajab MA, Gupta M. Comparison of percutaneous single-stage dilatational tracheostomy and surgical tracheostomy in critically ill patients: A randomized controlled trial. Int J Crit Illn Inj Sci. 2024 Jan-Mar;14(1):9-14. doi: 10.4103/ijciis.ijciis_53_23. Epub 2024 Mar 27. PMID: 38715748; PMCID: PMC11073646.
- Kim SY, Lee SW, Baek A, Park KN. Comparison between Real-Time Ultrasound-guided Percutaneous Dilatational Tracheostomy and Surgical Tracheostomy in critically ill Patients: A Randomized Controlled Trial. Clin Exp Otorhinolaryngol. 2023 Nov;16(4):388-394. doi: 10.21053/ceo.2023.01088. Epub 2023 Sep 25. PMID: 37752796; PMCID: PMC10710929.
- Pandit A, Swami G, Kumar KD. Comparative Study of Percutaneous Dilatational Tracheostomy and Conventional Surgical Tracheostomy in Critically Ill Adult Patients. Indian J Otolaryngol Head Neck Surg. 2023 Sep;75(3):1568-1572. doi: 10.1007/s12070-023-03666-9. Epub 2023 Mar 16. PMID: 37636705; PMCID: PMC10447733.
Beoordelingsdatum en geldigheid
Publicatiedatum : 26-01-2026
Beoordeeld op geldigheid : 26-01-2026
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire cluster ingesteld. Het cluster Intensive Care bestaat uit meerdere richtlijnen, zie hier voor de actuele clusterindeling. De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden geven hun expertise in, indien nodig. De volgende personen uit het cluster zijn betrokken geweest bij de herziening van deze module:
Clusterstuurgroep
- Dr. E.J. Wils, voorzitter, internist-intensivist, Franciscus Gasthuis & Vlietland, Rotterdam
- Dhr. K.H. de Groot, internist-intensivist, Máxima MC, Eindhoven
- Dhr. E.J. van Lieshout, internist-intensivist, Amsterdam UMC, Amsterdam
- Dr. J. van Paassen, internist-intensivist, LUMC, Leiden
- Prof. dr. K. Kaasjager, internist, UMC Utrecht, Utrecht
- Dhr. R.M. Wilting, chirurg-intensivist, Elisabeth-TweeSteden Ziekenhuis, Tilburg
- Mevr. S.J. Bakker, longarts-intensivist, Elkerliek Ziekenhuis, Helmond
- Dhr. R. van Vugt, anesthesioloog-intensivist, Sint Maartenskliniek, Nijmegen
- Dr. S.W.M. de Jong, longarts-intensivist, Franciscus Gasthuis & Vlietland, Rotterdam
Clusterexpertisegroep
- Drs. R.P.J. Segers, longarts-intensivist, MUMC+, Maastricht
- Dr. B.G. Fikkers, intensivist, Radboudumc, Nijmegen
- Dr. Q.L.M. Habes, intensivist, VieCuri Medisch centrum, Venlo
Met ondersteuning van
- Drs. F.M. Janssen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. L. Wesselman, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van de clusterleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Gemelde (neven)functies en belangen stuurgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Gemelde belangen |
Restrictie |
|
Wils |
Intensivist, Franciscus Gasthuis & Vlietland, Rotterdam (betaald) |
MICU-arts Zuidwest Nederland (betaald) Intensivist/arts-onderzoeker, ErasmusMC, Rotterdam (GVO; onbetaald) Lid Richtlijnencommissie NVIC (onbetaald) Taskforce 'Acute Infectiologische Bedreigingen' (onbetaald) Lid commissie kwaliteit NVIC (onbetaald) Lid commissie Wetenschap & Innovatie (onbetaald) Bestuurslid stichting Heilige Geest Huis (onbetaald) |
NORMO2 project (ZonMW projectnummer 10430102110007) Normo2: Niet-invasieve respiratoire ondersteuning bij COVID-19 longfalen: uitkomsten en risicofactoren (geen projectleider)
Beterketen: Harmoniseren, optimaliseren en verbeteren van nazorg na intensive Care behandeling (geen projectleider) |
Geen restricties |
|
Van Paassen |
Instituut: LUMC |
Lid Richtlijnencommissie NVIC (onbetaald) Lid Task force Acute infectiologische bedreigingen (onbetaald) Plaatsvervangend opleider IC (onbetaald) |
ZonMw Sparcs@ICU Antimicrobial steardship programs in the Dutch ICUs: a theory-to-practice Gap analysis, rol als projectleider |
Geen restricties |
|
De Groot |
Instituut: Franciscus Gasthuis & Vlietland Functie: Internist - intensivist Werkzaamheden: Klinisch |
Richtlijn commissie NVIC (onbetaald) Klankbordgroep Richtlijn bloeding tractus digestivus (onbetaald) |
REMAP-CAP, lokale hoofdonderzoeker |
Geen restricties |
|
Van Lieshout |
internist-intensivist, Amsterdam UMC, Intensive Care, locatie AMC |
onbetaald: |
nvt |
Geen restricties |
|
Kaasjager |
internist acute geneeskunde UMCU UU/Gelre 0.8 FTE |
bestuur NVIAG, onbetaald, |
nvt |
Geen restricties |
|
Wilting |
Chirurg-intensivist, Elisabeth-TweeSteden ziekenhuis Tilburg |
Landelijk/extern: Instructeur diverse cursussen (ATLS, HMIMS, basiscursus echografie NVIC) (onkostenvergoeding) Visiteur kwaliteitsvisitatie NVIC (onkostenvergoeding) Regio intensivist IC regio ZWN (geen vergoeding)
Ziekenhuis/intern (allen zonder vergoeding): Medisch Manager IC Tactisch planningsoverleg Kernteam kwaliteit en veiligheid Commissie nieuwbouw acute as Trauma commissie |
Nvt |
Geen restricties |
|
Bakker |
Longarts-intensivist Elkerliek Ziekenhuis Helmond |
Stuurgroeplid & instructeur Bronchoscopie echo thorax en tracheostomie cursus MUMC
Partner is orthopedisch chirurg in JBZ (geen belangenverstrengeling) |
|
Geen restricties |
|
Van Vugt |
Anestesioloog, Sint Maartenskliniek (loondienst) |
Stuurgroep Epilepsie (vacatiegelden) |
|
Geen restricties |
|
De Jong |
Longarts Intensivist ZGT Almelo |
FMS - Netwerk Startend Medisch Specialist - Onebtaald NVIC - Werkgroep arbeidsmarktproblematiek - Onbetaald NVALT - Sectie IC - Onbetaald |
Geen |
Geen restricties |
Gemelde (neven)functies en belangen expertisegroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Gemelde belangen |
Restrictie |
|
Fikkers |
Intensivist Radboudumc |
Geen |
Geen |
Geen restricties |
|
Segers |
Longarts-intensivist MUMC+ |
Regio-intensivist ICUZON (0,2 FTE), betaald door dit IC netwerk |
Geen |
Geen restricties |
|
Habes |
intensivist, VieCuri Medisch centrum |
Geen |
Deelname aan PRAISE studie vanuit Radboud UMC |
Geen restricties |
Gemelde (neven)functies en belangen ondersteuning Kennisinstituut
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Gemelde belangen |
Restrictie |
|
Janssen |
Adviseur Kennisinstituut |
PhD-kandidaat UMCU |
Vader werkzaam als directeur bij EMCM |
Geen restricties |
|
Wesselman |
Senior adviseur Kennisinstituut |
Geen |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerden de clusterleden conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Techniek voor tracheacanule plaatsing |
Geen financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5.000 patiënten) en zal daarom naar verwachting geen substantiële financiële gevolgen hebben voor de collectieve uitgaven. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.