Zeer premature partus (24-32 weken) bij eenlingzwangerschap in stuitligging
Uitgangsvraag
Heeft een primaire sectio of een vaginale baring de voorkeur bij een kind in stuitligging in de premature periode bij zwangeren met eenlingzwangerschap?
De uitgangsvraag omvat de volgende deelvraag:
Welke modus partus (vaginale partus of electieve sectio caesarea) dient geadviseerd te worden bij een zeer premature partus (24-32 weken) bij eenlingzwangerschap in stuitligging?
Aanbeveling
Licht patiënten met een (dreigende) vroeggeboorte van een kind in stuitligging tussen 24 en 32 weken voor over de voor- en nadelen van een sectio caesarea versus een vaginale partus voor de huidige en volgende zwangerschap om te komen tot een individuele afweging van de modus partus. Benoem hierbij in ieder geval de kans op perinatale sterfte, de maternale risico’s en de consequenties voor een volgende zwangerschap.
Bespreek ook dat de (veranderende) omstandigheden rond de geboorte kunnen maken dat de aanvankelijk geplande manier van bevallen op dat moment misschien niet meer wenselijk of haalbaar is.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
In de literatuuranalyse is onderzocht of een geplande primaire sectio of een vaginale baring de voorkeur heeft bij een kind in stuitligging in de premature periode bij zwangere vrouwen met eenlingzwangerschap, waarbij sprake is van een dreigende vroeggeboorte. Er is één systematische review van RCTs (Alfirevic, 2013) gevonden en er zijn daarnaast nog 15 observationele studies geïncludeerd (waarvan 8 met intention-to-treat analyse). Voor een zwangerschapsduur tussen de 24 en 32 weken vergeleken één RCT en dertien observationele studies een primaire sectio met een vaginale baring. Voor een zwangerschapsduur tussen de 32 en 37 weken vergeleken zes observationele studies een primaire sectio met een vaginale baring. Voor beide termijnen werd de bewijskracht voor de cruciale uitkomstmaten perinatale sterfte, asfyxie en postpartum bloeding >1000cc beoordeeld als zeer laag vanwege methodologische beperkingen, verschillen in de studiepopulatie en spreiding in het gevonden effect. Ook voor de belangrijke uitkomstmaten was de bewijskracht zeer laag.
Na onze literatuurselectie is een nieuwe systematische review gepubliceerd over dit onderwerp (Unger 2024). Deze studie onderzocht de relatie tussen de geplande en daadwerkelijke wijze van bevalling, neonatale sterfte en kortetermijnuitkomsten bij zwangerschappen tot 32 weken. Daarnaast werd een subgroepanalyse uitgevoerd, waaruit bleek dat premature eenlingen in stuitligging een significant lagere sterftekans hadden bij een sectio caesarea, zowel in de groep met een geplande sectio (OR 0,56; 95% CI 0,32-0,98) als in de groep waarin de sectio daadwerkelijk werd uitgevoerd (OR 0,34; 95% CI 0,13-0,88).
De review van Unger is vergeleken met onze literatuuranalyse. Het belangrijkste verschil ligt in de onderzochte populatie: Unger includeerde zowel eenling- als tweelingzwangerschappen en zowel hoofd- als stuitliggingen, terwijl onze analyse zich specifiek richtte op eenlingzwangerschappen in stuitligging. Alle relevante studies over eenlingen in stuitligging uit de review (zie sectie 4.4.1.c, pagina 14) zijn ook in onze analyse opgenomen. In tegenstelling tot Unger hebben wij observationele studies niet samengevoegd, vanwege te grote onderlinge verschillen.
Bij neonaten geboren in stuitligging tussen 24-32 weken wordt in de literatuur meer perinatale mortaliteit en asfyxie (gedefinieerd als Apgar score <7 op 5 minuten of pH <7.05) en minder bloedverlies gerapporteerd na een vaginale baring dan na een sectio caesarea. Hierbij moet worden opgemerkt dat de definitie van asfyxie, waarbij er kans is op lange termijn gevolgen voor de neonaat, tegenwoordig anders is (oa een Apgar-score <4 na 5 minuten). De bewijskracht voor alle uitkomsten is echter zeer laag en is grotendeels gebaseerd op uitkomsten van retrospectieve cohort studies en per protocol analyses in plaats van de geplande modus partus. Dit zou kunnen leiden tot vertekening van de resultaten; het is enerzijds niet ondenkbaar dat de uitkomsten van een geplande sectio in geval van een vroeggeboorte bij een stuitligging tussen 24-32 weken beter zijn voor het kind dan na een geplande vaginale baring. In geval van per protocol analyse zou dit de resultaten van in de sectiogroep ten onrechte kunnen verslechteren. Anderzijds laat de studie van van Bergen-Henegouwen (2015) geen verschillen zien in de neonatale uitkomsten tussen een geplande sectio en een secundaire sectio caesarea. Slechtere perinatale uitkomsten bij een vaginale baring lijken vooral gerelateerd te zijn aan problemen bij de geboorte van het nakomend hoofd. Het optreden hiervan is echter zeer zeldzaam en moet worden afgewogen tegen de mogelijke (lange termijn) gevolgen voor de moeder die het gevolg zijn van een (premature) sectio caesarea, zoals bijvoorbeeld bloedverlies of kans op een uterusruptuur of abnormale invasie van de placenta in een volgende zwangerschap. Het is niet bekend of deze risico’s hoger zijn bij een preterme sectio caesarea dan bij een aterme sectio caesarea. Voor de counseling wordt verwezen naar de richtlijn Beleid bij sectio in voorgeschiedenis.
Het gebrek aan bewijskracht impliceert de noodzaak van een grote prospectief gerandomiseerde studie. Echter aangezien mondiaal bij de meerderheid van de (premature) stuitbevallingen een primaire sectio caesarea wordt verricht lijkt een dergelijke studie niet haalbaar. Een groot prospectief cohort onderzoek zou waarschijnlijk het meest haalbare alternatief zijn.
In de Term breech Trial werden bij vaginale stuitbevallingen minder nadelige neonatale uitkomsten gezien bij patiënten van ervaren zorgverleners dan bij onervaren zorgverleners.
Zorgverleners werden hierbij geclassificeerd als “ervaren” als zij zowel door henzelf als door het hoofd van de afdeling als zodanig werden aangemerkt., Onervaren zorgverleners hadden echter soms meer dan 20 jaar klinische ervaring. Het ‘ervaren voelen’ lijkt dus de uitkomsten van a terme stuitbevallingen te beïnvloeden, en dit kan ook het geval zijn bij premature stuitbevallingen. Begrijpen waarom sommige verloskundige zorgverleners zich ervaren voelen en anderen met hetzelfde aantal klinische jaren niet, is waarschijnlijk de sleutel tot adequate trainingsprogramma's (Su, 2003).
Samenvattend is er onvoldoende bewijs om routinematig een primaire sectio caesarea te adviseren bij een premature partus tussen 24 en 32 weken. Gezien het mogelijke voordeel van een primaire sectio caesarea ten aanzien van neonatale mortaliteit en asfyxie (Apgar score <7 na 5minuten of ph<7.05) zullen individueel meer factoren meegewogen dienen te worden in de counseling van de patiënt, zoals het effect van een sectio caesarea op een volgende zwangerschap en de voorkeuren van de patiënt. Daarnaast dient het verloop van huidige en vorige zwangerschap(pen) en/of baring(en) en andere complicerende factoren, zoals groeivertraging en de reden van of indicatie voor de premature partus meegewogen te worden. Bovendien moet ook gewaakt worden voor het te vroeg verrichten van een sectio caesarea, terwijl dan tegelijkertijd het risico bestaat op een onverwacht snelle progressie van de baring. Gezien de omstandigheden kan een vaginale baring dan alsnog wenselijker of zelfs onontkoombaar zijn. Voor nuancering en uniformering waar mogelijk tijdens de counseling zie bijlage samenvattingstabel. Voor de extreme prematuren (24-26 weken) verwijzen wij ook naar de richtlijn Perinataal beleid bij Extreme vroeggeboorte.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Het is de taak van de zorgverlener om met de patiënt de individuele omstandigheden en risico’s af te wegen om te komen tot een goede keuze. Factoren als het maternale operatierisico, de gezinssamenstelling en de obstetrische toekomst zouden hierin meegewogen moeten worden. Er is geen bewijs dat een sectio caesarea tot betere uitkomsten zou leiden dan een vaginale baring en het is van belang dat dit wordt besproken met de patiënt. Indien de patiënt de keuze krijgt tussen een primaire sectio caesarea en een vaginale baring in het geval van een partus prematurus bij stuitligging, zal de individuele perceptie over de voordelen versus de nadelen van beiden dan ook een grote rol spelen in de uiteindelijke keuze.
Kosten (middelenbeslag)
Het lijkt aannemelijk dat met een vaginale partus minder kosten gemoeid zijn dan met een sectio caesaera en dat, in het kader van gezond leven binnen planetaire grenzen (milieu-impact), een vaginale partus waarschijnlijk een betere keuze is.
Er is op grond van de literatuur echter geen goede uitspraak te doen over het verschil in kosten bij een premature vaginale stuitbevalling en een premature primaire sectio. Met name bij partus < 32 weken zullen de kosten van de opname waarschijnlijk vooral bepaald worden door de opnameduur van het kind op de NICU of kinderafdeling.
Aanvaardbaarheid, haalbaarheid en implementatie
Zowel een vaginale baring als een primaire sectio caesarea zijn in Nederland reguliere behandelopties. Er is wel sprake van grote praktijkvariatie, zowel bij stuitbevallingen in het algemeen als bij premature stuitbevallingen. Het lijkt aannemelijk dat de ervaring van zorgverleners hierbij ook een belangrijke rol speelt. Het is van groot belang dat er zoveel mogelijk gestreefd wordt naar kansengelijkheid voor iedere vrouw, in iedere regio. De werkgroep is van mening dat het essentieel lijkt om te zorgen voor adequate scholing van de zorgverleners om hun vaardigheden rondom een vaginale stuitpartus op peil te houden; echter de literatuur om te komen tot een harde aanbeveling hoe deze trainingen uit zouden moeten zien, is beperkt. Begrijpen waarom sommige verloskundige zorgverleners zich ervaren voelen en anderen met hetzelfde aantal klinische jaren niet, is waarschijnlijk de sleutel tot adequate trainingsprogramma's. Voor het goed en veilig kunnen begeleiden van een stuitbevalling is hands-on training en bijhouden van de laatste literatuur op dit gebied essentieel.
Onderbouwing
De incidentie van stuitligging in preterme zwangerschappen is veel hoger dan a terme. Deze varieert van 47.1%–37.4% bij 22– 26 weken, 29.5%–24.2% bij 27–29 weken, 20.5%–12.5% bij 30–34 weeks tot 3%–4% a terme (Lorthe, 2017). Er bestaat in Nederland een richtlijn voor het beleid bij stuitligging a terme, maar niet voor stuitligging bij prematuriteit. Het beleid ten aanzien van de modus partus in geval van premature stuitligging kent daardoor een grote praktijkvariatie; In sommige klinieken wordt een primaire sectio geadviseerd, in sommige klinieken vindt counseling plaats waarbij de keuze aan de vrouw gelaten wordt en in andere klinieken wordt in principe een vaginale baring nagestreefd. Dit is een onwenselijke situatie.
Het doel van deze richtlijn is om een eenduidig advies te geven omtrent het beleid ten aanzien van modus partus in geval van premature stuitligging en de praktijkvariatie te verminderen.
|
Very low GRADE |
Vaginal delivery may reduce postpartum hemorrhage > 1000 cc when compared with a caesarean section for women giving birth with a singleton pregnancy at a gestational age of 24+0 weeks to 32 weeks with the child in breech position, but the evidence is very uncertain.
Source: (O’Reilly, 2018) |
|
Very low GRADE |
Vaginal delivery may reduce infection when compared with a caesarean section for women giving birth with a singleton pregnancy at a gestational age of 24+0 weeks to 32 weeks with the child in breech position, but the evidence is very uncertain.
Source: (Stohl, 2011) |
|
Very low GRADE |
Caesarean section may reduce perinatal mortality when compared with a vaginal delivery for women giving birth with a singleton pregnancy at a gestational age of 24+0 weeks to 32 weeks with the child in breech position, but the evidence is very uncertain.
Sources: (Alfirevic, 2013; Bergenhenegouwen, 2015; Hills, 2017; Herbst, 2007; Högberg, 2007; Kayem, 2008; Kayem, 2015; Pierre, 2021; Reddy, 2013; Schmidt, 2019; Stohl, 2011; Thomas, 2016) |
|
Very low GRADE |
The evidence is very uncertain about the effect of a caesarean section on asphyxia when compared with a vaginal delivery for women giving birth with a singleton pregnancy at a gestational age of 24+0 weeks to 32 weeks with the child in breech position.
Sources: (Alfirevic, 2013; Gasim, 2008; Kayem, 2008; Kayem, 2015; O’Reilly, 2018; Pierre, 2021; Schmidt, 2019; Stohl, 2011) |
|
Very low GRADE |
The evidence is very uncertain about the effect of a caesarean section on intraventricular hemorrhage when compared with a vaginal delivery for women giving birth with a singleton pregnancy at a gestational age of 24+0 weeks to 32 weeks with the child in breech position.
Sources: (Herbst, 2007; Kayem, 2008; Kayem, 2015; Pierre, 2021; Reddy, 2013; Schmidt, 2019; Stohl, 2011) |
|
Very low GRADE |
The evidence is very uncertain about the effect of a caesarean section on periventricular leukomalacia when compared with a vaginal delivery for women giving birth with a singleton pregnancy at a gestational age of 24+0 weeks to 32 weeks with the child in breech position.
Sources: (Kayem, 2008; Kayem, 2015; Pierre, 2021; Stohl, 2011) |
|
Very low GRADE |
The evidence is very uncertain about the effect of a caesarean section on infant respiratory distress syndrome when compared with a vaginal delivery for women giving birth with a singleton pregnancy at a gestational age of 24+0 weeks to 32 weeks with the child in breech position.
Sources: (Herbst, 2007; Reddy, 2013) |
|
NO GRADE |
No evidence was found regarding the effect of a caesarean section on IC admission, long-term adverse outcomes, uterine rupture in subsequent pregnancy, perinatal mortality in subsequent pregnancy, and maternal mortality in subsequent pregnancy when compared with a vaginal delivery for women giving birth with a singleton pregnancy at a gestational age of 24+0 weeks to 32 weeks with the child in breech position. |
Description of studies
In total, fourteen studies were included in the literature analysis that compared caesarean section with vaginal delivery for women with a premature singleton pregnancy in breech presentation with a gestational age between 24 and 32 weeks (table 1).
Table 1. Study characteristics
|
Study |
Gestational age |
Caesarean section |
Vaginal delivery |
Analysis |
|
Alfirevic 2013 (Penn 1996) |
26+0 to 31+6 weeks |
N=5 (planned) |
N=8 (planned) |
Intention-to-treat |
|
Bergenhenegouwen 2015 |
26+0 to 31+6 weeks |
N=366 |
N=1,125* |
Intention-to-treat |
|
Gasim 2008 |
24+0 to 31+6 weeks |
N=22 |
N=66 |
Per protocol |
|
Hills 2017 |
24+0 to 27+6 weeks |
N=104 |
N=34 |
Per protocol |
|
Herbst 2007 |
25+0 to 27+6 weeks |
N=324 |
N=63 |
Per protocol |
|
Högberg 2007 |
26+0 to 27+6 weeks |
N=54 |
N=12 |
Per protocol |
|
Kayem 2008 |
26+0 to 29+6 weeks |
N=85 (planned) |
N=84 (planned) |
Intention-to-treat |
|
Kayem 2015 |
26+0 to 29+6 weeks |
N=130 (planned) |
N=173 (planned) |
Intention-to-treat |
|
O’Reilly 2018 |
24+0 to 31+6 weeks |
N=113 |
N=56 |
Per protocol |
|
Pierre 2021 |
25+0 to 27+6 weeks |
N=80 (planned) |
N= 113 (n=4 caesarean section) |
Intention-to-treat |
|
Reddy 2013 |
24+0 to 31+6 weeks |
N=529 (planned) |
N=239 (attempted) |
Intention-to-treat |
|
Schmidt 2019 |
24+0 to 31+6 weeks |
N=368 |
N=204 |
Per protocol |
|
Stohl 2011 |
24+0 to 26+6 weeks |
N=39 |
N=26 |
Per protocol |
|
Thomas 2016 |
24+0 to 26+6 weeks |
N=89 |
N=37 |
Per protocol |
* vaginal delivery and emergency caesarean section; N=number of women
Alfirevic (2013) performed a systematic review and meta-analysis to assess the effects of a policy of planned immediate caesarean delivery versus planned vaginal birth for women in preterm labor. Searches were performed in the Cochrane Pregnancy and Childbirth Group’s Trials Register on 5 August 2013. It contains trials identified from the Cochrane Central Register of Controlled Trials, Medline, Embase, hand searches of 30 journals and the proceedings of major conferences, and weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts. No language restrictions were applied.
Inclusion criteria of the systematic review were any randomized trial which compared a policy of planned immediate caesarean delivery versus a policy aiming for vaginal birth for women at high risk of delivering a preterm baby and a study population comprising of women presenting or thought to be in preterm labor (less than 37 weeks), irrespective of fetal presentation. Quasi-randomized controlled trials were not included. Six studies (n=122 women) were included, but only four studies (n=116 women) contributed to the analyses. These studies were randomized controlled trials performed between 1984 and 1996 but were all stopped early. Only one study examined perinatal mortality, and the Apgar score <7 and matched with the predefined PICO (Penn, 1996). Penn (1996) included five women who delivered by caesarean section and eight women who had a vaginal delivery. Analysis was performed by intention-to-treat.
Bergenhenegouwen (2015) performed a retrospective cohort study to assess the association of the intended mode of delivery and perinatal mortality among breech fetuses who are delivered preterm. All women who delivered a singleton fetus in breech presentation between 26+0/7 and 36+6/7 weeks of gestation between 2000 and 2011 were included. Women with a severe maternal comorbidity or who delivered before 26+0/7 weeks of gestation were excluded. Other exclusion criteria were (lethal) congenital abnormalities, antepartum stillbirth, placental abruption (antenatally), unknown gestational age, small for gestational age (defined as a birth weight below the 10th percentile), maternal hypertension (defined as diastolic blood pressure 95 mm Hg or greater), gestational and insulin-dependent diabetes mellitus or non insulin-dependent diabetes mellitus, and preeclampsia (defined as hypertension with proteinuria). A subgroup analysis of women with a gestational age between 26+0 and 31+6 weeks was performed. In total, 366 women delivered by planned caesarean delivery and 1,125 by intended vaginal delivery (vaginal delivery and emergency caesarean section). Analysis was performed by intention to treat. Unknown if groups were comparable at baseline. For this subgroup, only the outcome perinatal mortality was reported.
Gasim (2008) performed a retrospective study to determine the incidence of singleton preterm breech babies born in a teaching hospital, and to study the influence of the mode of delivery on perinatal outcome in preterm births with breech presentation. All singleton breech deliveries between 24 and 36 weeks’ gestation between 1 January 1992 and 31 December 2001 were included. Exclusion criteria were intrauterine fetal death, multiple pregnancies, and lethal congenital fetal malformations. In total, 148 infants were born by vaginal delivery and 47 infants by a caesarean section. Analysis was performed per protocol, by delivery mode. Unknown if groups were comparable at baseline. Measured outcomes were the Apgar score <7, NICU admission, and IVH. For the Apgar score <7, a subgroup analysis of women between 24+0 and 31+6 weeks was available. Twenty-two infants were born by a caesarean section and 66 infants were born by vaginal delivery.
Hills (2017) performed a retrospective cohort study to determine if mode of delivery for singleton extreme preterm breech fetuses is associated with a difference in perinatal mortality, neonatal and maternal morbidity. Singleton breech fetuses between 23+0 to 27+6 weeks gestation between 1 January 2005 and 31 December 2014 were included. Exclusion criteria were multiple births, fetal presentation other than breech (cephalic, oblique, transverse), antepartum death, termination of pregnancy and lethal congenital anomalies. The subgroup of fetuses born before 24 weeks (23+0 to 23+6) were excluded in the literature analysis in order to match with the predefined PICO. In total, 104 caesarean sections and 34 vaginal deliveries were performed. Analysis was performed per protocol, by delivery mode. Groups were not comparable at baseline. Women who delivered by caesarean section had more previous caesarean sections than women who delivered vaginally. Perinatal mortality was measured as outcome.
Herbst (2007) performed a retrospective study to assess the association between mode of delivery and neonatal outcome in singleton pregnancy with breech presentation and preterm birth, due to premature labor and/or PPROM. All singleton preterm live births with breech presentation in (completed) gestational weeks 25 to 36 weeks with a diagnosis of preterm labor and/or PPROM between 1990 and 2002 were included. Pregnancies with a diagnosis of fetal malformations, immunization, fetal hydrops, intrauterine growth retardation, fetal hypoxia, fetal distress, chorioamnionitis, maternal infection or fever, placental abruption, vaginal bleeding, cord complications, uterine rupture, diabetes mellitus, gestational diabetes and eclampsia were excluded. A subgroup analysis of women between 25+0 and 27+6 weeks was available. In total, 324 caesarean sections and 63 vaginal deliveries were included. Analysis was performed per protocol, by delivery mode. Unknown if groups were comparable at baseline. Measured outcomes were IRDS, IVH and perinatal mortality.
Högberg (2007) performed a retrospective cohort study to analyze infant mortality among infants born extremely preterm in relation to mode of delivery, maternal diagnosis, and different institutional policies. Live-born infants delivered at 23+0 to 27+6 weeks of gestation at 7 tertiary health care hospitals with level III neonatal intensive care units (NICUs) between 1990 and 2002 were included. Children born in non-tertiary health care hospitals or children born to mothers with pre-eclampsia/eclampsia were excluded. Only a subgroup analysis of infants with a breech position during labour born at 26 or 27 weeks could be included (otherwise infants born below 24 weeks were also included). In total, 54 infants were born by a caesarean section and 12 infants by a vaginal delivery. Analysis was performed per protocol, by delivery mode. Unclear if groups were comparable at baseline. Perinatal mortality was the outcome of interest.
Kayem (2008) performed a retrospective study to compare neonatal death rates for preterm singleton breech deliveries in units with a policy of either PVD or PCD. Women with singleton pregnancies who were admitted for preterm labor with or without PPROM who gave birth between 26 weeks and 29 weeks 6 days of gestation from 1999 through 2005 were included. Cases with intrauterine growth restriction, preeclampsia, lethal congenital abnormalities, fetal death, placenta previa, or placental abruption were excluded. In total, 84 deliveries occurred under PVD policies and 85 deliveries under PCD policies. Analysis was performed by intention to treat. Groups were comparable at baseline. Measured outcomes were the Apgar score <7, perinatal mortality, periventricular leukomalacia, and intraventricular hemorrhage (IVH) grade 3 or 4.
Kayem (2015) performed a retrospective cohort study to compare neonatal morbidity and mortality rates in preterm singleton breech deliveries in centers with a policy of either planned vaginal delivery (PVD) or planned cesarean delivery (PCD). Women with singleton pregnancies admitted for preterm labor with or without PPROM and who gave birth between 26+0/7 and 29+6/7 from 1999 through 2010 were included. Cases in which the mother or fetus had diseases that might have increased neonatal mortality or morbidity (such as intrauterine growth restriction, preeclampsia, lethal congenital abnormalities, fetal death before labor, placenta previa, or placental abruption) or neonates delivered before 26 weeks or after 30 weeks were excluded. In total, 130 women delivered by PCD and 173 women by PVD. Analysis was performed by intention to treat. Groups were comparable at baseline. Measured outcomes were the Apgar score <7, PVL, IVH grade 3 or 4 and perinatal mortality.
O’Reilly (2018) performed a retrospective cohort study to compare outcomes of breech presenting preterm infants according to mode of delivery. All singleton preterm breech deliveries (<37-week gestation) from 1 January 2001 to 31 December 2011 were included. Stillbirths and lethal congenital anomalies were excluded. In total, 305 infants were born by a lower segment caesarean section and 108 infants were born by a vaginal delivery. A subgroup analysis of women between 24+0 and 31+6 weeks of gestation was performed. In total, 113 infants were born with a caesarean section and 56 infants were born by a vaginal delivery. Analysis was per protocol, by delivery mode. It was unknown if groups were comparable at baseline. Measured outcomes were the Apgar score <7 and postpartum hemorrhage.
Pierre (2021) performed a retrospective study to compare mortality associated with planned vaginal delivery (PVD) of fetuses in breech presentation with that of fetuses in breech presentation with a planned cesarean delivery (PCD). Women with a singleton pregnancy in breech or cephalic presentation who gave birth between 25+0 weeks and 27+6 weeks of gestation by vaginal or caesarean delivery to a liveborn infant with a birth weight of at least 500 grams from the start of 1997 to the end of 2015 were included. Other presentations, medically indicated terminations of pregnancy, fetal deaths, fetuses with congenital malformation, and pregnancies involving imminent threats to the mother or fetus justifying an emergency caesarean (e.g., eclampsia or placental abruption) were excluded. In total, 113 women had a fetus in breech PVD (of which four had a caesarean section during labor) and 80 women had a breech PCD. Analysis was performed by intention to treat. Groups were not comparable at baseline. Women delivered by caesarean section were older and had more previous caesarean sections than women in the vaginal delivery group. Measured outcomes were the Apgar score <7, perinatal mortality, IVH grade 3-4, and leukomalacia ≥3 or hyperechogenicity > 10 days.
Reddy (2013) performed a retrospective cohort study to assess neonatal outcomes in early preterm births by mode of planned delivery. All singleton deliveries between 24+0/7 and 31+6/7 weeks of gestation were included. Analysis was performed by intention to treat. Exclusion criteria were pregnancies complicated by fetal distress, placenta previa, abruption, antepartum stillbirth, and major anomalies. In total, 529 planned caesarean sections (n=265 between 24 and 27 weeks, and n=264 between 28 and 31 weeks) and 239 attempted vaginal deliveries (n=123 between 24 and 27 weeks, and n=116 between 28 and 31 weeks) were included. Groups were not comparable at baseline. Measured outcomes were perinatal mortality, IVH, and IRDS.
Schmidt (2019) performed a retrospective cohort study to determine neonatal outcomes for singleton breech infants by mode of delivery in a European cohort. Live born infants in a breech position with spontaneous onset of labor or PPROM from 24+0 to 31+6 weeks gestational age were included between March and July 2011. Births before 24 weeks of gestational age, severe congenital anomalies, multiple pregnancies, out-of-hospital deliveries, missing mode of delivery, situations in which caesarean section is indicated or strongly recommended (including preeclampsia, eclampsia, and HELLP), diagnosis of severe fetal growth restriction, caesarean section for maternal conditions, and other conditions for which caesarean section is indicated were exclusion criteria. In total, 368 infants were born by a caesarean delivery and 204 infants by a vaginal delivery. Analysis was performed per protocol, by delivery mode. Groups were not comparable at baseline. Measured outcomes were perinatal mortality, the Apgar score <7 and IVH 3-4/cPVL.
Stohl (2011) performed a retrospective study to compare the short-term maternal and neonatal outcomes of very low birth weight breech singletons by mode of delivery. Women with singleton pregnancies in breech position who delivered between 24+0/7 and 26+6/7 weeks’ gestation between 1 January 2000 to 31 December 2008 were included. Exclusion criteria were multiple gestations, pregnancies with intrauterine fetal death, fetuses with major congenital anomalies, fetuses in whom comfort of care only measures were planned pre-delivery. In total, 26 women delivered by spontaneous vaginal delivery and 39 women delivered by a caesarean section. Analysis was performed per protocol, by delivery mode. Groups were not comparable at baseline. Measured outcomes were the Apgar score <7, IVH, PVL, perinatal mortality, and infection.
Thomas (2016) performed a retrospective cohort study to assess whether neonatal survival or maternal outcomes were affected by the decision to perform a caesarean section between 23+0 and 26+6-weeks’ gestation. All liveborn neonates born between 23+0 and 26+6 weeks’ gestation with a prenatally determined plan for active resuscitation between January 1998 and December 2009 were included. Exclusion criteria were intended palliation, intrauterine fetal demise, known lethal fetal condition and known major congenital anomaly. In total, 89 infants in breech presentation were born by a caesarean section and 37 infants were delivered vaginally. Analysis was performed per protocol, by delivery mode. It was unknown if groups were comparable at baseline since no demographic factors were shown for the subgroup singletons in breech presentation. Perinatal mortality was derived from neonatal survival.
Results
1. Postpartum hemorrhage > 1000 cc (critical)
O’Reilly (2018) reported maternal blood loss >1000 mL. For women undergoing a caesarean section, 6 of the 113 women (5%) had a blood loss >1000 mL, while this did not occur in women who delivered vaginally (RR=6.50, 95%CI 0.37 to 113.37). This difference was clinically relevant favoring vaginal delivery.
2. IC admission (important)
Not reported.
3. Infection (important)
Stohl (2011) reported postpartum infection. Ten of the 39 women (26%) who underwent a caesarean section had an infection as compared to one of the 26 women (4%) who delivered vaginally (RR=6.67, 95%CI 0.91 to 49.01). This difference is clinically relevant favoring vaginal delivery.
4. Perinatal mortality (critical)
Twelve studies reported perinatal mortality, consisting of perinatal death and neonatal death.
Alfirevic (2013) included one study that assessed perinatal mortality (Penn, 1996). Penn (1996) reported no deaths after a caesarean section as compared to 1 of the 8 infants (12.5%) who were delivered vaginally (RD=-0.13, 95%CI -0.45 to 0.20). This difference is clinically relevant favoring caesarean section.
Bergenhenegouwen (2015) reported perinatal mortality. Twenty of the 366 infants (5%) born with a caesarean section had died as compared to 81 of the 1,125 infants (7%) born vaginally (RR=0.76, 95%CI 0.47 to 1.22). This difference is clinically relevant favoring caesarean section.
Hills (2017) reported perinatal mortality, defined as intrapartum stillbirths and neonatal deaths during nursery admission. Twenty of the 104 infants (19%) born with a caesarean section had died as compared to 16 of the 34 infants (47%) born vaginally (RR=0.41, 95%CI 0.24 to 0.70). This difference is clinically relevant favoring caesarean section.
Herbst (2007) reported neonatal death defined as death between 0 and 27 days. Thirty-one of the 324 infants (10%) born with a caesarean section had died as compared to 20 of the 63 infants (32%) born vaginally (RR=0.30, 95%CI 0.18 to 0.49). This difference is clinically relevant favoring caesarean section.
Högberg (2007) reported infant mortality (not defined). Thirteen of the 54 infants (24.1%) born with a caesarean section had died as compared to 5 of the 12 infants (41.7%) born vaginally (RR=0.25, 95%CI 0.25 to 1.31). This difference is clinically relevant favoring caesarean section.
Kayem (2008) reported neonatal death (not defined). Six of the 85 infants (7%) born with a caesarean section had died as compared to 9 of the 84 infants (11%) born vaginally (RR=0.66, 95%CI 0.25 to 1.77). This difference is clinically relevant favoring caesarean section.
Kayem (2015) reported newborn hospital death (fetal death before labor excluded). Fifteen of the 130 infants (12%) born with a caesarean section had died as compared to 28 of the 173 infants (16%) born by a vaginal delivery (RR=0.71, 95%CI 0.40 to 1.28). This difference is clinically relevant favoring caesarean section.
Pierre (2021) reported neonatal mortality, defined as death in the delivery room or in the NICU. Six of the 77 infants (8%) born with a caesarean section had died as compared to 22 of the 113 (20%) infants born vaginally (RR=0.40, 95%CI 0.17 to 0.94). This difference is clinically relevant favoring caesarean section.
Reddy (2013) reported mortality, defined as intrapartum death and neonatal death (not further defined). Thirty-nine of the 529 infants (7%) born with a caesarean section had died as compared to 38 of the 239 infants (16%) born vaginally (RR=0.46, 95%CI 0.30 to 0.71). This difference is clinically relevant favoring caesarean section.
Schmidt (2019) reported mortality including labour ward deaths and deaths in the neonatal units until discharge from hospital. Forty-one of the 368 infants (11%) born with a caesarean section had died as compared to 61 of the 204 infants (30%) born vaginally (RR=0.37, 95%CI 0.26 to 0.53). This difference is clinically relevant favoring caesarean section.
Stohl (2011) reported neonatal death before discharge. Eight of the 39 infants (21%) born with a caesarean section had died as compared to 7 of the 26 infants (27%) born vaginally (RR=0.76, 95%CI 0.31 to 1.85). This difference is clinically relevant favoring caesarean section.
Thomas (2016) reported neonatal survival for nonfootling breech infants, from which neonatal mortality is derived. Thirty-one of the 89 infants (35%) born with a caesarean section had died as compared to 21 of the 37 infants (57%) by vaginal delivery (RR=0.61, 95%CI 0.41 to 0.92). This difference is clinically relevant favoring caesarean section.
5. Asphyxia (critical)
5a. Apgar score <7 at five minutes
Alfirevic (2013) included one study that assessed the Apgar score <7 at five minutes (Penn, 1996). Two of the 4 infants (50%) born by a caesarean section had an Apgar score <7 at 5 minutes as compared to 2 of the 8 infants (25%) born by vaginal delivery (RR=2.0, 95%CI 0.42 to 9.42). This difference is clinically relevant favoring vaginal delivery.
Gasim (2008) reported that 14 of the 22 infants (64%) born by a caesarean section had an Apgar score <7 at 5 minutes as compared to 44 of the 66 infants (67%) born by vaginal delivery (RR=0.95, 95%CI 0.67 to 1.37). This difference is not clinically relevant.
Kayem (2008) reported that 8 of the 83 infants (10%) born by a caesarean section had an Apgar score <7 at 5 minutes as compared to 23 of the 78 infants (30%) born by vaginal delivery (RR=0.33, 95%CI 0.16 to 0.69). This difference is clinically relevant favoring caesarean section.
Kayem (2015) reported that 17 of the 130 infants (13%) born by a caesarean section had an Apgar score <7 at 5 minutes as compared to 44 of the 173 infants (26%) born by vaginal delivery (RR=0.51, 95%CI 0.31 to 0.86). This difference is clinically relevant favoring caesarean section.
O’Reilly (2018) reported that 25 of the 113 infants (22%) born by a caesarean section had an Apgar score <7 at 5 minutes as compared to 23 of the 56 infants (41%) born by vaginal delivery (RR=0.54, 95%CI 0.34 to 0.86). This difference is clinically relevant favoring caesarean section.
Pierre (2021) reported that 15 of the 79 infants (19%) born by a caesarean section had an Apgar score <7 at 5 minutes as compared to 17 of the 95 infants (18%) born by vaginal delivery (RR=1.06, 95%CI 0.57 to 1.99). This difference is not clinically relevant.
Schmidt (2019) reported that 80 of the 354 infants (23%) born with a caesarean section had an Apgar score <7 at 5 minutes as compared to 77 of the 186 infants (41%) born by vaginal delivery (RR=0.55, 95%CI 0.42 to 2.71). This difference is clinically relevant favoring caesarean section.
Stohl (2011) reported that 28 of the 39 infants (72%) born with a caesarean section had an Apgar score <7 at 5 minutes as compared to 14 of the 26 infants (54%) born by vaginal delivery (RR=1.33, 95%CI 0.89 to 2.00). This difference is clinically relevant favoring vaginal delivery.
5b. pH <7.05
O’Reilly (2018) reported that 5 of the 65 infants (7.7%) born with a caesarean section had a cord pH <7.0 as compared to 3 of the 33 infants (9.1%) born by vaginal delivery (RR=0.85, 95%CI 0.22 to 3.33). This difference is clinically relevant favoring caesarean section.
Pierre (2021) reported that 1 of the 68 infants (1.5%) born with a caesarean section had an umbilical artery pH <7.0 as compared to 2 of the 96 infants (2.1%) born by vaginal delivery (RR=0.71, 95%CI 0.07 to 7.63). This difference is clinically relevant favoring caesarean section.
6. Neonatal intensive care unit (NICU) admission (important)
Not reported.
7. Intraventricular hemorrhage (IVH) (important)
Herbst (2007) reported that 23 of the 324 women (7%) undergoing a caesarean section had an infant with IVH as compared to 7 of the 63 women (11%) who delivered vaginally (RR=0.64, 95%CI 0.29 to 1.42). This difference is clinically relevant favoring caesarean section.
Kayem (2008) reported an IVH grade 3 or 4. Five of the 85 infants (6%) born with a caesarean section had an IVH grade 3 or 4 as compared to 5 of the 84 infants (6%) born by a vaginal delivery (RR=0.99, 95%CI 0.30 to 3.29). This difference is not clinically relevant.
Kayem (2015) reported an IVH grade 3 or 4. Seven of the 130 infants (5%) born with a caesarean section had an IVH grade 3 or 4 as compared to 14 of the 173 infants (8%) born by a vaginal delivery (RR=0.67, 95%CI 0.28 to 1.60). This difference is clinically relevant favoring caesarean section.
Pierre (2021) reported an IVH grade 3 or 4. Nine of the 76 infants (12%) born with a caesarean section had an IVH grade 3 or 4 as compared to 8 of the 99 infants (8%) born by a vaginal delivery (RR=1.47, 95%CI 0.59 to 3.62). This difference is clinically relevant favoring vaginal delivery.
Reddy (2013) reported that 90 of the 529 women (17%) undergoing a caesarean section had an infant with IVH as compared to 36 of the 239 women (15%) who delivered vaginally (RR=1.13, 95%CI 0.79 to 1.61). This difference is not clinically relevant.
Schmidt (2019) reported severe intraventricular haemorrhage (IVH), according to Papile Grades III-IV or cystic periventricular leukomalacia (cPVL). Thirty-nine of the 359 infants (11%) born with a caesarean section had an IVH 3-4/cPVL as compared to 40 of the 174 infants (23%) born by vaginal delivery (RR=0.47, 95%CI 0.32 to 0.71). This difference is clinically relevant favoring caesarean section.
Stohl (2011) reported an IVH grade 3 or 4. Five of the 39 infants (13%) born with a caesarean section had an IVH grade 3 or 4 as compared to 8 of the 26 infants (31%) born by a vaginal delivery (RR=0.42, 95%CI 0.15 to 1.13). This difference is clinically relevant favoring caesarean section.
8. Periventricular leukomalacia (PVL) (important)
Kayem (2008) reported that one of the 85 infants (1%) born with a caesarean section had PVL as compared to 5 of the 84 infants (6%) born by a vaginal delivery (RR=0.20, 95%CI 0.02 to 1.66). This difference is clinically relevant favoring caesarean section.
Kayem (2015) reported that 4 of the 130 infants (3%) born with a caesarean section had PVL as compared to 9 of the 173 infants (5%) born by a vaginal delivery (RR=0.59, 95%CI 0.19 to 1.88). This difference is clinically relevant favoring caesarean section.
Pierre (2021) reported leukomalacia ≥ 3 or hyperechogenicity > 10 days. This was the case for 11 of the 72 infants (15%) born with a caesarean section as compared to 17 of the 99 infants (17%) born by a vaginal delivery (RR=0.89, 95%CI 0.44 to 1.78). This difference is not clinically relevant.
Stohl (2011) reported that 5 of the 39 infants (13%) born with a caesarean section had PVL as compared to none of the 26 infants (0%) born by a vaginal delivery (RR=7.42, 95%CI 0.43 to 128.83). This difference is clinically relevant favoring vaginal delivery.
9. Infant Respiratory Distress Syndrome (IRDS) (important)
Herbst (2007) reported that 141 of the 324 infants (44%) born with a caesarean section had infant respiratory distress syndrome as compared to 28 of the 63 infants (44%) who were born by a vaginal delivery (RR=0.98, 95%CI 0.72 to 1.33). This difference is not clinically relevant.
Reddy (2013) reported respiratory distress syndrome. Women undergoing a caesarean section had 389 of the 529 infants (74%) with RDS as compared to 173 of the 239 women who delivered vaginally (72%) (RR=1.02, 95%CI 0.93 to 1.12). This difference is not clinically relevant.
10. Long-term adverse outcome (important)
Not reported.
11. Uterine rupture in subsequent pregnancy (important)
Not reported.
12. Perinatal mortality in subsequent pregnancy (important)
Not reported.
13. Maternal mortality in subsequent pregnancy (important)
Not reported.
Level of evidence of the literature
According to GRADE, observational studies start at a low level of evidence.
The level of evidence regarding the outcome measure postpartum hemorrhage > 1000 cc was downgraded to very low because of methodological limitations (-1, risk of bias) and the 95% confidence interval crossed the lines of no (clinically relevant) difference (-2, imprecision).
The level of evidence regarding the outcome measure infection was downgraded to very low because the upper limit of the 95% confidence interval was >3 times higher than the point estimate (-2, imprecision).
The level of evidence regarding the outcome measure perinatal mortality was downgraded to very low because of differences in the study population (-1, inconsistency) and the 95% confidence interval crossed the lines of no (clinically relevant) difference (-2, imprecision).
The level of evidence regarding the outcome measure asphyxia was downgraded to very low because of methodological limitations (-1, risk of bias), differences in the study population (-1, inconsistency) and the 95% confidence interval crossed the lines of no (clinically relevant) difference (-2, imprecision).
The level of evidence regarding the outcome measure intraventricular hemorrhage was downgraded to very low because of differences in the study population (-1, inconsistency) and the 95% confidence interval crossed the lines of no (clinically relevant) difference (-2, imprecision).
The level of evidence regarding the outcome measure periventricular leukomalacia was downgraded to very low because of differences in the study population (-1, inconsistency) and the 95% confidence interval crossed the lines of no (clinically relevant) difference (-2, imprecision).
The level of evidence regarding the outcome measure infant respiratory distress syndrome was downgraded to very low because of differences in the study population (-1, inconsistency) and the 95% confidence interval crossed the lines of no (clinically relevant) difference (-2, imprecision).
The level of evidence regarding the outcome measures IC admission, NICU admission, long-term adverse outcomes, uterine rupture in subsequent pregnancy, perinatal mortality in subsequent pregnancy, and maternal mortality in subsequent pregnancy were not reported and therefore could not be assessed with GRADE.
A systematic review of the literature was performed to answer the following question:
Gestational age between 24+0 and 31+6 weeks
Which mode of delivery (vaginal delivery or elective caesarean section) should be advised in women in premature labour between 24-32 weeks with a singleton pregnancy and breech presentation?
| P: |
Women giving birth with a singleton pregnancy at a gestational age of 32+0 weeks to 37 weeks with the child in breech position |
| I: | Intended caesarean section |
| C: | Intended vaginal delivery |
| O: |
maternal outcomes: postpartum hemorrhage>1000cc, IC admission, infection neonatal outcomes: perinatal mortality, asphyxia, neonatal intensive care unit (NICU) admission, IVH (intraventricular hemorrhage), PVL (periventricular leukomalacia), IRDS (infant respiratory distress syndrome), long-term adverse outcomeother outcomes: uterine rupture in subsequent pregnancy, perinatal mortality in subsequent pregnancy, maternal mortality in subsequent pregnancy |
Relevant outcome measures
The guideline development group considered postpartum haemorrhage>1000cc, perinatal mortality and asphyxia as critical outcome measures for decision making; and IC admission, infection, NICU admission, IVH, PVL, IRDS and long-term adverse outcome, uterine rupture in subsequent pregnancy, perinatal mortality in subsequent pregnancy, and maternal mortality in subsequent pregnancy as important outcome measures for decision making.
The working group defined the outcome measure asphyxia as Apgar after 5 minute <7 or pH <7.05. Perinatal mortality included perinatal and neonatal death. The outcome measure maternal infection was defined as endometritis or sepsis. For the other outcome measures, the working group did not define the outcome measures listed above but used the definitions used in the studies.
The working group defined a 1% difference for perinatal mortality (RR < 0.99 or > 1.01) and 10% for asphyxia (RR < 0.9 or > 1.1) as a minimal clinically (patient) important difference. For the other outcomes, the GRADE-standard limit of 25% difference for dichotomous outcomes (RR < 0.8 or > 1.25) and 0.5 SD for continuous outcomes was taken as minimal clinically (patient) important difference.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2000 until February, 3rd 2022. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 204 hits. Studies were selected based on the following criteria:
- The study population had to meet the criteria as defined in the PICOs;
- The intervention had to be as defined in the PICOs;
- Research type: systematic review, randomized-controlled trial, or other comparative research;
- Articles written in English or Dutch.
Thirty-one studies were initially selected based on title and abstract screening. After reading the full text, 15 studies were excluded (see the table with reasons for exclusion under the tab Methods), and 16 studies were included.
Results
One systematic review and fifteen retrospective cohort studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 1 and 2 and the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Alfirevic Z, Milan SJ, Livio S. Caesarean section versus vaginal delivery for preterm birth in singletons. Cochrane Database Syst Rev. 2013 Sep 12;2013(9):CD000078. doi: 10.1002/14651858.CD000078.pub3. PMID: 24030708; PMCID: PMC7052739.
- Bergenhenegouwen L, Vlemmix F, Ensing S, Schaaf J, van der Post J, Abu-Hanna A, Ravelli ACJ, Mol BW, Kok M. Preterm Breech Presentation: A Comparison of Intended Vaginal and Intended Cesarean Delivery. Obstet Gynecol. 2015 Dec;126(6):1223-1230. doi: 10.1097/AOG.0000000000001131. PMID: 26551172.
- Gasim TG. Preterm singleton breech delivery in a teaching hospital of saudi arabia: vaginal versus cesarean delivery. J Family Community Med. 2008 May;15(2):65-70. PMID: 23012169; PMCID: PMC3377023.
- Herbst A, Källén K. Influence of mode of delivery on neonatal mortality and morbidity in spontaneous preterm breech delivery. Eur J Obstet Gynecol Reprod Biol. 2007 Jul;133(1):25-9. doi: 10.1016/j.ejogrb.2006.07.049. Epub 2006 Sep 20. PMID: 16996196.
- Hills F, Way M, Sekar R. Mode of delivery for singleton extreme preterm breech fetuses: A 10 year retrospective review from a single tertiary obstetric centre. Aust N Z J Obstet Gynaecol. 2018 Apr;58(2):178-184. doi: 10.1111/ajo.12681. Epub 2017 Aug 11. PMID: 28799276.
- Högberg U, Holmgren PA. Infant mortality of very preterm infants by mode of delivery, institutional policies and maternal diagnosis. Acta Obstet Gynecol Scand. 2007;86(6):693-700. doi: 10.1080/00016340701371306. PMID: 17520401.
- Kayem G, Baumann R, Goffinet F, El Abiad S, Ville Y, Cabrol D, Haddad B. Early preterm breech delivery: is a policy of planned vaginal delivery associated with increased risk of neonatal death? Am J Obstet Gynecol. 2008 Mar;198(3):289.e1-6. doi: 10.1016/j.ajog.2007.10.794. Epub 2008 Feb 1. PMID: 18241827.
- Kayem G, Combaud V, Lorthe E, Haddad B, Descamps P, Marpeau L, Goffinet F, Sentilhes L. Mortality and morbidity in early preterm breech singletons: impact of a policy of planned vaginal delivery. Eur J Obstet Gynecol Reprod Biol. 2015 Sep;192:61-5. doi: 10.1016/j.ejogrb.2015.06.019. Epub 2015 Jun 26. PMID: 26164568.
- Lorthe E, Quere M, Sentilhes L, Delorme P, Kayem G. Incidence and risk factors of caesarean section in preterm breech births: A population-based cohort study. Eur J Obstet Gynecol Reprod Biol. 2017 May;212:37-43. doi: 10.1016/j.ejogrb.2017.03.019. Epub 2017 Mar 10. PMID: 28334569.
- O'Reilly C, Hehir MP, Mahony R. Influence of mode of delivery on outcomes in preterm breech infants presenting in labor. J Matern Fetal Neonatal Med. 2020 Mar;33(5):731-735. doi: 10.1080/14767058.2018.1500542. Epub 2018 Sep 6. PMID: 30001666.
- Pierre C, Leroy A, Pierache A, Storme L, Debarge V, Depret S, Rakza T, Garabedian C, Subtil D. Is vaginal delivery of a fetus in breech presentation at an extremely preterm gestational age associated with an increased risk of neonatal death? A comparative study. PLoS One. 2021 Oct 20;16(10):e0258303. doi: 10.1371/journal.pone.0258303. PMID: 34669715; PMCID: PMC8528279.
- Reddy UM, Zhang J, Sun L, Chen Z, Raju TN, Laughon SK. Neonatal mortality by attempted route of delivery in early preterm birth. Am J Obstet Gynecol. 2012 Aug;207(2):117.e1-8. doi: 10.1016/j.ajog.2012.06.023. Epub 2012 Jun 19. PMID: 22840720; PMCID: PMC3408612.
- Schmidt S, Norman M, Misselwitz B, Piedvache A, Huusom LD, Varendi H, Barros H, Cammu H, Blondel B, Dudenhausen J, Zeitlin J, Weber T; EPICE Research Group. Mode of delivery and mortality and morbidity for very preterm singleton infants in a breech position: A European cohort study. Eur J Obstet Gynecol Reprod Biol. 2019 Mar;234:96-102. doi: 10.1016/j.ejogrb.2019.01.003. Epub 2019 Jan 11. PMID: 30682601.
- Stohl HE, Szymanski LM, Althaus J. Vaginal breech delivery in very low birth weight (VLBW) neonates: experience of a single center. J Perinat Med. 2011 Jul;39(4):379-83. doi: 10.1515/jpm.2011.040. Epub 2011 May 31. PMID: 21627491.
- Su M, McLeod L, Ross S, Willan A, Hannah WJ, Hutton E, et al. Factors associated with adverse perinatal outcome in the Term Breech Trial. Am J Obstet Gynecol. 2003;189: 740–5.
- Thomas PE, Petersen SG, Gibbons K. The influence of mode of birth on neonatal survival and maternal outcomes at extreme prematurity: A retrospective cohort study. Aust N Z J Obstet Gynaecol. 2016 Feb;56(1):60-8. doi: 10.1111/ajo.12404. Epub 2015 Sep 22. PMID: 26391211.
- Toivonen E, Palomäki O, Korhonen P, Huhtala H, Uotila J. Impact of the mode of delivery on maternal and neonatal outcome in spontaneous-onset breech labor at 32+0-36+6 weeks of gestation: A retrospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2018 Jun;225:13-18. doi: 10.1016/j.ejogrb.2018.03.054. Epub 2018 Mar 30. PMID: 29626709.
- Vinkenvleugel DAM, Slutter TJ, van Rheenen-Flach LE, de Sonnaville CMW, Hermsen BB, Velzel J, van Pampus MG. Breech deliveries in OLVG, the Netherlands: A retrospective cohort study of seven years. Eur J Obstet Gynecol Reprod Biol. 2020 May;248:37-43. doi: 10.1016/j.ejogrb.2020.02.031. Epub 2020 Feb 22. PMID: 32193024.
Evidence table for systematic review of RCTs and observational studies (intervention studies)
Research question:
UV2a: Which mode of delivery (vaginal delivery or elective caesarean section) should be advised in a premature (24-32 weeks) singleton pregnancy in breech presentation?
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Alfirevic et al, 2013
[individual study characteristics deduced from Alfirevic et al, 2013] |
SR and meta-analysis of 6 RCTs
Literature search up to August 2013
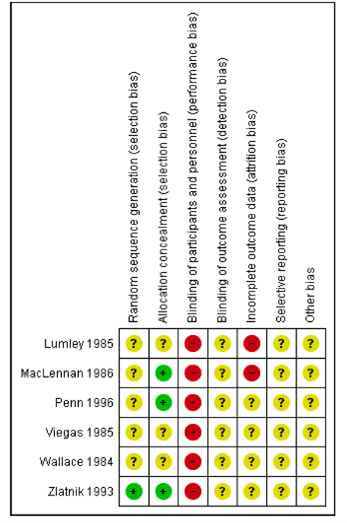
A: Lumley, 1985 B: MacLennan, 1986 C: Penn, 1996 D: Viegas, 1985 E: Wallace, 1984 F: Zlatnik, 1993
Study design: RCTs with parallel groups
Setting and Country: A: Queen Victoria Medical Centre, Melbourne, Australia B: Queen Victoria Hospital, Adelaide, Australia C: 26 centres in England (teaching and district general hospitals) D: 5 large delivery units in Singapore E: Los Angeles County/University of Southern California Medical Center F: University of Iowa Hospitals, USA
Source of funding and conflicts of interest: None known declarations of interest. |
Inclusion criteria SR:
Exclusion criteria SR: - quasi-randomised controlled trials
6 studies included, but 1 study used for literature analysis (Penn, 1996)
Important patient characteristics at baseline: A: 4 women. In labour; single fetus in cephalic or breech presentation between 26-31 weeks; no congenital abnormality at ultrasound examination; no other contraindication to caesarean or vaginal delivery
B: 2 women. Spontaneous labour; cephalic (or breech) presentation between 24-32 weeks; no contraindication to caesarean or vaginal delivery
C: 13 women.
D: 27 women. Single pregnancy; in established preterm labour in breech presentation between 28-36 weeks; no contraindication to caesarean or vaginal delivery; no congenital malformations; no severe pre-eclampsia or IUGR
E: 38 women.
F: 38 women. Unclear if groups were comparable at baseline
|
Describe intervention: A: Spontaneous birth B: Vaginal delivery C: Vaginal delivery D: Vaginal delivery E: Vaginal delivery F: Vaginal delivery
|
Describe control: A: Caesarean section as soon as labour starts B: Elective caesarean section C: Caesarean delivery D: Elective caesarean delivery E: Caesarean delivery F: Caesarean delivery
|
End-point of follow-up: A: Terminated after 5 months B: Not reported (trail terminated in recruitment phase) C: Terminated after 17 months D: Not reported E: Terminated after 6 months F: Terminated after 52 months
For how many participants were no complete outcome data available? 122 women (all studies were stopped early)
|
Asphyxia (defined by trialists) Risk Ratio (M-H, Fixed, 95% CI) 1.63 [0.84, 3.14] favoring vaginal delivery (only study C)
Perinatal death Effect measure: RR [95% CI] C: 0.5 [0.02,10.34] F: 0.22 [0.03,1.73]
Pooled effect: Risk Ratio (M-H, Fixed, 95% CI) 0.28 [0.05, 1.49] favoring caesarean section Heterogeneity (I2): 0%
Apgar score less than seven at five minutes Effect measure: RR [95% CI] C: 2 [0.42,9.42] D: 1.25 [0.09, 17.98] F: 0.49 [0.18,1.33]
Pooled effect: Risk Ratio (M-H, Fixed, 95% CI) 0.74 [0.34, 1.60] favoring caesarean section Heterogeneity (I2): 15.54%
Respiratory distress syndrome Effect measure: RR [95% CI] D: 0.42 [0.05, 3.51] F: 0.62 [0.25, 1.5]
Pooled effect: Risk Ratio (M-H, Fixed, 95% CI) 0.57 [0.25, 1.30] favoring caesarean section Heterogeneity (I2): 0%
Postpartum hemorrhage Effect measure: RR [95% CI] A: not estimatable D: 3.69 [0.16,83.27] F: not estimatable
Risk Ratio (M-H, Fixed, 95% CI) 3.69 [0.16, 83.27] favoring vaginal delivery
Maternal wound infection (outcome not prespecified) Effect measure: RR [95% CI] D: 0.37 [0.02,8.51] F: 3.69 [0.16,83.27]
Pooled effect: Risk Ratio (M-H, Fixed, 95% CI) 1.16 [0.18, 7.70] favoring vaginal delivery Heterogeneity (I2): 4.12%
Other maternal infection (outcome not prespecified) Effect measure: RR [95% CI] D: 3.69 [0.16,83.27] F: 2.5 [0.93,6.73]
Pooled effect: Risk Ratio (M-H, Fixed, 95% CI) 2.63 [1.02, 6.78] favoring vaginal delivery Heterogeneity (I2): 0% |
Author’s conclusion: “Any firm conclusions regarding the relative merits of planned immediate caesarean section versus planned vaginal delivery should not be drawn from this review in order to guide current clinical practice”.
Remarks Six studies were included between 1984 and 1996. Only four studies were used for the analysis, but these were all stopped early. Besides, a lot of unclear or high risk of bias.
Level of evidence: GRADE NO GRADE - Neonatal admission to intensive care unit - Mothers admission to intensive care
VERY LOW GRADE* - Asphyxia - Perinatal death - Postpartum haemorrhage - Maternal wound infection - Other maternal infection
* Downgraded 3 points because of risk of bias (RCT was stopped early) and imprecision (small sample size and wide confidence intervals crossing the boundary of clinical relevance)
Sensitivity analyses Subgroup analysis of breech presentation.
Heterogeneity: No clinically important heterogeneity in subgroup of breech presentation for selected outcomes. |
Evidence table for intervention studies
Research question:
UV2a: Which mode of delivery (vaginal delivery or elective caesarean section) should be advised in a premature (24-32 weeks) singleton pregnancy in breech presentation?
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Hills, 2017
23+0*1 to 27+6 weeks |
Type of study: Retrospective cohort study.
Setting and country: Royal Brisbane and Women’s Hospital (RBWH), a tertiary obstetric unit in Queensland (Australia).
Funding and conflicts of interest: No conflicts of interest or funding/grants.
|
Inclusion criteria: Singleton breech fetuses between 23+0 and 27+6 weeks gestation who were delivered at RBWH.
Exclusion criteria: - multiple births - fetal presentation other than breech (cephalic, oblique, transverse) - antepartum death - termination of pregnancy - lethal congenital anomalies
N total at baseline: Intervention: 104 Control: 34
Important prognostic factors2: Maternal age (mean ±±± SD) I: 30.3 ±±± 1.9 C: 28.6 ±±± 5.8
Prior caesarean I: 23 (22.1%) C: 2 (4.4%)
Groups not comparable at baseline |
Describe intervention (treatment/procedure/test): Caesarean delivery
|
Describe control (treatment/procedure/test): Vaginal delivery |
Length of follow-up: 1 January 2005 to 31 December 2014 (10 years).
Loss-to-follow-up: I: 2 (1.9%) C: 6 (13.3%) Because of stillbirth.
Incomplete outcome data: Not reported. |
Perinatal mortality* I: 20 (19.0%) C: 16 (35.6%) RR=0.41, 95%CI 0.24 to 0.70
*includes intrapartum stillbirths and neonatal deaths during nursery admission |
Authors’ conclusion “Caesarean section for singleton extreme preterm breech delivery is associated with reduced perinatal mortality, improved neonatal condition at delivery, and increased short-term maternal morbidity.”
Other remarks Subgroup analysis for perinatal mortality: 23+0 – 23+6 (excluded) 24+0 – 24+6 25+0 – 25+6 26+0 – 26+6 27+0 – 27+6
|
|
Högberg, 2007
23+0*2 to 27+6 weeks |
Type of study: Retrospective cohort study.
Setting and country: Medical Birth Register (MBR) at Epidemiological Centre of the Swedish National Board of Health and Welfare with data from 7 tertiary health care hospitals.
Funding and conflicts of interest: Not reported.
|
Inclusion criteria: Live-born infants delivered at 23+0 to 27+6 weeks of gestation at 7 tertiary health care hospitals with level III neonatal intensive care units (NICUs).
Exclusion criteria: - children born in non-tertiary health care hospitals - children born to mothers with pre-eclampsia/eclampsia
N total at baseline: Intervention: 54 Control: 12
Important prognostic factors2: Not reported for breech presentation separately.
Unclear if groups were comparable at baseline |
Describe intervention (treatment/procedure/test): Caesarean section. |
Describe control (treatment/procedure/test): Vaginal delivery. |
Length of follow-up: Between 1990 and 2002.
Loss-to-follow-up: Not reported.
Incomplete outcome data: Not reported.
|
Infant mortality I: 13 (24.1%) C: 5 (41.7%) RR=0.25, 95%CI 0.25 to 1.31
|
Author’s conclusion “In performing CS for very preterm infants, this study suggests a survival advantage for certain maternal conditions, but not for preterm labour with a vertex presentation without other obstetrical complications”.
Other remarks Subgroups: - hospital category - breech presentation - gestational age 23-25 weeks not included |
|
Kayem, 2008
26+0 to 29+6 weeks
|
Type of study: Retrospective cohort study.
Setting and country: Three tertiary care centres in France.
Funding and conflicts of interest: Not reported.
|
Inclusion criteria: Women with singleton breech pregnancies who were admitted for preterm labour with or without preterm premature rupture of membranes (PPROM) who gave birth between 26 weeks and 29 weeks 6 days of gestation.
Exclusion criteria: -intrauterine growth restriction - preeclampsia - lethal congenital abnormalities - fetal death - placenta previa - abruptio placentae
N total at baseline: Intervention: 85 Control: 84
Important prognostic factors2: Maternal age (mean±±±SD) I: 31.8 ±±± 4.7 C: 31.3 ±±± 5.5
Previous caesarean section: I: 10 (11.8%) C: 8 (9.5%)
Groups were probably comparable at baseline |
Describe intervention (treatment/procedure/test): Planned caesarean delivery.
Same for intervention and control: - All vaginal breech deliveries in both groups were performed by the attending senior obstetrician. - Tocolytics were administered continuously up to 30 weeks of gestation unless there were laboratory signs or clinical symptoms of chorioamnionitis. - Patients with PPROM received 2 g/d of amoxicillin for 7 days. - Corticosteroids were administered in preterm labour or after PPROM to enhance fetal lung maturity. - Fetal heart rate (FHR) monitoring was done daily before labour and continuously during labour. - Epidural analgesia was offered routinely.
“The units with a PVD policy performed caesarean deliveries when FHR was abnormal during labour, when labour was protracted, and when there was chorioamnionitis before labour. Units with a PCD policy limited vaginal deliveries to cases in which labour progressed too rapidly for caesarean delivery”. |
Describe control (treatment/procedure/test): Planned vaginal delivery. |
Length of follow-up: From 1999 through 2005.
Loss-to-follow-up: Not reported.
Incomplete outcome data: Apgar score: I: 2 (2.4%) C: 11 (13.1%) |
Neonatal death I: 6 (7.1%) C: 9 (10.7%) RR=0.66, 95%CI 0.25 to 1.77
Asphyxia (Apgar score <7 at five minutes) I: 8/83 (9.6%) C: 23/78 (29.5%) RR=0.33, 95%CI 0.16 to 0.69
IVH grade 3 or 4 I: 5 (5.9%) C: 5 (6.0%) RR=0.99, 95%CI 0.30 to 3.29 Periventricular leukomalacia I: 1 (1.2%) C: 5 (5.9%) RR=0.20, 95%CI 0.02 to 1.66 |
Author’s conclusion “Risk of neonatal death was not associated with any particular policy of mode of delivery”.
Other remarks: With or without PPROM as inclusion criterion. |
|
Kayem, 2015
26+0 to 29+6 weeks |
Type of study: Retrospective cohort study.
Setting and country: Five teaching tertiary care centres in France.
Funding and conflicts of interest: No conflicts of interest.
|
Inclusion criteria: Women with singleton pregnancies admitted for preterm labour with or without preterm premature rupture of membranes (PPROM) who gave birth between 26+0/7 and 29+6/7 weeks of gestation.
Exclusion criteria: - cases in which mother or fetus had diseases that might have increased neonatal mortality or morbidity, such as intrauterine growth restriction, preeclampsia, lethal congenital abnormalities, fetal death before labor, placenta previa, or abruptio placentae - neonates delivered before 26 weeks - neonates delivered after 30 weeks
N total at baseline: Intervention: 130 Control: 173
Important prognostic factors2: Maternal age (mean ±±± SD) I: 30.2±±±4.5 C: 30.6±±±6.0
Previous caesarean delivery I: 18 (14%) C: 22 (13%)
Groups were comparable at baseline |
Describe intervention (treatment/procedure/test): Policy of planned caesarean delivery |
Describe control (treatment/procedure/test): Policy of planned vaginal delivery |
Length of follow-up: 1999 through 2010.
Loss-to-follow-up: Not reported.
Incomplete outcome data: No incomplete outcome data for relevant outcomes.
|
Newborn Hospital death I: 15 (11.5%) C: 28 (16.2%) RR=0.71, 95%CI 0.40 to 1.28
Asphyxia (Apgar score <7 at five minutes) I: 17 (13%) C: 44 (26%) RR=0.51, 95%CI 0.31 to 0.86 Adjusted OR (95% CI)* = 2.38 (1.27 – 4.47)
IVH grade 3 or 4 I: 7 (5%) C: 14 (8%) RR=0.67, 95%CI 0.28 to 1.60 Adjusted OR (95% CI)* = 1.34 (0.47 – 3.80)
Periventricular leukomalacia I: 4 (3%) C: 9 (5%) RR=0.59, 95%CI 0.19 to 1.88 Adjusted OR (95% CI)* = 1.63 (0.48 – 5.49)
*adjusted for gestational age at delivery, prenatal corticotherapy, and preterm premature rupture of membrane before 24 weeks gestation |
Author’s conclusion “A policy of planned vaginal delivery is not associated with a detectable increased risk of newborn death or severe morbidity. Head entrapment leading to death is however possible in cases of vaginal delivery, but its rarity must be balanced with the maternal consequences of early preterm cesarean delivery”.
Other remarks Looked at policy of planned caesarean delivery or vaginal delivery |
|
Pierre, 2021
25+0 to 27+6 weeks
|
Type of study: Retrospective cohort study.
Setting and country: Files of patients in university hospital level 3 maternity ward of the University of Mississippi Medical Center, United States
Funding and conflicts of interest: Authors received no specific funding for this work. No conflicts of interest.
|
Inclusion criteria: Women with singleton pregnancy in breech or cephalic presentation who gave birth between 25+0 and 27+6 weeks of gestation by vaginal or caesarean delivery to a liveborn infant with a birth weight of at least 500 grams.
Exclusion criteria: - other presentations - medically indicated terminations of pregnancy - fetal deaths - fetuses with congenital malformation - pregnancies involving imminent threats to the mother or fetus justifying an emergency caesarean
N total at baseline: Intervention: 80 Control: 113 (n=4 (3.5%) caesarean deliveries)
Important prognostic factors2: Maternal age (mean±±±SD) I: 29.9 ± 5.5 C: 27.3 ± 6.0
BMI in kg/m2 (mean±±±SD) I: 25.1 ± 7.8 C: 23.5 ± 5.3
Previous caesarean section: I: 18/79 (22.8%) C: 6/113 (5.3%)
Groups not comparable at baseline |
Describe intervention (treatment/procedure/test): Planned caesarean delivery
|
Describe control (treatment/procedure/test): Planned vaginal delivery |
Length of follow-up: Start of 1997 to the end of 2015 (19 years).
Loss-to-follow-up: Not reported.
Incomplete outcome data: Missing values different for each outcome measure
Apgar score I: 1 (1.25%) C: 18 (15.9%)
Neonatal mortality I: 3 (3.8%) C: 0 (0.0%)
IVH I: 4 (5.0%) C: 14 (12.4%)
Leukomalacia I: 8 (10.0%) C: 14 (12.4%)
|
Neonatal mortality (in delivery room and NICU) I: 6/77 (7.8%) C: 22/113 (19.5%) RR=0.40, 95%CI 0.17 to 0.94 Adjusted OR (95% CI)* = 2.6 (0.8–9.3) *adjusted for weight, gestational age, and gender
Asphyxia (5-min Apgar < 7) I: 15/79 (19.0%) C: 17/95 (17.9%)
Intraventricular haemorrhage grade 3-4 I: 9/76 (11.8%) C: 8/99 (8.1%) RR=1.47, 95%CI 0.59 to 3.62
Leukomalacia ³≥³ 3 or hyperechogenicity > 10 days I: 11/72 (15.3%) C: 17/99 (17.2%) RR=0.89, 95%CI 0.44 to 1.78
|
Author’s conclusion: “Our study showed that among planned vaginal deliveries between 25 and 27 weeks, breech presentation was associated with neonatal mortality more than twice for that for breech presentations with PCD. Finally, our study shows a caesarean could be systematically proposed for breech presentations before 28 weeks of gestation”.
Other remarks Birth weight of at least 500 grams as inclusion criteria. |
|
Reddy, 2013
24+0 to 31+6 weeks |
Type of study: Retrospective cohort study.
Setting and country: The Consortium on Safe Labour (CSL) was a study conducted by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health. CSL involved data from 12 clinical centres and 19 hospitals representing nine American Congress of Obstetricians and Gynaecologists districts.
Funding and conflicts of interest: No conflicts of interest.
|
Inclusion criteria: All singleton deliveries occurring between 24+0/7 and 31+6/7 weeks of gestation.
Exclusion criteria: Pregnancies complicated by fetal distress, placenta previa, abruption, antepartum stillbirth, and major anomalies.
N total at baseline: Intervention: 529 Control: 239
Important prognostic factors2: Maternal age, BMI or previous deliveries not reported.
Unclear if groups were comparable at baseline |
Describe intervention (treatment/procedure/test): Planned caesarean section. |
Describe control (treatment/procedure/test): Attempted vaginal delivery.
|
Length of follow-up: Between 2002 and 2008.
Loss-to-follow-up: Not reported.
Incomplete outcome data: No missing data in important outcome measures.
|
Death (intrapartum death + neonatal death) I: 39 (7%) C: 38 (16%) RR=0.46, 95%CI 0.30 to 0.71
IVH I: 90 (17%) C: 36 (15%) RR=1.13, 95%CI 0.79 to 1.61
RDS I: 389 (74%) C: 173 (72%) RR=1.02, 95%CI 0.93 to 1.12
|
Authors’ conclusion “For breech-presenting fetuses less than 32 weeks’ gestation, attempting vaginal delivery was associated with a low success rate and planned CD was associated with lower neonatal mortality rates”.
Other remarks Subgroup of breech presentation and gestational age 24-27 weeks and 28-31 weeks. |
|
Schmidt, 2019
24+0 to 31+6 weeks |
Type of study: Cohort study.
Setting and country: Data from the EPICE (Effective Perinatal Intensive Care in Europe) study from 19 regions in 11 European countries.
Funding and conflicts of interest: No conflicts of interest. Funding from European Union’s Seventh Framework Programme
|
Inclusion criteria: Live born infants in a breech position with spontaneous onset of labour or preterm premature rupture of membranes (PPROM) from 24+0 to 31+6 weeks gestational age.
Exclusion criteria: - births before 24 weeks of gestational age - severe congenital anomalies - multiple pregnancies - out-of-hospital deliveries - missing mode of delivery - situations in which caesarean section is indicated or strongly recommended including preeclampsia, eclampsia, and HELLP - diagnosis of severe fetal growth restriction - caesarean section for maternal conditions - other conditions for which caesarean section is indicated
N total at baseline: Intervention: 368 Control: 204
Important prognostic factors2: Maternal age ³≥³ 35 years I: 97 (70.8%)
Groups not comparable at baseline |
Describe intervention (treatment/procedure/test): Caesarean delivery
|
Describe control (treatment/procedure/test): Vaginal delivery |
Length of follow-up: 12-month period between March and July 2011, except in France (6 months).
Loss-to-follow-up: Not reported.
Incomplete outcome data: Apgar score: I: 14 (3.8%) C: 18 (8.8%)
IVH/PVL I: 9 (2.4%) C: 30 (14.7%) |
Mortality: I: 41/368 (11.1%) C: 61/204 (29.9%) RR=0.37, 95%CI 0.26 to 0.53 Adjusted OR (95% CI)* = 0.51 (0.29 ; 0.88)
Asphyxia (Apgar score <7 after 5 minutes) I: 80/354 (11.1%) C: 77/186 (29.9%) RR=0.55, 95%CI 0.42 to 2.71 Adjusted OR (95% CI)* = 0.46 (0.27 ; 0.76)
IVH 3-4/cPVL I: 39/359 (10.9%) C: 40/174 (23.0%) RR=0.47, 95%CI 0.32 to 0.71 Adjusted OR (95% CI)* = 0.59 (0.33 ; 1.07)
* Adjusted for: maternal age, parity, previous CS, antenatal steroids, pregnancy complications, gestational age, sex, SGA, and level of maternity unit
|
Authors’ conclusion: “Point estimates indicated protective effects of caesarean delivery for very preterm breech infants in conventional statistical models. However, analyses using propensity scores and based on unit policies did not confirm statistically significant associations. Prospective large-scale studies are needed to establish best practice and could be implemented in European regions where vaginal delivery remains an option”.
Other remarks: - PPROM inclusion criteria - Subgroup 24-25 weeks and 26-31 |
|
Stohl, 2011
24+0 to 26+6 weeks |
Type of study: Retrospective cohort study.
Setting and country: Department of Gynaecology and Obstetrics, Johns Hopkins University, Baltimore, USA).
Funding and conflicts of interest: No conflicts of interest. |
Inclusion criteria: Women with singleton pregnancies who delivered at the institution between 24+0/7 and 26+6/7 weeks’ gestation from the breech presentation.
Exclusion criteria: - multiple gestations - pregnancies with intrauterine fetal death - fetuses with major congenital anomalies - fetuses in whom comfort care only measures were planned pre-delivery
N total at baseline: Intervention: 39 Control: 26
Important prognostic factors2: Maternal age (mean±±±SD) I: 27.1 ±±± 6.7 C: 24.2 ±±± 6.6
Groups were not comparable at baseline |
Describe intervention (treatment/procedure/test): Caesarean section.
Same for intervention and control: - All deliveries were performed by residents and attending obstetricians experienced in vaginal breech deliveries. - Tocolytic agents, antibiotics, epidural anaesthesia, magnesium sulphate, and corticosteroids for fetal lung maturity were administered for standard obstetric indications. - Women with a history of a prior CD were allowed to undergo a trial of labour for standard obstetric indications. |
Describe control (treatment/procedure/test): Spontaneous vaginal delivery.
|
Length of follow-up: 1 January 2000 to 31 December 2008.
Loss-to-follow-up: Not reported.
Incomplete outcome data: Not reported.
|
Postpartum infection (endometritis) I: 10 (26%) C: 1 (4%) RR=6.67, 95%CI 0.91 to 49.01
Death before discharge NICU I: 8 (21%) C: 7 (27%) RR=0.76, 95%CI 0.31 to 1.85
Asphyxia (Apgar <7 at five minutes) I: 28 (72%) C: 14 (54%) RR=1.33, 95%CI 0.89 to 2.00
IVH grade 3 or 4 I: 5 (13%) C: 8 (31%) RR=0.42, 95%CI 0.15 to 1.13
PVL I: 5 (13%) C: 0 (0%) RR=7.42, 95%CI 0.43 to 128.83 |
Author’s conclusion “Our study provides further evidence that planned CD does not offer consistent advantage over planned SVD in improving short-term outcomes in the VLBW neonate, but it uniformly increases maternal morbidity and jeopardizes future childbearing. Given the morbidity of classical caesarean sections, vaginal delivery of the breech VLBW infant may be safely considered”.
Other remarks Very low birth weight not defined and not mentioned as inclusion criterion. |
|
Thomas, 2016
23+0*3 to 26+6 weeks |
Type of study: Retrospective cohort study.
Setting and country: Mater Mothers’ Hospital, Brisbane, Australia
Funding and conflicts of interest: Not reported.
|
Inclusion criteria: All liveborn neonates born between 23 + 0 and 26 + 6 weeks’ gestation with a prenatally determined plan for active resuscitation.
Exclusion criteria: - intended palliation
N total at baseline: Intervention: 89 Control: 37
Important prognostic factors2: No prognostic factors were shown for singletons in breech presentation.
Unknown if groups were comparable at baseline |
Describe intervention (treatment/procedure/test): Caesarean section.
For intervention and control: - All parents received individualised multidisciplinary prenatal counselling by a consultant obstetrician and neonatologist, and their views were considered in the decisions on mode of birth and neonatal resuscitation. - Prenatal steroids (and tocolysis) were recommended for threatened or planned preterm birth. - Elective CS was performed if there was a contraindication to vaginal birth (e.g., placenta praevia). - Consultants were present at all births and neonatal resuscitations. - At all births, the decision to intubate, use surfactant, perform cardiopulmonary resuscitation and transfer to the NICU were at the discretion of the attending neonatologist. - All neonates admitted into the NICU were intubated for ventilatory support and managed according to the evidence-based departmental protocols |
Describe control (treatment/procedure/test): Vaginal birth.
|
Length of follow-up: Between January 1998 and December 2009.
Loss-to-follow-up: Not reported.
Incomplete outcome data: Not reported. |
Neonatal mortality (derived from neonatal survival)* I: 31/89 (35%) C: 21/37 (57%) RR=0.61, 95%CI 0.41 to 0.92
* 23-week cohort excluded |
Authors’ conclusion “Mode of birth did not affect neonatal survival or the rate of maternal morbidity for deliveries at 23–26 completed weeks’ gestation”.
Other remarks - subgroup of singleton in non-footling breech + singletons in spontaneous preterm labour with non-footling breech - subgroup of 24 weeks, 25 weeks, and 26 weeks |
*1 For survival/mortality outcomes: possibility to exclude women with gestation between 23+0 and 23+6 weeks
*2 Subgroup of breech without multiple birth for 26 and 27 weeks
*3 23-weeks cohort excluded from analysis
Both: 24-32 weeks and 32-37 weeks
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Bergenhenegouwen, 2015
26+0 to 36+6 weeks
|
Type of study: Retrospective cohort study.
Setting and country: Netherlands Perinatal Registry database.
Funding and conflicts of interest: No conflict of interest. |
Inclusion criteria: All women who delivered a singleton fetus in breech presentation between 26+0/7 and 36+6/7 weeks of gestation
Exclusion criteria: - (lethal) congenital abnormalities - antepartum stillbirth - placental abruption (antenatally) - unknown gestational age - small for gestational age (defined as a birth weight below the 10th percentile) - maternal hypertension (defined as diastolic blood pressure 95 mm Hg or greater) - gestational and insulin-dependent diabetes mellitus or noninsulin-dependent diabetes mellitus - preeclampsia (defined as hypertension with proteinuria) - women with a severe maternal comorbidity - women who delivered before 26+0/7 weeks of gestation
N total at baseline: 26 to 31+6 weeks Intervention: 366 Control: 1,125
32 to 36+6 weeks Intervention: 1,569 Control: 5,296
Important prognostic factors2: No information about prognostic factors for subgroups.
Unknown if groups were comparable at baseline |
Describe intervention (treatment/procedure/test): Intended caesarean delivery
|
Describe control (treatment/procedure/test): Intended vaginal delivery (including vaginal delivery and emergency caesarean delivery) |
Length of follow-up: Between 2000 and 2011
Loss-to-follow-up: Not reported.
Incomplete outcome data: Not reported.
|
Perinatal mortality 26 to 31+6 weeks I: 20 (5.4%) C: 81 (7.2%) RR=0.76, 95%CI 0.47 to 1.22
I: 6 (0.4%) C: 17 (0.3%) RR=1.35, 95%CI 0.52 to 3.47 Adjusted OR (95% CI)* = 1.09 (0.42–2.86)
*adjusted for nulliparity, gestational age (weeks), neonatal intensive care unit center, prolonged rupture of membranes (24 hours or greater), birth weight (grams), and ethnicity.
|
Author’s conclusion “In women delivering a preterm breech fetus, caesarean delivery is associated with reduced perinatal mortality and morbidity”.
Other remarks - Subgroups based on gestational age: 26+0/7 – 27+6/7 28+0/7 – 31+6/7 32+0/7 – 36+6/7 - Comparison between intended caesarean section, vaginal delivery, and emergency caesarean delivery |
|
Gasim, 2008
24 to 36+6 weeks |
Type of study: Retrospective cohort study.
Setting and country: King Fahd Hospital of the University Al-Khobar in Saudi Arabia.
Funding and conflicts of interest: Not reported.
|
Inclusion criteria: Singleton breech deliveries between 24 and 36 weeks’ gestation.
Exclusion criteria: - intrauterine fetal death - multiple pregnancies - lethal congenital fetal malformations
N total at baseline: 24 to 31+6 weeks Intervention: 22 Control: 66
32 to 36+6 weeks Intervention: 25 Control: 82
Important prognostic factors2: No characteristics reported for both groups.
Unknown if groups were comparable at baseline |
Describe intervention (treatment/procedure/test): Caesarean section.
Same for intervention and control: - Betamethasone, 12 mg intramuscular injection, every 24 hours for two doses had been administered to the mother when indicated. - The use of epidural analgesia had been encouraged as appropriate. - All the newborns were examined by a neonatologist for birth defects, Apgar scores and evidence of birth trauma immediately after delivery.
|
Describe control (treatment/procedure/test): Vaginal delivery.
All the vaginal breech deliveries had been conducted or supervised by an experienced obstetrician.
|
Length of follow-up: 1 January 1992 to 31 December 2001.
Loss-to-follow-up: Not reported.
Incomplete outcome data: Not reported.
|
Asphyxia (Apgar score <7 at 5 minutes) 24 to 31+6 weeks I: 14 (64%) C: 44 (67%) RR=0.95, 95%CI 0.67 to 1.37
32 to 36+6 weeks I: 7 (28%) C: 14 (17%) RR=1.64, 95%CI 0.74 to 3.61 |
Author’s conclusion “In view of the significantly higher neonatal mortality found in vaginal delivery, the present study favours abdominal delivery for a singleton preterm breech fetus”.
Other remarks Neonates divided into six categories according to gestational age and birth weight. |
|
Herbst, 2007
25 to 36 weeks |
Type of study: Retrospective cohort study.
Setting and country: Swedish Medical Birth Registry.
Funding and conflicts of interest: Not reported.
|
Inclusion criteria: - singleton preterm live births with breech presentation in (completed) gestational weeks 25–36 - diagnosis of PTL and/or PPROM.
Exclusion criteria - fetal malformations - intrauterine growth retardation - gestational diabetes - eclampsia
N total at baseline: 34 to 36+6 weeks Intervention: 1,223 Control: 557
25 to 27+6 weeks Intervention: 324 Control: 63
Important prognostic factors2: Not reported for subgroups
Unknown if groups were comparable at baseline
|
Describe intervention (treatment/procedure/test): Caesarean section.
|
Describe control (treatment/procedure/test): Vaginal delivery. |
Length of follow-up: 1990 to 2002.
Loss-to-follow-up: Not reported.
Incomplete outcome data: Not reported. |
Neonatal death 25 to 27+6 weeks I: 31 (10%) C: 20 (32%) RR=0.30, 95%CI 0.18 to 0.49 Adjusted OR (95% CI)* = 0.6 (0.3-1.2)
34 to 36+6 weeks I: 6 (0.5%) C: 5 (0.9%) RR=0.55, 95%CI 0.17 to 1.78
IVH 25 to 27+6 weeks I: 23 (7%) C: 7 (11%) RR=0.64, 95%CI 0.29 to 1.42 Adjusted OR (95% CI)* = 1.0 (0.4-2.6)
34 to 36+6 weeks I: 0 C: 1 (0.2%) RR=0.15, 95%CI 0.01 to 3.72
IRDS 25 to 27+6 weeks I: 141 (44%) C: 28 (44%) RR=0.98, 95%CI 0.72 to 1.33 Adjusted OR (95% CI)* = 1.7 (0.9-3.2)
34 to 36+6 weeks I: 29 (2%) C: 2 (0.4%) RR=6.60, 95%CI 1.58 to 27.58 Adjusted OR (95% CI)* = 7.2 (1.7-31)
*adjusted for maternal age, parity, year of birth, and gestational age |
Author’s conclusion “The lower neonatal mortality after CS supports a policy of caesarean delivery of the preterm breech”.
Other remarks - PTL or PPROM used as inclusion criteria - Subgroups 25-27 weeks, 28-33 weeks, and 34-36 weeks |
|
O’Reilly, 2018
24-31 weeks 32-36 weeks |
Type of study: Retrospective cohort study.
Setting and country: National Maternity Hospital, Holles St, in Dublin, Ireland
Funding and conflicts of interest: No potential conflict of interest was reported by the authors.
|
Inclusion criteria: Women with singleton preterm breech deliveries (<37-week gestation)
Exclusion criteria: - stillbirths - lethal congenital anomalies
N total at baseline: 24+0 to 31+6 weeks Intervention: 113 Control: 108
32 to 36+6 weeks Intervention: 192 Control: 52
Important prognostic factors2: Not reported
Unclear if groups were comparable at baseline because no baseline characteristics were reported |
Describe intervention (treatment/procedure/test): Lower Segment Caesarean Section
Same for intervention and control: Management of preterm breeches is judged on an individual case-by-case basis. If a patient arrives to hospital in labour, is making satisfactory progress with normal fetal monitoring then a vaginal breech delivery may be attempted provided the patient is counselled regarding potential complications. Patients are also informed about the possibility for a difficult caesarean delivery due to descent of the breech into the pelvis in advanced labour.
|
Describe control (treatment/procedure/test): Vaginal delivery
|
Length of follow-up: 1 January 2001 to 31 December 2011 (11 years).
Loss-to-follow-up: Not reported.
Incomplete outcome data: Not reported. |
Postpartum haemorrhage >1000 cc 24+0 to 31+6 weeks I: 6 (5%) C: 0 RR=6.50, 95%CI 0.37 to 113.37
32 to 36+6 weeks I: 10 (5%) C: 1 (2%) RR=2.71, 95%CI 0.35 to 20.68
Asphyxia (Apgar score <7 after 5 minutes) 24+0 to 31+6 weeks I: 25 (22%) C: 23 (41%) RR=0.54, 95%CI 0.34 to 0.86
32 to 36+6 weeks I: 15 (8%) C: 10 (19%) RR=0.41, 95%CI 0.19 to 0.85 |
Author’s conclusion “These results demonstrate that vaginal delivery of a preterm breech – presenting infant is a necessary skill for all birth attendants in contemporary practice, particularly prior to 28-week gestation”.
Other remarks: Distinction weeks of gestation: - Extreme prematurity: - Moderate prematurity: No data for combination of weeks of gestation |
Table of quality assessment for systematic reviews of RCTs and observational studies
|
Study
First author, year |
Appropriate and clearly focused question?1
Yes/no/unclear |
Comprehensive and systematic literature search?
Yes/no/unclear |
Description of included and excluded studies?3
Yes/no/unclear |
Description of relevant characteristics of included studies?4
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?5
Yes/no/unclear/notapplicable |
Assessment of scientific quality of included studies?6
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?7
Yes/no/unclear |
Potential risk of publication bias taken into account?8
Yes/no/unclear |
Potential conflicts of interest reported?9
Yes/no/unclear |
|
Alfirevic, 2013 |
Yes. Research question and inclusion criteria were clearly described. |
Yes. Search period and strategy described and Medline/Embase were searched. |
Yes. Table of excluded studies with reason for exclusion and references. |
Yes. Characteristics of included participants in individual studies were described. |
Not applicable. |
Yes. Risk of bias was assessed using the criteria in the Cochrane Handbook. |
Yes. Clinical and statistical heterogeneity were considered.
|
Yes. Publication bias was considered but not applicable here since there were less than ten studies in the meta-analysis.
|
No. Source of funding not indicated for each of the included studies. |
Risk of bias table
Research question:
UV2a: Which mode of delivery (vaginal delivery or elective caesarean section) should be advised in a premature (24-32 weeks) singleton pregnancy in breech presentation?
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors?
|
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables?
|
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed?
|
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Low, Some concerns, High |
|
|
Hills, 2017
23+0*1 to 27+6 weeks |
Definitely yes
Reason: Women selected from electronic perinatal database.
|
Definitely yes
Reason: Mode of delivery derived from electronic perinatal database. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Definitely yes
Reason: All maternal and neonatal medical record were individually reviewed for data collection.
|
Probably no
Reason: Only subgroup analysis for neonatal mortality. |
Definitely yes
Reason: All maternal and neonatal medical record were individually reviewed for data collection.
|
Probably no
Reason: More loss to follow-up in intervention group due to stillbirths. |
Probably yes
Reason: No other interventions used. |
Some concerns |
|
Hogberg, 2007
23+0*2 to 27+6 weeks |
Definitely yes
Reason: Women selected from Medical Birth Register.
|
Definitely yes
Reason: Delivery data retrieved from Medical Birth Register. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before.
|
Probably no
Reason: Demographic data not presented in study. |
Probably yes
Reason: Subgroup analysis of breech presentation without pre-eclampsia, multiple birth, PROM, or haemorrhage.
|
Definitely yes
Reason: Outcome derived from Medical Birth Register. |
Probably yes
Reason: No missing data reported. |
Probably yes
Reason: No other interventions. |
Some concerns |
|
Kayem, 2008
26+0 to 29+6 weeks
|
Definitely yes
Reason: Women were identified from databases.
|
Definitely yes
Reason: Groups were defined according to center policy. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Definitely yes
Reason: Patient medical records were used for extraction of characteristics. |
Definitely yes
Reason: Adjusted OR were calculated for variables with a probability value of <.10 on univariate analysis.
|
Definitely yes
Reason: Outcomes extracted from medical records. |
Probably no
Reason: Incomplete outcome data for Apgar score which is different for both groups. |
Probably yes
Reason: Other interventions probably similar for both groups. |
Low (other outcomes)
Some concerns (Outcome Apgar score) |
|
Kayem, 2015
26+0 to 29+6 weeks |
Definitely yes
Reason: Women selected from hospital databases. |
Definitely yes
Reason: Mode of delivery derived from search in hospital databases. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Definitely yes
Reason: Relevant information was gathered from maternal and neonatal charts by using a standardized data sheet.
|
Definitely yes
Reason: Adjusted for covariables previously described as risk factors for neonatal death and for variables found to be potential confounders in bivariate analyses.
|
Definitely yes
Reason: Relevant information was gathered from maternal and neonatal charts by using a standardized data sheet.
|
Probably yes
Reason: No missing data for relevant outcomes. |
Probably yes
Reason: No other interventions used. |
Low |
|
Pierre, 2021
25+0 to 27+6 weeks
|
Definitely yes
Reason: Women were selected from files.
|
Definitely yes
Reason: Exposure data derived from files.
|
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before.
|
Definitely yes
Reason: Characteristics were collected from obstetric files.
|
Definitely yes
Reason: Adjusted for confounding variables.
|
Definitely yes
Reason: Extracted data from medical files.
|
Probably no
Reason: Missing data more frequent in intervention group for Apgar score.
|
Probably yes
Reason: No other co-interventions performed.
|
Low (Outcome Neonatal mortality, IVH, PVL)
Some concerns (Outcome Apgar score)
|
|
Reddy, 2013
24+0 to 31+6 weeks |
Definitely yes
Reason: Women selected from Consortium on Safe Labor study.
|
Definitely yes
Reason: Delivery data extracted from electronic medical records. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Definitely yes
Reason: Demographic data derived from electronic medical records. |
Definitely yes
Reason: Adjusted for confounders. |
Definitely yes
Reason: Outcomes derived from electronic medical records. |
Probably yes
Reason: No missing data for relevant outcomes.
|
Probably yes
Reason: No other interventions used. |
Low |
|
Schmidt, 2019
24+0 to 31+6 weeks |
Definitely yes
Reason: Women were selected from data in EPICE study. |
Definitely yes
Reason: Data on the characteristics, policies and protocols of maternal and neonatal units were collected using structured pretested questionnaires sent to heads of services with at least 10 very preterm admissions per year.
|
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before.
|
Definitely yes
Reason: Data on the characteristics, policies and protocols of maternal and neonatal units were collected using structured pretested questionnaires sent to heads of services with at least 10 very preterm admissions per year. |
Definitely yes
Reason: Mixed effects model adjusted for potential confounders. |
Definitely yes
Reason: Investigators abstracted data from obstetrical and neonatal charts using a pretested standardized questionnaire with common definitions. |
Probably no
Reason: Missing data for Apgar score and IVH/PVL. For IVH/PVL it is more frequent in the intervention group. |
Probably yes
Reason: No other interventions. |
Low (OutcomeMortality and Apgar score)
Some concerns (Outcome IVH/PVL) |
|
Stohl, 2011
24+0 to 26+6 weeks |
Definitely yes
Reason: Women selected at a single institution. |
Definitely yes
Reason: Delivery data extracted from outpatient and inpatient electronic medical charts and hospital records.
|
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Definitely yes
Reason: Demographics extracted from outpatient and inpatient electronic medical charts and hospital records. |
Probably no
Reason: No adjustment for confounders. |
Definitely yes
Reason: Outcomes extracted from outpatient and inpatient electronic medical charts and hospital records. |
Probably yes
Reason: No missing data reported. |
Probably yes
Reason: Other interventions similar for both groups. |
Some concerns |
|
Thomas, 2016
23+0*3 to 26+6 weeks |
Definitely yes
Reason: Study population identified by searching obstetric and neonatal databases. |
Definitely yes
Reason: Delivery data obtained from database. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Probably no
Reason: Characteristics of whole population was shown, but no demographic data for singletons in breech presentation separately. |
Probably no
Reason: Adjusted for confounders for nonfootling breech but not for singletons separately. |
Definitely yes
Reason: Outcome data were retrieved from neonatal and obstetric databases and chart review. |
Probably yes
Reason: No missing data reported. |
Probably yes
Reason: Other interventions similar for both groups. |
Some concerns |
*1 For survival/mortality outcomes: possibility to exclude women with gestation between 23+0 and 23+6 weeks
*2 Subgroup of breech without multiple birth for 26 and 27 weeks
*3 23-weeks cohort excluded from analysis
Both: 24-32 weeks and 32-37 weeks
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors?
|
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables?
|
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed?
|
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Low, Some concerns, High |
|
|
Bergenhenegouwen, 2015
26+0 to 36+6 weeks |
Definitely yes
Reason: Women selected from the Netherlands Perinatal Registry.
|
Definitely yes
Reason: Mode of delivery derived from the Netherlands Perinatal Registry. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Definitely yes
Reason: Data gathered from the Netherlands Perinatal Registry.
|
Definitely yes
Reason: Adjusted for confounders. |
Definitely yes
Reason: Data gathered from the Netherlands Perinatal Registry. Cases of perinatal death were checked by obstetricians.
|
Probably yes
Reason: No missing data reported. |
Probably yes
Reason: No difference in interventions between groups; women were treated according to national guidelines. |
Low |
|
Gasim, 2008
24 to 36+6 weeks |
Definitely yes
Reason: Women selected from medical records at a single hospital.
|
Probably yes
Reason: Delivery data retrieved from medical records. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Probably no
Reason: No demographic data reported for both groups. |
Probably no
Reason: No adjustment for confounders, only subgroup analysis with gestational age for Apgar score. |
Probably yes
Reason: Outcomes extracted from medical records. |
Probably yes
Reason: No missing data reported. |
Probably yes
Reason: Other interventions similar for both groups. |
Some concerns |
|
Herbst, 2007
25 to 36 weeks |
Definitely yes
Reason: Women selected from Swedish Medical Birth Registry.
|
Definitely yes
Reason: Delivery data retrieved from Swedish Medical Birth Registry. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before.
|
Definitely yes
Reason: Demographic data retrieved from Swedish Medical Birth Registry. |
Definitely yes
Reason: Adjusted for confounders.
|
Definitely yes
Reason: Outcomes derived from Swedish Medical Birth Registry. |
Probably yes
Reason: No missing data reported. |
Probably yes
Reason: No other interventions. |
Low |
|
O’Reilly, 2018
24-31 weeks 32-36 weeks |
Probably yes
Reason: Women were probably selected based on stored data in the hospital (data were gathered as part of continuous hospital wide audit of practice).
|
Probably yes
Reason: Mode of delivery probably documented at hospital. |
Definitely yes
Reason: Outcomes related to mode of delivery, so not present before. |
Probably no
Reason: No characteristics reported. |
Probably no
Reason: No adjustement for confounding, only subgroups for gestational age. |
Probably yes
Reason: Probably extracted from recorded data. |
Probably yes
Reason: No missing data reported. |
Probably yes
Reason: Other interventions same for both groups. |
High |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Bergenhenegouwen LA, Meertens LJ, Schaaf J, Nijhuis JG, Mol BW, Kok M, Scheepers HC. Vaginal delivery versus caesarean section in preterm breech delivery: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2014 Jan;172:1-6. doi: 10.1016/j.ejogrb.2013.10.017. Epub 2013 Oct 16. PMID: 24199680. |
Better systematic review available: systematic review of old retrospective studies with no clear search strategy and risk of bias assessment |
|
Penn ZJ, Steer PJ, Grant A. A multicentre randomised controlled trial comparing elective and selective caesarean section for the delivery of the preterm breech infant. BJOG. 2014 Dec;121 Suppl 7:48-53. doi: 10.1111/1471-0528.13212. PMID: 25488088. |
Included in systematic review of Alfirevic 2013 |
|
Lodha A, Zhu Q, Lee SK, Shah PS; Canadian Neonatal Network. Neonatal outcomes of preterm infants in breech presentation according to mode of birth in Canadian NICUs. Postgrad Med J. 2011 Mar;87(1025):175-9. doi: 10.1136/pgmj.2010.107532. Epub 2011 Jan 25. PMID: 21266402. |
Wrong population: not only singleton presentation |
|
Niles KM, Barrett JFR, Ladhani NNN. Comparison of cesarean versus vaginal delivery of extremely preterm gestations in breech presentation: retrospective cohort study. J Matern Fetal Neonatal Med. 2019 Apr;32(7):1142-1147. doi: 10.1080/14767058.2017.1401997. Epub 2017 Nov 20. PMID: 29157039. |
Wrong population: not only singleton presentation |
|
Bergenhenegouwen L, Ensing S, Ravelli AC, Schaaf J, Kok M, Mol BW. Subsequent pregnancy outcome after preterm breech delivery, a population based cohort study. J Matern Fetal Neonatal Med. 2016;29(15):2540-4. doi: 10.3109/14767058.2015.1094050. Epub 2015 Nov 9. PMID: 26553533. |
Wrong population: not only breech fetuses |
|
Vidovics M, Jacobs VR, Fischer T, Maier B. Comparison of fetal outcome in premature vaginal or cesarean breech delivery at 24-37 gestational weeks. Arch Gynecol Obstet. 2014 Aug;290(2):271-81. doi: 10.1007/s00404-014-3203-y. Epub 2014 Mar 26. PMID: 24668252. |
Wrong study design: case series |
|
Robilio PA, Boe NM, Danielsen B, Gilbert WM. Vaginal vs. cesarean delivery for preterm breech presentation of singleton infants in California: a population-based study. J Reprod Med. 2007 Jun;52(6):473-9. PMID: 17694963. |
Wrong population: unknown how many weeks of gestation |
|
Zahedi-Spung LD, Raghuraman N, Macones GA, Cahill AG, Rosenbloom JI. Neonatal morbidity and mortality by mode of delivery in very preterm neonates. Am J Obstet Gynecol. 2022 Jan;226(1):114.e1-114.e7. doi: 10.1016/j.ajog.2021.07.013. Epub 2021 Jul 28. PMID: 34331893. |
Wrong population: no breech presentation |
|
Gupta V, Makhija A, Kumari N, Kumari R. Comparative study of vaginal and cesarean section delivery for fetuses in breech presentation. Journal of South Asian Federation of Obstetrics and Gynaecology. 2018 Jan 1;10(4S1):321-7. |
Wrong population: no elective caesarean section for a gestational age below 36 weeks |
|
Mousiolis A, Papantoniou N, Mesogitis S, Baglatzi L, Baroutis G, Antsaklis A. Optimum mode of delivery in gestations complicated by preterm premature rupture of the membranes. J Matern Fetal Neonatal Med. 2012 Jul;25(7):1044-9. doi: 10.3109/14767058.2011.614659. Epub 2011 Oct 4. PMID: 21854136. |
Wrong population: only 12 women with breech presentation |
|
Demirci O, Tuğrul AS, Turgut A, Ceylan S, Eren S. Pregnancy outcomes by mode of delivery among breech births. Arch Gynecol Obstet. 2012 Feb;285(2):297-303. doi: 10.1007/s00404-011-1956-0. Epub 2011 Jul 7. PMID: 21735191. |
Wrong population: unknown how many weeks of gestation |
|
Deutsch A, Salihu HM, Lynch O, Marty PJ, Belogolovkin V. Cesarean delivery versus vaginal delivery: impact on survival and morbidity for the breech fetus at the threshold of viability. J Matern Fetal Neonatal Med. 2011 May;24(5):713-7. doi: 10.3109/14767058.2010.516287. Epub 2010 Sep 14. PMID: 20836738. |
Wrong population: gestational age 23 weeks |
|
Milasinović L, Kapamadzija A, Petrović D, Nikolić L. Incidence of cerebral dysfunction as a parameter for decision making in the management of preterm labor. Med Pregl. 2000 Sep-Oct;53(9-10):485-92. English, Croatian. PMID: 11320730. |
Article not in English |
|
Toijonen A, Hinnenberg P, Gissler M, Heinonen S, Macharey G. Maternal and neonatal outcomes in the following delivery after previous preterm caesarean breech birth: a national cohort study. J Obstet Gynaecol. 2022 Jan;42(1):49-54. doi: 10.1080/01443615.2021.1871888. Epub 2021 May 2. PMID: 33938353. |
No separate data for outcomes of interest regarding different gestational ages |
|
Lorthe E, Sentilhes L, Quere M, Lebeaux C, Winer N, Torchin H, Goffinet F, Delorme P, Kayem G; EPIPAGE-2 Obstetric Writing Group. Planned delivery route of preterm breech singletons, and neonatal and 2-year outcomes: a population-based cohort study. BJOG. 2019 Jan;126(1):73-82. doi: 10.1111/1471-0528.15466. Epub 2018 Oct 9. PMID: 30216654. |
Wrong population: between 26 and 34 weeks (no subgroups) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 21-04-2026
Beoordeeld op geldigheid : 21-04-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met premature stuitligging.
Werkgroep
- Dr. M. (Marieke) Sueters (voorzitter) (NVOG)
- Dr. M.T.M (Maureen) Franssen (NVOG)
- Drs. E.C. (Eline) van der Wilk (NVOG)
- Dr. C.N.H. (Carolien) Abheiden (NVOG)
- Dr. S.M.T.A. (Simone) Goossens (NVOG)
- Drs. S.I.D.M. (Siska) Verburgh-Post (KNOV)
- Dr. S.A. (Sylvia) Obermann-Borst (Care4Neo)
Klankbordgroep
- Mr. Anouk Kaiser (Het Buikencollectief)
- Dr. C.V. (Christian) Hulzebos (NVK)
Met ondersteuning van
- Dr. M. (Mohammadreza) Abdollahi, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. I.M. (Irina) Mostovaya, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. D.A.M. (Danique) Middelhuis, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. L. (Laura) Viester, adviseur, Kennisinstituut van de Federatie Medisch Specialisten (tot juli 2022)
- Laura Boerboom, medisch informatie specialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
|
Achternaam werkgroeplid |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Getekend op |
|
Marieke Sueters |
Gynaecoloog-perinatoloog LUMC, universitair opleider gynaecologie en verloskunde |
Geen- voorzitter van de Koepel Opleiding van de NVOG |
Geen |
Geen |
Geen |
Geen |
Geen |
11-04-2025 |
|
Maureen Franssen |
Gynaecoloog-perinatoloog, UMC Groningen |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
01-05-2025 |
|
Eline Van der Wilk |
Gynaecoloog-perinatoloog Erasmus MC |
Lid NVOG Otterlo commissie |
Geen |
Geen |
Geen |
Geen |
Geen |
14-04-2025 |
|
Simone Goossens |
Gynaecoloog, Maxima mc Veldhoven |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
28-3-2025 |
|
Carolien Abheiden |
Gynaecoloog, UMC Groningen |
werkgroep Otterlo. Sectie redacteur gynaecologie Nederlands Tijdschrift voor Geneeskunde, onbetaald |
Geen |
Geen |
Stichting PLN: The impact of pregnancy on PLN phenotype. Projectleider. |
Geen |
Geen |
11-04-2025 |
|
Sylvia Obermann-Borst |
Directeur Zorg&Wetenschap Care4Neo 28 uur Huisarts -epideminoloog, zzp 18 uur |
Richtlijn werkgroep NHG ADHD Medicatie, vacatiegelden. Raad v Commissarissen Expertisecentrum Ontwikkeling Ondersteuning Prematuren, vacatiegelden. Huisarts-docent EBM-gastdocent Radboud UMC vergoeding/uur |
Geen |
Geen |
ZONmw: informatievoorziening dreigende vroeggeboorte. ZONmw: PRESAFE sepsis RCT biomarkers. ZONmw: PREPARE covid pandemie en daling vroeggeboorte. SPIN: EOS calculator, sepis. SPIN: neoPARTNER, FiCare. Gratama: beslisondersteuning NEC. EU: safeGFT, groetvertraging. |
Geen |
Geen |
4/15/2025 |
|
Siska Verburgh-Post |
Verloskundige 1e lijn - maatschaplid- Verloskundigen Etten-Leur Beleidsmedewerker richtlijnen KNOV (zzp) Lid van landelijke Transmurale Werkgroep Stuitligging (nvog) |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
30-04-2025 |
|
Anouk Kaiser |
Directeur van Stichting Zelfbewustzwanger |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
30-03-2025 |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door uitnodigen van Patientfederatie Nederland, Het Buikencollectief, Hellp Stichting en Care4Neo voor de invitational conference. Het verslag hiervan [zie aanverwante producten] is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan Patientfederatie Nederland, Het Buikencollectief, Hellp Stichting en Care4Neo en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Modus partus bij premature stuitligging - Zeer premature partus (24-32 weken) bij eenlingzwangerschap in stuitligging |
Geen financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5.000 patiënten per jaar). De richtlijn richt zich op een kleine groep zwangeren met een (dreigende) vroeggeboorte in stuitligging tussen 24 en 37 weken. Daarom worden geen substantiële financiële gevolgen voor de collectieve uitgaven verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Richtlijn: Richtlijnmodules Geboortezorg |
|
|
Uitgangsvraag: Uitgangsvraag: Heeft een primaire sectio of een vaginale baring de voorkeur bij een kind in stuitligging in de premature periode bij zwangeren met eenlingzwangerschap? Subvraag 1 Welke modus partus (vaginale partus of electieve sectio caesarea) dient geadviseerd te worden bij een premature (32-37 weken) eenlingzwangerschap in stuitligging? Subvraag 2 Welke modus partus (vaginale partus of electieve sectio caesarea) dient geadviseerd te worden bij een premature (24-32 weken) eenlingzwangerschap in stuitligging? |
|
|
Database(s): Medline (OVID), Embase |
Datum: 03-02-2022 |
|
Periode: >2000 |
Talen: Engels, Nederlands |
|
Literatuurspecialist: Laura Boerboom |
|
|
BMI zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/https://blocks.bmi-online.nl/https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting en opmerkingen:
→ Voor deze vraag is gezocht op de elementen stuitligging (in het blauw), vaginale baring (in het groen), sectio caesarea (in het rood) en premature zwangerschap (in het paars).
→ De werkgroep had drie sleutelpublicaties (Bergenhenegouwen (2014), Bergenhenegouwen (2015) en Lorthe (2019)). Deze drie sleutelpublicaties zitten in de search. |
|
|
Te gebruiken voor richtlijnen tekst: In de databases Embase (via embase.com) en Medline (via OVID) is op 03-02-2022 met relevante zoektermen gezocht naar systematische reviews, RCT’s en observationele studies over of een primaire sectio of een vaginale baring de voorkeur heeft bij een kind in stuitligging in de premature periode bij zwangeren met eenlingzwangerschap. De literatuurzoekactie leverde 204 unieke treffers op. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
22 |
8 |
22 |
|
RCTs |
34 |
7 |
34 |
|
Observationele studies |
142 |
73 |
148 |
|
Totaal |
198 |
88 |
204 |
Zoekstrategie
Embase.com & Medline OVID
|
Database |
Zoektermen |
||||||||||||||||||||||||||||||||||||||||||
|
Embase
|
|
||||||||||||||||||||||||||||||||||||||||||
|
Medline (OVID)
|
1 exp Breech Presentation/ or breech.ti,ab,kf. (5647) 2 ((vaginal or normal) adj2 (deliver* or birth*)).ti,ab,kf. (27432) 3 exp Cesarean Section/ or (caesarean or cesarean or cesarian or cesarotomy or caesarea or fetectom*).ti,ab,kf. (80420) 4 exp Premature Birth/ or (premature or preterm).ti,ab,kf. (203464) 5 1 and 2 and 3 and 4 (195) 6 limit 5 to (english or dutch) (106) 7 (meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf.) not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) (555338) 8 (exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw.) not (animals/ not humans/) (2218931) 9 Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or (cohort adj (study or studies)).tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] (3935074) 10 5 and 7 (8) – SR’s 11 (5 and 8) not 10 (7) – RCT’s 12 (5 and 9) not 10 not 11 (73) – Observationele studies 13 10 or 11 or 12 (88) |