Laparoscopische adhesiolysis versus open adhesiolysis
Uitgangsvraag
Wat is de waarde van laparoscopische adhesiolysis vergeleken met open adhesiolysis?
Aanbeveling
Start bij voorkeur een operatieve behandeling van strengileus laparoscopisch.
Gebruik geen selectielijsten uit de literatuur voor de selectie van laparoscopische kandidaten omdat deze te beperkend zijn.
Converteer laagdrempelig naar een open adhesiolysis bij gebrek aan chirurgisch overzicht gezien het hoger risico op darmletsel bij een laparoscopische behandeling.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Er is literatuuronderzoek verricht naar het effect van laparoscopische adhesiolyse vergeleken met open adhesiolyse in volwassen patiënten met strengileus. Voor de cruciale uitkomstmaten mortaliteit en complicaties werden klinisch relevante verschillen gevonden in het voordeel van de patiënten die laparoscopische adhesiolyse ondergingen. Zowel voor mortaliteit als complicaties werd een zeer lage bewijskracht gevonden. Daarnaast is het van belang om waakzaam te zijn voor het risico op selectiebias, i.e., patiënten die ernstiger ziek zijn en meer distentie in de buik hebben zullen sneller geselecteerd worden voor een open operatie.
Voor de belangrijke uitkomstmaten verblijfsduur in het ziekenhuis, IC opname, terugkeer van darmfunctie en voedingsstatus werd een klinisch relevant verschil gevonden in het voordeel van de patiënten die laparoscopische adhesiolyse ondergingen. De bewijskracht voor deze uitkomstmaten is zeer laag. Voor de belangrijke uitkomstmaat noodzaak tot operatie/ongeplande reoperatie werd geen klinisch relevant verschil gevonden, met een zeer lage bewijskracht. Voor de belangrijke uitkomstmaten recidief strengileus en darmletsel werd een klinisch relevant verschil gevonden in het voordeel van de patiënten die open adhesiolyse ondergingen. De bewijskracht voor deze uitkomstmaten is zeer laag. De belangrijke uitkomstmaat incisiebreuken werd niet gerapporteerd in de geïncludeerde studies.
Concluderend lijkt laparoscopische adhesiolyse op basis van de huidige literatuur voordelen te hebben op korte termijn uitkomstmaten, zoals kortere opnameduur en sneller herstel van darmfunctie. Tegelijkertijd moet men alert blijven op een mogelijk verhoogd risico op darmletsels bij laparoscopie, evenals het ontbreken van een aangetoond voordeel op langere termijn wat betreft het optreden van recidieven van strengileus.
In Nederland wordt ongeveer de helft van de patiënten in eerste instantie laparoscopisch geopereerd. Hierbij is sprake van een relatief hoog conversiepercentage van laparoscopie naar open chirurgie. Dit conversiebeleid wordt echter als positief beschouwd, omdat het kan bijdragen aan het voorkomen van ernstige complicaties zoals darmletsel.
Strikte selectiecriteria voor laparoscopische adhesiolyse kunnen ertoe leiden dat een groot deel van de patiënten uitgesloten wordt van een potentieel minder invasieve behandeling. In de literatuur is een voorbeeld beschreven (Farinella, 2009) waarin zeer stringente inclusiecriteria ertoe leidden dat slechts circa 10% van de patiënten laparoscopisch geopereerd kon worden. De werkgroep is van mening dat het hanteren van dergelijke rigide selectielijsten niet wenselijk is, omdat dit patiënten de kans ontneemt op sneller herstel via een laparoscopische benadering.
De werkgroep is daarom van mening dat de voorkeursbenadering is laparoscopisch starten en bij twijfel of technische belemmeringen (bijvoorbeeld slechte zichtbaarheid, ernstige adhesies of risico op darmletsel) tijdig en laagdrempelig te converteren naar een open procedure. Deze aanpak combineert het streven naar minimale invasie met patiëntveiligheid.
Als praktisch criterium voor laparoscopie adviseert de werkgroep om de buiktoegankelijkheid vooraf te beoordelen, o.a. op basis van vermindering van distentie na plaatsing van een neus-maaghevel en de mate van bekende verklevingen of littekenbreuken tegen de buikwand.
Kwaliteit van bewijs
De overall kwaliteit van bewijs is zeer laag. Dit betekent dat we zeer onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege ernstige:
- Risk of Bias: methodologische beperkingen: inadequate calculation of study size, inadequate control group, inadequate baseline equivalence, inadequate follow-up.
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grens van klinische relevantie overschrijdt.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
De meeste patiënten geven de voorkeur aan een laparoscopische benadering, met name vanwege het potentieel snellere herstel en de minder invasieve aard van de ingreep. Tegelijkertijd is het belangrijk om patiënten duidelijk te informeren dat, omwille van veiligheid, tijdens de ingreep alsnog een conversie naar een open procedure noodzakelijk kan zijn. Deze beslissing wordt intra-operatief genomen op basis van de chirurgische anatomie en technische haalbaarheid, en is dus niet afhankelijk van patiëntkenmerken zoals leeftijd of algehele conditie.
Sommige patiënten, met name die met een uitgebreide voorgeschiedenis van buikoperaties of complicaties, beschouwen juist een open benadering als veiliger en geven hieraan de voorkeur. Om die reden is het essentieel om patiënten actief te betrekken bij de besluitvorming rondom de operatietechniek. Goede voorlichting over de mogelijkheden, verwachte uitkomsten en risico’s is hierbij cruciaal voor gedeelde besluitvorming.
Kostenaspecten
Een laparoscopische adhesiolyse is in principe duurder dan een open procedure vanwege langere operatieduur en het gebruik van specifiek instrumentarium en materialen. Daar staat tegenover dat laparoscopie gepaard gaat met een kortere ziekenhuisopname en mogelijk een sneller herstel. Hierdoor kan het netto kostenplaatje gunstiger uitvallen. De totale zorgkosten kunnen daardoor lager zijn, ondanks hogere initiële procedurekosten.
Gelijkheid ((health) equity/equitable)
De interventie leidt niet tot verschillen in gezondheidsgelijkheid want. De interventie wordt bepaald op basis van chirurgische en anatomische overwegingen tijdens de ingreep, en is niet afhankelijk van factoren zoals sociaaleconomische status, leeftijd of achtergrond van de patiënt.
Aanvaardbaarheid:
Ethische aanvaardbaarheid
De interventie lijkt aanvaardbaar voor de betrokkenen. Er zijn geen ethische bezwaren.
Duurzaamheid
Bij de laparoscopische interventie spelen duurzaamheidsoverwegingen een rol, met name door het gebruik van meer wegwerpmaterialen en specifiek instrumentarium zoals trocars en scharen. Dit leidt tot een hogere milieubelasting dan bij een open procedure. Om de duurzaamheid van de laparoscopische benadering te verbeteren, kan worden overwogen om – waar veilig en technisch haalbaar – gebruik te maken van herbruikbare materialen en instrumenten.
Bij de open procedure zijn doorgaans minder wegwerpmaterialen nodig, waardoor de milieubelasting in theorie lager is. Echter, een mogelijk langere opnameduur bij open chirurgie kan de totale ecologische voetafdruk weer verhogen.
Haalbaarheid
De interventie lijkt goed haalbaar. Laparoscopische adhesiolyse is in de meeste Nederlandse ziekenhuizen technisch en organisatorisch uitvoerbaar, mede doordat laparoscopische apparatuur breed beschikbaar is en in veel centra 24/7 GE-chirurgen en laparoscopische teams inzetbaar zijn. De voorkeur en ervaring van de chirurg en het operatieteam kunnen echter invloed hebben op de keuze voor laparoscopie, aangezien het een technisch uitdagende ingreep betreft. Desondanks voorziet de werkgroep geen wezenlijke belemmeringen voor de haalbaarheid van deze interventie binnen de Nederlandse setting.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Laparoscopische adhesiolyse biedt mogelijk voordelen ten opzichte van een open procedure, zoals kortere opnameduur en sneller herstel, hoewel de bewijskracht van het bewijs zeer laag is. De werkgroep acht dit veilig en haalbaar mits laagdrempelig wordt geconverteerd bij onvoldoende zicht of verhoogd risico op complicaties. Het hanteren van strikte selectielijsten voor laproscopische adhesiolyse acht de werkgroep niet wenselijk omdat dit patienten de kans kan onemen op sneller herstel. Aangezien de voordelen op de langere termijn beperkt zijn en een open procedure even goed verdedigbaar is, dient de uiteindelijke keuze steeds te worden afgestemd op de klinische situatie en de voorkeur van het behandelteam.
Eindoordeel:
Zwakke aanbeveling voor laparoscopische adhesiolyse
Onderbouwing
It is currently unknown whether laparoscopic surgical treatment of cord ileus has advantages over open surgical treatment. Laparoscopy appears to be associated with a short hospital stay and faster recovery, but there are also concerns about a possible increased risk of bowel injury. Long-term outcomes, such as recurrence, are unknown.
Population: Adult patients with ASBO undergoing adhesiolysis
Intervention: Laparoscopic adhesiolysis
Comparator: Open adhesiolysis
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
Open adhesiolysis |
Laparoscopic adhesiolysis |
||||
|
Mortality (critical) |
Relative risk: 0.37 (CI 95% 0.27 - 0.49) Based on data from 37627 participants in 20 studies
|
48 per 1000 |
18 per 1000 |
Very low Due to serious risk of bias1 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on mortality when compared with open adhesiolysis in adult patients with ASBO |
|
Difference: 30 fewer per 1000 (CI 95% 35 fewer - 24 fewer) |
|||||
|
Complications (critical) |
Relative risk: 0.51 (CI 95% 0.42 - 0.61) Based on data from 30161 participants in 11 studies
|
188 per 1000 |
96 per 1000 |
Very low Due to serious risk of bias2 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on complications when compared with open adhesiolysis in adult patients with ASBO. |
|
Difference: 92 fewer per 1000 (CI 95% 109 fewer - 73 fewer) |
|||||
|
Need for surgery for reoperation (important) |
Relative risk: 0.82 (CI 95% 0.71 - 0.96) Based on data from 21857 participants in 10 studies
|
61 per 1000 |
50 per 1000 |
Very low Due to serious risk of bias, Due to serious imprecision3 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on need for surgery when compared with open adhesiolysis in adult patients with ASBO |
|
Difference: 11 fewer per 1000 (CI 95% 18 fewer - 2 fewer) |
|||||
|
Recurrence of ASBO (important) |
Relative risk: 1.34 (CI 95% 0.64 - 2.79) Based on data from 320 participants in 2 studies
|
70 per 1000 |
94 per 1000 |
Very low Due to very serious imprecision4 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on recurrence of ASBO when compared with open adhesiolysis in adult patients with ASBO |
|
Difference: 24 more per 1000 (CI 95% 25 fewer - 125 more) |
|||||
|
Bowel injuries (important) |
Relative risk: 1.5 (CI 95% 0.93 - 2.44) Based on data from 452 participants in 5 studies
|
107 per 1000 |
161 per 1000 |
Very low Due to serious risk of bias, Due to serious imprecision5 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on bowel injuries when compared with open adhesiolysis in adult patients with ASBO |
|
Difference: 54 more per 1000 (CI 95% 7 fewer - 154 more) |
|||||
|
Length of hospital stay (important) |
Measured by: Scale: - Lower better Based on data from 23258 participants in 7 studies
|
10.0 Mean |
6.0 Mean |
Very low Due to serious risk of bias6 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on length of hospital stay when compared with open adhesiolysis in adult patients with ASBO |
|
Difference: MD 3.97 lower (CI 95% 6.93 lower - 1.01 lower) |
|||||
|
IC admission (important) |
Based on data from 190 participants in 1 study
|
Krielen (2023) reported a RR of 0.68 (95% CI 0.39 to 1.18), in favor of the patients who underwent laparoscopic adhesiolysis. |
Very low Due to serious imprecision7 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on IC admission when compared with open adhesiolysis in adult patients with ASBO |
|
|
Return of bowel function (important) |
Based on data from 348 participants in 2 studies
|
Chin (2023) reported a median difference of -2 days, in favor of the patients who underwent laparoscopic adhesiolysis. |
Very low Due to serious imprecision8 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on return of bowel function when compared with open adhesiolysis in adult patients with ASBO |
|
|
Nutritional status (important) |
Based on data from 130 participants in 1 study
|
Furukawa (2025) reported a median difference of -1 day, in favor of the patients who underwent laparoscopic adhesiolysis. |
Very low Due to serious imprecision9 |
The evidence is very uncertain about the effect of laparoscopic adhesiolysis on nutritional status when compared with open adhesiolysis in adult patients with ASBO |
|
|
Incisional hernias (important) |
|
None of the included studies reported the outcome measure incisional hernias. |
|
|
|
|
Conversions (important) |
Conversion rates in laparoscopic adhesiolysis ranged from 13.5% to 46.8% (11 studies, n not pooled) |
Not applicable (non-comparative outcome) |
Not applicable (non-comparative outcome) |
Not applicable (non-comparative outcome) |
|
- Risk of Bias: serious. baseline equivalence not reported/inadequate baseline equivalence, inadequate calculation of study size, inadequate follow-up, ;
- Risk of Bias: serious. baseline equivalence not reported/inadequate baseline equivalence, inadequate endpoints;
- Risk of Bias: serious. inadequate calculation of study size, inadequate control group, inadequate baseline equivalence, inadequate follow-up; Imprecision: serious. Wide confidence intervals;
- Imprecision: very serious. Wide confidence intervals;
- Risk of Bias: serious. baseline equivalence not reported/inadequate, inadequate endpoints; Imprecision: serious. Wide confidence intervals;
- Risk of Bias: serious. baseline equivalence not reported/inadequate, inadequate endpoints;
- Imprecision: serious. Wide confidence intervals;
- Imprecision: serious. Wide confidence intervals;
- Imprecision: serious. Low number of patients;
Description of studies
A total of six studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Krielen (2020) performed a systematic review of the literature up to 20th of May 2019. The systematic review included RCTs, matched studies, and unmatched studies in which children or adults were included who have undergone full laparoscopic versus open adhesiolysis for adhesive small bowel obstruction. In total, one RCT and thirteen observational studies were included in the systematic review.
Quah (2019) performed a systematic review and meta-analysis up to 2017. RCTs and case-controlled studies that compared laparoscopic adhesiolysis with open adhesiolysis were included. In total, eighteen case-controlled studies were included in the systematic review. In addition to Krielen (2020), this analysis included two studies from Quah (2019): Grafen, 2010 and Chopra, 2003.
Darbyshire (2021) performed a single-centre prospective cohort study to compare characteristics and outcomes of patients having either open or laparoscopic adhesiolysis. Patients who underwent surgery for ASBO were included in the study.
Krielen (2023) performed a prospective cross-sectional cohort study to assess current practice and related outcomes of the management of ASBO in the Netherlands. All consecutive patients with a suspicion of ASBO during six months in all Dutch participating hospitals between April 2019 and December 2020 were included.
Chin (2023) performed a descriptive, retrospective study to compare the outcomes of laparoscopic interventions with that of open surgery for the surgical treatment of SBO. Patients admitted with SBO who underwent laparoscopic or open surgery at a single academic medical center from June 2016 to December 2019 were included.
Furukawa (2025) performed a retrospective, single-centre study to evaluate the feasibility of laparoscopic surgery for SBO by comparing to open surgery. All patients who underwent exploratory laparoscopy between 2014 and 2021 were included in the laparoscopy group and those who did not undergo exploratory laparoscopy between 2010 and 2013 were included in the open surgery group.
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
Included in systematic review Krielen, 2020 |
||||||
|
Sallinen, 2019 |
N at baseline: Intervention: 51 Control: 49
Age (median, IQR) Intervention: 73y (60-81) Control: 74y (60-84)
Sex (female) Intervention: 34 (67%) Control: 31 (63%) |
Intervention: Laparoscopy
Control: Open surgery |
NR |
Length of postoperative hospital stay
Time to bowel function
Death at 30 days
Iatrogenic bowel lesions
Readmission within 30 days |
Funding: Funded by Vatsatauten Tutkimussaatio Foundation, Mary and Georg Ehrnrooth’s Foundation, Martti I. Turunen Foundation, and Governmental competitive research funds. No commercial entities provided support or were involved in the trial.
Conflicts of interest: Some of the authors received grants from the above mentioned organizations. |
HIGH (blinding of participants and personnel) |
|
Hackenberg, 2017 |
N at baseline Intervention: 25 (50.0%) Control: 25 (50.0%)
Age (mean, SD) I: 63.8 years C: 72 years
Sex (male) I: 13 (52%) C: 22 (33%)
Conversion laparoscopic to open adhesiolysis: |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Serious complications
Iatogenic bowel lesions
Missed iatrogenic injuries
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
LOW |
|
Yao, 2017 |
N at baseline Intervention: 52 (50.0%) Control: 52 (50.0%)
Age (mean, SD) I: 69 years C: 77 years
Sex (male) I: 42 (53.8%) C: 39 (50%)
Conversion laparoscopic to open adhesiolysis: |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Time to flatus
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
LOW |
|
Behman, 2017 |
N at baseline Intervention: 673 (7.8%) Control: 7911 (92.2%)
Age (mean, SD) I: 63.4 years C: 67.2 years
Sex (male) I: 287 (42.6%) C: 3075 (38.9%)
Conversion laparoscopic to open adhesiolysis: NR |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Serious complications
Length of hospital stay
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
Some concerns (baseline equivalence of groups not reported) |
|
Byrne, 2014 |
N at baseline Intervention: 83 (30.9%) Control: 186 (69.1%)
Age (mean, SD) I: 65.1 years C: 66.5 years
Sex (male) I: 41 (49.4%) C: 71 (38.2%)
Conversion laparoscopic to open adhesiolysis: 32 (38.6%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Operartive time
Time to flatus
Readmissions
Unplanned reoperations
Missed iatrogenic |
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
HIGH (inadequate prospective calculation of study size, inadequate control group, inadequate baseline equivalence of groups) |
|
Davies, 2014 |
N at baseline Intervention: 38 (37.3%) Control: 64 (62.7%)
Age (mean, SD) I: 52.2 years C: 57 years
Sex (male) I: 13 (34.2%) C: 28 (43.8%)
Conversion laparoscopic to open adhesiolysis: 10 (26.3%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Readmissions
Unplanned reoperations
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
HIGH (inadequate follow-up period, loss-to-follow-up >5%, inadequate prospective calculation of study size, inadequate control group, inadequate baseline equivalence of groups) |
|
Kelly, 2014 |
N at baseline Intervention: 1434 (14.9%) Control: 8185 (85.1%)
Age (mean, SD) I: 58.2 years C: 63.5 years
Sex (male) I: 458 (31.9%) C: 3109 (38%)
Conversion laparoscopic to open adhesiolysis: NR |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Serious complications
Operative time
Length of hospital stay
Unplanned reoperations
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
LOW |
|
Lin, 2016 |
N at baseline Intervention: 101 (50.0%) Control: 101 (50.0%)
Age (mean, SD) I: 57.3 years C: 58.1 years
Sex (male) I: 48 (47.5%) C: 50 (49.5%)
Conversion laparoscopic to open adhesiolysis: NR |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Serious complications
Operative time
Time to flatus
Length of hospital stay
Unplanned reoperations
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
Some concerns (inadequate endpoints to the aim of the study, inadequate baseline equivalence of groups) |
|
Lombardo, 2014 |
N at baseline Intervention: 1256 (18.6%) Control: 5506 (81.4%)
Age (mean, SD) I: 57.4 years C: 63.4 years
Sex (male) I: 415 (33%) C: 2077 (37.7%)
Conversion laparoscopic to open adhesiolysis: 422 (33.6%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Serious complications
Unplanned reoperations |
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
LOW |
|
Mancini, 2008 |
N at baseline Intervention: 702 (11.4%) Control: 5463 (88.6%)
Age (mean, SD) I: 56.6 years C: 63.1 years
Sex (male) I: 218 (31.1%) C: 2021 (35.8%)
Conversion laparoscopic to open adhesiolysis: 121 (17.2%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
LOW |
|
Nordin, 2016 |
N at baseline Intervention: 34 (50.0%) Control: 34 (50.0%)
Age (mean, SD) I: 34 years C: 34 years
Sex (male) I: 13 (38.2%) C: 13 (38.2%)
Conversion laparoscopic to open adhesiolysis: NR |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Serious complications
Operative time
Length of hospital stay
Readmissions
Unplanned reoperations
Iatrogenic bowel lesions
Missed iatrogenic injuries |
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
LOW |
|
Saleh, 2014 |
N at baseline Intervention: 919 (19.9%) Control: 3697 (80.1%)
Age (mean, SD) I: 57 years C: 62.3 years
Sex (male) I: 285 (31%) C: 1381 (37.4%)
Conversion laparoscopic to open adhesiolysis: NR |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Serious complications
Length of stay
Unplanned reoperations
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
Some concerns (inadequate endpoints to the aim of the study, baseline equivalence of groups not reported) |
|
Sebastian-Valverde, 2019 |
N at baseline Intervention: 78 (29.8%) Control: 184 (70.2%)
Age (mean, SD) NR
Sex (male) NR
Conversion laparoscopic to open adhesiolysis: 30 (38.5%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Serious complications
Operative time
Readmissions
Unplanned reoperations
Missed iatrogenic injuries
|
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
Some concerns (inadequate prospective calculation of the study size, inadequate baseline equivalence of groups) |
|
Wullstein, 2003 |
N at baseline Intervention: 52 (50.0%) Control: 52 (50.0%)
Age (mean, SD) I: 59.3 years C: 64.8 years
Sex (male) I: 14 (26.9%) C: 12 (23.1%)
Conversion laparoscopic to open adhesiolysis: 27 (51.9%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Iatrogenic bowel lesions |
Age and gender data retrieved from SR Quah
No information about funding and conflicts of interest for individual studies |
HIGH (inadequate inclusion of consecutive patients, inadequate control group, inadequate statistical analyses) |
|
Included in systematic review Quah, 2019 |
||||||
|
Chopra, 2003 |
N at baseline Intervention: 23 Control: 52
Age (mean, SD) Intervention: 59.7 years Control: 58.7 years
Sex Intervention: NR Control: NR
Conversion laparoscopic to open adhesiolysis: 11 (not included in control group for this analysis) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Mortality
Length of stay
|
No information about funding and conflicts of interest for individual studies |
Some concerns |
|
Grafen, 2010 |
N at baseline Intervention: 90 Control: 3
Age (mean, SD) Intervention: 59 Control: 75
Sex (male) Intervention: 29 (32.2%) Control: 2 (66.7%)
Conversion laparoscopic to open adhesiolysis: NR |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
First bowel movement
Duration of hospital stay
Early mortality |
No information about funding and conflicts of interest for individual studies |
Some concerns |
|
Individual studies |
||||||
|
Darbyshire, 2021 |
N at baseline Intervention: 228 Control: 71
Age (mean, SD) Intervention: 70 (IQR 53-78) Control: 69 (IQR 52.5-80.5)
Sex (male) Intervention: 95 (41.7%) Control: 25 (35.2%)
Conversion laparoscopic to open adhesiolysis: 72 (31.6%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Inhospital mortality
Length of stay
Bowel resection |
The project did not receive funding. No conflicts of interest reported.
|
LOW |
|
Krielen, 2023 |
N at baseline Intervention: 97 Control: 93
Age (mean, SD) Intervention: 67.96 years (SD 15.82) Control: 68.38 years (SD 15.16)
Sex (male) Intervention: 47 (48.5%) Control: 47 (50.5%)
Conversion laparoscopic to open adhesiolysis: 35 (36%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
90 days |
Length of stay
ICU admission
In-hospital mortality
Complications
Recurrence |
No funding was received. No conflicts of interest were declared. |
Some concerns |
|
Chin, 2023 |
N at baseline Intervention: 109 Control: 170
Age (mean, SD) Intervention: 65 years (SD ± 16) Control: 64 years (SD ± 16)
Sex (male) Intervention: 51 (46.8%) Control: 65 (38.2%)
|
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
NR |
Length of stay
30-day mortality
Reoperation
Return of bowel function
|
Funding NR No conflicts of interest declared. |
Some concerns |
|
Furukawa, 2025 |
N at baseline Intervention: 65 Control: 65
Age (mean, SD) Intervention: 78 years (range 23-93) Control: 74 years (range 32-96)
Sex (male) Intervention: 30 Control: 33
Conversion laparoscopic to open adhesiolysis: 12 (18.5%) |
Intervention: Laparoscopic adhesiolysis Control: Open adhesiolysis |
27.3 months – 38.7 months |
Intraoperative organ injuries
Postoperative complications grade >2 / grade > 3
Mortality
Days from surgery to first oral intake
Postoperative hospital stay
Recurrence of SBO
Reoperation due to recurrence of SBO |
No funding received and no conflicts of interest reported. |
LOW |
*For further details, see risk of bias table in the appendix
Results
Mortality (critical)
One systematic review and six studies reported the outcome measure mortality (Chin, 2023; Chopra, 2003; Darbyshire, 2021; Furukawa, 2025; Grafen, 2010; Krielen, 2020; Krielen, 2023).
In total, 90 of the 5664 patients (1.6%) who underwent laparoscopic adhesiolysis died, compared with 1532 of the 31963 patients (4.8%) who underwent open adhesiolysis (Figure 1). The risk ratio was 0.37 (95% CI 0.27 to 0.49), in favor of the patients who received laparoscopic adhesiolysis. This difference is considered clinically relevant.
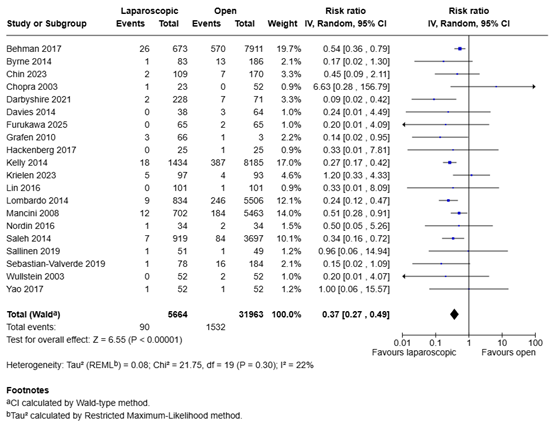
Figure 1. Mortality for laparoscopic adhesiolysis versus open adhesiolysis in adult patients with ASBO
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval.
Complications (critical)
One systematic review and two studies reported the outcome measure serious complications (Furukawa, 2025; Krielen, 2020; Krielen, 2023).
In total, 403 of the 4311 patients (9.3%) who underwent laparoscopic adhesiolysis suffered from a serious complication, compared with 4850 of the 25850 patients (18.8%) who underwent open adhesiolysis (Figure 2). The risk ratio was 0.51 (95% CI 0.42 to 0.61), in favor of the patients who received laparoscopic adhesiolysis. This difference is considered clinically relevant.
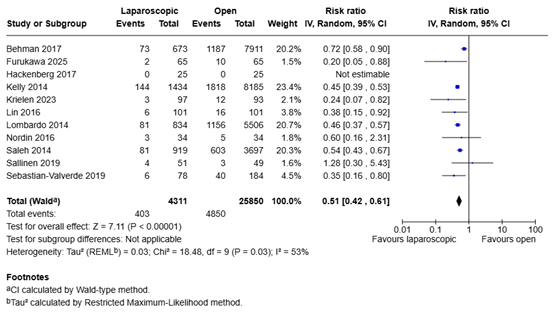
Figure 2. Complications for laparoscopic adhesiolysis versus open adhesiolysis in adult patients with ASBO
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval.
Length of hospital stay (important)
One systematic review and six studies reported the outcome measure length of hospital stay (Chin, 2023; Chopra, 2003; Darbyshire, 2021; Furukawa, 2025; Grafen, 2010; Krielen, 2020; Krielen, 2023).
The mean difference in length of hospital stay between the 3278 patients who underwent laparoscopic adhesiolysis and the 19980 patients who underwent open adhesiolysis was -3.97 days (95% CI -6.93 to -1.01), in favor of the patients who underwent laparoscopic adhesiolysis (Figure 3). This difference is considered clinically relevant.
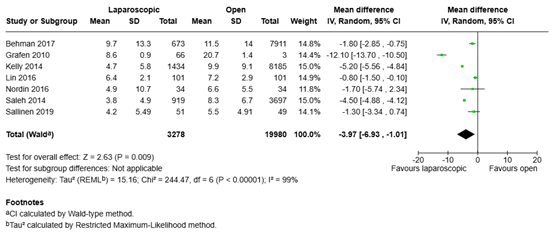
Figure 3. Length of hospital stay for laparoscopic adhesiolysis versus open adhesiolysis in adult patients with ASBO
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval.
Chin (2023) reported length of stay. Since a median and range was reported, the results could not be pooled. The patients who underwent laparoscopic adhesiolysis (n=109) had a median length of stay of 10 days (range 0-72), compared with a median length of stay of 16 days (range 0-246) for the patients who underwent open adhesiolysis (n=170). The median difference was -6 days, in favor of the patients who underwent laparoscopic adhesiolysis. This difference is considered clinically relevant.
Chopra (2003) reported length of stay. Since only a mean was reported, the results could not be pooled. The patients who underwent laparoscopic adhesiolysis (n=23) had a mean length of stay of 7.3 days, compared with a mean length of stay of 13.3 days for the patients who underwent open adhesiolysis (n=52). The mean difference was -6 days, in favor of the patients who underwent laparoscopic adhesiolysis.
Darbyshire (2021) reported length of stay. Since a median and IQR was reported, the results could not be pooled. The patients who underwent laparoscopic adhesiolysis (n=228) had a median length of stay of 8.3 days (IQR 5.2-15.7), compared with a median length of stay of 14.4 days (IQR 11.2-24.9) for the patients who underwent open adhesiolysis (n=71). The median difference was -6.1 days, in favor of the patients who underwent laparoscopic adhesiolysis. This difference is considered clinically relevant.
Furukawa (2025) reported postoperative hospital stay. Since a median and range was reported, the results could not be pooled. The patients who underwent laparoscopic adhesiolysis (n=65) had a median length of stay of 8 days (range 3-51), compared with a median length of stay of 12 days (range 1-89) for the patients who underwent open adhesiolysis (n=65). The median difference was -4 days, in favor of the patients who underwent laparoscopic adhesiolysis. This difference is considered clinically relevant.
Krielen (2023) reported length of stay. Since a median and range was reported, the results could not be pooled. The patients who underwent laparoscopic adhesiolysis (n=97) had a median length of stay of 8.00 days (range 0-109), compared with a median length of stay of 11.00 days (range 1-129) for the patients who underwent open adhesiolysis (n=93). The median difference was -3 days, in favor of the patients who underwent laparoscopic adhesiolysis. This difference is considered clinically relevant.
IC admission (important)
One study reported the outcome measure ICU admission (Krielen, 2023). In total, 17 of the 97 patients (17.5%) who underwent laparoscopic adhesiolysis were admitted to the ICU, compared with 24 of the 93 patients (25.8%) who underwent open adhesiolysis. The risk ratio was 0.68 (95% CI 0.39 to 1.18), in favor of the patients who underwent laparoscopic adhesiolysis. This difference is considered clinically relevant.
Need for surgery / (unplanned) reoperation (important)
One systematic review and one study reported the outcome measure (unplanned) reoperation (Chin, 2023; Krielen, 2020).
In total, 183 of the 3681 patients (5.0%) who underwent laparoscopic adhesiolysis received (unplanned) reoperation, compared with 1112 of the 18176 patients (6.1%) who underwent open adhesiolysis. The risk ratio was 0.82 (95% CI 0.71 to 0.96), in favor of the patients who underwent laparoscopic adhesiolysis. This difference is not considered clinically relevant.
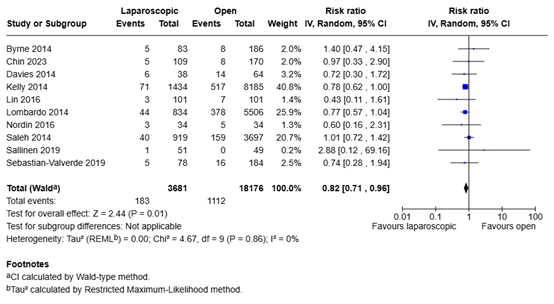
Figure 4. Need for surgery for laparoscopic adhesiolysis versus open adhesiolysis in adult patients with ASBO
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval.
Return of bowel function (important)
Two studies reported the outcome measure return of bowel function (Chin, 2023; Grafen, 2010). Since the studies reported the results differently, the results could not be pooled.
Chin (2023) reported the return of bowel function in days. The median amount of days until return of bowel function was 4 (range 0-20) for the patients who underwent laparoscopic adhesiolysis (n=109), compared with 6 (range 0-70) for the patients who underwent open adhesiolysis (n=170). The median difference was -2 days, in favor of the patients who underwent laparoscopic adhesiolysis. This difference is considered clinically relevant.
Grafen (2010) reported first bowel movement in days. The mean amount of days until first bowel movement was 2.5 (SD ± 0.3) for the patients who underwent laparoscopic adhesiolysis (n=66), compared with 7.6 (SD ± 4.3) for the patients who underwent open adhesiolysis (n=3). The mean difference was -5.10 days (95% CI -9.97 to -0.23), in favor of the patients who underwent laparoscopic adhesiolysis. This difference is considered clinically relevant.
Nutritional status (important)
One study reported the outcome measure days from surgery to first oral intake (Furukawa, 2025). The median amount of days from surgery to first oral intake was 4 (range 1-19) for the patients who underwent laparoscopic adhesiolysis (n=65), compared with 5 (range 2-89) for the patients who underwent open adhesiolysis (n=65). The median difference was -1 day, in favor of the patients who underwent laparoscopic adhesiolysis. This difference is considered clinically relevant.
Incisional hernias (important)
None of the studies reported the outcome measure incisional hernias.
Recurrence of ASBO (important)
Two studies reported the outcome measure recurrence of ASBO (Furukawa, 2025; Krielen, 2023).
In total, 15 of the 162 patients (9.3%) who underwent laparoscopic adhesiolysis had recurrence of ASBO, compared with 11 of the 158 patients (7.0%) who underwent open adhesiolysis (Figure 5). The risk ratio was 1.34 (95% CI 0.64 to 2.79), in favor of the patients who underwent open adhesiolysis. This difference is considered clinically relevant.
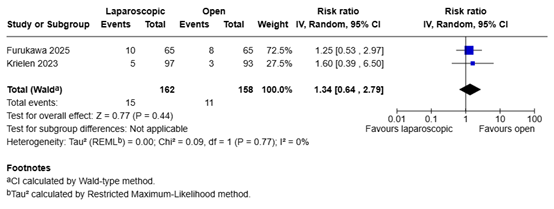
Figure 5. Recurrence of ASBO for laparoscopic adhesiolysis versus open adhesiolysis in adult patients with ASBO
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval.
Conversions (important)
The reported conversion rates in laparoscopic adhesiolysis ranged from 13.5% to 46.8% (Hackenberg, 2017; Yao, 2017; Byrne, 2014; Davies, 2014; Lombardo, 2014; Mancini, 2008; Sebastian-Valverde, 2019; Wullstein, 2003; Darbyshire, 2021; Krielen, 2023; Chin, 2023; Furukawa, 2025). This represents a non comparative outcome.
Bowel injuries (important)
One systematic review and one study reported the outcome measure bowel injuries / iatrogenic bowel lesions (Furukawa, 2025; Krielen, 2020).
In total, 37 of the 227 patients (16.3%) who underwent laparoscopic adhesiolysis had a bowel injury, compared with 24 of the 225 patients (10.7%) who underwent open adhesiolysis. The risk ratio was 1.50 (95% CI 0.93 to 2.44), in favor of the patients who underwent open adhesiolysis. This difference is considered clinically relevant.
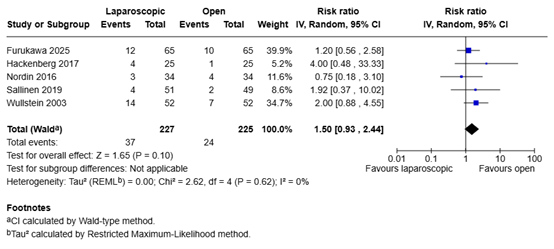
Figure 6. Bowel injuries for laparoscopic adhesiolysis versus open adhesiolysis in adult patients with ASBO
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval.
What are the favorable and unfavorable effects of laparoscopic surgery compared with open surgery for ASBO in adult patients?
Table 1. PICO
|
Patients |
Adult patients with ASBO undergoing adhesiolysis |
|
Intervention |
Laparoscopic adhesiolysis |
|
Control |
Open adhesiolysis |
|
Outcomes |
Mortality, complications, length of hospital stay, IC admission, need for surgery, return of bowel function, nutritional status, incisional hernias, recurrence of ASBO, conversions, bowel injuries |
|
Other selection criteria |
Study design: systematic reviews, randomized controlled trials, and observational studies |
Relevant outcome measures
The guideline panel considered mortality and complications as critical outcome measures for decision making; and length of hospital stay, IC admission, need for surgery, return of bowel function, nutritional status, incisional hernias, recurrence of ASBO, conversions, and bowel injuries as important outcome measures for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
The guideline panel defined the following as a minimal clinically (patient) important difference:
- Mortality: 25% (RR < 0.8 or RR > 1.25)
- Complications: 25% (RR < 0.8 or RR > 1.25)
- Length of hospital stay: 1 day
- IC admission: 25% (RR < 0.8 or RR > 1.25)
- Need for surgery: 25% (RR < 0.8 or RR > 1.25)
- Return of bowel function: 1 day
- Nutritional status: 1 day
- Incisional hernias: 25% (RR < 0.8 or RR > 1.25)
- Recurrence of ASBO: 25% (RR < 0.8 or RR > 1.25)
- Conversions (non comparative)
- Bowel injuries: 25% (RR < 0.8 or RR > 1.25)
Search and select (Methods)
A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. The databases were searched from 2019 up to 5th of May and 7th of May, respectively, for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) small bowel obstruction and (2) laparoscopic surgery. Duplicates were removed using EndNote software. After deduplication a total of 715 records were imported for title/abstract screening. Initially, 25 studies were selected based on title and abstract screening. After reading the full text, nineteen studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and six studies were included.
- Chin RL, Lima DL, Pereira X, Romero-Velez G, Friedmann P, Dawodu G, Sterbenz K, Yamada J, Sreeramoju P, Smith V, Malcher F. Assessing outcomes in laparoscopic vs open surgical management of adhesive small bowel obstruction. Surg Endosc. 2023 Feb;37(2):1376-1383. doi: 10.1007/s00464-022-09314-7. Epub 2022 May 19. PMID: 35587296.
- Chopra R, McVay C, Phillips E, Khalili TM. Laparoscopic lysis of adhesions. Am Surg. 2003 Nov;69(11):966-8. PMID: 14627257.
- Darbyshire AR, Kostakis I, Pucher PH, Toh S, Mercer SJ. The impact of laparoscopy on emergency surgery for adhesional small bowel obstruction: prospective single centre cohort study. Ann R Coll Surg Engl. 2021 Apr;103(4):255-262. doi: 10.1308/rcsann.2020.7079. Epub 2021 Mar 8. PMID: 33682461; PMCID: PMC10334926.
- Furukawa S, Kato K, Susa Y, Yamabuki T, Takada M, Kinoshita Y, Anbo Y, Nakamura F, Hirano S. Is Exploratory Laparoscopy the Optimal Surgical Strategy for Small Bowel Obstruction? A Single-Center Retrospective Cohort Study With Propensity Score- Matched Analysis. Asian J Endosc Surg. 2025 Jan-Dec;18(1):e70056. doi: 10.1111/ases.70056. PMID: 40189409.
- Grafen FC, Neuhaus V, Schöb O, Turina M. Management of acute small bowel obstruction from intestinal adhesions: indications for laparoscopic surgery in a community teaching hospital. Langenbecks Arch Surg. 2010 Jan;395(1):57-63. doi: 10.1007/s00423-009-0490-z. Epub 2009 Mar 28. PMID: 19330347.
- Krielen P, Di Saverio S, Ten Broek R, Renzi C, Zago M, Popivanov G, Ruscelli P, Marzaioli R, Chiarugi M, Cirocchi R. Laparoscopic versus open approach for adhesive small bowel obstruction, a systematic review and meta-analysis of short term outcomes. J Trauma Acute Care Surg. 2020 Jun;88(6):866-874. doi: 10.1097/TA.0000000000002684. PMID: 32195994.
- Krielen P, Kranenburg LPA, Stommel MWJ, Bouvy ND, Tanis PJ, Willemsen JJ, Migchelbrink J, de Ree R, Bormans EMG, van Goor H, Ten Broek RPG; ASBO Snapshot Study Group. Variation in the management of adhesive small bowel obstruction in the Netherlands: a prospective cross-sectional study. Int J Surg. 2023 Aug 1;109(8):2185- 2195. doi: 10.1097/JS9.0000000000000471. PMID: 37288588; PMCID: PMC10442142.
- Quah GS, Eslick GD, Cox MR. Laparoscopic versus open surgery for adhesional small bowel obstruction: a systematic review and meta-analysis of case-control studies. Surg Endosc. 2019 Oct;33(10):3209-3217. doi: 10.1007/s00464-018-6604-3. Epub 2018 Nov 20. PMID: 30460502.
- Sallinen V, Di Saverio S, Haukijärvi E, Juusela R, Wikström H, Koivukangas V, Catena F, Enholm B, Birindelli A, Leppäniemi A, Mentula P. Laparoscopic versus open adhesiolysis for adhesive small bowel obstruction (LASSO): an international, multicentre, randomised, open-label trial. Lancet Gastroenterol Hepatol. 2019 Apr;4(4):278-286. doi: 10.1016/S2468-1253(19)30016-0. Epub 2019 Feb 12. PMID: 30765264.
Beoordelingsdatum en geldigheid
Publicatiedatum : 09-04-2026
Beoordeeld op geldigheid : 09-04-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS)
De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met schouderinstabiliteit.
Werkgroep richtlijn strengileus
- dr. R.P.G. (Richard) ten Broek, chirurg Radboud UMC, NVvH – voorzitter richtlijnwerkgroep
- dr. C. (Caroline) Andeweg, chirurg St. Jansdal Harderwijk, NVvH
- Prof. dr. M. (Marja) Boermeester, chirurg Amsterdam UMC, NVvH
- Dhr. dr. F.T.J. (Floris) Ferenschild, chirurg Radboud UMC, NVvH
- dr. H.A. (Harmke) Polinder-Bos, klinisch geriater Erasmus MC, NVKG
- Mevr. E. (Elif) Kilicoglu, diëtist, CWZ Nijmegen, NVD
- Mevr. drs. M.W. (Wiesje) Prins, radioloog Maasziekenhuis, NVvR
- drs. T.W. (Thomas) van den Goorbergh, spoedeisende hulp, St. Antonius Ziekenhuis Nieuwegein, NVSHA
- Mevr. S. (Silvie) Dronkers, ervaringsdeskundige en patiëntvertegenwoordiger Stichting Darmkanker Nederland † (in herinnering)
Klankbordgroep richtlijn strengileus
- dr. A. (Sander) van der Beek, internist Ziekenhuis Rivierenland, NIV
- dr. C. (Cor) de Kroon, gynaecoloog LUMC, NVOG
- Mevr. S.D.M. (Sabine) Theuns-Valks, kinderarts Albert Schweitzer Ziekenhuis, NVK
Met ondersteuning van
- dr. L.M. (Lisette) van Leeuwen, adviseur Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. E.R.L. (Evie) Verweg, junior adviseur Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel 1 Gemelde (neven)functies en belangen werkgroep
|
Naam |
Hoofdfunctie |
Neven-werkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Datum |
Restrictie |
|
Werkgroepleden |
|||||||||
|
Richard Ten Broek |
Chirurg, Post-doctoraal onderzoeker bij Radboud UMC afdeling heelkunde (betaald)
|
Redacteur Wetenschap bij Nederlaqnd Tijdschrift voor Geneeskunde (betaald)
|
geen
|
geen
|
*Radboud Oncologie fonds: MISTIC studie naar gebruik MRI en cineMRI om coloncarcinomen beter te stadiëren *ZonMw/KCE, BENEFIT beurs voor onderzoek naar preventie van recidief ileus, rol als projectleider. |
Speaker and/ or instructor on congres symposia, workshops and courses that have been sponsored by industry: Baxter and PolyMedics Innovations. Courses related to epidemiology, diagnosis and treatment of adhesions, no specific products have been discussed or promoted.
|
geen
|
19-1-2024
|
Geen |
| Floris Ferenschild
|
Kinder- en gastro-intestinaal chirurg Radboudumc |
Chirurg: betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
11-1-2025 |
|
|
Silvie Dronkers (Overleden 18-12-2025) |
Coördinator Patiëntenparticipatie en Belangenbehartiging |
Voorzitter Wooninitiatief Noorderzon
|
Geen |
Geen |
Geen |
Geen |
Geen |
24-11-2023 |
Geen |
|
Harmke Polinder-Bos |
Klinisch geriater, Erasmus MC
|
Geen |
Geen |
Geen |
COOP studie, financiering van ZonMW, lange termijn uitkomsten na COVID bij ouderen. ZonMW: Klinische fellow beurs voor de GRISAILLE study. Intregrating Intrinsic capacity in clinical practice. Studie waarin ik een Intrinsic capacity score ontwikkel en deze toepas in oudere patienten die een intensieve behandeling krijgen zoals een operatie. |
Behoudens dat de inhoud raakt aan mijn expertise in klinisch werk en onderzoek geen belangen. |
Geen |
1-12-2023 |
Geen |
|
Thomas van den Goorbergh |
Arts in opleiding tot spoedeisende hulp arts in het St Antonius Ziekenhuis te Nieuwegein. |
Instructor Advanced Life Support bij QTtime in Nieuwegein, betaald |
Geen |
Geen |
Geen |
Geen |
Geen |
8-12-2023 |
Geen |
|
Elif Kilicoglu |
Diëtist in het Canisius Wilhelmina Ziekenhuis (CWZ) |
Geen |
Geen |
Geen
|
Geen |
Geen |
Geen |
30-12-2023 |
Geen |
|
Wiesje Prins-van Uden |
Radioloog, Maasziekenhuis Pantein |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
12-1-2024 |
Geen |
|
Marja Boermeester |
Amsterdam UMC
|
Medisch Ethische Commissie, Amsterdam UMC, locatie AMC |
Geen |
Geen |
Johnson&Johnson (voorkomen wondinfecties); 3M (voorkomen wondinfecties); New Compliance; Ipsen; ZonMW TelaBio (outcome hernia repair)
|
Speaker and/or instructor for J&J/Ethicon, 3M, BD, Gore, TelaBio, Medtronic, GD Medical, Smith&Nephew, Molnlycke, Angiodynamics. Voorzitter van diverse andere richtlijncommissies bij Kennisinstituut/FMS. Alle adviesraden vallen buiten het onderwerp van de richtlijn. |
Geen |
14-1-2024 |
Geen |
|
Caroline Andeweg
|
Werkzaam als chirurg in St Jansdal ziekenhuis in Hardewijk |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
25-3-2024 |
Geen |
|
Klankbordgroepleden |
|||||||||
|
Cor de Kroon |
LUMC, gynaecoloog |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
15-12-2023 |
Geen |
|
Sabine Theuns-Valks |
Kinderarts-maag darm leverziekten |
Kinderarts bij Seys centra locatie Zwijndrecht (2,5 u per week)
|
Geen |
Geen |
Geen |
Geen |
Geen |
9-1-2024 |
Geen |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland en Stichting Darmkanker voor de knelpunteninventarisatie. Daarnaast nam een patiëntvertegenwoordiger van Stichting Darmkanker deel aan de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan Patiëntenfederatie Nederland en Stichting Darmkanker en de eventueel aangeleverde commentaren zijn bekeken en verwerkt
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
De kwalitatieve raming volgt na de commentaarfase
|
Module |
Uitkomst raming |
Toelichting |
|
Module Laparoscopische adhesiolysis versus open adhesiolysis |
geen financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5.000 patiënten) en zal daarom naar verwachting geen substantiële gevolgen hebben voor de collectieve uitgaven. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling van deze richtlijn is hieronder weergegeven.