Glyceryltrinitraat versus calcium kanaal blokkers
Uitgangsvraag
Wat is de beste behandeling voor chronische anale fissuren?
Aanbeveling
Start met diltiazem 2% (crème of gel, zes weken, twee tot drie keer daags intra-anaal) en verdere basistherapie in de vorm van leefstijl- en dieetadviezen*, aangevuld met laxantia ten behoeve van het verzachten van de ontlasting.
Overweeg bij het niet verdragen of falen van diltiazem over te stappen naar ISDN 1% (zes weken, vijf tot zes keer daags intra-anaal)
Overweeg het gebruik van bilateraal 25 eenheden botulinetoxine intersfincterisch (of het equivalent dysport van tweemaal 50 eenheden).
Overweeg bij persisterende klachten na acht tot twaalf weken als step-up botox te herhalen, eventueel gecombineerd met een fissurectomie.
Overweeg bij refractaire fissuren een niet-sfinctersparende operatie (laterale interne sfincterotomie (LIS)) uit te laten voeren door een ervaren behandelaar.
Wees terughoudend met het uitvoeren van een laterale interne sfincterotomie (LIS) bij vrouwen.
Zie eveneens het stroomdiagram.
*Voldoende bewegen, voldoende drinken
Overwegingen
Voor- en nadelen van de interventie en kwaliteit van het bewijs
In de vorige richtlijn wordt voor de conservatieve behandeling van chronische anale fissuren aanbevolen om te behandelen met Diltiazem 2% indien dit nog niet eerder heeft plaatsgevonden. Als eerder gestart is met lokaal nitraat behandeling, kan deze bij falen van therapie worden omgezet naar Diltiazem 2%. Botulinetoxine kan worden overwogen als alternatieve stap binnen de behandeling, of als step-up indien lokale therapie faalt, alvorens wordt overgegaan tot chirurgische interventie. Voor chirurgische behandeling kan worden gekozen voor een sfinctersparende operatieve ingreep, waarbij fissurectomie (al dan niet in combinatie met botulinetoxine èn excisie van een eventueel aanwezige sentinel pile/ hypertrofische papil) de voorkeur heeft. Een niet sfinctersparende operatie zoals de laterale interne sfincterotomie dient alleen uitgevoerd te worden bij refractaire chronische hogedruk fissuren die dus niet reageren op bovengenoemde therapieën. Bij vrouwen dient men zeer terughoudend te zijn met de laterale interne sfincterotomie. De operatie dient te worden uitgevoerd door een chirurg met proctologische expertise.
Op basis van de uitkomstmaat genezing van de fissuur lijken de conservatieve interventies glyceryl nitraat en calcium channel blockers te resulteren in meer genezing van de wond dan een placebo of geen interventie. De literatuur is niet eenduidig over het effect op genezing van de fissuur door glyceryl nitraat, calcium channel blockers (duur van therapie), botulinetoxine (plaats van injectie, hoeveelheid eenheden).
Laterale interne sfincterotomie lijkt te resulteren in meer genezing van de fissuur ten opzichte van conservatieve behandeling (chemische sfincterotomie) binnen zes maanden postoperatief, en dit lijkt zich na zes maanden voort te zetten. De bewijskracht hiervoor is laag. Verder kan niet met zekerheid gezegd worden welke chirurgische interventie resulteert in de meeste genezing van de fissuur.
Voor de cruciale uitkomstmaat incontinentie lijkt er weinig verschil te zijn in de incidentie na conservatieve behandeling met glyceryl nitraat, isosorbide mononitraat, calcium channel blockers of na botulinetoxine. De bewijskracht hiervoor is laag. Daarentegen lijken deze conservatieve behandelingen te resulteren in minder incontinentie ten opzichte van laterale interne sfincterotomie. Literatuur over incontinentie na verschillende (chirurgische) technieken (open of gesloten laterale interne sfincterotomie, fissurectomie) of na percutaneous posterior tibial nerve stimulation (PTNS) is niet duidelijk, gedateerd of niet beschikbaar. (Arroyo 2004, Boulos 1984, Filinigeri 2005, Gupta 2014, Magdy 2012, Mousavi 2009, Puighari 2010, Youssef 2015, Wiley 2004)
Op basis van de belangrijke uitkomstmaat pijn lijken glyceryl nitraat, botulinetoxine, calcium channel blockers, (open en gesloten) laterale interne sfincterotomie, percutaneous posterior tibialis zenuwstimulatie geen vermindering van pijn te geven (Ahmed 2018, Nour 2020, Ruiz-Tovar 2017).
De huidige literatuur maakt het moeilijk een onbetwist advies te geven ten aanzien van de conservatieve behandeling van fissura ani. Dit komt mede door het feit dat de verschillende studies zeer heterogeen zijn met grote variatie in uitkomstmaten (genezing, incontinentie en pijn) en doordat de follow up duur doorgaans kort is. De heterogeniteit wordt door verschillende factoren veroorzaakt waaronder inclusie van patiënten met verschillende definities van een chronische fissuur, patiënten die reeds andere behandelingen ondergaan hebben en het toestaan van additionele behandelingen (bijvoorbeeld diltiazem naast botox).
Het starten met een conservatieve behandeling, naast dieetadviezen, laxantia en advies bekkenfysiotherapie / bekkenfysiotherapie bij hogedruk fissuren, heeft op basis van consensus van de werkgroep de voorkeur door de afwezigheid van risico op blijvende incontinentie. Van belang is goed te achterhalen of het eerste deel van de ontlasting daadwerkelijk soepel is en hierbij laagdrempelig laxantia te starten.
Het gebruik van bekkenfysiotherapie bij acute en/of chronische fissuren is niet voldoende onderzocht en derhalve op basis van wetenschappelijke bewijs niet aan te raden noch af te raden. Echter, op basis van expert opinion kan bekkenfysiotherapie op individuele basis bij patiënten met proctologische problematiek overwogen worden (Van Reijn-Baggen, 2022).
Gelet op de bijwerkingen en therapietrouw is Diltiazem 2% crème of gel twee keer daags eerste keuze. Zeker indien patiënt eerder behandeld is met lokale nitraten is een switch naar Diltiazem aan te bevelen. Andersom kan na 6 weken behandeling met Diltiazem en uitblijven van (voldoende) resultaat worden geswitcht naar ISDN 1% 5-6 dd. Indien de ingestelde therapie door de huisarts, mits volledig (dieet- en leefstijladviezen, laxantia, zalf), effect heeft kan overwogen worden om deze medicatie te herhalen. Bij falen van conservatieve therapie is botulinetoxine, fissurectomie eventueel gecombineerd met botulinetoxine zo nodig gevolgd door een laterale interne sfincterotomie ons voorstel van step-up benadering. Botuline heeft de voorkeur gezien het reversibele effect op de sfincterfunctie. Er is geen bewijs voor een hogere dosering maar met inachtneming van de kosten adviseren wij om de voorkeur te geven aan dysport 25 EH bilateraal intersfincterisch poliklinisch toe te dienen, indien geen fissurectomie nodig is. Dit kan herhaald worden na 8-12 weken. Indien wel een fissurectomie nodig wordt geacht, kan deze eventueel worden gecombineerd met de standaard dosering botulinetoxine (bilateraal 25EH).
Bloedplaatjes-rijk-plasma is niet gangbaar in Nederland maar is wellicht een therapie waarover in de toekomst meer bekend wordt.
Indien er sprake is van een chronische fissuur met andere pathogenese, dus zonder aanwijzingen voor hypertonie, bevestigd door anale manometrie, kan een fissurectomie dan wel VY-plastiek worden overwogen.
Voor ons advies behandelalgoritme verwijzen we u naar het stroomdiagram.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Starten met conservatieve maatregelen inclusief lokale topicale behandeling heeft verreweg de voorkeur vooral gezien de lage kans op incontinentie. Crème wordt hierin doorgaans beter verdragen dan gel. Indien dit te weinig effect heeft, adviseren wij een volgende stap niet te lang uit te stellen. Onderschat de impact op dagelijks leven niet van een chronische fissuur. Bespreek het doel van de behandeling voor de patiënt voor het overgaan tot niet-sfinctersparende maatregelen. Het risico op incontinentie kan bij de patiënt een overweging zijn om te kiezen voor behandelingen met hogere kans op uitblijven van volledig herstel. In individuele gemotiveerde gevallen kan bekkenfysiotherapie als aanvullende behandeling worden aangeboden. Zie voor het patiëntenperspectief de module Patiëntenperspectief bij proctologie.
Kosten (middelenbeslag)
De prijs voor gel of crème ontloopt niet veel, Diltiazem gel €16.99 per verpakking (tube) en creme €14,63. ISDN is goedkoper (€3,10 per tube). Botuline toxine A is verkrijgbaar van meerdere farmaceuten. Botox is per 100 EH verpakt en kost €206,45 per flacon, dysport is goedkoper, 300EH voor €170,63 (€56,90 per 100EH). In beide producten zit evenveel botuline A toxine, de eenheden zijn dus hetzelfde.
In de studie van Samim (2012) werden de kosten van de behandeling met Diltiazem 2% en botulinetoxine met elkaar vergeleken. De kosten per patiënt van de behandeling met Diltiazem waren €63,85, in vergelijking met €73,89 voor behandeling met botulinetoxine. In deze vergelijking worden alleen de directe kosten van de behandeling meegenomen (en bijvoorbeeld niet de kosten van additionele behandeling die nodig was voor patiënten die niet genazen na de eerste behandeling). In de praktijk wordt vaak beide gedaan. Er zijn geen kosteneffectiviteit analyses gedaan naar chirurgische interventies. Operatieve behandeling valt uiteraard vaak duurder uit. Bekkenfysiotherapie wordt bij veel verzekeringen beperkt vergoed.
Aanvaardbaarheid, haalbaarheid en implementatie
Conservatieve maatregelen zoals dieetadviezen en laxantia, adviezen ten aanzien van bekkenbodem zijn makkelijk toepasbaar en toegankelijk, te geven in een consult. Het stroomdiagram is goed uitvoerbaar in alle ziekenhuizen.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Samenvattend en concluderend wordt, net zoals in de vorige richtlijn, op basis van best beschikbare literatuur, aanbevolen om voor de conservatieve behandeling van chronische anale fissuren te behandelen met Diltiazem 2% (calciumantagonist) crème indien dit nog niet eerder heeft plaatsgevonden. Als eerder gestart is met lokaal nitraat behandeling, kan deze bij falen van therapie worden omgezet naar Diltiazem 2% (of vice versa). Botulinetoxine (intersfincterisch kan worden overwogen als alternatieve stap binnen de behandeling, of als step-up wanneer lokale therapie faalt, alvorens wordt overgegaan tot chirurgische interventie. Voor chirurgische behandeling kan worden gekozen voor een sfinctersparende operatieve ingreep, waarbij fissurectomie (al dan niet in combinatie met botulinetoxine) de voorkeur heeft. De literatuur geeft geen onderscheid ten aanzien van incontinentie bij mannen of vrouwen. Echter als werkgroep richtlijn Protoctologie adviseren wij gezien het verschil in anatomie en bekkenbodem kwaliteit, met name op latere leeftijd bij vrouwen, zeer terughoudend te zijn met het uitvoeren van een LIS. Een LIS dient, bij geselecteerde patiënten, zeer weloverwogen gedaan te worden aangezien de kans op sfincterschade leidend tot incontinentieklachten – ook in een later stadium pas - aanzienlijk is.
Onderbouwing
Achtergrond
Deze richtlijn behandelt de behandeling van benigne, ongecompliceerde fissura ani. Atypische fissuren (ten gevolge van M. Crohn, infectieuze oorzaken of maligniteit) worden buiten beschouwing gelaten maar moeten wel meegenomen worden in de differentiaaldiagnose als een patiënt zich presenteert.
De breed geaccepteerde definitie van een anale fissuur is een radiaire (ischemische) ulceratie van het anoderm, distaal van de linea dentata en meestal posterieur gelegen (80 tot 90%) (Nelson, 2010; Altomare, 2011; Schouten, 1996). Kenmerkend van een anale fissuur is pijn na defecatie die één á twee uur kan aanhouden. Een anale fissuur kan tevens zorgen voor helderrood bloedverlies (Nelson, 2012).
De definitie van een chronische fissura ani is minimaal zes weken pijnklachten in combinatie met een macroscopisch aantoonbare fissuur. Ook fysiologische kenmerken dragen bij aan de definitie van chronisch, zoals een ‘sentinel pile’, opgeworpen wondranden, het a vue zijn van sfinctervezels of een inflammatoire poliep aan de inwendige begrenzing van de fissuur (Altomare, 2011).
Een fissura ani wordt veroorzaakt door hypertonie van de interne anale sfincter. Ten gevolge van pijn treedt een spasme op van de interne anale sfincter (Nelson, 2012). Hierdoor wordt de vascularisatie nog verder gecompromitteerd en kan ulceratie het gevolg zijn (Schouten). De behandeling van fissura ani richt zich dan ook op het opheffen van deze spasme. Behandelstrategieën zijn grofweg in te delen in conservatieve maatregelen (chemische relaxatie glad spierweefsel) en chirurgische interventie (Essani, 2005).
Tot op heden wordt in de literatuur de (partiële) laterale interne sfincterotomie (LIS) aangevoerd als ‘gouden standaard’ met genoemde genezingspercentages van 90 tot 100%, maar ten koste van een risico op ‘soiling’ of incontinentie van flatus (Nelson, 2012; Magdy). Ondanks dat in recente literatuur incontinentie niet meer wordt beschreven en incontinentie voor vocht en flatus tijdelijk lijkt, wordt geadviseerd een LIS te bewaren voor therapieresistente fissuren (Nelson 2012; Magdy). Andere chirurgische behandelingen als fissurectomie en anoplastiek berusten het excideren en aviveren van de fissuur met een vermeend minder grote kans op postoperatieve incontinentie (Nelson, 2011).
Operatieve interventies zijn onderhevig aan verschillen in techniek en uitvoering van de chirurg, anesthesie en patiëntkarakteristieken. Recente studies hebben gekeken naar verschillende chirurgische technieken en het effect daarvan op genezing en op incontinentie. Deze richtlijn zal ingaan op de effectiviteit (kans op herstel of recidief) van en de daadwerkelijke risico’s op incontinentie (en andere bijwerkingen) van de verschillende chirurgische interventies of modulatie daarvan.
Conclusies / Summary of Findings
Non-healing of the fissure (critical)
|
Very Low GRADE |
The evidence is very uncertain about the effect of glyceryl trinitrate (GTN) on non-healing of the fissure when compared with calcium channel blockers (CCB) in patients with chronic anal fissures.
Sources: Abd Elhady, 2009; Ala, 2012; Ansari, 2020; Bansal, 2016; Bielecki, 2003; Cevik, 2012; Ezri, 2003; Jawaid, 2009; Khaledifar, 2015; Kocher, 2002; Mustafa, 2006; Sanei, 2009; Shrivastava, 2007; Uluutku, 2001. |
Incontinence (critical)
|
Very Low GRADE |
The evidence is very uncertain about the effect of glyceryl trinitrate (GTN) on incontinence when compared with calcium channel blockers (CCB) in patients with chronic anal fissures.
Sources: Jawaid, 2009; Mustafa, 2006. |
Pain (important)
|
No GRADE |
No literature was available regarding the outcome measure pain for treatment with glyceryl trinitrate (GTN) versus calcium channel blockers (CCB) in patients with chronic anal fissures.
Sources: - |
Samenvatting literatuur
Description of studies
The randomized controlled trial of Mustafa (2022) investigated the effect of topical 0.2% glyceryl trinitrate (GTN) compared to lateral internal sphincterotomy (LIS). In total, 94 patients were included and randomly assigned to one of the treatments. Patients in the intervention group (n=47) received topical 0.2% glyceryl trinitrate ointment, while patients in the control group (n=47) underwent lateral internal sphincterotomy. Stool softener was prescribed for both groups. Four patients in the GTN-group and three patients in the LIS-group were lost to follow-up. The length of follow-up was six months post-treatment. Mustafa (2022) reported non-healing of the fissure and incontinence.
The randomized controlled trial of Tahir (2022) investigated the effect of treatment with anal advanced flap compared to LIS in patients with chronic anal fissures. In total, 100 patients were included and randomly allocated to one of the treatments. Patients in the intervention group (n=50) were operated through anal advanced flap procedure. Patients in the control group (n=50) underwent lateral sphincterotomy. Lateral sphincterotomy was performed under regional anesthesia with lithotomic positioning under standard open technique. Four patients in the GTN-group and three patients in the LIS-group were lost to follow-up. The maximum length of follow-up was three months. The reported outcome in Tahir (2022) was non-healing of the fissure.
The randomized controlled trial of Herreros (2021) investigated the effect of botulinum toxin injection plus topical diltiazem with botulinum toxin injection plus a placebo. In total, 70 participants were included and randomly assigned to one of the treatments. Patients in the intervention group (n=35) were treated with a botulinum injection combined with topical diltiazem, while patients in the control group (n=35) were treated with placebo instead of diltiazem. The maximum length of follow-up was twelve weeks. Herreros (2021) reported non-healing of the fissure and incontinence.
The randomized controlled trial of Khan (2021) investigated the effect of topical Glyceryl trinitrate 0.2% (GTN) compared to LIS in patients with chronic anal fissures. In total, 60 patients were included and randomly allocated to one of the treatments. Patients in the intervention group (n=30) were treated with topical Nitroglycerin for four times per day. Patients in the control group (n=30) underwent lateral sphincterotomy. The maximum length of follow-up was six weeks. The reported outcome in Khan (2021) was non-healing of the fissure.
The randomized controlled trial of Malik (2021) investigated the effect of topical Glyceryl trinitrate 0.2% (GTN) compared to fissurectomy with LIS in patients with chronic anal fissures. In total, 100 patients were included and randomly allocated to one of the treatments. Patients in the intervention group (n=50) were treated with 0.2% Glyceryl trinitrate ointment. Dose of administration was applied 1,5 to two centimeter in the anal canal for two times per day for a total period of two weeks. Patients in the control group (n=30) underwent fissurectomy with lateral sphincterotomy. The maximum length of follow-up was two weeks. The reported outcome in Malik (2021) was pain.
Boland (2020) described a systematic review that aimed to review the current level one evidence regarding management options for the treatment of patients with chronic anal fissure. Boland (2020) searched Pubmed, the Cochrane Library Database, and Scopus to identify randomized controlled trials comparing treatment modalities for anal fissure published between January 2000 and February 2020. The last date of search was the 8th of February 2020. The study of Boland (2020) included randomized controlled trials that (1) were published in English language; (2) directly compared management strategies for anal fissure; (3) reported healing rates of fissure at 8 weeks post initiation of therapy; (4) reported healing as per definition of absence of pain and complete re-epithelialization; and (5) reported healing after one course of treatment only. Studies with non-randomized data, studies that did not compare management strategies, non-English studies, and studies with unclear methodology or unclear or poor definitions for healing were excluded. Boland (2020) identified nine randomized controlled trials, involving a total of 775 patients, that met the inclusion criteria for the systematic review (Alvandipour, 2018; Arroyo, 2005; Arroyo, 2004; Arslan, 2012; Berkel, 2014; Evans, 2001; Libertiny, 2002; Nasr, 2010; Valizadeh, 2012). The reported outcome measures in the study were non-healing and incontinence.
Sahebally (2018a) described a systematic review of randomized controlled trials that aimed to re-appraise the existing literature and perform an updated systematic review and meta-analysis to evaluate the efficacy, safety, and tolerability of botulinum toxin injection compared to application of nitroglycerin ointment in the treatment of chronic anal fissure. Sahebally (2018a) searched the online databases of Pubmed, EMBASE, Cochrane Central Register of Controlled Trials as well as Google Scholar for relevant articles. The last date of search was the 1st of April 2017. The study of Sahebally (2018a) included trials that were published in English language and directly compared local botulinum toxin injection versus topical nitrates. Studies that examined acute fissure only, studies that examined chronic fissure in children, and studies that examined anal stenosis/stricture were excluded. Studies that evaluated botulinum toxin (or topical nitrates) only, without direct comparison to the other therapeutic strategy were not eligible for inclusion. A total of six randomized controlled trials involving 393 patients were included (Abd Elhady, 2009; Berkel, 2014; Brisinda, 2007; Brisinda 1999; De Nardi, 2006; Festen, 2009). The reported outcome measures in the study were non-healing and incontinence.
The study of Sahebally (2018b) aimed to perform a systematic review and meta-analysis to compare the efficacy of lateral internal sphincterotomy with anal advancement flap in patients with chronic anal fissures. Sahebally (2018b) searched the online databases of Medline, CINAHL, EMBASE, Cochrane Central Register of Controlled Trials, Google Scholar, and colorectal conference abstracts. The latest search was performed on January 31st. Sahebally (2018b) only included studies that directly compared lateral internal sphincterotomy with anal advancement flap for the management of chronic anal fissures. Studies that evaluated lateral internal sphincterotomy (or anal advancement flap) only, without direct comparison to the other technique were excluded. A total of four studies involving 150 patients were included. Two studies were randomized controlled trials (Leong, 1995; Hancke 2010, Patel, 2011; Magdy, 2012). Two of these studies were randomized controlled trials and were included in this review (Leong, 1995; Magdy, 2012). The reported outcome measures in the study were non-healing and incontinence.
The systematic review and meta-analyses of Nelson (2017) assessed the effect of all published conservative and surgical treatment options for anal fissure. Nelson (2017) searched the Cochrane Central Register of Controlled Trials (Issue 3, 2017), Ovid Medline 1950 to January 18, 2017), EMBASE (January 17, 2017), ClinicalTrials.gov, the World Health Organization’s Internet clinical trial portal (March 7, 2017) and contacted authors for missing data. They included randomized trials with no language restriction in which 1) participants were randomized to a surgical procedure and either no treatment or an alternative surgical procedure; or 2) studies in which participants were randomized to non-surgical treatment for anal fissure. Non-randomized studies, studies with abstracts only from meeting presentation, and studies where fissure healing was not an endpoint of the study were excluded. For the surgical review, a total of 31 trials involving 2606 patients with fissure were included (Arroyo, 2004; Boulos, 1984; Dudhamal, 2014; Ellis, 2004; Elsebae, 2007; Filingeri, 2005; Fischer, 1976; Gupta, 2014; Gupta, 2008; Gupta, 2003; Hancke, 2003; Jensen, 1984; Kang, 2008; Kortbeek, 1992; Magdy, 2012; Marby, 1979; Mentes, 2008; Mentes, 2005; Mousavi, 2009; Olsen, 1987; Pujahari, 2010; Ram, 2007; Renzi, 2008; Saad, 1992; Tauro, 2011; Wang, 2011; Wang, 2005; Weaver, 1987; Wiley, 2004; Yucel, 2009). In the non-surgical portion of the review, 117 trials involving 9456 patients with fissure were included (Abd Elhady, 2009; Agrawal, 2013; Ahmed, 2007; Ahmed, 2012; Ala, 2012; Altomare, 2000; Antripoli, 1999; Arroyo, 2005; Arslan, 2013; Asim, 2014; Aslam, 2014; Bacher, 1997; Bailey, 2002; Bansal, 2016; Berkel, 2014; Bielicki, 2003; Boschetto, 2004; Brillantino, 2014; Brisinda, 2007; Brisinda, 2004; Brisinda, 2002; Brisinda, 1999; Bulus, 2013; Buyukyavuz, 2010; Carapeti, 1999; Carroccio, 2013; Cevik, 2012; Chaudhuri, 2001; Chen, 1992; Colak, 2003; deNardi, 2006; Dinç, 2014; di Visconte, 2009; di Visconte, 2006; El-Labban, 2010; Elwakeel, 2007; Emami, 2008; Eshghi, 2007; Evans, 2001; Ezri, 2003; Farooq, 2012; Festen, 2009; Fruehauf, 2006; Gagliardi, 2010; Gaj, 2006; Gandomkar, 2015; Giridhar, 2014; Golfam, 2019; Gough, 1983; Grekova, 2015; Gupta, 2006; Hanumanthappa, 2012; Ho, 2005; Host, 1999; Iswariah, 2005; Jawaid, 2009; Jensen, 1987; Jensen, 1986; Jonas, 2001; Jones, 2006; Katsinelos, 2006; Kennedy, 1999; Kenny, 2001; Khaledifar, 2015; Kocher, 2002; Libertiny, 2002; Lund, 1997; Maan, 2004; Maria, 1998; Maria, 2000; Mentes, 2008; Mentes, 2003; Mentes, 2001; Mishra, 2005; Moghami, 2006; Motie, 2016; Mustafa, 2006; Muthukumarassamy, 2005; Nasr, 2010; Oettle, 1997; Othman, 2010; Parellada, 2004; Peshala, 2014; Peng, 2013; Perrotti, 2002; Pitt, 2001; Prudente, 2011; Richard, 2000; Rosa, 2012; Sanei, 2009; Sahakitrungruang, 2011; Scholefield, 2003; Shrivastava, 2007; Siddique, 2008; Siproudhis, 2003; Sonmez, 2002; Suknaic, 2008; Suvarna, 2012; Tander, 1999; Tankova, 2002; Tankova, 2009; Tauro, 2011; Torrabadella, 2006; Uluutku, 2001; Vaithianathan, 2015; Valizadeh, 2012; Weinstein, 2004; Werre, 2001; Yakoot, 2009; Yetisir, 2012; Youssef, 2015; Zuberi, 2000). The reported outcome measures in the study were non-healing and incontinence.
Ansari (2020) conducted a prospective RCT to investigate the effectiveness of topical diltiazem cream over topical glyceryl trinitrate (GTN) ointment in the treatment of patients with chronic anal fissure. Patients with chronic anal fissure were included in the study and randomly divided in two groups. Chronic anal fissures in Ansari (2020) were defined as anal symptoms lasting for more than 8-12 weeks, with horizontal muscle fibers showing at the fissure base and/or the presence of a sentinel tag. Patients with anal fissures secondary to other diseases like inflammatory bowel disease, malignancy, sexually transmitted diseases, previous treatment with local ointment or surgery; patients who needed anal surgery for any concurrent disease like hemorrhoids, pregnant women and patients with significant cardiovascular conditions were excluded from the study. The first group was advised to apply a pea size (approximately 250 milligram) quantity of 2% diltiazem cream by fingertip to the anal verge twice daily for eight weeks. The second group was advised to apply 0.2% GTN ointment to the anal verge at the same regime as the first group. The maximum length of follow-up was six weeks. The reported outcome measure in the study was non-healing.
Nour (2020) described a randomized comparative clinical trial that compared the outcome of lateral internal sphincterotomy and botulinum toxin injection in patients with chronic anal fissure. Patients suffering chronic anal fissure and aged above sixteen years old were included in the study and randomized into two equally distributed groups. Patients with previous anal surgery, complicated anal fissure, unfit for surgery, specific diseases as Crohn’s disease, ulcerative colitis, and anorectal malignancy, malignancy, anal fistula or abscess, systemic disease requiring treatment with calcium channel blockers and/or nitrates, or hypersensitivity to botulinum toxins were excluded. The first group (n=48) received an 80 IU botulinum toxin injection under general anesthesia in the lithotomy position in four positions, each twenty IU in five, seven, eleven, and one O’clock positions in the internal sphincter not deeper than the midpoint of the anal canal. The second group (n=48) underwent lateral internal sphincterotomy under general anesthesia where the lower part of the internal sphincter was cut by electrocautery after opening the skin of the intersphincteric groove, on the left lateral site and not extending beyond the proximal end of the fissure. The chronic fissure complex was also removed. The wound was left open at the end of the procedure after sufficient hemostasis. The maximum length of follow-up was twelve months. The reported outcome measures in the study were non-healing, incontinence, and pain.
The prospective randomized controlled trial of Ahmed (2018) compared the complication of open lateral internal sphincterotomy with closed lateral internal sphincterotomy in patients with chronic anal fissure. Patients with chronic anal fissure and aged between twenty and 70 years old were included and randomly divided into two equally distributed groups. Patients with inflammatory bowel disease, known venereal disease, immunodeficiency, perianal abscesses, anal or rectal surgery within twelve weeks or signs of other rectal diseases, fistula, infection, or tumors were excluded. The first group (n=50) was treated with open lateral internal sphincterotomy. For the open lateral internal sphincterotomy, an endoscope was used for anal canal visualization. The second group (n=50) was treated with closed lateral internal sphincterotomy. In the control group, a cut entry point was made with a Von Graffe’s sharp edge, either into the intersphincteric groove or into the submucosa. The front line of the cutting edge was pivoted toward the interior sphincter and a halfway sphincterotomy was finished. The skin wound entry point was left open. Both procedures were done either under general or local anesthesia. The maximum length of follow-up was 24 hours. The reported outcome measures in the study were: incontinence and pain.
The prospective randomized controlled trial of Ruiz-Tovar (2017) compared the compliance rate among patients receiving glyceryl trinitrate treatment for chronic anal fissure with that among patients receiving percutaneous posterior tibial nerve stimulation. Patients with persistent anal fissure despite hygiene and dietary measures applied over at least a six-week period were included and randomly divided into two equally distributed groups. The first group (n=40) received 0.4% glyceryl trinitrate ointment. The dosage for all the patients was 375.0 milligram of ointment (containing 1.5 milligram of glyceryl trinitrate, applied with a gloved finger to the distal anal canal, every twelve hours for eight weeks. The second group (n=40) underwent one 30-minute session of percutaneous posterior tibial nerve stimulation, two days per week for eight consecutive weeks. Posterior tibial nerve stimulation was delivered using a needle electrode that was inserted three to four centimeters cephalad and two-centimeter posterior to the medial malleolus at a 60-degree angle toward the ankle joint to a depth of approximately 0.5 to 1.0 centimeter. Successful placement was confirmed by the presence of an electric sensation five cm above and below the insertion site or a digital plantar flexion. PPTNS was delivered at the highest amplification (0–20 mA) at a frequency of 20 Hz, causing neither a motor response nor pain. The maximum length of follow-up was 24 weeks. The reported outcome measures in the study were: non-healing and pain.
Results
Non-healing of the fissure (critical)
Thirteen studies compared GTN with CCB in patients with chronic anal fissures (Ala, 2012; Ansari, 2020; Bansal, 2016; Bielecki, 2003; Cevik, 2012; Ezri, 2003; Jawaid, 2009; Khaledifar, 2015; Kocher, 2002; Mustafa, 2006; Sanei, 2009; Shrivastava, 2007; Uluutku, 2001). The results of individual studies that reported on the incidence of non-healing of the fissure were retrieved and pooled in a meta-analysis. One study could not be pooled due to statistical heterogeneity in the outcome measure non-healing of the fissure. The results of these three studies were described separately. The pooled incidence of non-healing of the fissure in the GTN group was 127/395 (32.2%), compared to 128/409 (31.3%) in the CCB group. Pooled RR 1.00 (95% CI 0.73 to 1.36), not favoring one of the groups. This is not considered as a clinically (for the patient) important difference.
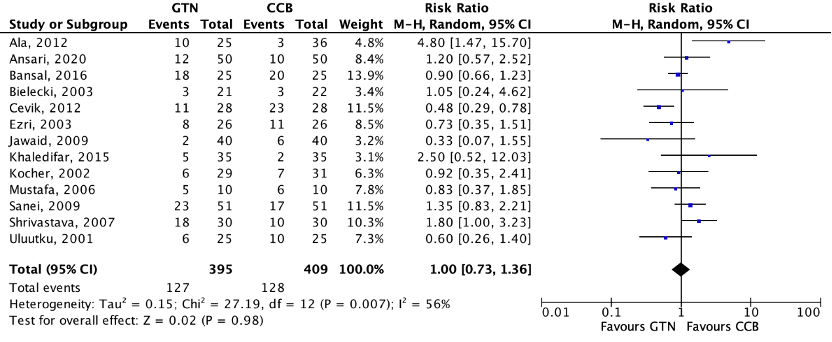
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval
One study reported the mean time to healing of chronic anal fissures between GTN and CCB (Abd Elhady, 2009). The mean (SD) time to healing in the GTN group was 5.0 (1.1) weeks, compared to 5.1 (1.13) weeks in the CCB group, favoring the GTN group. This is not considered as a clinically (for the patient) important difference.
Incontinence (critical)
Two studies compared GTN with CCB in patients with chronic anal fissures (Jawaid, 2009; Mustafa, 2006). Jawaid (2009) defined incontinence as flatus incontinence. Mustafa (2006) did not define incontinence. The incidence of incontinence in the study of Jawaid (2009) in the GTN group was 1/40 (2.5%), compared to 0/40 (0%) in the CCB group. The incidence of incontinence in the study of Mustafa (2006) in the GTN group was 0/10 (0%), compared to 0/10 (0%) in the CCB group. RD 0.02 (95% CI -0.04 to 0.08), favoring the CCB group. This is not considered as a clinically (for the patient) important difference.
Pain (important)
None of the included studies reported the outcome measure pain for the comparison of GTN versus CCB.
Level of evidence
Non-healing of the fissure (critical)
- Glyceryl trinitrate versus calcium channel blockers - The level of evidence regarding the outcome measure non-healing of the fissure comes from randomized controlled trials and therefore starts high. The level of evidence was downgraded by three levels because of risk of bias, the small numbers of included patients, wide confidence intervals crossing both boundaries of clinical relevance (imprecision), and conflicting results (inconsistency). The level of evidence is very low.
Incontinence (critical)
- Glyceryl trinitrate versus calcium channel blockers - The level of evidence regarding the outcome measure incontinence comes from randomized controlled trials and therefore starts high. The level of evidence was downgraded by three levels because of risk of bias, conflicting results (inconsistency), and the small number of included patients (imprecision). The level of evidence is very low.
Pain (important)
Because of a lack of data, it was not possible to grade the literature for the outcome measure pain for the comparison of GTN versus CCB.
Zoeken en selecteren
A systematic review of the literature was performed to answer the following questions:
- What is the best treatment for chronic anal fissures?
- What are the (un)beneficial effects of conservative medical treatment in comparison with other conservative medical treatment in patients with chronic anal fissures?
- What are the (un)beneficial effects of conservative medical treatment in comparison with surgical treatment in patients with chronic anal fissures?
- What are the (un)beneficial effects of surgical treatment in comparison with other surgical treatment in patients with chronic anal fissures?
Relevant outcome measures
The guideline development group considered non-healing of the fissure and incontinence as critical outcome measures for decision making; and pain as an important outcome measure for decision making.
For all outcome measures, the workgroup considered a 25% difference in relative risk (RR) for dichotomous outcomes, and 10% difference for continuous outcomes as a clinically relevant difference.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 24 February 2021. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 142 hits. Studies were selected based on the following criteria: systematic reviews and randomized controlled trials. Twenty-six studies regarding chronic anal fissures were initially selected based on title and abstract screening. After reading the full text, eighteen studies regarding chronic anal fissures were excluded (see the table with reasons for exclusion under the tab Methods). Finally, eight studies regarding chronic anal fissures were included.
Secondly, an update of the literature was performed. The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from the 24th of February 2021 until the 17th of April 2023. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 76 extra hits. Eight studies regarding chronic anal fissures were initially selected based on title and abstract screening. After reading the full text, three studies for chronic anal fissures were excluded (see the table with reasons for exclusion under the tab Methods). Five extra studies were included and added to the literature analysis of chronic anal fissures.
Results
Thirteen studies were included in the analysis of the literature for chronic anal fissures. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
Referenties
- Boland PA, Kelly ME, Donlon NE, Bolger JC, Larkin JO, Mehigan BJ, McCormick PH. Management options for chronic anal fissure: a systematic review of randomised controlled trials. Int J Colorectal Dis. 2020 Oct;35(10):1807-1815. doi: 10.1007/s00384-020-03699-4. Epub 2020 Jul 25. PMID: 32712929.
- Sahebally, S. M., Meshkat, B., Walsh, S. R., & Beddy, D. (2018). Botulinum toxin injection vs topical nitrates for chronic anal fissure: an updated systematic review and meta‐analysis of randomized controlled trials. Colorectal Disease, 20(1), 6-15.
- Sahebally SM, Walsh SR, Mahmood W, Aherne TM, Joyce MR. Anal advancement flap versus lateral internal sphincterotomy for chronic anal fissure- a systematic review and meta-analysis. Int J Surg. 2018 Jan;49:16-21. doi: 10.1016/j.ijsu.2017.12.002. Epub 2017 Dec 9. PMID: 29233787.
- Nelson RL, Manuel D, Gumienny C, Spencer B, Patel K, Schmitt K, Castillo D, Bravo A, Yeboah-Sampong A. A systematic review and meta-analysis of the treatment of anal fissure. Tech Coloproctol. 2017 Aug;21(8):605-625. doi: 10.1007/s10151-017-1664-2. Epub 2017 Aug 9. PMID: 28795245.
- ANSARI, N. A., BHORE, A., & MUSA, O. (2020). A Comparative Study of Topical Diltiazem (2%) with Topical Glyceryl Trinitrate (0.2%) as a Conservative Treatment for Anal Fissure. Journal of Clinical & Diagnostic Research, 14(7).
- Ahmed, F., Mengal, M. A., Ahmed, M., Akbar, S., Elahi, B., & Khan, A. (2018). Comparison of Complications of Open versus Closed Lateral Internal Sphincterotomy in Chronic Anal Fissures. PAKISTAN JOURNAL OF MEDICAL & HEALTH SCIENCES, 12(3), 1072-1074.
- Ruiz-Tovar J, Llavero C. Percutaneous Posterior Tibial Nerve Stimulation vs Perianal Application of Glyceryl Trinitrate Ointment in the Treatment of Chronic Anal Fissure: A Randomized Clinical Trial. Dis Colon Rectum. 2017 Jan;60(1):81-86. doi: 10.1097/DCR.0000000000000736. PMID: 27926561.
- Akinci, O., Abdulrahman, S. M. F., Güngör, Ö., Yüceyar, N. S., Perek, A., & Ertürk, M. S. (2020). Randomised Comparison of the Effect of 0.2% Glyceryl Trinitrate and 0.5% Topical Nifedipine in Acute Anal Fissure Treatment/Akut Anal Fissur Tedavisinde% 0, 2 Gliseril Trinitrat ile% 0, 5 Topikal Nifedipinin Etkilerinin Randomize Karsilastirilmasi. Turkish Journal of Colorectal Disease, 30(4), 246-253.
- Farooq, U., Farooq, S., Zahir, S., & Chaudhry, A. M. (2012). Comparison of surgical and chemical sphincterotomy in the management of acute anal fissures. Pak J Med Health Sci, 6, 24-31.
Evidence tabellen
Evidence table
Systematic reviews
| Study reference | Study characteristics | Patient characteristics | Intervention & control | Outcome measures and effect size | Comments |
| Nelson (2017) |
Inclusion criteria SR surgical part: Exclusion criteria SR surgical part: Inclusion criteria SR conservative part: Exclusion criteria SR conservative part: 31 studies included in the surgical part of the review and 117 studies included in the non-surgical part of the review. Important patient characteristics at baseline: Literature search up to March 7, 2017. Surgical intervention studies: Conservative intervention studies: Study design: Setting and Country: Source of funding and conflicts of interest: |
Describe interventions: Surgical comparisons Manual anal stretch vs LIS: Anal stretch versus LIS sensitivity analysis: Open LIS vs Closed LIS: LIS to the apex of the fissure vs Lis to dentate line; subgroup anal: Fissurectomy vs LIS: LIS versus V-Y flap cover: Lis posterior versus LIS lateral: Levatorplasty versus LIS: LIS closed wound versus LIS open wound: Pneumatic balloon dilation to 3 cm versus LIS: Speculum dilation 4.8 cm vs LIS: Dilation + fissurectomy vs LIS: LIS + polyp removal vs LIS alone: Unilateral LIS vs Bilateral LIS: Sphincterolysis vs Closed LIS: V-Y flap vs Fissurectomy: Ayurvedic suture of the fissure vs Dilation + anal stretch: Conservative comparisons GTN vs control: GTN vs Lidocaine: GTN high dose vs GTN low dose: GTN vs pt. self-dilation: GTN vs botox: GTN vs CCB: Botox vs control: CCB topical vs control: LIS vs any medical therapy: Lis vs any medical therapy follow-up >6 months: Solcodem vs control: Minoxadil vs lidocaine: Sildenafil vs control: Arginine vs LIS: Clove oil vs lidocaine: Lanolin vs control: Lanolin vs collagen spray: Healer cream vs GTN: Healer cream vs control Metronidazole vs control: Ayurvedic concoction vs Ayurvedic + CCB: Indoramin vs control: GTN vs ISMN: GTN topical vs GTN intra-anal: Botox anterior vs botox posterior: Botox posterior vs botox bilateral: GTN 40 days vs GTN 80 days: Diet vs control: Lidocaine vs hydrocortisone: PTNS vs LIS: Psyllium husk gum vs control: Sitz baths vs control: Botox low dose vs botox high dose: Botox vs botox + GTN: GTN ointment vs GTN dermal patch: Lidocaine vs lidocaine. + dilator: Botox vs Boxox disport: Lidocaine vs control children: CCB vs botox: PTNS vs GTN CCB topical vs CCB oral: Bran vs Lactulose: Describe interventions: Surgical comparisons Manual anal stretch vs LIS: Anal stretch versus LIS sensitivity analysis: Open LIS vs Closed LIS: LIS to the apex of the fissure vs Lis to dentate line; subgroup anal: Fissurectomy vs LIS: LIS versus V-Y flap cover: Lis posterior versus LIS lateral: Levatorplasty versus LIS: LIS closed wound versus LIS open wound: Pneumatic balloon dilation to 3 cm versus LIS: Speculum dilation 4.8 cm vs LIS: Dilation + fissurectomy vs LIS: LIS + polyp removal vs LIS alone: Unilateral LIS vs Bilateral LIS: Sphincterolysis vs Closed LIS: V-Y flap vs Fissurectomy: Ayurvedic suture of the fissure vs Dilation + anal stretch: Conservative comparisons GTN vs control: GTN vs Lidocaine: GTN high dose vs GTN low dose: GTN vs pt. self-dilation: GTN vs botox: GTN vs CCB: Botox vs control: CCB topical vs control: LIS vs any medical therapy: Lis vs any medical therapy follow-up >6 months: Solcodem vs control: Minoxadil vs lidocaine: Sildenafil vs control: Arginine vs LIS: Clove oil vs lidocaine: Lanolin vs control: Lanolin vs collagen spray: Healer cream vs GTN: Healer cream vs control Metronidazole vs control: Ayurvedic concoction vs Ayurvedic + CCB: Indoramin vs control: GTN vs ISMN: GTN topical vs GTN intra-anal: Botox anterior vs botox posterior: Botox posterior vs botox bilateral: GTN 40 days vs GTN 80 days: Diet vs control: Lidocaine vs hydrocortisone: PTNS vs LIS: Psyllium husk gum vs control: Sitz baths vs control: Botox low dose vs botox high dose: Botox vs botox + GTN: GTN ointment vs GTN dermal patch: Lidocaine vs lidocaine. + dilator: Botox vs Boxox disport: Lidocaine vs control children: CCB vs botox: PTNS vs GTN CCB topical vs CCB oral: Bran vs Lactulose: |
Surgical interventions
Non-healing of the fissure/recurrence
Open LIS vs Closed LIS: A; B; F; J; N; CC OR 1.00 (95% CI 0.4 to 2.48)
LIS to the apex of the fissure vs Lis to dentate line; subgroup anal: Q; R OR 7.1 (95% CI 1.2 to 50)
Fissurectomy vs LIS: S; Z OR 8.07 (95% CI 1.42 to 45.8)
LIS versus V-Y flap cover: S; Z OR 0.17 (95% CI 0.07 to 0.41)
Lis posterior versus LIS lateral: X; Y OR 0.3 (95% CI 0.01 to 7.87
Levatorplasty versus LIS: D OR 0.2 (95% CI 0.01 to 7.11
LIS closed wound versus LIS open wound: M OR 0.65 (95% CI 0.10 to 4.10)
Pneumatic balloon dilation to 3 cm versus LIS: W OR 1.47 (95% CI 0.29 to 7.37)
LIS + polyp removal vs LIS alone: H OR 1
Unilateral LIS vs Bilateral LIS: U OR 6.91 (95% CI 1.97 to 24.2)
Sphincterolysis vs Closed LIS: I OR 0.58 (95% CI 0.13 to 2.63)
V-Y flap vs Fissurectomy: AA OR 0.17 (95% CI 0.04 to 0.81
LIS vs V-Y anoplasty: O RR 0.44 (95% CI 0.20 to 0.97
Incontinence
Open LIS vs Closed LIS: A (Arroyo, 2004) Open LIS 2 months: 3/40 (7.5%) Open LIS 6 months: 2/40 (5%) Open LIS 1-2 years: 2/40 (5%) Closed LIS 2 months: 2/40 (5%) Closed LIS 6 months: 1/40 (2.5%) Closed LIS 1-2 years: 1/40 (5%)
B (Boulos, 1984) Open LIS incontinence of faeces: 0/14 (0%) Open LIS incontinence of flatus: 2/14 (14.3%) Closed LIS incontinence of faeces: 0/14 (0%) Closed LIS incontinence of flatus: 3/14 (21.4%)
F (Filingeri, 2005) Open LIS: 0/20 (0%) Close LIS: 0/20 (0%)
J (Gupta, 2014) Open LIS: 0/68 (0%) Closed LIS: 0/68 (0%)
N (Kortbeek, 1992) Incontinence not reported.
CC (Wiley, 2004) Open LIS 1 year: 2/41 (4.9%) Closed LIS 1 year: 1/38 (2.6%)
LIS to the apex of the fissure vs Lis to dentate line; subgroup anal: Q (Mentes, 2005) LIS apex mean (SD) postop anal incontinence score: 0.42 (0.76) LIS dentate line mean (SD) postop anal incontinence score: 0.58 (1.13)
R (Mentes, 2008) LIS apex mean (SD) postop anal incontinence score: 7 days: 0.71 (0.73) 28 days: 0.74 (0.68) 2 months: 0.39 (0.76) 6 months 0.35 (0.75)
Fissurectomy vs LIS: S (Mousavi, 2009) Fissurectomy incontinence to flatus or fecal soiling: 2/30 (6.7%) LIS incontinence to flatus or fecal soiling: 0/32 (0%)
Z (Wang, 2005) Studie alleen beschikbaar in chinees.
LIS versus V-Y flap cover: Geen studies
Lis posterior versus LIS lateral: X (Saad, 1992) Full tekst niet beschikbaar.
Y (Tauro, 2011) LIS posterior flatus incontinence and anal seepage: 4/30 LIS posterior fecal incontinence: 0/30 LIS lateral flatus incontinence and anal seepage: 1/30 LIS lateral fecal incontinence: 0/30)
Levatorplasty versus LIS: D (Ellis, 2004) Incontinence not reported.
LIS closed wound versus LIS open wound: M (Kang, 2008) LIS closed wound first week: 1/45 LIS closed wound fourth week: 1/45 LIS closed wound ninth week: 0/45 LIS open wound first week: 4/45 LIS open wound fourth week: 1/45 LIS open wound ninth week: 0/45
Pneumatic balloon dilation to 3 cm versus LIS: W (Renzi, 2008) Pneumatic balloon dilation 24 months: 0/24 (0%) LIS 24 months: 4/25 (16%)
Speculum dilation 4.8 cm vs LIS: DD (Yucel, 2009) Speculum dilation anal incontinence: 0/20 (0%) LIS anal incontinence: 0/20 (0%)
Dilation + fissurectomy vs LIS: K (Hancke, 2009) Dilation fecal incontinence: 3/27 (11%) LIS fecal incontinence: 6/30 (20%)
LIS + polyp removal vs LIS alone: H (Gupta, 2003) Incontinence not reported.
Unilateral LIS vs Bilateral LIS: U Pujahari, 2010) ULIS incontinence for flatus: 4/104 (3.8%) ULIS incontinence to liquid stools: 0/104 (0%) BLIS incontinence for flatus: 2/107 (1.9%) BLIS incontinence for liquid stools: 0/107 (0%)
Sphincterolysis vs Closed LIS: I (Gupta, 2008) Sphincterolysis detoration in continence 4 weeks: 2/42 (4.8%) Sphincterolysis detoration in continence 54 weeks: 0/42 (0%) Closed LIS detoration in continence 4 weeks: 3/43 (7.0%) Closed LIS detoration in continence 54 weeks: 1/43 (2.3%)
V-Y flap vs Fissurectomy: AA (wang, 2011) Artikel in chinees
Ayurvedic suture of the fissure vs Dilation + anal stretch: C (Dudhamal, 2014) Incontinence not reported.
LIS vs V-Y anoplasty: O RR 15.00 (95% CI 0.88 to 255.78
Outcome measures (non-surgical interventions)
Non-healing of the fissure/recurrence
GTN vs control: JJ; QQ; CCC; FFF; PPP; NNNN; OOOO; SSSS; TTTT; HHHHH; LLLLL; RRRRR; SSSSS; WWWWW; ZZZZZ; AAAAAA; BBBBBB; HHHHHH; IIIIII OR 0.69 (95% CI 0.63 to 0.77)
GTN vs Lidocaine: GG; PP; EEE; WWWWW; ZZZZZ OR 0.19 (95% CI 0.11 to 0.33)
GTN high dose vs GTN low dose: QQ; CCC; RRRRR; UUUUU OR 0.91 (95% CI 0.57 to 1.45)
GTN vs pt. self-dilation: UU (Boschetto, 2014) GTN non healing: 11/18 61.1%) Pt. self-dilation: 1/185.5%)
LLL (Di Visconte, 2006) GTN non healing: 5/16 Pt. Self-dilation non-healing: 4/16
XXX (Gaj, 2006)
OR 4.18 (95% CI 2.10 to 8.33)
GTN vs botox: EE; SS; WW; ZZ; JJJ; UUU; VVV; EEEEEE OR 1.78 (95% CI 0.83 to 1.96)
GTN vs CCB:
Botox vs control: OR 0.29 (95% CI 0.02 to 3.61
CCB topical vs control: FF; KK; EEE; AAAA; DDDD; IIIII; SSSSS OR 0.27 (95% CI 0.18 to 0.39)
LIS vs any medical therapy: EE; HH LL; OO; KKK; NNN; RRR; TTT; YYY; ZZZ; EEEE; FFFF; MMMM; RRRR; XXXX; YYYY; AAAAA; DDDDD; EEEEE; GGGGG; MMMMM; NNNNN; PPPPP; TTTTT; XXXXX; YYYYY; CCCCCC; FFFFFF; GGGGGG; KKKKKK; LLLLLL OR 0.22 (95% CI 0.16 to 0.28)
Lis vs any medical therapy follow-up >6 months: EE; LL; MM; YYY; FFFF; RRRR; AAAAA; GGGGG; XXXXX; CCCCCC; GGGGGG; KKKKKK; LLLLLL OR 0.12 (95% CI 0.07 to 0.21)
Solcodem vs control: GGG OR 0.26 (95% CI 0.1 to 0.67)
Minoxadil vs lidocaine: CCCCC OR 1.0 (95% CI 0.35 to 1.32)
Sildenafil vs control: ZZZZ OR 0 (95% CI 0.0 to 0.05)
Arginine vs LIS: QQQ OR 3.6 (95% CI 1.2 to 10.64)
Clove oil vs lidocaine: OOO OR 0.09 (95% CI 0.02 to 0.37)
Lanolin vs control: BBB OR 0.22 (95% CI 0.05 to 0.95)
Lanolin vs collagen spray: BBB OR 0.08 (95% CI 0 to 1.31)
Healer cream vs GTN: JJJJJJ OR 0.05 (95% CI 0.01 to 0.27)
Healer cream vs control JJJJJJ OR 0.17 (95% CI 0.03 to 0.92)
Metronidazole vs control: BBBB OR 0.15 (95% CI 0.02 to 1.12)
Ayurvedic concoction vs Ayurvedic + CCB: Indoramin vs control: JJJJJ OR 0.78 (95% CI 0.39 to 1.54)
GTN vs ISMN: KKKKK OR 1.25 (95% CI 0.54 to 4.64)
GTN topical vs GTN intra-anal: DDDDDD OR 3.33 (95% CI 0.46 to 24.5)
Botox anterior vs botox posterior: VVVV OR 0.20 (95% CI 0.05 to 0.96)
Botox posterior vs botox bilateral: FFFFF OR 1.00 (95% CI 0.39 to 2.56)
GTN 40 days vs GTN 80 days: WWW OR 1.13 (95% CI 0.63 to 2.0)
PTNS vs LIS: LLLLLL OR 20.6 (95% CI 2.91 to 495)
Botox low dose vs botox high dose: XX; LLLL OR 1.93 (95% CI 0.75 to 4.93)
Botox vs botox + GTN: NN; KKKK OR 1.38 (95% CI 0.75 to 4.93)
GTN ointment vs GTN dermal patch: III; MMMMMM OR 1.07 (95% CI 0.50 to 2.27)
Botox vs Boxox disport: YY OR 2.80 (95% CI 1.17 to 6.72)
CCB vs botox: PPPPP; EEEEE OR 1.39 (95% CI 0.82 to 2.35)
PTNS vs GTN OR 3.14 (95% CI 1.12 to 8.82)
CCB topical vs CCB oral: FF; JJJJ OR 0.76 (95% CI 0.33 to 1.76)
Incontinence
GTN vs control: PPP (Emami, 2008): GTN incontinence: 0/21 (0%) Placebo incontinence: 0/21 (0%)
AAAAAA (Tankova, 2002): GTN: 0/10 (0%) Placebo: 0/9 (0%)
BBBBBB (Tankova, 2009) GTN: 0/21 (0%) Placebo: 0/10 (0%)
GTN vs Lidocaine: None of the studies reported incontinence.
GTN high dose vs GTN low dose: None of the studies reported incontinence.
GTN vs pt. self-dilation: UU (Boschetto, 2004) GTN: 0/18 (0%) Pt. self-dilation: 0/18 (0%)
LLL (Di Visconte, 2006) GTN fecal incontinence: 0/16 Pt. self-dilation: 0/16
MMM (Di Visconte, 2009) GTN fecal soiling: 0/30 (0%) GTN fecal incontinence: 0/30 (0%) Pt. self-dilation fecal soiling: 0/30 (0%) Pt. self-dilation fecal incontinence: 0/30 (0%)
GTN vs botox: SS (Berkel, 2014) GTN incontinence: 4/33 (12.1%) Botox: 5/27 (18.5%)
WW (Brisinda, 1999) GTN: 0/25 (0%) Botox: 0/25 (0%)
ZZ (Brisinda, 2007) GTN feal incontinence: 0/50 (0%) Botox fecal incontinence: 3/50 (6%) > disappeared spontaneously after 3 weeks.
JJJ (DeNardi, 2006) GTN: 0/15 (0%) Botox: 0/15 (0%)
VVV (Fruehauf, 2006) Botox: 0/25 (0%)
GTN vs CCB: GGGG (Jawaid, 2009) GTN flatus incontinence: 1/40 (2.5%) CCB flatus incontinence: 0/40 (0%)
BBBBB (Mustafa, 2006) GTN: 0/10 (0%) CCB: 0/10 (0%)
Botox vs control: None of the studies reported incontinence.
CCB topical vs control: None of the studies reported incontinence.
Surgical vs non-surgical LIS vs any medical therapy: LL (Arroyo, 2005) LIS 2 month incontinence: 3/40 (7.5%) LIS 6 month incontinence: 2/40 (5%) LIS 1-2-3 years incontinence: 2/40 (5%) Botox 2 month incontinence: 2/40 (5%) Botox 6 month incontinence: 0/40 (0%) Botox 1-2-3- years incontinence: 0/40 (0%)
OO (Aslam, 2014) LIS: 2/30 (6.7%) GTN: 0/30 (0%)
KKK (Dinç, 2014) Botox: 0/30 (0%)
NNN (El-Labban, 2010) LIS: incontinence to flatus: 3/40 (7.5%) LIS: mild soiling: 2/40 (5%) GTN: 0/40 (0%)
RRR (Evans. 2001) LIS: minor incontinence for flatus: 2/31 (6.5%) GTN: 0/34 (0%)
TTT (Farooq, 2012) LIS: mild incontinence flatus: 5/50 (10%) Chemical sphincterotomy: 0/50 (0%)
YYY (Gandomkar, 2015) Partial LIS: incontinence: 8/50 (16%) Botox: 2/49 (4.1%)
FFFF (Iswariah, 2005) LIS: mean incontinence score 26 weeks (range) 0 (0) Botox: mean incontinence score 26 weeks (range): 0.18 (0-2)
MMMM (Katsinelos, 2005) LIS: 4/32 (12.5%) CCB: 0/32 (0%)
YYYY (Mishra, 2005) GTN: 0/20 (0%) LIS: flatus incontinence: 3/20 (15%)
DDDDD (Nasr, 2010) LIS: 6/40 (15%) Botox: 0/40 (0%)
GGGGG (Parellada, 2004) LIS: fecal incontinence: 0/12 (0%) GTN: fecal incontinence: 0/12 (0%)
NNNNN (De Rosa, 2013) LIS: flatus incontinence: 2/68 (3%) LIS: fecal incontinence: 0/68 (0%) CCB: flatus incontinence: 0/74 (0%) CCB: fecal incontinence: 0/74 (0%)
PPPPP (Samim, 2012) CCB: incontinence 4 weeks: 8/74 (10.8%) CCB: incontinence 8 weeks: 6/74 (8.1%) CCB: incontinence 12 weeks: 6/74 (8.1%) Botox: incontinence 4 weeks 7/60 (11.7%) Botox incontinence 8 weeks: 3/60 (5%) Botox: incontinence 12 weeks: 3/60 (5%)
TTTTT (Siddique, 1970) GTN: incontinence to flatus: 0/31 (0%)
YYYYY (Suvarna, 2012) LIS: flatus incontinence: 9/97 (9.3%) LIS: fecal incontinence: 5/97 (5.2%) CCB: flatus incontinence: 0/91 (0%) CCB: fecal incontinence: 0/91 (0%)
CCCCCC (Tauro, 2011) LIS: flatus incontinence: 1/30 LIS: anal seepage: 2/30 LIS: fecal incontinence: 0/30 (0%) GTN: faltus, fecal incontinence and anal seepage: 0/30 (0%)
FFFFFF (Vaithianathan, 2015) LIS: fecal or flatus incontinence: both 0/45 (0%) CCB: fecal of flatus incontinence: both 0/45 (0%)
GGGGGG (Valizadeh, 2012) LIS: incontinence 2 months: 12/25 (48%) LIS: incontinence 3 months: 5/25 (20%) LIS: incontinence 6 months: 4/25 (16%) LIS: incontinence 12 months: 1/25 (4%) Botox: incontinence 2 months: 3/25 (12%) Botox: incontinence 3 months: 0/25 (0%) Botox incontinence 6 months: 0/25 (0%) Botox: incontinence 12 months: 0/25 (0%)
LLLLLL (Youssef, 2015) LIS: anal incontinence 1 month: 3/37 (8.1%) LIS: anal incontinence 1 year: 1/37 (2.7%) TENS: anal incontinence 1 month: 0/36 (0%) TENS: anal incontinence 1 year: 0/36 (0%)
Solcodem vs control: Incontinence not reported.
Minoxadil vs lidocaine: Incontinence not reported.
Sildenafil vs control: Incontinence not reported.
Arginine vs LIS: Incontinence not reported.
Clove oil vs lidocaine: Incontinence not reported.
Lanolin vs control: Incontinence not reported.
Lanolin vs collagen spray: Incontinence not reported.
Healer cream vs GTN: Incontinence not reported.
Healer cream vs control Incontinence not reported.
Metronidazole vs control: Incontinence not reported.
Ayurvedic concoction vs Ayurvedic + CCB: Incontinence not reported.
Indoramin vs control: Incontinence not reported.
GTN vs placebo: GTN: fecal incontinence: 0/10 (0%) Placebo: 0/9 (0%)
GTN topical vs GTN intra-anal: Incontinence not reported.
Botox anterior vs botox posterior: Incontinence not reported.
Botox posterior vs botox bilateral: Incontinence not reported.
GTN 40 days vs GTN 80 days: Incontinence not reported.
Lidocaine vs hydrocortisone: Incontinence not reported.
PTNS vs LIS: Incontinence not reported.
Botox low dose vs botox high dose: Incontinence not reported. |
Facultative:
LIS is the most effective treatment for anal fissure, curing all but 6% of patients. Late recurrences are very rare after LIS versus with medical therapy [179]. Minor incontinence is more likely with LIS than medical therapy (Fig. 4). The difference between LIS and medical therapy is significant, but the absolute risk alteration is small, increasing from 3 cases per 1000 patients with medical therapy to 14 cases per 1000 with LIS (95% CI 6–31). Open and closed (a euphe- mism meaning less open) LIS are equally effective. Manual anal dilation is inferior to LIS, but recent small studies suggest that more controlled dilation, either pneumatic, by speculum or by patients at home are just as effective as LIS and are not associated with any risk of incontinence. GTN, Botox and CCBs have been extensively investigated as treatments for acute and chronic anal fissure. They appear to be effective, but most studies have been marred by inade- quate follow-up, thus missing late recurrences, which are common. Of the three, CCBs may be the most effective. More research is needed for all three with adequate follow- up. There is virtually no research on sequencing these drugs, i.e., if one fails, what is best to try next? Many other medi- cations have been tried because of the less-than-perfect track record of the three above, but none have proven better, and in any case, the studies are too small and too few. Clove oil and sildenafil may be worth further investigation. Many unpub- lished studies can be found in this field, especially in ICTRP, but no results are available. |
|
| Sahebally (2018a) |
SR and meta-analysis of RCTs. Literature search up to March 2017. Study design: Setting and Country: Source of funding and conflicts of interest: A. Brisinda, 1999 |
Inclusion criteria SR Exclusion criteria SR Six studies included in the review. Important patient characteristics at baseline: Sample size, N: Age, mean (SD or median (range): |
Describe intervention & intervention: A. 0.2% GTN ointment 6 weeks (N=25) vs 10 U botulinum toxin to each side of the anterior midline (20 U in total) |
Non-healing of the fissure at 8 weeks, n/N (%) Sphincterotomy, n/N (%): Botulinum toxin, n/N (%): Nitrates, n/N (%): Minoxidil, n/N (%): Diltiazem (CCB), n/N (%): Overall incontinence, n/N (%): Botulinum toxin, n/N (%): Nitrates, n/N (%): Minoxidil, n/N (%): Diltiazem (CCB), n/N (%): Permanent incontinence, n/N (%) Sphincterotomy, n/N (%): Botulinum toxin, n/N (%): Nitrates, n/N (%): Minoxidil, n/N (%): Diltiazem (CCB), n/N (%): Non-healing of the fissure, n/N (%) A. BT: 1/25 vs GTN: 10/25 Pooled effect RR (95% CI) random effects: Incontinence, n/N (%) Pooled effect RR (95% CI) random effects: |
Author’s conclusion: From a patient’s perspective, CAF is often an extremely debilitating and distressing condition, and it also represents a significant proportion of the coloproctology clinic workload. Though a benign problem, it can be considerably frustrating for patients, particularly given its recurrent nature. This review highlights the limited number of high-quality RCTs examining treatment modalities for CAF, specifically sphincter sparing procedures. It also highlights a lack of quality of life assessment. This study observed that lateral internal sphincterotomy has excellent healing rates at 8 weeks although topical nitrates and BT administration have reasonable results. Although the risk of permanent incontinence with LIS is low, its consideration should be tailored to the individual patient. This data demonstrates that the key in managing this benign, non-life-threatening condition with a range of acceptable treatments and variable complication profiles is open, high quality, documented patient counselling and consent. This tailored approach to the management of CAF is reflected in the proposed treatment algorithm |
Randomized controlled trials
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3 |
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Hassan (2022) |
Type of study: RCT.
Setting and country: Al-Kindy Teaching Hospital
Funding and conflicts of interest: None declared. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: N=100 GTN: N=52 LIS: N=60
Important prognostic factors2: age ± range: 32.3 years (18-65)
Sex: 60 males, 52 females.
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test: GTN |
Describe control (treatment/procedure/test: Diltiazem |
Length of follow-up: 8 weeks.
Loss-to-follow-up: None. |
Non-healing of the fissure, n/N (%) I: 17/52 (32.7%) C: 10/60 (16.7%)
|
Author’s conclusion Both (0.2%) GTN ointment and (2%) DTZ gel are quietly effective in treating acute fissure in anus. However, topical DTZ gel is superior to topical GTN ointment, better tolerated with few side effects and recurrence rate. |
|
Herreros (2021) |
Type of study: RCT.
Setting and country: a tertiary care center, Spain.
Funding and conflicts of interest: None declared. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 25 Control: N = 30
Important prognostic factors2: age ± SD: I: 51.17 (13.6) C: 48.86 (11.7)
Sex: I: 62.9 % M C: 54.3% M
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test: Diltiazem after botox injection.
|
Describe control (treatment/procedure/test: Placebo after botox injection. |
Length of follow-up: 12 weeks.
Loss-to-follow-up: None. |
Non-healing I: 12/25 (48%) C: 19/30 (63.3%)
|
Author’s conclusion: Our results suggest that combined therapy with BT injection and topical diltiazem is not superior to BT injection alone in the treatment of CAF. Both options offer suboptimal healing rates. Clearly, late recurrences are high (more than 80% at 10 years) and may appear at any time after healing. Further randomized controlled trials, including more patients with long-term follow-up, are needed to confirm our results and to identify subgroups of patients with CAF who could potentially benefit from nonsurgical treatments.
|
|
Khan (2021) |
Type of study: RCT.
Setting and country: General surgery department, Peshawar.
Funding and conflicts of interest: None declared. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 30 Control: N = 30
Important prognostic factors2: age ± SD: I: 30 (2.77) C:29 (2.53)
Sex: I: 43% M C: 40% M
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test: LIS
|
Describe control (treatment/procedure/test: Topical Nitroglycerin. |
Length of follow-up: Six weeks.
Loss-to-follow-up: None. |
Fissure healing I: 27/30 (90%) C: 20/30 (66.7%) |
Author’s conclusion: Lateral internal sphincterotomy is comparatively of increased effectiveness than topical Glyceryl trinitrate in treating chronic anal fissure.
|
|
Malik (2021) |
Type of study: RCT.
Setting and country: Hospital, Rawalpindi Pakistan.
Funding and conflicts of interest: No information. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 50 Control: N = 50
Important prognostic factors2: age ± SD: I: 31.48 (8.88) C: 30.26 (8.76)
Sex: I: 34/50 (68%) M C: 30/50 (60(%) M
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test) LIS |
Describe control (treatment/procedure/test: Topical GTN |
Length of follow-up: 2 weeks.
Loss-to-follow-up: None. |
Painfree I: 48/50 (96%) C: 35/50 (70%)
|
Author’s conclusion: It is concluded that 2% nifedipine paste is as effective as 0.5% GTN ointment in terms of efficacy in management of chronic anal fissure. However, the study was conducted on a limited number of patients and many aspects of nifedipine, e.g., side effects were not compared with GTN, it is suggested that further research could help in adapting the nifedipine as a first line treatment in chronic anal fissure.
|
|
Mustafa (2022) |
Type of study: RCT.
Setting and country: Colorectal surgery unit, department of surgery, Bagabandhu Sheikh Mujib Medical University.
Funding and conflicts of interest: No information. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 47 Control: N = 47
Important prognostic factors2: age ± SD: I: 34.6 (10.4) C: 33.2 (8.6)
Sex: I: 25/47 (53.2%) M C: 19/47 (40.4%) M
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test: GTN
|
Describe control (treatment/procedure/test: LIS |
Length of follow-up: 6 months.
Loss-to-follow-up: I: N = 4 C: N = 3 |
Non-healing of the fissure: I: 11/43 C: 2/44
Incontinence I: 0/43 C: 4/44 |
Author’s conclusion: See original publication. |
|
Tahir (2022) |
Type of study: RCT.
Setting and country: Hospital, Lahore Pakistan.
Funding and conflicts of interest: None declared. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 50 Control: N = 50
Important prognostic factors2: age ± SD: I: 39.5 (4.7) C: 38.9 (5.1)
Sex: I: 23/50 46(%) M C: 27/50 (44%) M
Groups comparable at baseline? Yes.
|
Describe intervention (treatment/procedure/test: LIS
|
Describe control (treatment/procedure/test: Anal advancement flap. |
Length of follow-up: 3 months.
Loss-to-follow-up: None. |
Fissure healing I: 44/50 (88%) C: 48/50 (96%) |
Author’s conclusion: Anal advancement flap surgical method is considerably a better treatment method for the treatment of anal fissures. Low post- operative infections rate was also observed anal fissure flap group as compared to lateral sphinecterotomy group.
|
|
Nour, 2020 |
Type of study: Randomized comparative clinical trial
Setting and country: General surgery department, Zagazig Faculty of Medicine, Egypt.
Funding and conflicts of interest: Not reported. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Botox: N=48 LIS: N=48
Important prognostic factors2: age ± SD: Botox: 33.46 (10.18) LIS: 32.29 (9.88) P=0.29
Sex: I: 32/48 (66.7%) M C: 26/48 (54.2%) M P=0.21
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test:
Botulinum toxin (BOTOX) injection; was performed under general anesthesia in the lithotomy position, where 80 IU of (BOTOX) was injected in four positions each 20 IU namely in 5, 7, 11, and 1 O’clock positions in the internal sphincter not deeper than the midpoint of the anal canal. |
Describe control (treatment/procedure/test:
Lateral internal sphincterotomy; was performed under general anesthesia where the lower part of the internal sphincter was cut by electerocautery after opening the skin of the intersphincteric groove, on the left lateral site and not extending beyond the proximal end of the fissure, the chronic fissure complex was also removed. The wound was left open at the end of the procedure after sufficient hemostasis. |
Length of follow-up: 1 week and 1, 2, 3, 6, 9, and 12 months.
Loss-to-follow-up: None.
Incomplete outcome data: None. |
Non-healing per month, 1st month, n/N (%): Botox: 31/48 (64.6%) LIS: 30/48 (62.5%) P=0.42
Non-healing per month, 2nd month, n/N (%): Botox: 11/48 (22.9%) LIS: 4/48 (8.3%) P=0.024
Incontinence to flatus 1st months, n/N (%): Botox: 8/48 (16.6%) LIS: 5/48 (10.4%) P=0.37
Incontinence to flatus after 6 months, n/N (%): Botox: 0/48 (0%) LIS: 2/48 (4.2%) P=0.15
|
Author’s conclusion:
(BOTOX) injection is safer than (LIS) in treatment of CAF but with less efficacy, its dose need to be adjusted, (LIS) is more efficient but anal sphincter tone need to be assessed before the operation. |
|
Venkatesh (2019) |
Type of study: Comparative randomized controlled trial.
Setting and country: Rajarajeswari Medical College and Hospital Bengaluru
Funding and conflicts of interest: None declared. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Diltiazem (CCB): N=50 GTN: N=50
Important prognostic factors2: age ± SD: Diltiazem: 38 GTN: 36
Sex: Diltiazem: 24/50 (48%) M GTN: 27/50 (54%) M
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test:
Patients were advised to apply a pea size (approx. 250 mg) quantity of 2% DTZ cream by fingertip to the anal verge twice daily for 8 weeks.
|
Describe control (treatment/procedure/test:
Patients were advised to apply a pea size (approx. 250 mg) quantity of 0.2% GTN ointment by fingertip to the anal verge twice daily for 8 weeks. |
Length of follow-up: 8 weeks
Loss-to-follow-up: None.
Incomplete outcome data: None. |
Non-healing of the fissure, n/N (%)
2nd week: Diltiazem: 49/50 (98.0%) GTN: 48/50 (96.0%)
4th week: Diltiazem: 18/50 (36%) GTN: 20/50 (40%)
6th week: Diltiazem: 10/50 (20%) GTN: 12/50 (24%) |
Author’s conclusion:
To conclude, CAF healing was found in 80% of the cases who received topical DTZ. The duration of the treatment was quite long with topical agents hence causing less patient compliance. Topical 2% DTZ appeared to be well tolerated and effective preferred first-line method of chemical sphincterotomy with less side effects. |
|
Ahmed (2018) |
Type of study: Prospective, randomized clinical study.
Setting and country: Department of general surgery, Bolan Medical Complex Hospital, Quetta Pakistan.
Funding and conflicts of interest: Not reported in the study. |
Inclusion criteria: Patients with CAF having age 20 years to 70 years.
Exclusion criteria: Patients with anal fissure with associated other anorectal disorders e.g. anorectal abscess or fistula, with history of previous dilatation of anus and previous perineal surgery were excluded.
N total at baseline: N=100 Closed LIS: N=50 Open LIS: N=50
Important prognostic factors2: age ± SD: CLIS: 39.12 (12.34) OLIS: 41.40 (11.6) P=0.35
Sex: CLIS: 32/50 (64%) M OLIS: 35/50 (70%) M P=0.52
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test):
IN CLIS patients, a cut entry point was made with a Von Graffe's sharp edge, either into the inter-sphincteric groove or into the submucosa. The front line of the cutting edge was pivoted toward the interior sphincter and a halfway sphincterotomy was finished. The skin wound entry point was left open. |
Describe control (treatment/procedure/test):
For OLIS, we use endoscope for anal canal visualization. A longitudinal entry point was made in the anoderm, and the distal portion of the internal anal sphincter was partitioned under direct vision took after by closing of the mucosa. |
Length of follow-up: 5 days post-op
Loss-to-follow-up: None.
Incomplete outcome data: None. |
(fecal) Incontinence, n/N (%):
CLIS: 3/50 (6.0%) OLIS: 9/50 (18.0%) P=0.06
Pain, mean (SD), 12 hours postop CLIS: 5.76 (0.91) OLIS: 6.45 (0.79) P<0.0001
Pain, mean (SD), 24 hours postop CLIS: 2.00 (0.29) OLIS: 2.39 (0.61) P=0.01 |
Author’s conclusion:
Closed lateral internal sphincterotomy (CLIS) is superior to open lateral internal sphincterotomy (OLIS) for the surgical management of chronic anal fissure (CIF). |
|
Ruiz-Tovar (2017) |
Type of study: Prospective randomized study.
Setting and country: Garcilaso Clinic, Madrid, Spain.
Funding and conflicts of interest: Not reported in the study. |
Inclusion criteria: `patients with a diagnosis of chronic anal fissure treated at the Garcilaso Clinic between January 2014 and July 2015.
Exclusion criteria: Patients with associated anal pathologies, intestinal inflammation disorders, immunosuppression, or fissures secondary to underlying diseases (eg, aiDs, tuberculosis, or sexually transmitted diseases). Also excluded were patients with a history of headaches, heart disease, or intolerance to nitrates; pregnant or lactating women; patients with closed angle glaucoma; and patients <18 years of age.
N total at baseline: N=80 GTN: N=40 PPTNS: N=40
Important prognostic factors2: age ± SD: GTN: 46.8 (8.1) PPTNS: 50.0 (9.0) P=0.34
Sex: GTN: 16/40 (40%) M PPTNS: 18/40 (45%) M P=0.82
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test):
375.0 mg of ointment (containing 1.5mg of glyceryl trinitrate), applied with a gloved finger to the distal anal canal, every 12 hours for 8 weeks. |
Describe control (treatment/procedure/test):
Subjects underwent one 30-minute session 2 days per week for 8 consecutive weeks. The patients attended the outpatient clinic to undergo the treatments. All of the patients went on their own, without medical transport. Patients were placed in the su- pine position without anesthesia. PPtns was delivered using a needle electrode that was inserted 3 to 4 cm cepha- lad and 2cm posterior to the medial malleolus at a 60o angle toward the ankle joint to a depth of ≈0.5 to 1.0 cm. successful placement was confirmed by the presence of an electric sensation 5 cm above and below the insertion site or a digital plantar flexion. PPtns was delivered at the highest amplification (0–20 ma) at a frequency of 20 hz, causing neither a motor response nor pain. |
Length of follow-up:
Loss-to-follow-up: Intervention: N=6 (%) Reasons (describe)
Control: N=0 (0%) |
Non-healing of the fissure, n/N (%):
2 weeks GTN: 14/40 (35%) PPTNS: 10/40 (25%)
8 weeks GTN: 13/40 (32.5%) PPTNS: 5/40 (12.5%)
Pain, median (IQR) GTN: 4 (0-9) PTNS: 3 (0-8) |
Author’s conclusion:
GTN treatment is associated with incapacitating headache that leads to treatment discontinuation in 15% of patients. By contrast, PPTNS achieved an 87.5% healing rate (vs 65.0% for GTN) with no adverse effects. PPTNS can thus be considered a safe and effective alternative to GTN for treatment of chronic anal fissure, which is in some ways superior to GTN. |
|
Akinci, 2020 |
Type of study: Prospective, randomized controlled trial.
Setting and country: Hakkari State Hospital General Surgery Clinic, Hakkari, Turkey.
Funding and conflicts of interest: None declared. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: N=100 GTN: N=50 Topical nifedipine (ND): N=50
Important prognostic factors2: age ± SD: GTN: 29.36 (8.97) ND: 30.78 (8.55) P=0.288
Sex: GTN: 25/50 (50%) M ND: 27/50 (54%%) M P=0.689
Groups comparable at baseline? Yes. |
Describe intervention (treatment/procedure/test):
0.2% glyceryl trinitrate (GTN) |
Describe control (treatment/procedure/test):
0.5% topical nifedipine (ND) |
Length of follow-up: 21 days
Loss-to-follow-up: None.
Incomplete outcome data: None. |
Non-healing of the fissure, n/N (%):
GTN: 18/50 (36%) ND: 7/50 (14%) P=0.011
Recurrence, n/N (%):
GTN: 19/50 (38%) ND: 9/50 (18%) P=0.026 |
Author’s conclusion
Data obtained from our study shows that both glyceryl trinitrate and topical nifedipine have favorable effects on anal fissure treatment. However, topical 0.5% nifedipine is superior to 0.2% glyceryl trinitrate in the treatment of anal fissure in terms of symptomatic relief, decrease in pain score, healing, drug side effects, and recurrence. But, it is a fact that there is a need for prospective clinical studies with a larger number of patients, long-term follow-up, and that are supported with manometric measurements. |
|
Akhtar, 2016 |
Type of study: Randomized controlled trial
Setting and country: Department of Surgery Nishter Hospital Multan, Pakistan
Funding and conflicts of interest: Not reported. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: N=94 LIS: 47 GTN: N=47
Important prognostic factors2: age ± SD: LIS: GTN:
Sex: LIS: 30/47 (63.8%) M GTN: 17/47 (36.2%) M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Lateral internal sphincterotomy (LIS) |
Describe control (treatment/procedure/test):
Glyceryl trinitrate (GTN) 0.2% cream |
Length of follow-up: Six weeks
Loss-to-follow-up: None.
Incomplete outcome data: None. |
Non-healing of the fissure, n/N (%)
LIS: 6/47 (12.77%) GTN: 18/47 (38.3%) |
Author’s conclusion
Results of this study revealed that frequency of healing in patients with acute anal fissure is better in patients managed with Lateral internal sphincterotomy as compare to patients managed the GTN cream. In male patients there is no statistical difference between healing rate of both groups but female patients found with higher healing rate in Lateral internal sphincterotomy group as compare to GTN cream group. |
|
Farooq, 2012 |
Type of study: Quasi-experimental study.
Setting and country: Department of surgery (unit-I), Sir Ganga Ram Hospital, Lahore.
Funding and conflicts of interest: Not reported. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: N=100 GTN: N=50 LIS: N=50
Important prognostic factors2: age ± SD: GTN: 36.56 (8.42) LIS: 35.14 (9.48) P>0.05
Sex: GTN: 22/50 (44%) M LIS: 17/50 (34%)% M P>0.05
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
0.2% GTN ointment locally 3 to 4 times daily along with sitz bath and stool softeners |
Describe control (treatment/procedure/test):
Lateral internal sphincterotomy (LIS) |
Length of follow-up: 2nd postoperative day, the end of the first week, third week, sixth week, and after 3 months.
Loss-to-follow-up: None.
Incomplete outcome data: None. |
Non-healing of the fissure, n/N (%)
GTN: 18/50 (36%) LIS: 0/50 (0%) P<0.05
(flatus) Incontinence, n/N (%): GTN: 0/50 (0%) LIS: 5/50 (10%) |
Author’s conclusion
Surgical sphincterotomy is better than chemical sphincterotomy in the management of acute anal fissure in terms of early symptomatic relief and high healing rates. However, chemical sphincterotomy heals 54% of patients in out patient setting, associated with less work loss that is no hospital admission is required and is not detrimental to continence so it has a definite role in the management of acute anal fissure. |
Risk of bias table
Systematic review(s)
|
Study
First author, year |
Appropriate and clearly focused question?1
Yes/no/unclear |
Comprehensive and systematic literature search?2
Yes/no/unclear |
Description of included and excluded studies?3
Yes/no/unclear |
Description of relevant characteristics of included studies?4
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?5
Yes/no/unclear/notapplicable |
Assessment of scientific quality of included studies?6
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?7
Yes/no/unclear |
Potential risk of publication bias taken into account?8
Yes/no/unclear |
Potential conflicts of interest reported?9
Yes/no/unclear |
|
Nelson, 2017 |
Yes |
Yes |
Yes |
Yes |
Not applicable |
Yes |
Yes |
Yes |
Yes |
Randomized controlled trial(s)
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated? a
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?b
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?c
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded? Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?d
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?e
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?f
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measureg
LOW Some concerns HIGH |
|
Hassan (2022) |
Probably yes. |
No information |
No information |
Definitely no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns
Reason: Allocation of concealment process not reported; blinding unclear. |
|
Mustafa (2022) |
Definitely yes.
Reason: Randomization with lottery. |
No information. |
No information. |
Probably no
Reason: LTFU almost equal in both groups. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns
Reason: Allocation of concealment process not reported; blinding unclear. |
|
Tahir (2022) |
Definitely yes.
Reason: The patients were randomly selected by computer generated numbers into two groups. |
No information. |
No information. |
Definitely no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns
Reason: Allocation of concealment process not reported; blinding unclear. |
|
Herreros (2021) |
Definitely yes
Reason: A randomized, controlled, double-blind, 2-arm, parallel- group trial was conducted |
Probably yes.
Reason: All patients received a local injection of BT. They were randomly assigned to local gel by a free computer-gener- ated table of random numbers with a 1:1 allocation rate |
Definitely yes.
Reason: All patients and researchers involved in the different phases of the study were blinded to treatments. |
Definitely no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Low |
|
Malik (2021) |
Definitely yes.
Reason: The patients were randomly selected by computer generated numbers into two groups. |
No information. |
No information. |
Definitely no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns
Reason: Allocation of concealment process not reported; blinding unclear. |
|
Khan (2021) |
Definitely yes.
Reason: The patients were randomly selected by computer generated numbers into two groups. |
No information. |
No information. |
Definitely no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns
Reason: Allocation of concealment process not reported; blinding unclear. |
|
Nour, 2020 |
Definitely yes
Reason: The participants were randomly allocated into two groups. |
Definitely yes
Reason: Randomization was achieved using computer generated cards. , study sample size was calculated by the statistical unit of IRB in our institute. |
No information |
Definitely no
Reason: no lost to follow-up in the study. |
Definitely yes
Reason: all predefined outcome measures were reported. |
Probably yes |
Low |
|
Venkatesh, 2019 |
No information |
No information |
No information |
Definitely no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns
Reason: randomization and allocation of concealment process not reported; blinding unclear. |
|
Akinci, 2020 |
No information |
No information |
No information |
Definitely no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns/high
Reason: no information regarding allocation sequence, allocation concealment, blinding and other problems that could put it at a risk of bias. |
|
Ahmed (2018) |
No information |
No information |
No information |
Probably no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns: randomization process not reported; allocation concealment not reported; blinding not reported. |
|
Ruiz-Tovar, 2017 |
Definitely yes
Reason: patients were randomly assigned to one of the treatment groups. |
Definitely yes
Reason A simple computerized randomization scheme at a 1:1 ratio was used. |
Probably yes
Reason: Data were collected by an independent data manager and analyzed by an independent statistician. An independent data monitoring committee supervised the compliance with the study protocol and the correct collection of the data. |
Probably yes:
Reason: more lost to follow-up in GTN group compared to PPTNS group (N=6 vs N=0). |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns: Differences in lost to follow-up. |
|
Akhtar, 2016 |
Definitely yes
Reason: All included patients were offered to pick up a slip from total mixed up slips (half-slips were contain letter “A” and other half-slips contain letter “B”) and he/she was placed in that group (Group-A or Group-B according to slip). |
Definitely yes
Reason: All included patients were offered to pick up a slip from total mixed up slips (half-slips were contain letter “A” and other half-slips contain letter “B”) and he/she was placed in that group (Group-A or Group-B according to slip). |
No information |
Probably no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns
Reason: blinding not reported of outcome assessors not reported. |
|
Farooq, 2012 |
Probably yes
Reason: Patients were randomly divided into two treatment groups A and B. |
No information |
No information |
Probably no
Reason: no lost to follow-up in the study. |
Probably yes
Reason: all predefined outcome measures were reported. |
No information |
Some concerns
Reason: no information regarding allocation concealment, blinding and other possible bias. |
Table of excluded studies
|
Author and year |
Reason for exclusion |
|
Gupta (2023) |
Does not match PICO. |
|
Van Reijn-Baggen (2022) |
Does not match PICO. |
|
Shahid (2022) |
Does not match PICO. |
|
Sungurtekin (2022) |
Does not match PICO. |
|
Mert (2022) |
Does not match PICO. |
|
Nordholm-Carstensen, 2020 |
Does not match PICO |
|
Mosleh, 2020 |
Does not match PICO |
|
Emile, 2020 |
Does not match PICO |
|
Nelson, 2020 |
Does not match PICO |
|
Sekmen, 2020 |
Does not match PICO |
|
Emile, 2020 |
Does not match PICO |
|
Yilmaz, 2020 |
Intervention not relevant for Dutch practice. |
|
Acharya, 2019 |
Does not match PICO |
|
Tavakoli-Dastjerdi, 2019 |
Does not match PICO |
|
Alvandipour, 2018 |
Does not match PICO |
|
Chiaretti, 2018 |
Does not match PICO |
|
Pilkington, 2018 |
Does not match PICO |
|
Ebinger, 2017 |
No additional studies/information compared to Nelson (2017), Boland (2020), and Sahebally (2018a) |
|
Ala, 2016 |
Does not match PICO |
|
Lin, 2016 |
Does not match PICO |
|
Bockiewicz, 2016 |
Does not match PICO |
|
Khaledifar, 2015 |
Does not match PICO |
|
Vaithianathan, 2015 |
Does not match PICO |
Verantwoording
Beoordelingsdatum en geldigheid
Publicatiedatum : 27-05-2024
Beoordeeld op geldigheid : 07-05-2024
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financierder heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2020 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor hemorroïden, anusscheurtjes en perianale fistels.
Belangenverklaringen
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Mw. dr. M.S. (Mich) Dunker |
Colorectaal chirurg |
Geen. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen Geen.
|
Geen restricties. |
|
Dhr. dr. D.D.E. (David) Zimmerman |
Colorectaal chirurg |
* Lid Executive Committee European Society Coloproctology (onbetaald) * Lid Education Committee European Society Coloproctology (onbetaald) * Voorzitter werkgroep richtlijn 'Perianal Fistula', European Society Coloproctology (onbetaald) * Secretaris Examencommissie UEMS, Divisie Coloproctologie (onbetaald) * Vice voorzitter Dutch Society of Colorectal Surgery (onbetaald).
|
Persoonlijke financiële belangen Adviseur, Takeda, eenmalig, onkostenvergoeding ontvangen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen Geen. |
Geen restricties. |
|
Mw. dr. S.O. (Stefanie) Breukink |
Chirurg |
Chair guideline commitee ESCP, onbetaald. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek PI RCT Napoleon study: Cost-effectiveness and effectiveness of rubber band ligation versus sutured mucopexy versus haemorrhoidectomy in patients with recurrent haemorrhoidal disease: a multicentre, randomized controlled trial. ZonMw subsidie.
Intellectuele belangen en reputatie PI van richtlijn ESCP haemorrhoidal disease
ESCP = European Society of Coloproctology
escp.eu.com/images/guidelines/documents/escp-guidelines-haemorrhoidal-disease.
Overige belangen Geen.
|
Geen restricties. |
|
Mw. dr. O. (Oddeke) van Ruler
|
Chirurg |
Geen. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek PI ALERT-CD trial. Onderzoek naar praktijkvariatie en kwaliteit van leven bij patiënten met Crohnse perianale fistels. Funding TAKEDA. Crohnse fistels zijn geen onderdeel van deze richtlijn.
Intellectuele belangen en reputatie PI onderzoek naar autologe celtherapie bij cryptoglandulaire en Crohnse perianale fistels. Nog in experimentele fase derhalve geen onderdeel van deze richtlijn.
Overige belangen Geen.
|
Geen restricties. |
|
Mw. dr. J.M.T. (Jikke) Omloo |
Chirurg, Gelre ziekenhuizen |
Geen. |
Persoonlijke financiële belangen Niet van toepassing.
Persoonlijke relaties Niet van toepassing.
Extern gefinancierd onderzoek Niet van toepassing.
Intellectuele belangen en reputatie Niet van toepassing.
Overige belangen Niet van toepassing.
|
Geen restricties. |
|
Mw. dr. R.J.F. (Richelle) Felt - Bersma |
Maag- Darm – Leverarts |
MDL-arts aan de VU regulier, daarbij 1 dag ge/outsourced naar de Proctoskliniek te Bilthoven. Voorts 12/13x per jaar op de vrijdagmiddag Proctologie in MCV de Veluwe. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen Geen.
|
Geen restricties. |
|
Mw. dr. N.H.N. (Nynke) Meijer – de Vrieze |
Dermatoloog |
Geen. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen Geen.
|
Geen restricties. |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland voor de schriftelijke knelpuntenanalyse. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptmodules zijn tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Methode ontwikkeling
Evidence based
Implementatie
|
Aanbeveling |
Tijdspad voor implementatie: 1 tot 3 jaar of > 3 jaar |
Verwacht effect op kosten |
Randvoorwaarden voor implementatie (binnen aangegeven tijdspad) |
Mogelijke barrières voor implementatie1 |
Te ondernemen acties voor implementatie2 |
Verantwoordelijken voor acties3 |
Overige opmerkingen |
|
Alle aanbevelingen |
< 1 jaar |
Geen. |
Geen. |
Geen. |
Promoten verschijnen nieuwe richtlijn Proctologie |
Werkgroepleden en Kennisinstituut. Nederlandse Vereniging voor Heelkunde |
Geen. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten die hemorroïden, anusscheurtjes of perianale fistels ervaren. Tevens zijn er knelpunten aangedragen door middel van een schriftelijke knelpuntenanalyse. Een verslag hiervan is opgenomen onder aanverwante producten.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
Definitie |
|
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Zoekverantwoording
Algemene informatie
|
Richtlijn: Proctologie |
|
|
Uitgangsvraag: Wat is de beste conservatieve behandeling van fissura ani? |
|
|
Database(s): Medline (OVID), Embase |
Datum: 17-04-2023 |
|
Periode: >2015 |
Talen: Engels, Nederlands |
|
Literatuurspecialist: Linda Niesink |
|
|
BMI zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting en opmerkingen:
→ Voor deze vraag is breed gezocht op het element fissura ani (in het blauw).
→ De opgegeven sleutelartikelen van Sahebally (2017, 2018), Ruiz-Tovar (2017), Lin (2016) en Bobkiewicz (2016) worden gevonden met de zoekopdracht. De artikelen van Nelson (2012), Berry (2013), Ala (2012) en Samim (2012) vallen er buiten op jaartal (<2015).
Dit is een update van de search op 24-02-2021 en daarna ook ontdubbeld met de opbrengst van de originele search. Dit leverde nog 76 nieuwe referenties op. Met de originele 142 treffers samen levert dat in totaal 218 referenties op.
|
|
|
Te gebruiken voor richtlijnen tekst: In de databases Embase (via embase.com) en Medline (via OVID) is op 17-04-2023 met relevante zoektermen gezocht naar systematische reviews en RCT’s over fissura ani. De literatuurzoekactie leverde 218 unieke treffers op. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
20 |
18 |
21 |
|
RCTs |
52 |
21 |
55 |
|
Totaal |
72 |
39 |
76 |
Zoekstrategie
|
Database |
Zoektermen |
||||||||||||||||||||||||
|
Embase
|
|
||||||||||||||||||||||||
|
Medline (OVID)
|
1 exp Fissure in Ano/ or ((fissura or fissure or fissures or ulcer or ulcers) adj3 (ani or ano or anal or anus or anorectal)).ti,ab,kf. (3045) 2 limit 1 to (yr="2021 -Current" and (dutch or english)) (184) 3 2 not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) (174) 4 (meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf.) (662248) 5 (exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw.) not (animals/ not humans/) (2377153) 6 3 and 4 (18) – SRs 7 (3 and 5) not 6 (21) – RCTs 8 6 or 7 (39)
|