Chirurgische behandeling
Uitgangsvraag
Wat is de plaats van chirurgische behandeling bij patiënten met ganglion?
Aanbeveling
Overweeg chirurgische behandeling bij falen van niet-operatieve behandeling of bij persisterende klachten. Vermeld dan wel de kans op een recidief.
Doe geen aspiratie bij polsganglion, tenzij er zwaarwegende contra-indicaties zijn voor een operatieve behandeling of een sterke wens van de patiënt voor niet-operatieve behandeling die wel tot snelle resolutie van symptomen kan leiden. Vermeld hierbij dan wel de hoge recidiefkans.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is literatuuronderzoek verricht naar plaats van chirurgische behandeling (arthroscopische of open excisie) van een polsganglion ten opzichte van niet-chirurgische behandelingen, waarbij de opties waren: expectatief beleid (‘wait and see'); handtherapie; en aspiratie, al dan niet met het achterlaten van een injectie. Het had de voorkeur om chirurgie te vergelijken met een expectatief beleid, aangezien die optie als beste voortkwam uit het onderzoek uitgevoerd in de module Niet-chirurgische behandeling. Pijnklachten en handfunctie of het uitvoeren van dagelijkse activiteiten werden gedefinieerd als cruciale uitkomstmaten en kwaliteit van leven, tevredenheid met het behandelresultaat, het aantal dagen wanneer iemand weer in staat is om te werken, complicaties, recidief, de bewegelijkheid van de pols, kracht, ernst van de symptomen en handesthetiek werden als belangrijke uitkomstmaten gedefinieerd.
Op basis van het literatuuronderzoek kan worden geconcludeerd dat de literatuur zeer onzeker is over het effect van chirurgie vergeleken met niet-chirurgische behandelingen op handfunctie, pijnklachten na de behandeling, de ernst van de symptomen, de complicaties van een behandeling, de recidiefkans, en het aantal dagen wanneer iemand weer in staat is om te werken na de behandeling van een polsganglion. De bewijskracht hiervoor is zeer laag. De redenen voor de zeer lage bewijskracht zijn observationele designs van de geïncludeerde studies, alsmede de kleine aantallen patiënten en brede betrouwbaarheidsintervallen per uitkomstmaat.
Er is een studie gevonden die arthroscopische of open excisie heeft vergeleken met een expectatief beleid, maar deze observationele studie is uitgevoerd onder kinderen. Er zijn geen studies gevonden die chirurgische behandeling hebben vergeleken met handtherapie.
De afweging van de voor- en nadelen van een interventie dienen hierbij in het licht van de aard en ernst van de klachten te worden gezien. Voor een patiënt bij wie functionele klachten op voorgrond staan, zullen de voor- en nadelen anders wegen dan voor de patiënt die zuiver cosmetische klachten ervaart.
Chirurgische behandelingen ten opzichte van niet-chirurgische behandelingen
Er is slechts een studie die chirurgie vergeleken heeft met expectatief beleid, en die studie was onder kinderen (Zinger, 2020). Deze studie vond dat kinderen na chirurgie een kleinere kans hebben op persistence/recurrence. Echter, ze vonden ook dat bijna de helft van de ganglia zelf oplost, en dat als dat gebeurt het binnen 18 maanden is. Gezien eventuele complicaties en risico’s behorend bij chirurgie, raden zij aan om ten minste 18 maanden expectatief beleid aan te houden alvorens chirurgie in overweging te nemen.
Op basis van het huidige onderzoek lijkt aspiratie met of zonder het achterlaten van een werkzame stof niet effectiever te zijn dan een expectatief beleid (zie module Niet-chirurgische behandeling. Daarnaast worden er na aspiratie enige complicaties gerapporteerd, gerelateerd aan de aspiratie of injectie, met name pijnklachten, huidafwijkingen (bij infiltratie met corticosteroïden) en infecties (Dias, 2003; Dias, 2007; Head, 2015). Daarom heeft een expectatief beleid de voorkeur boven aspiratie. De literatuur laat ook zien dat er een kleinere recidiefkans is na chirurgie ten opzichte van aspiratie (Khan, 2011; Limpaphayom,2004; Dias, 2003; Dias, 2007, Wright, 1994; Rollins, 2013; Head, 2015; Ahmed Shah, 2019; Maaz-Ul-Hassan, 2017). Een recidief betekent niet noodzakelijkerwijs dat de behandeling gefaald is, tenzij de klachten gelijk of groter zijn dan voor de behandeling.
Bij het maken van de keuze voor een chirurgische excisie dient de duur en de ernst van de klacht behorende bij het polsganglion afgewogen te worden. Met name bij patiënten met ernstige, langdurige of toenemende klachten kan chirurgie overwogen worden, vooral als er sprake is (herhaalde) recurrence. Een nadeel van chirurgie is de grotere kans op complicaties (Khan, 2011; Limpaphayom,2004; Dias, 2003; Dias, 2007, Wright, 1994; Head, 2015) en meer werkverzuim dan bij aspiratie (Dias, 2003; Dias, 2007; Head, 2015). Daarnaast resulteert een open excisie in een litteken.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Patiënten die zorg zoeken bij polsganglionklachten presenteren zich met verschillende behandeldoelstellingen. Naast pijn zijn esthetiek, functiebeperking of mobiliteitsbeperking problemen die ervaren worden. Door de aanwezigheid van deze problemen kunnen patiënten beperkt worden bij het uitvoeren van hun dagelijkse activiteiten, hobby’s en werkzaamheden. De zwaarte die door de patiënt aan bovenstaande problemen wordt gewogen kan verschillen. Daarom is het van belang dat alle behandelopties en de bijbehorende voor- en nadelen worden besproken, wat het mogelijk maakt de best passende behandeling te kiezen.
Niet-chirurgische behandeling
Zie voor informatie over de niet-chirurgische behandelingen (expectatief beleid, aspiratie, handtherapie) module Niet-chirurgische behandeling.
Chirurgisch beleid (arthroscopische of open excisie)
Voordeel van een chirurgisch beleid is de directe resolutie. De polsganglion is niet meer zichtbaar en veel van de klachten zullen direct opgelost zijn. Echter, de eerste dagen tot weken kan de patiënt last hebben van pijnklachten en meer beperkingen in activiteiten en participatie ten gevolge van de ingreep. De patiënt zal mogelijk hulp nodig hebben bij dagelijkse activiteiten. Ook is er een kans op complicaties. De pijn, beperkingen, werkverzuim en risico’s van de ingreep zullen echter voor een groep patiënten niet opwegen tegen de directe resolutie.
Kosten (middelenbeslag)
Chirurgie is duur, met name voor de maatschappij. De kosten van chirurgie worden grotendeels betaald vanuit de basisverzekering, afgezien van het eigen risico. Het werkverzuim dat in de meeste gevallen na chirurgie volgt, is ook duur.
Er zijn geen kosten verbonden aan een expectatief beleid, tenzij er beperkingen zijn in het arbeidsproces. De directe kosten van aspiratie zijn relatief laag en worden ook betaald vanuit de basisverzekering.
Hand-ergotherapie is (in 2023) opgenomen in de basisverzekering en wordt volledig vergoed tot een maximum van 10 uren per kalenderjaar per verzekerde. Wel gelden de kosten van het vastgestelde eigen risico dat jaarlijks door de zorgverzekeraar in rekening wordt gebracht. Handtherapie door een fysiotherapeut wordt (in 2023) niet vergoed vanuit de basisverzekering.
Daarom zijn de kosten voor de patiënt van handtherapie mogelijk hoger vergeleken met de kosten voor chirurgie. Mogelijk wordt er na chirurgie ook nog handtherapie aangeboden. Bij functiebeperkingen die leiden tot problemen in het arbeidsproces zullen de kosten voor chirurgie beter te verdedigen zijn dan bij esthetische argumenten.
Aanvaardbaarheid, haalbaarheid en implementatie
De werkgroep schat in dat alle behandelopties (chirurgie, afwachtend beleid, handtherapie) in principe aanvaardbaar zijn voor patiënten, al zullen zij de voor- en nadelen anders wegen. Het betalen van het eigen risico voor chirurgie, handtherapie en aspiratie kan als bezwaar worden gezien door patiënten, net als een eventuele eigen bijdrage voor handtherapie. Alle opties zijn reeds geïmplementeerd en beschikbaar.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Er is bewijs van zeer lage kwaliteit dat chirurgie en een expectatief beleid niet verschillen op het gebied van handfunctie. Een operatie geeft echter wel kans op bijwerkingen, zoals stijfheid, littekenproblematiek, infectie, doofheid, spierzwakte. Daarnaast volgt een herstelperiode direct na de ingreep. Daarom wordt aangeraden om altijd eerst een expectatief beleid te hanteren.
Er is bewijs van zeer lage kwaliteit dat chirurgie en aspiratie niet verschillen op het gebied van handfunctie, pijn en tevredenheid. De kans op een recidief is kleiner na chirurgie dan na aspiratie. Na aspiratie gaan patiënten wel weer sneller aan het werk dan na chirurgie. Ook is de kans op complicaties groter bij chirurgie dan bij aspiratie. Aspiratie wordt op basis van de huidige onderzoeken niet beter geacht dan expectatief beleid en daarom afgeraden (zie module Niet-chirurgische behandelin). Voor patiënten na een gefaald expectatief beleid of persisterende klachten en een wens tot snelle resolutie van symptomen kan chirurgie overwogen worden. Hierbij dient benoemd te worden dat chirurgie een hoge recidiefkans heeft.
Onderbouwing
Het natuurlijke beloop van een polsganglion is gunstig en de zwelling kan na jaren spontaan verdwijnen. Symptomatische polsganglia kunnen worden behandeld. Niet-chirurgische behandelmethodes bestaan uit wegdrukken, aspiratie van de ganglioninhoud en eventuele infiltratie met corticosteroïden en/of hyaluronidase (deze beste niet-chirurgische behandeling is onderzocht in Module Niet-chirurgische behandeling. Chirurgische behandeling is gericht op het verwijderen van de zwelling tot in het gewricht. De behandeling van polsganglions is berucht door de hoge recidiefkans. Derhalve is het van belang een goede balans te vinden tussen de ernst van de klachten, de mate van invasie en de kans op recidief.
I) Surgery versus expectative policy
1. Hand function/activities of daily life (critical)
|
Very low GRADE |
The evidence is very uncertain about the effect of arthroscopic or open surgery on hand function/activities of daily life when compared with expectative policy in patients with a wrist ganglion cyst.
Source: Zinger (2020) |
6. Complications (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of arthroscopic or open surgery on complications when compared with expectative policy in patients with a wrist ganglion cyst.
Source: Zinger (2020) |
7. Revision/recurrence (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of arthroscopic or open surgery on revision/recurrence when compared with expectative policy in patients with a wrist ganglion cyst.
Sources: Zinger (2020) |
Pain (critical), health-related QoL, satisfaction with treatment results, return to work/sport/hobby, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics (important)
|
- GRADE |
No evidence was found regarding the effect of surgery on pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, range of motion, grip and pinch strength, severity of symptoms, or hand aesthetics when compared with expectative policy in patients with a wrist ganglion cyst.
Sources: - |
II) Surgery versus aspiration
1. Hand function/activities of daily life (critical)
|
Very low GRADE |
The evidence is very uncertain about the effect of arthroscopic or open surgery on hand function/activities of daily life when compared with aspiration in patients with a wrist ganglion cyst.
Sources: Head (2015) (Dias, 2003; Dias, 2007) |
2. Pain (critical)
|
Very low GRADE |
The evidence is very uncertain about the effect of arthroscopic or open surgery on pain when compared with aspiration in patients with a wrist ganglion cyst.
Sources: Head (2015) (Dias, 2003; Dias, 2007) |
5. Return to work/sport/hobby (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of arthroscopic or open surgery on return to work/sport/hobby when compared with aspiration in patients with a wrist ganglion cyst.
Sources: Head (2015) (Dias, 2003; Dias, 2007). |
6. Complications (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of arthroscopic or open surgery on complications of treatment when compared with aspiration in patients with a wrist ganglion cyst.
Sources: Head (2015) (Khan, 2011; Limpaphayom,2004; Dias, 2003; Dias, 2007, Wright, 1994), Zinger (2020) |
7. Revision/recurrence (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of arthroscopic or open surgery on revision/recurrence when compared with aspiration in patients with a wrist ganglion cyst.
Sources: Head (2015) (Khan, 2011; Limpaphayom,2004; Dias, 2003; Dias, 2007, Wright, 1994; Rollins, 2013), Ahmed Shah (2019), Maaz-Ul-Hassan (2017) |
Health-related QoL, satisfaction with treatment results, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics, (important)
|
- GRADE |
No evidence was found regarding the effect of arthroscopic or open surgery on health-related QoL, satisfaction with treatment results, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics when compared with aspiration in patients with a wrist ganglion cyst.
Sources: - |
Description of studies
I) Surgery versus expectative policy
From the included studies, only the cohort study of Zinger (2020) compared surgical excision with non-surgical treatment; expectative policy (observation). Zinger included 40 participants in the surgery group with a follow-up of 6 years, and 50 in the observation group, with a follow-up of 3.5 years. They reported outcomes on recurrence/persistence, hand function, pain, and surgical complications. The participants, however, were 17 years or younger at the time of the cyst appearance.
II) Surgery versus aspiration
The systematic review of Head (2015) aimed to review the clinical outcomes of treatment for adult wrist ganglion cysts. Head (2015) included studies in which the study population included adult patients with wrist ganglion cysts, where recurrence or persistence of ganglion cysts was a measured outcome, and where patients had not previously received the treatment under investigation. Review articles, case studies, response letters, and conference proceedings were excluded. Studies in which a portion of the study population met inclusion criteria were included if the results of the subpopulation were presented separately. To identify relevant publications, Head (2015) searched MEDLINE and EMBASE, including studies from 1990 to December 2013. In total, six studies were included. All six studies, involving 591 participants, were included for our guideline (Wright, 1994; Dias, 2003; Limpaphayom, 2004; Dias, 2007; Khan, 2011; Rolllins, 2013). The methodological quality of the included (experimental and observational) studies in Head (2015) was evaluated with a modified Newcastle-Ottawa Scale by two independent authors.
Two studies had an RCT study design and compared surgical excision with aspiration (with or without corticosteroid). Limpaphayom (2004) included 11 patients that underwent surgical excision, and 13 patients that had aspiration followed by methylprednisolone acetate injection and immobilization. The follow up was 6 months. Khan (2011) included 18 patients that underwent surgical excision, and 18 patients that had aspiration followed by methylprednisolone acetate injection and immobilization. The follow up was 12 months. The reported outcomes in both trials were recurrence and adverse events.
Four studies had a cohort study design and compared surgical or arthroscopic excision with aspiration (with or without corticosteroid). Wright (2004) included 60 participants that had an excision and 24 that had aspiration with a follow-up of 5 years. Rollins (2013) included 28 participants in the excision group and 58 in the aspiration group with a follow-up of 1 year. Both studies reported recurrence as outcome measure. In the study of Dias (2007), patients who had their ganglion aspirated, had either aspiration alone or aspiration and injection of steroid (the number of patients with and without aspiration in combination with steroids were not reported). Dias (2003) included 77 participants with two- and five-years follow-up. Dias (2007) included 133 participants with a follow-up of more than five years. The reported outcomes in these studies were recurrence, complications, return to work, hand function, and pain.
Additionally, two studies (Maaz-Ul-Hassan, 2017; Ahmed Shah, 2019) from after the search date of Head compared surgical excision with aspiration (with or without corticosteroid). The trial of Maaz-Ul-Hassan, 2017 included 50 patients that had surgical excision and 50 patients that had aspiration with steroid injection with a follow-up of only 3 months. The reported outcome measure was recurrence. The cohort study of Ahmed Shah, 2019 included 18 patients that had surgical excision and 68 patients that had an aspiration followed by intralesional steroid (triamcinolone acetate) injection with a follow-up of 1 year. The outcome measure was recurrence.
Results
I) Surgery versus expectative policy
1. Hand function/activities of daily life (critical)
Zinger (2020) measured hand function with the Quick Disabilities of Arm, Shoulder, Hand (QuickDASH). The QuickDASH is a questionnaire with 11 items on performing activities and the severity of symptoms, ranging from 0 (no disability) to 100 (most severe disability). Participants that underwent surgical excision reported a mean of 12 (median 0, range: 0-70, a lower score reflects more ability) on hand function. Participants without treatment reported a mean of 15 (median 7, range: 0-73). This was not considered as a clinically relevant difference.
2. Pain (critical)
None of the included studies reported pain intensity for the comparison surgery versus expectative policy.
3. Health-related QoL (important)
None of the included studies reported the outcome health-related QoL.
4. Satisfaction with treatment results (important)
None of the included studies reported the outcome satisfaction with treatment results.
5. Return to work/sport/hobby (important)
None of the included studies reported (work)participation for the comparison surgery versus expectative policy.
6. Complications (important)
Zinger (2020) reported a surgical complication rate of 12/40 (30%) for the surgery group, including scar problems, joint stiffness, infection, numbness, and slight weakness. No surgical complications were reported for the expectative group, and therefore no risk difference is reported. No clinical relevance can be determined.
7. Revision/recurrence (important)
Zinger (2020) reported an overall persistence rate of 26/50 (52%) for those treated nonsurgically, compared with a recurrence rate of 6/40 (15%) in those treated surgically. No patients who had a recurrence had a revision. The risk ratio (95% CI) for persistence or recurrence is 0.29 (0.13-0.63) in favor of the surgical group. This was considered as a clinically relevant difference.
8. Range of motion (important)
None of the included studies reported physical measures for the comparison surgery versus expectative policy.
9. Grip and pinch strength (important)
None of the included studies reported the outcome grip and pinch strength.
10. Severity of symptoms (important)
None of the included studies reported the outcome severity of symptoms.
11. Hand aesthetics (important)
None of the included studies reported the outcome hand aesthetics.
II) Surgery versus aspiration
1. Hand function/activities of daily life (critical)
No included study measured hand function with a preferable instrument. However, two studies reported the outcome hand function in the systematic review of Head (2015) (Dias, 2003; Dias, 2007). Hand function was measured with the Patient Evaluation Measure (PEM) hand disability score. The PEM is a questionnaire, ranging from zero to 100 (in which a score of zero means no disability and 100 the worst disability), that evaluates the process of treatment, the current state of the hand, and provides an overall assessment. Six questions are related to symptoms, three to the impact of the disorder on the patient, two to satisfaction and three to general disability and handicap.
The results comparing surgery with aspiration were pooled in a meta-analysis. In the study of Dias (2003), the mean hand function score of the surgery group was 14.1, whereas the mean of the aspiration score was 17.1 (a lower score reflects a better function). In the study of Dias (2007), the mean function score of the surgery group was 19.2, whereas the mean score in the aspiration group was 13.8. This resulted in a pooled mean difference (MD) of 2.1 (95% CI -5.91 to 10.15), in favor of the aspiration group (Figure 1). This was not considered as a clinically relevant difference.
Figure 1. Forest plot of cohort studies showing the comparison between surgery (open or arthroscopic excision) relative to aspiration for hand function.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.

2. Pain (critical)
No included study measured pain with a preferable instrument. However, two studies reported the outcome pain in the systematic review of Head (2015) (Dias, 2003; Dias, 2007). The results were pooled in a meta-analysis. The pooled number of patients that reported pain after treatment of a wrist ganglion cyst in the surgery group was 41/182 (23%), compared to 30/117 (26%) in the aspiration group. This resulted in a pooled relative risk ratio (RR) of 0.92 (95% CI 0.61 to 1.38), in favor of the surgery group (Figure 2). This was not considered as a clinically relevant difference.
Figure 2. Forest plot of cohort studies showing the comparison between surgery (open or arthroscopic excision) relative to aspiration for pain.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.

3. Health-related QoL (important)
None of the included studies reported the outcome health-related QoL.
4. Satisfaction with treatment results (important)
No included study reported on patient satisfaction with the treatment results.
However, Dias (2003) reported that 83% of both the patients that underwent surgery as the patients that underwent aspiration were satisfied. Dias (2007) reported that 83% of the patients that underwent surgery and 81% of the patients that underwent aspiration were satisfied. This was not considered as a clinically relevant difference.
5. Return to work/sport/hobby (important)
Two studies reported the number of days off work in the systematic review of Head, 2015. The results were pooled in a meta-analysis. In the study of Dias (2007), the mean days off work was 10.9 in the surgery group, whereas the mean days off work was 3.2 in the aspiration group. In the study of Dias (2003), the mean days off work was 14.1 in the surgery group, whereas the mean days off work was 3.5 in the aspiration group. This resulted in a pooled mean difference (MD) of 8.9 days (95% CI 5.81 to 11.87), in favor of the aspiration group (Figure 3). This was considered as a clinically relevant difference.
Figure 3. Forest plot of cohort studies showing the comparison between surgery (open or arthroscopic excision) relative to aspiration for days off work
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.

6. Complications (important)
Five studies reported the outcome complications in the systematic review of Head (2015) (Limpaphayom, 2004; Khan, 2011; Dias, 2003; Dias, 2007, Wright, 1994). No complications occurred in the trials of Khan (2011) and Limpaphayom (2004). Wright (1994) reported a complication rate of 6/84 (7%) for the whole group. Complications included superficial infection, tendinitis, and pain dystrophy. Dias (2003) reported a complication rate of 16/79 (20%) for the excision group, and 2/38 (5%) for the aspiration group. Complications included wound infection, neuroma formation, hypertrophic scar, numbness in the distribution of palmar cutaneous branch of the median nerve and radial artery damage in one case. Dias (2007) reported the following complication rate for the aspiration group: 2/78 (3%), including scar tenderness. The complication rate reported for the surgical excision: 8/103 (8%), including numbness, scar tenderness and keloid formation.
The pooled number of patients with complications of wrist ganglion cyst treatment in the surgical excision group was 24/182 (13%), compared to 4/116 (3%) in the aspiration group. This resulted in a pooled relative risk ratio (RR) of 0.09 (95% CI -0.01 to 0.19), in favor of the aspiration group (Figure 4). This was not considered as a clinically relevant difference.
Figure 4. Forest plot of randomized controlled trials showing the comparison between surgery (open or arthroscopic excision) relative to aspiration for complications.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.

7. Revision/recurrence (important)
All six studies reported the outcome recurrence in the systematic review of Head (2015) (trials: Limpaphayom, 2004; Khan, 2011, cohort studies: Wright, 2004; Dias, 2003; Dias, 2007; Rollins, 2013). All three additional studies also reported the outcome recurrence.
In the trial of Limpaphayom, 2004, recurrence was determined by palpation at the dorsal of the wrist in flexion position. If this could detect the mass at six months, it would be considered as recurrence. The trial of Khan, 2011 used the same palpation method to determine recurrence. Detecting the swelling 1 year after the initial treatment was considered as recurrence. Maaz-Ul-Hassan, 2017 does not describe the determination of recurrence. They found that 6 of 50 (6%) of the patients that underwent surgical excision had a recurrence. From the patients that underwent aspiration with steroid injection, 29 of 50 (59%) had a recurrence. Due to the limited follow-up of only 3 months, we could not add the study of Maaz-Ul-Hassan to the meta-analysis.
From the RCT’s comparing surgery with aspiration, the pooled number of patients with recurrence of wrist ganglion cysts the surgical excision group was 3/29 (10%), compared to 15/31 (48%) in the aspiration group. This resulted in a pooled relative risk ratio (RR) of 0.24 (95% CI 0.08 to 0.71), in favor of the surgical excision group (Figure 5). This was considered as a clinically relevant difference.
Figure 5. Forest plot of randomized controlled trials showing the comparison between surgery (open or arthroscopic excision) relative to aspiration for recurrence.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.

Considering the cohort studies, Dias (2003) considered the ganglion to have recurred if it was present at either the 1-, 2- or 5-year follow-up, though this could represent either recurrence or the formation of a new ganglion at the same site. After initial treatment, if a ganglion had recurred at 2 years follow-up but subsequently disappeared before the 5-year follow-up, it was still considered to have recurred after the initial intervention. In the study of Dias (2007), the ganglion was considered to have recurred if it reappeared at the same site anytime between intervention and final follow-up, representing either a recurrence or the formation of a new ganglion. If a ganglion had recurred at the second-year follow-up but subsequently disappeared by the sixth-year follow-up, it was still recorded as a recurrence. In the study of Rollins (2013), the treatment was deemed to be successful if the patient did not develop recurrence within the minimum 12-month follow-up period. Wright (1994) determined recurrence with a patient-reported questionnaire, asking whether there was recurrence of the ganglion (i.e., further surgical, or conservative treatment). Subsequently, a retrospective chart review was performed, and patients reporting recurrence were personally contacted. Follow-up of the patients averaged 5 years (range: 2-11 years).
In the study of Ahmed Shah (2019) the ganglion was considered to have recurred if it was present at the 1-year follow-up. They reported a recurrence rate of 3/18 (17%) for the surgery group and 9/68 (13%) for the aspiration group. Due to the low quality of this study (no information about possible confounders, no correction for confounding factors, very limited number of surgical participants), we did not include this study in the meta-analysis.
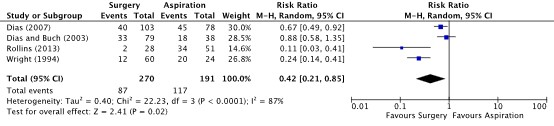
From the included cohort studies, the pooled number of patients with recurrence of wrist ganglion cysts the surgery group was 87/279 (31%), compared to 117/191 (61%) in the aspiration group. This resulted in a pooled relative risk ratio (RR) of 0.42 (95% CI 0.21 to 0.85), in favor of the surgery group (Figure 6). This was considered as a clinically relevant difference.
Figure 6. Forest plot of cohort studies showing the comparison between surgery (open or arthroscopic excision) relative to aspiration for recurrence.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.
8. Range of motion (important)
None of the included studies reported the outcome range of motion.
9. Grip and pinch strength (important)
None of the included studies reported the outcome grip and pinch strength.
10. Severity of symptoms (important)
None of the included studies reported the outcome severity of symptoms.
11. Hand aesthetics (important)
None of the included studies reported the outcome hand aesthetics.
Level of evidence of the literature
I) Surgery versus expectative policy
1. Hand function/activities of daily life (critical)
The level of evidence regarding the outcome measure hand function/activities of daily life comes from one observational study and therefore started low. The level of evidence was downgraded by two levels because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision), and the small number of patients and events (imprecision), and because the patient population (children) did not align with our PICO (indirectness). The level of evidence was very low.
6. Complications (important)
The level of evidence regarding the outcome measure complications comes from one observational study and therefore started low. The level of evidence was downgraded by two levels because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision), and the small number of patients and events (imprecision), and because the patient population (children) did not align with our PICO (indirectness). The level of evidence was very low.
7. Revision/recurrence (important)
The level of evidence regarding the outcome measure revision/recurrence comes from one observational study and therefore started low. The level of evidence was downgraded by three levels because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision), the small number of patients and events (imprecision), and because the patient population (children) did not align with our PICO (indirectness). The level of evidence was very low.
Pain (critical), health-related QoL, satisfaction with treatment results, return to work/sport/hobby, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics (important)
No evidence was found regarding the outcome measures pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics and therefore the level of evidence could not be graded.
II) Surgery versus aspiration
1. Hand function/activities of daily life (critical)
The level of evidence regarding the outcome measure hand function/activities of daily life comes from observational studies and therefore starts low. The level of evidence was downgraded by one level because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision). The level of evidence was very low.
2. Pain (critical)
The level of evidence regarding the outcome measure pain comes from observational studies and therefore starts low. The level of evidence was downgraded by one level because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision). The level of evidence was very low.
5. Return to work/sport/hobby (important)
The level of evidence regarding the outcome measure return to work/sport/hobby comes from observational studies and therefore starts low. The level of evidence was downgraded by one level because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision). The level of evidence was very low.
6. Complications (important)
The level of evidence regarding the outcome measure complications comes from both RCTs and observational studies and therefore starts low. The level of evidence was downgraded by two levels because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision) and because of the low number of patients and events (imprecision). The level of evidence was very low.
7. Revision/recurrence (important)
The level of evidence regarding the outcome measure revision/recurrence comes from both RCTs and observational studies and therefore started low. The level of evidence was downgraded by two levels because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision), and high heterogeneity (inconsistency). The level of evidence was very low.
Health-related QoL, satisfaction with treatment results, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics, (important)
No evidence was found regarding the outcome measures Health-related QoL, satisfaction with treatment results, range of motion, grip and pinch strength, severity of symptoms, and hand aesthetics and therefore the level of evidence could not be graded.
A systematic review of the literature was performed to answer the following question:
What are the beneficial and harmful effects of surgery compared to non-surgical treatment (expectative policy, hand therapy or aspiration) for ganglion cysts?
|
P (Patients) |
Patients aged older than 16 years with ganglion cysts (both dorsal and volar of the wrist) |
|
I (Intervention) |
Surgery (open or scopic) |
|
C (Comparison) |
Non-surgical treatment (expectative policy, hand therapy or aspiration (with or without infiltration)) |
|
O (Outcome) |
Hand function/activities of daily life, pain, health-related Quality of Life (QoL), satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics |
Relevant outcome measures
The guideline development group considered hand function/activities of daily life and pain as critical outcomes for decision making; and health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics as important outcomes for decision making as important outcomes for decision making.
The guideline development group defined the outcome measures as follows:
- Hand function/activities of daily life: preferably measured with Boston Carpal Tunnel Questionnaire (BCTQ), subscale Functional Status Scale (FSS) (Levine, 1993; Smits, 2014), Michigan Hand Outcomes Questionnaire (MHQ) or Patient-Rated Wrist/Hand Evaluation (PRWHE)
- Pain: preferably measured with a Numeric Rating Scale (NRS), or Visual Analogue Scale (VAS)
- Health-related Quality of Life (HR-QOL): preferably measured with EQ-5D-5L
- Satisfaction with treatment results: A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
- Return to work/sport/hobby: time off work, sport, or hobbies in days
- Complications: complications up to 30 days postoperative/start treatment
- Revision/recurrence: report of any repeat operation for the same condition in the same patient due to disease progression or recurrence, or as follow-up to failed previous surgery. Subsequently, description of new / additional treatment (within final time point of tracks) (Wouters, 2021)
- Range of motion: evaluated via Goniometry and Kapandji Score (Wouters, 2021)
- Grip and pinch strength: Grip: evaluated via hand-held dynamometer, Pinch: evaluated via Lateral/Key Pinch and Tip Pinch (Wouters, 2021)
- Severity of symptoms: preferably measured with BCTQ, subscale Symptom Severity Scale (SSS) (Levine, 1993; Smits, 2014)
- Hand aesthetics: A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
The following limits were used for minimal clinically (patient) important differences per outcome:
- Hand function/activities of daily life: 28% difference in BCTQ-FSS (De Kleermaker, 2019)
- Pain: 2 points on a NRS or VAS scale, on a scale from 0 to 10.
- Health-related QoL: GRADE standard limits*
- Satisfaction with treatment results: GRADE standard limits*
- Return to work/sport/hobby: 1 working week (5 days)
- Complications: GRADE standard limits*
- Recurrence/revision: GRADE standard limits*
- Range of motion: GRADE standard limits*
- Grip and pinch strength: GRADE standard limits*
- Severity of symptoms: 46% difference in BCTQ-SSS (De Kleermaker, 2019)
- Hand aesthetics: GRADE standard limits*
* Default thresholds proposed by the international GRADE working group were used: a 25% difference in relative risk (RR) for dichotomous outcomes (RR <0.80 or RR >1.25), or 0.5 standard deviations (SD) for continuous outcomes
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until June 8th, 2022. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 250 hits.
Studies were selected based on the following criteria: study type is a systematic review, randomized controlled trials, or observational studies. The study made a comparison between surgery and non-surgical treatment in patients with wrist ganglion cysts and reported at least one outcome of interest.
Twenty studies were initially selected based on title and abstract screening. After reading the full text, 16 studies were excluded (see the table with reasons for exclusion under the tab Methods), and 4 studies, including a systematic review, were included. The included systematic review of Head, 2015, two trials and four cohort studies met our PICO and were therefore included. One RCT (Maaz-Ul-Hassan, 2017) and two cohort studies (Ahmad Shah, 2019 and Zinger, 2020) published after the search date in Head, 2015 were included. In total, we included 3 RCTs and 6 cohort studies in the literature analysis.
Results
Nine studies were included in the analysis of the literature. One study compared surgery with expectative policy, and eight studies compared surgery with aspiration. No studies were found that compared surgery with hand therapy. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables. The results are presented separately for the comparison of surgery versus expectative policy and surgery versus aspiration.
- Ahmad Shah, A., Raina, A. H., Ganie, M. A., & Kumar, I. A. (2019). Comparison of Aspiration Followed by Intra-Lesional Steroid Injection and Surgical Excision in Management of Dorsal Wrist Ganglion. World journal of plastic surgery, 8(2), 181-184.
- Dias, J., & Buch, K. (2003). Palmar wrist ganglion: Does intervention improve outcome A prospective study of the natural history and patient-reported treatment outcomes. Journal of Hand Surgery, 28(2), 172-176.
- Dias, J. J., Dhukaram, V., & Kumar, P. (2007). The natural history of untreated dorsal wrist ganglia and patient reported outcome 6 years after intervention. Journal of Hand Surgery (European Volume), 32(5), 502-508.
- Head, L., Gencarelli, J. R., Allen, M., & Boyd, K. U. (2015). Wrist ganglion treatment: systematic review and meta-analysis. The Journal of hand surgery, 40(3), 546-553.
- Khan, P. S., & Hayat, H. (2011). Surgical excision versus aspiration combined with intralesional triamcinolone acetonide injection plus wrist immobilization therapy in the treatment of dorsal wrist ganglion; a randomized controlled trial. Journal of hand and microsurgery, 3(02), 55-57.
- Limpaphayom, N., & Wilairatana, V. (2004). Randomized controlled trial between surgery and aspiration combined with methylprednisolone acetate injection plus wrist immobilization in the treatment of dorsal carpal ganglion. J Med Assoc Thai, 87(12), 1513-1517.
- Maaz-Ul-Hassan, Ali, M. T., & Nadeem, A. (2017). Comparison of Surgical Excision versus Aspiration and Injection of Steroid of Wrist Ganglion. Pakistan Journal of Medical & Health Sciences, 11(4), 1412-1414.
- Rollins, K. E., Ollivere, B. J., & Johnston, P. (2013). Predicting successful outcomes of wrist and finger ganglia. Hand Surgery, 18(01), 41-44.
- Wright, T. W., Cooney, W. P., & Ilstrup, D. M. (1994). Anterior wrist ganglion. The Journal of hand surgery, 19(6), 954-958.
- Zinger, G., Michailevich, M., Bregman, A., Yudkevich, G., Steinberg, K., & Peyser, A. (2020). Wrist ganglia in children: nonsurgical versus surgical treatment. The Journal of Hand Surgery, 45(6), 551-e1.
Evidence table for systematic review of RCTs and observational studies (intervention studies)
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Head (2015) |
SR and meta-analysis of RCT’s and cohort studies Literature search up to December 2013 (from 1990)
Study design:
Setting and Country: A: SKIMS Medical College Hospital, Bemina Srinagar Kashmir, India B. Department of Orthopedic, King Chulalongkorn Memorial hospital, Thai Red Cross society, Thailand. C, D: From the Faculty of Medicine, University of Ottawa; and the Division of Plastic Surgery, Ottawa Hospital, Ottawa, Ontario, Canada. E. Department of Trauma and Orthopaedics, Addenbrookes Hospital Hills Road, Cambridge, CB2 0QQ, United Kingdom F.
Source of funding and conflicts of interest: No benefits in any form have been received or will be received related directly or indirectly to the subject of this article. |
Inclusion criteria SR:
Exclusion criteria SR:
All 6 included studies met our PICO and were included in the analyses.
Important patient characteristics at baseline:
N:
Mean age (range or SE):
C: 31 (17-45) B I: 29.9 (9.8) C: 32.0 (13.1)
C: 48.2 (2.5)
C: 37.7 (1.6)
Sex:
C: 3 M/ 14 F
C: 2 M / 11 F
C: 22M / 35 F
C: 25 M / 75 F
Groups comparable at baseline? Most studies are comparable at baseline. However, Rollins also included finger ganglia and reported baseline characteristics for the whole group. In the results, there has been stratified on wrist. Rollins and Wright included patients from of respectively 5 and 13 years old. |
Describe intervention:
A, B, C, D, E, F. Open surgical or arthroscopic excision
|
Describe control: A, B, C, D, E, F. Aspiration with or without corticosteroid
|
End-point of follow-up:
For how many participants were no complete outcome data available? (intervention/control)
A, C, D, E, F : None. B: 4
|
Outcome measure: recurrence
C: 7/18 (39%)
C: 8/13 (62%)
C: 18/38 (47%)
C: 34/51 (67%)
C: 20/24 (83%)
For the RCT’s (A &B): Pooled effect relative risk ratio (random effects model): RR 0.24 (95% CI 0.08 to 0.71) favoring excision. Heterogeneity (I2): 0% For the cohort studies (C, D, E, F): Pooled effect relative risk ratio (random effects model): RR 0.42 (95% CI 0.21 to 0.85) favoring excision. Heterogeneity (I2): 87%
Outcome measure: pain A, B, E, F: Not reported
C: 7/39 (18%)
Outcome measure: complications
C: 0/18 (0%)
C: 0/13 (0%)
C: 2/38 (5%)
C: 2/78 (3%)
Outcome measure: Patient Evaluation Measure (PEM) hand disability score, mean (SE) A, B, E, F: not reported. C: I: 14.1 (2.5) C: 17.1 (4.3) D: I: 19.2 (2.1) Outcome measure: Satisfaction (PEM), %
Outcome measure: time off work (days), mean (SE) A, B, E, F: not reported.
C: I: 14.1 (1.96)
|
Conclusions:
|
Evidence table for intervention studies (randomized controlled trials and non-randomized observational studies [cohort studies, case-control studies, case series])
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Zinger (2020) |
Type of study: Retrospective cohort study
Setting and country: A clinic and a hospital in Israel
Funding and conflicts of interest: None |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: 40 Control: 50
Important prognostic factors2: age ± SD: I: 13 (5-17.5) C: 12 (5-17.5)
Sex: I: 11 M (27%) / 29 F (73%) C: 16 M (32%)/ 34 F (64%)
Groups comparable at baseline?
Groups seem comparable based on the reported characteristics. |
Describe intervention:
Surgical excision |
Describe control (treatment/procedure/test):
Observation alone |
Length of follow-up: I: 70 months (range: 12-282) (6 years) C: 44 months (range: 12-84) (3,5 years)
Loss-to-follow-up: Intervention group: 6 (13%) patients Reasons: could not be contacted or were not willing to participate
Control group: 17 (25%) patients Reasons: 15 could not be contacted and 2 were not willing to participate
|
Outcome measures and effect size (include 95%CI and p-value if available):
Outcome measure: recurrence (surgical)/ persistence (nonsurgical):
Intervention: 6/40 (15%)
Control: 26/50 (52%)
Outcome measure: function and pain (evaluated using QuickDASH scores, mean/median and range):
I: 12/0 (0-70) C: 15/6.8 (0-73)
Outcome measure: surgical complications
I: 12/40 (30%) C: - |
Conclusion: Although surgery was more successful in all groups, there was a 30% rate of minor surgical complications. Therefore, considering both the literature review and our experience, we recommend observation for at least 18 months, because 94% of cysts that ultimately resolved did so within that interval. If the cyst persists and is symptomatic, surgical excision is a safe and reasonable option. Patients and their parents should be aware of the 15% recurrence rate.
|
|
Ahmad Shah (2019)
|
Type of study: cohort study
Setting and country: From Aug 2016 to Aug 2018 in Department of General Surgery, Government Medical College Srinagar, India
Conflict of interest: none
|
Inclusion criteria: Dorsal wrist ganglion of at least 1 cm in size, older than 15 years, history of trauma and previous treatment and willingness for follow-up
Exclusion criteria: No additional exclusion criteria
N total at baseline: I: 68 C: 18
Important prognostic factors2: Age ± SD: Only reported for the whole group: 24.8±7.69 (range: 16-48)
Sex: I: 13 M (19%)/ 55 F (81%) C: 5 M (28%)/ 13 F (72%)
Groups comparable at baseline?
Not enough information to compare the two groups. |
Describe intervention: Aspiration followed by intralesional steroid (triamcinolone acetate) injection |
Describe control: Surgical excision of the dorsal wrist ganglion, including the entire cyst complex, pedicle, and a cuff of adjacent joint capsule. |
Length of follow-up: 12 months after treatment
Loss to follow-up: None |
Outcome measures and effect size (include 95%CI and p-value if available):
Outcome measure: recurrence
I: 9/68 (13%) C: 3/18 (17%)
|
Conclusion: In our study, we found 13.23% recurrence with aspiration followed by steroid injection and 16.66% recurrence was noted after surgical excision. The maximum follow-up time was 1 year. Janson reported that most of the ganglia recured in first 6 months period. So aspiration followed by intralesional steroid (triamcinolone acetate) injection was shown to be a better mode of management than surgical excision. |
|
Maaz-Ul-Hassan (2017) |
Type of study: RCT
Setting and country: from 1st November 2016 to 30th June 2017 in Shalamar Medical & Dental College Hospital Lahore and Shahida Islam Medical Complex Lodhran, Pakistan
Funding and conflicts of interest: Not reported |
Inclusion criteria: All patients with ganglion at wrist between 20 to 60 years of age of either gender were included
Exclusion criteria: No additional exclusion criteria
N total at baseline: I: 50 C: 50
Important prognostic factors2: Age: I: 48.47±5.14 C: 46.23±6.78
Sex: I: 22 M (44%)/ 28 F (56%) C: 20 M (40%)/ 30 F (60%)
Groups comparable at baseline?
Groups seem comparable based on the reported characteristics. |
Describe intervention: Surgical excision |
Describe control: Aspiration with steroid injection |
Length of follow-up: 3 months
Loss to follow-up: None
|
Outcome measures and effect size (include 95%CI and p-value if available):
Outcome measure: recurrence I: 6/50 (12%) C: 29/50 (58%) |
Conclusion: The successful rate of excision of a ganglion is significantly higher in surgical excision as compared to those undergoing aspiration and injection of steroid.
|
Risk of bias tables
Risk of bias table for systematic reviews
|
Study
First author, year |
Appropriate and clearly focused question?1
Yes/no/unclear |
Comprehensive and systematic literature search?2
Yes/no/unclear |
Description of included and excluded studies?3
Yes/no/unclear |
Description of relevant characteristics of included studies?4
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?5
Yes/no/unclear/not applicable |
Assessment of scientific quality of included studies?6
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?7 Yes/no/unclear |
Potential risk of publication bias taken into account?8 Yes/no/unclear |
Potential conflicts of interest reported?9 Yes/no/unclear |
|
Head, 2015 |
Yes
“The objectives of this study were to review recurrence and complication rates reported for modalities used to treat adult wrist ganglions and to generate a meta-analysis comparing the 2 most common options: open surgical excision and aspiration.” |
Yes
“To identify relevant publications, we searched MEDLINE and EMBASE, including studies from 1990 to December 2013. Only studies published since 1990 were included to ensure that findings reflected contemporary clinical practices, because recent studies have been unable to reproduce the low recurrence rates reported previously.” |
Yes |
Yes |
Unclear |
Yes
“Methodological quality of cohort studies was assessed using the Newcastle Ottawa Scale (NOS) (maximum score of 9).” |
Yes |
Yes |
Unclear |
Risk of bias table for intervention studies (randomized controlled trials; based on Cochrane risk of bias tool and suggestions by the CLARITY Group at McMaster University)
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Maaz-Ul-Hassan (2017) |
Unknown
Reason: not reported |
Unknown
Reason: not reported |
Unknown
Reason: not reported |
Definitely yes
Reason: no loss to follow-up |
Probably yes
Reason: there was just one outcome, however, complications such as an infection should have been reported because of the consequences for the treatment |
Probably no
Reason:
|
HIGH
|
Risk of bias table for interventions studies (cohort studies based on risk of bias tool by the CLARITY Group at McMaster University)
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors?
|
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables? |
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed?
|
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Low, Some concerns, High |
|
|
Zinger (2020) |
Definitely yes
Reason: Participants were selected from a registry
|
Definitely yes
Reason: Secure record from registry
|
Definitely yes
Reason: the outcome of interest is recurrence or persistence, which can only be present after a treatment or follow-up time |
Definitely yes
Reason: Based on chart review and recent phone interview |
Definitely no
Reason: No adjustment was done |
Definitely yes
Reason: Based on chart review and recent phone interview |
Probably no
Reason: Because this was a retrospective study, people were not lost to follow-up during the study. However, only 75% of patients without treatment (only observation) were included in the study (compared to 87% in the surgical group). Moreover, the follow-up time in the surgical group was longer (18 months) compared to the non-surgical group (14 months) |
Definitely yes
Reason: Most or all relevant co-interventions that might influence the outcome of interest are documented to be similar in the exposed and unexposed
|
Some concerns
|
|
Ahmad Shah (2019)
|
Definitely yes
Reason: Participants were selected from a registry
|
Probably yes
Reason: Diagnosis of ganglion was based on history and clinical examination. In some patients, radiological investigations like X-ray and ultrasonography were done to rule out other lesions.) |
Definitely yes
Reason: the outcome of interest is recurrence, which can only be present after a treatment or follow-up time. |
Probably yes
Reason: Based on chart review |
Definitely no
Reason: few confounding factors reported per group, no adjustment for confounding factors performed. |
Probably yes
Reason: Record linkage |
Definitely yes
Reason: There was no loss to follow up and the follow-up time of 1 year seems adequate |
Probably yes
Reason: It is not reported whether certain patients received co-intervention between baseline and 12 months follow-up |
Some concerns |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Abe, Y., Watson, H. K., & Renaud, S. (2004). Flexor tendon sheath ganglion: analysis of 128 cases. Hand Surgery, 9(01), 1-4. |
Within the search date of Head (2015) |
|
Ahsan, Z. S., & Yao, J. (2014). Arthroscopic dorsal wrist ganglion excision with color-aided visualization of the stalk: minimum 1-year follow-up. Hand, 9(2), 205-208. |
Not matching PICO (observational study on arthroscopic excision with color-aided technique, but no comparator) |
|
Alturki, M. A., Al Luhayb, W. A., Alshuhayb, A. H., Alahmad, H. M., Alfarhan, S. H., Aldhufairi, A. M., ... & Almatari, M. A. (2022). An overview on evaluation of wrist ganglion cysts diagnostic and management approach. Int j pharm res allied sci [Internet], 11(1), 11-6. |
Wrong study design (narrative review) |
|
Aslani, H., Najafi, A., & Zaaferani, Z. (2012). Prospective outcomes of arthroscopic treatment of dorsal wrist ganglia. Orthopedics, 35(3), e365-e370. |
Within the search date of Head (2015) |
|
Balazs, G. C., Dworak, T. C., Tropf, J., Nanos III, G. P., & Tintle, S. M. (2016). Incidence and risk factors for volar wrist ganglia in the US military and civilian populations. The Journal of Hand Surgery, 41(11), 1064-1070. |
Wrong study desgin (etiological study) |
|
d'Ailly, P. N., Koopman, J. E., Selles, C. A., Rahimtoola, Z. O., & Schep, N. W. (2020). Patient-related outcomes of arthroscopic resection of ganglion cysts of the wrist. Journal of Wrist Surgery, 10(01), 031-035. |
Not matching PICO (observational study on arthroscopic resection, but no comparator) |
|
Dias, J. J., Dhukaram, V., & Kumar, P. (2007). The natural history of untreated dorsal wrist ganglia and patient reported outcome 6 years after intervention. Journal of Hand Surgery (European Volume), 32(5), 502-508. |
Included in Head (2015) |
|
Dias, J., & Buch, K. (2003). Palmar wrist ganglion: does intervention improve outcome a prospective study of the natural history and patient-reported treatment outcomes. Journal of Hand Surgery, 28(2), 172-176. |
Included in Head (2015) |
|
Farzam, R., Deilami, M., Jalili, S., & Kamali, K. (2021). Comparison of anesthesia results between Wide Awake Local Anesthesia no Tourniquet (WALANT) and Forearm Tourniquet Bier Block in hand surgeries: A randomized clinical trial. Archives of Bone and Joint Surgery, 9(1), 116. |
Not matching PICO (comparison of two types of anesthesia in patients undergoing hand surgery) |
|
Hansen, T., Patrick, N. C., Bernstein, D., Fear, K., & Hammert, W. C. (2021). PROMIS Measures in Patients with Ganglion Cysts: Who Chooses Surgical Excision Over Non-Operative Management?. The Journal of Hand Surgery (Asian-Pacific Volume), 26(04), 519-524. |
No follow up data |
|
Khan, P. S., & Hayat, H. (2011). Surgical excision versus aspiration combined with intralesional triamcinolone acetonide injection plus wrist immobilization therapy in the treatment of dorsal wrist ganglion; a randomized controlled trial. Journal of hand and microsurgery, 3(02), 55-57. |
Included in Head (2015) |
|
Kumar, K., & Sharma, D. (2016). Comparison of efficacy of methyl prednisolone and triamcinolone in wrist ganglion using double dart technique and its application in an Indian population. Current Orthopaedic Practice, 27(6), 614-617. |
Does not match PICO (comparison of aspiration with two types of injection (double dart technique)) |
|
Latif, A., Ansar, A., & Butt, M. Q. (2014). Treatment of ganglions; a five year experience. J Pak Med Assoc, 64(11), 1278-81. |
Not matching PICO (the authors call it an RCT, but no randomization/blinding/allocation took place. Studies in patients with ganglia in the wrist, ancle, or knee) |
|
Limpaphayom, N., & Wilairatana, V. (2004). Randomized controlled trial between surgery and aspiration combined with methylprednisolone acetate injection plus wrist immobilization in the treatment of dorsal carpal ganglion. J Med Assoc Thai, 87(12), 1513-7. |
Included in Head (2015) |
|
Paramhans, D., Nayak, D., Mathur, R. K., & Kushwah, K. (2010). Double dart technique of instillation of triamcinolone in ganglion over the wrist. Journal of Cutaneous and Aesthetic Surgery, 3(1), 29. |
Within the search date of Head (2015) |
|
Tadjerbashi, K., Rosales, R. S., & Atroshi, I. (2014). Intervention randomized controlled trials involving wrist and shoulder arthroscopy: a systematic review. BMC Musculoskeletal Disorders, 15(1), 1-10. |
Not matching PICO (systematic review on wrist and shoulder atrhoscopy. Studies in patients with ganglion compared open excision with arthroscopic excision) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 22-02-2024
Beoordeeld op geldigheid : 20-02-2024
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met ganglion.
Werkgroep
- Prof. dr. E. (Erik) Heineman, hoogleraar chirurgie, gepensioneerd chirurg UMC Groningen, NVvH (voorzitter)
- Drs. M. (Martijn) ten Berge, chirurg, HagaZiekenhuis, NVvH
- Dr. A. (Annechien) Beumer, orthopedisch en hand chirurg, Amphia ziekenhuis en Amsterdam UMC, NOV en Nederlandse Vereniging voor Handchirurgie
- Drs. H.L. (Luitzen) de Boer, plastisch chirurg, Catharina ziekenhuis en Xpert Clinics, NVPC en Nederlandse Vereniging voor Handchirurgie
- Drs. J. (Joost) van Dijsseldonk, orthopedisch chirurg, Maxima Medisch Centrum Velthoven, NOV
- C.E.J. (Chantal) Essink, hand- en fysiotherapeut, Welzorg, NVHT, Ergotherapie Nederland, KNGF
- Dr. A.P.A. (Alexander) Greeven, chirurg, HagaZiekenhuis en Juliana kinderziekenhuis, NVvH en Nederlandse Vereniging voor Handchirurgie
- Dr. A.C. (Aimee) Kok-Pigge, huisarts, wetenschappelijk medewerker NHG, NHG
- Drs. B. (Bas) van Ooij, zelfstandig bedrijfsarts, VisieCare Arbo & HR, NVAB.
Meelezers
- I. (Ilse) van Ee, adviseur patiëntenbelang, Patiëntenfederatie Nederland
- M. (Maike) Broere, adviseur patiëntenbelang, Patiëntenfederatie Nederland
Met ondersteuning van
- dr. A. (Anja) van der Hout, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Heineman |
- Hoogleraar Chirurgie, gepensioneerd, - 0-aanstelling het UMCG/RUG. Begeleiding promovendi (3) (tot mei 2023) |
- Vrijwilliger bij netwerk organisatie 'Gezond en Gelukkig Den Haag'. |
Geen |
Geen restricties |
|
De Boer |
- Plastisch chirurg Catherina ziekenhuis en Xpert Clinics |
Lid beroepsgenoot tuchtrecht voor de gezondheidszorg |
Vrijgevestigd specialist waarbij ik handchirurg ben zowel in het Catherina ziekenhuis als de Xpert Clinics |
Geen restricties |
|
Greeven
|
- Chirurg, Hagaziekenhuis & Juliana Kinderziekenhuis |
Opleider Heelkunde, Hagaziekenhuis
|
Geen |
Geen restricties |
|
Kok-Pigge
|
- Wetenschappelijk medewerker, Richtlijnontwikkeling en Wetenschap, NHG (0,2 fte; - Huisarts in opleiding (tot sept 2023) |
Geen |
Overeenstemming/discrepanties met nieuwe NHG Standaard Hand-en Polsklachten.
|
Geen restricties |
|
Beumer
|
- 80 % Orthopedisch en Handchirurg, Vakgroep Orthopedie Amphia Ziekenhuis |
- Bestuurslid Handpols Werkgroep Nederlandse Orthopeden vereniging (NOV) (niet meer bij einde richtlijn) - Voorzitter richtlijn werkgroep generieke module over arbeidsparticipatie |
Geen |
Geen restricties |
|
Essink
|
- Hand- en fysiotherapeut bij Xpert Handtherapie (tot okt 2023) - Paramedisch adviseur bij Welzorg BV (per okt 2023)
|
Geen
|
Geen |
Geen restricties |
|
Van Ooij
|
- Zelfstandig bedrijfsarts, in samenwerking met VisieCare Arbo & HR - AIOS bedrijfsgeneeskunde bij Arbodienst (tot sept 2022) |
Geen |
Geen |
Geen restricties |
|
Van Dijsseldonk
|
- Orthopedisch Chirurg |
ATLS, stichting ALSG |
Geen |
Geen restricties |
|
Ten Berge
|
- Traumachirurg, Hagaziekenhuis, Den Haag |
Geen |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van Patiëntenfederatie Nederland voor de invitational conference. Patiëntenfederatie Nederland heeft ook meegelezen met de richtlijn. Het verslag van de invitational conference (zie bijlage) is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Wkkgz & Kwalitatieve raming van mogelijke substantiële financiële gevolgen
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijn is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling zijn richtlijnmodules op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
|
Module |
Uitkomst raming |
Toelichting |
|
Module Diagnostiek |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Niet-chirurgische behandeling |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Chirurgische behandeling |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Postoperatieve nabehandeling |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module secundaire preventie en werk |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met polsganglion. Tevens zijn er knelpunten aangedragen door de NVvH, NOV, NHG, Nederlandse Vereniging voor Handchirurgie, NVAB, KNGF, Nederlandse Vereniging voor Handtherapie, Adviesraad Handtherapie, Ergotherapie Nederland en Patiëntenfederatie Nederland via een invitational conference op 14-09-2021. Een verslag hiervan is opgenomen in de bijlage. Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen van de betreffende modules.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Literature search strategy
Zoekverantwoording
Algemene informatie
|
Richtlijn: Ganglion |
|
|
Uitgangsvraag/modules: Wat is de plaats van chirurgische behandeling bij patiënten met ganglion? |
|
|
Database(s): Ovid/Medline, Embase.com |
Datum: 8-6-2022 |
|
Periode: 2000 - heden |
Talen: Engels, Nederlands |
|
Literatuurspecialist: Miriam van der Maten |
|
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: à Voor deze vraag is gezocht op de elementen:
à De search van de eerder ontwikkelde module over dit onderwerp (niet gepubliceerd - richtlijn Algemene chirurgie) was niet toereikend voor deze search. Er zijn wel delen van gebruikt (maar aangepast) om deze search mee op te stellen
à Het zoekblok voor hand/pols ganglion is iets aangepast t.o.v. de andere searches voor deze richtlijn omdat er bij de resultaten in eerste instantie veel ruis zat over andere type ganglions.
à De sleutelartikelen worden gevonden met de zoekopdracht. |
|
|
Te gebruiken voor richtlijnen tekst: In de databases Embase.com en Ovid/Medline is op 8 juni 2022 met relevante zoektermen gezocht naar systematische reviews, RCT en observationele studies over chirurgische behandeling bij patiënten met ganglion. De literatuurzoekactie leverde 250 unieke treffers op. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
15 |
9 |
14 |
|
RCT |
16 |
8 |
19 |
|
Observationele studies |
156 |
143 |
217 |
|
Totaal |
187 |
160 |
250 |
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#13 |
#10 OR #11 OR #12 |
187 |
|
#12 |
#6 AND #9 NOT (#10 OR #11) |
156 |
|
#11 |
#6 AND #8 NOT #10 |
16 |
|
#10 |
#6 AND #7 |
15 |
|
#9 |
'major clinical study'/de OR 'clinical study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) OR 'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
14895009 |
|
#8 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
1839814 |
|
#7 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
733409 |
|
#6 |
#4 AND #5 AND ([english]/lim OR [dutch]/lim) AND [2000-2022]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
391 |
|
#5 |
'surgery'/exp OR 'surgery'/lnk OR surgical:ti,ab,kw OR surger*:ti,ab,kw OR operation*:ti,ab,kw OR operative:ti,ab,kw OR 'arthroscopy'/exp OR arthroscop*:ti,ab,kw OR 'excision'/exp OR excision:ti,ab,kw |
8113010 |
|
#4 |
'wrist ganglion'/exp OR ('ganglion cyst'/exp/mj AND ('arm'/exp/mj OR 'upper extremit*':ti,ab,kw OR upperextremit*:ti,ab,kw OR 'upper-limb*':ti,ab,kw OR upperlimb*:ti,ab,kw OR hand*:ti,ab,kw OR wrist*:ti,ab,kw OR finger*:ti,ab,kw OR thumb*:ti,ab,kw OR metacarp*:ti,ab,kw OR interphalang*:ti,ab,kw OR phalang*:ti,ab,kw OR carpus:ti,ab,kw OR carpal:ti,ab,kw)) OR 'mucoid cyst*':ti,ab,kw OR (((ganglion* OR ganglia) NEAR/3 (hand* OR wrist*)):ti,ab,kw) |
856 |
Ovid/Medline
|
# |
Searches |
Results |
|
12 |
9 or 10 or 11 |
160 |
|
11 |
(7 and 8) not (9 or 10) |
143 |
|
10 |
(6 and 8) not 9 |
8 |
|
9 |
5 and 8 |
9 |
|
8 |
limit 4 to ((english language or dutch) and yr="2000 -Current") |
355 |
|
7 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ or Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
6864017 |
|
6 |
(exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf.) not (animals/ not humans/) |
1381879 |
|
5 |
(meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf.) not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) |
569795 |
|
4 |
2 and 3 |
510 |
|
3 |
exp Surgical Procedures, Operative/ or exp Specialties, Surgical/ or su.fs. or (surgical or surger* or operation* or operative).ti,ab,kf. or exp Arthroscopy/ or arthroscop*.ti,ab,kf. or excision.ti,ab,kf. |
5232166 |
|
2 |
(exp Ganglion Cysts/ and (exp Wrist/ or exp Hand Joints/ or exp Upper Extremity/ or 'upper extremit*'.ti,ab,kf. or upperextremit*.ti,ab,kf. or 'upper-limb*'.ti,ab,kf. or upperlimb*.ti,ab,kf. or hand*.ti,ab,kf. or wrist*.ti,ab,kf. or finger*.ti,ab,kf. or thumb*.ti,ab,kf. or metacarp*.ti,ab,kf. or interphalang*.ti,ab,kf. or phalang*.ti,ab,kf. or carpus.ti,ab,kf. or carpal.ti,ab,kf.)) or 'mucoid cyst*'.ti,ab,kf. or ((ganglion* or ganglia) adj3 (hand* or wrist*)).ti,ab,kf. |
744 |