Niet-chirurgische behandeling
Uitgangsvraag
Wat is de optimale niet-operatieve behandeling van een ganglion van de pols?
De uitgangsvraag omvat de volgende deelvragen:
- Wat is de waarde van een expectatief beleid ten opzichte van handtherapie bij patiënten met een polsganglion?
- Wat is de waarde van een expectatief beleid ten opzichte van aspiratie (met of zonder infiltratie) bij patiënten met een polsganglion?
- Wat is de waarde van handtherapie ten opzichte van aspiratie (met of zonder infiltratie) bij patiënten met een polsganglion?
Aanbeveling
Wacht af bij kort bestaande, milde tot matige klachten van een polsganglion. Overweeg een periode van minimaal 12 weken af te wachten, tenzij de klachten significant toenemen.
Overweeg handtherapie alleen bij een symptomatisch polsganglion, met name als er sprake is van functionele klachten, relevante comorbiditeit zoals laxiteit of handartrose, sterk vermoeden op onderhoudende (werk- of houdingsafhankelijke) factoren, of bij recidieven ondanks een andere vorm van behandeling.
Doe geen aspiratie (met of zonder achterlaten van een werkzame stof) bij een polsganglion. Is er sprake van significante klachten met een behandelwens én zwaarwegende contra-indicaties voor een operatieve behandeling of een sterke wens van de patiënt voor niet-operatieve behandeling én een duidelijke behoefte aan snelle (tijdelijke) klachtenverlichting, overweeg dan het bespreken van een aspiratie. Benoem hierbij de hoge recidiefkans.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is literatuuronderzoek verricht naar de meest optimale behandeling van een polsganglion, waarbij de opties waren: expectatief beleid (‘wait and see'), handtherapie en aspiratie, al dan niet met infiltratie van een medicament. Pijnklachten en handfunctie werden gedefinieerd als cruciale uitkomstmaten en recidief, ernst van de symptomen, complicaties, het aantal dagen wanneer iemand weer in staat is om te werken en hand esthetiek werden als belangrijke uitkomstmaten gedefinieerd.
Op basis van het literatuuronderzoek kan worden geconcludeerd dat de literatuur zeer onzeker is over het effect van een expectatief beleid (in de studies betekende dit geruststellen) vergeleken met aspiratie op pijnklachten na de behandeling, de handfunctie, recidieven van een polsganglion, de ernst van de symptomen, de complicaties van een behandeling en het aantal dagen wanneer iemand weer in staat is om te werken na de behandeling van een polsganglion. De bewijskracht hiervoor is zeer laag. De redenen voor de zeer lage bewijskracht zijn observationele designs van de geïncludeerde studies, alsmede de kleine aantallen patiënten en brede betrouwbaarheidsintervallen per uitkomstmaat.
Er zijn geen studies gevonden die expectatief beleid hebben vergeleken met handtherapie of die handtherapie hebben vergeleken met aspiratie.
De afweging van de voor- en nadelen van een interventie dienen hierbij in het licht van de aard en ernst van de klachten te worden gezien. Voor een patiënt bij wie functionele klachten op voorgrond staan, zullen de voor- en nadelen anders wegen dan voor de patiënt die zuiver cosmetische klachten ervaart.
Expectatief beleid
Indien er gekozen wordt voor geen interventie, is dit in vele gevallen te verdedigen met de kennis uit de literatuur, waarbij gezien wordt dat er in het natuurlijke beloop ook spontane genezing kan optreden bij ganglia van de pols. Belangrijk wordt dan ook gevonden dat patiënten hier voorlichting over ontvangen, zodat het begrip voor de keuze van geen actieve behandeling aanwezig is. De werkgroepleden geven aan dat er overwogen dient te worden om minimaal 12 weken af te wachten. Daarbij wordt wel van belang geacht dat de patiënt gedurende de periode van een expectatief beleid geen verergering van symptomen ervaart. In het geval hier wel sprake van is, is het van belang dat de patiënt weet wat de volgende stappen zijn die doorlopen kunnen worden. Bij het maken van de keuze voor een expectatief beleid dient de duur en de ernst van de klacht behorende bij het polsganglion afgewogen te worden. Met name patiënten met milde tot geen en kortdurende klachten zijn geschikte kandidaten hiervoor. Ook bij patiënten met zuiver cosmetische klachten is een expectatief beleid een passende optie.
Aspiratie
Ondanks het gebrek aan bewijs worden symptomatische ganglia nog frequent geaspireerd. Op basis van het huidige bewijs lijkt een aspiratie niet effectiever dan een expectatief beleid. Ook is er geen bewijs dat het achterlaten van een werkzame stof de kans op recidief verlaagd (Dias, 2003; Dias, 2007). Wel worden bijwerkingen beschreven in de geïncludeerde studies, gerelateerd aan de aspiratie of injectie, met name pijnklachten, huidafwijkingen (bij infiltratie met corticosteroïden) en een kleine kans op infecties (Dias, 2003; Dias, 2007; Head, 2015).
Handtherapie
Handtherapie wordt gegeven door een ergotherapeut of fysiotherapeut met kennis van handpathologie, eventueel CHT-NL gecertificeerd. Handtherapie richt zich in het algemeen op de bovenste extremiteit, in het specifiek de hand en pols. Bij handtherapie kan gebruik worden gemaakt van oefen- en spalktherapie en adviezen omtrent hulpmiddelen, gedrag en belasting.
Andere (aanvullende) behandelvormen zoals manipulaties, dry needling of shockwave vallen hier niet onder.
Momenteel is er ook geen bewijs voor de effectiviteit van handtherapie. De voor- en nadelen van handtherapie in vergelijking met andere behandelopties (inclusief expectatief beleid) zijn daarom niet met bewijslast te onderbouwen.
Verwacht wordt dat de begeleiding voor een deel van de patiënten als voordeel gezien kan worden. Bespreek met de patiënt wat de behandelopties zijn en of de patiënt hier voordeel voor hem/haar in ziet. Naast de focus op pijndemping, kan de handtherapeut aandacht besteden aan het verbeteren van de belastbaarheid van de hand, en de patiënt inzage bieden in de balans tussen belasting en belastbaarheid. De verwachte bijwerkingen en complicaties van handtherapie zijn vergelijkbaar met een expectatief beleid en beperkter dan bij een aspiratie of operatie worden beschreven.
De nadelen van handtherapie zijn met name gericht op tijds- en kostenaspecten. De investering van tijd komt voornamelijk van de kant van de patiënt die bezig gaat met huiswerkoefeningen en aanwezig is tijdens de behandelsessies. De kosten kunnen voor zowel de patiënt als de zorgverzekeraar zijn. Informeer de patiënt over de opties en de daarbij behorende kosten. Bovendien is het van belang dat er geen bewijs gevonden dat handtherapie een effect heeft op het volume van het polsganglion.
De werkgroep is van mening dat handtherapie vooral overwogen kan worden bij de groep patiënten die pijn- en/of functiebeperkingen ervaren, welke bijvoorbeeld resulteren in dat de patiënt werk, schooltaken of hobby’s niet of in mindere mate kan uitvoeren. Dergelijke behandeldoelstellingen zijn namelijk goed voor de therapeut meetbaar. Er is geen behandelindicatie als er alleen sprake is van een esthetische hulpvraag.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Patiënten die zorg zoeken bij polsganglion klachten presenteren zich met verschillende behandeldoelstellingen. Naast pijn zijn esthetiek, functiebeperking of mobiliteitsbeperking problemen welke ervaren worden. Door de aanwezigheid van deze problemen kunnen patiënten beperkt worden bij het uitvoeren van hun dagelijkse activiteiten, hobby’s en werkzaamheden. De zwaarte welke door de patiënt aan bovenstaande problemen wordt gewogen is verschillend. Daarom is het van belang dat alle behandelopties en de bijbehorende voor- en nadelen worden besproken, wat het mogelijk maakt de best passende behandeling te kiezen.
Expectatief beleid
Voordelen van een expectatief beleid zijn dat hieraan geen duidelijke complicaties of kosten verbonden zijn. Er wordt ook niets verwacht van de patiënt in de thuissituatie. Voor sommige patiënten met een symptomatisch polsganglion kan afwachten echter onacceptabel zijn, vanwege de ernst van de klachten, hinderlijke lokalisatie van het polsganglion of het reeds hebben van een recidief. Het verkrijgen van snelle verbetering van de klachten kan hierin meewegen. Voor andere patiënten zullen juist de mogelijke risico’s of nadelen van een interventie niet opwegen tegen de voordelen.
Aspiratie
Wanneer er voor aspiratie gekozen wordt, kan directe resolutie voor de patiënt erg prettig zijn. Wel kunnen aspiratiebehandelingen als pijnlijk worden ervaren en wordt er door patiënten met regelmaat angst voor naalden beschreven. De grote kans op een recidief van het polsganglion is hierbij een negatief punt.
Handtherapie
Bij handtherapeutische behandeling kan aandacht voor de patiënt, verdere uitleg en inzage in klachten als een positief aspect worden gezien. Bovendien kunnen eventueel bijkomstige klachten zoals onderliggende artrose of instabiliteit mede worden behandeld, wat ook als positief kan worden ervaren. Echter kan de patiënt ook moeite hebben met de therapietrouwheid. Ook het investeren van tijd en eventueel geld kan als een nadeel worden ervaren. De eventuele kosten van handtherapie kunnen voor sommige patiënten een bezwaar vormen om deze optie te overwegen (zie ook hieronder bij ‘Kosten (middelenbeslag)’.
Kosten (middelenbeslag)
Er zijn geen kosten verbonden aan een expectatief beleid. De directe kosten van aspiratie zijn relatief laag. De kosten van handtherapie zijn relatief gezien hoger. Daarnaast kan er een eigen bijdrage voor de patiënt zijn. Bij functiebeperkingen welke leiden tot problemen in het arbeidsproces zullen deze kosten beter te verdedigen zijn, dan bij esthetische argumenten.
Hand-ergotherapie is (in 2023) opgenomen in de basisverzekering en wordt volledig vergoed tot een maximum van 10 uren per kalenderjaar per verzekerde. Wel gelden de kosten van het vastgestelde eigen risico dat jaarlijks door de zorgverzekeraar in rekening wordt gebracht. Handtherapie door een fysiotherapeut wordt (in 2023) niet vergoed vanuit de basisverzekering.
Aanvaardbaarheid, haalbaarheid en implementatie
De werkgroep schat in dat alle behandelopties aanvaardbaar zijn voor de patiënten en zorgverleners. Daarnaast zijn de opties reeds geïmplementeerd en beschikbaar in de praktijk waardoor deze haalbaar zijn in de uitvoering.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Er is bewijs van zeer lage kwaliteit dat een expectatief beleid en een aspiratie niet verschillen op het gebied van pijn, handfunctie en kans op recidief. Een aspiratie geeft echter wel kans op bijwerkingen en complicaties, zoals pijnklachten, huidafwijkingen of in een klein geval kans op infectie. Het aspireren van een polsganglion wordt daarom afgeraden. Een uitzondering hierop zijn patiënten met ernstige klachten en een wens tot snelle resolutie van symptomen die een sterke voorkeur hebben voor een niet-operatieve behandeling of die een contra-indicatie hebben voor een operatie. Hierbij dient benoemt te worden dat ook na aspiratie een zeer grote kans op recidief van de polsganglion bestaat.
Er is momenteel geen onderzoek naar het effect van op de klachten van een symptomatische polsganglion handtherapie in vergelijking met een expectatief beleid of aspiratie. Het is de mening van de werkgroep dat er daarom geen plaats is voor het routinematig voorschrijven van handtherapie bij deze groep. Wel ziet de werkgroep een meerwaarde voor handtherapie in het geval van een symptomatisch ganglion van de pols waarbij pijn- of functiebeperking op de voorgrond staat, met name als er sprake is van relevante comorbiditeit, zoals laxiteit of handartrose, sterk vermoeden op onderhoudende (werk- of houdingsafhankelijke) factoren, of bij recidieven ondanks een andere vorm van behandeling. Bespreek de behandelopties en de voor- en nadelen met de patiënt en zoek samen naar de best passende behandeling.
Onderbouwing
Het is onduidelijk welke niet-operatieve behandeling het meest effectief is voor adolescente en volwassen patiënten met een symptomatisch ganglion van de pols, waardoor consensus over de optimale behandelstrategie ontbreekt. De conservatieve behandelopties zijn een expectatief beleid, handtherapie en aspiratie, al dan niet met infiltratie van een medicament. In Nederland zijn meest voorkomende middelen hierbij corticosteroïden, hyaluronzuur of glucose.
I) Expectative policy versus hand therapy
Hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics
|
- GRADE |
No evidence was found regarding the effect of an expectative policy on the outcome measures hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms or hand aesthetics when compared with hand therapy in patients with a wrist ganglion cyst.
Sources: - |
II) Expectative policy versus aspiration
1. Hand function/activities of daily life (critical)
|
Very low GRADE |
The evidence is very uncertain about the effect of an expectative policy on hand function/activities of daily life when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: Head (2015) (Dias, 2003) |
2. Pain (critical)
|
Very low GRADE |
The evidence is very uncertain about the effect of an expectative policy on pain when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: Head (2015) (Dias, 2003; Dias, 2007). |
3. Health-related QoL (important)
|
- GRADE |
No evidence was found regarding the effect of an expectative policy on health-related QoL when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: - |
4. Satisfaction with treatment results (important)
|
- GRADE |
No evidence was found regarding the effect of an expectative policy on satisfaction with treatment results when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: - |
5. Return to work/sport/hobby (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of an expectative policy on return to work/sport/hobby when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: Head (2015) (Dias, 2003; Dias, 2007). |
6. Complications (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of an expectative policy on complications of treatment when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: Head (2015) (Dias, 2003; Dias, 2007). |
7. Revision/recurrence (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of an expectative policy on revision/recurrence when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: Head (2015) (Dias, 2003; Dias, 2007). |
8. Range of motion (important)
|
- GRADE |
No evidence was found regarding the effect of an expectative policy on range of motion when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: - |
9. Grip and pinch strength (important)
|
- GRADE |
No evidence was found regarding the effect of an expectative policy on grip and pinch strength when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: - |
10. Severity of symptoms (important)
|
- GRADE |
No evidence was found regarding the effect of an expectative policy on symptom severity when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: - |
11. Hand aesthetics (important)
|
- GRADE |
No evidence was found regarding the effect of an expectative policy on hand aesthetics when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: - |
III) Hand therapy versus aspiration
Hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics
|
- GRADE |
No evidence was found regarding the effect of hand therapy on the outcome measures hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms or hand aesthetics when compared with aspiration (with or without infiltration) in patients with a wrist ganglion cyst.
Sources: - |
Description of studies
I) Expectative policy versus hand therapy
Not applicable.
II) Expectative policy versus aspiration
The systematic review of Head (2015) aimed to review the clinical outcomes of treatment for adult wrist ganglion cysts. Head (2015) included studies in which the study population included adult patients with wrist ganglion cysts, where recurrence or persistence of ganglion cysts was a measured outcome, and where patients had not previously received the treatment under investigation. Review articles, case studies, response letters, and conference proceedings were excluded. Studies in which a portion of the study population met inclusion criteria were included if the results of the subpopulation were presented separately. To identify relevant publications, Head (2015) searched MEDLINE and EMBASE, including studies from 1990 to December 2013. In total, six studies were included. Four of these studies did not meet our inclusion criteria and were excluded. Eventually two studies, involving 209 participants, were included for our guideline (Dias, 2003; Dias, 2007). Both studies had a cohort study design and compared no treatment with aspiration (with or without corticosteroid). In the study of Dias (2007), patients who had their ganglion aspirated had either aspiration alone or aspiration and injection of steroid (the number of patients with and without aspiration in combination with steroids were not reported). Dias (2003) included 77 participants with two- and five-years follow-up. Dias (2007) included 133 participants with a follow-up of more than five years. The methodological quality of the included (observational) studies in Head (2015) was evaluated with a modified Newcastle-Ottawa Scale by two independent authors. The reported outcomes in the study were recurrence, complications, return to work, hand function, and pain.
III) Hand therapy versus aspiration
Not applicable.
Results
I) Expectative policy versus hand therapy
Hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics
No studies were identified that compared expectative policy with hand therapy in patients with ganglion.
II) Expectative policy versus aspiration
1. Hand function/activities of daily life (critical)
One study reported the outcome hand function in systematic review of Head (2015) (Dias, 2003). Hand function was measured with the Patient Evaluation Measure (PEM) hand disability score. The PEM is a questionnaire, ranging from zero to 100 (in which a score of zero means a better state of the wrist and 100 a worse state of the wrist), that evaluates the process of treatment, the current state of the hand, and provides an overall assessment. Six questions are related to symptoms, three to the impact of the disorder on the patient, two to satisfaction and three to general disability and handicap.
Dias (2003) reported that the mean (SD) PEM hand disability score in the reassurance group was 15.5 (31.9), compared to 17.1 (38.0) in the aspiration group. This resulted in a relative risk ratio (RR) of 1.60 (95% CI -10.32 to 13.52), in favor of the reassurance group. This was not considered as a clinically relevant difference.
2. Pain (critical)
Two studies reported the outcome pain in systematic review of Head (2015) (Dias, 2003; Dias, 2007). The results were pooled in a meta-analysis. The pooled number of patients that reported pain after treatment of a wrist ganglion cyst in the no treatment group was 26/93 (28.0%), compared to 30/116 (25.9%) in the aspiration group. This resulted in a pooled relative risk ratio (RR) of 0.91 (95% CI 0.58 to 1.44), in favor of the aspiration group. This was not considered as a clinically relevant difference.

Figure 1. Forest plot showing the comparison between aspiration relative to reassurance for the number of patients that reported about pain after treatment of a wrist ganglion cyst.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.
3. Health-related QoL (important)
None of the included studies reported the outcome health-related QoL.
4. Satisfaction with treatment results (important)
None of the included studies reported the outcome satisfaction with treatment results.
5. Return to work/sport/hobby (important)
Two studies reported the outcome return to work after wrist ganglion cyst treatment in the systematic review of Head (2015) (Dias, 2003; Dias, 2007). Both studies reported the time off work (in days) after the intervention.
The pooled mean difference (MD) time off work (in days) between the reassurance group (N=93) and the aspiration group (N=116) was 1.60 (95% CI -1.93 to 5.13) days, in favor of the reassurance group (Figure 4). This was not considered as a clinically relevant difference.
Figure 4. Forest plot showing the comparison between aspiration relative to reassurance for return to work.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.

6. Complications (important)
Two studies reported the outcome complications in the systematic review of Head (2015) (Dias, 2003; Dias, 2007).
Dias (2003) reported: Patients with untreated ganglia had no complications. There was a complication rate of 5% for the aspiration group. Complications included wound infection, neuroma formation, hypertrophic scar, numbness in the distribution of palmar cutaneous branch of the median nerve and radial artery damage in one case. Dias (2007) reported the following complications: patients with wait and see: 0/55 (0%), aspiration: 2/78 (3%): 2-Scar tender.
The pooled number of patients with complications of wrist ganglion cyst treatment in the reassurance group was 0/93 (0%), compared to 4/116 (3.4%) in the aspiration group. This resulted in a pooled risk difference (RD) of 0.03 (95% CI -0.01 to 0.07), in favor of the reassurance group (Figure 3). This was not considered as a clinically relevant difference. Complications included wound infection, neuroma formation, hypertrophic scar, numbness in the distribution of palmar cutaneous branch of the median nerve, scar tenders, and radial artery damage in one case.
Figure 3. Forest plot showing the comparison between aspiration relative to reassurance for complications.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.

7. Revision/recurrence (important)
Two studies reported the outcome recurrence in the systematic review of Head (2015) (Dias, 2003; Dias, 2007).
In the study of Dias (2003), the ganglion was considered to have recurred if it was present at either the 1-, 2- or 5-year follow-up, though this could represent either recurrence or the formation of a new ganglion at the same site. After initial treatment, if a ganglion had recurred at 2 years follow-up but subsequently disappeared before the 5-year follow-up, it was still considered to have recurred after the initial intervention. In the study of Dias (2007), the ganglion was considered to have recurred if it reappeared at the same site anytime between intervention and final follow-up, representing either a recurrence or the formation of a new ganglion. If a ganglion had recurred at the second-year follow-up but subsequently disappeared by the sixth-year follow-up, it was still recorded as a recurrence.
The pooled number of patients with recurrence of wrist ganglion cysts the reassurance group and aspiration group was 50/93 (53.8%), compared to 63/116 (54.3%) in the aspiration group. This resulted in a pooled relative risk ratio (RR) of 0.99 (95% CI 0.77 to 1.28), in favor of any of the aspiration group (Figure 2). This was not considered as a clinically relevant difference.
Figure 2. Forest plot showing the comparison between aspiration relative to reassurance for recurrence.
Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.

8. Range of motion (important)
None of the included studies reported the outcome range of motion.
9. Grip and pinch strength (important)
None of the included studies reported the outcome grip and pinch strength.
10. Severity of symptoms (important)
None of the included studies reported the outcome severity of symptoms.
11. Hand aesthetics (important)
None of the included studies reported the outcome hand aesthetics.
III) Hand therapy versus aspiration
Hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics
No studies were identified that compared hand therapy with aspiration in patients with ganglion cysts.
Level of evidence of the literature
I) Expectative policy versus hand therapy
Hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics
No evidence was found regarding the effect of expectative policy on the outcomes hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms or hand aesthetics when compared with hand therapy in patients with a wrist ganglion cyst, and therefore the level of evidence could not be graded.
II) Expectative policy versus aspiration
1. Hand function/activities of daily life (critical)
The level of evidence regarding the outcome measure hand function/activities of daily life comes from observational studies and therefore starts low. The level of evidence was downgraded by one level because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision). The level of evidence was very low.
2. Pain (critical)
The level of evidence regarding the outcome measure pain comes from observational studies and therefore starts low. The level of evidence was downgraded by one level because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision). The level of evidence was very low.
3. Health-related QoL (important)
No evidence was found regarding the outcome measure health-related QoL, and therefore the level of evidence could not be graded.
4. Satisfaction with treatment results (important)
No evidence was found regarding the outcome measure satisfaction with treatment results, and therefore the level of evidence could not be graded.
5. Return to work/sport/hobby (important)
The level of evidence regarding the outcome measure return to work/sport/hobby comes from observational studies and therefore starts low. The level of evidence was downgraded by one level because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision). The level of evidence was very low.
6. Complications (important)
The level of evidence regarding the outcome measure complications comes from observational studies and therefore starts low. The level of evidence was downgraded by one level because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision). The level of evidence was very low.
7. Revision/recurrence (important)
The level of evidence regarding the outcome measure revision/recurrence comes from observational studies and therefore starts low. The level of evidence was downgraded by one level because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision). The level of evidence was very low.
8. Range of motion (important)
No evidence was found regarding the outcome measure range of motion, and therefore the level of evidence could not be graded.
9. Grip and pinch strength (important)
No evidence was found regarding the outcome measure grip and pinch strength, and therefore the level of evidence could not be graded.
10. Severity of symptoms (important)
No evidence was found regarding the outcome measure severity of symptoms, and therefore the level of evidence could not be graded.
11. Hand aesthetics (important)
No evidence was found regarding the outcome measure hand aesthetics, and therefore the level of evidence could not be graded.
III) Hand therapy versus aspiration
Hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics
No evidence was found regarding the effect of hand therapy on the outcome measures hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms or hand aesthetics when compared with aspiration in patients with a wrist ganglion cyst, and therefore the level of evidence could not be graded.
A systematic review of the literature was performed to answer the following questions:
I) What are the beneficial and harmful effects of wait and see compared to hand therapy in patients with ganglion cysts?
|
P (Patients) |
patients aged older than 16 years with ganglion cysts (both dorsal and volar of the wrist) |
|
I (Intervention) |
wait and see |
|
C (Comparison) |
hand therapy |
|
O (Outcome) |
hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics |
II) What are the beneficial and harmful effects of wait and see compared to aspiration (with or without infiltration) therapy in patients with ganglion cysts?
|
P (Patients) |
patients aged older than 16 years with ganglion cysts (both dorsal and volar of the wrist) |
|
I (Intervention) |
wait and see |
|
C (Comparison) |
aspiration with or without infiltration (corticosteroids, hyaluronic acid, or glucose) |
|
O (Outcome) |
hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics |
III) What are the beneficial and harmful effects of hand therapy compared to aspiration (with or without infiltration) therapy in patients with ganglion cysts?
|
P (Patients) |
patients aged older than 16 years with ganglion cysts (both dorsal and volar of the wrist) |
|
I (Intervention) |
hand therapy |
|
C (Comparison) |
aspiration with or without infiltration (corticosteroids, hyaluronic acid, or glucose) |
|
O (Outcome) |
hand function/activities of daily life, pain, health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics |
Relevant outcome measures
The guideline development group considered hand function/activities of daily life and pain as critical outcomes for decision making; and health-related QoL, satisfaction with treatment results, return to work/sport/hobby, complications, revision/recurrence, range of motion, grip and pinch strength, severity of symptoms, hand aesthetics as important outcomes for decision making.
The guideline development group defined the outcome measures as follows:
- Hand function/activities of daily life: preferably measured with Boston Carpal Tunnel Questionnaire (BCTQ), subscale Functional Status Scale (FSS) (Levine, 1993; Smits, 2014), Michigan Hand Outcomes Questionnaire (MHQ) or Patient-Rated Wrist/Hand Evaluation (PRWHE)
- Pain: preferably measured with a Numeric Rating Scale (NRS), or Visual Analogue Scale (VAS)
- Health-related QoL: preferably measured with EQ-5D-5L
- Satisfaction with treatment results: A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
- Return to work/sport/hobby: time off work, sport, or hobbies in days
- Complications: complications up to 30 days postoperative/start treatment
- Revision/recurrence: report of any repeat operation for the same condition in the same patient due to disease progression or recurrence, or as follow-up to failed previous surgery. Subsequently, description of new / additional treatment, (within final time point of tracks). (Wouters, 2021)
- Range of motion: evaluated via Goniometry and Kapandji Score (Wouters, 2021)
- Grip and pinch strength: grip: Evaluated via hand-held dynamometer, pinch: Evaluated via Lateral/Key Pinch and Tip Pinch (Wouters, 2021)
- Severity of symptoms: preferably measured with BCTQ, subscale Symptom Severity Scale (SSS) (Levine, 1993; Smits, 2014)
- Hand aesthetics: A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
The following limits were used for minimal clinically (patient) important differences per outcome:
- Hand function/activities of daily life: 28% difference in BCTQ-FSS (De Kleermaker, 2019)
- Pain: 2 points on a NRS or VAS scale, on a scale from 0 to 10.
- Health-related QoL: GRADE standard limits*
- Satisfaction with treatment results: GRADE standard limits*
- Return to work/sport/hobby: 1 working week (5 days)
- Complications: GRADE standard limits*
- Recurrence/revision: GRADE standard limits*
- Range of motion: GRADE standard limits*
- Grip and pinch strength: GRADE standard limits*
- Severity of symptoms: 46% difference in BCTQ-SSS (De Kleermaker, 2019)
- Hand aesthetics: GRADE standard limits*
* Default thresholds proposed by the international GRADE working group were used: a 25% difference in relative risk (RR) for dichotomous outcomes (RR <0.80 or RR >1.25), or 0.5 standard deviations (SD) for continuous outcomes
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 29 November 2021. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 342 hits. Studies were selected based on the following criteria: systematic reviews, randomized controlled trials, and observational studies, that made a comparison between expectative policy, hand therapy and/or aspiration in patients with wrist ganglion cysts, and reported at least one outcome of interest.
Eighteen studies were initially selected based on title and abstract screening. After reading the full text, seventeen studies were excluded (see the table with reasons for exclusion under the tab Methods), and one study was included.
Results
I) Expectative policy versus hand therapy
No studies were included in the analysis of the literature that compared expectative policy with hand therapy.
II) Expectative policy versus aspiration
One study was included in the analysis of the literature that compared expectative policy with aspiration. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
III) Hand therapy versus aspiration
No studies were included in the analysis of the literature that compared hand therapy with aspiration.
- De Kleermaeker, F. G., Boogaarts, H. D., Meulstee, J., & Verhagen, W. I. (2019). Minimal clinically important difference for the Boston Carpal Tunnel Questionnaire: new insights and review of literature. Journal of Hand Surgery (European Volume), 44(3), 283-289.
- Dias, J., & Buch, K. (2003). Palmar wrist ganglion: Does intervention improve outcome A prospective study of the natural history and patient-reported treatment outcomes. Journal of Hand Surgery, 28(2), 172-176.
- Dias, J. J., Dhukaram, V., & Kumar, P. (2007). The natural history of untreated dorsal wrist ganglia and patient reported outcome 6 years after intervention. Journal of Hand Surgery (European Volume), 32(5), 502-508.
- Head, L., Gencarelli, J. R., Allen, M., & Boyd, K. U. (2015). Wrist ganglion treatment: systematic review and meta-analysis. The Journal of hand surgery, 40(3), 546-553.
- Levine, D. W., Simmons, B. P., Koris, M. J., Daltroy, L. H., Hohl, G. G., Fossel, A. H., & Katz, J. N. (1993). A self-administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. The Journal of bone and joint surgery. American volume, 75(11), 1585-1592.
- Shauver, M. J., & Chung, K. C. (2009). The minimal clinically important difference of the Michigan hand outcomes questionnaire. The Journal of hand surgery, 34(3), 509-514.
- Smits, F. V. M., Ottenhof, M., Feitz, R., & Kreulen, M. (2014). Nederlandse vertaling van de 'Boston carpal Tunnel Questionnaire' voor evaluatie van het carpaletunnel-syndroom (BcTQ-dlV). Nederlands tijdschrift voor plastische chirurgie, 5, 70-3.
- Wouters, R. M., Jobi-Odeneye, A. O., de la Torre, A., Joseph, A., Shin, A. Y., MacDermid, J. C., ... & Hovius, S. E. (2021). A standard set for outcome measurement in patients with hand and wrist conditions: consensus by the international consortium for health outcomes measurement hand and wrist working group. The Journal of Hand Surgery, 46(10), 841-855.
II) Expectative policy versus aspiration
Systematic reviews
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C) |
Follow-up |
Outcome measures and effect size |
Comments |
|
Head (2015) |
SR and meta-analysis of cohort studies
Literature search up to December 2013 (from 1990).
Study design:
Setting and Country: From the Faculty of Medicine, University of Ottawa; and the Division of Plastic Surgery, Ottawa Hospital, Ottawa, Ontario, Canada.
Source of funding and conflicts of interest: No benefits in any form have been received or will be received related directly or indirectly to the subject of this article. |
Inclusion criteria SR:
Exclusion criteria SR:
Six studies included, of which two studies met our PICO and were included in our analyses.
Important patient characteristics at baseline:
N:
Mean (SE) age:
C: 48.2 (2.5)
C: 39.0 (1.9)
Sex:
Groups comparable at baseline? Yes. |
|
|
End-point of follow-up:
For how many participants were no complete outcome data available? (intervention/control)
|
Outcome measure: recurrence
C: 18/38 (28%)
Pooled effect relative risk ratio (random effects model): 0.99 (95% CI 0.77 to 1.28) favoring aspiration. Heterogeneity (I2): 0%
Outcome measure: pain
C: 7/38 (18%)
C: 23/78 (29%)
Outcome measure: complications
C: 2/38 (5%)
C: 2/78 (3%)
Outcome measure: Patient Evaluation Measure (PEM) hand disability score, mean (SE)
C: 17.1 (4.3)
Outcome measure: time off work (days), mean (SE)
C: 3.5 (1.5)
C: 3.2 (1.5) |
Conclusions: A. In conclusion, this study indicates that the only longterm benefit of aspiration or excision of palmar wrist ganglia is the patients’ perception of the ganglions’ unsightliness. Patients with a persisting ganglion are more symptomatic although over time fewer patients had symptoms.
B. In our opinion, intervention for dorsal wrist ganglia is only justified if it provides better relief of symptoms, less recurrence and/or fewer risks compared to no treatment. Neither surgical excision nor aspiration provides a clear long-term benefit over the natural history of the dorsal wrist ganglion. Forty two percent (23/55) of the untreated ganglia resolved spontaneously. The recurrence rate was higher (45/78 – 58%) following aspiration than after excision (40/103 – 39%). The probable benefit of surgery is early resolution of the swelling in the 61% of patients in whom the ganglion did not recur. |
Quality assessment
II) Expectative policy versus aspiration
Systematic reviews
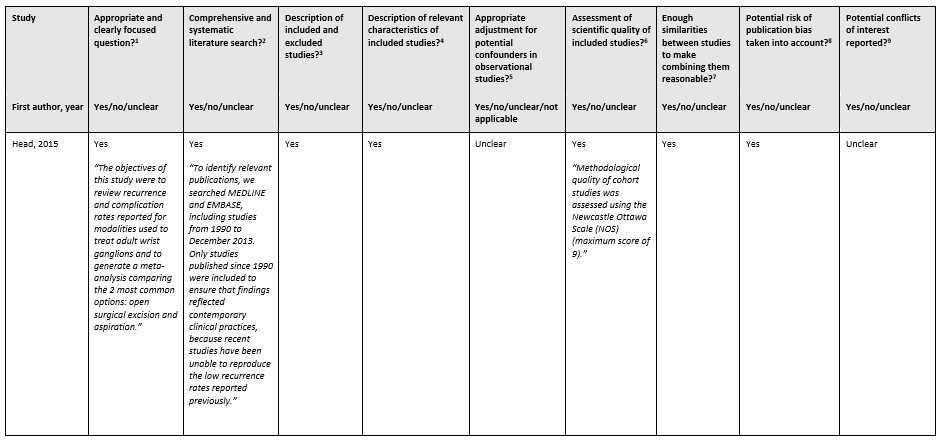
Table of excluded studies
|
Author and year |
Reason for exclusion |
|
Chatterjee, Shamita, et al. "Comparative study of recurrence and complications using various sclerosants by single dart technique in treatment of ganglion cysts." Indian Journal of Surgery 76 (2014): 350-353. |
Wrong comparison |
|
Chen, J., Liu, Q., Xiong, J., Lu, L., Zhu, S., Zhong, Z., ... & Chen, Z. (2020). Effect of fire needle for ganglion cysts: A protocol of systematic review and meta-analysis of randomized controlled trials. Medicine, 99(41). |
Protocol article |
|
MOWP study group: (2020). The presentation, diagnosis and management of non-traumatic wrist pain: an evaluation of current practice in secondary care in the UK NHS. Rheumatology Advances in Practice, 2020, 4.2: rkaa030. |
Wrong comparison |
|
Gitto, S., Lee, S. C., & Miller, T. T. (2019). Ultrasound‐guided percutaneous treatment of volar radiocarpal ganglion cysts: Safety and efficacy. Journal of Clinical Ultrasound, 47(6), 339-344. |
Wrong comparison |
|
Hassan, M. U., Ali, M. T., & Nadeem, A. (2017). Comparison of Surgical Excision versus Aspiration and Injection of Steroid of Wrist Ganglion. |
Wrong comparison |
|
Hatchell, A., Meathrel, K., Farrokhyar, F., & Hynes, N. (2019). A prospective randomized controlled trial of aspiration and Fibrin Sealant Use versus aspiration alone in the treatment of dorsal wrist ganglia. Plastic Surgery, 27(1), 22-28. |
Wrong comparison |
|
Head, L., Allen, M., & Boyd, K. U. (2015). Long-term outcomes and patient satisfaction following wrist ganglion aspiration. Plastic Surgery, 23(1), 51-53. |
Non-comparative study |
|
Ho, P. C., Griffiths, J., Lo, W. N., Yen, C. H., & Hung, L. K. (2001). Current treatment of ganglion of the wrist. Hand Surgery, 6(01), 49-58. |
Wrong study design |
|
Hussain, S. H. A. B. A. B., Akhtar, S., Aslam, V., & Khan, S. M. (2015). Efficacy of aspiration and steroid injection in treatment of ganglion cyst. Pak J Med Health Sci, 9(4), 1403-1405. |
Wrong comparison |
|
Khan, P. S., & Hayat, H. (2011). Surgical excision versus aspiration combined with intralesional triamcinolone acetonide injection plus wrist immobilization therapy in the treatment of dorsal wrist ganglion; a randomized controlled trial. Journal of hand and microsurgery, 3(02), 55-57. |
Wrong comparison |
|
Kim, K. M., Kang, E. Y., Lee, S. H., Jung, A. Y., Nam, D. H., & Cheon, J. H. (2014). Therapeutic approach of wrist ganglion using electroacupuncture: two case reports. Annals of Rehabilitation Medicine, 38(3), 415-420. |
Wrong study design |
|
Kumar, K., & Sharma, D. (2016). Comparison of efficacy of methyl prednisolone and triamcinolone in wrist ganglion using double dart technique and its application in an Indian population. Current Orthopaedic Practice, 27(6), 614-617. |
Wrong comparison |
|
Limpaphayom, N., & Wilairatana, V. (2004). Randomized controlled trial between surgery and aspiration combined with methylprednisolone acetate injection plus wrist immobilization in the treatment of dorsal carpal ganglion. J Med Assoc Thai, 87(12), 1513-7. |
Wrong comparison |
|
Meena, S., & Gupta, A. (2014). RETRACTED: Dorsal wrist ganglion: Current review of literature. Journal of clinical orthopaedics and trauma, 5(2), 59-64. |
Article was retracted |
|
Mulders, M. A. M., Sulkers, G. S. I., Videler, A. J., Strackee, S. D., & Smeulders, M. J. C. (2018). Long-term functional results of a wrist exercise program for patients with palmar midcarpal instability. Journal of Wrist Surgery, 7(03), 211-218. |
Wrong comparison |
|
Shakya, A., Garje, V., & Rathore, A. (2021). The triple technique: A simple and effective outpatient procedure for the dorsal wrist ganglion. Journal of Clinical Orthopaedics and Trauma, 23, 101619. |
Wrong comparison |
|
Sinha, M. K., Mishra, P., Mishra, T. S., & Barman, A. (2019). Aspiration and steroid injection in ganglion cysts: An ultrasound guided evaluation of the response. Journal of Clinical Orthopaedics and Trauma, 10, S252-S257. |
Wrong comparison |
|
Suen, M., Fung, B., & Lung, C. P. (2013). Treatment of ganglion cysts. International Scholarly Research Notices, 2013. |
Wrong publication type |
Beoordelingsdatum en geldigheid
Publicatiedatum : 22-02-2024
Beoordeeld op geldigheid : 20-02-2024
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met ganglion.
Werkgroep
- Prof. dr. E. (Erik) Heineman, hoogleraar chirurgie, gepensioneerd chirurg UMC Groningen, NVvH (voorzitter)
- Drs. M. (Martijn) ten Berge, chirurg, HagaZiekenhuis, NVvH
- Dr. A. (Annechien) Beumer, orthopedisch en hand chirurg, Amphia ziekenhuis en Amsterdam UMC, NOV en Nederlandse Vereniging voor Handchirurgie
- Drs. H.L. (Luitzen) de Boer, plastisch chirurg, Catharina ziekenhuis en Xpert Clinics, NVPC en Nederlandse Vereniging voor Handchirurgie
- Drs. J. (Joost) van Dijsseldonk, orthopedisch chirurg, Maxima Medisch Centrum Velthoven, NOV
- C.E.J. (Chantal) Essink, hand- en fysiotherapeut, Welzorg, NVHT, Ergotherapie Nederland, KNGF
- Dr. A.P.A. (Alexander) Greeven, chirurg, HagaZiekenhuis en Juliana kinderziekenhuis, NVvH en Nederlandse Vereniging voor Handchirurgie
- Dr. A.C. (Aimee) Kok-Pigge, huisarts, wetenschappelijk medewerker NHG, NHG
- Drs. B. (Bas) van Ooij, zelfstandig bedrijfsarts, VisieCare Arbo & HR, NVAB.
Meelezers
- I. (Ilse) van Ee, adviseur patiëntenbelang, Patiëntenfederatie Nederland
- M. (Maike) Broere, adviseur patiëntenbelang, Patiëntenfederatie Nederland
Met ondersteuning van
- dr. A. (Anja) van der Hout, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Heineman |
- Hoogleraar Chirurgie, gepensioneerd, - 0-aanstelling het UMCG/RUG. Begeleiding promovendi (3) (tot mei 2023) |
- Vrijwilliger bij netwerk organisatie 'Gezond en Gelukkig Den Haag'. |
Geen |
Geen restricties |
|
De Boer |
- Plastisch chirurg Catherina ziekenhuis en Xpert Clinics |
Lid beroepsgenoot tuchtrecht voor de gezondheidszorg |
Vrijgevestigd specialist waarbij ik handchirurg ben zowel in het Catherina ziekenhuis als de Xpert Clinics |
Geen restricties |
|
Greeven
|
- Chirurg, Hagaziekenhuis & Juliana Kinderziekenhuis |
Opleider Heelkunde, Hagaziekenhuis
|
Geen |
Geen restricties |
|
Kok-Pigge
|
- Wetenschappelijk medewerker, Richtlijnontwikkeling en Wetenschap, NHG (0,2 fte; - Huisarts in opleiding (tot sept 2023) |
Geen |
Overeenstemming/discrepanties met nieuwe NHG Standaard Hand-en Polsklachten.
|
Geen restricties |
|
Beumer
|
- 80 % Orthopedisch en Handchirurg, Vakgroep Orthopedie Amphia Ziekenhuis |
- Bestuurslid Handpols Werkgroep Nederlandse Orthopeden vereniging (NOV) (niet meer bij einde richtlijn) - Voorzitter richtlijn werkgroep generieke module over arbeidsparticipatie |
Geen |
Geen restricties |
|
Essink
|
- Hand- en fysiotherapeut bij Xpert Handtherapie (tot okt 2023) - Paramedisch adviseur bij Welzorg BV (per okt 2023)
|
Geen
|
Geen |
Geen restricties |
|
Van Ooij
|
- Zelfstandig bedrijfsarts, in samenwerking met VisieCare Arbo & HR - AIOS bedrijfsgeneeskunde bij Arbodienst (tot sept 2022) |
Geen |
Geen |
Geen restricties |
|
Van Dijsseldonk
|
- Orthopedisch Chirurg |
ATLS, stichting ALSG |
Geen |
Geen restricties |
|
Ten Berge
|
- Traumachirurg, Hagaziekenhuis, Den Haag |
Geen |
Geen |
Geen restricties |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van Patiëntenfederatie Nederland voor de invitational conference. Patiëntenfederatie Nederland heeft ook meegelezen met de richtlijn. Het verslag van de invitational conference (zie bijlage) is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Wkkgz & Kwalitatieve raming van mogelijke substantiële financiële gevolgen
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijn is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling zijn richtlijnmodules op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
|
Module |
Uitkomst raming |
Toelichting |
|
Module Diagnostiek |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Niet-chirurgische behandeling |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Chirurgische behandeling |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Postoperatieve nabehandeling |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module secundaire preventie en werk |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met polsganglion. Tevens zijn er knelpunten aangedragen door de NVvH, NOV, NHG, Nederlandse Vereniging voor Handchirurgie, NVAB, KNGF, Nederlandse Vereniging voor Handtherapie, Adviesraad Handtherapie, Ergotherapie Nederland en Patiëntenfederatie Nederland via een invitational conference op 14-09-2021. Een verslag hiervan is opgenomen in de bijlage. Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen van de betreffende modules.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Literature search strategy
Algemene informatie
|
Richtlijn: Ganglion |
|
|
Uitgangsvraag: Wat is de optimale niet-chirurgische behandeling van ganglion? |
|
|
Database(s): Ovid/Medline, Embase |
Datum: 29 november 2021 |
|
Periode: 2000 - heden |
Talen: Engels, Nederlands |
|
Literatuurspecialist: Miriam van der Maten |
|
|
BMI zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting:
|
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
13 |
53 |
41 |
|
RCTs |
31 |
27 |
41 |
|
Observationele studies |
209 |
112 |
260 |
|
Totaal |
253 |
192 |
342 |
Zoekstrategie
Embase
|
No. |
Query |
Results |
|
#12 |
#9 OR #10 OR #11 |
253 |
|
#11 |
#5 AND #8 NOT (#9 OR #10) = Observationeel |
209 |
|
#10 |
#5 AND #7 NOT #9 = RCT |
31 |
|
#9 |
#5 AND #6 = SR |
13 |
|
#8 |
'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) OR 'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
14389659 |
|
#7 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
1846266 |
|
#6 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
733409 |
|
#5 |
#1 AND (#2 OR #3 OR #4) AND ([english]/lim OR [dutch]/lim) AND [2000-2021]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) |
492 |
|
#4 |
'arthrocentesis'/exp OR 'aspiration'/exp OR 'joint aspiration'/exp OR arthrocentes*:ti,ab,kw OR aspiration*:ti,ab,kw OR 'intraarticular drug administration'/exp OR 'injection'/exp OR inject*:ti,ab,kw OR 'corticosteroid'/exp OR corticosteroid*:ti,ab,kw OR glucocorticoid*:ti,ab,kw OR 'adrenal cortex hormone*':ti,ab,kw OR 'prednisolone derivative'/exp OR 'cortisone'/exp OR 'hydrocortisone'/exp OR 'hyaluronic acid'/exp OR 'glucose'/exp OR 'triamcinolone'/exp OR 'prednisolone':ti,ab,kw OR 'cortisone':ti,ab,kw OR 'hyaluronic acid':ti,ab,kw OR 'glucose':ti,ab,kw OR 'triamcinolon*':ti,ab,kw OR hydrocortisone:ti,ab,kw OR 'methylprednisolone':ti,ab,kw |
3058242 |
|
#3 |
'manipulative medicine'/exp OR 'physiotherapy'/exp OR 'physiotherapist'/exp OR 'hand therapy'/exp OR 'occupational therapy'/exp OR 'occupational therapist'/exp OR 'splinting'/exp OR 'splint'/exp OR 'exercise'/exp OR 'training'/exp OR 'kinesiotherapy'/exp OR (((manual OR physi* OR occupational OR hand) NEAR/3 therap*):ti,ab,kw) OR exercise*:ti,ab,kw OR train*:ti,ab,kw OR splint*:ti,ab,kw OR physiotherapy*:ti,ab,kw OR handtherap*:ti,ab,kw OR kinesiotherapy*:ti,ab,kw |
1517811 |
|
#2 |
'conservative treatment'/exp OR 'expectant management':ti,ab,kw OR 'wait and see':ti,ab,kw OR conservative:ti,ab,kw OR nonsurgical:ti,ab,kw OR nonoperative:ti,ab,kw OR 'watchful waiting':ti,ab,kw |
808958 |
|
#1 |
'wrist ganglion'/exp OR (('ganglion cyst'/exp OR 'ganglion'/exp OR ganglion*:ti,ab,kw) AND ('arm'/exp OR 'upper extremit*':ti,ab,kw OR upperextremit*:ti,ab,kw OR 'upper-limb*':ti,ab,kw OR upperlimb*:ti,ab,kw OR hand*:ti,ab,kw OR wrist*:ti,ab,kw OR finger*:ti,ab,kw OR thumb*:ti,ab,kw OR metacarp*:ti,ab,kw OR interphalang*:ti,ab,kw OR phalang*:ti,ab,kw OR carpus:ti,ab,kw OR carpal:ti,ab,kw)) OR 'mucoid cyst*':ti,ab,kw |
4794 |
Ovid/Medline
|
# |
Searches |
Results |
|
13 |
10 or 11 or 12 |
192 |
|
12 |
(6 and 9) not (10 or 11) = Observationeel |
112 |
|
11 |
(6 and 8) not 10 = RCT |
27 |
|
10 |
6 and 7 = SR |
53 |
|
9 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) or Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ |
6647451 |
|
8 |
exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf. |
1463431 |
|
7 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. or review.ti,ab,kf. |
2054140 |
|
6 |
limit 5 to yr="2000 -Current" |
430 |
|
5 |
1 and (2 or 3 or 4) |
661 |
|
4 |
exp Arthrocentesis/ or exp Injections, Intra-Articular/ or exp Injections/ or Adrenal Cortex Hormones/ or exp Prednisolone/ or exp Cortisone/ or exp Hydrocortisone/ or exp Hyaluronic Acid/ or exp Glucose/ or exp Triamcinolone/ or arthrocentes*.ti,ab,kf. or aspiration*.ti,ab,kf. or inject*.ti,ab,kf. or corticosteroid*.ti,ab,kf. or glucocorticoid*.ti,ab,kf. or 'adrenal cortex hormone*'.ti,ab,kf. or 'prednisolone'.ti,ab,kf. or 'cortisone'.ti,ab,kf. or 'hyaluronic acid'.ti,ab,kf. or 'glucose'.ti,ab,kf. or 'triamcinolon*'.ti,ab,kf. or hydrocortisone.ti,ab,kf. or 'methylprednisolone'.ti,ab,kf. |
1942097 |
|
3 |
exp Physical Therapy Modalities/ or exp Physical Therapists/ or exp Occupational Therapy/ or exp Occupational Therapists/ or exp Splints/ or exp Exercise/ or exp Exercise Therapy/ or ((manual or physi* or occupational or hand) adj3 therap*).ti,ab,kf. or exercise*.ti,ab,kf. or train*.ti,ab,kf. or splint*.ti,ab,kf. or physiotherapy*.ti,ab,kf. or handtherap*.ti,ab,kf. or kinesiotherapy*.ti,ab,kf. |
1141949 |
|
2 |
exp Conservative Treatment/ or exp Watchful Waiting/ or 'Expectant management'.ti,ab,kf. or "wait and see".ti,ab,kf. or conservative.ti,ab,kf. or nonsurgical.ti,ab,kf. or nonoperative.ti,ab,kf. or 'Watchful Waiting'.ti,ab,kf. |
152110 |
|
1 |
((exp Ganglion Cysts/ or ganglion*.ti,ab,kf.) and (exp Wrist/ or exp Hand Joints/ or exp Upper Extremity/ or 'upper extremit*'.ti,ab,kf. or upperextremit*.ti,ab,kf. or 'upper-limb*'.ti,ab,kf. or upperlimb*.ti,ab,kf. or hand*.ti,ab,kf. or wrist*.ti,ab,kf. or finger*.ti,ab,kf. or thumb*.ti,ab,kf. or metacarp*.ti,ab,kf. or interphalang*.ti,ab,kf. or phalang*.ti,ab,kf. or carpus.ti,ab,kf. or carpal.ti,ab,kf.)) or 'mucoid cyst*'.ti,ab,kf. |
3334 |