Cabergoline in de preventie van OHSS
Uitgangsvraag
Wat is de plaats van cabergoline in de preventie van OHSS?
Aanbeveling
Overweeg cabergoline toe te voegen aan de behandeling bij patiënten met een hoog risico op OHSS die een HCG trigger hebben gehad.
Gebruik een dosis van 0,50 mg dagelijks gedurende 5, 7 of 8 dagen vanaf de dag van de hCG trigger.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
De werkgroep heeft een literatuurstudie verricht naar de effectiviteit (preventie ovarieel hyperstimulatiesyndroom (OHSS)) en veiligheid van cabergoline vergeleken met placebo of geen cabergoline bij vrouwen in een ART behandelingstraject en een hoog risico op OHSS. Op basis van de resultaten van een systematische review uit 2021 lijkt toediening van cabergoline het risico op de cruciale uitkomstmaat (OHSS) te verlagen vergeleken met placebo of geen toediening cabergoline. De bewijskracht werd beoordeeld als ‘laag’ voor uitkomstmaat preventie van OHSS. Er is geen literatuur gevonden voor de specifieke uitkomstmaat ‘ernstig OHSS’. In de Cochrane review van 2016 (Mourad et al) werd het effect als moderate beoordeeld en in het artikel van Pfeiffer et al als ‘good’.
De werkgroep is niet zeker over het effect van cabergoline op de kans op zwangerschap, meerlingzwangerschappen en miskraamkans.
Langdurig gebruik van cabergoline kan fibrose en hartklepaandoeningen veroorzaken. Dit wordt niet beschreven in de studies waarbij cabergoline als preventie is gebruikt. Mogelijk komt dit door de korte duur (5-8 dagen) van gebruik.
Vasculaire endotheliale groeifactor (VEGF) speelt een belangrijke rol bij het tot stand komen van OHSS. Cabergoline blokkeert de toename van vasculaire permeabiliteit door VEGF receptoren te defosfoliseren. Anti-VEGF medicatie zoals SU5416 kunnen niet worden gebruikt vanwege de bijwerkingen zoals tromboembolisme (Glade-Bender, 2003; Kuenen, 2003). Dopamine agonisten hebben vergelijkbare effecten op de vasculaire doorlaatbaarheid zonder deze bijwerkingen. Dopamine agonisten worden al jaren gebruikt om het prolactine te verlagen bij patiënten met een prolactinoom.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Het medicament kan in pilvorm worden gebruikt. De bijwerkingen (dyspneu, misselijkheid, braken en ziekenhuisopname, pijnklachten, trombose, opnameduur, kwaliteit van leven) die worden ervaren zijn over het algemeen mild. De kans op cardiale problemen, wat gezien wordt bij langduriger gebruik van cabergoline, lijkt bij kort gebruik niet op te treden. Om deze redenen verwacht de werkgroep dat toediening van cabergoline ter preventie van OHSS over het algemeen geen grote belasting is voor de patiënt.
Kosten (middelenbeslag)
De kosten van cabergoline zijn laag. Vroegtijdig interveniëren in de cascade richting het ontstaan voor OHSS zal potentieel leiden tot minder ernstige OHSS en dus minder langdurige OHSS behandeling en eventueel bijkomende ziekenhuisopname. Het effect is vooralsnog alleen onderzocht bij de groep met een hoog risico op OHSS.
Aanvaardbaarheid, haalbaarheid en implementatie
De werkgroep is van mening dat kortdurend gebruik van cabergoline bij patiënten met een hoog risico op OHSS zou kunnen bijdragen in een lagere kans op OHSS. Wel is het van belang de potentiële bijwerkingen (dyspneu, misselijkheid, braken en ziekenhuisopname, pijnklachten, trombose, opnameduur, kwaliteit van leven) te bespreken met patiënten. De kans op cardiale problemen, wat gezien wordt bij langduriger gebruik van cabergoline, lijkt bij kort gebruik niet op te treden. Het is een goedkoop middel dat makkelijk te gebruiken is. Een verlaagde kans op OHSS scheelt mogelijk ziekenhuisopnames. Bij patiënten met hartklepafwijkingen kunnen andere overwegingen worden gebruikt.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Cabergoline lijkt het risico op OHSS te verminderen bij patiënten met een verhoogd risico op OHSS. De kans op ernstige bijwerkingen is niet verhoogd (bewijskracht moderate). Gebruik van cabergoline lijkt geen effect te hebben op het aantal doorgaande zwangerschappen en het miskraamrisico.
Onderbouwing
OHSS is characterized by a shift of intravascular fluid to the third space due to increased capillary permeability and ovarian neoangiogenesis. Cabergoline (dopamine agonist) prevents leakage from the veins. Prophylactic cabergoline administration is thought to prevent (severe) OHSS.
|
Low GRADE |
Administration of cabergoline may result in lower risk of developing OHSS as compared to placebo or no cabergoline in women undergoing ovarian stimulation for IVF/ICSI who are at high risk of developing OHSS.
Source: (Tang, 2021) |
|
No GRADE |
No evidence was found regarding the effect of cabergoline on the risk of severe OHSS in women undergoing ovarian stimulation for IVF/ICSI who are at high risk of developing OHSS, compared to placebo or no cabergoline.
Source: None |
Description of studies
Tang (2021) wrote a Cochrane systematic literature review to assess the effectiveness and safety of dopamine agonists for preventing OHSS in women at high risk of OHSS when undergoing any ART treatment in combination with hCG trigger. A search was performed in Cochrane Gynaecology and Fertility Specialised Register, CENTRAL, MEDLINE, Embase, CINAHL, and PsycINFO for randomised controlled trials (RCTs) from inception until May 2020, supplemented with a handsearch of reference lists and grey literature. Included in this review were RCTs that compared dopamine agonists with placebo/no intervention or another intervention for preventing OHSS in ART. Primary outcome measures were incidence of moderate or severe OHSS and live birth rate. Secondary outcomes were rates of clinical pregnancy, multiple pregnancy, miscarriage, and adverse events. The dopamine agonists in this review were cabergoline, quinagolide, and bromocriptine. Quasirandomised trials were excluded and, in the case of cross-over trials, only pre-crossover data were included. In total, 22 RCTs were included involving 3171 women at high risk of OHSS, of which 7 studies (N=701 women) focused on cabergoline versus placebo or no cabergoline. These 7 RCTs had sample sizes ranging between 40 and 146. The RCTs were performed in Spain, Israel, Russia, Tunisia, Turkey, United Arab Emirates and India. One RCT also used coasting in almost half of the women in both the intervention and control group, it was unclear exactly which women received coasting and whether these women developed OHSS. Another RCT also had a third treatment arm of oral prednisolone daily from the day of hCG injection to the day of the pregnancy test. The results were meta-analyzed using a fixed effects model and the authors did not observe differences in results when performing a random effects model.
Results
OHSS
Tang (2021) reported as primary outcome that 46/370 women in the cabergoline group and 98/331 women in the placebo/no intervention group developed OHSS. Thus cabergoline was associated with a lower risk of moderate or severe OHSS than placebo/no cabergoline with a fixed-effects odds ratio of 0.34 [0.23, 0.51].
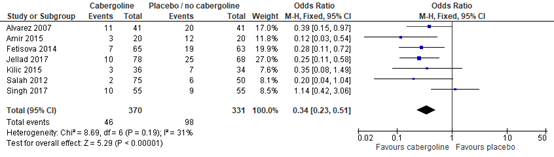
Figure 1. moderate or severe OHSS, comparison between cabergoline and placebo / no cabergoline. Adapted from Tang (2021)
Severe OHSS
No literature was found on the outcome measure severe OHSS only.
Level of evidence of the literature
The level of evidence regarding the outcome measure prevention of OHSS started as high for systematic reviews of RCTs (therapeutic question). The level of evidence was downgraded by two levels because of study limitations (risk of bias); low number of events (imprecision).
As none of the studies selected for the summary of literature reported results for severe OHSS, no GRADE conclusions could be drawn.
A systematic review of the literature was performed to answer the following question:
What is the effectiveness and safety of cabergoline compared with no cabergoline for women with high risk of OHSS undergoing IVF/ovarian stimulation for IVF??
| P: | Women with IVF treatment and high risk of OHSS |
| I: | Cabergoline added to stimulation |
| C: | No cabergoline |
| O: | Developing OHSS, preventing severe OHSS |
Relevant outcome measures
The working group considered prevention of OHSS and severe OHSS as a critical outcome measures for decision making.
A priori, the working group did not define the outcome measure above but used the definitions used in the studies.
The working group defined a 25% difference for dichotomous outcomes (OR < 0.8 or > 1.25) as minimal clinically (patient) important difference.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 9 October 2023. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 331 hits. Studies were selected based on the following criteria: systematic reviews, randomized controlled trials or observational (case-control and cohort) studies comparing cabergoline with no cabergoline in women with IVF treatment and high risk of OHSS and reporting numbers of patients with OHSS. Two studies were initially selected based on title and abstract screening. After reading the full text, 1 study was excluded (see the table with reasons for exclusion under the tab Methods), and 1 study was included.
Results
One Cochrane review was included in the analysis of the literature. Important study characteristics, results and the assessment of risk of bias are summarized in the evidence tables.
- Glade-Bender J, Kandel JJ, Yamashiro DJ. VEGF blocking therapy in the treatment of cancer. Expert Opin Biol Ther. 2003 Apr;3(2):263-76. doi: 10.1517/14712598.3.2.263. PMID: 12662141.
- Kuenen BC, Levi M, Meijers JC, van Hinsbergh VW, Berkhof J, Kakkar AK, Hoekman K, Pinedo HM. Potential role of platelets in endothelial damage observed during treatment with cisplatin, gemcitabine, and the angiogenesis inhibitor SU5416. J Clin Oncol. 2003 Jun 1;21(11):2192-8. doi: 10.1200/JCO.2003.08.046. PMID: 12775746.
- Tang H, Mourad SM, Wang A, Zhai SD, Hart RJ. Dopamine agonists for preventing ovarian hyperstimulation syndrome. Cochrane Database Syst Rev. 2021 Apr 14;4(4):CD008605. doi: 10.1002/14651858.CD008605.pub4. PMID: 33851429; PMCID: PMC8092425.
Evidence table for systemtic review of RCTs and observational studies (intervention studies)
Research question: What is the effectiveness and safety of cabergoline compared with no cabergoline (standard treatment?) for women with OHSS?
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison/ control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Tang, 2021
|
Cochrane SR and meta-analysis of RCTs
Cochrane Gynaecology and Fertility Specialised Register, CENTRAL, MEDLINE, Embase, CINAHL, and PsycINFO were searched until May 2020, supplemented with a handsearch of reference lists and grey literature.
7 included studies: A: Alvarez, 2007 B: Amir, 2015 C: Fetisova, 2014 D: Jellad, 2017 E: Kilic, 2015 F: Salah, 2012 G: Singh, 2017
Study design: Only RCTs were included.
Setting and Country: A: Spain B: Israel C: Russia D: Tunisia E: Turkey F: United Arab Emirates G: India
Source of funding and conflicts of interest: Several internal funding sources were disclosed, but no external funding was received for this study. |
Inclusion criteria SR: Included in this review were published and unpublished RCTs that compared dopamine agonists with placebo/no intervention or another intervention for preventing OHSS in ART. Conference abstracts were handled the same way as full publications.
Exclusion criteria SR: Quasirandomised trials and, in the case of cross-over trials, included only pre-crossover data.
Important patient characteristics at baseline:
N (age is not reported per study) A: 82 B: 40 C: 128 D: 146 E: 70 F: 75 cabergoline (200 total) G: 110
Groups comparable at baseline? A: yes B: unclear C: yes D: unclear E: unclear F: unclear G: unclear
|
Describe intervention: A: cabergoline tablet 0.5 mg/day for 8 days from the day of hCG injection B: cabergoline tablet 0.5 mg/day for 8 days from the day of hCG injection. Did apply coasting to both groups in about 50% of women if serum E2 > 5000 pg/mL C: cabergoline 0.5 mg/day from the day after oocyte retrieval for 5 days before embryo transfer day D: cabergoline 0.5 mg/day for 8 days starting on day of hCG injection E: cabergoline 0.5 mg/day for 8 days from the day of hCG administration F: cabergoline 0.5 mg tablets, 1 tablet on 2 successive days, starting from day of hCG injection, and repeated 1 week later G: cabergoline (no further details are described)
|
Describe control: A: placebo tablet daily for 8 days B: no cabergoline. Did apply coasting to both groups in about 50% of women if serum E2 > 5000 pg/mL C: no intervention D: no medication treatment E: did not receive cabergoline F: No intervention G: placebo
|
End-point of follow-up: Follow-up time per included study not reported in the SR.
For how many participants were no complete outcome data available? (intervention/control)
A: unclear B: none C: none D: unclear E: none F: 7/200 G: 3 from cabergoline group and 5 from placebo group
|
Primary outcome measures were incidence of moderate or severe OHSS and live birth rate.
Moderate or severe OHSS Effect measure: OR [95% CI]: A: 0.39 [0.15, 0.97] B: 0.12 [0.03, 0.54] C: 0.28 [0.11, 0.72] D: 0.25 [0.11, 0.58] E: 0.35 [0.08, 1.49] F: 0.20 [0.04, 1.04] G: 1.14 [0.42, 3.06]
Pooled effect (fixed effects model): 0.34 [95% CI 0.23 , 0.51] Heterogeneity (I2): 31%
|
Risk of bias (high, some concerns or low): Tool used by authors: Cochrane’s tool for assessing risk of bias A: Low B: Some concerns C: Low D: Some concerns E: Low F: Some concerns G: Some concerns
Brief description of author’s conclusion: Dopamine agonists probably reduce the incidence of moderate or severe OHSS compared to placebo/no intervention, while we are uncertain of the effect on adverse events and pregnancy outcomes (live birth, clinical pregnancy, miscarriage).
Personal remarks on study quality, conclusions, and other issues:
GRADE (per comparison and outcome measure) including reasons for down/upgrading by the authors: For outcome incidence of moderate or severe OHSS and intervention dopamine agonist (so not only cabergoline): Moderate GRADE. Downgraded one level for risk of bias associated with poor reporting of study methods. |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Mourad S, Brown J, Farquhar C. Interventions for the prevention of OHSS in ART cycles: an overview of Cochrane reviews. Cochrane Database Syst Rev. 2017 Jan 23;1(1):CD012103. doi: 10.1002/14651858.CD012103.pub2. PMID: 28111738; PMCID: PMC6469542. |
Four years older than the most recent Cochrane review by Tang 2021 |
Beoordelingsdatum en geldigheid
Publicatiedatum : 02-01-2026
Beoordeeld op geldigheid : 02-01-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met OHSS.
Werkgroep
- Dr. G. (Gijs) Teklenburg (voorzitter)(NVOG)
- Dr. A. (Arno) van Peperstraten (NVOG)
- Prof. dr. F. (Frank) Broekmans (NVOG)
- Drs. E. (Eefje) Oude Lohuis (NVOG)
- Dr. S. (Sanne) Braam (NVOG)
- Dr. L. (Leonie) van Houten (NVOG)
- Drs. H.G.I. (Hans) van Weering (NVOG)
- Dr. M. (Mèlanie) van IJsselmuiden (NVOG)
- Dr. S. (Sietske) Gaykema (NVOG)
- Dr. L. (Lotte) Weimar (NVOG)
- Dr. A. (Annelien) de Kat (NVOG)
- Drs. E.C.G. (Esther) van Duinen (VVF)
- Drs. M. (Marloes) Vermeulen (FREYA) (tot november 2024)
- Simone Sinjorgo (FREYA) (van december 2024)
Met ondersteuning van
- Dr. M. (Mohammadreza) Abdollahi, adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Dr. I.M. (Irina) Mostovaya, senior adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Dr. Y.J. (Yvonne) Labeur, adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Dr. J. (Jana) Tuijtelaars, adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Drs. D.A.M. (Danique) Middelhuis, adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Dr. M. (Majke) van Bommel, adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Dr. T. (Tiny) Hoekstra, senior adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Dr. L. (Leanne) Küpers, adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Drs. T. (Thibaut) Dederen, junior adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Drs. D.A.M. (Fieke) Pepping, junior adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
- Alies van der Wal, medisch informatie specialist, Kennisinstituut van de Federatie Medisch Specialisten
- Esther van der Bijl, medisch informatie specialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Overige belangen |
Datum |
Restrictie |
|
Gijs Teklenburg |
Gynaecoloog, subspecialist voortplantings geneeskunde. |
Medical advisor Gedeon Richter Medical advisor Merck |
Geen |
Geen |
Geen |
Geen |
Geen |
02/05/2025 |
|
|
Annelien de Kat |
Gynaecoloog Amsterdam UMC |
Geen |
Geen |
Geen |
Geen onderzoeksgelden <3 jaar geleden ontvangen (in 2017 wetenschapsbeurs van de KNAW). |
Geen |
Geen |
29/04/2025 |
|
|
Arno van Peperstraten |
Gynaecoloog bij UMC Utrecht |
Geen |
Laatste drie jaar enkele keren vergoeding gastvrijheid ontvangen (Merck en Ferring), onkosten (Merck) en ook dienstverlening honorarium (Merck). |
Geen |
Geen |
Geen |
Geen |
09/05/2025 |
|
|
Frank Broekmans |
Hoogleraar Voortplantingsgeneeskunde, UMC Utrecht Gynaecoloog, Centrum voor Kinderwens, Dijklander ziekenhuis, Purmerend |
Onderwijs en advies via: FrankSchoolRforL Education - Consultation - Coaching In Human Reproductive Medicine Research manager Stichting Long Covid Waarnemend voorzitter Promoties Geneeskunde Universiteit Utrecht |
lid adviesraad Merck B.V. lid adviesraad Ferring B.V. Lid adviesraad Abbott Lid adviesraad Besins |
Geen |
Geen |
Geen |
Geen |
30/04/2025 |
|
|
Eefje Oude Lohuis |
Gynaecoloog, subspecialist voortplantingsgeneeskunde, Haaglanden Medisch Centrum Den Haag |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
13/05/2025 |
|
|
Sanne Braam |
lid werkgroep, NVOG, onbetaald. |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
29/04/2025 |
|
|
Leonie van Houten |
Gynaecoloog Amphia Ziekenhuis Breda subspecialist VPG Amphia Ziekenhuis Breda. |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
06/05/2025 |
|
|
Hans van Weering |
Gynaecoloog, subspecialist voortplantingsgeneeskunde.Rode Kruisziekenhuis BV, Beverwijk, thans WHC Amsterdam |
Geen |
Geen |
Geen |
Scratch OFO trial |
Geen |
Deels door Merck vergoede congresreis ESHRE 2019, 2022 en LH symposium 2022 (conform CGR) Deelname aan Merck Business Academy |
26/04/2025 |
|
|
Charlotte Weimar |
Gynaecoloog, Werkgever: UMC Utrecht |
Geen |
Geen |
Geen |
Geen |
Geen |
Niet bij mij bekend. Enige nog te noemen is mijn deelname (dec 2022) aan de ESHRE campus course ("Implantation failure, recurrent pregnancy loss and endometrial disorders" ) omdat die reis deels gefinancierd werd door Ferring BV. |
12/05/2025 |
|
|
Mèlanie van IJsselmuiden |
Gynaecoloog, Isala Zwolle |
Geen |
Geen |
Geen |
Ik heb van enkele farmaceuten een kleine financiële bijdrage gekregen voor het drukken van mijn proefschrift in de zomer van 2020 (niet gerelateerd aan OHSS) |
Geen |
Geen |
13/05/2025 |
|
|
Sietske Gaykema |
Treant zorggroep gynaecoloog |
Commissie onderwijs nvog |
Geen |
Geen |
Geen |
Geen |
Geen |
05/05/2025 |
|
|
Esther van Duinen |
Fertiliteitsarts, 36 uur per week. Betaald. Sint Antonius Ziekenhuis. |
Voorzitter van VVF (Vereniging van Fertiliteitsartsen). Niet betaald. |
Geen financieel voordeel derhalve ik zelf niets te maken heb met de financiën van mijn praktiserend instituut (het ziekenhuis) of mijn afdeling. |
Geen |
Geen |
Geen |
Geen |
28/04/2025 |
|
|
Marloes Vermeulen (tot november 2024) |
Freya, medewerker externe relaties |
Verloskundige 1e lijn. |
Geen |
Geen |
Geen |
Geen. |
Geen. |
27/09/2022 |
|
|
Simone Sinjorgo |
Parttime medewerker patiëntenperspectief bij Freya (14 uur, betaald). Betrokken bij richtlijnontwikkeling en onderzoek op het gebied van fertiliteit (OFO, OHSS, mannelijke subfertiliteit) ter vertegenwoordiging van het patiëntenperspectief. |
Lichaamsgericht psychosociaal therapeut (zzp, eigen praktijk in Dongen-Vaart, geregistreerd bij RBCZ). Daarnaast docent psychosociale bijscholing voor therapeuten en vrouwencoach-opleiding (betalingen via eigen praktijk) |
Geen |
Geen |
Geen |
Geen |
Geen |
27/04/2025 |
|
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door de Patiëntenfederatie Nederland en FREYA uit te nodigen voor de schriftelijke knelpunteninventarisatie, en door deelname van een afgevaardigde van FREYA in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De richtlijn is tevens voor commentaar voorgelegd aan Patientfederatie Nederland en FREYA en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
| Module |
Uitkomst raming |
Toelichting |
|
Cabergoline in de preventie van OHSS |
geen financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5.000 patiënten) en zal daarom naar verwachting geen substantiële financiële gevolgen hebben voor de collectieve uitgaven. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Zoekstrategie
Embase.com - 9 oktober 2023
|
No. |
Query |
Results |
|
#1 |
'ovary hyperstimulation'/exp OR (((ovar* OR ovulation) NEAR/3 (hyperstimulation OR stimulation OR overstimulation OR induc*)):ti,ab,kw) OR ohss:ti,ab,kw OR 'in vitro fertilization'/exp OR ((('in vitro' OR extracorporeal) NEAR/3 (fertilisation OR fertilization)):ti,ab,kw) OR ivf:ti,ab,kw OR 'intracytoplasmic sperm injection'/exp OR 'intracytoplasmic sperm injection*':ti,ab,kw OR 'intra cytoplasmic sperm injection*':ti,ab,kw OR icsi:ti,ab,kw OR 'ovulation induction'/exp OR 'superovulation'/exp OR superovulation:ti,ab,kw OR 'super ovulation':ti,ab,kw OR hyperovulation:ti,ab,kw OR 'hyper ovulation':ti,ab,kw OR 'infertility therapy'/exp OR (('assisted reproduct*' NEAR/3 (techn* OR therap* OR treatment*)):ti,ab,kw) OR (((fertilit* OR infertilit*) NEAR/3 (therap* OR treatment*)):ti,ab,kw) OR (((oocye* OR egg*) NEAR/3 (preparat* OR process* OR vitrificat* OR retriev*)):ti,ab,kw) |
206398 |
|
#2 |
'cabergoline'/exp OR 'cabaser*':ti,ab,kw OR 'cabergolin*':ti,ab,kw OR 'dostinex':ti,ab,kw OR 'galastop':ti,ab,kw OR 'dopamine receptor stimulating agent'/exp OR ((dopamin* NEAR/3 (agent* OR agonist*)):ti,ab,kw) OR 'ergoline derivative'/exp OR 'ergoline'/exp OR 'ergolin*':ti,ab,kw |
250436 |
|
#3 |
#1 AND #2 |
1515 |
|
#4 |
#3 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
1115 |
|
#5 |
#4 AND [2000-2023]/py |
626 |
|
#6 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
967213 |
|
#7 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
3887247 |
|
#8 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
7867992 |
|
#9 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
14472008 |
|
#10 |
#5 AND #6 - SR |
84 |
|
#11 |
#5 AND #7 NOT #10 - RCT |
125 |
|
#12 |
#5 AND (#8 OR #9) NOT (#10 OR #11) - Observationeel |
114 |
|
#13 |
#10 OR #11 OR #12 |
323 |
Ovid/Medline - 9 oktober 2023
|
# |
Searches |
Results |
|
1 |
Ovarian Hyperstimulation Syndrome/ or ((ovar* or ovulation) adj3 (hyperstimulation or stimulation or overstimulation or induc*)).ti,ab,kf. or ohss.ti,ab,kf. or exp Fertilization in Vitro/ or ((in vitro or extracorporeal) adj3 (fertilisation or fertilization)).ti,ab,kf. or ivf.ti,ab,kf. or exp sperm injections, intracytoplasmic/ or intracytoplasmic sperm injection*.ti,ab,kf. or intra cytoplasmic sperm injection*.ti,ab,kf. or icsi.ti,ab,kf. or exp Ovulation Induction/ or exp superovulation/ or superovulation.ti,ab,kf. or super ovulation.ti,ab,kf. or hyperovulation.ti,ab,kf. or hyper ovulation.ti,ab,kf. or (assisted reproduct* adj3 (techn* or therap* or treatment*)).ti,ab,kf. or ((fertilit* or infertilit*) adj3 (therap* or treatment*)).ti,ab,kf. or ((oocyte* or egg*) adj3 (preparat* or process* or vitrificat* or retriev*)).ti,ab,kf. |
101531 |
|
2 |
exp Ergolines/ or Dopamine Agonists/ or cabaser*.ti,ab,kf. or cabergolin*.ti,ab,kf. or dostinex.ti,ab,kf. or galastop.ti,ab,kf. or (dopamin* adj3 (agent* or agonist*)).ti,ab,kf. or ergolin*.ti,ab,kf. |
40856 |
|
3 |
1 and 2 |
457 |
|
4 |
3 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
383 |
|
5 |
limit 4 to yr=2000-2023 |
172 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
697610 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2640644 |
|
8 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4548180 |
|
9 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5526305 |
|
10 |
5 and 6 - SR |
21 |
|
11 |
(5 and 7) not 10 - RCT |
39 |
|
12 |
(5 and (8 or 9)) not (10 or 11) - Observationeel |
29 |
|
13 |
10 or 11 or 12 |
89 |