Foam-echo
Uitgangsvraag
Is een foam-echo even betrouwbaar voor tubadiagnostiek als hysterosalpingografie (HSG) met contrast?
Aanbeveling
Bespreek dat een HSG en foam-echo even betrouwbaar zijn in het vaststellen van tubapathologie.
Bespreek de verschillen in voor- en nadelen tussen HSG en foam-echo en maak samen een keuze.
Zie stroomschema Oriënterend fertiliteitsonderzoek.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Er zijn verschillende mogelijkheden om tubapathologie te diagnosticeren, namelijk minimaal invasief middels een foam-echo of HSG en meer invasief middels een diagnostische laparoscopie. Deze laatste methode is de zogenaamde gouden standaard en wordt in de literatuur als referentietest gebruikt.
Omdat algemeen beschouwd wordt dat alleen dubbelzijdige tubapathologie klinisch relevant is in het verlagen van de kans op een spontane zwangerschap, is deze vorm van tubapathologie het meest relevant om te diagnosticeren (Verhoeve, 2011).
Naast de diagnostische accuratesse van de diverse tubatesten zijn ook de bijwerkingen, ervaren pijn, de kans op een spontane zwangerschap en de kosten van belang.
Bijkomend voordeel van een foam-echo is dat de relatie van de tubae tot de ovaria bekeken kan worden. Dit is bij een HSG niet zichtbaar. Daar staat tegenover dat de vorm van het cavum uteri met een HSG beter beoordeeld kan worden. Deze twee punten worden buiten beschouwing gelaten in deze richtlijn.
In studie (Dreyer, 2014) staat duidelijk beschreven dat de hoogrisico patiënten zijn geëxcludeerd, in de andere studies staat dit niet duidelijk beschreven. Wel is het zo dat in alle geselecteerde studies de patiënten in een fertiliteitsworkup zaten en daarbij tubadiagnostiek werd verricht middels HSG en/of foam-echo, waarbij er geen indicatie was voor meer invasieve tubadiagnostiek.
In 4 van de geselecteerde studies (van Welie, 2022; Dreyer, 2014; Serrano González, 2022; Maxim, 2021) werden geen klinische of significante verschillen gevonden tussen de foam-echo en het HSG in het diagnosticeren van tubapathologie. In deze studies waren de deelnemers en zorgprofessionals niet geblindeerd voor de ingreep, dit is dan ook lastig uitvoerbaar. Daarnaast is er sprake van imprecisie (studies met lage aantallen deelnemers en lage aantallen events). De studie van Maheux-Lacroix, 2014 is een systematische review waarin foam-echo en HSG werden vergeleken met als referentietest de diagnostische laparoscopie. Ook hier werd geen verschil gezien in diagnostische accuratesse. Deze studie laat zien dat sensitiviteit en specificiteit voor foam-echo (respectievelijk 0.95 en 0.93) vergelijkbaar zijn met de sensitiviteit en specificiteit voor HSG (respectievelijk 0.94 en 0.92).
Op basis van de literatuursamenvatting kan geconcludeerd worden dat bij subfertiele vrouwen de foam-echo vergelijkbaar lijkt met het HSG wat betreft het aantonen dan wel uitsluiten van uni- en bilaterale tubapathologie. Dit betekent dat het in de klinische praktijk niet uit lijkt te maken of gekozen wordt voor een foam-echo of een HSG om de diagnose tubapathologie meer of minder waarschijnlijk te maken.
In 4 van de studies (van Welie, 2022; Dreyer, 2014; Serrano González, 2022; Maxim, 2021), met in totaal 1331 patiënten geïncludeerd, is tevens gekeken naar de ervaren pijn van de tubatest. Ondanks de eerder genoemde beperkingen ten aanzien van blindering en imprecisie, lijkt de foam-echo minder pijn te geven dan een HSG, met een verschil in pijnscore op een visual analogue scale (VAS) van -2.99 (95% -3.93 tot -2.04). Dit verschil in ervaren pijn kan klinisch relevant zijn en is van belang om te bespreken met de patiënt. Belangrijk om te vermelden is dat in de studie van Van Welie (2022) paracetamol of een NSAID vooraf aan de ingreep werd gegeven en in de studie van Maxim, (2021) en Dreyer (2014) geen pijnmedicatie vooraf werd gegeven. Bij Maxim (2021) werd er verbale anesthesie toegepast tijdens de ingreep. In de studie van Serrano Gonzalez (2022) is het wel of niet gebruik van pijnmedicatie vooraf niet beschreven. Het innemen van pijnmedicatie vooraf aan tubadiagnostiek kan van invloed zijn op de ervaren pijn en dient meegenomen te worden in de counseling met de patiënt.
Tot slot is het verschil in bijwerkingen maar in 1 studie onderzocht (Maxim, 2021). Hierbij is gekeken naar een vagale reactie op de procedure. Er is een statistisch significant verschil gevonden, maar mede gezien de lage aantallen van events kan hier geen betrouwbare uitspraak over gedaan worden. Opvallend is dat niet is gekeken naar ongewenste effecten zoals infectie of contrastembolie. Dit kan verklaard worden doordat dit weinig tot zelden voorkomt.
Ook de kans op een spontane zwangerschap is maar in 1 studie onderzocht (Dreyer, 2014), waardoor ook hier geen betrouwbare uitspraak over gedaan kan worden. In de literatuursearch zijn geen uitkomsten gevonden over kans op miskraam of EUG, effect op de neonaat en het verschil in kosten.
Kwaliteit van bewijs
De overall kwaliteit van bewijs is zeer laag tot laag, vanwege de beperkingen ten aanzien van blindering en aantallen geïncludeerde patiënten en aantallen events. Dit betekent dat we onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaat.
Er is afgewaardeerd vanwege ernstige:
- Risk of Bias: er zijn in de studies methodologische beperkingen met name betreft blindering van deelnemers en assessors/personeel, mogelijke selectiebias en het is niet altijd duidelijk hoe de uitvoering van de (volgorde van de) interventie is gegaan. Dit geldt voor alle 5 de geïncludeerde studies (Maheux-Lacroix, 2014; van Welie, 2022; Dreyer, 2014; Serrano González, 2022; Maxim, 2021).
- Inconsistentie ten aanzien van de resultaten die hebben gerapporteerd over pijn bij de ingreep (van Welie, 2022; Dreyer, 2014; Serrano González, 2022; Maxim, 2021).
- Imprecisie ten aanzien van de resultaten over ervaren pijn bij de ingreep, aangezien we deze zelf hebben berekend en imprecisie ten aanzien van het aantonen van tubapathologie in 4 van de studies vanwege een zeer klein aantal events bij een kleine steekproefgrootte (van Welie, 2022; Dreyer, 2014; Serrano González, 2022; Maxim, 2021). Dit laatste geldt ook ten aanzien van de rapportage over kans op spontane zwangerschap (Dreyer, 2014).
Waarden en voorkeuren van patiënten (en eventueel hun partner)
De gevonden resultaten laten zien dat er geen verschil lijkt te zijn tussen foam-echo en HSG ten aanzien van diagnostische accuratesse. Wel is er mogelijk een verschil in ervaren pijn van de ingreep, waarbij de foam-echo minder pijnlijk lijkt. Bijwerkingen en de kans op een spontane zwangerschap zijn onvoldoende onderzocht om hier een betrouwbare uitspraak over te doen. Als sprake is van een indicatie om onderzoek naar tubapathologie te verrichten, is het van belang om in de spreekkamer bovenstaande uitkomsten te bespreken en samen met de patiënt te beslissen welke vorm van tubadiagnostiek verricht zal worden.
Gelijkheid ((health) equity/equitable)
Op dit moment is in vrijwel alle Nederlandse klinieken die fertiliteitszorg aanbieden de mogelijkheid aanwezig om een HSG te verrichten. Als die mogelijkheid er niet is, wordt verwezen naar een andere kliniek voor het uitvoeren van een HSG. Nog niet alle klinieken hebben de mogelijkheid om een foam-echo uit te voeren. Dit aspect kan leiden tot mogelijke ongelijkheid in de zorg, waarbij het van belang lijkt dat zorgprofessionals zorgen voor een meer gelijke beschikbaarheid van beide vormen van tubadiagnostiek.
Aanvaardbaarheid
Ethische aanvaardbaarheid
De interventies lijken beide aanvaardbaar voor de betrokkenen. Er zijn geen ethische bezwaren.
Duurzaamheid
Bij beide interventie kunnen de duurzaamheidsaspecten een rol spelen, er valt hier te denken aan gebruik van (disposable) materiaal en het gebruik van röntgenstraling bij een HSG. Er is geen onderzoek verricht naar de verschillen in duurzaamheid bij beide interventies.
Haalbaarheid
De interventies lijken haalbaar en zijn over het algemeen al standaardzorg in de praktijk.
In de literatuur hebben we geen betrouwbare onderzoeken kunnen vinden die de kosten van een foam-echo hebben vergeleken met de kosten van een HSG. We kunnen daarom geen uitspraak doen over het verschil in kosten.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Als er een indicatie is voor tubadiagnostiek is de voorkeur dit zo minimaal invasief mogelijk te verrichten. De twee bestudeerde vormen van weinig invasieve tubadiagnostiek zijn hysterosalpingografie (HSG) en foam-echo. In de literatuur worden geen verschillen gevonden in de diagnostische accuratesse van beide vormen van tubadiagnostiek (foam-echo en HSG). Er zijn nog nauwelijks studies beschikbaar die bijwerkingen en het verschil in de kans op spontane zwangerschap hebben beschreven. Er werd wel een verschil gevonden in de ervaren pijn, echter was er verschil in de premedicatie die vooraf werd gegeven en de (verbale) anesthesie tijdens de interventie wat maakt dat het bewijs voor dit verschil onzeker is.
De werkgroep adviseert om bij een indicatie voor tubadiagnostiek samen met de patiënt te beslissen of er een foam-echo of HSG verricht wordt en de genoemde verschillen mee te nemen in deze counseling.
Eindoordeel:
Zwakke aanbeveling: Bespreken van de opties voor tubadiagnostiek.
- Een foam-echo is even betrouwbaar voor tubadiagnostiek als hysterosalpingografie (HSG) met contrast.
- Bespreek met vrouwen die een indicatie voor tubadiagnostiek hebben de voor- en nadelen van een foam-echo en een HSG en maak samen een keuze.
- Neem de volgende overwegingen mee in de counseling tussen een foam-echo of HSG:
- Bespreek dat er geen verschil is tussen foam-echo en HSG in diagnostische accuratesse.
- Bespreek dat er mogelijk minder pijn ervaren wordt bij een foam-echo vergeleken met een HSG.
- Benoem dat het niet duidelijk is of er verschil tussen foam-echo en HSG wat betreft bijwerkingen en kans op spontane zwangerschap.
- Bespreek dat er geen gegevens bekend zijn over het verschil in effect op neonaat en kans op miskraam of EUG bij de foam-echo en HSG.
Onderbouwing
Foam ultrasound, also called hystero-salpingo-foam sonography (HyFoSy), and Hystero-salpingo-contrast sonography (HyCoSy), is an alternative diagnostic tool for checking tubal patency. Foam ultrasound is increasingly used as diagnostic test and seems to be less painful than hysterosalpingography (HSG). In this PICO we investigate reliability (diagnostic value) of HyFoSy (foam ultrasound) compared to HSG. Moreover, side effects and chance of spontaneous pregnancy are investigated.
Population: Women from sub fertile couples at low risk for tubal pathology
Intervention: foam ultrasound
Comparator: HSG
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Conclusions |
|
|
HSG |
foam ultrasound |
||||
|
Side effects (important) |
Based on data from 56 participants in 1 study
|
15 per 100 |
0 per 100 |
Very low Due to serious risk of bias (open-label) and due to very serious imprecision (low event rate)1 |
We are uncertain whether foam ultrasound increases or decreases side effects (Maxim, 2021) |
|
Chance of spontaneous pregnancy (important) |
Based on data from 28 participants in 1 study
|
32 per 100 |
34 per 100 |
Very low Due to serious risk of bias and very serious imprecision2 |
We are uncertain whether foam ultrasound has influence on the chances of a spontaneous pregnancy (Dreyer, 2014) |
|
Pain (important) |
Measured by: VAS Scale: 1.0 - 10.0 Lower better Based on data from 1331 participants in 4 studies
|
Range |
Range |
Very low Due to very serious risk of bias, serious inconsistency, and very serious imprecision.3 |
We are uncertain whether foam ultrasound increases or decreases pain (van Welie, 2022; Dreyer, 2014; Serrano González, 2022; Maxim, 2021) |
|
Difference: MD -2.99 lower (CI 95% -3.93 lower - -2.04 lower) |
|||||
|
Diagnostic accuracy (specificity) (critical) |
Measured by: Scale: 0 - 1 High better Based on data from 528 participants in 9 studies
|
0.93 (95% CI: 0.74 – 0.99) |
0.92 (95% CI: 0.87 – 0.95) |
Low Due to very serious risk of bias4 |
Foam ultrasound may have little or no difference on diagnostic accuracy (specificity) (Maheux-Lacroix, 2014) |
|
Diagnostic accuracy (sensitivity) (critical) |
Measured by: Scale: 0 - 1 High better Based on data from 528 participants in 9 studies
|
0.94 (95% CI: 0.74 – 0.99) |
0.95 (95% CI: 0.78 – 0.99) |
Low Due to very serious risk of bias5 |
Foam ultrasound may have little or no difference on sensitivity of the diagnostic accuracy (Maheux-Lacroix, 2014) |
|
Detection of tubal pathology (critical) |
Based on data from 1331 participants in 4 studies
|
No clinical or significant differences were found in tuba obstructions when using either foam ultrasound or HSG |
Very low Due to risk of bias, and very serious imprecision and inconsistency6 |
We are uncertain whether foam ultrasound increases or decreases detection of tuba pathology (van Welie, 2022; Dreyer, 2014; Serrano González, 2022; Maxim, 2021) |
|
1. Risk of Bias: serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias; Imprecision: very serious. Only data from one study with few patients and few to zero events;
2. Risk of Bias: serious. No information provided on how and if assessors and participants were blinded; Imprecision: very serious. Data from only one study with few patients and few events;
3. Risk of Bias: very serious. Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias, Incomplete data and/or large loss to follow up, Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias; Inconsistency: serious. The magnitude of statistical heterogeneity was high, with I^2:89 %.; Imprecision: very serious. due to recalculating the mean (SD) and a lack of subgroup analysis in a cross-over design;
4. Risk of Bias: very serious. due to many areas of the Risk of bias and applicability concerns based on QUADAS-2 being labeled as unclear.;
5. Risk of Bias: very serious. due to many areas of the Risk of bias and applicability concerns based on QUADAS-2 being labeled as unclear.;
6. Risk of Bias: serious. Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias; Inconsistency: serious. due to not being able to pool the studies; Imprecision: very serious. Low number of patients and low number of events.
Description of studies
A total of five studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 1. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Maheux-Lacroix (2014) performed a systematic review with meta-analysis on the accuracy of hysterosalpingosonography (sono-HSG), representing foam ultrasound, for diagnosing tubal occlusion in subfertile women and how it performs compared with hysterosalpingography (HSG). The systematic review did not provide information about whether a CAT was performed among patients in the included studies. In nine studies representing 582 women and 1055 tubes, all participants underwent HSG in addition to sono-HSG and laparoscopy, allowing direct comparison of the accuracy of sono-HSG and HSG. Studies were searched in Medline, Embase, Cochrane Library and the Web of Science from inception to 14 November 2012. Biosis was used to identify relevant abstracts and conference proceedings. Only studies using exclusively laparoscopy as reference standard were included.
Van Welie (2022) conducted a multicenter, prospective, comparative noninferiority trial of hysterosalpingo-foam sonography (HyFoSy) versus hysterosalpingography (HSG), with randomization of couples with discordant test results. Women included in this study were infertile, between 18 and 41 years and scheduled for tubal patency testing during their fertility work-up. All women underwent both tubal patency tests in a randomized order. Of the 1160 consenting women that were assigned to undergo the two tubal patency tests, 1026 received both tests and were included in the analysis. The sample included patients with high- and low risk for tubal pathology. Data regarding risk for tubal pathology was available for 888 women, of whom 135 (15%) had a high risk.
Dreyer (2014) conducted a two-center, prospective, open-label, randomized, controlled trial comparing tubal testing by HyFoSy versus HSG. Inclusion criteria were women aged 18 – 41 years who had a valid indication for tubal patency testing as part of their fertility workup according to the Dutch NVOG guidelines. Women with a high risk for tubal pathology were excluded. In total, 40 women were enrolled in the study and randomized to receive either the HyFoSy procedure or the HSG. No form of premedication was given before tubal patency testing.
Serrano González (2022) conducted a prospective multicenter study with the consecutive data of 210 women. The inclusion criteria were women aged 18–40 years undergoing assisted reproduction that required a tubal patency test, including women with a male partner and a history of sterility/ infertility (have not achieved ongoing pregnancy leading to live birth after at least a year of attempt), women with a female partner and single women who wished to become pregnant. Patients were premedicated with oral azithromycin (1 g) the night before the test, and with a step 1 WHO Pain Ladder drug (Aneker, 2021) 1 h before the test. Among the study population were patients with medical history related to the internal genital tract (0% versus 8.4% in the HSG and HyFoSy group respectively). Previous abdominopelvic surgery was reported in both groups (26.8% versus 36.5% in the HSG and HyFoSy group respectively).
Maxim (2021) conducted a prospective, intervention case-control study. Inclusion criteria were: female patients aged between 18-40 years with a history of infertility, previously uninvestigated for uterine or tubal anomalies, presenting to the fertility center for an initial diagnostic work-up. Whether patients were tested for chlamydia antibodies was not reported. A total of 56 patients were randomized. Women in both groups did not receive any pain medication before undergoing the procedure and no antibiotic therapy was
prescribed.
Table 1. Characteristics of included studies
*For further details, see risk of bias table in the appendix
† For the studies included in the systematic review of Maheux-Lacroix (2014) the RoB is based on the risk of bias and applicability concerns of the studies based on QUADAS-2 presented in the supplementary data of the systematic review. When ≥ 3 of the areas were labeled as unclear, the overall RoB was unclear.
VAS: Visual Analogue Scale
Results
(Diagnostic accuracy of) unilateral or bilateral tubal pathology – Critical outcome
All studies reported on the outcome (Diagnostic accuracy of) unilateral or bilateral tubal pathology. This outcome is split into diagnostic accuracy and the detection of tubal pathology.
Diagnostic accuracy (sensitivity and specificity)
The systematic review of Maheux-Lacroix (2014) compared the diagnostic accuracy between sono-HSG and HSG and found no statistically significant differences between the two techniques (p=0.4). The laparoscopy was used as a reference test. For sono-HSG, pooled estimates of sensitivity and specificity were 0.95 (95% CI: 0.78–0.99) and 0.93 (95% CI: 0.89–0.96), respectively. For HSG, pooled estimates of sensitivity and specificity were 0.94 (95% CI: 0.74–0.99) and 0.92 (95% CI: 0.87–0.95), respectively. The differences between the estimated sensitivity and specificity between HSG and sono-HSG were not clinically relevant. There is no mention of inconclusive test results for either sono-HSG or HSG.
Detection of tubal pathology
Four studies reported the outcome detection of tubal pathology, without using a reference test (van Welie (2022); Dreyer (2014); Serrano González (2022); Maxim (2021)). We only report the amount of tubal pathologies detected per studies. There is no certainty whether a higher detection rate of tubal pathology also means a better diagnostic accuracy since, due to the lack of a reference test, no information was provided on the amount of false positive and false negative test results. Overall, there seems to be no large difference in the detection of tubal pathology when comparing the foam ultrasound to HSG.
Van Welie (2022) compared the results between HyFoSy and HSG. Of the 1026 women that underwent HyFoSy, 129 (13%) had a test result of tubal pathology, either one-sided tubal pathology (n=90, 9%) or double-sided tubal pathology (n=39, 4%). Of the 1026 women that underwent HSG, 134 (13%) had a test result of tubal pathology, either one-sided tubal pathology (n=104, 10%) or double-sided tubal pathology (n=28, 3%). The proportion of women with one-or dual-sided pathology was comparable (13% vs. 13%).
Dreyer (2014) reported the outcome conclusion after tubal testing which had four levels: both tubes patent, unilateral proximal occlusion, bilateral proximal occlusion or other. Two of the 19 (11%) women that underwent HyFoSy appeared to have a unilateral proximal occlusion compared to 1 of the 20 (5%) women that underwent HSG. None of the 19 women that underwent HyFoSy appeared to have a bilateral proximal occlusion compared to 1 of the 20 (5%) women that underwent HSG.
Serrano González (2022) reported the results for tubal patency. Bilateral obstruction was found in 8 of the 107 (7.5%) women in the HyFoSy group and in 3 of the 82 (3.7%) women in the HSG group (p = 0.267).
Maxim (2021) reported the unilateral and bilateral obstruction in the study groups. Three of the 29 (10.3%) women in the HyCoSy and 3 of the 27 (11.1%) women in the HSG had an unilateral obstruction (p=1), whereas 2 of the 29 (6.9%) women in the HyCoSy and 5 of the 27 (18.5%) women in the HSG had a bilateral obstruction (p=0.2).
Chance of spontaneous pregnancy – important outcome
Dreyer (2014) reported the prognostic chance in percentage on natural conception during 12 months following the tubal pathology test. This chance on natural conception was 34.3% (IQR 18.8) in women who underwent HyFoSy (based on 16 patients) and 32.3% (IQR 19.2) in women who underwent HSG (based on 12 patients) (p=0.60).
Side effects – important outcome
Maxim (2021) reported the side-effects in both treatments. In the HSG group, 4 of the 27 (14.8%) women reported a vagal effect compared to none of the women in the HyCoSy group of 29 women (p < 0.001). This difference is not considered clinically relevant.
Pain – Important outcome
Four of the five studies reported on the outcome pain. All studies used a pain score measured using the 1 – 10 Visual Analogue Scale (VAS), as scoring system with a range from 1 (‘no pain’) to 10 (‘pain as bad as it could possibly be’).
In the study by Van Welie (2022) VAS pain scores for HyFoSy were reported by 1003 of the 1026 women (98%) and VAS scores for HSG were reported by 953 of the 1026 women (93%). The mean VAS pain score for HyFoSy was 3.1 (SD 2.2) and the mean VAS score for HSG was 5.4 (SD 2.5). Although the mean VAS pain score of HyFoSy was not affected by the order of the tests (P = 0.57), the mean VAS pain score of HSG was higher when it was administered first, before HyFoSy (P = 0.01). Dreyer (2014) reported a lower VAS pain score for the HyFoSy procedure (median 1.7 cm IQR 2.1) compared with HSG (median 3.7 cm IQR 4.2) (P<0.01). Serrano González (2022) reported a significantly lower median VAS in the HyFoSy group (2 (P25; P75: 1; 3)) compared to the HSG group (5 (4; 8)) (p < 0.001). Maxim (2021) also reported a lower VAS score for the HyCoSy group (median: 1; P25: 1, P75: 2) compared with HSG (median: 5; P25: 4; P75: 6) (P<0.001).
All outcomes were recalculated to their mean (SD) and the pooled together, see figure 1. The mean difference in the pain score between foam ultrasound and HSG is -2.99 (95% -3.93 to -2.04). The difference in pain score between the foam ultrasound and the HSG is considered clinically relevant.
Figure 1. Forest plot of the mean difference in reported pain score in women undergoing diagnosis for tubal pathology using foam ultrasound or HSG
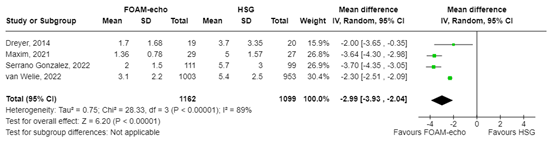
a For Dreyer (2014), Maxim (2021), and Serrano González (2022), the mean (SD) was calculated using the reported median (IQR) or median (P25;P75)
b For van Welie (2022), patients that reported their VAS pain scores are taken into this analysis twice since they received both interventions in a randomized order
A systematic review of the literature was performed to answer the following question(s):
What is the value of foam ultrasound in comparison to HSG in terms of diagnosing tubal pathology, complications of treatment and chance of spontaneous pregnancy?
| Patients | Women from infertile couples at low risk for tubal pathology |
| Intervention | Foam ultrasound |
| Control | HSG |
| Outcomes | (diagnostic accuracy of) unilateral or bilateral tubal pathology, chance of spontaneous pregnancy, , risk of miscarriage, etopic pregnancy, side effects, pain, costs |
| Other selection criteria |
Study design: systematic reviews and randomized controlled trials There is a minimal follow-up of six months for the following outcomes: chance of spontaneous pregnancy, risk of miscarriage, etopic pregnancy, and costs |
Relevant outcome measures
The guideline panel considered diagnostic accuracy of tubal pathology as a critical outcome measure for decision making; and chance of spontaneous pregnancy, risk of miscarriage, ectopic pregnancy, side effects, pain, and costs as an important outcome measure for decision making.
A priori, the guideline panel did not define the outcome measures but used the definitions used in the studies.
The guideline panel defined a 25% difference (RR < 0.8 or > 1.25) for dichotomous outcomes and 0.5 SD for continuous outcomes as a minimal clinically (patient) important difference. A 2-point difference on the 10-point Visual Analogue Scale (VAS) pain scale was considered as a minimal clinically (patient) important difference
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2011 until March 13, 2024. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 299 hits. Studies were selected based on the following criteria: studies reporting original data, systematic reviews and RCTs on foam ultrasound. Thirty-three studies were initially selected based on title and abstract screening. After reading the full text, twenty-eight studies were excluded (see the exclusion table under the tab ‘Appendices’), and five studies were included.
- Anekar AA, Hendrix JM, Cascella M. WHO Analgesic Ladder. 2023 Apr 23. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 32119322.
- Dreyer K, Out R, Hompes PG, Mijatovic V. Hysterosalpingo-foam sonography, a less painful procedure for tubal patency testing during fertility workup compared with (serial) hysterosalpingography: a randomized controlled trial. Fertil Steril. 2014 Sep;102(3):821-5. doi: 10.1016/j.fertnstert.2014.05.042. Epub 2014 Jul 1. PMID: 24996498.
- Maheux-Lacroix S, Boutin A, Moore L, Bergeron ME, Bujold E, Laberge P, Lemyre M, Dodin S. Hysterosalpingosonography for diagnosing tubal occlusion in subfertile women: a systematic review with meta-analysis. Hum Reprod. 2014 May;29(5):953-63. doi: 10.1093/humrep/deu024. Epub 2014 Feb 26. PMID: 24578476.
- Maxim AR, Gligor OH, Badea RI. Comparison of Hystero-salpingography and Hysterosalpingo-Contrast Sonography for tubal patency testing: technical success, pain perception, side effects and complications. Med Ultrason. 2021 Aug 11;23(3):283-288. doi: 10.11152/mu-2692. Epub 2021 Mar 14. PMID: 33793700.
- Serrano González L, Pérez-Medina T, Bueno Olalla B, Royuela A, De La Cuesta MLR, Saéz de la Mata D, Domínguez-Franjo E, Calles-Sastre L, Engels V. Is hysterosalpingo-foam sonography (HyFoSy) more tolerable in terms of pain and anxiety than hysterosalpingography (HSG)? A prospective real-world setting multicentre study. BMC Womens Health. 2022 Feb 13;22(1):41. doi: 10.1186/s12905-022-01606-3. PMID: 35152893; PMCID: PMC9909448.
- van Welie N, van Rijswijk J, Dreyer K, van Hooff MHA, de Bruin JP, Verhoeve HR, Mol F, van Baal WM, Traas MAF, van Peperstraten AM, Manger AP, Gianotten J, de Koning CH, Koning AMH, Bayram N, van der Ham DP, Vrouenraets FPJM, Kalafusova M, van de Laar BIG, Kaijser J, Lambeek AF, Meijer WJ, Broekmans FJM, Valkenburg O, van der Voet LF, van Disseldorp J, Lambers MJ, Tros R, Lambalk CB, Stoker J, van Wely M, Bossuyt PMM, Mol BWJ, Mijatovic V. Can hysterosalpingo-foam sonography replace hysterosalpingography as first-choice tubal patency test? A randomized non-inferiority trial. Hum Reprod. 2022 May 3;37(5):969-979. doi: 10.1093/humrep/deac034. PMID: 35220432; PMCID: PMC9071226.
- Verhoeve HR, Coppus SF, Van der Steeg JW, Steures P, Hompes PG, Boudrez P, Bossuyt PMM, Van der Veen F. Mol BWJ. The capacity of hysterosalpingography and laparoscopy to predict natural conception. Hum Reprod. 2011 Jan; 26(1):134-142. Doi 10.1093/humrep/deq263; PMID: 2108801.
Risk of bias tables
Research question: What is the value of a foam-echo in comparison to HSG in terms of diagnosing tubal pathology, complications of treatment, and chance of spontaneous pregnancy?
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Van Welie, 2022 |
Definitely yes;
Reason: randomized with computer generated randomization sequence, stratified for centre with block size 2 and 4. |
Definitely no;
Reason: Women were probably aware of which test was performed.
|
Probably no
Reason: The physician who performed the assigned test were aware of the test, however the physician who performed the second assigned test was blinded from the results of the first performed test. No information was provided on blinding of the outcome assessors and data analysts. |
Definitely yes;
Reason: Loss to follow-up was infrequent in intervention and control group. |
Definitely no;
Reason: The outcome miscarriage was not reported. |
Definitely yes;
Reason: No other problems noted |
Some concerns (all) |
|
Dreyer, 2014 |
Definitely yes;
Reason: randomized with computer-generated randomization list. |
Probably no;
Reason: No information provided |
Definitely no:
Reason: Open-label trial |
Definitely yes;
There was no loss to follow-up |
Definitely no;
Reason: Not all outcomes reported in the result section were described in the method section. |
Definitly no;
Reason: Supported by IQ medica ventures BV (producers of the intervention product) but the funders had no role in study design, data collection, and analyses, decision to publish, or preparation of the manuscript. |
High (all) |
|
Serrano Gonzalez, 2022 |
Definitely no;
Reason: no randomization performed as treatment was dependent on the different centra. |
Definitely no;
Reason: no randomization performed |
Definitely no;
Reason: no randomization performed and no information on blinding provided. |
Definitely no;
Failure in the HSG group is mainly related to tolerance factors (66.7% of test failures, 6/9); while in the HyFoSy group, the main cause was cervical stenosis (50% of test failures, 2/4) |
Definitely yes;
All relevant outcomes were reported |
Definitely no;
Recruitment bias due to lack of randomization. There was a significant difference in medical history related to the internal genital tract between the intervention and control group. |
High (all) |
|
Maxim, 2021 |
Definitely yes;
Reason: randomized by means of a sealed envelope system. |
Probably no;
Reason: no information provided |
Probably no;
Reason: no information provided |
Definitely yes;
Reason: no loss to follow up |
Definitely yes;
All relevant outcomes were reported |
Definitely yes;
Reason: no other problems noted |
Some concerns (all) |
Table of excludes studies
|
Reference |
Reason for exclusion |
|
Panchal S, Nagori C. Imaging techniques for assessment of tubal status. J Hum Reprod Sci. 2014 Jan;7(1):2-12. doi: 10.4103/0974-1208.130797. PMID: 24829524; PMCID: PMC4018793. |
Narrative review |
|
Piccioni MG, Tabacco S, Merlino L, Del Negro V, Mazzeo A, Logoteta A, Del Prete F, Riganelli L, Giannini A, Monti M. Does hysterosalpingo-foam sonography have any therapeutic effect? A systematic review. Minerva Ginecol. 2020 Feb;72(1):55-58. doi: 10.23736/S0026-4784.20.04514-1. PMID: 32153165. |
No information on selection criteria and method. Seems like narrative review. Most studies included are retrospective.
|
|
Boned-López J, Alcázar JL, Errasti T, Ruiz-Zambrana A, Rodriguez I, Pascual MA, Guerriero S. Severe pain during hysterosalpingo-contrast sonography (HyCoSy): a systematic review and meta-analysis. Arch Gynecol Obstet. 2021 Dec;304(6):1389-1398. doi: 10.1007/s00404-021-06188-3. Epub 2021 Aug 21. PMID: 34417840. |
Wrong comparison |
|
Lo Monte G, Capobianco G, Piva I, Caserta D, Dessole S, Marci R. Hysterosalpingo contrast sonography (HyCoSy): let's make the point! Arch Gynecol Obstet. 2015 Jan;291(1):19-30. doi: 10.1007/s00404-014-3465-4. Epub 2014 Sep 19. PMID: 25234517. |
Wrong comparison |
|
Exalto N, Emanuel MH. Clinical Aspects of HyFoSy as Tubal Patency Test in Subfertility Workup. Biomed Res Int. 2019 Jul 8;2019:4827376. doi: 10.1155/2019/4827376. PMID: 31360713; PMCID: PMC6644241. |
Narrative review |
|
van Welie N, Portela M, Dreyer K, Schoonmade LJ, van Wely M, Mol BWJ, van Trotsenburg ASP, Lambalk CB, Mijatovic V, Finken MJJ. Iodine contrast prior to or during pregnancy and neonatal thyroid function: a systematic review. Eur J Endocrinol. 2021 Jan;184(1):189-198. doi: 10.1530/EJE-20-0627. PMID: 33112287. |
No comparison |
|
Alcázar JL, Martinez-Astorquiza Corral T, Orozco R, Dominguez-Piriz J, Juez L, Errasti T. Three-Dimensional Hysterosalpingo-Contrast-Sonography for the Assessment of Tubal Patency in Women with Infertility: A Systematic Review with Meta-Analysis. Gynecol Obstet Invest. 2016;81(4):289-95. doi: 10.1159/000443955. Epub 2016 Jan 30. PMID: 26824833. |
Wrong comparison |
|
Saunders RD, Shwayder JM, Nakajima ST. Current methods of tubal patency assessment. Fertil Steril. 2011 Jun;95(7):2171-9. doi: 10.1016/j.fertnstert.2011.02.054. Epub 2011 Mar 31. PMID: 21457959. |
Wrong intervention and narrative review |
|
Melcer Y, Zilberman Sharon N, Nimrodi M, Pekar-Zlotin M, Gat I, Maymon R. Hysterosalpingo-Foam Sonography for the Diagnosis of Tubal Occlusion: A Systematic Review and Meta-analysis. J Ultrasound Med. 2021 Oct;40(10):2031-2037. doi: 10.1002/jum.15607. Epub 2020 Dec 28. PMID: 33368463. |
No comparison |
|
Wang R, van Welie N, van Rijswijk J, Johnson NP, Norman RJ, Dreyer K, Mijatovic V, Mol BW. Effectiveness on fertility outcome of tubal flushing with different contrast media: systematic review and network meta-analysis. Ultrasound Obstet Gynecol. 2019 Aug;54(2):172-181. doi: 10.1002/uog.20238. Epub 2019 Jun 26. Erratum in: Ultrasound Obstet Gynecol. 2019 Nov;54(5):708. doi: 10.1002/uog.21879. PMID: 30740799. |
Wrong comparison |
|
Zen M, Kirby A, Dowthwaite S, Gibson R, Mizia K. Lipiodol visibility under ultrasound. Aust N Z J Obstet Gynaecol. 2020 Aug;60(4):598-604. doi: 10.1111/ajo.13150. Epub 2020 Mar 23. PMID: 32207160. |
Wrong comparison |
|
Chunyan G, Bin P, Ping Y, Yue Z, Yang X, Hongju T, Li S, Xi X. Assessment of the Influence on Spontaneous Pregnancy of Hysterosalpingo-Contrast Sonography. Biomed Res Int. 2018 Sep 20;2018:4901281. doi: 10.1155/2018/4901281. PMID: 30327778; PMCID: PMC6171212. |
Wrong comparison |
|
Engels V, Medina M, Antolín E, Ros C, Bermejo C, Manzour N, Pelayo I, Amaro A, Martinez-Ten P, De-Guirior C, Rodríguez R, Sotillo L, Brotons I, de la Cuesta-Benjumea R, Martinez O, Sancho J, Alcázar JL. Factors Associated with a Post-Procedure Spontaneous Pregnancy after a Hysterosapingo-Foam-Sonography (HyFoSy): Results from a Multicenter Observational Study. Diagnostics (Basel). 2023 Jan 30;13(3):504. doi: 10.3390/diagnostics13030504. PMID: 36766609; PMCID: PMC9914236. |
No comparison |
|
Melcer Y, Shamir-Kaholi N, Vainer-Rotbart S, Pekar-Zlotin M, Youngster M, Gat I, Maymon R. Spontaneous pregnancy rates in infertile women after sequential hydrosonography and hysterosalpingo-foam sonography. Eur J Obstet Gynecol Reprod Biol. 2022 Apr;271:219-222. doi: 10.1016/j.ejogrb.2022.02.025. Epub 2022 Feb 24. PMID: 35231747. |
No comparison |
|
Piccioni MG, Riganelli L, Filippi V, Fuggetta E, Colagiovanni V, Imperiale L, Caccetta J, Panici PB, Porpora MG. Sonohysterosalpingography: Comparison of foam and saline solution. J Clin Ultrasound. 2017 Feb;45(2):67-71. doi: 10.1002/jcu.22412. Epub 2016 Oct 18. PMID: 27753111. |
Wrong comparison |
|
Engels V, Medina M, Antolín E, Ros C, Amaro A, De-Guirior C, Manzour N, Sotillo L, De la Cuesta R, Rodríguez R, San-Frutos L, Peralta S, Martin-Martínez A, Alcázar JL. Feasibility, tolerability, and safety of hysterosalpingo-foam sonography (hyfosy). multicenter, prospective Spanish study. J Gynecol Obstet Hum Reprod. 2021 May;50(5):102004. doi: 10.1016/j.jogoh.2020.102004. Epub 2020 Nov 23. PMID: 33242678. |
No comparison |
|
Ludwin A, Ludwin I, Banas T, Knafel A, Miedzyblocki M, Basta A. Diagnostic accuracy of sonohysterography, hysterosalpingography and diagnostic hysteroscopy in diagnosis of arcuate, septate and bicornuate uterus. J Obstet Gynaecol Res. 2011 Mar;37(3):178-86. doi: 10.1111/j.1447-0756.2010.01304.x. Epub 2011 Feb 11. PMID: 21314802. |
Wrong comparison |
|
Qu E, Zhang M, Ju J, Chen Y, Lin X, Zhang X. Is Hysterosalpingo-Contrast Sonography (HyCoSy) Using Sulfur Hexafluoride Microbubbles (SonoVue) Sufficient for the Assessment of Fallopian Tube Patency? A Systematic Review and Meta-Analysis. J Ultrasound Med. 2023 Jan;42(1):7-15. doi: 10.1002/jum.15988. Epub 2022 Apr 20. PMID: 35441714. |
No comparison |
|
Exalto N, Stassen M, Emanuel MH. Safety aspects and side-effects of ExEm-gel and foam for uterine cavity distension and tubal patency testing. Reprod Biomed Online. 2014 Nov;29(5):534-40. doi: 10.1016/j.rbmo.2014.07.015. Epub 2014 Aug 12. PMID: 25219517. |
Wrong study design and no comparison |
|
Lim SL, Jung JJ, Yu SL, Rajesh H. A comparison of hysterosalpingo-foam sonography (HyFoSy) and hysterosalpingo-contrast sonography with saline medium (HyCoSy) in the assessment of tubal patency. Eur J Obstet Gynecol Reprod Biol. 2015 Dec;195:168-172. doi: 10.1016/j.ejogrb.2015.10.008. Epub 2015 Oct 23. PMID: 26547487. |
Wrong comparison |
|
Ludwin I, Ludwin A, Wiechec M, Nocun A, Banas T, Basta P, Pitynski K. Accuracy of hysterosalpingo-foam sonography in comparison to hysterosalpingo-contrast sonography with air/saline and to laparoscopy with dye. Hum Reprod. 2017 Apr 1;32(4):758-769. doi: 10.1093/humrep/dex013. PMID: 28184447. |
Wrong comparison |
|
Ramos J, Caligara C, Santamaría-López E, González-Ravina C, Prados N, Carranza F, Blasco V, Fernández-Sánchez M. Diagnostic Accuracy Study Comparing Hysterosalpingo-Foam Sonography and Hysterosalpingography for Fallopian Tube Patency Assessment. J Clin Med. 2021 Sep 15;10(18):4169. doi: 10.3390/jcm10184169. PMID: 34575278; PMCID: PMC8466769. |
Wrong study design |
|
Robertshaw IM, Sroga JM, Batcheller AE, Martinez AM, Winter TC 3rd, Sinning K, Maxwell R, Lindheim SR. Hysterosalpingo-Contrast Sonography With a Saline-Air Device Is Equivalent to Hysterosalpingography Only in the Presence of Tubal Patency. J Ultrasound Med. 2016 Jun;35(6):1215-22. doi: 10.7863/ultra.15.08008. Epub 2016 Apr 28. PMID: 27126400. |
Wrong study design |
|
Siam, E. M. (2011). Pregnancy outcome after hystero-salpingo-contrast-sonography (HyCoSy) versus hysterosalpingography (HSG) using different contrast media. Middle East Fertility Society Journal, 16(4), 265-271. |
Many flaws, not trustworthy |
|
Xiang X, Hu B, Chen S, Wu Q, Yang Y, (2022). Comparsion on efficacy of four-dimensional hysterosalpingo-contrast sonography and hysterosalpingography for evaluation on tubal patency: Meta-analysis |
Wrong comparison |
|
Capobianco, G., & Capobianco, G. (2019). Saline infusion sonography: technique, advantages and limits for the study of uterus and fallopian tubes. Review and care pathway. |
Wrong comparison and outcome |
|
Xu, H., Wang, L., Luo, Y., Gao, X., & Tang, J. (2016). 3D hysterosalpingo-contrast sonography (3D-HyCoSy) diagnoses of tubal patency in infertile patients: a meta-analysis. Int J Clin Exp Med, 9(2), 1480-1489. |
Wrong comparison |
|
Elsharkawy, S., & El-Rheem, A. Spontaneous pregnancy rate after hysterosalpingography versus saline infusion sonogram done under high pressure: a randomized controlled trial. |
No full text available |
Beoordelingsdatum en geldigheid
Publicatiedatum : 30-10-2025
Beoordeeld op geldigheid : 07-10-2025
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met subfertiliteit.
Werkgroep
- Verhoeve H.R. (Harold) voorzitter, gynaecoloog, OLVG te Amsterdam, NVOG
- Van Dongen A.J.C.M. (Angelique), gynaecoloog, Ziekenhuis Gelderse Vallei te Ede, NVOG
- Tanahatoe S.J. (Sandra), gynaecoloog, Universitair Medisch Centrum Utrecht te Utrecht, NVOG
- Lahley E.E.L.O. (Lisa), gynaecoloog, subspecialist voortplantingsgeneeskunde, Leids Universitair Medisch Centrum te Leiden, NVOG
- Twisk M. (Moniek), gynaecoloog, BovenIJ ziekenhuis te Amsterdam, NVOG
- Van den Boogaard N.M. (Noortje), gynaecoloog, Flevoziekenhuis te Almere, NVOG
- Bailleux B.B.E.P. (Bart), klinisch chemicus endocrinoloog, Leids Universitair Medisch Centrum te Leiden, NVKC
- Bijnevelt L. (Lianne), Fertiliteitsarts, Sint Antonius Ziekenhuis te Utrecht, VVF
- Silvius A.M. (Hèlen), huisarts, Huisartsenplartijk Laila te Den Haag, NHG
- Sinjorgo S.C.H. (Simone), medewerker medewerker patientenperspectief wetenschappelijk onderzoek en richtlijnen, Freya (vanaf december 2024)
- Vermeulen M. (Marloes), medewerker patientenperspectief wetenschappelijk onderzoek en richtlijnen, Freya (tot december 2024)
- Boomsma C. (Carolien), gynaecoloog, Bravis Ziekenhuis te Roosendaal, NVOG (tot december 2023)
Met ondersteuning van
- Mostovaya I.M. (Irina), senior-adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Pepping F. (Fieke), junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Middelhuis D. (Danique), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Schultink J.M. (Janneke), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel Gemelde (neven)functies en belangen werkgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke Financiële Belangen |
Persoonlijke Relaties |
Extern gefinancierd onderzoek |
Intell. belangen en reputatie |
Overige belangen |
Datum |
Acties |
|
Harold Verhoeve (voorzitter) |
Gynaecoloog OLVG |
Lid Adviesraad Ferring (1-2 keer per jaar), betaald |
geen |
nvt |
Ik ben betrokken bij de consortiumstudies van de voortplantingsgeneeskunde, als hoofdonderzoeker op lokatie OLVG. Hier vallen alle consortium-studies onder die over de eileider testen gaan. Het consortium concept houdt in dat zoveel mogelijk Nederlands klinieken aan de studies deelnemen. Deelname aan studies is ook een kwaliteitscriterium die wordt getoetst tijdens kwaliteitsvisitaties en gestimuleerd.
1. The effectiveness of immediate versus delayed tubal flushing with oil-based contrast in women with unexplained infertility (H2Oil-timing study) study protocol of a randomised controlled trial: D. Kamphuis et al. BMC womens Health. 2023 May 6 doi:10.1186 Projectleider (nee) Externe financiering : ZonMW Periode tot 2023 (studie inclusie compleet) 2. FOil study: Effectiveness of tubal flushing with oil-based contrast during hysterosalpingography and tubal flushing by hysterosalpingo-foam sonography in infertile women undergoing fertility work-up: study protocol of a randomised controlled trial (FOil study): D.Kamphuis et al. Accepted BMJ open 2024. Projectleider (nee) Externe financiering : ZonMW Periode 2023 tot inclusie is voltooid |
geen |
geen |
24/10/2022 |
Geen restricties. Deelname aan de adviesraad is met de heer Verhoeve besproken. Hieruit bleek dat er geen producten worden gemaakt die relevant zijn voor het orienterend fertiliteitsonderzoek. |
|
Sandra Tanahatoe |
Gynaecoloog, UMC Utrecht |
geen |
geen |
geen |
geen |
geen |
geen |
23/12/2022 |
Geen restricties. |
|
Lisa Lashley |
Gynaecoloog, specialist voortplantingsgeneeskunde LUMC |
Geen |
Geen |
nvt |
Geen onderzoek waarbij de financier belang kan hebben. Het betreft de DONOR studie (onderzoek naar prognose en ontwikkeling van pre eclampsie bij eiceldonatie) en de PREMI studie (onderzoek naar effect prednisolone bij herhaalde miskramen). Hoofdonderzoeker en projectleider bij beiden studies. |
Geen |
Geen |
1/11/2022 |
Geen restricties. |
|
Angelique van Dongen |
gynaecoloog - ZGV Ede - 0.75 fte (patiëntenzorg, betaald) gynaecoloog-docent - Radboudumc Nijmegen - 0.3 fte (onderwijs, betaald) |
geen |
geen |
geen |
De H2OlieTiming studie heeft in 15 Nederlandse klinieken gelopen, waaronder de kliniek waar ik werk. Omdat ik binnen ons fertiliteitsteam de enige gynaecoloog ben met een BROKregistratie, ben ik (automatisch) de lokale hoofdonderzoeker. 1 van onze fertiliteitsartsen is betrokken bij de selectie van kandidaten en invoeren van de lokale resultaten.
Ik ben niet betrokken geweest bij de opzet van deze studie, ook niet bij het studieprotocol, niet bij de resultaten en niet bij de interpretatie hiervan. Ik heb ook geen inzage in de resultaten van deze studie m.u.v. de inclusies vanuit mijn eigen kliniek. Ik ben minimaal betrokken geweest bij de publicatie: ik ben als lokale hoofdonderzoeker mede-auteur van het artikel en heb in die hoedanigheid de laatste versie vooraf aan het submitten wel gelezen. Ik heb geen invloed gehad op de publicatie en heb hier ook geen belang bij. Overigens is Harold Verhoeve ook betrokken bij deze studie (en ook mede-auteur van het artikel).
Tenslotte krijgt onze afdeling per geïncludeerde patiënt een (onkosten)vergoeding, ikzelf ontvang geen financiering hiervoor als lokale hoofdonderzoeker. Projectleider: NEE |
geen |
geen |
28/09/2022 |
Geen restricties. Mevrouw van Dongen is als meelezer betrokken bij de uitgangsvraag waarin de H2Olie studie mogelijk wordt gebruikt, op basis van de gegeven beschrijving van betrokkenheid aan deze studie worden geen restricties opgelegd. |
|
Moniek Twisk |
Gynaecoloog BovenIJ ziekenhuis |
Lesgeven O&G opleiding deel fertiliteit Amstelacademie |
Geen |
Geen |
Geen |
Geen |
Geen |
14/09/2022 |
Geen restricties. |
|
Noortje van den Boogaard |
Gynaecoloog Flevoziekenhuis Almere |
geen |
geen |
geen |
geen |
geen |
geen |
27/09/2022 |
Geen restricties. |
|
Carolien Boomsma |
gynaecoloog Bravis ziekenhuis. |
moet instructeur bestuur endometriose werkgroep opleidingsdagen opleiding gynaecologie |
geen. |
nee |
geen |
geen |
geen |
20/09/2022 |
Geen restricties. |
|
Bart Ballieux |
Laboratoriumspecialist Klinische Chemie en Endocrinologie Afdeling KCL, LUMC, Leiden |
nvt |
geen persoonlijke financiele belangen |
Geen relevante persoonlijke relaties die van invloed kunnen zijn op mijn adviezen |
geen |
Geen intellectuele belangen bij mijn adviezen |
Geen overige belangen |
10/01/2023 |
Geen restricties. |
|
Lianne Bijnevelt |
Fertiliteitsarts, St. Antonius ziekenhuis Utrecht |
Lid VVF |
Geen |
Geen |
Geen |
Geen |
Geen |
20/10/2022 |
Geen restricties. |
|
Hèlen Silvius |
Waarnemend huisarts bij huisartsenpraktijk Laila, Hadoks en De Limes Huisarts Docent bij PHEG LUMC (functie vervalt per 01-01-2023) Huisarts Docent bij Huisartsopleiding Amsterdam UMC per 01-11-2022) |
FMS, vertegenwoordiging NHG |
Geen |
Geen |
Geen |
Geen |
Ik heb kinderen. Ik hoop dat zij in de toekomst deze richtlijn niet nodig zullen hebben maar als dat wel zo is wil ik dat hij zo goed mogelijk is. |
18/10/2022 |
Geen restricties. |
|
Simone Sinjorgo |
Parttime medewerker patientenperspectief en -participatie bij Freya (vereniging voor mensen met vruchtbaarheidsproblemen) - betaald 14 uur https://www.freya.nl/over-freya/wie-we-zijn/de-werknemers. Ter info: door mijn functie bij Freya ben ik betrokken bij diverse richtlijnontwikkeling en/of onderzoeken op het gebied van fertiliteit. In de vorm van toelichten, belichten en/of vertegenwoordigen van alleen het patiëntenperspectief tav het bepaalde onderwerp, zoals bij deze 3 richtlijnen OFO, OHSS en mannelijke subfertiliteit. |
Lichaamsgericht psychosociaal therapeut - zzp eigen praktijk in Dongen-Vaart - geregistreerd therapeut RBCZ incl. AGB-codes. www.praktijkdediamant.nl
- Psychosociaal docent Bijscholing Instituut voor therapeuten - betaling via praktijk https://bivt.nl/?s=lichaamsgericht+coachen
- Psychosociaal docent vrouwencoach opleiding - betaling via praktijk https://www.devrouwencoach.nl/vrouwencoach-opleiding/ |
Geen |
Geen |
Geen |
Geen |
Geen |
03/12/2024 |
Geen restricties. |
|
Marloes Vermeulen |
Medewerker externe relaties, Freya |
N.v.t. |
Geen. |
Nee. |
Nee. |
N.v.t. |
Geen. |
27/09/2022 |
Geen restricties, mevrouw is niet langer werkzaam bij Freya en wordt vervangen door mevrouw Sinjorgo. |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door het uitnodigen van Freya en de Patiëntenfederatie Nederland voor de invitational conference. Daarnaast zat namens Freya een afgevaardigde in de werkgroep. Het verslag van de invitational conference is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen (zie kop waarden en voorkeuren van patienten). De conceptrichtlijn is tevens voor commentaar voorgelegd aan Freya en de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Foam-echo |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling breed toepasbaar is (5.000-40.000 patiënten), volgt ook dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Voor één module (Hysteroscopie) werd een adaptatie van de internationale ESHRE-richtlijn Unexplained infertility (Romualdi 2023) uitgevoerd. De werkwijze wordt in onderstaande alineas beschreven.
Werkwijze internationale richtlijn
De methode van de internationale richtlijn is beschreven in de ESHRE-guideline manual en de ESHRE-guideline Unexplained Infertility Annex 4: Methodology (p.107-111). Hier volgt een korte samenvatting.
Zoekstrategie
De zoekstrategie, uitgevoerd door een onafhankelijke zoekspecialist, is uitgevoerd in verschillende databases. Er is gezocht in MEDLINE/PubMed en de Cochrane bibliotheek tot 24 oktober 2022.
Literatuurselectie
De literatuur is voorgeselecteerd op titel (soms ook abstract) door de ESHRE-onderzoekspecialist en de uiteindelijke abstract-full tekst-selectie is gedaan door de werkgroep. Het selectieproces en de lijst van geëxcludeerde artikelen zijn terug te vinden in ‘Annex 6 Literature study’ van de ESHRE-guideline Unexplained infertility (los document). De zoekstrategie is bij de internationale werkgroep op te vragen.
Bewijskracht
De internationale werkgroep deed allereerst een kwaliteitscheck op elke individuele studie, om de studies eruit te halen die niet relevant waren of een zeer lage bewijskracht hadden (behalve als er geen betere studies beschikbaar waren). Hiervoor werden verschillende checklists gebruikt, zoals de AMSTAR-kwaliteitschecklist voor systematische reviews. Vervolgens werden evidence-tabellen opgesteld, door middel van het standaard template van Guidelines International Network (http://www.g-i-n.net/). The GRADE-methode werd gebruikt om een evidence-profiel op te stellen en ‘summary of findings’ tabellen. Deze zijn te vinden in ‘Annex 8 Summary of Evidence’ (los document). De kwaliteit van bewijs samen resulteerde in een ‘body of evidence’ van 4 niveaus:
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
De kwaliteit van bewijs werd beoordeeld door te beginnen met het studie design (trials of observationele studie) en vervolgens af te waarderen door factoren die de kwaliteit van bewijs verlagen en op te waarderen voor factoren die de kwaliteit van bewijs verhogen:
|
Bron van de ‘body of evidence’ |
Initiële kwaliteit van bewijs |
Factoren die de kwaliteit van bewijs verlagen |
Factoren die de kwaliteit van bewijs verhogen |
Kwaliteit van de ‘body of evidence’ |
|
RCT’s |
Hoog |
1. Risico op bias
|
1. Groot effect |
Hoog + + + + Gemiddeld + + + - Laag + + - - Zeer laag + - - -
|
|
Observationele studies |
Laag |
Aanbevelingen
Na de selectie en samenvatting van het bewijs werden door de internationale groep aanbevelingen opgesteld. Er werden ‘sterke’ en ‘conditionele’ aanbevelingen geformuleerd. Termen als ‘recommend’ en ‘concludes to’ werden gebruikt voor sterke aanbevelingen en ‘consider’ en ‘suggest’ werden gebruikt voor conditionele aanbevelingen. Interpretatie van sterke of conditionele aanbevelingen voor patiënten, behandelaars en beleidsmakers zijn als volgt:
|
|
Sterke aanbeveling |
Conditionele aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Conceptversie en publicatie
Nadat de conceptversie gereed was, werd het review proces gestart. De beoordelaars bestonden onder andere uit coördinators en afgevaardigden van de ESHRE SIG Reproductive Endocrinology, SIG Andrology, SIG Reproductive Surgery, SIG Safety and Quality in ART and SIG Nursing and Midwifery, contactpersonen en afgevaardigden van patiëntenverenigingen en organisaties door heel Europa. Tot slot zijn ook contactpersonen van internationale en nationale verenigingen met als aandachtsgebied IVF/ICSI in Europa benaderd. De lijst met peer-beoordelaars is te vinden in Annex 5 ‘Stakeholder consultation’ (p. 112-113) van de ESHRE-richtlijnUnexplained Infertility. De richtlijn is gepubliceerd op de ESHRE-website en in ‘Human Reproduction’.
Methode adaptatie
Toetsing internationale richtlijn op geschiktheid voor adaptatie
De internationale richtlijn is getoetst op basis van de adviezen uit het adviesrapport MSR 3.0. Dit bestond uit (1) onafhankelijkheid van de richtlijn, (2) methodologische kwaliteit, (3) inschatting of het adapteren leidt tot een kosten en/of tijdsbesparing ten opzichte van het ontwikkelen van een nieuwe richtlijn. Het stappenplan ‘adaptatietraject’ uit het adviesrapport MSR 3.0 is gevolgd om de tekst uit de internationale richtlijn naar een Nederlandse versie te adapteren.
Van bewijs naar aanbeveling
De literatuursamenvattingen zijn onvertaald overgenomen van de internationale richtlijn. De internationale aanbevelingen (‘recommendations’) en overwegingen (‘justifications’) zijn kritisch beoordeeld en aangepast naar de Nederlandse situatie. Hierbij is rekening gehouden met nieuwe literatuur, die verschenen is na het uitkomen van de ESHRE-richtlijn, en raakvlak met andere Nederlandse richtlijnen. Ook is rekening gehouden met de aspecten (1) balans tussen gewenste en ongewenste effecten, (2) waarden en voorkeuren van patiënten, (3) kostenaspecten (4) gelijkheid, (5) aanvaardbaarheid (ethisch en duurzaamheid) en haalbaarheid.
Zoekverantwoording
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
'hysterosalpingo foam sonography'/exp OR 'hysterosalpingo contrast sonography'/exp OR ('hysterosalpingography'/exp AND ('contrast medium'/exp OR 'contrast enhancement'/exp OR 'contrast media':ti,ab,kw OR 'contrast medium':ti,ab,kw OR 'contrast agent*':ti,ab,kw)) OR (((hysterosalpingo* OR hysterosalpyngo* OR 'hystero salpingo*' OR 'hystero salpyngo*' OR hsg OR sonohystero* OR hysterosono* OR sonosalpingo* OR sonohysterosalpingo* OR sonohysterosalpyngo* OR 'sonohystero salpingo*' OR 'sonohystero salpyngo*' OR sonogra* OR uterosalpingograph*) NEAR/3 foam):ti,ab,kw) OR ((hystero* NEAR/3 contrast NEAR/3 (sonogra* OR sonosalpingo* OR echo* OR ultrasound*)):ti,ab,kw) OR ((hysterocontrast NEAR/3 sonogra*):ti,ab,kw) OR hysterocontrastsono*:ti,ab,kw OR ((sonohystero* NEAR/3 contrast*):ti,ab,kw) OR hyfosy:ti,ab,kw OR hycosy:ti,ab,kw OR 'hy co sy':ti,ab,kw |
1302 |
|
#2 |
#1 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) AND [2011-2024]/py |
404 |
|
#3 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1009437 |
|
#4 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
3989646 |
|
#5 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8118160 |
|
#6 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
14898483 |
|
#7 |
#2 AND #3 - SR |
52 |
|
#8 |
#2 AND #4 NOT #7 - RCT |
122 |
|
#9 |
#2 AND (#5 OR #6) NOT (#7 OR #8) - observationeel |
118 |
|
#10 |
#7 OR #8 OR #9 |
292 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
(exp Hysterosalpingography/ and (exp Contrast Media/ or 'contrast media'.ti,ab,kf. or 'contrast medium'.ti,ab,kf. or 'contrast agent*'.ti,ab,kf.)) or ((hysterosalpingo* or hysterosalpyngo* or 'hystero salpingo*' or 'hystero salpyngo*' or hsg or sonohystero* or hysterosono* or sonosalpingo* or sonohysterosalpingo* or sonohysterosalpyngo* or 'sonohystero salpingo*' or 'sonohystero salpyngo*' or sonogra* or uterosalpingograph*) adj3 foam).ti,ab,kf. or (hystero* adj3 contrast adj3 (sonogra* or sonosalpingo* or echo* or ultrasound*)).ti,ab,kf. or (hysterocontrast adj3 sonogra*).ti,ab,kf. or hysterocontrastsono*.ti,ab,kf. or (sonohystero* adj3 contrast*).ti,ab,kf. or hyfosy.ti,ab,kf. or hycosy.ti,ab,kf. or 'hy co sy'.ti,ab,kf. |
937 |
|
2 |
1 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
886 |
|
3 |
limit 2 to yr="2011 -Current" |
241 |
|
4 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
732082 |
|
5 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2701090 |
|
6 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4675029 |
|
7 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5643187 |
|
8 |
3 and 4 - SR |
31 |
|
9 |
(3 and 5) not 8 - RCT |
48 |
|
10 |
(3 and (6 or 7)) not (8 or 9) - observationeel |
87 |
|
11 |
8 or 9 or 10 |
166 |