Interlaminaire versus transforaminale endoscopie
Uitgangsvraag
Wat is de beste chirurgische ingreep bij patiënten met HNP?
Aanbeveling
Verwijderen van slechts het sequester indien deze wortelcompressie veroorzaakt lijkt voldoende te zijn, dit kan door middel van een open of endoscopische benadering, op basis van de literatuur is geen van de technieken superieur.
Baseer de keuze voor open of endoscopische benadering op basis van patiëntkarakteristieken, de voorkeur van patiënt en de expertise van de chirurg.
Baseer de keuze – indien bij een endoscopische benadering - voor interlaminair of transforaminaal op basis van patiëntkarakteristieken en expertise van de chirurg.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Er werden vier studies gevonden die een interlaminaire endoscopische interventie vergeleken met een transforaminale endoscopische interventie bij patiënten met lumbale hernia’s. De studies rapporteerden geen verschil tussen de TELD en IELD op de cruciale uitkomstmaten pijn en functioneren. Ook rapporteerden zij geen verschil tussen TELD en IELD op basis van de belangrijke uitkomstmaat complicaties. Geen van de studies rapporteerde over de belangrijk uitkomstmaat opioïden gebruik.
Bovenstaande informatie is afkomstig uit de systematische literatuuranalyse. Aanvullend haalt de werkgroep hieronder nog andere technische en patiëntgebonden overwegingen aan. Soms kan de locatie van de hernia danwel het niveau een rol spelen bij keuze welke techniek wordt toegepast. Ook patiëntgebonden factoren zoals roken/obesitas/scoliose kunnen een rol spelen in de keuze van een benadering/techniek. Op individuele basis kan bepaald worden welke techniek het best van toepassing is voor de betreffende patiënt.
Kwaliteit van bewijs
Interlaminaire versus transforaminale endoscopie
De overall kwaliteit van bewijs is laag. Dit betekent dat we onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten. Er is afgewaardeerd vanwege ernstige Risk of Bias: methodologische beperkingen door beperkte of afwezige blindering, en ernstige imprecisie: de optimale groepsgrootte om het gevonden effect te schatten is niet gehaald.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Indien de operateur de benaderingen gelijkwaardig acht, is het goed de voorkeur van de patiënt mee te laten spelen in de uiteindelijke behandelkeuze. In dit geval speelt samen-beslissen een grotere rol. Instrumenten om samen beslissen te ondersteunen moeten nog ontwikkeld worden. Het is nog niet bekend welke specifieke groepen baat hebben bij een specifieke benadering. Per interventie lijkt er geen verschil in bijvoorbeeld hersteltijd, heropnames of risico op complicaties.
Kostenaspecten
In een kosteneffectiviteitsstudie van Gadjradj (2021) lijken de medische kosten tussen PTED en de open techniek niet veel te verschillen. Maatschappelijk gezien leek PTED mogelijk goedkoper te zijn dan de open techniek voor de uitkomsten beenpijn en QALY’s (als het in dagbehandeling uitgevoerd kan worden). Het is volgens de werkgroep niet uit te sluiten dat dit verschil in maatschappelijke kosten wegvalt wanneer bijvoorbeeld de microdiscotomie in dagbehandeling zou uitgevoerd worden. De beperkingen van deze studie (voortijdig gestopt vanwege trage inclusie) leiden er daarnaast toe dat de werkgroep geen harde conclusies trekt uit deze resultaten.
Over de overige endoscopische technieken anders dan PTED zijn geen gerandomiseerde studies over de kosteneffectiviteit bij de werkgroep bekend.
Gezondheidsgelijkheid
De interventies zijn allemaal beschikbaar op verschillende locaties door het land heen, en leidt daarom waarschijnlijk niet tot gezondheidsongelijkheid. Beide interventies zijn onderdeel van het basispakket.
Aanvaardbaarheid
Ethische aanvaardbaarheid
De interventie lijkt aanvaardbaar voor de betrokkenen. De werkgroep ziet geen ethische bezwaren.
Duurzaamheid
Bij de interventie spelen duurzaamheidsaspecten een rol; bij PTED wordt gebruik gemaakt van meer disposables.
Haalbaarheid
Voor de endoscopische interventies bestaat een leercurve waar rekening mee gehouden dient te worden. Voor de besluitvorming rond de introductie van endoscopische technieken verwijst de werkgroep naar de leidraad NIKP: Nieuwe interventies in de Klinische Praktijk (Orde van Medisch Specialisten, 2014). Daarnaast verwijst de werkgroep voor de haalbaarheid naar de brief van de betreffende beroepsgroepen (NOV, NVvN) aan Zorginstituut Nederland. Hierin worden onder andere onderwerpen omtrent training/scholing/randvoorwaarden, leercurve, evaluatie van zorguitkomsten en financiële risico’s benoemd.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
De werkgroep baseert zich bij de aanbevelingen op gevonden literatuur waarin geen superioriteit voor een van de interventies is aangetoond. Daarnaast spelen kosten en duurzaamheid en de leercurve een rol in de overwegingen, maar deze aspecten zijn niet van doorslaggevende waarde in het formuleren van de aanbevelingen.
Onderbouwing
Both minimally invasive techniques (minimally invasive discectomy) and endoscopic techniques for hernia removal (e.g., PTED) can be performed either through the middle of the spine (intralaminarly) or from the side (transforaminally). The choice depends on the location of the hernia, but there is a gray area where both intralaminar and transforaminal approaches are defensible options. Currently, it is unclear what the position of both approaches is within the Dutch guidelines compared to the current standard. Therefore, the question arises which approach is recommended in this case.
Summary of findings
PICO 2. Interlaminar endoscopy (IELD) versus transforaminal endoscopy (TELD)
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
||
|
IELD |
TELD |
|||||
|
Pain (critical)
|
Measured by: Visual analogue scale. (Scale: 0 – 10) Lower is better Based on data from 351 participants in 4 studies |
Pain was defined by the visual analogue scale in all studies. However, follow-up time differed from 4 weeks to over 2 years and the definition of pain location was not equal between studies. Therefore, studies were not pooled. However, none of the studies showed any clinically important difference. |
Low GRADE Due to serious risk of bias, and serious imprecision1 |
IELD might result in little to no difference in pain when compared with TELD in individuals with lumbar hernia. (Nie, 2016, Mo, 2019, Chen, 2022, Zhang, 2022) |
||
|
Functioning (critical)
|
Measured by: Oswestry Disability Index. (Scale: 0 – 100) Lower is better. Based on data from 351 participants in 4 studies. |
Difference: MD 1.20 higher in favor of the TELD group (CI 95% 1.19 lower to 3.59 higher) |
Low GRADE Due to serious risk of bias, and serious imprecision1 |
IELD might result in little to no difference in function when compared with TELD in individuals with lumbar hernia. (Nie, 2016, Mo, 2019, Chen, 2022, Zhang, 2022) |
||
|
Complications (important)
|
Risk ratio 1.09 (CI 95% 0.15 to 8.07) Based on data from 233 participants in 3 studies |
43 per 1000 |
47 per 1000 |
Low GRADE Due to serious risk of bias and serious inconsistency2 |
IELD might result in little to no difference in complications when compared with TELD in individuals with lumbar hernia. (Nie, 2016, Mo, 2019, Chen, 2022) |
|
|
Difference: 4 more per 1000 in the TELD group (CI 95% 37 fewer to 304 more) |
||||||
|
Opiod Use (important) |
No studies |
- |
No GRADE |
No studies reported on the effect of IELD on opiod use compared to TELD in individuals with lumbar hernia. |
||
|
Abbreviations: IELD – interlaminar endoscopic lumbar disectomy; TELD – transforaminal endoscopic lumbar discectomy |
||||||
1. Risk of Bias: serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias, Missing intention-to-treat analysis; Imprecision: serious. Optimal information size not reached for most studies.
2. Risk of Bias: serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias, Missing intention-to-treat analysis; Inconsistency: serious. Inconsistency of results.
The comparison between interlaminar and transforaminal endoscopic interventions is described in this literature summary.
Four studies were included in the analysis of the literature. Important study characteristics and results are summarized in table 3. The assessment of the risk of bias is summarized in the risk of bias tables (under the heading ‘Evidence tabellen’).
Chen (2022) compared the effectiveness of interlaminar versus transforaminal full endoscopic lumbar discectomy under local anesthesia for L5/S1 disc herniation in an RCT design with a follow-up of 24 months or longer. They included adults aged 18-70 years diagnosed with L5/S1 disc herniation confirmed by MRI and CT, who had persistent leg pain for more than two months, unresponsive to conservative treatments. Additional inclusion criteria were: only one compressed side nerve root, American Society of Anesthesiologist fitness grade I or II. Exclusion criteria were: multiple segments of lumbar disc herniation requiring surgical treatment, history of lumbar spine surgery, CT scan showing severe calcification or ossification, foraminal or extraforaminal disc herniation, other spinal pathologies such as spinal stenosis or spondylolisthesis.
Mo (2019) compared the effectiveness of interlaminar full endoscopic lumbar discectomy under general anesthesia to the transforaminal approach under local anesthesia for L5/S1 disc herniation in an RCT design with a follow-up of 16 months. They included individuals with unilateral radicular leg pain diagnosed with L5/S1 disc herniation confirmed by MRI who were unresponsive to conservative treatment for at least 3 months. Exclusion criteria were: any nonaxillar type confirmed during surgery, recurrent disk herniation, lumbar instability, intervertebral disk inflammation or tuberculosis, sever central stenosis and cauda equina syndrome.
Nie (2016) compared the effectiveness of interlaminar percutaneous endoscopic lumbar discectomy under general anesthesia to the transforaminal approach under local anesthesia for L5/S1 disc herniation in an RCT design with a follow-up of 24 months and longer. They included adults with L5/S1 disc herniation who were unresponsive to formal, conservative treatment. Exclusion criteria were: intervertebral disc inflammation or tuberculosis, recurrent disc herniation, multiple segments of disc herniation, lumbar instability and far lateral lumbar disc herniation.
Zhang (2022) compared the effectiveness of interlaminar versus transforaminal visual intervertebral foraminal endoscopy under local anesthesia for lumbar disc herniation in an RCT design with a follow-up of 4 weeks. They included individuals diagnosed with lumbar disc herniation confirmed by MRI, CT and X-ray with clinical manifestations of lower back pain or limited mobility that had no clear history of trauma. Exclusion criteria were: cardiopulmonary dysfunction, severe fracture-dislocation, thoracolumbar burst fracture, paraplegia or hemiplegia, and severe osteoporosis.
Table 3. Characteristics of included studies (interlaminar versus transforaminal)
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
Individual studies |
||||||
|
Chen, 2022 China |
N at baseline TELD: 53 | IELD: 50
Age (mean ± SD) TELD: 34.8 ± 9.1| IELD: 36.2± 8.6
Sex (% female) TELD: 46 | IELD: 47
Preop-ODI (mean ± SD) TELD: 58.7 ± 14.6 | IELD: 56.5±15.7
Preop-VAS leg (mean ± SD) TELD: 3.5 ± 1.7 | IELD: 4.8 ± 2.2† |
Lumbar disc herniation treatment for the L5-S1 segment:
Local anesthesia (1% lidocaine)
Local anesthesia (1% lidocaine) |
Mean [range]: 28.5 months [24 to 38]
Missing data at 2 y TELD: 7/53 (13%) IELD: 5/50 (10%) |
Leg pain (VAS) Functioning (ODI) Complications
|
No conflicts of interest reported
|
Some concerns/ Low (see ROB table) |
|
Mo, 2019 China |
N at baseline TELD: 39 | IELD: 41
Age (mean ± SD) TELD: 40.8 ± 12.0 | IELD: 43.3 ± 13.3
Sex (% female) TELD: 38 | IELD: 56
Preop-ODI (mean ± SD) TELD: 74.4 ± 10.3 | IELD: 76.3 ± 8.8
Preop-VAS leg (mean ± SD) TELD: 6.9±1.2 | IELD: 7.1±1.1 |
Percutaneous Endoscopic Lumbar Diskectomy for Axillar Herniation at L5-S1
General anesthesia
Local anesthesia |
TELD: 16,59 ± 4.10 months IELD: 16.71 ± 3.72 months |
Pain (VAS) Functioning (ODI) Complications |
“In the PETD group, one patient was switched to the PEID group because of pain during foraminoplasty but was finally completed successfully”
No conflicts of interest reported |
Some concerns |
|
Nie, 2016 China |
N at baseline TELD: 30 | IELD: 30
Age (mean, SD NR) TELD: 36.6 | IELD: 38.2
Sex (% female) TELD: 40 | IELD: 33
Preop-ODI (mean ± SD) TELD: 60.1 ± 13.7 | IELD: 59 ± 16
Preop-VAS leg (mean ± SD) TELD: 7.6 ±1.4 | IELD: 7.9 ± 1.4 |
Percutatneous endoscopic lumbar discectomy for L5-S1 Disc herniation
General anesthesia
Local anesthesia 0.5 % lidocaine |
27.7 months [24 to 37 months] |
Pain (VAS) Functioning (ODI) Complications
|
‘In the PETD group, one patient was switched to the PEID group because of pain during foraminoplasty but was finally completed successfully ‘
No conflicts of interest reported
|
Some concerns |
|
Zhang, 2022 China |
N at baseline TELD: 58 | IELD: 62
Age (mean ± SD) TELD: 54.3 ± 5.0 | IELD: 54.1 ± 5.1
Sex (% female) TELD: 44 | IELD: 41
Preop-ODI (mean ± SD) TELD: 60.0 ± 1.9 | IELD: 55.7 ± 2.8
Preop-VAS leg (mean ± SD) TELD: 7.8 ± 2.9 | IELD: 7.9 ± 1.8 |
Visual intervertebral foraminal endoscopy
TELD (control); transforaminal approach Local anesthesia
IELD (observation); interlaminar approach Local anesthesia
|
4 weeks |
Pain (VAS) Function (ODI
|
Short follow-up compared to other studies. |
High |
|
Abbreviations: IELD – interlaminar endoscopic lumbar disectomy; ODI -oswestry disability scale; TELD – transforaminal endoscopic lumbar disectomy; VAS – visual analogue scale; † significantly different between groups |
||||||
*For further details, see risk of bias table in the appendix
Results
1. Pain (critical)
Pain was reported by all studies and assessed with the visual analogue scale (VAS; scale of 0 to 10 with 0 representing no pain and 10 the worst pain imaginable). Mo (2019) reported on leg pain only. Zhang (2022) reported both leg and back pain. Two studies did not specify the pain location that was assessed with the VAS (Chen, 2022 and Nie, 2016). The results are presented in Figure 1. No clinically relevant differences in pain were reported between interventions.

Figure 1. Pain (leg pain, back pain and pain not specified, measured through VAS) for transforaminal versus interlaminar endoscopic interventions in patients with a herniated disc (HNP)
2. Functioning: Activities of daily living (ALD), work, social functioning (critical)
Functioning was described in all studies and assessed with the Oswestry disability scale (ODI; scale of 0 to 100 with 0 representing no disability and 100 representing 100% disability). Results are presented in Figure 2. The pooled difference was not clinically relevant.
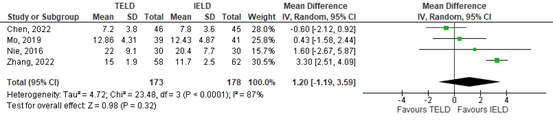
Figure 2. Functioning measured through the Oswestry Disability Index (ODI) for transforaminal versus interlaminar endoscopic interventions in patients with a herniated disc (HNP)
3. Opioid use (important)
None of the included studies reported on opioid use.
4. Complications (within 30 days and recurrences) (important)
Chen (2022) reports no surgery-related complications in either group. However, they do report on two patients in the IELD group experiencing postoperative neuropathic pain that resolved with conservative treatment.
Mo (2019) reported 5 complications (13%) in the PETD group (n=3 postoperative dysesthesia, n=1 incomplete decompression, n=1 hyperalgesia and 2 complications in the IELD group (n= 1 postoperative dysesthesia and n=1 dural tear).
Nie (2016) reported 1 complication (3%) in the PETD group (n=1 postoperative dysesthesia, and 3 (10%) in the IELD group (n= 2 postoperative dysesthesia and n=1 recurrent disc herniation).
Zhang (2022) does not report on complications.
Figure 3 displays the risk ratio for complications occurring in TELD compared to IELD.
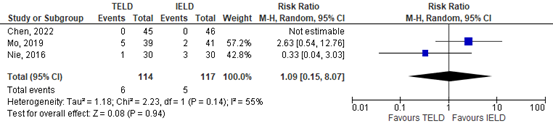
Figure 3. Risk ratio in complications between TELD and IELD
A systematic review of the literature was performed to answer the following question:
What are the positive and negative effects of interlaminar endoscopic interventions on an HNP compared to transforaminal endoscopic interventions?
Table 1. PICO
| Patients | Patients with HNP (lumbar hernias) |
| Intervention | Interlaminar endoscopy (IELD) |
| Control | Transforaminal endoscopy (TELD) |
| Outcomes | Leg pain, functioning: ADL, work, social functioning, opioid use, back pain, (procedure-related) complications (within 30 days and recurrences) |
| Other selection criteria | Study design: systematic reviews and randomized controlled trials |
Relevant outcome measures
The guideline panel considered leg pain, functioning (including ADL, work, and social functioning) as critical outcome measures for decision making; and opioid use, back-pain, (procedure-related) complications (within 30 days and recurrences) as important outcome measures for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
For determining the Minimal Clinically Important Difference (MCID), we utilized the article by Ostelo (2008), which considers a 20% to 30% improvement from the baseline measurement as a minimally clinically relevant difference (within-group change). This roughly corresponds to the values in table 3. The working group applies the same values as clinically relevant differences between groups (between-group change). Statements regarding the clinical relevance of a difference are made only if a statistically significant difference is found in an outcome measure. This was considered best estimate at the moment of this guideline development.
Table 2. Minimal Important difference (MCID) for outcomes
|
|
MCID (between group change) |
|
VAS or NRS (scale 0-10) |
2 |
|
Roland Disability Questionnaire (scale 0-24) |
5 |
|
Oswestry Disability Questionnaire (scale 0-100) |
15 |
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until January 26th, 2024. The detailed search strategy is available upon request. The systematic literature search resulted in 606 hits. Studies were selected based on the following criteria:
- Systematic reviews (searched in at least two databases, detailed search strategy, risk of bias assessment and results of individual studies available), or randomized controlled trials (RCTs).
- Studies including twenty or more participants (³ ten per arm).
- Studies with a minimum follow-up of 6 weeks.
- Studies according to PICO 1 or PICO 2 and
- Studies with English language full-text publication.
Initially, 39 studies were selected based on title and abstract screening. After reading the full text, 35 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’).
Four studies were included (Chen, 2022; Mo; 2019; Nie, 2016 and Zhang, 2022) for PICO 2.
- Chen Z, Wang X, Cui X, Zhang G, Xu J, Lian X. Transforaminal Versus Interlaminar Approach of Full-Endoscopic Lumbar Discectomy Under Local Anesthesia for L5/S1 Disc Herniation: A Randomized Controlled Trial. Pain Physician. 2022 Nov;25(8):E1191-E1198. PMID: 36375189.
- Mo X, Shen J, Jiang W, Zhang X, Zhou N, Wang Y, Hu Z, Hao J. Percutaneous Endoscopic Lumbar Diskectomy for Axillar Herniation at L5-S1 via the Transforaminal Approach Versus the Interlaminar Approach: A Prospective Clinical Trial. World Neurosurg. 2019 May;125:e508-e514. doi: 10.1016/j.wneu.2019.01.114. Epub 2019 Jan 31. PMID: 30710722.
- Nederlandse vereniging voor Neurochirurgie (NVvN) en Nederlandse Orthopaedische Vereniging (NOV). PTED- Uw verzoek tot opstellen waarborgen document en reactie op uw brief van 8 september 2021. 2021. Beschikbaar via: https://www.zorginstituutnederland.nl/binaries/zinl/documenten/brief/2021/12/16/brief-nvvv-en-nov-over-pted/Brief+NVvV+en+NOV+aan+Zorginstituut+Nederland+over+leidraad+en+voorwaarden+introductie+PTED-operatie.pdf.
- Nie H, Zeng J, Song Y, Chen G, Wang X, Li Z, Jiang H, Kong Q. Percutaneous Endoscopic Lumbar Discectomy for L5-S1 Disc Herniation Via an Interlaminar Approach Versus a Transforaminal Approach: A Prospective Randomized Controlled Study With 2-Year Follow Up. Spine (Phila Pa 1976). 2016 Oct;41 Suppl 19:B30-B37. doi: 10.1097/BRS.0000000000001810. PMID: 27454540.
- Orde van Medisch Specialisten. Leidraad NIKP: Nieuwe interventies in de Klinische praktijk. Kennisinsituut van Medisch Specialisten. 2014. Beschikbaar via: https://demedischspecialist.nl/sites/default/files/Leidraad%20Nieuwe%20interventies%20in%20de%20klinische%20praktijk%20def.pdf.
- Zhang ZH, Du Q, Wu FJ, Liao WB. Optimal approach for total endoscopic discectomy and its effect on lumbar and leg function in patients with disc herniation. World J Clin Cases. 2022 Dec 16;10(35):12928-12935. doi: 10.12998/wjcc.v10.i35.12928. PMID: 36569011; PMCID: PMC9782947.
- Zorginstituut Nederland. Standpunt Percutane transforaminale endoscopische discectomie (PTED) bij een lumbale hernia nuclei pulposi en radiculaire beenpijn. 2020. Beschikbaar via: https://www.zorginstituutnederland.nl/binaries/zinl/documenten/standpunten/2020/11/30/standpunt-pted-bij-lage-rughernia-en-uitstralende-beenpijn/Brief+MZS+met+standpunt+PTED+bij+een+lumbale+hernia+nuclei+pulposi+en+radiculaire+beenpijn.pdf.
Risk of Bias tables
Risk of bias table for intervention studies (randomized controlled trials; based on Cochrane risk of bias tool and suggestions by the CLARITY Group at McMaster University)
|
Study reference
|
Was the allocation sequence adequately generated?
|
Was the allocation adequately concealed?
|
Blinding: Was knowledge of the allocated interventions adequately prevented? |
Was loss to follow-up (missing outcome data) infrequent?
|
Are reports of the study free of selective outcome reporting? |
Was the study apparently free of other problems that could put it at a risk of bias? |
Overall risk of bias
LOW Some concerns HIGH |
|
Chen, 2022 |
Definitely yes;
Reason: Central randomization with computer generated random numbers |
Probably yes;
Reason: “And then every patient was given a serial number by another researcher according to the consecutive sequence of recruitment.” |
Definitely no.
Reason: data collectors, outcome assessors and data analyst were blinded. Patients and physicians were not blinded. |
Probably no
Reason: Loss to follow-up was around 10% at 2 years in both groups. No ITT analysis was performed. |
Definitely yes;
Reason: All relevant outcomes were reported |
Definitely yes
Reason: no other problems noted |
Some concerns (pain, functioning)/LOW
Reason: Self-reported patient measures in a non-blinded trial, no intention-to-treat analysis. |
|
Mo, 2019 |
Probably yes;
Reason: randomization through “single-blind and random alphabet methods” |
No information |
Definitely no.
Reason: Patients and physicians were not blinded. Blinding of data collectors, outcome assessors and data analyst not reported |
Probably yes
All outcomes are reported for all individuals. No loss to follow-up reported. |
Definitely yes;
Reason: All relevant outcomes were reported |
Definitely yes
Reason: no other problems noted |
Some concerns (pain, functioning)
Reason: Self-reported patient measures in a non-blinded trial. |
|
Nie, 2016 |
Probably yes;
Reason: randomization through “single-blind and random alphabet methods” |
No information |
Definitely no.
Reason: Patients and physicians were not blinded. Blinding of data collectors, outcome assessors and data analyst not reported |
Probably yes
All outcomes are reported for all individuals. No loss to follow-up reported. |
Definitely yes;
Reason: All relevant outcomes were reported |
Definitely yes
Reason: no other problems noted |
Some concerns (pain, functioning)
Reason: Self-reported patient measures in a non-blinded trial. |
|
Zhang, 2022 |
No information |
No information |
Probably no
Reason: No information on blinding reported |
Probably yes
All outcomes are reported for all individuals. No loss to follow-up reported. |
Probably no;
No information on complications is reported. |
Probably no
Reason: very short follow-up of 4 weeks for a surgical intervention |
HIGH
Reason: Self-reported patient measures in a non-blinded trial. Randomization protocol unclear. Very short follow-up. |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Guo Z, Zhang Y, Wang H, Li B. Efficacy and safety of unilateral biportal endoscopic discectomy and conventional endoscopic discectomy in the treatment of lumbar disc herniation: a systematic review and meta-analysis. Ann Palliat Med. 2023 Jan;12(1):171-180. doi: 10.21037/apm-22-1364. PMID: 36747391. |
Verkeerde vergelijking: unilateral biportal endoscopic discectomy and conventional endoscopic discectomy |
|
Bansal P, Vatkar AJ, Baburaj V, Kumar V, Dhatt SS. Effect of obesity on results of endoscopic versus open lumbar discectomy: a systematic review and meta-analysis. Arch Orthop Trauma Surg. 2023 Sep;143(9):5589-5601. doi: 10.1007/s00402-023-04870-6. Epub 2023 Apr 12. PMID: 37041263. |
obese versus non-obese patients, wrong comparison |
|
Jitpakdee K, Liu Y, Kotheeranurak V, Kim JS. Transforaminal Versus Interlaminar Endoscopic Lumbar Discectomy for Lumbar Disc Herniation: A Systematic Review and Meta-Analysis. Global Spine J. 2023 Mar;13(2):575-587. doi: 10.1177/21925682221120530. Epub 2022 Aug 21. PMID: 35993298; PMCID: PMC9972290. |
search maart 2022. beperkte RoB, en zeer beperkte search: "endoscopic, discectomy, disc herniation, PELD, transforaminal, TELD, interlaminar, and IELD" |
|
Conceição, R. T., & Santana, R. N. D. A. (2022). The microscopic and endoscopic techniques in lumbar discectomy: a systematic review. Coluna/Columna, 21(1), e246193. |
in data-analyse observationeel en RCT gecombineerd |
|
Zhang J, Gao Y, Zhao B, Li H, Hou X, Yin L. Comparison of percutaneous transforaminal endoscopic discectomy and open lumbar discectomy for lumbar disc herniations: A systematic review and meta-analysis. Front Surg. 2022 Nov 11;9:984868. doi: 10.3389/fsurg.2022.984868. PMID: 36439526; PMCID: PMC9691761. |
Beperkte RoB, beperkte search (april 20th 2022): The final search string was: “percutaneous transforaminal endoscopic discectomy” OR “open lumbar discectomy” OR “traditional discectomy” AND “lumbar disc herniation”. |
|
Li WS, Yan Q, Cong L. Comparison of Endoscopic Discectomy Versus Non-Endoscopic Discectomy for Symptomatic Lumbar Disc Herniation: A Systematic Review and Meta-Analysis. Global Spine J. 2022 Jun;12(5):1012-1026. doi: 10.1177/21925682211020696. Epub 2021 Aug 17. PMID: 34402320; PMCID: PMC9344526. |
search minder uitgebreid dan Gadjradj 2021, wel RoB... |
|
Lu H, Yao Y, Shi L. Percutaneous Endoscopic Lumbar Discectomy for Recurrent Lumbar Disc Herniation: An Updated Systematic Review and Meta-Analysis. Indian J Orthop. 2022 Apr 22;56(6):983-995. doi: 10.1007/s43465-022-00636-1. PMID: 35669028; PMCID: PMC9123128. |
search 2016, less recent than Gadjradj (2021) |
|
Zhao XM, Chen AF, Lou XX, Zhang YG. Comparison of Three Common Intervertebral Disc Discectomies in the Treatment of Lumbar Disc Herniation: A Systematic Review and Meta-Analysis Based on Multiple Data. J Clin Med. 2022 Nov 8;11(22):6604. doi: 10.3390/jcm11226604. PMID: 36431083; PMCID: PMC9696245. |
beperkte RoB (4 domeinen), beperkte search strategie gepresenteerd: "the following main key words were used: lumbar disc herniation, percutaneous transforaminal endoscopic discectomy, percutaneous endoscopic discectomy, microendoscopic discectomy, fenestration discectomy, open discectomy surgery, and controlled clinical trials, its synonyms and close synonyms, among others, to repeatedly retrieve relevant publications." |
|
Zhu, M. T., Hu, B. S., Chen, C. M., Liu, H. Q., & Lin, G. X. (2024). Comparison of Full Endoscopic Lumbar Diskectomy Using the Transforaminal Approach versus Interlaminar Approach for L5–S1 Lumbar Disk Herniation Treatment: A Meta-Analysis. Journal of Neurological Surgery Part A: Central European Neurosurgery, 85(05), 501-512. |
search 2021. RoB met Jadad, uitgesplitst. Search “percutaneous endoscopic lumbar discectomy,” “full endoscopic lumbar discectomy,” “PELD,” “FELD,” “percutaneous endoscopic transforaminal discectomy,” “percutaneous endoscopic interlaminar discectomy,” “PETD,” “PEID,” “lumbar disc herniation,” and “LDH.” Minder recent dan Jitpakdee 2022 |
|
Aiyer R, Noori S, Schirripa F, Schirripa M, Jain S, Aboud T, Mehta N, Elowitz E, Pahuta M, Datta S. A systematic review of full endoscopic versus micro-endoscopic or open discectomy for lumbar disc herniation. Pain Manag. 2022 Jan;12(1):87-104. doi: 10.2217/pmt-2021-0037. Epub 2021 Aug 23. PMID: 34420416. |
search acceptabel “Endoscopic Discectomy and Lumbar Disc”, “Endoscopic Discectomy and Lumbar Disc Herniation”, “Endoscopic Discectomy and Herniation”, “Endoscopic Discectomy and Lumbar Herniation”, “Percutaneous Discectomy and Lumbar Disc”, “Percutaneous Discectomy and Lumbar Disc Herniation”, “Percutaneous Discectomy and Lumbar Discectomy” and “Endoscopic Lumbar Discectomy”, “Minimally Invasive Discectomy and Lumbar Disc”, “Minimally Invasive Discectomy and Lumbar Disc Herniation” and “Minimally Invasive Lumbar Discectomy”. Minder recent dan Gadjradj 2022 |
|
Yang CC, Chen CM, Lin MH, Huang WC, Lee MH, Kim JS, Chen KT. Complications of Full-Endoscopic Lumbar Discectomy versus Open Lumbar Microdiscectomy: A Systematic Review and Meta-Analysis. World Neurosurg. 2022 Dec;168:333-348. doi: 10.1016/j.wneu.2022.06.023. PMID: 36527213. |
alleen complicaties PICO 1, staan ook in Gadjradj 2021 |
|
Wei FL, Li T, Gao QY, Yang Y, Gao HR, Qian JX, Zhou CP. Eight Surgical Interventions for Lumbar Disc Herniation: A Network Meta-Analysis on Complications. Front Surg. 2021 Jul 20;8:679142. doi: 10.3389/fsurg.2021.679142. PMID: 34355013; PMCID: PMC8329383. |
NMA, resultaten PELD versus OD, maar alleen in OR weergegeven. Minder recent dan Gadjradj 2022 |
|
Bai X, Lian Y, Wang J, Zhang H, Jiang M, Zhang H, Pei B, Hu C, Yang Q. Percutaneous endoscopic lumbar discectomy compared with other surgeries for lumbar disc herniation: A meta-analysis. Medicine (Baltimore). 2021 Mar 5;100(9):e24747. doi: 10.1097/MD.0000000000024747. PMID: 33655938; PMCID: PMC7939231. |
search 2018, less recent than Gadjradj (2021) |
|
He DW, Xu YJ, Chen WC, Miao XX, Wu H, Wu TL, Jia JY, Cheng XG. Meta-analysis of the operative treatment of lumbar disc herniation via transforaminal percutaneous endoscopic discectomy versus interlaminar percutaneous endoscopic discectomy in randomized trials. Medicine (Baltimore). 2021 Feb 5;100(5):e23193. doi: 10.1097/MD.0000000000023193. PMID: 33592819; PMCID: PMC7870223. |
Onduidelijk welke studiedesigns zijn meegenomen, meer dan alleen RCT. Individuele studies niet vindbaar |
|
Gadjradj PS, Harhangi BS, Amelink J, van Susante J, Kamper S, van Tulder M, Peul WC, Vleggeert-Lankamp C, Rubinstein SM. Percutaneous Transforaminal Endoscopic Discectomy Versus Open Microdiscectomy for Lumbar Disc Herniation: A Systematic Review and Meta-analysis. Spine (Phila Pa 1976). 2021 Apr 15;46(8):538-549. doi: 10.1097/BRS.0000000000003843. PMID: 33290374; PMCID: PMC7993912. |
Older search, not including newest trial |
|
Rickers KW, Pedersen PH, Tvedebrink T, Eiskjær SP. Comparison of interventions for lumbar disc herniation: a systematic review with network meta-analysis. Spine J. 2021 Oct;21(10):1750-1762. doi: 10.1016/j.spinee.2021.02.022. Epub 2021 Mar 3. PMID: 33667683. |
NMA, hier lijken trials die wel zijn meegenomen in Gadjradj (2021) zoals Dai (2020), en de studies van Tacconi in te missen. |
|
Yuan C, Zhou Y, Pan Y, Wang J. Curative effect comparison of transforaminal endoscopic spine system and traditional open discectomy: a meta-analysis. ANZ J Surg. 2020 Jan;90(1-2):123-129. doi: 10.1111/ans.15579. Epub 2019 Dec 11. PMID: 31828889. |
geen zoekstrategie gepresenteerd, gezocht op zoekwoorden 'transforaminal endoscopic spine system' |
|
Zhao XM, Yuan QL, Liu L, Shi YM, Zhang YG. Is It Possible to Replace Microendoscopic Discectomy with Percutaneous Transforaminal Discectomy for Treatment of Lumbar Disc Herniation? A Meta-Analysis Based on Recurrence and Revision Rate. J Korean Neurosurg Soc. 2020 Jul;63(4):477-486. doi: 10.3340/jkns.2019.0229. Epub 2020 May 8. PMID: 32380585; PMCID: PMC7365273. |
geen zoekstrategie gepresenteerd, gezocht op "LDH, PTED, MED, recurrence rate, residual rate, revision rate and synonyms, etc." |
|
Yin J, Jiang Y, Nong L. Transforaminal approach versus interlaminar approach: A meta-analysis of operative complication of percutaneous endoscopic lumbar discectomy. Medicine (Baltimore). 2020 Jun 19;99(25):e20709. doi: 10.1097/MD.0000000000020709. PMID: 32569205; PMCID: PMC7310843. |
minder recent dan Jitpakdee 2022 |
|
Huang Y, Yin J, Sun Z, Song S, Zhuang Y, Liu X, Du S, Rui Y. Percutaneous endoscopic lumbar discectomy for LDH via a transforaminal approach versus an interlaminar approach: a meta-analysis. Orthopade. 2020 Apr;49(4):338-349. English. doi: 10.1007/s00132-019-03710-z. PMID: 30989258. |
minder recent dan Jitpakdee 2022 |
|
Xu J, Li Y, Wang B, Lv G, Li L, Dai Y, Jiang B, Zheng Z. Minimum 2-Year Efficacy of Percutaneous Endoscopic Lumbar Discectomy versus Microendoscopic Discectomy: A Meta-Analysis. World Neurosurg. 2020 Jun;138:19-26. doi: 10.1016/j.wneu.2020.02.096. Epub 2020 Feb 26. PMID: 32109644. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Chen P, Hu Y, Li Z. Percutaneous endoscopic transforaminal discectomy precedes interlaminar discectomy in the efficacy and safety for lumbar disc herniation. Biosci Rep. 2019 Feb 15;39(2):BSR20181866. doi: 10.1042/BSR20181866. PMID: 30705086; PMCID: PMC6379230. |
onduidelijk welke studies RCTs zijn |
|
Shi R, Wang F, Hong X, Wang YT, Bao JP, Liu L, Wang XH, Xie ZY, Wu XT. Comparison of percutaneous endoscopic lumbar discectomy versus microendoscopic discectomy for the treatment of lumbar disc herniation: a meta-analysis. Int Orthop. 2019 Apr;43(4):923-937. doi: 10.1007/s00264-018-4253-8. Epub 2018 Dec 13. PMID: 30547214. |
onduidelijk welke studies RCTs zijn |
|
Barber SM, Nakhla J, Konakondla S, Fridley JS, Oyelese AA, Gokaslan ZL, Telfeian AE. Outcomes of endoscopic discectomy compared with open microdiscectomy and tubular microdiscectomy for lumbar disc herniations: a meta-analysis. J Neurosurg Spine. 2019 Sep 6;31(6):802-815. doi: 10.3171/2019.6.SPINE19532. PMID: 31491760. |
geen uitgebreide zoekstrategie gepresenteerd: [search strategy: “(((Discectomy OR Microdiscectomy)) AND Lumbar) AND (Tubular OR tube OR endoscop*)”]. |
|
Yu P, Qiang H, Zhou J, Huang P. Percutaneous Transforaminal Endoscopic Discectomy versus Micro-Endoscopic Discectomy for Lumbar Disc Herniation. Med Sci Monit. 2019 Mar 30;25:2320-2328. doi: 10.12659/MSM.913326. PMID: 30927349; PMCID: PMC6452773. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Kim M, Lee S, Kim HS, Park S, Shim SY, Lim DJ. A Comparison of Percutaneous Endoscopic Lumbar Discectomy and Open Lumbar Microdiscectomy for Lumbar Disc Herniation in the Korean: A Meta-Analysis. Biomed Res Int. 2018 Aug 7;2018:9073460. doi: 10.1155/2018/9073460. PMID: 30175149; PMCID: PMC6106715. |
geen RCTs, verkeerd design |
|
Li WS, Yan Q, Cong L. Comparison of Endoscopic Discectomy Versus Non-Endoscopic Discectomy for Symptomatic Lumbar Disc Herniation: A Systematic Review and Meta-Analysis. Global Spine J. 2022 Jun;12(5):1012-1026. doi: 10.1177/21925682211020696. Epub 2021 Aug 17. PMID: 34402320; PMCID: PMC9344526. |
PTED versus fenestration discectomy, verkeerde controlegroep |
|
Zhang B, Liu S, Liu J, Yu B, Guo W, Li Y, Liu Y, Ruan W, Ning G, Feng S. Transforaminal endoscopic discectomy versus conventional microdiscectomy for lumbar discherniation: a systematic review and meta-analysis. J Orthop Surg Res. 2018 Jul 5;13(1):169. doi: 10.1186/s13018-018-0868-0. PMID: 29976224; PMCID: PMC6034279. |
Transforaminal endoscopic discectomy versus conventional microdiscectomy. Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020), Choi (2018), Chang (2018), Xu (2020) |
|
Qin R, Liu B, Hao J, Zhou P, Yao Y, Zhang F, Chen X. Percutaneous Endoscopic Lumbar Discectomy Versus Posterior Open Lumbar Microdiscectomy for the Treatment of Symptomatic Lumbar Disc Herniation: A Systemic Review and Meta-Analysis. World Neurosurg. 2018 Dec;120:352-362. doi: 10.1016/j.wneu.2018.08.236. Epub 2018 Sep 8. PMID: 30205219. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Phan K, Xu J, Schultz K, Alvi MA, Lu VM, Kerezoudis P, Maloney PR, Murphy ME, Mobbs RJ, Bydon M. Full-endoscopic versus micro-endoscopic and open discectomy: A systematic review and meta-analysis of outcomes and complications. Clin Neurol Neurosurg. 2017 Mar;154:1-12. doi: 10.1016/j.clineuro.2017.01.003. Epub 2017 Jan 8. PMID: 28086154. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Cong L, Zhu Y, Tu G. A meta-analysis of endoscopic discectomy versus open discectomy for symptomatic lumbar disk herniation. Eur Spine J. 2016 Jan;25(1):134-143. doi: 10.1007/s00586-015-3776-6. Epub 2015 Jan 30. PMID: 25632840. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Fan, L., Shu, T., Wang, Q. Y., Wu, C. Z., Xu, Y. C., & Chen, X. X. (2016). Percutaneous endoscopic lumbar discectomy as the new standard surgery in disc herniation: a meta-analysis. Int J Clin Exp Med, 9(8), 16283-16291. |
verkeerde vergelijking (Percutaneous endoscopic lumbar discectomy (PELD) versus microendoscopic discectomy (MED)) |
|
Peng, K., Zou, J., Chen, L., Wang, H., Peng, J., & Liao, Q. (2016). Percutaneous endoscopic lumbar discectomy versus conventional discectomy for lumbar disc herniation. Int J Clin Exp Med, 9(7), 12678-12686. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Li, X., Hu, Z., Cui, J., Han, Y., Pan, J., Yang, M., ... & Li, L. (2016). Percutaneous endoscopic lumbar discectomy for recurrent lumbar disc herniation. International Journal of Surgery, 27, 8-16. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Ruan W, Feng F, Liu Z, Xie J, Cai L, Ping A. Comparison of percutaneous endoscopic lumbar discectomy versus open lumbar microdiscectomy for lumbar disc herniation: A meta-analysis. Int J Surg. 2016 Jul;31:86-92. doi: 10.1016/j.ijsu.2016.05.061. Epub 2016 May 31. PMID: 27260312. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Li, X., Han, Y., Di, Z., Cui, J., Pan, J., Yang, M., ... & Li, L. (2016). Percutaneous endoscopic lumbar discectomy for lumbar disc herniation. Journal of Clinical Neuroscience, 33, 19-27. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
|
Rasouli MR, Rahimi-Movaghar V, Shokraneh F, Moradi-Lakeh M, Chou R. Minimally invasive discectomy versus microdiscectomy/open discectomy for symptomatic lumbar disc herniation. Cochrane Database Syst Rev. 2014 Sep 4;2014(9):CD010328. doi: 10.1002/14651858.CD010328.pub2. PMID: 25184502; PMCID: PMC10961733. |
Missende trials: Tao (2018), Tacconi (2019), Tacconi (2020), Dai (2020) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 02-06-2026
Beoordeeld op geldigheid : 02-06-2026
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodules is in 2023 een multidisciplinair cluster ingesteld. Het cluster Wervelkolomgerelateerde aandoeningen bestaat uit meerdere richtlijnen. De actuele indeling welke richtlijn in welk cluster valt is hier te vinden, en op de startpagina’s van elke richtlijn staat aangegeven hoe de modules uit dit cluster zich inhoudelijk tot elkaar verhouden. De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepleden brengen hun expertise in, indien nodig. De volgende personen uit het cluster zijn betrokken geweest bij de herziening van deze module:
Clusterstuurgroep
- Dr. V. ter Wengel (voorzitter), neurochirurg, Spaarne Gasthuis/ Haaglanden Medisch Centrum, Haarlem en Den Haag (NVvN)
- Drs. L. Elzinga, anesthesioloog-pijnspecialist, Bravis Ziekenhuis (NVA)
- Drs. M.P.C. van Woensel, revalidatiearts, Stichting Spine& Joint Centre, Rotterdam (VRA)
- Drs. M.E. Havinga, orthopedisch chirurg, OCON (NOV)
- Dr. M.F. Boomsma, radioloog, Isala, Zwolle (NVvR)
- Drs. M. Liedorp, neuroloog, Kliniek Lange Voorhout, Rijswijk (NVN)
Leden betrokken bij de module Beste ingreep HNP (stuur- en expertisegroepleden):
- Dr. D.H.R. Kempen, orthopedisch chirurg, OLVG/ Amsterdam UMC, Amsterdam (NOV)
- Dr. R. Post, neurochirurg, Amsterdam UMC, Amsterdam (NVvN)
- Drs. M. Liedorp, neuroloog, Kliniek Lange Voorhout, Rijswijk (NVN)
Leden betrokken bij de module Preoperatieve adviezen en oefentherapie (stuur- en expertisegroepleden):
- Drs. G.L. van Anrooij-Jochemsen, ergotherapeut, Fysiotherapiepraktijk Bardoel van Lier, Hilversum (EN)
- Drs. M.G. Mooren, oefentherapeut Mensendieck, Zorgwaard, Heerhugowaard (VvOCM)
- Drs. M.P.J. Melief, fysiotherapeut, VMfysio, Amsterdam (KNGF)
- Dr. V. ter Wengel, neurochirurg, Spaarne Gasthuis/ Haaglanden Medisch Centrum, Haarlem en Den Haag (NVvN)
Met ondersteuning van:
- Dr. M.M.J. van Rooijen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten Utrecht
- Drs. B. Vogelaar, adviseur, Kennisinstituut van de Federatie Medisch Specialisten Utrecht
Belangenverklaringen
Een overzicht van de belangen van de clusterleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Clusterstuurgroepleden
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Extern gefinancierd onderzoek |
Overige belangen (intellectueel, persoonlijke relaties en financiële belangen) |
Restrictie |
|
Boomsma |
Radioloog, Isala |
onderwijs, wetenschap, regionalisering |
Onderzoek samen met:
Geen persoonlijke vergoedingen ontvangen. Een enkele keer research grant ontvangen voor aanstelling van een promovendus. |
Geen |
Geen restricties * |
|
Elzinga |
Anesthesioloog-Pijnspecialist, Bravis Ziekenhuis |
Bestuurslid Sectie Pijn en Palliatieve Geneeskunde NVA. Reiskostenvergoeding enkele maal per jaar. |
Geen |
Geen |
Geen restricties |
|
Havinga |
Orthopedisch chirurg, OCON |
Geen |
Geen |
Geen |
Geen restricties |
|
Liedorp |
Neuroloog, Kliniek Lange Voorhout, Rijswijk (0.6 FTE) |
(alle onbetaald) |
Geen |
Geen |
Geen restricties |
|
Ter Wengel (voorzitter) |
|
Stuurgroeplid Cluster trauma Knowledge forum AO Spine spinal cord injury |
D SCIRET studie (effect timing chirurgie op neurologisch letsel bij traumatische wervelkolomletsels) – Principal investigator
Financiering: CSRS; Rapenburg race; EANS |
Geen |
Geen* |
|
van Woensel |
Revalidatiearts,Stichting Spine & Joint Centre Rotterdam |
Revalidatiearts Capri Hartrevalidatie Revalidatiegeneeskundige expertises via MediLibra |
Geen |
Geen |
Geen restricties |
* De commercieel gesponsorde onderzoeken vallen buiten de afbakening van de richtlijnmodules
Betrokken clusterexpertisegroepleden Beste ingreep HNP
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Extern gefinancierd onderzoek |
Overige belangen (intellectueel, persoonlijke relaties en financiële belangen) |
Restrictie |
|
Kempen |
OLVG (1 FTE) Amsterdam UMC (0.05 FTE) |
Geen |
Alle vergoedingen voor het onderzoek gaan naar ziekenhuizen. |
Geen |
Geen restricties * |
|
Post |
|
Geen |
FONDS NUTS OHRA: RCT naar tranexaminezuur bij patiënten na een SAB |
Geen |
Geen restricties* |
|
Voogt |
Voorzitter patiëntenvereniging NVVR de Wervelkolom |
Geen |
Geen |
namens de NVVR de Wervelkolom heb ik zitting in werkgroepen richtlijnontwikkeling |
Geen restricties |
* De commercieel gesponsorde onderzoeken vallen buiten de afbakening van de richtlijnmodules
Betrokken clusterexpertisegroepleden Preoperatieve adviezen en oefentherapie
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Extern gefinancierd onderzoek |
Overige belangen (intellectueel, persoonlijke relaties en financiële belangen) |
Restrictie |
|
Anrooij |
Ergotherapeut bij Fysiotherapiepraktijk Bardoel van Lier; locatie Villa Overbosch in Hilversum (Korian) |
Geen |
Geen |
Geen |
Geen restricties |
|
Melief |
Praktijk eigenaar en fysio-/manueeltherpeut |
Geen |
Geen |
Geen |
Geen restricties |
|
Mooren |
Oefentherapeut Mensendieck, werkzaam als zelfstandige bij praktijk Zorgwaard in Heerhugowaard. |
Manager/ voorzitter bij Coöperatieve Vereniging Rug-netwerk UA (2 dagen per week, deels betaalde functie, deels vrijwilligerswerk) |
Project ZiN: Zinnige Zorg voor klachten vanuit de lage rug, 2021 Project ZiN: Ketenrichtlijn Lage rugklachten, 2022, staat on hold. Beide ZiN projecten op vrijwilligersbasis, geen vacatievergoeding. |
|
Geen restricties |
|
Voogt |
Voorzitter patiëntenvereniging NVVR de Wervelkolom |
Geen |
Geen |
namens de NVVR de Wervelkolom heb ik zitting in werkgroepen richtlijnontwikkeling |
Geen restricties |
Inbreng patiëntenperspectief
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerden de clusterleden conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Beste ingreep HNP - Interlaminaire versus transforaminale endoscopie |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft]. Er worden daarom geen substantiële financiële gevolgen verwacht.
|
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Cluster Wervelkolomgerelateerde aandoeningen |
|
|
Uitgangsvraag/modules: UV1 Wat is de beste chirurgische ingreep bij patiënten met HNP? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 26 januari 2024 |
|
Periode: vanaf febr 2016 (vorige search) |
Talen: geen restrictie |
|
Literatuurspecialist: Alies Oost |
Rayyan review: https://rayyan.ai/reviews/911562 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl:9777/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen:
De sleutelartikelen worden gevonden met deze search |
|
|
Te gebruiken voor richtlijntekst: In de databases Embase.com en Ovid/Medline is op 26 januari 2024 systematisch gezocht naar systematische reviews en RCTs over endoscopische technieken voor het opereren van een HNP. De literatuurzoekactie leverde 606 unieke treffers op. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
208 |
139 |
231 |
|
RCT |
345 |
166 |
375 |
|
Totaal |
553 |
305 |
606* |
*in Rayyan
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
('intervertebral disk hernia'/exp OR 'intervertebral disk'/exp OR 'radiculopathy'/exp) AND ('hernia'/de OR 'lumbar vertebra'/exp OR 'back'/exp OR lumb*:ti,ab,kw) OR 'sciatica'/exp OR 'sciatic neuropathy'/exp OR (((radicul* OR lumboradicul*) NEAR/5 syndrome*):ti,ab,kw) OR ((herniat* NEAR/1 disc*):ti,ab,kw) OR ((herni* NEAR/2 pulposi*):ti,ab,kw) OR ((herni* NEAR/1 lumb*):ti,ab,kw) OR ((lumbar:ti,ab,kw OR vertebrae:ti,ab,kw OR vertebra:ti,ab,kw) AND hernia*:ti,ab,kw AND (disc*:ti,ab,kw OR disk*:ti,ab,kw OR prolapse*:ti,ab,kw)) OR (((lumbosacral OR lumbar) NEAR/5 radiculopath*):ti,ab,kw) OR radiculitis:ti,ab,kw OR (((herniat* OR lumb*) NEAR/3 (disc* OR disk*)):ti,ab,kw) OR ((radicular NEAR/1 symptom*):ti,ab,kw) OR ((lumb* NEAR/3 radiculopath*):ti,ab,kw) OR 'lumbar nerve root':ti,ab,kw OR sciatica:ti,ab,kw |
73965 |
|
#2 |
'endoscopy'/exp OR 'endoscopic surgery'/exp OR 'percutaneous discectomy'/exp OR endoscop*:ti,ab,kw OR endosurg*:ti,ab,kw OR ped:ti,ab,kw OR pted:ti,ab,kw OR peld:ti,ab,kw OR ield:ti,ab,kw OR (((percutaneous OR interlaminar OR intralaminar OR transforaminal) NEAR/3 (diskectom* OR discectom* OR decompression)):ti,ab,kw) |
1045312 |
|
#3 |
#1 AND #2 |
4264 |
|
#4 |
#3 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
3569 |
|
#5 |
#4 AND [01-02-2016]/sd |
2187 |
|
#6 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
997121 |
|
#7 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
3959541 |
|
#8 |
#5 AND #6 - SR |
208 |
|
#9 |
#5 AND #7 NOT #8 - RCT |
345 |
|
#10 |
#8 OR #9 |
553 |
|
#11 |
35190388:ui OR 31703056:ui OR 29303469:ui OR 30175149:ui OR l2027243521 |
5 |
|
#12 |
#10 AND #11 – sleutelartikelen worden gevonden |
5 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
((exp Intervertebral Disc Displacement/ or exp Intervertebral Disc/ or exp Radiculopathy/) and (Hernia/ or exp Lumbar Vertebrae/ or exp Back/ or lumb*.ti,ab,kf.)) or exp Sciatica/ or exp Sciatic Neuropathy/ or ((radicul* or lumboradicul*) adj5 syndrome*).ti,ab,kf. or (herniat* adj1 disc*).ti,ab,kf. or (herni* adj2 pulposi*).ti,ab,kf. or (herni* adj1 lumb*).ti,ab,kf. or ((lumbar or vertebrae or vertebra) and hernia* and (disc* or disk* or prolapse*)).ti,ab,kf. or ((lumbosacral or lumbar) adj5 radiculopath*).ti,ab,kf. or radiculitis.ti,ab,kf. or ((herniat* or lumb*) adj3 (disc* or disk*)).ti,ab,kf. or (radicular adj1 symptom*).ti,ab,kf. or (lumb* adj3 radiculopath*).ti,ab,kf. or 'lumbar nerve root'.ti,ab,kf. or sciatica.ti,ab,kf. |
40738 |
|
2 |
exp Endoscopy/ or exp Diskectomy, Percutaneous/ or endoscop*.ti,ab,kf. or endosurg*.ti,ab,kf. or ped.ti,ab,kf. or pted.ti,ab,kf. or peld.ti,ab,kf. or ield.ti,ab,kf. or ((percutaneous or interlaminar or intralaminar or transforaminal) adj3 (diskectom* or discectom* or decompression)).ti,ab,kf. |
544404 |
|
3 |
1 and 2 |
2995 |
|
4 |
3 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
2884 |
|
5 |
4 and 20160201:20240126.(dt). |
1650 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
721881 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2682623 |
|
8 |
5 and 6 - SR |
139 |
|
9 |
(5 and 7) not 8 - RCT |
166 |
|
10 |
8 or 9 |
305 |
|
11 |
("35190388" or "31703056" or "29303469" or "38171312" or "30175149").ui. |
5 |
|
12 |
10 and 11 – sleutelartikelen worden gevonden |
5 |