Screeningsinstrumenten
Uitgangsvraag
Welk signaleringsinstrument kan gebruikt worden voor het signaleren en herkennen van geweld in afhankelijkheidsrelaties bij volwassenen van 18 tot 65 jaar op de spoedeisende hulp (SEH)?
Aanbeveling
Let tijdens het consult op de spoedeisende hulp op verschillende signalen (risicofactoren, waarnemingen) van geweld in afhankelijkheidsrelaties bij volwassenen.
Bouw een signaleringsvraag in in het EPD ter bewustwording tijdens het consult, bijvoorbeeld “Is er een vermoeden op de aanwezigheid van geweld in afhankelijkheidsrelaties?”.
Zorg voor adequate en periodieke scholing van het zorgpersoneel.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Het is aangetoond dat het gebruik van signaleringsinstrumenten leidt tot het ontdekken van meer gevallen van geweld in afhankelijkheidsrelaties bij volwassenen (Nelson, 2004; Morrison, 2000). Het gebruik van een signaleringsinstrument wordt dan ook aangeraden op de spoedeisende hulp (SEH). In deze richtlijn willen we gaan onderzoeken welk signaleringsinstrument het beste te gebruiken is op de SEH in Nederland.
In deze literatuursamenvatting werd een systematische review geïncludeerd die de sensitiviteit en specificiteit van verschillende signaleringsinstrumenten voor geweld in afhankelijkheidsrelaties bij volwassenen, gedefinieerd als ‘intimate partner violence’, rapporteerde. De review was een update voor de US Preventive Services Task Force en includeerde alleen artikelen uit landen met een vergelijkbaar (zorg)systeem als Amerika. Van de geïncludeerde signaleringsinstrumenten werden de PVS, OVAT, STaT, OAS en AAS gebruikt in de acute zorg of op de spoedeisende hulp. De PVS onderzoekt of er sprake is van geweld in afhankelijkheidsrelaties bij volwassenen in het afgelopen jaar; de andere instrumenten laten zien of er sprake is van geweld in afhankelijkheidsrelaties op het moment van afnemen.
Tabel 1 geeft een overzicht van de sensitiviteit en specificiteit van de instrumenten.
Tabel 1. Overzicht van de range in sensitiviteit en specificiteit van de instrumenten

In het algemeen is de kwaliteit van het bewijs laag. De onderzoeken gebruiken een andere gouden standaard ter vergelijking, wat de interpretatie en het vergelijken van de uitslagen beïnvloed. Daarnaast zijn niet alle onderzoeken uitgevoerd op de SEH, is een smaller definitie gebruikt voor geweld in afhankelijkheidsrelaties (namelijk ‘intimate partner violence’) en verschilt het (zorg)systeem vaak veel van die van Nederland.
Op basis van de cruciale uitkomstmaat sensitiviteit, zouden de STaT en AAS worden geprefereerd. Echter is de specificiteit van deze instrumenten laag, wat betekent dat er mensen positief worden gescreend op mishandeling, maar dat er in werkelijkheid geen sprake is van mishandeling (veel foutpositieven).
Op basis van de belangrijke uitkomstmaat specificiteit, zou de OAS worden geprefereerd, maar deze heeft een lage sensitiviteit. Dit betekent dat er veel mensen zullen zijn die negatief gescreend worden, maar in werkelijkheid wel geweld in afhankelijkheidsrelaties plaatsvindt (veel foutnegatieven). Met de lage sensitiviteit is het als signaleringsinstrument in de praktijk niet optimaal.
De WAST is minder goed bruikbaar, omdat deze gaat over de aanwezigheid van geweld in afhankelijkheidsrelaties in het afgelopen jaar in plaats van op het moment zelf.
Daarom wordt op basis van zowel de sensitiviteit als specificiteit de OVAT geprefereerd. Echter de bewijskracht van de psychometrische accuratesse van de OVAT is laag, wat met name wordt veroorzaakt door risico op vertekening in de studies geïncludeerd in de review en de lage aantallen patiënten.
Als we kijken naar de praktijk, zou bij gebruik van de STaT en AAS het aantal foutpositieven hoog zijn. Dit zou betekenen dat veel patiënten die op de SEH zijn, die niet worden mishandeld, volgens het instrument wel positief gescreend worden. Dit zorgt voor veel onterechte onrust en wellicht sociale gevolgen. Tevens zorgt het voor extra werk voor zowel de zorgprofessional als Veilig Thuis. Bij gebruik van de OAS zullen er veel gevallen van geweld gemist worden door de lage sensitiviteit. Dit is als signaleringsinstrument niet wenselijk. Voor de praktijk lijkt de OVAT het meest geschikt, echter is de beoordeling van de bewijskracht laag. Bij voorkeur zou dit instrument moeten worden onderzocht in grotere patiënten aantallen.
Als conclusie kunnen wij trekken dat er geen geschikt instrument is tot op heden voor de signalering van geweld in afhankelijkheidsrelaties bij volwassenen op de SEH, met in bijzonder voor het Nederlands zorgsysteem.
Het advies van de werkgroep is om bij het ontbreken van een juist signaleringsinstrument de beslissing tot het komen tot een melding te baseren op signalen die worden waargenomen tijdens het consult, bijvoorbeeld signalen uit de anamnese en lichamelijk onderzoek. De signalen bij slachtoffers zijn complex. Kennis van de signalen helpt om de kans op geweld in afhankelijkheidsrelaties goed in te schatten. Aanwezigheid van één risicofactor wil niet automatisch zeggen dat er sprake móét zijn van geweld in afhankelijkheidsrelaties, maar wel dat er een verhoogde kans is dat dit gebeurt (Verwijs, 2012). Naarmate er meer signalen worden waargenomen, neemt de overtuiging toe dat er mogelijk sprake is van deze vorm van geweld, wat kan leiden tot een vermoeden. Uit onderzoek blijkt ook dat hoe meer risicofactoren er aanwezig zijn, hoe hoger de kans is op geweld in afhankelijkheidsrelaties (McCauley, 1995).
De signalen voor geweld in afhankelijkheidsrelaties bestaan uit risicofactoren en waarnemingen. Wees alert dat tijdens het lichamelijk onderzoek letsels bedekt kunnen zijn, bijvoorbeeld bij gebruik van make-up, of onder kleding, sieraden of een pruik (Guth, 2000).
Helaas ontbreken specifieke signalen en risicofactoren voor geweld in afhankelijkheidsrelaties. Wel zijn er algemene risicofactoren en waarnemingen om op te letten tijdens het consult: (Campell, 2002; Gazmararian, 1996; Guth, 2000; Hegarty, 2004; McCauley, 1995; Reijnders, 2006; Verwijs, 2012)
Risicofactoren pleger:
- Onder 35 jaar
- Laag opleidingsniveau, werkeloosheid
- Gedwongen huwelijk, relatieproblemen, (dreiging met) verstoting of echtscheiding
- (problematisch) Alcohol/drugsmisbruik
- Pleger/getuige/slachtoffer geweest van geweld
- Aanraking criminele circuit, afpersing, chantage
- Psychiatrische aandoening (persoonlijkheidsstoornis)
- Mishandeling van huisdieren
- Geestelijke/lichamelijke handicap
Risicofactoren slachtoffer:
- Pleger/getuige/slachtoffer geweest van geweld
- Psychiatrische aandoening (persoonlijkheidsstoornis, depressie, angststoornis)
- (problematisch) Alcohol/drugsmisbruik
- Slecht ervaren lichamelijke gezondheid, laag zelfbeeld, weinig zelfvertrouwen
- Laag opleidingsniveau, laag inkomen, geen betaald werk
- Gedwongen huwelijk, relatieproblemen, (dreiging met) verstoting of echtscheiding
- Zwangerschap, het hebben van kinderen, dreigen met afpakken kinderen
Waarnemingen:
- Het tijdverschil tussen het ontstaan van het letsel en het zoeken naar hulp
- Letsels die niet kloppen met het verhaal, inconsistentie in het verhaal
- Afwerende reacties, geen open communicatie, vermijden oogcontact
- Overbezorgde partner
- Partner antwoordt voor patiënt, maakt afspraken en ziet erop toe dat patiënt niet alleen gezien wordt
- Herhaalde bezoeken bij huisarts/SEH in verband met lichamelijke klachten
- Veelvuldig onverklaarbare klachten
- Hoge medische consumptie binnen maar vooral buiten kantooruren
- Uitstellen of afzeggen van (herhalings)afspraken
- Het hebben van multipele verwondingen, oude letsels of letsels in diverse stadia van genezing, afweerletsel, letsel gelaat borst hals extremiteiten
- Slechte verzorging
- Onder invloed van alcohol of drugs op het consult verschijnen
- Geen oppas kunnen regelen
Als er tijdens het consult een vermoeden op geweld in afhankelijkheidsrelaties is, volg dan de stappen van de KNMG-meldcode (KNMG, 2023). Overleg zo nodig met de huisarts, indien er twijfels zijn of als een duidelijker beeld van de thuissituatie wenselijk is. Vraag uit of er zorg wordt gedragen voor minderjarige kinderen, de zogenaamde “Kind-check”. Als er zorg wordt gedragen voor minderjarige kinderen, volg de richtlijn voor kindermishandeling.
Ook is het advies van de werkgroep om in het Elektrische Patiënten Dossier (EPD) dat gebruikt wordt op de SEH, een vraag in te bouwen, zodat tijdens het consult wordt overwogen of er sprake is van geweld in afhankelijkheidsrelaties. Een voorbeeld zou kunnen zijn: “Is er een vermoeden op de aanwezigheid van geweld in afhankelijkheidsrelaties?”. Zo wordt er bewustwording gecreëerd bij het personeel.
Waarden en voorkeuren van patiënten (en eventueel hun verzorgers)
In de geneeskunde zijn de waarden en voorkeuren van een patiënt altijd belangrijk - het gaat immers om zijn of haar lichaam. Nu is dit een gevoelige kwestie, waarbij veel factoren invloed hebben op de beslissing van de patiënt om te vertellen over de geweldssituatie. De geweldpleger is iemand waar de patiënt afhankelijk van is, op welke manier dan ook. Dit brengt vaak met zich mee dat er drempel is voor de patiënt om zich over het geweld uit te spreken. Juist daarom is het belangrijk om een instrument te gebruiken waarbij de sensitiviteit hoog is, zodat er weinig gevallen gemist worden. Het doel is hiermee om de patiënt te helpen door laagdrempelig te signaleren of er sprake is van geweld in afhankelijkheidsrelaties Het is een gevoelig onderwerp om over te beginnen, je breekt immers in in iemands privé situatie. Vaak is er sprake van schaamte of schuldgevoel. Echter blijkt uit onderzoek dat vrouwen het waarderen als er begonnen wordt over het vermoeden van het bestaan van geweld in afhankelijkheidsrelatie (Bureau van de Europese Unie voor de grondrechten, 2014). Met dit in ons achterhoofd, moeten we niet terughoudend zijn om het slachtoffer te willen helpen. Het doorbreekt een taboe en de drempel voor het slachtoffer om te gaan vertellen wat haar of hem overkomt. Probeer het onderwerp bespreekbaar te maken als er voldoende aanwijzingen voor een vermoeden op geweld in afhankelijkheidsrelaties tijdens een consult op de SEH. Het is belangrijk om naar de slachtoffers te luisteren, zonder te vooroordelen. Maak duidelijk dat deze vorm van geweld nooit geoorloofd is. Tevens is het belangrijk om de vertrouwelijkheid te benadrukken en te bewaken. Indien het slachtoffer niet bekend, maar er toch een groot vermoeden is, geef dan informatie mee en maak duidelijk waar er eventueel alsnog hulp gezocht kan worden (Chang, 2005; Lo Fo Wong, 2005).
Bij deze vorm van geweld dient er sterk rekening gehouden te worden met de autonomie van het slachtoffer. Als patiënt wilsbekwaam is, en niet geholpen wil worden, moet je in eerste instantie de wens van het slachtoffer respecteren. Echter sommige situaties kunnen ervoor zorgen dat je alsnog je beroepsgeheim doorbreekt en toch een melding maakt. Er is sprake van een ‘conflict van plichten’ (KNMG, 2024). Hiervan is sprake als een concreet belang zwaarder weegt (in dit geval de ernst van de mishandeling) en met het doorbreken van het beroepsgeheim kan ernstig nadeel voorkomen worden (bijvoorbeeld ernstig letsel of zelfs de dood van slachtoffer).
Kosten (middelenbeslag)
Een signaleringsinstrument zorgt voor de (snellere) herkenning van geweld in afhankelijkheidsrelaties. Het slachtoffer kan geholpen worden en andere incidenten in de toekomst kunnen voorkomen worden, op zowel fysiek als mentaal gebied. Geweld in afhankelijkheidsrelaties heeft ernstige gevolgen voor de gezondheid (Campbell, 2002). Deze impact is cumulatief; hoe langer en ernstiger het geweld is, hoe erger de gezondheidsgevolgen (Registered Nurses' Association of Ontario, 2005). Geweld in afhankelijkheidsrelatie is geassocieerd met verhoogde mortaliteit en invaliditeit, verwondingen, slechtere algemene gezondheid, chronische aandoeningen en pijn, middelenmisbruik, fertiliteitsproblemen en zwangerschapscomplicaties (Plitcha, 2004). Er is (helaas) nog geen direct bewijs gevonden dat signalering van geweld in afhankelijkheidsrelaties leidt tot een afname van de gezondheidsgevolgen (Nelson, 2004).
Echter een instrument met een lage specificiteit zorgt voor veel foutpositieven, waardoor de kosten weer zullen stijgen, omdat er extra kosten bijkomen van zorgprofessionals die tijd kwijt zijn met de afhandeling en er bij Veilig Thuis mogelijk een hogere druk komt te liggen met alle (onnodige) onderzoeken in de thuissituatie.
De implementatie en gebruik van het instrument zorgt bij de start voor kosten. Het personeel moet geschoold worden in het gebruik van het instrument en er moeten evaluatiemomenten plaatsvinden om het gebruik van het instrument te evalueren. Een signaleringsinstrument kan een goed hulpmiddel zijn, maar kennis over deze vorm van geweld en de juiste gespreksvaardigheden zijn ook belangrijk. Scholing van het personeel en het belang om alert te zijn is van groot belang. Het moet bestaan uit feiten van deze vorm van geweld (met de risicofactoren en waarnemingen die van belang zijn het signaleren) maar ook over de juiste attitude tijdens het consult en gespreksvaardigheden. Het kan helpen om het gesprek over geweld in afhankelijkheidsrelaties te beginnen en te structureren. Tevens is het belangrijk om aandacht te hebben voor de veiligheid tijdens het consult, en de bedreiging daarvan. De scholing brengt kosten met zich mee. Tegenwoordig wordt er in de meeste opleidingen gelukkig aandacht hieraan geschonken en is het afhankelijk van de kennis van het personeel nodig om alsnog (bij)scholing te geven.
Aanvaardbaarheid, haalbaarheid en implementatie
Voor het gebruik van het signaleringsinstrument en voor goede afhandeling hiervan moet het instrument geïmplementeerd moeten in het EPD. De implementatie van een signaleringsinstrument in het EPD, indien beschikbaar, brengt hoge kosten met zich mee.
Voor start van gebruik van het gekozen signaleringsinstrument, zou met de beheerders van het EPD besproken worden hoe dit het beste te verwerken in het EPD. Het personeel moet geschoold worden en er moeten evaluatie momenten ingepland worden om het gebruikersgemak en haalbaarheid te evalueren. Dit brengt naast kosten, ook tijd met zich mee. Er moeten goede afspraken gemaakt worden bij wie de verantwoordelijkheid ligt om het signaleringsinstrument in te vullen. Tevens is het belang om iedereen nauw te betrekken om alert te zijn op signalen van geweld in afhankelijkheidsrelaties. Het belang van een goede signalering voor deze vorm van geweld moet goed duidelijk zijn.
Om de effectiviteit zo hoog mogelijk en de belasting voor de patiënt en zorgverleners zo klein mogelijk te houden, is het belangrijk om gebruik te maken van een instrument met een zo hoog mogelijke sensitiviteit en specificiteit, voor een zo laag mogelijk aantal foutpositieven en -negatieven. Om de toegankelijkheid van het signaleringsinstrument voor zorgverleners zo hoog mogelijk te houden, is het belangrijk dat het signaleringsinstrument kort en gebruiksvriendelijk is.
Indien er een geschikt signaleringsinstrument wordt geïmplementeerd en gebruikt, is het van belang dat er regelmatig een evaluatie plaatsvindt of het beoogde doel uiteindelijk bereikt wordt. Met behulp van wetenschappelijk onderzoek moet onder andere onderzocht worden of de eerder gevonden hoge sensitiviteit en specificiteit, die wenselijk is bij screening, ook daadwerkelijk met het nieuwe instrument bereikt wordt op de lange termijn.
Rationale van de aanbeveling: weging van argumenten voor en tegen de diagnostische procedure
Het gebruik van signaleringsinstrumenten voor het vroegtijdig opsporen van geweld in afhankelijkheidsrelaties is van groot belang. Hierdoor kan (vroegtijdig) hulp voor het slachtoffer ingezet worden. Hiermee worden problemen in de toekomst voorkomen, zowel of fysiek als mentaal gebied op de korte en lange termijn. Echter is er op dit moment geen betrouwbaar en gevalideerd signaleringsinstrument dat in de praktijk gebruikt kan worden. In de bestaande literatuur is er geen signaleringsinstrument met de juiste sensitiviteit en specificiteit om accuraat te kunnen opsporen. Tevens zijn alle instrumenten ontwikkeld in niet-Nederlandse zorgsystemen. Het advies van de werkgroep is om bij het ontbreken van een juist signaleringsinstrument de beslissing tot het komen tot een melding te baseren op signalen die worden waargenomen tijdens het consult. Volg vervolgens de stappen van de meldcode.
Scholing van personeel over geweld in afhankelijkheidsrelaties en de alertheid tijdens het consult op de spoedeisende hulp wordt sterk aangeraden.
Om de bewustwording te vergroten, is het advies van de werkgroep om een signaleringsvraag in het EPD in te bouwen, zodat er bij elk consult bij stil gestaan kan worden of er sprake is van geweld in afhankelijkheidsrelaties.
Onderbouwing
Achtergrond
Abuse in dependent relationships in adults between 18 and 65 years old refers to violence perpetrated by an individual upon whom the victim is dependent. This can include partners, ex-partners, family members, or family friends, often characterized by a significant power imbalance. When children are involved (even only as witnesses), the situation falls under the so called “Child-Check” of the KNMG reporting code and the child abuse directive must be followed. If the victim is 65 years or older, it is called elder abuse.
As a healthcare provider, it is crucial to recognize the signs of such violence promptly and initiate appropriate support to prevent further harm to both the patient and those around them. Currently, healthcare providers identify potential abuse based on a combination of signals including patient history, physical examination findings, risk factors, and other observations. Once abuse is suspected, the step-by-step protocol outlined in the Child Abuse and Domestic Violence Reporting Code is followed.
A key distinction between this type of violence and child abuse is the presence of volitional capacity. In cases of violence among adults, if the adult victim consciously and willingly refuses help and does not consent to further intervention, an assessment must be conducted to evaluate the risk of severe physical or psychological harm or death. Reporting is warranted only if the danger cannot be mitigated by other means.
There is currently no validated screening instrument available for this issue. Such a tool would assist professionals in considering, recognizing and identifying the possibility of abuse in dependent relationships among adults.
Conclusies / Summary of Findings
In the conclusions, the following cut-off values are used: ≥90% excellent, ≥80% <90% good, ≥70% <80% moderate, <70% poor.
Woman Abuse Screening tool (WAST)
|
Moderate GRADE |
The WAST tool likely has good sensitivity and specificity for screening on IPV in the past year, with the CAS tool as reference test.
Source: Wathen, 2008 |
Extended Hurt, Insulted, Threaten, Scream (E-HITS) Tool
|
Low GRADE |
The E-HITS tool may have moderate sensitivity and good specificity for screening on IPV in the past year, with the CTS-2 tool as reference test.
Source: Iverson, 2015 |
Hurt, Insulted, Threaten, Scream (HITS) tool
|
Low GRADE |
The HITS tool may have poor to moderate sensitivity and good specificity for screening on IPV, psychological aggression, and physical violence in the past year, with the CAS tool as reference test.
Sources: Iverson, 2015; Iverson, 2013, Mills, 2006 |
Partner Violence Screen (PVS) tool
|
Low GRADE |
The PVS tool may have poor to moderate sensitivity and good specificity for screening on IPV, psychological aggression, and physical violence in the past year, with the CTS tool as reference test.
Sources: Feldhaus, 1997; Mills, 2006 |
Ongoing Violence Assessment Tool (OVAT)
|
Low GRADE |
The OVAT may have good sensitivity and specificity for screening on IPV on the current moment, with the ISA tool as reference test.
Source: Ernst, 2004 |
Slapped, Things, Threaten (STaT) tool
|
Low GRADE |
The STaT tool may have excellent sensitivity and poor specificity for screening on IPV on the current moment/recent, with the ISA tool as reference test.
Source: Paranjape, 2006 |
Ongoing Abuse Screen (OAS) tool
|
Moderate GRADE |
The OAS tool likely has poor sensitivity and excellent specificity for screening on IPV on the current moment, with the ISA tool as reference test.
Source: Weiss, 2003 |
Abuse Assessment Screen (AAS) tool
|
Moderate GRADE |
The AAS tool likely has excellent sensitivity and poor specificity for screening on IPV on the current moment, with the ISA tool as reference test.
Source: Weiss, 2003 |
Samenvatting literatuur
Description of studies
Feltner (2018) performed a systematic review to assess the accuracy of screening questionnaires or tools to identify adults and adolescents with current, past, or increased risk for intimate partner violence (IPV). The review was an update of the 2011 evidence report for the US Preventive Services Task Force, so the literature search was performed from 2011 through October 4, 2017. Fifteen studies were included for the research question on accuracy of screening instruments. Screening instruments that were evaluated were:
- Woman Abuse Screening tool (WAST): 8 items assess physical and emotional IPV, no cutoff provided;
- Extended Hurt, Insulted, Threaten, Scream (E-HITS) Tool: 5 items, including all 4 HITS items and an additional sexual violence item, with a score of ≥7 representing positive screening for IPV;
- Hurt, Insulted, Threaten, Scream (HITS) tool: 4 items assess the frequency of IPV, with a score of ≥10 representing positive screening for IPV;
- Partner Violence Screen (PVS) tool: 3 items that assess physical IPV in the last year and current safety, with cutoff for IPV being affirmative response to ≥1 items (assuming person harming or making the respondent feel unsafe is a current or past partner);
- Ongoing Violence Assessment Tool (OVAT): 4 items assess ongoing physical and emotional IPV, with cutoff for IPV used affirmative response to items 1+H5, 2, or 4 and response of ≥3 for item 3;
- Slapped, Things, Threaten (STaT) tool: 3 items (2 assess physical IPV, 1 assesses threats), with a score of ≥1 representing positive screening for IPV;
- Ongoing Abuse Screen (OAS) tool: 5 items adapted from the AAS that assess ongoing physical, sexual, emotional IPV, and fear, with affirmative response to ≥1 item(s) used as cutoff;
- Abuse Assessment Screen (AAS) tool: 5 items assess physical, emotional, and sexual violence, with affirmative response to ≥1 item(s) used as cutoff.
Included studies used the following reference standards to determine the presence of IPV:
- Composite Abuse Scale (CAS): 43-item measure of partner abuse, including four dimensions: Severe Combined Abuse, Emotional Abuse, Physical Abuse, and Harassment;
- Conflicts Tactics Scale (CTS): 80 items to explore intrafamily conflict and violence;
- Revised Conflicts Tactics Scale (CTS-2): 39-item measure of individual engagement in or experience of physical or psychological violence with an intimate partner, based on the Conflict Tactic Scale;
- Index of Spousal Abuse (ISA): 30 item self-reported scale to measure physical and non-physical spouse abuse. It is used by clinicians to evaluate change in the degree or severity of both physical nonphysical abuse as perceived by female;
- Semi structured interviews.
Two studies were performed in primary care, so these are not reported in this literature analysis. In total, 4460 patients were included, and all studies enrolled adults, mostly women. The prevalence of current or recent IPV ranged from 11% to 29%, with a median of 24%. The quality of all studies was rated as fair.
Results
The studies reporting instruments used in primary care (Chen, 2005; Dubowitz, 2007; McMillan, 2006; Sohal, 2007; Zink, 2007), lifetime abuse (Paranjape, 2003), and predicting future abuse (Koziol-McLain, 2001) are not reported here.
Feltner (2018) reported that for screening instruments on past-year IPV, sensitivity ranged from 65% to 87% and specificity ranged from 80% to 95%. For instruments identifying ongoing or recurrent relationship violence, sensitivity ranged from 46% to 94% and specificity ranged from 38% to 95%. See Figure 1 for an overview. Because TP, TN, FP and FN were not reported by the authors, no other diagnostic accuracy outcomes such as PPV and NPV could be calculated.
Figure 1. Overview of sensitivity and specificity reported in the individual studies included in Feltner (2018)
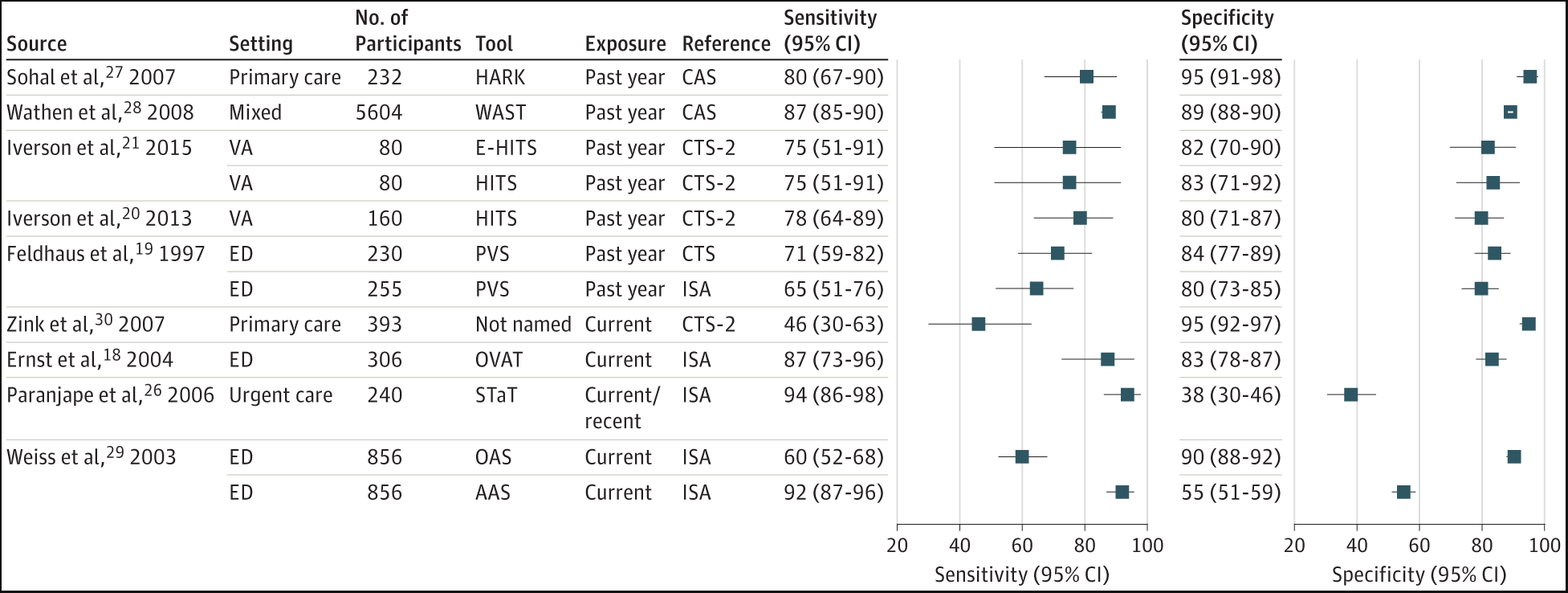
Figure is directly retrieved from Feltner (2018)
Woman Abuse Screening tool (WAST)
Wathen (2008), included in Feltner (2018), reported a IPV sensitivity of 88% (95%CI 85 to 90) and specificity of 89% (95%CI 88 to 90) for the WAST. The recall period was past year IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (CAS tool) was 14%. The study was performed in primary, acute, and specialty care centres in Canada. Participants were English-speaking and reading woman aged 18-64 years with a male partner in the past year, and 5604 participants were included. All included participants were woman and the mean age in the screen group was 39 years. The quality of the study was rated as fair.
Extended Hurt, Insulted, Threaten, Scream (E-HITS) Tool
Iverson (2015), included in Feltner (2018), reported a IPV sensitivity of 75% (95%CI 55 to 95) and specificity of 82% (95%CI 72 to 90) for the E-HITS tool. The recall period was past year IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (CTS-2 tool) was 25%. The study was performed using mailed surveys in the United States. Participants were female veterans aged ≥18 years found through Veterans Health Administration database who reported an intimate relationship in the past year, and 80 participants were included. All included participants were woman, and the mean age was 49 years. The quality of the study was rated as fair.
Hurt, Insulted, Threaten, Scream (HITS) tool
Iverson (2015), included in Feltner (2018), reported a IPV sensitivity of 75% (95%CI 55 to 95) and specificity of 83% (95%CI 73 to 92) for the HITS tool. The recall period was past year IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (CTS-2 tool) was 25%. The study was performed using mailed surveys in the United States. Participants were female veterans aged ≥18 years found through Veterans Health Administration database who reported an intimate relationship in the past year, and 80 participants were included. All included participants were woman, and the mean age was 49 years. The quality of the study was rated as fair.
Iverson (2013), included in Feltner (2018), reported a IPV sensitivity of 78% (95%CI 63 to 89) and specificity of 80% (95%CI 71 to 87) for the HITS tool. The recall period was past year IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (CTS-2 tool) was 29%. The study was performed using mailed surveys in the United States. Participants were female veterans aged ≥18 years found through Veterans Health Administration database who reported an intimate relationship in the past year, and 160 participants were included. All included participants were woman, and the mean age was 48 years. The quality of the study was rated as fair.
Mills (2006), included in Feltner (2018), reported a IPV sensitivity of 30% (95%CI 13 to 54) and specificity of 88% (95%CI 71 to 96) for psychological aggression and a sensitivity of 46% (95%CI 18 to 75) and specificity of 88% (95%CI 74 to 96) for physical violence for the HITS tool. The recall period was past year IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (CTS-2 tool) was 39% for psychological aggression and 20% for physical violence. The study was performed in Emergency departments in the United States. Participants were men aged ≥18 years triaged to the medical or trauma sections, and 53 participants were included. All included participants were men, and the mean age was 40 (SD = 11) years. The quality of the study was rated as fair.
Partner Violence Screen (PVS) tool
Feldhaus (1997), included in Feltner (2018), reported a IPV sensitivity of 64% (95%CI 51 to 76) and specificity of 80% (95%CI 74 to 86) for the PVS tool with the ISA tool and sensitivity of 71% (95%CI 59 to 82) and specificity of 84% (95%CI 78 to 90) with the CTS tool. The recall period was past year IPV exposure. The prevalence of IPV in the analysed population based on the reference standard ISA was 24% and based on the CTS 27%. The study was performed in emergency departments in the Unites States. Participants were English-speaking woman aged ≥18 years who were noncritical, and 255 participants were included in the ISA group and 230 in the CTS group. All included participants were woman, and the mean age was 36 (SD = 16) years. The quality of the study was rated as fair.
Mills (2006), included in Feltner (2018), reported a IPV sensitivity of 35% (95%CI 16 to 59) and specificity of 84% (95%CI 67 to 94) for psychological aggression and a sensitivity of 46% (95%CI 18 to 75) and specificity of 83% (95%CI 68 to 92) for physical violence for the PVS tool. The recall period was past year IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (CTS-2 tool) was 39% for psychological aggression and 20% for physical violence. The study was performed in Emergency departments in the United States. Participants were men aged ≥18 years triaged to the medical or trauma sections, and 53 participants were included. All included participants were men, and the mean age was 40 (SD = 11) years. The quality of the study was rated as fair.
Ongoing Violence Assessment Tool (OVAT)
Ernst (2004), included in Feltner (2018), reported a IPV sensitivity of 86% (95%CI 75 to 93) and specificity of 83% (95%CI 78 to 88) for the OVAT. The recall period was current IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (ISA tool) was 20%. The study was performed in emergency departments in the Unites States. Participants were English-speaking patients, and 306 participants were included. In total, 70% was woman, and the mean age was 34 (SD = 10) years. The quality of the study was rated as fair.
Slapped, Things, Threaten (STaT) tool
Paranjape (2006), included in Feltner (2018), reported a IPV sensitivity of 95% (95%CI 90 to 100) and specificity of 37% (95%CI 29 to 44) for the STaT tool. The recall period was current IPV exposure or most recent relationship. The prevalence of IPV in the analysed population based on the reference standard (ISA tool) was 33% during most recent relationship and 15% currently. The study was performed in urgent care in the Unites States. Participants were English-speaking women aged 18-65 years, and 240 participants were included. All included participants were woman, and the mean age was 38 (SD = 10) years. The quality of the study was rated as fair.
Ongoing Abuse Screen (OAS) tool
Weiss (2003), included in Feltner (2018), reported a IPV sensitivity of 60% (95%CI 52 to 67) and specificity of 90% (95%CI 87 to 92) for the OAS tool. The recall period was current IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (ISA tool) was 19%. The study was performed in emergency departments in the Unites States. Participants were patients with a current partner who were not too ill to participate, and 856 participants were included. In total, 62% was woman, and the mean age was 36 years. The quality of the study was rated as fair.
Abuse Assessment Screen (AAS) tool
Weiss (2003), included in Feltner (2018), reported a IPV sensitivity of 92% (95%CI 87 to 96) and specificity of 55% (95%CI 52 to 59) for the AAS tool. The recall period was current IPV exposure. The prevalence of IPV in the analysed population based on the reference standard (ISA tool) was 19%. The study was performed in emergency departments in the Unites States. Participants were patients with a current partner who were not too ill to participate, and 856 participants were included. In total, 62% was woman, and the mean age was 36 years. The quality of the study was rated as fair.
Level of evidence of the literature
Woman Abuse Screening tool (WAST)
The level of evidence regarding the outcome measure sensitivity was downgraded by one level because of study limitations of the individual study (risk of bias) to MODERATE.
The level of evidence regarding the outcome measure specificity was downgraded by one level because of study limitations of the individual study (risk of bias) to MODERATE.
Extended Hurt, Insulted, Threaten, Scream (E-HITS) Tool
The level of evidence regarding the outcome measure sensitivity was downgraded by two levels because of study limitations of the individual study (risk of bias) and low number of included participants (imprecision) to LOW.
The level of evidence regarding the outcome measure specificity was downgraded by two levels because of study limitations of the individual study (risk of bias) and low number of included participants (imprecision) to LOW.
Hurt, Insulted, Threaten, Scream (HITS) tool
The level of evidence regarding the outcome measure sensitivity was downgraded by two levels because of study limitations of the individual studies (risk of bias) and low number of included participants (imprecision) to LOW.
The level of evidence regarding the outcome measure specificity was downgraded by two levels because of study limitations of the individual studies (risk of bias) and low number of included participants (imprecision) to LOW.
Partner Violence Screen (PVS) tool
The level of evidence regarding the outcome measure sensitivity was downgraded by two levels because of study limitations of the individual studies (risk of bias) and low number of included participants (imprecision) to LOW.
The level of evidence regarding the outcome measure specificity was downgraded by two levels because of study limitations of the individual studies (risk of bias) and low number of included participants (imprecision) to LOW.
Ongoing Violence Assessment Tool (OVAT)
The level of evidence regarding the outcome measure sensitivity was downgraded by two levels because of study limitations of the individual study (risk of bias) and low number of included participants (imprecision) to LOW.
The level of evidence regarding the outcome measure specificity was downgraded by two levels because of study limitations of the individual study (risk of bias) and low number of included participants (imprecision) to LOW.
Slapped, Things, Threaten (STaT) tool
The level of evidence regarding the outcome measure sensitivity was downgraded by two levels because of study limitations of the individual study (risk of bias) and low number of included participants (imprecision) to LOW.
The level of evidence regarding the outcome measure specificity was downgraded by two levels because of study limitations of the individual study (risk of bias) and low number of included participants (imprecision) to LOW.
Ongoing Abuse Screen (OAS) tool
The level of evidence regarding the outcome measure sensitivity was downgraded by one level because of study limitations of the individual study (risk of bias) to MODERATE.
The level of evidence regarding the outcome measure specificity was downgraded by one level because of study limitations of the individual study (risk of bias) to MODERATE.
Abuse Assessment Screen (AAS) tool
The level of evidence regarding the outcome measure sensitivity was downgraded by one level because of study limitations of the individual study (risk of bias) to MODERATE.
The level of evidence regarding the outcome measure specificity was downgraded by one level because of study limitations of the individual study (risk of bias) to MODERATE.
Zoeken en selecteren
A systematic review of the literature was performed to answer the following question:
Which validated screening instrument can be used (by all caregivers in the emergency department) for signalling and recognizing domestic violence in adults in secondary care?
| P: |
Adults in secondary care (or emergency department; ED) |
| I: |
Screening instrument on violence |
| C: |
Questions posed by clinician (what happened to you) or another screening instrument |
| R: |
Psychiatric assessment |
| O: |
Diagnostic accuracy (crucial: sensitivity; important: specificity) |
| T&S: | All caregivers |
Relevant outcome measures
The guideline development group considered sensitivity as a critical outcome measure for decision making; and specificity as an important outcome measure for decision making.
A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 7 December 2023. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 2082 hits. Due to the high amount of hits, we decided to only select systematic reviews, which were 145 hits. Studies were selected based on the following criteria: systematic reviews about violence, adults, and screening instruments. Fourteen studies were initially selected based on title and abstract screening. After reading the full text, 13 studies were excluded (see the table with reasons for exclusion under the tab Methods), and one study was included.
Results
One study was included in the analysis of the literature. Important study characteristics and results are summarized in the evidence table. The assessment of the risk of bias is summarized in the risk of bias table.
Referenties
- Bureau van de Europese Unie voor de grondrechten. Geweld tegen vrouwen: een Europese enquête: resultaten in het kort [internet]. Luxemburg: Publications Office; 2014 [geciteerd 16 okt 2024]. Beschikbaar via: https://data.europa.eu/doi/10.2811/615.
- Campbell J, Jones AS, Dienemann J, Kub J, Schollenberger J, O'Campo P, Gielen AC, Wynne C. Intimate partner violence and physical health consequences. Arch Intern Med. 2002 May 27;162(10):1157-63. doi: 10.1001/archinte.162.10.1157. PMID: 12020187.
- CBS. Prevalentiemonitor huiselijk geweld en seksueel grensoverschrijdend gedrag 2024: 9. Totaalbeeld huiselijk geweld en seksueel grensoverschrijdend gedrag [Internet]. Den Haag: Centraal Bureau voor de Statistiek; 2024 [geciteerd op 2025 apr 16]. Beschikbaar via: https://www.cbs.nl/nl-nl/longread/rapportages/2024/prevalentiemonitor-huiselijk-geweld-en-seksueel-grensoverschrijdend-gedrag-2024/9-totaalbeeld-huiselijk-geweld-en-seksueel-grensoverschrijdend-gedrag.
- Chang JC, Cluss PA, Ranieri L, Hawker L, Buranosky R, Dado D, McNeil M, Scholle SH. Health care interventions for intimate partner violence: what women want. Womens Health Issues. 2005 Jan-Feb;15(1):21-30. doi: 10.1016/j.whi.2004.08.007. PMID: 15661584.
- Ernst AA, Weiss SJ, Cham E, Hall L, Nick TG. Detecting ongoing intimate partner violence in the emergency department using a simple 4-question screen: the OVAT. Violence Vict. 2004 Jun;19(3):375-84. doi: 10.1891/vivi.19.3.375.65769. PMID: 15631287.
- Feldhaus KM, Koziol-McLain J, Amsbury HL, Norton IM, Lowenstein SR, Abbott JT. Accuracy of 3 brief screening questions for detecting partner violence in the emergency department. JAMA. 1997 May 7;277(17):1357-61. PMID: 9134940.
- Feltner C, Wallace I, Berkman N, Kistler CE, Middleton JC, Barclay C, Higginbotham L, Green JT, Jonas DE. Screening for Intimate Partner Violence, Elder Abuse, and Abuse of Vulnerable Adults: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2018 Oct 23;320(16):1688-1701. doi: 10.1001/jama.2018.13212. PMID: 30357304.
- Gazmararian JA, Lazorick S, Spitz AM, Ballard TJ, Saltzman LE, Marks JS. Prevalence of violence against pregnant women. JAMA. 1996 Jun 26;275(24):1915-20. Erratum in: JAMA 1997 Apr 9;277(14):1125. PMID: 8648873.
- Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts CH; WHO Multi-country Study on Women's Health and Domestic Violence against Women Study Team. Prevalence of intimate partner violence: findings from the WHO multi-country study on women's health and domestic violence. Lancet. 2006 Oct 7;368(9543):1260-9. doi: 10.1016/S0140-6736(06)69523-8. PMID: 17027732.
- Guth AA, Pachter L. Domestic violence and the trauma surgeon. Am J Surg. 2000 Feb;179(2):134-40. doi: 10.1016/s0002-9610(00)00245-2. PMID: 10970242.
- Hegarty K, Gunn J, Chondros P, Small R. Association between depression and abuse by partners of women attending general practice: descriptive, cross sectional survey. BMJ. 2004 Mar 13;328(7440):621-4. doi: 10.1136/bmj.328.7440.621. PMID: 15016694; PMCID: PMC381136.
- Iverson KM, King MW, Resick PA, Gerber MR, Kimerling R, Vogt D. Clinical utility of an intimate partner violence screening tool for female VHA patients. J Gen Intern Med. 2013 Oct;28(10):1288-93. doi: 10.1007/s11606-013-2534-x. Epub 2013 Jul 4. PMID: 23824907; PMCID: PMC3785669.
- Iverson KM, King MW, Gerber MR, Resick PA, Kimerling R, Street AE, Vogt D. Accuracy of an intimate partner violence screening tool for female VHA patients: a replication and extension. J Trauma Stress. 2015 Feb;28(1):79-82. doi: 10.1002/jts.21985. Epub 2015 Jan 26. PMID: 25624170.
- Koninklijke Nederlandsche Maatschappij tot bevordering der Geneeskunst. KNMG-meldcode Kindermishandeling en huiselijk geweld. Utrecht: KNMG; 2023. Beschikbaar van: https://knmg-meldcode.maglr.com/meldcode-kindermishandeling-en-huiselijk-geweld/cover.
- KNMG. Beroepsgeheim: wat is het medisch beroepsgeheim? [internet]. Utrecht: KNMG; [geciteerd 16 okt 2024]. Beschikbaar via: https://www.knmg.nl/actueel/dossiers/beroepsgeheim/medisch-beroepsgeheim/wanneer-doorbreken.
- Lo Fo Wong SH, Lagro-Janssen AL. Mishandeling van vrouwen binnen de partnerrelatie: signalering in de medische praktijk [Intimate partner abuse of women: identification of victims in medical practice]. Ned Tijdschr Geneeskd. 2005 Jan 1;149(1):6-9. Dutch. PMID: 15651495.
- McCauley J, Kern DE, Kolodner K, Dill L, Schroeder AF, DeChant HK, Ryden J, Bass EB, Derogatis LR. The "battering syndrome": prevalence and clinical characteristics of domestic violence in primary care internal medicine practices. Ann Intern Med. 1995 Nov 15;123(10):737-46. doi: 10.7326/0003-4819-123-10-199511150-00001. PMID: 7574191.
- Mills TJ, Avegno JL, Haydel MJ. Male victims of partner violence: prevalence and accuracy of screening tools. J Emerg Med. 2006 Nov;31(4):447-52. doi: 10.1016/j.jemermed.2005.12.029. PMID: 17046494.
- Morrison LJ, Allan R, Grunfeld A. Improving the emergency department detection rate of domestic violence using direct questioning. J Emerg Med. 2000 Aug;19(2):117-24. doi: 10.1016/s0736-4679(00)00204-3. PMID: 10903457.
- Nelson HD, Nygren P, McInerney Y, Klein J; U. S. Preventive Services Task Force. Screening women and elderly adults for family and intimate partner violence: a review of the evidence for the U. S. Preventive Services Task Force. Ann Intern Med. 2004 Mar 2;140(5):387-96. doi: 10.7326/0003-4819-140-5-200403020-00015. PMID: 14996681.
- Paranjape A, Rask K, Liebschutz J. Utility of STaT for the identification of recent intimate partner violence. J Natl Med Assoc. 2006 Oct;98(10):1663-9. PMID: 17052059; PMCID: PMC2569753.
- Plichta SB. Intimate partner violence and physical health consequences: policy and practice implications. J Interpers Violence. 2004 Nov;19(11):1296-323. doi: 10.1177/0886260504269685. PMID: 15534333.
- Registered Nurses' Association of Ontario. Woman abuse: screening, identification and initial response [internet]. Toronto (Canada): Registered Nurses' Association of Ontario; 2005 [geciteerd 16 okt 2024]. Beschikbaar via: https://rnao.ca/bpg/guidelines/woman-abuse-screening-identification-and-initial-response
- Reijnders UJ, van der Leden ME, de Bruin KH. Letsels door huiselijk geweld tegen vrouwen: locaties op het lichaam, soorten letsel en wijzen van toebrengen [Injuries due to domestic violence against women: sites on the body, types of injury and the methods of infliction]. Ned Tijdschr Geneeskd. 2006 Feb 25;150(8):429-35. Dutch. PMID: 16538843.
- Verwijs LM, Lünnemann K. Partnergeweld: achtergrond en risicofactoren. Utrecht: Verwey-Jonker Instituut; 2012.
- Wathen CN, Jamieson E, MacMillan HL; McMaster Violence Against Women Research Group. Who is identified by screening for intimate partner violence? Womens Health Issues. 2008 Nov-Dec;18(6):423-32. doi: 10.1016/j.whi.2008.08.003. PMID: 19041594.
- Weiss SJ, Ernst AA, Cham E, Nick TG. Development of a screen for ongoing intimate partner violence. Violence Vict. 2003 Apr;18(2):131-41. doi: 10.1891/vivi.2003.18.2.131. PMID: 12816400.
Evidence tabellen
Evidence table for systematic reviews of diagnostic test accuracy studies
|
Study reference |
Study characteristics |
Patient characteristics
|
Intervention |
Reference test
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Feltner, 2018
Individual study characteristics and results deduced from Feltner, 2018, unless stated otherwise.
|
Systematic review of RCTs, cross-sectional studies and cohort studies.
Literature search from 2011 through October 4, 2017. Studies published before 2011 were identified from the prior systematic reviews for the USPSTF. For IPV screening and treatment in men and adolescents (not included in the prior reviews), searches were conducted from database inception through October 4, 2017.
Setting and Country: Primary care settings and emergency departments. Research conducted in populations similar to US populations.
Source of funding and conflicts of interest: No conflicts of interest.
This research was funded under contract HHSA-290-2012-00015-I, Task Order 5, from the Agency for Healthcare Research and Quality (AHRQ), US Department of Health and Human Services, under a contract to support the USPSTF. Role of the Funder/Sponsor: Investigators worked with USPSTF members and AHRQ staff to develop the scope, analytic framework, and key questions for this review. AHRQ had no role in study selection, quality assessment, or synthesis. AHRQ staff provided project oversight, reviewed the report to ensure that the analysis met methodological standards, and distributed the draft for peer review. Otherwise, AHRQ had no role in the conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript findings. The opinions expressed in this document are those of the authors and do not reflect the official position of AHRQ or the US Department of Health and Human Services. |
Inclusion criteria SR:
Studies assessing the accuracy of tools designed to detect current, past, or risk of abuse were eligible for KQ2 (screening test accuracy). Only studies that compared a screening tool with an acceptable reference standard, such as the Conflicts Tactics Scale (CTS), were eligible.
Exclusion criteria SR: Studies restricted to populations seeking care for IPV or for obvious signs or symptoms of abuse. Screening tests designed to identify perpetrators of IPV.
Theory or survey development and validation without correlation to abuse outcomes, studies that focus only on particular risk factors, or assessment of provider or participant attitudes toward the instrument.
15 studies included
Characteristics See figure 1.
Prevalence The prevalence of current or recent IPV ranged from 11% to 29%, with a median of 24%. |
See figure 1 and 3. |
See figure 2 and 3. |
Not reported. |
See figure 2 and 3. |
Study quality (ROB): See figure 4.
Author’s conclusion In the 5 studies assessing accuracy of tools for detecting past-year IPV in women (HARK, HITS, E-HITS, PVS, and WAST), sensitivity ranged from 65%to 87%and specificity from 80% to 95%. When limiting to studies enrolling participants from non–emergency department settings (ie, primary care or community samples only), sensitivity was slightly higher (range, 75%-87%) and specificity was unchanged. Estimates of screening test accuracy for detecting past-year IPV were derived from populations with an IPV prevalence of 14% to 27%. See figure 5. |
Figure 1. Characteristics of the included studies in Feltner (2018). Figure is directly retrieved from Feltner (2018)
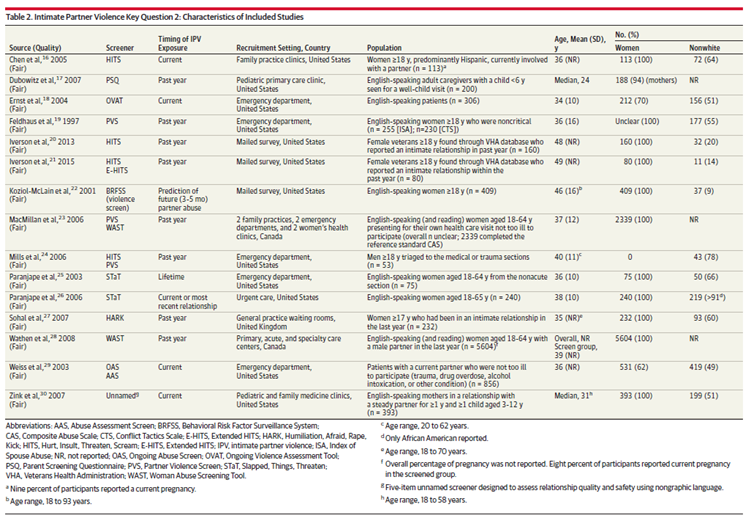
Figure 2. Sensitivity and specificity of the screening tools. Figure is directly retrieved from Feltner (2018)

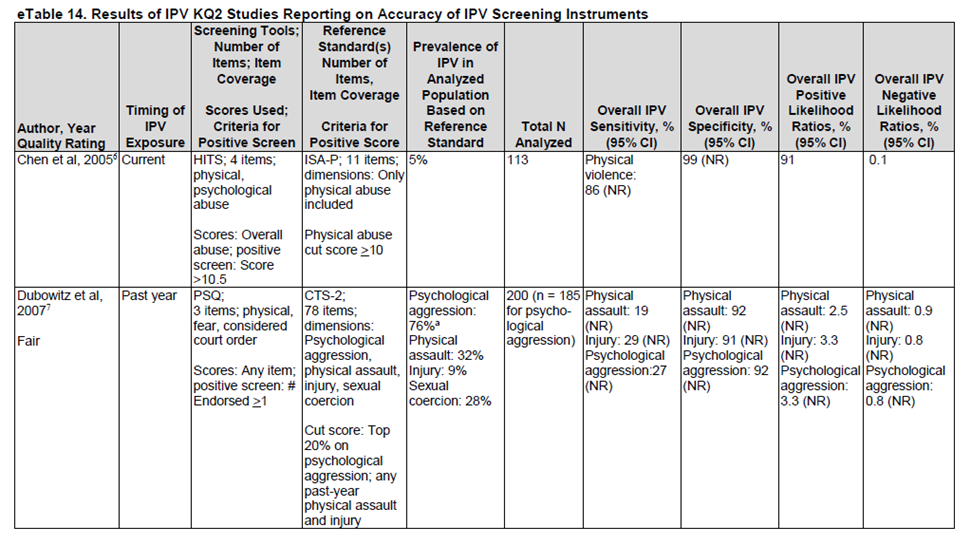
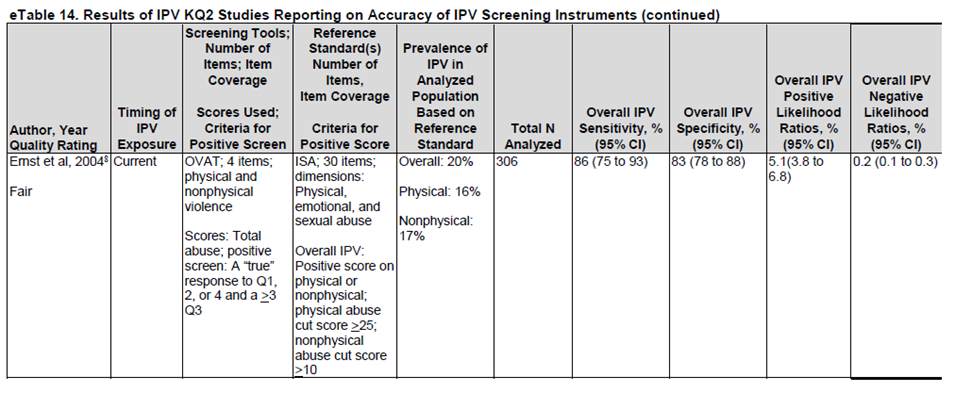
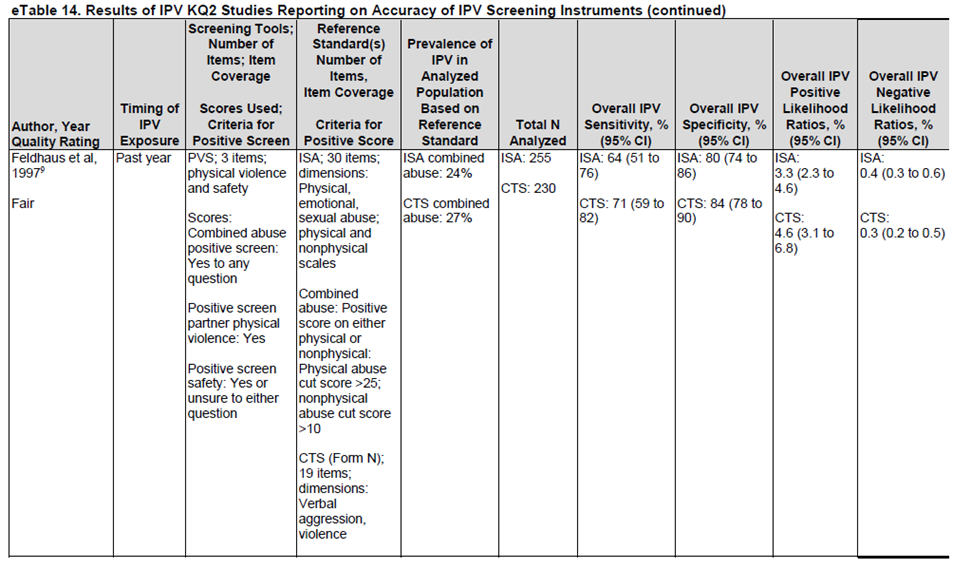
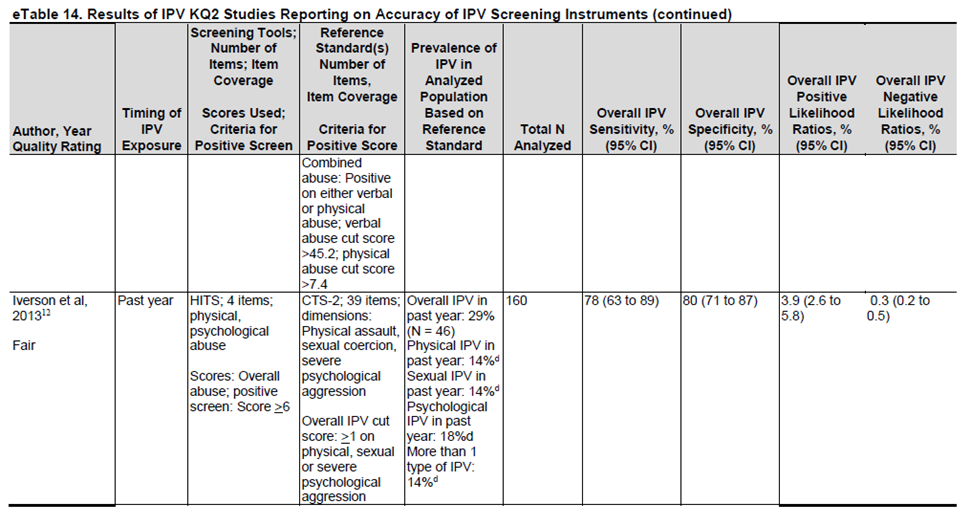
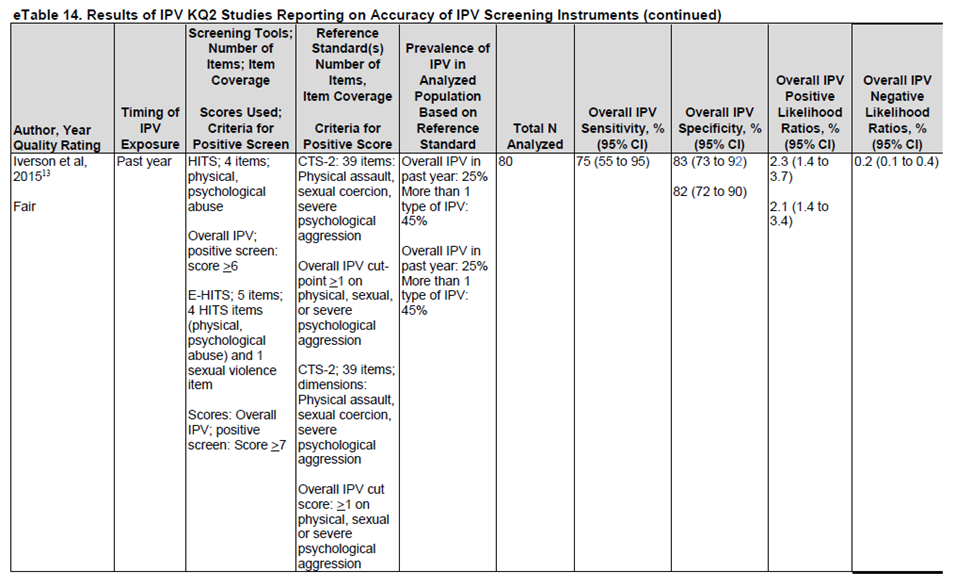
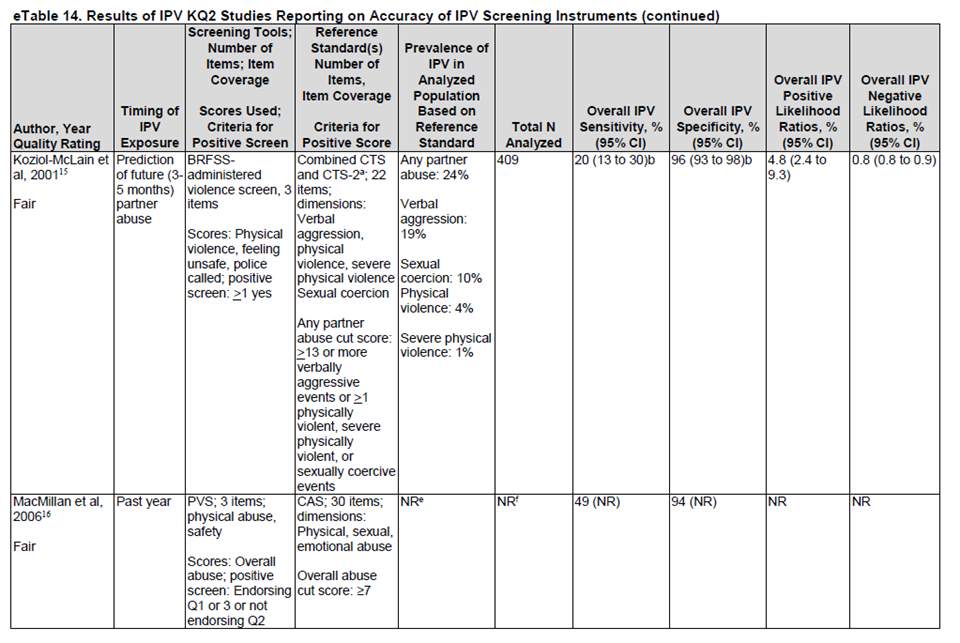
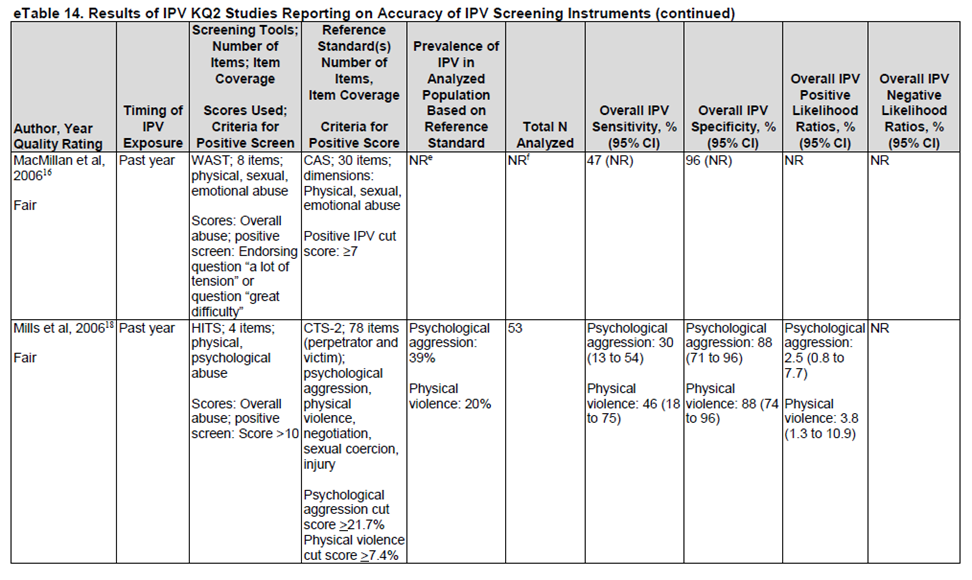
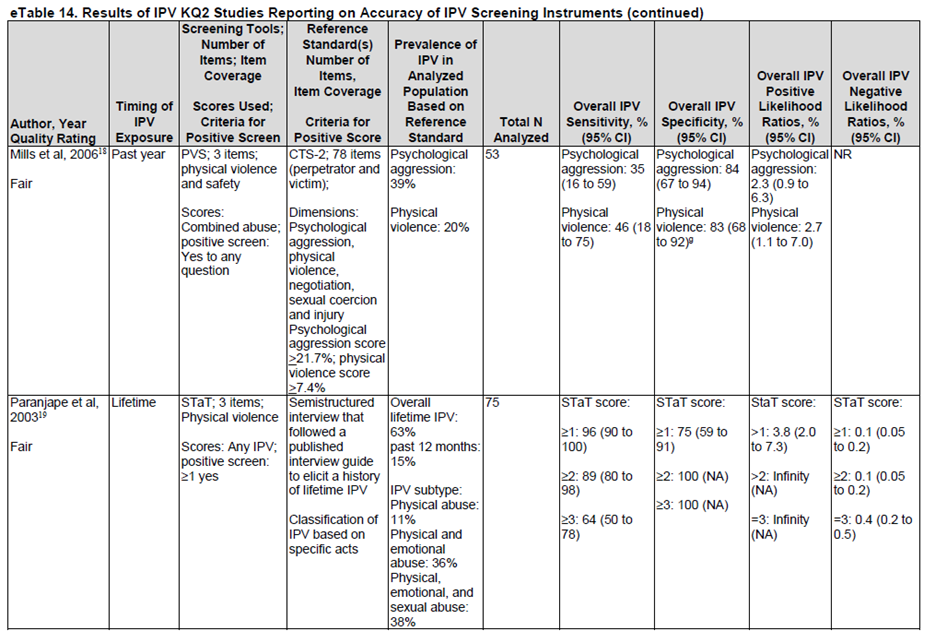
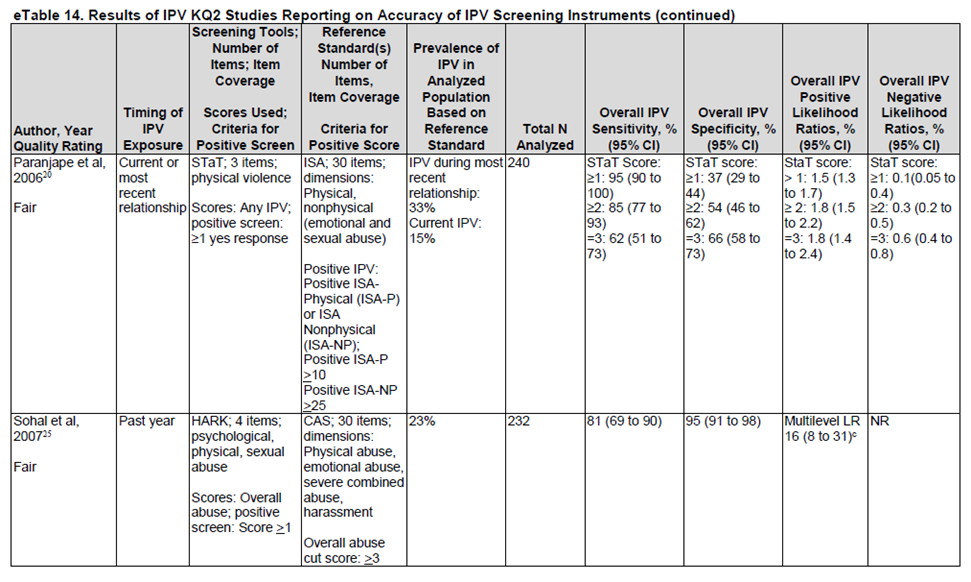
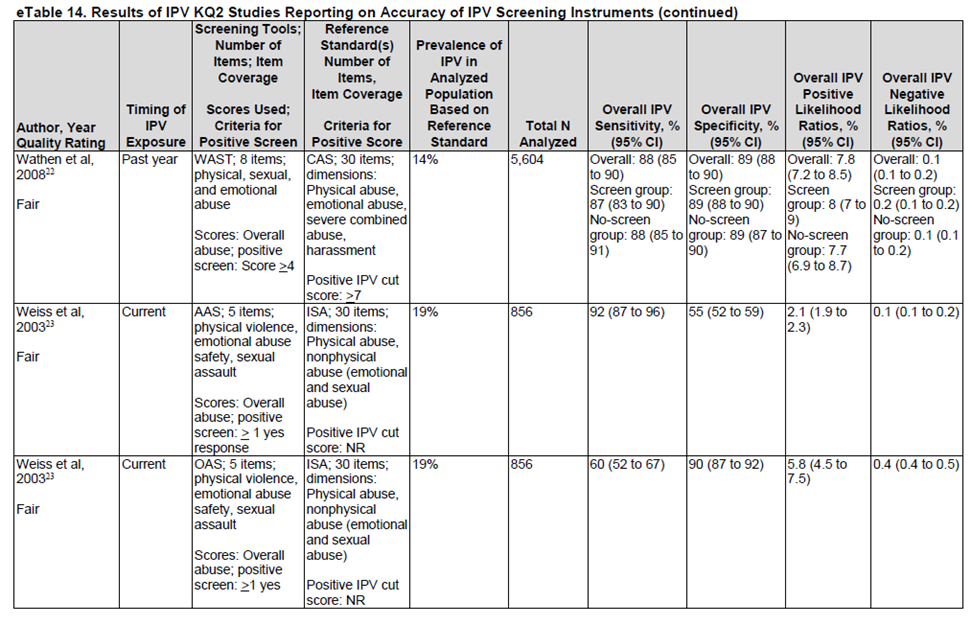
Figure 3. Results of the studies included in Feltner (2018). Figure is directly retrieved from Feltner (2018)
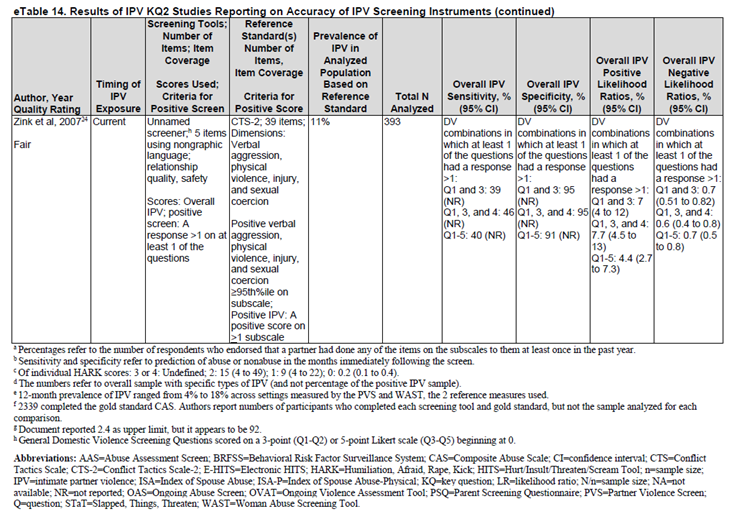
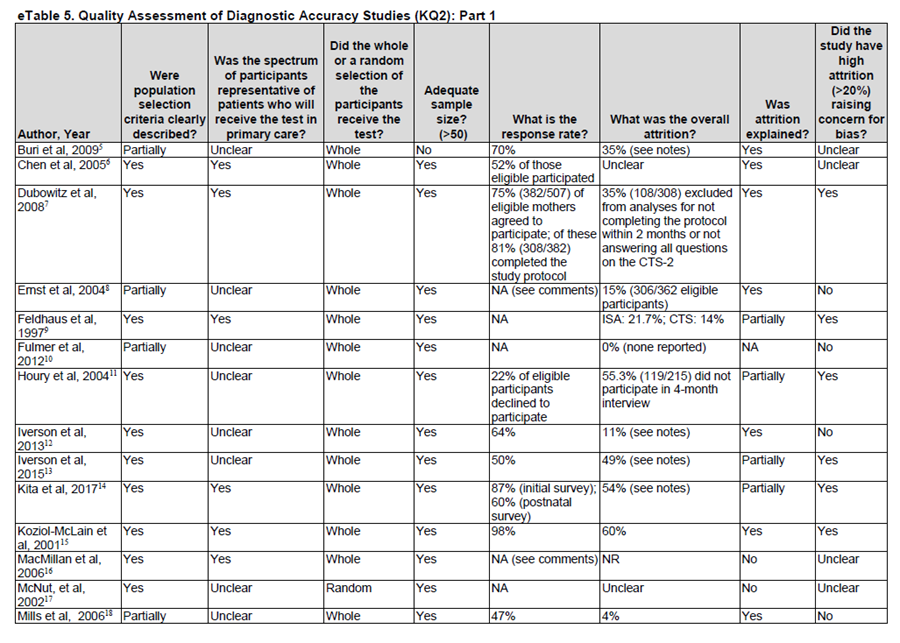
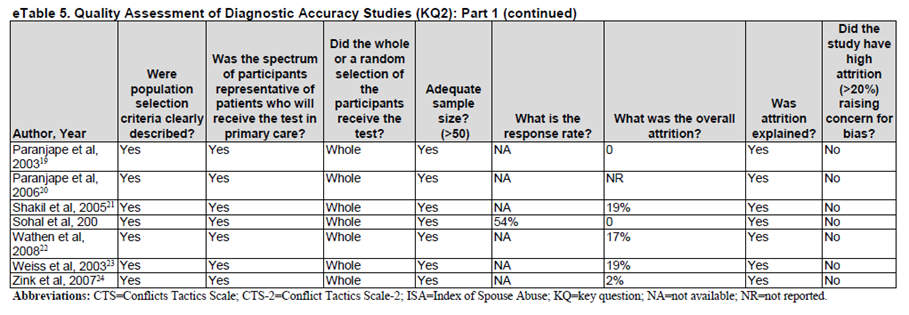
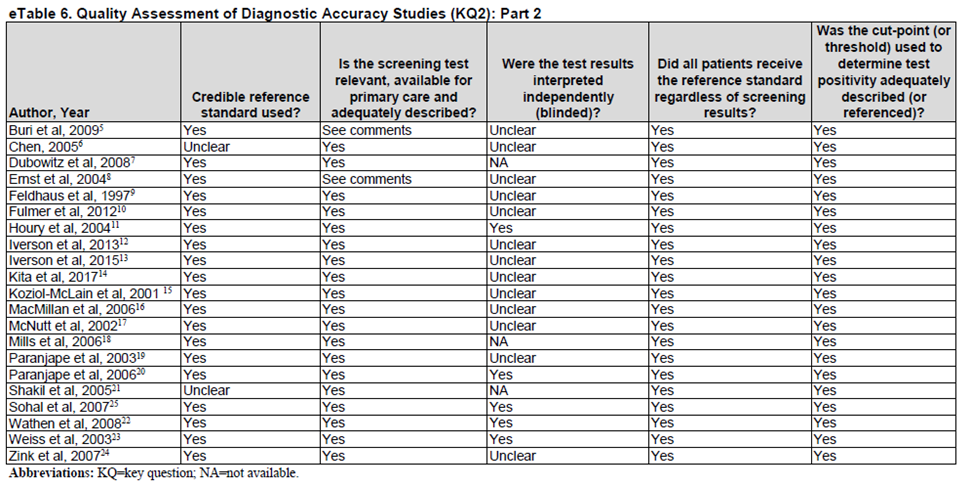
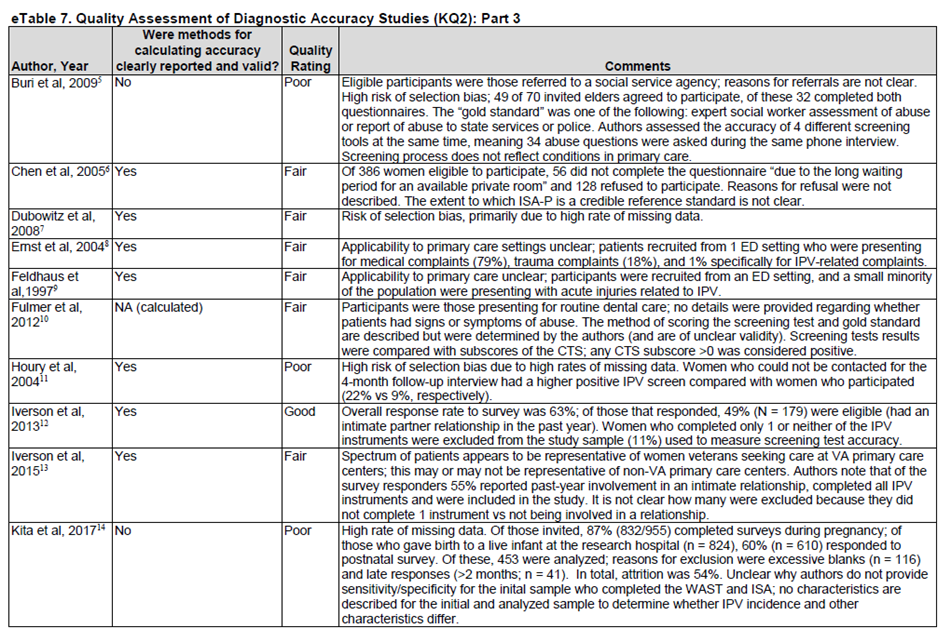
Figure 4. Quality assessment of the studies included in Feltner (2018). Figure is directly retrieved from Feltner (2018)
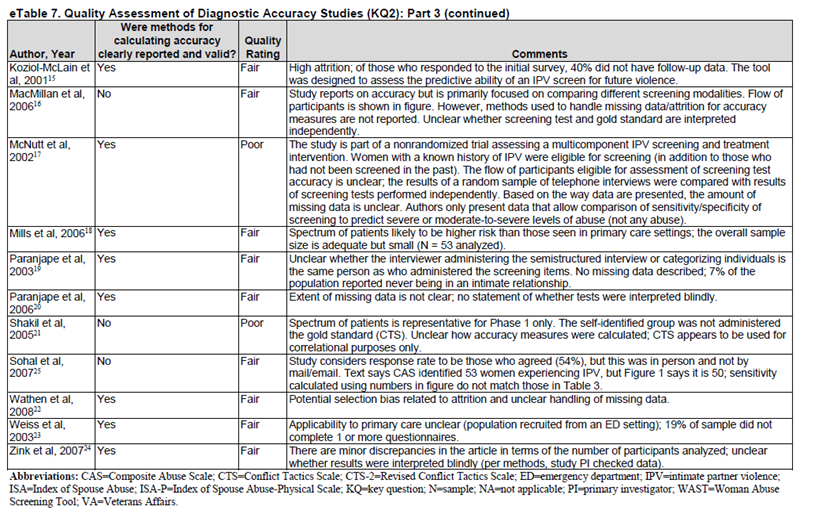
Figure 5. Summary of evidence. Figure is directly retrieved from Feltner (2018)

Risk of bias table
Table of quality assessment for systematic reviews of diagnostic studies
Based on AMSTAR checklist (Shea et al.; 2007, BMC Methodol 7: 10; doi:10.1186/1471-2288-7-10) and PRISMA checklist (Moher et al 2009, PLoS Med 6: e1000097; doi:10.1371/journal.pmed1000097)
|
Study
First author, year |
Appropriate and clearly focused question?
Yes/no/unclear |
Comprehensive and systematic literature search?
Yes/no/unclear |
Description of included and excluded studies?
Yes/no/unclear |
Description of relevant characteristics of included studies?
Yes/no/unclear |
Assessment of scientific quality of included studies?
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?
Yes/no/unclear |
Potential risk of publication bias taken into account?
Yes/no/unclear |
Potential conflicts of interest reported?
Yes/no/unclear |
|
Feltner, 2018 |
Yes |
Yes |
Yes |
Yes |
Yes |
Not applicable; studies are not combined in meta-anslysis. |
No |
Yes |
Table of excluded studies
|
Author, year |
Title |
Exclusion reason |
|
Tiwari, 2007 |
Identifying intimate partner violence: comparing the Chinese Abuse Assessment Screen with the Chinese Revised Conflict Tactics Scales |
Wrong aim: validation of Chinese version of screening instrument |
|
Taft, 2008 |
Screening women for intimate partner violence in health care settings |
Wrong design: protocol and wrong outcomes: odds ratios (effectiveness) |
|
Costa, 2016 |
Instruments to Assess Intimate Partner Violence: A Scoping Review of the Literature |
More recent systematic review included, reference checking performed. |
|
Feder, 2009 |
How far does screening women for domestic (partner) violence in different health-care settings meet criteria for a screening programme? Systematic reviews of nine UK, National Screening Committee criteria |
More recent systematic review included, reference checking performed. |
|
Alexander, 2022 |
Evaluating Measures of Intimate Partner Violence Using Consensus-Based Standards of Validity |
Study does not provide any quality assessment and data on which the results are based. Therefore, the systematic review of Feltner (2018) is preferred. Reference checking performed. |
|
Syed, 2021 |
Predictive value of indicators for identifying child maltreatment and intimate partner violence in coded electronic health records: A systematic review and meta-analysis |
Wrong P: screening for intimate partner voilence is performed in women aged 12 to 55 years |
|
Moyer, 2013 |
Screening for intimate partner violence and abuse of elderly and vulnerable adults: U.S. Preventive Services Task Force recommendation statement |
Clinical guideline that only provides recommendations, and the included review of Alexander is recenter. Reference checking performed. |
|
Graham, 2021 |
The Validity and Reliability of Available Intimate Partner Homicide and Reassault Risk Assessment Tools: A Systematic Review |
Screening tools for risk of reassault |
|
Nelson, 2012 |
Screening women for intimate partner violence: a systematic review to update the U.S. Preventive Services Task Force recommendation |
Feltner (2018) is an update of this review |
|
Nelson, 2012 |
Screening Women for Intimate Partner Violence and Elderly and Vulnerable Adults for Abuse: Systematic Review to Update the 2004 U.S. Preventive Services Task Force Recommendation |
Feltner (2018) is an update of this review |
|
Rabin, 2009 |
Intimate Partner Violence Screening Tools. A Systematic Review |
More recent systematic review included, reference checking performed. |
|
Davis, 2021 |
Brief Intimate Partner Violence Perpetration Screening Tools: A Scoping Review |
This is a scoping review, so the systematic review of Feltner is preferred. Reference checking performed. |
|
Ford-Gilboe, 2016 |
Development of a brief measure of intimate partner violence experiences: the Composite Abuse Scale (Revised)-Short Form (CASR-SF) |
Wrong O: no diagnostic accuracy |
Verantwoording
Beoordelingsdatum en geldigheid
Laatst beoordeeld : 15-07-2025
Algemene gegevens
De ontwikkeling van deze richtlijnmodules werden ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werden gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodules.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodules is in 2023 een multidisciplinaire cluster ingesteld. Dit cluster bestaat uit vertegenwoordigers van alle relevante organisaties die betrekking hebben op de zorg voor patiënten met vermoeden van mishandeling.
Het cluster Mishandeling bestaat uit meerdere richtlijnen, zie hier voor de actuele clusterindeling. De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden worden indien nodig gevraagd om hun expertise in te zetten voor een specifieke richtlijnmodule. Het cluster Mishandeling bestaat uit de volgende personen:
Clusterstuurgroep
- Drs. A.H. (Rian) Teeuw, kinderarts sociale pediatrie, werkzaam in het Amsterdam UMC - Emma Kinderziekenhuis te Amsterdam, NVK
- Drs. M.E. (Miriam) van Houten, sociaal medisch adviseur, klinisch geriater niet praktiserend, promovendus, werkzaam bij Trompetter & Partners en voor het RadboudUMC te Nijmegen (alsook per 01-11-2025 voor UMCG Groningen als arts A&G), NVKG
- Dr. M.J. (Marie-Jose) van Hoof, kinder- en jeugdpsychiater, werkzaam bij iMindU te Leiden, NVvP
- H. (Hester) Rippen-Wagner, directeur-bestuurder, Stichting Kind en Ziekenhuis
Clusterexpertisegroep
- Drs. N.C.M. (Nicky) Platte-van Attekum, jeugdarts, werkzaam bij GGD Zuid-Limburg te Heerlen, AJN
- Drs. I. (Inge) van Eck, forensisch arts KNMG, werkzaam bij GGD Hollands Noorden, FMG
- Dr. M. (Marjan) van den Berg, arts seksuoloog, werkzaam bij Seksuologiepraktijk Van den Berg te Groningen, NVOG
- Drs. A.W. (Anita) Lekx, spoedeisende hulparts, werkzaam bij het VieCuri Medisch Centrum te Venlo, NVSHA
- Drs. M. (Marjolijn) van de Merwe, vertrouwensarts, werkzaam bij Veilig Thuis Zuid Holland Zuid te Dordrecht, VVAK
- Dr. R. (Roel) Bakx, kinderchirurg, werkzaam in het Amsterdam UMC - Emma Kinderziekenhuis te Amsterdam, NVvH
- Drs. B. (Bente) Allessie, jeugd- en VoorZorg verpleegkundige bij GGD Gelderland Midden, V&VN
- Drs. I. (Imke) van Kessel, kinderarts, werkzaam in het Amsterdam UMC - Emma Kinderziekenhuis te Amsterdam, NVK
- Dr. M. (Monique) Trijbels-Smeulders, kinderarts en medisch directeur, werkzaam bij Stichting Landelijk Expertise Centrum Kindermishandeling te Utrecht, NVK
- Drs. E.A.L. (Eline) van den Heuvel, kinderarts, werkzaam bij UMC Utrecht - Wilhelmina Kinderziekenhuis te Utrecht, NVK
- Prof. dr. E. (Elise) van de Putte, hoogleraar kindergeneeskunde, werkzaam bij UMC Utrecht - Wilhelmina Kinderziekenhuis te Utrecht, NVK
- Drs. S. (Sacha) van der Poll, klinisch geriater, werkzaam bij het Canisius Wilhelmina Ziekenhuis te Nijmegen, NVKG
- G. (Ger) Deleij, beleidsadviseur Belangenbehartiging, werkzaam bij KBO-PCOB te Nieuwegein, KBO-PCOB
- Drs. M.C. (Kristine) Beumer, forensisch arts, werkzaam bij het Nederlands Forensisch Instituut te Den Haag, NFI
- Dr. H.G.T. (Huub) Nijs, forensisch arts, werkzaam bij het Nederlands Forensisch Instituut te Den Haag, NFI
- Drs. K.A. (Kelsey) van Son, spoedeisende hulparts, werkzaam bij het Canisius Wilhelmina Ziekenhuis te Nijmegen, NVSHA
- H. (Henrique) Sachse, vertrouwens- en jeugdarts, VVAK
Met ondersteuning van
- Dr. J. (Janneke) Hoogervorst-Schilp, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. L.A.M. (Liza) van Mun, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. R. (Renee) Bolijn, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle clusterstuurgroepleden en actief betrokken expertisegroepsleden (fungerend als schrijver en/of meelezer bij tenminste één van de geprioriteerde richtlijnmodules) hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een richtlijnmodule worden wijzigingen in belangen aan de projectleider doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase. Een overzicht van de belangen van de clusterleden en betrokken expertisegroepsleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
Clusterstuurgroep
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Rian Teeuw |
Kinderarts sociale pediatrie bij Emma Kinderziekenhuis- Amsterdam UMC. |
Geen |
Co-auteur van Hoedeman F, Puiman PJ, van den Heuvel EAL, Affourtit MJ, Bakx R, Langendam MW, van de Putte EM, Russel-Kampschoer IMB, Schouten MCM, Teeuw AH, de Koning HJ, Moll HA. A validated Screening instrument for Child Abuse and Neglect (SCAN) at the emergency department. Eur J Pediatr. 2023 Jan;182(1):79-87. doi: 10.1007/s00431-022-04635-0. Epub 2022 Oct 5. PMID: 36198865; PMCID: PMC9534589. |
Geen restricties |
|
Miriam van Houten |
PhD student RadboudUMC, geen officiële aanstelling, onbetaald Arts A&G UMCG Groningen |
lid richtlijn disseminatie van richtlijnen, alleen vacatiegeld, onlangs afgerond |
VWS 2019: subsidie VWS voor onderzoek screeningsinstrument ouderenmishandeling ontwikkelen en ZONMW: validatie screeningsinstrument ouderenmishandeling
Ik doe onderzoek naar ouderenmishandeling en ik werk bij een bedrijf waar ik beoordelingen doe in het kader van een vermoeden van bv financieel misbruik. |
Geen restricties |
|
Marie-José van Hoof |
Bestuurder/geneesheer-directeur iMindU GGZ |
Onbezoldigd: - lid portefeuille wetenschap en inkomend voorzitter Afdeling Psychotherapie Nederlandse - Vereniging voor Psychiatrie (NVvP); - redactielid Tijdschrift voor Psychotherapie; - voorzitter expertgroep Trauma en kindermishandeling Kenniscentrum Kinder- en Jeugdpsychiatrie; - onderzoeker Amsterdam AMC; - betrokken bij aanpak complexe scheidingen en bij aanpak dwingende controle in spontaan ontstane multisectorele en multidisciplinaire samenwerkingsverbanden; - initiatiefnemer en voorzitter Special Interest Group on child abuse and neglect and domestic violence in particular coercive control @ IACAPAP (international Association of Child and Adolescent Psychiatrists and Allied Professionals Bezoldigd: -lid Raad van Comissarissen De Velse GGZ |
ideëel belang: implementatie van een door mij ontwikkeld model van zorg en zorgorganisatie dat ook toegepast kan worden op integrale aanpak KMHG en Kindermishandeling door falsificatie. |
Geen restricties |
|
Hester Rippen-Wagner |
Directeur-bestuurder Stichting Kind en Ziekenhuis
|
• Eigenaar en Oprichter FIDUZ Management: freelance Manager/Consultant Project- en Interimmanagement •Lid Raad van Toezicht Stichting Nazorg bij Postinfectieuze aandoeningen (waaronder ook Q-support en C-support) •Raad van Toezicht MEEr-groep •Bestuurslid College Perinatale zorg (CPZ) •Coördinator (/president) European Association for Children in Hospital (EACH) •Voorzitter Landelijke Borstvoedingsraad •Voorzitter MKS Landelijke coördinatieteam Integrale Kindzorg •Voorzitter Expertiseraad Kenniscentrum kinderpalliatieve zorg |
Geen |
Geen restricties |
Clusterexpertisegroep
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Nicky Platte-van Attekum |
28uur/week Jeugdarts KNMG arts maatschappij en gezondheid bij de GGD Zuid Limburg, waaronder ik ook uren heb als aandachtsfunctionaris kindermishandeling. |
Geen |
Geen |
Geen restricties |
|
Anita Lekx |
Spoedeisende Hulp arts VieCuri Medisch Centrum (fulltime) |
Lid sectie Mishandeling en Geweld van de Nederlandse Vereniging voor Spoedeisende Hulp Artsen (NVSHA) (onbetaald) |
Als sectie expertisefunctie bij onze landelijke vereniging en achterban |
Geen restricties |
|
Roel Bakx |
Kinderchirurg, betaald |
Voorzitter richtlijnencommissie NVvH (betaald) |
ZonMw: APAC trail (antibiotica versus operatie bij appendictitis), projectleider. ZEGG doematigheid: CAPP trail (analyse behandeling complexe appendictitis). Co-auteur van Hoedeman F, Puiman PJ, van den Heuvel EAL, Affourtit MJ, Bakx R, Langendam MW, van de Putte EM, Russel-Kampschoer IMB, Schouten MCM, Teeuw AH, de Koning HJ, Moll HA. A validated Screening instrument for Child Abuse and Neglect (SCAN) at the emergency department. Eur J Pediatr. 2023 Jan;182(1):79-87. doi: 10.1007/s00431-022-04635-0. Epub 2022 Oct 5. PMID: 36198865; PMCID: PMC9534589. |
Geen restricties |
|
Imke van Kessel |
Kinderarts, fellow sociale pediatrie, Amphia Ziekenhuis Breda |
Geen |
Geen |
Geen restricties |
|
Monique Trijbels |
kinderarts, medisch directeur van de Stichting Landelijk Expertise Centrum Kindermishandeling (UMC Utrecht) |
Geen |
Geen |
Geen restricties |
|
Eline van den Heuvel |
Kinderarts, fellow sociale pediatrie UMC Utrecht |
Fellowship sociale pediatrie (0,6 fte): hierbinnen werkzaam als junior-LECK arts en gedetacheerd bij het Nederlands Forensisch Instituut (NFI) Promotieonderzoek (0,2 fte): signaleren kindermishandeling op de spoedeisende hulp |
Signaleren kindermishandeling op de SEH, inclusief implementatie NSK is gefinancierd door ZonMw “ Geweld hoort nergens thuis”
Het NSK wordt geïmplementeerd door ziekenhuizen zelf (verzamelde data is gedeeld intellectueel eigendom). Nationale implementatie van het NSK is doel van de begeleidingscommissie van het implementatie onderzoek. Ik heb hierbij geen financieel of persoonlijk (reputatie) belang.
Co-auteur van Hoedeman F, Puiman PJ, van den Heuvel EAL, Affourtit MJ, Bakx R, Langendam MW, van de Putte EM, Russel-Kampschoer IMB, Schouten MCM, Teeuw AH, de Koning HJ, Moll HA. A validated Screening instrument for Child Abuse and Neglect (SCAN) at the emergency department. Eur J Pediatr. 2023 Jan;182(1):79-87. doi: 10.1007/s00431-022-04635-0. Epub 2022 Oct 5. PMID: 36198865; PMCID: PMC9534589. |
Geen restricties |
|
Elise van de Putte |
Emeritus hoogleraar kindergeneeskunde | Divisie Kinderen, Sociale pediatrie |
|
ZonMW implementatie NSK
De implementatie van het Nationaal Signaleringsinstrument Kindermishandeling is mogelijk gemaakt door financiering van ZonMw. Het uiteindelijke doel is om dit instrument in heel Nederland te implementeren. Dat is niet een persoonlijk doel maar een doel van de begeleidingscommissie die geïnstalleerd is rond deze implementatie. Er zijn geen enkele financiële belangen voor mijzelf en ik zie het ook niet als een persoonlijk reputatie belang. Co-auteur van Hoedeman F, Puiman PJ, van den Heuvel EAL, Affourtit MJ, Bakx R, Langendam MW, van de Putte EM, Russel-Kampschoer IMB, Schouten MCM, Teeuw AH, de Koning HJ, Moll HA. A validated Screening instrument for Child Abuse and Neglect (SCAN) at the emergency department. Eur J Pediatr. 2023 Jan;182(1):79-87. doi: 10.1007/s00431-022-04635-0. Epub 2022 Oct 5. PMID: 36198865; PMCID: PMC9534589. |
Geen restricties |
|
Kristine Beumer |
Senior Wetenschappelijk Medewerker (NFI deskundige forensische geneeskunde minderjarigen bij Nederlands Forensisch Instituut, betaald, 1 fte. Forensisch arts KNMG bij Veiligheids-en-Gezondheidsregio-Gelderland-Midden, betaalde functie, 0,33 fte. |
Secretaris bestuur Forensisch Medisch genootschap, onbetaalde functie |
ZonMw: Werkgroep richtlijn forensisch medisch onderzoek letsel en zeden. |
Geen restricties |
|
Huub Nijs |
Forensisch arts, Nederlands Forensisch Instituut |
Geen |
Rijksambtenaar, 1fte bij het Nederlands Forensisch Instituut |
Geen restricties |
|
Kelsey van Son |
SEH-arts in het Canisius Wilhelmina Ziekenhuis te Nijmegen |
Lid sectie Mishandeling en Geweld van de Nederlandse Vereniging voor Spoedeisende Hulp Artsen (NVSHA) |
Geen |
Geen restricties |
|
Henrique Sachse |
Vereniging Vertrouwensartsen Kindermishandeling en huiselijk geweld |
adviseur update richtlijn Kindermishandeling Jeugdgezondheidszorg |
alleen vacatiegelden richtlijn Kindermishandeling Jeugdgezondheidszorg |
Geen restricties |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door deelname van relevante patiëntenorganisaties aan de need-for-update en/of prioritering. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijnmodules zijn tevens ter commentaar voorgelegd aan alle relevante patiëntenorganisaties in de stuur- en expertisegroep (zie ‘Samenstelling cluster’ onder ‘Verantwoording’) en aan alle patiëntenorganisaties die niet deelnemen aan de stuur- en expertisegroep, maar wel hebben deelgenomen aan de need-for-update (zie ‘Need-for-update’ onder ‘Verantwoording’). De eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Wkkgz & Kwalitatieve raming van mogelijke substantiële financiële gevolgen
Bij de richtlijnmodules zijn conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling zijn de richtlijnmodules op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
|
Module |
Uitkomst raming |
Toelichting |
|
Signalering van geweld in afhankelijkheidsrelaties op de SEH - screeningsinstrumenten |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen financiële gevolgen verwacht. |
De kwalitatieve raming volgt na de commentaarfase.
Werkwijze
AGREE
Deze richtlijnmodules zijn opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 3.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Need-for-update, prioritering en uitgangsvragen
Tijdens de need-for-update fase (maart 2023) inventariseerde het cluster de geldigheid van de richtlijnmodules binnen het cluster. Naast de partijen die deelnemen aan de stuur- en expertisegroep zijn hier ook andere stakeholders voor benaderd. Per richtlijnmodule is aangegeven of deze geldig is, herzien moet worden, kan vervallen of moet worden samengevoegd. Ook was er de mogelijkheid om nieuwe onderwerpen aan te dragen die aansluiten bij één (of meerdere) richtlijn(en) behorend tot het cluster. De richtlijnmodules waarbij door één of meerdere partijen werd aangegeven herzien te worden, werden doorgezet naar de prioriteringsronde. Ook suggesties voor nieuwe richtlijnmodules werden doorgezet naar de prioriteringsronde. Afgevaardigden vanuit de partijen in de stuur- en expertisegroep werden gevraagd om te prioriteren (zie ‘Samenstelling cluster’ onder ‘Verantwoording’). Hiervoor werd de RE-weighted Priority-Setting (REPS) – tool gebruikt. De uitkomsten (ranklijst) werd gebruikt als uitgangspunt voor de discussie. Voor de geprioriteerde richtlijnmodules zijn door de het cluster concept-uitgangsvragen herzien of opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde het cluster welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. Het cluster waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde het cluster tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd indien mogelijk gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding). GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
Tabel Gradaties voor de kwaliteit van wetenschappelijk bewijs
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in een richtlijnmodule volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
COSMIN
The COSMIN Risk of Bias tool was used to assess the quality of single studies for each measurement property. Thereby, the worst-score-counts method was used to determine the risk of bias, this means that the lowest rating given in a box determines the final rating, i.e., the quality of the study. The results of each reported measurement property was rated against the updated criteria for good measurement properties (Table 1). Each result was rated as either sufficient (+), insufficient (–), or indeterminate (?).
Table 1. Criteria for good measurement properties (Prinsen, 2018)
The level of evidence of the literature was evaluated as described in the COSMIN user manual for systematic reviews of patient-reported outcome measures (Prinsen, 2018). The following four factors were taken into account: (1) risk of bias (i.e., the methodological quality of the studies), (2) inconsistency (i.e., unexplained inconsistency of results across studies), (3) imprecision (i.e., total sample size of the available studies), and (4) indirectness (i.e., evidence from different populations than the population of interest in the review). The quality of evidence could be downgraded with one level (e.g., from high to moderate evidence) if there is serious risk of bias, with two levels (e.g., from high to low) if there is very serious risk of bias, or with three levels (i.e., from high to very low) if there is extremely risk of bias. The quality of the evidence could be downgraded with one or two levels for inconsistency, imprecision (-1 if total N=50-100; -2 if total N<50) and indirectness. Observational studies start at low quality of evidence.
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door het cluster wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. Het cluster heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
Tabel Sterkte van de aanbevelingen
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
Bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de richtlijnmodule Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd voorgelegd aan alle partijen die benaderd zijn voor de need-for-update fase. De commentaren werden verzameld en besproken met het cluster. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door het cluster. De definitieve richtlijnmodule werd ter autorisatie of goedkeuring voorgelegd aan de partijen die beschreven staan bij ‘Initiatief en autorisatie’ onder ‘Verantwoording’.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Prinsen CAC, Mokkink LB, Bouter LM, Alonso J, Patrick DL, de Vet HCW, Terwee CB. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018 May;27(5):1147-1157. doi: 10.1007/s11136-018-1798-3. Epub 2018 Feb 12. PMID: 29435801; PMCID: PMC5891568.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Zoekacties zijn opvraagbaar. Neem hiervoor contact op met de Richtlijnendatabase.