Cholecystectomie bij acute cholecystitis
Uitgangsvraag
Moet acute cholecystitis behandeld worden met een directe of uitgestelde cholecystectomie?
Aanbeveling
Opereer bij voorkeur cholecystitis in de acute fase van de ziekte binnen 72 uur na presentatie.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Er is literatuuronderzoek verricht naar het effect van vroege cholecystectomie (binnen 72 uur) vergeleken met enkele weken uitgestelde cholecystectomie (“afkoelen”) in patiënten met acute cholecystitis. Er werden twee systematische reviews en vier individuele studies geïncludeerd die deze vergelijking onderzochten. De cruciale uitkomstmaat kwaliteit van leven werd niet gerapporteerd in de geïncludeerde studies. De cruciale uitkomstmaat complicaties werd op verschillende manieren gerapporteerd in de studies. Voor verschillen in postoperatieve complicaties werd geen klinisch relevant verschil gevonden, met een zeer lage bewijskracht. Voor verschillen in risico op galwegletsel werd geen klinisch relevant verschil gevonden, terwijl voor bloedverlies wel een klinisch relevant verschil werd gevonden, in het voordeel van vroege cholecystectomie. Voor zowel het risico op galwegletsel als voor bloedverlies werd een zeer lage bewijskracht gevonden. Voor de belangrijke uitkomstmaten conversie en totale verblijfsduur in het ziekenhuis werd een redelijke bewijskracht gevonden. Vroege cholecystectomie verlaagt mogelijk het conversiepercentage en de verblijfsduur in het ziekenhuis ten opzichte uitgestelde cholecystectomie. Vroege cholecystectomie verlaagt met name de kans op recidief cholecystitis. Voor de belangrijke uitkomstmaat operatieduur werd geen klinisch relevant verschil en een zeer lage bewijskracht gevonden. Eén studie rapporteerde de belangrijke uitkomstmaat mortaliteit. Er werd geen mortaliteit gezien in beide groepen.
Routinematig uitstellen van cholecystectomie bij cholecystitis lijkt te leiden tot meer opname dagen, terwijl er geen klinisch relevante winst uit voortvloeit voor een van de onderzochte parameters.
In de geïncludeerde studies ontbrak informatie over de totale duur van de symptomen. Voor het bepalen van het interval tot operatie werd gerekend vanaf de presentatie. In deze vergelijking zijn resultaten afgezet van opereren binnen 72 uur na presentatie (op SEH) versus na enkele weken uitstel. Niet beantwoord is de vraag hoe lang symptomen mogen bestaan om nog te kunnen spreken van een acute cholecystitis. Het is denkbaar dat de duur van klachten voorafgaand aan presentatie, invloed heeft op de peroperatieve situatie bij een operatie in de acute fase.
Kwaliteit van bewijs
De overall kwaliteit van bewijs is zeer laag. Dit betekent dat we zeer onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege ernstige:
- Risk of Bias: methodologische beperkingen manier van toewijzing van randomisatie en blindering.
- Inconsistentie: inconsistentie van de resultaten.
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grenzen van klinische relevantie overschrijdt.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Vanuit patiënt perspectief en vanuit (zorg)economisch perspectief lijkt er nadeel te kunnen ontstaan door het routinematig uitstellen van cholecystectomie voor acute cholecystitis. Het totaal aantal ziektedagen neemt toe, zonder daarvoor in de plaats een aantoonbaar gezondheidsvoordeel te bereiken. Door een acuut uitgevoerde cholecystectomie is een patiënt dus sneller geholpen. In hoeverre dit zijn weerslag heeft op de kwaliteit van leven is weliswaar niet onderzocht maar het lijkt voor de hand liggend dat verkorten van de ziekteduur voor de patiënt en diens omgeving voordelig is.
Kostenaspecten
Het is onwaarschijnlijk dat een vroege cholecystectomie tot toename van zorgkosten leidt. Aannemelijker is het dat zowel de zorg gebonden kosten (ziekenhuisverblijf) als te verwachten economische kosten (uitval van patiënt uit het maatschappelijk verkeer en daarmee uit diens bijdrage aan de productiviteit) juist lager zijn dan na een uitgestelde operatie, aangezien het enige klinisch relevante verschil in uitkomsten lijkt te zijn dat de totale opnameduur korter is na een vroege cholecystectomie.
Gelijkheid ((health) equity/equitable)
De gezondheidsgelijkheid is niet in het geding bij de afweging tussen opereren in de acute fase versus na uitstel. Er is geen te verwachten verschil dat hiertoe aanleiding zou kunnen geven.
Aanvaardbaarheid:
Ethische aanvaardbaarheid
De interventie lijkt aanvaardbaar voor de betrokkenen. Er zijn geen ethische bezwaren. Er is geen aantoonbaar verhoogd risico of ander relevant nadeel door de interventie voor de patiënt.
Duurzaamheid
Bij de vergelijking is het belangrijkste duurzaamheidsaspect de totale opnameduur en daarmee beslag op beschikbare middelen in de (acute) zorg. Er is op grond van deze analyse mogelijk enig duurzaamheidsvoordeel te verwachten in de interventiearm (acute cholecystectomie).
Haalbaarheid
De interventie is haalbaar. De interventie is zeker in een deel van de Nederlandse praktijk al standaardzorg en zou probleemloos moeten kunnen worden ingevoerd in alle Nederlandse ziekenhuizen.
Voor acute versus uitgestelde cholecystectomie is geen andere zorg of zorgverlener en geen ander materiaal benodigd, dan de chirurgische basiszorg die in alle ziekenhuizen in Nederland voorhanden is. Aangezien spoedeisende chirurgische zorg in heel Nederland goed toegankelijk is voor alle patiënten, is het voor de hand liggend om bij presentatie met acute cholecystitis in de regel te kiezen voor een vroege cholecystectomie.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Op grond van de geanalyseerde literatuur mag worden geconcludeerd dat er in termen van veiligheid geen belangrijke voor- of nadelen lijken te bestaan voor het uitvoeren van een cholecystectomie in de acute fase van cholecystitis. Omdat er in logistieke zin (totale duur van opname en dus ziekte) wel voordeel lijkt te bestaan voor een acuut uitgevoerde cholecystectomie en daarmee waarschijnlijk het patiënt comfort en het gebruik van middelen verbeteren, is de werkgroep van mening dat het aan te bevelen is om bij voorkeur een cholecystectomie uit te voeren in de acute fase van cholecystitis.
Eindoordeel:
Sterke aanbeveling voor.
Onderbouwing
Cholecystitis in most cases requires a surgical intervention. The optimal timing of surgery is open for debate. Immediate or semi-acute cholecystectomy provides the quickest relief of symptoms but may technically be more challenging and may thus hold an increased risk of surgical complications. Alternatively the operation can be postponed for several weeks aiming for improved circumstances, but accepting the risk of interval relapse or complications of biliary obstruction. Delayed surgery also introduces the potential difficulty of handling tissue changes due to inflammation and scarring. Which strategy provides most safety and at the same time reduces the duration of symptoms most effectively is the issue underlying this literature analysis
Summary of Findings
Early cholecystectomy compared with delayed cholecystectomy for acute cholecystitis
Population: Patients with acute cholecystitis
Intervention: Early cholecystectomy (<72h)
Comparator: Delayed cholecystectomy
|
Outcome Timeframe |
Study results and measurements |
Absolute effect estimates |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
Delayed cholecystectomy |
Early cholecystectomy |
||||
|
Postoperative complications (critical)
|
Relative risk: 0.81 (CI 95% 0.46 - 1.43) Based on data from 967 participants in 10 studies
|
120 per 1000 |
97 per 1000 |
Very low Due to serious inconsistency, Due to very serious imprecision1 |
The evidence is very uncertain about the effect of early cholecystectomy on postoperative complications when compared with delayed cholecystectomy in patients with acute cholecystitis. |
|
Difference: 23 fewer per 1000 (CI 95% 65 fewer - 52 more) |
|||||
|
Bile duct injury (critical)
|
Relative risk: 1.04 (CI 95% 0.07 - 15.79) Based on data from 420 participants in 4 studies
|
90 per 1000 |
94 per 1000 |
Very low Due to serious risk of bias, Due to very serious imprecision, Due to serious inconsistency2 |
The evidence is very uncertain about the effect of early cholecystectomy on bile duct injury when compared with delayed cholecystectomy in patients with acute cholecystitis. |
|
Difference: 4 more per 1000 (CI 95% 84 fewer - 1331 more) |
|||||
|
Bile leak (critical)
|
Relative risk: 0.7 (CI 95% 0.03 - 16.56) Based on data from 240 participants in 3 studies
|
17 per 1000 |
12 per 1000 |
Very low Due to serious risk of bias, Due to very serious imprecision3 |
The evidence is very uncertain about the effect of early cholecystectomy on bile leak when compared with delayed cholecystectomy in patients with acute cholecystitis. |
|
Difference: 5 fewer per 1000 (CI 95% 16 fewer - 265 more) |
|||||
|
Wound infection (critical)
|
Relative risk: 0.45 (CI 95% 0.33 - 0.62) Based on data from 350 participants in 5 studies
|
166 per 1000 |
75 per 1000 |
Low Due to serious risk of bias, Due to serious imprecision4 |
Early cholecystectomy may result in little to no difference in wound infection when compared with delayed cholecystectomy in patients with acute cholecystitis. |
|
Difference: 91 fewer per 1000 (CI 95% 111 fewer - 63 fewer) |
|||||
|
Conversion rate (important)
|
Relative risk: 0.48 (CI 95% 0.31 - 0.72) Based on data from 1317 participants in 14 studies
|
112 per 1000 |
54 per 1000 |
Moderate Due to serious risk of bias5 |
Early cholecystectomy probably decreases conversion rate (important) |
|
Difference: 58 fewer per 1000 (CI 95% 77 fewer - 31 fewer) |
|||||
|
Blood loss (critical)
|
Measured by: Scale: - Lower better Based on data from 370 participants in 3 studies
|
Mean |
Mean |
Very low Due to serious risk of bias, Due to serious imprecision, Due to serious inconsistency6 |
The evidence is very uncertain about the effect of early cholecystectomy on blood loss when compared with delayed cholecystectomy in patients with acute cholecystitis. |
|
Difference: MD 14.47 lower (CI 95% 99.46 lower - 70.52 higher) |
|||||
|
Total length of hospital stay (important)
|
Measured by: Scale: - Lower better Based on data from 1267 participants in 13 studies
|
Mean |
Mean |
Moderate Due to serious risk of bias7 |
Early cholecystectomy probably decreases total length of hospital stay (important) |
|
Difference: MD 3.85 lower (CI 95% 5.15 lower - 2.55 lower) |
|||||
|
Duration of surgery (important)
|
Measured by: Scale: - Lower better Based on data from 1169 participants in 11 studies
|
Mean |
Mean |
Very low Due to serious risk of bias, Due to serious inconsistency, Due to serious imprecision8 |
The evidence is very uncertain about the effect of early cholecystectomy on duration of surgery when compared with delayed cholecystectomy in patients with acute cholecystitis. |
|
Difference: MD 5.30 lower (CI 95% 19.10 lower - 8.49 higher) |
|||||
|
Mortality (important)
|
Based on data from 100 participants in 1 studies
|
Lal (2021) reported no mortality in the early cholecystectomy and late cholecystectomy group. |
Low Due to serious risk of bias, Due to very serious imprecision9 |
Early cholecystectomy may have little or no difference on mortality (critical) |
|
|
Quality of life (critical)
|
|
No studies were found that looked at quality of life (important) |
|
|
|
1. Inconsistency: serious. Point estimates vary widely, The direction of the effect is not consistent between the included studies; Imprecision: very serious. Overlap of both limits of the 95% confidence interval with the minimal clinically important difference;
2. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias; Inconsistency: serious. The direction of the effect is not consistent between the included studies; Imprecision: very serious. Overlap of both limits of the 95% confidence interval with the minimal clinically important difference;
3. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias; Imprecision: very serious. Overlap of both limits of the 95% confidence interval with the minimal clinically important difference;
4. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias; Imprecision: serious. Overlap of the lower limit of the 95% confidence interval with the minimal clinically important difference;
5. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias;
6. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias; Inconsistency: serious. The direction of the effect is not consistent between the included studies; Imprecision: serious. Wide confidence intervals;
7. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias;
8. Risk of Bias: serious. Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Inadequate/lack of blinding of outcome assessors, resulting in potential for detection bias; Inconsistency: serious. The direction of the effect is not consistent between the included studies; Imprecision: serious. Overlap of the lower limit of the 95% confidence interval with the minimal clinically important difference;
9. Imprecision: very serious. Low number of patients, Only data from one study.
Description of studies
A total of two systematic reviews and four additional randomized controlled trials were included in the analysis of the literature. Important study characteristics and results are summarized in table 2. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Systematic reviews
Wu (2023) performed a systematic review to investigate differences in efficacy, safety, and potential benefits between early laparoscopic cholecystectomy (ELC) and delayed laparoscopic cholecystectomy (DLC) in patients with acute cholecystitis. PubMed, Springer, and Cochrane Library were searched for studies published between January 1st 1999 and January 1st 2022. Randomized controlled trials or retrospective comparative studies which compared ELC to DLC irrespective of age, and which analyzed at least one of the primary outcomes were included in the systematic review. In total, the systematic review included 34 studies, of which 21 were RCTs. This analysis only included the RCTs that used <72 hours for the ELC group.
Borzellino (2021) performed a systematic review to explore the hypothesis that immediate cholecystectomy (within 24h) could reduce post-operative complications when compared with delayed cholecystectomy. PubMed, Cochrane Library, Embase, and ChlinicalTrials.gov were searched. Randomized trials comparing different timings of laparoscopic cholecystectomy were included if the criteria for diagnosis of acute cholecystitis, the population, timing for surgery, and data on post-operative complications were reported. In total, fifteen studies were included in the systematic review. This analysis only included four RCTs in addition to the systematic review of Wu (2023).
Randomized controlled trials
Yadav (2023) performed a randomized controlled trial to compare early laparoscopic cholecystectomy with delayed laparoscopic cholecystectomy in patients with acute cholecystitis. The study was conducted on patients admitted to SMS Hospital in Jaipur, India. The inclusion criteria were: eighteen years of age and older, either sex, acute symptoms and a diagnosis of acute cholecystitis based on clinical and laboratory investigations, confirmed cases of cholelithiasis by USG/CT/MRCP, and written informed consent.
Lal (2021) performed a randomized controlled trial to compare outcomes between early and delayed laparoscopic cholecystectomies. The study was conducted on patients admitted to ESI-PGIMSR and Model Hospital in New Delhi, India. The inclusion criteria were: age from eighteen to 60 years of either sex, ASA grade I and II.
Mustafa (2016) performed a randomized controlled trial to compare early versus delayed laparoscopic cholecystectomy in patients with acute cholecystitis. The study was conducted at Ghurki Trust Teaching Hospital in Lahore, Pakistan. The inclusion criteria were: right upper quadrant pain and tenderness for more than six hours with fever >100 degrees Fahrenheit and total leukocyte count >10.000/mm3, and confirmed diagnosis on abdominal ultrasound showing presence of gall stones, distended gallbladder and gallbladder wall thickness >3mm.
Faizi (2013) performed a randomized controlled trial to compare early and interval laparoscopic cholecystectomy. The study was conducted on patients admitted to Nishtar Hospital Multan or Ali Shirazi Hospital Sahiwal in Pakistan. The inclusion criteria were: diagnosis of acute cholecystitis on the basis of history, clinical examination, and investigations.
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
Included in systematic review Wu, 2023 |
||||||
|
Lo, 1998 |
N at baseline I: 45 C: 41
Age (mean ± SD) NR
Sex NR
Pathological chracteristics: NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (8-12 weeks) |
NR |
Conversion rate, Postoperative complications, Operation time, Postoperative hospital stay time, Total hospital stay time
|
NR |
LOW |
|
Serralta, 2003 |
N at baseline I: 82 C: 87
Age (mean ± SD) NR
Sex NR
Pathological characteristics Phlegmonous gangrenous
|
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (>72 h) |
NR |
Conversion rate, Postoperative complications, Operation time, Postoperative hospital stay time, Total hospital stay time
|
NR |
LOW |
|
Al-Mulhim, 2008 |
N at baseline I: 82 C: 114
Age (mean ± SD) NR
Sex NR
Pathological characteristics NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (>72h)
|
NR |
Conversion rate, Postoperative complications, Postoperative hospital stay time, Total hospital stay time
|
NR |
LOW |
|
Macafee, 2009 |
N at baseline I: 36 C: 36
Age (mean ± SD) NR
Sex NR
Pathological characteristics NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (>12 weeks) |
NR |
Conversion rate, Intraoperative complications, Postoperative complications, Postoperative hospital stay time, Total hospital stay time
|
NR |
LOW |
|
Gul, 2013 |
N at baseline I: 30 C: 30
Age (mean ± SD) NR
Sex NR
Pathological characteristics NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (6-8 weeks) |
NR |
Conversion rate, Postoperative complications, Operation time, Total hospital stay time
|
NR |
LOW |
|
Ozkardes, 2014 |
N at baseline I: 30 C: 30
Age (mean ± SD) NR
Sex NR
Pathological characteristics NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (6-8 weeks) |
NR |
Conversion rate, Intraoperative complications, Postoperative complications, Operation time, Total hospital stay time
|
NR |
LOW |
|
Rajcok, 2016 |
N at baseline I: 31 C: 31
Age (mean ± SD) NR
Sex NR
Pathological characteristics NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (6-8 weeks) |
NR |
Conversion rate, Postoperative complications, Operation time, Total hospital stay time
|
NR |
LOW |
|
Roulin, 2016 |
N at baseline I: 42 C: 44
Age (mean ± SD) NR
Sex NR
Pathological characteristics NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (>6 weeks) |
NR |
Conversion rate, Intraoperative complications, Postoperative complications, Operation time, Total hospital stay time
|
NR |
LOW |
|
Isil, 2021 |
N at baseline I: 88 C: 88
Age (mean ± SD) NR
Sex NR
Pathological characteristics NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (4-8 weeks) |
NR |
Conversion rate, Postoperative complications, Operation time, Total hospital stay time
|
NR |
LOW |
|
Included in systematic review Borzellino, 2021 |
||||||
|
El Kordy, 2019 |
N at baseline I: 20 C: 20
Age (mean ± SD) NR
Sex NR
Existence of symptoms: <72 hours |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (6-8 weeks) |
NR |
Post-operative complications, Conversion, Hospital stay |
NR |
Some concerns (no outcome blinding) |
|
Jan, 2016 |
N at baseline I: 50 C: 50
Age (mean ± SD) NR
Sex NR
Existence of symptoms: <72 hours |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (>72h) |
NR |
Post-operative complications Operative time, Postoperative stay, Total hospital stay, Conversion rate |
NR |
Some concerns (no outcome blinding) |
|
Individual studies |
||||||
|
Yadav, 2023 |
N at baseline I: 30 C: 30
Age (mean ± SD) NR
Sex NR
Existence of symptoms: Presentation to emergency department with acute symptoms |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (6-8 weeks) |
NR |
Operative time, Blood loss, Conversion, Total hospital stay, Postoperative complications |
No conflicts of interest declared, no funding |
Some concerns |
|
Lal, 2021 |
N at baseline I: 50 C: 50
Age (mean ± SD) I: 41.0 ± 12.29 C: 38.04 ± 11.30
Sex (male/ female) I: 8/42 C: 10/40
Pain duration (mean ± SD): I: 25.0 ± 9.539 C: 23.24 ± 7.305 |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (6-12 weeks) |
NR |
Operative time, Blood loss, Conversion, Intraoperative complications, Postoperative complications, Mortality Hospital stay |
No conflicts of interest declared, no funding |
Some concerns |
|
Mustafa, 2016 |
N at baseline I: 105 C: 105
Age (mean ± SD) I: 50.30 ± 8.46 C: 51.95 ± 7.58
Sex (male/ female) I: 19/86 C: 21/84
Existence of symptoms: At least 6 hours |
Intervention: Early cholecystectomy (48-72h)
Control: delayed cholecystectomy (6-12 weeks) |
NR |
Operative time, Blood loss, Bile duct injury, Postoperative pain |
NR |
Some concerns |
|
Faizi, 2013 |
N at baseline I: 25 C: 25
Age (mean ± SD) I: 40.21 ± 3.33 C: 42.87 ± 4.54
Sex (male/ female) I: 11/14 C: 15/10
Existence of symptoms: NR |
Intervention: Early cholecystectomy (<72h)
Control: delayed cholecystectomy (NR) |
1 week (for com-plications) |
Post-operative complications, Conversion |
NR |
Some concerns |
*For further details, see risk of bias table in the appendix
Results
Quality of life (critical)
None of the studies reported the outcome measure quality of life.
Complications (critical)
Postoperative complications
Two systematic reviews reported the outcome measure postoperative complications (Borzellino, 2021; Wu, 2023). Of the 466 patients who underwent early cholecystectomy, 47 (10.1%) patients had a postoperative complication, compared with 60 of the 501 patients (12.0%) who underwent delayed cholecystectomy (Figure 1). The risk ratio was 0.81 (95% CI 0.46 to 1.43), in favor of the patients who underwent early cholecystectomy. The risk difference was -0.01 (95% CI -0.09 to 0.06), in favor of the patients who underwent early cholecystectomy. This difference is not considered clinically relevant.
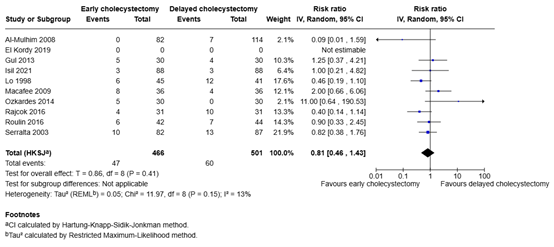
Figure 1. Postoperative complications for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Wound infection
One systematic review and three individual studies reported the outcome measure wound infection (Borzellino, 2021; Faizi, 2013; Lal, 2021; Yadav, 2023). Of the 175 patients who underwent early cholecystectomy, 13 patients (7.4%) had a wound infection, compared with 29 of the 175 patients (16.6%) who underwent delayed cholecystectomy (Figure 2). The risk ratio was 0.45 (95% CI 0.33 to 0.62), in favor of the patients who underwent early cholecystectomy. The risk difference was -0.08 (95% CI -0.25 to 0.09), in favor of the patients who underwent early cholecystectomy. This difference is not considered clinically relevant.
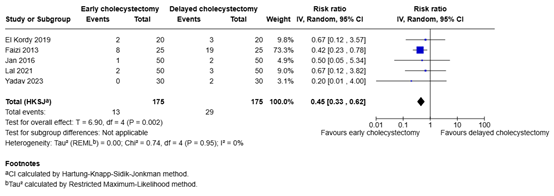
Figure 2. Wound infection for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Bile leak
One systematic review and one individual study reported the outcome measure bile leak (Borzellino, 2021; Lal, 2021). Of the 120 patients who underwent early cholecystectomy, 1 patient (0.8%) had bile leak, compared with 2 of the 120 patients (1.7%) who underwent delayed cholecystectomy (Figure 3). The risk ratio was 0.70 (95% CI 0.03 to 16,56), and the risk difference was -0.01 (95% CI -0.07 to 0.04), in favor of the patients who underwent early cholecystectomy. This difference is not considered clinically relevant.
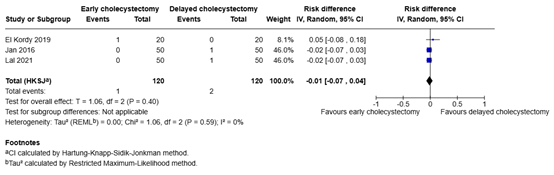
Figure 3. Bile leak for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Bile duct injury
One systematic review and three individual studies reported the outcome measure bile duct injury (Faizi, 2013; Jan, 2016; Mustafa, 2016; Yadav, 2023). Of the 210 patients who underwent early cholecystectomy, 17 patients (8.1%) had bile duct injury, compared with 19 of the 210 patients (9.0%) who underwent delayed cholecystectomy (Figure 4). The risk ratio was 1.04 (95% CI 0.07 to 15.79), in favor of the patients who underwent delayed cholecystectomy. The risk difference was -0.07 (-0.27 to 0.13), in favor of the patients who underwent early cholecystectomy. This difference is considered clinically relevant.
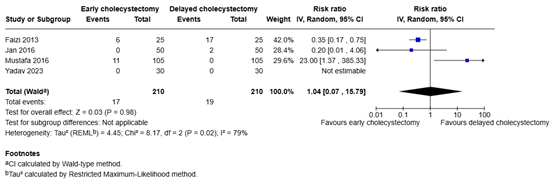
Figure 4. Bile duct injury for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Blood loss
Three individual studies reported the outcome measure blood loss (Lal, 2021; Mustafa, 2016; Yadav, 2023). The mean difference in blood loss between the 185 patients who underwent early cholecystectomy and the 185 patients who underwent delayed cholecystectomy was -14.47 mL (95% CI -99.46 to 70.52), in favor of the patients who underwent early cholecystectomy (Figure 5). This difference is considered clinically relevant.
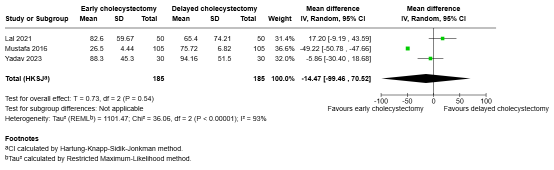
Figure 5. Blood loss for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Length of hospital stay (important)
Total length of hospital stay
Two systematic reviews and two individual studies reported the outcome measure total length of hospital stay (Borzellino, 2021; Lal, 2021; Wu, 2023; Yadav, 2023). The mean difference in total length of hospital stay between the 616 patients who underwent early cholecystectomy and the 651 patients who underwent delayed cholecystectomy was -3.85 days (95% CI -5.15 to -2.55), in favor of the patients who underwent early cholecystectomy (Figure 6). This difference is considered clinically relevant.
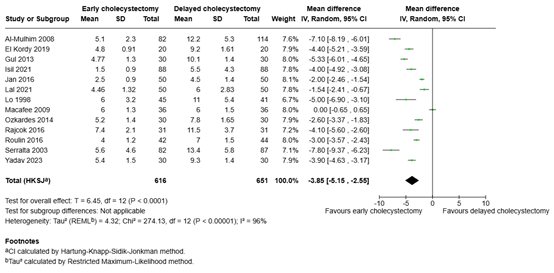
Figure 6. Total length of hospital stay for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Postoperative length of hospital stay
Two systematic reviews and one individual studies reported the outcome measure postoperative length of hospital stay (Borzellino, 2021; Lal, 2021; Wu, 2023). The mean difference in postoperative length of hospital stay between the 345 patients who underwent early cholecystectomy and the 278 patients who underwent delayed cholecystectomy was 0.16 days (95% CI -1.09 to 1.41), in favor of the patients who underwent delayed cholecystectomy (Figure 7). This difference is not considered clinically relevant.
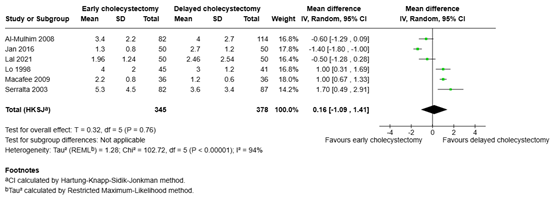
Figure 7. Postoperative length of hospital stay for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Conversion rate (important)
Two systematic reviews and four individual studies reported the outcome measure conversion rate (Borzellino, 2021; Faizi, 2013; Jan, 2016; Lal, 2021; Wu, 2023; Yadav, 2023). Of the 641 patients who underwent early cholecystectomy, 34 patients (5.3%) underwent conversion, compared with 76 of the 676 patients (11.2%) who underwent delayed cholecystectomy. The risk ratio was 0.48 (95% CI 0.31 to 0.72), in favor of the patients who underwent early cholecystectomy (Figure 8). The risk difference was -0.04 (95% CI -0.09 to 0.00), in favor of the patients who underwent early cholecystectomy. This difference is not considered clinically relevant.
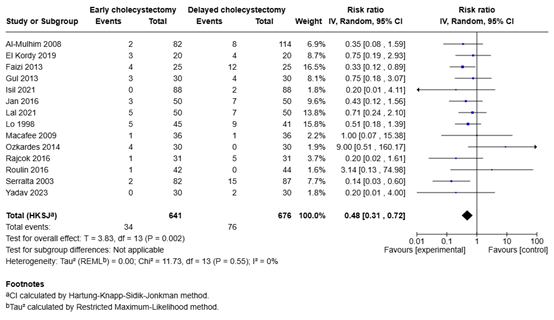
Figure 8. Conversion rate for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Duration of surgery (important)
Two systematic reviews and three individual studies reported the outcome measure postoperative operation time (Borzellino, 2021; Lal, 2021; Mustafa, 2016; Wu, 2023; Yadav, 2023). The mean difference in operation time between the 583 patients who underwent early cholecystectomy and the 586 patients who underwent delayed cholecystectomy was -5.30 minutes (95% CI -19.10 to 8.49), in favor of the patients who underwent early cholecystectomy (Figure 9). This difference is not considered clinically relevant.
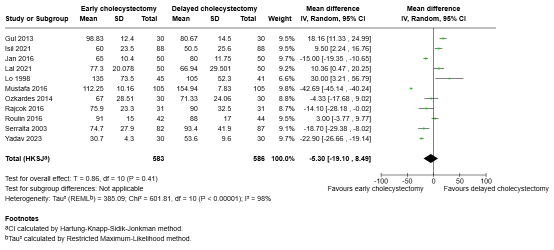
Figure 9. Operation time for early cholecystectomy versus delayed cholecystectomy in patients with acute cholecystitis
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Mortality (important)
One study reported the outcome measure mortality (Lal, 2021). No mortality was reported in both the intervention and control groups. Therefore, there is no clinically relevant difference between the groups.
A systematic review of the literature was performed to answer the following question(s):
What are (un)favorable effects of immediate cholecystectomy in patients with acute cholecystitis versus delay of the operation?
Table 1. PICO
| Patients | Patients with acute cholecystitis |
| Intervention | Early cholecystectomy (within 72 hours) |
| Control | Delayed cholecystectomy |
| Outcomes | Mortality, , length of hospital stay, , conversion rate, quality of life, duration of surgery, complications (surgical): bile duct injury, infection in gallbladder, per-operative blood loss |
| Other selection criteria | Study design: systematic reviews and randomized controlled trials |
Relevant outcome measures
The guideline panel considered quality of life and complications (bile duct injury, persistence or relapse of cholecystitis, intra-abdominal infection (abscess), as critical outcome measures for decision making; and mortality, length of hospital stay, conversion rate, and duration of surgery as important outcome measures for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
The guideline panel defined the following as minimal clinically (patient) important differences:
- Mortality: ARD 1%.
- Complications: ARD 5%:
- Wound infection: ARD 10%.
- Bile leak: ARD 2% .
- Length of hospital stay: 1 day.
- Conversion rate: ARD 10%.
- Quality of life: verschil van 10% van de maximale score.
- Duration of surgery: 15 min.
Search and select (Methods)
A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2000 to 19 January 2025 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) acute cholecystitis; (2) delayed cholecystectomy. Duplicates were removed using EndNote software. After deduplication a total of 1214 records were selected for title/abstract screening. Initially, 46 studies were selected based on title and abstract screening. After reading the full text, 40 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and six studies were included.
- Borzellino G, Khuri S, Pisano M, Mansour S, Allievi N, Ansaloni L, Kluger Y. Timing of early laparoscopic cholecystectomy for acute calculous cholecystitis: a meta-analysis of randomized clinical trials. World J Emerg Surg. 2021 Mar 25;16(1):16. doi:10.1186/s13017-21-00360-5. PMID: 33766077; PMCID: PMC7992835.
- El-Kordy, M. M., Aboulyazid, A. S. B., & Mahmoud, A. F. A. (2019). Comparison of outcomes of early versus delayed laparoscopic cholecystectomy in acute calcular cholecystitis. The Egyptian Journal of Hospital Medicine, 76(5), 4162-4168.
- Faizi, K. S., Ahmed, I., & Ahmad, H. (2013). Comparison of early versus delayed laparoscopic cholecystectomy: choosing the best. Pak J Medical Health Sci, 7, 212-5.
- Jan, Y., Shah, M., Hussain, S., Din, W., & Khan, A. (2016). Variables affecting outcome of laparoscopic cholecystectomy in acute cholecystitis. Pak J Surg, 32(1), 16-21.
- Lal, S., Rohitaj, R., Najim, M., Dua, M., Singh, V. K., & Chakravarti, S. (2021). Early and Delayed Laparoscopic Cholecystectomy in Acute Calculus Cholecystitis: A Prospective Randomized-comparative Study. World, 14(3), 150.
- Mustafa, M. I. T., Mustafa, A. I. T., Chaudhry, S. M., & Mustafa, R. I. T. (2016). Early vs delayed 1laparoscopic cholecystectomy in acute cholecystitis. Pak J Med Health Sci, 10(2), 371-3.
- Wu H, Liao B, Cao T, Ji T, Huang J, Luo Y, Ma K. Comparison of the safety profile, conversion rate and hospitalization duration between early and delayed laparoscopic cholecystectomy for acute cholecystitis: a systematic review and meta-analysis. Front Med (Lausanne). 2023 Dec 11;10:1185482. doi: 10.3389/fmed.2023.1185482. PMID: 38148916; PMCID: PMC10750350.
- Yadav, Rahul & RAO, HARSHITA & GOEL, GAURAB. (2023). A RANDOMIZED COMPARATIVE STUDY OF EARLY AND DELAYED LAPAROSCOPIC CHOLECYSTECTOMY IN ACUTE CHOLECYSTITIS: A TERTIARY CENTER EXPERIENCE AND REVIEW OF LITERATURE. International Journal of Current Pharmaceutical Research. 78-82.10.22159/ijcpr.2023v15i5.3059.
Risk of Bias tables
Risk of bias table for intervention studies (randomized controlled trials; based on Cochrane risk of bias tool and suggestions by the CLARITY Group at McMaster University)
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Yadav, 2023 |
Definitely yes
Reason: Single random technique through chit box method. |
Probably no
Reason: Not reported. |
Probably no
Reason: Not reported. |
Probably yes
Reason: No loss to follow-up reported. |
Definitely yes
Reason: All relevant outcomes were reported. |
Probably yes
Reason: No other problems noted. |
LOW (mortality) Some concerns (other outcomes)
|
|
Lal, 2021 |
Definitely yes
Reason: Block randomization was used. |
Definitely yes
Reason: Randomly generated opaque sealed envelopes were used. |
Probably no
Reason: Not reported. |
Definitely no
Reason: Loss-to-follow-up was more than 10% in both the intervention and control group. |
Definitely yes
Reason: All relevant outcomes were reported. |
Probably yes
Reason: No other problems noted. |
LOW (mortality) Some concerns (other outcomes)
|
|
Mustafa, 2016 |
Definitely yes
Reason: Randomization using lottery method. |
Probably no
Reason: Not reported. |
Probably no
Reason: Not reported. |
Probably yes
Reason: No loss to follow-up reported. |
Definitely yes
Reason: All relevant outcomes were reported. |
Probably yes
Reason: No other problems noted. |
LOW (mortality) Some concerns (other outcomes)
|
|
Faizi, 2013 |
Definitely yes
Reason: Randomization using random number table. |
Probably no
Reason: Not reported. |
Probably no
Reason: Not reported. |
Probably yes
Reason: No loss to follow-up reported. |
Probably no
Reason: The outcome measure postoperative hospital stay is not reported. |
Probably yes
Reason: No other problems noted. |
LOW (mortality) Some concerns (other outcomes)
|
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Agrawal R, Sood KC, Agarwal B. Evaluation of Early versus Delayed Laparoscopic Cholecystectomy in Acute Cholecystitis. Surg Res Pract. 2015;2015:349801. doi: 10.1155/2015/349801. Epub 2015 Feb 3. PMID: 25729775; PMCID: PMC4333337. |
Included in SR Wu |
|
Akhtar, N. N., Fawad, A. H. M. A. D., & Allam, K. M. (2016). Early versus delayed laparoscopic cholecystectomy in acute cholecystitis. Pak J Med Health Sci, 10(3), 1039-43. |
Not conform PICO: wrong P (delayed group consisted of patients with uncomplicated cholelithiasis) |
|
Alenezi AT, Bin Jerais SA, Al Yami NMH, Alluhaida AA, Alharbi AK, Al Salamah FSJ, Assiri FFM, Tahir E Hayat Mohammed M, Alqahtani FMD, Otayf MM. Impact of Surgical Timing on Outcomes in Patients With Acute Cholecystitis: A Systematic Review. Cureus. 2024 Oct 22;16(10):e72090. doi: 10.7759/cureus.72090. PMID: 39575012; PMCID: PMC11579627. |
Wrong study design: observational studies |
|
Bagepally BS, Haridoss M, Sasidharan A, Jagadeesh KV, Oswal NK. Systematic review and meta-analysis of gallstone disease treatment outcomes in early cholecystectomy versus conservative management/delayed cholecystectomy. BMJ Open Gastroenterol. 2021 Jul;8(1):e000675. doi: 10.1136/bmjgast-2021-000675. PMID: 34261757; PMCID: PMC8280848. |
Not conform PICO: wrong patients (gallstones, CBD stones or cholecystitis), early = within 7 days |
|
Cao AM, Eslick GD, Cox MR. Early Cholecystectomy Is Superior to Delayed Cholecystectomy for Acute Cholecystitis: a Meta-analysis. J Gastrointest Surg. 2015 May;19(5):848-57. doi: 10.1007/s11605-015-2747-x. Epub 2015 Mar 7. PMID: 25749854. |
Overlap with SR Wu |
|
Chandler CF, Lane JS, Ferguson P, Thompson JE, Ashley SW. Prospective evaluation of early versus delayed laparoscopic cholecystectomy for treatment of acute cholecystitis. Am Surg. 2000 Sep;66(9):896-900. PMID: 10993625. |
Included in SR Wu |
|
Coccolini F, Solaini L, Binda C, Catena F, Chiarugi M, Fabbri C, Ercolani G, Cucchetti A. Laparoscopic Cholecystectomy in Acute Cholecystitis: Refining the Best Surgical Timing Through Network Meta-Analysis of Randomized Trials. Surg Laparosc Endosc Percutan Tech. 2022 Dec 1;32(6):755-763. doi: 10.1097/SLE.0000000000001103. PMID: 36223286. |
Wrong comparison: between different moments of surgery |
|
Gu, X., Jing, L., & Ma, D. (2023). Meta analysis of the efficacy and safety of early and delayed laparoscopic surgery in acute cholecystitis. Archives of Clinical Psychiatry, 50(1). |
Wrong study design: case control studies |
|
Gul R, Dar RA, Sheikh RA, Salroo NA, Matoo AR, Wani SH. Comparison of early and delayed laparoscopic cholecystectomy for acute cholecystitis: experience from a single center. N Am J Med Sci. 2013 Jul;5(7):414-8. doi: 10.4103/1947-2714.115783. PMID: 24020050; PMCID: PMC3759068. |
Included in SR Wu |
|
Gurusamy K, Samraj K, Gluud C, Wilson E, Davidson BR. Meta-analysis of randomized controlled trials on the safety and effectiveness of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg. 2010 Feb;97(2):141-50. doi: 10.1002/bjs.6870. Erratum in: Br J Surg. 2010 Apr;97(4):624. PMID: 20035546. |
Overlap with SR Wu |
|
Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD005440. doi: 10.1002/14651858.CD005440.pub2. Update in: Cochrane Database Syst Rev. 2013 Jun 30;(6):CD005440. doi: 10.1002/14651858.CD005440.pub3. PMID: 17054258. |
Overlap with SR Wu |
|
Gutt CN, Encke J, Köninger J, Harnoss JC, Weigand K, Kipfmüller K, Schunter O, Götze T, Golling MT, Menges M, Klar E, Feilhauer K, Zoller WG, Ridwelski K, Ackmann S, Baron A, Schön MR, Seitz HK, Daniel D, Stremmel W, Büchler MW. Acute cholecystitis: early versus delayed cholecystectomy, a multicenter randomized trial (ACDC study, NCT00447304). Ann Surg. 2013 Sep;258(3):385-93. doi: 10.1097/SLA.0b013e3182a1599b. PMID: 24022431. |
Included in SR Wu |
|
Johansson M, Thune A, Blomqvist A, Nelvin L, Lundell L. Impact of choice of therapeutic strategy for acute cholecystitis on patient's health-related quality of life. Results of a randomized, controlled clinical trial. Dig Surg. 2004;21(5-6):359-62. doi: 10.1159/000081352. Epub 2004 Oct 7. PMID: 15475664. |
Same patient data as in SR Wu |
|
Johansson M, Thune A, Blomqvist A, Nelvin L, Lundell L. Management of acute cholecystitis in the laparoscopic era: results of a prospective, randomized clinical trial. J Gastrointest Surg. 2003 Jul-Aug;7(5):642-5. doi: 10.1016/s1091-255x(03)00065-9. PMID: 12850677. |
Included in SR Wu |
|
Kao LS, Ball CG, Chaudhury PK; for Members of the Evidence Based Reviews in Surgery Group. Evidence-based Reviews in Surgery: Early Cholecystectomy for Cholecystitis. Ann Surg. 2018 Dec;268(6):940-942. doi: 10.1097/SLA.0000000000002867. PMID: 29916874. |
Wrong study design: narrative review |
|
Kolla SB, Aggarwal S, Kumar A, Kumar R, Chumber S, Parshad R, Seenu V. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis: a prospective randomized trial. Surg Endosc. 2004 Sep;18(9):1323-7. doi: 10.1007/s00464-003-9230-6. Epub 2004 Jul 7. PMID: 15803229. |
Included in SR Wu |
|
Koti RS, Davidson CJ, Davidson BR. Surgical management of acute cholecystitis. Langenbecks Arch Surg. 2015 May;400(4):403-19. doi: 10.1007/s00423-015-1306-y. Epub 2015 May 14. PMID: 25971374. |
Wrong study design: narrative review |
|
Kumar, A., Nandini, S. O., & Shayana, A. (2024). A COMPARATIVE STUDY OF EARLY AND DELAYED LAPAROSCOPIC CHOLECYSTECTOMY IN MANAGEMENT OF ACUTE CHOLECYSTITIS. Int J Acad Med Pharm, 6(2), 990-996. |
Not conform PICO: wrong I (surgery within 7 days) |
|
Kumar, R., Achuta, S. G., Arjun, S., Chalapathi, D. V., Prakash, J., & Chowdary, G. T. (2019). A comparative study of early versus delayed laparoscopic cholecystectomy in acute cholecystitis and its associated complication. New Indian J Surg, 10(2), 205-12. |
Full text not available |
|
Lau H, Lo CY, Patil NG, Yuen WK. Early versus delayed-interval laparoscopic cholecystectomy for acute cholecystitis: a metaanalysis. Surg Endosc. 2006 Jan;20(1):82-7. doi: 10.1007/s00464-005-0100-2. Epub 2005 Oct 24. PMID: 16247580. |
Overlap with SR Wu |
|
Lyu Y, Cheng Y, Wang B, Zhao S, Chen L. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis: an up-to-date meta-analysis of randomized controlled trials. Surg Endosc. 2018 Dec;32(12):4728-4741. doi: 10.1007/s00464-018-6400-0. Epub 2018 Aug 23. PMID: 30167953. |
Overlap with SR Wu |
|
Macafee DA, Humes DJ, Bouliotis G, Beckingham IJ, Whynes DK, Lobo DN. Prospective randomized trial using cost-utility analysis of early versus delayed laparoscopic cholecystectomy for acute gallbladder disease. Br J Surg. 2009 Sep;96(9):1031-40. doi: 10.1002/bjs.6685. PMID: 19672930. |
Included in SR Wu |
|
Mahmood, K., Imran, M., & Asif, K. (2018). Early versus interval laparoscopic cholecystectomy in acute cholecystitis. Pak J Med Health Sci, 12, 972-973. |
Wrong study design: quasi-experimental |
|
Menahem B, Mulliri A, Fohlen A, Guittet L, Alves A, Lubrano J. Delayed laparoscopic cholecystectomy increases the total hospital stay compared to an early laparoscopic cholecystectomy after acute cholecystitis: an updated meta-analysis of randomized controlled trials. HPB (Oxford). 2015 Oct;17(10):857-62. doi: 10.1111/hpb.12449. Epub 2015 Jul 27. PMID: 26218858; PMCID: PMC4571752. |
Overlap with SR Wu |
|
Mohapatra. Early and Delayed Laparoscopic Cholecystectomy in Case of Acute Cholecystitis |
Wrong study design: observational study |
|
Ozkardeş AB, Tokaç M, Dumlu EG, Bozkurt B, Ciftçi AB, Yetişir F, Kılıç M. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis: a prospective, randomized study. Int Surg. 2014 Jan-Feb;99(1):56-61. doi: 10.9738/INTSURG-D-13-00068.1. PMID: 24444271; PMCID: PMC3897343. |
Included in SR Wu |
|
Papi C, Catarci M, D'Ambrosio L, Gili L, Koch M, Grassi GB, Capurso L. Timing of cholecystectomy for acute calculous cholecystitis: a meta-analysis. Am J Gastroenterol. 2004 Jan;99(1):147-55. doi: 10.1046/j.1572-0241.2003.04002.x. PMID: 14687156. |
SR with studies from before 2000 |
|
Prasad, 2023. The Comparative Study Between Early and Late Laparoscopic Cholecystectomy in the Treatment of Acute Cholecystitis. |
Wrong study design: no randomisation |
|
Pushpalatha, 2023. A Comparative Study of Clinical Outcome in Early and Interval Cholecystectomy in Acute Calculous Cholecystitis. |
Wrong study design: observational study |
|
Rajcok M, Bak V, Danihel L, Kukucka M, Schnorrer M. Early versus delayed laparoscopic cholecystectomy in treatment of acute cholecystitis. Bratisl Lek Listy. 2016;117(6):328-31. doi: 10.4149/bll_2016_065. PMID: 27546364. |
Included in SR Wu |
|
Reddy, P., Bhosale, S. J., & Katkar, A. (2022). A Comparative Analysis Of Interval Cholecystectomy And Early Cholecystectomy Among Patients Of Acute Cholecystitis At A Tertiary Care Centre. Journal of Pharmaceutical Negative Results, 13. |
Not conform PICO: early = symptoms 72-96h, delayed = symptoms 3-5 days |
|
Roulin D, Saadi A, Di Mare L, Demartines N, Halkic N. Early Versus Delayed Cholecystectomy for Acute Cholecystitis, Are the 72 hours Still the Rule?: A Randomized Trial. Ann Surg. 2016 Nov;264(5):717-722. doi: 10.1097/SLA.0000000000001886. PMID: 27741006. |
Included in SR Wu |
|
Schuld J, Glanemann M. Acute Cholecystitis. Viszeralmedizin. 2015 Jun;31(3):163-5. doi: 10.1159/000431275. Epub 2015 Jun 8. PMID: 26468309; PMCID: PMC4569253. |
Wrong study design: narrative review |
|
Shikata S, Noguchi Y, Fukui T. Early versus delayed cholecystectomy for acute cholecystitis: a meta-analysis of randomized controlled trials. Surg Today. 2005;35(7):553-60. doi: 10.1007/s00595-005-2998-3. PMID: 15976952. |
Overlap with SR Wu |
|
Siddiqui T, MacDonald A, Chong PS, Jenkins JT. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis: a meta-analysis of randomized clinical trials. Am J Surg. 2008 Jan;195(1):40-7. doi: 10.1016/j.amjsurg.2007.03.004. PMID: 18070735. |
Overlap with SR Wu |
|
Song GM, Bian W, Zeng XT, Zhou JG, Luo YQ, Tian X. Laparoscopic cholecystectomy for acute cholecystitis: early or delayed?: Evidence from a systematic review of discordant meta-analyses. Medicine (Baltimore). 2016 Jun;95(23):e3835. doi: 10.1097/MD.0000000000003835. Erratum in: Medicine (Baltimore). 2016 Jul 18;95(28):e0916. doi: 10.1097/01.md.0000489580.04709.16. PMID: 27281088; PMCID: PMC4907666. |
Wrong study design: analysis of previous meta-analyses |
|
Wu XD, Tian X, Liu MM, Wu L, Zhao S, Zhao L. Meta-analysis comparing early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg. 2015 Oct;102(11):1302-13. doi: 10.1002/bjs.9886. Epub 2015 Aug 12. PMID: 26265548. |
More recent SR included
|
|
Yadav RP, Adhikary S, Agrawal CS, Bhattarai B, Gupta RK, Ghimire A. A comparative study of early vs. delayed laparoscopic cholecystectomy in acute cholecystitis. Kathmandu Univ Med J (KUMJ). 2009 Jan-Mar;7(25):16-20. doi: 10.3126/kumj.v7i1.1759. PMID: 19483447. |
Included in SR Wu |
|
Zainai, 2023. COMPARATIVE STUDY ON EARLY VERSUS INTERVAL LAPAROSCOPIC CHOLECYSTECTOMY IN ACUTE CHOLECYSTITIS WITH LATE PRESENTATION |
Not conform PICO: early = after 72h
|
|
Zhou MW, Gu XD, Xiang JB, Chen ZY. Comparison of clinical safety and outcomes of early versus delayed laparoscopic cholecystectomy for acute cholecystitis: a meta-analysis. ScientificWorldJournal. 2014;2014:274516. doi: 10.1155/2014/274516. Epub 2014 Jul 14. PMID: 25133217; PMCID: PMC4123505. |
Overlap with SR Wu |
Beoordelingsdatum en geldigheid
Publicatiedatum : 01-06-2026
Beoordeeld op geldigheid : 01-06-2026
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinair cluster ingesteld. Het cluster GE-chirurgie bestaat uit meerdere richtlijnen (zie hier de actuele clusterindeling). De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden brengen hun expertise in, indien nodig. De volgende personen uit het cluster zijn betrokken geweest bij de herziening van deze module:
Clusterstuurgroepleden
- Prof. dr. M.A. (Marja) Boermeester, voorzitter, chirurg (NVvH), Amsterdam UMC
- Dr. B.R. (Boudewijn) Toorenvliet, chirurg (NVvH), Ikazia, Rotterdam
- Dr. C.C. (Charles) van Rossem, chirurg (NVvH), Maasstad Ziekenhuis, Rotterdam
- Dr. I. (Ian) Faneyte, Chirurg (NVvH), ZGT, Almelo
- Prof. dr. M.W. (Markus) Hollmann, anesthesioloog (NVA), Amsterdam UMC
- Prof. dr. P.D. (Peter) Siersema, MDL-arts (NVMDL), Erasmus MC, Rotterdam
- Prof. dr. R.G.H. (Regina) Beets-Tan, radioloog (NVvR), Netherlands Cancer Insitute (NKI), Amsterdam
- Mevr. E.C. (Esen) Doganer, beleidsmedewerker, Stichting Kind & Ziekenhuis
Betrokken clusterexpertisegroepleden
- Dr. I. (Ian) Faneyte, chirurg (NVvH), ZGT, Almelo
- Dr. P. (Philip) de Reuver, chirurg (NVvH), Radboudumc, Nijmegen
Met ondersteuning van
- Dr. M.S. (Matthijs) Ruiter, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. E.R.L. (Evie) Verweg, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- E. (Esther) van der Bijl, literatuurspecialist, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van de clusterleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Gemelde (neven)functies en belangen stuurgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen |
Overige belangen |
Datum |
Restrictie |
|
Boermeester |
Chirurg |
Medisch Ethische Commissie, Amsterdam UMC, locatie AMC |
Hieronder staan de beroepsmatige relaties met bedrijfsleven vermeld waarbij eventuele financiële belangen via de AMC Research B.V. lopen, dus institutionele en geen persoonlijke gelden zijn: |
Geen |
Institutionele grants van Solventum/3M, Johnson&Johnson
|
Ik maak me sterk voor een 100% evidence-based benadering van maken van aanbevelingen, volledig transparant en reproduceerbaar. Dat is mijn enige belang in deze; geen persoonlijk gewin.
|
Geen |
31-10-2024 |
Geen restricties |
|
Hollmann |
Afdelingshoofd Anesthesiologie Amsterdam UMC locatie AMC en afgevaardigde van NVA
|
Executive Section Editor Pharmacology Anesthesia & Analgesia |
Geen |
Geen |
ZonMw Doelmatigheid (onderzoeken hebben geen betrekking op het onderwerp GE-chirurgie, met name beademingsstudies) |
Geen |
Geen |
19-10-2022 |
Geen restricties |
|
Van Rossem |
Gastro-intestinaal chirurg, Maasstad Ziekenhuis Rotterdam |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
06-03-2021 |
Geen restricties |
|
Beets-Tan |
Hoofd Radiologie |
Scientific Director Eur Institute for Biomedical Research (onbetaald). Adviseur Eur Innovation Council |
Geen |
Geen |
Geen |
Geen |
Geen |
09-03-2021 |
Geen restricties |
|
Toorenvliet |
Chirurg, Maatschap Chirurgen en Plastisch Chirurgen Ikazia, Rotterdam |
Chirurg, Heelkunde instituut Nederland (betaald) |
Geen |
Geen |
Geen |
Geen |
Geen |
28-02-2021 |
Geen restricties |
|
Faneyte |
Chirurg Ziekenhuisgroep Twente (ZGT) / Chirurgen Cooperatie Oost-Nederland (ChirCON) |
Voorzitter ChirCON
|
Geen |
Geen |
Geen |
Geen |
Geen |
31-10-2024 |
Geen restricties |
|
Siersema |
Maag-Darm-Leverarts |
Editor in Chief Endoscopie betaald
|
Geen |
Geen |
FujiFilm, Pentax, Sanofi/Regeneron, Magentiq Eye
|
Geen |
Geen |
01-11-2024 |
Geen restricties |
|
Doganer |
Alle projecten van Rowy Uitzinger |
Stichting Kind en Ziekenhuis, Junior Projectmanager/beleidsmedewerker |
Geen |
Geen |
Geen |
Geen |
Geen |
16-06-2022 |
Geen restricties |
Gemelde (neven)functies en belangen expertisegroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intellectuele belangen |
Overige belangen |
Datum |
Restrictie |
|
Faneyte |
Zie tabel 1 |
||||||||
|
De Reuver |
Chirurg, Radboud UMC |
Geen |
Geen |
Geen |
ZonMW, kosteneffectiviteit keuzehulpen bij oa galblaaschirurgie. MLDS, onderzoek naar verbeteren van zorg voor patienten met pijn in de bovenbuik |
Geen |
Geen |
22-09-2022 |
Geen restricties |
Inbreng patiëntenperspectief
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerden de clusterleden conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Cholecystectomie bij acute cholecystitis |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: GE-chirurgie - Galsteenlijden - Module Cholecystectomie bij acute cholecystitis |
|
|
Uitgangsvraag/modules: Moet acute cholecystitis behandeld worden met een directe of uitgestelde cholecystectomie? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 19 januari 2025 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
Rayyan review: https://new.rayyan.ai/reviews/1293794/overview |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen acute cholecystitis EN uitgestelde cholecystectomie.
De sleutel- en achtergrondartikelen worden gevonden met deze search. |
|
|
Te gebruiken voor richtlijntekst: A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2000 to 19th of Januari 2025 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from two primary search concepts: (1) acute cholecystitis; (2) delayed cholecystectomy. Duplicates were removed using EndNote software. After deduplication a total of 1214 records were imported for title/abstract screening. |
|
Zoekopbrengst - 19 januari 2025
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
107 |
90 |
111 |
|
RCT |
243 |
121 |
271 |
|
Observationele studies |
743 |
646 |
832 |
|
Totaal |
1093 |
857 |
1214* |
*in Rayyan
Zoekstrategie - 19 januari 2025
Embase.com
|
No. |
Query |
Results |
|
#1 |
'acute cholecystitis'/exp OR (((acut* OR haemorrhag* OR hemorrhag*) NEAR/4 (cholecystit* OR colecystit* OR colecistit*)):ti,ab,kw) OR ((acut* NEAR/3 (gallbladder* OR 'gall bladder*') NEAR/3 inflammat*):ti,ab,kw) |
17072 |
|
#2 |
'cholecystectomy'/exp OR 'laparoscopic surgery'/exp OR ((('gall bladder*' OR gallbladder*) NEAR/3 (dissect* OR excis* OR extirpat* OR remov* OR resect*)):ti,ab,kw) OR cholecystectom*:ti,ab,kw OR 'chole cystectom*':ti,ab,kw OR laparoscop*:ti,ab,kw OR celioscop*:ti,ab,kw OR coelioscop*:ti,ab,kw OR abdominoscop*:ti,ab,kw OR peritoneoscop*:ti,ab,kw |
338177 |
|
#3 |
'time to treatment'/exp OR 'delayed surgery'/exp OR delay*:ti,ab,kw OR timing*:ti,ab,kw OR ((interval* NEAR/3 (cholecystectom* OR period*)):ti,ab,kw) OR postpon*:ti,ab,kw OR deferr*:ti,ab,kw OR late:ti,ab,kw OR later:ti,ab,kw OR deferment*:ti,ab,kw OR elective*:ti,ab,kw |
2623165 |
|
#4 |
#1 AND #2 AND #3 |
2816 |
|
#5 |
#4 AND [2000-2025]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
1461 |
|
#6 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR 'systematic review'/exp OR 'systematic review (topic)'/exp OR 'scoping review'/exp OR 'rapid review'/exp OR 'umbrella review'/exp OR 'cochrane database of systematic reviews'/jt OR 'network meta-analysis'/exp OR 'networkmeta analy*':ti,ab,kw OR 'networkmetaanaly*':ti,ab,kw OR metaanaly*:ti,ab,kw OR 'meta analy*':ti,ab,kw OR metanaly*:ti,ab,kw OR prisma:ti,ab,kw OR prospero:ti,ab,kw OR metaanali*:ti,ab,kw OR 'meta anali*':ti,ab,kw OR metanali*:ti,ab,kw OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab,kw) OR (((structured OR systemic*) NEAR/3 (review* OR overview* OR synth*) NEAR/3 literature):ti,ab,kw) OR ((systemic* NEAR/1 review*):ti,ab,kw) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab,kw) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab,kw) OR (((literature NEAR/3 (review* OR overview*)):ti,ab,kw) AND (search*:ti,ab,kw OR database*:ti,ab,kw OR 'data base*':ti,ab,kw)) OR (('data extraction*':ti,ab,kw OR 'data source*':ti,ab,kw) AND ('study selection*':ti,ab,kw OR 'studies selection*':ti,ab,kw)) OR ('search strateg*':ti,ab,kw AND 'selection criteria*':ti,ab,kw) OR ('data source*':ti,ab,kw AND 'data synth*':ti,ab,kw) OR medline*:ti,ab,kw OR pubmed*:ti,ab,kw OR 'pub med*':ti,ab,kw OR embase:ti,ab,kw OR cochrane*:ti,ab,kw OR (((critical* OR rapid*) NEAR/2 (review* OR overview* OR synth*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synth*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynth*:ti,ab,kw OR 'meta synth*':ti,ab,kw OR 'review* of review*':ti,ab,kw |
1114430 |
|
#7 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4189384 |
|
#8 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8605029 |
|
#9 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
15728549 |
|
#10 |
#5 AND #6 - SR |
107 |
|
#11 |
#5 AND #7 NOT #10 - RCT |
243 |
|
#12 |
#5 AND (#8 OR #9) NOT (#10 OR #11) - Observationeel |
743 |
|
#13 |
#10 OR #11 OR #12 - Totaal |
1093 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Cholecystitis, Acute/ or ((acut* or haemorrhag* or hemorrhag*) adj4 (cholecystit* or colecystit* or colecistit*)).ti,ab,kf. or (acut* adj3 (gallbladder* or gall bladder*) adj3 inflammat*).ti,ab,kf. |
10248 |
|
2 |
exp Cholecystectomy/ or exp Laparoscopy/ or ((gall bladder* or gallbladder*) adj3 (dissect* or excis* or extirpat* or remov* or resect*)).ti,ab,kf. or cholecystectom*.ti,ab,kf. or chole cystectom*.ti,ab,kf. or laparoscop*.ti,ab,kf. or celioscop*.ti,ab,kf. or coelioscop*.ti,ab,kf. or abdominoscop*.ti,ab,kf. or peritoneoscop*.ti,ab,kf. |
209758 |
|
3 |
exp Treatment Delay/ or exp Time-to-Treatment/ or delay*.ti,ab,kf. or timing*.ti,ab,kf. or (interval* adj3 (cholecystectom* or period*)).ti,ab,kf. or postpon*.ti,ab,kf. or deferr*.ti,ab,kf. or late.ti,ab,kf. or later.ti,ab,kf. or deferment*.ti,ab,kf. or elective*.ti,ab,kf. |
1881097 |
|
4 |
1 and 2 and 3 |
1621 |
|
5 |
limit 4 to yr="2000 -Current" |
1257 |
|
6 |
5 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
1226 |
|
7 |
exp Meta-Analysis/ or exp "Meta-Analysis as Topic"/ or exp Network Meta-Analysis/ or exp Systematic Review/ or exp "Systematic Reviews as Topic"/ or (networkmeta analy* or networkmetaanaly* or metaanaly* or meta analy* or metanaly* or prisma or prospero or metaanali* or meta anali* or metanali*).ti,ab,kf. or ((systemati* or scoping or umbrella or structured literature) adj3 (review* or overview*)).ti,ab,kf. or ((structured or systemic*) adj3 (review* or overview* or synth*) adj3 literature).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 (review* or overview*)) and (search* or database* or data base*)).ti,ab,kf. or ((data extraction* or data source*) and (study selection* or studies selection*)).ti,ab,kf. or (search strateg* and selection criteria*).ti,ab,kf. or (data source* and data synth*).ti,ab,kf. or (medline* or pubmed* or pub med* or embase or cochrane*).ti,ab,kf. or cochrane.jw. or ((critical* or rapid*) adj2 (review* or overview* or synth*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synth*)) and (search* or database* or data base*)).ab. or metasynth*.ti,ab,kf. or meta synth*.ti,ab,kf. |
806871 |
|
8 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2832573 |
|
9 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4935535 |
|
10 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5884618 |
|
11 |
6 and 7 - SR |
90 |
|
12 |
(6 and 8) not 11 - RCT |
121 |
|
13 |
(6 and (9 or 10)) not (11 or 12) - Observationeel |
646 |
|
14 |
11 or 12 or 13 - Totaal |
857 |