Autoloog bloed injectie (ABI)
Uitgangsvraag
Wat is de plaats van autoloog bloed injecties (ABI) bij de behandeling van patiënten met fasciopathie plantaris?
Aanbeveling
Pas autologe bloed injecties niet toe bij patiënten met fasciopathie plantaris.
Bespreek met de patiënt het beperkte bewijs dat ABI niet effectief is en de onbekende risico’s van een autologe bloed injectie.
Overwegingen
Slechts 1 studie rapporteert een positief effect op de cruciale uitkomst pijn op 3 maanden na een autoloog bloedinjectie (Digra, 2023). Het gepoolde effect van deze uitkomst is niet statistisch significant. De overige cruciale uitkomsten pijn (6 maanden) en functie zijn ook niet statistisch significant en blijven onder de vooraf gedefinieerde drempel van klinische relevantie (een verschil > 10%). De studies rapporteerden niet over de cruciale uitkomstmaat bijwerkingen, en ook niet over de belangrijke uitkomstmaten kwaliteit van leven en terugkeer naar sport. De kwaliteit van bewijs is zeer laag. De werkgroep raadt het gebruik van autoloog bloed bij de behandeling van FP af.
Kwaliteit van bewijs
De studies rapporteerden niet over de cruciale uitkomstmaat bijwerkingen. De overall kwaliteit van bewijs is daarom zeer laag. Dit betekent dat we zeer onzeker zijn over het gevonden geschatte effect van autoloog bloed op de cruciale uitkomstmaten pijn en functie.
Er is daarnaast afgewaardeerd vanwege:
- Risk of Bias: i.e. methodologische beperkingen m.b.t. toewijzing van behandeling en blindering.
- Inconsistentie: inconsistentie van de resultaten, door heterogeniteit.
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval de grens van klinische relevantie overschrijdt en het niet bereiken van de optimale steekproefgrootte.
Voor de cruciale uitkomst bijwerkingen, en de belangrijke uitkomsten kwaliteit van leven en terugkeer naar sport of spel waren geen studies beschikbaar en is er dus geen bewijs.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
De waarden en voorkeuren van patiënten met fasciopathie plantaris zijn in de Nederlandse setting onbekend en ook niet onderzocht in het kader van deze richtlijn ontwikkeling. In Scandinavische landen is kwalitatief onderzoek verricht naar de impact van fasciopathie plantaris vanuit patiënt perspectief (Cotchett, 2020; Mørk, 2023). Uit de ervaringen van deze patiënten komt vooral naar voren dat het voor hen een strijd is om fysiek actief te blijven vanwege pijn, wat leidt tot frustratie, emotionele uitdagingen en sociale beperkingen. Patiënten uiten bezorgdheid over langdurige inactiviteit en het effect hiervan op hun gewicht, gezondheid en welzijn. Ze benadrukken het belang van alternatieve manieren om actief te blijven, zoals fietsen, maar verlangen nog steeds naar het wandelen zonder pijn. Wat betreft medische behandelingen, geven patiënten de voorkeur aan behandelingen die duidelijk zijn, specifiek voor hun situatie en realistische verwachtingen bieden. Ze zoeken niet alleen naar pijnverlichting, maar ook naar begeleiding van empathische professionals die tijd nemen om naar hun zorgen te luisteren. Dit laatste kwam ook duidelijk naar voren in een gepubliceerde best practice guide in het Verenigd Koninkrijk (Morrissey, 2021). Hoewel dit de waarden en voorkeuren ten opzichte van een injectie behandeling niet direct weergeeft, is wel duidelijk dat patiënten zoeken naar eerlijke en betrouwbare informatie, zodat zij goed kunnen inschatten wat verwachtingen van een behandeling zijn. Wegens de zeer lage bewijskracht, waarbij ook voor veel uitkomstmaten er geen klinisch relevant effect werd gevonden, worden autologe bloed injecties niet toegepast bij patiënten met fasciopathie plantaris. De zorgverlener dient het beperkte bewijs dat ABI niet efficiënt is met de patiënt te bespreken, maar ook de onbekende risico’s van een autologe bloed injectie.
Kostenaspecten
De interventie kost meer in vergelijking met het continueren van een beleid dat bestaat uit oefentherapie en belasting management. Of deze extra kosten opwegen tegen de potentiële gezondheidswinst in termen van kwaliteit van leven, tijdiger hervatten werk en/of sport is niet duidelijk. Studies die de kosteneffectiviteit beoordelen zijn niet gevonden.
Gezondheidsgelijkheid
De interventie leidt tot een mogelijke toename van gezondheidsongelijkheid. Mensen met een lage sociaaleconomische positie kunnen mogelijk minder snel voor deze behandeling kiezen.
Injecties met autologe bloedproducten worden niet vergoed vanuit de basisverzekering en dat betekent dat patiënten die deze behandelingen overwegen een extra eigen financiële bijdrage moeten leveren. Het is van belang om de patiënt hierover te informeren, alsmede de andere behandelopties en de eventuele kosten die de diverse behandelopties met zich meebrengen. Op deze manier kan de patiënt samen met behandelaar kiezen voor de beste behandeloptie.
Aanvaardbaarheid
Ethische aanvaardbaarheid
Er zijn -behoudens de mogelijke gezondheidsongelijkheid bij het toepassen van injecties met autologe bloedproducten - geen grote ethische bezwaren voor autoloog bloed.
Duurzaamheid
Bij autoloog bloed spelen duurzaamheidsaspecten geen grote rol.
Haalbaarheid
Een autoloog bloed injectie is beter haalbaar dan PRP doordat er geen apparatuur nodig is en de middelen in de reguliere medische centra beschikbaar zijn (middelen voor bloedafname en injectiemateriaal).
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Er is beperkte bewijskracht dat een Autologe bloedinjectie (ABI) op korte en lange termijn niet effectiever is dan placebo in zowel pijnverlichting als verbetering van de functie bij patiënten met fasciopathie plantaris. De geïncludeerde studies laten geen klinisch relevant voordeel zien van ABI in vergelijking met placebo. Geen van de geïncludeerde studies hebben bijwerkingen als uitkomstmaat gerapporteerd/geëvalueerd. De kwaliteit van het bewijs is zeer laag. Op grond van het feit dat studies van zwakke methodologische kwaliteit het effect van een interventie meestal overschatten, is het zeer aannemelijk dat onderzoeken met hogere methodologische kwaliteit leiden tot vergelijkbare conclusies. Daarom kiest de werkgroep ervoor om ABI af te raden.
Eindoordeel:
Sterke aanbeveling tegen autoloog bloed (NIET doen).
Onderbouwing
Summary of Findings
Table 3. Summary of findings table including GRADE for AWB
|
Outcome |
Short or long term |
Study results and measurements |
Absolute effect estimates* |
Certainty |
Conclusions |
|
|
AWB injection
|
placebo |
|
||||
|
Pain (crucial)
|
Short term (3 months) |
Measured by VAS/NRS on a 0-10 scale.
Based on 2 studies including data from 130 patients |
Difference: MD 2.48 lower (95% CI: 6.75 lower to 1.80 higher)
Favoring AWB |
Very Low
Due to serious risk of bias, serious inconsistency and serious imprecision3 |
The evidence is very uncertain about the short-term effect of AWB injection on pain when compared with placebo in patients with plantar fasciopathy.
Digra (2023), Wheeler (2022) |
|
|
Long term (6 months) |
Measured by VAS/NRS on a 0-10 scale.
Based on 2 studies including data from 140 patients |
Difference: MD 0.39 higher (95% CI: 0.50 lower to 1.28 higher)
Favoring placebo |
Low
Due to serious risk of bias and serious imprecision1 |
AWB injections may result in little to no difference on long term pain compared with placebo in patients with plantar fasciopathy.
Weeler (2022), Kalaci (2009) |
||
|
Function (crucial)
|
Short term (3 months) |
Function was measured by FFI-r, on a 0-100 scale with lower scores representing better function
Based on 1 study including data from 90 patients |
Difference: MD 1.50 lower (95% CI: -10.93 lower to 7.93 higher)
Favoring AWB |
Low
Due to serious risk of bias and serious imprecision1
|
AWB injections may result in little to no difference on short term function compared with placebo in patients with plantar fasciopathy.
Wheeler (2022) |
|
|
Long term (6 months) |
Function was measured by FFI-r, on a 0-100 scale with lower scores representing better function;
Based on 1 study including data from 90 patients. |
Difference: MD 5.90 higher (95% CI: -3.75 lower to 15.55 higher)
Favoring placebo
|
Low
Due to serious risk of bias, due to seriousimprecision1
|
AWB injections may result in little to no difference on long term function compared with placebo in patients with plantar fasciopathy.
Wheeler (2022) |
||
|
Adverse events (crucial) |
|
No studies |
-
|
No GRADE
|
No evidence was found regarding the effect of AWB injections on adverse events when compared with placebo in patients with plantar fasciopathy. |
|
|
Quality of life (important) |
|
No studies |
-
|
No GRADE
|
No evidence was found regarding the effect of AWB injections on quality of life when compared with placebo in patients with plantar fasciopathy. |
|
|
Return to sport (important) |
|
No studies |
-
|
No GRADE
|
No evidence was found regarding the effect of AWB injections on return to sport when compared with placebo in patients with plantar fasciopathy. |
|
Reasons for downgrading certainty of evidence (levels of downgrading -1 or -2)
1. Risk of Bias: Potential RoB mainly due to lack of detailed information on allocation, blinding and potential loss to follow up (-1 level)
Imprecision: due to overlap of the 95% CI with the minimal clinically important difference, i.e. boundary of CI includes possibility of benefit or harm (-1 level)
2. Risk of Bias: Potential RoB mainly due to lack of detailed information on allocation, blinding and potential loss to follow up (-1 level)
Imprecision: results included patients from only one study, limited sample size; not reaching the optimal information size (-1 level)
3. Risk of Bias: Potential RoB. mainly due to lack of detailed information on allocation and blinding (-1 level)
Inconsistency: large heterogeneity with no overlap in confidence intervals (-1 level)
Imprecision: due to overlap of the 95% CI with the minimal clinically important difference, i.e. boundary of CI includes possibility of benefit and harm (-2 levels)
Description of studies
A total of 3 RCTs were included in the analysis of the literature. Digra (2023), Wheeler (2022) and Kalaci (2009) compared AWB injections with placebo.
All these studies, except Wheeler (2022), used a 3-arm comparison including a AWB injection, a corticosteroid (CS) injection and a placebo injection group. We excluded the CS -group in the literature analysis, as this specifically focused on AWB injections. CS was dealt with in the module ‘Corticosteroid-injections’. Important study characteristics and results are summarized in table 5. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Digra (2023) performed a RCT comparing Autologous Whole-Blood (AWB), CS and placebo (saline) injections in Plantar Fasciitis (PF). A total of 60 patients (20 per arm) with at least 2 weeks of heel pain and clinically diagnosed PF were included. Each patient received 2 injections: one at inclusion and one after 2 weeks. Relevant outcome measures included pain (VAS score). These were measured at 3 weeks, 6 weeks and 3 months (12 weeks). In this literature analysis only the follow up at 3 months were included.
Wheeler (2022) performed a RCT comparing autologous blood and placebo (ultrasound guided dry needling) in patients with chronic PF. A total of 90 patients (45 per arm), ³18 years, with chronic (> 6 months) (ultrasound or MRI confirmed) PF, who failed to improve with a home exercise program of > 3 months were included. Patients were excluded in case of previous or current partially / full thickness tears of the PF seen on ultrasonography/ MRI, other known causes for pain, unable/ unwilling to do structured rehabilitation program alongside the injection, CS injection within 3 months, or patients on anticoagulation. Each patient received one injection: an ultrasound guided AB injection including dry needling or a dry needling injection alone, both groups received an additional structured home exercise program. Relevant outcome measures included pain (Numeric Rating Scale score) and function (revised Foot Functin Index (FFI-r); measuring function as pain and stiffness, difficulty in daily functioning, activity limitations, social issues on functioning due to foot problems). In addition, other Patient Reported Outcome Measures were used but these were not included in this literature analysis due to the lack of detailed data to assess between group differences. Outcomes were measured at baseline, 2 weeks, 6 weeks, 3 months and 6 months follow-up. In this literature analysis only the follow up at 3 and 6 months were included.
Kalaci (2009) performed a multicenter RCT comparing autologous blood, CS, CS with peppering and placebo (local anesthetic injection with peppering) injection in patients with PF. A total of 100 patients (25 per arm) with PF without previous injection or surgery for PF in the previous 6 months were included. Each patient received one injection. Relevant outcome measures included pain (VAS score) and function (categorized Roles and Maudsley scores). Only the results for pain were included in this literature analysis due to the lack of detailed data to assess between group differences. Outcomes were measured at baseline, after 3 weeks and 6 months follow up. In this literature analysis only the follow up at 6 months was included.
Table 2. Characteristics of included studies
|
RCT (author year) |
Intervention |
Participants (number, age, sex, duration of symptoms) |
Control |
Participants (number, age, other important characteristics) |
Follow-up |
Outcome measures |
Risk of bias (per outcome measure)* |
Remarks |
|
Digra (2023) |
Injection 2ml AWB (drawn from antecubital vein) & 2ml lignocaine
Adminstration: location of greatest discomfort was palpated to determine the injection site using the walkover technique. At baseline and 2 weeks |
N at baseline: 20
Age (mean ± sd): 41.5 y ± not reported
Sex: 55% male (total population)
Duration of symptoms: not reported
|
Injection 2 ml saline & 2ml lignocaine
Adminstration: location of greatest discomfort was palpated to determine the injection site using the walkover technique. At baseline and 2 weeks |
N at baseline: 20
Age (mean ± sd): 42.2 y, not reported
Sex: 55% male (total population)
Duration of symptoms: not reported
|
3 and 6 weeks, 3 months |
Pain (VAS); scale 0-100
|
High (pain)
|
Additional arm CS not included |
|
Wheeler (2022) |
Injection 3-4 ml Autologous whole blood & 1- 2 ml lidocaine using US guided dry needling
Administration: close to plantar fascia at site of thickening, insertion using the peppering method. |
N at baseline: 45
Age (mean ± sd): 48.5 y ± 9.0
Sex: 42.2% male
Duration of symptoms (mean ± sd): 45.7 months ± 32.5 |
Ultrasound guided dry needling.
Administration: close to plantar fascia at site of thickening, insertion using the peppering method
|
N at baseline: 45
Age (mean ± sd): 50.4 y ± 8.9
Sex: 24.4% male
Duration of symptoms (mean ± sd): 34.3 m ± 22.0 |
Baseline, 2 and 6 weeks, 3 and 6 months |
Pain and stiffness (NRS); scale 0-10
Functional FFI-r ; scale 0-100
Other PROMs to assess function and Quality of life: (MOXFQ/FAAM/EQ5D/HADS/PSQI) not included for further analysis |
Some concerns (all outcome measures)
|
- |
|
Kalaci (2009) |
Injection 2 ml autologous blood
Administration: point of maximum tenderness in the heel using the peppering method.
|
N at baseline: 25
Age (mean ± sd): 52.9 y ± 11.1
Sex: 24% male
Duration of symptoms (mean± sd): 8.1 months ± 12.8
|
2 ml lidocaine+ peppering
Administration: point of maximum tenderness in the heel using the peppering method.
|
N at baseline: 25
Age (mean ± sd): 49.9y ± 10.8
Sex: 28% male
Duration of symptoms (mean ± sd): 11.9 months ± 20.6
|
Baseline, 3 weeks, 6 months |
Pain (VAS); scale 0-10
Function (categorized R&M); not included for further analysis
|
High (all outcome measures) |
Additional arms (CS, CS & peppering) not included |
*For further details, see risk of bias table in the appendix
Results
Results are described per outcome measure. All results are summarized and presented in the Summary of Findings table, including the level of evidence, using GRADE (table 6).
1. Pain (crucial)
Pain was assessed at short term (3 months) and long term (6 months). All five studies reported pain using the VAS (Visual Analogue Score) on a 0-10 or 0-100 scale or NRS (Numeric Rating scale) on a 0-10 scale. Higher scores indicated more pain. To pool the results, the VAS measured on a 0-100 scale was divided by 10.
Short-term pain (measured at 3 months follow-up) for AWB was assessed in two studies.
Digra (2023) and Wheeler (2022) compared AWB versus placebo (saline or ultrasound guided dry needling, resp.) including 65 patients in each arm. The pooled mean difference was -2.48 (95% CI: -6.75 to 1.80) favoring the AWB group, which was clinically relevant (>10% on a 0-10 scale), but statistically not significant.
Long-term pain (measured at 6 months follow-up) for AWB was assessed in two studies.
Wheeler (2022) and Kalaci (2009) compared AWB versus placebo (ultrasound guided dry needling or lidocaine and peppering, resp.) including 70 patients in each arm.
The pooled mean difference was 0.39 (95% CI: -0.50 to 1.28) favoring the placebo group. Which was as well as not statistically significant as not clinically relevant (< 10% on a 0-10 scale).
Results are summarized in a forest plot (Figure 1).
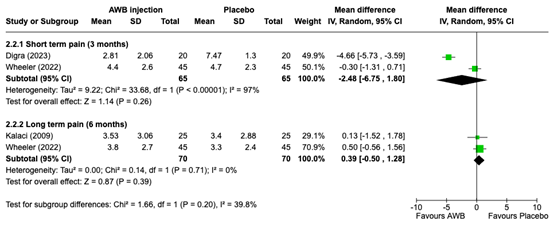
Figure 1. forest plot showing pooled results for short- and long- term pain for AWB
2. Function (crucial)
Only one study Wheeler (2022) compared AWB versus placebo (ultrasound guided dry needling) to measure short-term (3 months) and long-term function (6 months), including 45 patients in each arm. Function was measured using the FFI-r scale (on a 0-100 scale), with lower scores representing better function.
For short-term function (measured at 3 months follow-up) a mean difference of -1.50 (95% CI: -10.93 to 7.93) was found favouring the AWB group. For long-term function (measured at 6 months follow-up) a mean difference of 5.90 (95% CI: -3.75 to 15.55) was found favouring the placebo group. Both results were not statistically significant and clinically relevant (<10% on a 0-100 scale). Results are presented in a forest plot (Figure 2).

Figure 2. forest plot showing pooled results for short- and long-term function for AWB
3. Adverse events (crucial)
No studies reported on the effect of AWB injections on adverse events.
4. Quality of life (important)
Wheeler (2022) assessed several PROMS (MOXFQ, FAAM, EQ5D 5L, PSQI and HADS to assess general health and impact of symptoms on several areas of patient functioning including quality of life. However, no detailed information was provided to extract between group differences for Quality of Life.
5. Return to sport (important)
No studies reported on the effect of AWB injections on return to sport.
A systematic review of the literature was performed to answer the following question:
What is the effectiveness of Platelet Rich Plasma (PRP) or Autologous Whole Blood (AWB) injections compared to placebo in patients with Plantar fasciopathy (PF)?
The overall search encompassed two questions and two PICO’s (both PRP and AWB). Below, the selection process of autologous (whole) blood (AWB) injections is described in detail.
Table 1. PICO 2
| Patients | Patients with Plantar fasciopathy |
| Intervention |
Autologous (whole) blood (AWB) injections |
| Control | Placebo (or as add-on on exercise therapy) |
| Outcomes | Pain (crucial), function (crucial), adverse events (crucial), quality of life (important), return to sport (important) |
| Other selection criteria | Study design: systematic reviews, meta -analyses and randomized controlled trials |
Relevant outcome measures
The guideline panel considered pain, function and adverse events as crucial outcome measures for decision making; and quality of life or return to sport as important outcome measures for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies. The guideline panel was explicitly interested in a follow-up period of at least 3 months.
The guideline panel defined 10% as a minimal clinically important difference for both continuous as well as dichotomous outcome measures. This includes a 10% difference on the outcome measurement on a continuous scale or an increase/decrease of relative risk (RRR) of 10% or more.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 28 March 2024. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 155 hits. Studies were selected based on the following criteria:
- Randomized controlled trials (RCTs), systematic reviews and/or meta-analyses.
- Studies according to the PICO.S
- Studies including a minimum of 20 patients (10 patients per study arm).
- Full text English language publication.
Initially, 19 studies were selected based on title and abstract screening. After reading the full text, 14 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and 5 studies were included for PRP and AWB. Below, 3 studies evaluating AWB are described.
- Cotchett M, Rathleff MS, Dilnot M, Landorf KB, Morrissey D, Barton C. Lived experience and attitudes of people with plantar heel pain: a qualitative exploration. J Foot Ankle Res. 2020 Mar 6;13(1):12. doi: 10.1186/s13047-020-0377-3. PMID: 32143679; PMCID: PMC7059663.
- Digra N, Beri A, Sharma S, Verma R. Autologous Whole-Blood Versus Corticosteroid Local Injection in Treatment of Plantar Fasciitis: A Randomized Single Blind Placebo-Controlled Study. Cureus. 2023 Sep 20;15(9):e45588. doi: 10.7759/cureus.45588. PMID: 37868394; PMCID: PMC10587858.
- Dohan Ehrenfest DM, Andia I, Zumstein MA, Zhang CQ, Pinto NR, Bielecki T. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine: current consensus, clinical implications and perspectives. Muscles Ligaments Tendons J. 2014 May 8;4(1):3-9. PMID: 24932440; PMCID: PMC4049647.
- Franchini M, Cruciani M, Mengoli C, Marano G, Pupella S, Veropalumbo E, Masiello F, Pati I, Vaglio S, Liumbruno GM. Efficacy of platelet-rich plasma as conservative treatment in orthopaedics: a systematic review and meta-analysis. Blood Transfus. 2018 Nov;16(6):502-513. doi: 10.2450/2018.0111-18. Epub 2018 Sep 3. PMID: 30201082; PMCID: PMC6214820.
- Kalaci A, Cakici H, Hapa O, Yanat AN, Dogramaci Y, Sevinç TT. Treatment of plantar fasciitis using four different local injection modalities: a randomized prospective clinical trial. J Am Podiatr Med Assoc. 2009 Mar-Apr;99(2):108-13. doi: 10.7547/0980108. PMID: 19299346.
- Kiter E, Celikbas E, Akkaya S, Demirkan F, Kiliç BA. Comparison of injection modalities in the treatment of plantar heel pain: a randomized controlled trial. J Am Podiatr Med Assoc. 2006 Jul-Aug;96(4):293-6. doi: 10.7547/0960293. PMID: 16868321.
- Kumar VA, Khalid KM, Vajrangi A, Sherikar N, Srinivas R, Rakshith CHY, Kurupati RB, Rajanna P. A Comparative Study Between Platelet-Rich Plasma And Corticosteroid Injection For Plantar Fasciitis. Research journal of pharmaceutical, biological and chemical sciences. 2024. 15(1), 159‐166.doi:10.33887.
- Mahindra P, Yamin M, Selhi HS, Singla S, Soni A. Chronic Plantar Fasciitis: Effect of Platelet-Rich Plasma, Corticosteroid, and Placebo. Orthopedics. 2016 Mar-Apr;39(2):e285-9. doi: 10.3928/01477447-20160222-01. Epub 2016 Feb 25. PMID: 26913766.
- Mørk M, Soberg HL, Hoksrud AF, Heide M, Groven KS. The struggle to stay physically active-A qualitative study exploring experiences of individuals with persistent plantar fasciopathy. J Foot Ankle Res. 2023 Apr 15;16(1):20. doi: 10.1186/s13047-023-00620-4. PMID: 37061709; PMCID: PMC10105408.
- Morrissey D, Cotchett M, Said J'Bari A, Prior T, Griffiths IB, Rathleff MS, Gulle H, Vicenzino B, Barton CJ. Management of plantar heel pain: a best practice guide informed by a systematic review, expert clinical reasoning and patient values. Br J Sports Med. 2021 Oct;55(19):1106-1118. doi: 10.1136/bjsports-2019-101970. Epub 2021 Mar 30. PMID: 33785535; PMCID: PMC8458083.
- Wheeler PC, Dudson C, Gregory KM, Singh H, Boyd KT. Autologous Blood Injection With Dry-Needling vs Dry-Needling Alone Treatment for Chronic Plantar Fasciitis: A Randomized Controlled Trial. Foot Ankle Int. 2022 May;43(5):646-657. doi: 10.1177/10711007211061365. Epub 2022 Jan 24. PMID: 35068224.
Risk of bias table for intervention studies (randomized controlled trials; based on Cochrane risk of bias tool and suggestions by the CLARITY Group at McMaster University)
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
|
Was the allocation adequately concealed?
|
Blinding: Was knowledge of the allocated interventions adequately prevented? |Were patients blinded? | Were healthcare providers blinded? | Were data collectors blinded? | Were outcome assessors blinded? | Were data analysts blinded? |
Was loss to follow-up (missing outcome data) infrequent?
|
Are reports of the study free of selective outcome reporting?
|
Was the study apparently free of other problems that could put it at a risk of bias?
|
Overall risk of bias If applicable/necessary, per outcome measure
LOW/Some concerns/ HIGH |
|
Digra (2023) |
Probably no
Reason: No details given, just stated: “patients were divided into three groups by simple randomization” |
Probably no
Reason: no information provided on concealment of allocation |
Probably no
Reason: no description of blinding of patients, healthcare providers, data collectors/assessors/analysts |
Probably no
Seems no loss to follow up (short period) but no desription of any loss to follow up given |
Probably yes
Reason: All outcomes reported, though not clearly pre specified in methodology so difficult to assess
|
Probably no:
Reason: potential bias due to lack of detailed information on chosen methodology to assess the completeness of reporting, but no baseline characteristics reported for main outcome or reporting of adverse events. |
HIGH (all outcome measures)
Reason: Unclear allocation and blinding procedure, missing info on loss to follow up, selective reporting or completeness |
|
Wheeler (2022) |
Probably yes;
Reason: Allocation and randomization by study nurse practitioner independent from the rest of the study |
Definitely yes
Reason: allocation with sealed envelopes |
Probably yes:
Reason: blinding of participants, data collectors and outcome assessors but administering clinician and study nurse practitioner not blinded though the administering clinician had no further participant contact |
Probably yes:
Reason: Loss to follow up (6m) 1 patient and a small (max n=5) number of interim apppointments missed but no other reasons for loss to follow up |
Probably yes:
Reason: All predefined outcomes have been reported (partly in supplementary material) |
Probably yes:
Reason: seems no other risks of biases, but detailed information for its assessment is lacking and sample size is small for the assessment of several outcomes
|
Some concerns (for all outcome measures)
Reason: Blinding not complete, No detailed / missing information on performance of home exercise program in both groups |
|
Kalaci (2009) |
Probably no:
Reason: No allocation sequence predefined, based on order of presentation |
Probably no:
Reason: no description of allocation |
Probably no
Reasos: patients were blinded, and reviewers were blinded, other groups not blinded. |
Probably yes
Reason: no loss to follow up but 2 additional groups (saline & peppering and AB & peppering) were excluded based due to to much pain caused by the procedure |
Probably no
Reason all outcomes reported though not clearly pre specified in methodology so difficult to assess
|
Probably no;
Reason: study reports all important features yet lacks a clear well predefined methodology section so difficult to assess (f.e. in abstract a multicenter approach is stated but in article no mentioning of any centers at all) or stop of procedure for 2 additional groups due to pain when was decided to stop procedures and exclude patients |
High (all outcome measures)
Reason: Blinding not complete, unclear allocation, methodology briefly described, seems not based on well pre-defined choices.
|
|
Kiter (2022) |
Probably yes;
Reason: Allocation by drawing lots, but no further specification given |
Probably no;
No description of allocation concealment |
Probably no:
Reason: no data on blinding of patients/ healthcare providers/ data collectors/ analysts/ outcome assessors/ |
Probably yes:
Reason: 1 patient was lost to follow up but no further data or reasons provided. |
Probably yes;
Reason: all outcomes have been reported but no detailed description of these outcomes in methods |
Probably no:
Reason: the number of injections differed largely, without further specification on reasons or potential impact on outcomes |
High (all outcome measures)
Reason; allocation, blinding, loss to fu all poorly described and a different number of injections per patient/ group |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Johnson-Lynn S, Cooney A, Ferguson D, Bunn D, Gray W, Coorsh J, Kakwani R, Townshend D. A Feasibility Study Comparing Platelet-Rich Plasma Injection With Saline for the Treatment of Plantar Fasciitis Using a Prospective, Randomized Trial Design. Foot Ankle Spec. 2019 Apr;12(2):153-158. doi: 10.1177/1938640018776065. Epub 2018 May 21. PMID: 29779399. |
No data presented to provide effect estimates |
|
Shetty SH, Dhond A, Arora M, Deore S. Platelet-Rich Plasma Has Better Long-Term Results Than Corticosteroids or Placebo for Chronic Plantar Fasciitis: Randomized Control Trial. J Foot Ankle Surg. 2019 Jan;58(1):42-46. doi: 10.1053/j.jfas.2018.07.006. Epub 2018 Nov 15. PMID: 30448183. |
No data presented to provide effect estimates |
|
de Vos RJ, van Veldhoven PL, Moen MH, Weir A, Tol JL, Maffulli N. Autologous growth factor injections in chronic tendinopathy: a systematic review. Br Med Bull. 2010;95:63-77. doi: 10.1093/bmb/ldq006. Epub 2010 Mar 2. PMID: 20197290. |
Wrong population (FP and others) and wrong control group (no placebo with/without exercise therapy) |
|
Karimzadeh A, Raeissadat SA, Erfani Fam S, Sedighipour L, Babaei-Ghazani A. Autologous whole blood versus corticosteroid local injection in treatment of plantar fasciitis: A randomized, controlled multicenter clinical trial. Clin Rheumatol. 2017 Mar;36(3):661-669. doi: 10.1007/s10067-016-3484-6. Epub 2016 Dec 12. PMID: 27957618. |
Wrong control group (no placebo with/without exercise therapy) |
|
Chew KT, Leong D, Lin CY, Lim KK, Tan B. Comparison of autologous conditioned plasma injection, extracorporeal shockwave therapy, and conventional treatment for plantar fasciitis: a randomized trial. PM R. 2013 Dec;5(12):1035-43. doi: 10.1016/j.pmrj.2013.08.590. Epub 2013 Aug 22. PMID: 23973504. |
Wrong control group (no placebo with/without exercise therapy) |
|
Gao R, Sun J, Zhang L, Chen S, Dong W, Yu H, Han B, Tan M, Li X. Comparative Effectiveness of Minimally Invasive Nonsurgical Treatments for Plantar Fasciitis: A Network Meta-analysis of 30 Randomized Controlled Trials. Pain Physician. 2021 Nov;24(7):E955-E971. PMID: 34704707. |
Wrong comparison (no direct comparison PRP with placebo with/without exercise therapy) |
|
Li H, Lv H, Lin T. Comparison of efficacy of eight treatments for plantar fasciitis: A network meta-analysis. J Cell Physiol. 2018 Jan;234(1):860-870. doi: 10.1002/jcp.26907. Epub 2018 Aug 4. PMID: 30078188. |
Wrong control group (no placebo with/without exercise therapy, 1 RCT already included) |
|
Guimarães JS, Arcanjo FL, Leporace G, Metsavaht LF, Conceição CS, Moreno MVMG, Vieira TEM, Moraes CC, Gomes Neto M. Effects of therapeutic interventions on pain due to plantar fasciitis: A systematic review and meta-analysis. Clin Rehabil. 2023 Jun;37(6):727-746. doi: 10.1177/02692155221143865. Epub 2022 Dec 26. PMID: 36571559. |
Wrong comparison (no direct comparison PRP with placebo with/without exercise therapy) |
|
Franchini M, Cruciani M, Mengoli C, Marano G, Pupella S, Veropalumbo E, Masiello F, Pati I, Vaglio S, Liumbruno GM. Efficacy of platelet-rich plasma as conservative treatment in orthopaedics: a systematic review and meta-analysis. Blood Transfus. 2018 Nov;16(6):502-513. doi: 10.2450/2018.0111-18. Epub 2018 Sep 3. PMID: 30201082; PMCID: PMC6214820. |
Wrong population (FP and others) and wrong control group (no placebo with/without exercise therapy) |
|
Assad S, Ahmad A, Kiani I, Ghani U, Wadhera V, Tom TN. Novel and Conservative Approaches Towards Effective Management of Plantar Fasciitis. Cureus. 2016 Dec 5;8(12):e913. doi: 10.7759/cureus.913. PMID: 28083457; PMCID: PMC5215813. |
Wrong control group (no placebo with/without exercise therapy, 1 RCT already included) |
|
Yu T, Xia J, Li B, Zhou H, Yang Y, Yu G. Outcomes of platelet-rich plasma for plantar fasciopathy: a best-evidence synthesis. J Orthop Surg Res. 2020 Sep 21;15(1):432. doi: 10.1186/s13018-020-01783-7. PMID: 32958046; PMCID: PMC7504858. |
Wrong control group (no placebo with/without exercise therapy, 1 RCT already included) |
|
Herber A, Covarrubias O, Daher M, Tung WS, Gianakos AL. Platelet rich plasma therapy versus other modalities for treatment of plantar fasciitis: A systematic review and meta-analysis. Foot Ankle Surg. 2024 Jun;30(4):285-293. doi: 10.1016/j.fas.2024.02.004. Epub 2024 Feb 15. PMID: 38395675. |
Wrong control group (no placebo with/without exercise therapy, 1 RCT already included) |
|
Masiello F, Pati I, Veropalumbo E, Pupella S, Cruciani M, De Angelis V. Ultrasound-guided injection of platelet-rich plasma for tendinopathies: a systematic review and meta-analysis. Blood Transfus. 2023 Mar;21(2):119-136. doi: 10.2450/2022.0087-22. Epub 2022 Oct 17. PMID: 36346880; PMCID: PMC10072988. |
Wrong population (FP and others) and wrong control group (no placebo with/without exercise therapy) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 17-02-2026
Beoordeeld op geldigheid : 17-02-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire werkgroep samengesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met fasciopathie plantaris.
Werkgroep
- Dhr. prof. dr. Fred Hartgens (voorzitter), sportarts, namens de Vereniging voor Sportgeneeskunde (VSG)
- Dhr. dr. Bernard te Boekhorst, sportarts, namens de VSG
- Dhr. drs. Daan Gelsing, extended scope specialist, echografist en manueel therapeut, namens de Nederlandse Vereniging voor Manuele Therapie en het Koninklijk Nederlands Genootschap voor Fysiotherapie (NVMT/KNGF)
- Dhr. drs. David Hanff, radioloog, namens de Nederlandse Vereniging voor Radiologie (NVvR)
- Dhr. dr. Eric Bakker, fysiotherapeut en klinisch epidemioloog, namens het Koninklijk Nederlands Genootschap voor Fysiotherapie (KNGF)
- Mevr. drs. Eva Hoefnagels, orthopedisch chirurg, namens de Nederlandse Orthopaedische Vereniging (NOV)
- Mevr. drs. Inge Koetser, radioloog, namens de NVvR
- Mevr. drs. Kayleigh van Amelsfort, podotherapeut en gezondheidswetenschapper, namens de Nederlandse Vereniging voor Podotherapeuten (NVvP)
- Dhr. drs. Niek Vink, fysiotherapeut en fysiotherapiewetenschapper, namens de KNGF
- Dhr. dr. Robert-Jan de Vos, sportarts, namens de VSG
- Dhr. drs. Thomas Eggen, orthopedisch chirurg, namens de NOV
Klankbordgroep
- Dhr. dr. Dorus Fennis, neuroloog, namens de Nederlandse Vereniging voor Neurologie (NVN)
- Dhr. dr. Florus van der Giesen, physician assistant reumatologie, namens de Nederlandse Vereniging voor Reumatologie (NVR)
- Mevr. drs. Juliette Starmans, AIOS bedrijfsgeneeskunde en orthopedisch chirurg, namens de Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (NVAB)
- Mevr. drs. Lisette de Graauw, register podoloog, namens Stichting LOOP
Met ondersteuning van
- Mevr. drs. Beatrix Vogelaar, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. drs. Isabelle Laseur, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Tabel Gemelde (neven)functies en belangen werkgroep
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Fred Hartgens (voorzitter) |
Hoofd Afdeling Sportgeneeskunde en Hoogleraar Klinische Sportgeneeskunde in UMC Utrecht (0,8 fte) |
Op free lance basis praktiserend sportarts in Zuid-Limburg en sportarts-docent voor andere organisaties (in totaal 10-15 uur per maand) VSG vertegenwoordiger bij FMS Raad Wetenschap & Innovatie Lid van Werkgroep Herziening Kennisagenda VSG VSG vertegenwoordiger in SKMS Beweeg Alliantie |
UTC lmaging B.V: The effects of tendinopathy and reliability of hamstrings Ultrasiund Tissue Characterisation (UTC) echo types - geen projectleidersrol BioActor B.V. : The Effect of a Citrus and Pomegranate Complex on Physical Fitness and Mental Well-Being in Healthy Elde a Randomized Placebo controlled Trial - geen projectleidersrol
Allebei afgerond |
Geen restricties |
|
Bernard te Boekhorst |
SMA sportarts middennederland |
- |
- |
Geen restricties |
|
Daan Gelsing |
Echo On The Spot - eigenaar, MSK-echografist Rembrandt fysiotherapie - echografist en manueel therapeut Echo On The Spot - het uitvoeren van echografisch diagnostisch onderzoek in de eerstelijns zorg. Rembrandt fysiotherapie - fysiotherapeutische zorg. |
Geven van mini-klinieken en examinator aan de SOMT University |
|
Geen restricties |
|
Eric Bakker |
Epidemioloog(B) master EBPiHC, Amsterdam UMC locatie AMC, Amsterdam 0,3 FtE. Onderwijs en begeleidingen onderzoek van de studenten epidemiologie. Betaald
|
Eigenaar wetenschappelijk adviesbureau KOKD.nl. Betaald. Niet over onderwerpen in de richtlijn |
|
Geen restricties |
|
Eva Hoefnagels
|
Sint maartenskliniek orthopedisch chirurg betaald |
Voorzitter nederlandse voet en enkel vereniging (onbetaald) |
Promotie onderzoek fasciitis plantaris, onderzoek is afgerond en data al verwerkt, dit onderzoek heeft geen invloed op de data Bestuur Nederlandse voet en enkelvereniging. Uitkomst onderzoek heeft geen invloed op mijn functie daar. Promotieonderzoek lopend, geen financier. Publicaties sinds 2019: - PAPPI: Personalized analysis of plantar pressure images using statistical modelling and parametric mapping - The effect of lengthening the gastrocnemius muscle in chronic therapy resistant plantar fasciitis
Promotie onderzoek over operatieve behandeling bij chronische fasciitis plantaris. Is al begonnen in 2017 en data zijn al verzameld tot 2020. Voor de start van deze richtlijn. De data van mijn onderzoek is niet van invloed voor de richtlijn en de uitkomst van de richtlijn niet voor het onderzoek. Mijn onderzoeks data zijn niet gebruikt voor de richtlijn. |
Geen restricties |
|
Inge Koetser
|
Radioloog, Reade |
GAIA commissie
|
- |
Geen restricties |
|
Kayleigh van Amelsfort
|
Podotherapeut, Podotherapie Inka (betaald, 20 uur) |
Bestuurslid Wetenschap & Vakinhoud, Nederlandse Vereniging van Podotherapeuten (betaald, 10 uur) |
- |
Geen restricties |
|
Niek Vink |
Manager en docent Nationaal Trainingscentrum voor echografie (NT-e) |
Manager van het opleidingscentrum NT-e. Hier worden post-HBO opleidingen gegeven in echografie, shockwave therapie en percutane electrolyse (ook bij plantaire hielpijnklachten). Ik geef een dag in de week les binnen de opleidingen voor echografie. Het NT-e is onderdeel van Fyzzio International BV. Fyzzio verkoopt apparatuur voor bovenvermelde activiteiten. Ik ben bij het NT-e in loondienst, heb geen aandelen in het bedrijf en krijg ook geen bonussen. Ik heb geen financiële belangen bij een bepaalde uitkomst van de richtlijn. |
- |
Geen restricties |
|
Robert-Jan de Vos |
Sportarts en Universitair Hoofddocent, Erasmus MC Universitair Medisch Centrum Rotterdam (0.8 fte) |
Consulent SBV Excelsior Rotterdam (onbetaald). Associate editor British Journal of Sports Medicine (onbetaald). Voorzitter multidisciplinaire richtlijn achilles tendinopathie (onbetaald). Werkgroeplid multidisciplinaire richtlijn achillespeesruptuur (onbetaald). Werkgroeplid Kennisagenda VSG 2023 (onbetaald). Werkgroeplid SKMS richtlijnen commissie (betaald). |
In de afgelopen 5 jaar zijn er onderzoeksprojecten uitgevoerd onder mijn supervisie die zijn gefinancierd door ReumaNederland, Annafonds, ZonMw, GE Healthcare, de National Basketball Association (NBA), het Trustfonds en de Erasmus MC Foundation. Deze financiers hebben echter geen belangen bij de aanbevelingen die zullen worden gedaan in deze richtlijn. Ik heb een consultancy functie voor een project naar nieuwe injectie behandeling voor Achilles tendinopathie, gesponsord door Novartis (2021), dit raakt niet aan het onderwerp van de richtlijn. Tevens is deze injectie behandeling nog niet ontwikkeld voor de huidige klinische zorg en daardoor zal deze ook niet in de richtlijn kunnen worden behandeld. Daarnaast is de consultancy functie eenmalig geweest en niet meer actief, en inkomsten zijn voor de instelling waarin ik werk en niet voor persoonlijke doeleinden). Op dit moment is er geen commercieel gefinancieerd onderzoek dat loopt onder mijn leiding. Ik ben aan het oriënteren met Causeway Therapeutics of we een onderzoek gaan opstarten met een nieuwe injectable voor epicondylaire tendinopthie, maar ook daarvoor geldt dat het niet direct zal zijn gerelateerd aan fasciopathie plantaris. Het is niet mijn verwachting dat dit leidt tot belangenverstrengeling.
In de afgelopen 5 jaar zijn er onderzoeksprojecten uitgevoerd onder mijn supervisie die zijn gefinancierd door HORIZON MSCA, ReumaNederland, Annafonds, ZonMw, GE Healthcare, de National Basketball Association (NBA), het Trustfonds en de Erasmus MC Foundation. Deze financiers hebben echter geen belangen bij de aanbevelingen die worden gedaan in deze richtlijn. Ik heb een consultancy functie gehad voor een project naar nieuwe injectie behandeling voor Achilles tendinopathie (Novartis, 2021) en laterale epicondylaire tendinopathie (Causeway therapeutics. 2025). Dit raakt niet aan het onderwerp van de richtlijn. Tevens zijn deze injectie behandelingen nog niet ontwikkeld voor de huidige klinische zorg en daardoor worden deze behandelingen ook niet in de richtlijn behandeld. Daarnaast zijn deze consultancy functies eenmalig geweest en niet meer actief, en inkomsten zijn voor de instelling waarin ik werk en niet voor persoonlijke doeleinden).
Op dit moment is er geen commercieel gefinancierd onderzoek dat loopt onder mijn leiding. HORIZON MSCA Postdoctoral Fellowship – Identifying Predictive factors for the Recovery of Achilles Tendinopathy (PReAcT trial) NWO / ReumaNederland – The State of the Cartilage (START project) ReumaNederland / Annafonds – High-Volume injectie Achilles tendinopathie (HAT trial) ZonMW – Preventie hardloopblessures (INSPIRE trial en SPRINT trial) GE Healthcare / NBA – Oefentherapie Patella tendinopathie (JUMPER trial) Trustfonds / Erasmus MC Foundation – Normwaarden echografie achillespezen (REVEAL trial) Causeway therapeutics – Consultancy voor trial nieuwe injectable laterale epicondylaire tendinopathie Novartis – Consultancy voor trial nieuwe injectable achilles tendinopathie |
Geen restricties |
|
Thomas Eggen |
Orthopedisch chirurg Canisius Wilhelmina Ziekenhuis |
Dagvoorzitter NOV en LVO congressen Orthopedisch consultant op KNMG carriere beurs Mede-oprichter BotCast orthopedische podcast (educatief/informatief). Mogelijke tegemoetkoming vanuit Orlymedia BV (sponsor kan farmaceut zijn). |
- |
Geen restricties |
|
David Hanff |
Voorzitter van de MSK sectie Nederlandse Vereniging voor Radiologie |
Nederlandse Vereniging voor Radiologie |
- |
Geen restricties |
|
Dorus Fennis (klankbordgroep) |
Geen werkgever maar vrijgevestigd meidsch specialist bij Cooperatie Medische Staf St Jansdal UA |
- |
- |
Geen restricties |
|
Juliëtte Starmans (klankbordgroep) |
AIOS bedrijfsgeneeskunde. Ik werk als ZZP’er en ben aldus aangesloten bij Immediator. Tijdens mijn opleiding ben ik werkzaam bij een klant, waar ik betaalde werkzaamheden verricht. |
Naast AIOS bedrijfsgeneeskunde ben ik werkzaam als orthopedisch chirurg. In deze hoedanigheid werk ik eveneens als ZZP’er in mijn éénmansbedrijf: Starmans orthopedische expertises. Via dit bedrijf verricht ik orthopedische expertises voor verzekeringen. Tevens ben ik via dit bedrijf als medisch adviseur werkzaam voor Medisch Advies Bureau. Alle werkzaamheden voor Starmans orthopedische expertises zijn betaalde werkzaamheden. |
- |
Geen restricties |
|
Florus van der Giesen (klankbordgroep) |
Physician assistant reumatologie |
- |
- |
Geen restricties |
|
Lisette de Graauw (klankbordgroep) |
Zorgverlener in zowel de eerste als tweede lijngezondheidszorg.
|
- |
Ik werk in de voetzorg, dus ja, als blijkt dat de uitkomsten van de richtlijn laten zien dat de door mijn beroepsgroep geleverde zorg werkt, dan heb ik (en mijn beroepsgroep) daar voordeel bij. |
Geen restricties |
Inbreng patiëntenperspectief
De werkgroep besteedde aandacht aan het patiëntenperspectief door de Patiëntenfederatie Nederland te betrekken in de klankbordgroep-fase. De verkregen input is meegenomen bij het opstellen van de overwegingen (zie kop “Waarden en voorkeuren van patiënten”). De conceptrichtlijn is tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerde de werkgroep conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Autologe bloedproducten – Autologe bloedinjecties (ABI) |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (5.000- 40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Fasciopathie Plantaris - UV8 Autologe factoren |
|
|
Uitgangsvraag/modules: Wat is de plaats van autologe bloedproducten bij de behandeling van patiënten met fasciopathie plantaris? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 28-3-2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Esther van der Bijl |
Rayyan review: https://rayyan.ai/reviews/980355 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen fasciopathie plantaris EN autologe bloedproducten.
→ De sleutelartikelen worden gevonden met deze search.
|
|
|
Te gebruiken voor richtlijntekst: In de databases Embase.com en Ovid/Medline is op 28 maart 2024 systematisch gezocht naar systematische reviews en RCTs over de plaats van autologe bloedproducten bij de behandeling van patiënten met fasciopathie plantaris. De literatuurzoekactie leverde 155 unieke treffers op. |
|
Zoekopbrengt - 28 maart 2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
58 |
43 |
62 |
|
RCT |
86 |
48 |
93 |
|
|
|
|
|
|
Totaal |
144 |
91 |
155* |
*in Rayyan
Zoekstrategie - 28 maart 2024
Embase.com
|
No. |
Query |
Results |
|
#1 |
'plantar fasciitis'/exp OR 'plantar fasciopathy'/exp OR 'heel spur'/exp OR 'policeman heel'/exp OR (((calcane* OR heel* OR subcalcane*) NEAR/3 (spur* OR exostos* OR pain* OR policeman* OR jogger*)):ti,ab,kw) OR ((plant* NEAR/3 (fasciitis OR fasciopath* OR fascios* OR inflam*)):ti,ab,kw) OR (((baxter* OR plant* OR calcane* OR heel) NEAR/3 neuropath*):ti,ab,kw) OR calcaneodyn*:ti,ab,kw OR 'calcane* periostitis':ti,ab,kw |
6372 |
|
#2 |
'thrombocyte rich plasma'/exp OR 'platelet-rich plasma cell'/exp OR 'blood autotransfusion'/exp OR (((blood OR plasma) NEAR/3 (autotransfusion* OR autologous OR 'platelet rich*' OR 'thrombocyte rich*')):ti,ab,kw) OR ((prp NEAR/3 inject*):ti,ab,kw) OR 'autoh*emotransfusion':ti,ab,kw |
47371 |
|
#3 |
#1 AND #2 |
292 |
|
#4 |
#3 AND [2000-2024]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
249 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1014761 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4001894 |
|
#7 |
#4 AND #5 – SR’s |
58 |
|
#8 |
#4 AND #6 NOT #7 – RCT’s |
86 |
|
#9 |
#7 OR #8 |
144 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Fasciitis, Plantar/ or exp Heel Spur/ or ((calcane* or heel* or subcalcane*) adj3 (spur* or exostos* or pain* or policeman* or jogger*)).ti,ab,kf. or (plant* adj3 (fasciitis or fasciopath* or fascios* or inflam*)).ti,ab,kf. or ((baxter* or plant* or calcane* or heel) adj3 neuropath*).ti,ab,kf. or calcaneodyn*.ti,ab,kf. or calcane* periostitis.ti,ab,kf. |
4416 |
|
2 |
exp Platelet-Rich Plasma/ or exp Blood Transfusion, Autologous/ or ((blood or plasma) adj3 (autotransfusion* or autologous or 'platelet rich*' or 'thrombocyte rich*')).ti,ab,kf. or (prp adj3 inject*).ti,ab,kf. or 'autoh*emotransfusion'.ti,ab,kf. |
32277 |
|
3 |
1 and 2 |
155 |
|
4 |
limit 3 to yr="2000 -Current" |
155 |
|
5 |
4 not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
144 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
735289 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2706138 |
|
8 |
5 and 6 – SR’s |
43 |
|
9 |
(5 and 7) not 8 – RCT’s |
48 |
|
10 |
8 or 9 |
91 |