Preventie hypoglykemie met sensor bij diabetes mellitus type 2
Uitgangsvraag
Wat is de rol van sensoren in de preventie van (ernstige) hypoglykemie bij volwassen patiënten met diabetes mellitus type 2?
Aanbeveling
Overweeg bij patiënten met diabetes mellitus type 2 die met insuline worden behandeld en derhalve een indicatie hebben voor glucosemonitoring om te starten met een glucosesensor.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Voor de module is een search uitgevoerd naar het effect van Continue Glucose Monitoring (CGM) en Flash Glucose Monitoring (FGM) vergeleken met SMBG (vingerprik test) op de preventie van hypoglykemie bij patiënten met diabetes mellitus type 2. Voor de definitie van hypoglykemieën is uitgegaan van de classificatie in drie niveaus, zoals gepubliceerd door de International Hypoglycaemia Study Group (IHSG, 2017): Er is een review geïncludeerd (Jancv, 2024) met daarin twaalf RCT’s. Hiervan hebben acht trials het effect van CGM (rtCGM) onderzocht en vier trials het effect van FGM (isCGM).
•CGM
Voor de cruciale uitkomstmaten hypoglykemie en ernstige hypoglykemie kon geen richting gegeven worden voor het bewijs, vanwege inconsistentie in het rapporteren van de resultaten (hypoglykemie) en vanwege imprecisie door een zeer laag aantal events en risk of bias (ernstige hypoglykemie). Voor de belangrijke uitkomstmaten time in range (TIR), time above range (TAR) en HbA1c is met lage bewijskracht bewijs gevonden voor een verbetering bij CGM vergeleken met SMBG. Met redelijke bewijskracht is bewijs gevonden voor een niet-klinisch relevante verbetering van de time below range (TBR).
•FGM
Voor de cruciale uitkomstmaten hypoglykemie en ernstige hypoglykemie kon geen richting gegeven worden voor het bewijs, vanwege inconsistentie in het rapporteren van de resultaten (hypoglykemie) en vanwege imprecisie door een zeer laag aantal events en risk of bias (ernstige hypoglykemie). Voor TIR en HbA1c is met gemiddeld hoge bewijskracht bewijs gevonden voor een niet-klinisch relevante verbetering. Voor TBR is met lage bewijskracht bewijs gevonden voor een verbetering bij FGM vergeleken met SMBG. Voor TAR is eveneens een niet-klinisch relevante verbetering gevonden (lage bewijskracht).
Kwaliteit van bewijs
De overall kwaliteit van bewijs is zeer laag. Dit betekent dat we zeer onzeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten.
Er is afgewaardeerd vanwege
- Risk of Bias: methodologische beperkingen door gebreken in het randomisatieproces en selectieve uitkomstrapportage
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval een of meerdere grenzen voor klinische relevantie overschrijdt bij meerdere uitkomstmaten en (bij (ernstige) hypoglykemie) vanwege een zeer klein aantal events.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Hypoglykemieën zijn de meest voorkomende ‘bijwerkingen’ van behandeling met insuline en medicijnen die afgifte van insuline stimuleren (met name SU derivaten) bij mensen met DM2 en kunnen een grote inbreuk maken op het dagelijks leven en de kwaliteit van leven. Vermindering van het aantal hypoglykemieën en de angst hiervoor kunnen daardoor van grote betekenis zijn voor mensen met DM2 die met insuline worden behandeld. De continue registratie van glucose en de mogelijkheid om gebruik te maken van alarmen maakt het mogelijk hypoglykemieën op tijd te registreren en te voorkomen. Door de continue registratie is er ook inzicht in de bloedglucosewaarden, waardoor angst voor hypo’s kan verminderen en de kwaliteit van leven behoorlijk kan verbeteren. Naasten en verzorgers kunnen daarbij op afstand monitoren, wat in bepaalde situaties waardevol kan zijn. Dit moet worden afgezet tegen de mogelijk grotere druk om zelfcontrole uit te voeren, het kunnen omgaan met deze technologie, en het omgaan met de grote hoeveelheid data die sensoren genereren en die als overweldigend kan worden ervaren. In hoeverre inzet van CGM kan helpen om het verhoogde valrisico gerelateerd aan hypoglykemieën bij ouderen te verminderen verdient nader onderzoek.
Kostenaspecten
De interventie levert meer kosten ten opzichte van de controle behandeling. Deze meerkosten moeten worden afgewogen tegen de meerwaarde van betere glucoseregulatie, met name weerspiegeld in betere tijd in doelbereik (TIR), minder tijd in lage (TBR) en hoge (TAR) waarden en geringe verbetering van het HbA1c. Een verbetering van TIR van 5% of meer wordt als klinisch relevant gezien, omdat een 5% hogere TIR geassocieerd is met een lager risico op vasculaire complicaties, hetgeen op de lange kostenbesparing op zou kunnen leveren. Ook een betere productiviteit door betere glucoseregulatie en vermindering van hypoglykemieën kan een positief effect hebben op de baten van sensortechnologie. Tot slot maakt behandeling met glucosesensoren zorg op afstand (beter) mogelijk met navenante reductie in zorgkosten. Kosteneffectiviteitsonderzoek is nodig om deze verschillende effecten af te wegen tegen de kosten.
Gelijkheid ((health) equity/equitable)
De interventie leidt tot een toename van gezondheidsgelijkheid. Een aantal (soorten) glucosesensoren is op de (online) markt beschikbaar voor iedereen die daar interesse in heeft. Dit creëert een ongelijkheid voor mensen met diabetes (type 2) voor wie dergelijke behandeling (nog) niet wordt vergoed, aangezien de kosten voor veel mensen (te) hoog zal liggen. Vergoeding van sensoren voor iedereen met diabetes (type 2) die met insuline wordt behandeld zal aan deze ongelijkheid een einde maken.
Aanvaardbaarheid:
Ethische aanvaardbaarheid
De interventie lijkt aanvaardbaar voor alle betrokkenen. Er zijn geen algemeen geldende ethische bezwaren. Wel zal niet iedereen een glucosesensor willen gebruiken, vanwege voortdurende ‘confrontatie’ met (afwijkende) glucosewaarden, de zichtbaarheid op het lichaam (met mogelijk bijdragen aan diabetes stigma) en de vraag naar delen van gegevens met de omgeving (bijv. de partner).
Duurzaamheid
Bij de interventie spelen duurzaamheidsaspecten geen grote rol rol. Sensoren zorgen logischerwijs voor afval, maar een deel hiervan zal herbruikbaar zijn.
Haalbaarheid
De haalbaarheid van de beschreven interventie hangt af van de bereidwilligheid van zorgverzekeraars dergelijke behandeling te vergoeden, eventueel onder voorwaarden. De kosten van een jaar lang behandeling met een glucosesensor bedragen ongeveer €1500, al kunnen onderlinge prijsafspraken tussen aanbieders en zorgverzekeraars tot een lagere prijs leiden. Het gaat tegenwoordig in bijna alle gevallen om zogenaamde ‘real-time’ sensoren; scannen is bijna nooit meer nodig, zodat de termen ‘flash’ of ‘intermittent scanning’ waarschijnlijk zullen verdwijnen. Het is goed denkbaar dat glucosesensoren binnen afzienbare tijd de ‘nieuwe norm’ gaan worden voor glucose monitoring voor mensen met diabetes die insuline gebruiken, zoals dat tot op heden gold voor glucosemeters die glucose meten in capillair bloed (uit vingerprikken).
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Toevoeging van een glucosesensor aan de behandeling van DM2 is geassocieerd met een verbetering van de tijd in doelbereik (TIR) van 4.97% (isCGM) en respectievelijk 7.48% (rtCGM) ten opzichte van vingerprikmetingen, hetgeen vooral ‘ten koste’ gaat van een lagere TAR. Gelijktijdig is er sprake van een geringe afname van de TBR. Hoewel deze afname op zichzelf te gering is om als klinisch relevant te duiden, moet dit beschouwd worden in het licht van de toename aan TIR. Omdat verbetering van glucoseregulatie nogal eens leidt tot een grotere incidentie van hypoglykemieën en meer TBR (Gerstein, 2008; Patel, 2008), zijn deze verbeteringen gezamenlijk klinisch relevant.
Het is belangrijk om op te merken dat de uitkomsten niet werden beïnvloed door de behandeling met insuline. Bij de meeste studies gebruikten de deelnemers een combinatie van insuline en verschillende andere glucoseverlagende medicijnen, maar zaten er ook deelnemers tussen die geen insuline gebruikten en was bij twee onderzoeken juist helemaal geen sprake van insulinegebruik. Hoewel onduidelijk is of het bij insulinegebruik ging om alleen basaal (suppletie) insuline of om een basaal-bolusschema, suggereert dit dat dit voor de uitkomsten niet uitmaakt. Het onderliggende ‘mechanisme’ van verbetering is bij insulinegebruikers versus niet-insulinegebruikers waarschijnlijk wel verschillend, omdat insulinegebruik gepaard gaat met risico op hypoglykemieën en de meeste overige glucoseverlagende medicatie (met uitzondering van SU-derivaten) niet. Bij laatstgenoemde groep speelt biofeedback mogelijk een grote rol bij de bereikte resultaten, maar dat betrof hier niet de voornaamste vraagstelling. Daarom wordt de aanbeveling betrokken op degenen met insulinegebruik, onafhankelijk van het toegepaste schema.
Het is in dit kader belangrijk om vast te stellen dat de primaire uitkomstmaat bij geen van de onderzoeken hypoglykemieën of TBR betrof, maar vrijwel in alle gevallen HbA1c en eenmaal gebruiksgemak. Hypoglykemieën werden weinig of helemaal niet gerapporteerd en vaak ook niet of onvoldoende bijgehouden. HbA1c is geen geschikte uitkomstmaat voor de schatting van het risico op hypoglykemieën. Waarschijnlijk werden patiënten met een verhoogd risico op hypoglykemieën, zoals degenen met verminderde awareness voor hypoglykemieën of ernstige hypoglykemieën in de voorgeschiedenis van deelname uitgesloten. Het is aannemelijk dat bij deze patiënten de toegevoegde waarde van een glucosesensor wat meer verschoven zal zijn in de richting van vermindering van hypoglykemieën en TBR ten opzichte van de toename aan TIR.
Er is geen onderzoek gedaan waarbij rtCGM en isCGM met elkaar zijn vergeleken. Afgaande op het bereikte resultaat van TIR lijkt gebruik van rtCGM iets effectiever dan dat van isCGM, waarbij de toename van de TIR bij de eerste als klinisch relevant werd geïnterpreteerd en die van isCGM (net) niet, omdat die onder de 5% zat. Voor de dagelijkse praktijk is dit echter niet langer meer relevant, omdat isCGM (ook wel flash glucose monitoring genoemd) van de markt zal verdwijnen. Bij de meest toegepaste vorm van isCGM is scannen (flashen) niet meer nodig; daarmee is isCGM ook een volwaardige rtCGM geworden.
Onderbouwing
Hypoglycaemia is by far the most common complication among people with diabetes who are treated with insulin or insulin secretagogues, with frequencies averaging 2-3 events per week in those with type 1 and 2-3 events per month in those with type 2 diabetes. Hypoglycaemia is defined by three levels according to the International Hypoglycaemia Study Group (IHSG, 2017). Level 1 refers to glucose <3.9 mmol/l, level 2 to glucose <3.0 mmol/l and level 3 to severe hypoglycaemia. In addition, severe hypoglycaemia, defined by the need for external help because of cognitive decline and occurring at a yearly basis, puts these people at high risk of physical harm, including increased risk of mortality. Many people with diabetes and their family members fear hypoglycaemic events, often more so than (chronic) hyperglycaemia. As a consequence, hypoglycaemia is an important barrier to achieve optimal glucose control, thus maintaining high risks of micro- and macrovascular complications of diabetes. In itself, hypoglycaemia has been associated with increased risks of cardiovascular morbidity and mortality, probably in part through its pro-inflammatory effects. Current technology, i.e. continuous glucose monitoring and closed-loop systems, has been shown to be highly effective in reducing the incidence of (severe) hypoglycaemia among people with type 1 diabetes. Whether and to what extent this is also the case for people with type 2 diabetes is less clear.
•rtCGM
|
Outcome
|
Study results and measurements |
Absolute effect estimates1 |
Certainty of the evidence (Quality of evidence) |
Summary* |
|
|
SMBG |
rtCGM |
||||
|
Severe hypoglycemia
|
Relative risk: 0.51 (CI 95% 0.03 - 7.99) Based on data from 175 participants in 1 studies
|
2 per 100 |
1 per 100 |
Very low Due to serious risk of bias and to extremely serious imprecision |
The evidence is very uncertain about the effect of rtCGM on severe hypoglycemia comapared to SMBG in patients with DM2. |
|
Difference: 1 fewer per 100 (CI 95% 2 fewer - 14 more) |
|||||
|
Hypoglycemia |
Due to inconsistent evidence, no effect estimate could be calculated Based on data from 245 participants in 2 studies |
- |
No GRADE |
Due to inconsistent evidence, no GRADE conclusion could be drawn. |
|
|
TIR
|
Measured by: Scale: - High better Based on data from 533 participants in 5 studies
|
Difference: MD 7.48 higher (CI 95% 2.83 higher - 12.13 higher) |
Low Due to serious risk of bias and serious imprecision
|
rtCGM may result in in a higher TIR compared to SMBG in patients with DM2. |
|
|
TBR
|
Measured by: Scale: - Lower better Based on data from 552 participants in 6 studies
|
Difference: MD 0.48 lower (CI 95% 0.88 lower - 0.08 lower) |
Moderate Due to serious risk of bias
|
rtCGM likely results in little to no difference in TBR compared to SMBG in patients with DM2. |
|
|
TAR
|
Measured by: Scale: - Lower better Based on data from 533 participants in 5 studies
|
Difference: MD 6.84 lower (CI 95% 11.63 lower - 2.05 lower) |
Low Due to serious risk of bias and serious imprecision
|
rtCGM may result in in a lower TAR compared to SMBG in patients with DM2. |
|
|
HbA1c
|
Measured by: Scale: - Lower better Based on data from 720 participants in 8 studies
|
Difference: MD 3.95 lower (CI 95% 5.46 lower - 2.44 lower) |
Low Due to serious risk of bias and serious imprecision
|
rtCGM may result in little to no difference in HbA1c compared to SMBG in patients with DM2. |
|
1Mean results per treatment group were not reported for continuous outcomes, only mean differences between group.
• isCGM/FGM
|
Outcome |
Study results and measurements |
Absolute effect estimates1 |
Certainty of the evidence (Quality of evidence) |
Summary |
|
|
SMBG |
FGM |
||||
|
Severe hypoglycemia
|
Relative risk: 0.73 (CI 95% 0.11 - 4.8) Based on data from 365 participants in 2 studies
|
2 per 1000 |
1 per 1000 |
Very low Due to extremely serious imprecision |
The evidence is very uncertain about the effect of isCGM/FGM on severe hypoglycemia compared to SMBG in patients with DM2. |
|
Difference: 1 fewer per 1000 (CI 95% 2 fewer - 8 more) |
|||||
|
Hypoglycemia |
Due to inconsistent evidence, no effect estimate could be calculated Based on data from 245 participants in 2 studies |
- |
No GRADE |
Due to inconsistent evidence, no GRADE conclusion could be drawn. |
|
|
TIR
|
Measured by: Scale: - High better Based on data from 404 participants in 3 studies
|
Difference: MD 4.97 higher (CI 95% 3.98 lower - 13.91 higher) |
Moderate Due to serious imprecision |
isCGM/FGM likely results in little to no difference in TIR compared to SMBG in patients with DM2. |
|
|
TBR
|
Measured by: Scale: - Lower better Based on data from 404 participants in 3 studies
|
Difference: MD 1.60 lower (CI 95% 5.48 lower - 2.28 higher) |
Low Due to very serious imprecision
|
isCGM/FGM may result in a lower TBR compared to SMBG in patients with DM2. |
|
|
TAR
|
Measured by: Scale: - Lower better Based on data from 404 participants in 3 studies
|
Difference: MD 3.64 lower (CI 95% 16.70 lower - 9.42 higher) |
Low Due to very serious imprecision
|
isCGM/FGM may result in little to no difference in TAR compared to SMBG in patients with DM2. |
|
|
HbA1c
|
Measured by: Scale: - Lower better Based on data from 528 participants in 4 studies
|
Difference: MD 1.79 lower (CI 95% 5.28 lower - 1.69 higher) |
Moderate Due to serious imprecision
|
isCGM/FGM may result in little to no difference in HbA1c compared to SMBG in patients with DM2. |
|
1Mean results per treatment group were not reported for continuous outcomes, only mean differences between group.
Description of studies
One study (systematic review) was included in the analysis of the literature (Jancev, 2024). Important study characteristics and results of the individual studies are summarized in table 2. The assessment of the risk of bias of the individual studies is summarized in Figure 2 of the supplementary file of Jancev (2024).
Jancev (2024) searched Embase, MEDLINE (via PubMed), Web of Science, Scopus and ClinicalTrials for relevant articles from inception until 2 May 2023. Studies were eligible if they compared CGM (rtCGM or isCGM) to SMBG (or isCGM when rtCGM was the main intervention, although no trials were included fort his reason) and reported HbA1c as an outcome measure. RCTs with a minimum intervention period of 6 weeks of consecutive or intermittent use of CGM among adults with type 2-diabetes (irrespective of diabetes treatment) in an outpatient setting were included. Studies with pregnant women or individuals with type 1-diabetes, studies that investigated GlucoWatch or a professional CGM (pCGM) device (e.g. Abbott Freestyle Libre Pro IQ or Dexcom G6 Pro) or an intervention that consisted of CGM combined with an additional glucose-lowering treatment strategy were excluded. A total of twelve RCT’s were included in the systematic review, of which eight trials investigated the effectivity of rtCGM versus SMBGand four trials investigated isCGM. Risk of bias was rated using the Cochrane risk-of-bias tool version 2. Eight individual studies were rated as ‘some concerns for risk of bias’ (Bergenstal, 2022; Cosson, 2009; Haak, 2017; Moon, 2022; Price, 2021; Vigersky, 2012; Yaron, 2019; Yoo, 2008) while the remaining four studies were rated as ‘low risk’ (Ajjan, 2023; Beck, 2017; Martens, 2021; Wada, 2020).
Table 2. Characteristics of included studies
|
Study |
Participants |
Comparison |
|
Follow-up |
Outcome measures |
Comments |
Risk of bias (per outcome measure)* |
|
|
|
Included in systematic review by Jancev, 2024 (all RCT’s) |
|||||||
|
Ajjan, 2023 |
N at baseline Intervention: 69 Control: 72
Age (mean) Intervention: 63.2 Control: 62.0
Sex (males) Intervention: 74% Control: 72%
Insulin use Intervention: 52% Control: 47% |
Intervention: isCGM
Control: SMBG |
|
43 weeks |
Severe hypoglycemia, TBR, TIR, TAR, HbA1c |
|
Low risk (all outcome measures) |
|
|
Beck, 2017 |
N at baseline Intervention: 79 Control: 79
Age (mean) Intervention: 60.0 Control: 60.0
Sex (males) 43.7% (total)
Insulin use 100% |
Intervention: rtCGM
Control: SMBG |
|
24 weeks |
Severe hypoglycemia, TBR, TIR, TAR, HbA1c |
|
Low risk (all outcome measures) |
|
|
Bergenstal, 2022 |
N at baseline Intervention: 59 Control: 55
Age (mean) Intervention: 59.3 Control: 58.8
Sex (males) 46.5% (total)
Insulin use Not specified |
Intervention: rtCGM
Control: SMBG |
|
16 weeks |
TBR, TIR, TAR, HbA1c |
|
Some concerns (all outcome measures) |
|
|
Cosson, 2009 |
N at baseline Intervention: 11 Control: 14
Age (mean) Intervention: 57.2 Control: 57.3
Sex (males) 68.0% (total)
Insulin use Intervention: 27% Control: 43% |
Intervention: rtCGM
Control: SMBG |
|
12 weeks |
TBR, HbA1c |
|
Some concerns (all outcome measures) |
|
|
Haak, 2017 |
N at baseline Intervention: 149 Control: 75
Age (mean) Intervention: 59.0 Control: 59.5
Sex (males) Intervention: 63% Control: 75%
Insulin use 100% |
Intervention: isCGM
Control: SMBG |
|
24 weeks |
Severe hypoglycemia, hypoglycemia, TBR, TIR, TAR, HbA1c |
|
Some concerns (all outcome measures) |
|
|
Martens, 2021 |
N at baseline Intervention: 116 Control: 59
Age (mean) Intervention: 56.0 Control: 59.0
Sex (males) Intervention: 47% Control: 54%
Insulin use 100% |
Intervention: rtCGM
Control: SMBG |
|
34 weeks |
Severe hypoglycemia, hypoglycemia, TBR, TIR, TAR, HbA1c |
|
Low risk (all outcome measures) |
|
|
Moon, 2023 |
N at baseline Intervention: 15 Control: 15
Age (mean) Intervention: 53.9 Control: 50.7
Sex (males) 54.2% (total)
Insulin use 0% |
Intervention: rtCGM
Control: SMBG |
|
24 weeks |
Severe hypoglycemia, TBR, TIR, TAR, HbA1c |
|
Some concerns (all outcome measures) |
|
|
Price, 2021 |
N at baseline Intervention: 46 Control: 24
Age (mean) Intervention: 58.9 Control: 60.9
Sex (males) Intervention: 59% Control: 42%
Insulin use 0% |
Intervention: rtCGM
Control: SMBG |
|
36 weeks |
Severe hypoglycemia, hypoglycemia, TBR, TIR, TAR, HbA1c |
|
Some concerns (all outcome measures) |
|
|
Vigersky, 2012 |
N at baseline Intervention: 50 Control: 50
Age (mean) Intervention: 55.5 Control: 60.0
Sex (males) Intervention: 66% Control: 44%
Insulin use Intervention: 38% Control: 28% |
Intervention: rtCGM
Control: SMBG |
|
52 weeks |
HbA1c |
|
Some concerns (all outcome measures) |
|
|
Wada, 2020 |
N at baseline Intervention: 49 Control: 51
Age (mean) Intervention: 58.1 Control: 58.7
Sex (males) Intervention: 67% Control: 69%
Insulin use 0% |
Intervention: isCGM
Control: SMBG |
|
24 weeks |
Severe hypoglycemia, hypoglycemia, TBR, TIR, TAR, HbA1c |
|
Low risk (all outcome measures) |
|
|
Yaron, 2019 |
N at baseline Intervention: 53 Control: 48
Age (mean) Intervention: 67.6 Control: 65.9
Sex (males) Intervention: 70% Control: 58%
Insulin use 100% |
Intervention: isCGM
Control: SMBG |
|
10 weeks |
Severe hypoglycemia, hypoglycemia, HbA1c |
|
Some concerns (all outcome measures) |
|
|
Yoo, 2008 |
N at baseline Intervention: 32 Control: 33
Age (mean) Intervention: 54.6 Control: 57.5
Sex (males) Intervention: 34% Control: 50%
Insulin use Intervention: 14% Control: 18% |
Intervention: rtCGM
Control: SMBG |
|
10 weeks |
Severe hypoglycemia, HbA1c |
|
Some concerns (all outcome measures) |
|
*For further details, see Figure 2 in supplementary file by Jancev (2024).
Results
The results are reported separately for rtCGM and isCGM/FGM. For the outcomes Time in range (TIR), time below range (TBR) and time above range (TAR), the following definitions were used in the review by Jancev (2024):
TIR: percentage of time glucose between 3.9–10mmol/l [70–180 mg/dl]
TBR: percentage of time glucose <3.9 mmol/l [<70 mg/dl]
TAR percentage of time glucose >10 mmol/l [>180 mg/dl]
•rtCGM
Severe hypoglycemia
A total of five studies that investigated the effectivity of rtCGM in the review by Jancev (2024) reported on severe hypoglycemia (definition not reported), although in only one study events of severe hypoglycemia occurred. Martens (2021), reported severe hypoglycemia in 1/116 (0.9%) patients of the intervention group, compared to 1/59 (1.7%) patients in the control group.
Hypoglycemia
A total of two studies reported on hypoglycemia events. Price (2021) reported no events of hypoglycemia in the intervention group (n=46), compared to one event of hypoglycemia in the control group (n=24). However, it was not reported which cut-off point was used to define hypoglycemia.
Martens (2021) reported on hypoglycemia as event rate/week, in which a hypoglycemic event was defined as 15 consecutive minutes with a sensor glucose value below 3.0 mmol/l (at least 2 sensor values <3 mmol/L that are ≥15 minutes apart plus no intervening values of ≥3 mmol/L are required to define an event). The end of the hypoglycemic event was defined as a minimum of 30 consecutive minutes with a sensor glucose concentration of 3.9 mmol/l or greater (at least 2 sensor values ≥3.9mmol/L that are ≥30 minutes apart with no intervening values <3.9 mmol/L were required to define the end of an event).
The hypoglycemia event rate/week was 0.0 (± 0.0) in the intervention group, compared to 0.2 (± 0.4) in the control group. With a follow-up of eight months, this indicates zero events in the intervention group (n = 116) and seven events in the control group (n = 59). As only events were reported and not the number of patients in which these events occurred, a risk ratio cannot be calculated.
Time in range (TIR)
A total of five studies in the review by Jancev (2024) reported on TIR, see Figure 1. The mean change (MD, 95%CI) in TIR was 7.48 (2.83 to 12.13), in favor of the intervention group, which is considered clinically relevant.
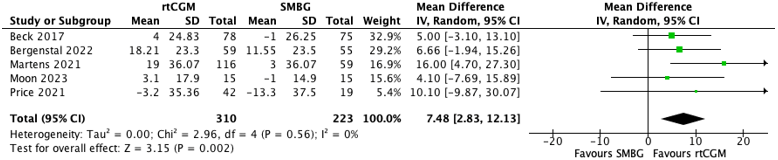
Figure 1. Forest plot of pooled analysis of change in TIR in patients with type DM2 using rtCGM vs. SMBG.
Time below range (TBR)
A total of six studies that investigated the effectivity of rtCGM in the review by Jancev (2024) reported on TBR, see Figure 2. The mean change (MD, 95%CI) in TBR was -0.48 (-0.88 to -0.08), in favor of the intervention group, which is not considered clinically relevant.
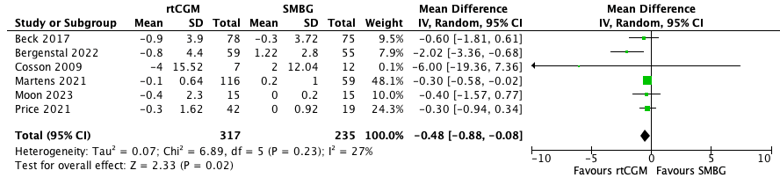
Figure 2. Forest plot of pooled analysis of change in TBR in patients with type DM2 using rtCGM vs. SMBG.
Time above range (TAR)
A total of five studies that investigated the effectivity of rtCGM in the review by Jancev (2024) reported on TAR, see Figure 3. The mean change (MD, 95%CI) in TAR was -6.84 (-11.63 to -2.05), in favor of the intervention group, which is considered clinically relevant.

Figure 3. Forest plot of pooled analysis of change in TAR in patients with type DM2 using rtCGM vs. SMBG.
HbA1c
All eight studies that investigated the effectivity of isCGM in the review by Jancev (2024) reported on HbA1c. The MD (95%CI) in HbA1c level was -3.95 (-5.46 to -2.44), in favor of the intervention group. In percentage, the mean difference was -0.36%, which is not considered clinically relevant. See Figure 1 in the study article by Jancev (2024) for details on the results.
Jancev (2024) also performed subanalyses for the effectivity of isCGM compared to SMBG on HbA1c.
•HbA1c levels
No clinically relevant differences were found for patients with a HbA1c level > 69 mmol/mol (MD -3.19 (95%CI -5.41 to -0.97)) and a HbA1c level <69 mmol/mol (MD -3.53 (95%CI -5.35 to -1.71)).
•Intervention duration
No clinically relevant differences were found for intervention duration ≤ 12 weeks (MD -4.04 (95%CI -5.70 to -2.39)) and intervention duration > 12 weeks (MD -2.66 (95%CI -5.32 to -0.01)).
•Age
No clinically relevant differences were found for patients aged >58.9 years (MD -2.30 (95%CI -4.59 to -0.01)) and patients aged <58.9 years (MD -4.17 (95%CI -5.79 to -2.55)).
•Insulin use
No clinically relevant differences were found for patients who use insulin (MD -3.27 (95%CI -6.22 to -0.31)), patients who do not use insulin (MD -3.22 (95%CI -5.39 to -1.05)) and patients who use insulin or other glucose lowering medication (MD -3.65 (95%CI -6.14 to -1.15)). In this last group, studies were included in which patients used insulin and/or glucose lowering medication (in contrast to the first group).
•isCGM/FGM
Severe hypoglycemia
All four studies that investigated the effectivity of isCGM in the review by Jancev (2024) reported on severe hypoglycemia, although in only two studies events of severe hypoglycemia occurred (Ajjan, 2023; Haak, 2017). Ajjan (2023), reported severe hypoglycemia in 0/69 (0%) patients of the intervention group, compared to 2/72 (2.8%) patients in the control group.
Hypoglycemia
A total of three studies reported on hypoglycemia. Wada (2020) reported a total of three hypoglycemia adverse events, experienced by three participants (2/49 in the intervention group and 1/51 in the control group). However, it was not reported which cut-off point was used.
Yaron (2019) reported the number of patients with one or more hypoglycemic events separately for glucose levels <3.9 mmol/L and glucose levels <3.0 mmol/L.
•Hypoglycemia <3.9 mmol/L
A total of 15/52 (28%) patients in the intervention group had one or more hypoglycemic events (glucose level <3.9 mmol/L), compared to 16/44 (36%) patients in the control group. The corresponding risk ratio (95% CI) is 0.79 (0.44 to 1.42), in favor of the intervention group, which is not considered clinically relevant.
•Hypoglycemia <3.0 mmol/L
A total of 6/52 (11%) patients in the intervention group had one or more hypoglycemic events (glucose level <3.0 mmol/L, compared to 4/44 (9%) patients in the control group. The corresponding risk ratio (95% CI) is 1.27 (0.38 to 4.21), in favor of the control group, which is considered clinically relevant.
Haak (2017) reported the mean differences in number of hypoglycemic events/day between the intervention and control group, separately for glucose levels <3.9 mmol/L and glucose levels <3.1 mmol. However, no baseline values were reported.
•Hypoglycemia <3.9 mmol/L
Haak reported that the frequency of events with glucose <3.9 mmol/L was 28% less (-0.16 ± 0.065 per day mean ± SE) in the intervention group compared with the control group. This is considered clinically relevant.
•Hypoglycemia <3.0 mmol/L
The frequency of events <3.1 mmol/L was 44% less (-0.12 ± 0.037) in the intervention group compared with the control group. This is considered clinically relevant.
The total number of patients experiencing hypoglycemic adverse events was 10/149 (6.7%) in the intervention group compared to 7/75 (9.3%) in the control group. The corresponding risk ratio (95% CI) is 0.72 (0.29 to 1.81), in favor of the intervention group, which is considered clinically relevant. However, it was not reported which cut-off point was used.
Time in range (TIR)
A total of three studies that investigated the effectivity of isCGM in the review by Jancev (2024) reported on TIR, see Figure 4. The mean change (MD, 95%CI) in TIR was 4.97 (-3.96 to 13.91), in favor of the intervention group, which is not considered clinically relevant.

Figure 4. Forest plot of pooled analysis of change in TIR in patients with type DM2 using isCGM vs. SMBG.
Time below range (TBR)
A total of three studies that investigated the effectivity of isCGM within the review by Jancev (2024) reported on TBR, see Figure 5. The mean change (MD, 95%CI) in TBR was -1.60 (-5.48 to 2.28), in favor of the intervention group, which is considered clinically relevant.

Figure 5. Forest plot of pooled analysis of change in TBR in patients with type DM2 using isCGM vs. SMBG.
Time above range (TAR)
A total of three studies that investigated the effectivity of in the review by Jancev (2024) reported on TAR, see Figure 6. The mean change (MD, 95%CI) in TAR was -3.64 (-16.70 to 9.42), in favor of the intervention group, which is not considered clinically relevant.

Figure 6. Forest plot of pooled analysis of change in TAR in patients with type DM2 using isCGM vs. SMBG.
HbA1c
All four studies that investigated the effectivity of isCGM in the review by Jancev (2024) reported on HbA1c. The MD (95%CI) in HbA1c level was -1.79 (-5.28 to 1.69), in favor of the intervention group. In percentage, the mean difference was -0.16%, which is not considered clinically relevant. See Figure 1 in the study article by Jancev (2024) for details on the results.
A systematic review of the literature was performed to answer the following question(s):
What is the effectivity of continuous glucose monitoring (CGM) and flash glucose monitoring (FGM) in the prevention of hypoglycemia compared to self-monitoring of blood glucose (SMBG) in adult patients with diabetes mellitus type 2?
Table 1. PICO
|
Patients |
Adult patients with diabetes mellitus type 2 |
|
Intervention |
Continuous glucose monitoring (CGM), flash glucose monitoring (FGM) |
|
Control |
Self-monitoring of blood glucose (SMBG) |
|
Outcomes |
(severe) hypoglycemia, time in range (TIR), time below range (TBR), time above range (TAR), HbA1c |
|
Other selection criteria |
Study design: systematic reviews and randomized controlled trials, observational studies |
Relevant outcome measures
The guideline panel considered (severe) hypoglycemia as a critical outcome measure for decision making; and TBR, TIR, TAR and HbA1c as an important outcome measure for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies. For the definition of hypoglycaemia, the 3-level IHSG classification was used in which level 1 refers to glucose <3.9 mmol/l, level 2 to glucose <3.0 mmol/l and level 3 to severe hypoglycaemia as defined above
The guideline panel defined the following cut-off points as a minimal clinically (patient) important difference:
Hypoglycemia/severe hypoglycemia: Difference of 25%
TBR: Absolute difference of 1%
TIR and TAR: Absolute difference of 5%
HbA1c: Difference of 5 mmol/mol (~0.5%)
Search and select (Methods)
A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2004 to 11 December 2024 for systematic reviews, RCTs and observational studies. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from three primary search concepts: (1) diabetes mellitus; (2) continuous glucose monitoring; (3) hypoglycemia. Duplicates were removed using EndNote software. After deduplication a total of 359 records were imported for title/abstract screening. Initially, 25 studies were selected based on title and abstract screening. After reading the full text, 24 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’), and 1 study was included.
- Action to Control Cardiovascular Risk in Diabetes Study Group; Gerstein HC, Miller ME, Byington RP, Goff DC Jr, Bigger JT, Buse JB, Cushman WC, Genuth S, Ismail-Beigi F, Grimm RH Jr, Probstfield JL, Simons-Morton DG, Friedewald WT. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008 Jun 12;358(24):2545-59. doi: 10.1056/NEJMoa0802743. Epub 2008 Jun 6. PMID: 18539917; PMCID: PMC4551392.
- ADVANCE Collaborative Group; Patel A, MacMahon S, Chalmers J, Neal B, Billot L, Woodward M, Marre M, Cooper M, Glasziou P, Grobbee D, Hamet P, Harrap S, Heller S, Liu L, Mancia G, Mogensen CE, Pan C, Poulter N, Rodgers A, Williams B, Bompoint S, de Galan BE, Joshi R, Travert F. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008 Jun 12;358(24):2560-72. doi: 10.1056/NEJMoa0802987. Epub 2008 Jun 6. PMID: 18539916.
- Ajjan RA, Heller SR, Everett CC, et al. Multicenter randomized trial of intermittently scanned continuous glucose monitoring versus self-monitoring of blood glucose in individuals with type 2 diabetes and recent-onset acute myocardial infarction: results of the LIBERATES trial. Diabetes Care. 2023;46(2):441–449. doi: 10.2337/dc22-1219.
- Beck RW, Riddlesworth TD, Ruedy K, et al. Continuous glucose monitoring versus usual care in patients with type 2 diabetes receiving multiple daily insulin injections. Ann Intern Med. 2017;167(6):365–374. doi: 10.7326/M16-2855.
- Bergenstal RM, Mullen DM, Strock E, Johnson ML, Xi MX. Randomized comparison of self-monitored blood glucose (BGM) versus continuous glucose monitoring (CGM) data to optimize glucose control in type 2 diabetes. J Diabetes Complications. 2022;36(3):108106. doi: 10.1016/j.jdiacomp.2021.108106.
- Cosson E, Hamo-Tchatchouang E, Dufaitre-Patouraux L, Attali JR, Pariès J, Schaepelynck-Bélicar P. Multicentre, randomised, controlled study of the impact of continuous sub-cutaneous glucose monitoring (GlucoDay®) on glycaemic control in type 1 and type 2 diabetes patients. Diabetes Metab. 2009;35(4):312–318. doi: 10.1016/j.diabet.2009.02.006.
- Haak T, Hanaire H, Ajjan R, Hermanns N, Riveline J-P, Rayman G. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: a multicenter, open-label randomized controlled trial. Diabetes Ther. 2017;8(1):55–73. doi: 10.1007/s13300-016-0223-6.
- International Hypoglycaemia Study Group. Glucose concentrations of less than 3.0 mmol/l (54 mg/dl) should be reported in clinical trials: a joint position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2017 Jan;60(1):3-6. doi: 10.1007/s00125-016-4146-6. Erratum in: Diabetologia. 2017 Feb;60(2):377. doi: 10.1007/s00125-016-4168-0. PMID: 27872948; PMCID: PMC6518070.
- Jancev M, Vissers TACM, Visseren FLJ, van Bon AC, Serné EH, DeVries JH, de Valk HW, van Sloten TT. Continuous glucose monitoring in adults with type 2 diabetes: a systematic review and meta-analysis. Diabetologia. 2024 May;67(5):798-810. doi: 10.1007/s00125-024-06107-6. Epub 2024 Feb 16. PMID: 38363342; PMCID: PMC10954850.
- Martens T, Beck RW, Bailey R et al (2021) Effect of continuous glucose monitoring on glycemic control in patients with type 2 diabetes treated with basal insulin: a randomized clinical trial. JAMA 325(22):2262–2272. 10.1001/jama.2021.7444.
- Moon SJ, Kim KS, Lee WJ, Lee MY, Vigersky R, Park CY. Efficacy of intermittent short-term use of a real-time continuous glucose monitoring system in non-insulin–treated patients with type 2 diabetes: a randomized controlled trial. Diabetes Obes Metab. 2023;25(1):110–120. doi: 10.1111/dom.14852.
- Price DA, Deng Q, Kipnes M, Beck SE. Episodic real-time CGM use in adults with type 2 diabetes: results of a pilot randomized controlled trial. Diabetes Ther. 2021;12(7):2089–2099. doi: 10.1007/s13300-021-01086-y.
- Vigersky RA, Fonda SJ, Chellappa M, Walker MS, Ehrhardt NM. Short- and long-term effects of real-time continuous glucose monitoring in patients with type 2 diabetes. Diabetes Care. 2012;35(1):32–38. doi: 10.2337/dc11-1438.
- Wada E, Onoue T, Kobayashi T, et al. Flash glucose monitoring helps achieve better glycemic control than conventional self-monitoring of blood glucose in non-insulin-treated type 2 diabetes: a randomized controlled trial. BMJ Open Diabetes Res Care. 2020;8(1):10–17. doi: 10.1136/bmjdrc-2019-001115.
- Yaron M, Roitman E, Aharon-Hananel G, et al. Effect of flash glucose monitoring technology on glycemic control and treatment satisfaction in patients with type 2 diabetes. Diabetes Care. 2019;42(7):1178–1184. doi: 10.2337/dc18-0166.
- Yoo HJ, An HG, Park SY, et al. Use of a real time continuous glucose monitoring system as a motivational device for poorly controlled type 2 diabetes. Diabetes Res Clin Pract. 2008;82(1):73–79. doi: 10.1016/j.diabres.2008.06.015.
Risk of Bias tables
See Figure 2 in supplementary file by Jancev (2024).
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Ontario Health (Quality). Flash Glucose Monitoring System for People with Type 1 or Type 2 Diabetes: A Health Technology Assessment. Ont Health Technol Assess Ser. 2019 Dec 12;19(8):1-108. PMID: 31942227; PMCID: PMC6939983. |
More recent review available, only on FGM. |
|
Azhar A, Gillani SW, Mohiuddin G, Majeed RA. A systematic review on clinical implication of continuous glucose monitoring in diabetes management. J Pharm Bioallied Sci. 2020 Apr-Jun;12(2):102-111. doi: 10.4103/jpbs.JPBS_7_20. Epub 2020 Apr 10. PMID: 32742108; PMCID: PMC7373113. |
More recent review available |
|
Bano A, Künzler J, Wehrli F, Kastrati L, Rivero T, Llane A, Valz Gris A, Fraser AG, Stettler C, Hovorka R, Laimer M, Bally L; CORE‐MD investigators. Clinical evidence for high-risk CE-marked medical devices for glucose management: A systematic review and meta-analysis. Diabetes Obes Metab. 2024 Oct;26(10):4753-4766. doi: 10.1111/dom.15849. Epub 2024 Aug 14. PMID: 39143655. |
Only five studies included on DM2, only partilly according to PICO. |
|
Bidonde J, Fagerlund BC, Frønsdal KB, Lund UH, Robberstad B. FreeStyle Libre Flash Glucose Self-Monitoring System: A Single-Technology Assessment [Internet]. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Aug 21. Report from the Norwegian Institute of Public Health No. 2017-07. PMID: 29553668. |
More recent review available, only on FGM. |
|
Carlson AL, Daniel TD, DeSantis A, Jabbour S, Karslioglu French E, Kruger D, Miller E, Ozer K, Elliott T. Flash glucose monitoring in type 2 diabetes managed with basal insulin in the USA: a retrospective real-world chart review study and meta-analysis. BMJ Open Diabetes Res Care. 2022 Jan;10(1):e002590. doi: 10.1136/bmjdrc-2021-002590. PMID: 35058312; PMCID: PMC8783803. |
Only FGM, retrospective. |
|
Castellana M, Parisi C, Di Molfetta S, Di Gioia L, Natalicchio A, Perrini S, Cignarelli A, Laviola L, Giorgino F. Efficacy and safety of flash glucose monitoring in patients with type 1 and type 2 diabetes: a systematic review and meta-analysis. BMJ Open Diabetes Res Care. 2020 Jun;8(1):e001092. doi: 10.1136/bmjdrc-2019-001092. PMID: 32487593; PMCID: PMC7265013. |
More recent review available, only on FGM. |
|
Di Molfetta S, Caruso I, Cignarelli A, Natalicchio A, Perrini S, Laviola L, Giorgino F. Professional continuous glucose monitoring in patients with diabetes mellitus: A systematic review and meta-analysis. Diabetes Obes Metab. 2023 May;25(5):1301-1310. doi: 10.1111/dom.14981. Epub 2023 Feb 14. PMID: 36661362. |
More recent review available, only on FGM. |
|
Gao Y, Zhou M, Xu X, Chen WY. Effects of flash glucose monitoring on glycemic control in participants with diabetes mellitus: A meta-analysis of randomized controlled trials. J Diabetes Complications. 2022 Nov;36(11):108314. doi: 10.1016/j.jdiacomp.2022.108314. Epub 2022 Sep 28. PMID: 36208566. |
More recent review available, only on FGM. |
|
Ida S, Kaneko R, Murata K. Utility of Real-Time and Retrospective Continuous Glucose Monitoring in Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trials. J Diabetes Res. 2019 Jan 15;2019:4684815. doi: 10.1155/2019/4684815. PMID: 30775385; PMCID: PMC6350576. |
More recent review available, only on CGM. |
|
Janapala RN, Jayaraj JS, Fathima N, Kashif T, Usman N, Dasari A, Jahan N, Sachmechi I. Continuous Glucose Monitoring Versus Self-monitoring of Blood Glucose in Type 2 Diabetes Mellitus: A Systematic Review with Meta-analysis. Cureus. 2019 Sep 12;11(9):e5634. doi: 10.7759/cureus.5634. PMID: 31700737; PMCID: PMC6822918. |
More recent review available. |
|
Kong SY, Cho MK. Effects of Continuous Glucose Monitoring on Glycemic Control in Type 2 Diabetes: A Systematic Review and Meta-Analysis. Healthcare (Basel). 2024 Feb 29;12(5):571. doi: 10.3390/healthcare12050571. PMID: 38470682; PMCID: PMC10931178. |
Only on CGM, results not reported separately for insulin versus non-insulin users. |
|
Liang B, Koye DN, Hachem M, Zafari N, Braat S, Ekinci EI. Efficacy of Flash Glucose Monitoring in Type 1 and Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Front Clin Diabetes Healthc. 2022 Feb 22;3:849725. doi: 10.3389/fcdhc.2022.849725. PMID: 36992733; PMCID: PMC10012125. |
Only on FGM. |
|
Lu J, Ying Z, Wang P, Fu M, Han C, Zhang M. Effects of continuous glucose monitoring on glycaemic control in type 2 diabetes: A systematic review and network meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2024 Jan;26(1):362-372. doi: 10.1111/dom.15328. Epub 2023 Oct 12. PMID: 37828805. |
Only on CGM |
|
Maiorino MI, Signoriello S, Maio A, Chiodini P, Bellastella G, Scappaticcio L, Longo M, Giugliano D, Esposito K. Effects of Continuous Glucose Monitoring on Metrics of Glycemic Control in Diabetes: A Systematic Review With Meta-analysis of Randomized Controlled Trials. Diabetes Care. 2020 May;43(5):1146-1156. doi: 10.2337/dc19-1459. PMID: 32312858. |
More recent review available. |
|
Park C, Le QA. The Effectiveness of Continuous Glucose Monitoring in Patients with Type 2 Diabetes: A Systematic Review of Literature and Meta-analysis. Diabetes Technol Ther. 2018 Sep;20(9):613-621. doi: 10.1089/dia.2018.0177. Epub 2018 Aug 10. PMID: 30095980. |
More recent review available. |
|
Seidu S, Kunutsor SK, Ajjan RA, Choudhary P. Efficacy and Safety of Continuous Glucose Monitoring and Intermittently Scanned Continuous Glucose Monitoring in Patients With Type 2 Diabetes: A Systematic Review and Meta-analysis of Interventional Evidence. Diabetes Care. 2024 Jan 1;47(1):169-179. doi: 10.2337/dc23-1520. PMID: 38117991. |
Intervention of at least 8 weeks, also observational studies included. |
|
Uhl S, Choure A, Rouse B, Loblack A, Reaven P. Effectiveness of Continuous Glucose Monitoring on Metrics of Glycemic Control in Type 2 Diabetes Mellitus: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J Clin Endocrinol Metab. 2024 Mar 15;109(4):1119-1131. doi: 10.1210/clinem/dgad652. PMID: 37987208. |
Review with more recent search date available. |
|
Aggarwal A, Pathak S, Goyal R. Clinical and economic outcomes of continuous glucose monitoring system (CGMS) in patients with diabetes mellitus: A systematic literature review. Diabetes Res Clin Pract. 2022 Apr;186:109825. doi: 10.1016/j.diabres.2022.109825. Epub 2022 Mar 9. PMID: 35278520. |
More recent review available. |
|
Cowart K, Updike W, Bullers K. Systematic Review of Randomized Controlled Trials Evaluating Glycemic Efficacy and Patient Satisfaction of Intermittent-Scanned Continuous Glucose Monitoring in Patients with Diabetes. Diabetes Technol Ther. 2020 May;22(5):337-345. doi: 10.1089/dia.2019.0345. PMID: 31859531. |
More recent review available. |
|
Dicembrini I, Mannucci E, Monami M, Pala L. Impact of technology on glycaemic control in type 2 diabetes: A meta-analysis of randomized trials on continuous glucose monitoring and continuous subcutaneous insulin infusion. Diabetes Obes Metab. 2019 Dec;21(12):2619-2625. doi: 10.1111/dom.13845. Epub 2019 Sep 13. PMID: 31368658. |
More recent review available. |
|
Evans M, Welsh Z, Ells S, Seibold A. The Impact of Flash Glucose Monitoring on Glycaemic Control as Measured by HbA1c: A Meta-analysis of Clinical Trials and Real-World Observational Studies. Diabetes Ther. 2020 Jan;11(1):83-95. doi: 10.1007/s13300-019-00720-0. Epub 2019 Oct 31. PMID: 31673972; PMCID: PMC6965602. |
More recent review available. |
|
Evans M, Welsh Z, Seibold A. Reductions in HbA1c with Flash Glucose Monitoring Are Sustained for up to 24 Months: A Meta-Analysis of 75 Real-World Observational Studies. Diabetes Ther. 2022 Jun;13(6):1175-1185. doi: 10.1007/s13300-022-01253-9. Epub 2022 Apr 27. PMID: 35476279; PMCID: PMC9174370. |
Older review, only observational studies included. |
|
Kamusheva M, Tachkov K, Dimitrova M, Mitkova Z, García-Sáez G, Hernando ME, Goettsch W, Petrova G. A Systematic Review of Collective Evidences Investigating the Effect of Diabetes Monitoring Systems and Their Application in Health Care. Front Endocrinol (Lausanne). 2021 Mar 16;12:636959. doi: 10.3389/fendo.2021.636959. PMID: 33796074; PMCID: PMC8008960. |
More recent review available. |
|
Cowart K. A Review of the First Long-term Implantable Continuous Glucose Monitoring System Available in the United States. J Diabetes Sci Technol. 2021 Jan;15(1):160-166. doi: 10.1177/1932296819890865. Epub 2019 Dec 13. PMID: 31833388; PMCID: PMC7782996. |
More recent review available. Specific on LTI CGM. |
Beoordelingsdatum en geldigheid
Publicatiedatum : 02-05-2026
Beoordeeld op geldigheid : 02-05-2026
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire cluster ingesteld. Het cluster Diabetes Mellitus bestaat uit meerdere richtlijnen, zie hier voor de actuele clusterindeling. De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden geven hun expertise in, indien nodig. De volgende personen uit het cluster zijn betrokken geweest bij de herziening van deze module:
Clusterstuurgroep
- Dr. E.H. (Erik) Serné, internist in het AUMC te Amsterdam, NIV, voorzitter cluster
- Dr. L.P.F. (Luc) Janssens, kinderarts in het Isala te Zwolle, NVK
- Dr. W.J. (Wouter) de Waal, kinderarts in het Sint Antonius Ziekenhuis te Nieuwegein, NVK
- Dr. R.C. (Rebecca) Painter, gyneaocoloog in het AUMC te Amsterdam, NVOG
- Dr. B.E. (Bastiaan) de Galan, internist in het MUMC te Maastricht, NIV
- T.M. (Ties) Obers, patiëntvertegenwoordiger, Diabetesvereniging Nederland
Betrokken clusterexpertisegroepleden
- Dr. B.E. (Bastiaan) de Galan, internist in het MUMC te Maastricht, NIV
- Dr. H.W. (Harold) de Valk, internist in het UMCU te Utrecht, NIV
- Dr. M.G.J. (Martin) Willink, huisarts, NHG
Met ondersteuning van
- Dr. A.N. (Anh Nhi) Nguyen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten.
- Dr. L. (Leanne) Küpers, adviseur, Kennisinstituut van de Federatie Medisch Specialisten.
- Drs. J.M.H. (Harm-Jan) van der Hart, adviseur, Kennisinstituut van de Federatie Medisch Specialisten.
- Drs. F.A. (Fieke) Pepping, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten.
Belangenverklaringen
Een overzicht van de belangen van de clusterleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Clusterstuurgroepleden
Tabel 9 Gemelde (neven)functies en belangen stuurgroep
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Restrictie |
|
Dr. E.H. (Erik) Serné |
Internist-Vasculaire Geneeskunde binnen Amsterdam UMC, locatie VUmc |
Clustervertegenwoordiger (NIV, NVK, NHG) binnen bestuur Nederlandse Diabetes Federatie (betaald) Lid van Rondetafel Diabeteszorg (onbetaald) Hoofdredacteur Nederlands Tijdschrift voor Diabetologie (betaald) Redactielid platform Diabetesgeneeskunde.nl (betaald) Medisch directeur van Diabeter Centrum Amsterdam, een joint venture tussen Amsterdam UMC en Diabeter; aangesteld via een detacheringscontract vanuit Amsterdam UMC (betaald). Medtronic is deels eigenaar van Diabeter. |
Geen |
Doelmatigheidsproject ZonMw betreffende behandeling patiënten met 'hypoglycemia unawareness' met 'stepped care' bestaande uit cursus HypoBewust en vervolgens evetueel continueglucose monitoring (CGM) versus directe start CGM
Veelbelovende zorg ZonMw-project betreffende Bi-hormonale kunstalvleesklier bij volwassen patiënten met diabetes type 1 die hun behandeldoelen niet halen; Automated blood glucose control in type 1 diabetes: effectiveness of the artificial pancreas (DARE-study)
Doelmatigheidsproject ZonMw betreffende LOFIT: Lifestyle front Office For Integrating lifestyle medicine in the Treatment of patients: a novel care-model towards community-based options for lifestyle change |
Advisering binnen Ronde Tafel Diabeteszorg betreffende doelmatige inzet nieuwe behandelingen toont belangrijke parallellen met richtlijnvorming. Beide maken gebruik van 'evidence-based medicine' en GRADE om de beschikbare data te duiden. Hierbij is dus geen sprake van belangenverstrengeling, maar van synergie. |
Restrictie t.a.v. besluitvorming bij modules HCl bij zwangerschap met DM1 en Preventie hypoglykemie met sensor bij diabetes mellitus type 2 |
|
Dr. L.P.F. (Luc) Janssens |
Kinderarts Isala |
Geen |
Geen |
Geen |
Geen |
Geen |
|
Dr. W.J. (Wouter) de Waal |
Kinderarts Diakonessenhuis Utrecht |
Kinderarts Diabetes Centraal |
Geen |
Geen |
Geen |
Geen |
|
Dr. R.C. (Rebecca) Painter |
Gynaecoloog-perinatoloog Amsterdam UMC, hoogleraar verloskunde Vrije Universiteit Per 1 sept: Gynaecoloog-perinatoloog Erasmus MC, Hoogleraar Erasmus Universiteit |
Wetenschappelijk Adviseur Stichting ZEHG (onbetaald) Voorzitter werkgroep NVOG Richtlijn "schildklier en zwangerschap" (vacatiegelden) Lid werkgroep NVOG Richtlijn "Hyperemesis gravidarum" (vacatiegelden) Lid Koepel Wetenschap NVOG, namense Pijler FMG (onbetaald) Vice voorzitter NVOG Pijler FMG Wetenschapscommissie (onbetaald) Voorzitter NVOG SIG Diabetes en Zwangerschap (onbetaald) Lid Stadscoaltie Amsterdam Kansrijke Start (onbetaald) Projectleider en lid kernteam Netwerk Geboortezorg Noordwest Nederland (onbetaald) Bestuurslid NRCG, Nederlandse Regionale Consortia Geboortezorg (onbetaald) Lid Bestuurd Verloskundig Samenwerkingsverband Amsterdam UMC (onbetaald) Projectleider en hoofdonderzoeker SugarDip, TANGO-DM, PI NL RCTs (onbetaald) |
Geen |
ZonMW: SugarDip, projectleider PI NL, projectleider Netwerk Geboortezorg Noordwest Nederland, projectleider VSV stimulering implementatie basiskader, projectleider Minder dieren, meer kennis: Metformine in diermodellen systematic review, project leider NRCG, nationale regionale geboorteconsortia, geen projectleider
Diabetes Fonds: Register Diabetes en Zwangerschap, geen projectleider
Leading the Change: Tango DM, projectleider
Toegevoegd tijdens vergadering: CRISTAL studie (HCL bij zwangeren met DM1). Deze studie is niet gefinancierd door een farmaceut maar Medtronic heeft wel middelen geleverd. |
Projectleider TANGO DM, onderzoekt de afkapwaarden die gebruikt worden voor de diagnose diabetes gravidarum.
Medeprojectleider van SugarDip, over de medicamenteuze behandeling van diabetes gravidarum (insuline vs orale therapie). |
Geen |
|
Dr. B.E. (Bastiaan) de Galan |
Internist, MUMC+, Maastricht (0,6 fte) Hoogleraar interne geneeskunde/diabetologie, UM, Maastricht (0,2 fte) Internist, Radboudumc, Nijmegen (0,2 fte) |
Docent/cursusleider DESG cursus voor aios interne geneeskunde en kindergeneeskunde (betaald; naar MUMC+) Associate editor Diabetologia (betaald; naar MUMC) Bestuurslid Nederlandse Vereniging voor Endocrinologie (NVE; onbetaald) Voozitter accreditatiecommissie NIV (vacatiegelden) Voorzitter Commissie van Uitvoering voor het Accreditatieoverleg (onbetaald) Organisatie nascholingsreeks Diabetes Overleg (betaald, naar MUMC) Organisatie nascholingsreeks Dutch Diabetes Academy (betaald, naar MUMC) Secretaris International Hypoglycaemia Study Group (onbetaald) |
Geen |
Horizon Europe Framework Programme: Hypo-RESOLVE (Hypoglycaemia - redefining solutions for better lives) 2018-2023 (afgerond). Novo Nordisk, Lilly, Medtronic en Abbott betrokken als research partners, projectleider: ja
MELISSA (mobile artificial intelligence solution for diabetes adaptive care) 2022-2026. Novo Nordisk levert insuline, projectleider: ja
REDDIE (Real-world evidence for decisions in diabetes) 2023-2027. Novo Nordisk betrokken als research partner, projectleider: nee
Novo Nordisk: ADREM study (investigator initiated trial naar aanpassing van degludec bij sport bij mensen met type 1 diabetes, unrestricted grant) 2021-2022 (afgerond). |
Geen |
Geen |
|
T.M. (Ties) Obers |
Beleidsadviseur Belangenbehartiging (0,6 FTE) Diabetesvereniging Nederland
Directeur (0,2 FTE) Stichting Knowledge for Children Nederland
Freelance Adviseur Non-Profit (0,2 FTE) Groei voor Goed |
Geen |
Geen |
Geen |
Bescherming van de reputatie/positie van Diabetesvereniging Nederland. Boegbeeldfunctie bij patiëntenorganisatie Diabetesvereniging Nederland. |
Geen |
Betrokken clusterexpertisegroepleden
Tabel 10 Gemelde (neven)functies en belangen betrokken clusterexpertisegroepleden
|
Naam |
Hoofdfunctie |
Nevenwerkzaamheden |
Persoonlijke financiële belangen |
Extern gefinancierd onderzoek |
Intellectuele belangen en reputatie |
Restrictie |
|
Dr. B.E. (Bastiaan) de Galan |
Zie tabel 1 |
|||||
|
Dr. H.W. (Harold) de Valk |
Internist-endocrinoloog UMC Utrecht |
Geen |
Geen |
DARE-trial (multicenter onderzoek) naar het effect van een bihormonale pomp (insuline en glucagon). Op basis van een subsidie van ZonMW en participatie van de maker van de bihormonale pomp (Inreda, gevestigd in Goor 1. ZonMW - Interventie-onderzoek bij type 1 diabetes met een combinatie van insuline en glucagon (Projectleider JA) 2. DPARD - DICA-register diabetes (Projectleider JA) |
Geen |
Geen |
|
Dr. M.G.J. (Martin) Willink |
Eigenaar huisartsenpraktijk Willink |
Bestuurslid Stichting Langerhans, onafhankelijk diabetes onderwijs (betaald) Diabetes Kaderhuisarts , medisch adviseur DM Huisartsenzorg Oude IJssel (betaald) |
Geen |
OMED2 studie. Optimalization of Medication in Elderly with Diabetes 1. ZonMW goed gebruik geneesmiddelen - Ontwikkeling van een deprescribing programma om deprescribing te bevorden van diabetes medicatie (projectleider NEE) |
Geen |
Geen |
Inbreng patiëntenperspectief
Via een enquête op het internet zijn de knelpunten bij diabetespatiënten geïnventariseerd.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerden de clusterleden conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
|
Module |
Uitkomst raming |
Toelichting |
|
Preventie hypoglykemie met sensor bij diabetes mellitus type 2 |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Cluster Diabetes mellitus |
|
|
Uitgangsvraag/modules: UV5 Hoe kunnen hypoglykemieen het beste voorkomen worden bij volwassen patiënten met diabetes mellitus? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 11 december 2024 en 7 maart 2025 |
|
Periode: vanaf 2004 |
Talen: geen restrictie |
|
Literatuurspecialist: Alies Oost |
|
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen:
àIn overleg met de adviseur is (gezien de grote aantallen) besloten om in eerste instantie de SRs te screenen. In een later stadium zal evt. aanvullend naar recente RCTs worden gezocht. àDe sleutelartikelen worden gevonden met deze search, maar doordat er is besloten om in eerste instantie alleen de SRs te screenen vallen de artikelen van Bosi, Heinemann en Van Beers buiten dit resultaat. àOp 7 maart 2025 is een update van de search naar SRs gedaan en is aanvullend naar RCTs gezocht. |
|
|
Te gebruiken voor richtlijntekst: A systematic literature search was performed by a medical information specialist using the following bibliographic databases: Embase.com and Ovid/Medline. Both databases were searched from 2004 to December 11, 2024 for systematic reviews. Systematic searches were completed using a combination of controlled vocabulary/subject headings (e.g., Emtree-terms, MeSH) wherever they were available and natural language keywords. The overall search strategy was derived from three primary search concepts: (1) diabetes mellitus; (2) controlled glucose monitoring (CGM); (3) hypoglycemia. Duplicates were removed using EndNote software. After deduplication a total of 359 records were imported for title/abstract screening. |
|
Zoekopbrengst 11-12-2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
327 |
223 |
359 |
|
Totaal |
|
|
359* |
*in Rayyan
Zoekopbrengst 07-03-2025
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld (ook t.o.v. resultaat 11-12-2024) |
|
SR |
348 |
232 |
19 |
|
RCT |
2103 |
1630 |
2483 |
|
Totaal |
2451 |
1862 |
2502* |
*in Rayyan
Zoekstrategie 11-12-2024
Embase.com
|
No. |
Query |
Results |
|
#1 |
'diabetes mellitus'/exp OR diabete*:ti,ab,kw OR diabetic*:ti,ab,kw OR 'dm 1':ti,ab,kw OR 'dm 2':ti,ab,kw OR t1d*:ti,ab,kw OR t2d*:ti,ab,kw OR dm1:ti,ab,kw OR dm2:ti,ab,kw OR tidm:ti,ab,kw OR tiidm:ti,ab,kw OR 'dm type 1':ti,ab,kw OR 'dm type 2':ti,ab,kw OR 'dm type i':ti,ab,kw OR 'dm type ii':ti,ab,kw OR 'type 1 dm':ti,ab,kw OR 'type 2 dm':ti,ab,kw OR 'type i dm':ti,ab,kw OR 'type ii dm':ti,ab,kw OR iddm:ti,ab,kw OR iddm1:ti,ab,kw OR iddm2:ti,ab,kw OR iddmi:ti,ab,kw OR iddmii:ti,ab,kw |
1629170 |
|
#2 |
'continuous glucose monitoring'/exp OR 'continuous glucose monitoring system'/exp OR cgm:ti,ab,kw OR cgms:ti,ab,kw OR iscgm:ti,ab,kw OR rtcgm:ti,ab,kw OR fgm:ti,ab,kw OR (((continuous OR controlled OR bluetooth OR flash OR 'real time' OR realtime OR 'intermittent* scan*') NEAR/3 glucos* NEAR/3 (monitor* OR meter* OR system*)):ti,ab,kw) OR ((freestyle NEAR/3 (navigator OR libre)):ti,ab,kw) |
23770 |
|
#3 |
'hypoglycemia'/exp OR hypoglycem*:ti,ab,kw OR hypoglycaem*:ti,ab,kw OR 'glycaemic control':ti,ab,kw OR 'glycemic control':ti,ab,kw OR 'glucose control':ti,ab,kw OR hba1c:ti,ab,kw OR ((time NEAR/3 (below OR in OR above) NEAR/3 range):ti,ab,kw) OR tir:ti,ab,kw OR tar:ti,ab,kw OR tbr:ti,ab,kw |
301389 |
|
#4 |
#1 AND #2 AND #3 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab,kw OR child*:ti,ab,kw OR schoolchild*:ti,ab,kw OR infant*:ti,ab,kw OR girl*:ti,ab,kw OR boy*:ti,ab,kw OR teen:ti,ab,kw OR teens:ti,ab,kw OR teenager*:ti,ab,kw OR youth*:ti,ab,kw OR pediatr*:ti,ab,kw OR paediatr*:ti,ab,kw OR puber*:ti,ab,kw) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab,kw OR man:ti,ab,kw OR men:ti,ab,kw OR woman:ti,ab,kw OR women:ti,ab,kw)) AND [2004-2025]/py |
5923 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1085389 |
|
#6 |
#4 AND #5 |
327 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Diabetes Mellitus/ or diabete*.ti,ab,kf. or diabetic*.ti,ab,kf. or iddm.ti,ab,kf. or 'dm 1'.ti,ab,kf. or 'dm 2'.ti,ab,kf. or t1d*.ti,ab,kf. or t2d*.ti,ab,kf. or dm1.ti,ab,kf. or dm2.ti,ab,kf. or TIDM.ti,ab,kf. or TIIDM.ti,ab,kf. or 'dm type 1'.ti,ab,kf. or 'dm type 2'.ti,ab,kf. or 'dm type i'.ti,ab,kf. or 'dm type ii'.ti,ab,kf. or 'type 1 dm'.ti,ab,kf. or 'type 2 dm'.ti,ab,kf. or 'type i dm'.ti,ab,kf. or 'type ii dm'.ti,ab,kf. or iddm.ti,ab,kf. or iddm1.ti,ab,kf. or iddm2.ti,ab,kf. or iddmi.ti,ab,kf. or iddmii.ti,ab,kf. |
916305 |
|
2 |
exp Continuous Glucose Monitoring/ or cgm.ti,ab,kf. or cgms.ti,ab,kf. or iscgm.ti,ab,kf. or rtcgm.ti,ab,kf. or fgm.ti,ab,kf. or ((continuous or controlled or bluetooth or flash or 'real time' or realtime or 'intermittent* scan*') adj3 glucos* adj3 (monitor* or meter* or system*)).ti,ab,kf. or (freestyle adj3 (navigator or libre)).ti,ab,kf. |
12249 |
|
3 |
exp Hypoglycemia/ or hypoglycem*.ti,ab,kf. or hypoglycaem*.ti,ab,kf. or 'glycaemic control'.ti,ab,kf. or 'glycemic control'.ti,ab,kf. or 'glucose control'.ti,ab,kf. or hba1c.ti,ab,kf. or (time adj3 (below or in or above) adj3 range).ti,ab,kf. or tir.ti,ab,kf. or tar.ti,ab,kf. or tbr.ti,ab,kf. |
174643 |
|
4 |
(1 and 2 and 3) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) not ((Adolescent/ or Child/ or Infant/ or adolescen*.ti,ab,kf. or child*.ti,ab,kf. or schoolchild*.ti,ab,kf. or infant*.ti,ab,kf. or girl*.ti,ab,kf. or boy*.ti,ab,kf. or teen.ti,ab,kf. or teens.ti,ab,kf. or teenager*.ti,ab,kf. or youth*.ti,ab,kf. or pediatr*.ti,ab,kf. or paediatr*.ti,ab,kf. or puber*.ti,ab,kf.) not (Adult/ or adult*.ti,ab,kf. or man.ti,ab,kf. or men.ti,ab,kf. or woman.ti,ab,kf. or women.ti,ab,kf.)) |
4825 |
|
5 |
limit 4 to yr="2004 -Current" |
4749 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
795792 |
|
7 |
5 and 6 |
223 |
Zoekstrategie 07-03-2025
Embase.com
|
No. |
Query |
Results |
|
#1 |
'diabetes mellitus'/exp OR diabete*:ti,ab,kw OR diabetic*:ti,ab,kw OR 'dm 1':ti,ab,kw OR 'dm 2':ti,ab,kw OR t1d*:ti,ab,kw OR t2d*:ti,ab,kw OR dm1:ti,ab,kw OR dm2:ti,ab,kw OR tidm:ti,ab,kw OR tiidm:ti,ab,kw OR 'dm type 1':ti,ab,kw OR 'dm type 2':ti,ab,kw OR 'dm type i':ti,ab,kw OR 'dm type ii':ti,ab,kw OR 'type 1 dm':ti,ab,kw OR 'type 2 dm':ti,ab,kw OR 'type i dm':ti,ab,kw OR 'type ii dm':ti,ab,kw OR iddm:ti,ab,kw OR iddm1:ti,ab,kw OR iddm2:ti,ab,kw OR iddmi:ti,ab,kw OR iddmii:ti,ab,kw |
1655640 |
|
#2 |
'continuous glucose monitoring'/exp OR 'continuous glucose monitoring system'/exp OR cgm:ti,ab,kw OR cgms:ti,ab,kw OR iscgm:ti,ab,kw OR rtcgm:ti,ab,kw OR fgm:ti,ab,kw OR (((continuous OR controlled OR bluetooth OR flash OR 'real time' OR realtime OR 'intermittent* scan*') NEAR/3 glucos* NEAR/3 (monitor* OR meter* OR system*)):ti,ab,kw) OR ((freestyle NEAR/3 (navigator OR libre)):ti,ab,kw) |
24524 |
|
#3 |
'hypoglycemia'/exp OR hypoglycem*:ti,ab,kw OR hypoglycaem*:ti,ab,kw OR 'glycaemic control':ti,ab,kw OR 'glycemic control':ti,ab,kw OR 'glucose control':ti,ab,kw OR hba1c:ti,ab,kw OR ((time NEAR/3 (below OR in OR above) NEAR/3 range):ti,ab,kw) OR tir:ti,ab,kw OR tar:ti,ab,kw OR tbr:ti,ab,kw |
306050 |
|
#4 |
#1 AND #2 AND #3 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab,kw OR child*:ti,ab,kw OR schoolchild*:ti,ab,kw OR infant*:ti,ab,kw OR girl*:ti,ab,kw OR boy*:ti,ab,kw OR teen:ti,ab,kw OR teens:ti,ab,kw OR teenager*:ti,ab,kw OR youth*:ti,ab,kw OR pediatr*:ti,ab,kw OR paediatr*:ti,ab,kw OR puber*:ti,ab,kw) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab,kw OR man:ti,ab,kw OR men:ti,ab,kw OR woman:ti,ab,kw OR women:ti,ab,kw)) AND [2004-2025]/py |
6172 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1111969 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4223580 |
|
#7 |
#4 AND #5 |
348 |
|
#8 |
#4 AND #6 NOT #7 |
2103 |
|
#9 |
#7 OR #8 |
2451 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Diabetes Mellitus/ or diabete*.ti,ab,kf. or diabetic*.ti,ab,kf. or iddm.ti,ab,kf. or 'dm 1'.ti,ab,kf. or 'dm 2'.ti,ab,kf. or t1d*.ti,ab,kf. or t2d*.ti,ab,kf. or dm1.ti,ab,kf. or dm2.ti,ab,kf. or TIDM.ti,ab,kf. or TIIDM.ti,ab,kf. or 'dm type 1'.ti,ab,kf. or 'dm type 2'.ti,ab,kf. or 'dm type i'.ti,ab,kf. or 'dm type ii'.ti,ab,kf. or 'type 1 dm'.ti,ab,kf. or 'type 2 dm'.ti,ab,kf. or 'type i dm'.ti,ab,kf. or 'type ii dm'.ti,ab,kf. or iddm.ti,ab,kf. or iddm1.ti,ab,kf. or iddm2.ti,ab,kf. or iddmi.ti,ab,kf. or iddmii.ti,ab,kf. |
928638 |
|
2 |
exp Continuous Glucose Monitoring/ or cgm.ti,ab,kf. or cgms.ti,ab,kf. or iscgm.ti,ab,kf. or rtcgm.ti,ab,kf. or fgm.ti,ab,kf. or ((continuous or controlled or bluetooth or flash or 'real time' or realtime or 'intermittent* scan*') adj3 glucos* adj3 (monitor* or meter* or system*)).ti,ab,kf. or (freestyle adj3 (navigator or libre)).ti,ab,kf. |
12622 |
|
3 |
exp Hypoglycemia/ or hypoglycem*.ti,ab,kf. or hypoglycaem*.ti,ab,kf. or 'glycaemic control'.ti,ab,kf. or 'glycemic control'.ti,ab,kf. or 'glucose control'.ti,ab,kf. or hba1c.ti,ab,kf. or (time adj3 (below or in or above) adj3 range).ti,ab,kf. or tir.ti,ab,kf. or tar.ti,ab,kf. or tbr.ti,ab,kf. |
177183 |
|
4 |
(1 and 2 and 3) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) not ((Adolescent/ or Child/ or Infant/ or adolescen*.ti,ab,kf. or child*.ti,ab,kf. or schoolchild*.ti,ab,kf. or infant*.ti,ab,kf. or girl*.ti,ab,kf. or boy*.ti,ab,kf. or teen.ti,ab,kf. or teens.ti,ab,kf. or teenager*.ti,ab,kf. or youth*.ti,ab,kf. or pediatr*.ti,ab,kf. or paediatr*.ti,ab,kf. or puber*.ti,ab,kf.) not (Adult/ or adult*.ti,ab,kf. or man.ti,ab,kf. or men.ti,ab,kf. or woman.ti,ab,kf. or women.ti,ab,kf.)) |
5005 |
|
5 |
limit 4 to yr="2004 -Current" |
4929 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
814202 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2853313 |
|
8 |
5 and 6 |
232 |
|
9 |
(5 and 7) not 8 |
1630 |
|
10 |
8 or 9 |
1862 |