Leefstijladviezen bij MCI
Uitgangsvraag
Wat is de aanbevolen strategie voor het toepassen van leefstijlinterventies voor patiënten met MCI?
De uitgangsvraag omvat de volgende deelvragen:
1. Wat is de plaats van bewegingsinterventies bij de behandeling van patiënten met MCI?
2. Wat is de plaats van voedingsinterventies bij de behandeling van patiënten met MCI?
3. Wat is de plaats van combineerde voeding- en bewegingsinterventies bij de behandeling van patiënten met MCI?
Aanbeveling
Bewegingsinterventies
Adviseer bewegingsinterventies bij patiënten met MCI conform de gangbare richtlijnen. Er is geen reden om af te zien van de algemene Nederlandse beweegnormen en -adviezen.
Voedingsinterventies
Adviseer voedingsinterventies bij patiënten met MCI, conform de schijf van vijf afhankelijk van de voorkeuren van patiënt. Er is geen reden om af te zien van algemene Nederlandse adviezen van het voedingscentrum.
Gecombineerde leefstijlinterventies (voeding en beweging)
De aanbevelingen omtrent de bewegings- en voedingsinterventies kunnen ook gecombineerd gegeven worden bij patiënten met MCI. Er is nog onvoldoende wetenschappelijk bewijs of deze combinaties een synergistisch effect hebben. Derhalve doet het cluster geen aanbevelingen omtrent het toepassen van gecombineerde leefstijlinterventies.
Overwegingen
1. Bewegingsinterventies
Kwaliteit van bewijs
Er zijn voor deze module over bewegingsinterventies twee systematic reviews (Liu, 2024; Wang, 2024) gevonden, waarin beweeginterventies bij personen met MCI werden vergeleken met een controlegroep zonder beweeginterventies, ten aanzien van cognitief functioneren en kwaliteit van leven.
De overall kwaliteit van bewijs is laag. Dit betekent dat we onzeker zijn over het gevonden geschatte effect van de belangrijke uitkomstmaten cognitief functioneren en kwaliteit van leven. Voor de cruciale uitkomstmaten werden geen resultaten gevonden.
In geen van de twee reviews is, conform de PICO, de RCT van Stuckenschneider (2021) meegenomen (een studie naar multicomponent beweeginterventie bij mensen met MCI, waarbij de beweeginterventie na 1 jaar niet leidde tot verbetering).
Er is afgewaardeerd vanwege:
- Risk of Bias: methodologische beperkingen waaronder ontbreken van de blindering en ontbrekende informatie over de randomisatieprocedure
- Inconsistentie: inconsistentie van de resultaten.
- Imprecisie: onnauwkeurigheid, omdat het betrouwbaarheidsinterval één grens van klinische relevantie overschrijdt.
Balans tussen gewenste en ongewenste effecten
Er zijn voor deze module over bewegingsinterventies twee systematic reviews (Liu, 2024; Wang, 2024) gevonden, waarin beweeginterventies bij personen met MCI werden vergeleken met een controlegroep zonder beweeginterventies, ten aanzien van cognitief functioneren en kwaliteit van leven.
Bij de interpretatie van de resultaten is het van belang om onderscheid te maken tussen statistische significantie en klinische relevantie. Voor enkele vaak gebruikte uitkomstmaten in MCI en milde AD, zoals de ADAS-Cog14 (waar een verschil van 2-4 punten mogelijk klinisch relevant is op een schaal van 0-90) en de CDR-SB (waar een verschil van 1 punt, of 1-2 punten voor MCI en milde AD, als mogelijk klinisch relevant verschil wordt beschouwd), is enige informatie over effectgroottes beschikbaar (Andrews, 2019; Schrag, 2011). Voor andere schalen (e.g. ADCS-ADL-MCI, ADCOMS) welke worden gebruikt door Liu (2024) en Wang (2024) is bij het cluster geen literatuur bekend over klinisch relevante verschillen.
Omdat er onvoldoende bekende afkapwaarden voor mininaal klinisch relevante verschillen zijn en deze per patient anders gewaardeerd kunnen worden, zijn voor deze huidige richtlijnmodule daarom de gangbare standaarden gebruikt (dichotome uitkomstmaten: 0.8 ≥ RR ≥ 1.25, conitue uitkomstmaten: 0.5 SD) gebruikt.
Uit beide studies (Liu, 2024; Wang, 2024) blijkt dat het risico op nadelige effecten door bewegingsinterventies bij personen met MCI zeer laag is en dat er mogelijk een positief netto effect bestaat. Daarnaast geven beide studies aan dat het effect van bewegingsinterventies op zowel cognitief functioneren als kwaliteit van leven mogelijk klinisch relevant is. Hierbij acht het cluster het belangrijk te benadrukken dat de literatuur geen uitspraken doet over het effect van bewegingsinterventies op de progressie van MCI naar dementie.
Daarnaast wordt bewegingsinterventie, los van het mogelijke effect op het cognitief functioneren, aanbevolen vanwege de bredere gezondheidsvoordelen, zoals een verbeterde cardiovasculaire gezondheid, een lagere kans op mobiliteitsproblemen en een positief effect op de algehele fysieke en mentale gezondheid.
Voor een overzicht van de algemene Nederlandse beweegrichtlijnen die adviseren hoeveel beweging nodig is voor een goede lichamelijke en mentale gezondheid, verwijst het cluster naar de Nederlandse beweegrichtlijnen (https://www.gezondheidsraad.nl/documenten/adviezen/2017/08/22/beweegrichtlijnen-2017) en het Kenniscentrum Sport en Bewegen (https://www.kenniscentrumsportenbewegen.nl/beweegrichtlijnen/).
2. Voedingsinterventies
Kwaliteit van bewijs
Er zijn geen studies gevonden naar het effect van voedingsinterventies (Mediterraan, ketogeen of MIND dieet) op zowel de cruciale als belangrijke uitkomstmaten bij mensen met MCI (conform de PICO). Er kan daarom geen uitspraak worden gedaan over de kwaliteit van het bewijs en de bewijskracht.
Het cluster heeft wel oriënterend gekeken naar systematic reviews (n=5, zie Tabel 2) die over voedingsinterventies gaan. Deze studies geven inzicht in hoeverre voedingsinterventies kunnen bijdragen in patiënten met MCI.
De vijf systematic reviews (Devranis, 2023; Price, 2023; Bohnen, 2023; García-Casares, 2021; Gutierrez, 2021) geven aan dat voedingsinterventies veelbelovende leefstijlinterventies kunnen zijn om cognitieve functies bij mensen met MCI te behouden/verbeteren. De effectiviteit van interventies lijkt af te hangen van factoren zoals de aard en naleving van het eetpatroon, en gebruik van specifieke voedingsmiddelen en voedingssupplementen.
Voedinsginterventies (zowel een Mediterraan, ketogeen of MIND dieet) lijken een positief effect te hebben op cognitieve functies, maar hier ligt een kennislacune. Daarnaast is er onvoldoende inzicht op potententiele schadelijke effecten van bijvoorbeeld het ketogeen dieet.
Balans tussen gewenste en ongewenste effecten
Observationele studies suggereren dat voeding cognitieve voordelen kan bieden. Maar systematische reviews van gerandomiseerde trials tonen grotendeels geen significant effect op cognitieve uitkomsten, met inconsistenties en beperkingen (Yassine, 2022). Door unieke uitdagingen in voedingsonderzoek zijn high-quality trials beperkt. Gezien deze unieke uitdagingen is het onduidelijk of de effecten van voeding op het cognitief functioneren onafhankelijk zijn of vertekend zijn door andere factoren zoals bijvoorbeeld beweging. Epidemiologische studies wijzen echter op onafhankelijke effecten van voeding, los van fysieke activiteit (Yassine, 2022; Scarmeas, 2009).
Voor een overzicht van de reguliere voedingsadviezen die adviseren welke voeding geadviseerd wordt voor een goede lichamelijke en mentale gezondheid alsmede een toelichting op het mediterraan, mind of ketogeen dieet, verwijst het cluster naar het Voedingscentrum (www.voedingscentrum.nl).
3. Gecombineerde voeding- en bewegingsinterventies
Kwaliteit van bewijs
Er zijn geen studies gevonden naar het effect van gecombineerde voeding- en bewegingsinterventies op zowel de cruciale als belangrijke uitkomstmaten bij mensen met MCI (conform de PICO). Er kan daarom geen uitspraak worden gedaan over de kwaliteit van het bewijs en de bewijskracht.
Het cluster heeft wel oriënterend gekeken naar systematic reviews (n=4, zie Tabel 3) die over gecombineerde voeding- en bewegingsinterventies gaan. Deze studies geven inzicht in hoeverre gecombineerde interventies bijdragen aan de behandeling van patiënten met mild cognitive impairment.
Multicomponent- en gecombineerde interventies (beweging en voeding) studies ontbreken. De vier systematic reviews (Ding, 2023; Xue, 2023; Shao, 2022; Liu, 2021) impliceren dat bewegingsinterventies veelbelovende leefstijlinterventies vormen om cognitieve functies bij mensen met MCI te bevorderen. De effectiviteit van interventies lijkt af te hangen van factoren zoals frequentie, intensiteit, duur, setting en type. Er zijn aanwijzingen dat een gepersonaliseerde aanpak bij de inzet van gecombineerde leefstijlinterventies een positief effect kan hebben op het verbeteren van cognitief functioneren. Een gepersonaliseerde aanpak houdt in dat de begeleiding wordt verzorgd door een leefstijlcoach en een verpleegkundige, waarbij persoonlijke doelen worden opgesteld en gevolgd. Deze aanpak zorgt voor een meer op maat gemaakte ondersteuning die beter aansluit bij de individuele behoeften van de patiënt (Yaffe, 2023). Multicomponent- en gecombineerde interventies (beweging en voeding) lijken een positief effect te hebben op cognitieve functies, maar hier ligt een kennislacune.
Balans tussen gewenste en ongewenste effecten
Het is onduidelijk of er een synergistisch effect is van gecombineerde voeding- en bewegingsinterventies. Derhalve doet het cluster geen aanbevelingen rondom het toepassen van deze gecombineerde voeding- en bewegingsinterventies.
Studies naar het effect van gecombineerde leefstijlinterventies lopen op dit ogenblik. Deze studies richten zich op mensen zonder cognitieve stoornissen maar met modificeerbare risicofactoren voor dementie, en zijn gebaseerd op de Finger trial. Wereldwijd lopen meerdere studies. In Nederland is dit de FINGER-NL studie, die beweging, voeding, mindfullness-stress, bloeddruk- en cholesterolverlaging (indien verhoogd), slaap, en cognitieve training combineert (Deckers, 2024). Drie belangrijke afgeronde gecombineerde leefstijlinterventie studies zijn benoemd in Tabel 4 (Yassine, 2022).
Tabel 2. Voedingsinterventies: Overzicht van fulltext beoordeelde studies, die niet aan de PICO voldoen (in Engels)
|
Comparator |
Search period (databases) |
Outcomes |
Conclusion authors |
Comment PICO |
|||||
|
To summarize the evidence of three dietary patterns (i.e. the Mediterranean diet, the ketogenic diet, the MIND diet) for the prevention of cognitive decline. |
Mediterranean (n=11 RCTs), ketogenic (n=7 RCTs), MIND (n=1 RCT) |
Not specified (various) |
Until January 2022 (PubMed, ScienceDirect, Web of Science) |
Cognitive outcomes (e.g. MMSE) |
All three dietary interventions have been shown to slow the rate of cognitive decline in the included studies.
|
Wrong P (no patients with MCI) |
|||
|
Adults aged 18 years or older with a diagnosis of PD, AD or MCI |
Not specified (various) |
N.R. (PubMed, Scopus, Google Scholar) |
|
Ketogenic therapies have promise in PD, AD, and MCI for symptom improvement although larger studies are needed to support their implementation in clinical practice. |
Wrong P, wrong comparison (only 5/15 studies in patients with MCI; but with wrong comparison: Modified Adkins diet, low vs high carbohydrate diet, ketogene drank vs sunflower oil, MCT vs canola oil) |
||||
|
|
|
Not specified (various) |
N.R. (from 2005 in Pubmed) |
|
Ketogenic interventions are probably effective for cognitive improvement in patients with mild-to-moderate AD who are APOε4- and in patients with MCI.
Taking all considerations into account, we recognize the potential for a multidimensional model geared toward optimizing the effectiveness of ketogenic interventions as dictated by clinical setting. |
Wrong P (too broad), unclear selection criteria, no search strategy, no pooled data of outcomes. |
|||
|
To determine the effects of a higher adherence to Mediterranean on MCI and AD. |
Non-AD participants but with AD risk
|
Not specified (various) |
Until June of 2021 (PubMed, Scopus and The Cochrane Library Plus)
|
|
Higher adherence to Mediterranean diet reduce the risk to develop MCI and AD.
|
Wrong studies (only association studies included, MD adherence and MCI / AD risk) |
|||
|
To evaluate the impact of dietary counselling interventions, food-based
|
Not specified (various) |
January 2018-July 2021 (Pubmed)
|
Cognitive functioning
|
|
Wrong P; wrong comparison (14/61 studies in patients with MSI, but with wrong comparisons: wel/geen olive oil, cheeses, vitamin D, probiotics, vish oil, foliumzuur, aminozuren) |
Tabel 3. Gecombineerde voeding- en bewegingsinterventies: Overzicht van fulltext beoordeelde studies, die niet aan de PICO voldoen (in Engels)
Tabel 4. Samenvatting van drie belangrijke gecombineerde leefstijlinterventies ter preventie van dementie, gebasseerd op Yassin (2022) (in Engels)
|
|
PREDIVA |
FINGER |
MAPT |
|
Country |
The Netherlands |
Finland |
France |
|
Participant age (years) |
70–78 |
60–77 |
≥70 |
|
Sample size |
3526 |
1260 |
1680 |
|
Intervention |
1890 in the multidomain cardiovascular intervention; 1636 in intervention; 629 in the control group (usual care) |
631 in the multidomain group (general health advice)
|
420 in the multi-domain intervention (physical activity, cognitive training, and nutritional advice) with placebo; 417 in the multi-domain intervention with omega-3 polyunsaturated fatty acids; 423 in the omega-3 polyunsaturated fatty acid alone group; 420 in the placebo alone group |
|
Original duration (years) |
6-8 |
2 |
3 |
|
Outcome |
Clinically assessed; dementia incidence; disability score |
Neuropsychological test battery Z score
|
Z score combining 4 cognitive tests; disability score; frailty score |
|
Authors conclusion |
A nurse-led multidomain intervention showed no dementia reduction in older adults, possibly due to low baseline risks and high usual care standards; future studies should target selected groups. |
This large RCT suggests multidomain interventions may improve or maintain cognitive function in at-risk elderly individuals from the general population. |
Neither multidomain intervention nor polyunsaturated fatty acids significantly impacted cognitive decline over three years in elderly individuals with memory complaints; optimal strategies and populations need identification. |
|
Comments (Yassine, 2022) |
The study featured a large, representative population with average dementia risk, long duration, low-intensity intervention, and clinically relevant but insensitive outcomes. |
The study had a population with high dementia risk, a small sample size, and a short duration; the outcome was sensitive, and the intervention intense.
|
The study had a large sample size, a long duration, and a heterogeneous population (higher reserve, low vascular and low dementia risk); the outcomes were sensitive; the nutrition intervention could have been of better content and intensity.
|
|
Reference |
Moll van Charante EP, et al. Effectiveness of a 6-year multidomain vascular care intervention to prevent dementia (preDIVA): a cluster-randomised controlled trial. Lancet. 2016 Aug 20;388(10046):797-805. doi: 10.1016/S0140-6736(16)30950-3) |
Ngandu T, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015 Jun 6;385(9984):2255-63. doi: 10.1016/S0140-6736(15)60461-5)
|
Andrieu S, et al. MAPT Study Group. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): a randomised, placebo-controlled trial. Lancet Neurol. 2017 May;16(5):377-389. doi: 10.1016/S1474-4422(17)30040-6) |
|
FINGER=Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability. MAPT=Multi-domain Alzheimer's Prevention Trial. PREDIVA=Prevention of Dementia by Intensive Vascular care. |
|||
Algemeen: 1. Bewegingsinterventies; 2. Voedingsinterventies; 3. Gecombineerde voeding- en bewegingsinterventies
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Leefstijlinterventies, waaronder beweeginterventies en voedingsinterventies, hebben een bewezen positief effect op de algehele gezondheid en het welzijn van patiënten (Gezondheidsraad, 2017; Gezondheidsraad, 2015; beweegrichtlijnen; voedingsadviezen). Er zijn daarnaast aanwijzingen dat deze interventies een klinisch relevant effect kunnen hebben op cognitief functioneren en kwaliteit van leven bij mensen met MCI.
Beweeg- en voedingsinterventies kennen een laag risico op nadelige effecten en kunnen laagdrempelig worden ingezet. Een belangrijke uitdaging is echter dat het realiseren van een duurzame leefstijlverandering complex is. Gedragsverandering vraagt om langdurige inzet en motivatie van de patiënt, waarbij steun vanuit de sociale omgeving een cruciale rol speelt. Het betrekken van naasten en zorgverleners kan bijdragen aan het succes van leefstijlinterventies.
Samenvattend, acht het cluster de gewenste effecten op patiëntrelevante uitkomstmaten mogelijk aanwezig, de literatuur laat immers geen sterke consistente resultaten zien. De ongewenste effecten op patiëntrelevante uitkomstmaten zijn echter verwaarloosbaar en wegen niet tegen de mogelijke voordelen op.
Kostenaspecten
Beweeg- en voedingsinterventies kunnen bijdragen aan een vermindering van medische en ziekenhuiskosten op de lange termijn door het verbeteren van de algehele gezondheid van de patiënt. Er ligt een kennislacune of de uiteindelijke interventie kosteneffectief zal zijn.
Gezondheidsgelijkheid
Bij leefstijlveranderingen speelt de sociale omgeving een cruciale rol. Steun van familie, vrienden en zorgverleners kan het succes van beweeg- en voedingsinterventies aanzienlijk vergroten. Echter, niet alle patiënten hebben dezelfde mate van ondersteuning, wat kan leiden tot ongelijkheid in de effectiviteit van deze interventies.
Daarnaast kan de sociaaleconomische status een belangrijke belemmering vormen. Mensen met een lagere sociaaleconomische status hebben mogelijk minder toegang tot sportfaciliteiten, gezondheidsvoorlichting en ondersteuning bij gedragsverandering. Bovendien zijn de kosten van gezonde voeding vaak hoger dan die van minder gezonde alternatieven, wat kan leiden tot financiële barrières voor patiënten met beperkte middelen.
Bij de implementatie van leefstijlinterventies is het daarom van belang om rekening te houden met deze ongelijkheden en te streven naar toegankelijke en betaalbare opties voor alle patiënten.
Aanvaardbaarheid
Een belangrijk aandachtspunt bij de implementatie van gecombineerde leefstijlinterventies is de preventieparadox (Martin, 2025). Dit houdt in dat interventies gericht op het verbeteren van de gezondheid op populatieniveau mogelijk niet direct merkbare voordelen opleveren voor individuen die al in goede gezondheid verkeren, terwijl ze juist het grootste effect hebben voor de risicogroepen. Dit kan leiden tot een lage aanvaardbaarheid van de interventie bij gezonde personen, aangezien zij het gevoel kunnen hebben dat de interventie voor hen niet noodzakelijk is. Het is daarom van belang om de voordelen van dergelijke interventies goed te communiceren en te benadrukken, ook voor gezonde individuen, door te wijzen op de lange-termijn voordelen van preventie en het behoud van gezondheid. Wanneer de voordelen van leefstijlinterventies duidelijk zijn, kunnen patiënten hier zelf actief mee aan de slag gaan en controle nemen over hun eigen gezondheid. Dit kan de motivatie vergroten en bijdragen aan een gevoel van eigen regie.
Tegelijkertijd kunnen sommige patiënten moeite hebben met het aanpassen van hun leefstijl door culturele overtuigingen, persoonlijke voorkeuren of een gebrek aan interesse. Om de aanvaardbaarheid te vergroten, is het belangrijk om interventies zoveel mogelijk op maat aan te bieden. Door rekening te houden met individuele behoeften en voorkeuren kan de kans op succes toenemen en wordt beter aangesloten bij de leefwereld van de patiënt.
Een belangrijke kanttekening bij de preventieparadox is dat de verantwoordelijkheid voor preventie bij gezonde personen vaak op populatieniveau ligt via overheidsmaatregelen of interventies in de publieke gezondheidszorg. Artsen en zorgverleners zien voornamelijk individuele patiënten, wat betekent dat zij minder brede impact kunnen maken bij gezonde mensen, terwijl de kosten van individuele interventies relatief hoog zijn. Interventies op populatieniveau, zoals voorlichting of algemene leefstijlprogramma’s, het subsidiëren van gezonde voeding door hogere belasting op ongezonde voeding, een strenger beleid gericht op terugdringen van roken, etc. kunnen daarentegen een veel groter effect bereiken tegen lagere kosten. Dit benadrukt het belang van een geïntegreerde benadering van preventie, waarbij zowel individuele zorg als bredere publieke gezondheidsmaatregelen elkaar aanvullen (Martin, 2025).
Ethische aanvaardbaarheid
De interventie lijkt zeker aanvaardbaar voor de betrokkenen. Het cluster voorziet geen ethische bezwaren.
Duurzaamheid
Bij de beweeg- en voedingsinterventies spelen duurzaamheidsaspecten naar verwachting geen grote rol.
Haalbaarheid
Het realiseren van een duurzame leefstijlverandering is complex. Gedragsverandering vraagt om langdurige inzet en motivatie van de patiënt, waarbij steun vanuit de sociale omgeving een cruciale rol speelt. Het betrekken van naasten en zorgverleners kan bijdragen aan het succes van leefstijlinterventies.
Leefstijlinterventies kunnen flexibel worden aangepast aan de omstandigheden en behoeften van patiënten. Door interventies op maat aan te bieden, kunnen ze beter aansluiten bij de mogelijkheden en beperkingen van individuele patiënten. Dit vergroot de haalbaarheid en maakt het eenvoudiger om veranderingen in het dagelijks leven door te voeren.
Rationale van aanbeveling Bewegingsinterventies: weging van argumenten voor en tegen de interventies
Bewegen volgens de algemene Nederlandse beweegnormen wordt aanbevolen bij patiënten met MCI. Het bewijs in de literatuur is beperkt, maar de bijwerkingen en risico’s van de interventie zijn minimaal. Om de aanbevelingen concreter te maken, verwijst het cluster naar algemene Nederlandse beweegnormen en -adviezen.
(https://www.gezondheidsraad.nl/documenten/adviezen/2017/08/22/beweegrichtlijnen-2017) en het Kenniscentrum Sport en Bewegen https://www.kenniscentrumsportenbewegen.nl/beweegrichtlijnen/) .
Eindoordeel: Zwakke aanbeveling voor.
Rationale van aanbeveling Voedingsinterventies: weging van argumenten voor en tegen de interventies
Goede voeding volgens de algemene voedingsadviezen van het voedingscentrum wordt aanbevolen bij patiënten met MCI. Het bewijs in de literatuur is beperkt, maar de bijwerkingen en risico’s van de interventie zijn minimaal. Om de aanbevelingen concreter te maken, verwijst het cluster algemene Nederlandse voedingsadviezen (www.voedingscentrum.nl).
Eindoordeel: Zwakke aanbeveling voor.
Rationale van aanbeveling Gecombineerde leefstijlinterventies (voeding en beweging: weging van argumenten voor en tegen de interventies
Er zijn geen studies gevonden naar het effect van gecombineerde voeding- en bewegingsinterventies op zowel de cruciale als belangrijke uitkomstmaten bij mensen met MCI. Studies naar het effect van gecombineerde leefstijlinterventies lopen op dit ogenblik. Hoewel het aannemelijk is dat gecombineerde voeding- en bewegingsinterventies bijdragen aan de goede gezondheid van patiënten met MCI, en dat er een synergistisch effect zal zijn van gecombineerde voeding- en bewegingsinterventies, ontbreekt er op dit moment voldoende wetenschappelijk bewijs waarin dit is aangetoond. Derhalve doet het cluster geen aanbevelingen rondom het toepassen van deze gecombineerde voeding- en bewegingsinterventies.
Eindoordeel: Zwakke aanbeveling voor.
Onderbouwing
Achtergrond
Various studies suggest that a substantial proportion (ranging from 35% to 49%) of all dementia patients could be explained by potentially modifiable risk factors (Ashby-Mitchell, 2017; Livingston, 2024). Frequently reported risk factors are obesity, hypertension, physical inactivity, smoking, and diabetes.
Research has been conducted to assess whether, in patients with mild cognitive impairment (MCI), lifestyle interventions can indeed potentially reduce progression to dementia. Several studies show some (small) positive results or no difference for various non-pharmacological interventions, including certain diets and physical activity (Yassine, 2022; Liu, 2024; Stuckenschneider, 2021).
In current practice, the use and content of lifestyle interventions in patients with MCI varies across hospitals. It is unclear to what extent, what, and how lifestyle interventions should be adviced (e.g. which intervention, which frequency). This module evaluates the role of lifestyle interventions after diagnosis of MCI. The cluster focuses on three types of lifestyle interventions: nutrition-, exercise-, and combined interventions.
Conclusies / Summary of Findings
Summary of Findings
1. Summary of Findings table: Exercise interventions in patients with MCI
Population: People with MCI
Intervention: Exercise interventions
Comparator: No exercise interventions
|
Outcome |
Study results and measurements |
Absolute effect estimates |
Certainty of the Evidence (Quality of evidence) |
Summary |
||
|
Exercise interventions |
No exercise interventions |
|||||
|
Progression to dementia (critical) |
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of exercise interventions on progression to dementia when compared with no exercise interventions in patients with MCI. |
||
|
Time to progression to dementia (critical) |
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of exercise interventions on time to progression to dementia when compared with no exercise interventions in patients with MCI. |
||
|
Cognitive functioning (important) |
Measured by MoCA, SMMSE and ADAS-Cog. Based on data from 1509 participants in 24 studies. |
(Mean) - |
(Mean) - |
Low Due to serious risk of bias*, Due to serious inconsistency1 |
Exercise interventions may be related to higer levels of cognitive functioning at follow-up when compared with no exercise interventions in patients with MCI. (Liu, 2024; Wang, 2024) |
|
|
Difference: SMD 1.06 higher (CI 95% 0.72 fewer – 1.41 higher) |
||||||
|
Quality of life (important)
|
Measured by SF-12, QOL-AD-C and SF-36. Based on data from 289 participants in 3 studies. |
(Mean) - |
(Mean) - |
Low Due to serious risk of bias*, Due to serious imprecision2 |
Exercise interventions may improve quality of life when compared with no exercise interventions in patients with MCI. (Liu, 2024; Wang, 2024) |
|
|
Difference: SMD 0.55 higher (CI 95% 0.12 fewer – 0.99 higher) |
||||||
|
Patient satisfaction (important) |
- |
- |
No GRADE (no evidence was found) |
No evidence was found regarding the effect of exercise interventions on patient satisfaction when compared with no exercise interventions in patients with MCI. |
||
|
1 Risk of Bias: serious. Due to lack of blinding, missing information about the randomization procedure. Inconsistency: serious. Due to conflicting results. 2 Risk of Bias: serious. Due to lack of blinding, missing information about the randomization procedure. Imprecision: serious. Due to overlap of confidence interval with border of clinical relevance. *For further details, see risk of bias table in the appendix |
||||||
2. Summary of Findings table: Nutrition interventions in patients with MCI; 3. Summary of Findings table: Combined interventions in patients with MCI
No results found conform PICO.
Samenvatting literatuur
1. Subquestion 1 ‘exercise interventions’ - Description of studies
Two systematic reviews were included in analysis of the literature (Liu, 2024; Wang, 2024). Important study characteristics are summarized in Table 1. The assessment of the risk of bias is summarized in the risk of bias tables (under the tab ‘Evidence tabellen’).
Liu (2024) aimed to assess the effect of exercise intervention for elderly with MCI and provide the most effective exercise intervention to slow down cognitive decline. Four international databases (PubMed, EMBASE, Web of Science, Cochrane Library) and four Chinese databases (Chinese National Knowledge Infrastructure, VIP database and Wanfang database) were searched until 25 September 2022. The Cochrane risk of bias tool for assessing risk of bias in randomized trials was used for quality assessment. The study included 20 RCTs with a total of 1393 subjects with MCI, including 733 in the experimental group and 660 in the control group. Studies included in Liu that assessed the effectiveness of any traditional Thai or Chinese exercise (n=4) were excluded. The median intervention period for all studies was 16 weeks. Outcome measure was cognitive function, measured with the Montreal Cognitive Scale (MoCA) (no specific MCID reported).
Wang (2024) aimed to investigate the effects of multicomponent exercise on global cognition in people with MCI. Six electronic databases (PubMed, Medline, EMBASE, Web of Science, Cochrane Library, and CINAHL) were systematically searched from inception to 1 January 2023. The Cochrane collaborative bias assessment tool was used to assess risk of bias. The study included 20 RCTs with a total of 1155 participants, including 580 in the intervention group and 575 in the control group. Eventually, 8 out of 20 RCTs were included in the current analysis because of various reasons: 5 studies overlapped with Liu (2024), 5 studies did not have a control group as specified in the PICO (low resistance exercise [n=2], pharmacological treatment [n=2], free sports activity [n=1]), one study did not report on any of the outcomes as specified in the PICO, and one study was a manuscript). Outcome measure was cognitive function, measured with the MoCA, Mini-Mental State Examination (MMSE), or Cognitive section of the Alzheimer's Disease Assessment Scale (ADAS-Cog) (no specific MCID reported).
Table 1. Characteristics of included studies in Liu (2024) and Wang (2024)
2. Subquestion 2 ‘nutrition interventions’ - Description of studies; 3. Subquestion 3 ‘combined interventions’ - Description of studies
No studies were found conform the PICO and could be included.
1. Subquestion 1 ‘exercise interventions’ - Results
1.1. Cognitive functioning
All studies included in Liu (2024) and Wang (2024) reported on the outcome measure cognitive functioning assessed by using the MoCA (range: 0-30), standardized MMSE (SMMSE) (range: 0-30) or ADAS-Cog (range: 0-70). Higher MoCA and SMMSE scores represent greater cognitive function, whereas higher ADAS-Cog scores indicate greater cognitive impairment. ADAS-Cog scores were converted before pooling the data.
The pooled data show a standardized mean difference (SMD) of 1.06 (95%CI 0.72 to 1.41) in favour of exercise interventions (Figure 1). This difference is considered clinically relevant (assuming the threshold of 0.5 SD). SMD was used due to the lack of uniform diagnostic criteria for MCI, inconsistent measurement time points of the outcome, and the different instruments to assess cognitive function.
Figure 1. The effect of exercise interventions on cognitive functioning
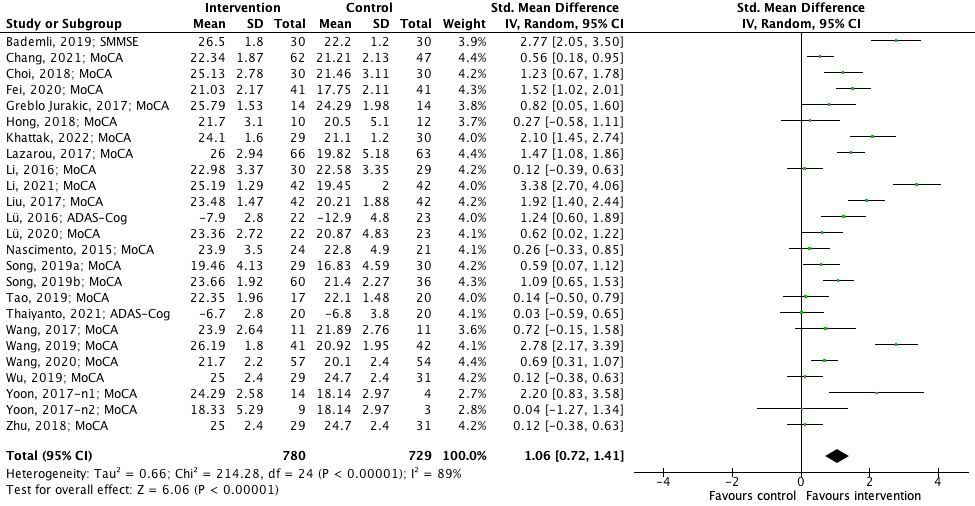
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval
1.2. Quality of life
Two studies included in Liu (2024) as well as Wang (2024) and one study included only in Wang (2024) reported on the outcome measure quality of life. Chang (2021) reported on quality of life assessed by using the Short-Form 12 Health Survey (SF-12) (range: 0-100), in which higher scores indicate better quality of life. Song (2019b) reported on quality of life assessed by using the Quality of Life-Alzheimer’s disease (Chinese version, QOL-AD-C) (range: 13-52). Higher scores on the QOL-AD-C indicate better quality of life. Zhu (2018) assessed quality of life by the Short-Form 36 Health Survey (SF-36) (range: 0-149), in which higher scores reflect better quality of life.
The pooled data show a SMD of 0.55 (95%CI 0.12 to 0.99) in favour of exercise interventions (Figure 2). This difference is considered clinically relevant (assuming the threshold of 0.5 SD). SMD was used due to the lack of uniform diagnostic criteria for MCI, inconsistent measurement time points of the outcome, and the usage of different instruments to assess quality of life.
Figure 2. The effect of exercise interventions on quality of life

Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: confidence interval
1.3. Progression to dementia, 1.4. Time to progression to dementia, 1.5. Patient satisfaction
None of the studies included in Liu (2024) or Wang (2024) reported on the outcome measures progression to dementia, time to progression to dementia, and patient satisfaction.
2. Subquestion 2 ‘nutrition interventions’ – Results; 3. Subquestion 3 ‘combined interventions’ – Results
No studies were found.
Zoeken en selecteren
A systematic review of the literature was performed to answer the following question(s):
What is the effectiveness of lifestyle interventions for people with mild cognitive impairment (MCI)?
Table PICO
| Patients | People with MCI |
|
Intervention 1 Intervention 2 Intervention 3 |
= Nutritional interventions (Mediterranean diet, MIND diet, ketogenic diet) = Physical activity interventions (no Tai Chi, exergaming or traditional Chinese medicine-based exercise) = Combination of both nutritional and physical activity interventions |
| Control | No lifestyle recommendations |
| Outcomes | Progression to dementia, time to progression to dementia, cognitive functioning/decline, patient satisfaction, quality of life |
| Other selection citeria | Study design: Systematic reviews
Minimal follow-up: 2 years Size study population: ≥ 10 patients per arm Period: from 2010 |
Relevant outcome measures
The guideline panel considered progression to dementia and time to progression to dementia as critical outcome measures for decision making; and cognitive functioning/decline, patient satisfaction, quality of life as an important outcome measures for decision making.
A priori, the guideline panel did not define the outcome measures listed above but used the definitions used in the studies.
For all outcome measures the guideline panel defined a 25% difference for dichotomous outcomes (0.8 ≥ RR ≥ 1.25) and 0.5 SD for continuous outcomes as a minimal clinically (patient) important difference:
- Cognitive functioning/decline: RR ≤0.8 or ≥1.25 (dichotomous); 0.5 SD (continuous)
- Time to progression to dementia: RR ≤0.8 or ≥1.25 (dichotomous); 0.5 SD (continuous)
- Progression to dementia: RR ≤0.8 or ≥1.25 (dichotomous); 0.5 SD (continuous)
- Patient satisfaction: RR ≤0.8 or ≥1.25 (dichotomous); 0.5 SD (continuous)
- Quality of life: RR ≤0.8 or ≥1.25 (dichotomous); 0.5 SD (continuous)
If studies use different rating instruments (e.g. Cognitive functioning could be measures with the valided scales MMSE, MOCA, or ADAS-Cog) to measure the same outcome measure, then the standardized mean difference (SMD) is calculated. For SMDs, results were clinically relevant if they were smaller than -0.5 or higher than 0.5. Based on Cohens D, values of 0.2-0.5 are considered small, values of 0.5-0.8 are considered medium, and values >0.8 are considered large.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2010 until 21 August 2024. The detailed search strategy is listed under the tab ‘Literature search strategy’. The systematic literature search resulted in 884 hits. Studies were selected based on the following criteria:
- Systematic reviews in which searches were performed in at least two databases, with a detailed search strategy, risk of bias assessment and results of individual studies available, randomized controlled trials or (observational) comparative studies.
- Studies published between 2010-2024.
- Full-text English or Dutch language publication and
- Studies according to the PICO.
Initially, 51 studies were selected based on title and abstract screening. After reading the full text, 49 studies were excluded (see the exclusion table under the tab ‘Evidence tabellen’). For subquestion 1 ‘exercise interventions’ two systematic reviews were included (Liu, 2024; Wang, 2024). For subquestion 2 ‘nutrition interventions’ and subquestion 3 ‘combined interventions’ no studies were included. For the latter two subquestions an overview in the ‘overwegingen’ is provided of the studies that were found in the search but were not according to the PICO (subquestion 2: n=5; subquestion 3: n=4).
Referenties
- Andrews JS, Desai U, Kirson NY, Zichlin ML, Ball DE, Matthews BR. Disease severity and minimal clinically important differences in clinical outcome assessments for Alzheimer's disease clinical trials. Alzheimers Dement (N Y). 2019 Aug 2;5:354-363. doi: 10.1016/j.trci.2019.06.005. PMID: 31417957; PMCID: PMC6690415.
- Ashby-Mitchell K, Burns R, Shaw J, Anstey KJ. Proportion of dementia in Australia explained by common modifiable risk factors. Alzheimers Res Ther. 2017 Feb 17;9(1):11. doi: 10.1186/s13195-017-0238-x. PMID: 28212674; PMCID: PMC5316209.
- Bohnen JLB, Albin RL, Bohnen NI. Ketogenic interventions in mild cognitive impairment, Alzheimer's disease, and Parkinson's disease: A systematic review and critical appraisal. Front Neurol. 2023 Feb 9;14:1123290. doi: 10.3389/fneur.2023.1123290. PMID: 36846143; PMCID: PMC9947355.
- Deckers K, Zwan MD, Soons LM, Waterink L, Beers S, van Houdt S, Stiensma B, Kwant JZ, Wimmers SCPM, Heutz RAM, Claassen JAHR, Oosterman JM, de Heus RAA, van de Rest O, Vermeiren Y, Voshaar RCO, Smidt N, Broersen LM, Sikkes SAM, Aarts E; MOCIA consortium; FINGER-NL consortium; Köhler S, van der Flier WM. A multidomain lifestyle intervention to maintain optimal cognitive functioning in Dutch older adults-study design and baseline characteristics of the FINGER-NL randomized controlled trial. Alzheimers Res Ther. 2024 Jun 13;16(1):126. doi: 10.1186/s13195-024-01495-8. PMID: 38872204; PMCID: PMC11170777.
- Devranis P, Vassilopoulou Ε, Tsironis V, Sotiriadis PM, Chourdakis M, Aivaliotis M, Tsolaki M. Mediterranean Diet, Ketogenic Diet or MIND Diet for Aging Populations with Cognitive Decline: A Systematic Review. Life (Basel). 2023 Jan 6;13(1):173. doi: 10.3390/life13010173. PMID: 36676122; PMCID: PMC9866105.
- Ding Z, Leung PY, Lee TL, Chan AS. Effectiveness of lifestyle medicine on cognitive functions in mild cognitive impairments and dementia: A systematic review on randomized controlled trials. Ageing Res Rev. 2023 Apr;86:101886. doi: 10.1016/j.arr.2023.101886. Epub 2023 Feb 18. PMID: 36806378.
- García-Casares N, Gallego Fuentes P, Barbancho MÁ, López-Gigosos R, García-Rodríguez A, Gutiérrez-Bedmar M. Alzheimer's Disease, Mild Cognitive Impairment and Mediterranean Diet. A Systematic Review and Dose-Response Meta-Analysis. J Clin Med. 2021 Oct 10;10(20):4642. doi: 10.3390/jcm10204642. PMID: 34682764; PMCID: PMC8537524.
- Gezondheidsraad, 2017. Beweegrichtlijnen 2017. Gezondheidsraad. Nr. 2017/08. Geraadpleegd: 13 februari 2025. Link: https://www.gezondheidsraad.nl/documenten/adviezen/2017/08/22/beweegrichtlijnen-2017
- Gezondheidsraad, 2015. Richtlijnen goede voeding 2015. Gezondheidsraad. Nr. 2015/24, Den Haag, 4 november 2015. Geraadpleegd: 13 februari 2025. Link: https://www.gezondheidsraad.nl/documenten/adviezen/2015/11/04/richtlijnen-goede-voeding-2015.
- Gutierrez L, Folch A, Rojas M, Cantero JL, Atienza M, Folch J, Camins A, Ruiz A, Papandreou C, Bulló M. Effects of Nutrition on Cognitive Function in Adults with or without Cognitive Impairment: A Systematic Review of Randomized Controlled Clinical Trials. Nutrients. 2021 Oct 22;13(11):3728. doi: 10.3390/nu13113728. PMID: 34835984; PMCID: PMC8621754.
- Liu T, Li N, Hou Z, Liu L, Gao L, Wang L, Tan J. Nutrition and exercise interventions could ameliorate age-related cognitive decline: a meta-analysis of randomized controlled trials. Aging Clin Exp Res. 2021 Jul;33(7):1799-1809. doi: 10.1007/s40520-020-01730-w. Epub 2020 Oct 14. PMID: 33052590.
- Liu X, Liu L, Liu C. Summary of the effect of an exercise intervention on elderly with mild cognitive impairment: A systematic review and meta-analysis. Medicine (Baltimore). 2024 Jun 14;103(24):e38025. doi: 10.1097/MD.0000000000038025. PMID: 38875404; PMCID: PMC11175880.
- Livingston G, Huntley J, Liu KY, Costafreda SG, Selbæk G, Alladi S, Ames D, Banerjee S, Burns A, Brayne C, Fox NC, Ferri CP, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Nakasujja N, Rockwood K, Samus Q, Shirai K, Singh-Manoux A, Schneider LS, Walsh S, Yao Y, Sommerlad A, Mukadam N. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet. 2024 Aug 10;404(10452):572-628. doi: 10.1016/S0140-6736(24)01296-0. Epub 2024 Jul 31. PMID: 39096926.
- Martin SA, Johansson M, Heath I, Lehman R, Korownyk C. Sacrificing patient care for prevention: distortion of the role of general practice. BMJ. 2025 Jan 21;388:e080811. doi: 10.1136/bmj-2024-080811. PMID: 39837625.
- Price S, Ruppar TM. Ketogenic therapies in Parkinson's disease, Alzheimer's disease, and mild cognitive impairment: An integrative review. Appl Nurs Res. 2023 Dec;74:151745. doi: 10.1016/j.apnr.2023.151745. Epub 2023 Oct 28. PMID: 38007248.
- Scarmeas N, Luchsinger JA, Schupf N, Brickman AM, Cosentino S, Tang MX, Stern Y. Physical activity, diet, and risk of Alzheimer disease. JAMA. 2009 Aug 12;302(6):627-37. doi: 10.1001/jama.2009.1144. PMID: 19671904; PMCID: PMC2765045.
- Schrag A, Schott JM; Alzheimer's Disease Neuroimaging Initiative. What is the clinically relevant change on the ADAS-Cog? J Neurol Neurosurg Psychiatry. 2012 Feb;83(2):171-3. doi: 10.1136/jnnp-2011-300881. Epub 2011 Oct 21. PMID: 22019547.
- Shao Z, Hu M, Zhang D, Zeng X, Shu X, Wu X, Kwok TCY, Feng H. Dose-response relationship in non-pharmacological interventions for individuals with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. J Clin Nurs. 2022 Dec;31(23-24):3390-3401. doi: 10.1111/jocn.16240. Epub 2022 Jan 30. PMID: 35098610.
- Stuckenschneider T, Sanders ML, Devenney KE, Aaronson JA, Abeln V, Claassen JAHR, Guinan E, Lawlor B, Meeusen R, Montag C, Olde Rikkert MGM, Polidori MC, Reuter M, Schulz RJ, Vogt T, Weber B, Kessels RPC, Schneider S. NeuroExercise: The Effect of a 12-Month Exercise Intervention on Cognition in Mild Cognitive Impairment-A Multicenter Randomized Controlled Trial. Front Aging Neurosci. 2021 Jan 14;12:621947. doi: 10.3389/fnagi.2020.621947. PMID: 33519425; PMCID: PMC7840533.
- Wang Z, Xu X, Yang X, Wang SS, Zhou Y, Li Y. Effects of multicomponent exercise on cognitive function in persons with mild cognitive impairment: A systematic review and meta-analysis. Int J Nurs Stud. 2024 Oct;158:104843. doi: 10.1016/j.ijnurstu.2024.104843. Epub 2024 Jun 24. PMID: 39116586.
- Xue H, Li Y, Xu Z. A Systematic Review and Evaluation of Non-Pharmacological Interventions for Elderly Patients with Mild Cognitive Impairment. Altern Ther Health Med. 2023 Oct;29(7):74-79. PMID: 37632951.
- Yaffe K, Vittinghoff E, Dublin S, Peltz CB, Fleckenstein LE, Rosenberg DE, Barnes DE, Balderson BH, Larson EB. Effect of Personalized Risk-Reduction Strategies on Cognition and Dementia Risk Profile Among Older Adults: The SMARRT Randomized Clinical Trial. JAMA Intern Med. 2024 Jan 1;184(1):54-62. doi: 10.1001/jamainternmed.2023.6279. PMID: 38010725; PMCID: PMC10682943.
- Yassine HN, Samieri C, Livingston G, Glass K, Wagner M, Tangney C, Plassman BL, Ikram MA, Voigt RM, Gu Y, O'Bryant S, Minihane AM, Craft S, Fink HA, Judd S, Andrieu S, Bowman GL, Richard E, Albensi B, Meyers E, Khosravian S, Solis M, Carrillo M, Snyder H, Grodstein F, Scarmeas N, Schneider LS. Nutrition state of science and dementia prevention: recommendations of the Nutrition for Dementia Prevention Working Group. Lancet Healthy Longev. 2022 Jul;3(7):e501-e512. doi: 10.1016/s2666-7568(22)00120-9. Epub 2022 Jul 4. PMID: 35821792; PMCID: PMC9273104.
Evidence tabellen
Risk of Bias tables
For further details about the risk of bias assessment, see
- For Liu (2024): https://pmc.ncbi.nlm.nih.gov/articles/PMC11175880/#sec29
- For Wang (2024): https://doi.org.10.1016/j.ijnurstu.2024.104843
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Ahn J, Kim M. Effects of aerobic exercise on global cognitive function and sleep in older adults with mild cognitive impairment: A systematic review and meta-analysis. Geriatr Nurs. 2023 May-Jun;51:9-16. doi: 10.1016/j.gerinurse.2023.02.008. Epub 2023 Mar 3. PMID: 36871328. |
Less recent compared to Liu (2024) |
|
Ahn J, Kim M. Effects of exercise therapy on global cognitive function and, depression in older adults with mild cognitive impairment: A systematic review and meta-analysis. Arch Gerontol Geriatr. 2023 Mar;106:104855. doi: 10.1016/j.archger.2022.104855. Epub 2022 Nov 17. PMID: 36436448. |
Less recent compared to Liu (2024), focus on aerobic exercise |
|
Akalp K, Ferreira JP, Soares CM, Ribeiro MJ, Teixeira AM. The effects of different types of exercises on cognition in older persons with mild cognitive impairment: A systematic review and meta-analysis. Arch Gerontol Geriatr. 2024 Nov;126:105541. doi: 10.1016/j.archger.2024.105541. Epub 2024 Jun 18. PMID: 38981326. |
No clear description of control group of the included studies |
|
Ballarín-Naya L, Malo S, Moreno-Franco B. Efecto de intervenciones basadas en ejercicio físico y dieta sobre la evolución de deterioro cognitivo leve a demencia en sujetos mayores de 45 años. Revisión sistemática [Effect of physical exercise and diet based interventions on the evolution of cognitive impairment to dementia in subjects older than 45 years. A systematic review.]. Rev Esp Salud Publica. 2021 Feb 24;95:e202102032. Spanish. PMID: 33624616. |
Foreign language (Spanish) |
|
Biazus-Sehn LF, Schuch FB, Firth J, Stigger FS. Effects of physical exercise on cognitive function of older adults with mild cognitive impairment: A systematic review and meta-analysis. Arch Gerontol Geriatr. 2020 Jul-Aug;89:104048. doi: 10.1016/j.archger.2020.104048. Epub 2020 May 12. PMID: 32460123. |
Less recent compared to Liu (2024) |
|
Bohnen JLB, Albin RL, Bohnen NI. Ketogenic interventions in mild cognitive impairment, Alzheimer's disease, and Parkinson's disease: A systematic review and critical appraisal. Front Neurol. 2023 Feb 9;14:1123290. doi: 10.3389/fneur.2023.1123290. PMID: 36846143; PMCID: PMC9947355. |
Wrong publication type (results are narratively described) |
|
Bray NW, Pieruccini-Faria F, Bartha R, Doherty TJ, Nagamatsu LS, Montero-Odasso M. The effect of physical exercise on functional brain network connectivity in older adults with and without cognitive impairment. A systematic review. Mech Ageing Dev. 2021 Jun;196:111493. doi: 10.1016/j.mad.2021.111493. Epub 2021 Apr 19. PMID: 33887281. |
Includes only three studies among MCI patients, wrong outcome (functional brain network connectivity) |
|
Braz de Oliveira MP, Moreira Padovez RFC, Serrão PRMDS, Gomes Dos Santos J, Silva DCPD, Andrade LP. Is physical exercise effective at improving body structure & function and activity outcomes in individuals with Mild Cognitive Impairment? a systematic review with quality of evidence assessment. Disabil Rehabil. 2023 Feb;45(4):575-587. doi: 10.1080/09638288.2022.2040609. Epub 2022 Feb 23. PMID: 35195496. |
Wrong outcomes (muscle strength, postural balance, cardiorespiratory function, mobility, gait, activities of daily living) |
|
Buckinx F, Aubertin-Leheudre M. Nutrition to Prevent or Treat Cognitive Impairment in Older Adults: A GRADE Recommendation. J Prev Alzheimers Dis. 2021;8(1):110-116. doi: 10.14283/jpad.2020.40. PMID: 33336232. |
Wrong publication type (GRADE recommendation) |
|
Cai H, Zhang K, Wang M, Li X, Ran F, Han Y. Effects of mind-body exercise on cognitive performance in middle-aged and older adults with mild cognitive impairment: A meta-analysis study. Medicine (Baltimore). 2023 Aug 25;102(34):e34905. doi: 10.1097/MD.0000000000034905. PMID: 37653776; PMCID: PMC10470775. |
Wrong intervention (physical and mental exercises such as taijiquan, Ba Duan Jin, qigong, meditation, yoga, music and dance) |
|
Cai X, Xu L, Zhang H, Sun T, Yu J, Jia X, Hou X, Sun R, Pang J. The effects of exergames for cognitive function in older adults with mild cognitive impairment: a systematic review and metaanalysis. Front Neurol. 2024 Jul 16;15:1424390. doi: 10.3389/fneur.2024.1424390. PMID: 39081342; PMCID: PMC11286570. |
Wrong intervention (exergames) |
|
Cai Z, Ma Y, Li L, Lu GZ. Effects of exergaming in older individuals with mild cognitive impairment and dementia: A systematic review and meta-analysis. Geriatr Nurs. 2023 May-Jun;51:351-359. doi: 10.1016/j.gerinurse.2023.03.028. Epub 2023 Apr 24. PMID: 37099867. |
Wrong intervention (exergames) |
|
Cammisuli DM, Innocenti A, Franzoni F, Pruneti C. Aerobic exercise effects upon cognition in Mild Cognitive Impairment: A systematic review of randomized controlled trials. Arch Ital Biol. 2017 Jul 1;155(1-2):54-62. doi: 10.12871/000398292017126. PMID: 28715598. |
Publication year prior to 2019 |
|
Chan, J.Y.C., Liu, J., Chan, A.T.C. et al. Exergaming and cognitive functions in people with mild cognitive impairment and dementia: a meta-analysis. npj Digit. Med. 7, 154 (2024). https://doi.org/10.1038/s41746-024-01142-4 |
Wrong intervention (exergames) |
|
Chen H, Wang Y, Zhang M, Wang N, Ge S, Liu Y. Effectiveness of Tai Chi on cognitive function among older adults with mild cognitive impairment: a systematic review and meta-analysis of randomized controlled trials. Aging Ment Health. 2024 Jan-Feb;28(2):285-293. doi: 10.1080/13607863.2023.2253183. Epub 2024 Jan 31. PMID: 37728939. |
Wrong intervention (Tai Chi) |
|
Deng J, Wang H, Fu T, Xu C, Zhu Q, Guo L, Zhu Y. Physical activity improves the visual-spatial working memory of individuals with mild cognitive impairment or Alzheimer's disease: a systematic review and network meta-analysis. Front Public Health. 2024 Mar 28;12:1365589. doi: 10.3389/fpubh.2024.1365589. PMID: 38605880; PMCID: PMC11007231. |
Wrong publication type (network meta-analysis) |
|
Devranis P, Vassilopoulou Ε, Tsironis V, Sotiriadis PM, Chourdakis M, Aivaliotis M, Tsolaki M. Mediterranean Diet, Ketogenic Diet or MIND Diet for Aging Populations with Cognitive Decline: A Systematic Review. Life (Basel). 2023 Jan 6;13(1):173. doi: 10.3390/life13010173. PMID: 36676122; PMCID: PMC9866105. |
Includes no studies among MCI patients |
|
Dieckelmann M, González-González AI, Banzer W, Berghold A, Jeitler K, Pantel J, Pregartner G, Schall A, Tesky VA, Siebenhofer A. Effectiveness of exercise interventions to improve long-term outcomes in people living with mild cognitive impairment: a systematic review and meta-analysis. Sci Rep. 2023 Oct 23;13(1):18074. doi: 10.1038/s41598-023-44771-7. PMID: 37872230; PMCID: PMC10593841. |
Less recent compared to Liu (2024) |
|
Ding Z, Leung PY, Lee TL, Chan AS. Effectiveness of lifestyle medicine on cognitive functions in mild cognitive impairments and dementia: A systematic review on randomized controlled trials. Ageing Res Rev. 2023 Apr;86:101886. doi: 10.1016/j.arr.2023.101886. Epub 2023 Feb 18. PMID: 36806378. |
Includes no studies that combine nutritional and physical activity recommendations |
|
García-Casares N, Gallego Fuentes P, Barbancho MÁ, López-Gigosos R, García-Rodríguez A, Gutiérrez-Bedmar M. Alzheimer's Disease, Mild Cognitive Impairment and Mediterranean Diet. A Systematic Review and Dose-Response Meta-Analysis. J Clin Med. 2021 Oct 10;10(20):4642. doi: 10.3390/jcm10204642. PMID: 34682764; PMCID: PMC8537524. |
Includes association studies only (about MD adherence and MCI/AD risk) |
|
Gkotzamanis V, Magriplis E, Panagiotakos D. The effect of physical activity interventions on cognitive function of older adults: A systematic review of clinical trials. Psychiatriki. 2022 Dec 7;33(4):291-300. doi: 10.22365/jpsych.2022.060. Epub 2022 Feb 21. PMID: 35255465. |
Wrong publication type (results are narratively described; narrative review) |
|
Gu R, Gao Y, Zhang C, Liu X, Sun Z. Effect of Tai Chi on Cognitive Function among Older Adults with Cognitive Impairment: A Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2021 Aug 5;2021:6679153. doi: 10.1155/2021/6679153. PMID: 34394392; PMCID: PMC8360724. |
Wrong intervention (Tai Chi) |
|
Gutierrez L, Folch A, Rojas M, Cantero JL, Atienza M, Folch J, Camins A, Ruiz A, Papandreou C, Bulló M. Effects of Nutrition on Cognitive Function in Adults with or without Cognitive Impairment: A Systematic Review of Randomized Controlled Clinical Trials. Nutrients. 2021 Oct 22;13(11):3728. doi: 10.3390/nu13113728. PMID: 34835984; PMCID: PMC8621754. |
Includes no studies that are conform our PICO (5/15 studies are among MCI patients, but these studied wrong interventions such as cheeses, probiotics, vitamin D, olive oil) |
|
Han C, Sun W, Zhang D, et al Effects of different aerobic exercises on the global cognitive function of the elderly with mild cognitive impairment: a meta-analysis BMJ Open 2023;13:e067293. doi: 10.1136/bmjopen-2022-067293 |
Less recent compared to Liu (2024) |
|
Huang X, Zhao X, Li B, Cai Y, Zhang S, Wan Q, Yu F. Comparative efficacy of various exercise interventions on cognitive function in patients with mild cognitive impairment or dementia: A systematic review and network meta-analysis. J Sport Health Sci. 2022 Mar;11(2):212-223. doi: 10.1016/j.jshs.2021.05.003. Epub 2021 May 16. PMID: 34004389; PMCID: PMC9068743. |
Wrong publication type (network meta-analysis) |
|
Karamacoska D, Butt A, Leung IHK, Childs RL, Metri NJ, Uruthiran V, Tan T, Sabag A, Steiner-Lim GZ. Brain function effects of exercise interventions for cognitive decline: a systematic review and meta-analysis. Front Neurosci. 2023 May 16;17:1127065. doi: 10.3389/fnins.2023.1127065. PMID: 37260849; PMCID: PMC10228832. |
Wrong publication type (results are narratively described; scoping review) |
|
Lai X, Wen H, Li Y, Lu L, Tang C. The Comparative Efficacy of Multiple Interventions for Mild Cognitive Impairment in Alzheimer's Disease: A Bayesian Network Meta-Analysis. Front Aging Neurosci. 2020 Jun 5;12:121. doi: 10.3389/fnagi.2020.00121. PMID: 32581760; PMCID: PMC7289916. |
Wrong publication type (network meta-analysis) |
|
Lam FM, Huang MZ, Liao LR, Chung RC, Kwok TC, Pang MY. Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia: a systematic review. J Physiother. 2018 Jan;64(1):4-15. doi: 10.1016/j.jphys.2017.12.001. Epub 2017 Dec 27. PMID: 29289581. |
Publication year prior to 2019 |
|
Law CK, Lam FM, Chung RC, Pang MY. Physical exercise attenuates cognitive decline and reduces behavioural problems in people with mild cognitive impairment and dementia: a systematic review. J Physiother. 2020 Jan;66(1):9-18. doi: 10.1016/j.jphys.2019.11.014. Epub 2019 Dec 13. PMID: 31843427. |
No clear description of control group of the included studies, less recent compared to Liu (2024) |
|
Lee J. Effects of Aerobic and Resistance Exercise Interventions on Cognitive and Physiologic Adaptations for Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis of Randomized Control Trials. Int J Environ Res Public Health. 2020 Dec 9;17(24):9216. doi: 10.3390/ijerph17249216. PMID: 33317169; PMCID: PMC7764103. |
Less recent compared to Liu (2024), includes only five studies that report on cognitive function (MMSE) |
|
Li H, Su W, Dang H, Han K, Lu H, Yue S, Zhang H. Exercise Training for Mild Cognitive Impairment Adults Older Than 60: A Systematic Review and Meta-Analysis. J Alzheimers Dis. 2022;88(4):1263-1278. doi: 10.3233/JAD-220243. PMID: 35811527; PMCID: PMC9484098. |
Less recent compared to Liu (2024) |
|
Liang JH, Xu Y, Lin L, Jia RX, Zhang HB, Hang L. Comparison of multiple interventions for older adults with Alzheimer disease or mild cognitive impairment: A PRISMA-compliant network meta-analysis. Medicine (Baltimore). 2018 May;97(20):e10744. doi: 10.1097/MD.0000000000010744. PMID: 29768349; PMCID: PMC5976284. |
Publication year prior to 2019 |
|
Lin JC, Chen IH, Cheng FY. Review articles (Meta-Analyses) effects of walking on cognitive function in individuals with mild cognitive impairment: a systematic review and meta-analysis. BMC Geriatr. 2023 Aug 21;23(1):500. doi: 10.1186/s12877-023-04235-z. PMID: 37605156; PMCID: PMC10441758. |
Wrong intervention (focus on walking) |
|
Lin M, Ma C, Zhu J, Gao J, Huang L, Huang J, Liu Z, Tao J, Chen L. Effects of exercise interventions on executive function in old adults with mild cognitive impairment: A systematic review and meta-analysis of randomized controlled trials. Ageing Res Rev. 2022 Dec;82:101776. doi: 10.1016/j.arr.2022.101776. Epub 2022 Nov 1. PMID: 36332758. |
Wrong intervention (focus on walking) |
|
Lin R, Cui S, Yang J, Yang H, Feng Z, Wahner-Roedler DL, Zhou X, Salinas M, Mallory MJ, Do A, Bublitz SE, Chon TY, Tang C, Bauer BA, Xu M. Effects of Tai Chi on Patients with Mild Cognitive Impairment: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Biomed Res Int. 2021 Apr 12;2021:5530149. doi: 10.1155/2021/5530149. Retraction in: Biomed Res Int. 2023 Jul 12;2023:9789542. doi: 10.1155/2023/9789542. PMID: 33977103; PMCID: PMC8087475. |
Wrong intervention (Tai Chi) |
|
Liu DQ, Li RM, Zhang MQ, Chen YY, Zhang HP. Meta-analysis of the effect of aerobic exercise on mild cognitive impairment in the elderly. Chinese Journal of Tissue Engineering Research. 2019. |
Full-text not available |
|
Liu T, Li N, Hou Z, Liu L, Gao L, Wang L, Tan J. Nutrition and exercise interventions could ameliorate age-related cognitive decline: a meta-analysis of randomized controlled trials. Aging Clin Exp Res. 2021 Jul;33(7):1799-1809. doi: 10.1007/s40520-020-01730-w. Epub 2020 Oct 14. PMID: 33052590. |
Includes one study on the combination of nutrition and physical exercise, but wrong intervention (DHA/EPA intake) |
|
Liu X, Wang G, Cao Y. The effectiveness of exercise on global cognitive function, balance, depression symptoms, and sleep quality in patients with mild cognitive impairment: A systematic review and meta-analysis. Geriatr Nurs. 2023 May-Jun;51:182-193. doi: 10.1016/j.gerinurse.2023.03.013. Epub 2023 Apr 1. PMID: 37011490. |
Less recent compared to Liu (2024) |
|
Liu X, Wang G, Cao Y. Association of nonpharmacological interventions for cognitive function in older adults with mild cognitive impairment: a systematic review and network meta-analysis. Aging Clin Exp Res. 2023 Mar;35(3):463-478. doi: 10.1007/s40520-022-02333-3. Epub 2023 Jan 6. PMID: 36607554. |
Wrong publication type (network meta-analysis) |
|
Loprinzi PD, Blough J, Ryu S, Kang M. Experimental effects of exercise on memory function among mild cognitive impairment: systematic review and meta-analysis. Phys Sportsmed. 2019 Feb;47(1):21-26. doi: 10.1080/00913847.2018.1527647. Epub 2018 Oct 8. PMID: 30246596. |
Wrong outcome (memory function) |
|
Meng Q, Yin H, Wang S, Shang B, Meng X, Yan M, Li G, Chu J, Chen L. The effect of combined cognitive intervention and physical exercise on cognitive function in older adults with mild cognitive impairment: a meta-analysis of randomized controlled trials. Aging Clin Exp Res. 2022 Feb;34(2):261-276. doi: 10.1007/s40520-021-01877-0. Epub 2021 Aug 12. PMID: 34383248. |
Wrong intervention (combined intervention cognitive intervention and physical exercise) |
|
Price S, Ruppar TM. Ketogenic therapies in Parkinson's disease, Alzheimer's disease, and mild cognitive impairment: An integrative review. Appl Nurs Res. 2023 Dec;74:151745. doi: 10.1016/j.apnr.2023.151745. Epub 2023 Oct 28. PMID: 38007248. |
Includes no studies that are conform our PICO (5/15 studies are among MCI patients, but these studied wrong interventions such as carbohydrate diet, Modified Adkins diet) |
|
Rampengan DD, Gunawan FA, Rampengan JA, Ramadhan RN, Iqhrammullah M, Yufika A. Effectiveness of Tai Chi as a non-invasive intervention for mild cognitive impairment in the elderly: A comprehensive review and meta-analysis. Narra J. 2024 Apr;4(1):e724. doi: 10.52225/narra.v4i1.724. Epub 2024 Apr 24. PMID: 38798853; PMCID: PMC11125395. |
Wrong intervention (Tai Chi) |
|
Rodrigues SLDS, Silva JMD, Oliveira MCC, Santana CMF, Carvalho KM, Barbosa BJAP. Physical exercise as a non-pharmacological strategy for reducing behavioral and psychological symptoms in elderly with mild cognitive impairment and dementia: a systematic review of randomized clinical trials. Arq Neuropsiquiatr. 2021 Dec;79(12):1129-1137. doi: 10.1590/0004-282X-ANP-2020-0539. PMID: 34877985. |
Wrong population (no studies among MCI patients included) |
|
Sánchez-Alcalá M, Aibar-Almazán A, Afanador-Restrepo DF, Carcelén-Fraile MDC, Achalandabaso-Ochoa A, Castellote-Caballero Y, Hita-Contreras F. The Impact of Rhythmic Physical Activity on Mental Health and Quality of Life in Older Adults with and without Cognitive Impairment: A Systematic Review and Meta-Analysis. J Clin Med. 2023 Nov 14;12(22):7084. doi: 10.3390/jcm12227084. PMID: 38002696; PMCID: PMC10672098. |
Includes only four studies among MCI patients |
|
Seok JW, Kim G, Kim JU. Comparative efficacy of seven nonpharmacological interventions on global cognition in older adults with and without mild cognitive impairment: a network meta-analysis of randomized controlled trials. Sci Rep. 2024 Apr 10;14(1):8402. doi: 10.1038/s41598-024-58232-2. PMID: 38600212; PMCID: PMC11006946. |
Wrong publication type (network meta-analysis) |
|
Shao Z, Hu M, Zhang D, Zeng X, Shu X, Wu X, Kwok TCY, Feng H. Dose-response relationship in non-pharmacological interventions for individuals with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. J Clin Nurs. 2022 Dec;31(23-24):3390-3401. doi: 10.1111/jocn.16240. Epub 2022 Jan 30. PMID: 35098610. |
Includes no studies that combine nutritional and physical activity recommendations |
|
Song D, Yu D, Zhou J, Zeng L, Fan T. Effects of traditional Chinese medicine-based exercises on cognitive function in older people with mild cognitive impairment: A systematic review and meta-analysis. Geriatr Nurs. 2022 Jul-Aug;46:98-104. doi: 10.1016/j.gerinurse.2022.05.005. Epub 2022 May 30. PMID: 35653946. |
Wrong intervention (traditional Chinese medicine-based exercises) |
|
Song D, Yu DSF, Li PWC, Lei Y. The effectiveness of physical exercise on cognitive and psychological outcomes in individuals with mild cognitive impairment: A systematic review and meta-analysis. Int J Nurs Stud. 2018 Mar;79:155-164. doi: 10.1016/j.ijnurstu.2018.01.002. Epub 2018 Jan 4. PMID: 29334638. |
Publication year prior to 2019 |
|
Su K, Yuan J, Liu H, Luo M, Li Q, Liu S, Feng X. The Comparative Effectiveness of Traditional Chinese Medicine Exercise Therapies in Elderly People With Mild Cognitive Impairment: A Systematic Review and Network Meta-Analysis. Front Neurol. 2022 Mar 16;13:775190. doi: 10.3389/fneur.2022.775190. PMID: 35370918; PMCID: PMC8966650. |
Wrong intervention (traditional Chinese medicine exercise) |
|
Turner DT, Hu MX, Generaal E, Bos D, Ikram MK, Heshmatollah A, Fani L, Ikram MA, Penninx BWJH, Cuijpers P. Physical Exercise Interventions Targeting Cognitive Functioning and the Cognitive Domains in Nondementia Samples: A Systematic Review of Meta-Analyses. J Geriatr Psychiatry Neurol. 2021 Mar;34(2):91-101. doi: 10.1177/0891988720915523. Epub 2020 Apr 15. PMID: 32295450; PMCID: PMC7859677. |
Wrong publication type (systematic review of meta-analyses) |
|
Vega-Ávila GC, Afanador-Restrepo DF, Rivas-Campo Y, García-Garro PA, Hita-Contreras F, Carcelén-Fraile MDC, Castellote-Caballero Y, Aibar-Almazán A. Rhythmic Physical Activity and Global Cognition in Older Adults with and without Mild Cognitive Impairment: A Systematic Review. Int J Environ Res Public Health. 2022 Sep 27;19(19):12230. doi: 10.3390/ijerph191912230. PMID: 36231532; PMCID: PMC9566681. |
Includes only six studies among MCI patients, less recent compared to Liu (2024) |
|
Venegas-Sanabria LC, Cavero-Redondo I, Lorenzo-Garcia P, Sánchez-Vanegas G, Álvarez-Bueno C. Efficacy of Nonpharmacological Interventions in Cognitive Impairment: Systematic Review And Network Meta-Analysis. Am J Geriatr Psychiatry. 2024 Dec;32(12):1443-1465. doi: 10.1016/j.jagp.2024.06.012. Epub 2024 Jul 9. PMID: 39034265. |
Wrong publication type (network meta-analysis) |
|
Wang R, Zhang H, Li H, Ren H, Sun T, Xu L, Liu Y, Hou X. The influence of exercise interventions on cognitive functions in patients with amnestic mild cognitive impairment: A systematic review and meta-analysis. Front Public Health. 2022 Nov 15;10:1046841. doi: 10.3389/fpubh.2022.1046841. PMID: 36457329; PMCID: PMC9706097. |
Includes patients with aMCI as well, less recent compared to Liu (2024) |
|
Wang S, Yin H, Wang X, Jia Y, Wang C, Wang L, Chen L. Efficacy of different types of exercises on global cognition in adults with mild cognitive impairment: a network meta-analysis. Aging Clin Exp Res. 2019 Oct;31(10):1391-1400. doi: 10.1007/s40520-019-01142-5. Epub 2019 Feb 9. PMID: 30739298. |
Wrong publication type (network meta-analysis) |
|
Wang YQ, Jia RX, Liang JH, Li J, Qian S, Li JY, Xu Y. Effects of non-pharmacological therapies for people with mild cognitive impairment. A Bayesian network meta-analysis. Int J Geriatr Psychiatry. 2020 Jun;35(6):591-600. doi: 10.1002/gps.5289. Epub 2020 Mar 12. PMID: 32119152. |
Wrong publication type (network meta-analysis) |
|
Wang YY, Wang XX, Chen L, Liu Y, Li YR. A systematic review and network meta-analysis comparing various non-pharmacological treatments for older people with mild cognitive impairment. Asian J Psychiatr. 2023 Aug;86:103635. doi: 10.1016/j.ajp.2023.103635. Epub 2023 May 26. PMID: 37270875. |
Wrong publication type (network meta-analysis) |
|
Wei L, Chai Q, Chen J, Wang Q, Bao Y, Xu W, Ma E. The impact of Tai Chi on cognitive rehabilitation of elder adults with mild cognitive impairment: a systematic review and meta-analysis. Disabil Rehabil. 2022 Jun;44(11):2197-2206. doi: 10.1080/09638288.2020.1830311. Epub 2020 Oct 12. PMID: 33043709. |
Wrong intervention (Tai Chi) |
|
Xue H, Li Y, Xu Z. A Systematic Review and Evaluation of Non-Pharmacological Interventions for Elderly Patients with Mild Cognitive Impairment. Altern Ther Health Med. 2023 Oct;29(7):74-79. PMID: 37632951. |
Wrong publication type (systematic review of systematic reviews and meta-analyses) |
|
Yang J, Zhang L, Tang Q, Wang F, Li Y, Peng H, Wang S. Tai Chi is Effective in Delaying Cognitive Decline in Older Adults with Mild Cognitive Impairment: Evidence from a Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2020 Mar 25;2020:3620534. doi: 10.1155/2020/3620534. PMID: 32308706; PMCID: PMC7132349. |
Wrong intervention (Tai Chi) |
|
Yong L, Liu L, Ding T, Yang G, Su H, Wang J, Yang M, Chang J. Evidence of Effect of Aerobic Exercise on Cognitive Intervention in Older Adults With Mild Cognitive Impairment. Front Psychiatry. 2021 Jul 20;12:713671. doi: 10.3389/fpsyt.2021.713671. PMID: 34354619; PMCID: PMC8329556. |
Less recent compared to Liu (2024), docus on aerobic exercise |
|
Yuan Y, Li X, Liu W. Dance activity interventions targeting cognitive functioning in older adults with mild cognitive impairment: A meta-analysis. Front Psychol. 2022 Sep 27;13:966675. doi: 10.3389/fpsyg.2022.966675. PMID: 36237681; PMCID: PMC9553227. |
Less recent compared to Liu (2024), focus on dance interventions |
|
Zawaly K, Fortier R, Buetow S, Tippett L, Kerse N. Exploring Cognitively Loaded Physical Activity Compared With Control to Improve Global Cognitive Function in Older Community-Dwelling Adults With Mild Cognitive Impairment: Systematic Review With Meta-Analysis. Am J Lifestyle Med. 2019 Sep 27;16(1):141-149. doi: 10.1177/1559827619876887. PMID: 35185436; PMCID: PMC8848110. |
Wrong intervention (behavioral intervention) |
|
Zhang L, Li B, Yang J, Wang F, Tang Q, Wang S. Meta-analysis: Resistance Training Improves Cognition in Mild Cognitive Impairment. Int J Sports Med. 2020 Oct;41(12):815-823. doi: 10.1055/a-1186-1272. Epub 2020 Jun 29. PMID: 32599643. |
Includes only five studies that are conform our PICO, less recent compared to Liu (2024) |
|
Zhang Q, Hu J, Wei L, Cao R, Ma R, Song H, Jin Y. Effects of traditional Chinese exercise on cognitive and psychological outcomes in older adults with mild cognitive impairment: A systematic review and meta-analysis. Medicine (Baltimore). 2019 Feb;98(7):e14581. doi: 10.1097/MD.0000000000014581. PMID: 30762810; PMCID: PMC6408103. |
Wrong intervention (traditional Chinese exercise) |
|
Zhao Y, Feng H, Wu X, Du Y, Yang X, Hu M, Ning H, Liao L, Chen H, Zhao Y. Effectiveness of Exergaming in Improving Cognitive and Physical Function in People With Mild Cognitive Impairment or Dementia: Systematic Review. JMIR Serious Games. 2020 Jun 30;8(2):e16841. doi: 10.2196/16841. PMID: 32602841; PMCID: PMC7367532. |
Wrong intervention (exergames) |
|
Zheng G, Xia R, Zhou W, Tao J, Chen L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2016 Dec;50(23):1443-1450. doi: 10.1136/bjsports-2015-095699. Epub 2016 Apr 19. PMID: 27095745. |
Publication year prior to 2019 |
|
Zhou K, Liu M, Bao D, Zhou J. Effects of Traditional Chinese Exercises on Cognitive Function in Older Adults With Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Front Hum Neurosci. 2022 Mar 25;16:849530. doi: 10.3389/fnhum.2022.849530. PMID: 35399354; PMCID: PMC8989961. |
Wrong intervention (traditional Chinese exercise) |
|
Zhou XL, Wang LN, Wang J, Zhou L, Shen XH. Effects of exercise interventions for specific cognitive domains in old adults with mild cognitive impairment: A meta-analysis and subgroup analysis of randomized controlled trials. Medicine (Baltimore). 2020 Jul 31;99(31):e20105. doi: 10.1097/MD.0000000000020105. PMID: 32756073; PMCID: PMC7402775. |
Less recent compared to Liu (2024) |
|
Zhou Y, Li LD. Exercise training for cognitive and physical function in patients with mild cognitive impairment: A PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore). 2022 Aug 26;101(34):e30168. doi: 10.1097/MD.0000000000030168. PMID: 36042589; PMCID: PMC9410583. |
No clear description of control group of the included studies, less recent compared to Liu (2024) |
|
Zhou Z, Yun J, Li W, He S, He L. Efficacy of non-pharmacological intervention on cognitive function of elderly patients with mild cognitive impairment: a network meta-analysis. Chinese Journal of Evidence-Based Medicine. 2023 |
Wrong publication type (network meta-analysis) |
|
Zhu Y, Zhong Q, Ji J, Ma J, Wu H, Gao Y, Ali N, Wang T. Effects of Aerobic Dance on Cognition in Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. J Alzheimers Dis. 2020;74(2):679-690. doi: 10.3233/JAD-190681. PMID: 32083578. |
Less recent compared to Liu (2024), focus on dance interventions |
|
Zou, C., Amos-Richards, D., Jagannathan, R. et al. Effect of home-based lifestyle interventions on cognition in older adults with mild cognitive impairment: a systematic review. BMC Geriatr 24, 200 (2024). https://doi.org/10.1186/s12877-024-04798-5 |
Wrong intervention (home-based interventions) |
|
Zou L, Loprinzi PD, Yeung AS, Zeng N, Huang T. The Beneficial Effects of Mind-Body Exercises for People With Mild Cognitive Impairment: a Systematic Review With Meta-analysis. Arch Phys Med Rehabil. 2019 Aug;100(8):1556-1573. doi: 10.1016/j.apmr.2019.03.009. Epub 2019 Apr 12. PMID: 30986409. |
Wrong intervention (combined intervention cognitive intervention and physical exercise) |
Verantwoording
Beoordelingsdatum en geldigheid
Publicatiedatum : 03-11-2025
Beoordeeld op geldigheid : 23-10-2025
Algemene gegevens
De verantwoording zal op de Richtlijnendatabase (Richtlijnendatabase.nl) bij elke geprioriteerde module die is ontwikkeld binnen dit cluster worden geplaatst. De betrokken expertiseleden, de kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) en de autoriserende partijen kunnen variëren per module.
De ontwikkeling van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinair cluster ingesteld. Het cluster Cognitieve stoornissen en dementie bestaat uit meerdere richtlijnen (zie hier de actuele clusterindeling). De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden brengen hun expertise in, indien nodig. De volgende personen uit het cluster zijn betrokken geweest bij de herziening van deze module:
Clusterstuurgroepleden
- Dhr. prof. dr. M.G.M. (Marcel) Olde Rikkert (voorzitter), klinisch geriater; NVKG
- Dhr. prof. dr. A.R. (Tony) Absalom, anesthesioloog; NVA
- Dhr. dr. J.H.J.M. (Jeroen) de Bresser, radioloog; NVvR
- Mevr. dr. I.K. (Indrag) Lampe, psychiater; NVvP
- Mevr. R. (Renske) Leistra, patiëntvertegenwoordiger; Alzheimer Nederland
- Mevr. prof. dr. B.C. (Barbara) van Munster, internist; NIV
- Dhr. prof. dr. E. (Edo) Richard, neuroloog; NVN
- Mevr. prof. dr. Ir. C. (Charlotte) Teunissen, klinisch chemicus; NVKC
- Dhr. dr. R.A.W. (Ronald) Verhagen, orthopedisch chirurg; NOV
Betrokken clusterexpertisegroepleden
- Dhr. dr. A.P.A. (Auke) Appelman, radioloog; NVvR
- Mevr. dr. R.L. (Rozemarijn) van Bruchem-van Visser, internist ouderengeneeskunde; NIV
- Dhr. drs. B.P.H. (Bas) ter Brugge, specialist ouderengeneeskunde; Verenso
- Dhr. dr. J.A.H.R. (Jurgen) Claassen, klinisch geriater; NVKG
- Dhr. dr. P.L.J. (Paul) Dautzenberg, klinisch geriater; NVKG
- Mevr. dr. M.E.A. (Marlise) van Eersel, internist; NIV
- Mevr. drs. C.M. (Christa) de Geus, neurogeneticus; NVKG
- Mevr. dr. E.M. (Elsmarieke van de Giessen), radioloog; NVNG
- Mevr. drs. M. (Marjolein) Groeneveld, verpleegkundig Consulent Geriatrie, klinisch epidemioloog; V&VN
- Mevr. drs. H. (Hiltsje) Heemskerk, klinisch geriater; NVKG
- Dhr. dr. R.B. (Rients) Huitema, klinisch neuropsycholoog; NIP
- Dhr. drs. A. (Ali) Lahdidioui, internist; NIV
- Dhr. dr. J. (Jules) Lavalaye, nucleair geneeskundige; NVNG
- Mevr. drs. L. (Lieke) Mitrov, ziekenhuisapotheker; NVZA
- Mevr. dr. M. (Marieke) Perry, huisarts/onderzoeker; NHG
- Dhr. dr. G. (Gerwin) Roks, neuroloog; NVN
- Mevr. dr. T.R. (Rikje) Ruiter, internist; NIV
- Mevr. A.J.B.P. (Astrid) Schoonbrood, ergotherapeut; EN
- Mevr. dr. N. (Niki) Schoonenboom, neuroloog; NVN
- Dhr. dr. H. (Harro) Seelaar, neuroloog; NVN
- Dhr. dr. K.S. (Koen) Simons, intensivist-internist; NVIC
- Mevr. drs. M.M.E. (Marlies) Sleegers-Kerkenaar, klinisch geriater; NVKG
- Mevr. drs. VCJ (Vera) van Stek-Smits, neuropsycholoog-gezondheidszorgpsycholoog; NIP
- Mevr. dr. E.M. (Eveline) Veltman, psychiater; NVvP
- Dhr. drs. D. (Dave) Verkaik, AIOS geriatrie; NVKG
- Mevr. prof. dr. M. (Meike) Vernooij, radioloog; NVvR
- Dhr. dr. E.G.B. (Jort) Vijverberg, neuroloog; NVN
- Mevr. dr. M.A. (Marjolein) Wijngaarden, internist; NIV
Met ondersteuning van
- Mevr. dr. C.T.J. (Charlotte) Michels, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. dr. L.C. (Lotte) Houtepen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Mevr. drs. L.C. (Laura) van Wijngaarden, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
Een overzicht van de belangen van de clusterleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
Clusterstuurgroepleden
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Olde Rikkert* |
Hoogleraar Geriatrie, Radboudumc, Nijmegen |
Hoofdredacteur Nederlands Tijdschrift voor Geneeskunde |
Geen; uitsluitend ZonMw gefinancierd onderzoek dat overheidsbelang centraal stelt. Sinds 2017 geen farma-onderzoek meer. |
Geen restrictie |
|
Absalom |
Hoogleraar Anesthesiologie, UMCG, Groningen |
Consultancy werkzaamheden (betaald, alle betalingen aan UMCG) 6. Consultancy werk voor Becton Dickinson (Eysins, Switzerland) en Terumo (Tokyo, Japan) – technische advies over spuitpompen. Niet gerelateerd aan dementie/ MCI/ delier. |
Extern gefinancierd onderzoeken, maar financier heeft geen belangen bij de richtlijn. * Rigel Pharmaceuticals (San Francisco, USA) (PAST) * The Medicines Company (Parsippany, NJ, USA)(PAST) |
Geen restricties, omdat adviseurswerk niet gerelateerd is aan de afbakening van het cluster |
|
De Bresser |
- Neuroradioloog 1.0fte, LUMC, Leiden |
Geen |
Mijn onderzoek wordt mede gesponsord door Alzheimer Nederland. Deze financier heeft geen belang bij bepaalde uitkomsten van de richtlijn. |
Geen restrictie |
|
Lampe |
Psychiater, OLVG Ziekenhuis, Amsterdam |
Geen |
Geen |
Geen restrictie |
|
Leistra |
Belangenbehartiger, Alzheimer Nederland |
Casemanager Dementie bij de King Arthur Groep |
Geen |
Geen restrictie |
|
Richard |
Hoogleraar neurologie: * afdeling neurologie Radboudumc (0.8fte) * afdeling Public and Occupational Health Amsterdam UMC (0.2 fte) |
- Neuroloog-onderzoeker AmsterdamUMC, locatie AMC, gastvrijheidsaanstelling. - Hoofdredacteur Leerboek Neurologie (Bohn Staffleu van Loghem) |
Geen, uitsluitend onderzoek financiering van non-profit instellingen (e.g. ZonMw, Europese Commissie). |
Geen restrictie |
|
Teunissen |
Hoofd Neurochemisch laboratorium, Afdeling Klinische Chemie, AmsterdamUMC, lokatie VUmc, Amsterdam |
*Adviseur voor educatief blad: Mednet Neurologie (betaald). * Alle betalingen zijn aan het AmsterdamUMC. |
*Wetenschappelijke samenwerking met ADxNeurosciences, Olink, Quanterix, Roche in kader van o.a. Marie Curie subsidie. Het doel van het Marie Curie project is om een nieuwe generatie van onderzoekers in het biomarker veld op te leiden, tot experts in alle aspecten van biomarker onderzoek. Aan het einde van de ontwikkeling van biomarkers zullen deze via bedrijven op de markt moeten komen, en omdat niet alle wetenschappers uiteindelijk in de academische wereld blijven, is het belangrijk dat jonge onderzoekers ervaring opdoen met de manier van onderzoek doen in het bedrijfsleven. In marie curie projecten gebeurt dat door een deel van het onderzoek bij een bedrijf uit te voeren. *Het Neurochemisch laboratorium doet contractresearch voor Acumen, ADx Neurosciences, AC-Immune, Alamar, Aribio, Axon Neurosciences, Beckman-Coulter, BioConnect, Bioorchestra, Brainstorm Therapeutics, Celgene, Cognition Therapeutics, EIP Pharma, Eisai, Eli Lilly, Fujirebio, Instant Nano Biosensors, Novo Nordisk, Olink, PeopleBio, Quanterix, Roche, Toyama, Vivoryon. Dit zijn meestal biomarker-analyses voor hun trials, bij inclusies en als uitkomstmaten. *Grants: Research of CET is supported by the European Commission (Marie Curie International Training Network, grant agreement No 860197 (MIRIADE) and TAME, Innovative Medicines Initiatives 3TR (Horizon 2020, grant no 831434) EPND ( IMI 2 Joint Undertaking (JU), grant No. 101034344) and JPND (bPRIDE, CCAD), European Partnership on Metrology, co-financed from the European Union’s Horizon Europe Research and Innovation Programme and by the Participating States ((22HLT07 NEuroBioStand), CANTATE project funded by the Alzheimer Drug Discovery Foundation, Alzheimer Association, Michael J Fox Foundation, Health Holland, the Dutch Research Council (ZonMW), Alzheimer Drug Discovery Foundation, The Selfridges Group Foundation, Alzheimer Netherlands. CT is recipient of ABOARD, which is a public-private partnership receiving funding from ZonMW (#73305095007) and Health~Holland, Topsector Life Sciences & Health (PPP-allowance; #LSHM20106). CT is recipient of TAP-dementia, a ZonMw funded project (#10510032120003) in the context of the Dutch National Dementia Strategy. |
Geen restrictie |
|
Van Munster |
* Hoogleraar Interne Geneeskunde, Ouderengeneeskunde/Geriatrie, UMCG, Groningen. *Plaatsvervangend opleider Geriatrie, UMCG, Groningen. |
- 2020 – heden Voorzitter Alzheimer Centrum Groningen (alle functies zijn onbetaald) |
*2022 ZONMw: Young Onset Dementia- INCLUDED: Advance care planning. 2022 ZEGG/ZONMw: "The impact of a comprehensive geriatric assessment including advance care planning in acutely hospitalized frail patients with cognitive disorders: the GOAL study" |
Geen restrictie |
|
Verhagen |
Orthopedisch chirurg/opleider in Tergooi MC |
Geen |
Geen |
Geen restrictie |
Clusterexpertisegroepleden
Richtlijn Dementie: Module ‘Antipsychotica bij dementie’
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Mitrov |
Ziekenhuisapotheker, Flevoziekenhuis, Almere |
Special Interest Group Farmacotherapie bij ouderen (NVKG/NVZA), onbetaald |
Geen |
Geen restrictie |
|
Verkaik |
Aios geriatrie, betaalde functie. In opleiding vanuit Gelre ziekenhuizen Apeldoorn en Zutphen. |
Deelname pvc commissie als aios lid voor kwaliteits visitaties (onbetaald) |
Geen |
Geen restrictie |
Richtlijn Dementie: Module ‘Antidepressiva bij dementie’
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Heemskerk |
Klinisch geriater, Arkin Ouderen (GGZ, Amsterdam) |
NVKG, commissie ouderenpsychiatrie |
Geen |
Geen restrictie |
|
Veltman |
Psychiater, UMCU |
Geen |
Geen |
Geen restrictie |
Richtlijn MCI: Module 'Biomarkers’
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Van de Giessen |
Radioloog (aandachtsgebeid nucleaire geneeskunde), Amsterdam UMC |
- NVNG, commissie onderwijs en themagroep neuro |
Beoordelingen PET scans voor Ixico (betaald aan instituut) Contract research voor Roche (betaald aan instituut) Onderzoeksfinanciering van non-profit instelingen (o.a. ZonMw, Alzheimer Nederland, Hersenstichting, Health~Holland, KWF) |
Geen restrictie |
|
Richard |
Hoogleraar neurologie: * afdeling neurologie Radboudumc (0.8fte) * afdeling Public and Occupational Health Amsterdam UMC (0.2 fte) |
- Neuroloog-onderzoeker AmsterdamUMC, locatie AMC, gastvrijheidsaanstelling. - Hoofdredacteur Leerboek Neurologie (Bohn Staffleu van Loghem) |
Geen, uitsluitend onderzoek financiering van non-profit instellingen (e.g. ZonMw, Europese Commissie). |
Geen restrictie |
Richtlijn MCI: Module ‘Leefstijladviezen’
|
Clusterlid
|
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Groeneveld |
Verpleegkundig consulent geriatrie (16 uur) Verpleegkundig onderzoeker Waardengedreven zorg (16 uur) |
Geen
|
Extern gefinancieerd onderzoek: * Catharina onderzoeksfonds: Prestatie en acceptatie van een predictiemodel voor vallen in het ziekenhuis (rol als projectleider) *KIPZ subsidie t/m 31 december: Prestatie en acceptatie van een predictiemodel voor vallen in het ziekenhuis (ja) |
Geen restrictie |
|
Ruiter |
*Internist ouderen geneeskunde en klinische farmacologie Maasstad Ziekenhuis 0,8fte *Post-doctoraal onderzoeker & Epidemioloog B Erasmus MC dept. Epidemiologie 0,1 fte * Lid van het College ter beoordeling van geneesmiddelen |
*Lid raad van toezicht Stichting Landelijk Wonen Klein Houtdijk (Onbetaald). *Secretaris Forum Visitatorum NIV (Onbetaald). *Redactielid Tijdschrift Geriatrie en Gerontologie (Onbetaald). * Voorzitter commissie beroepsbelangen kerngroep ouderengeneeskunde NIV. |
Geen |
Geen restrictie |
|
Claassen |
Universitair hoofddocent en klinisch geriater (1.0 fte), Radboudumc, Nijmegen |
Geen |
*Fase 3 onderzoek Novo Nordisk (EVOKE, NCT04777396. Wereldwijde geneesmiddelenstudie (semaglutide) over Alzheimer. Rol als lokale PI. Middel komt niet aan bod in huidige vijf modules. *MOCIA-project, gefinancierd door ZonMW (www.mocia.nl). *ABOARD onderzoek (gefinancierd door ZonMW en Health Holland, projectnummer: 73305095007) |
Geen restrictie |
Richtlijn MCI: Module ‘Follow-up’
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Claassen |
Universitair hoofddocent en klinisch geriater (1.0 fte), Radboudumc, Nijmegen |
Geen |
*Fase 3 onderzoek Novo Nordisk (EVOKE, NCT04777396. Wereldwijde geneesmiddelenstudie (semaglutide) over Alzheimer. Rol als lokale PI. Middel komt niet aan bod in huidige vijf modules. *MOCIA-project, gefinancierd door ZonMW (www.mocia.nl). *ABOARD onderzoek (gefinancierd door ZonMW en Health Holland, projectnummer: 73305095007) |
Geen restrictie |
|
Perry |
* Huisarts, Huisartsenpraktijk Velp, 0.5 fte * Senior-onderzoeker afdelingen eerstelijnsgeneeskunde en Geriatrie van het Radboudumc en bij het Radboud Alzheimer Centrum, 0.5 fte |
Auteur hoofdstuk Vergeetachtigheid in Álledaagse klachten 2020 (onkostenvergoeding) Commissielid werkgroep multidisciplinaire richtlijn Dementie 2018 - 2020 (onkostenvergoeding) Commissielid werkgroep heziening NHG standaard Dementie 2017 - 2020 (onkostenvergoeding) Commissielid werkgroep Addendum MCI bij multidisciplinaire richtlijn Dementie 20 1 6-20 1 B (onkostenvergoeding) Auteur online nascholing dementie Accredidact huisartsen 2016 en doktersassistenten 2017 (betaald) Auteur twee boekhoofdstukken dementie (palliatieve zorg en diagnostische verrichtingen) 2017 en 2018 in opdracht van het NHG (onkostenvergoeding) Auteur hoofdtsuk Vergeetachtigheid (Alledaagse klachten in de huisartsgeneeskunde) 2020 Onkostenvergoeding Expert bij www.dementie.nl tot heden (vrijwillig) Columnist Alz (donateursblaadje Alzheimer Nederland) tot 2016 (vrijwillig) |
Projectleider DementieNet (financiering door Giekes-Strijbis fonds, Alzheimer Nederland en ZonMw) Andere ZonMw/Memorabel projecten: - Decidem (anticiperende besluitvorming met mensen met dementie door huisartsen), medeprojectleider - Crisisreductie in de dementiezorg, medeaanvrager - SHiMMy en SHARED (relatie sociale gezondheid en ontstaan en progressie van dementie), medeaanvrager - S-Decided (gezamelijke besluitvorming bij diagnostiek bij geheugenklachten), medeaanvrager
Diverse projecten omtrent transmurale/interprofessionele aanpak van advance care planning van Zorginstituut Nederland, Stoffels-Hornstra fonds, ZonMw EPOS: Extramurale praktijkontwikkeling specialist ouderengeneeskunde UNICITY: dementie op jonge leeftijd, oa signalering door huisartsen en onderscheid met depressie, burn-out
*DementieNet aanpak, generieke benadering voor lokale eerstelijns netwerkzorg *Expert bij www.dementie.nl, website van Alzheimer Nederland (vrijwillig) *Columnist Alz (donateursblaadje Alzheimer Nederland) tot 2016 (vrijwillig) *Diverse malen gastspreker bij verschillende Alzheimer Cafés (vrijwillig) |
Geen restrictie |
|
Roks |
Neuroloog ETZ Tilburg |
METC Brabant, lid en vice voorzitter (onkostenvergoeding) |
Geen |
Geen restrictie |
Algemene herziening: Nieuwe concept indeling (richtlijn Dementie en richtlijn MCI)
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Lampe |
Psychiater, OLVG ziekenhuis |
Geen |
Geen |
Geen restrictie |
|
Olde Rikkert* |
Hoogleraar Geriatrie, Radboudumc, Nijmegen |
Hoofdredacteur Nederlands Tijdschrift voor Geneeskunde |
Geen; uitsluitend ZonMw gefinancierd onderzoek dat overheidsbelang centraal stelt. Sinds 2017 geen farma-onderzoek meer. |
Geen restrictie |
|
Perry |
* Huisarts, Huisartsenpraktijk Velp, 0.5 fte * Senior-onderzoeker afdelingen eerstelijnsgeneeskunde en Geriatrie van het Radboudumc en bij het Radboud Alzheimer Centrum, 0.5 fte |
Auteur hoofdstuk Vergeetachtigheid in Álledaagse klachten 2020 (onkostenvergoeding) Commissielid werkgroep multidisciplinaire richtlijn Dementie 2018 - 2020 (onkostenvergoeding) Commissielid werkgroep heziening NHG standaard Dementie 2017 - 2020 (onkostenvergoeding) Commissielid werkgroep Addendum MCI bij multidisciplinaire richtlijn Dementie 20 1 6-20 1 B (onkostenvergoeding) Auteur online nascholing dementie Accredidact huisartsen 2016 en doktersassistenten 2017 (betaald) Auteur twee boekhoofdstukken dementie (palliatieve zorg en diagnostische verrichtingen) 2017 en 2018 in opdracht van het NHG (onkostenvergoeding) Auteur hoofdtsuk Vergeetachtigheid (Alledaagse klachten in de huisartsgeneeskunde) 2020 Onkostenvergoeding Expert bij www.dementie.nl tot heden (vrijwillig) Columnist Alz (donateursblaadje Alzheimer Nederland) tot 2016 (vrijwillig) |
Projectleider DementieNet (financiering door Giekes-Strijbis fonds, Alzheimer Nederland en ZonMw) Andere ZonMw/Memorabel projecten: - Decidem (anticiperende besluitvorming met mensen met dementie door huisartsen), medeprojectleider - Crisisreductie in de dementiezorg, medeaanvrager - SHiMMy en SHARED (relatie sociale gezondheid en ontstaan en progressie van dementie), medeaanvrager - S-Decided (gezamelijke besluitvorming bij diagnostiek bij geheugenklachten), medeaanvrager
Diverse projecten omtrent transmurale/interprofessionele aanpak van advance care planning van Zorginstituut Nederland, Stoffels-Hornstra fonds, ZonMw EPOS: Extramurale praktijkontwikkeling specialist ouderengeneeskunde UNICITY: dementie op jonge leeftijd, oa signalering door huisartsen en onderscheid met depressie, burn-out
*DementieNet aanpak, generieke benadering voor lokale eerstelijns netwerkzorg *Expert bij www.dementie.nl, website van Alzheimer Nederland (vrijwillig) *Columnist Alz (donateursblaadje Alzheimer Nederland) tot 2016 (vrijwillig) *Diverse malen gastspreker bij verschillende Alzheimer Cafés (vrijwillig) |
Geen restrictie |
|
Richard |
Hoogleraar neurologie: * afdeling neurologie Radboudumc (0.8fte) * afdeling Public and Occupational Health Amsterdam UMC (0.2 fte) |
- Neuroloog-onderzoeker AmsterdamUMC, locatie AMC, gastvrijheidsaanstelling. - Hoofdredacteur Leerboek Neurologie (Bohn Staffleu van Loghem) |
Geen, uitsluitend onderzoek financiering van non-profit instellingen (e.g. ZonMw, Europese Commissie). |
Geen restrictie |
Inbreng patiëntenperspectief
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule voerden de clusterleden conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uit om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema bij Werkwijze).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
| Module |
Uitkomst raming |
Toelichting |
|
Leefstijladviezen bij MCI |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt uit de toetsing dat het overgrote deel van de zorgverleners al aan de norm voldoet, het geen nieuwe manier van zorgverlening betreft, het geen toename in het aantal voltijdsequivalenten of wijziging in het opleidingsniveau van zorgverleners betreft. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Cluster cognitieve stoornissen en dementie |
|
|
Uitgangsvraag/modules: UV4 Wat is de aanbevolen strategie voor het toepassen van leefstijladviezen voor personen met MCI? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 21 augustus 2024 |
|
Periode: vanaf 2010 |
Talen: geen restrictie |
|
Literatuurspecialist: Alies Oost |
|
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl/ |
|
|
In de databases Embase.com en Ovid/Medline is op 21 augustus 2024 systematisch gezocht naar systematische reviews vanaf 2010 over leefstijladviezen (voeding/ lichamelijke activiteit) voor personen met mild cognitive impairment. De literatuurzoekactie leverde 884 unieke treffers op. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
613 |
611 |
884* |
|
RCT |
838 |
1051 |
1385 |
|
Totaal |
1451 |
1662 |
2269 |
*in Rayyan
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
'mild cognitive impairment'/exp OR 'mild cognitive impair*':ti,ab,kw OR mci:ti,ab,kw OR (('cognitive impair*' NEAR/3 ('no dement*' OR 'without dement*' OR 'not dement*')):ti,ab,kw) OR cind:ti,ab,kw OR vcind:ti,ab,kw |
72156 |
|
#2 |
'lifestyle modification'/exp OR 'lifestyle intervention'/exp OR 'diet'/exp OR 'diet therapy'/exp OR 'dietary supplement'/exp OR 'kinesiotherapy'/exp OR ((('life style*' OR lifestyle*) NEAR/3 (modificat* OR chang* OR intervention* OR promot*)):ti,ab,kw) OR (((diet* OR 'food*' OR nutrition*) NEAR/3 ('intervention*' OR 'therap*' OR 'treatment*' OR 'advic*' OR 'additive*' OR supplement* OR formula*)):ti,ab,kw) OR (((oral OR multivitamin* OR vitamin*) NEAR/3 supplement*):ti,ab,kw) OR ((('physical*' OR movement OR activit*) NEAR/3 (exercis* OR intervention* OR program* OR promot* OR advic* OR training*)):ti,ab,kw) OR ((exercis* NEAR/3 (therap* OR treatment* OR intervention* OR program* OR promot* OR advic* OR training*)):ti,ab,kw) OR (('lifestyle'/exp OR 'exercise'/exp OR 'physical activity'/de OR (('physical*' NEAR/3 activit*):ti,ab,kw) OR 'exercis*':ti,ab,kw OR nutrition*:ti,ab,kw OR 'diet*':ti,ab,kw) AND (intervention*:ti,ab,kw OR program*:ti,ab,kw OR promot*:ti,ab,kw OR advic*:ti,ab,kw)) |
1569508 |
|
#3 |
#1 AND #2 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab,kw OR child*:ti,ab,kw OR schoolchild*:ti,ab,kw OR infant*:ti,ab,kw OR girl*:ti,ab,kw OR boy*:ti,ab,kw OR teen:ti,ab,kw OR teens:ti,ab,kw OR teenager*:ti,ab,kw OR youth*:ti,ab,kw OR pediatr*:ti,ab,kw OR paediatr*:ti,ab,kw OR puber*:ti,ab,kw) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab,kw OR man:ti,ab,kw OR men:ti,ab,kw OR woman:ti,ab,kw OR women:ti,ab,kw)) |
2971 |
|
#4 |
#3 AND [2010-2024]/py |
2796 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1054862 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4091782 |
|
#7 |
#4 AND #5 - SR |
613 |
|
#8 |
#4 AND #6 NOT #7 - RCT |
838 |
|
#9 |
#7 OR #8 |
1451 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
Cognitive Dysfunction/ or 'mild cognitive impair*'.ti,ab,kf. or mci.ti,ab,kf. or ('cognitive impair*' adj3 ('no dement*' or 'without dement*' or 'not dement*')).ti,ab,kf. or cind.ti,ab,kf. or vcind.ti,ab,kf. |
65123 |
|
2 |
exp Diet/ or exp Nutrition Therapy/ or exp Dietary Supplements/ or exp Exercise Therapy/ or (('life style*' or lifestyle*) adj3 (modificat* or chang* or intervention* or promot*)).ti,ab,kf. or ((diet* or 'food*' or nutrition*) adj3 ('intervention*' or 'therap*' or 'treatment*' or 'advic*' or 'additive*' or supplement* or formula*)).ti,ab,kf. or ((oral or multivitamin* or vitamin*) adj3 supplement*).ti,ab,kf. or (('physical*' or movement or activit*) adj3 (exercis* or intervention* or program* or promot* or advic* or training*)).ti,ab,kf. or (exercis* adj3 (therap* or treatment* or intervention* or program* or promot* or advic* or training*)).ti,ab,kf. or ((exp Life Style/ or exp Healthy Lifestyle/ or exp Exercise/ or ('physical*' adj3 activit*).ti,ab,kf. or 'exercis*'.ti,ab,kf. or nutrition*.ti,ab,kf. or 'diet*'.ti,ab,kf.) and (intervention* or program* or promot* or advic*).ti,ab,kf.) |
1057664 |
|
3 |
(1 and 2) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) not ((Adolescent/ or Child/ or Infant/ or adolescen*.ti,ab,kf. or child*.ti,ab,kf. or schoolchild*.ti,ab,kf. or infant*.ti,ab,kf. or girl*.ti,ab,kf. or boy*.ti,ab,kf. or teen.ti,ab,kf. or teens.ti,ab,kf. or teenager*.ti,ab,kf. or youth*.ti,ab,kf. or pediatr*.ti,ab,kf. or paediatr*.ti,ab,kf. or puber*.ti,ab,kf.) not (Adult/ or adult*.ti,ab,kf. or man.ti,ab,kf. or men.ti,ab,kf. or woman.ti,ab,kf. or women.ti,ab,kf.)) |
3461 |
|
4 |
limit 3 to yr="2010 -Current" |
3362 |
|
5 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
768920 |
|
6 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2766837 |
|
7 |
4 and 5 - SR |
611 |
|
8 |
(4 and 6) not 7 - RCT |
1051 |
|
9 |
7 or 8 |
1662 |