Toediening van Botulinetoxine
Uitgangsvraag
Welke methode van injecteren verdient de voorkeur bij het toedienen van botulinetoxine door middel van intramusculaire injecties bij patiënten met cerebrale en/of spinale spasticiteit?
Aanbeveling
Gebruik bij voorkeur echografie voor de plaatsbepaling van injecties met botulinetoxine in spastische spieren bij patiënten met cerebrale en/of spinale spasticiteit.
Plaatsbepaling door elektrostimulatie kan ook worden overwogen, indien hiermee ervaring bestaat, en er geen beschikbaarheid is van een echoapparaat.
Gebruik een combinatie van echografie en elektrostimulatie:
- Bij moeilijke visualisatie van de injectieplaats (bijv. diep gelegen spieren, morfologische veranderingen van spier- en bindweefsel, of subcutaan vocht).
- Bij een hoog-selectieve behandeling waarbij het nodig is dat met elektrostimulatie de juiste injectieplaats wordt bevestigd (bijv. de flexoren van een specifieke vinger).
- Als specifiek ‘neuromuscular junctions’ worden getarget om het aantal injecties en de dosering zo laag mogelijk te houden. Hiervoor bestaat echter nog beperkt bewijs.
- Wanneer de behandelaar nog relatief weinig ervaring heeft met alleen echogeleid injecteren.
Gebruik van de palpatoire techniek (op basis van landmarks) wordt in het algemeen afgeraden, tenzij onder omstandigheden dat er geen betere localisatietechniek beschikbaar is en de betreffende doelspieren goed kunnen worden geïdentificeerd.
Overwegingen
Balans tussen gewenste en ongewenste effecten
Met betrekking tot de uitkomstmaten accuratesse en spasticiteit (modified Ashworth scale, MAS) lijkt het wenselijker om een begeleidende techniek toe te passen voor de plaatsbepaling van de injectie. Hierbij lijken echografie en elektrostimulatie gelijkwaardige opties, die de voorkeur verdienen boven elektromyografie. Ook voor de uitkomstmaat lopen lijken echografie en elektrostimulatie even goed. De overall kwaliteit van bewijs is laag. Dit betekent dat we beperkt zeker zijn over het gevonden geschatte effect van de cruciale uitkomstmaten (accuratesse van injectie). Er is afgewaardeerd vanwege risico op bias omdat blindering onvoldoende is, en vanwege imprecisie, omdat de conclusie wat betreft accuratesse gebaseerd is op een enkele studie met een beperkte hoeveelheid patiënten.
Naast de gegevens uit de geselecteerde literatuur zijn ook praktijkervaringen met de verschillende injectietechnieken van belang.
Voor- en nadelen van elektrostimulatie
Bij gebruik van elektrostimulatie kan het voorkomen dat de doelspier niet gestimuleerd kan worden, terwijl men toch in de goede spier zit. Een eenduidige verklaring hiervoor is er niet, maar het komt in de praktijk vaker voor bij een hoge rusttonus van de te behandelen spier. Ook kan er sprake zijn van morfologische verandering van de spier zoals atrofie, vervetting en/of verbindweefseling, waardoor de prikkelbaarheid van de spier afneemt. Ook kunnen artrogene en/of capsulogene contracturen ertoe leiden dat er geen gewenste (selectieve) beweging plaatsvindt in de extremiteit die nodig is om de juiste locatie vast te stellen. Een voordeel van elektrostimulatie is dat men met een lage stroomsterkte kan zoeken naar een locatie met relatief veel “neuromuscular junctions” (NMJ’s) (zie verder).
Voor- en nadelen van echografie
Gebruik van echografie maakt het mogelijk om het verloop van de te behandelen spier te bekijken voorafgaand aan het injecteren. De optimale injectieplaats binnen de doelspier kan geselecteerd worden, omdat (beduidende) morfologische veranderingen van (een gedeelte van) de spier worden herkend, zoals vervetting en verbindweefseling. Het injecteren van botulinetoxine in morfologisch sterk veranderde spieren is waarschijnlijk minder zinvol; een injectieplek kan worden gekozen met de minste morfologische veranderingen. Aanvullend kan de injectieplaats bepaald worden op basis van anatomische kennis over de verdeling van NMJ’s. Ook kan met echografie tevoren worden vastgesteld welke type naald men nodig heeft om doelspieren te bereiken, zodat een zo klein mogelijke naald kan worden gekozen.
De zichtbaarheid van de naald op echografie kan ook juist verminderd zijn door deze morfologische veranderingen, of door veranderingen op subcutaan niveau zoals vochtcollecties. Ook bij dieper gelegen spieren (>8 cm diepte), zoals de m. piriformis of m.psoas bij dorsolaterale benadering, is met echografie het uiteinde van de naald moeilijker te zien, en is het dus moeilijker om zeker te zijn dat de injectie in de juiste spier wordt gezet. Bij sterke morfologische afwijkingen of bij diepe locaties is een combinatie van echografie en elektrostimulatie wenselijk.
Bijwerkingen botulinetoxine
Eén van de bijwerkingen, tevens risico’s van toediening van botulinetoxine, is een algemene reactie buiten de behandelde spiergroepen. Het betreft bijvoorbeeld algemene spierzwakte, ademhalings- en slikproblematiek, incontinentie voor urine, en dubbelzien. Dit kan gepaard gaan met verslechtering van functionele mogelijkheden zoals vermindering van sta-, loop- en hand-armvaardigheid. De kans op deze bijwerkingen is bij alle toedieningsvormen vergelijkbaar klein, indien men handelt volgens de regels wat betreft (1) de maximale dosis per behandeling, (2) het voorkómen van intravasale toediening door vóór het injecteren te aspireren, en (3) voorzichtigheid te betrachten bij patiënten met ademhalings-, slik- en continentieproblematiek.
Nieuwe techniek
Uit een studie blijkt dat pijn tijdens de injectie en complicaties ongeveer gelijk zijn tussen echografie en elektrostimulatie (Hauret, 2023). Pijn kan mogelijk gereduceerd worden door het gebruik van een nieuwe techniek, waarbij gericht gezocht wordt naar concentraties van motorische eindplaten (NMJ’s) als optimale injectieplaats door een combinatie van echografie en elektrostimulatie. De injecties worden gezet nabij de NMJ’s, indien met lage stroomsterktes een sterke bewegingsuitslag wordt gevonden in de betreffende spier. Eén studie suggereert dat men kan volstaan met één injectie, met bovendien kleinere hoeveelheden botulinetoxine, om hetzelfde effect van behandeling te bewerkstelligen als wanneer bijvoorbeeld alleen echografie wordt gebruikt (Rekand, 2019). Deze veronderstelling lijkt logisch, maar behoeft nadere wetenschappelijke bevestiging.
Subgroepen
Hoewel elektrostimulatie en echografie ongeveer even accuraat lijken voor het bepalen van de injectieplaats, is de ervaring dat met name bij bepaalde patiëntgroepen (zoals dwarslaesiepatiënten en patiënten met hereditaire spastische paraparese) elektrostimulatie tijdens de behandeling tot plotselinge pijnlijke toename van tonus en clonus van de gestimuleerde spier kan leiden. Voor hen lijkt echografie de voorkeur te hebben.
Bij een gerichte hoog selectieve behandeling van de flexoren van een bepaalde vinger, heeft juist een combinatie van echografie en elektrostimulatie een grote meerwaarde. Met behulp van echografie kan de doelspier goed en snel opgezocht worden, waarna met behulp van elektrostimulatie de bij een bepaalde vinger behorende spiervezels beter gelokaliseerd kunnen worden.
Waarden en voorkeuren van patiënten (en eventueel hun naasten/verzorgers)
Bij het overwegen van de techniek voor injecteren, zijn 3 uitgangspunten belangrijk:
- Een zo kort mogelijke behandeling.
- Een zo pijnvrij mogelijke behandeling.
- De kans op het beste effect/zekerheid van effect.
Een zo kort mogelijke behandeling: Bij echografie geleid injecteren zijn deze 3 factoren gunstiger dan bij elektrostimulatie. De snelheid van de behandeling wordt bij alle injectietechnieken bepaald door meerdere factoren, waaronder de ervaring van de behandelaar met de gebruikte injectietechniek en de accuratesse van het handelen. Uit één studie blijkt dat injecties bij echografie sneller gezet kunnen worden dan bij elektrostimulatie (Hauret, 2023).
Een zo pijnvrij mogelijke behandeling: Injecteren onder elektrostimulatie kan pijnlijk zijn. Elektrostimulatie op zich kan pijnsensatie geven, maar ook de spiercontracties die door de elektrostimulatie worden opgewekt. Bij het gebruik van echogeleiding is er visuele controle van het positioneren van de naald, waardoor de kans op (pijnlijke) lokale complicaties, zoals iatrogeen vaat- of zenuwletsel, het kleinst is ten opzichte van andere methoden.
De kans op het beste effect: Het effect van de behandeling en mogelijk de duur ervan is afhankelijk van de accuratesse van de toediening en de juiste dosering van botulinetoxine. Van groot belang is het voorafgaand specialistisch onderzoek gericht op het herkennen van de bij een spastisch patroon betrokken spiergroepen en het opstellen van een behandelplan. Echografie kan, in tegenstelling tot palpatie en elektrostimulatie, bijdragen aan het opstellen van een behandelplan, omdat een hypertone spier soms herkenbaar is door een ronde, gecontraheerde vorm, die door uitwendige druk niet goed te veranderen is. Dit wordt sono-elastografie genoemd en is een gevalideerd meetinstrument. Ook kan een clonus zichtbaar zijn, evenals spontane contracties (bijv. myoclonieën) wat een aanwijzing is voor welke spier daadwerkelijk betrokken is bij het patroon. De mate van morfologische veranderingen van het spierweefsel wordt bepaald door middel van Heckmatt schaal.
Een ander voordeel van echografie boven elektrostimulatie of EMG, is dat de patiënt zelf kan meekijken bij de behandeling, en daardoor actief betrokken wordt. De zorgverlener kan de spierlagen, en het moment van injecteren laten zien, wat een zinvolle interactie met de patiënt geeft.
Kostenaspecten
Injecteren onder echogeleiding kan ten opzichte van elektrostimulatie goedkoper zijn. De kosten van de bij de behandeling gebruikte naalden zijn een bepalende factor hierbij. Bij echogeleide injectietechniek kan gebruik worden gemaakt van gewone naalden terwijl men bij gebruik van elektrostimulatie aangewezen is op het gebruik van (vaak veel duurdere) speciale geïsoleerde naalden met een cuff. Het verschil in naaldkosten kan oplopen tot factor 200. Echter, bij gebruik van speciale echogene naalden tijdens echografie wordt het verschil kleiner. Qua apparatuur zijn een goed echo-apparaat en transducer veel kostbaarder dan een eenvoudig elektrostimulatie-apparaat. Qua ondersteuning is voor beide methodieken evenveel personeel nodig. Tevens kunnen beide technieken zowel poliklinisch als bijv. in een operatiekamer worden gebruikt.
Gelijkheid ((health) equity/equitable)
Het gebruik van echografie of elektrostimulatie voor injecteren van botulinetoxine leidt niet tot een verschil in gezondheidsgelijkheid. In de tweede en derde lijn is meestal geen sprake van toegangsproblematiek wat betreft de kennis, beschikbaarheid van geschoolde behandelaars en de benodigde apparatuur. Bij de behandeling op andere locaties, zoals verpleeghuizen, neemt de consulent/behandelaar de benodigde apparatuur zelf mee.
Aanvaardbaarheid
Ethische aanvaardbaarheid
Echogeleid injecteren, of met behulp van elektrostimulatie, lijkt aanvaardbaar voor de betrokkenen. Er zijn geen ethische bezwaren.
Duurzaamheid
Zowel echografie als elektrostimulatie zorgen voor afvalmateriaal. Bij echo gaat het om een naald en een hoesje (of reinigingsmiddel en schoonmaakdoekje) voor de echokop, bij elektrostimulatie om een naald en een kabeltje. Duurzaamheidsoverwegingen spelen derhalve geen grote rol in de keuze voor echografie of elektrostimulatie.
Haalbaarheid
De belangrijkste overwegingen met betrekking tot haalbaarheid zijn de beschikbaarheid van materiaal (een echoapparaat of elektrostimulatie-apparaat), en adequate scholing van de behandelaars en ondersteunend personeel.
Uit bedrijfstechnisch oogpunt telt de beschikbaarheid en/of aanschafkosten van de benodigde apparatuur. Dit geldt voor beschikbaarheid van een elektrostimulatie-, en/of echoapparaat (zie ook kopje ‘kosten’). Lokale situaties waarbij een apparaat gedeeld wordt met andere vakgroepen kan tot goedkopere oplossingen leiden. Tegenwoordig zijn in bijna elk ziekenhuis meerdere echoapparaten beschikbaar.
Met betrekking tot adequate scholing bestaan er verschillende mogelijkheden voor het opdoen van kennis over sono-anatomie en de toepassing hiervan in het aanleren van echogeleide injectietechnieken. De meest omvattende, aanbevolen scholing voor het aanleren van echogeleid injecteren in Nederland is de POBOT cursus (Boerhave Nascholing, Leiden), die wordt verzorgd door een groep ervaren docenten-revalidatieartsen. Verder worden landelijk en in het buitenland diverse cursussen gegeven gericht op het opdoen van kennis van de sono-anatomie
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Uit de literatuur blijkt dat echografie en elektrostimulatie even accuraat de plaats voor injecties met botulinetoxine kunnen bepalen waar het gaat om het treffen van de juiste doelspieren. Het bijkomende voordeel van echografie is echter dat de spier daadwerkelijk gezien kan worden, tot op ca. 10 cm diepte. Hierdoor kan beter een behandelplan worden opgesteld, dat waarschijnlijk leidt tot een beter effect en minder kans op complicaties. Ook is echografie minder pijnlijk dan elektrostimulatie. Het nadeel van echografie is echter dat het meer vaardigheid vereist, en dat diep gelegen spieren soms niet of minder goed gezien kunnen worden. In die situaties is een combinatie van echografie en elektrostimulatie wenselijk.
Onderbouwing
One of the methods for focal treatment of increased muscle tone or spasticity is intramuscular administration of botulinum toxin (BoNT-A). Currently, four injection techniques are commonly used:
- Using anatomical knowledge, where so-called landmarks play an important role in locating the muscle groups to be treated;
- Locating the muscle groups to be treated with the help of electrostimulation, where a response in the form of movement in the corresponding part of the extremity is the leading indicator;
- Injecting under ultrasound guidance, where ultrasound images are used to locate the muscles to be treated, guide the injection needle, and provide real-time visual confirmation of the accuracy of the injection site by viewing the botulinum toxin depot;
- A combination of ultrasound and electrostimulation.
The question is which of these methods is preferred based on the accuracy of locating the target muscles to be treated, injection accuracy, patient-friendliness, and safety.
Note: BoNT-A treatment under EMG-guidance (electromyography) is not further mentioned or discussed in this module, as it is considered an inappropriate localization technique in the case of spasticity.
1. Technique
|
Low GRADE |
Electrostimulation-guidance and ultrasound for botulinum toxin injections may be more accurate than a manual placement technique, in patients with cerebral or spinal spasticity.
Source: (Picelli, 2012a) |
2. Symptoms
|
Moderate GRADE |
Ultrasound-guidance and electrostimulation-guidance for botulinum toxin injections likely reduce the spasticity (modified Ashworth scale score) more than electromyography-guidance or a manual placement technique, in patients with cerebral or spinal spasticity.
Source: (Asimakidou, 2023) |
3. Functioning
|
Very low GRADE |
The evidence is very uncertain about a differential effect between ultrasound-guidance and electrostimulation for botulinum toxin injections on walking in patients with cerebral spasticity.
Source: (Turna, 2018) |
Description of studies
One network meta-analysis from the search was included in the analysis of the literature. Important study characteristics and results are summarized in table 3. The assessment of the risk of bias is summarized in the risk of bias tables (under the heading ‘Evidence tabellen’).
From the previous version of the module, one study was separately addressed in this revision because it provided information about accuracy of injection; the other relevant RCTs from the previous version of the module were part of the newly included network meta-analysis.
The network meta-analysis by Asimakidou (2023) investigated if guided BoNT injections would lead to a better clinical outcome in adults with limb spasticity compared to non-guided injections. Databases were searched to December 2022. Articles were eligible for inclusion if two or more guidance techniques were compared (electromyography, electrostimulation, manual needle placement and ultrasound), in adults with upper or lower limb spasticity treated with BoNT injections. Six studies were included: five RCTs and one non-randomized trial, totaling 245 participants. See Table 3 for further information of the individual studies included in Asimakidou (2023).
Picelli (2012a) investigated the accuracy of manual needle placement and electrical stimulation guidance for BoNT-A injections into the gastrocnemius. Adult patients with spastic equinus after stroke (>6 months ago) and spasticity of the gastrocnemius of at least 1 on the MAS were included. The accuracy of needle positioning with MNP and ES was compared by measuring positioning with ultrasound: to confirm the needle placement into the targeted muscle and measure muscle thickness. Characteristics of the study are shown in table 3.
Table 3. Characteristics of included studies
|
Study |
Participants |
Comparison |
Follow-up |
Outcomes |
Comments |
Risk of bias* |
|
Included in systematic review Asimakidou, 2023 |
||||||
|
Turna, 2018
Prospective cohort |
N at baseline: Intervention: 20 | Control: 20
Age (mean, SD): I: 51.3 (7.6) | C: 56.2 (5.1) Sex: 58% male
Cause of spasticity: ischemic or hemorrhagic stroke Location: ankle plantar flexors |
Intervention: BoNT-A injections guided by ES
Control: BoNT-A injections guided by US |
2 weeks and 3 months |
Barthel MAS Walking (10m WT) |
No funding was received. Authors reported no conflicts of interests |
High |
|
Zeuner, 2016
Crossover RCT |
N at baseline: Intervention: 24 | Control: 11
Age (mean, SD): I: 58 (13) | C: 52 (15) Sex: 43% male
Cause of spasticity: ischemic or hemorrhagic stroke Location: upper limb |
Intervention: BonT-A injections guided by EMG or US
Control: BoNT-A injections through MNP |
4 weeks |
Barthel MAS |
US equipment provided by Allergan, lecture fees and support received by authors from non-commercial organizations, and several commercial organizations. |
High |
|
Picelli, 2014
Parallel-group RCT |
N at baseline: Intervention: 40 | Control: 20
Age (mean, SD): ES: 60 (16) | US: 64 (12) | C: 65 (11) Sex: 53% male
Cause of spasticity: ischemic or hemorrhagic stroke Location: wrists and fingers |
Intervention: BonT-A injections guided by ES or US
Control: BoNT-A injections through MNP |
4 weeks |
MAS Tardieu
|
No funding received and authors reported no conflicts of interests |
Some concerns |
|
Ploumis, 2013
Parallel-group RCT |
N at baseline: Intervention: 15 | Control: 12
Age (mean, SD): I: 40.3 (15.8) | C: 41.8 (17.8) Sex: 26% male
Cause of spasticity: stroke, traumatic brain injury, spinal cord injury, cerebral palsy, hypoxic encephalopathy Location: upper and lower extremities |
Intervention: BonT-A injections guided by EMG
Control: BoNT-A injections through MNP |
3 weeks and 3 months |
MAS Barthel Index |
Allergan provided injection needle electrode and EMG amplifier freely, but had no influence on data collection or analysis. Authors reported no conflicts of interests |
Low |
|
Picelli, 2012b
Parallel-group RCT |
N at baseline: Intervention: 32 | Control: 15
Age (mean, SD): ES: 55 (17) | US: 61 (12) | C: 63 (14) Sex: 66% male
Cause of spasticity: ischemic or hemorrhagic stroke Location: calf (gastrocnemius for spastic equinus)
|
Intervention: BonT-A injections guided by ES or US
Control: BoNT-A injections through MNP |
4 weeks |
MAS Tardieu |
Authors reported no conflicts of interests. Funding unclear. |
Some concerns |
|
Mayer, 2008
Parallel-group RCT |
N at baseline: Intervention: 18 | Control: 18
Age (mean, SD): I: 37.9 (19.9) | C: 34.7 (21.9) Sex: 50% male
Cause of spasticity: stroke, traumatic brain injury, hypoxic encephalopathy Location: elbow |
Intervention: BoNT-A injections guided by EMG
Control: BoNT-A injections guided by ES |
3 weeks |
Ashworth Tardieu |
Supported by commercial and non-commercial grant. Conflicts of interest not reported. |
High |
|
Individual studies |
||||||
|
Picelli, 2012a
Parallel-group RCT |
N at baseline: Intervention: 39 | Control: 42
Age (mean, SD): overall 59.2 (15.2) Sex: 64% male
Cause of spasticity: ischemic or hemorrhagic stroke Location: calf (gastrocnemius for spastic equinus)
|
Intervention: BonT-A injections guided by ES
Control: BoNT-A injections through MNP |
During injection |
Accuracy of needle placement determined by ultrasound |
Conflicts of interest and funding not reported in study. |
Low |
Results
The results per outcome measure are presented.
1. Technique
1a. Accuracy of injection
One study described accuracy of injection (Picelli, 2012a). Accuracy of needle placement (in terms of percentage of injections in the right target muscle) for MNP varied from 64.3% to 92.9%, and for ES from 87.2% to 94.9% (depending on whether the m. gastrocnemius medialis or m. gastrocnemius lateralis was targeted, and whether the proximal or distal site of the muscle was targeted).
In a multivariate logistic model predicting accurate placement, MNP seemed to result in a lower odds of accurate injection compared to ES guidance (OR 0.33; 95% CI 0.16 to 0.67). The m. gastrocnemius medialis was easier to target than the m. gastrocnemius lateralis, regardless of guidance technique.
1b. Duration of injection
None of the included studies reported on the duration of the guidance techniques.
1c. Patient burden
None of the included studies reported on the patient burden of the guidance techniques.
2. Symptoms (clinical outcomes)
2a. Modified Ashworth Scale (MAS)
Asimakidou (2023) determined the hierarchy of guidance techniques based on the difference of means in MAS pre- and post-injection, through a Bayesian network meta-analysis. A SUCRA-score was used (surface under the cumulative ranking curve), indicating the ranking: the closer an intervention is to 100, the more likely this intervention will be top-ranked. Figure 1 shows the change in MAS of EMG, ES and US compared to MNP (depicted as mean differences). The hierarchy was determined to be:
|
Rank |
Guidance technique |
SUCRA |
|
1 |
Ultrasound (US) |
83.40 |
|
2 |
Electrostimulation (ES) |
82.48 |
|
3 |
Electromyography (EMG) |
33.16 |
|
4 |
Manual Needle placement (MNP) |
0.95 |
However, the difference between US and ES was not clinically relevant.
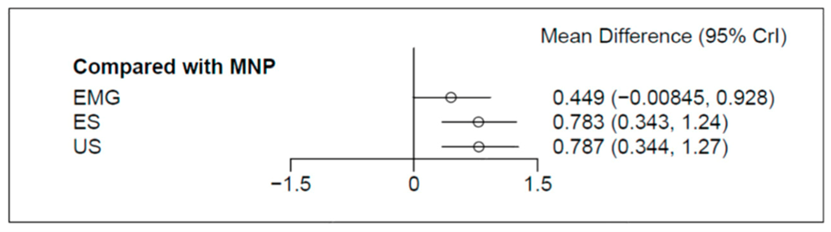
Figure 1. Forest plot of mean difference of change in MAS between different guidance techniques for BoNT-A injection (From: Asimakidou, 2023)
2b. Tardieu
Concerning outcomes on the Tardieu scale, the review by Asimakidou (2023) reported only qualitatively the results, because Tardieu was reported differently in the individual included studies; as degrees or scores 0-4.

2c. Effect duration
The effect duration of BoNT-A per guidance technique was not reported in the included studies.
3. Functioning
3a. Walking
Only the comparison between ES-guided injections and US-guided injections was reported, in the study by Turna (2018), who reported the results from the 10-meter walking test (10mWT). In both groups, the average walking speed increased with 0.08 m/s after 2 weeks of treatment.
3b. Barthel Index
Concerning outcomes on the Barthel index, the review by Asimakidou (2023) reported:

Evidence of the literature
The level of evidence started at high, because it was based on RCTs.
1. Technique
The level of evidence was downgraded:
- 1a. Accuracy of injection: by 2 levels because of risk of bias (no blinding of outcome assessor) and imprecision (single study with low number of patients) (to Low).
- 1b. Duration of injection: as no studies were found, no GRADE assessment was performed
- 1c. Patient burden: as no studies were found, no GRADE assessment was performed
2. Symptoms
The level of evidence was downgraded:
- 2a. Modified Ashworth Scale (MAS): by 2 levels because of risk of bias (no blinding in all studies, some studies with serious randomization issues – see risk of bias table)) (to Moderate). No downgrading took place for inconsistency, indirectness, publication bias, intransitivity or incoherence.
- 2b. Tardieu index: the results from the study by Asimakidou (2023) are presented qualitatively. Therefore, no GRADE assessment can be performed.
- 2c. Effect duration: as no studies were found, no GRADE assessment was performed.
3. Functioning
- 3a. Walking: by 3 levels due to risk of bias (unclear randomization, no blinding) and imprecision (confidence interval crosses both borders of clinical relevance, single study with low number of included patients) (to Very low)
- 3b. Barthel index: the results from the study by Asimakidou (2023) are presented qualitatively. Therefore, no GRADE assessment can be performed.
A systematic review of the literature was performed to answer the following question(s):
Which injection technique for administering botulinum toxin is most accurate compared to administering botulinum toxin based on landmarks and palpation?
| Patients | Adult patients with cerebral or spinal spasticity |
| Intervention | Different methods for intramuscular injection of botulinum toxin (using electrostimulation, ultrasound, or a combination) |
| Control |
Palpation or other methods to determine the injection site of botulinum toxin (BoNT-A) |
| Outcomes |
Technique: accuracy of injection, duration of injection procedure, patient burden, patient safety and risk of complications and/or risk of iatrogenic (nerve) injury Symptoms: muscle tone (e.g. modified Ashworth scale, Tardieu score) and duration of effects Functioning: e.g. walking, Barthel Index |
| Other selection criteria |
Study design: systematic reviews, randomized controlled trials, and observational studies Minimal follow-up: 3-6 weeks after botulinum toxin injection |
Relevant outcome measures
The working group considered accuracy of injection and effect on muscle tone as critical outcome measures for decision making; and the other outcome measures (duration of injection, patient burden, duration of effect and effects on skills and abilities) as important outcome measures for decision making.
The guideline panel defined the outcome measures as shown in table 2.
Table 2. Definitions and minimal clinically important differences for assessed outcome measures
|
Outcome units |
Outcome measures |
Definition |
Minimal clinically important difference |
|
Technique |
Accuracy of injection |
Confirmation by ultrasound or professional conviction that the injection is placed in de right muscle |
Not applicable |
|
Duration of injection procedure |
Amount of time injection takes, including the localization technique |
Not applicable |
|
|
Patient burden |
measured with Visual Analog Scale, or Numeric (Pain) Rating Scale |
1.65 point difference (scale 0 to 10) or 16.55 (scale 0 to 100) |
|
|
Effects on body functions and structures (ICF-impairments) |
Muscle tone/ spasticity |
measured with the (modified) Ashworth scale (AS) or (modified) Tardieu scale (TS) |
0.25 point on the (m)AS if ultrasound, electrostimulation and/ or EMG compared to palpation or using anatomical landmarks* |
|
Effects on skills and abilities (ICF-activities) |
Arm function |
Measured with Action Research Arm Test (ARAT) or 9HPT (9-hole peg test) |
5.7 points on the ARAT (Lang, 2008) and 20% in test score for the 9HPT (Feys, 2017) |
|
Gait pattern and gait speed (walking) |
measured with 10-meter walking test (10MWT), 6-min WT, |
0.1 m/s gait speed difference for 10-meter WT; 54 meter difference for 6MWT (Wise, 2005) |
|
|
Standing and balance |
Berg Balance Scale (or other) |
6 points on Berg Balance Scale |
|
|
Activities of Daily Living (ADL) |
for example using Barthel Index, including social functioning |
Barthel Index: 1.85 points (scale 0-20) (Hsieh, 2007) |
|
|
Duration of effect |
After which period of time the effect of the intervention wears off |
not applicable |
|
|
Adverse events and patient safety |
Considered of specific interest were complications related to the injection and iatrogenic nerve injury. |
not applicable |
|
*Different from Glossary, specific for this module
Search and select (Methods)
The previous guideline module on this topic has been revised, in which the evidence and literature previously assessed has been reassessed for the formulated PICO, and supplemented with newer literature. The process for the search and selection of the new literature is described below.
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from the last revision of the module (September 2015) until April 19th, 2024. The detailed search strategy is available upon request. The systematic literature search resulted in 192 hits. Studies were selected based on the following criteria:
- Adult patients with cerebral or spinal spasticity.
- Comparing different (guidance of) injection techniques of botulinum toxin (BoNT-A).
Initially, seven studies were selected based on title and abstract screening. After reading the full text, six studies were excluded (see the exclusion table under the heading ‘Evidence tabellen’), and one study was included (in addition to one study from the previous version of the module).
- Asimakidou E, Sidiropoulos C. A Bayesian Network Meta-Analysis and Systematic Review of Guidance Techniques in Botulinum Toxin Injections and Their Hierarchy in the Treatment of Limb Spasticity. Toxins (Basel). 2023 Mar 31;15(4):256. doi: 10.3390/toxins15040256. PMID: 37104194; PMCID: PMC10145352.
- Hauret I, Dobija L, Givron P, Goldstein A, Pereira B, Coudeyre E. Effectiveness of Ultrasound-guided VS Electrical-stimulation-guided Botulinum Toxin Injections in Triceps Surae Spasticity after Stroke: A Randomized Controlled Study. J Rehabil Med. 2023 Jul 11;55:jrm11963. doi: 10.2340/jrm.v55.11963. PMID: 37434519; PMCID: PMC10358278.
- Mayer NH, Whyte J, Wannstedt G, Ellis CA. Comparative impact of 2 botulinum toxin injection techniques for elbow flexor hypertonia. Arch Phys Med Rehabil. 2008 May;89(5):982-7. doi: 10.1016/j.apmr.2007.10.022. PMID: 18452749.
- Picelli A, Bonetti P, Fontana C, Barausse M, Dambruoso F, Gajofatto F, Tamburin S, Girardi P, Gimigliano R, Smania N. Accuracy of botulinum toxin type A injection into the gastrocnemius muscle of adults with spastic equinus: manual needle placement and electrical stimulation guidance compared using ultrasonography. J Rehabil Med. 2012a May;44(5):450-2. doi: 10.2340/16501977-0970. PMID: 22549655.
- Picelli A, Tamburin S, Bonetti P, Fontana C, Barausse M, Dambruoso F, Gajofatto F, Santilli V, Smania N. Botulinum toxin type A injection into the gastrocnemius muscle for spastic equinus in adults with stroke: a randomized controlled trial comparing manual needle placement, electrical stimulation and ultrasonography-guided injection techniques. Am J Phys Med Rehabil. 2012b Nov;91(11):957-64. doi: 10.1097/PHM.0b013e318269d7f3. PMID: 23085706.
- Picelli A, Lobba D, Midiri A, Prandi P, Melotti C, Baldessarelli S, Smania N. Botulinum toxin injection into the forearm muscles for wrist and fingers spastic overactivity in adults with chronic stroke: a randomized controlled trial comparing three injection techniques. Clin Rehabil. 2014 Mar;28(3):232-42. doi: 10.1177/0269215513497735. Epub 2013 Aug 14. PMID: 23945164.
- Ploumis A, Varvarousis D, Konitsiotis S, Beris A. Effectiveness of botulinum toxin injection with and without needle electromyographic guidance for the treatment of spasticity in hemiplegic patients: a randomized controlled trial. Disabil Rehabil. 2014;36(4):313-8. doi: 10.3109/09638288.2013.791727. Epub 2013 May 14. PMID: 23672209.
- Turna IF, Erhan B, Gunduz NB, Turna O. The effects of different injection techniques of botulinum toxin a in post-stroke patients with plantar flexor spasticity. Acta Neurol Belg. 2020 Jun;120(3):639-643. doi: 10.1007/s13760-018-0969-x. Epub 2018 Jul 5. PMID: 29978276.
- Zeuner KE, Knutzen A, Kühl C, Möller B, Hellriegel H, Margraf NG, Deuschl G, Stolze H. Functional impact of different muscle localization techniques for Botulinum neurotoxin A injections in clinical routine management of post-stroke spasticity. Brain Inj. 2017;31(1):75-82. doi: 10.1080/02699052.2016.1218545. Epub 2016 Nov 23. PMID: 27880052.
Risk of Bias tables
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated? |
Was the allocation adequately concealed? |
Blinding: Was knowledge of the allocated interventions adequately prevented? Blinding of (1) patients, (2) healthcare providers, (3) data collectors, (4) outcome assessors, (5) data analysts?
|
Was loss to follow-up (missing outcome data) infrequent?
|
Are reports of the study free of selective outcome reporting?
|
Was the study apparently free of other problems that could put it at a risk of bias?
|
Overall risk of bias If applicable/necessary, per outcome measure
|
|
|
|
Definitely yes Probably yes Probably no Definitely no |
Definitely yes Probably yes Probably no Definitely no |
Definitely yes Probably yes Probably no Definitely no |
Definitely yes Probably yes Probably no Definitely no |
Definitely yes Probably yes Probably no Definitely no |
Definitely yes Probably yes Probably no Definitely no |
LOW Some concerns HIGH
|
|
|
Turna, 2018 |
Definitely no
Reason: divided according to the order of admission to the hospital |
Definitely no
Reason: no adequate randomization procedure |
Definitely no
Reason: no blinding described. |
Probably yes
Reason: no loss to follow-up |
Definitely yes;
Reason: All relevant outcomes were reported |
Unclear
Reason: very little text is provided. |
High
|
|
|
Zeuner, 2016 |
Unclear
Reason: randomization procedure not described |
Unclear
Reason: randomization procedure not described |
Definitely no
Reason: only examiner was blinded; patients and caregivers were not. |
Definitely no
Reason: 23% loss to follow-up, no imputation methods used |
Probably yes
Reason: all relevant outcome measures from methods were reported. Research protocol not available. |
Probably no
Reason: Study did not include number of patients from sample size calculation |
High
|
|
|
Picelli, 2014 |
Probably yes
Reason: allocation using a restricted randomization scheme generated by software |
Definitely no
Reason: one of the investigators checked correct patient allocation according to the randomization list |
Definitely no
Reason: only examiner was blinded; patients and caregivers were not. |
Definitely yes
Reason: no loss to follow-up |
Probably yes
Reason: all relevant outcome measures from methods were reported. Research protocol not available. |
Probably no
Reason: single “injector” was used; injectors skilled in each technique would prevent bias of personal skills |
Some concerns
|
|
|
Ploumis, 2013 |
Unclear
Reason: numbered series of pre-filled envelopes, unclear how series were generated |
Definitely yes
Reason: pre-filled closed envelopes with numbered series specifying the group |
Definitely no
Reason: only examiner was blinded; patients and caregivers were not. |
Definitely yes
Reason: no loss to follow-up |
Probably yes
Reason: all relevant outcome measures from methods were reported. Research protocol not available |
Probably no
Reason: single “injector” was used; injectors skilled in each technique would prevent bias of personal skills |
Low
|
|
|
Picelli, 2012b |
Probably yes
Reason: allocation using a simple randomization scheme generated by software |
Definitely no
Reason: one of the investigators checked correct patient allocation according to the randomization list |
Definitely no
Reason: only examiner was blinded; patients and caregivers were not. |
Probably yes
Reason: Loss to follow-up was infrequent both groups. No imputation methods were used. |
Probably yes
Reason: all relevant outcome measures from methods were reported. Research protocol not available. |
Probably yes
Reason: No other problems noted |
Some concerns:
|
|
|
Mayer, 2008 |
Probably no
Reason: randomization procedure not described |
Probably no
Reason: randomization procedure not described |
Definitely no
Reason: only examiner was blinded; patients and caregivers were not. |
Unclear
Reason: unclear how many patients were eligible for inclusion |
Probably yes
Reason: all relevant outcome measures from methods were reported. Research protocol not available |
Probably yes
Reason: No other problems noted |
High:
|
|
|
Picelli, 2012a |
Definitely yes
Reason: Software-generated randomization scheme. |
Unclear
Reason: no further information on randomization provided |
Definitely no
Reason: patient, care giver, outcome assessor not blinded. |
Definitely yes
Reason: no loss to follow-up (outcome immediately measured) |
Probably yes
Reason: all relevant outcome measures from methods were reported. Research protocol not available |
Probably yes
Reason: no other problems noted, though overfitting of the multivariate model |
Low
|
|
* No downgrading for intransitivity of Asimakidou (2023) took place, as the authors report: Substantial heterogeneity across the studies was not identified, neither in technical parameters (such as volume, dilution and injection sites) nor in clinical characteristics. To ensure transitivity, probable effect modifiers were critically appraised. The effect of some divergencies in individual studies, in terms of study design, utilized assessment scale and age of eligible participants, was checked in the sensitivity analyses but no major alterations were detected
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Rekand T, Biering-Sörensen B, He J, Vilholm OJ, Christensen PB, Ulfarsson T, Belusa R, Ström T, Myrenfors P, Maisonobe P, Dalager T. Botulinum toxin treatment of spasticity targeted to muscle endplates: an international, randomised, evaluator-blinded study comparing two different botulinum toxin injection strategies for the treatment of upper limb spasticity. BMJ Open. 2019 May 5;9(5):e024340. doi: 10.1136/bmjopen-2018-024340. PMID: 31061021; PMCID: PMC6502046. |
Wrong comparison between I and C |
|
Grigoriu AI, Dinomais M, Rémy-Néris O, Brochard S. Impact of Injection-Guiding Techniques on the Effectiveness of Botulinum Toxin for the Treatment of Focal Spasticity and Dystonia: A Systematic Review. Arch Phys Med Rehabil. 2015 Nov;96(11):2067-78.e1. doi: 10.1016/j.apmr.2015.05.002. Epub 2015 May 14. PMID: 25982240. |
More recent SR available (Asimakidou, 2023) with same included studies |
|
Hauret I, Dobija L, Givron P, Goldstein A, Pereira B, Coudeyre E. Effectiveness of Ultrasound-guided VS Electrical-stimulation-guided Botulinum Toxin Injections in Triceps Surae Spasticity after Stroke: A Randomized Controlled Study. J Rehabil Med. 2023 Jul 11;55:jrm11963. doi: 10.2340/jrm.v55.11963. PMID: 37434519; PMCID: PMC10358278. |
Outcomes unclear for analysis |
|
Turna IF, Erhan B, Gunduz NB, Turna O. The effects of different injection techniques of botulinum toxin a in post-stroke patients with plantar flexor spasticity. Acta Neurol Belg. 2020 Jun;120(3):639-643. doi: 10.1007/s13760-018-0969-x. Epub 2018 Jul 5. PMID: 29978276. |
Study already included in review van Asimakidou 2023 (which is included)
|
|
Zhang C, Chen YT, Liu Y, Magat E, Gutierrez-Verduzco M, Francisco GE, Zhou P, Li S, Zhang Y. Improving Botulinum Toxin Efficiency in Treating Post-Stroke Spasticity Using 3D Innervation Zone Imaging. Int J Neural Syst. 2021 Apr;31(4):2150007. doi: 10.1142/S0129065721500076. Epub 2021 Jan 12. PMID: 33438529. |
Wrong intervention (3DIZI-guided injections) |
|
Chen HX, Wang W, Xiao HQ, Wang H, Ding XD. Ultrasound-guided botulinum toxin injections and EMG biofeedback therapy the lower limb muscle spasm after cerebral infarction. Eur Rev Med Pharmacol Sci. 2015;19(9):1696-9. PMID: 26004611. |
No RCT. |
Beoordelingsdatum en geldigheid
Publicatiedatum : 06-01-2026
Beoordeeld op geldigheid : 06-01-2026
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met Cerebrale en/of spinale spasticiteit.
Werkgroep
- prof. dr. A.C.H. Geurts (voorzitter), hoogleraar neurorevalidatie, Radboud UMC en Sint Maartenskliniek, namens de Nederlandse Vereniging voor Revalidatieartsen
- drs. A.M.V. Dommisse, revalidatiearts, Isala Klinieken Zwolle, namens de Nederlandse Vereniging voor Revalidatieartsen
- drs. P.J. van Dongen, patiëntvertegenwoordiger bij Hersenletsel.nl
- Dr. M. van Eijk, specialist ouderengeneeskunde, Marnix Medisch B.V., namens Verenso
- dr. J.F.M. Fleuren, revalidatiearts, Jeroen Bosch Ziekenhuis / Tolbrug, ‘s Hertogenbosch, namens de Nederlandse Vereniging voor Revalidatieartsen
- F. van Gorp-Swart, MSc, ziekenhuisapotheker, Diakonessenhuis, Utrecht/Zeist/Doorn, namens de Nederlandse Vereniging voor Ziekenhuisapothekers
- prof. dr. G. Kwakkel, hoogleraar neurorevalidatie, Amsterdam UMC, Amsterdam, namens het Koninklijk Nederlands Genootschap voor Fysiotherapie
- drs. E. Kurt, neurochirurg, Radboud UMC en Canisius Wilhelmina Ziekenhuis, Nijmegen, namens de Nederlandse Vereniging voor Neurochirurgie
- Prof. dr. C.G.M. Meskers, hoogleraar revalidatiegeneeskunde, Amsterdam UMC, Amsterdam, namens de Nederlandse Vereniging voor Revalidatieartsen
- dr. H.A. Moser, anesthesioloog, Radboud UMC, Nijmegen en Care4homecare, Bladel, namens de Nederlandse Vereniging voor Anesthesiologie
- drs. W.P. Polomski, revalidatiearts (gepensioneerd), voorheen in Spaarne Gasthuis, Hoofddorp, namens de Nederlandse Vereniging voor Revalidatieartsen
- drs. M.N. Ruissen-Eversdijk, ergotherapeut en bewegingswetenschapper, Reade, Amsterdam, namens Ergotherapie Nederland
- dr. A.V.C.M. Zeegers, orthopedisch chirurg, Medisch Spectrum Twente, Enschede, namens de Nederlandse Orthopaedische Vereniging
- dr. J.M. Zuidam, plastisch chirurg, Erasmus MC, namens de Nederlandse Vereniging voor Plastische Chirurgie
Klankbordgroep
- P.M. van Lamoen, gepensioneerd, namens Dwarslaesieorganisatie Nederland
- M. Pol, Dwarslaesie Organisatie Nederland, tot september 2024*
- Dr. A.E. Tigchelaar, Dwarslaesie Organisatie Nederland, vanaf september 2024
- Dr. W.J. Kruithof, revalidatiearts, Universitair Medisch Centrum Utrecht
- Dr. I.H. Zaal-Schuller, arts verstandelijk gehandicapten/kaderarts palliatieve zorg
*Overleden
Met ondersteuning van
- Dr. M.L. Molag, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. M.M.J. van Rooijen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Geurts (voorzitter) |
Hoogleraar neurorevalidatie, Radboud UMC, Nijmegen en Sint Maartenskliniek |
|
Geen. |
Geen restricties. |
|
Dommisse |
Revalidatiearts, Vogellanden |
Geen |
Speakerfee bij Ipsen farmaceutica voor:
|
Geen restricties; e-learning en presentaties betreffen de volle breedte van de behandel opties |
|
van Dongen |
Patiëntvertegenwoordiger Hersenletsel.nl |
Deelname andere werkgroepen |
Geen |
Geen restricties. |
|
van Eijk |
Specialist Ouderengeneeskunde, Marnix Medisch B.V |
|
Extern gefinancierd onderzoek over heupfracturen: 1. FITHIP; onderzoek naar valangst bij patienten met heupfractuur 2. GR HIP; onderzoek naar herstel na heupfractuur 3. HIPCARE; onderzoek naar herstel en biomarkers bij heupfractuur |
Geen restricties; De webinars waren gericht op samenwerking specialisten ouderengeneeskunde en revalidatieartsen |
|
Fleuren |
Revalidatiearts, Tolbrug |
Bestuurslid VRA (onbetaald) |
Geen. |
Geen restricties. |
|
van Gorp |
Ziekenhuisapotheker |
Lid werkgroep interacties KNMP |
Geen. |
Geen restricties. |
|
Kwakkel |
Hoogleraar neurorevalidatie, Amsterdam UMC, locatie VUMC |
|
Geen |
Geen restricties. |
|
Kurt |
Neurochirurg, Radboud UMC, Nijmegen |
Geen |
Geen |
Geen restricties. |
|
Meskers |
Revalidatiearts, Amsterdam UMC locatie VUMC |
Geen |
Geen. |
Geen restricties. |
|
Moser |
Anesthesioloog, Radboud UMC, Nijmegen en Care4homecare, Bladel |
Geen |
Geen |
Geen restricties. |
|
Polomski |
Revalidatiearts Spaarne Gasthuis (gepensioneerd vanaf 1 mei 2023). |
Geen |
Lid Adviesraad Merz Benelux, raakt niet aan de modules |
Restrictie ten aanzien van besluitvorming met betrekking tot botulinetoxine |
|
Ruissen-Eversdijk |
Ergotherapeut bij Reade Revalidatie. |
Geen. |
Geen. |
Geen restricties. |
|
Zeegers |
Orthopedisch chirurg, Medisch Spectrum Twente, Enschede (tot 1-6-2025), en UMCG (vanaf 1-6-2025) |
|
Geen. |
Geen restricties. |
|
Zuidam |
Plastisch chirurg, Erasmus MC Rotterdam |
Geen. |
Geen. |
Geen restricties. |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door uitnodigen van Hersenletsel.nl en Dwarslaesie Organisatie Nederland (DON) bij de schriftelijke knelpuntenanalyse. DON heeft een enquête bij hun achterban uitgezet, en knelpunten werden meegenomen in het proces. Het verslag van deze enquête is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. In de werkgroep heeft een vertegenwoordiger van Hersenletsel.nl deelgenomen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan Hersenletsel.nl, DON, MS Nederland en Spierziekten Nederland.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase). Uit deze kwalitatieve raming bleek dat er geen grote financiële gevolgen te verwachten zijn.
|
Module |
Uitkomst raming |
Toelichting |
|
Toediening van botulinetoxine |
geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: VRA Behandeling van Cerebrale en/of spinale spasticiteit bij volwassenen |
|
|
Uitgangsvraag/modules: UV12 Welke methode van injecteren verdient de voorkeur bij het toedienen van botulinetoxine door middel van intramusculaire injecties bij patiënten met cerebrale en/of spinale spasticiteit? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 19 april 2024 |
|
Periode: vanaf september 2015 (search vorige versie richtlijn) |
Talen: geen restrictie |
|
Literatuurspecialist: Alies Oost |
Rayyan review: https://rayyan.ai/reviews/1004184 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl:9777/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen: cerebrale en/of spinale spasticiteit botulinetoxine injectietechniek De sleutelartikelen worden gevonden met deze search, m.u.v. het artikel van Kassam et al. (2023) ‘Canadian Physicians’ Use of Intramuscular Botulinum Toxin Injections for Shoulder Spasticity: A National Cross-Sectional Survey’. Deze voldoet niet aan het opgegeven studydesign (SR/ RCT/ observationeel). |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
32 |
11 |
33 |
|
RCT |
82 |
35 |
87 |
|
Observationele studies |
64 |
50 |
72 |
|
Totaal |
178 |
96 |
192* |
*in Rayyan
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
('spinal cord injury'/exp OR 'spine injury'/exp OR 'spinal cord disease'/exp OR 'multiple sclerosis'/exp OR 'brain injury'/exp OR 'head injury'/exp OR 'cerebrovascular disease'/exp OR 'brain hemorrhage'/exp OR 'brain infarction'/exp OR 'intracranial aneurysm'/exp OR 'stroke patient'/exp OR 'cerebral palsy'/exp OR (((spinal OR spine OR head) NEAR/2 (injur* OR trauma*)):ti,ab,kw) OR tbi:ti,ab,kw OR cva:ti,ab,kw OR cvas:ti,ab,kw OR stroke:ti,ab,kw OR poststroke:ti,ab,kw OR (((cerebrovascular OR 'cerebro vascular' OR cerebral OR intracerebral OR cerebellum OR brain OR 'corpus callosum' OR intracranial OR intraventricular OR periventricular OR subarachnoid) NEAR/3 (accident* OR attack* OR infarct* OR insult* OR event* OR diseas* OR injur* OR trauma OR arrest OR failure OR bleed* OR microbleed* OR aneurysm* OR hemorrhage* OR haemorrhage* OR microhemorrhage* OR microhaemorrhage* OR ischemi* OR ischaemi* OR haematoma* OR hematoma* OR thrombo* OR emboli* OR occlus*)):ti,ab,kw) OR palsy:ti,ab,kw OR apoplex*:ti,ab,kw OR encephalorrhagia:ti,ab,kw OR myelopath*:ti,ab,kw OR neuromyelopath*:ti,ab,kw OR (((multiple OR disseminated OR insular OR multiplex) NEAR/2 scleros*):ti,ab,kw)) AND ('spasticity'/exp OR 'spastic paraplegia'/exp OR 'spastic paresis'/exp OR 'muscle spasm'/de OR 'dystonia'/exp OR 'muscle hypertonia'/de OR spastic*:ti,ab,kw OR spasm*:ti,ab,kw OR hypertonia:ti,ab,kw OR dystonia:ti,ab,kw) |
47503 |
|
#2 |
'botulinum toxin'/exp OR 'botulinum toxin a'/exp OR (((botulin* OR onabotulin*) NEAR/3 (toxin* OR neurotoxin* OR a)):ti,ab,kw) OR botox:ti,ab,kw OR bta:ti,ab,kw OR btx:ti,ab,kw OR btxa:ti,ab,kw OR bont:ti,ab,kw OR incobotulinumtoxin*:ti,ab,kw OR onabotulinumtoxin*:ti,ab,kw OR xeomin*:ti,ab,kw OR abobotulinumtoxin*:ti,ab,kw OR dysport:ti,ab,kw |
54349 |
|
#3 |
('electrostimulation'/exp OR 'neuromuscular electrical stimulation'/exp OR 'electromyography'/exp OR ((neuromusc* NEAR/3 stimulat*):ti,ab,kw) OR nmes:ti,ab,kw OR fes:ti,ab,kw OR estim:ti,ab,kw OR electrostimulation:ti,ab,kw OR 'electr* stimulation':ti,ab,kw OR electromyograph*:ti,ab,kw OR 'electr* myograph*':ti,ab,kw OR emg:ti,ab,kw OR semg:ti,ab,kw OR iemg:ti,ab,kw OR 'ultrasound'/exp OR 'ultrasound scanner'/exp OR 'echography'/exp OR ultraso*:ti,ab,kw OR sonograph*:ti,ab,kw OR echograph*:ti,ab,kw OR sonogram*:ti,ab,kw) AND ('intramuscular drug administration'/exp OR 'subcutaneous drug administration'/exp OR 'injection'/exp OR intramuscular:ti,ab,kw OR 'intra muscular':ti,ab,kw OR injection*:ti,ab,kw) OR 'interventional ultrasonography'/exp OR (((ultraso* OR sonogr* OR echo* OR us OR usg OR es OR electr* OR emg OR semg OR iemg) NEAR/4 (guid* OR loca* OR inject*)):ti,ab,kw) OR (((injection OR guid* OR locali* OR tracking) NEAR/3 (technique* OR method*)):ti,ab,kw) OR ((inject* NEAR/3 (accura* OR preci* OR guid*)):ti,ab,kw) |
315464 |
|
#4 |
#1 AND #2 AND #3 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) AND [01-09-2015]/sd |
238 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1020805 |
|
#6 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4014801 |
|
#7 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8181527 |
|
#8 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
15008212 |
|
#9 |
#4 AND #5 - SR |
32 |
|
#10 |
#4 AND #6 NOT #9 - RCT |
82 |
|
#11 |
#4 AND (#7 OR #8) NOT (#9 OR #10) - observationeel |
64 |
|
#12 |
#9 OR #10 OR #11 |
178 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
(exp Spinal Cord Injuries/ or exp Spinal Injuries/ or exp Spinal Cord Diseases/ or exp Multiple Sclerosis/ or exp Brain Injuries/ or Head Injuries, Closed/ or exp Cerebrovascular Disorders/ or exp Stroke/ or exp Intracranial Hemorrhages/ or exp Brain Infarction/ or exp Cerebral Palsy/ or ((spinal or spine or head) adj2 (injur* or trauma*)).ti,ab,kf. or tbi.ti,ab,kf. or cva.ti,ab,kf. or cvas.ti,ab,kf. or stroke.ti,ab,kf. or poststroke.ti,ab,kf. or ((cerebrovascular or 'cerebro vascular' or cerebral or intracerebral or cerebellum or brain or 'corpus callosum' or intracranial or intraventricular or periventricular or subarachnoid) adj3 (accident* or attack* or infarct* or insult* or event* or diseas* or injur* or trauma or arrest or failure or bleed* or microbleed* or aneurysm* or hemorrhage* or haemorrhage* or microhemorrhage* or microhaemorrhage* or ischemi* or ischaemi* or haematoma* or hematoma* or thrombo* or emboli* or occlus*)).ti,ab,kf. or palsy.ti,ab,kf. or apoplex*.ti,ab,kf. or encephalorrhagia.ti,ab,kf. or myelopath*.ti,ab,kf. or neuromyelopath*.ti,ab,kf. or ((multiple or disseminated or insular or multiplex) adj2 scleros*).ti,ab,kf.) and (exp Muscle Spasticity/ or exp Spasm/ or exp Paraparesis, Spastic/ or exp Muscle Hypertonia/ or exp Dystonia/ or spastic*.ti,ab,kf. or spasm*.ti,ab,kf. or (hypertonia or dystonia).ti,ab,kf.) |
24776 |
|
2 |
exp Botulinum Toxins/ or ((botulin* or onabotulin*) adj3 (toxin* or neurotoxin* or a)).ti,ab,kf. or botox.ti,ab,kf. or bta.ti,ab,kf. or btx.ti,ab,kf. or btxa.ti,ab,kf. or bont.ti,ab,kf. or incobotulinumtoxin*.ti,ab,kf. or onabotulinumtoxin*.ti,ab,kf. or xeomin*.ti,ab,kf. or abobotulinumtoxin*.ti,ab,kf. or dysport.ti,ab,kf. |
30500 |
|
3 |
((exp Electric Stimulation/ or exp Electromyography/ or (neuromusc* adj3 stimulat*).ti,ab,kf. or nmes.ti,ab,kf. or fes.ti,ab,kf. or estim.ti,ab,kf. or electrostimulation.ti,ab,kf. or 'electr* stimulation'.ti,ab,kf. or electromyograph*.ti,ab,kf. or 'electr* myograph*'.ti,ab,kf. or emg.ti,ab,kf. or semg.ti,ab,kf. or iemg.ti,ab,kf. or exp Ultrasonography/ or exp Ultrasonics/ or ultraso*.ti,ab,kf. or sonograph*.ti,ab,kf. or echograph*.ti,ab,kf. or sonogram*.ti,ab,kf.) and (exp Injections, Intramuscular/ or exp Injections, Subcutaneous/ or Injections/ or (intramuscular or 'intra muscular' or injection*).ti,ab,kf.)) or Ultrasonography, Interventional/ or ((ultraso* or sonogr* or echo* or us or usg or es or electr* or emg or semg or iemg) adj4 (guid* or loca* or inject*)).ti,ab,kf. or ((injection or guid* or locali* or tracking) adj3 (technique* or method*)).ti,ab,kf. or (inject* adj3 (accura* or preci* or guid*)).ti,ab,kf. |
218809 |
|
4 |
(1 and 2 and 3) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
324 |
|
5 |
4 and 20150901:20240419.(dt). |
142 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
740450 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2714984 |
|
8 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4704189 |
|
9 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5669928 |
|
10 |
5 and 6 - SR |
11 |
|
11 |
(5 and 7) not 10 - RCT |
35 |
|
12 |
(5 and (8 or 9)) not (10 or 11) - observationeel |
50 |
|
13 |
10 or 11 or 12 |
96 |