Passief rekken
Uitgangsvraag
What is the effect of passive stretching in patients with cerebral and/or spinal spasticity?
Aanbeveling
Integreer passieve rekoefeningen (ter behoud van spierlengte en ROM van gewrichten) in de actieve oefentherapie van de individuele patiënt met cerebrale en/of spinale spasticiteit en, zo mogelijk, in zijn/haar dagelijkse routines, en houdt daarbij rekening met individuele patiëntkenmerken en -voorkeuren. Actieve oefentherapie is van belang om de functionaliteit te verbeteren en mogelijke nadelige effecten van spasticiteitbehandeling op spierkracht, functionaliteit en spieruithoudingsvermogen tegen te gaan.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Veiligheid
In de eerdere versie van deze richtlijn is reeds vastgesteld dat actieve oefentherapie in de vorm van spierversterking en functionele training een gunstig effect heeft op spierkracht bij patiënten met spasticiteit. Aanvullend is nu onderzocht wat het effect is van het passief (dynamisch of statisch ) rekken op spiertonus, ROM en functionaliteit. Hiervoor bleek helaas weinig gecontroleerd onderzoek voorhanden. Evenmin kunnen er uitspraken worden gedaan in welke vorm het rekken van spastische spieren het beste gedaan kan worden (statisch of dynamisch) en hoe vaak en lang het rekken, al dan niet gebruikmakend van orthesen, moet worden uitgevoerd, wil het effect hebben op spiertonus of ROM.
De literatuur suggereert dat het passief rekken in welke vorm dan ook en ongeacht de oorzaak van spasticiteit (bijvoorbeeld MS, CVA, dwarslaesie) geen nadelige effecten heeft en veilig kan worden uitgevoerd. Drie kleine studies vonden aanwijzingen voor een afname in spiertonus, echter overall werden geen significante noch klinisch relevante effecten gevonden op spiertonus of ROM bij patiënten met een CVA. Bij patiënten met MS of een dwarslaesie zijn de effecten nog onbekend.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Los van het gebrek aan bewijs voor statisch of dynamisch spierrekken om een verminderde ROM van gewrichten te verbeteren bij volwassenen met cerebrale en/of spinale spasticiteit, is het van belang dat de bewegingsrange van gewrichten behouden blijft door preventief (spastische) spieren te rekken ten behoeve van (behoud van) functionaliteit en kwaliteit van leven. De klinische ervaring leert immers dat spierfuncties, zowel actief als passief, verloren gaan als ze niet meer worden gebruikt. Om deze reden dient passief rekken een vast onderdeel te zijn van de oefentherapie die aan patiënten met cerebrale en/of spinale spasticiteit wordt aangeboden dan wel geadviseerd op basis van zelf-management.
Kosten (middelenbeslag)
De kosten van passief rekken als onderdeel van een uitgebreider oefenprogramma bij een fysiotherapeut / oefentherapeut worden vergoed door de zorgverzekeraar. Echter, de eerste 10 behandeluren worden niet vergoed. Er kan desgewenst wel een chronische indicatie voor fysiotherapie worden voorgeschreven, maar ook dan zullen de eerste tien behandeluren door de patiënt zelf moeten worden betaald. Uiteraard dient het passief rekken zo veel mogelijk op een actieve manier (self-stretching, see introduction) te gebeuren.
Aanvaardbaarheid, haalbaarheid en implementatie
De aanvaardbaarheid en haalbaarheid van oefentherapie hangen sterk af van de ernst van spasticiteit en contractuurvorming, naast de voorkeuren en context van de individuele patiënt. Patiënten zullen spierrekoefeningen gemakkelijker accepteren als ze goed geïnformeerd zijn over het preventieve belang ervan en als ze deze gemakkelijk kunnen inpassen in hun overige oefentherapie of dagelijkse routines. Het is essentieel dat oefentherapeuten gericht op zoek gaan met patiënten naar welke oefeningen het beste werken en tevens haalbaar zijn voor de individuele patiënt in diens situatie. Spierrekken wordt door veel patiënten ervaren als oncomfortabel en saai, terwijl men geen zichtbaar resultaat ervaart. Om deze reden is het verstandig te kijken naar rekoefeningen die gemakkelijk en kortdurend kunnen worden toegepast, geïntegreerd in een actief oefentherapieprogramma.
Onderbouwing
Passive stretching (muscle elongation) is often used with the aim to reduce pain, improve function, maintain or increase the extensibility of soft tissue and joint range of motion (ROM), and normalize muscle tone in subjects with cerebral and/or spinal spasticity. Despite its use in rehabilitation of patients with stroke, MS or SCI, its underlying mechanisms are unclear. Passive stretching may be applied manually by a therapist, by using (serial) splints or molds, or through self-stretching by for example activating the antagonist muscles. There are different forms of passive stretching neuromechanical structures, such as static and dynamic stretching. Both types of stretching primarily aim to increase ROM and reduce muscle tone and secondarily to improve activities.
In this chapter, the effects of passive (i.e., static or dynamic) applied by a therapist will be discussed on muscle tone, ROM and functional abilities. Static stretching is often defined as actively or passively keeping or holding a stretched position for a prolonged period, typically 30 to 90 seconds, while dynamic stretching involves repetitive movements to force a specific muscle group actively to its full ROM. In this chapter, we will focus on the effects of passive stretching, irrespective of type of stretching technique, by lack of evidence between static or dynamic forms of stretching.
In the previous guidelines it has already been shown that exercise therapy in terms of muscle strengthening and functional training within muscle synergies may prevent weakness and support activities, in particular when applied during or after an invasive spasmolytic treatment such as intramuscular injections with botulinum toxin type A (BoNT-A), focal neurolysis or intrathecally administered baclofen. Therefore, the effects of exercise therapy will not be addressed in this module.
Effects on body functions and structures – Muscle tone/ spasticity
|
Very low GRADE |
The evidence is very uncertain about the differential effect of passive stretching on muscle tone when compared to no stretching or standard care in patients with stroke.
Source: Gomez-Cuaresma, 2021 |
Effects on skills and abilities – Range of Motion (ROM)
|
Very low GRADE |
The evidence is very uncertain about the differential effect of passive stretching on passive ROM compared to no stretching or standard care in patients with cerebral stroke.
Source: Gomez-Cuaresma, 2021 |
Effects on body functions and structures – Muscle tone/ spasticity
|
No GRADE |
The evidence is very uncertain about the differential effect of passive stretching on muscle tone when compared to no stretching or standard care in patients with MS.
Source: Ergul, 2022 |
Description of studies – Stroke
Gomez-Cuaresma (2021) conducted a systematic review on patients who had experienced a stroke. The systematic literature search was performed across multiple electronic databases, including Medline/PubMed, CINAHL, Scopus, Cochrane Library, Web of Science, and Physiotherapy Evidence Database (PEDro). Inclusion were based on the PICOS framework:
- Population (P): Patients who had suffered a stroke
- Intervention (I): Passive (static and/or dynamic) stretching
- Comparison (C): Conventional physiotherapy, other interventions, or no intervention
- Outcomes (O): Spasticity, range of motion (ROM), functional assessment in activities of daily living (ADL), motor function, muscle strength and power, gait, fall risk, pain, and neural and mechanical muscular properties
- Study design (S): Randomized controlled trials (RCTs).
Studies involving long-term orthotic device use or combined stretching with other techniques were excluded. The primary outcomes assessed were spasticity (measured using the Modified Ashworth Scale (MAS) and Modified Modified Ashworth Scale (MMAS), and ROM. The methodological quality of the included trials was evaluated using the PEDro scale, with an average score of 5.5, indicating moderate to good study quality.
Description of studies – MS
Ergul (2022) conducted a systematic review on spasticity management in patients with multiple sclerosis. The systematic literature search was performed across several electronic databases, including PubMed, Scopus, Web of Science, Elsevier, ProQuest, Sage Journals, Physiotherapy Evidence Database and the Cochrane Library.
Originally, the systematic review included 10 trials, however, studies investigating pharmacological, BoNT-A interventions, cold therapy and vibration were also included. Only one trial in this systematic review (N=40) specifically investigated the effect of 2 hours weekly passive stretching in a group or by self-management during 4 weeks (Hugos, 2017).
Results
Results – Stroke
1. Effects on body functions and structures – Muscle tone/ spasticity
The meta-analysis by Gomez-Cuaresma (2021) on individuals with stroke found a heterogeneous effect on muscle tone for passive movement using the MAS or MMAS with a standardized mean difference (SMD) of -0.50 (95% CI -1.55 to 0.55). The results showed no detrimental effects of active or passive movement either.
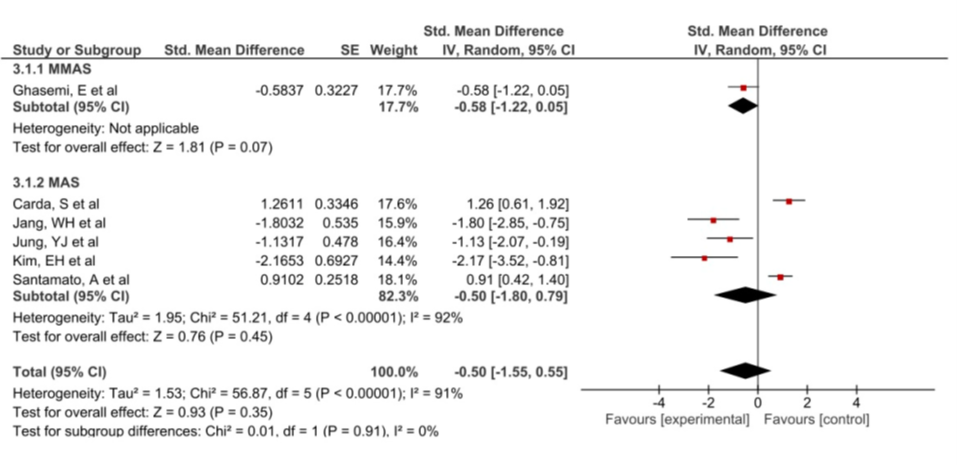
Figure 1. Forest plot comparing the effects of passive movement versus conventional therapy on MAS/MMAS in patients with cerebral spasticity after stroke
2. Effects on skills and abilities
1.1. Range of Motion (ROM)
The meta-analysis by Gomez-Cuaresma (2021) on individuals with stroke included three small sampled trials on passive ROM showing a standardized mean difference of 0.01 (95% CI -0.57 to 0.60).
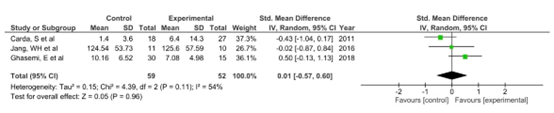
Figure 2. Forest plot comparing passive movement with conventional therapy on ROM in patients with cerebral spasticity after stroke
2.2 Other active functions
No evidence was found for effects on other outcomes such as muscle strength, gait, or basic ADL in the review by Gomez-Cuaresma (2021).
Results – MS
After 4 weeks, no significant effects were found for MAS nor for walking ability. ROM or functional outcomes were not evaluated (Hugos, 2017).
Results – Spinal spasticity
For the effects of passive stretching in patients with spinal cord injury no studies were found that met the inclusion criteria.
Level of evidence of the literature for passive stretching
Stroke
1. Effects on body functions and structures – Muscle tone/ spasticity
The level of evidence regarding muscle tone was downgraded by 3 levels because of limitations in the included study (-1, risk of bias), and because of the confidence intervals crossing the border for statistical and clinical relevance (-2, imprecision).
2. Effects on skills and abilities – Range of Motion (ROM)
The level of evidence regarding the outcome measure Range of Motion (ROM) was downgraded by 3 levels because of study limitations (-1, risk of bias) and broad confidence intervals around the estimates, based on a low number of included patients (-2, imprecision).
MS
1. Effects on body functions and structures – Muscle tone/ spasticity
The level of evidence regarding muscle tone could not be graded as no quantitative data was provided.
A systematic review of the literature was performed to answer the following question: What are the positive and negative effects of passive stretching in patients with cerebral and/or spinal spasticity?
Table 1. PICO
| P: | Patients with cerebral and/or spinal spasticity (including MS, stroke, and spinal cord injury) |
| I: | Passive (static or dynamic) stretching |
| C: | A comparison group without exercise therapy / receiving standard care |
| O: | See outcome measures overview |
Relevant outcome measures
The guideline development group considered effects on spasticity and daily tasks and activities related to reduction of spasticity symptoms as critical outcome measures for decision making.
The working group defined the outcome measures as shown in Table 2.
Table 2. Definitions and minimal clinically important differences for assessed outcome measures.
|
Outcome units |
Outcome measures |
Definition |
Minimal clinically important difference |
|
Effects on body functions and structures (ICF-impairments) |
Muscle tone/ spasticity |
measured with the (modified) Ashworth scale (AS) or (modified) Tardieu scale (TS) |
1 point on the (m)AS, PSFS or (m)TS |
|
Effects on skills and abilities (ICF-activities) |
Range of Motion (ROM) |
Angles or degrees a limb can move. |
10% or more increase in ROM |
|
Arm function |
Measured with Action Research Arm Test (ARAT) or 9HPT (9-hole peg test) |
5.7 points on the ARAT (Lang, 2008) and 20% in test score for the 9HPT (Feys, 2017) |
|
|
Gait pattern and gait speed (walking) |
measured with 10-meter walking test (10MWT), 6-min WT, |
0.1 m/s gait speed difference for 10-meter WT; 54 meter difference for 6MWT (Wise, 2005) |
|
|
Standing and balance |
Berg Balance Scale (or other) |
6 points on Berg Balance Scale |
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2014 until 7 January 2025. The detailed search strategy is available upon request. The systematic literature search resulted in 505 unique hits. Studies were selected based on the following criteria:
- Randomized controlled trial, systematic review and/or meta-analysis.
- Included adults with cerebral or spinal spasticity.
- Passive (static and/or dynamic) stretching as the primary intervention.
- No stretching therapy as the comparative intervention.
- Muscle tone, joint ROM, and/or functional skills and abilities as outcome measures.
Studies involving exercise therapy including muscle strengthening, whole body vibration or robot-assisted training were excluded. Following title and abstract screening, ten studies were initially selected. After full-text review, eight studies were excluded (see the table with reasons for exclusion under the heading Evidence tables), and two studies were included.
Results
Two systematic reviews about stroke and MS were included in the literature analysis.
- Ergul M, Moghadam AN, Soh R. The effectiveness of interventions targeting spasticity in patients with multiple sclerosis: a systematic review of clinical trials. Eur J Physiother 2022; 24 (1):21-29.
- Gomez-Cuaresma L, Lucena-Anton D, Gonzalez-Medina G, Martin-Vega FJ, Galan-Mercant A, Luque-Moreno C. Effectiveness of Stretching in Post-Stroke Spasticity and Range of Motion: Systematic Review and Meta-Analysis. J Pers Med. 2021 Oct 24;11(11):1074. doi: 10.3390/jpm11111074. PMID: 34834426; PMCID: PMC8619362.
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Barbosa PHFA, Glinsky JV, Fachin-Martins E, Harvey LA. Physiotherapy interventions for the treatment of spasticity in people with spinal cord injury: a systematic review. Spinal Cord. 2021 Mar;59(3):236-247. doi: 10.1038/s41393-020-00610-4. Epub 2021 Feb 9. PMID: 33564117. |
Article could not be retrieved |
|
Chacon-Barba JC, Moral-Munoz JA, De Miguel-Rubio A, Lucena-Anton D. Effects of Resistance Training on Spasticity in People with Stroke: A Systematic Review. Brain Sci. 2024 Jan 6;14(1):57. doi: 10.3390/brainsci14010057. PMID: 38248272; PMCID: PMC10813883. |
Only descriptive results |
|
Del Blanco JA, Taboada-Iglesias Y. Effects of resistance exercise in patients with spasticity: Systematic review. Apunts Sports Medicine. 2021 56: |
Only descriptive results |
|
Ellapen TJ, Hammill HV, Swanepoel M, Strydom GL. The benefits of hydrotherapy to patients with spinal cord injuries. Afr J Disabil. 2018 May 16;7(0):450. doi: 10.4102/ajod.v7i0.450. PMID: 29850439; PMCID: PMC5968875. |
No outcome measures assessed spasticity |
|
Torres-Pareja M, Sánchez-Lastra MA, Iglesias L, Suárez-Iglesias D, Mendoza N, Ayán C. Exercise Interventions for Improving Flexibility in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Medicina (Kaunas). 2019 Nov 2;55(11):726. doi: 10.3390/medicina55110726. PMID: 31684026; PMCID: PMC6915647. |
No outcome measures assessed spasticity, focus on flexibility and ROM |
|
Veldema J, Jansen P. Aquatic therapy in stroke rehabilitation: systematic review and meta-analysis. Acta Neurol Scand. 2021 Mar;143(3):221-241. doi: 10.1111/ane.13371. Epub 2020 Nov 22. PMID: 33141446. |
No outcome measures assessed spasticity, only 1 study included MAS |
|
Veldema J, Jansen P. Resistance training in stroke rehabilitation: systematic review and meta-analysis. Clin Rehabil. 2020 Sep;34(9):1173-1197. doi: 10.1177/0269215520932964. Epub 2020 Jun 11. PMID: 32527148. |
Only descriptive results |
|
Veldema J, Jansen P. Ergometer Training in Stroke Rehabilitation: Systematic Review and Meta-analysis. Arch Phys Med Rehabil. 2020 Apr;101(4):674-689. doi: 10.1016/j.apmr.2019.09.017. Epub 2019 Nov 2. PMID: 31689416. |
Only descriptive results |
Beoordelingsdatum en geldigheid
Publicatiedatum : 06-01-2026
Beoordeeld op geldigheid : 06-01-2026
De Nederlandse Vereniging van Revalidatieartsen geeft bestuurlijke goedkeuring onder voorwaarde van autorisatie door de ALV van 17 april 2026.
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2023 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met Cerebrale en/of spinale spasticiteit.
Werkgroep
- prof. dr. A.C.H. Geurts (voorzitter), hoogleraar neurorevalidatie, Radboud UMC en Sint Maartenskliniek, namens de Nederlandse Vereniging voor Revalidatieartsen
- drs. A.M.V. Dommisse, revalidatiearts, Isala Klinieken Zwolle, namens de Nederlandse Vereniging voor Revalidatieartsen
- drs. P.J. van Dongen, patiëntvertegenwoordiger bij Hersenletsel.nl
- Dr. M. van Eijk, specialist ouderengeneeskunde, Marnix Medisch B.V., namens Verenso
- dr. J.F.M. Fleuren, revalidatiearts, Jeroen Bosch Ziekenhuis / Tolbrug, ‘s Hertogenbosch, namens de Nederlandse Vereniging voor Revalidatieartsen
- F. van Gorp-Swart, MSc, ziekenhuisapotheker, Diakonessenhuis, Utrecht/Zeist/Doorn, namens de Nederlandse Vereniging voor Ziekenhuisapothekers
- prof. dr. G. Kwakkel, hoogleraar neurorevalidatie, Amsterdam UMC, Amsterdam, namens het Koninklijk Nederlands Genootschap voor Fysiotherapie
- drs. E. Kurt, neurochirurg, Radboud UMC en Canisius Wilhelmina Ziekenhuis, Nijmegen, namens de Nederlandse Vereniging voor Neurochirurgie
- Prof. dr. C.G.M. Meskers, hoogleraar revalidatiegeneeskunde, Amsterdam UMC, Amsterdam, namens de Nederlandse Vereniging voor Revalidatieartsen
- dr. H.A. Moser, anesthesioloog, Radboud UMC, Nijmegen en Care4homecare, Bladel, namens de Nederlandse Vereniging voor Anesthesiologie
- drs. W.P. Polomski, revalidatiearts (gepensioneerd), voorheen in Spaarne Gasthuis, Hoofddorp, namens de Nederlandse Vereniging voor Revalidatieartsen
- drs. M.N. Ruissen-Eversdijk, ergotherapeut en bewegingswetenschapper, Reade, Amsterdam, namens Ergotherapie Nederland
- dr. A.V.C.M. Zeegers, orthopedisch chirurg, Medisch Spectrum Twente, Enschede, namens de Nederlandse Orthopaedische Vereniging
- dr. J.M. Zuidam, plastisch chirurg, Erasmus MC, namens de Nederlandse Vereniging voor Plastische Chirurgie
Klankbordgroep
- P.M. van Lamoen, gepensioneerd, namens Dwarslaesieorganisatie Nederland
- M. Pol, Dwarslaesie Organisatie Nederland, tot september 2024*
- Dr. A.E. Tigchelaar, Dwarslaesie Organisatie Nederland, vanaf september 2024
- Dr. W.J. Kruithof, revalidatiearts, Universitair Medisch Centrum Utrecht
- Dr. I.H. Zaal-Schuller, arts verstandelijk gehandicapten/kaderarts palliatieve zorg
*Overleden
Met ondersteuning van
- Dr. M.L. Molag, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. M.M.J. van Rooijen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten via secretariaat@kennisinstituut.nl.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Geurts (voorzitter) |
Hoogleraar neurorevalidatie, Radboud UMC, Nijmegen en Sint Maartenskliniek |
|
Geen. |
Geen restricties. |
|
Dommisse |
Revalidatiearts, Vogellanden |
Geen |
Speakerfee bij Ipsen farmaceutica voor:
|
Geen restricties; e-learning en presentaties betreffen de volle breedte van de behandel opties |
|
van Dongen |
Patiëntvertegenwoordiger Hersenletsel.nl |
Deelname andere werkgroepen |
Geen |
Geen restricties. |
|
van Eijk |
Specialist Ouderengeneeskunde, Marnix Medisch B.V |
|
Extern gefinancierd onderzoek over heupfracturen: 1. FITHIP; onderzoek naar valangst bij patienten met heupfractuur 2. GR HIP; onderzoek naar herstel na heupfractuur 3. HIPCARE; onderzoek naar herstel en biomarkers bij heupfractuur |
Geen restricties; De webinars waren gericht op samenwerking specialisten ouderengeneeskunde en revalidatieartsen |
|
Fleuren |
Revalidatiearts, Tolbrug |
Bestuurslid VRA (onbetaald) |
Geen. |
Geen restricties. |
|
van Gorp |
Ziekenhuisapotheker |
Lid werkgroep interacties KNMP |
Geen. |
Geen restricties. |
|
Kwakkel |
Hoogleraar neurorevalidatie, Amsterdam UMC, locatie VUMC |
|
Geen |
Geen restricties. |
|
Kurt |
Neurochirurg, Radboud UMC, Nijmegen |
Geen |
Geen |
Geen restricties. |
|
Meskers |
Revalidatiearts, Amsterdam UMC locatie VUMC |
Geen |
Geen. |
Geen restricties. |
|
Moser |
Anesthesioloog, Radboud UMC, Nijmegen en Care4homecare, Bladel |
Geen |
Geen |
Geen restricties. |
|
Polomski |
Revalidatiearts Spaarne Gasthuis (gepensioneerd vanaf 1 mei 2023). |
Geen |
Lid Adviesraad Merz Benelux, raakt niet aan de modules |
Restrictie ten aanzien van besluitvorming met betrekking tot botulinetoxine |
|
Ruissen-Eversdijk |
Ergotherapeut bij Reade Revalidatie. |
Geen. |
Geen. |
Geen restricties. |
|
Zeegers |
Orthopedisch chirurg, Medisch Spectrum Twente, Enschede (tot 1-6-2025), en UMCG (vanaf 1-6-2025) |
|
Geen. |
Geen restricties. |
|
Zuidam |
Plastisch chirurg, Erasmus MC Rotterdam |
Geen. |
Geen. |
Geen restricties. |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door uitnodigen van Hersenletsel.nl en Dwarslaesie Organisatie Nederland (DON) bij de schriftelijke knelpuntenanalyse. DON heeft een enquête bij hun achterban uitgezet, en knelpunten werden meegenomen in het proces. Het verslag van deze enquête is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. In de werkgroep heeft een vertegenwoordiger van Hersenletsel.nl deelgenomen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan Hersenletsel.nl, DON, MS Nederland en Spierziekten Nederland.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase). Uit deze kwalitatieve raming bleek dat er geen grote financiële gevolgen te verwachten zijn.
|
Module |
Uitkomst raming |
Toelichting |
|
Passief rekken |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
Voor meer details over de gebruikte richtlijnmethodologie verwijzen wij u naar de Werkwijze. Relevante informatie voor de ontwikkeling/herziening van deze richtlijnmodule is hieronder weergegeven.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Cluster Myopathie & Spierdystrofie/ Behandeling van cerebrale en/of spinale spasticiteit bij volwassenen |
|
|
Uitgangsvraag/modules: Module 2 What is the effect of passive stretching in patients with cerebral and/or spinal spasticity? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 7 januari 2025 |
|
Periode: vanaf 2014 |
Talen: geen restrictie |
|
Literatuurspecialist: Alies Oost |
Rayyan: https://new.rayyan.ai/reviews/1280463/screening |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen:
De sleutelartikelen worden gevonden met deze search, m.u.v. die van Rietberg (Exercise therapy for multiple sclerosis/ PMID 15674920) en Pak (Strengthening to promote functional recovery poststroke/ PMID 18647724). Deze zijn van voor 2014. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
446 |
291 |
505* |
*in Rayyan
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
('spinal cord injury'/exp OR 'spine injury'/exp OR 'spinal cord disease'/exp OR 'multiple sclerosis'/exp OR 'brain injury'/exp OR 'head injury'/exp OR 'cerebrovascular disease'/exp OR 'brain hemorrhage'/exp OR 'brain infarction'/exp OR 'intracranial aneurysm'/exp OR 'stroke patient'/exp OR 'cerebral palsy'/exp OR (((spinal OR spine OR head) NEAR/2 (injur* OR trauma*)):ti,ab,kw) OR tbi:ti,ab,kw OR cva:ti,ab,kw OR cvas:ti,ab,kw OR stroke:ti,ab,kw OR poststroke:ti,ab,kw OR (((cerebrovascular OR 'cerebro vascular' OR cerebral OR intracerebral OR cerebellum OR brain OR 'corpus callosum' OR intracranial OR intraventricular OR periventricular OR subarachnoid) NEAR/3 (accident* OR attack* OR infarct* OR insult* OR event* OR diseas* OR injur* OR trauma OR arrest OR failure OR bleed* OR microbleed* OR aneurysm* OR hemorrhage* OR haemorrhage* OR microhemorrhage* OR microhaemorrhage* OR ischemi* OR ischaemi* OR haematoma* OR hematoma* OR thrombo* OR emboli* OR occlus*)):ti,ab,kw) OR palsy:ti,ab,kw OR apoplex*:ti,ab,kw OR encephalorrhagia:ti,ab,kw OR myelopath*:ti,ab,kw OR neuromyelopath*:ti,ab,kw OR (((multiple OR disseminated OR insular OR multiplex) NEAR/2 scleros*):ti,ab,kw)) AND ('spasticity'/exp OR 'spastic paraplegia'/exp OR 'spastic paresis'/exp OR 'muscle spasm'/de OR 'dystonia'/exp OR 'muscle hypertonia'/de OR spastic*:ti,ab,kw OR spasm*:ti,ab,kw OR paretic:ti,ab,kw OR hypertonia:ti,ab,kw OR dystonia:ti,ab,kw) |
53113 |
|
#2 |
'exercise'/exp OR 'training'/exp OR 'functional training'/exp OR 'fitness'/exp OR 'physical activity'/exp OR 'sport'/exp OR 'balance training'/exp OR 'robotics'/de OR 'hypnotherapy'/exp OR 'vibration'/exp OR (('physical*' NEAR/3 (activit* OR 'effort*' OR 'exertion*' OR 'fitness*')):ti,ab,kw) OR 'exercis*':ti,ab,kw OR training:ti,ab,kw OR 'work-out':ti,ab,kw OR 'workout':ti,ab,kw OR 'work-outs':ti,ab,kw OR 'workouts':ti,ab,kw OR 'aqua* therap*':ti,ab,kw OR 'hydrotherap*':ti,ab,kw OR swimming:ti,ab,kw OR (((walk* OR ambulat* OR gait OR balanc*) NEAR/3 (train* OR therap*)):ti,ab,kw) OR bicycling:ti,ab,kw OR cycling:ti,ab,kw OR 'weight lift*':ti,ab,kw OR robot*:ti,ab,kw OR hypnotherap*:ti,ab,kw OR vibration:ti,ab,kw OR 'physiotherapy'/exp OR physiotherap*:ti,ab,kw OR 'physio therap*':ti,ab,kw OR 'physical therap*':ti,ab,kw OR 'kinesiotherapy'/exp OR kinesiotherap*:ti,ab,kw OR kinesitherap*:ti,ab,kw OR ((rehabilitation NEAR/1 (therapy OR therapies)):ti,ab,kw) |
2470981 |
|
#3 |
#1 AND #2 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab,kw OR child*:ti,ab,kw OR schoolchild*:ti,ab,kw OR infant*:ti,ab,kw OR girl*:ti,ab,kw OR boy*:ti,ab,kw OR teen:ti,ab,kw OR teens:ti,ab,kw OR teenager*:ti,ab,kw OR youth*:ti,ab,kw OR pediatr*:ti,ab,kw OR paediatr*:ti,ab,kw OR puber*:ti,ab,kw) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab,kw OR man:ti,ab,kw OR men:ti,ab,kw OR woman:ti,ab,kw OR women:ti,ab,kw)) |
6924 |
|
#4 |
#3 AND [2014-2025]/py |
3850 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR 'systematic review'/exp OR 'systematic review (topic)'/exp OR 'scoping review'/exp OR 'rapid review'/exp OR 'umbrella review'/exp OR 'cochrane database of systematic reviews'/jt OR 'network meta-analysis'/exp OR 'networkmeta analy*':ti,ab,kw OR 'networkmetaanaly*':ti,ab,kw OR metaanaly*:ti,ab,kw OR 'meta analy*':ti,ab,kw OR metanaly*:ti,ab,kw OR prisma:ti,ab,kw OR prospero:ti,ab,kw OR metaanali*:ti,ab,kw OR 'meta anali*':ti,ab,kw OR metanali*:ti,ab,kw OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab,kw) OR (((structured OR systemic*) NEAR/3 (review* OR overview* OR synth*) NEAR/3 literature):ti,ab,kw) OR ((systemic* NEAR/1 review*):ti,ab,kw) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab,kw) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab,kw) OR (((literature NEAR/3 (review* OR overview*)):ti,ab,kw) AND (search*:ti,ab,kw OR database*:ti,ab,kw OR 'data base*':ti,ab,kw)) OR (('data extraction*':ti,ab,kw OR 'data source*':ti,ab,kw) AND ('study selection*':ti,ab,kw OR 'studies selection*':ti,ab,kw)) OR ('search strateg*':ti,ab,kw AND 'selection criteria*':ti,ab,kw) OR ('data source*':ti,ab,kw AND 'data synth*':ti,ab,kw) OR medline*:ti,ab,kw OR pubmed*:ti,ab,kw OR 'pub med*':ti,ab,kw OR embase:ti,ab,kw OR cochrane*:ti,ab,kw OR (((critical* OR rapid*) NEAR/2 (review* OR overview* OR synth*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synth*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynth*:ti,ab,kw OR 'meta synth*':ti,ab,kw OR 'review* of review*':ti,ab,kw |
1110718 |
|
#6 |
#4 AND #5 |
446 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
(exp Spinal Cord Injuries/ or exp Spinal Injuries/ or exp Spinal Cord Diseases/ or exp Multiple Sclerosis/ or exp Brain Injuries/ or Head Injuries, Closed/ or exp Cerebrovascular Disorders/ or exp Stroke/ or exp Stroke Rehabilitation/ or exp Intracranial Hemorrhages/ or exp Brain Infarction/ or exp Cerebral Palsy/ or ((spinal or spine or head) adj2 (injur* or trauma*)).ti,ab,kf. or tbi.ti,ab,kf. or cva.ti,ab,kf. or cvas.ti,ab,kf. or stroke.ti,ab,kf. or poststroke.ti,ab,kf. or ((cerebrovascular or 'cerebro vascular' or cerebral or intracerebral or cerebellum or brain or 'corpus callosum' or intracranial or intraventricular or periventricular or subarachnoid) adj3 (accident* or attack* or infarct* or insult* or event* or diseas* or injur* or trauma or arrest or failure or bleed* or microbleed* or aneurysm* or hemorrhage* or haemorrhage* or microhemorrhage* or microhaemorrhage* or ischemi* or ischaemi* or haematoma* or hematoma* or thrombo* or emboli* or occlus*)).ti,ab,kf. or palsy.ti,ab,kf. or apoplex*.ti,ab,kf. or encephalorrhagia.ti,ab,kf. or myelopath*.ti,ab,kf. or neuromyelopath*.ti,ab,kf. or ((multiple or disseminated or insular or multiplex) adj2 scleros*).ti,ab,kf.) and (exp Muscle Spasticity/ or exp Spasm/ or exp Paraparesis, Spastic/ or exp Muscle Hypertonia/ or exp Dystonia/ or spastic*.ti,ab,kf. or spasm*.ti,ab,kf. or paretic.ti,ab,kf. or (hypertonia or dystonia).ti,ab,kf.) |
28443 |
|
2 |
exp Exercise/ or exp Exercise Therapy/ or exp Sports/ or Robotics/ or Hypnosis/ or exp Vibration/ or (physical* adj3 (activit* or effort* or exertion* or fitness*)).ti,ab,kf. or exercis*.ti,ab,kf. or training.ti,ab,kf. or work-out.ti,ab,kf. or workout.ti,ab,kf. or work-outs.ti,ab,kf. or workouts.ti,ab,kf. or 'aqua* therap*'.ti,ab,kf. or 'hydrotherap*'.ti,ab,kf. or swimming.ti,ab,kf. or ((walk* or ambulat* or gait or balanc*) adj3 (train* or therap*)).ti,ab,kf. or bicycling.ti,ab,kf. or cycling.ti,ab,kf. or 'Weight Lift*'.ti,ab,kf. or robot*.ti,ab,kf. or hypnotherap*.ti,ab,kf. or vibration.ti,ab,kf. or exp Physical Therapy Modalities/ or exp Physical Therapy Specialty/ or exp Occupational Therapy/ or physiotherap*.ti,ab,kf. or 'physio therap*'.ti,ab,kf. or 'physical therap*'.ti,ab,kf. or kinesiotherap*.ti,ab,kf. or kinesitherap*.ti,ab,kf. or (rehabilitation adj1 (therapy or therapies)).ti,ab,kf. |
1635998 |
|
3 |
(1 and 2) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) not ((Adolescent/ or Child/ or Infant/ or adolescen*.ti,ab,kf. or child*.ti,ab,kf. or schoolchild*.ti,ab,kf. or infant*.ti,ab,kf. or girl*.ti,ab,kf. or boy*.ti,ab,kf. or teen.ti,ab,kf. or teens.ti,ab,kf. or teenager*.ti,ab,kf. or youth*.ti,ab,kf. or pediatr*.ti,ab,kf. or paediatr*.ti,ab,kf. or puber*.ti,ab,kf.) not (Adult/ or adult*.ti,ab,kf. or man.ti,ab,kf. or men.ti,ab,kf. or woman.ti,ab,kf. or women.ti,ab,kf.)) |
4379 |
|
4 |
limit 3 to yr="2014 -Current" |
2443 |
|
5 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
800268 |
|
6 |
4 and 5 |
291 |