Postoperatieve ademhalingsondersteuning
Uitgangsvraag
Wat is de plaats van non-invasieve postoperatieve ademhalingsondersteuning met positieve druk om de kans op pulmonale complicaties bij pulmonaal belaste patiënten te verkleinen?
Aanbeveling
Pas non-invasieve ademhalingsondersteuning met positieve druk postoperatief niet routinematig toe bij pulmonaal belaste patiënten.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is literatuuronderzoek verricht naar het effect van preventieve non-invasieve postoperatieve ademhalingsondersteuning met NIV, CPAP of HFNO op het ontstaan van PPC’s bij pulmonaal belaste patiënten die een niet-pulmonale operatie hebben ondergaan. Er werd 1 systematische review geïncludeerd waarvan 12 RCT’s relevant waren voor de huidige analyse. Ook werden er 5 aanvullende RCT’s opgenomen in de literatuursamenvatting. In de studies werd het preventief inzetten van NIV, CPAP of HFNO vergeleken met standaard postoperatieve zorg bij patiënten die een electieve niet-cardiothoracale operatie hebben ondergaan.
De cruciale uitkomstmaat is de incidentie van PPC’s. Deze overkoepelende uitkomstmaat werd in 7 studies gerapporteerd. De sub-uitkomsten longontsteking en aspiratie, als potentiële bijwerking van de interventie, werden door respectievelijk 12 en 2 studies gerapporteerd. De geïncludeerde studies zijn echter vooral kleine studies, met een wisselende incidentie van PPC’s en verschillende patiëntenpopulaties. De bewijskracht van de cruciale uitkomstmaat is dan ook zeer laag. Er is afgewaardeerd voor indirectheid vanwege een bredere patiëntenpopulatie die ook niet-pulmonaal belaste patiënten bevat en imprecisie vanwege brede betrouwbaarheidsintervallen en/of een klein aantal events. Door de zeer lage overall bewijskracht van de cruciale uitkomstmaat kan de literatuur geen richting geven aan besluitvorming.
Verblijfsduur in het ziekenhuis is als belangrijke uitkomstmaat gedefinieerd. Deze uitkomstmaat werd door 12 studies gerapporteerd. Preventieve postoperatieve ademhalingsondersteuning met NIV, CPAP of HFNO lijkt geen vermindering in verblijfsduur te geven ten opzichte van standaardzorg. Voor de HFNO geldt hier dat 2 positieve studies worden tegengesproken door twee studies zonder verschil op opnameduur. De bewijskracht van al deze studies was echter laag. Er is afgewaardeerd voor indirectheid vanwege een bredere patiëntenpopulatie en imprecisie vanwege brede betrouwbaarheidsintervallen.
Er bestaat een kennisvraag omtrent het effect van preventieve non-invasieve postoperatieve ademhalingsondersteuning op pulmonaal belaste patiënten die een niet-pulmonale ingreep ondergaan. De aanbevelingen zijn daarom voornamelijk gebaseerd op expertopinie en waar mogelijk onderbouwd met indirecte literatuur.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
De meerwaarde voor het toepassen van non-invasieve beademing met positieve druk in de postoperatieve fase zit voor individuele patiënten in de potentiële gezondheidswinst van de interventie. Indien deze interventie leidt tot een kleinere kans op complicaties en/of kortere opname duur door vlotter herstel in het ziekenhuis kan dat van groot voordeel zijn voor zowel de patiënt als hun eventuele verzorgers.
Het is belangrijk om de patiënt goed te informeren over de mogelijke meerwaarde en nadelen van de behandeling, zodat deze samen met de zorgverlener een weloverwogen beslissing kan nemen over de toepasbaarheid van non-invasieve beademing met positieve druk.
De interventie zelf kan voor patiënten leiden tot meer discomfort tijdens het toepassen ervan. Voor de HFNO geldt dat het onbehagen voornamelijk voortkomt uit het suizende geluid en/of de grotere ‘neusbril’ die hierbij gebruikt wordt. Tijdens het toepassen van CPAP/NIV wordt het meeste onbehagen ervaren door de strak afsluitende kap die hierbij noodzakelijk is.
Het bovengenoemde nadeel zal voor het overgrote deel van de patiënten overkomelijk zijn, indien het een bewezen voordeel in gezondheidswinst zou hebben.
Kosten (middelenbeslag)
Voor het kunnen toepassen van non-invasieve beademing met positieve druk in de postoperatieve fase bij een grotere patiëntengroep zullen kosten gemaakt moeten worden. Het gaat hier om beperkte kosten per patiënt voor het gebruik van aanvullende materialen zoals NIV/CPAP-maskers, HFNO-neusbrillen en de bijbehorende slangen- en bevochtiging-sets. Daarnaast zullen ziekenhuizen mogelijk een investering moeten maken voor meer apparatuur waarmee een behandeling met non-invasieve beademing of HFNC mogelijk gemaakt kan worden. Indien de genoemde behandelingen voor specifieke patiënten in de direct postoperatieve fase wel reeds beschikbaar is, zal er geen directe noodzaak zijn voor aanvullende scholing van personeel.
Aanvaardbaarheid, haalbaarheid en implementatie
Er zijn geen studies gedaan naar de haalbaarheid en aanvaardbaarheid voor het routinematig toepassen van non-invasieve positieve druk beademing in de postoperatieve fase bij grotere patiëntengroepen. Gezien deze interventie voor individuele patiënten met een specifieke indicatie wel beschikbaar is, zal voornamelijk de schaalvergroting een probleem kunnen zijn.
Meer arbeidsintensievere patiëntenzorg kan leiden tot een vraag naar meer personeel. Ook de doorstroming in de direct postoperatieve fase, zoals op een verkoever, zal bij een brede invoering van deze interventie mogelijk negatief beïnvloed worden. Deze nadelen kunnen worden afgewogen indien er sprake zou zijn van bewezen voordelen van de invoering van deze interventie.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Op dit moment is er te weinig bewijs om non-invasieve positieve drukbeademing op routinematige basis toe te passen in de directe postoperatieve fase. Het potentiële voordeel zoals op basis van fysiologie verwacht zou kunnen worden kan in klinische eindpunten niet in grote patiëntengroepen onomstotelijk aangetoond worden. Hoewel het voor de totale populatie onduidelijk is of deze vorm van beademing meerwaarde heeft, kunnen sommige patiënten hier toch baat bij hebben. Dit is een individuele klinische afweging waar deze richtlijn geen sturing in kan geven. De potentiële risico’s, zoals aspiratie, dienen vanzelfsprekend meegenomen te worden in deze afweging.
Onderbouwing
Introduction
Currently, patients in the postoperative phase generally receive no other respiratory support than oxygen administration via a mask or nasal cannula. There is no routine application of non-invasive positive pressure support, such as Continuous Positive Airway Pressure (CPAP), Non-Invasive Ventilation (NIV), or High Flow Nasal Oxygen (HFNO). The physiological rationale for applying these techniques is to reduce atelectasis, which can develop intraoperatively, particularly during general anesthesia. Although the specific etiology of postoperative respiratory complications remains unclear, it is thought that atelectasis plays a detrimental role in this process. Therefore, in recent years, there is growing interest in the application of positive pressure ventilation in the postoperative phase. However, a well-founded, standardized policy in this area is still lacking.
|
Very low GRADE |
The evidence is very uncertain for the effect of routine postoperative non-invasive respiratory support (NIV, CPAP or HFNO) on postoperative pulmonary complications in patients with a pulmonary precondition undergoing non-pulmonary surgery.
Sources: Hui, 2022; Fulton, 2021; Li, 2022; Frassanito, 2023 |
|
Very low GRADE |
The evidence is very uncertain for the effect of routine postoperative non-invasive respiratory support (NIV, CPAP or HFNO) on pneumonia in patients with a pulmonary precondition undergoing non-pulmonary surgery.
Source: Hui, 2022; Soliman, 2022; Sun, 2024 |
|
Very low GRADE |
The evidence is very uncertain for the risk of routine postoperative non-invasive respiratory support (NIV, CPAP or HFNO) on pulmonary aspiration in patients with a pulmonary precondition undergoing non-pulmonary surgery.
Source: Hui, 2022 |
|
Low GRADE |
Routine postoperative respiratory support with positive pressure (NIV, CPAP or HFNO) may not reduce length of hospital stay compared to respiratory support without positive pressure in patients with a pulmonary precondition undergoing non-pulmonary surgery.
Source: Hui, 2022; Fulton, 2021; Soliman, 2022; Sun, 2024 |
Description of studies
Hui (2022) conducted a systematic review and meta-analysis of RCTs comparing the routine use of continuous positive airway pressure (CPAP), noninvasive ventilation (NIV), or high-flow nasal oxygen (HFNO) against standard postoperative care in the adult population. Twelve relevant studies were extracted from the systematic review. Five individual RCTs were also included in the analysis of the literature. Relevant study characteristics are reported in Table 1.
Table 1. Study characteristics
|
I1: 257; 63.4 years; NR; 13 (5%) I2: 256; 64.7 years; NR; 18 (8%) |
||||||
|
CPAP: 15; 49 years; NR; 0 (0%) |
||||||
|
42/41; 61/55 years; female 42/41; chronic respiratory disease 5 (12%)/ 2 (5%) |
||||||
PPC: postoperative pulmonary complications; GI: gastrointestinal; HPB: Hepato-pancreato-biliary; CPAP: continuous positive airway pressure; NIV: non-invasive ventilation; HFNO: high-flow nasal oxygen; LOS: length of stay; NR: not reported.
1 bias due to randomization
2 bias due to deviations from intended intervention
3 bias due to missing data
4 bias due to outcome measurement
5 bias due to selection of reported result
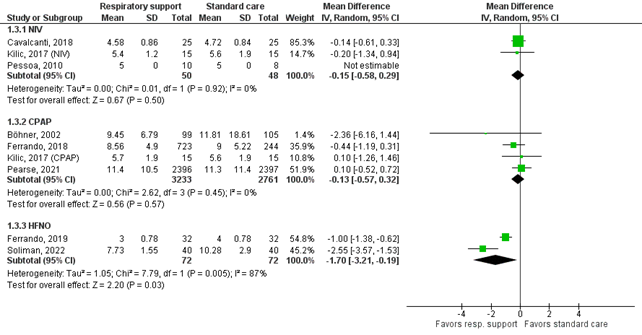
Definition of PPCs
Hui (2022) reported the outcome postoperative pulmonary complications (PPCs) as a secondary outcome. Ideally, the included studies in the systematic review defined PPCs according to the STEP-COMPAC criteria (Abbott, 2018), see Box 1. The primary outcome of the systematic review from Hui (2022) was pneumonia, which is also part of the composite PPC definition. The outcome pulmonary aspiration were also reported separately in the systematic review.
Box 1. Recommended definition of PPCs by Abott (2018)
Results
Postoperative pulmonary complications (composite outcome)
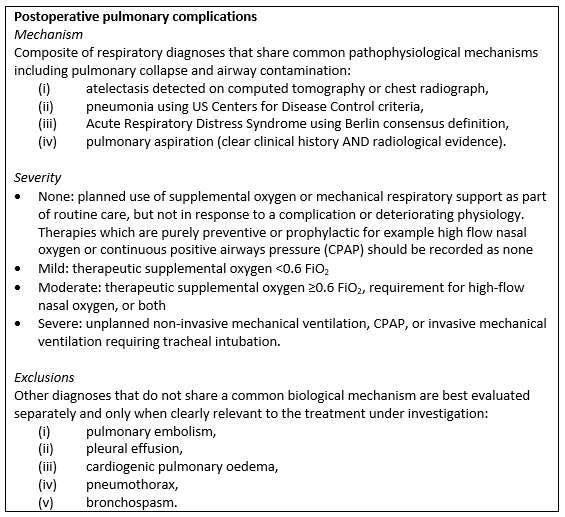
Four studies included in the systematic review of Hui (2022) reported the PPC incidence for both groups (Alexandropolou, 2019; Ferrando, 2018; Kilic, 2017; Lindner, 1987). Additionally, Frassanito (2023), Fulton (2021) and Li (2022) also reported the incidence of postoperative pulmonary complications. The study results are shown in Figure 1.
NIV
Alexandropolou (2019) and Kilic (2017) compared NIV with standard postoperative care. The pooled RR of 0.28 (95%CI 0.02 to 3.75) is clinically relevant in favor of the NIV group. However, the confidence interval is very wide and crosses the border of clinical relevance.
CPAP
Ferrando (2018), Kilic (2017) and Lindner (1987) compared CPAP with standard postoperative care. The pooled RR of 0.73 (95%CI 0.43 to 1.26) is clinically relevant in favor of the CPAP group, but the confidence interval crosses the border of clinical relevance.
HFNO
Frassanito (2023), Fulton (2021) and Li (2022) compared HFNO with standard postoperative care and reported the composite outcome postoperative pulmonary complications. The pooled RR of 1.09 (95%CI 0.40 to 2.95) is not clinically relevant.
Soliman (2022) also compared HFNO with standard postoperative case, but only reported the outcomes pneumonia and atelectasis separately. A composite outcome cannot be calculated based on these numbers, because patients may have experienced both pneumonia and atelectasis.
Figure 1. Forest plot of the effect of routine postoperative non-invasive respiratory support on postoperative pulmonary complications
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
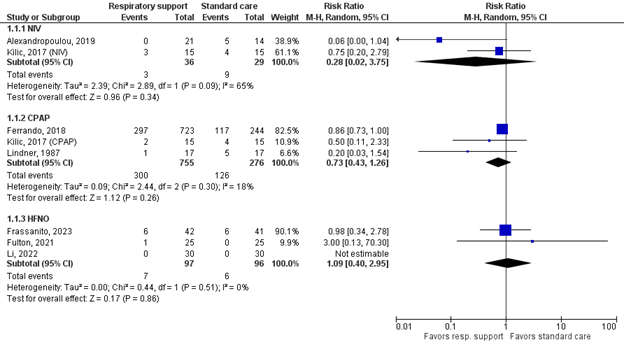
Pneumonia
Twelve studies reported the outcome pneumonia, see Figure 2. The overall pooled RR of 0.94 (95%CI 0.74 to 1.1) is not clinically relevant.
NIV
Alexandropolou (2019) and Cavalcanti (2018) compared NIV with standard postoperative care. The pooled RR of 0.57 (95%CI 0.23 to 1.45) is clinically relevant in favor of the NIV group, but the confidence interval is very wide and crosses two borders of clinical relevance.
CPAP
Böhner (2002), Ferrando (2018), Hewidy (2016), Lindner (1987) and Pearse (2021) compared CPAP with standard postoperative care. The pooled RR of 1.05 (95%CI 0.83 to 1.33) is not considered clinically relevant.
HFNO
Ferrando (2019), Soliman (2022) and Sun (2024) compared HFNO with standard postoperative care. The pooled RR of 0.35 (95%CI 0.10 to 1.29) is clinically relevant in favor of the HFNO group, but the confidence interval is very wide and crosses both borders of clinical relevance.
Figure 2. Forest plot of the effect of routine postoperative non-invasive respiratory support on pneumonia
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
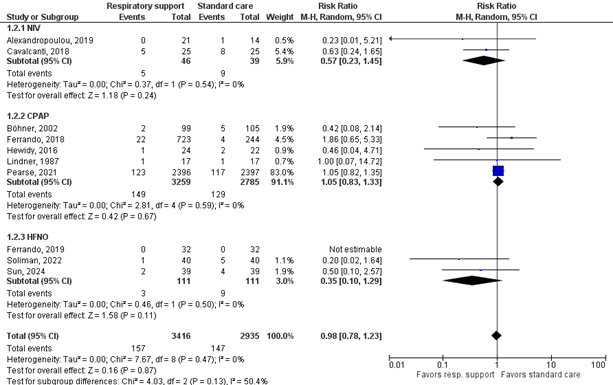
Length of hospital stay
Ten studies reported the mean length of hospital stay, see Figure 3. Taken together, the mean difference was -0.62 in favor of respiratory support with positive pressure (95%CI -1.18 to -0.05) the difference was not considered clinically relevant.
NIV
Cavalcanti (2018), Kilic (2017), and Pessoa (2010) compared NIV with standard postoperative care and reported the outcome length of hospital stay in days. The mean difference of -0.15 days (SD -0.58 to 0.29) is not clinically relevant.
CPAP
Böhner (2002), Ferrando (2018), Kilic (2017), and Pearse (2021) compared CPAP with standard postoperative care and reported the outcome length of hospital stay in days. The pooled mean difference of -0.13 days (95%CI -0.57 to 0.32) is not clinically relevant.
HFNO
Ferrando (2019) reported a mean length of stay of 3 days (SD 0.78) for the HFNO group and 4 days (SD 0.78) for the control group, leading to a mean difference of -1 days (95%CI -1.38 to -0.62). Soliman (2022) reported a mean length of stay of 7.73 days (SD 1.55) for the HFNO group and 10.28 days (SD 2.9) for the control group, leading to a mean difference of -2.55 days (95%CI -3.57 to -1.53). The pooled mean difference of -1.70 days (95%CI -3.21 to -0.19) is considered clinically relevant in favor of the HFNO group.
Additionally, Fulton (2021) reported a median length of stay of 2 days (IQR 2 to 2) for both groups. Sun (2024) reported a median length of stay of 10 days (IQR 9 to 12) for the HFNO group and 10 days (IQR 9 to 11 days) for the control group.
Figure 3. Forest plot of the effect of routine postoperative non-invasive respiratory support on length of hospital stay
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
Pulmonary aspiration
Only two studies reported the outcome pulmonary aspiration, a possible risk of positive pressure respiratory support. Both compared CPAP with standard postoperative care. Ferrando (2018) and reported no events in either group and Pearse (2021) reported that 13 of 2,395 patients experienced pulmonary aspiration in the CPAP group compared with 12 of 2,394 patients in the control group. The RR of 1.08 (95%CI 0.50 to 2.37) is not considered clinically relevant.
Level of evidence of the literature
The level of evidence regarding the outcome measures postoperative pulmonary complications, pneumonia, pulmonary aspiration started at high and was downgraded by three levels to very low because of applicability because the study population also included patients without a pulmonary precondition (indirectness, -1); confidence intervals crossing the border of clinical relevance and/or a very low number of events (imprecision, -2).
The level of evidence regarding the outcome measure length of stay started at high and was downgraded by two levels to low because of applicability because the study population also included patients without a pulmonary precondition (indirectness, -1) and wide confidence intervals crossing the border of clinical relevance (imprecision, -1).
A systematic review of the literature was performed to answer the following question:
What are the benefits and harms of using postoperative respiratory support with positive pressure (CPAP/NIV/HFNO) compared with respiratory support without positive pressure in patients with a pulmonary precondition who have undergone non-pulmonary surgery?
| P (Patients): | Patients with a pulmonary precondition who have undergone non-pulmonary surgery |
| I (Intervention): | Positive pressure respiratory support (CPAP/NIV/HFNO) |
| C (Comparison): | Respiratory support without positive pressure |
| O (Outcomes): |
Postoperative pulmonary complications, length of hospital stay, pneumonia, aspiration |
Relevant outcome measures
The guideline development group considered postoperative pulmonary complications as a critical outcome measure for decision making; and length of stay, pneumonia, and aspiration (as potential risk of positive pressure ventilation) as important outcome measures for decision making.
A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
The working group defined 25% as a minimal clinically (patient) important difference (MCID) for dichotomous outcomes (risk ratio ≤0.8 or ≥1.25), and 1 day for hospital length of stay.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 24 May 2024. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 497 hits.
Studies were selected based on the following criteria: (systematic review of) RCTs comparing prophylactic respiratory support (CPAP/ NIV/ HFNO) with standard postoperative care in patients who have undergone non-pulmonary surgery; reporting at least one of the specified outcomes.
Initially, 36 studies were selected based on title and abstract screening. After reading the full text, 30 studies were excluded (see the table with reasons for exclusion under the tab Methods), and six studies were included: one systematic review and five individual studies.
Results
Six studies were included in the analysis of the literature: one systematic review of which twelve studies are included in the current analysis and five additional individual studies. Important study characteristics and the assessment of the risk of bias are summarized in Table 1.
- Abbott TEF, Fowler AJ, Pelosi P, Gama de Abreu M, Møller AM, Canet J, Creagh-Brown B, Mythen M, Gin T, Lalu MM, Futier E, Grocott MP, Schultz MJ, Pearse RM; StEP-COMPAC Group. A systematic review and consensus definitions for standardised end-points in perioperative medicine: pulmonary complications. Br J Anaesth. 2018 May;120(5):1066-1079. doi: 10.1016/j.bja.2018.02.007. Epub 2018 Mar 27. PMID: 29661384.
- Frassanito L, Grieco DL, Zanfini BA, Catarci S, Rosà T, Settanni D, Fedele C, Scambia G, Draisci G, Antonelli M. Effect of a pre-emptive 2-hour session of high-flow nasal oxygen on postoperative oxygenation after major gynaecologic surgery: a randomised clinical trial. Br J Anaesth. 2023 Oct;131(4):775-785. doi: 10.1016/j.bja.2023.07.002. Epub 2023 Aug 4. PMID: 37543437.
- Fulton R, Millar JE, Merza M, Johnston H, Corley A, Faulke D, Rapchuk IL, Tarpey J, Fanning JP, Lockie P, Lockie S, Fraser JF. Prophylactic Postoperative High Flow Nasal Oxygen Versus Conventional Oxygen Therapy in Obese Patients Undergoing Bariatric Surgery (OXYBAR Study): a Pilot Randomised Controlled Trial. Obes Surg. 2021 Nov;31(11):4799-4807. doi: 10.1007/s11695-021-05644-y. Epub 2021 Aug 13. PMID: 34387826.
- Hui S, Fowler AJ, Cashmore RMJ, Fisher TJ, Schlautmann J, Body S, Lan-Pak-Kee V, Webb M, Kyriakides M, Ng JY, Chisvo NS, Pearse RM, Abbott TEF. Routine postoperative noninvasive respiratory support and pneumonia after elective surgery: a systematic review and meta-analysis of randomised trials. Br J Anaesth. 2022 Feb;128(2):363-374. doi: 10.1016/j.bja.2021.10.047. Epub 2021 Dec 13. PMID: 34916050.
- Li XN, Zhou CC, Lin ZQ, Jia B, Li XY, Zhao GF, Ye F. High-flow nasal cannula oxygen therapy during anesthesia recovery for older orthopedic surgery patients: A prospective randomized controlled trial. World J Clin Cases. 2022 Aug 26;10(24):8615-8624. doi: 10.12998/wjcc.v10.i24.8615. PMID: 36157835; PMCID: PMC9453384.
- Soliman, H. A. Z., Fikry, D. M., El-Attar, A. M., & El Hadidy, M. S. (2022). High flow nasal cannula effect on pulmonary complications after major elective upper abdominal surgeries: a randomized control study. Egyptian Journal of Anaesthesia, 38(1), 656-664.
- Sun L, Wang J, Wei P, Ruan WQ, Guo J, Yin ZY, Li X, Song JG. Randomized Controlled Trial Investigating the Impact of High-Flow Nasal Cannula Oxygen Therapy on Patients Undergoing Robotic-Assisted Laparoscopic Rectal Cancer Surgery, with a Post-Extubation Atelectasis as a Complication. J Multidiscip Healthc. 2024 Jan 26;17:379-389. doi: 10.2147/JMDH.S449839. PMID: 38292922; PMCID: PMC10826707.
Risk of bias
Risk of bias as assessed by Hui (2022):
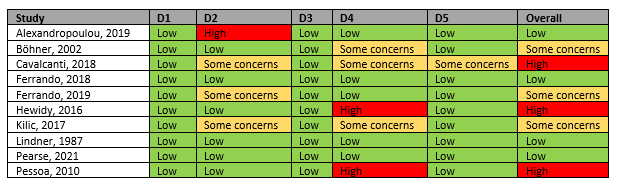
Domains:
D1: bias due to randomization
D2: bias due to deviation from intended intervention
D3: bias due to missing data
D4: bias due to outcome measurement
D5: bias due to selection of reported result
Risk of bias individual studies
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Fulton, 2021 |
Definitely yes
Reason: Prior to surgery, patients were randomised in a 1:1 fashion (using a computer-generated sequence based on block sizes of 4, 6, or 8). |
Definitely yes
Reason: An investigator, not involved in the perioperative care of a patient, obtained the allocation in a sealed envelope and informed the intensive care unit staff. The surgical and anaesthetic teams were blinded to the patient’s allocation until return to the ICU, after which treatment allocation was unblinded. |
Definitely no
Reason: No blinding. Due to the research design, neither the individual collecting data nor patient can be blinded to treatment allocation. |
Definitely yes
Reason: There was no loss to follow-up. |
Definitely yes
Reason: The trial was prospectively registered with the Australian New Zealand Clinical Trials Registry (ACTRN12617000694314). |
Probably yes
Reason: No other problems noted. |
PPCs: Some concerns Length of stay: LOW
Reason: lack of blinding |
|
Li, 2022 |
Probably yes
Reason: random grouping using random codes made in advance |
Definitely yes
Reason: The envelope method was adopted for random grouping using random codes made in advance, with each code placed into the envelope and independently sealed. After the patients who met the inclusion criteria were enrolled into the study, the envelopes were opened in sequence. |
Definitely no
Reason: No blinding after allocation possible. |
Definitely yes
Reason: No loss to follow-up reported. |
Probably yes
Reason: Relevant outcomes reported, but no protocol/trial register available. |
Probably yes
Reason: No other problems noted. |
PPCs: Some concerns Length of stay: LOW
Reason: lack of blinding |
|
Soliman, 2022 |
Probably yes
Reason: Patients were randomly allocated. |
Definitely yes
Reason: Postoperatively, at the intensive care unit using the closed-envelope technique, patients were randomly allocated into two groups. |
Definitely no
Reason: Only outcome assessor blinded according to trial registry. |
Definitely yes
Reason: No loss to follow-up reported. |
Definitely yes
Reason: All relevant outcomes reported. ClinicalTrials.gov Identifier: NCT05548309, IRB NO: 00012098. |
Probably yes
Reason: No other problems noted. |
PPCs: Some concerns Length of stay: LOW
Reason: lack of blinding |
|
Frassanito, 2023 |
Definitely yes
Reason: Patients were randomized in a 1:1 ratio to receive HFNO or conventional oxygen therapy via a Venturi mask continuously for 2 h after PACU admission. The randomization sequence (pseudo-random number generator of Wichmann and Hill as modified by McLeod, www.randomization.com) [...]. |
Definitely yes
Reason: The randomisation sequence […] was stored in sequentially numbered, opaque, sealed, and stapled envelopes. On the day of surgery, a researcher not involved in clinical care opened the envelope when the patient was extubated and had met all eligibility criteria. |
Definitely no/ definitely yes
Reason: Open-label trial. Blinding of treatment not possible for patient and healthcare provider.
Ultrasound images were stored and analyzed by two investigators (LF and DLG) blinded to study group assignment. |
Definitely yes
Reason: Infrequent: 2/42 vs 1/41 patients excluded because the ultrasound was not available. |
Definitely yes
Reason: All relevant outcomes reported. Study registered on ClinicalTrials.gov (NCT04566419) |
Probably yes
Reason: No other problems noted. |
PPCs: Some concerns Length of stay: LOW
Reason: lack of blinding |
|
Sun, 2024 |
Definitely yes
Reason: Each patient was assigned a distinct identification number using MS Excel software, and corresponding random numbers were generated. These numbers were then arranged in ascending order, and patients were randomized into either the HFNC or control group, maintaining an equal 1:1 ratio. |
Definitely yes
Reason: To maintain the integrity of the allocation process, the assignments were concealed within sealed envelopes, which were only opened by a research nurse upon the patient’s arrival at the post-anesthesia care unit (PACU), ensuring that the group assignments remained undisclosed until the appropriate time. |
Definitely no/ definitely yes
Reason: Patient and PACU nurse administrating intervention not blinded.
The evaluator conducting lung ultrasonography and the investigators collecting postoperative data were unaware of the group allocation, ensuring blinding. The PACU nurses were aware of the group allocation but were not involved in data collection and administered the designated interventions (HFNC or conventional nasal cannula oxygen therapy) according to patient group assignment. |
Definitely yes
Reason: Loss to follow-up infrequent: 1 patient in both groups discontinued the intervention due to severe subcutaneous emphysema. |
Definitely yes
Reason: All relevant outcomes reported. Study was registered in the Chinese Clinical Trial Registry (ChiCTR2100047235; date of registration: 11/06/2021). |
Probably yes
Reason: No other problems noted. |
LOW (all outcomes)
Reason: - |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Aboelsuod MAA, Farhat AEA, Abdalla AM, Hassnin FSB. Effect of pressure support ventilation vs. spontaneous ventilation on lung atelectasis during recovery from anesthesia for laparoscopic gastric sleeve surgery. Anaesth Pain Intensive Care. 2023;27(3):301-307. |
Wrong intervention/comparison |
|
Abrard S, Rineau E, Seegers V, Lebrec N, Sargentini C, Jeanneteau A, Longeau E, Caron S, Callahan JC, Chudeau N, Beloncle F, Lasocki S, Dupoiron D. Postoperative prophylactic intermittent noninvasive ventilation versus usual postoperative care for patients at high risk of pulmonary complications: a multicentre randomised trial. Br J Anaesth. 2023 Jan;130(1):e160-e168. doi: 10.1016/j.bja.2021.11.033. Epub 2022 Jan 5. PMID: 34996593. |
Wrong surgery (also includes pulmonary surgery, no separate results reported) |
|
Amaru P, Delannoy B, Genty T, Desebbe O, Laverdure F, Rezaiguia-Delclaux S, Stéphan F. Effect of Recruitment Maneuvers and PEEP on Respiratory Failure After Cardiothoracic Surgery in Obese Subjects: A Randomized Controlled Trial. Respir Care. 2021 Aug;66(8):1306-1314. doi: 10.4187/respcare.08607. Epub 2021 May 11. PMID: 33975901. |
Wrong intervention/comparison, wrong type of surgery (cardiothoracic) |
|
Ball L, Almondo C, Pelosi P. Perioperative Lung Protection: General Mechanisms and Protective Approaches. Anesth Analg. 2020 Dec;131(6):1789-1798. doi: 10.1213/ANE.0000000000005246. PMID: 33186165. |
Relevant studies from this SR already included via SR Hui (2022) |
|
Blecha S, Hager A, Gross V, Seyfried T, Zeman F, Lubnow M, Burger M, Pawlik MT. Effects of Individualised High Positive End-Expiratory Pressure and Crystalloid Administration on Postoperative Pulmonary Function in Patients Undergoing Robotic-Assisted Radical Prostatectomy: A Prospective Randomised Single-Blinded Pilot Study. J Clin Med. 2023 Feb 12;12(4):1460. doi: 10.3390/jcm12041460. PMID: 36835995; PMCID: PMC9960679. |
Wrong intervention/comparison |
|
Boscolo A, Pettenuzzo T, Sella N, Zatta M, Salvagno M, Tassone M, Pretto C, Peralta A, Muraro L, Zarantonello F, Bruni A, Geraldini F, De Cassai A, Navalesi P. Noninvasive respiratory support after extubation: a systematic review and network meta-analysis. Eur Respir Rev. 2023 Apr 5;32(168):220196. doi: 10.1183/16000617.0196-2022. Erratum in: Eur Respir Rev. 2023 Jun 21;32(168):225196. doi: 10.1183/16000617.5196-2022. PMID: 37019458; PMCID: PMC10074166. |
Wrong population (adult ICU patients, not necessarily post-operative)
|
|
Burra V, Putta G, Prasad SR, Manjunath V. A prospective study on use of thrive (transnasal humidified rapid insufflation ventilatory exchange) versus conventional nasal oxygenation following extubation of adult cardiac surgical patients. Ann Card Anaesth. 2021 Jul-Sep;24(3):353-357. doi: 10.4103/aca.ACA_16_20. PMID: 34269267; PMCID: PMC8404600. |
Wrong type of surgery (cardiac) |
|
Chaudhuri D, Granton D, Wang DX, Burns KEA, Helviz Y, Einav S, Trivedi V, Mauri T, Ricard JD, Mancebo J, Frat JP, Jog S, Hernandez G, Maggiore SM, Mbuagbaw L, Hodgson CL, Jaber S, Goligher EC, Brochard L, Rochwerg B. High-Flow Nasal Cannula in the Immediate Postoperative Period: A Systematic Review and Meta-analysis. Chest. 2020 Nov;158(5):1934-1946. doi: 10.1016/j.chest.2020.06.038. Epub 2020 Jun 29. PMID: 32615190. |
No relevant RCTs included in SR (wrong surgery type) |
|
Ferreyro BL, Angriman F, Munshi L, Del Sorbo L, Ferguson ND, Rochwerg B, Ryu MJ, Saskin R, Wunsch H, da Costa BR, Scales DC. Association of Noninvasive Oxygenation Strategies With All-Cause Mortality in Adults With Acute Hypoxemic Respiratory Failure: A Systematic Review and Meta-analysis. JAMA. 2020 Jul 7;324(1):57-67. doi: 10.1001/jama.2020.9524. PMID: 32496521; PMCID: PMC7273316. |
Wrong population (patients with acute hypoxemic respiratory failure) |
|
Frei DR, Beasley R, Campbell D, Forbes A, Leslie K, Mackle D, Martin C, Merry A, Moore MR, Myles PS, Ruawai-Hamilton L, Short TG, Young PJ. A vanguard randomised feasibility trial comparing three regimens of peri-operative oxygen therapy on recovery after major surgery. Anaesthesia. 2023 Oct;78(10):1272-1284. doi: 10.1111/anae.16103. Epub 2023 Aug 2. PMID: 37531294. |
Wrong intervention/comparison (3 peri-operative regimens) |
|
Kokotovic D, Berkfors A, Gögenur I, Ekeloef S, Burcharth J. The effect of postoperative respiratory and mobilization interventions on postoperative complications following abdominal surgery: a systematic review and meta-analysis. Eur J Trauma Emerg Surg. 2021 Aug;47(4):975-990. doi: 10.1007/s00068-020-01522-x. Epub 2020 Oct 7. PMID: 33026459. |
Relevant studies from this SR already included via SR Hui (2022) |
|
Li J, Jing G, Scott JB. Year in Review 2019: High-Flow Nasal Cannula Oxygen Therapy for Adult Subjects. Respir Care. 2020 Apr;65(4):545-557. doi: 10.4187/respcare.07663. PMID: 32213602. |
Wrong study design (narrative review) |
|
Li R, Liu L, Wei K, Zheng X, Zeng J, Chen Q. Effect of noninvasive respiratory support after extubation on postoperative pulmonary complications in obese patients: A systematic review and network meta-analysis. J Clin Anesth. 2023 Dec;91:111280. doi: 10.1016/j.jclinane.2023.111280. Epub 2023 Oct 4. PMID: 37801822. |
Also includes wrong types of surgery (cardiac), relevant studies already included via SR Hui (2022) or individually |
|
Liu C, Lin Q, Li D. High-flow nasal cannula therapy versus conventional oxygen therapy for adult patients after cardiac surgery: A systemic review and meta-analysis. Heart Lung. 2024 Jun-Aug;66:47-55. doi: 10.1016/j.hrtlng.2024.03.008. Epub 2024 Apr 6. PMID: 38582067. |
Wrong type of surgery (cardiac) |
|
Lockstone J, Denehy L, Truong D, Whish-Wilson GA, Boden I, Abo S, Parry SM. Prophylactic Postoperative Noninvasive Ventilation in Adults Undergoing Upper Abdominal Surgery: A Systematic Review and Meta-Analysis. Crit Care Med. 2022 Oct 1;50(10):1522-1532. doi: 10.1097/CCM.0000000000005628. Epub 2022 Jul 26. PMID: 35881511. |
Relevant studies already included via SR Hui (2022) |
|
Lockstone J, Parry SM, Denehy L, Robertson IK, Story D, Boden I. Non-Invasive Positive airway Pressure thErapy to Reduce Postoperative Lung complications following Upper abdominal Surgery (NIPPER PLUS): a pilot randomised control trial. Physiotherapy. 2022 Dec;117:25-34. doi: 10.1016/j.physio.2022.06.001. Epub 2022 Jun 13. PMID: 36242928. |
Wrong intervention (physiotherapy-led non-invasive ventilation) |
|
Lu Z, Chang W, Meng S, Xue M, Xie J, Xu J, Qiu H, Yang Y, Guo F. The Effect of High-Flow Nasal Oxygen Therapy on Postoperative Pulmonary Complications and Hospital Length of Stay in Postoperative Patients: A Systematic Review and Meta-Analysis. J Intensive Care Med. 2020 Oct;35(10):1129-1140. doi: 10.1177/0885066618817718. Epub 2018 Dec 26. PMID: 30587060. |
No relevant RCTs in systematic review (due to surgery type and therapeutic interventions) |
|
Lusquinhos J, Tavares M, Abelha F. Postoperative Pulmonary Complications and Perioperative Strategies: A Systematic Review. Cureus. 2023 May 9;15(5):e38786. doi: 10.7759/cureus.38786. PMID: 37303413; PMCID: PMC10249998. |
No relevant studies in SR |
|
Mishra S, Kothari N, Sharma A, Goyal S, Rathod D, Meshram T, Bhatia P. Comparison of Oxygen Delivery Devices in Postoperative Patients with Hypoxemia: An Open-labeled Randomized Controlled Study. Indian J Crit Care Med. 2024 Mar;28(3):294-298. doi: 10.5005/jp-journals-10071-24659. PMID: 38477006; PMCID: PMC10926037. |
Wrong population (hypoxemic patients) |
|
Mutar MF, Ben Hamada H, Askar TRM, Hassini L, Naija W, Kahloul M. Intraoperative Use of High-Flow Nasal Cannula in Elderly Patients Undergoing Hip Fracture Repair Under Spinal Anesthesia: A Randomized Controlled Study. Cureus. 2024 Mar 9;16(3):e55846. doi: 10.7759/cureus.55846. PMID: 38590487; PMCID: PMC11001159. |
Wrong intervention (intra-operative) |
|
Odor PM, Bampoe S, Gilhooly D, Creagh-Brown B, Moonesinghe SR. Perioperative interventions for prevention of postoperative pulmonary complications: systematic review and meta-analysis. BMJ. 2020 Mar 11;368:m540. doi: 10.1136/bmj.m540. PMID: 32161042; PMCID: PMC7190038. |
Wrong intervention (perioperative interventions) |
|
Osterkamp JTF, Strandby RB, Henningsen L, Marcussen KV, Thomsen T, Mortensen CR, Achiam MP, Jans Ø. Comparing the effects of continuous positive airway pressure via mask or helmet interface on oxygenation and pulmonary complications after major abdominal surgery: a randomized trial. J Clin Monit Comput. 2023 Feb;37(1):63-70. doi: 10.1007/s10877-022-00857-7. Epub 2022 Apr 16. PMID: 35429325; PMCID: PMC9013185. |
Wrong comparison (2 types of CPAP, no control group) |
|
Pettenuzzo T, Boscolo A, Pistollato E, Pretto C, Giacon TA, Frasson S, Carbotti FM, Medici F, Pettenon G, Carofiglio G, Nardelli M, Cucci N, Tuccio CL, Gagliardi V, Schiavolin C, Simoni C, Congedi S, Monteleone F, Zarantonello F, Sella N, De Cassai A, Navalesi P. Effects of non-invasive respiratory support in post-operative patients: a systematic review and network meta-analysis. Crit Care. 2024 May 8;28(1):152. doi: 10.1186/s13054-024-04924-0. PMID: 38720332; PMCID: PMC11077852. |
Wrong type of surgery (also includes pulmonary and cardiac surgery), wrong type of intervention (also includes therapeutic respiratory support) |
|
Pieczkoski SM, de Oliveira AL, Haeffner MP, Azambuja ACM, Sbruzzi G. Positive expiratory pressure in postoperative cardiac patients in intensive care: A randomized controlled trial. Clin Rehabil. 2021 May;35(5):681-691. doi: 10.1177/0269215520972701. Epub 2020 Nov 24. PMID: 33233946. |
Wrong type of surgery (cardiac) |
|
PRISM trial group. Postoperative continuous positive airway pressure to prevent pneumonia, re-intubation, and death after major abdominal surgery (PRISM): a multicentre, open-label, randomised, phase 3 trial. Lancet Respir Med. 2021 Nov;9(11):1221-1230. doi: 10.1016/S2213-2600(21)00089-8. Epub 2021 Jun 18. Erratum in: Lancet Respir Med. 2021 Sep;9(9):e95. doi: 10.1016/S2213-2600(21)00371-4. PMID: 34153272. |
Already included via SR Hui (2022) |
|
Rosén J, Frykholm P, Fors D. Effect of high-flow nasal oxygen on postoperative oxygenation in obese patients: A randomized controlled trial. Health Sci Rep. 2022 Apr 18;5(3):e616. doi: 10.1002/hsr2.616. PMID: 35509395; PMCID: PMC9059212. |
No relevant outcomes reported |
|
Salal, M., Ubaid, S., Batool, A., Razzaq, M., Rana, M., Suleman, H., ... & Muneeb, M. (2022). Effect of Continuous Positive Airway Pressure in Phase-I Cardiac Rehabilitation after CABG. Pakistan Journal of Medical & Health Sciences, 16(09), 501-501. |
Wrong type of surgery (cardiac) |
|
Theologou S, Ischaki E, Zakynthinos SG, Charitos C, Michopanou N, Patsatzis S, Mentzelopoulos SD. High Flow Oxygen Therapy at Two Initial Flow Settings versus Conventional Oxygen Therapy in Cardiac Surgery Patients with Postextubation Hypoxemia: A Single-Center, Unblinded, Randomized, Controlled Trial. J Clin Med. 2021 May 12;10(10):2079. doi: 10.3390/jcm10102079. PMID: 34066244; PMCID: PMC8151420. |
Wrong type of surgery (cardiac), wrong population (hypoxemic patients) |
|
Xiang GL, Wu QH, Xie L, Song JQ, Wu X, Hao SY, Zhong M, Li SQ. High flow nasal cannula versus conventional oxygen therapy in postoperative patients at high risk for pulmonary complications: A systematic review and meta-analysis. Int J Clin Pract. 2021 Mar;75(3):e13828. doi: 10.1111/ijcp.13828. Epub 2020 Nov 30. PMID: 33169477. |
Wrong type of surgery (also includes pulmonary and cardiac surgery) |
|
Zayed Y, Kheiri B, Barbarawi M, Rashdan L, Gakhal I, Ismail E, Kerbage J, Rizk F, Shafi S, Bala A, Sidahmed S, Bachuwa G, Seedahmed E. Effect of oxygenation modalities among patients with postoperative respiratory failure: a pairwise and network meta-analysis of randomized controlled trials. J Intensive Care. 2020 Jul 17;8:51. doi: 10.1186/s40560-020-00468-x. PMID: 32690993; PMCID: PMC7366473. |
Wrong population (patients with postoperative respiratory failure) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 29-09-2025
Beoordeeld op geldigheid : 09-07-2025
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met een hoog risico op pulmonale complicaties die een niet-pulmonale ingreep ondergaan.
Werkgroep
Drs. R.P. (Peter) Meijer (voorzitter), anesthesioloog, NVA
Dr. J.P. (Jop) van den Berg, anesthesioloog, NVA
Dr. S.N.T. (Sabrine) Hemmes, anesthesioloog, NVA
Dr. M. (Marije) Marsman, anesthesioloog, NVA
Drs. M.W. (Mart) Groot, anesthesioloog-intensivist, NVIC
Drs. M. (Marjolein) van Laren, longarts, NVALT
Klankbordgroep
Dr. M. (Martijn) Boon, anesthesioloog, NVA
Drs. J.L.A (Jurriën) Embrechts, KNO-arts, NVKNO
Dr. H.J. (Erik) Hulzebos, klinisch inspanningsfysioloog en (sport)fysiotherapeut, KNGF
Drs. Y.J. (Yvonne) Kappe, senior beleidsadviseur/ patiëntvertegenwoordiger, Longfonds
Met ondersteuning van
Drs. F. (Femke) Janssen, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten, t/m mei 2023
Drs. A.E. (Amber) van der Meij, adviseur, Kennisinstituut van de Federatie Medisch Specialisten, vanaf maart 2023
Dr. M.S. (Matthijs) Ruiter, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Romke Peter Meijer (voorzitter) |
Anesthesioloog, Amsterdam UMC adjunct medisch directeur, Amsterdam UMC tot 1-5-2019
|
Geen |
Geen |
Geen |
|
Johannes Pieter (Jop) van den Berg |
Anesthesioloog in het UMC Groningen, 0,9FTE, betaald. |
Medisch Manager Evenementenzorg, Rode Kruis, vrijwillig (inmiddels afgerond) Lid Medische Raad, Nederlandse Reanimatieraad, vrijwillig |
Uitsluitend de afdeling anesthesiologie ontving (soms) funding voor lopend onderzoek. Er zijn geen individuele financiële conflicten van belangen te vermelden. |
Geen |
|
Marjolein van Laren |
Longarts Dijklander Ziekenhuis Hoorn en Purmerend |
Geen |
Geen |
Geen |
|
Marije Marsman |
Anesthesioloog UMC Utrecht |
Geen |
Artikel gepubliceerd bij NTVG dat gaat over mate van implementatie van deze richtlijn in het UMC Utrecht. |
Geen |
|
Mart Wouter Groot |
Anesthesioloog-intensivist, Erasmus MC |
Geen |
Geen |
Geen |
|
Sabrine Nienke Tallechina Hemmes |
Anesthesioloog, Het Nederlands Kanker Instituut – Antoni van Leeuwenhoek Ziekenhuis, Afdeling Anesthesiologie. |
Geen |
Publicaties over postoperative pulmonale complicaties. Enkele gepubliceerde onderzoeken werden deels gefinancieerd door onderzoek-specifieke beurzen van de ESAIC. |
Geen |
|
Amber van der Meij |
Adviseur, Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Geen |
Geen |
|
Matthijs Ruiter |
Senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Geen |
Geen |
|
Klankbord-groeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Erik Hulzebos
|
Medisch Fysioloog en (sport)fysiotherapeut, UMC Utrecht |
Secretaris VHVL |
Extern gefinancierd onderzoek: Prinses Beatrix Spierfonds |
Geen |
|
Jurriën Embrechts |
Rhinologist / anterior skull base surgeon, Christchurch city hospital, (New Zealand).
|
Data scientist, Expertisecentrum Zorgalgoritmen |
Geen |
Geen |
|
Martijn Boon |
Anesthesioloog Leids Universitair Medisch Centrum |
Geen |
Extern gefinancierd onderzoek: 2. MSD: Invloed van diepe neuromusculaire blokkade op de incidentie van intraoperatieve adverse events, projectleider Ja |
Geen |
|
Yvonne Kappe (Longfonds) |
Senior Beleidsadviseur Longfonds |
Beleidsadviseur astmaVereniging Nederland en Davos |
Geen |
Geen |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland en Longfonds voor de knelpunteninventarisatie en deelname van Longfonds aan de klankbordgroep. De binnengekomen reacties tijdens op de knelpunteninventarisatie zijn besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voorgelegd aan Longfonds en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
|
Module |
Uitkomst kwalitatieve raming |
Toelichting |
|
Postoperatieve ademhalingsondersteuning |
Geen substantiële financiële gevolgen |
De aanbevelingen om niet routinematig ademhalingsondersteuning toe te passen, kunnen leiden tot een reductie in kosten. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase beoordeelde de werkgroep de aanbevelingen uit de eerdere richtlijn Perioperatieve pulmonale complicaties (NVA, 2012) op noodzaak tot revisie. Daarnaast inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met een hoog risico op pulmonale complicaties die een niet-pulmonale ingreep ondergaan. Tevens zijn er knelpunten aangedragen door de NVA, NVKNO en NVKG via een schriftelijke knelpunteninventarisatie. Een overzicht hiervan is opgenomen onder aanverwante producten.
Op basis van de uitkomsten van de knelpunteninventarisatie zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwaliteit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Algemene informatie
|
Database(s): Embase.com, Ovid/Medline |
Datum: 13 februari 2024 en 24 mei 2024 |
|
Periode: vanaf 2020 (RCTs vanaf invoerdatum 27 juli 2021) |
Talen: geen restrictie |
Zoekopbrenst
13-02-2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
142 |
64 |
145 |
|
RCT |
552 |
200 |
570 |
|
Totaal |
|
|
145* |
*in Rayyan
24-05-2024
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
150 |
68 |
154 (waarvan 9 nieuw) |
|
RCT |
470 |
141 |
488 |
|
Totaal |
620 |
209 |
497* |
*in Rayyan
Zoekstrategie
Embase.com 13-02-2024
|
No. |
Query |
Results |
|
#1 |
'postoperative period'/exp OR 'postoperative complication'/de OR postsurg*:ti,ab,kw OR 'post surg*':ti,ab,kw OR postoperati*:ti,ab,kw OR 'post operati*':ti,ab,kw OR ((surgery NEAR/3 (associated OR derived OR induced OR related OR after)):ti,ab,kw) |
1935729 |
|
#2 |
'positive pressure ventilation'/exp OR (('positive pressure' NEAR/3 (breath* OR respirat* OR ventilat* OR constant OR continuous OR intermittent)):ti,ab,kw) OR 'positive airway pressure':ti,ab,kw OR ((hyperbaric NEAR/3 (respirat* OR ventilat*)):ti,ab,kw) OR 'positive end expiratory pressure':ti,ab,kw OR 'positive endexpiratory pressure':ti,ab,kw OR peep:ti,ab,kw OR cpap:ti,ab,kw OR cppb:ti,ab,kw OR cppv:ti,ab,kw OR ippb:ti,ab,kw OR ippv:ti,ab,kw OR bipap:ti,ab,kw OR bpap:ti,ab,kw OR epap:ti,ab,kw OR autoepap:ti,ab,kw OR 'noninvasive ventilation'/exp/mj OR ((('non invasive' OR noninvasive) NEAR/4 (ventilat* OR respir* OR ppv OR 'positive pressure' OR insufflat*)):ti,ab,kw) OR niv:ti,ab,kw OR nippv:ti,ab,kw OR 'ni ppv':ti,ab,kw OR nppv:ti,ab,kw OR 'hfnc':ti,ab,kw OR 'hfno':ti,ab,kw OR ((('high flow' OR highflow OR hf) NEAR/3 (nasal OR oxygen*)):ti,ab,kw) |
114133 |
|
#3 |
#1 AND #2 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab,kw OR child*:ti,ab,kw OR schoolchild*:ti,ab,kw OR infant*:ti,ab,kw OR girl*:ti,ab,kw OR boy*:ti,ab,kw OR teen:ti,ab,kw OR teens:ti,ab,kw OR teenager*:ti,ab,kw OR youth*:ti,ab,kw OR pediatr*:ti,ab,kw OR paediatr*:ti,ab,kw OR puber*:ti,ab,kw) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab,kw OR man:ti,ab,kw OR men:ti,ab,kw OR woman:ti,ab,kw OR women:ti,ab,kw)) AND [2020-2024]/py |
1665 |
|
#4 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1001928 |
|
#5 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
3969998 |
|
#6 |
#3 AND #4 - SR |
142 |
|
#7 |
#3 AND #5 NOT #6 - RCT |
552 |
|
#8 |
#6 OR #7 |
694 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Postoperative Period/ or exp Postoperative Care/ or Postoperative Complications/ or postsurg*.ti,ab,kf. or 'post surg*'.ti,ab,kf. or postoperati*.ti,ab,kf. or 'post operati*'.ti,ab,kf. or (surgery adj3 (associated or derived or induced or related or after)).ti,ab,kf. |
1258824 |
|
2 |
'exp Positive-Pressure Respiration/ or ('positive pressure' adj3 (breath* or respirat* or ventilat* or constant or continuous or intermittent)).ti,ab,kf. or 'positive airway pressure'.ti,ab,kf. or (hyperbaric adj3 (respirat* or ventilat*)).ti,ab,kf. or 'positive end expiratory pressure'.ti,ab,kf. or 'positive endexpiratory pressure'.ti,ab,kf. or (peep or CPAP or CPPB or CPPV or IPPB or IPPV or BiPAP or BPAP or epap or autoepap).ti,ab,kf. or exp Noninvasive Ventilation/ or (('non invasive' or noninvasive) adj4 (ventilat* or respir* or ppv or 'positive pressure' or insufflat*)).ti,ab,kf. or niv.ti,ab,kf. or nippv.ti,ab,kf. or 'ni ppv'.ti,ab,kf. or NPPV.ti,ab,kf. or 'hfnc'.ti,ab,kf. or 'hfno'.ti,ab,kf. or (('high flow' or highflow or hf) adj3 (nasal or oxygen*)).ti,ab,kf. |
48650 |
|
3 |
(1 and 2) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) not ((Adolescent/ or Child/ or Infant/ or adolescen*.ti,ab,kf. or child*.ti,ab,kf. or schoolchild*.ti,ab,kf. or infant*.ti,ab,kf. or girl*.ti,ab,kf. or boy*.ti,ab,kf. or teen.ti,ab,kf. or teens.ti,ab,kf. or teenager*.ti,ab,kf. or youth*.ti,ab,kf. or pediatr*.ti,ab,kf. or paediatr*.ti,ab,kf. or puber*.ti,ab,kf.) not (Adult/ or adult*.ti,ab,kf. or man.ti,ab,kf. or men.ti,ab,kf. or woman.ti,ab,kf. or women.ti,ab,kf.)) |
2863 |
|
4 |
limit 3 to yr="2020 -Current" |
663 |
|
5 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
726274 |
|
6 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2690929 |
|
7 |
4 and 5 - SR |
64 |
|
8 |
(4 and 6) not 7 - RCT |
200 |
|
9 |
7 or 8 |
264 |
Embase.com 24-05-2024
|
No. |
Query |
Results |
|
#1 |
'postoperative period'/exp OR 'postoperative complication'/de OR postsurg*:ti,ab,kw OR 'post surg*':ti,ab,kw OR postoperati*:ti,ab,kw OR 'post operati*':ti,ab,kw OR ((surgery NEAR/3 (associated OR derived OR induced OR related OR after)):ti,ab,kw) |
1971364 |
|
#2 |
'positive pressure ventilation'/exp OR (('positive pressure' NEAR/3 (breath* OR respirat* OR ventilat* OR constant OR continuous OR intermittent)):ti,ab,kw) OR 'positive airway pressure':ti,ab,kw OR ((hyperbaric NEAR/3 (respirat* OR ventilat*)):ti,ab,kw) OR 'positive end expiratory pressure':ti,ab,kw OR 'positive endexpiratory pressure':ti,ab,kw OR peep:ti,ab,kw OR cpap:ti,ab,kw OR cppb:ti,ab,kw OR cppv:ti,ab,kw OR ippb:ti,ab,kw OR ippv:ti,ab,kw OR bipap:ti,ab,kw OR bpap:ti,ab,kw OR epap:ti,ab,kw OR autoepap:ti,ab,kw OR 'noninvasive ventilation'/exp/mj OR ((('non invasive' OR noninvasive) NEAR/4 (ventilat* OR respir* OR ppv OR 'positive pressure' OR insufflat*)):ti,ab,kw) OR niv:ti,ab,kw OR nippv:ti,ab,kw OR 'ni ppv':ti,ab,kw OR nppv:ti,ab,kw OR 'hfnc':ti,ab,kw OR 'hfno':ti,ab,kw OR ((('high flow' OR highflow OR hf) NEAR/3 (nasal OR oxygen*)):ti,ab,kw) |
116530 |
|
#3 |
#1 AND #2 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab,kw OR child*:ti,ab,kw OR schoolchild*:ti,ab,kw OR infant*:ti,ab,kw OR girl*:ti,ab,kw OR boy*:ti,ab,kw OR teen:ti,ab,kw OR teens:ti,ab,kw OR teenager*:ti,ab,kw OR youth*:ti,ab,kw OR pediatr*:ti,ab,kw OR paediatr*:ti,ab,kw OR puber*:ti,ab,kw) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab,kw OR man:ti,ab,kw OR men:ti,ab,kw OR woman:ti,ab,kw OR women:ti,ab,kw)) AND [2020-2024]/py |
1789 |
|
#4 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1031375 |
|
#5 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4038853 |
|
#6 |
#3 AND #4 - SR |
150 |
|
#7 |
#3 AND #5 NOT #6 AND [27-07-2021]/sd - RCT |
470 |
|
#8 |
#6 OR #7 |
620 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Postoperative Period/ or exp Postoperative Care/ or Postoperative Complications/ or postsurg*.ti,ab,kf. or 'post surg*'.ti,ab,kf. or postoperati*.ti,ab,kf. or 'post operati*'.ti,ab,kf. or (surgery adj3 (associated or derived or induced or related or after)).ti,ab,kf. |
1277269 |
|
2 |
'exp Positive-Pressure Respiration/ or ('positive pressure' adj3 (breath* or respirat* or ventilat* or constant or continuous or intermittent)).ti,ab,kf. or 'positive airway pressure'.ti,ab,kf. or (hyperbaric adj3 (respirat* or ventilat*)).ti,ab,kf. or 'positive end expiratory pressure'.ti,ab,kf. or 'positive endexpiratory pressure'.ti,ab,kf. or (peep or CPAP or CPPB or CPPV or IPPB or IPPV or BiPAP or BPAP or epap or autoepap).ti,ab,kf. or exp Noninvasive Ventilation/ or (('non invasive' or noninvasive) adj4 (ventilat* or respir* or ppv or 'positive pressure' or insufflat*)).ti,ab,kf. or niv.ti,ab,kf. or nippv.ti,ab,kf. or 'ni ppv'.ti,ab,kf. or NPPV.ti,ab,kf. or 'hfnc'.ti,ab,kf. or 'hfno'.ti,ab,kf. or (('high flow' or highflow or hf) adj3 (nasal or oxygen*)).ti,ab,kf. |
49497 |
|
3 |
(1 and 2) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) not ((Adolescent/ or Child/ or Infant/ or adolescen*.ti,ab,kf. or child*.ti,ab,kf. or schoolchild*.ti,ab,kf. or infant*.ti,ab,kf. or girl*.ti,ab,kf. or boy*.ti,ab,kf. or teen.ti,ab,kf. or teens.ti,ab,kf. or teenager*.ti,ab,kf. or youth*.ti,ab,kf. or pediatr*.ti,ab,kf. or paediatr*.ti,ab,kf. or puber*.ti,ab,kf.) not (Adult/ or adult*.ti,ab,kf. or man.ti,ab,kf. or men.ti,ab,kf. or woman.ti,ab,kf. or women.ti,ab,kf.)) |
2907 |
|
4 |
limit 3 to yr="2020 -Current" |
708 |
|
5 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
748214 |
|
6 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2729562 |
|
7 |
4 and 5 - SR |
68 |
|
8 |
(4 and 6) not 7 |
217 |
|
9 |
limit 8 to dt="20210727-20240524" - RCT |
141 |
|
10 |
7 or 9 |
209 |