Anesthesietechniek
Uitgangsvraag
Aanbeveling
Informeer pulmonaal belaste patiënten over het kleine voordeel van locoregionale technieken in plaats van algehele anesthesie ten aanzien van de kans op postoperatieve pulmonale complicaties.
Beslis samen met de patiënt welke anesthesietechniek het meest passend is.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is literatuuronderzoek gedaan naar het verschil in incidentie van PPC’s tussen regionale en algehele anesthesie bij pulmonaal belaste patiënten die niet-pulmonaire chirurgie ondergaan. Op basis van drie observationele studies lijkt regionale anesthesie de incidentie van PPC’s te verminderen bij patiënten met COPD die abdominale chirurgie of een grote operatie aan de extremiteiten ondergaan. De bewijskracht is door het observationele karakter van de studies laag.
In de niet pulmonaal belaste populatie zijn ook enkele studies die beschrijven dat het aantal PPC’s gereduceerd wordt bij regionale anesthesie. Een studie van Regan (2013) laat algehele anesthesie als voorspeller voor postoperatieve pulmonale complicaties bij patiënten met COPD zien. Omdat in deze studie niet geheel duidelijk wordt welke ‘andere strategieën’ er zijn toegepast, kon deze in de literatuurstudie zoals eerder genoemd niet worden meegenomen. In een meta-analyse van patiënten die een amputatie van de onderste extremiteit ondergingen (Mufarrih, 2023) kwam naar voren dat het gebruik van algehele anesthesie geassocieerd wordt met een hogere kans op postoperatief respiratoir falen en sepsis, maar niet op andere morbiditeiten, opnameduur of 30 dagen mortaliteit. Li en collega’s (2023) verrichtten een review en meta-analyse naar het verschil van uitkomsten tussen locoregionale anesthesie en algehele anesthesie bij patiënten die revascularisaties van de onderste extremiteiten ondergingen. Hier werd bij gerandomiseerde studies wel een verschil gezien in pulmonale complicaties ten gunste van locoregionale anesthesie, maar niet op mortaliteit.
Hoewel de bewijskracht laag is, lijkt een advies in de richting van neuraxiale of locoregionale technieken op zijn plaats om de kans op postoperatief respiratoir falen te verkleinen.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
De anesthesioloog geeft op basis van patiënt kenmerken (zoals gebruik van antistolling) en chirurgische kenmerken (zoals type operatie en operatieduur) aan of er überhaupt een keuze is tussen algehele anesthesie en locoregionale anesthesiologie. Medisch inhoudelijk kan er bij deze keuze aangegeven worden dat ten aanzien van de kans op postoperatieve pulmonale complicaties een medische voorkeur lijkt te zijn voor een locoregionale/neuraxiale techniek bij patiënten met pre-existent longlijden. Ten aanzien van andere uitkomstmaten lijkt er geen verschil te zijn tussen de twee technieken. Er kan aan patiënten aangegeven worden dat wanneer er een pulmonale complicatie optreedt dit ook de kans op langere ziekenhuis opname verhoogt. Naast medisch-inhoudelijke argumenten kunnen ook andere redenen meewegen om een patiënt locoregionale/neuraxiale anesthesie aan te raden boven algehele anesthesie. Uiteindelijk zal de patiënt op basis van de verschillende voor-en nadelen een keuze maken tussen algehele anesthesie en locoregionale/neuraxiale anesthesie.
Kosten (middelenbeslag)
Het voorkomen van PPC’s is een onderdeel van zinnige zorg. PPC’s leiden tot verlengde opnameduur en verhogen ook de kans op opname op een intensive care en de daaropvolgende hoge morbiditeit en mortaliteit. Het voorkomen van deze complicaties zal leiden tot een kostenreductie.
Aanvaardbaarheid, haalbaarheid en implementatie
Locoregionale en neuraxiale technieken behoren tot het standaardarsenaal aan mogelijkheden van de anesthesioloog. De hedendaagse anesthesioloog is vaardig in het toepassen van deze technieken en de adviezen in deze richtlijnen zullen dus logischerwijs niet leiden tot belemmerende factoren.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Locoregionale technieken of neuraxiale technieken, al dan niet in combinatie met algehele anesthesie, zijn eenvoudige, hoogstwaarschijnlijk kosteneffectieve manieren om de kans op PPC’s te verminderen. Het strekt daarom tot de aanbeveling om bij pulmonaal belaste patiënten of patiënten die een verhoogd risico hebben op PPC’s deze technieken mee te nemen in een afweging voor de af te spreken anesthesietechniek. Op basis van de beschikbare literatuur is het niet mogelijk een hard advies uit te brengen voor de keuze voor een anesthesietechniek. Of neuraxiale/locoregionale technieken in combinatie met algehele anesthesie ook bijdragen aan een reductie van PPC’s, is op basis van de beschikbare literatuur niet te concluderen.
Onderbouwing
Introduction
Anaesthesia can be applied in different ways. During general anaesthesia a tube or laryngeal mask is used to assist mechanical ventilation. During locoregional or neuraxial techniques spontaneous ventilation remains. It is unknown whether the type of anaesthesia contributes to the occurrence of pulmonary complications during non-pulmonary surgery. This module aims to provide guidance in the choice of anaesthetic technique and the prevention of pulmonary complications. Procedural sedation (richtlijn Sedatie en analgesie bij volwassenen) is beyond the scope of this module.
|
Low GRADE |
Regional anesthesia (spinal, epidural, or peripheral nerve block) may reduce incidence of PPCs compared to general anesthesia in patients with (severe) COPD undergoing abdominal surgery or major surgery to the extremities.
Sources: Hausman, 2015; Kalko, 2007; Ramkumar, 2023. |
Description of studies
Hausman (2015) compared regional anesthesia with general anesthesia in surgical patients with chronic obstructive pulmonary disease (COPD). Patients who met the National Surgical Quality Improvement Program (NSQIP) definition for severe COPD and underwent surgery under general, spinal, epidural, or peripheral nerve block anesthesia were included in this retrospective propensity-matched cohort study. NSQIP data were collected from 186 hospitals, across a wide variety of case types. Patients were excluded if they required ventilator-assisted respiration within 48 hours before surgery or if they had a preoperative pulmonary infection, as were patients undergoing cardiac surgery, solid organ transplant, emergency surgery, reoperation within 30 days of initial operation, or were American Society of Anesthesiologists (ASA) classification 5 or 6. Matching resulted in 2,644 patients who received regional anesthesia (age 72±10, 59% male) and 2,644 patients who underwent identical operations under general anesthesia (age 71±10, 60% male). Surgical procedures included carotid/vertebral endarterectomy, knee/hip arthroplasty, amputation above/below the knee, inguinal hernia repair, AAA repair, lower extremity bypass surgery or thrombectomy and cystoscopy. The publication did not report PPC as an outcome, but did report pulmonary infection, ventilator dependence and unplanned intubation. The study had low risk of bias.
Kalko (2007) compared the use of epidural with general anesthesia in the treatment of abdominal aortic aneurysms (AAA) through mini-laparotomy in patients with severe chronic obstructive pulmonary disease (COPD). Of 197 patients treated for AAA at the institution, 23 patients who had severe COPD and who received elective infrarenal AAA repair, were retrospectively analyzed. All the operations were performed by a single surgeon through a mini-laparotomy approach. Patients were all male and were divided into two groups : those receiving epidural anaesthesia (Group I, n=10 patients) and those receiving general anaesthesia (Group II, n=13 patients). The mean age was 64 years (range 57 to 71) in group I and 67 years (range 62 to 77) in group II. The diagnosis of severe COPD was established by the presence of one or more of the following criteria: room air PaO2 ≤ 60 mmHg, PaCO2 ≥ 45 mmHg, and FEV1 ≤ 50% and FVC ≤ 75% of predicted value. The were some concerns for risk of bias, due to possible confounding by indication.
Ramkumar (2023) studied COPD patients who underwent elective abdominal surgery in their institution and compared various factors associated with the development of PPC. The prospective observational study (mean age 56.63 ± 8, 78% male) compared general anesthesia (N=130) with regional anesthesia (N=119). A diagnosis of COPD was established based on the GOLD 2016 guidelines. Patients undergoing emergency surgery with an active or past history of pulmonary tuberculosis, restrictive lung diseases, obstructive sleep apnea, severe renal and liver disease, and cardiac disease were excluded from the study. Sixty-one (24.5%) patients underwent laparoscopic abdominal surgery, and 188 (75.5%) underwent laparotomy. The ARISCAT risk index was used to predict PPC. The publication had a high risk of bias, because confounding factors were not considered in the analysis.
Table 1. Study characteristics and results
Study characteristics from the included studies and results for the predefined outcomes are summarized in table 1. Due to differences in outcome definitions, results could not be pooled.
Results
Hausman (2015) reported that the use of general anesthesia in COPD patients was associated with a higher risk of pulmonary infection (3.3% vs 2.3%, absolute difference with 95% confidence interval = 1.0% [95%CI 0.09, 1.88]). There was also a higher risk of prolonged ventilator dependence (2.1% vs 0.9%, risk difference = 1.2% [95%CI 0.51, 1.83]) and a higher risk of unplanned postoperative intubation (2.6% vs 1.8%, risk difference = 0.8% [95%CI 0.04, 1.62]). Patients undergoing general anesthesia had a higher composite morbidity, when including pulmonary complications (15.4% vs 12.6%, risk difference = 2.8% [95%CI 0.93, 4.67]).
Kalko (2017) found that none of the patients operated on under epidural anesthesia developed postoperative respiratory complications. There was one in-hospital mortality due to prolonged entubation and sepsis related to pulmonary infections on the 35th postoperative day from group II.
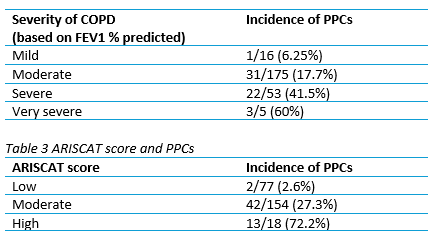
Ramkumar (2023) reported that patients who had surgery under general anesthesia had a significant increase in PPC incidence compared to those who received regional anesthesia (33.8% vs. 10.9%; risk difference: -23% [95%CI -33%, -13%]). Furthermore, the study analyzed the association between PPCs and COPD severity and ARISCAT score. Results are presented in tables 2 and 3, respectively. However, cut-off points for ARISCAT were not specified.
Table 2. COPD severeness and PPCs
Taken together, studies report a lower incidence of PPCs in regional anesthetics (spinal, epidural, or peripheral nerve block) compared to general anesthesia.
Level of evidence of the literature
The level of evidence regarding the outcome measure PPC is based on observational data and therefore starts at low. The level of evidence was not downgraded and was considered LOW.
A systematic review of the literature was performed to answer the following question:
What are the benefits and harms of anesthesia without ventilation compared with general anesthesia in patients with pulmonary precondition undergoing abdominal surgery or major surgery to the extremities?
| P (Patients): | Adult patients with pulmonary precondition undergoing abdominal surgery or major surgery to the extremities |
| I (Intervention): | Neuraxial (spinal, epidural) or locoregional anesthesia (without ventilation) |
| C (Comparison): | General anesthesia |
| O (Outcomes): |
Postoperative pulmonary complications |
Relevant outcome measures
The guideline development group considered postoperative pulmonary complications as a critical outcome measure for decision making. The working group did not define the outcome measure a priori, but followed definitions used in the studies.
Search and select (Methods)
On the May 10, 2024, a systematic search was performed in the databases Embase.com and Ovid/Medline for systematic reviews, RCTs and observational studies comparing different types of anesthesia in patients with pulmonary precondition undergoing abdominal surgery or major surgery to the extremities. The search resulted in 400 unique hits. Studies were selected based on the following criteria: a comparison between anesthesia without ventilation (spinal, epidural or locoregional) and general anesthesia in patients with pulmonary precondition, undergoing non-pulmonary surgery. Sixteen studies were initially selected based on title and abstract screening. After reading the full text, thirteen studies were excluded (see the table with reasons for exclusion under the tab Methods) and three studies were included.
Results
Three observational studies were included in the literature analysis. The assessment of the risk of bias is summarized in the risk of bias table.
- Hausman MS Jr, Jewell ES, Engoren M. Regional versus general anesthesia in surgical patients with chronic obstructive pulmonary disease: does avoiding general anesthesia reduce the risk of postoperative complications? Anesth Analg. 2015 Jun;120(6):1405-12. doi: 10.1213/ANE.0000000000000574. PMID: 25526396.
- Kalko Y, Ugurlucan M, Basaran M, Aydin U, Kafa U, Kosker T, Suren M, Yasar T. Epidural anaesthesia and mini-laparotomy for the treatment of abdominal aortic aneurysms in patients with severe chronic obstructive pulmonary disease. Acta Chir Belg. 2007 Jun;107(3):307-12. doi: 10.1080/00015458.2007.11680062. PMID: 17685259.
- Li A, Dreksler H, Nagpal SK, Brandys T, Jetty P, Dubois L, Parsons Leigh J, Stelfox HT, McIsaac DI, Roberts DJ. Outcomes After Neuraxial or Regional Anaesthesia Instead of General Anaesthesia for Lower Limb Revascularisation Surgery: A Systematic Review and Meta-Analysis of Randomised and Non-Randomised Studies. Eur J Vasc Endovasc Surg. 2023 Mar;65(3):379-390. doi: 10.1016/j.ejvs.2022.10.046. Epub 2022 Nov 3. PMID: 36336286.
- Mufarrih SH, Qureshi NQ, Yunus RA, Katsiampoura A, Quraishi I, Sharkey A, Mahmood F, Matyal R. A systematic review and meta-analysis of general versus regional anesthesia for lower extremity amputation. J Vasc Surg. 2023 May;77(5):1542-1552.e9. doi: 10.1016/j.jvs.2022.10.005. Epub 2022 Oct 13. PMID: 36243265.
- Ramkumar PP, Kalaiyarasan K, Sridhar R, Sendhil R. Postoperative pulmonary complications in chronic obstructive pulmonary disease patients undergoing abdominal surgery in a tertiary care institute. International Journal of Academic Medicine and Pharmacy. 2023; 5 (4) :633-639.
- Regan EA, Radcliff TA, Henderson WG, Cowper Ripley DC, Maciejewski ML, Vogel WB, Hutt E. Improving hip fractures outcomes for COPD patients. COPD. 2013 Feb;10(1):11-9. doi: 10.3109/15412555.2012.723072. Epub 2012 Dec 28. PMID: 23272668.
Risk of bias table for interventions studies (cohort studies based on risk of bias tool by the CLARITY Group at McMaster University)
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors?
|
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables?
|
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed?
|
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Low, Some concerns, High |
|
|
Hausman, 2015 |
Definitely yes
Reason: Participants were selected from a registry |
Definitely yes
Reason: participants were matched by surgery and anesthesia type |
Definitely yes
Reason: selection criteria were used excluding participants with the outcome of interest at the start date |
Probably yes
Reason: patients and interventions were matched. |
Probably yes
Reason: patients were propensity matched. |
Probably yes
Reason: Outcomes were clearly defined. |
Definitely yes
Reason: Follow up was appropriate for the outcome. |
Probably yes
Reason: no problems noted. |
LOW |
|
Kalko, 2007 |
Definitely yes
Reason: patients had similar morbidity and the same intervention by the same surgeon. |
Probably no
Reason: possible confounding by indication in this retrospective analysis. |
Probably yes
Reason: patients were prepared and pre-operative respiratory parameters were analyzed. |
Probably yes
Reason: pre-operative variables were specified and similar between groups at baseline. |
Probably yes
Reason: pre-operative variables included in analysis. |
Probably yes
Reason: Outcomes were clearly defined. |
Definitely yes
Reason: Follow up was appropriate for the outcome. |
Probably yes
Reason: no problems noted. |
Some concerns due to patient selection
|
|
Ramkumar, 2023 |
Probably yes
Reason: COPD and similar intervention. |
Probably no
Reason: possible confounding by indication in this cross sectional analysis. |
Probably yes
Reason: all relevant information was collected pre-operatively |
Probably yes
Reason: questionnaire data with ascertainment rules was used. |
Probably no
Reason: No adjustment for confounding factors. |
Probably yes
Reason: outcomes were clearly defined |
Definitely yes
Reason: Follow up was appropriate for the outcome. |
Probably yes
Reason: no problems noted. |
HIGH
|
Footnotes
Selection of participants Example of low risk of bias: Exposed and unexposed drawn for same administrative database of patients presenting at same points of care over the same time frame
Exposure Examples of low risk of bias: Secure record (e.g. surgical records, pharmacy records); Repeated interview or other ascertainment asking about current use/exposure
Confounding Examples of low risk of bias regarding assessment: Interview of all participants; Self-completed survey from all participants; Review of charts with reproducibility demonstrated; From database with documentation of accuracy of abstraction of prognostic data.
Example of low risk of bias regarding analysis: Comprehensive matching (e.g. with propensity score) or adjustment for all plausible confounding variables
NB: Preferably, the working group determined the minimal set of confounding variables which should be adjusted for. This should be done before the literature search and selection.
Assessment of outcome Examples of low risk of bias: Independent blind assessment; Record linkage; For some outcomes (e.g. fractured hip), reference to the medical record is sufficient to satisfy the requirement for confirmation of the fracture
Follow up Examples of low risk of bias: No missing outcome data; Reasons for missing outcome data unlikely to be related to true outcome (for
survival data, censoring is unlikely to introduce bias); Missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups; Missing data have been imputed using appropriated methods
Co-interventions Example of low risk of bias: Most or all relevant co-interventions that might influence the outcome of interest are documented to be similar in the exposed and unexposed
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Regan EA, Radcliff TA, Henderson WG, Cowper Ripley DC, Maciejewski ML, Vogel WB, Hutt E. Improving hip fractures outcomes for COPD patients. COPD. 2013 Feb;10(1):11-9. doi: 10.3109/15412555.2012.723072. Epub 2012 Dec 28. PMID: 23272668. |
Wrong comparison |
|
Sgroi MD, McFarland G, Mell MW. Utilization of regional versus general anesthesia and its impact on lower extremity bypass outcomes. J Vasc Surg. 2019 Jun;69(6):1874-1879. doi: 10.1016/j.jvs.2018.08.190. Epub 2019 Feb 18. PMID: 30792062. |
wrong population, no useful subgroup data |
|
Zhang G, Chen H, Zha J, Zhang J, Di J, Wang X, Hu X, Xu X, Guo J. Effect of General vs. Regional Anesthesia on Mortality, Complications, and Prognosis in Older Adults Undergoing Hip Fracture Surgery: A Propensity-Score-Matched Cohort Analysis. J Clin Med. 2022 Dec 22;12(1):80. doi: 10.3390/jcm12010080. PMID: 36614881; PMCID: PMC9821019. |
wrong population, no useful subgroup data |
|
Van Orden K, Farber A, Schermerhorn ML, Goodney PP, Kalish JA, Jones DW, Rybin D, Siracuse JJ; Vascular Quality Initiative. Local anesthesia for percutaneous endovascular abdominal aortic aneurysm repair is associated with fewer pulmonary complications. J Vasc Surg. 2018 Oct;68(4):1023-1029.e2. doi: 10.1016/j.jvs.2017.12.064. Epub 2018 Mar 27. PMID: 29602472. |
wrong population, no useful subgroup data |
|
Ayoub CH, Chalhoub V, El-Achkar A, Abou Heidar N, Tamim H, Maroun-Aouad M, El Hajj A. Sedation as an alternative anesthetic technique for frail patients in transurethral resection of the prostate. Ther Adv Urol. 2023 Jan 19;15:17562872221150217. doi: 10.1177/17562872221150217. PMID: 36699641; PMCID: PMC9869224. |
wrong population, no useful subgroup data |
|
Wei C, Gu A, Muthiah A, Fassihi SC, Sculco PK, Nunley RM, Bernstein BA, Liu J, Berger JS. Neuraxial anaesthesia is associated with improved outcomes and reduced postoperative complications in patients undergoing aseptic revision total hip arthroplasty. Hip Int. 2022 Mar;32(2):221-230. doi: 10.1177/1120700020975749. Epub 2020 Nov 26. PMID: 33241947. |
wrong population |
|
Yeh KT, Wu WT, Lee RP, Wang JH, Chen TY. The Incidence of Acute Respiratory Infection Was Higher in the Older Adults with Lower Limb Fracture Who Receive Spinal Anesthesia Than Those Who Receive General Anesthesia. Int J Environ Res Public Health. 2022 Nov 1;19(21):14260. doi: 10.3390/ijerph192114260. PMID: 36361140; PMCID: PMC9654406. |
wrong population |
|
Brovman EY, Wallace FC, Weaver MJ, Beutler SS, Urman RD. Anesthesia Type Is Not Associated With Postoperative Complications in the Care of Patients With Lower Extremity Traumatic Fractures. Anesth Analg. 2019 Oct;129(4):1034-1042. doi: 10.1213/ANE.0000000000004270. PMID: 31219925. |
wrong population |
|
Khetarpal R, Bali K, Chatrath V, Bansal D. Anesthetic considerations in the patients of chronic obstructive pulmonary disease undergoing laparoscopic surgeries. Anesth Essays Res. 2016 Jan-Apr;10(1):7-12. doi: 10.4103/0259-1162.165500. PMID: 26957682; PMCID: PMC4767086. |
Wrong study design: narrative review |
|
Henzler D, Rossaint R, Kuhlen R. Anaesthetic considerations in patients with chronic pulmonary disease. Curr Opin Anaesthesiol. 2003 Jun;16(3):323-30. doi: 10.1097/00001503-200306000-00014. PMID: 17021479. |
Wrong study design: narrative review |
|
Ghanami RJ, Hurie J, Andrews JS, Harrington RN, Corriere MA, Goodney PP, Hansen KJ, Edwards MS. Anesthesia-based evaluation of outcomes of lower-extremity vascular bypass procedures. Ann Vasc Surg. 2013 Feb;27(2):199-207. doi: 10.1016/j.avsg.2012.04.006. Epub 2012 Sep 1. PMID: 22944010; PMCID: PMC4279240. |
Wrong population |
|
Panaretou V, Toufektzian L, Siafaka I, Kouroukli I, Sigala F, Vlachopoulos C, Katsaragakis S, Zografos G, Filis K. Postoperative pulmonary function after open abdominal aortic aneurysm repair in patients with chronic obstructive pulmonary disease: epidural versus intravenous analgesia. Ann Vasc Surg. 2012 Feb;26(2):149-55. doi: 10.1016/j.avsg.2011.04.009. Epub 2011 Oct 22. PMID: 22018500. |
Wrong comparison |
|
Harris AB, Valenzuela J, Andrade N, Agarwal A, Gu A, Golladay G, Thakkar S. Comparison of Pneumonia and Major Complications After Total Joint Arthroplasty With Spinal Versus General Anesthesia: A Propensity-matched Cohort Analysis. J Am Acad Orthop Surg. 2024 Jan 1;32(1):33-40. doi: 10.5435/JAAOS-D-23-00192. Epub 2023 Aug 21. PMID: 37603703. |
wrong population, no useful subgroup data |
Beoordelingsdatum en geldigheid
Publicatiedatum : 29-09-2025
Beoordeeld op geldigheid : 09-07-2025
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met een hoog risico op pulmonale complicaties die een niet-pulmonale ingreep ondergaan.
Werkgroep
Drs. R.P. (Peter) Meijer (voorzitter), anesthesioloog, NVA
Dr. J.P. (Jop) van den Berg, anesthesioloog, NVA
Dr. S.N.T. (Sabrine) Hemmes, anesthesioloog, NVA
Dr. M. (Marije) Marsman, anesthesioloog, NVA
Drs. M.W. (Mart) Groot, anesthesioloog-intensivist, NVIC
Drs. M. (Marjolein) van Laren, longarts, NVALT
Klankbordgroep
Dr. M. (Martijn) Boon, anesthesioloog, NVA
Drs. J.L.A (Jurriën) Embrechts, KNO-arts, NVKNO
Dr. H.J. (Erik) Hulzebos, klinisch inspanningsfysioloog en (sport)fysiotherapeut, KNGF
Drs. Y.J. (Yvonne) Kappe, senior beleidsadviseur/ patiëntvertegenwoordiger, Longfonds
Met ondersteuning van
Drs. F. (Femke) Janssen, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten, t/m mei 2023
Drs. A.E. (Amber) van der Meij, adviseur, Kennisinstituut van de Federatie Medisch Specialisten, vanaf maart 2023
Dr. M.S. (Matthijs) Ruiter, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Romke Peter Meijer (voorzitter) |
Anesthesioloog, Amsterdam UMC adjunct medisch directeur, Amsterdam UMC tot 1-5-2019
|
Geen |
Geen |
Geen |
|
Johannes Pieter (Jop) van den Berg |
Anesthesioloog in het UMC Groningen, 0,9FTE, betaald. |
Medisch Manager Evenementenzorg, Rode Kruis, vrijwillig (inmiddels afgerond) Lid Medische Raad, Nederlandse Reanimatieraad, vrijwillig |
Uitsluitend de afdeling anesthesiologie ontving (soms) funding voor lopend onderzoek. Er zijn geen individuele financiële conflicten van belangen te vermelden. |
Geen |
|
Marjolein van Laren |
Longarts Dijklander Ziekenhuis Hoorn en Purmerend |
Geen |
Geen |
Geen |
|
Marije Marsman |
Anesthesioloog UMC Utrecht |
Geen |
Artikel gepubliceerd bij NTVG dat gaat over mate van implementatie van deze richtlijn in het UMC Utrecht. |
Geen |
|
Mart Wouter Groot |
Anesthesioloog-intensivist, Erasmus MC |
Geen |
Geen |
Geen |
|
Sabrine Nienke Tallechina Hemmes |
Anesthesioloog, Het Nederlands Kanker Instituut – Antoni van Leeuwenhoek Ziekenhuis, Afdeling Anesthesiologie. |
Geen |
Publicaties over postoperative pulmonale complicaties. Enkele gepubliceerde onderzoeken werden deels gefinancieerd door onderzoek-specifieke beurzen van de ESAIC. |
Geen |
|
Amber van der Meij |
Adviseur, Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Geen |
Geen |
|
Matthijs Ruiter |
Senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Geen |
Geen |
|
Klankbord-groeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Erik Hulzebos
|
Medisch Fysioloog en (sport)fysiotherapeut, UMC Utrecht |
Secretaris VHVL |
Extern gefinancierd onderzoek: Prinses Beatrix Spierfonds |
Geen |
|
Jurriën Embrechts |
Rhinologist / anterior skull base surgeon, Christchurch city hospital, (New Zealand).
|
Data scientist, Expertisecentrum Zorgalgoritmen |
Geen |
Geen |
|
Martijn Boon |
Anesthesioloog Leids Universitair Medisch Centrum |
Geen |
Extern gefinancierd onderzoek: 2. MSD: Invloed van diepe neuromusculaire blokkade op de incidentie van intraoperatieve adverse events, projectleider Ja |
Geen |
|
Yvonne Kappe (Longfonds) |
Senior Beleidsadviseur Longfonds |
Beleidsadviseur astmaVereniging Nederland en Davos |
Geen |
Geen |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland en Longfonds voor de knelpunteninventarisatie en deelname van Longfonds aan de klankbordgroep. De binnengekomen reacties tijdens op de knelpunteninventarisatie zijn besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voorgelegd aan Longfonds en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
|
Module |
Uitkomst kwalitatieve raming |
Toelichting |
|
Anesthesietechniek |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn, volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van het zorgpersoneel betreft. Mogelijk leiden de aanbevelingen zelfs tot een reductie in kosten. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase beoordeelde de werkgroep de aanbevelingen uit de eerdere richtlijn Perioperatieve pulmonale complicaties (NVA, 2012) op noodzaak tot revisie. Daarnaast inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met een hoog risico op pulmonale complicaties die een niet-pulmonale ingreep ondergaan. Tevens zijn er knelpunten aangedragen door de NVA, NVKNO en NVKG via een schriftelijke knelpunteninventarisatie. Een overzicht hiervan is opgenomen onder aanverwante producten.
Op basis van de uitkomsten van de knelpunteninventarisatie zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwaliteit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Algemene informatie
|
Database(s): Embase.com, Ovid/Medline |
Datum: 10 mei 2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
46 |
16 |
53 |
|
RCT |
111 |
30 |
123 |
|
Observationele studies |
196 |
81 |
224 |
|
Totaal |
353 |
127 |
400* |
*in Rayyan
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
'asthma'/exp OR 'bronchus hyperreactivity'/exp OR (((airway OR airflow OR repirator*) NEAR/2 (obstruct* OR occlusion* OR closure)):ti,ab,kw) OR ((bronch* NEAR/2 (hyperreactiv* OR 'hyper reactiv*' OR hyperrespons* OR 'hyper respons*')):ti,ab,kw) OR asthma*:ti,ab,kw OR wheez*:ti,ab,kw OR 'chronic obstructive lung disease'/exp OR ('chronic obstructive' NEAR/2 (lung OR pulmonary OR airway)) OR 'copd':ab,ti,kw OR 'chronic bronchitis':ab,ti,kw OR emphysema:ab,ti,kw OR aecopd:ti,ab,kw OR 'lung disease'/de OR 'autoimmune lung disease'/exp OR 'chronic lung disease'/exp OR 'congenital lung disease'/exp OR 'interstitial lung disease'/exp OR 'interstitial syndrome'/exp OR 'lung calcification'/exp OR 'lung emphysema'/exp OR 'obstructive lung disease'/exp OR 'pulmonary vascular disease'/exp OR (((lung* OR pulmon* OR pneumo* OR pleuropulm* OR bronchopulm* OR cardiopulm*) NEAR/3 (disease* OR disorder*)):ti,ab,kw) OR 'lung fibrosis'/exp OR (((pulmon* OR lung* OR interstitial) NEAR/2 (fibros* OR scleros*)):ti,ab,kw) OR 'pneumosclerosis':ti,ab,kw OR (('high risk' NEAR/3 patient*):ti,ab,kw) |
1280420 |
|
#2 |
'surgery'/exp OR 'surgical patient'/exp OR 'surgical risk'/exp OR 'perioperative period'/exp OR 'surgery'/lnk OR surgic*:ti,ab,kw OR surger*:ti,ab,kw OR operation*:ti,ab,kw OR operative:ti,ab,kw OR presurg*:ti,ab,kw OR preoperati*:ti,ab,kw OR perisurg*:ti,ab,kw OR perioperati*:ti,ab,kw OR postsurg*:ti,ab,kw OR postoperati*:ti,ab,kw OR laparoscop*:ti,ab,kw OR intraoperati*:ti,ab,kw |
8009805 |
|
#3 |
'spinal anesthesia'/exp OR 'epidural anesthesia'/exp OR 'regional anesthesia'/exp OR 'locoregional anesthesia'/exp OR 'interscalene block'/exp OR 'femoral nerve block'/exp OR 'ilioinguinal nerve block'/exp OR (((spinal* OR lumbar OR epidural OR region* OR locoregional OR conduction OR neuraxial) NEAR/3 (anaesth* OR anesth* OR block* OR analges*)):ti,ab,kw) OR (((autonomic OR nerve* OR neurogenic OR interscalen* OR supraclavicular OR infraclavicular OR axillary OR 'quadratus lumborum' OR ql OR 'femoral nerve*' OR 'ischiatic nerve' OR 'sciatic nerve' OR 'ischiadic nerve' OR 'nervus ischiadicus' OR 'nervus sciaticus' OR popliteal OR saphenus OR saphenous OR ilioinguinal OR 'transvers* abdomin* plane' OR tap) NEAR/3 block*):ti,ab,kw) OR ((awake NEAR/4 (surg* OR operat*)):ti,ab,kw) |
162249 |
|
#4 |
'pneumonia'/exp OR pneumoni*:ti,ab,kw OR (((lung OR pulmon*) NEAR/3 inflammat*):ti,ab,kw) OR 'disease exacerbation'/de OR exacerbat*:ti,ab,kw OR 'hypoxemia'/exp OR hypoxemi*:ti,ab,kw OR hypoxaemi*:ti,ab,kw OR hypoxidosis:ti,ab,kw OR anoxemia:ti,ab,kw OR anoxaemia:ti,ab,kw OR anoxia:ti,ab,kw OR hypoxi*:ti,ab,kw OR 'pulmonary complication'/exp OR (((pulmonary OR cardiopulmonary OR cardiorespiratory OR respirat* OR lung*) NEAR/3 complication*):ti,ab,kw) OR 'atelectasis'/exp OR atelectasis:ti,ab,kw OR (((pulmonary OR lung*) NEAR/3 (collaps* OR deflat*)):ti,ab,kw) OR 'respiratory failure'/exp OR (((respirat* OR pulmonary OR cardiopulmonary OR cardiorespiratory OR lung*) NEAR/3 (failure OR deficien* OR disturb* OR insufficien* OR arrest OR collaps*)):ti,ab,kw) OR 'bronchospasm'/exp OR bronchospas*:ti,ab,kw OR bronchiospas*:ti,ab,kw OR bronchismus:ti,ab,kw OR bronchostriction:ti,ab,kw OR (((bronchial OR bronchus OR broncho*) NEAR/3 (constrict* OR spasm* OR spastica)):ti,ab,kw) |
1466600 |
|
#5 |
#1 AND #2 AND #3 AND #4 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab,kw OR child*:ti,ab,kw OR schoolchild*:ti,ab,kw OR infant*:ti,ab,kw OR girl*:ti,ab,kw OR boy*:ti,ab,kw OR teen:ti,ab,kw OR teens:ti,ab,kw OR teenager*:ti,ab,kw OR youth*:ti,ab,kw OR pediatr*:ti,ab,kw OR paediatr*:ti,ab,kw OR puber*:ti,ab,kw) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab,kw OR man:ti,ab,kw OR men:ti,ab,kw OR woman:ti,ab,kw OR women:ti,ab,kw)) AND [2000-2024]/py |
782 |
|
#6 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1026297 |
|
#7 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4026349 |
|
#8 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8209389 |
|
#9 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
15055789 |
|
#10 |
#5 AND #6 - SR |
46 |
|
#11 |
#5 AND #7 NOT #10 - RCT |
111 |
|
#12 |
#5 AND (#8 OR #9) NOT (#10 OR #11) - observationeel |
196 |
|
#13 |
#10 OR #11 OR #12 |
353 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
exp Asthma/ or Bronchial Hyperreactivity/ or ((airway or airflow or repirator*) adj2 (obstruct* or occlusion* or closure)).ti,ab,kf. or (bronch* adj2 (hyperreactiv* or hyper reactiv* or hyperrespons* or hyper respons*)).ti,ab,kf. or asthma*.ti,ab,kf. or wheez*.ti,ab,kf. or exp Pulmonary Disease, Chronic Obstructive/ or ('chronic obstructive' adj2 (lung or pulmonary or airway)).ti,ab,kf. or copd.ti,ab,kf. or 'chronic bronchitis'.ti,ab,kf. or exp Emphysema/ or emphysema.ti,ab,kf. or aecopd.ti,ab,kf. or Lung Diseases/ or exp Cystic Fibrosis/ or exp Lung Diseases, Interstitial/ or exp Lung Diseases, Obstructive/ or ((lung* or pulmon* or pneumo* or pleuropulm* or bronchopulm* or cardiopulm*) adj3 (disease* or disorder*)).ti,ab,kf. or Pulmonary Fibrosis/ or ((pulmon* or lung* or interstitial) adj2 (fibros* or scleros*)).ti,ab,kf. or 'pneumosclerosis'.ti,ab,kf. or ('high risk' adj3 patient*).ti,ab,kf. |
735600 |
|
2 |
exp Surgical Procedures, Operative/ or exp Specialties, Surgical/ or su.fs. or exp Perioperative Period/ or surgic*.ti,ab,kf. or surger*.ti,ab,kf. or operation*.ti,ab,kf. or operative.ti,ab,kf. or presurg*.ti,ab,kf. or preoperati*.ti,ab,kf. or perisurg*.ti,ab,kf. or perioperati*.ti,ab,kf. or postsurg*.ti,ab,kf. or postoperati*.ti,ab,kf. or nonsurg*.ti,ab,kf. or nonoperatic*.ti,ab,kf. or laparoscop*.ti,ab,kf. |
5737618 |
|
3 |
exp Anesthesia, Spinal/ or exp Anesthesia, Epidural/ or exp Nerve Block/ or exp Anesthesia, Local/ or ((spinal* or lumbar or epidural or region* or locoregional or conduction or neuraxial) adj3 (anaesth* or anesth* or block* or analges*)).ti,ab,kf. or ((autonomic or nerve* or neurogenic or interscalen* or supraclavicular or infraclavicular or axillary or 'quadratus lumborum' or ql or 'femoral nerve*' or 'ischiatic nerve' or 'sciatic nerve' or 'ischiadic nerve' or 'nervus ischiadicus' or 'nervus sciaticus' or popliteal or saphenus or saphenous or ilioinguinal or 'transvers* abdomin* plane' or tap) adj3 block*).ti,ab,kf. or (awake adj4 (surg* or operat*)).ti,ab,kf. |
116355 |
|
4 |
exp Pneumonia/ or pneumoni*.ti,ab,kf. or ((lung or pulmon*) adj3 inflammat*).ti,ab,kf. or exacerbat*.ti,ab,kf. or Hypoxia/ or exp Hypoxia, Brain/ or hypoxemi*.ti,ab,kf. or hypoxaemi*.ti,ab,kf. or hypoxidosis.ti,ab,kf. or anoxemia.ti,ab,kf. or anoxaemia.ti,ab,kf. or anoxia.ti,ab,kf. or hypoxi*.ti,ab,kf. or ((pulmonary or cardiopulmonary or cardiorespiratory or respirat* or lung*) adj3 complication*).ti,ab,kf. or exp Pulmonary Atelectasis/ or atelectasis.ti,ab,kf. or ((pulmonary or lung*) adj3 (collaps* or deflat*)).ti,ab,kf. or exp Respiratory Insufficiency/ or ((respirat* or pulmonary or cardiopulmonary or cardiorespiratory or lung*) adj3 (failure or deficien* or disturb* or insufficien* or arrest or collaps*)).ti,ab,kf. or exp Bronchial Spasm/ or bronchospas*.ti,ab,kf. or bronchiospas*.ti,ab,kf. or bronchismus.ti,ab,kf. or bronchostriction.ti,ab,kf. or ((bronchial or bronchus or broncho*) adj3 (constrict* or spasm* or spastica)).ti,ab,kf. |
1045826 |
|
5 |
(1 and 2 and 3 and 4) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) not ((Adolescent/ or Child/ or Infant/ or adolescen*.ti,ab,kf. or child*.ti,ab,kf. or schoolchild*.ti,ab,kf. or infant*.ti,ab,kf. or girl*.ti,ab,kf. or boy*.ti,ab,kf. or teen.ti,ab,kf. or teens.ti,ab,kf. or teenager*.ti,ab,kf. or youth*.ti,ab,kf. or pediatr*.ti,ab,kf. or paediatr*.ti,ab,kf. or puber*.ti,ab,kf.) not (Adult/ or adult*.ti,ab,kf. or man.ti,ab,kf. or men.ti,ab,kf. or woman.ti,ab,kf. or women.ti,ab,kf.)) |
484 |
|
6 |
limit 5 to yr="2000 -Current" |
327 |
|
7 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
744780 |
|
8 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2723256 |
|
9 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4721082 |
|
10 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5685434 |
|
11 |
6 and 7 - SR |
16 |
|
12 |
(6 and 8) not 11 - RCT |
30 |
|
13 |
(6 and (9 or 10)) not (11 or 12) - observationeel |
81 |
|
14 |
11 or 12 or 13 |
127 |