Niet-medicamenteuze interventies
Uitgangsvraag
Wat is de plaats van niet-medicamenteuze interventies bij patiënten die een chirurgische procedure ondergaan?
Aanbeveling
Overweeg het gebruik van niet-medicamenteuze interventies ter aanvulling op de postoperatieve pijnbehandeling, ter vermindering van angst en vergroting van comfort en de patiënttevredenheid.
Overweeg binnen de lokale instelling een aantal aanvullende, niet-invasieve technieken te faciliteren als niet-medicamenteuze opties voor de behandeling van postoperatieve pijn.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is een systematische literatuuranalyse uitgevoerd naar de effectiviteit van niet-medicamenteuze interventies op postoperatieve pijn. Hierbij is gekeken naar interventies in drie categorieën, namelijk: 1) massage en relaxatie, 2) communicatie en therapeutische suggestie en 3) virtual reality.
Postoperatieve pijn was de cruciale uitkomstmaat, welke is onderzocht voor de drie categorieën. Voor de categorie ‘massage en relaxatie’ werden er drie systematische reviews, die 4, 5 en 8 studies beschreven, en 13 individuele gerandomiseerde gecontroleerde studies (RCTs) geïncludeerd. Voor de categorie ‘communicatie en therapeutische suggestie’ werden er vier individuele studies geïdentificeerd. Voor de categorie ‘virtual reality’ werden er 1 systematische review die 8 studies beschreef en 1 individuele RCT geïncludeerd.
De studies waren heterogeen in studiepopulatie, type chirurgie, interventie en follow-up (zie tabel 1). De studies waren vaak niet adequaat gerandomiseerd, de maskering van randomisatie was niet adequaat of niet beschreven, de blindering was vaak beperkt, dataverwerking, de analyses en ontbrekende data waren niet goed beschreven en veel trials waren niet geregistreerd. Hierom is bij alle drie de categorieën afgewaardeerd voor methodologische beperkingen (risk of bias, -1). Aanvullend werd afgewaardeerd voor het overschrijven van de grenzen van klinische relevantie (imprecisie, -1) of inclusie van in totaal relatief weinig patiënten (imprecisie, -1). De bewijskracht van de literatuur voor alle drie de categorieën was laag (low GRADE). Hiermee is de overall bewijskracht laag.
De resultaten van de studies in alle drie de categorieën lieten kleine positieve effecten zien. Voor de categorie massage en relaxatie bereikte het verschil de grens van klinische relevantie. Hierdoor kan, met een lage bewijskracht, gezegd worden dat dit type interventie mogelijk de postoperatieve pijn vermindert.
Interventies in de categorieën communicatie en therapeutische suggestie en ook virtual reality lieten kleine positieve effecten zien, maar deze bereikten de grens van klinische relevantie (-1 punt/10 punten) niet.
Op basis van de resultaten met lage bewijskracht kan er richting gegeven worden aan de besluitvorming.
Niet-medicamenteuze interventies kunnen toegevoegd worden aan bestaande medicamenteuze interventies. De werking van niet-medicamenteuze interventies op pijn is niet altijd duidelijk. Indien interventies een positief effect hebben op bijvoorbeeld angst en spanning, zal dit ook de ervaren pijn positief beïnvloeden.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Het belangrijkste doel van het gebruik van niet-medicamenteuze interventies is allereerst de vermindering van postoperatieve pijn. Daarnaast kunnen deze interventies bijdragen aan de ontspanning en afleiding van de patiënt alsmede het verminderen van angst en vergroten van de patiënttevredenheid. Voor het gebruik van ontspannende massage en positief taalgebruik geldt dat er geen bijwerkingen worden ervaren. De virtual reality bril kan wel voor enige desoriëntatie of misselijkheid zorgen.
Kosten (middelenbeslag)
Ontspannende massages worden in sommige ziekenhuizen reeds aangeboden met behulp van vrijwilligers en brengen derhalve geen grote kosten met zich mee. Het scholen van medewerkers in positief taalgebruik vergt wel een investering, evenals de aanschaf van een virtual reality bril en software.
Er is weinig bekend over de kosteneffectiviteit van deze interventies. De interventies lijken over het algemeen eenvoudig uitvoerbaar en de kosten lijken beperkt. Daardoor zou het een relatief goedkope manier zijn om de patiëntbeleving positief te beïnvloeden.
Aanvaardbaarheid, haalbaarheid en implementatie
De keuze van de interventie is zeer sterk afhankelijk van de voorkeur van de patiënt. Niet iedereen staat bijvoorbeeld open voor massage of het gebruik van positieve taal. Wat voor de één ontspannend werkt, werkt bij een ander wellicht helemaal niet. Er lijkt vanuit de literatuur wel een positief effect te komen voor het gebruik van deze interventies ten aanzien van pijn en patiënttevredenheid. Derhalve is het een overweging om een scala aan niet-medicamenteuze technieken te kunnen aanbieden binnen de instelling naar de lokale voorkeuren en mogelijkheden. Een belangrijke voorwaarde voor het gebruik van de interventies is dat de zorgprofessionals op de hoogte zijn van de mogelijkheden en dat allen betrokken bij de zorg op dezelfde wijze communiceren en de positieve invloed van deze interventies uitdragen (bijv. bij positief taalgebruik, maar niet alleen hierbij).
Het op juiste wijze uitvoeren van de interventies vraagt om training, waarvan voor sommige interventies mogelijk in de praktijk te oefenen zijn. Voor andere interventies, zoals hypnose, is uitgebreide scholing nodig.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
De werkgroep ziet potentiële voordelen in het gebruik van niet-medicamenteuze interventies als aanvulling op medicamenteuze therapie ten behoeve van de bestrijding van postoperatieve pijn. Er zijn echter vele niet-medicamenteuze methoden beschikbaar ter afleiding, ontspanning of pijnbestrijding, welke niet allemaal in deze richtlijn zijn onderzocht (bijv. muziek, medische hypnose). Velen van deze methoden zijn relatief makkelijk in te zetten en geven weinig tot geen bijwerkingen. Het gebruik van deze technieken hangt af van de pijndiagnostiek, voorkeur van de patiënt, de lokale beschikbaarheid van noodzakelijke materialen en eventueel (scholing van) personeel.
Het is echter belangrijk dat deze methoden gezien het beperkte effect op pijn (met lage bewijskracht) alleen als aanvullend in combinatie met medicamenteuze interventies ingezet kunnen worden.
Onderbouwing
De huidige situatie is dat er bij het behandelen van postoperatieve pijn veelal medicamenteuze interventies worden toegepast, die systemische bijwerkingen kunnen hebben. Niet-medicamenteuze interventies kunnen de nociceptieve processen in het perifere en centrale zenuwstelsel op verschillende manieren beïnvloeden. Zij dienen ingezet te worden op basis van de bevindingen bij pijndiagnostiek. Zo kan bij zwelling een lidmaat hoog worden gelegd of koude worden toegepast (‘basis’ niet-medicamenteuze interventies).
Wat vaak voorkomt, is een verhoogde arousal in het centrale zenuwstelsel door angst of negatieve verwachtingen, waardoor nociceptie versterkt wordt waargenomen en de pijnbeleving negatief beïnvloed. Het hebben van vertrouwen, comfort en positieve gedachten kan een gunstig effect hebben. Niet-medicamenteuze technieken, gebaseerd op ontspanning, afleiding en het toevoegen van comfort kunnen een belangrijke interventie zijn met weinig extra kosten en/of bijwerkingen.
Er zijn vele niet-medicamenteuze methoden beschikbaar ter afleiding, ontspanning en het aanbrengen van meer comfort. In het kader van deze richtlijn ligt de focus op ontspannende massage, positief taalgebruik en het gebruik van virtual reality.
Er bestaat echter ook literatuur ten aanzien van het gebruik van muziek, medische hypnose en verschillende afleidingstechnieken (welke bijvoorbeeld ook gebruikt worden door de zorgverleners binnen de kindergeneeskunde). Voor het gebruik van muziek verwijzen wij naar de modules ‘muziek in de operatiekamer’. Muziek kan worden ingezet om pijn en angst bij de patiënt te verminderen. Muziek kan in overleg met de patiënt worden aangeboden tijdens de operatie, op de verkoeverkamer en tijdens het postoperatieve verblijft. Hierbij worden de kenmerken van de muziek (frequentie, duur, genre en volume) afgestemd op de voorkeuren van de patiënt. (Muziek rondom de operatie - Richtlijn - Richtlijnendatabase)
Er is ook toenemend bewijs voor het positieve effect van hypnose op postoperatieve pijn (Kekecs, 2014). Daarbij moet nadrukkelijk vermeld worden dat niet iedereen hypnose kan uitvoeren en dat er scholing nodig is voor adequate behandeling van patiënten met hypnose.
|
Low GRADE |
Massage and relaxation interventions may result in less postoperative pain when compared to standard of care or sham procedure in adult surgical patients.
Source: Boitor, 2017, Ju, 2019; Abbaspoor, 2014; Babamohamadi, 2021; Boitor, 2019; Eymir, 2021; Forward, 2015; Gavin, 2006; Hasanpour-Dehkordi, 2019; Koraş, 2019; Lin, 2012; Mizrak Sahin, 2021; Sözen, 2020; Weekes, 2021; Xue, 2016. |
|
Low GRADE |
Communication and therapeutic suggestion interventions may result in little to no difference in postoperative pain when compared to standard of care or sham procedure in adult surgical patients.
Source: Gonzales, 2010; Forward, 2015; Shah, 2021; Nowak, 2020. |
|
Low GRADE |
Virtual reality interventions may result in little to no difference in postoperative pain when compared to standard of care or sham procedure in adult surgical patients.
Source: Ding, 2020; Gianola, 2020. |
A total of 43 studies (25 from systematic review and 18 single RCTs) were included in the analysis of the literature. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
Description of studies
The main characteristics of the studies are provided in Table 1. Different controls were used and studies were conducted in different type of surgery settings. Additional information can be found in the ‘evidence tables’.
Three systematic reviews were included, describing 8, 4 and 5 studies that met the PICO respectively. In addition, 13 individual RCTs were included. The number of patients per arm varied from 15 to 202. In total, 1655 patients were included in the intervention group and 1541 patients in the control group.
Table 1. Study descriptions.
|
Review (if applicable) |
Author |
Year |
N intervention group |
N control group |
Surgery type |
Intervention |
Control |
|
Boitor 2017 |
Albert |
2009 |
126 |
126 |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - body |
Standard of care |
|
Boitor 2017 |
Bauer |
2010 |
62 |
51 |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - body |
standard care with quiet relaxation |
|
Boitor 2017 |
Boitor |
2015 |
21 |
19 |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - hand |
sham massage |
|
Boitor 2017 |
Braun |
2012 |
75 |
71 |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - body |
standard care |
|
Boitor 2017 |
Cutshall |
2010 |
30 |
28 |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - body |
standard care with quiet time |
|
Boitor 2017 |
Kshettry |
2006 |
49 |
50 |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - NS |
standard care with rest period |
|
Boitor 2017 |
Mitchinson |
2007 |
200 |
202 |
64% cardiac surgery requiring sternal incision & 36% abdominal surgery |
Massage - back |
attention control; Comparator 2: |
|
Boitor 2017 |
Najafi |
2014 |
35 |
35 |
Coronary Artery Bypass Graft |
Massage - body |
attention control |
|
Ju, 2019 |
Rejeh |
2013 |
62 |
62 |
NS |
Systematic relaxation |
NS |
|
Ju, 2019 |
Solehati and Rustina |
2015 |
30 |
30 |
Caesarean |
Benson's relaxation |
NS |
|
Ju, 2019 |
Devi and Saharia |
2017 |
20 |
20 |
Appendicectomy, cholecystectomy, hernioplasty, gastrectomy, gastro-jejunostomy |
Progressive muscle relaxation |
NS |
|
Ju, 2019 |
Ismail and Elgzar |
2018 |
40 |
40 |
Caesarean |
Progressive muscle relaxation |
NS |
|
Zimpel, 2020 |
Degirmen |
2010 |
50 |
25 |
Caesarean |
Massage - hand and or foot |
standard of care |
|
Zimpel, 2020 |
Hanan |
2011 |
75 |
75 |
Caesarean |
Massage - hand & foot |
standard of care |
|
Zimpel, 2020 |
Irani |
2015 |
40 |
40 |
Caesarean |
Massage - hand & foot |
standard of care |
|
Zimpel, 2020 |
Sharma |
2019 |
30 |
30 |
Caesarean |
Massage - hand & foot |
standard of care |
|
Zimpel, 2020 |
Varghese |
2014 |
30 |
30 |
Caesarean |
Foot reflexology |
standard of care |
|
|
Abbaspoor |
2014 |
40 |
40 |
Caesarean |
Massage - hand & foot |
attention |
|
|
Babamohamadi |
2021 |
30 |
30 |
Coronary Artery Bypass Graft Surgery |
rhythmic breathing |
Standard of care |
|
|
Boitor |
2019 |
20 |
20 |
Cardiac surgery patients |
Massage - hand |
Standard of care |
|
|
Eymir |
2021 |
55 |
51 |
total knee arthroplasty |
progressive muscle relaxation |
standard physiotherapy alone |
|
|
Forward |
2015 |
75 |
74 |
hip replacement or knee replacement |
M-technique (registered method of structured touch) |
Standard of care |
|
|
Gavin |
2006 |
31 |
27 |
lumbar and spinal surgery |
preoperative relaxation training |
standard preparation alone |
|
|
Hasanpour-Dehkordi |
2019 |
35 |
35 |
gastrointestinal tract surgery |
Progressive muscle relaxation |
standard preparation alone |
|
|
Koraş |
2019 |
85 |
82 |
laparoscopic cholecystectomy surgery |
Massage - foot |
Standard of care |
|
|
Lin |
2012 |
45 |
48 |
joint replacement surgery |
breath relaxation and guided imagery tape |
Standard of care |
|
|
Mizrak Sahin |
2021 |
15 |
15 |
Gynecologic Surgery |
Massage - NS |
Standard of care |
|
|
Sözen |
2020 |
65 |
34 |
laparoscopic cholecystectomy |
Massage - hand |
Standard of care |
|
|
Sözen |
2020 |
63 |
34 |
laparoscopic cholecystectomy |
Massage - foot |
Standard of care |
|
|
Weekes |
2021 |
74 |
72 |
Arthroscopic Rotator Cuff Repair |
relaxation, breathing exercises |
Standard of care |
|
|
Xue |
2016 |
47 |
45 |
Caesarean delivery |
Massage - foot |
Standard of care |
This table presents the author and year, type of surgery, intervention and control regime and number of patients that were included in the study. NS: not specified;
Results
1. Postoperative pain
All of the 26 studies reported postoperative pain. As 24 studies reported the mean (SD) pain score, these studies were pooled in a meta-analysis (figure 1).
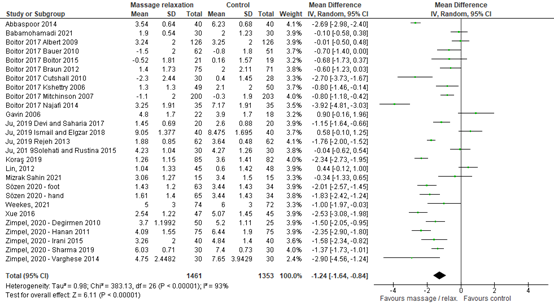
Figure 1: Pain scores ‘massage and relaxation’ studies.
This figure shows the individual study results of studies on the effect of massage and relaxation on postoperative pain. Study details can be found in Table 1 and in the evidence table.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
The pooled analysis shows a standardized mean difference of -1.24 (95% CI -1.64 to -0.84), in favour of the intervention group. This difference does reach the threshold for clinically relevant (-1 point).
Four studies did not report the mean (SD) result and are therefore reported separately.
- Boitor (2019) reported that the median (IQR) pain score was 0 (0 - 7) in the intervention group and 2 (0 - 4.5) in the control group. The median difference was 2, which is a clinically relevant difference in favour of the intervention group.
- Eymir (2021) reported that the median (IQR) pain score was 3.0 (IQR 2.0 - 4.0) in the intervention group and 3.0 (2.0 - 5.0) in the control group. This indicates no difference between groups.
- Forward (2015) reported a mean pain score of 2.6 for the intervention group and 3.6 for the control group. SDs were not provided. The mean difference of 1.0 could be interpreted as a clinically relevant difference, in favour of the intervention group. As the SD is missing, the imprecision of these results cannot be evaluated.
- Hasanpour-Dehkordi (2019) used a continuous scale to assess pain and reported pain severity in 4 categories. It is unclear which scores are included in which categories. In the intervention group, 77% of the patients reported a very low pain level and 23% a low pain level. In the control group, 65% of the patients reported a very low pain level and 35% reported a low pain level. None of the patients reported intermediate or severe pain. It cannot be assessed whether this difference between groups is clinically relevant as the definition of the categories is lacking.
Taken together, the results in this category vary from ‘no difference between groups’ to ‘a clinically relevant difference in favour of the intervention group’.
Level of evidence of the literature
The level of evidence regarding the outcome measure postoperative pain started as high, because the studies were RCTs. The level of evidence was downgraded by two levels because of study limitations (risk of bias -1) and crossing the threshold of clinical relevance (imprecision -1). The level of evidence is low (GRADE).
PICO 2: Communication and therapeutic suggestion
Summary of literature
Description of studies
Four individual RCTs were included. The number of patients per arm varied from 16 to 194. In total, 304 patients were included in the intervention group and 306 patients in the control group.
Table 2. Study descriptions.
|
Review (if applicable) |
Author |
Year |
N intervention group |
N control group |
Surgery type |
Intervention |
Control |
|
|
Gonzales |
2010 |
22 |
22 |
same-day surgical procedures |
Guided imagery |
no intervention |
|
|
Forward |
2015 |
75 |
74 |
hip replacement or knee replacement |
Guided imagery |
Standard of care |
|
|
Shah |
2021 |
16 |
16 |
vaginal hysterectomy with minimally invasive sacrocolpopexy |
therapeutic suggestion |
Standard of care |
|
|
Nowak |
2020 |
191 |
194 |
surgery for 1-3 hours under general anaesthesia |
audiotape of background music and positive suggestions |
blank tape |
This table presents the author and year, type of surgery, intervention and control regime and number of patients that were included in the study. NS: not specified;
Results
1. Postoperative pain
Four studies reported postoperative pain scores after a ‘communication and therapeutic suggestion’ intervention. The studies reported the mean (SD), mean without SD or median (IQR scores). Therefore, results were not pooled.
Gonzales (2010) reported that the mean (SD) score was 20.00 (28.92) in the intervention group and 34.72 (27.54) in the control group (scale 0-100). The MD was -14.72 (95% CI -31.41 to 1.97), in favour of the intervention group. This difference was considered clinically relevant.
Forward (2015) reported that the mean pain score was 2.9 in the intervention group and 3.5 in the control group. No SDs were available. The MD was -0.6, which was not considered clinically relevant.
Shah (2021) reported that the median (IQR) pain score was 4 (3 – 5) in the intervention group and 4 (3 – 5) in the control group, indicating no difference between groups.
Nowask (2020) reported that the median (IQR) score was 4 (3 – 6) in the intervention group and 5 (4 – 7) in the control group. The median difference was -1, in favour of the intervention group. This indicates a clinically relevant difference between groups.
Level of evidence of the literature
The level of evidence regarding the outcome measure postoperative pain started as high, because the studies were RCTs. The level of evidence was downgraded by two levels because of study limitations (risk of bias -1) and number of included patients (imprecision -1). The level of evidence is low (GRADE).
PICO 3: Virtual reality
Summary of literature
Description of studies
One systematic review describing 8 studies that met the PICO was identified. In addition, one individual RCT was included. The number of patients per arm varied from 15 to 91. In total, 407 patients were included in the intervention group and 401 patients in the control group.
Table 3. Study descriptions.
|
Review (if applicable) |
Author |
Year |
N intervention group |
N control group |
Surgery type |
Intervention |
Control |
|
Ding, 2020 |
Bekelis |
2017 |
64 |
63 |
Craniotomy/spine surgery |
Virtual reality |
routine audiovisual descriptions of the operative experience |
|
Ding, 2020 |
Ding |
2019 |
91 |
91 |
Hemorrhoidectomy |
Virtual reality |
Standard pharmacological analgesic intervention |
|
Ding, 2020 |
Jahanishoorab |
2015 |
15 |
15 |
Episiotomy repair |
Virtual reality |
Pharmacological anesthesia |
|
Ding, 2020 |
Jin |
2018 |
33 |
33 |
Knee surgery |
Virtual reality |
Conventional rehabilitation protocol |
|
Ding, 2020 |
Li |
2018 |
39 |
39 |
Knee surgery |
Virtual reality |
Conventional rehabilitation protocol |
|
Ding, 2020 |
Piqueras |
2013 |
72 |
70 |
Knee surgery |
Virtual reality |
Standard clinical protocol of rehabilitation |
|
Ding, 2020 |
Sweta |
2019 |
25 |
25 |
Dental surgery |
Virtual reality |
Local anesthesia |
|
Ding, 2020 |
Yang |
2019 |
24 |
24 |
Knee surgery |
Virtual reality |
standard preoperative information |
|
|
Gianola |
2020 |
44 |
41 |
total knee arthroplasty |
Virtual reality |
traditional rehabilitation |
This table presents the author and year, type of surgery, intervention and control regime and number of patients that were included in the study. NS: not specified;
Results
1. Postoperative pain
For eight studies, the mean (SD) pain score using a VAS scale (0 – 10 points; a higher score indicates more pain) was reported. Figure 2 shows the mean differences of the separate studies. The pooled mean difference was -0.64 (95% CI -1.05 to -0.22). This is not considered a clinically relevant difference.
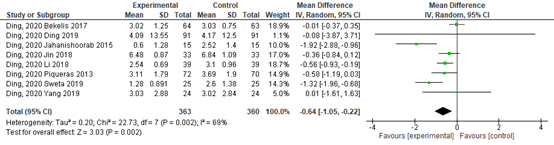
Figure 2: Pain scores ‘virtual reality’ studies.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
Gianola (2020) reported the mean VAS (0-100) difference before en after the intervention. The difference was -23.03 (95% CI -0.26 to -15.79) in the intervention group and -28.97 (95% CI -36.82 to -1.12) in the control group. The difference between these difference scores was -5.94, which is not considered clinically relevant.
Level of evidence of the literature
The level of evidence regarding the outcome measure postoperative pain started as high, because the studies were RCTs. The level of evidence was downgraded by two levels because of study limitations (risk of bias -1) and number of included patients (imprecision -1). The level of evidence is low (GRADE).
A systematic review of the literature was performed to answer the following question:
What is the effectiveness of adding non-pharmacological interventions perioperatively to standard care in surgical patients on postoperative pain, adverse outcomes and rescue analgesic consumption?
Three PICOs were defined:
P patients: Surgical patients.
I intervention: non-pharmacological intervention + standard of care:
I-1: massage and relaxation
I-2: communication and therapeutic suggestion
I-3: virtual reality
C control: Standard of care (+ sham intervention).
O outcome measure: Postoperative pain.
Relevant outcome measures
The guideline development group considered postoperative pain as a critical outcome measure for decision making. The working group defined the outcome measure as follows:
Validated pain scale (Visual Analogue Scale (VAS), Numeric Rating Scale (NRS) or Verbal Rating Scale (VRS)) at post-anesthesia care unit (PACU) arrival.
A priori, the working group did not define the other outcome measures listed above but used the definitions used in the studies. The working group defined one point as a minimal clinically (patient) important difference on a 10-point pain score and 10 mm on a 100 mm pain scale.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 21-7-2021. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 1881 hits. Studies were selected based on the following criteria:
- Systematic review or randomized controlled trials (RCTs)
- Published ≥ 2000
- Patients ≥ 18 years
- Conform PICO
A total of 115 studies was initially selected based on title and abstract screening. After reading the full text, 94 studies were excluded (see the table with reasons for exclusion under the tab Methods) and one study was additionally identified. Four reviews and 18 individuals RCTs were included, describing 43 studies in total.
Results will be provided separately for three categories:
PICO 1: massage and relaxation
PICO 2: communication and therapeutic suggestion
PICO 3: virtual reality
- Abbaspoor Z, Akbari M, Najar S. Effect of foot and hand massage in post-cesarean section pain control: a randomized control trial. Pain Manag Nurs. 2014 Mar;15(1):132-6. doi: 10.1016/j.pmn.2012.07.008. Epub 2013 Jan 24. PMID: 23352729.
- Babamohamadi H, Karkeabadi M, Ebrahimian A. The Effect of Rhythmic Breathing on the Severity of Sternotomy Pain after Coronary Artery Bypass Graft Surgery: A Randomized Controlled Clinical Trial. Evid Based Complement Alternat Med. 2021 Jun 10;2021:9933876. doi: 10.1155/2021/9933876. PMID: 34221093; PMCID: PMC8213490.
- Boitor M, Martorella G, Maheu C, Laizner AM, Gélinas C. Does Hand Massage Have Sustained Effects on Pain Intensity and Pain-Related Interference in the Cardiac Surgery Critically Ill? A Randomized Controlled Trial. Pain Manag Nurs. 2019 Dec;20(6):572-579. doi: 10.1016/j.pmn.2019.02.011. Epub 2019 May 15. PMID: 31103505.
- Boitor M, Gélinas C, Richard-Lalonde M, Thombs BD. The Effect of Massage on Acute Postoperative Pain in Critically and Acutely Ill Adults Post-thoracic Surgery: Systematic Review and Meta-analysis of Randomized Controlled Trials. Heart Lung. 2017 Sep-Oct;46(5):339-346. doi: 10.1016/j.hrtlng.2017.05.005. Epub 2017 Jun 12. PMID: 28619390.
- Ding L, Hua H, Zhu H, Zhu S, Lu J, Zhao K, Xu Q. Effects of virtual reality on relieving postoperative pain in surgical patients: A systematic review and meta-analysis. Int J Surg. 2020 Oct;82:87-94. doi: 10.1016/j.ijsu.2020.08.033. Epub 2020 Aug 31. PMID: 32882400.
- Eymir M, Unver B, Karatosun V. Relaxation exercise therapy improves pain, muscle strength, and kinesiophobia following total knee arthroplasty in the short term: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2022 Aug;30(8):2776-2785. doi: 10.1007/s00167-021-06657-x. Epub 2021 Jul 6. PMID: 34230983.
- Forward JB, Greuter NE, Crisall SJ, Lester HF. Effect of Structured Touch and Guided Imagery for Pain and Anxiety in Elective Joint Replacement Patients--A Randomized Controlled Trial: M-TIJRP. Perm J. 2015 Fall;19(4):18-28. doi: 10.7812/TPP/14-236. Epub 2015 Jul 24. PMID: 26222093; PMCID: PMC4625990.
- Gavin M, Litt M, Khan A, Onyiuke H, Kozol R. A prospective, randomized trial of cognitive intervention for postoperative pain. Am Surg. 2006 May;72(5):414-8. PMID: 16719196.
- Gianola S, Stucovitz E, Castellini G, Mascali M, Vanni F, Tramacere I, Banfi G, Tornese D. Effects of early virtual reality-based rehabilitation in patients with total knee arthroplasty: A randomized controlled trial. Medicine (Baltimore). 2020 Feb;99(7):e19136. doi: 10.1097/MD.0000000000019136. PMID: 32049833; PMCID: PMC7035049.
- Gonzales EA, Ledesma RJ, McAllister DJ, Perry SM, Dyer CA, Maye JP. Effects of guided imagery on postoperative outcomes in patients undergoing same-day surgical procedures: a randomized, single-blind study. AANA J. 2010 Jun;78(3):181-8. PMID: 20572403.
- Hasanpour-Dehkordi A, Solati K, Tali SS, Dayani MA. Effect of progressive muscle relaxation with analgesic on anxiety status and pain in surgical patients. Br J Nurs. 2019 Feb 14;28(3):174-178. doi: 10.12968/bjon.2019.28.3.174. PMID: 30746976.
- Ju W, Ren L, Chen J, Du Y. Efficacy of relaxation therapy as an effective nursing intervention for post-operative pain relief in patients undergoing abdominal surgery: A systematic review and meta-analysis. Exp Ther Med. 2019 Oct;18(4):2909-2916. doi: 10.3892/etm.2019.7915. Epub 2019 Aug 19. PMID: 31555379; PMCID: PMC6755420.
- Kekecs Z, Nagy T, Varga K. The effectiveness of suggestive techniques in reducing postoperative side effects: a meta-analysis of randomized controlled trials. Anesth Analg. 2014 Dec;119(6):1407-19. doi: 10.1213/ANE.0000000000000466. PMID: 25289661.
- Kora? K, Karabulut N. The Effect of Foot Massage on Postoperative Pain and Anxiety Levels in Laparoscopic Cholecystectomy Surgery: A Randomized Controlled Experimental Study. J Perianesth Nurs. 2019 Jun;34(3):551-558. doi: 10.1016/j.jopan.2018.07.006. Epub 2018 Nov 20. PMID: 30470466.
- Lin PC. An evaluation of the effectiveness of relaxation therapy for patients receiving joint replacement surgery. J Clin Nurs. 2012 Mar;21(5-6):601-8. doi: 10.1111/j.1365-2702.2010.03406.x. Epub 2011 Feb 9. PMID: 21306457.
- Mizrak Sahin B, Culha I, Gursoy E, Yalcin OT. Effect of Massage With Lavender Oil on Postoperative Pain Level of Patients Who Underwent Gynecologic Surgery: A Randomized, Placebo-Controlled Study. Holist Nurs Pract. 2021 Jul-Aug 01;35(4):221-229. doi: 10.1097/HNP.0000000000000400. PMID: 32657903.
- Nowak H, Zech N, Asmussen S, Rahmel T, Tryba M, Oprea G, Grause L, Schork K, Moeller M, Loeser J, Gyarmati K, Mittler C, Saller T, Zagler A, Lutz K, Adamzik M, Hansen E. Effect of therapeutic suggestions during general anaesthesia on postoperative pain and opioid use: multicentre randomised controlled trial. BMJ. 2020 Dec 10;371:m4284. doi: 10.1136/bmj.m4284. PMID: 33303476; PMCID: PMC7726311.
- Shah NM, Andriani LA, Mofidi JL, Ingraham CF, Tefera EA, Iglesia CB. Therapeutic Suggestion in Postoperative Pain Control: A Randomized Controlled Trial. Female Pelvic Med Reconstr Surg. 2021 Jul 1;27(7):409-414. doi: 10.1097/SPV.0000000000000906. PMID: 32541300.
- Sözen KK, Karabulut N. Efficacy of Hand and Foot Massage in Anxiety and Pain Management Following Laparoscopic Cholecystectomy: A Controlled Randomized Study. Surg Laparosc Endosc Percutan Tech. 2020 Apr;30(2):111-116. doi: 10.1097/SLE.0000000000000738. PMID: 31855924.
- Weekes DG, Campbell RE, Wicks ED, Hadley CJ, Chaudhry ZS, Carter AH, Pepe MD, Tucker BS, Freedman KB, Tjoumakaris FP. Do Relaxation Exercises Decrease Pain After Arthroscopic Rotator Cuff Repair? A Randomized Controlled Trial. Clin Orthop Relat Res. 2021 May 1;479(5):870-884. doi: 10.1097/CORR.0000000000001723. PMID: 33835103; PMCID: PMC8051979.
- Xue M, Fan L, Ge LN, Zhang Y, Ge JL, Gu J, Wang Y, Chen Y. Postoperative Foot Massage for Patients after Caesarean Delivery. Z Geburtshilfe Neonatol. 2016 Aug;220(4):173-8. doi: 10.1055/s-0042-104802. Epub 2016 Aug 10. PMID: 27509141.
- Zimpel SA, Torloni MR, Porfírio GJ, Flumignan RL, da Silva EM. Complementary and alternative therapies for post-caesarean pain. Cochrane Database Syst Rev. 2020 Sep 1;9:CD011216. doi: 10.1002/14651858.CD011216.pub2. PMID: 32871021.
Evidence tables
(per category; first study descriptives, then results)
Massage and relaxation
|
Review (if applicable) |
Author |
Year |
N INT |
N CNTL |
Age Sex |
Surgery |
Intervention |
Regime |
Control |
Regime |
|
Boitor 2017 |
Albert |
2009 |
126 |
126 |
65 (SD 12) Male: 73% |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - body |
Duration: 30 Frequency/day: 1 Sessions: 2 Protocol: specific (back, arms, legs) |
standard care |
Duration: - Frequency**: - Sessions: - |
|
Boitor 2017 |
Bauer |
2010 |
62 |
51 |
66 (SD 13) Male: 69% |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - body |
Duration: 20 min Frequency/day: 1 Sessions: 2 Protocol: specific (hands, feet, back, arms, legs, neck, shoulders, head, pt preference) |
standard care with quiet relaxation |
Duration: 20 min Frequency**: 1 Sessions: 2 |
|
Boitor 2017 |
Boitor |
2015 |
21 |
19 |
67 (SD 11) Male: 78% |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - hand |
Duration: 15 min Frequency/day: 2e3 Sessions: 2e3 Protocol: specific (hands) |
sham massage |
Duration: 15 min Frequency**: 2-3 Sessions: 2-3 Type: sham massage |
|
Boitor 2017 |
Braun |
2012 |
75 |
71 |
67 (SD 12) Male: 75% |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - body |
Duration: 20 min Frequency/day: 1 Sessions: 2 Protocol: unclear (hands, feet, back, legs, neck, shoulders, head, pt preference) |
standard care |
Duration: 20 min |
|
Boitor 2017 |
Cutshall |
2010 |
30 |
28 |
66 (SD 16) Male: 75% |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - body |
Duration: 20 min Frequency/day: 1 Sessions: 1 Protocol: unclear (back, arms, legs, neck, shoulders, head, pt preference) |
standard care with quiet time |
Duration: 20 min |
|
Boitor 2017 |
Kshettry |
2006 |
49 |
50 |
63 (SD 14) Male: 72% |
Coronary Artery Bypass Graft and/or valve replacement |
Massage - unclear |
Duration: 30 min Frequency/day: 1 Sessions: 1 Protocol: unclear |
standard care with rest period |
Duration: 20 min Frequency**: 1 Sessions: 1 Type: standard care with rest period |
|
Boitor 2017 |
Mitchinson |
2007 |
200 |
202 |
64 (SD 10) Male: 99% |
64% cardiac surgery requiring sternal incision & 36% abdominal surgery |
Massage - back |
Duration: 20 min Frequency/day: 1 Sessions: up to 5 Protocol: specific (back) |
standard of care |
Duration: 20 min Frequency**: 1 Sessions: up to 5 Type: attention control |
|
Boitor 2017 |
Najafi |
2014 |
35 |
35 |
60 (SD 7) Male: 54% |
Coronary Artery Bypass Graft |
Massage - body |
Duration: 30 min Frequency/day: 1 Sessions: 1 Protocol: unclear (hands, feet, back, arms, legs, neck, shoulders, pt preference) |
attention control |
Duration: 30 min |
|
Ju, 2019 |
Rejeh |
2013 |
62 |
62 |
65-92y M: 32 |
NS |
Systematic relaxation |
Relaxation therapy repeated 3 times. Post-test measured after 15 min,6h and 12h recovery following ambulation. |
standard of care |
information about their surgery and the current ward protocols regarding ambulation afterwards |
|
Ju, 2019 |
Solehati and Rustina |
2015 |
30 |
30 |
NS F: 60 |
Caesarean |
Benson's relaxation |
Relaxation therapy performed 2 h after the operation, continued twice daily for 4 days. |
standard of care |
regular care as room procedure |
|
Ju, 2019 |
Devi and Saharia |
2017 |
20 |
20 |
20-40y M: 20 |
Appendicectomy, cholecystectomy, hernioplasty, gastrectomy, gastro-jejunostomy |
Progressive muscle relaxation |
For 3 post-operative days, relaxation therapy performed for 15 min. |
NS |
NS |
|
Ju, 2019 |
Ismail and Elgzar |
2018 |
40 |
40 |
20-35y F: 100% |
Caesarean |
Progressive muscle relaxation |
Relaxation therapy performed thrice daily for 30 min on post-operative days 0 and 1. |
NS |
NS |
|
Zimpel, 2020 |
Degirmen |
2010 |
50 |
25 |
27.3 ± 4.77 F: 100% |
Caesarean |
Massage - hand and or foot |
20 minutes' massage include petrissage, kneading and friction; the foot massage group received 10 minutes' massage. The massage intervention was applied 2.5 ± 1.0 hours after the administration of analgesics in the intervention groups. |
standard of care |
NS |
|
Zimpel, 2020 |
Hanan |
2011 |
75 |
75 |
NS F: 100% |
Caesarean |
Massage - hand & foot |
foot and hand massage for 20 minutes, 5 minutes for each hand then 5 minutes for each foot. The massage was applied 3 times at 5:40, 11:40, 17:40 hour after delivery. |
standard of care |
NS |
|
Zimpel, 2020 |
Irani |
2015 |
40 |
40 |
29.25±4.78 and 29.35±4.88 F: 100% |
Caesarean |
Massage - hand & foot |
massage was performed for 20 minutes on participant’s extremities (5 minutes for each). The main specialised massage techniques included rotational friction movements, stretching, grasping and flexing on different parts of hands and feet from wrist to toes without focusing on a certain point. |
attention |
In the control group, in the other group, the researcher went to the participants’ bedside for 20 minutes, and had an informal chat with them. |
|
Zimpel, 2020 |
Sharma |
2019 |
30 |
30 |
age 21 to 35 years F: 100% |
Caesarean |
Massage - hand & foot |
NS |
|
|
|
Zimpel, 2020 |
Varghese |
2014 |
30 |
30 |
NS F: 100% |
Caesarean |
Foot reflexology |
15-minute foot reflexology session at the same time each evening for five consecutive days. |
|
|
|
|
Abbaspoor 2014 |
2014 |
40 |
40 |
18–35 years; F: 100% |
Caesarean |
Massage - hand & foot |
Foot and hand massage included petrissage, kneading, and friction applied to the patients’ hands and feet. Massage initiated 1.5–2 h after spinal anaesthesia medication. Hand massage applied to each hand for 5 min. Foot massage followed |
attention |
Nurse talked to women for 20 min. Analgesics available for both groups |
|
|
Babamohamadi |
2021 |
30 |
30 |
61.58 ± 9.7 M: 51 |
Coronary Artery Bypass Graft Surgery |
rhythmic breathing |
Patients were asked to close their eyes in the supine position, inhale through the nose, then hold their breath, and exhale through the mouth, while counting from 1 to 3 in each step. All the patients in the intervention group were trained to focus only on air entry and exit while breathing, and they were asked to perform RB once every five minutes, lasting one minute each time, for 20 minutes (totally four times every 20 minutes) [32]. Supervised by researcher, RB was performed every 12 hours (9 a.m. and 9 p.m.) for 3 consecutive days. |
standard of care |
(opioids, such as morphine) with no additional interventions |
|
|
Boitor |
2019 |
20 |
20 |
NS |
cardiac surgery patients |
Massage - hand |
20-minute hand massage |
standard of care |
standard of care, no addition |
|
|
Eymir |
2021 |
55 |
51 |
I: 68.0 (60.5/ 73.0) M: 26 |
total knee arthroplasty |
progressive muscle relaxation |
The PMR therapy was administered according to the instruction of a PMR audiotape prepared by the Psychologists Association. Patients listened to the PMR audiotape using an audio player with headphones and performed the PMR exercise under the supervision of the physiotherapist to be familiarized with the intervention. POD 1 - 3 for 2 times a day |
standard physiotherapy alone |
During the inpatient period, standard PT was administered to all patients twice daily and lasted approximately 30 min. The same physiotherapist delivered the standard PT or PMR exercise+standard PT in patients’ rooms. After discharge, the same home exercise program was given to all patients to be performed twice daily. The standard post-operative PT and home exercise program were administered according to a standardized protocol |
|
|
Forward |
2015 |
75 |
74 |
38 to 90 years M: 33.9% |
hip replacement or knee replacement |
M-technique; The “M” Technique (M) is a registered method of structured touch; series of gentle, slow, stroking movements done in a set sequence that causes the person being touched (receiver) to experience a greater sense of relaxation; focus on repetitive sequences signals |
M was performed on the hands and the feet for 18 to 20 minutes, with touch equally distributed among available extremities, paralleling the length of the guided imagery audio program and the duration of massage shown to be most effective at anxiety and pain reduction in previously reported studies. The level of pressure rendered in M is always 3 on a scale in which the maximum pressure is 10 as perceived by the recipient |
standard of care |
NS |
|
|
Gavin |
2006 |
31 |
27 |
NS |
lumbar and spinal surgery |
preoperative relaxation training |
NS |
standard preparation alone |
NS |
|
|
Hasanpour-Dehkordi |
2019 |
35 |
35 |
NS M: 52% |
gastrointestinal tract surgery |
Progressive muscle relaxation |
training on the method of Benson's relaxation training. Intervention for 20 minutes, every 6 hours for 2 days, until 2 hours before the operation. |
standard preparation alone |
NS |
|
|
Koraş |
2019 |
85 |
82 |
NS Male: 50 female: 117 |
laparoscopic cholecystectomy surgery |
Massage - foot |
1x40 (total 40 min, 20 min for each foot) |
standard of care |
standard of care, no addition |
|
|
Lin |
2012 |
45 |
48 |
71,0 (SD 11,1) y M: 33 (35.5%) |
joint replacement surgery |
breath relaxation and guided imagery tape |
listen to a breath relaxation and guided imagery tape for 20 minutes daily (2x 10 min tape) |
standard of care |
There were no interventions for patients in the control group and, instead, they were encouraged to rest in bed |
|
|
Mizrak Sahin |
2021 |
15 |
15 |
NS |
Gynecologic Surgery |
Massage - unclear |
massage with lavender oil |
standard of care |
standard of care, no addition |
|
|
Sözen |
2020 |
65 |
34 |
51y or older: 47% M: 32.7% |
laparoscopic cholecystectomy |
Hand massage (1/2 treatment arms) |
20 minutes; 10 minutes per hand |
standard of care |
standard of care, no addition |
|
|
Sözen |
2020 |
63 |
34 |
51y or older: 47% M: 32.7% |
laparoscopic cholecystectomy |
Foot Massage (1/2 treatment arms) |
20 minutes; 10 minutes per foot |
standard of care |
standard of care, no addition |
|
|
Weekes |
2021 |
74 |
72 |
60±10 years M: 80/146 (55%) |
Arthroscopic Rotator Cuff Repair |
relaxation, breathing exercises |
Patients in the relaxation group |
standard of care |
All patients in the control and relaxation groups received an ultrasound-guided interscalene nerve block with ropiva-caine preoperatively. The nerve block was per-formed in a similar fashion by board-certified anesthesiologists (nonauthors). General anesthesia was used in all patients. Local anesthesia was not used. The use of postoperative intravenous ketorolac was not standardized. Patients in both groups received 10-mg tablets of oxycodone, 12.5 mg of promethazine hydro-chloride, 100 mg of docusate sodium, and a cold therapy shoulder cuff. If oxycodone tablets could not be prescribed, 10-mg hydrocodone tablets were prescribed. Postoperative NSAID and acetaminophen use was not standardized. |
|
|
Xue |
2016 |
47 |
45 |
25.5±3.77y (range 20-35) F: 100% |
Caesarean delivery |
foot massage |
2.5 ± 1 h after administration of analgesics; 20 minutes foot massage |
standard of care |
standard of care, no addition |
|
Review (if applicable) |
Author |
Year |
follow up |
incomplete data |
outcome measure |
timing of result used in summary |
Result intervention group |
Result control group |
Mean difference [95% CI] (unless stated otherwise) |
|
Boitor 2017 |
Albert |
2009 |
NS |
NS |
VAS 0-10, mean diff score |
2 or 3 days since surgery at 1st administration |
3.24 ± 2 |
3.25 ± 2 |
-0.01 [-0.50, 0.48] |
|
Boitor 2017 |
Bauer |
2010 |
NS |
NS |
VAS 0-10 |
2 days since |
-1,5 ± 2 |
-0,8 ± 1.8 |
-0.70 [-1.40, 0.00] |
|
Boitor 2017 |
Boitor |
2015 |
NS |
NS |
FPT 0-10 |
0 days since |
-0.52 ± 1.81 |
0.16 ± 1.57 |
-0.70 [-1.40, 0.00] |
|
Boitor 2017 |
Braun |
2012 |
NS |
NS |
VAS 0-10 |
3 or 4 days since |
1.4 ± 1.73 |
2 ± 2.11 |
-0.70 [-1.40, 0.00] |
|
Boitor 2017 |
Cutshall |
2010 |
NS |
NS |
VAS 0-10 |
2 - 5 days since |
-2.3 ± 2.44 |
-0.4 ± 1.45 |
-2.70 [-3.73, -1.67] |
|
Boitor 2017 |
Kshettry |
2006 |
NS |
NS |
NRS 0-10 |
2 or 3 days since surgery at 1st administration |
1.3 ± 1.3 |
2.1 ± 2 |
-0.80 [-1.46, -0.14] |
|
Boitor 2017 |
Mitchinson |
2007 |
NS |
NS |
VAS 0-10 |
1 day since surgery at 1st administration |
-1.1 ± 2 |
-0.3 ± 1.9 |
-0.80 [-1.18, -0.42] |
|
Boitor 2017 |
Najafi |
2014 |
NS |
NS |
VAS 0-10 |
3 days since surgery at 1st administration |
7.17±1.71 |
3.25±1.91 |
3.92 [3.07, 4.77] |
|
Ju, 2019 |
Rejeh |
2013 |
up to 12hours after intervention |
NS |
pain score, NS |
12 hours after intervention |
1.88 ± 0.85 |
3.64 ± 0.48 |
-1.76 [-2.00, -1.52] |
|
Ju, 2019 |
Solehati and Rustina |
2015 |
NS |
NS |
pain score, NS |
12 hours after intervention |
4.23 ± 1.04 |
4.27 ± 1.26 |
-0.04 [-0.62, 0.54] |
|
Ju, 2019 |
Devi and Saharia |
2017 |
3 postop days |
NS |
pain score, NS |
1 hour after intervention at postop day 3 |
1.45 ± 0.69 |
2.60 ± 0.88 |
-1.15 [-1.64, -0.66] |
|
Ju, 2019 |
Ismail and Elgzar |
2018 |
3 postop days |
NS |
pain score, VAS |
after 6 sessions, at postop day 3 |
9.050 ± 1.377 |
8.475 ± 1.695 |
0.58 [-0.10, 1.25] |
|
Zimpel, 2020 |
Degirmen |
2010 |
up to 90 minutes after intervention |
NS |
NRS 0-10 |
90 minutes after intervention |
3.7 ± 1.1992 |
5.2 ± 1.11 |
-1.27 [-1.79, -0.74] |
|
Zimpel, 2020 |
Hanan |
2011 |
18 hours after delivery |
NS |
NRS 0-10 |
6 hours after delivery |
4.09 ± 1.55 |
6.44 ± 1.90 |
-1.35 [-1.70, -0.99] |
|
Zimpel, 2020 |
Irani |
2015 |
up to 90 minutes after intervention |
NS |
VAS 0-10 |
90 minutes after the massage |
32.60 ± 20 |
48.40 ± 14 |
-0.91 [-1.37, -0.45] |
|
Zimpel, 2020 |
Sharma |
2019 |
between 48 and 120 hours |
NS |
NS |
Up to 24 hours |
6.03 ± 0.71 |
7.4 ± 0.73 |
-1.88 [-2.49, -1.26] |
|
Zimpel, 2020 |
Varghese |
2014 |
NS |
NS |
NS |
More than 48 up to 120 hours |
4.75 ± 2.4482 |
7.65 ± 3.9429 |
-0.87 [-1.40, -0.34] |
|
|
Abbaspoor 2014 |
2014 |
intervention started 1.5-2 h after spinal medication; measurement 90 min after intervention |
NS |
NRS 0-10 |
90 minutes after intervention; intervention 1.5-2 h after spinal medication. |
3.54 ± 0.64 |
6.23 ± 0.68 |
-2.69 [-2.98, -2.40] |
|
|
Babamohamadi |
2021 |
third day after intervention |
in both groups 2 patients (2/32) were lost to FU during the 3 days intervention |
pain score; VAS 0-10 |
second day after the intervention, 9 a.m. |
1.90 ± 0.54 |
2 ± 1.23 |
-0.10 [-0.58, 0.38] |
|
|
Boitor |
2019 |
24h |
substantial missing data |
NRS 0-10 |
second postoperative day |
median 0 [IQR 0-7] |
median 2 [IQR 0-4.5] |
median diff: -2 |
|
|
Eymir |
2021 |
postop third day |
I: 1 lost to FU |
pain score, NPRS Numeric Pain Rating |
Postop 2nd day |
median 3.0 (IQR 2.0 - 4.0) |
median 3.0 (IQR 2.0 - 5.0) |
median diff: 0 |
|
|
Forward |
2015 |
2 postop days |
none reported |
Numeric Visual Anxiety Scale (NVAS), Pain Numeric Rating Scale (PNRS) |
Postoperative day 1 |
2.6 (SD not provided) |
3.6 (SD not provided) |
-1.0 |
|
|
Gavin |
2006 |
2 postop days |
I: 5/27 |
verbal pain score (0-10) controlled for PACU narcotic use |
postop day 1 |
4.8 ± 1.7; Cl,1.5-8.1; N=22 |
3.9 ± 1.7; CI,0.6-7.2; N=18 |
0.90 [-0.16, 1.96] |
|
|
Hasanpour-Dehkordi |
2019 |
24 hours |
none reported |
Bayer numerical scale, pain; 0 – 10 presented in 4 categories of pain severity (unclear how categories were created) |
24 hours |
Very low 77% |
Very low 65% |
|
|
|
Koraş |
2019 |
120 min after intervention; |
NS |
VAS 0-10 |
120 minutes after intervention |
1.26 ± 1.15 |
3.60 ± 1.41 |
-2.34 [-2.73, -1.95] |
|
|
Lin |
2012 |
postop third day |
NS |
pain score; VAS 0-10; |
Postop 2nd day |
1.04 ± 1.33 |
0.60 ± 1.42 |
0.44 [-0.12, 1.00] |
|
|
Mizrak Sahin |
2021 |
Massage application was performed 3 hours after analgesic application; measurement 30 min & 3h after massage |
NS |
VRS 0-10 |
3rd h after the massage |
3.06 ± 1.27 |
3.40 ± 1.50 |
-0.34 [-1.33, 0.65] |
|
|
Sözen (hand) |
2020 |
150 minutes after massage |
NS |
VAS 0-10 |
150 minutes after massage |
1.61 ± 1.40 |
3.44 ± 1.43 |
-1.83 [-2.42, -1.24] |
|
|
Sözen (foot) |
2020 |
150 minutes after massage |
NS |
VAS 0-10 |
150 minutes after massage |
1.43 ± 1.20 |
3.44 ± 1.43 |
-2.01 [-2.57, -1.45] |
|
|
Weekes |
2021 |
5 days postoperatively |
I: 15/74 not included in analysis |
pain at rest VAS score |
Postoperative day 1 |
5 ± 3 |
6 ± 3 |
-1.00 [-1.97, -0.03] |
|
|
Xue |
2016 |
60 minutes after massage |
NS |
NRS 0-10 |
60 minutes after massage |
2.54 ± 1.22 |
5.07 ± 1.45 |
-2.53 [-3.08, -1.98] |
Communication and therapeutic suggestion
|
Review (if applicable) |
Author |
Year |
N INT |
N CNTL |
Age Sex |
Surgery |
Intervention |
Regime |
Control |
Regime |
|
|
Gonzales |
2010 |
22 |
22 |
I: 35.91 ± 15.13
M: 13/22 |
same-day surgical procedures |
Guided imagery |
This CD led the patient through a progressive relaxation and guided imagery exercise. (.) This CD consisted of |
usual care |
NS |
|
|
Forward |
2015 |
75 |
74 |
aged 38 to 90 years
M: 33.9% |
hip replacement or knee replacement |
Guided imagery |
The guided imagery program selected was Guided Meditation for Procedures or Surgery, created by Diane Tusek. This selection was based on |
usual care |
NS |
|
|
Shah |
2021 |
16 |
16 |
median 57 (IQR 54-63) y F: 100% |
vaginal hysterectomy with minimally invasive sacrocolpopexy |
therapeutic suggestion |
therapeutic suggestions per protocol; |
usual care |
NS |
|
|
Nowak |
2020 |
191 |
194 |
Median (interquartile range) age (years)
Female I: 115/191 (60%) |
surgery for 1-3 hours under general anaesthesia |
audiotape of background music and positive suggestions |
played repeatedly for 20 minutes followed by 10 minutes of silence to patients through earphones during general anaesthesia |
blank tape |
same regime as intervention, but blank tape |
|
Review (if applicable) |
Author |
Year |
follow up |
incomplete data |
outcome measure |
timing of result used in summary |
Results intervention group |
Result control group |
Mean difference [95% CI] (unless stated otherwise) |
|
Posadzki, 2012 |
Gonzales |
2010 |
2-hour FU |
NS |
pain score; v(vertical)VAS 0-100 |
in ambulatory procedure unit (PACU length of stay on average for control group and intervention group 43 ± 20 and 34 ±10 minutes, and stay in APU 103 ±44 and 103 ±55 resp. |
20.00 ± 28.92 |
34.72 ± 27.54 |
-14.72 [-31.41, 1.97] |
|
|
Forward |
2015 |
2 postop days |
none reported |
Numeric Visual Anxiety Scale (NVAS), Pain Numeric Rating Scale (PNRS) |
postop day 1 |
2.9 (SD onbekend) |
3.5 (SD onbekend) |
MD 0.6; |
|
|
Shah 2021 |
2021 |
2 weeks |
NS |
VAS 0-10 |
24 h |
median 4 (3-5) |
median 4 (3-5) |
Median diff 0 |
|
|
Nowak |
2020 |
postoperative 24 hours |
NS |
NRS 0-10 |
24 hours (asked for maximum pain scores in 24h period) |
median 4 (IQR 3-6) |
median 5 (IQR 4-7) |
Median diff 1 |
Virtual reality
|
Review (if applicable) |
Author |
Year |
N INT |
N CNTL |
Age Sex |
Surgery |
Intervention |
Regime |
Control |
Regime |
|
Ding, 2020 |
Bekelis |
2017 |
64 |
63 |
55.3 ± 14.0 NS |
Craniotomy/ spine surgery |
Virtual reality |
Watching a 5-min video through the VR glasses which describes the operative experience; 5min (not available), Before the surgery |
Provided with routine audiovisual descriptions of the operative experience |
NS |
|
Ding, 2020 |
Ding |
2019 |
91 |
91 |
45.8 ± 12.6 NS |
Hemorrhoi-dectomy |
Virtual reality |
VR distraction through the VR glasses plus standard pharmacological analgesic intervention; 20–30min (1/d), After the surgery |
Standard pharmacological analgesic intervention |
NS |
|
Ding, 2020 |
Jahanishoorab |
2015 |
15 |
15 |
24.1 ± 4.1 NS |
Episiotomy repair |
Virtual reality |
VR distraction the VR glasses plus pharmacological anesthesia; 30min (1/d), during the surgery |
Pharmacological anesthesia |
NS |
|
Ding, 2020 |
Jin |
2018 |
33 |
33 |
I:66.45 ± 3.49 NS |
Knee surgery |
Virtual reality |
Receiving the rehabilitation in the immersive virtual environment through the VR glasses plus conventional; 30min (3/d), after the surgery |
Conventional rehabilitation protocol |
NS |
|
Ding, 2020 |
Li |
2018 |
39 |
39 |
71.82 ± 7.98 C: 72.97 ± 7.82 NS |
Knee surgery |
Virtual reality |
Receiving the rehabilitation in the immersive virtual environment through the VR glasses plus conventional rehabilitation protocol; 30min (3/d) After the surgery |
Conventional rehabilitation protocol |
NS |
|
Ding, 2020 |
Piqueras |
2013 |
72 |
70 |
73.3 ± 6.5 NS |
Knee surgery |
Virtual reality |
Receiving rehabilitation through an interactive virtual software platform which has a 3D avatar that shows the exercises to be undertaken; 60min (1/d) After the surgery |
Receiving the standard clinical protocol of rehabilitation |
NS |
|
Ding, 2020 |
Sweta |
2019 |
25 |
25 |
39.72 ± 15.93 NS |
Dental surgery |
Virtual reality |
VR distraction through the VR glasses plus local anesthesia; NS, During the surgery |
Local anesthesia |
NS |
|
Ding, 2020 |
Yang |
2019 |
24 |
24 |
I:32.5 (15.0–62.0) NS |
Knee surgery |
Virtual reality |
Watching a 3D model of their own MRIs through the VR glasses; 20–30min (1/d) Before the surgery |
Receiving standard preoperative information about their MRIs through a picturearchiving and communications system |
NS |
|
|
Gianola |
2020 |
44 |
41 |
68.6 (±8.8) y68.6 (±8.8) y F: 48/85 (56.5% |
total knee arthroplasty |
Virtual reality |
VR via the Virtual Reality Rehabilitation System (VRRS); passive knee motion on a Kinetec knee continuous passive motion system (Rimec, Chions, Italy) and functional exercises (stair negotiation and level walking) daily for 60 minutes on at least 5 days |
traditional rehabilitation, providing the same exercises without VR |
passive knee motion on a Kinetec knee continuous passive motion system (Rimec, Chions, Italy) and functional exercises (stair negotiation and level walking) daily for 60 minutes on at least 5 days |
|
Review (if applicable) |
Author |
Year |
follow up |
incomplete data |
outcome measure |
Results intervention group |
Result control group |
Mean difference [95% CI] (unless stated otherwise) |
|
Ding, 2020 |
Bekelis |
2017 |
NS |
NS |
pain score; VAS 0-10 |
3.02 ± 1.25 |
3.03 ± 0.75 |
-0.01 [-0.37. 0.35] |
|
Ding, 2020 |
Ding |
2019 |
NS |
NS |
pain score; VAS 0-10 |
4.09 ± 13.55 |
4.17 ± 12.5 |
-0.08 [-3.87. 3.71] |
|
Ding, 2020 |
Jahanishoorab |
2015 |
NS |
NS |
pain score; NRS 0-10 |
0.6 ± 1.28 |
2.52 ± 1.4 |
-1.92 [-2.88. -0.96] |
|
Ding, 2020 |
Jin |
2018 |
NS |
NS |
pain score; VAS 0-10 |
6.48 ± 0.87 |
6.84 ± 1.09 |
-0.36 [-0.84. 0.12] |
|
Ding, 2020 |
Li |
2018 |
NS |
NS |
pain score; VAS 0-10 |
2.54 ± 0.69 |
3.1 ± 0.96 |
-0.56 [-0.93. -0.19] |
|
Ding, 2020 |
Piqueras |
2013 |
NS |
NS |
pain score; VAS 0-10 |
3.11 ± 1.79 |
3.69 ± 1.9 |
-0.58 [-1.19. 0.03] |
|
Ding, 2020 |
Sweta |
2019 |
NS |
NS |
pain score; VAS 0-10 |
1.28 ± 0.891 |
2.6 ± 1.38 |
-1.32 [-1.96. -0.68] |
|
Ding, 2020 |
Yang |
2019 |
NS |
NS |
pain score; VAS 0-10 |
3.03 ± 2.88 |
3.02 ± 2.84 |
0.01 [-1.61. 1.63] |
|
|
Gianola |
2020 |
3-4 days after surgery |
NS |
VAS pain difference score (0-100) |
-23.03 (95% CI -0.26 to -15.79) |
-28.97 (95% CI -36.82 to -1.12) |
NS |
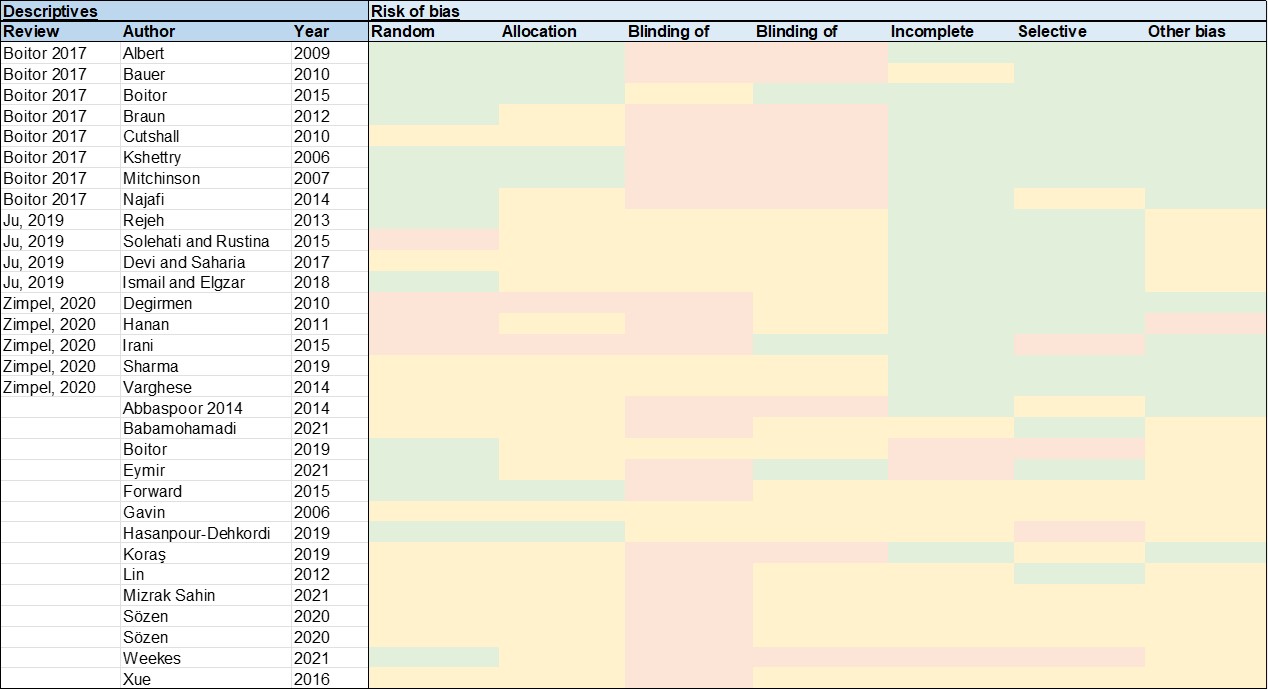
Risk of bias tables
The following 7 criteria were assessed: Random sequence generation (selection bias)
- Allocation concealment (selection bias)
- Blinding of participants and personnel (performance bias): All outcomes
- Blinding of outcome assessment (detection bias): All outcomes
- Incomplete outcome data (attrition bias): All outcomes
- Selective reporting (reporting bias)
- Other bias
Risk of bias is indicated by colours: green: Low risk of bias; yellow: Unclear risk of bias; red: High risk of bias
Massage and relaxation
Communication and therapeutic suggestion

Virtual reality
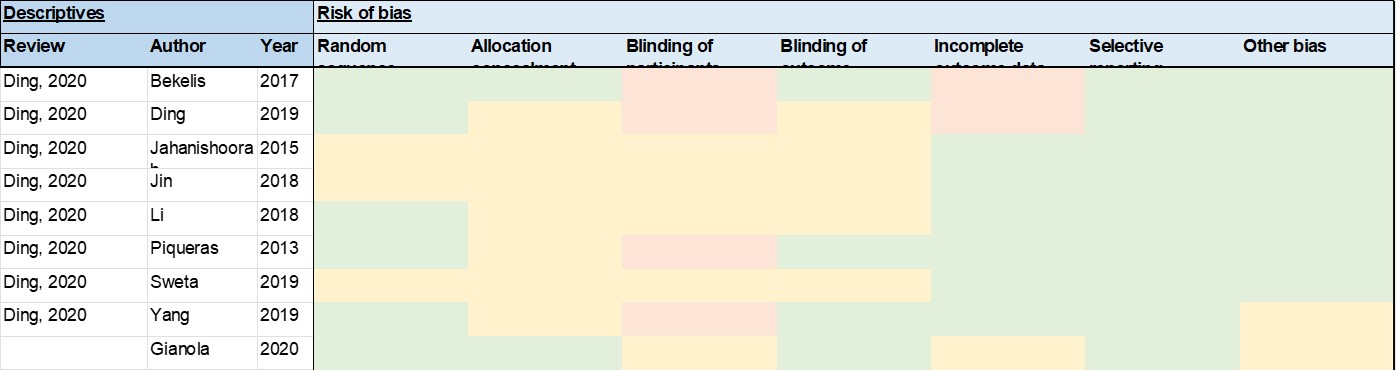
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Gorsky K, Black ND, Niazi A, Saripella A, Englesakis M, Leroux T, Chung F, Niazi AU. Psychological interventions to reduce postoperative pain and opioid consumption: a narrative review of literature. Reg Anesth Pain Med. 2021 Oct;46(10):893-903. doi: 10.1136/rapm-2020-102434. Epub 2021 May 25. PMID: 34035150. |
Design |
|
Szeverenyi C, Kekecs Z, Johnson A, Elkins G, Csernatony Z, Varga K. The Use of Adjunct Psychosocial Interventions Can Decrease Postoperative Pain and Improve the Quality of Clinical Care in Orthopedic Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Pain. 2018 Nov;19(11):1231-1252. doi: 10.1016/j.jpain.2018.05.006. Epub 2018 May 25. PMID: 29803669. |
does not meet PICO (I,C,O) |
|
Sears SR, Bolton S, Bell KL. Evaluation of "Steps to Surgical Success" (STEPS): a holistic perioperative medicine program to manage pain and anxiety related to surgery. Holist Nurs Pract. 2013 Nov-Dec;27(6):349-57. doi: 10.1097/HNP.0b013e3182a72c5a. PMID: 24121700. |
does not meet PICO (I) |
|
Fu D, Yang J, Zhu R, Pan Q, Shen X, Peng Y. Guo, X. R.; Wang, F. Z. Preoperative psychoprophylactic visiting alleviates maternal anxiety and stress and improves outcomes of cesarean patients: A randomized, double-blind and controlled trial. Healthmed 2012; 6(1):263-277. |
does not meet PICO (I) |
|
Good M, Albert JM, Anderson GC, Wotman S, Cong X, Lane D, Ahn S. Supplementing relaxation and music for pain after surgery. Nurs Res. 2010 Jul-Aug;59(4):259-69. doi: 10.1097/NNR.0b013e3181dbb2b3. PMID: 20585222. |
does not meet PICO (O) |
|
Gündüz CS, Çalişkan N. The Effect of Preoperative Video Based Pain Training on Postoperative Pain and Analgesic Use in Patients Undergoing Total Knee Arthroplasty: A Non-randomized Control Group Intervention Study. Clin Nurs Res. 2021 Jul;30(6):741-752. doi: 10.1177/1054773820983361. Epub 2020 Dec 31. PMID: 33383995. |
does not meet PICO (I) |
|
Rejeh N, Heravi-Karimooi M, Vaismoradi M, Jasper M. Effect of systematic relaxation techniques on anxiety and pain in older patients undergoing abdominal surgery. Int J Nurs Pract. 2013 Oct;19(5):462-70. doi: 10.1111/ijn.12088. Epub 2013 May 28. PMID: 24093737. |
include in SR |
|
Cizmic Z, Edusei E, Anoushiravani AA, Zuckerman J, Ruden R, Schwarzkopf R. The Effect of Psychosensory Therapy on Short-term Outcomes of Total Joint Arthroplasty: A Randomized Controlled Trial. Orthopedics. 2018 Nov 1;41(6):e848-e853. doi: 10.3928/01477447-20181010-04. Epub 2018 Oct 16. PMID: 30321440. |
does not meet PICO (I) |
|
Posadzki P, Lewandowski W, Terry R, Ernst E, Stearns A. Guided imagery for non-musculoskeletal pain: a systematic review of randomized clinical trials. J Pain Symptom Manage. 2012 Jul;44(1):95-104. doi: 10.1016/j.jpainsymman.2011.07.014. Epub 2012 Jun 5. PMID: 22672919. |
relevant studies included individually |
|
Faruki A, Nguyen T, Proeschel S, Levy N, Yu J, Ip V, Mueller A, Banner-Goodspeed V, O'Gara B. Virtual reality as an adjunct to anesthesia in the operating room. Trials. 2019 Dec 27;20(1):782. doi: 10.1186/s13063-019-3922-2. PMID: 31882015; PMCID: PMC6935058. |
study protocol |
|
Antall GF, Kresevic D. The use of guided imagery to manage pain in an elderly orthopaedic population. Orthop Nurs. 2004 Sep-Oct;23(5):335-40. doi: 10.1097/00006416-200409000-00012. PMID: 15554471. |
N < 10 |
|
Ding J, He Y, Chen L, Zhu B, Cai Q, Chen K, Liu G. Virtual reality distraction decreases pain during daily dressing changes following haemorrhoid surgery. J Int Med Res. 2019 Sep;47(9):4380-4388. doi: 10.1177/0300060519857862. Epub 2019 Jul 25. PMID: 31342823; PMCID: PMC6753557. |
include in SR |
|
Huang MY, Scharf S, Chan PY. Effects of immersive virtual reality therapy on intravenous patient-controlled sedation during orthopaedic surgery under regional anesthesia: A randomized controlled trial. PLoS One. 2020 Feb 24;15(2):e0229320. doi: 10.1371/journal.pone.0229320. PMID: 32092098; PMCID: PMC7039521. |
does not meet PICO (O) |
|
Laghlam D, Naudin C, Coroyer L, Aidan V, Malvy J, Rahoual G, Estagnasié P, Squara P. Virtual reality vs. Kalinox® for management of pain in intensive care unit after cardiac surgery: a randomized study. Ann Intensive Care. 2021 May 13;11(1):74. doi: 10.1186/s13613-021-00866-w. PMID: 33983498; PMCID: PMC8119554. |
does not meet PICO (O) |
|
Chooi CS, White AM, Tan SG, Dowling K, Cyna AM. Pain vs comfort scores after Caesarean section: a randomized trial. Br J Anaesth. 2013 May;110(5):780-7. doi: 10.1093/bja/aes517. Epub 2013 Feb 5. PMID: 23384734. |
does not meet PICO (I, C) |
|
Chuang CC, Lee CC, Wang LK, Lin BS, Wu WJ, Ho CH, Chen JY. An innovative nonpharmacological intervention combined with intravenous patient-controlled analgesia increased patient global improvement in pain and satisfaction after major surgery. Neuropsychiatr Dis Treat. 2017 Apr 6;13:1033-1042. doi: 10.2147/NDT.S131517. PMID: 28435273; PMCID: PMC5388275. |
study design |
|
Tian Y, Lin J, Gao F. The effects of comfort care on the recovery quality of oral and maxillofacial surgery patients undergoing general anesthesia. Am J Transl Res. 2021 May 15;13(5):5003-5010. PMID: 34150085; PMCID: PMC8205744. |
does not meet PICO (I) |
|
Grafton-Clarke C, Grace L, Roberts N, Harky A. Can postoperative massage therapy reduce pain and anxiety in cardiac surgery patients? Interact Cardiovasc Thorac Surg. 2019 May 1;28(5):716-721. doi: 10.1093/icvts/ivy310. PMID: 30508186. |
Design |
|
Meena S. ASSESS THE EFFECTIVENESS OF HAND AND FOOT MASSAGE IN REDUCING POSTOPERATIVE PAIN AMONG ABDOMINAL SURGERY PATIENTS. Int. Res. J. Pharm. 2019, 10 (4). DOI: 10.7897/2230-8407.1004137 |
Low quality; does not report findings of control group |
|
Miller J, Dunion A, Dunn N, Fitzmaurice C, Gamboa M, Myers S, Novak P, Poole J, Rice K, Riley C, Sandberg R, Taylor D, Gilmore L. Effect of a Brief Massage on Pain, Anxiety, and Satisfaction With Pain Management in Postoperative Orthopaedic Patients. Orthop Nurs. 2015 Jul-Aug;34(4):227-34. doi: 10.1097/NOR.0000000000000163. PMID: 26213879. |
Crossover design without seperated result section |
|
Mitchinson AR, Kim HM, Geisser M, Rosenberg JM, Hinshaw DB. Social connectedness and patient recovery after major operations. J Am Coll Surg. 2008 Feb;206(2):292-300. doi: 10.1016/j.jamcollsurg.2007.08.017. Epub 2007 Nov 12. PMID: 18222382. |
Does not meet PICO (I, C, O) |
|
Rosen J, Lawrence R, Bouchard M, Doros G, Gardiner P, Saper R. Massage for perioperative pain and anxiety in placement of vascular access devices. Adv Mind Body Med. 2013 Winter;27(1):12-23. PMID: 23341418. |
Results on pain not available per treatment group |
|
Boitor M, Martorella G, Laizner AM, Maheu C, Gélinas C. The Effectiveness of Hand Massage on Pain in Critically Ill Patients After Cardiac Surgery: A Randomized Controlled Trial Protocol. JMIR Res Protoc. 2016 Nov 7;5(4):e203. doi: 10.2196/resprot.6277. PMID: 27821384; PMCID: PMC5118583. |
trial protocol |
|
Bauer BA, Cutshall SM, Wentworth LJ, Engen D, Messner PK, Wood CM, Brekke KM, Kelly RF, Sundt TM 3rd. Effect of massage therapy on pain, anxiety, and tension after cardiac surgery: a randomized study. Complement Ther Clin Pract. 2010 May;16(2):70-5. doi: 10.1016/j.ctcp.2009.06.012. Epub 2009 Jul 14. PMID: 20347836. |
included in SR; Boitor 2017 |
|
Boitor M, Martorella G, Arbour C, Michaud C, Gélinas C. Evaluation of the preliminary effectiveness of hand massage therapy on postoperative pain of adults in the intensive care unit after cardiac surgery: a pilot randomized controlled trial. Pain Manag Nurs. 2015 Jun;16(3):354-66. doi: 10.1016/j.pmn.2014.08.014. PMID: 26025795. |
included in SR; Boitor 2017 |
|
Hui X, Bingxin K, Chenxin G, Chi Z, Xirui X, Songtao S, Jun X, Lianbo X, Qi S. Effectiveness of Tuina in the treatment of pain after total knee arthroplasty in patients with knee osteoarthritis. Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (18): 2840-2845.doi: 10.3969/j.issn.2095-4344.3845
|
does not meet PICO (I) |
|
Midilli TS, Eser I. Effects of Reiki on Post-cesarean Delivery Pain, Anxiety, and Hemodynamic Parameters: A Randomized, Controlled Clinical Trial. Pain Manag Nurs. 2015 Jun;16(3):388-99. doi: 10.1016/j.pmn.2014.09.005. PMID: 26025798. |
does not meet PICO (I) |
|
Mitchinson AR, Kim HM, Rosenberg JM, Geisser M, Kirsh M, Cikrit D, Hinshaw DB. Acute postoperative pain management using massage as an adjuvant therapy: a randomized trial. Arch Surg. 2007 Dec;142(12):1158-67; discussion 1167. doi: 10.1001/archsurg.142.12.1158. PMID: 18086982. |
included in SR; Boitor 2017 |
|
Najafi SS, Rast F, Momennasab M, Ghazinoor M, Dehghanrad F, Mousavizadeh SA. The effect of massage therapy by patients' companions on severity of pain in the patients undergoing post coronary artery bypass graft surgery: a single-blind randomized clinical trial. Int J Community Based Nurs Midwifery. 2014 Jul;2(3):128-35. PMID: 25349854; PMCID: PMC4201205. |
included in SR; Boitor 2017 |
|
Sagkal Midilli T, Ciray Gunduzoglu N. Effects of Reiki on Pain and Vital Signs When Applied to the Incision Area of the Body After Cesarean Section Surgery: A Single-Blinded, Randomized, Double-Controlled Study. Holist Nurs Pract. 2016 Nov/Dec;30(6):368-378. doi: 10.1097/HNP.0000000000000172. PMID: 27763932. |
does not meet PICO (I) |
|
Shaybak E, Abdollahimohammad A, Rahnama M, Masinaeinezhad N, Azadi-Ahmadabadi C, Firouzkohi M. The effect of reiki energy healing on CABG postoperative chest pain caused by coughing and deep breathing. Indian Journal of Public Health Research and Development 2017; Volume 8, Issue 2, April-June, Pages 305-310 |
does not meet PICO (I) |
|
Simonelli MC, Doyle LT, Columbia M, Wells PD, Benson KV, Lee CS. Effects of Connective Tissue Massage on Pain in Primiparous Women After Cesarean Birth. J Obstet Gynecol Neonatal Nurs. 2018 Sep;47(5):591-601. doi: 10.1016/j.jogn.2018.07.006. Epub 2018 Aug 11. PMID: 30102886. |
does not meet PICO (I) |
|
Attias S, Sivan K, Avneri O, Sagee A, Ben-Arye E, Grinberg O, Sroka G, Matter I, Schiff E. Analgesic Effects of Reflexology in Patients Undergoing Surgical Procedures: A Randomized Controlled Trial. J Altern Complement Med. 2018 Aug;24(8):809-815. doi: 10.1089/acm.2017.0167. Epub 2018 Jun 8. PMID: 29883188. |
does not meet PICO (I) |
|
Khorsand A, Tadayonfar MA, Badiee S, Aghaee MA, Azizi H, Baghani S. Evaluation of the Effect of Reflexology on Pain Control and Analgesic Consumption After Appendectomy. J Altern Complement Med. 2015 Dec;21(12):774-80. doi: 10.1089/acm.2014.0270. Epub 2015 Sep 24. PMID: 26401598. |
does not meet PICO (I) |
|
Tsay SL, Chen HL, Chen SC, Lin HR, Lin KC. Effects of reflexotherapy on acute postoperative pain and anxiety among patients with digestive cancer. Cancer Nurs. 2008 Mar-Apr;31(2):109-15. doi: 10.1097/01.NCC.0000305694.74754.7b. PMID: 18490886. |
does not meet PICO (I) |
|
Mohammadi S, Pouladi S, Ostovar, A, Ravanipour M.. Effects of foot reflexology massage on pain and fatigue in patients undergoing coronary artery bypass graft. Annals of Tropical Medicine and Public Health 2018; 8, 0, S513 |
does not meet PICO (I) |
|
Haase O, Schwenk W, Hermann C, Müller JM. Guided imagery and relaxation in conventional colorectal resections: a randomized, controlled, partially blinded trial. Dis Colon Rectum. 2005 Oct;48(10):1955-63. doi: 10.1007/s10350-005-0114-9. PMID: 15991068. |
no description of relevant outcome |
|
Good M, Albert JM, Arafah B, Anderson GC, Wotman S, Cong X, Lane D, Ahn S. Effects on postoperative salivary cortisol of relaxation/music and patient teaching about pain management. Biol Res Nurs. 2013 Jul;15(3):318-29. doi: 10.1177/1099800411431301. Epub 2012 Apr 3. PMID: 22472905. |
does not meet PICO (C) |
|
Mehling WE, Jacobs B, Acree M, Wilson L, Bostrom A, West J, Acquah J, Burns B, Chapman J, Hecht FM. Symptom management with massage and acupuncture in postoperative cancer patients: a randomized controlled trial. J Pain Symptom Manage. 2007 Mar;33(3):258-66. doi: 10.1016/j.jpainsymman.2006.09.016. PMID: 17349495. |
does not meet PICO (I) |
|
Weston E, Raker C, Huang D, Parker A, Robison K, Mathews C. The Association Between Mindfulness and Postoperative Pain: A Prospective Cohort Study of Gynecologic Oncology Patients Undergoing Minimally Invasive Hysterectomy. J Minim Invasive Gynecol. 2020 Jul-Aug;27(5):1119-1126.e2. doi: 10.1016/j.jmig.2019.08.021. Epub 2019 Aug 23. PMID: 31449907. |
study design |
|
Hadi N, Hanid AA. Lavender essence for post-cesarean pain. Pak J Biol Sci. 2011 Jun 1;14(11):664-7. doi: 10.3923/pjbs.2011.664.667. PMID: 22235509. |
does not meet PICO (I) |
|
Kim JT, Ren CJ, Fielding GA, Pitti A, Kasumi T, Wajda M, Lebovits A, Bekker A. Treatment with lavender aromatherapy in the post-anesthesia care unit reduces opioid requirements of morbidly obese patients undergoing laparoscopic adjustable gastric banding. Obes Surg. 2007 Jul;17(7):920-5. doi: 10.1007/s11695-007-9170-7. PMID: 17894152. |
does not meet PICO (I) |
|
Kim JT, Wajda M, Cuff G, Serota D, Schlame M, Axelrod DM, Guth AA, Bekker AY. Evaluation of aromatherapy in treating postoperative pain: pilot study. Pain Pract. 2006 Dec;6(4):273-7. doi: 10.1111/j.1533-2500.2006.00095.x. PMID: 17129308. |
does not meet PICO (I) |
|
Marzouk T, Barakat R, Ragab A, Badria F, Badawy A. Lavender-thymol as a new topical aromatherapy preparation for episiotomy: A randomised clinical trial. J Obstet Gynaecol. 2015;35(5):472-5. doi: 10.3109/01443615.2014.970522. PMID: 25384116. |
does not meet PICO (I) |
|
Najafi B, Fariba F, Daem R, Ghaderi L, Seidi J. The effect of lavender essence on pain severity after cesarean section under spinal anesthesia. Journal of chemical and pharmaceutical sciences, 2016, 2016, 66‐69 |
does not meet PICO (I) |
|
Nazari M, Kamrani F, Sahebalzamani M, Amin, GR. On the investigation of the effect of aromatherapy on pain after orthopedic surgery: clinical trial. Acta Medica Mediterranea, 2016, 32: 1513 |
does not meet PICO (I) |
|
Bikmoradi A, Seifi Z, Poorolajal J, Araghchian M, Safiaryan R, Oshvandi K. Effect of inhalation aromatherapy with lavender essential oil on stress and vital signs in patients undergoing coronary artery bypass surgery: A single-blinded randomized clinical trial. Complement Ther Med. 2015 Jun;23(3):331-8. doi: 10.1016/j.ctim.2014.12.001. Epub 2014 Dec 11. PMID: 26051567. |
does not meet PICO (I) |
|
Stallings Welden LM, Leatherland P, Schitter MB, Givens A, Stallings JD. Abdominal Surgical Patients Randomized to Aromatherapy for Pain Management. J Perianesth Nurs. 2021 Jun;36(3):291-299.e3. doi: 10.1016/j.jopan.2020.08.005. Epub 2021 Jan 24. PMID: 33500169. |
does not meet PICO (I) |
|
Kekecs Z, Nagy T, Varga K. The effectiveness of suggestive techniques in reducing postoperative side effects: a meta-analysis of randomized controlled trials. Anesth Analg. 2014 Dec;119(6):1407-19. doi: 10.1213/ANE.0000000000000466. PMID: 25289661. |
does not meet PICO (I) |
|
Akgul A, Guner B, Çırak M, Çelik D, Hergünsel O, Bedirhan S. The Beneficial Effect of Hypnosis in Elective Cardiac Surgery: A Preliminary Study. Thorac Cardiovasc Surg. 2016 Oct;64(7):581-588. doi: 10.1055/s-0036-1580623. Epub 2016 Apr 4. PMID: 27043785. |
does not meet PICO (I) |
|
Langiano E, Chiarello M, Leo A, Pontani R, Lorenzetti V, Sassaroli G, Boccolini C, Ciccola T, Massari M, Olivieri G, Venturi S, Bocci G. Anaesthesia of a prevalently analgesic nature vs. anaesthesia of a prevalently hypnotic nature in minor gynaecological surgical procedures. Acta Anaesthesiologica Italica / Anaesthesia and Intensive Care in Italy 2005; 56(1):38-51 |
does not meet PICO (I) |
|
Montgomery GH, Bovbjerg DH, Schnur JB, David D, Goldfarb A, Weltz CR, Schechter C, Graff-Zivin J, Tatrow K, Price DD, Silverstein JH. A randomized clinical trial of a brief hypnosis intervention to control side effects in breast surgery patients. J Natl Cancer Inst. 2007 Sep 5;99(17):1304-12. doi: 10.1093/jnci/djm106. Epub 2007 Aug 28. PMID: 17728216. |
does not meet PICO (I) |
|
Joudi M, Fathi M, Izanloo A, Montazeri O, Jangjoo A. An Evaluation of the Effect of Hypnosis on Postoperative Analgesia following Laparoscopic Cholecystectomy. Int J Clin Exp Hypn. 2016 Jul-Sep;64(3):365-72. doi: 10.1080/00207144.2016.1171113. PMID: 27267679. |
does not meet PICO (I) |
|
Raddaoui K, Radhouani M, Zoghlami K, Trigui E, Maghraoui H, Kaabachi O. Preoperative hypnosis for pain management after arthroscopic repair of anterior cruciate ligament. Tunis Med. 2020 Feb;98(2):156-160. PMID: 32395806. |
does not meet PICO (I) |
|
Kerai S, Saxena KN, Taneja B, Sehrawat L. Role of transcutaneous electrical nerve stimulation in post-operative analgesia. Indian J Anaesth. 2014 Jul;58(4):388-93. doi: 10.4103/0019-5049.138966. PMID: 25197104; PMCID: PMC4155281. |
does not meet PICO (I) |
|
Johnson MI, Paley CA, Howe TE, Sluka KA. Transcutaneous electrical nerve stimulation for acute pain. Cochrane Database Syst Rev. 2015 Jun 15;2015(6):CD006142. doi: 10.1002/14651858.CD006142.pub3. PMID: 26075732; PMCID: PMC8094447. |
does not meet PICO (I) |
|
Xie YJ, Wang S, Gong QJ, Wang JX, Sun FH, Miyamoto A, Ou X, Wang L, Wang SQ, Zhang C. Effects of electromyography biofeedback for patients after knee surgery: A systematic review and meta-analysis. J Biomech. 2021 May 7;120:110386. doi: 10.1016/j.jbiomech.2021.110386. Epub 2021 Mar 15. PMID: 33794414. |
does not meet PICO (I) |
|
Freynet A, Falcoz PE. Is transcutaneous electrical nerve stimulation effective in relieving postoperative pain after thoracotomy? Interact Cardiovasc Thorac Surg. 2010 Feb;10(2):283-8. doi: 10.1510/icvts.2009.219576. Epub 2009 Nov 12. PMID: 19910359. |
does not meet PICO (I) |
|
Eidy M, Fazel MR, Janzamini M, Haji Rezaei M, Moravveji AR. Preemptive Analgesic Effects of Transcutaneous Electrical Nerve Stimulation (TENS) on Postoperative Pain: A Randomized, Double-Blind, Placebo-Controlled Trial. Iran Red Crescent Med J. 2016 Apr 12;18(4):e35050. doi: 10.5812/ircmj.35050. PMID: 27275401; PMCID: PMC4893426. |
does not meet PICO (I) |
|
Huang S, Peng W, Tian X, Liang H, Jia Z, Lo T, He M, Feng Y. Effects of transcutaneous electrical acupoint stimulation at different frequencies on perioperative anesthetic dosage, recovery, complications, and prognosis in video-assisted thoracic surgical lobectomy: a randomized, double-blinded, placebo-controlled trial. J Anesth. 2017 Feb;31(1):58-65. doi: 10.1007/s00540-015-2057-1. Epub 2015 Sep 8. PMID: 26350110. |
does not meet PICO (I) |
|
Jaafarpour M, Khani, A, Javadifar N, Taghinejad H, Mahmoudi R, Saadipour KH. The analgesic effect of transcutaneous electrical nerve stimulation (TENS) on caesarean under spinal anaesthesia. Journal of Clinical and Diagnostic Research. 2008; 2 (3); 815-819 |
does not meet PICO (I) |
|
Kasapoğlu I, Kasapoğlu Aksoy M, Çetinkaya Demir B, Altan L. The efficacy of transcutaneous electrical nerve stimulation therapy in pain control after cesarean section delivery associated with uterine contractions and abdominal incision. Turk J Phys Med Rehabil. 2020 May 18;66(2):169-175. doi: 10.5606/tftrd.2020.3225. PMID: 32760894; PMCID: PMC7401685. |
does not meet PICO (I) |
|
Moon DH, Park J, Kang DY, Lee HS, Lee S. Intramuscular stimulation as a novel alternative method of pain management after thoracic surgery. J Thorac Dis. 2019 Apr;11(4):1528-1535. doi: 10.21037/jtd.2019.03.24. PMID: 31179096; PMCID: PMC6531751. |
does not meet PICO (I) |
|
Oztas B, Iyigun E. The effects of two different electrical stimulation methods on the pain intensity of the patients who had undergone abdominal surgery with a midline incision: Randomized controlled clinical trial. Contemp Nurse. 2019 Apr-Jun;55(2-3):122-138. doi: 10.1080/10376178.2019.1628650. Epub 2019 Jun 14. PMID: 31169066. |
does not meet PICO (I) |
|
Parseliunas A, Paskauskas S, Kubiliute E, Vaitekunas J, Venskutonis D. Transcutaneous Electric Nerve Stimulation Reduces Acute Postoperative Pain and Analgesic Use After Open Inguinal Hernia Surgery: A Randomized, Double-Blind, Placebo-Controlled Trial. J Pain. 2021 May;22(5):533-544. doi: 10.1016/j.jpain.2020.11.006. Epub 2020 Dec 10. PMID: 33309784. |
does not meet PICO (I) |
|
Pitangui AC, de Sousa L, Gomes FA, Ferreira CH, Nakano AM. High-frequency TENS in post-episiotomy pain relief in primiparous puerpere: a randomized, controlled trial. J Obstet Gynaecol Res. 2012 Jul;38(7):980-7. doi: 10.1111/j.1447-0756.2011.01824.x. Epub 2012 May 8. PMID: 22568611. |
does not meet PICO (I) |
|
Ramanathan D, Saleh A, Klika AK, Higuera CA, Barsoum WK. The Use of Transcutaneous Electrical Nerve Stimulation After Total Knee Arthroplasty: A Prospective Randomized Controlled Trial. Surg Technol Int. 2017 Jul 25;30:425-434. PMID: 28537354. |
does not meet PICO (I) |
|
Solak O, Turna A, Pekcolaklar A, Metin M, Sayar A, Solak O, Gürses A. Transcutaneous electric nerve stimulation for the treatment of postthoracotomy pain: a randomized prospective study. Thorac Cardiovasc Surg. 2007 Apr;55(3):182-5. doi: 10.1055/s-2006-924631. PMID: 17410506. |
does not meet PICO (I) |
|
Szmit M, Agrawal S, Goździk W, Kübler A, Agrawal A, Pruchnicki P, Woźniak M, Nowak M, Bartoszewicz B, Rudnicki J. Transcutaneous Electrical Acupoint Stimulation Reduces Postoperative Analgesic Requirement in Patients Undergoing Inguinal Hernia Repair: A Randomized, Placebo-Controlled Study. J Clin Med. 2021 Jan 4;10(1):146. doi: 10.3390/jcm10010146. PMID: 33406735; PMCID: PMC7794768. |
does not meet PICO (I) |
|
Xiao H, She SZ, Xu LX. Effects of transcutaneous electric nerve stimulation on the postoperative analgesia with PCEA and recovery after surgery. Chinese Journal of Clinical Rehabilitation 2002; 6 (12): 1784-1785 |
does not meet PICO (I) |
|
Zhou X, Cao SG, Tan XJ, Liu XD, Li ZQ, Kong LX, Tian YL, Liu D, Shen S, Sun YQ, Jiang HT, Zhou YB. Effects of Transcutaneous Electrical Acupoint Stimulation (TEAS) on Postoperative Recovery in Patients with Gastric Cancer: A Randomized Controlled Trial. Cancer Manag Res. 2021 Feb 12;13:1449-1458. doi: 10.2147/CMAR.S292325. PMID: 33603487; PMCID: PMC7886100. |
does not meet PICO (I) |
|
Bjerså K, Andersson T. High frequency TENS as a complement for pain relief in postoperative transition from epidural to general analgesia after pancreatic resection. Complement Ther Clin Pract. 2014 Feb;20(1):5-10. doi: 10.1016/j.ctcp.2013.11.004. Epub 2013 Nov 20. PMID: 24439637. |
does not meet PICO (I) |
|
Chakravarthy M, Prashanth A, George A. Evaluation of Percutaneous Electrical Nerve Stimulation of the Auricle for Relief of Postoperative Pain Following Cesarean Section. Med Acupunct. 2019 Oct 1;31(5):281-288. doi: 10.1089/acu.2019.1352. Epub 2019 Oct 17. PMID: 31624527; PMCID: PMC6795276. |
does not meet PICO (I) |
|
Blank JJ, Liu Y, Yin Z, Spofford CM, Ridolfi TJ, Ludwig KA, Otterson MF, Peterson CY. Impact of Auricular Neurostimulation in Patients Undergoing Colorectal Surgery with an Enhanced Recovery Protocol: A Pilot Randomized, Controlled Trial. Dis Colon Rectum. 2021 Feb 1;64(2):225-233. doi: 10.1097/DCR.0000000000001752. PMID: 33417346. |
does not meet PICO (I) |
|
Martimbianco AL, Gomes da Silva BN, de Carvalho AP, Silva V, Torloni MR, Peccin MS. Effectiveness and safety of cryotherapy after arthroscopic anterior cruciate ligament reconstruction. A systematic review of the literature. Phys Ther Sport. 2014 Nov;15(4):261-8. doi: 10.1016/j.ptsp.2014.02.008. Epub 2014 Mar 13. PMID: 24713365. |
does not meet PICO (I) |
|
Klintberg IH, Larsson ME. Shall we use cryotherapy in the treatment in surgical procedures, in acute pain or injury, or in long term pain or dysfunction? - A systematic review. J Bodyw Mov Ther. 2021 Jul;27:368-387. doi: 10.1016/j.jbmt.2021.03.002. Epub 2021 Mar 20. PMID: 34391260. |
does not meet PICO (I) |
|
Raggio BS, Barton BM, Grant MC, McCoul ED. Intraoperative Cryoanalgesia for Reducing Post-Tonsillectomy Pain: A Systemic Review. Ann Otol Rhinol Laryngol. 2018 Jun;127(6):395-401. doi: 10.1177/0003489418772859. PMID: 29776324. |
does not meet PICO (I) |
|
Ebrahimi-Rigi H, Feizi A, Abdollahimohammad A, Ebrahimi-Rigi Z, Salehi-Ardabili S. Effect of cold therapy on the pain of deep-breathing and coughing in patients after coronary artery bypass grafting. Der Pharmacia Lettre 2016; 8 (10): 201-205 |
not in primary search strategy |
|
Koç M, Tez M, Yoldaş O, Dizen H, Göçmen E. Cooling for the reduction of postoperative pain: prospective randomized study. Hernia. 2006 Apr;10(2):184-6. doi: 10.1007/s10029-005-0062-2. Epub 2006 Jan 24. PMID: 16432641. |
not in primary search strategy |
|
Lu YY, Su ML, Gau ML, Lin KC, Au HK. The efficacy of cold-gel packing for relieving episiotomy pain - a quasi-randomised control trial. Contemp Nurse. 2015;50(1):26-35. doi: 10.1080/10376178.2015.1010257. Epub 2015 Jun 10. PMID: 26058405. |
not in primary search strategy |
|
Navvabi Rigi SH, Kerman-saravi F, Saroneh Rigi M, Abedian Z. Cold and Reduced Episiotomy Pain Interfere with Mood and Daily Activity. Shiraz E-Medical Journal 2011; 12 (2) |
not in primary search strategy |
|
Ozkan B, Cavdar I. The Effect of Cold Therapy Applied to the Incision Area After Abdominal Surgery on Postoperative Pain and Analgesic Use. Pain Manag Nurs. 2021 Dec;22(6):775-782. doi: 10.1016/j.pmn.2021.03.007. Epub 2021 Apr 24. PMID: 33903052. |
not in primary search strategy |
|
Seweid MM, Ahmed NT, Ramadan BA, Ahmed FR. Effect of cold application on incisional pain associated with incentive spirometry after coronary artery bypass graft surgery. International Journal of Africa Nursing Sciences 2021; Volume 15, 100315 doi: 10.1016/j.ijans.2021.100315 |
not in primary search strategy |
|
Sheikhan F, Jahdi F, Khoie EM, Shamsalizadeh N, Sheikhan H, Haghani H. Episiotomy Discomforts Relief Using Cold Gel Pads in Primiparaus Iranian Women (A Comparative Study). Research Journal of Medical Sciences 2011; 5(3):150-154. DOI: 10.3923/rjmsci.2011.150.154 |
not in primary search strategy |
|
Vieira L, Nissen L, Sela G, Amara Y, Fonseca V. Reducing postoperative pain from tonsillectomy using monopolar electrocautery by cooling the oropharynx. Int Arch Otorhinolaryngol. 2014 Apr;18(2):155-8. doi: 10.1055/s-0033-1363783. Epub 2014 Jan 6. PMID: 25992083; PMCID: PMC4297033. |
not in primary search strategy |
|
Wittig-Wells D, Johnson I, Samms-McPherson J, Thankachan S, Titus B, Jacob A, Higgins M. Does the use of a brief cryotherapy intervention with analgesic administration improve pain management after total knee arthroplasty? Orthop Nurs. 2015 May-Jun;34(3):148-53. doi: 10.1097/NOR.0000000000000143. PMID: 25989123. |
not in primary search strategy |
|
Agency for Healthcare Research and Quality (US); AHRQ Comparative Effectiveness Reviews. 2005 Rockville (MD) |
Relevant studies included individually |
|
Gamboa J, Cameron MC, Fathi R, Alkousakis T. A review of non-pharmacologic approaches to enhance the patient experience in dermatologic surgery. Dermatol Online J. 2020 Mar 15;26(3):13030/qt7mp372nd. PMID: 32609440. |
Study design |
|
Moon M, Oh EG, Baek W, Kim YM. Effects of Nurse-Led Pain Management Interventions for Patients with Total Knee/Hip Replacement. Pain Manag Nurs. 2021 Apr;22(2):111-120. doi: 10.1016/j.pmn.2020.11.005. Epub 2021 Jan 19. PMID: 33353818. |
Does not fit PICO |
|
Fan M, Chen Z. A systematic review of non-pharmacological interventions used for pain relief after orthopedic surgical procedures. Exp Ther Med. 2020 Nov;20(5):36. doi: 10.3892/etm.2020.9163. Epub 2020 Sep 1. PMID: 32952627; PMCID: PMC7480131. |
does not meet PICO (P) |
|
Tedesco D, Gori D, Desai KR, Asch S, Carroll IR, Curtin C, McDonald KM, Fantini MP, Hernandez-Boussard T. Drug-Free Interventions to Reduce Pain or Opioid Consumption After Total Knee Arthroplasty: A Systematic Review and Meta-analysis. JAMA Surg. 2017 Oct 18;152(10):e172872. doi: 10.1001/jamasurg.2017.2872. Epub 2017 Oct 18. Erratum in: JAMA Surg. 2018 Apr 1;153(4):396. PMID: 28813550; PMCID: PMC5831469. |
does not meet PICO (I) |
|
Nelson EA, Dowsey MM, Knowles SR, Castle DJ, Salzberg MR, Monshat K, Dunin AJ, Choong PF. Systematic review of the efficacy of pre-surgical mind-body based therapies on post-operative outcome measures. Complement Ther Med. 2013 Dec;21(6):697-711. doi: 10.1016/j.ctim.2013.08.020. Epub 2013 Sep 8. PMID: 24280480. |
include studie individual |
|
Gatewood CT, Tran AA, Dragoo JL. The efficacy of post-operative devices following knee arthroscopic surgery: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2017 Feb;25(2):501-516. doi: 10.1007/s00167-016-4326-4. Epub 2016 Oct 1. PMID: 27695905. |
does not meet PICO (I) |
|
Fischer HB, Simanski CJ, Sharp C, Bonnet F, Camu F, Neugebauer EA, Rawal N, Joshi GP, Schug SA, Kehlet H; PROSPECT Working Group. A procedure-specific systematic review and consensus recommendations for postoperative analgesia following total knee arthroplasty. Anaesthesia. 2008 Oct;63(10):1105-23. doi: 10.1111/j.1365-2044.2008.05565.x. Epub 2008 Jul 10. PMID: 18627367. |
does not meet PICO (I); studies <2005 |
Beoordelingsdatum en geldigheid
Publicatiedatum : 26-09-2023
Beoordeeld op geldigheid : 01-09-2023
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS).
De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met postoperatieve pijn.
Samenstelling van de werkgroep
Werkgroep
Prof. dr. J. (Jörgen) Bruhn, anesthesioloog, (voorzitter) NVA
Prof. dr. dr. M.W. (Markus) Hollmann, anesthesioloog, NVA
Dr. M.F. (Markus) Stevens, anesthesioloog, NVA
Drs. L.J.H. (Lea) van Wersch, anesthesioloog, NVA
Dr. M.H.J. (Margot) Roozekrans, anesthesioloog, NVA
Dr. S.A.S. (Sandra) van den Heuvel, anesthesioloog/pijnspecialist, NVA
Drs. S.J. (Stijn) Westerbos, orthopeed, NOV
Drs. W.L. (Wilson) Li, cardiothoracaal chirurg, NVT
S.F. (Cedric) Lau MSc, ziekenhuisapotheker, NVZA
Dr. R.L.M. (Rianne) van Boekel, verpleegkundig pijnconsulent, V&VN
Drs. I.L. (Ilona) Thomassen-Hilgersom, patiëntvertegenwoordiger, Samenwerkingverband Pijnpatiënten naar één stem
Klankbordgroep
Drs. N.C. (Niels) Gritters van den Oever, intensivist, NVIC
J.P. (Patrick) Rensink, anesthesiemedewerker/pijnconsulent, NVAM
Dr. G. (Gijs) Helmerhorst, orthopeed, NOV
Dr. C.D. (Cor) de Kroon, gynaecoloog-oncoloog, NVOG
Dr. W.J. (Wietse) Eshuis, chirurg, NVvH
Dr. D. (Daphne) Roos, chirurg, NVvH
Met ondersteuning van
Dr. F. Willeboordse, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Dr. L.M.P. Wesselman, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Dr. L.M. van Leeuwen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
I. van Dijk, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Bruhn, voorzitter |
Professor & Afdelingshoofd afdeling Anesthesiologie, Radboud UMC |
Editorial Board Journal of Clinical Monitoring and Computing, onbetaald |
Geen |
Geen actie |
|
Hollmann |
Professor & Afdelingshoofd afdeling Anesthesiologie, Amsterdam UMC, locatie AMC |
|
Geen |
Restricties t.a.v. modules over ketamine en lidocaïne. |
|
Lau |
|
Nationale Werkgroep morbide obesitas en bariatrische chirurgie (KNMP), vergoeding voor bestede uren |
Geen belangenverstrengeling, promotie-onderzoek is op een ander vlak dan waar beoogde werkgroep zich over buigt
|
Geen actie |
|
Boekel, van |
|
|
Geen |
Geen actie |
|
Thomassen-Hilgersom |
Voorzitter Samenwerkingsverband Pijnpatiënten naar één stem vrijwilliger en geen werkgever |
|
Geen |
Geen actie |
|
Li |
Cardiothoracaal chirurg (Radboudumc, Nijmegen) |
Bestuurslid NVT (Nederlandse Vereniging voor Thoraxchirurgie) |
Radboudumc zal in 2021 meedoen aan een RCT naar de optimale vorm van pijnstilling ten tijde van longchirugie (epiduraal versus paravertebraal) OPtriAL - met ZonMw subsidie, geïniteerd vanuit het MMC |
Geen actie |
|
Roozekrans |
Anesthesioloog - Pijnspecialist - Noordwest Ziekenhuisgroep |
Geen |
Geen |
Geen actie |
|
Stevens |
Chef de Clinique kinderanesthesie AUMC locatie AMC |
|
Geen |
Geen actie |
|
Heuvel, van den |
Anesthesioloog-pijnarts, Radboud UMC |
Geen |
Geen |
Geen actie |
|
Wersch, van |
Anesthesioloog, Maasziekenhuis Pantein |
Geen |
Geen |
Geen actie |
|
Westerbos |
Orthopeed, Alrijne ziekenhuis |
Geen |
Geen |
Geen actie |
|
Gritters van den Oever |
Anesthesioloog-intensivist Treant Zorggroep |
|
Geen |
Geen actie |
|
Rensink |
|
|
Geen |
Geen actie |
|
Kroon, de |
Gynaecoloog-oncoloog Leids Univesitair Medisch Centrum (1.0 fte) |
|
Geen |
Geen actie |
|
Roos |
Chirurg |
Geen |
Geen |
Geen actie |
|
Eshuis |
Chirurg, Amsterdam UMC |
Geen |
Geen |
Geen actie |
|
Willeboordse |
Senior adviseur Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Partner werkzaam bij Janssen Vaccines, onderdeel van Johnsson &Johnsson, via partner ook financiële belangen (aandelen J&J) |
Geen actie |
|
Wesselman |
Adviseur Kennisinstituut van de Federatie Medisch Specialisten |
|
|
Geen actie |
|
Leeuwen, van |
Adviseur Kennisinstituut van de Federatie Medisch Specialisten |
|
|
Geen actie |
|
Dijk, van |
Junior adviseur Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Geen |
Geen actie |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door zitting van een afgevaardigde van de patiëntenvereniging (Pijnpatiënten naar één stem) in de werkgroep. De Patiëntenfederatie Nederland en Pijnpatiënten naar één stem werden uitgenodigd voor de invitational conference. Het verslag hiervan [zie aanverwante producten] is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en Pijnpatiënten naar één stem en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Wkkgz & Kwalitatieve raming van mogelijke substantiële financiële gevolgen
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijn is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling zijn richtlijnmodules op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
|
Module |
Uitkomst raming |
Toelichting |
|
Module Organisatie van Zorg |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Transitionele Pijn Service (TPS) |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten). Hoewel de aanbeveling aangeeft dat een andere of nieuwe manier van zorgverlening gewenst is (i.e. andere manier van samenwerking/afstemming tussen zorgverleners) waarbij een TPS-model met TPS-team geïnitieerd wordt, laten eerste kosten-effectiviteitsstudies kostenbesparingen zien. De verwachting is dat TPS leidt tot betere zorg-op-maat, waarbij chronische postoperatieve pijn zorg doelmatiger wordt behandeld. Per ziekenhuis zal de vorm, intensiteit en organisatie van het TPS-model variëren. Zo kunnen ziekenhuizen ook kiezen voor een minder uitgebreid TPS. De aanbeveling geeft relatief veel ruimte voor de precieze invulling. Alle overwegingen tezamen, worden er geen substantiële financiële gevolgen verwacht. |
|
Module Pijnmeting |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Niet-medicamenteuze interventies |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Buikwandblokken |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Borstwandblokken bij mammachirurgie |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Borstwandblokken intrathoracaal |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Continue Wond infusie |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Cryoanalgesie |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5.000 patiënten) en zal daarom naar verwachting geen substantiële financiële gevolgen hebben voor de collectieve uitgaven. |
|
Module Dexmethason |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Gabapentinoïden |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Ketamine |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Magnesium |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Methadon |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Beta blokkers -Esmolol |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Alpha 2 agonist - Clonidine |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Alpha 2 agonist – Dexmedetomidine |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Lidocaïne |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Multimodale pijnbestrijding |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met postoperatieve pijn.
De werkgroep beoordeelde de aanbevelingen uit de eerdere richtlijn Postoperatieve pijn (NVA, 2013) op noodzaak tot revisie. Tevens zijn er knelpunten aangedragen door relevante partijen middels een invitational conference.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
De beoordelingen van de literatuur en de conclusies zijn gedaan op basis van de GRADE systematiek. De werkgroep vindt het belangrijk om relevante beperkingen hiervan aan te geven.
De klinische vraag gaat vaak over een reductie van ernstige postoperatieve pijn en opioïdenconsumptie in een aantal patiënten met resp. over een klinisch relevante reductie van ernstige postoperatieve pijn opioïdenconsumptie bij een individuele patiënt. Hetzelfde geldt voor opioïdenconsumptie; de keuze van een absolute drempelwaarde in mg (i.p.v. een relatieve drempelwaarde in %) maakt dit afhankelijk van tijdstip, ingreep en ernst van de pijn: vroege postoperatieve tijdstippen en (studies met) ingrepen met relatief lage opioïdconsumptie kunnen vaak de MCID niet bereiken.
De keuze van de MCID heeft een bepaalde mate van willekeurigheid en is niet absoluut te zien. Ook zijn de conclusies zo geformuleerd (en geven alleen beperkt antwoord op het effect op een individuele patiënt voor een specifieke ingreep).
In de literatuur worden de eindpunten pijnscores en opioïdenconsumptie separaat van elkaar weer gegeven, suggererend dat deze onafhankelijk van elkaar zijn. Echter kunnen deze twee eindpunten niet onafhankelijk van elkaar beoordeeld worden; in ieder protocol is opgenomen dat pijn behandeld moet worden. Deze separate beoordeling geeft niet altijd een adequaat antwoord op de klinische vraag naar het analgetische effect van een interventie.
Daarnaast worden multimodale componenten als aparte interventies beoordeeld, echter de klinische vraag is naar de effectiviteit als bouwsteen van een multimodale werkwijze.
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Zoekverantwoording
|
In de databases Embase.com en Pubmed is op 21-7-2021 met relevante zoektermen gezocht naar RCT’s en Systematic Reviews en Observationele studies over niet medicamenteuze interventies bij patiënten die een chirurgische procedure ondergaan. De literatuurzoekactie leverde 1274 (SR+RCT) unieke treffersop. |
Zoekopbrengst
|
|
EMBASE |
PUBMED |
Ontdubbeld |
|
SRs |
169 |
187 |
286 |
|
RCTs |
779 |
504 |
988 |
|
Observationele studies |
205 |
549 |
611 |
|
Totaal |
|
|
1274 |
Zoekstrategie
Embase
|
No. |
Query |
Results |
|
#16 |
#12 AND #14 |
0 |
|
#15 |
24280480 AND nelson |
1 |
|
#14 |
10801169 |
1 |
|
#13 |
#11 NOT #10 NOT #9 |
205 |
|
#12 |
#10 NOT #9 |
779 |
|
#11 |
#5 AND #8 |
787 |
|
#10 |
#5 AND #7 |
874 |
|
#9 |
#5 AND #6 |
169 |
|
#8 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
6600961 |
|
#7 |
('clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti) NOT 'conference abstract':it |
2596771 |
|
#6 |
('meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT ('conference abstract'/it OR 'conference review'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) |
574167 |
|
#5 |
#4 AND [1-1-2005]/sd NOT (('adolescent'/exp OR 'child'/exp OR adolescent*:ti,ab OR child*:ti,ab OR schoolchild*:ti,ab OR infant*:ti,ab OR girl*:ti,ab OR boy*:ti,ab OR teen:ti,ab OR teens:ti,ab OR teenager*:ti,ab OR youth*:ti,ab OR pediatr*:ti,ab OR paediatr*:ti,ab OR puber*:ti,ab) NOT ('adult'/exp OR 'aged'/exp OR 'middle aged'/exp OR adult*:ti,ab OR man:ti,ab OR men:ti,ab OR woman:ti,ab OR women:ti,ab)) NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
1721 |
|
#4 |
#1 AND #2 AND #3 |
4143 |
|
#3 |
'postoperative period'/de OR 'postoperative complication'/de OR 'post operat*':ti,ab,kw OR (((after OR following) NEAR/3 (operation* OR surg*)):ti,ab,kw) OR postoperat*:ti,ab,kw OR 'postoperative pain'/exp/mj OR 'postoperative pain' OR 'postsurgical':ti,ab,kw OR 'surgery'/exp/mj OR 'surgical patient'/exp/mj OR 'surgical patient*':ti,ab,kw |
3456908 |
|
#2 |
'comfort'/exp OR 'massage'/exp OR 'cooling'/exp OR 'neurolinguistic programming'/exp OR 'hypnosis'/exp OR 'virtual reality'/exp OR 'breathing exercise'/exp OR 'mindfulness'/exp OR 'guided imagery'/exp OR 'alternative medicine'/exp OR distract*:ti,ab,kw OR nonpharmacolog*:ti,ab,kw OR 'non pharmacolog*':ti,ab,kw OR nlp:ti,ab,kw OR 'neurolinguistic program*':ti,ab,kw OR hypnosis:ti,ab,kw OR 'breathing exercise*':ti,ab,kw OR 'virtual reality':ti,ab,kw OR movie:ti,ab,kw OR 'low stimul*':ti,ab,kw OR lighting:ti,ab,kw OR cooling:ti,ab,kw OR decor:ti,ab,kw OR comfort:ti,ab,kw OR massage:ti,ab,kw OR 'stress reduct*':ti,ab,kw OR relaxation:ti,ab,kw OR 'mindfulness':ti,ab,kw OR 'mind body medicine':ti,ab,kw OR 'therapeutic communication':ti,ab,kw OR 'comfort talk':ti,ab,kw OR 'guided imagery':ti,ab,kw OR 'alternative medicine':ti,ab,kw |
476490 |
|
#1 |
'analgesic agent'/exp/mj OR 'analgesic agent':ti,ab,kw OR 'analgesia'/exp/mj OR 'analgesia':ti,ab,kw OR analgesi*:ti,ab,kw OR 'pain relief':ti,ab,kw |
589247 |
Pubmed
|
Search |
Query |
Results |
|
#13 |
Search: #11 NOT #10 NOT #9 Sort by: Most Recent |
|
|
#12 |
Search: #10 NOT #9 Sort by: Most Recent |
|
|
#11 |
Search: #5 AND #8 Sort by: Most Recent |
|
|
#10 |
Search: #5 AND #7 Sort by: Most Recent |
|
|
#9 |
Search: #5 AND #6 Sort by: Most Recent |
|
|
#8 |
Search: "Epidemiologic Studies"[Mesh] OR cohort[tiab] OR (case[tiab] AND (control[tiab] OR controll*[tiab] OR comparison[tiab] OR referent[tiab])) OR risk[tiab] OR causation[tiab] OR causal[tiab] OR "odds ratio"[tiab] OR etiol*[tiab] OR aetiol*[tiab] OR "natural history"[tiab] OR predict*[tiab] OR prognos*[tiab] OR outcome[tiab] OR course[tiab] OR retrospect*[tiab] Sort by: Most Recent |
|
|
#7 |
Search: ((random*[tiab] AND (controlled[tiab] OR control[tiab] OR placebo[tiab] OR versus[tiab] OR vs[tiab] OR group[tiab] OR groups[tiab] OR comparison[tiab] OR compared[tiab] OR arm[tiab] OR arms[tiab] OR crossover[tiab] OR cross-over[tiab]) AND (trial[tiab] OR study[tiab])) OR ((single[tiab] OR double[tiab] OR triple[tiab]) AND (masked[tiab] OR blind*[tiab]))) Sort by: Most Recent |
|
|
#6 |
Search: ("Meta-Analysis" [Publication Type] OR "Meta-Analysis as Topic"[Mesh] OR metaanaly*[tiab] OR meta-analy*[tiab] or metanaly*[tiab] OR "Systematic Review" [Publication Type] OR systematic[sb] OR "Cochrane Database Syst Rev"[Journal] or prisma[tiab] OR preferred reporting items[tiab] OR prospero[tiab] OR ((systemati*[ti] OR scoping[ti] OR umbrella[ti] OR structured literature[ti]) AND (review*[ti] OR overview*[ti])) OR systematic review*[tiab] OR scoping review*[tiab] OR umbrella review*[tiab] OR structured literature review*[tiab] OR systematic qualitative review*[tiab] OR systematic quantitative review*[tiab] OR systematic search and review[tiab] OR systematized review[tiab] OR systematised review[tiab] OR systemic review[tiab] OR systematic literature review*[tiab] OR systematic integrative literature review*[tiab] OR systematically review*[tiab] OR scoping literature review*[tiab] OR systematic critical review[tiab] OR systematic integrative review*[tiab] OR systematic evidence review[tiab] OR Systematic integrative literature review*[tiab] OR Systematic mixed studies review*[tiab] OR Systematized literature review*[tiab] OR Systematic overview*[tiab] OR Systematic narrative review*[tiab] OR ((systemati*[tiab] OR literature[tiab] OR database*[tiab] OR data-base*[tiab] OR structured[tiab] OR comprehensive*[tiab] OR systemic*[tiab]) AND search*[tiab]) OR (Literature[ti] AND review[ti] AND (database*[tiab] OR data-base*[tiab] OR search*[tiab])) OR ((data extraction[tiab] OR data source*[tiab]) AND study selection[tiab]) OR (search strategy[tiab] AND selection criteria[tiab]) OR (data source*[tiab] AND data synthesis[tiab]) OR medline[tiab] OR pubmed[tiab] OR embase[tiab] OR Cochrane[tiab] OR ((critical[ti] OR rapid[ti]) AND (review*[ti] OR overview*[ti] OR synthes*[ti])) OR (((critical*[tiab] OR rapid*[tiab]) AND (review*[tiab] OR overview*[tiab] OR synthes*[tiab]) AND (search*[tiab] OR database*[tiab] OR data-base*[tiab]))) OR metasynthes*[tiab] OR meta-synthes*[tiab]) NOT ("Comment" [Publication Type] OR "Letter" [Publication Type] OR "Editorial" [Publication Type] OR (("Animals"[Mesh] OR "Models, Animal"[Mesh]) NOT "Humans"[Mesh])) Sort by: Most Recent |
|
|
#5 |
Search: #4 AND ("2005/01"[Date - Entrez] : "3000"[Date - Entrez]) Sort by: Most Recent |
|
|
#4 |
Search: #1 AND #2 AND #3 Sort by: Most Recent |
|
|
#3 |
Search: "Postoperative Period"[Mesh] OR "Postoperative Complications"[Mesh] OR "post operat*"[tiab] OR "post operat*"[tiab] OR ((after[tiab] OR following[tiab]) AND operation*[tiab] OR surg*[tiab]) OR postoperat*[tiab] OR "Pain, Postoperative"[Mesh] OR "postoperative pain"[tiab] OR postsurgical[tiab] OR "General Surgery"[Mesh] OR surger*[tiab] OR "surgical patient"[tiab] Sort by: Most Recent |
|
|
#2 |
Search: "Patient Comfort"[Mesh] OR "Massage"[Mesh] OR "Cool-Down Exercise"[Mesh] OR "Neurolinguistic Programming"[Mesh] OR "Hypnosis"[Mesh] OR "Virtual Reality Exposure Therapy"[Mesh] OR "Virtual Reality"[Mesh] OR "Breathing Exercises"[Mesh] OR "Mindfulness"[Mesh] OR "Mind-Body Therapies"[Mesh] OR distract*[tiab] OR nonpharmacolog*[tiab] OR non pharmacolog*[tiab] OR nlp[tiab] OR "neurolinguistic program*"[tiab] OR hypnosis[tiab] OR "breathing exercise*"[tiab] OR "virtual reality"[tiab] OR movie[tiab] OR "low stimul*"[tiab] OR lighting[tiab] OR cooling[tiab] OR décor[tiab] OR comfort[tiab] OR massage[tiab] OR "stress reduct*"[tiab] OR relaxation[tiab] OR mindfulness[tiab] OR "mind body"[tiab] OR "therapeutic communication"[tiab] OR "comfort talk"[tiab] OR "guided imagery"[tiab] Sort by: Most Recent |
|
|
#1 |
Search: "Analgesics"[Mesh] OR "Analgesia"[Mesh] OR "Analgesics" [Pharmacological Action] OR analgesia[tiab] OR analgesi*[tiab] OR "pain relief"[tiab] OR "analgesic agent"[tiab] Sort by: Most Recent |