Magnesium
Uitgangsvraag
Wat is de meerwaarde van de toevoeging van perioperatief magnesium bij patiënten die een chirurgische ingreep ondergaan?
Aanbeveling
Overweeg de toediening van magnesium intraveneus bij hemodynamisch stabiele patiënten.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is een systematische literatuuranalyse uitgevoerd naar de effectiviteit van perioperatief magnesium vergeleken met standaardzorg bij patiënten die een chirurgische ingreep ondergingen. Postoperatieve pijn was de cruciale uitkomstmaat en het postoperatieve gebruik van opioïden en adverse events waren de belangrijke uitkomstmaten voor klinische besluitvorming.
Omdat de systematic review van Ng (2020) het uitgangspunt was, kon de werkgroep alleen conclusies trekken over de uitkomstmaten die zij rapporteerden. Dat waren postoperatieve pijn op 24 uur, postoperatief opiaatgebruik in 24 uur en bradycardie.
De bewijskracht voor pijnscores op 24 uur postoperatief is redelijk. Er is alleen afgewaardeerd voor risico op bias. Er werd geen klinisch relevant verschil gevonden tussen de groepen.
Voor het effect van magnesium op postoperatief opioïdengebruik is een redelijke bewijskracht gevonden voor 24 uur postoperatief, maar weer was het effect niet klinisch relevant.
In een eerdere systematische review van Murphy (2013) werd beschreven dat er bij de gepoolde pijnscores op 4-6 uur postoperatief een groter pijnstillend effect was dan 20-24 uur postoperatief met een gewogen gemiddeld verschil van -0,67 (-1,12 tot -0,23).
Ook werd het verschil in pijnscores en opioïdengebruik separaat als niet klinisch relevant beoordeeld, zo wijst toch de combinatie van een vermindering van pijnscores > 0,5 en een vermindering van opioïdengebruik > 5 mg op een aanwezig analgetisch effect.
De bewijskracht van het effect van magnesium op bradycardie is laag (GRADE), omdat er studies werden geïncludeerd met weinig patiënten en weinig events. Daarnaast was er ook risico op bias. Dit maakt het effect op bradycardie onzeker. De gemiddelde stijging in postoperatieve magnesiumspiegels lijkt beperkt (+0.59 mmol/L) na toediening van magnesium. Het is daardoor te verwachten dat het risico op bradycardie zal meevallen.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Voor patiënten is het belangrijk om adequate postoperatieve pijnstilling te hebben met zo min mogelijk complicaties. De voorkeur gaat ernaar uit om het gebruik van opioïden zoveel mogelijk te beperken. Magnesium lijkt in multimodale analgesie het gebruik van opiaten iets terug te kunnen dringen, maar het verschil bereikt de grens voor klinische relevantie niet. Er is een mogelijk beperkt toegenomen risico op bradycardie. Daar staat tegenover dat magnesium een geneesmiddel is dat reeds wordt toegediend op de operatiekamer en de werking geantagoneerd kan worden door calciumgluconaat.
Kosten (middelenbeslag)
De algehele kosteneffectiviteit van magnesium zijn nog niet in kaart gebracht. Uitgaande van het gebruik van spuitenpompen zal de tijd van klaarmaken van een extra middel beperkt zijn. Magnesiumsulfaat is een middel dat reeds op de operatiekamer wordt toegediend. Er is daardoor geen extra scholing of kwalificatie van personeel nodig. Als er minder opioïden perioperatief kort postoperatief gegeven worden, zal dat administratietijd schelen die verbonden is aan de opiumwetgeving. Waarschijnlijk zal de implementatie van magnesiumsulfaat tot een vergelijkbare perioperatieve tijdsbesteding hebben.
Aanvaardbaarheid, haalbaarheid en implementatie
Er is geen procesevaluatie gedaan die de implementatie van magnesiumsulfaat in de Nederlandse setting beschrijft. Daarentegen zijn er meer dan vijftig studies gedaan naar magnesiumsulfaat intra-operatief. Hieruit kan afgeleid worden dat de toepassing haalbaar moet zijn. Bovendien wordt magnesiumsulfaat intraveneus al reeds toegepast op de operatiekamers.
Een bezwaar zou zijn dat magnesium kan leiden tot hemodynamische instabiliteit. Het risico lijkt uit de literatuur zeer beperkt, hoewel de evidence hiervoor niet groot is. Omdat niet onderzocht is bij hemodynamisch instabiele patiënten is het advies om terughoudend te zijn om magnesiumsulfaat toe te passen bij kwetsbare patiënten.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Magnesium intraveneus geeft in aanvulling op de standaardanesthesie een lichte reductie op pijnscores. De hoeveelheid gebruikte opioïden die benodigd is gedurende 24 uur of gehele postoperatieve periode lijkt licht af te nemen. Vanwege dit gecombineerde effect is magnesium te overwegen ten behoeve van postoperatieve pijnstilling. Het effect van magnesium als mono-interventie zal echter beperkt zijn. Er zijn geen verschillen gevonden in het effect op bradycardie, maar gezien er potentieel een effect zou kunnen zijn, is er enige terughoudendheid geboden bij hemodynamische instabiele patiënten.
Onderbouwing
Achtergrond
Multidomale pijnbestrijding wordt gezien als perioperatieve standaardzorg. Verschillende niet-opioïden worden hiervoor gebruikt, waaronder magnesium. Magnesium kan via het effect op de NDMA-receptor de pijnstilling van andere nociceptieve stoffen vergroten. Het is belangrijk om de positieve analgetische effecten van magnesium af te wegen tegen mogelijke hemodynamische bijwerkingen zoals bradycardie en ECG-afwijkingen.
Conclusies / Summary of Findings
Postoperative pain
|
No GRADE |
No evidence was found regarding the effect of perioperative magnesium on pain scores at PACU arrival, at 6 hours, at 12 hours, and 48 post-surgery when compared to standard care in surgical patients.
Source: - |
|
Moderate GRADE |
Perioperative magnesium likely does not reduce pain scores at 24 hours post-surgery when compared to standard care in surgical patients.
Source: Benevides, 2021; Dehkordy, 2020; Kayalha, 2019; Lu, 2021; Mahajan, 2019; Ng, 2020; Sohn, 2021; Yazdi, 2022. |
Postoperative opioid consumption
|
No GRADE |
No evidence was found regarding the effect of perioperative magnesium on postoperative opioid consumption in PACU and in the total postoperative period when compared to standard care in surgical patients.
Sources: - |
|
Moderate GRADE |
Perioperative magnesium likely does not reduce postoperative opioid consumption in 24 hours when compared to standard care in surgical patients.
Sources: Dehkordy, 2020; El Mourad, 2019; Farouk, 2021; Kayalha, 2019; Mahajan, 2019; Ng, 2020; Sohn, 2021; Tsaousi, 2020; Yazdi, 2022. |
Adverse events
|
Low GRADE |
Perioperative magnesium may not increase the incidence of bradycardia compared to standard care in surgical patients.
Sources: Dehkordy, 2020; El Mourad, 2019; Gao, 2020; Kim, 2021; Lu, 2021; Ng, 2020; Tsaousi, 2020. |
Samenvatting literatuur
Description of studies
As shown in table 1, different regimens were used in various surgeries and using different scales to assess postoperative pain. All studies were RCTs.
Ng (2020) included studies administering intravenous magnesium (perioperative) and placebo in adult patients undergoing any type of noncardiac surgery. A total of 52 RCTs with
3341 patients were included in Ng (2020) for qualitative analysis. Out of these RCTs, 35 were conform the PICO and thus included in this literature analysis.
There was a wide range in the applied doses of magnesium among the studies. The majority of the studies applied a bolus dosing based on weight, of which most of the studies were followed by a continuous infusion. One study did not mention the used dose (Mireskandari 2015).
Table 1. Characteristics of studies that compared magnesium with standard of care.
|
Author, year |
Intervention |
Control |
Surgery type |
N total |
||||
|
bolus |
infusion |
|||||||
|
Studies from Ng, 2020 |
||||||||
|
Ahmed 2018 |
50 mg/kg |
- |
n.s. |
Thoracic surgery |
60 |
|||
|
Ayoglu 2005 |
50 mg/kg |
8 mg/kg/h |
n.s. |
Abdominal surgery |
40 |
|||
|
Benhaj Amor 2008 |
50 mg/kg |
500 mg/h |
n.s. |
Open cholecystectomy, |
48 |
|||
|
Bhatia 2004 |
50 mg/kg |
15 mg/kg/h |
n.s. |
Open cholecystectomy |
50 |
|||
|
Cizmeci 2007 |
50 mg/kg |
8 mg/kg/h |
n.s. |
Septorhinoplasty |
60 |
|||
|
Dabbagh 2009 |
- |
8 mg/kg/h |
n.s. |
Lower limb orthopaedic surgery |
60 |
|||
|
Demiroglu 2016 |
50 mg/kg |
- |
n.s. |
Lumbar disc surgery |
50 |
|||
|
Elsersy 2017 |
- |
30 mg/kg/1h, then 9 mg/kg/h |
n.s. |
Functional endoscopy surgery |
294 |
|||
|
Frassanito 2015 |
40 mg/kg |
10 mg/kg/h |
n.s. |
Total knee amputation |
40 |
|||
|
Gozdemir 2010 |
80 mg/kg |
2 g/h |
n.s. |
Transurethral prostatectomy |
60 |
|||
|
Haryalchi 2017 |
- |
15 mg/kg/h |
n.s. |
Total abdominal hysterectomy |
40 |
|||
|
Hwang 2010 |
50 mg/kg |
15 mg/kg/h |
n.s. |
Total hip arthroplasty |
40 |
|||
|
Ibrahim 2014 |
50 mg/kg |
2 mg/kg/h |
n.s. |
Lower extraperitoneal and lower limb surgery |
80 |
|||
|
Jaoua 2010 |
50 mg/kg |
10 mg/kg/h |
n.s. |
Gastrointestinal surgery |
38 |
|||
|
Kaya 2009 |
30 mg/kg |
500 mg/h |
n.s. |
Abdominal hysterectomy |
40 |
|||
|
Kim 2015 |
50 mg/kg |
- |
n.s. |
Endoscopic submucosal |
60 |
|||
|
Kiran 2011 |
50 mg/kg |
- |
n.s. |
Inguinal surgery |
100 |
|||
|
Kizilcik 2018 |
30 mg/kg |
20 mg/kg/h |
n.s. |
Sleeve gastrectomy |
80 |
|||
|
Ko 2011 |
50 mg/kg |
15 mg/kg/h |
n.s. |
Abdominal hysterectomy |
58 |
|||
|
Kocman 2013 |
- |
5 mg/kg/h |
n.s. |
Elective subumbilical surgery |
60 |
|||
|
Kumar 2013 |
50 mg/kg |
10 mg/kg/h |
n.s. |
Laparoscopic cholecystectomy |
60 |
|||
|
Mireskandari 2015 |
50 mg/kg |
- |
n.s. |
Caesarean section |
50 |
|||
|
Muthiah 2016 |
- |
150 mg/h |
n.s. |
Arthroscopic anterior cruciate ligament repair |
40 |
|||
|
Oguzhan 2008 |
30 mg/kg |
10 mg/kg/h |
n.s. |
Lumbar orthopaedic surgery |
50 |
|||
|
Olgun 2012 |
40 mg/kg |
10 mg/kg/h |
n.s. |
Laparoscopic cholecystectomy |
60 |
|||
|
Ryu 2016 |
50 mg/kg |
15 mg/kg/h |
n.s. |
Laparoscopic gastrectomy |
74 |
|||
|
Seyhan 2006 |
40 mg/kg |
10 mg/kg/h, 20 mg/kg/h |
n.s. |
Total abdominal hysterectomy |
60 |
|||
|
Shin 2016 |
50 mg/kg |
15 mg/kg/h |
n.s. |
Bilateral total knee amputation |
44 |
|||
|
Sohn 2017 |
50 mg/kg |
15 mg/kg/h |
n.s. |
Thoracoscopic surgery |
62 |
|||
|
Song 2011 |
30 mg/kg |
10 mg/kg/h |
n.s. |
Thyroidectomy |
84 |
|||
|
Sousa 2016 |
20 mg/kg |
2 mg/kg/h |
n.s. |
Laparoscopic gynaecological |
36 |
|||
|
Taheri 2015 |
50 mg/kg |
- |
n.s. |
Abdominal hysterectomy |
40 |
|||
|
Walia 2018 |
30 mg/kg |
- |
n.s. |
Elective surgery |
80 |
|||
|
Wilder-Smith 1997 |
200 mg |
200 mg/h |
n.s. |
Hysterectomy |
24 |
|||
|
Zarauza 2000 |
30 mg/kg |
10 mg/kg/h |
n.s. |
Colorectal surgery |
92 |
|||
|
Additional RCTs |
||||||||
|
Author, year |
Intervention |
Control |
Surgery type |
Start of infusion |
End of infusion |
N total |
||
|
bolus |
infusion |
|||||||
|
Benevides 2021 |
50 mg/kg |
15 mg/kg/h |
Placebo |
Abdominal hysterectomy |
Before anesthesia |
End of surgery |
92 |
|
|
Dehkordy 2020 |
50 mg/kg |
15 mg/kg/h |
Placebo |
Posterior lumbar spinal fusion surgery |
Before induction |
End of surgery |
80 |
|
|
El Mourad 2019 |
30 mg/kg |
- |
Placebo |
Laparoscopic sleeve gastrectomy |
Before dissection |
n.a. |
80 |
|
|
Farouk 2021 |
- |
15 mg/kg/h |
Placebo |
Bilateral inguinal hernial surgery |
Before anesthesia |
End of surgery |
40 |
|
|
Gao 2020 |
50 mg/kg |
15 mg/kg/h |
Placebo |
Hysteroscopy |
Before anesthesia |
End of surgery |
70 |
|
|
Kayalha 2019 |
5 mg/kg |
|
Placebo |
Femur or hip fracture surgery |
After block |
n.a. |
60 |
|
|
Kim 2021 |
50 mg/kg |
10 mg/kg/h |
Placebo |
Elective robotic radical prostatectomy |
Before anesthesia |
End of surgery |
60 |
|
|
Lu 2021 |
20 mg/kg |
20 mg/kg/h |
Placebo |
Laparoscopic cholecystectomy |
10 min before intubation |
End of surgery |
90 |
|
|
Mahajan 2019 |
50 mg/kg |
25 mg/kg/h |
Placebo |
Elective craniotomy |
‘intra-operative’ |
‘intraoperative’ |
45 |
|
|
Moon 2020 |
40 mg/kg |
10 mg/kg/h |
Placebo |
Laparoscopic gynaecological |
Before anesthesia |
End of surgery |
132 |
|
|
Sohn 2021 |
30 mg/kg |
15 mg/kg/h |
Placebo |
Major spine surgery |
After intubation |
End of surgery |
72 |
|
|
Tsaousi 2020 |
20 mg/kg |
20 mg/kg/h |
Placebo |
Single-space lumbar spine laminectomy |
Before anesthesia |
End of surgery |
74 |
|
|
Yazdi 2022 |
- |
25 mg/kg/1h, then 100 mg/kg/24 h |
Placebo |
Major cancer abdominal surgery |
Post- surgery |
24 hours post-surgery |
84 |
|
n.a. not available, n.s. normal saline
Results
If applicable, means and standard deviations were estimated from the medians and interquartile ranges using the method by Hozo (2005).
1. Postoperative pain
1.1 Postoperative pain at PACU arrival
Ng (2020) did not report postoperative pain at PACU arrival.
1.2 Postoperative pain at 6 hours post-surgery
Ng (2020) did not report postoperative pain at 6 hours.
1.3 Postoperative pain at 12 hours post-surgery
Ng (2020) did not report postoperative pain at 12 hours.
1.4 Postoperative pain at 24 hours post-surgery
Postoperative pain at 24 hours post-surgery was reported by Ng (2020) with data from 18 RCTs and 8 additional RCTs. The results are presented in figure 1. A mean difference (MD) of -0.50 (95% confidence interval (CI): -0.78 to -0.23) was found in favour of magnesium. This difference was not considered clinically relevant.
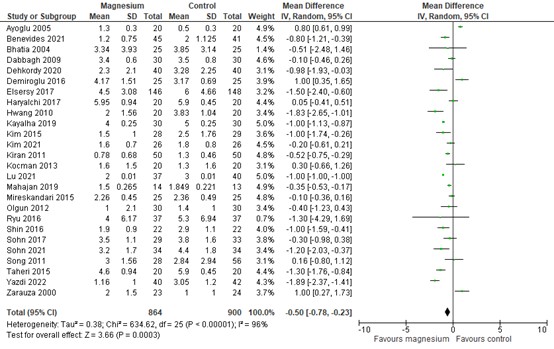
Figure 1. Postoperative pain at 24h post-surgery
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
In addition to the pooled data, 3 RCTs presented pain scores at 24 hours post-surgery in figures.
El Mourad (2019) presented VAS (scale 0-10) scores in figures. Pain scores were similar (both approximately 3.5 to 4; P= 0.193).
Moon (2020) reported NRS scores (scale 0-10) in figures. Median pain scores were approximately 3 (IQR 2-5) in the control group and 3 (IQR 1–4) in the magnesium group.
Tsaousi (2020) presented pain scores (scale 0-10) in figures. Median pain scores were approximately 1 (IQR 0-2) for magnesium and 2 (IQR 2-3) for control. Out of these three described studies, this is the only one describing a clinically relevant difference in favour of magnesium.
1.5 Postoperative pain at 48 hours post-surgery
Ng (2020) did not report postoperative pain at 48 hours.
2. Postoperative opioid consumption
2.1 In PACU
Ng (2020) did not report postoperative opioid consumption in PACU.
2.2 In 24h
Postoperative opioid consumption in 24 hours was reported by Ng (2020) with data from 18 RCTs and 9 additional RCTs. The results are presented in figure 2. A MD of -5.49 (95% CI: -6.74 to -4.25) was found in favour of magnesium. This difference was not considered clinically relevant.
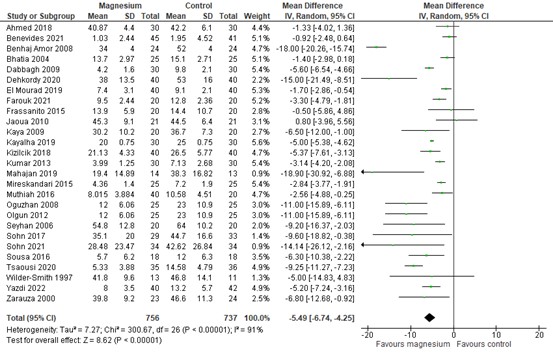
Figure 2. Postoperative opioid consumption in 24h post-surgery
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
In addition to the pooled data, one RCT provided data on postoperative opioid consumption in 24 hours post-surgery.
Moon (2020) reported cumulative postoperative fentanyl consumption (i.v.) at 24 hours post-surgery in figures. Fentanyl consumption was approximately 24 mg MME (i.v.) versus 32.5 mg MME (i.v.) in the magnesium and control group, respectively.
2.3 Total postoperative period
Ng (2020) did not report postoperative opioid consumption in the total postoperative period.
3. Adverse events
Bradycardia
The incidence of bradycardia was reported by Ng (2020) with data from 9 RCTs and 6 additional RCTs. The results are presented in figure 3. A risk difference (RD) of -0.00 (95% -0.03 to 0.02) was found.
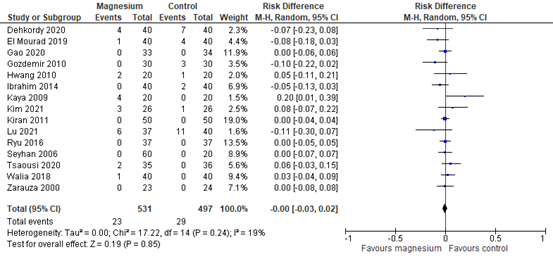
Figure 3. Adverse events - bradycardia
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
In addition to the pooled data, one RCT reported bradycardia without raw data.
Benevides (2021) reported a higher incidence of bradycardia in the magnesium group (11.1% vs 0%; P = 0.05), with a similar mean HR in both groups (p=0.054).
Level of evidence of the literature
The level of evidence regarding the outcome measures postoperative pain, postoperative opioid consumption and adverse events started as high, because the studies were RCTs.
The level of evidence regarding the outcome measure postoperative pain at PACU arrival, at 6 hours, at 12 hours and at 48 hours post-surgery could not be assessed, as the included systematic review did not report these outcomes.
The level of evidence regarding the outcome measure postoperative pain at 24 hours post-surgery was downgraded by 1 level because of study limitations (risk of bias; -1). The level of evidence for postoperative opioid consumption in 24 hours is moderate (GRADE).
The level of evidence regarding the outcome measure postoperative opioid consumption in PACU and in the total postoperative period could not be assessed, as the included systematic review did not report these outcomes.
The level of evidence regarding the outcome measure postoperative opioid consumption in 24 hours was downgraded by 1 level because of study limitations (risk of bias; -1). The level of evidence for postoperative opioid consumption in 24 hours is moderate (GRADE).
The level of evidence regarding the outcome measure bradycardia was downgraded by 2 levels because of study limitations (risk of bias; -1) and imprecision (very low number of events; -1). The level of evidence for bradycardia is low (GRADE).
Zoeken en selecteren
A systematic review of the literature was performed to answer the following question:
What is the effectiveness of adding magnesium perioperatively to standard care in surgical patients on postoperative pain, adverse outcomes and rescue analgesic consumption?
P (patients) patients undergoing a surgical procedure
I (intervention) perioperative i.v. magnesium + standard care
C (comparison) (placebo +) standard care
O (outcomes) postoperative pain
postoperative opioid consumption
adverse events (bradycardia)
Relevant outcome measures
The guideline development group considered postoperative pain as a critical outcome measure for decision making; and postoperative opioid consumption and adverse events as an important outcome measure for decision making.
The working group defined the outcome measures as follows:
Postoperative pain at rest: Validated pain scale (Visual Analogue Scale (VAS), Numeric Rating Scale (NRS) or Verbal Rating Scale (VRS)) at post-anesthesia care unit (PACU) arrival, 6, 12, 24 and 48 hours post-surgery. Postoperative opioid consumption was assessed in PACU, 24 hours post-surgery and total postoperative period.
A priori, the working group did not define adverse events but used the definitions used in the studies.
Chronic postoperative pain is acknowledged by the working group as a relevant patient outcomes measure, however scarcely studied. In this literature analysis, chronic postoperative pain is not described in the PICO and results only mentioned in the knowledge gaps.
The working group defined one point as a minimal clinically (patient) important difference on a 10-point pain score and 10 mm on a 100 mm pain scale. Regarding postoperative opioid consumption, a difference of 10 mg was considered clinically relevant. For dichotomous variables, a difference of 10% was considered clinically relevant (RD 0.10).
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms to identify systematic reviews published until 13-07-2022. This systematic literature search resulted in 317 hits. Studies were selected based on the following criteria:
- Systematic review (SR)
- Published between inception up to 13-07-2022
- Patients ≥ 18 years
- Conform PICO
After identifying the most relevant SR, the databases were searched to identify relevant randomized controlled trials (RCTs) from January 2019 (search date: Ng, 2020) up to 13-07-2022. This systematic literature search resulted in 398 hits. Studies were selected based on the following criteria:
- RCT
- Published between January 2019 and 13-07-2022
- Patients ≥ 18 years
- Conform PICO
The detailed search strategy is depicted under the tab Methods.
A total of 46 studies were initially selected based on title and abstract screening. After reading the full text, 32 studies were excluded (see the table with reasons for exclusion under the tab Methods), and 14 studies were included.
Results
Fourteen publications (1 SR reporting on 35 studies and 13 individual RCTs) were included in the analysis of the literature. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
Referenties
- Benevides ML, Fialho DC, Linck D, Oliveira AL, Ramalho DHV, Benevides MM. Intravenous magnesium sulfate for postoperative analgesia after abdominal hysterectomy under spinal anesthesia: a randomized, double-blind trial. Braz J Anesthesiol. 2021 Sep-Oct;71(5):498-504. doi: 10.1016/j.bjane.2021.01.008. Epub 2021 Mar 21. PMID: 33762190; PMCID: PMC9373682.
- Dehkordy ME, Tavanaei R, Younesi E, Khorasanizade S, Farsani HA, Oraee-Yazdani S. Effects of perioperative magnesium sulfate infusion on intraoperative blood loss and postoperative analgesia in patients undergoing posterior lumbar spinal fusion surgery: A randomized controlled trial. Clin Neurol Neurosurg. 2020 Sep;196:105983. doi: 10.1016/j.clineuro.2020.105983. Epub 2020 Jun 2. PMID: 32521394.
- El Mourad MB, Arafa SK. Effect of intravenous versus intraperitoneal magnesium sulfate on hemodynamic parameters and postoperative analgesia during laparoscopic sleeve gastrectomy-A prospective randomized study. J Anaesthesiol Clin Pharmacol. 2019 Apr-Jun;35(2):242-247. doi: 10.4103/joacp.JOACP_208_18. PMID: 31303716; PMCID: PMC6598561.
- Farouk I, Hassan MM, Fetouh AM, Elgayed AEA, Eldin MH, Abdelhamid BM. Analgesic and hemodynamic effects of intravenous infusion of magnesium sulphate versus dexmedetomidine in patients undergoing bilateral inguinal hernial surgeries under spinal anesthesia: a randomized controlled study. Braz J Anesthesiol. 2021 Sep-Oct;71(5):489-497. doi: 10.1016/j.bjane.2021.02.004. Epub 2021 Feb 3. PMID: 34537120; PMCID: PMC9373243.
- Gao PF, Lin JY, Wang S, Zhang YF, Wang GQ, Xu Q, Guo X. Antinociceptive effects of magnesium sulfate for monitored anesthesia care during hysteroscopy: a randomized controlled study. BMC Anesthesiol. 2020 Sep 21;20(1):240. doi: 10.1186/s12871-020-01158-9. PMID: 32957926; PMCID: PMC7504853.
- Kayalha H, Yaghoubi S, Yazdi Z, Izadpanahi P. Effect of Intervenous Magnesium Sulfate on Decreasing Opioid Requirement after Surgery of the Lower Limb Fracture by Spinal Anesthesia. Int J Prev Med. 2019 May 6;10:57. doi: 10.4103/ijpvm.IJPVM_320_17. PMID: 31143431; PMCID: PMC6528420.
- Kim HY, Lee SY, Lee HS, Jun BK, Choi JB, Kim JE. Beneficial Effects of Intravenous Magnesium Administration During Robotic Radical Prostatectomy: A Randomized Controlled Trial. Adv Ther. 2021 Mar;38(3):1701-1712. doi: 10.1007/s12325-021-01643-8. Epub 2021 Feb 21. PMID: 33611742.
- Lu J, Wang JF, Guo CL, Yin Q, Cheng W, Qian B. Intravenously injected lidocaine or magnesium improves the quality of early recovery after laparoscopic cholecystectomy: A randomised controlled trial. Eur J Anaesthesiol. 2021 Mar 1;38(Suppl 1):S1-S8. doi: 10.1097/EJA.0000000000001348. PMID: 33074940.
- Mahajan C, Mishra RK, Jena BR, Kapoor I, Prabhakar H, Rath GP, Chaturvedi A. Effect of magnesium and lignocaine on post-craniotomy pain: A comparative, randomized, double blind, placebo-controlled study. Saudi J Anaesth. 2019 Oct-Dec;13(4):299-305. doi: 10.4103/sja.SJA_837_18. PMID: 31572073; PMCID: PMC6753769.
- Murphy JD, Paskaradevan J, Eisler LL, Ouanes JP, Tomas VA, Freck EA, Wu CL. Analgesic efficacy of continuous intravenous magnesium infusion as an adjuvant to morphine for postoperative analgesia: a systematic review and meta-analysis. Middle East J Anaesthesiol. 2013 Feb;22(1):11-20. PMID: 23833845.
- Moon S, Lim S, Yun J, Lee W, Kim M, Cho K, Ki S. Additional effect of magnesium sulfate and vitamin C in laparoscopic gynecologic surgery for postoperative pain management: a double-blind randomized controlled trial. Anesth Pain Med (Seoul). 2020 Jan 31;15(1):88-95. doi: 10.17085/apm.2020.15.1.88. PMID: 33329796; PMCID: PMC7713852.
- Ng KT, Yap JLL, Izham IN, Teoh WY, Kwok PE, Koh WJ. The effect of intravenous magnesium on postoperative morphine consumption in noncardiac surgery: A systematic review and meta-analysis with trial sequential analysis. Eur J Anaesthesiol. 2020 Mar;37(3):212-223. doi: 10.1097/EJA.0000000000001164. PMID: 31977626.
- Sohn HM, Kim BY, Bae YK, Seo WS, Jeon YT. Magnesium Sulfate Enables Patient Immobilization during Moderate Block and Ameliorates the Pain and Analgesic Requirements in Spine Surgery, Which Can Not Be Achieved with Opioid-Only Protocol: A Randomized Double-Blind Placebo-Controlled Study. J Clin Med. 2021 Sep 22;10(19):4289. doi: 10.3390/jcm10194289. PMID: 34640307; PMCID: PMC8509453.
- Tsaousi G, Nikopoulou A, Pezikoglou I, Birba V, Grosomanidis V. Implementation of magnesium sulphate as an adjunct to multimodal analgesic approach for perioperative pain control in lumbar laminectomy surgery: A randomized placebo-controlled clinical trial. Clin Neurol Neurosurg. 2020 Oct;197:106091. doi: 10.1016/j.clineuro.2020.106091. Epub 2020 Jul 18. PMID: 32721845.
- Yazdi AP, Esmaeeli M, Gilani MT. Effect of intravenous magnesium on postoperative pain control for major abdominal surgery: a randomized double-blinded study. Anesth Pain Med (Seoul). 2022 Jul;17(3):280-285. doi: 10.17085/apm.22156. Epub 2022 Jul 28. PMID: 35918860; PMCID: PMC9346203.
Evidence tabellen
Evidence tables
Table of quality assessment for systematic reviews of RCTs and observational studies
|
Study
First author, year |
Appropriate and clearly focused question?1
Yes/no/unclear |
Comprehensive and systematic literature search?2
Yes/no/unclear |
Description of included and excluded studies?3
Yes/no/unclear |
Description of relevant characteristics of included studies?4
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?5
Yes/no/unclear/not applicable |
Assessment of scientific quality of included studies?6
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?7
Yes/no/unclear |
Potential risk of publication bias taken into account?8
Yes/no/unclear |
Potential conflicts of interest reported?9
Yes/no/unclear |
|
Ng, 2020 |
Yes |
Yes |
Yes |
Yes |
MD and OR values reported; no analysis corrected for confounding factors |
Yes; 6x low risk 11x high risk Rest: unclear |
Yes |
Yes |
Yes (for review, not for individual studies) |
Risk of bias of RCTs included in SR Ng, 2020 (from: Ng, 2020, according to the Cochrane Risk of Bias Tool)
|
Study |
Sequence generation |
Allocation concealment |
Blinding of participants and personnel |
Blinding of outcome assessment |
Incomplete outcome data |
Selective outcome reporting |
Other sources of bias |
Overall |
|
Wilder-Smith 1997 |
Unclear |
Unclear |
Unclear |
Unclear |
High |
Unclear |
High |
High |
|
Koinig 1998 |
Unclear |
Unclear |
High |
High |
Low |
Low |
High |
High |
|
Zarauza 2000 |
High |
Unclear |
Unclear |
Unclear |
Low |
Unclear |
High |
High |
|
Schulz-stubner 2001 |
Unclear |
Unclear |
Unclear |
Unclear |
Low |
Low |
Low |
Unclear |
|
Levaux 2003 |
Unclear |
Unclear |
Low |
Low |
Low |
Low |
Low |
Unclear |
|
Mavrommati 2004 |
Unclear |
Unclear |
High |
High |
Low |
Low |
High |
High |
|
Bhatia 2004 |
Unclear |
Unclear |
Unclear |
Unclear |
Low |
Low |
Low |
Unclear |
|
Ayoglu 2005 |
Low |
Low |
Low |
Low |
Low |
Unclear |
Low |
Unclear |
|
Seyhan 2006 |
Low |
Unclear |
Unclear |
Unclear |
Low |
Low |
Low |
Unclear |
|
Tauzin-Fin 2006 |
Low |
Unclear |
Low |
Low |
Low |
Unclear |
Low |
Unclear |
|
Cizmeci 2007 |
Unclear |
Unclear |
Unclear |
Unclear |
Low |
Unclear |
Low |
Unclear |
|
Tramer 2007 |
Low |
Low |
Unclear |
Low |
Low |
Low |
Low |
Unclear |
|
Mentes 2008 |
Unclear |
Unclear |
Unclear |
Unclear |
Low |
Low |
Unclear |
Unclear |
|
Benhaj amor 2008 |
Low |
Low |
Low |
Low |
Low |
Unclear |
Low |
Unclear |
|
Ryu 2008 |
Low |
Low |
Low |
Low |
Low |
Unclear |
Low |
Unclear |
|
Oguzhan 2008 |
Low |
Low |
Low |
Low |
High |
High |
Unclear |
High |
|
Kaya 2009 |
Low |
Unclear |
Unclear |
Low |
Low |
Unclear |
Unclear |
Unclear |
|
Dabbagh 2009 |
Low |
Unclear |
Low |
Low |
Low |
High |
Low |
Unclear |
|
Hwang 2010 |
Low |
Low |
Unclear |
Low |
Low |
High |
Low |
Unclear |
|
Jaoua 2010 |
Low |
Unclear |
Unclear |
Low |
High |
Low |
Low |
Unclear |
|
Saadawy 2010 |
Low |
Low |
Low |
Unclear |
High |
Low |
Low |
Unclear |
|
Gozdemir 2010 |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
|
Ko 2011 |
Unclear |
Unclear |
Unclear |
Unclear |
High |
Unclear |
Low |
Unclear |
|
Song 2011 |
Low |
Low |
Low |
Low |
High |
Unclear |
High |
High |
|
Kiran 2011 |
Low |
Unclear |
Unclear |
Unclear |
Low |
Low |
Low |
Unclear |
|
Olgun 2012 |
Low |
Unclear |
Unclear |
Unclear |
Low |
Low |
Low |
Unclear |
|
Khafagy 2012 |
Low |
Unclear |
Unclear |
Unclear |
Low |
Unclear |
Low |
Unclear |
|
Kocman 2013 |
Unclear |
Unclear |
Unclear |
Unclear |
Low |
Low |
Low |
Unclear |
|
Kumar 2013 |
Unclear |
Unclear |
Low |
Unclear |
Low |
Low |
Low |
Unclear |
|
DeOliveira 2014 |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
|
Ibrahim 2014 |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
|
Kahraman 2014 |
Unclear |
Low |
Unclear |
Unclear |
High |
Unclear |
High |
High |
|
Mireskandari 2015 |
Low |
Unclear |
Unclear |
Low |
Low |
Low |
Low |
Unclear |
|
Frassanito 2015 |
Low |
Low |
Unclear |
Low |
Low |
Low |
Low |
Unclear |
|
Taheri 2015 |
Low |
Unclear |
Unclear |
Low |
Low |
Low |
Low |
Unclear |
|
Kim 2015 |
Low |
Low |
Unclear |
Low |
High |
Unclear |
High |
High |
|
Asadollah 2015 |
Unclear |
Unclear |
Low |
Low |
low |
High |
High |
High |
|
Shah 2016 |
Low |
Unclear |
Unclear |
Low |
Low |
High |
Unclear |
Unclear |
|
Demiroglu 2016 |
Unclear |
Unclear |
Unclear |
Unclear |
Low |
High |
Unclear |
Unclear |
|
Ryu 2016 |
Low |
Unclear |
Low |
Low |
High |
Unclear |
Unclear |
Unclear |
|
Vickovic 2016 |
Unclear |
Unclear |
Unclear |
Unclear |
Low |
Unclear |
Unclear |
Unclear |
|
Muthiah 2016 |
Low |
Low |
Unclear |
Low |
Low |
High |
Low |
Unclear |
|
Shin 2016 |
Low |
Low |
Unclear |
Low |
Low |
Low |
Low |
Unclear |
|
Sousa 2016 |
Unclear |
Low |
Low |
Low |
High |
Low |
Low |
Unclear |
|
Gucyetmez 2016 |
Unclear |
Unclear |
Unclear |
Unclear |
Low |
Low |
Unclear |
Unclear |
|
Shal 2017 |
Low |
Low |
Low |
Unclear |
Low |
Low |
Low |
Unclear |
|
Sohn 2017 |
Low |
Low |
Low |
Low |
High |
Low |
High |
High |
|
Elsersy 2017 |
Low |
Low |
Unclear |
Unclear |
High |
Low |
Low |
Unclear |
|
Haryalchi 2017 |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
|
Walia 2018 |
Low |
Low |
Low |
Low |
High |
High |
Unclear |
High |
|
Kizilcik 2018 |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
|
Ahmed 2018 |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
Risk of bias of additional RCTs included
Risk of bias table for intervention studies (randomized controlled trials; based on Cochrane risk of bias tool and suggestions by the CLARITY Group at McMaster University)
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Benevides, 2021 |
Definitely yes;
Reason: Computer-generated randomization lists. |
Definitely yes;
Reason: Sealed, black envelopes were used |
Probably yes;
Reason: Patients and outcome assessor blinded. |
Probably yes
Reason: Loss to follow-up was infrequent in intervention and control group. |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Dehkordy, 2020 |
Probably no;
Reason: no details on randomization method, except that block randomization was used |
Probably no;
Reason: not described |
Definitely yes;
Reason: everybody involved in the study was blinded |
Definitely yes;
Reason: No loss to follow-up reported |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
El Mourad, 2019 |
Definitely yes;
Reason: Computer-generated randomization sequence |
Definitely yes;
Reason: Sealed, opaque envelopes were used |
Probably yes;
Reason: Patient, health care provider, data collectors were blinded. Analysts are not reported. |
Definitely yes;
Reason: No loss to follow-up reported |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Farouk, 2021 |
Definitely yes;
Reason: Computer-generated randomization sequence |
Definitely yes;
Reason: Concealment with serially numbered sealed opaque envelopes |
Probably yes;
Reason: Patient, health care provider, data collectors were blinded. Analysts are not reported. |
Definitely yes;
Reason: No loss to follow-up reported |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Gao, 2020 |
Definitely yes;
Reason: computer-generated randomization Web-based, random number generator
|
Probably no;
Reason: not described |
Probably yes;
Reason: Patient, health care provider, data collectors were blinded. Analysts are not reported. |
Probably yes
Reason: Loss to follow-up was infrequent in intervention and control group. |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Kayalha, 2019 |
Probably no;
Reason: ‘randomization by colorful cards’, no details provided |
Probably no;
Reason: not described |
Probably yes;
Reason: Patients and anesthesiologist were uninformed of the group assignment. No further details provided. |
Definitely yes;
Reason: No loss to follow-up reported |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Kim, 2021 |
Definitely yes;
Reason: computer-generated randomization technique |
Probably no;
Reason: not described |
Probably yes;
Reason: Patient, health care provider, data collectors were blinded. Analysts are not reported. |
Definitely yes;
Reason: No loss to follow-up reported |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Lu, 2021 |
Probably yes;
Reason: randomization by a random number table generated by SPSS |
Definitely yes;
Reason: Sealed, opaque envelopes were used |
Probably yes;
Reason: Patient, health care provider, data collectors were blinded. Analysts are not reported. |
Probably no;
Reason: Somewhat frequent loss to follow-up (17.8% in intervention group) |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
Some concerns |
|
Mahajan, 2019 |
Definitlely yes;
Reason: computer‑generated table of random numbers |
Definitely yes;
Reason: Sealed, opaque envelopes were used |
Probably yes;
Reason: Patient, health care provider, data collectors were blinded. Analysts are not reported. |
Probably yes;
Reason: only loss to follow-up in the control group (17.8%) |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Moon, 2020 |
Probably yes;
Reason: drawing envelopes |
Probably yes;
Reason: sealed envelopes were used |
Probably yes;
Reason: Patient, health care provider, data collectors were blinded. Analysts are not reported. |
Probably yes
Reason: Loss to follow-up was infrequent in intervention and control group. |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Sohn, 2021 |
Probably yes;
Reason: Computer-generated block randomization with blocks of size 4 |
Probably yes;
Reason: sealed envelopes were used |
Probably yes;
Reason: Patient, health care provider, data collectors were blinded. Analysts are not reported. |
Probably yes
Reason: Loss to follow-up was infrequent in intervention and control group. |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Tsaousi, 2020 |
Definitely yes;
Reason: computer-generated randomization technique |
Probably yes;
Reason: sealed envelopes were used |
Probably yes;
Reason: Patient, health care provide were blinded. Data collectors and analysts were not reported. |
Probably yes
Reason: Loss to follow-up was infrequent in intervention and control group. |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
|
Yazdi, 2022 |
Probably yes;
Reason: online random number table |
Probably yes;
Reason: sealed envelopes were used |
Probably yes;
Reason: Patient, health care provide were blinded. Data collectors and analysts were not reported. |
Probably yes
Reason: Loss to follow-up was infrequent in intervention and control group. |
Definitely yes
Reason: All relevant outcomes were reported; |
Definitely yes;
Reason: No other problems noted |
LOW |
Evidence table for intervention studies – SRs – descriptives
|
Study reference |
RCT reference |
Study designs |
Setting and country |
Funding and conflicts of interest |
N at baseline; age (sd) |
Type of surgery; timing of intervention |
Intervention regime |
Intervention |
Control |
Postoperative analgesia |
Loss-to-follow-up / etamizole data |
|
Ng, 2020 |
A: Wilder-Smith, 1997 B: Koinig, 1998 C: Zarauza, 2000 D: Schulz-Stübner, 2001 E: Levaux, 2003 F: Mavrommati, 2004 G: Bhatia, 2004 H: Ayoglu, 2005 I: Seyhan, 2006 J: Tauzin-Fin, 2006 K: Cizmeci, 2007 L: Tramer, 2007 M: Mentes, 2008 N: Benhaj Amor, 2008 O: Ryu, 2008 P: Oguzhan, 2008 Q: Kaya, 2009 R: Dabbagh, 2009 S: Hwang, 2010 T: Jaouda, 2010 U: Saadawy, 2010 V: Gozdemir, 2010 W: Koinig, 2011 X: Song, 2011 Y: Kiran, 2011 Z: Olgun, 2012 AA: Khafagy, 2012 BB: Kocman, 2013 CC: Kumar, 2013 DD: de Oliveira, 2013 EE: Ibrahim, 2014 FF: Kahraman, 2014 GG: Mireskandari, 2015 HH: Frassanito, 2015 II: Taheri, 2015 JJ: Kim, 2015 KK: Asadollah, 2015 LL: Shah, 2016 MM: Demiroglu, 2016 NN: Ryu, 2016 OO: Vickovic, 2016 PP: Muthiah, 2016 QQ: Shin, 2016 RR: Sousa, 2016 SS: Gucyetmez, 2016 TT: Shal, 2017 UU: Sohn, 2017 VV: Elsersy, 2017 WW: Haryalchi, 2017 XX: Walia, 2018 YY: Kizilcik, 2018 ZZ: Ahmed, 2018 |
A: RCT B: RCT C: RCT D: RCT E: RCT F: RCT G: RCT H: RCT I: RCT J: RCT K: RCT L: RCT M: RCT N: RCT O: RCT P: RCT Q: RCT R: RCT S: RCT T: RCT U: RCT V: RCT W: RCT X: RCT Y: RCT Z: RCT AA: RCT BB: RCT CC: RCT DD: RCT EE: RCT FF: RCT GG: RCT HH: RCT II: RCT JJ: RCT KK: RCT LL: RCT MM: RCT NN: RCT OO: RCT PP: RCT QQ: RCT RR: RCT SS: RCT TT: RCT UU: RCT VV: RCT WW: RCT XX: RCT YY: RCT ZZ: RCT |
A: n.s., Switserland B: n.s., Austria C: n.s., Spain D: n.s., Germany E: n.s., Belgium F: n.s., Greece G: n.s., India H: n.s., Europe I: n.s., Turkey J: n.s., France K: n.s., Turkey L: n.s., Switserland M: n.s., Turkey N: n.s., France O: n.s., South Korea P: n.s., Turkey Q: n.s., Turkey R: n.s., Iran S: n.s., South Korea T: n.s., Tunesia U: n.s., Egypt V: n.s., Turkey W: n.s., South Korea X: n.s., South Korea Y: n.s., India Z: n.s., Turkey AA: n.s., Egypt BB: n.s., Croatia CC: n.s., India DD: n.s., USA EE: n.s., Egypt FF: n.s., Turkey GG: n.s., Iran HH: n.s., Italy II: n.s., Iran JJ: n.s., South Korea KK: n.s., Iran LL: n.s., India MM: n.s., Turkey NN: n.s., South Korea OO: n.s., Serbia PP: n.s., India QQ: n.s., South Korea RR: n.s., Brazil SS: n.s., Turkey TT: n.s., Egypt UU: n.s., South Korea VV: n.s., Egypt WW: n.s., Iran XX: n.s., India YY: n.s., Turkey ZZ: n.s., Egypt |
A: n.s. B: n.s. C: n.s. D: n.s. E: n.s. F: n.s. G: n.s. H: n.s. I: n.s. J: n.s. K: n.s. L: n.s. M: n.s. N: n.s. O: n.s. P: n.s. Q: n.s. R: n.s. S: n.s. T: n.s. U: n.s. V: n.s. W: n.s. X: n.s. Y: n.s. Z: n.s. AA: n.s. BB: n.s. CC: n.s. DD: n.s. EE: n.s. FF: n.s. GG: n.s. HH: n.s. II: n.s. JJ: n.s. KK: n.s. LL: n.s. MM: n.s. NN: n.s. OO: n.s. PP: n.s. QQ: n.s. RR: n.s. SS: n.s. TT: n.s. UU: n.s. VV: n.s. WW: n.s. XX: n.s. YY: n.s. ZZ: n.s. |
A: 24; n.s. (n.s.) B: 46; n.s. (n.s.) C: 92; n.s. (n.s.) D: 50; n.s. (n.s.) E: 24; n.s. (n.s.) F: 42; n.s. (n.s.) G: 50; n.s. (n.s.) H: 40; n.s. (n.s.) I: 60; n.s. (n.s.) J: 30; n.s. (n.s.) K: 60; n.s. (n.s.) L: 200; n.s. (n.s.) M: 83; n.s. (n.s.) N: 48; n.s. (n.s.) O: 50; n.s. (n.s.) P: 50; n.s. (n.s.) Q: 40; n.s. (n.s.) R: 60; n.s. (n.s.) S: 40; n.s. (n.s.) T: 38; n.s. (n.s.) U: 80; n.s. (n.s.) V: 60; n.s. (n.s.) W: 58; n.s. (n.s.) X: 84; n.s. (n.s.) Y: 100; n.s. (n.s.) Z: 60; n.s. (n.s.) AA: 60; n.s. (n.s.) BB: 60; n.s. (n.s.) CC: 60; n.s. (n.s.) DD: 46; n.s. (n.s.) EE: 80; n.s. (n.s.) FF: 38; n.s. (n.s.) GG: 50; n.s. (n.s.) HH: 40; n.s. (n.s.) II: 40; n.s. (n.s.) JJ: 60; n.s. (n.s.) KK: 30; n.s. (n.s.) LL: 108; n.s. (n.s.) MM: 50; n.s. (n.s.) NN: 74; n.s. (n.s.) OO: 100; n.s. (n.s.) PP: 40; n.s. (n.s.) QQ: 44; n.s. (n.s.) RR: 36; n.s. (n.s.) SS: 70; n.s. (n.s.) TT: 70; n.s. (n.s.) UU: 62; n.s. (n.s.) VV: 294; n.s. (n.s.) WW: 40; n.s. (n.s.) XX: 80; n.s. (n.s.) YY: 80; n.s. (n.s.) ZZ: 60; n.s. (n.s.) |
A: Hysterectomy; Before anaesthesia induction B: Arthroscopic knee surgery; After anaesthesia induction C: Colorectal surgery; Before anaesthesia induction D: Pars plana vitrectomy; After anaesthesia induction E: Lumbar orthopaedics surgery; Before anaesthesia induction F: Abdominal hernioplasty; After anaesthesia induction G: Open cholecystectomy; Before anaesthesia induction H: Abdominal surgery; Before anaesthesia induction I: Total abdominal hysterectomy; Before anaesthesia induction J: Radical prostatectomy; After anaesthesia induction K: Septorhinoplasty; Before anaesthesia induction L: Ambulatory ilioinguinal hernia repair/ varicose vein operation; After anaesthesia induction M: Laparoscopic cholecystectomy; After anaesthesia induction N: Open cholecystectomy, gastrojejunal surgery; During anaesthesia induction O: Abdominal hysterectomy; Before anaesthesia induction P: Lumbar orthopaedic surgery; After anaesthesia induction Q: Abdominal hysterectomy; Before anaesthesia induction R: Lower limb orthopaedic surgery; After anaesthesia induction S: Total hip arthroplasty; After anaesthesia induction T: Gastrointestinal surgery; Before anaesthesia induction U: Laparoscopic cholecystectomy; Before anaesthesia induction V: Transurethral prostatectomy; After anaesthesia induction W: Abdominal hysterectomy; After anaesthesia induction X: Thyroidectomy; After anaesthesia induction Y: Inguinal surgery; Before anaesthesia induction Z: Laparoscopic cholecystectomy; Before anaesthesia induction AA: Open cholecystectomy; After anaesthesia induction BB: Elective subumbilical surgery; Before anaesthesia induction CC: Laparoscopic cholecystectomy; Before anaesthesia induction DD: Segmental mastectomy; Before anaesthesia induction EE: Lower extraperitoneal and lower limb surgery; Before anaesthesia induction FF: Abdominal hysterectomy; After anaesthesia induction GG: Caesarean section; Before anaesthesia induction HH: Total knee amputation; After anaesthesia induction II: Abdominal hysterectomy; Before anaesthesia induction JJ: Endoscopic submucosal dissection of gastric neoplasm; Before anaesthesia induction KK: Hysterectomy/ Myomectomy; Before anaesthesia induction LL: Lower abdominal and lower limb surgery; After anaesthesia induction MM: Lumbar disc surgery; After anaesthesia induction NN: Laparoscopic gastrectomy; After anaesthesia induction OO: Abdominal, orthopaedic, urology surgery; Before anaesthesia induction PP: Arthroscopic anterior cruciate ligament repair; Before anaesthesia induction QQ: Bilateral total knee amputation; During anaesthesia induction RR: Laparoscopic gynaecological surgery; After anaesthesia induction SS: Liver transplant; After anaesthesia induction TT: Arthroscopic knee surgery; Before anaesthesia induction UU: Thoracoscopic surgery; After anaesthesia induction VV: Functional endoscopy surgery; Before anaesthesia induction WW: Total abdominal hysterectomy; During anaesthesia induction XX: Elective surgery; Before anaesthesia induction YY: Sleeve gastrectomy; Before anaesthesia induction ZZ: Thoracic surgery; Before anaesthesia induction |
A: Bolus + infusion B: Bolus + infusion C: Bolus + infusion D: Bolus E: Bolus F: Bolus + infusion G: Bolus + infusion H: Bolus + infusion I: Bolus + infusion J: Bolus K: Bolus + infusion L: Bolus M: Infusion N: Bolus + infusion O: Bolus + infusion P: Bolus + infusion Q: Bolus + infusion R: Infusion S: Bolus + infusion T: Bolus + infusion U: Bolus + infusion V: Infusion W: Bolus + infusion X: Bolus + infusion Y: Infusion Z: Bolus + infusion AA: Infusion BB: Infusion CC: Bolus + infusion DD: Bolus + infusion EE: Bolus + infusion FF: Infusion GG: Bolus HH: Bolus + infusion II: Infusion JJ: Infusion KK: Bolus + infusion LL: Bolus + infusion MM: Infusion NN: Bolus + infusion OO: Bolus + infusion PP: Infusion QQ: Bolus + infusion RR: Bolus + infusion SS: Infusion TT: Bolus + infusion UU: Bolus + infusion VV: Infusion WW: Infusion XX: Infusion YY: Bolus + infusion ZZ: Infusion |
A: 200 mg/h B: 8 mg/kg/h C: 10 mg/kg/h D: n.a. E: n.a. F: 6 mg/kg/h G: 15 mg/kg/h H: 8 mg/kg/h I: 10 mg/kg/h, 20 mg/kg/h J: n.a. K: 8 mg/kg/h L: n.a. M: 50 mg/kg/h N: 500 mg/h O: 15 mg/kg/h P: 10 mg/kg/h Q: 500 mg/h R: 8 mg/kg/h S: 15 mg/kg/h T: 10 mg/kg/h U: 25 mg/kg/h V: 80 mg/kg/h, 2 g/h W: 15 mg/kg/h X: 10 mg/kg/h Y: 50 mg/kg/h Z: 10 mg/kg/h AA: 8 mg/kg/h BB: 5 mg/kg/h CC: 10 mg/kg/h DD: 15 mg/kg/h EE: 2 mg/kg/h FF: 65 mg/kg/h GG: n.a. HH: 10 mg/kg/h II: 50 mg/kg/h JJ: 50 mg/kg/h KK: 8 mg/kg/h LL: 20 mg/kg/h MM: 50 mg/kg/h NN: 15 mg/kg/h OO: 10 mg/kg/h PP: 150 mg/h QQ: 15 mg/kg/h RR: 2 mg/kg/h SS: 50 mg/kg/h TT: 10 mg/kg/h UU: 15 mg/kg/h VV: 30 mg/kg/h WW: 15 mg/kg/h XX: 30 mg/kg/h YY: 20 mg/kg/h ZZ: 50 mg/kg/h |
A: n.s. B: n.s. C: n.s. D: n.s. E: n.s. F: n.s. G: n.s. H: n.s. I: n.s. J: n.s. K: n.s. L: n.s. M: n.s. N: n.s. O: n.s. P: n.s. Q: n.s. R: n.s. S: n.s. T: n.s. U: n.s. V: n.s. W: n.s. X: n.s. Y: n.s. Z: n.s. AA: n.s. BB: n.s. CC: n.s. DD: n.s. EE: n.s. FF: n.s. GG: n.s. HH: n.s. II: n.s. JJ: n.s. KK: n.s. LL: n.s. MM: n.s. NN: n.s. OO: n.s. PP: n.s. QQ: n.s. RR: n.s. SS: n.s. TT: n.s. UU: n.s. VV: n.s. WW: n.s. XX: n.s. YY: n.s. ZZ: n.s. |
A: PCA morphine B: IV fentanyl C: PCA morphine NSAIDs IV paracetamol IV metamizole D: IV metamizol IV nalbuphine E: IV metamizol IV nalbuphine F: IV fentanyl G: IV morphine H: IV alfentanil I: PCA morphine J: PCA tramadol PCA droperidol K: IV meperidine L: Oral/rectal NSAID IV/IM opioid M: PCA tramadol N: PCA morphine O: PCA mixture, ketorolac and morphine P: PCA morphine Q: PCA morphine R: IV morphine S: PCA mixture, ketorolac and morphine T: PCA morphine U: PCA morphine. The actual dose was not provided V: IV pethidine W: IV lidocaine PCA fentanyl X: Tab Ultracet IM tramadol Y: IV pethidine IM diclofenac Z: PCA morphine AA: IV meperidine BB: IV metamizol IV diclofenac IV tramadol CC: IV morphine DD: IV hydromorphone EE: IV meperidine FF: IV tramadol GG: PCA morphine HH: IV paracetamol IV ketorolac PCA morphine II: IV pethidine JJ: IV ketorolac IV tramadol KK: IV pethidine LL: IV tramadol MM: IM diclofenac PCA tramadol NN: PCA fentanyl OO: IV fentanyl PP: IV morphine QQ: PCA fentanyl IV ketoprofen RR: PCA morphine SS: IV tramadol TT: IV pethidine UU: IV morphine IV fentanyl IV NSAIDs" VV: IV pethidine WW: IV fentanyl XX: IV propofol YY: PCA morphine IV fentanyl" ZZ: PCA morphine |
A: n.s. B: n.s. C: n.s. D: n.s. E: n.s. F: n.s. G: n.s. H: n.s. I: n.s. J: n.s. K: n.s. L: n.s. M: n.s. N: n.s. O: n.s. P: n.s. Q: n.s. R: n.s. S: n.s. T: n.s. U: n.s. V: n.s. W: n.s. X: n.s. Y: n.s. Z: n.s. AA: n.s. BB: n.s. CC: n.s. DD: n.s. EE: n.s. FF: n.s. GG: n.s. HH: n.s. II: n.s. JJ: n.s. KK: n.s. LL: n.s. MM: n.s. NN: n.s. OO: n.s. PP: n.s. QQ: n.s. RR: n.s. SS: n.s. TT: n.s. UU: n.s. VV: n.s. WW: n.s. XX: n.s. YY: n.s. ZZ: n.s. |
|
|
Postoperative pain 24h
|
Postoperative morphine consumption – 24h |
Adverse events: bradycardia |
||||||||||||||||
|
Study reference |
Studies |
Intervention |
Control |
Intervention |
Control |
Intervention |
Control |
||||||||||||
|
|
|
Mean |
SD |
N |
Mean |
SD |
N |
Mean |
SD |
N |
Mean |
SD |
N |
Events |
Total |
|
Events |
Total |
|
|
Ng, 2020 |
A: Wilder-Smith, 1997 |
|
|
|
|
|
|
41.8 |
9.6 |
13 |
46.8 |
14.1 |
11 |
|
|
|
|
|
|
|
B: Koinig, 1998 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C: Zarauza, 2000 |
2.0 |
1.5 |
23 |
1.0 |
1.0 |
24 |
39.8 |
9.2 |
23 |
46.6 |
11.3 |
24 |
0 |
23 |
|
0 |
24 |
|
|
|
D: Schulz-Stübner, 2001 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E: Levaux, 2003 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F: Mavrommati, 2004 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G: Bhatia, 2004 |
3.34 |
3.93 |
25 |
3.85 |
3.14 |
25 |
13.7 |
2.97 |
25 |
15.1 |
2.71 |
25 |
|
|
|
|
|
|
|
|
H: Ayoglu, 2005 |
1.3 |
0.3 |
20 |
0.5 |
0.3 |
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I: Seyhan, 2006 |
|
|
|
|
|
|
54.8 |
12.8 |
20 |
64.0 |
10.2 |
20 |
0 |
60 |
|
0 |
20 |
|
|
|
J: Tauzin-Fin, 2006 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
K: Cizmeci, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L: Tramer, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M: Mentes, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N: Benhaj Amor, 2008 |
|
|
|
|
|
|
34.0 |
4.0 |
24 |
52.0 |
4.0 |
24 |
|
|
|
|
|
|
|
|
O: Ryu, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P: Oguzhan, 2008 |
|
|
|
|
|
|
12.0 |
6.06 |
25 |
23.0 |
10.9 |
25 |
|
|
|
|
|
|
|
|
Q: Kaya, 2009 |
|
|
|
|
|
|
30.2 |
10.2 |
20 |
36.7 |
7.3 |
20 |
4 |
20 |
|
0 |
20 |
|
|
|
R: Dabbagh, 2009 |
3.4 |
0.6 |
30 |
3.5 |
0.8 |
30 |
4.2 |
1.6 |
30 |
9.8 |
2.1 |
30 |
|
|
|
|
|
|
|
|
S: Hwang, 2010 |
2.0 |
1.56 |
20 |
3.83 |
1.04 |
20 |
|
|
|
|
|
|
2 |
20 |
|
1 |
20 |
|
|
|
T: Jaouda, 2010 |
|
|
|
|
|
|
45.3 |
9.1 |
21 |
44.5 |
6.4 |
21 |
|
|
|
|
|
|
|
|
U: Saadawy, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V: Gozdemir, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
0 |
30 |
|
3 |
30 |
|
|
|
W: Koinig, 2011 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
X: Song, 2011 |
3.0 |
1.56 |
28 |
2.84 |
2.94 |
56 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y: Kiran, 2011 |
0.78 |
0.68 |
50 |
1.3 |
0.46 |
50 |
|
|
|
|
|
|
0 |
50 |
|
0 |
50 |
|
|
|
Z: Olgun, 2012 |
1.0 |
2.1 |
30 |
1.4 |
1.0 |
30 |
12.0 |
6.06 |
25 |
23.0 |
10.9 |
25 |
|
|
|
|
|
|
|
|
AA: Khafagy, 2012 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BB: Kocman, 2013 |
1.6 |
1.5 |
20 |
1.3 |
1.6 |
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CC: Kumar, 2013 |
|
|
|
|
|
|
3.99 |
1.25 |
30 |
7.13 |
2.68 |
30 |
|
|
|
|
|
|
|
|
DD: de Oliveira, 2013 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EE: Ibrahim, 2014 |
|
|
|
|
|
|
|
|
|
|
|
|
0 |
40 |
|
2 |
40 |
|
|
|
FF: Kahraman, 2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GG: Mireskandari, 2015 |
2.26 |
0.45 |
25 |
2.36 |
0.49 |
25 |
4.36 |
1.4 |
25 |
7.2 |
1.9 |
25 |
|
|
|
|
|
|
|
|
HH: Frassanito, 2015 |
|
|
|
|
|
|
13.9 |
5.9 |
20 |
14.4 |
10.7 |
20 |
|
|
|
|
|
|
|
|
II: Taheri, 2015 |
4.6 |
0.94 |
20 |
5.9 |
0.45 |
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
JJ: Kim, 2015 |
1.5 |
1.0 |
28 |
2.5 |
1.76 |
29 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
KK: Asadollah, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LL: Shah, 2016 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM: Demiroglu, 2016 |
4.17 |
1.51 |
25 |
3.17 |
0.69 |
25 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NN: Ryu, 2016 |
4.0 |
6.17 |
37 |
5.3 |
6.94 |
37 |
|
|
|
|
|
|
0 |
37 |
|
0 |
37 |
|
|
|
OO: Vickovic, 2016 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PP: Muthiah, 2016 |
|
|
|
|
|
|
8.015 |
3.884 |
40 |
10.58 |
4.51 |
20 |
|
|
|
|
|
|
|
|
QQ: Shin, 2016 |
1.9 |
0.9 |
22 |
2.9 |
1.1 |
22 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RR: Sousa, 2016 |
|
|
|
|
|
|
5.7 |
6.2 |
18 |
12.0 |
6.3 |
18 |
|
|
|
|
|
|
|
|
SS: Gucyetmez, 2016 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TT: Shal, 2017 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UU: Sohn, 2017 |
3.5 |
1.1 |
29 |
3.8 |
1.6 |
33 |
35.1 |
20.0 |
29 |
44.7 |
16.6 |
33 |
|
|
|
|
|
|
|
|
VV: Elsersy, 2017 |
4.5 |
3.08 |
146 |
6.0 |
4.66 |
148 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WW: Haryalchi, 2017 |
5.95 |
0.94 |
20 |
5.9 |
0.45 |
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
XX: Walia, 2018 |
|
|
|
|
|
|
|
|
|
|
|
|
1 |
40 |
|
0 |
40 |
|
|
|
YY: Kizilcik, 2018 |
|
|
|
|
|
|
21.13 |
4.33 |
40 |
26.5 |
5.77 |
40 |
|
|
|
|
|
|
|
|
ZZ: Ahmed, 2018 |
|
|
|
|
|
|
40.87 |
4.4 |
30 |
42.2 |
6.1 |
30 |
|
|
|
|
|
|
|
Evidence table for intervention studies (additional randomized controlled trials)
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Abdelgalil A, Shoukry AA, Kamel MA, Heikal AMY, Ahmed NA. Analgesic Potentials of Preoperative Oral Pregabalin, Intravenous Magnesium Sulfate, and their Combination in Acute Postthoracotomy Pain. Clin J Pain. 2019 Mar;35(3):247-251. doi: 10.1097/AJP.0000000000000673. PMID: 30730476. |
Wrong population |
|
Adhikary SD, Thiruvenkatarajan V, McFadden A, Liu WM, Mets B, Rogers A. Analgesic efficacy of ketamine and magnesium after laparoscopic sleeve gastrectomy: A randomized, double-blind, placebo-controlled trial. J Clin Anesth. 2021 Feb;68:110097. doi: 10.1016/j.jclinane.2020.110097. Epub 2020 Oct 23. PMID: 33120301. |
Wrong intervention |
|
Bansal, K., Santpur, M. U., Garg, U., Goel, K., Vijay, D., & Venugopal, T. Effect of intravenous magnesium sulphate on hemodynamic response to pneumoperitoneum in laparoscopic cholecystectomy: A prospective, double blind study. Anaesthesia, Pain & Intensive Care. 2021; 290-294. |
Wrong outcomes |
|
Choi GJ, Kim YI, Koo YH, Oh HC, Kang H. Perioperative Magnesium for Postoperative Analgesia: An Umbrella Review of Systematic Reviews and Updated Meta-Analysis of Randomized Controlled Trials. J Pers Med. 2021 Dec 2;11(12):1273. doi: 10.3390/jpm11121273. PMID: 34945745; PMCID: PMC8708823. |
Wrong publication type |
|
Deshpande JP, Patil KN. Evaluation of magnesium as an adjuvant to ropivacaine-induced axillary brachial plexus block: A prospective, randomised, double-blind study. Indian J Anaesth. 2020 Apr;64(4):310-315. doi: 10.4103/ija.IJA_833_19. Epub 2020 Mar 28. PMID: 32489206; PMCID: PMC7259414. |
Wrong intervention |
|
Fei S, Xia H, Chen X, Pang D, Xu X. Magnesium sulfate reduces the rocuronium dose needed for satisfactory double lumen tube placement conditions in patients with myasthenia gravis. BMC Anesthesiol. 2019 Aug 31;19(1):170. doi: 10.1186/s12871-019-0841-4. PMID: 31472669; PMCID: PMC6717642. |
Wrong outcomes |
|
Gol M, Aghamohammadi D. Effect of intravenous infusion of magnesium sulfate on opioid use and hemodynamic status after hysterectomy: double-blind clinical trial. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2019;22(7):32-8. |
Wrong language |
|
Hassan WF, Tawfik MH, Nabil TM, Abd Elkareem RM. Could intraoperative magnesium sulphate protect against postoperative cognitive dysfunction? Minerva Anestesiol. 2020 Aug;86(8):808-815. doi: 10.23736/S0375-9393.20.14012-4. Epub 2020 May 22. PMID: 32449335. |
Wrong outcomes |
|
Hassan ME, Mahran E. Effect of magnesium sulfate with ketamine infusions on intraoperative and postoperative analgesia in cancer breast surgeries: a randomized double-blind trial. Braz J Anesthesiol. 2021 Jul 29:S0104-0014(21)00296-7. doi: 10.1016/j.bjane.2021.07.015. Epub ahead of print. PMID: 34332956. |
Wrong comparison |
|
Jitsinthunun T, Raksakietisak M, Pantubtim C, Mahatnirunkul P. Effects of Magnesium Sulfate on Intraoperative Blood Loss and Anesthetic Requirement in Meningioma Patients Undergoing Craniotomy with Tumor Removal: A Prospective Randomized Study. Journal of Neuroanaesthesiology and Critical Care. 2022 Jul 20. |
Wrong outcomes |
|
Kamel AA, Ibrahem Amin OA. The Effect of preoperative nebulized: Magnesium sulfate versus lidocaine on the prevention of post-intubation sore throat. Egyptian Journal of Anaesthesia. 2020 Jan 1;36(1):1-6. |
Wrong intervention |
|
Kosucu M, Tugcugil E, Arslan E, Omur S, Livaoglu M. Effects of perioperative magnesium sulfate with controlled hypotension on intraoperative bleeding and postoperative ecchymosis and edema in open rhinoplasty. Am J Otolaryngol. 2020 Nov-Dec;41(6):102722. doi: 10.1016/j.amjoto.2020.102722. Epub 2020 Sep 14. PMID: 32950829. |
Wrong outcomes |
|
Mashak B, Pouryaghobi SM, Rezaee M, Rad SS, Ataei M, Borzabadi A. Evaluation of the Effects of Magnesium Sulfate on Prevention of Post-dural-Puncture Headache in Elective Cesarean in Kamali Hospital. ELECTRON J GEN MED. 2020;17(3), em199. |
Wrong outcomes |
|
Masoudifar, M., Mostashfi, M., Hirmanpour, A. Comparative Study of the Effect of Prophylactic Administration of Two Doses of Magnesium Sulfate and Placebo on Cardiovascular Changes during General Anesthesia in Gynecologic Laparoscopic Surgeries. Journal of Isfahan Medical School, 2019; 37(528): 572-579. doi: 10.22122/jims.v37i528.11214 |
Wrong language |
|
Mendonça FT, Pellizzaro D, Grossi BJ, Calvano LA, de Carvalho LSF, Sposito AC. Synergistic effect of the association between lidocaine and magnesium sulfate on peri-operative pain after mastectomy: A randomised, double-blind trial. Eur J Anaesthesiol. 2020 Mar;37(3):224-234. doi: 10.1097/EJA.0000000000001153. PMID: 31977625. |
Wrong comparator |
|
Modir H, Modir A, Rezaei O, Mohammadbeigi A. Comparing remifentanil, magnesium sulfate, and dexmedetomidine for intraoperative hypotension and bleeding and postoperative recovery in endoscopic sinus surgery and tympanomastoidectomy. Med Gas Res. 2018 Jul 3;8(2):42-47. doi: 10.4103/2045-9912.235124. PMID: 30112164; PMCID: PMC6070837. |
Wrong intervention |
|
Sabaa M A, Elbadry A A, Hegazy S, El Malla D A. Intravenous Versus Wetting Solution Magnesium Sulphate to Counteract Epinephrine Cardiac Adverse Events in Abdominal Liposuction: A Randomized Controlled Trial. Anesth Pain Med. 2022;12(5):e129807. https://doi.org/10.5812/aapm-129807. |
Wrong intervention |
|
Saeed R, Sarwar M, Javed A, Qamar I, Bangash T, Kakepotto IA. Atracurium With and Without Administrating Magnesium Sulphate in Patients Undergoing Abdominal Surgeries. |
Wrong outcomes |
|
Sane S, Mahdkhah A, Golabi P, Hesami SA, Kazemi Haki B. Comparison the effect of bupivacaine plus magnesium sulfate with ropivacaine plus magnesium sulfate infiltration on postoperative pain in patients undergoing lumbar laminectomy with general anesthesia. Br J Neurosurg. 2020 Dec 17:1-4. doi: 10.1080/02688697.2020.1861430. Epub ahead of print. PMID: 33332200. |
Wrong comparison |
|
Sharma A, Jaswal S, Jaswal V, Pathania J. Effect of Magnesium Sulphate as an Adjuvant to Bupivacaine in Interscalene Brachial Plexus Block for Postoperative Analgesia. Journal of Clinical & Diagnostic Research. 2019 Oct 1;13(10). |
Wrong intervention |
|
Shim JW, Cha S, Moon HW, Moon YE. Effects of Intraoperative Magnesium and Ketorolac on Catheter-Related Bladder Discomfort after Transurethral Bladder Tumor Resection: A Prospective Randomized Study. J Clin Med. 2022 Oct 27;11(21):6359. doi: 10.3390/jcm11216359. PMID: 36362587; PMCID: PMC9659173. |
Wrong outcomes |
|
Shukla U, Singh D, Yadav JBS, Azad MS. Dexmedetomidine and Magnesium Sulfate as Adjuvant to 0.5% Ropivacaine in Supraclavicular Brachial Plexus Block: A Comparative Evaluation. Anesth Essays Res. 2020 Oct-Dec;14(4):572-577. doi: 10.4103/aer.AER_28_21. Epub 2021 May 27. PMID: 34349322; PMCID: PMC8294421. |
Wrong intervention |
|
Silva Filho SE, Sandes CS, Vieira JE, Cavalcanti IL. Analgesic effect of magnesium sulfate during total intravenous anesthesia: randomized clinical study. Braz J Anesthesiol. 2021 Sep-Oct;71(5):550-557. doi: 10.1016/j.bjane.2021.02.008. Epub 2021 Feb 3. PMID: 34537125; PMCID: PMC9373246. |
Wrong comparator |
|
Silva Filho SE, Dainez S, Gonzalez MAMC, Angelis F, Vieira JE, Sandes CS. Intraoperative Analgesia with Magnesium Sulfate versus Remifentanil Guided by Plethysmographic Stress Index in Post-Bariatric Dermolipectomy: A Randomized Study. Anesthesiol Res Pract. 2022 Oct 26;2022:2642488. doi: 10.1155/2022/2642488. PMID: 36339775; PMCID: PMC9629917. |
Wrong comparator |
|
Sohair A. Megalla, Khaled A. Abdou & Ahmed I. Mohamed (2019) Bispectral index guided attenuation of hemodynamic and arousal response to endotracheal intubation using magnesium sulfate and fentanyl. Randomized, controlled trial, Egyptian Journal of Anaesthesia, 35:1, 43-48, DOI: 10.1080/11101849.2019.1595346 |
Wrong outcomes |
|
Soliman R, Abukhudair W. The perioperative effect of magnesium sulfate in patients with concentric left ventricular hypertrophy undergoing cardiac surgery: A double-blinded randomized study. Ann Card Anaesth. 2019 Jul-Sep;22(3):246-253. doi: 10.4103/aca.ACA_34_18. PMID: 31274484; PMCID: PMC6639894. |
Wrong outcomes |
|
Queiroz Rangel Micuci AJ, Verçosa N, Filho PAG, de Boer HD, Barbosa DD, Cavalcanti IL. Effect of pretreatment with magnesium sulphate on the duration of intense and deep neuromuscular blockade with rocuronium: A randomised controlled trial. Eur J Anaesthesiol. 2019 Jul;36(7):502-508. doi: 10.1097/EJA.0000000000001003. PMID: 30985540. |
Wrong outcomes |
|
Tan W, Qian DC, Zheng MM, Lu X, Han Y, Qi DY. Effects of different doses of magnesium sulfate on pneumoperitoneum-related hemodynamic changes in patients undergoing gastrointestinal laparoscopy: a randomized, double-blind, controlled trial. BMC Anesthesiol. 2019 Dec 20;19(1):237. doi: 10.1186/s12871-019-0886-4. PMID: 31862004; PMCID: PMC6925413. |
Wrong outcomes |
|
Varas V, Bertinelli P, Carrasco P, Souper N, Álvarez P, Danilla S, Egaña JI, Penna A, Sepúlveda S, Arancibia V, Álvarez MG, Vergara R. Intraoperative Ketamine and Magnesium Therapy to Control Postoperative Pain After Abdominoplasty and/or Liposuction: A Clinical Randomized Trial. J Pain Res. 2020 Nov 16;13:2937-2946. doi: 10.2147/JPR.S276710. PMID: 33235492; PMCID: PMC7678693. |
Wrong comparison |
Verantwoording
Beoordelingsdatum en geldigheid
Publicatiedatum : 26-09-2023
Beoordeeld op geldigheid : 01-09-2023
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS).
De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met postoperatieve pijn.
Samenstelling van de werkgroep
Werkgroep
Prof. dr. J. (Jörgen) Bruhn, anesthesioloog, (voorzitter) NVA
Prof. dr. dr. M.W. (Markus) Hollmann, anesthesioloog, NVA
Dr. M.F. (Markus) Stevens, anesthesioloog, NVA
Drs. L.J.H. (Lea) van Wersch, anesthesioloog, NVA
Dr. M.H.J. (Margot) Roozekrans, anesthesioloog, NVA
Dr. S.A.S. (Sandra) van den Heuvel, anesthesioloog/pijnspecialist, NVA
Drs. S.J. (Stijn) Westerbos, orthopeed, NOV
Drs. W.L. (Wilson) Li, cardiothoracaal chirurg, NVT
S.F. (Cedric) Lau MSc, ziekenhuisapotheker, NVZA
Dr. R.L.M. (Rianne) van Boekel, verpleegkundig pijnconsulent, V&VN
Drs. I.L. (Ilona) Thomassen-Hilgersom, patiëntvertegenwoordiger, Samenwerkingverband Pijnpatiënten naar één stem
Klankbordgroep
Drs. N.C. (Niels) Gritters van den Oever, intensivist, NVIC
J.P. (Patrick) Rensink, anesthesiemedewerker/pijnconsulent, NVAM
Dr. G. (Gijs) Helmerhorst, orthopeed, NOV
Dr. C.D. (Cor) de Kroon, gynaecoloog-oncoloog, NVOG
Dr. W.J. (Wietse) Eshuis, chirurg, NVvH
Dr. D. (Daphne) Roos, chirurg, NVvH
Met ondersteuning van
Dr. F. Willeboordse, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Dr. L.M.P. Wesselman, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Dr. L.M. van Leeuwen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
I. van Dijk, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Bruhn, voorzitter |
Professor & Afdelingshoofd afdeling Anesthesiologie, Radboud UMC |
Editorial Board Journal of Clinical Monitoring and Computing, onbetaald |
Geen |
Geen actie |
|
Hollmann |
Professor & Afdelingshoofd afdeling Anesthesiologie, Amsterdam UMC, locatie AMC |
|
Geen |
Restricties t.a.v. modules over ketamine en lidocaïne. |
|
Lau |
|
Nationale Werkgroep morbide obesitas en bariatrische chirurgie (KNMP), vergoeding voor bestede uren |
Geen belangenverstrengeling, promotie-onderzoek is op een ander vlak dan waar beoogde werkgroep zich over buigt
|
Geen actie |
|
Boekel, van |
|
|
Geen |
Geen actie |
|
Thomassen-Hilgersom |
Voorzitter Samenwerkingsverband Pijnpatiënten naar één stem vrijwilliger en geen werkgever |
|
Geen |
Geen actie |
|
Li |
Cardiothoracaal chirurg (Radboudumc, Nijmegen) |
Bestuurslid NVT (Nederlandse Vereniging voor Thoraxchirurgie) |
Radboudumc zal in 2021 meedoen aan een RCT naar de optimale vorm van pijnstilling ten tijde van longchirugie (epiduraal versus paravertebraal) OPtriAL - met ZonMw subsidie, geïniteerd vanuit het MMC |
Geen actie |
|
Roozekrans |
Anesthesioloog - Pijnspecialist - Noordwest Ziekenhuisgroep |
Geen |
Geen |
Geen actie |
|
Stevens |
Chef de Clinique kinderanesthesie AUMC locatie AMC |
|
Geen |
Geen actie |
|
Heuvel, van den |
Anesthesioloog-pijnarts, Radboud UMC |
Geen |
Geen |
Geen actie |
|
Wersch, van |
Anesthesioloog, Maasziekenhuis Pantein |
Geen |
Geen |
Geen actie |
|
Westerbos |
Orthopeed, Alrijne ziekenhuis |
Geen |
Geen |
Geen actie |
|
Gritters van den Oever |
Anesthesioloog-intensivist Treant Zorggroep |
|
Geen |
Geen actie |
|
Rensink |
|
|
Geen |
Geen actie |
|
Kroon, de |
Gynaecoloog-oncoloog Leids Univesitair Medisch Centrum (1.0 fte) |
|
Geen |
Geen actie |
|
Roos |
Chirurg |
Geen |
Geen |
Geen actie |
|
Eshuis |
Chirurg, Amsterdam UMC |
Geen |
Geen |
Geen actie |
|
Willeboordse |
Senior adviseur Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Partner werkzaam bij Janssen Vaccines, onderdeel van Johnsson &Johnsson, via partner ook financiële belangen (aandelen J&J) |
Geen actie |
|
Wesselman |
Adviseur Kennisinstituut van de Federatie Medisch Specialisten |
|
|
Geen actie |
|
Leeuwen, van |
Adviseur Kennisinstituut van de Federatie Medisch Specialisten |
|
|
Geen actie |
|
Dijk, van |
Junior adviseur Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Geen |
Geen actie |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door zitting van een afgevaardigde van de patiëntenvereniging (Pijnpatiënten naar één stem) in de werkgroep. De Patiëntenfederatie Nederland en Pijnpatiënten naar één stem werden uitgenodigd voor de invitational conference. Het verslag hiervan [zie aanverwante producten] is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en Pijnpatiënten naar één stem en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Wkkgz & Kwalitatieve raming van mogelijke substantiële financiële gevolgen
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijn is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling zijn richtlijnmodules op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
|
Module |
Uitkomst raming |
Toelichting |
|
Module Organisatie van Zorg |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Transitionele Pijn Service (TPS) |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten). Hoewel de aanbeveling aangeeft dat een andere of nieuwe manier van zorgverlening gewenst is (i.e. andere manier van samenwerking/afstemming tussen zorgverleners) waarbij een TPS-model met TPS-team geïnitieerd wordt, laten eerste kosten-effectiviteitsstudies kostenbesparingen zien. De verwachting is dat TPS leidt tot betere zorg-op-maat, waarbij chronische postoperatieve pijn zorg doelmatiger wordt behandeld. Per ziekenhuis zal de vorm, intensiteit en organisatie van het TPS-model variëren. Zo kunnen ziekenhuizen ook kiezen voor een minder uitgebreid TPS. De aanbeveling geeft relatief veel ruimte voor de precieze invulling. Alle overwegingen tezamen, worden er geen substantiële financiële gevolgen verwacht. |
|
Module Pijnmeting |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Niet-medicamenteuze interventies |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Buikwandblokken |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Borstwandblokken bij mammachirurgie |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Borstwandblokken intrathoracaal |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Continue Wond infusie |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Cryoanalgesie |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5.000 patiënten) en zal daarom naar verwachting geen substantiële financiële gevolgen hebben voor de collectieve uitgaven. |
|
Module Dexmethason |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Gabapentinoïden |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Ketamine |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Magnesium |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Methadon |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Beta blokkers -Esmolol |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Alpha 2 agonist - Clonidine |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Alpha 2 agonist – Dexmedetomidine |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Lidocaïne |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Multimodale pijnbestrijding |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet en/of het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met postoperatieve pijn.
De werkgroep beoordeelde de aanbevelingen uit de eerdere richtlijn Postoperatieve pijn (NVA, 2013) op noodzaak tot revisie. Tevens zijn er knelpunten aangedragen door relevante partijen middels een invitational conference.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
De beoordelingen van de literatuur en de conclusies zijn gedaan op basis van de GRADE systematiek. De werkgroep vindt het belangrijk om relevante beperkingen hiervan aan te geven.
De klinische vraag gaat vaak over een reductie van ernstige postoperatieve pijn en opioïdenconsumptie in een aantal patiënten met resp. over een klinisch relevante reductie van ernstige postoperatieve pijn opioïdenconsumptie bij een individuele patiënt. Hetzelfde geldt voor opioïdenconsumptie; de keuze van een absolute drempelwaarde in mg (i.p.v. een relatieve drempelwaarde in %) maakt dit afhankelijk van tijdstip, ingreep en ernst van de pijn: vroege postoperatieve tijdstippen en (studies met) ingrepen met relatief lage opioïdconsumptie kunnen vaak de MCID niet bereiken.
De keuze van de MCID heeft een bepaalde mate van willekeurigheid en is niet absoluut te zien. Ook zijn de conclusies zo geformuleerd (en geven alleen beperkt antwoord op het effect op een individuele patiënt voor een specifieke ingreep).
In de literatuur worden de eindpunten pijnscores en opioïdenconsumptie separaat van elkaar weer gegeven, suggererend dat deze onafhankelijk van elkaar zijn. Echter kunnen deze twee eindpunten niet onafhankelijk van elkaar beoordeeld worden; in ieder protocol is opgenomen dat pijn behandeld moet worden. Deze separate beoordeling geeft niet altijd een adequaat antwoord op de klinische vraag naar het analgetische effect van een interventie.
Daarnaast worden multimodale componenten als aparte interventies beoordeeld, echter de klinische vraag is naar de effectiviteit als bouwsteen van een multimodale werkwijze.
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Zoekverantwoording
Embase 8-12-2022
|
No. |
Query |
Results |
|
#6 |
#4 AND #6 |
435 |
|
#5 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
1991134 |
|
#4 |
#3 AND [1-1-2019]/sd NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
2980 |
|
#3 |
#1 AND #2 |
14904 |
|
#2 |
'magnesium'/exp OR (mg:ti,ab,kw AND magnesium:ti,ab,kw) OR 'magnesium':ti,ab,kw OR 'magnesium sulfate'/exp OR ((magnesium NEAR/3 sulphate):ti,ab,kw) OR ((magnesium NEAR/3 sulfate):ti,ab,kw) OR romag:ti,ab,kw |
151160 |
|
#1 |
'surgery'/exp OR 'surger*':ti,ab,kw OR 'operation':ti,ab,kw OR 'operation care':ti,ab,kw OR 'operative intervention':ti,ab,kw OR 'operative repair':ti,ab,kw OR 'operative restoration':ti,ab,kw OR 'operative surgery':ti,ab,kw OR intraoperative:ti,ab,kw OR 'postoperative':ti,ab,kw OR 'operative surgical procedure':ti,ab,kw OR 'operative surgical procedures':ti,ab,kw OR 'operative treatment':ti,ab,kw OR 'research surgery':ti,ab,kw OR 'resection':ti,ab,kw OR 'surgery':ti,ab,kw OR 'surgical care':ti,ab,kw OR 'surgical correction':ti,ab,kw OR 'surgical diagnosis':ti,ab,kw OR 'surgical diagnostic techniques':ti,ab,kw OR 'surgical exposure':ti,ab,kw OR 'surgical intervention':ti,ab,kw OR 'surgical operation':ti,ab,kw OR 'surgical practice':ti,ab,kw OR 'surgical repair':ti,ab,kw OR 'surgical research':ti,ab,kw OR 'surgical restoration':ti,ab,kw OR 'surgical service':ti,ab,kw OR 'surgical speciality':ti,ab,kw OR 'surgical specialties':ti,ab,kw OR 'surgical specialty':ti,ab,kw OR 'surgical therapy':ti,ab,kw OR 'surgical treatment':ti,ab,kw OR 'surgical management':ti,ab,kw |
6660512 |
Embase 13-7-2022
|
No. |
Query |
Results |
|
#8 |
#4 AND #6 |
152 |
|
#7 |
#4 AND #5 |
71 |
|
#6 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
1932521 |
|
#5 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
839911 |
|
#4 |
#3 AND [1-1-2021]/sd NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
661 |
|
#3 |
#1 AND #2 |
6308 |
|
#2 |
'magnesium'/exp OR (mg:ti,ab,kw AND magnesium:ti,ab,kw) OR 'magnesium':ti,ab,kw OR 'magnesium sulfate'/exp OR ((magnesium NEAR/3 sulphate):ti,ab,kw) OR ((magnesium NEAR/3 sulfate):ti,ab,kw) OR romag:ti,ab,kw |
148161 |
|
#1 |
'surgery'/mj OR 'surger*':ti,ab,kw OR 'operation':ti,ab,kw OR 'operation care':ti,ab,kw OR 'operative intervention':ti,ab,kw OR 'operative repair':ti,ab,kw OR 'operative restoration':ti,ab,kw OR 'operative surgery':ti,ab,kw OR intraoperative:ti,ab,kw OR 'postoperative':ti,ab,kw OR 'operative surgical procedure':ti,ab,kw OR 'operative surgical procedures':ti,ab,kw OR 'operative treatment':ti,ab,kw OR 'research surgery':ti,ab,kw OR 'resection':ti,ab,kw OR 'surgery':ti,ab,kw OR 'surgical care':ti,ab,kw OR 'surgical correction':ti,ab,kw OR 'surgical diagnosis':ti,ab,kw OR 'surgical diagnostic techniques':ti,ab,kw OR 'surgical exposure':ti,ab,kw OR 'surgical intervention':ti,ab,kw OR 'surgical operation':ti,ab,kw OR 'surgical practice':ti,ab,kw OR 'surgical repair':ti,ab,kw OR 'surgical research':ti,ab,kw OR 'surgical restoration':ti,ab,kw OR 'surgical service':ti,ab,kw OR 'surgical speciality':ti,ab,kw OR 'surgical specialties':ti,ab,kw OR 'surgical specialty':ti,ab,kw OR 'surgical therapy':ti,ab,kw OR 'surgical treatment':ti,ab,kw OR 'surgical management':ti,ab,kw |
3160476 |
Ovid/Medline 9-12-2022
|
# |
Searches |
Results |
|
7 |
5 and 6 |
197 |
|
6 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2527144 |
|
5 |
4 not ((exp animals/ or exp models, animal/) not humans/) not (letter/ or comment/ or editorial/) |
723 |
|
4 |
limit 3 to yr="2019 -Current" |
839 |
|
3 |
1 and 2 |
5723 |
|
2 |
exp Magnesium/ or exp Magnesium Sulfate/ or ('mg' and magnesium).ti,ab,kf. or magnesium.ti,kw,kf. or 'romag'.ti,ab,kf. or (magnesium adj4 (sulfate or sulphate)).ti,ab,kf. |
90993 |
|
1 |
exp General Surgery/ or exp Surgical Procedures, Operative/ or (surgical or surger* or operation* or operative).ti,ab,kf. |
4871469 |
Ovid/Medline 13-7-2022
|
# |
Searches |
Results |
|
1 |
exp General Surgery/ or exp Surgical Procedures, Operative/ or (surgical or surger* or operation* or operative).ti,ab,kf. |
4791660 |
|
2 |
exp Magnesium/ or exp Magnesium Sulfate/ or ('mg' and magnesium).ti,ab,kf. or magnesium.ti,kw,kf. or 'romag'.ti,ab,kf. or (magnesium adj4 (sulfate or sulphate)).ti,ab,kf. |
90039 |
|
3 |
1 and 2 |
5630 |
|
4 |
limit 3 to yr="2021 -Current" |
364 |
|
5 |
4 not ((exp animals/ or exp models, animal/) not humans/) not (letter/ or comment/ or editorial/) |
316 |
|
6 |
(meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf.) not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) |
576752 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2475030 |
|
8 |
5 and 6 |
24 |
|
9 |
5 and 7 |
74 |