Meetinstrumenten interferentie van chronische pijn
Uitgangsvraag
Welke meetinstrumenten kunnen het beste gebruikt worden voor de beoordeling van interferentie op het dagelijks functioneren van chronische pijn bij pre verbale kinderen/ neonaten, verbale kinderen, adolescenten en kinderen met neurobiologische ontwikkelingsstoornissen?
Aanbeveling
Gebruik voor het evalueren van de interferentie van chronische pijn op het dagelijks functioneren van kinderen met chronische pijn een meetinstrument.
Overweeg de PROMIS PPIS (Pediatric Pain Interference Scale) te gebruiken bij verbale kinderen en adolescenten die zelf een vragenlijst kunnen invullen. In voorkomende gevallen kunnen ziektespecifieke vragenlijsten bestaan waarin chronische pijn ook wordt uitgevraagd.
Overweeg de PROMIS PPPIS (Pediatric Proxy Pain Interference Scale) te gebruiken bij non-verbale kinderen en adolescenten en kinderen met neurobiologische ontwikkelingsstoornissen die geen vragenlijst kunnen invullen.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is een systematische literatuur analyse uitgevoerd naar welke meetinstrumenten het beste gebruikt kunnen worden voor de beoordeling van de mate van pijn interferentie. Er werd een systematische review gevonden, die zich focuste op kinderen niet in staat om zelf vragenlijsten in te vullen, maar die ook studies includeerde over verbale kinderen en adolescenten. Daarnaast werden er twee losse studies gevonden in verbale kinderen en adolescenten.
In de systematische review van Smith (2023) werd de validiteit en betrouwbaarheid van de Bath Adolescent Pain Questionnaire for Parents (BAPQ-P), Child Activity Limitations Interview-Parent (CALI-P), Paediatric Pain Profile (PPP), Patient-Reported Outcomes Measurement Instrument System Pediatric Proxy Pain Interference Scale (PROMIS-PPPIS), Modified Brief Pain Inventory (mBPI), Pain Burden Inventory – Caregiver Report (PBI-CR) en Pain Interference Index – Parent (PII-P) onderzocht bij kinderen niet in staat om zelf in vragenlijsten in te vullen.
Voor verbale kinderen en adolescenten wordt op basis van validiteit de PROMIS PPPIS (hoge bewijskracht) en BAPQ-P (gemiddelde bewijskracht) geprefereerd boven de andere vragenlijsten. Op basis van betrouwbaarheid worden de BAPQ-P, CALI-P, PROMIS PPPIS, PBI-CR en PII-P (lage bewijskracht) geprefereerd. Dit resulteert in de voorkeur van de PROMIS PPPIS en eventueel de BAPQ-P op basis van zowel validiteit als betrouwbaarheid.
Algemeen geld dat het de voorkeur geniet om verbale kinderen en adolescenten zelf de vragenlijsten in te laten vullen. De PROMIS PPPIS is een directe vertaling van de zelf report PROMIS PPIS (Patient-Reported Outcomes Measurement Instrument System Pediatric Pain Interference Scale). De PROMIS PPIS heeft voldoende validiteit en daarom wordt deze geprefereerd voor verbale kinderen en adolescenten. De PROMIS PPIS bestaat uit 20 items, de PROMIS PPIS short form uit 13 items terwijl de BAPQ uit 61 items bestaat. De uitgebreidheid van de BAPQ maakt deze minder geschikt als routine meetinstrument.
Voor kinderen niet in staat om zelf vragenlijsten in te vullen, beveelt Smith (2023) de PPP aan, vanwege sterke psychometrische eigenschappen en de enige tool met bewijs van voldoende kwaliteit voor content validiteit en interne consistentie in kinderen die niet in staat zijn om zelf vragenlijsten in te vullen. Ze geven aan dat de PROMIS PPPIS ook gebruikt kan worden, maar het nadeel is dat deze niet is getest in kinderen niet in staat om zelf vragenlijsten in te vullen. Echter blijkt uit deze literatuursamenvatting dat de PROMIS PPPIS wel in een grotere studiepopulatie is onderzocht en betere psychometrische eigenschappen met een betere bewijskracht laat zien dan de PPP. Daarom wordt toch de PROMIS PPPIS geprefereerd.
In Smith (2023) werd benoemd dat kinderen niet in staat om zelf vragenlijsten in te vullen dit vaak niet konden door beperkte taal, wat een gevolg kan zijn van een communicatieve, motorische of cognitieve stoornissen. Daarom kan het gevonden bewijs mogelijk ook geëxtrapoleerd worden naar non-verbale kinderen en kinderen met neurobiologische ontwikkelingsstoornissen (subgroep 1 en 4 uit de PICO).
De twee losse gevonden studies (Kashikar-Zuch (2011) en Hermann (2008)) onderzochten de Functional Disability Inventory (FDI), Pain Experience Questionnaire for Children (PEQ-C) en Pain Experience Questionnaire for Children – parent version (PEQ-P) in verbale kinderen en adolescenten. Er werden geen gegevens gerapporteerd over validiteit, maar er werd een gemiddelde betrouwbaarheid gerapporteerd voor alle drie de meetinstrumenten.
Concluderend kunnen voor verbale kinderen en adolescenten het beste de PROMIS PPIS en eventueel de BAPQ worden gebruikt om pijn interferentie bij chronische pijn te meten. Voor non-verbale kinderen en kinderen met neurobiologische ontwikkelingsstoornissen, kan de PROMIS PPPIS en eventueel PPP worden gebruikt.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Alle kinderen, maakt niet uit van welke leeftijd of neurobiologisch ontwikkelingsniveau, kunnen chronische pijn ervaren. Het is van groot belang dat de interferentie van chronische pijn op het dagelijks functioneren van kinderen met chronische pijn regelmatig wordt geëvalueerd over de tijd om het resultaat van de behandeling vast te stellen.
Kosten (middelenbeslag)
Toepassing van een meetinstrument voor bepalen van interferentie op het dagelijks functioneren van chronische pijn bij kinderen en registratie van de uitkomst kost tijd. In de praktijk blijkt dat meetinstrumenten die snel toegepast kunnen worden een duidelijke voorkeur hebben boven meetinstrumenten die vaak meer tijd in beslag nemen. Een eenduidig advies ten aanzien van de juiste balans tussen tijdsinvestering en opbrengst van toepassing van een meetinstrument voor bepalen van interferentie op het dagelijks functioneren van chronische pijn bij kinderen is in deze richtlijn niet te formuleren maar moet wel punt van aandacht zijn in de dagelijkse praktijk.
Aanvaardbaarheid, haalbaarheid en implementatie
Er wordt in de huidige praktijk nog weinig gebruik gemaakt van de interferentie van chronische pijn op het dagelijks functioneren van kinderen. Voordeel van het toepassen van een uniform instrument is niet alleen het kunnen vergelijken van resultaten maar ook continuïteit van methode bij netwerkzorg of het kunnen aanbieden van standaarden in de meest gebruikte ICT systemen.
Rationale van de aanbeveling: weging van argumenten voor en tegen de diagnostische procedure
Voor verbale kinderen en adolescenten wordt, op basis van (psychometrische) eigenschappen en voorkeur voor het zelf laten invullen, de PROMIS PPIS en eventueel de BAPQ geprefereerd boven de andere vragenlijsten.
Opgemerkt dient te worden dat deze aanbeveling voor de PROMIS PPISS en BAPQ is op basis van een systematische review bij kinderen niet in staat om zelf vragenlijsten in te vullen. De PROMIS PPIS verdient de voorkeur boven de BAPQ, gezien de kortere lengte en gevalideerde vertaling in het Nederlands van de PROMIS PPIS.
Voor kinderen niet in staat om zelf vragenlijsten in te vullen, wordt op basis van validiteit de PROMIS PPPIS geprefereerd (gemiddelde bewijskracht). De PROMIS PPPIS is reeds vertaald naar het Nederlands-Vlaams (Dutch-Flemish PROMIS item banks.xlsx (dutchflemishpromis.nl)). BAPQ en BAPQ-P zijn (nog) niet vertaald naar Nederlands-Vlaams en dus niet bruikbaar.
Concluderend kan voor verbale kinderen en adolescenten het beste de PROMIS PPIS worden gebruikt om pijn interferentie bij chronische pijn te meten. Voor non-verbale kinderen en kinderen met neurobiologische ontwikkelingsstoornissen, kan de PROMIS PPPIS worden gebruikt.
Onderbouwing
Achtergrond
When assessing chronic pain in children, it is important to also measure the impact of chronic pain on relevant aspects of the child's life. Measurements may relate to the impact of pain on social (culturally related), cognitive, emotional, physical, and recreational activities, as well as on sleep and quality of life. The impact of chronic pain on the child’s life is called pain interference and can be measured with several instruments. Therefore, this module focusses on identifying the best measurement instrument for pain interference in preverbal and verbal children, adolescents, and children with neurodevelopmental disorders with chronic pain.
Conclusies / Summary of Findings
Subgroup verbal children and adolescents with chronic pain
BAPQ-P
|
Moderate GRADE |
The Bath Adolescent Pain Questionnaire – Parent (BAPQ-P) is probably a valid measurement tool (content validity, hypothesis testing) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Bath Adolescent Pain Questionnaire – Parent (BAPQ-P) could possibly be a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
CALI-P
|
Very low GRADE |
It is unclear whether the Child Activity Limitations Interview – Parent (CALI-P) could be a valid measurement tool (content validity, hypothesis testing, structural validity) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Child Activity Limitations Interview – Parent (CALI-P) could possibly be a reliable measurement tool (internal consistency, reliability, responsiveness) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
PPP
|
Low GRADE |
The Paediatric Pain Profile (PPP) could possibly be a valid measurement tool (content validity, hypothesis testing) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
|
Very low GRADE |
It is unclear whether the Paediatric Pain Profile (PPP) could be a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
PROMIS PPPIS
|
High GRADE |
The Patient-Reported Outcomes Measurement Information System Pediatric Proxy Pain Interference Scale (PROMIS PPPIS) is a valid measurement tool (content validity, hypothesis testing, measurement invariance) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Patient-Reported Outcomes Measurement Information System Pediatric Proxy Pain Interference Scale (PROMIS PPPIS) could possibly be a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
mBPI
|
Moderate GRADE |
The Modified Brief Pain Inventory (mBPI) is probably a valid measurement tool (hypothesis testing) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
|
Very low GRADE |
It is unclear whether the Modified Brief Pain Inventory (mBPI) could be a reliable measurement tool (internal consistency) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
PBI-CR
|
Moderate GRADE |
The Pain Burden Inventory – Caregiver Report (PBI-CR) is probably a valid measurement tool (hypothesis testing) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Pain Burden Inventory – Caregiver Report (PBI-CR) could possibly be a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
PII-P
|
Low GRADE |
The Pain Interference Index – Parent (PII-P) could possibly be a valid measurement tool (content validity, hypothesis testing) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Pain Interference Index – Parent (PII-P) could possibly be a reliable measurement tool (internal consistency) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Smith (2023) |
FDI
|
No GRADE |
No evidence was found regarding the validity of the Functional Disability Inventory (FDI) for the assessment of pain interference in verbal children and adolescents with chronic pain. |
|
Moderate GRADE |
The Functional Disability Inventory (FDI) is probably a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Kashikar-Zuch (2011) |
PEQ-C
|
No GRADE |
No evidence was found regarding the validity of the Pain Experience Questionnaire for Children (PEQ-C) for the assessment of pain interference in verbal children and adolescents with chronic pain. |
|
Moderate GRADE |
The Pain Experience Questionnaire for Children (PEQ-C) is probably a reliable measurement tool (internal consistency) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Hermann (2008) |
PEQ-P
|
No GRADE |
No evidence was found regarding the validity of the Pain Experience Questionnaire for Children – parent version (PEQ-P) for the assessment of pain interference in verbal children and adolescents with chronic pain. |
|
Moderate GRADE |
The Pain Experience Questionnaire for Children – parent version (PEQ-P) is probably a reliable measurement tool (internal consistency) for the assessment of pain interference in verbal children and adolescents with chronic pain.
Source: Hermann (2008) |
Subgroup children unable to self-report
BAPQ-P
|
Moderate GRADE |
The Bath Adolescent Pain Questionnaire – Parent (BAPQ-P) is probably a valid measurement tool (content validity, hypothesis testing) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Bath Adolescent Pain Questionnaire – Parent (BAPQ-P) could possibly be a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
CALI-P
|
Very low GRADE |
It is unclear whether the Child Activity Limitations Interview – Parent (CALI-P) could be a valid measurement tool (content validity, hypothesis testing, structural validity) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
|
Very low GRADE |
It is unclear whether the Child Activity Limitations Interview – Parent (CALI-P) could be a reliable measurement tool (internal consistency, reliability, responsiveness) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
PPP
|
Low GRADE |
The Paediatric Pain Profile (PPP) could possibly be a valid measurement tool (content validity, hypothesis testing) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Paediatric Pain Profile (PPP) could possibly be a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference children unable to self-report with chronic pain.
Source: Smith (2023) |
PROMIS PPPIS
|
Moderate GRADE |
The Patient-Reported Outcomes Measurement Information System Pediatric Proxy Pain Interference Scale (PROMIS PPPIS) is probably a valid measurement tool (content validity, hypothesis testing, measurement invariance) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Patient-Reported Outcomes Measurement Information System Pediatric Proxy Pain Interference Scale (PROMIS PPPIS) could possibly be a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
mBPI
|
High GRADE |
The Modified Brief Pain Inventory (mBPI) is a valid measurement tool (hypothesis testing) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
|
Low GRADE |
The Modified Brief Pain Inventory (mBPI) could possibly be a reliable measurement tool (internal consistency) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
PBI-CR
|
Low GRADE |
The Pain Burden Inventory – Caregiver Report (PBI-CR) could possibly a valid measurement tool (hypothesis testing) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
|
Very low GRADE |
It is unclear whether the Pain Burden Inventory – Caregiver Report (PBI-CR) could be a reliable measurement tool (internal consistency, reliability) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
PII-P
|
Very low GRADE |
It is unclear whether the Pain Interference Index – Parent (PII-P) could be a valid measurement tool (content validity, hypothesis testing) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
|
Very low GRADE |
It is unclear whether the Pain Interference Index – Parent (PII-P) could be a reliable measurement tool (internal consistency) for the assessment of pain interference in children unable to self-report with chronic pain.
Source: Smith (2023) |
Samenvatting literatuur
Description of studies
Smith (2023) performed a systematic review to identify available tools for assessing pain interference in children, adolescents, and adults >2 years with and without the ability to self-report. They also determined the psychometric properties of the tools. MEDLINE, Embase, and PsychInfo were searched from inception to 15th February 2022. A second subsequent search was completed in the same databases, on 29th March 2022. A ‘late breaking’ search was completed on 29th July 2022. Citation searching and targeted reference scanning were also used to minimize the likelihood of missing key articles. Articles were included if they studied psychometric properties of an assessment tool that could be used to assess pain interference in children, adolescents, or adults with chronic pain and the inability to self-report. The psychometric properties of the tools were reported according to the criteria outlined in the COSMIN manual for evaluating the methodological quality of studies on measurement properties. Risk of bias was assessed using the ‘COSMIN Risk of Bias tool to assess the methodological quality of studies on reliability or measurement error of outcome measurement instruments’ and the ‘COSMIN risk of bias checklist for Patient-Reported Outcome Measures (PROMs)’. In total, 33 studies were included in the article, of which 22 reported outcomes in children and adolescents. Of these, one study specifically investigated psychometric properties in the population of children and adolescents unable to self-report.
Smith (2023) reported the following tools for assessing pain interference in children and adolescents with chronic pain:
- Bath Adolescent Pain Questionnaire for Parents (BAPQ-P): five options ranging from ‘never’ to ‘always’ on social life, activities, feelings, general worries, specific worries about its pain, and family life and five options ranging from ‘very behind’ to ‘very ahead’ on how the child sees itself and acts.
- Child Activity Limitations Interview-Parent (CALI-P): includes individually scorable subscales that describe limitations in active versus routine domains, and a prospective 8-item version to use for daily dairy data collection.
- Paediatric Pain Profile (PPP): 20-item behaviour rating scale, each item is rated on a four point scale as occurring ‘not at all’ to ‘a great deal’ in any given time period.
- Patient-Reported Outcomes Measurement Instrument System Pediatric Proxy Pain Interference Scale (PROMIS-PPPIS): five answer options ranging from ‘never’ to ‘almost always’.
- Modified Brief Pain Inventory (mBPI): 11-point numerical rating scale where 0 = ‘does not interfere’ and 10 = ‘interferes completely’ in the past week.
- Pain Burden Inventory – Caregiver Report (PBI-CR): 7-item measure, scale is unclear.
- Pain Interference Index – Parent (PII-P): six-item rating items on a 0-6 scale, in the past two weeks.
Kashikar-Zuck (2011) performed a cross-sectional multicenter dataset study of pediatric patients (8 to 18 years) with chronic pain able to self-report. The study determined the clinical utility and validity of the Functional Disability Inventory (FDI). This is a 15-item instrument, scored on a five-point scale, where higher scores indicate more interference. Cut-off points were 0-12 ‘no/minimal’, 13-20 ‘mild’, 21-29 ‘moderate’, ≥30 ‘severe’. Patients primary presented with chronic or recurrent pain, referred by a variety of medical subspecialties and primary care pediatricians were included. Patients were excluded if they had significant developmental delays or impairments that affected their ability to respond to self-report measures. In total, 1300 children were included, with mean age 14.22 (SD 2.42), 75.7% was female and 86.5% Caucasian. The most frequently reported primary complaints were widespread pain, head pain, abdominal pain, and back pain.
Hermann (2008) performed a cross-sectional development and initial validation study of the Pain Experience Questionnaire for Children (PEQ-C) and its parent version (PEQ-P) in children able to self-report. The PEQ-C and PEQ-P were developed based on the German Multidimensional Pain Inventory for adults, and included the subscales pain interference, affective distress, and social support. Only the results of the subscale pain interference will be reported in this literature summary. Patients were included if they did not meet the exclusion criteria, which were younger than seven years, pain due to cancer or serious disease, pain duration less than six months, and problems with the German language. A total of 111 patients were included, with mean age 11.52 (SD 1.78) and 58% females. Most patients suffered from migraine or tension headache (n=73). The article reported that pain-related interference was significantly higher in girls than boys for both the PEQ-C and PEC-P (PEQ-C F(1,109) = 5.87, p<.05l PEQ-P: F(1,108) = 5.50, p=.02).
Results
The results of the outcomes of the included studies were summarized in tables 1 and 2 and described here.
1. Validity (critical outcome)
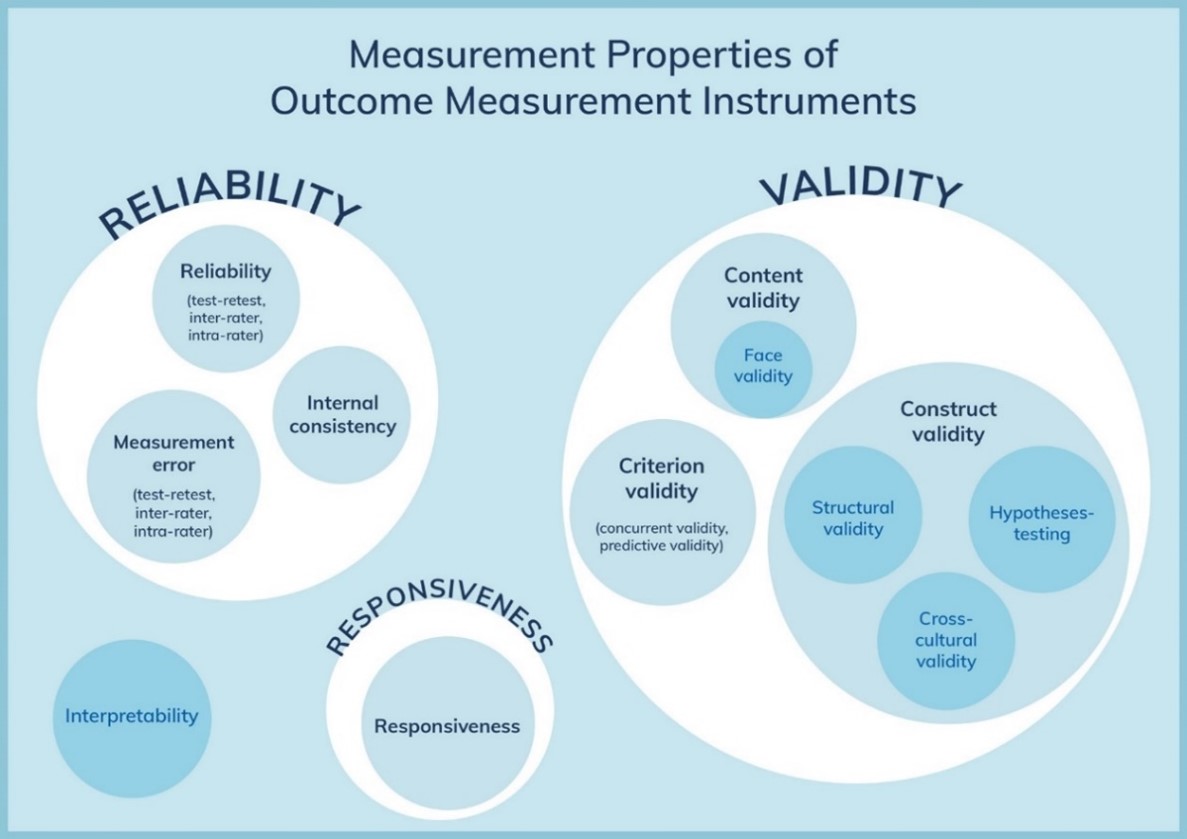
The domain validity refers to the degree to which an outcome measure measures the construct it purports to measure and contains the measurement properties content validity (including face validity), construct validity (including structural validity, hypotheses testing, and cross-cultural validity/measurement invariance) and criterion validity.
1.1 Content validity
Smith (2023) reported sufficient content validity of the BAPQ-P.
Smith (2023) reported sufficient overall content validity of the CALI-P (n=4).
Smith (2023) reported sufficient content validity of the PPP (n=1).
Smith (2023) reported sufficient content validity of the PROMIS PPPIS (n=3).
Smith (2023) reported sufficient content validity of the PII-P (n=1).
1.2 Construct validity
1.2.1 Structural validity
Smith (2023) reported inconsistent results for the 21- and 9-iteam versions of the CALI-P (n=2) (evidence of unidimensionality).
1.2.2 Hypotheses testing
Smith (2023) reported sufficient construct validity of the BAPQ-P (n=3) (3/3 hypotheses supported).
Smith (2023) reported insufficient construct validity of the CALI-P (9/13 hypotheses supported).
Smith (2023) reported sufficient construct validity of the PPP (n=2) (3/4 hypotheses supported), in children unable to self-report.
Smith (2023) reported sufficient construct validity of the PROMIS PPPIS (n=11) (16/21 hypotheses supported, 76%).
Smith (2023) reported sufficient construct validity of the mBPI (n=1) (2/2 hypotheses supported).
Smith (2023) reported sufficient construct validity of the PBI-CR (n=1) (5/6 hypotheses supported).
Smith (2023) reported indeterminate construct validity of the PII-P (n=1) (2/4 hypotheses supported).
1.2.3 Cross-cultural validity
Not reported.
1.2.4 Measurement invariance
Smith (2023) reported sufficient measurement invariance of the PROMIS PPPIS (no significant difference between scores of children 5-7 years and 8-17 years, no DIF found) (n=1).
1.2.5. Convergent validity
The domain convergent validity refers to the degree to which the measurement is related to other measurements that measure the same (or similar) constructs.
1.3 Criterion validity
Not reported.
2. Reliability (important outcome)
The domain reliability refers to the degree to which the measurement is free from measurement error, and it contains the measurement properties internal consistency, reliability, and measurement error.
2.1 Internal consistency
Smith (2023) reported sufficient internal consistency of the BAPQ-P (n=2) (Cronbach’s alpha = 0.87-0.90 for 3 subscales).
Smith (2023) reported sufficient internal consistency of the CALI-P (n=4) (Cronbach’s alpha = 0.86-0.95).
Smith (2023) reported sufficient internal consistency of the PPP (n=2) (Cronbach’s alpha = 0.75-0.95), in children unable to self-report.
Smith (2023) reported sufficient internal consistency of the PROMIS PPPIS (n=1) (Cronbach’s alpha = 0.938).
Smith (2023) reported sufficient internal consistency for the mBPI (n=1) (Cronbach’s alpha = 0.96)
Smith (2023) reported indeterminate internal consistency of the PBI-CR (n=1) (Cronbach’s alpha = 0.792).
Smith (2023) reported indeterminate internal consistency of the PII-P (n=1) (Cronbach’s alpha = 0.94-0.96).
Kashikar-Zuck (2011) reported sufficient internal consistency for factor I (Cronbach’s alpha = 0.91) and adequate internal consistency for factor II (Cronbach’s alpha = 0.77) of the FDI.
Hermann (2008) reported sufficient internal consistency of the subscale interference of the PEQ-C (Cronbach’s alpha = 0.87).
Hermann (2008) reported sufficient internal consistency of the subscale interference of the PEQ-P (Cronbach’s alpha = 0.86).
2.2 Reliability
Smith (2023) reported sufficient test-retest reliability of the BAPQ-P (n=3) (r=0.94-0.98 for 3 subscales).
Smith (2023) reported sufficient reliability of the CALI-P (n=3), with parent/child inter-rater ICC=0.73 and test-retest (intra-rater) r=0.32.
Smith (2023) reported indeterminate test-retest reliability of the PPP (n=2), with parent/health professional interrater ICC 0.62-0.87 and intra-rater ICC=0.90, in children unable to self-report.
Smith (2023) reported indeterminate interrater reliability of the PROMIS PPPIS (n=5), with parent/child inter-rater ICC=0.51-0.80 and weighted kappa =0.24.
Smith (2023) reported sufficient reliability of the PBI-CR (n=1), with child/parent concordance r=0.822, p<0.01.
Kashikar-Zuck (2011) reported insufficient test-retest reliability of the FDI (Pearson r = 0.58, p < 0.001).
2.3 Measurement error
Not reported.
2.4 Responsiveness
Smith (2023) reported sufficient responsiveness of the CALI-P (n=1) (1/1 hypotheses supported).
Smith (2023) reported insufficient responsiveness to change of the PPP (n=1) (2/3 hypotheses supported), in children unable to self-report.
Table 1. Validity and reliability of measures of chronic pain intensity in verbal children and adolescents
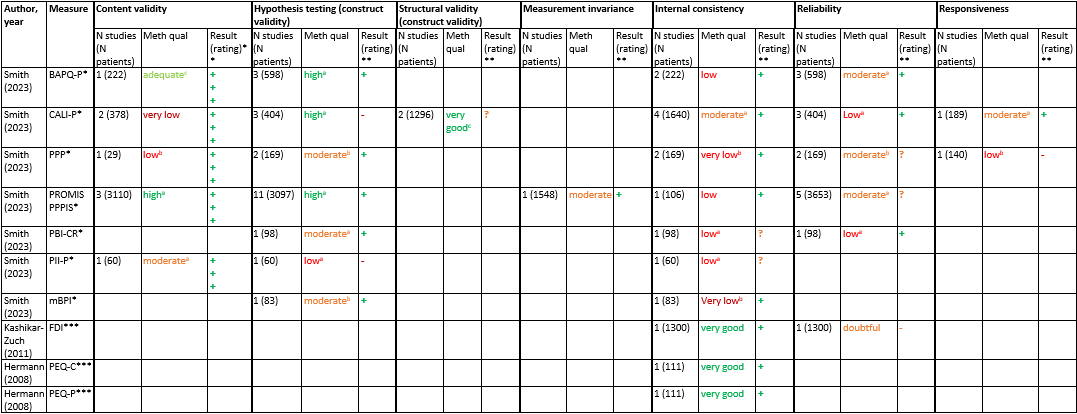
*Methodological quality (GRADE) based on the judgement of the authors of Smith (2023), provided in the article text.
**Measurement properties of each study could be rated based on table 1 as: sufficient (+), insufficient (–), or indeterminate (?)
*** Risk of bias assessment based on COSMIN risk of bias tool: lowest score counts
a The judgement of methodological quality is upgraded with one level because the outcomes is measured in patients able to self-report. Smith (2023) downgraded for indirectness because their population of interest were patients unable to self-report.
b The judgement on methodological quality is downgraded with one level because the outcome is measured in patients unable to self-report (indirectness).
c Risk of bias judgement based on Smith (2023), because GRADE level was not reported in the article.
Abbreviations: BAPQ-P=Bath Adolescent Pain Questionnaire – Parent, CALI=Child Activity Limitations Interview – Parent, FDI=Functional Disability Inventory, mBPI=Modified Brief Pain Inventory, PBI-CR= Pain Burden Inventory – Caregiver Report, PEQ-C=Pain Experience Questionnaire for Children, PEQ-P=Pain Experience Questionnaire for Children – parent version, PII-P=Pain Interference Index parent, PPP=Paediatric Pain Profile, PROMIS-PPIS=Patient-Reported Outcomes Measurement Information System Pediatric Proxy Pain Interference Scale
Table 2. Validity and reliability of measures of chronic pain intensity in children unable to self-report
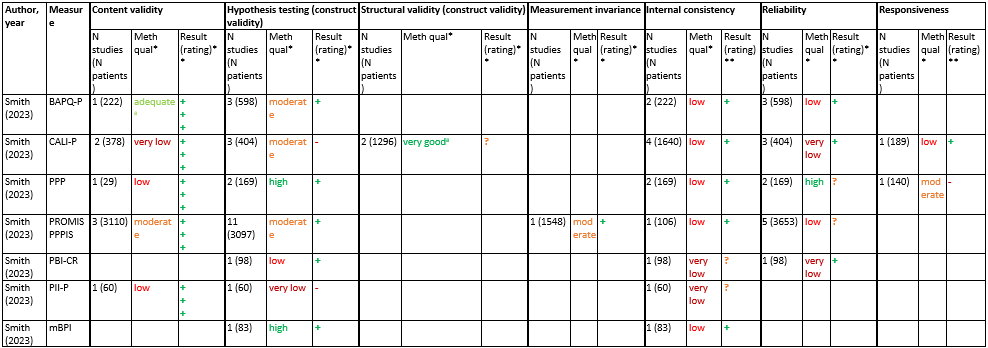
*Methodological quality (GRADE) based on the judgement of the authors of Smith (2023), provided in the article text.
**Measurement properties of each study could be rated based on table 1 as: sufficient (+), insufficient (–), or indeterminate (?)
a Risk of bias judgement based on Smith (2023), because GRADE level was not reported in the article.
Abbreviations: BAPQ-P=Bath Adolescent Pain Questionnaire – Parent, CALI=Child Activity Limitations Interview – Parent, mBPI=Modified Brief Pain Inventory, PBI-CR= Pain Burden Inventory – Caregiver Report, PII-P=Pain Interference Index parent, PPP=Paediatric Pain Profile, PROMIS-PPIS=Patient-Reported Outcomes Measurement Information System Pediatric Proxy Pain Interference Scale
Level of evidence of the literature
The level of evidence (GRADE) of the measures included in Smith (2023) is presented in tables 2 (children and adolescents) and 3 (children unable to self-report).
BAPQ-P
The level of evidence regarding the outcome content validity was downgraded by one level because of low number of included patients (imprecision) to MODERATE.
FDI
The level of evidence regarding the outcome measure internal consistency was not downgraded, which results in HIGH GRADE.
The level of evidence regarding the outcome measure reliability was downgraded by one level because of study limitations (risk of bias due to analysis methods) to MODERATE.
The level of evidence regarding the outcomes content validity, structural validity, hypothesis testing, cross-cultural validity, convergent validity, criterion validity, measurement error, and responsiveness were not assessed because no studies were included investigating these outcomes.
PEQ-C
The level of evidence regarding the outcome measure internal consistency was downgraded by one level because of low number of included patients (imprecision) to MODERATE.
The level of evidence regarding the outcomes content validity, structural validity, hypothesis testing, cross-cultural validity, convergent validity, criterion validity, reliability, measurement error, and responsiveness were not assessed because no studies were included investigating these outcomes.
PEQ-P
The level of evidence regarding the outcome measure internal consistency was downgraded by one level because of low number of included patients (imprecision) to MODERATE.
The level of evidence regarding the outcomes content validity, structural validity, hypothesis testing, cross-cultural validity, convergent validity, criterion validity, reliability, measurement error, and responsiveness were not assessed because no studies were included investigating these outcomes.
Zoeken en selecteren
A systematic review of the literature was performed to answer the following question: What is the validity and reliability of measures for the assessment of pain interference in preverbal children/neonates, verbal children, adolescents, and children with neurodevelopmental disorders with chronic pain?
|
P: |
P1. preverbal children/neonates (<1 month) with chronic pain P2. verbal children with chronic pain P3. adolescents (up to 18 years) with chronic pain P4. children with neurodevelopmental disorders with chronic pain |
| I: |
Measures for the assessment of pain interference
|
| C: | Other measures for the assessment of pain interference |
| O: | Validity and reliability |
Relevant outcome measures
The guideline development group considered validity as a critical outcome measure for decision making; and reliability as an important outcome measure for decision making.
The measurement properties were defined following the taxonomy of the Consensus-based Standards for the selection of health Measurement INstruments (COSMIN) (Mokkink, 2010).
The working group defined the discriminate validity of the screening tools as follows:
AUC < 0.7: poor; 0.7 ≤ AUC < 0.8: acceptable; 0.8 ≤ AUC < 0.9: excellent; AUC ≥ 0.9: outstanding. The working group defined the reliability of the screening tools as follows: ICC < 0.5: poor; 0.5 ≤ ICC < 0.75: moderate; 0.75 ≥ ICC < 0.9: good; ICC≥ 0.9: excellent.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 2007 until 20-06-2023. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 453 hits.
Studies were selected based on the following criteria:
- Systematic review or meta-analysis or observational study (cohort study or case control study)
- Reporting the validity and/or reliability of measures for the assessment of interference pain in preverbal children/neonates, verbal children, adolescents and children with neurodevelopmental disorders with chronic pain.
Twelve studies were initially selected based on title and abstract screening. After reading the full text, nine studies were excluded (see the table with reasons for exclusion under the tab Methods), and three studies were included.
Results
Three studies were included in the analysis of the literature. The studies only concerned subgroups 2 (verbal children), 3 (adolescents), and 4 (children with neurobiological development disorders). No studies were included for subgroup 1 (pre-verbal children). Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables. The COSMIN Risk of Bias tool was used to assess the quality of single studies for each measurement property (see Methods section in ‘Verantwoording’). Test-retest reliability was defined as sufficient when the p-value <0.5 and Pearson correlation coefficient (Pearson’s r) > 0.7 and insufficient when the p-value >0.5 or Pearson correlation coefficient (Pearson’s r) < 0.7, based on https://www.scalestatistics.com/test-retest-reliability.html.
Referenties
- 1 - Hermann C, Hohmeister J, Zohsel K, Tuttas ML, Flor H. The impact of chronic pain in children and adolescents: Development and initial validation of a child and parent version of the Pain Experience Questionnaire. Pain. 2008 Apr;135(3):251-261. doi: 10.1016/j.pain.2007.06.002. Epub 2007 Jul 5. PMID: 17618825.
- 2 - Kashikar-Zuck S, Flowers SR, Claar RL, Guite JW, Logan DE, Lynch-Jordan AM, Palermo TM, Wilson AC. Clinical utility and validity of the Functional Disability Inventory among a multicenter sample of youth with chronic pain. Pain. 2011 Jul;152(7):1600-1607. doi: 10.1016/j.pain.2011.02.050. Epub 2011 Mar 31. PMID: 21458162; PMCID: PMC3114262.
- 3 - Mokkink LB, de Vet HCW, Prinsen CAC, Patrick DL, Alonso J, Bouter LM, Terwee CB. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual Life Res. 2018 May;27(5):1171-1179. doi: 10.1007/s11136-017-1765-4. Epub 2017 Dec 19. PMID: 29260445; PMCID: PMC5891552.
- 4 - Smith MG, Farrar LC, Gibson RJ, Russo RN, Harvey AR. Chronic pain interference assessment tools for children and adults who are unable to self-report: A systematic review of psychometric properties. Dev Med Child Neurol. 2023 Aug;65(8):1029-1042. doi: 10.1111/dmcn.15535. Epub 2023 Feb 5. PMID: 36740907.
Evidence tabellen
Evidence table for systematic reviews of RCTs and observational studies (intervention studies)
Research question: What is the validity and reliability of measures for the assessment of pain interference in preverbal children/neonates, verbal children, adolescents and children with neurodevelopmental disorders with chronic pain?
|
Study reference |
Study characteristics |
Patient characteristics
|
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Smith, 2023
[individual study characteristics deduced from Smith, 2023]
PS., study characteristics and results are extracted from the SR (unless stated otherwise) |
SR
Literature search up from inception to July 2022
Study design: Not reported
Setting and Country: Not reported
Source of funding and conflicts of interest: Not reported
|
Inclusion criteria SR: Articles were included if they studied psychometric properties of an assessment tool that could be used to assess pain interference in children, adolescents, or adults with chronic pain and the inability to self-report
Exclusion criteria SR: Assessment tools that (1) did not assess pain interference as a primary or secondary focus (one or fewer pain interference items, only assessed pain behaviour or assessed presence of pain during function rather than pain interference with function); (2) did not assess chronic pain (recall period <24hours); (3) were administered through self-report; or (4) were developed for assessing pain specific to a condition other than generalized chronic pain (e.g. headaches).
33 studies included
Important patient characteristics: Not reported
|
Measurements for assessment of pain interference in children:
• Bath Adolescent Pain Questionnaire for Parents (BAPQ-P) • Child Activity Limitations Interview-Parent (CALI-P) • Paediatric Pain Profile (PPP) • Patient-Reported Outcomes Measurement Instrument System Pediatric Proxy Pain Interference Scale (PROMIS-PPPIS) • Modified Brief Pain Inventory (mBPI) • Pain Burden Inventory – Caregiver Report (PBI-CR) • Pain Interference Index – Parent (PII-P) |
Not applicable
|
End-point of follow-up: Not reported
For how many participants were no complete outcome data available? Not reported |
Content validity Sufficient (all +++ for relevance, comprehensiveness, and comprehensibility): BAPQ-P, CALI-P, PPP, PROMIS PPPIS, PII-P
Construct validity Hypothesis testing Sufficient:
Insufficient:
Structural validity Unidimensional: CALI-P; evidence of unidimensionality
Measurement invariance Moderate: PROMIS PPPIS; no DIF found when comparing children aged 5-7 years with 8-17 years of age.
Internal consistency Sufficient:
Indeterminate:
Reliability Sufficient:
Insufficient:
Responsiveness Sufficient:
Insufficient:
|
Authors conclusion: This review has identified 10 tools for assessing chronic pain interference in children and adults who are unable to self-report. The PPP is recommended for use in children and adolescents (<18 years).
Data on adults not reported here.
|
Evidence table for intervention studies (randomized controlled trials and non-randomized observational studies [cohort studies, case-control studies, case series])
Research question: What is the validity and reliability of measures for the assessment of pain interference in preverbal children/neonates, verbal children, adolescents and children with neurodevelopmental disorders with chronic pain?
Table of excluded studies
|
Author, year |
Title |
Exclusion reason |
|
Holley, 2018 |
The CALI-9: A brief measure for assessing activity limitations in children and adolescents with chronic pain |
Wrong O: measures no psychometric properties |
|
Clifford, 2015 |
Psychometric properties of the Swedish version of the Functional Disability Inventory |
Wrong design: Swedish validation |
|
Eccleston, 2007 |
Development and preliminary psychometric evaluation of the parent report version of the Bath Adolescent Pain Questionnaire (BAPQ-P): A multidimensional parent report instrument to assess the impact of chronic pain on adolescents |
Included in Smith (2023) |
|
Offenbächer, 2016 |
Functional limitations in children and adolescents suffering from chronic pain: validation and psychometric properties of the German Functional Disability Inventory (FDI-G) |
Wrong design: German validation |
|
Palerma, 2008 |
Validation of a self-report questionnaire version of the Child Activity Limitations Interview (CALI): The CALI-21 |
No comparator and no psychometric properties measured |
|
Hainsworth, 2007 |
Development and Preliminary Validation of the Child Activity Limitations Questionnaire: Flexible and Efficient Assessment of Pain-Related Functional Disability |
Included in Smith (2023) |
|
Kashikar-Zuck, 2016 |
Longitudinal evaluation of patient-reported outcomes measurement information systems measures in pediatric chronic pain |
Wrong C: study compares PROMIS with legacy scales (existing questionnaires). Wrong O: reports the psychometric measures of the PROMIS measures, which also focus on other concepts besides pain interference |
|
Cunningham, 2017 |
Development and validation of the self-reported PROMIS pediatric pain behavior item bank and short form scale |
Report no subgroup analysis on psychometric measures for pain interference. Only report bivariate correlation between PROMIS pain interference and PCS-C (Pain Catastrophizing Scale) |
|
Gudmundsdottir, 2023 |
Psychometric evaluation of an Icelandic translation of the adolescent and parent report versions of the BATH pain questionnaires and investigation of the psychosocial impact of pain on adolescents with chronic disease |
Wrong design: Icelandic validation |
Verantwoording
Beoordelingsdatum en geldigheid
Publicatiedatum : 11-06-2024
Beoordeeld op geldigheid : 19-04-2024
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS).
De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor kinderen met pijn.
Kernwerkgroep
- Drs. M.A. (Maarten) Mensink, kinderanesthesioloog en pijnarts, werkzaam in het Prinses Máxima Centrum voor Kinderoncologie te Utrecht, NVA, voorzitter
- Drs. J.F. (Joanne) Goorhuis, algemeen kinderarts, werkzaam in het Medisch Spectrum Twente, NVK
- Dr. F (Felix) Kreier, algemeen kinderarts, werkzaam in het OLVG te Amsterdam, NVK
- Drs. M.S. (Sukru) Genco, algemeen kinderarts, werkzaam in het OLVG te Amsterdam, NVK
- Dr. S.H. (Steven) Renes, anesthesioloog-pijnspecialist, werkzaam in het Radboud UMC te Nijmegen, NVA
- Dr. P. (Petra) Honig-Mazer, psychotherapeut, werkzaam in het Erasmus MC Sophia te Rotterdam, NIP/LVMP
- Drs. M. (Marjorie) de Neef, kinder-IC verpleegkundige, werkzaam in het Amsterdam UMC, V&VN
- R. (Rowy) Uitzinger, junior projectmanager en beleidsmedewerker, Stichting Kind en Ziekenhuis, tot 1 juni 2022
- E.C. (Esen) Doganer, junior projectmanager en beleidsmedewerker, Stichting Kind en Ziekenhuis, vanaf 1 juni 2022
Werkgroep
- Drs. L.A.M. (Lonneke) Aarts, algemeen kinderarts, werkzaam in het RadboudUMC Amalia kinderziekenhuis te Nijmegen, NVK
- Prof. dr. W.J.E. (Wim) Tissing, kinderoncoloog, werkzaam in het UMCG te Groningen en Prinses Máxima Centrum te Utrecht, NVK
- Prof. dr. S.N. (Saskia) de Wildt, kinderintensivist, werkzaam in het RadboudUMC te Nijmegen, NVK (tot 9-9-2022)
- Prof. dr. N.M. (Nico) Wulffraat, kinderreumatoloog, werkzaam in het UMC Utrecht te Utrecht, NVK (tot 1-11-2022)
- Drs. P. (Petra) Hissink-Muller, kinderreumatoloog, werkzaam in het Erasmus MC Sophia te Rotterdam (vanaf 1-11-2022)
- Drs. A.M. (Arine) Vlieger, algemeen kinderarts, werkzaam in het St. Antonius Ziekenhuis te Utrecht, NVK
- Dr. S.H.P. (Sinno) Simons, kinderarts-neonatoloog, werkzaam in het Erasmus MC Sophia te Rotterdam, NVK
- Drs. K. (Karina) Elangovan, kinderanesthesioloog, werkzaam in het Erasmus MC Sophia te Rotterdam, NVA
- Dr. C.M.G. (Claudia) Keyzer – Dekker, kinderchirurg, werkzaam in het Erasmus MC Sophia te Rotterdam, NVvH
- A.P. (Annette) van der Kaa, kinderfysiotherapeut, werkzaam in het Erasumc MC Sophia te Rotterdam, NVFK en KNGF
- Drs. A. H. (Agnes) Dommerholt, klinisch psycholoog, werkzaam in het OLVG te Amsterdam, NIP/LVMP (vanaf 1-1-2023)
Klankbordgroep
- Drs. J. (Judig) Blaauw, kinderrevalidatiearts, VRA
- Dr. H. (Hanneke) Bruijnzeel, AIOS, werkzaam in het UMC Utrecht te Utrecht, NVKNO
- Dr. A.M.J.W. (Anne-Marie) Scheepers, ziekenhuisapotheker, werkzaam in het MUMC te Maastricht, NVZA
- Dr. S.A. (Sylvia) Obermann-Borst, ervaringsdeskundige ouder & huisarts-epidemioloog, Care4Neo (voorheen Vereniging van Ouders van Couveusekinderen - VOC)
- Dr. I.H. (Ilse) Zaal-Schuller, arts voor verstandelijk gehandicapten/kaderarts palliatieve zorg i.o., werkzaam bij Prinsenstichting Purmerend/ AmsterdamUMC locatie AMC, NVAVG
- M. (Miep) van der Doelen, CliniClowns Nederland (tot 1-9-2023)
- Dr. E. (Eva) Schaffrath, anesthesioloog, werkzaam in het Maastricht UMC te Maastricht, PROSA Kenniscentrum
- M. (Mirjam) Jansen op de Haar, HME-MO Vereniging Nederland
Met ondersteuning van
- Dr. J. (Janneke) Hoogervorst – Schilp, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. C. (Cécile) Overman, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. T. (Tim) Christen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. D.A.M. (Danique) Middelhuis, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. M. (Mark) van Eck, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Drs. L. (Liza) van Mun, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van (kern)werkgroepleden en klankbordgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Betrokkenen |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Werkgroep |
||||
|
Aarts |
Algemeen kinderarts in het Amalia kinderziekenhuissinds november 2017 |
Interne functies onbetaald: 1. voorzitter Pijn werkgroep Amalia kinderziekenhuis. 2. Verbonden aan werkgroep procedurele sedatie bij kinderen. 3. Implementatie VR in Amalia. |
Onderzoek naar effect comfort talk technieken; maar eenmalige subsidie gekregen voor uitvoer. Geen extern belang qua uitkomst. |
Geen actie |
|
Dommerholt |
Klinisch psycholoog KJ, vakgroep kindergeneeskunde OLVG |
Praktijk Dommerholt, praktijk voor kinder- en jeugdpsychotherapie, supervisie en doceren. (momenteel inactief). Lid vakgroep en medische staf, uitvoeren van psychologische diagnostiek en behandeling van kinderen en hun systeem, opleider. |
Geen |
Geen actie |
|
Elangovan |
Universitair medisch specialist Anesthesioloog-pijnspecialist; ErasmusMC |
Geen |
Geen |
Geen actie |
|
Genco |
Kinderarts, OLVG, Amsterdam |
- Eigenaar Genco Med. Beheer B.V. |
Directe belangen bij eigen B.V. maar geen relatie met de bezigheden van de werkgroep. Bijvangst van het project kan zijn: nieuwe kennis en ervaring om binnen onze organisatie te delen. |
Geen actie |
|
Goorhuis |
Algemeen kinderarts - acute kindergeneeskunde |
Geen |
Geen |
Geen actie |
|
Hissink-Muller |
Kinderreumatoloog, Erasmus MC Sophia |
|
|
|
|
Kaa, van der |
Kinderfysiotherapeut |
-Docent Master Kinderfysiotherapie bij Breederode Hogeschool - Universitair docent -Kinderfysiotherapeut 1e lijn (Fysio van der Linden) |
Geen |
Geen actie |
|
Keyzer-Dekker |
Kinderchirurg Sophia Kinderziekenhuis ErasmusMC te Rotterdam |
APLS instructeur SSHK Riel, dagvergoeding |
Geen |
Geen actie |
|
Kreier |
Kinderarts OLVG Amsterdam |
Medeauteur en -oprichter “De hamster in je brein” |
Geen |
Geen actie |
|
Mensink* |
kinderanesthesioloog - pijnarts - Prinses Máxima Centrum voor kinderoncologie |
Bestuurslid sectie Pijn&palliatieve geneeskunde NVA - onbetaalde functie |
Geen |
Geen actie |
|
Neef, de |
Verpleegkundig onderzoeker, Kinder IC, Amsterdam UMC |
Geen |
Geen |
Geen actie |
|
Petra Honig-Mazer |
Erasmus MC - Sophia Kinderziekenhuis Afdeling Kinder- en Jeugdpsychiatrie/psychologie Unit Psychosociale Zorg Psychotherapeut BIG |
Kleine eigen praktijk: Praktijk voor Psychotherapie Honig-Mazer, betaald |
Geen |
Geen actie |
|
Renes |
Anesthesioloog-pijnspecialist Radboudumc |
Kwaliteitsvisitaties Nederlandse Vereniging Anesthesiologie, vacatiegeld |
Geen |
Geen actie |
|
Simons |
Kinderarts - neonatoloog - klinisch farmacoloog (Universitair Medische Specialist) |
Lid geneesmiddelencommissie Erasmus MC (onbetaald) |
Geen |
Geen actie |
|
Tissing |
Kinderoncoloog, Hoogleraar supportive care in de kinderoncologie. 0.6 fte Prinses Maxima Centrum, 0,4 fte UMCG |
PI van onderzoek naar app over invloed van laagdrempelig contact op pijn bij patiënten met kanker. |
Geen |
Geen actie |
|
Uitzinger |
Junior Project manager en beleidsmedewerker Stichting kind en ziekenhuis |
Geen |
Geen |
Geen actie |
|
Vlieger |
1. Kinderarts St Antonius ziekenhuis Nieuwegein |
1. Les geven via Cure en Care en via het Prinses MAxima Centrum op het gebiedvan hypnose bij kinderen. Dit is betaald. |
Aangezien ik les geef op het gebied van non-farmacologische methoden om pijn en angst te voorkomen cq te behandelen kan ik daar theoretisch voordeel van ondervinden als nog meer afdelingen hun personeel geschoold wilt hebben in non-farmacologische technieken. in de richtlijn komen uiteraard geen namen van bedrijven te staan, dus ik verwacht geen evident voordeel. Mijn mede eigenaars van het skills4comfort bedrijf. Overigens loopt dit al heel goed. Iedereen is gelukkig al overtuigd van het belang van het aanleren van positief taalgebruik, afleiden, echt contact maken en een vertrouwensband opbouwen. |
Uitsluiten van besluitvorming voor modules over non-farmacologische pijnbestrijding. Mag wel meelezen. |
|
Wildt, de |
Kinderarts-intensivist, hoogleraar klinische farmacologie, Radboudumc |
Directeur stichting Nederlands Kenniscentrum Farmacotherapie Kinderen (detachering |
Patent: Gebruik van PENK voor nierfunctiebepaling bij kinderen (aangevraagd). Bill and Melinda Gates Foundation: model-informed dosing for pediatric dosing |
Geen actie |
|
Wulffraat |
Hoogleraar kinderimmunologie/reumatologie. UMCU |
Voorzitter (coordinator) ERN-RITA (european reference network (onbetaald). |
Onze vakgroep heeft zeer veel extern gefinancierd onderzoek. Er is geen direct belang van de financier bij deze richtlijn. Onderzoekslijn chronische pijn bij jeugdreuma is puur academisch. Mensink (aangesteld in PMC) is hier de promovendus. Ik ben de promotor. |
Geen actie |
|
Klankbordgroep |
||||
|
Bruijnzeel |
Arts-assistent Keel-, Neus- en Oorheelkunde, UMC Utrecht |
Kerngroep Pediatrie (KNO vereniging) - onbetaald |
Geen |
Geen actie |
|
Scheepers |
ziekenhuisapotheker, Maastricht UMC+ |
Geen |
Geen |
Geen actie |
|
Obermann-Borst |
Coördinator Wetenschap bij Care4Neo 10 u per week |
Coördinator Wetenschap bij Care4Neo 75% betaald/25% vrijwillig verzorgen van bijdrage vanuit patientenperspectief aan wetenschap, richtlijnen en kwaliteit van zorg namens de patientenvereniging voor ouders van en voor kinderen die te vroeg, te klein en/of ziek geboren zijn. |
Geen |
Geen actie |
|
Zaal Schuller |
Arts voor verstandelijk gehandicapten |
Arts voor verstandelijk gehandicapten, betaald. |
Geen |
Geen actie |
|
Schaffrath |
Kinderanesthesioloog MUMC |
Faculty member PROSA (tegen dagvergoeding) |
Geen |
Geen actie |
|
Blaauw |
Kinderrevalidatiearts |
Geen |
Geen |
Geen actie |
|
Bruijn, de (interim) |
Kinderrevalidatiearts bij Revalidatie Friesland |
Lid kwaliteitscommissie VRA (deels betaald, vacatiegeld) |
Geen |
Geen actie |
|
Doelen |
CliniClown bij stichting CliniClowns 28 uur per week |
Bestuurslid theaterproducties Natuurtheater de Kersouwe in Heeswijk Dinther (onbetaald) |
Hoofddoel van mijn bijdrage aan de werkgroep is de kennis en ervaring van CliniClowns in te zetten bij het geven van feedback op de gemaakte stukken. |
Geen actie |
|
Haar, van der |
Freelance consultant Moonshot |
Bestuurslid HME-MO Vereniging Nederland |
Geen |
Geen actie |
* Voorzitter
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door afvaardiging van Stichting Kind en Ziekenhuis in de kernwerkgroep en Care4Neo, CliniClowns Nederland en HME-MO Vereniging Nederland in de klankbordgroep. Op verschillende momenten is input gevraagd tijdens een invitational conference en bij het opstellen van het raamwerk. Het verslag van de invitational conference [zie aanverwante producten] is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan de patiëntenorganisaties en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Module |
Uitkomst raming |
Toelichting |
|
Module Meetinstrumenten interferentie van chronische pijn |
Geen financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft, het geen toename in het aantal in te zetten voltijdsequivalenten aan zorgverleners betreft en het geen wijziging in het opleidingsniveau van zorgpersoneel betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Voorafgaand aan de voorbereidende fase is een invitational conference georganiseerd over herkenning en behandeling van pijn binnen de kindzorg. Een verslag hiervan is opgenomen onder aanverwante producten. Daarnaast werd tijdens de voorbereidende fase van de richtlijn een schriftelijke knelpunteninventarisatie gehouden. Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur en de beoordeling van de risk-of-bias van de individuele studies is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie https://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
COSMIN
The COSMIN Risk of Bias tool was used to assess the quality of single studies for each measurement property. Thereby, the worst-score-counts method was used to determine the risk of bias, this means that the lowest rating given in a box determines the final rating, i.e. the quality of the study. The result of each study on a measurement property were rated against the updated criteria for good measurement properties (Table 1). Each result was rated as either sufficient (+), insufficient (–), or indeterminate (?).
Table 1. Criteria for good measurement properties (Mokkink, 2018)
|
Measurement property |
Rating[1] |
Criteria |
|
Structural validity |
+ |
CTT: CFA: CFI or TLI or comparable measure >0.95 OR RMSEA <0.06 OR SRMR <0.08[2] IRT/Rasch: No violation of unidimensionality[3]: CFI or TLI or comparable measure >0.95 OR RMSEA <0.06 OR SRMR <0.08 AND no violation of local independence: residual correlations among the items after controlling for the dominant factor < 0.20 OR Q3's < 0.37 AND no violation of monotonicity: adequate looking graphs OR item scalability >0.30 AND adequate model fit: IRT: χ2 >0.01 Rasch: infit and outfit mean squares ≥ 0.5 and ≤ 1.5 OR Z-standardized values > ‐2 and <2 |
|
? |
CTT: Not all information for ‘+’ reported IRT/Rasch: Model fit not reported |
|
|
- |
Criteria for ‘+’ not met |
|
|
Internal consistency |
+ |
At least low evidence[4] for sufficient structural validity[5] AND Cronbach's alpha(s) ≥ 0.70 for each unidimensional scale or Subscale.[6] |
|
? |
Criteria for “At least low evidence for sufficient structural validity” not met |
|
|
- |
At least low evidence4 for sufficient structural validity5 AND Cronbach’s alpha(s) < 0.70 for each unidimensional scale or Subscale.6 |
|
|
Reliability |
+ |
ICC or weighted Kappa ≥ 0.70 |
|
? |
ICC or weighted Kappa not reported |
|
|
- |
ICC or weighted Kappa < 0.70 |
|
|
Measurement error |
+ |
SDC or LoA < MIC |
|
? |
MIC not defined |
|
|
- |
SDC or LoA > MIC |
|
|
Hypotheses testing for construct validity |
+ |
The result is in accordance with the hypothesis[7] |
|
? |
No hypothesis defined (by the review team) |
|
|
- |
The result is not in accordance with the hypothesis |
|
|
Cross‐cultural validity\measurement invariance |
+ |
No important differences found between group factors (such as age, gender, language) in multiple group factor analysis OR no important DIF for group factors (McFadden's R2 < 0.02) |
|
? |
No multiple group factor analysis OR DIF analysis performed |
|
|
- |
Important differences between group factors OR DIF was found |
|
|
Criterion validity |
+ |
Correlation with gold standard ≥ 0.70 OR AUC ≥ 0.70 |
|
? |
Not all information for ‘+’ reported |
|
|
- |
Correlation with gold standard < 0.70 OR AUC < 0.70 |
|
|
Responsiveness |
+ |
The result is in accordance with the hypothesis OR AUC ≥ 0.70 |
|
? |
No hypothesis defined (by the review team) |
|
|
- |
The result is not in accordance with the hypothesis OR AUC < 0.70 |
|
|
AUC: area under the curve, CFA: confirmatory factor analysis, CFI: comparative fit index, CTT: classical test theory, DIF: differential item functioning, ICC: intraclass correlation coefficient, IRT: item response theory, LoA: limits of agreement, MIC: minimal important change, RMSEA: Root Mean Square Error of Approximation, SEM: Standard Error of Measurement, SDC: smallest detectable change, SRMR: Standardized Root Mean Residuals, TLI = Tucker‐Lewis Index |
||
[1] “+” = sufficient, ” –“ = insufficient, “?” = indeterminate
[2] To rate the quality of the summary score, the factor structures should be equal across studies
[3] unidimensionality refers to a factor analysis per subscale, while structural validity refers to a factor analysis of a (multidimensional) patient‐reported outcome measure
[4] As defined by grading the evidence according to the GRADE approach
[5] This evidence may come from different studies
[6] The criteria ‘Cronbach alpha < 0.95’ was deleted, as this is relevant in the development phase of a PROM and not when evaluating an existing PROM.
[7] The results of all studies should be taken together and it should then be decided if 75% of the results are in accordance with the hypotheses
The level of evidence of the literature was evaluated as described in the COSMIN user manual for systematic reviews of patient-reported outcome measures (Mokkink, 2018). The following four factors were taken into account: (1) risk of bias (i.e. the methodological quality of the studies), (2) inconsistency (i.e. unexplained inconsistency of results across studies), (3) imprecision (i.e. total sample size of the available studies), and (4) indirectness (i.e. evidence from different populations than the population of interest in the review). The quality of evidence could be downgraded with one level (e.g. from high to moderate evidence) if there is serious risk of bias, with two levels (e.g. from high to low) if there is very serious risk of bias, or with three levels (i.e. from high to very low) if there is extremely risk of bias. The quality of the evidence could be downgraded with one or two levels for inconsistency, imprecision (-1 if total N=50-100; -2 if total N<50) and indirectness.
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE-methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Referenties
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Schünemann HJ, Oxman AD, Brozek J, Glasziou P, Jaeschke R, Vist GE, Williams JW Jr, Kunz R, Craig J, Montori VM, Bossuyt P, Guyatt GH; GRADE Working Group. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ. 2008 May 17;336(7653):1106-10. doi: 10.1136/bmj.39500.677199.AE. Erratum in: BMJ. 2008 May 24;336(7654). doi: 10.1136/bmj.a139.
Schünemann, A Holger J [corrected to Schünemann, Holger J]. PubMed PMID: 18483053; PubMed Central PMCID: PMC2386626.
Wessels M, Hielkema L, van der Weijden T. How to identify existing literature on patients' knowledge, views, and values: the development of a validated search filter. J Med Libr Assoc. 2016 Oct;104(4):320-324. PubMed PMID: 27822157; PubMed Central PMCID: PMC5079497.
Zoekverantwoording
Literature search strategy
Embase
|
No. |
Query |
Results |
|
#17 |
#4 AND #16 sleutelartikelen gevonden |
3 |
|
#16 |
#13 OR #14 OR #15 |
432 |
|
#15 |
#9 NOT #13 NOT #14 Overige |
87 |
|
#14 |
#9 AND (#11 OR #12) NOT #13 OBS |
316 |
|
#13 |
#9 AND #10 SR |
29 |
|
#12 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
14179941 |
|
#11 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
6767914 |
|
#10 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
733409 |
|
#9 |
#8 AND [2007-2023]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
432 |
|
#8 |
#5 AND #6 AND #7 |
711 |
|
#7 |
'patient-reported outcome'/exp OR 'brief pain inventory'/exp OR 'brief pain inventory':ti,ab,kw OR 'pain disability index'/exp OR 'pain disability questionnaire'/exp OR 'pain disability assessment scale'/exp OR 'pediatric pain questionnaire'/exp OR 'pain interference score'/exp OR 'pain interference'/exp OR 'bath adolescent pain questionnaire'/exp OR ((('pain disability' OR 'pediatric pain' OR 'paediatric pain' OR 'adolescent pain') NEAR/2 (index OR questionnaire* OR assess*)):ti,ab,kw) OR 'pain interferen*':ti,ab,kw OR bapq*:ti,ab,kw OR 'child activity limitations interview':ti,ab,kw OR clinrom:ti,ab,kw OR 'consensus based standards for the selection of health measurement instruments':ti,ab,kw OR cosmin:ti,ab,kw OR (((observer* OR parent* OR clinician* OR self OR patient* OR adolescent* OR physician*) NEAR/3 'reported outcome'):ti,ab,kw) OR obsrom:ti,ab,kw OR 'pediatric pain profile':ti,ab,kw OR 'paediatric pain profile':ti,ab,kw OR 'functional disability inventory'/exp OR 'functional disability inventory':ti,ab,kw |
73223 |
|
#6 |
'adolescent'/exp OR 'baby'/exp OR 'boy'/exp OR 'child'/exp OR 'minors'/exp/mj OR 'pediatric patient'/exp OR 'pediatrics'/exp OR 'schoolchild'/exp OR infan*:ti,ab OR newborn*:ti,ab OR 'new born*':ti,ab OR perinat*:ti,ab OR neonat*:ti,ab OR baby*:ti,ab OR babies:ti,ab OR toddler*:ti,ab OR minors*:ti,ab OR boy:ti,ab OR boys:ti,ab OR boyfriend:ti,ab OR boyhood:ti,ab OR girl*:ti,ab OR kid:ti,ab OR kids:ti,ab OR child*:ti,ab OR children*:ti,ab OR schoolchild*:ti,ab OR adolescen*:ti,ab OR juvenil*:ti,ab OR youth*:ti,ab OR teen*:ti,ab OR pubescen*:ti,ab OR pediatric*:ti,ab OR paediatric*:ti,ab OR peadiatric*:ti,ab OR school:ti,ab OR school*:ti,ab OR prematur*:ti,ab OR preterm*:ti,ab |
5710648 |
|
#5 |
'chronic pain'/exp OR 'chronic pain syndrome'/exp OR (((chronic* OR lifelong) NEAR/4 pain*):ti,ab,kw) OR chronicit*:ti,ab,kw |
161353 |
|
#4 |
#1 OR #2 OR #3 sleutelartikelen |
3 |
|
#3 |
'chronic pain interference assessment tools for children and adults who are unable to self-report: a systematic review of psychometric properties' |
1 |
|
#2 |
'evaluating the statistical properties of the pain interference index in children and adolescents with chronic pain' |
1 |
|
#1 |
'development and validation of the self-reported promis pediatric pain behavior item bank and short form scale' |
1 |
Ovid/Medline
|
# |
Searches |
Results |
|
12 |
9 not 10 not 11 Overige |
73 |
|
11 |
((7 or 8) and 9) not 10 OBS |
91 |
|
10 |
6 and 9 SR |
7 |
|
9 |
5 not ((exp animals/ or exp models, animal/) not humans/) not (letter/ or comment/ or editorial/) |
171 |
|
8 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5449144 |
|
7 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4465539 |
|
6 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
675255 |
|
5 |
limit 4 to yr="2017 -Current" |
171 |
|
4 |
1 and 2 and 3 |
254 |
|
3 |
exp Patient Reported Outcome Measures/ or brief pain inventory.ti,ab,kf. or ((pain disability or pediatric pain or paediatric pain or adolescent pain) adj2 (index or questionnaire* or assess*)).ti,ab,kf. or pain interferen*.ti,ab,kf. or bapq*.ti,ab,kf. or child activity limitations interview.ti,ab,kf. or clinrom.ti,ab,kf. or consensus based standards for the selection of health measurement instruments.ti,ab,kf. or cosmin.ti,ab,kf. or ((observer* or parent* or clinician* or self or patient* or physician* or adolescent*) adj3 reported outcome).ti,ab,kf. or obsrom.ti,ab,kf. or pediatric pain profile.ti,ab,kf. or paediatric pain profile.ti,ab,kf. or functional disability inventory.ti,ab,kf. |
33117 |
|
2 |
(child* or schoolchild* or infan* or adolescen* or pediatri* or paediatr* or neonat* or boy or boys or boyhood or girl or girls or girlhood or youth or youths or baby or babies or toddler* or childhood or teen or teens or teenager* or newborn* or postneonat* or postnat* or puberty or preschool* or suckling* or picu or nicu or juvenile?).tw. |
2904505 |
|
1 |
Chronic Pain/ or ((chronic* or lifelelong) adj4 pain*).ti,ab,kf. or chronicit*.ti,ab,kf. |
100532 |