Cognitieve gedragstherapie bij volwassenen met overgewicht of obesitas
Uitgangsvraag
Wat is de toegevoegde waarde van cognitieve gedragstherapie (CGT) toegevoegd aan een gecombineerde leefstijlinterventie (GLI) bij volwassenen met overgewicht (in combinatie met een vergrote buikomvang en/of comorbiditeit) of obesitas?
Aanbeveling
- Overweeg bij patiënten met een BMI ≥ 40 kg/m2 of ≥ 35 BMI < 40 kg/m2 in combinatie met een vergrote buikomvang en/of comorbiditeit, op geleide van bevindingen tijdens de diagnostische fase, doorverwijzing naar een gespecialiseerde GLI waarbij cognitieve gedragstherapie onderdeel uitmaakt van deze GLI (zie module ‘Gespecialiseerde GLI’).
- Adviseer een GLI met cognitieve gedragstherapie (gespecialiseerde GLI) indien er sprake is van milde psychische problematiek die de behandeling van obesitas belemmert.
- Adviseer cognitieve gedragstherapie indien er sprake is van matig tot ernstig verstoord eetgedrag en/of bijkomende psychopathologie.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Cognitieve gedragstherapie (CGT) toegevoegd aan een gecombineerde leefstijl interventie levert mogelijk een gewichtsdaling op. De meeste studies rapporteren gewichtsdaling maar zijn beperkt in de follow-up duur waardoor deze studies alleen korte termijn data presenteren <12 maanden. Slechts twee studies (Forman, 2016; Lillis 2016) hebben het effect van CGT toegevoegd gerapporteerd met een follow-up >2 jaar waarbij sprake lijkt van een trend ten gunste van de toevoeging van CGT aan een GLI. Over het effect op de belangrijke uitkomstmaten de eet psychopathologie en de kwaliteit van leven is geen lange termijn data beschikbaar.
Gewichtsverlies
De gevonden bewijskracht voor de cruciale uitkomstmaat gewicht is laag. De bewijskracht wordt met name beperkt door ernstige imprecisie en het risico van bias in de studie opzet.
Alle geïncludeerde studies hebben cognitieve gedragstherapie (CGT) toegevoegd aan een GLI vergeleken met standaard gedragstherapie (SGT) binnen een GLI. De interventies betroffen acceptatie en commitment therapie, cognitieve technieken, Mindfulness Based Cognitieve Therapie, compassie training, dialectische gedragstherapie, gedragstherapeutische technieken, gedragstechnieken met betrekking tot omgevingsverandering, motiverende gespreksvoering, emotie-regulatietraining en impulsregulatietraining, stimulus controle, zelfmonitoring, doelen stellen, probleemoplossende vaardigheden vergroten en sociale steun zoeken of geen/minimale therapie (vaak omdat deelnemers op een wachtlijst stonden). Deze studies lieten een positief effect zien met betrekking tot het toevoegen van CGT aan een GLI, waardoor het zinvol lijkt om aandacht te hebben voor bovenstaande technieken.
Binnen de psychologie wordt gewichtsverlies ook zelden als enige doel genomen en is inzicht in en verandering van gedrag de focus van behandeling. De module ‘Uitkomstmaten’ geeft inzicht in de andere uitkomstmaten die voor de patiënt en behandeling relevant zijn. CGT betreft verder ook één van de beschikbare behandelmodaliteiten als onderdeel van de behandeling van obesitas. Gepersonaliseerde behandeling van obesitas is essentieel (zie module ‘Gepersonaliseerde zorg’). Hierbij is het eveneens van belang dat zorgverleners eerst inzicht krijgen in eventuele onderliggende aandoeningen, bijdragende en in standhoudende factoren voor obesitas (zie module ‘Diagnostiek’), voordat men start met een gepersonaliseerde behandeling van obesitas.
Met betrekking tot de belangrijke uitkomstmaten gewichtsbehoud, leefstijlveranderingen, eetpsychopathologie en kwaliteit van leven is de bewijskracht beoordeeld als zeer laag, waardoor deze geen richting kan geven aan de besluitvorming. Het is onduidelijk of CGT een effect heeft op gewichtsbehoud en leefstijlverandering. De hypothese is dat CGT geïndiceerd is voor patiënten die gemotiveerd zijn en de mogelijkheid hebben om gedrag en gedachten die samenhangen met gewichtsbehoud en leefstijlverandering onder de loep te nemen en aan te passen.
Eetpathologie:
Lijngericht eetpatroon
Psychologische behandeling lijkt effectief te zijn bij een lijngericht eetpatroon. Uit de systematische review van Jacob (2018) blijkt dat CGT een significant effect heeft op lijngericht eetpatroon. Lijngericht eetpatroon wordt gezien als niet effectief bij obesitas, omdat het gepaard gaat met een afwisselend te lage calorie inname en te hoge restrictie waarna er periodiek ontremming is en verhoogde calorie inname. CGT geeft inzicht in dit patroon door onder meer registratie en heeft als effect dat het eetpatroon (regelmatig en gezond) wordt genormaliseerd en excessen worden voorkomen (Keijsers, 2017).
In de review van Lawlor (2020) wordt CGT vergeleken met SGT waarbij geen verschil wordt gevonden in effectiviteit tussen beide groepen.
Emotie eten
Uit de review van Jacob (2018) blijkt dat CGT ten opzichte van SGT een significant maar geen klinisch relevant effect heeft op emotie eten. Lawlor (2020) concludeert dat er geen verschil is in effectiviteit tussen personen behandeld met CGT t.o.v. personen behandeld met SGT. Emotie eten wordt in psychologische behandeling veranderd door vergroten van inzicht in emotionele triggers die leiden tot over-eten (meer eten dan gepland, vaak hoog calorisch), en omgezet in effectieve coping bij emoties (hulp zoeken, zelf geruststellende of helpende gedachten formuleren, probleem oplossende vaardigheden vergroten).
Eetbuien
Uit de studie van Raman (2019) blijkt dat CGT effectief is in afname van aantal eetbuien ten opzichte van de controlegroep: in deze studie werd cognitieve remediatie therapie toegepast: deze behandeling gaat uit van de veronderstelling dat mensen met een eetstoornis minder goed in staat zijn om van oplossingsstrategie te wisselen. Met oefeningen en gedragsexperimenten wordt de mentale flexibiliteit vergroot met als doel de eetbuien (als enige strategie) te verminderen.
Ontremming
Uit de review van Lawlor (2020) blijkt dat CGT in vergelijking met SGT een significant effect heeft op vermindering van de ontremming. Naast dat ontremming een aangeleerd gedragspatroon kan zijn bij patiënten met obesitas groeit inzicht in de belangrijke rol van hormonen op ontremming.
Mindful eten
Uit twee studies die Lawlor (2020) beschrijft, blijkt dat CGT in vergelijking met SGT een klinische relevant effect heeft op het aanleren van mindful eten. Deze derde generatie CGT zal mogelijk in de komende jaren een grotere rol krijgen in het onderzoek naar effectieve verandering van eetgedrag. Mindfulness richt training op aandacht voor het hier-en-nu. Met betrekking tot eetgedrag leidt het onder meer tot verbetering van moment van verzadiging.
Honger
Vier studies in de review van Lawlor (2020) konden geen klinisch relevant effect aantonen van de behandeling met CGT in vergelijking met SGT op de mate van honger. Honger zal voor een groot deel samenhangen met verstoord/verminderd verzadigingsgevoel bij obesitas.
Lichaamsontevredenheid/ negatief zelfbeeld
Uit twee studies die Lawlor (2020) beschrijft, blijkt er geen verschil te zijn in behandeling met CGT in vergelijking met SGT met betrekking tot de verbetering van lichaamsbeeld. Succesvolle behandeling wordt echter niet enkel bepaald door verbetering van het lichaamsbeeld maar hangt mede af van de gestelde behandeldoelen (zie module ‘Uitkomstmaten’). Voor de aanpak van een negatief zelfbeeld zou een patiënt baat kunnen hebben bij een psychologische behandeling gericht op aanpak van het negatieve zelfbeeld. Meest toegepast is de COMET (COmpetitive MEmory Training) (Korrelboom, 2011).
Kwaliteit van leven:
Depressie
De reviews van Lawlor (2020) en Jacob (2018) laten geen vermindering zien van depressieve symptomatologie na CGT, terwijl Raman (2019) wel een afname van aantoont in de RCT van de patiënten die de Cognitieve Remediatie Therapie ondergingen in vergelijking met patiënten die SGT ondergingen.
Vergroting van mentale flexibiliteit kan depressieve symptomatologie verminderen (Keijsers, 2017).
Stress
In de review van Lawlor (2020) werd er op basis van vier studies geen effect gevonden van behandeling middels derde generatie CGT op stress. Stress werd hier niet als primaire behandelfocus gekozen maar als bij-effect van de CGT gericht op obesitas.
Angst
Binnen de review van Lawlor (2020) werd er op basis van vier studies geen verschil gevonden in de effectiviteit van derde generatie CGT in vergelijking met SGT op angst. Angst werd niet als primaire behandelfocus gekozen maar als bij-effect van de CGT op obesitas.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
CGT behandeling wordt op maat (i.e. de inzet van bepaalde technieken) aangeboden, wat de samenwerking zal optimaliseren en de inzet zal vergroten. Patiënten vinden het prettig als de zorg dichtbij huis kan plaatsvinden, flexibel is in tijd en ruimte, aansluit bij hun behoefte, voorkeur en cultuur. Patiënten vinden het prettig als er contact is met lotgenoten bij wie ze herkenning ervaren.
Kosten (middelenbeslag)
CGT heeft een vastomlijnd aantal sessies, waarbinnen doelen regelmatig geëvalueerd worden, gaat uit van de doelen die voor de patiënt belangrijk zijn en helpt probleemoplossende vaardigheden te vergroten. Hiermee verkrijgt de patiënt vaardigheden die ook een gunstig effect hebben op de andere levensgebieden, terwijl de kosten van deze therapie beperkt zijn.
Alhoewel er een CGT protocol is voor de behandeling van obesitas binnen de GGZ, is er geen DBC GGZ Obesitas. Dit maakt dat op dit moment patiënten niet verwezen kunnen worden met de diagnose obesitas voor psychologische behandeling binnen de GGZ. Voor de andere diagnoses, zoals een eetstoornis in engere zin, en andere GGZ problematiek wel.
Aanvaardbaarheid, haalbaarheid en implementatie
Bij gedragsverandering is het belangrijk om obesitas te beschouwen als ziekte en de patiënt te laten beseffen dat het overgewicht niet zijn eigen schuld is. De zorgverlener dient helder te maken dat eigen inzet is gevraagd om ziekte-last en verergering te verkleinen. Doelen dienen in samenspraak met de patiënt/cliënt te worden gesteld en dienen realistisch en persoonsgericht te zijn. Hierbij dient men ook rekening te houden bij wat past bij de patiënt en wat er beschikbaar is in de omgeving. Het is belangrijk om niet enkel te focussen op gewichtsverlies en buikomvang, maar ook op verbetering van kwaliteit van leven en comorbiditeiten. Motiveer in ieder geval tot gewichtsbehoud (zie module ‘Uitkomstmaten’ voor relevante uitkomstmaten met betrekking tot de behandeling van patiënten met obesitas). Bekrachtig alle kleine stappen die worden gezet en betrek partner en naasten bij doelstellingen. Wees tenslotte alert op psychische problematiek als belemmerende factor bij inzetten GLI gericht op gedragsverandering.
Een ander belangrijk aspect in verbetering van de (praktische) toegankelijkheid voor psychosociale zorg en psychologische behandeling bij obesitas is gebruikmaking van nieuwe technieken in telefonische, online behandeling en VR toepassingen. Momenteel wordt dit onderzoek vooral toegepast in bariatrische trajecten (Cassin 2016, Manzoni 2016).
Een voorwaarde die drempelverhogend is voor CGT is een bepaalde mate van gezondheidsvaardigheden en beheersing van de Nederlandse taal: er wordt uitgegaan van de mogelijkheid te kunnen schrijven (registreren), informatie kunnen lezen en psychologisch reflecteren op gedrag en gedachten. Alhoewel er steeds meer hulpmiddelen worden ontwikkeld voor anderstaligen en laaggeletterden, dient hier nog een belangrijke afstand in te worden overbrugd. 1 op de 3 Nederlanders heeft beperkte gezondheidsvaardigheden. Zij hebben moeite om informatie over gezondheid te vinden, te begrijpen en toe te passen. Voor deze groepen is het belangrijk dat informatie op maat gegeven wordt (bijv. gesprekskaarten van Pharos).
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
In hoeverre een behandeling succesvol genoemd kan worden, hangt mede af van de gestelde behandeldoelen en welke doelen voor de patiënt van waarde zijn (zie module ‘Uitkomstmaten’). Houd bij de behandeling van obesitas rekening met bijdragende psychosociale factoren die een rol spelen bij het ontstaan en in stand houden van obesitas: maatwerk is essentieel. Kijk per situatie of de behandeling van deze psychosociale factoren nodig is. Besteed aandacht aan psychosociale factoren, maar deze hoeven de behandeling van obesitas, middels een GLI, niet in de weg te staan. Indien door de zorgverlener wordt ingeschat dat CGT noodzakelijk is voor duurzame gedragsverandering wordt doorverwijzing naar een multidisciplinair team aanbevolen. De psychische stoornissen die veel voorkomen zijn belemmerend voor het kunnen profiteren van een behandeling gericht op obesitas en dienen eerst behandeld te worden (zie module ‘Diagnostiek’). Licht verstoord eetgedrag zoals lijngericht en emotie eten past binnen een basis GLI. CGT naast een GLI is raadzaam wanneer de obesitas gepaard gaat met psychische problematiek die een succesvolle behandeling belemmert. Indien er sprake is van een matige tot ernstige vorm van verstoord eetgedrag en/of bijkomende psychopathologie dan hoort dit thuis binnen de psychologische behandeling van de basis GGZ (B-GGZ) en gespecialiseerde GGZ (S-GGZ). Eetstoornissen worden behandeld binnen de B-GGZ en S-GGZ (zie Zorgstandaard eetstoornissen). Het is van belang dat het effect van de psychologische behandeling geëvalueerd wordt en gekeken wordt welke volgende stap nodig is (zie module ‘Uitkomstmaten’). De aanbeveling is tot stand gekomen door de gegevens uit de studies te combineren met de ervaringen vanuit de huidige praktijk van ondersteuning en zorg voor volwassenen met overgewicht of obesitas.
Onderbouwing
Achtergrond
Binnen de behandeling van obesitas is regelmatig psychologische ondersteuning nodig, zowel bij verandering van gedrag (op eetpatroon en leefstijl) als bij andere veelvoorkomende psychische klachten. Het Zorginstituut Nederland (2020) heeft recent onderzocht wat de werkzame onderdelen zijn bij een gespecialiseerde Gecombineerde Leefstijl Interventie (GLI) en constateerde dat Cognitieve Gedragstherapie (CGT) een werkzaam element is bij GLI om langdurige gedragsverandering te bewerkstelligen. Ook werd gesteld dat het bij de toepassing van deze technieken belangrijk is dat er gekeken wordt naar psychische comorbiditeiten die vaak voorkomen bij de populatie.
De werkwijze van CGT is gericht op gedrag en cognities. De technieken die we onder CGT scharen zijn: registratie, stimulus controle, cue exposure, en onderdelen uit de stromingen mindfulness, Acceptance and Commitment Therapy (ACT), Dialectische Gedragstherapie (DGT), EMDR en schema therapie. Hiermee worden zelfregulering, eigen effectiviteit, probleemoplossend vermogen verbeterd. Een aantal van deze technieken worden ook gebruikt bij reguliere psychologische interventies gericht op gedragsverandering. CGT wordt uitgeoefend door Klinisch Psychologen, Psychotherapeuten en GZ psychologen, basispsychologen, POH GGZ en cognitief gedragstherapeutisch medewerkers. Onderdelen van deze behandeling (i.e. verschillende technieken zoals stimuluscontrole, zelfmonitoring en eigen effectiviteit) worden uitgevoerd door gekwalificeerde professionals betrokken bij een GLI of gespecialiseerde GLI (leefstijlcoaches, diëtisten, bewegingsagogen).
Om de toegevoegde waarde van CGT bij (ernstige) obesitas te bepalen wordt gekeken naar de onderzoeken van de afgelopen jaren om tot een advies te komen in welke mate CGT kan bijdragen aan de behandeling. In de internationale literatuur is GLI geen standaard behandeling bij obesitas en wordt derhalve meer algemeen gekeken naar werkzame onderdelen van CGT bij obesitas.
Introduction
Treatment of obesity often requires regular support from psychological treatment, both for support with behaviour change (regarding diet and lifestyle) and other psychological complaints that often occur.The National Health Care Institute recently (2020) investigated the active components of a specialized Combined Lifestyle Intervention (CLI) and found that Cognitive Behavioral Therapy (CBT) is an effective element in a CLI to achieve long-term behavioural change. It was also stated that when applying these techniques it is important to look for psychological comorbidities that often occur within this population.
CBT focuses on behaviour and cognitions. Techniques used in CGT therapy are:registration, stimulus control, cue exposure, and components from the fields of mindfulness, Acceptance and Commitment Therapy (ACT), Dialectical Behavior Therapy, EMDR and schema therapy. This improves self-regulation, self-effect, problem-solving ability. Some of these techniques are also used in regular psychological interventions aimed at behavioural change. CBT is practiced by Clinical Psychologists, Psychotherapists and GZ psychologists, master psychologists and cognitive behavioral workers. Parts of this treatment (i.e. different techniques such as stimulus control, self-monitoring and self-efficacy) are performed by qualified professionals involved in a CLI or specialized CLI (lifestyle coaches, dieticians).
Studies of recent years are examined In order to determine the added value of CBT in (severe) obesity, to give an advice on the extent to which CBT can contribute to treatment. In the international literature, CLI is not a standard treatment for obesity and therefore active components of CBT in obesity are more generally looked at.
Conclusies / Summary of Findings
|
low GRADE |
Weight loss
It is likely that cognitive behavioural therapy may result in little to no difference in reduction of weight at 3 to 9 months follow up compared to standard behavioural therapy, in adults with obesity or overweight.
Sources: Jacob, 2018; Lawlor, 2020 |
|
Low GRADE |
It is likely that cognitive behavioural therapy may result in little to no difference in reduction of weight at 3 to 9 months follow up compared to no/minimal intervention, in adults with obesity or overweight.
Sources: Jacob, 2018; Lawlor, 2020 |
|
low GRADE |
It is likely that cognitive behavioural therapy may result in little to no difference in reduction of weight at 12 to 36 months follow up compared to standard behavioural therapy, in adults with obesity or overweight.
Sources: Jacob, 2018; Lawlor, 2020 |
|
Very low GRADE |
Weight maintenance
It is not clear from the literature if cognitive behavioural therapy may increase weight maintenance compared to standard behavioural therapy, in adults with obesity or overweight.
Sources: 1e Madjd, 2020 |
|
Very ow GRADE |
Lifestyle changes
It is not clear from the literature if cognitive behavioural therapy may increase physical activity compared to standard behavioural therapy, in adults with obesity or overweight.
Sources: 1e Madjd, 2020; Godfrey, 2019 |
|
Very low GRADE |
Eating psychopathology
It is not clear from the literature if cognitive behavioural therapy may improve eating psychopathology compared to standard behavioural therapy, in adults with obesity or overweight.
Sources: Jacob, 2018; Lawlor, 2020 |
|
Very low GRADE |
Quality of life
It is not clear from the literature if cognitive behavioural therapy may improve quality of life compared to standard behavioural therapy, in adults with obesity or overweight.
Sources: Jacob, 2018; Lawlor, 2020; Raman, 2019 |
Samenvatting literatuur
Description of studies
The systemic review and meta-analysis by Jacob (2018) compares the effects of cognitive behavioural therapy (CBT) weight loss interventions on weight loss and psychological outcomes in adults with overweight or obesity, by comparing CBT to a comparison group that either included only behavioural techniques (e.g. stimulus control, self-monitoring, goal setting), or targeting a lifestyle factor (e.g. physical activity or diet and/or education). The article did not described whether interventions were delivered as group sessions or individual sessions. Jacob (2018) covers the literature until May 2016 and includes 12 RCTs conducted between 2005 and 2015. Sample sizes ranged from 18 to 5,145 participants. The median age of study participants was 46 years (range of average age, 11–59 years). Follow-up periods ranged from 4 to 162 months. Six studies were conducted in the United States and six in Europe. The duration of the interventions ranged from 4 weeks to 48 months (median=26 weeks) and the mean number of sessions was 27. The Downs and Black reporting quality score was used to assess the quality of reporting of the studies. Ranges were defined as follows: excellent (26–28); good (20 –25); fair (15–19); and poor (≤14 and these ranges were then dichotomized into two categories: (a) good reporting quality studies with a score ≥20; and (b) lower quality reporting studies with a score of ≤19. Using this score seven out of 12 studies (58%) were deemed to be of good quality, with a median score of 23 (ranging from 20 to 25) and five out of 12 (42%) were deemed low quality, with a median score of 17 (ranging from 16 to 19).
The systemic review and network meta-analysis by Lawlor (2020) searched for the effectiveness of third-wave CBTs (3wCBT): Acceptance and Commitment Therapy, Dialectal Behaviour Therapy, Mindfulness Based Cognitive Behavioural Therapy and Compassion-focused Therapy. On body weight and psychological outcomes in adults with overweight or obesity, 3wCBT was compared to no/minimal intervention or standard behavioural treatment (SBT) including diet, physical activity advice and standard behaviour change techniques (e.g. Goal setting, Self-monitoring, problem solving, social support). Lawlor (2020) covers the literature until September 2019 and included 37 studies, of which 17 studies used a two-group RCT, four used a three-group RCT, and one used a two-group cluster RCT design. Fourteen studies used a pre-intervention to post-intervention one-group design, and one study was a non-randomized three-group study. In 25 studies, the intervention was delivered as group sessions, 4 studies examined individual sessions and in seven studies group sessions and individual sessions were combined. Included studies were conducted in the United States (n=28), New Zealand (n=1), Italy (n=1), United Kingdom (n=3), the Netherlands (n=2), Finland (n=1), and Portugal (n=1). Studies sample sizes ranged from 10 to 283 participants. In total, studies included 2726 participants with 75% being female (n=2035/2726). Mean age was 46 years (ranged from 21 to 58 years), and mean BMI was 35.6 kg/m2. Risk of bias was assessed using the Risk of Bias 2 tool (RoB 2) or the Risk Of Bias In Non-randomized Studies of Interventions tool (ROBINS-I), dependent upon study design. Of the RCTs, the risk of bias was rated as 'high' in four 'some concern' in eleven and 'low' in seven studies. Of the 15 non-RCTs, the risk of bias was rated as 'serious' in nine and 'moderate' in six studies (see Table S4b; Lawlor, 2020).
Raman (2018) conducted an RCT comparing cognitive remediation therapy (CRT) following a behavioural weight loss program for obesity versus no treatment following a behavioural weight loss program within a randomised controlled trial, in terms of improving cognitive flexibility, reducing binge eating behaviour, improving quality of life and helping with weight loss. The behavioural weight loss program targets diet and exercise through behavioural modification techniques and wass delivered individually. Raman (2018) included adults with overweight or obesity BMI ≥30 kg/m2, age 18-55 years and a current weight under 180 kg (n=80). All participants received behaviour weight loss therapy for 3 weeks before being randomized to either the CRT group (n=42) or the no treatment group (n=38). Outcomes included weight change, binge eating, BMI, depression and quality of life. Data were collected at baseline, end-of-treatment and the 3-month follow-up. Participants were mostly female (86 %). At baseline participants in the control group had a mean BMI of 39.2 (SD=7) kg/m2, weight of 108.1 (SD=18.7) kg, mean age of 42.2 (SD=8.8) years, and scored 13.3 (SD=12.2) on depression and 45.7 (SD=9.4) on health related quality of life. Participants in the treatment group had a mean BMI of 40.3 (SD=7.8) kg/m2, weight of 111.7 (SD=21.5) kg, mean age of 40.6 (SD=7.0) years, and scored 19.1 (SD=11.2) on depression and 46.9 (SD=8.4) on health related quality of life. Baseline measures did not show any significant difference between groups except for depression scores, which were higher in the treatment group
Godfrey (2019) conducted an RCT comparing the effect of acceptance based therapy (ABT) versus SBT on intentions for physical activity. Godfrey (2019) included adults with overweight or obesity BMI of 27–50 kg/m2 and aged 18–70 years (n=189). Participants were assigned to SBT (n=90) or ABT (n=99) groups using randomization stratified by gender and ethnicity. The intervention was delivered as group sessions. The baseline assessment was conducted during the first 3 weeks of weight loss treatment. Mid-treatment and end-of-treatment assessments were conducted at 6 and 12 months, respectively. Outcomes included physical activity intention, physical activity behaviour and weight. Participants had a mean baseline BMI of 36.9 kg/m2 (SD=5.8), mean baseline weight of 100.7 kg (SD=18.9) and mean age of 51.1 years (SD=9.8). Participants were mostly female (82.0%), Caucasian (69.3%). These demographic characteristics did not differ between group.
Madjd (2020) conducted an RCT comparing the effect of CBT versus no treatment on weight maintenance. The RCT by Madjd (2020) was sponsored by a non-commercial organisation. Madjd (2020) included adults who lost at least 10% of their body weight with a post weight loss BMI of 23–30 kg/m2 and aged 18–45 years (n=113). Participants randomly assigned to the CBT group (n=56) or control group (n=57). The intervention was delivered as group sessions. The primary outcome addressed in this study was the difference in maintenance of body weight loss after the 24-week CBT program. Anthropometric measurements including weight, BMI, and WC were taken at the start of the weight-maintenance program as baseline, at 12 weeks and after 24 weeks. At baseline participants in the control group had a mean BMI of 27.58 kg/m2 (SD=1.78), weight of 72.14 (SD=4.39) kg, mean age of 32 (SD=6.3) years, and waist circumference of 88 (SD=6.07) cm. Participants in the treatment group had a mean BMI of 17.56 kg/m2 (SD=1.83), weight of 71.32 (SD=5.52) kg, mean age of 31 (SD=6), and waist circumference of 87 (SD=7.35) cm. Baseline measures did not show any significant difference between groups.
Results
Weight loss
Jacob (2018) converted weight to kilograms and pre/post intervention values were used to conduct the analysis. Compared to control conditions CBT resulted in a significant, but not a clinical relevant mean difference of -1.70 kg; (95%CI -2.53 to -0.87), meaning that on average participants receiving CBT lost 1.70 kg more compared to participants in the control group including behavioural techniques, education or waiting list (Figure 5.1). The pooled effect estimate (standardized mean difference, SMD) on weight demonstrated a significant, but not a clinical relevant difference (SMD=-0.30; 95%CI -0.51 to -0.09) with a low level of heterogeneity (I2=1%), favouring CBT (Figure 5.2).
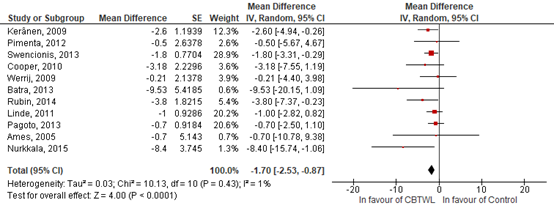
Figure 5.1. Forrest plot showing the effect of cognitive behavioural treatment on weight compared to standard behavioural treatment. Mean differences, random effects model (Jacob, 2018).
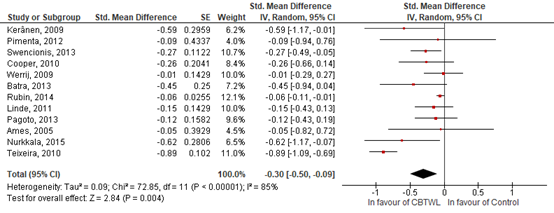
Figure 5.2 Forrest plot showing the effect of cognitive behavioural treatment on weight compared to standard behavioural treatment. Standardized mean differences, random effects model (Jacob, 2018).
Lawlor (2020) included 25 studies that reported an absolute weight change (kg or lb), four studies reported percent change from baseline weight, and six studies reported BMI change. Standardized mean difference in weight or BMI for 3wCBT was SMD=−0.84; (95%CI −1.06 to −0.62; I2=93%) from baseline to post-intervention, equating an absolute weight change of 5.5 kg in favour of the 3wCBT group compared to the control group. This is a significant, but not a clinical relevant difference.
Pairwise random-effects meta-analysis by Lawlor (2020) showed that 3wCBT does not result in significant or clinical relevant greater weight loss compared to no/minimal intervention at post intervention (SMD=−0.21; 95% CI −0.43 to 0.01; I2 = 0%), 3 months (SMD=−0.17; 95% CI −0.75 to 0.41), 6 month (SMD=−0.01; 95%CI −0.46 to 0.44), and 9 months follow-up from baseline (SMD=−0.21; 95% CI −0.46 to 0.04; I2 = 0%) (Figure 3).
Pairwise random-effects meta-analysis by Lawlor (2020) showed that 3wCBT does not result in significant or clinical relevant greater weight loss compared to SBT at post-intervention (SMD=-0.09; 95% CI -0.22 to 0.04; I2=32%), 3 months (SMD=−0.04; 95% CI −0.24 to 0.16; I2=34%), 6 months (SMD=−0.07; 95%CI −0.21 to 0.06; I2=17%), and 9 months (SMD=−0.11; 95% CI −0.29 to 0.51; I2=41%) (Figure 5.3).
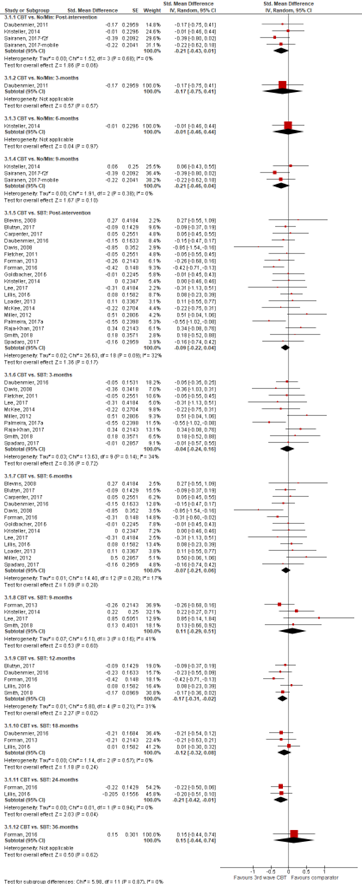
Figure 5.3 Forrest plot showing the effect of cognitive behavioural treatment on weight compared to no/minimum treatment and compared to standard behavioural treatment. Standardized mean differences, random effects model (Lawlor, 2020).
Raman (2018) defined weight change as the difference (percentage reduction) in weight between weight at baseline period and 3 month follow up. The CRT group reported significantly higher weight change percentage compared to control after 3 months follow-up (P <0.001). After 3 months follow-up, participants who completed CRT had lost on average 6.6%; (95% CI 5.6; 9.1), of weight which crosses the threshold of clinical relevance (5%). In contrast, controls gained 1.2% (95% CI -4.6 to 2.5) of weight. The effect size for this difference between groups was large, with a Cohen's d of 1.3 (95% CI -2.007 to -0.589). In addition, more participants in the CRT group (68%) achieved weight loss of 5% or more compared to the control group (15%). The RR for achieving weight loss was 4.98 (95% CI 2.35 to 10.55) in favour of the CRT group. This is a significant and clinical relevant difference.
Weight loss – long term results
Lawlor (2020) included five studies that reported long term follow-up weight loss results. five studies reported results after 12 months follow-up, three after 18 months follow-up, two after 24 months follow-up and one after 36 months follow-up. Pairwise random-effects meta-analysis by Lawlor (2020) showed that 3wCBT does not result in significant or clinical relevant greater weight loss compared to SBT at 12 months (SMD=−0.17; 95%CI −0.31 to 0.02; I2=31%), 18 months (SMD=−0.12; 95% CI −0.32 to 0.08; I2=0%), 24 months (SMD=−0.21; 95% CI −0.42 to 0.00) and 36 months (SMD=−0.15; 95% CI −0.44 to 0.74) (Figure 3).
Weight maintenance
Madjd (2020) reported on weight maintenance in women receiving CBT who lost at least 10% of their body weight and found significant difference in weight change between groups. Compared with control group, CBT improved weight loss maintenance with a mean difference (MD)=−2.2 kg; (95% CI −3.50 to −0.94) at the end of the 24-week intervention, which is considered clinical relevant. In line with improved weight loss, CBT also significantly improved BMI (MD=−0.77 kg/m²; 95% CI −1.25 to −0.28), and waist circumference (MD=−2.08 cm; 95% CI −3.31 to −0.844) at the end of the 24-week intervention, compared with the control group.
Lifestyle changes
Madjd (2020) compared physical activity based on daily steps between groups and found them to be similar at baseline with daily steps of 5897 (SD=537) in the control and 5757 (SD=551) in the CBT group. Compared with baseline, daily steps of participants in the control group decreased over time but in the CBT group daily steps increased significantly (P < 0.001, absolute numbers were not reported).
Godfrey (2019) compares physical activity intentions between groups and shows that participants in the ABT group show higher intentions to undertake physical activity compared to the SBT group. ABT had a significantly higher increase than SBT in physical activity intention minutes at mid-treatment and end of treatment (p < 0.001, absolute numbers were not reported), and both groups had nonlinear increases in moderate-to-vigorous physical activity that were not significantly different. Mixed effects models of minutes of moderate-to-vigorous physical activity per week did not find an significant effect for between treatment groups (P=0.74, absolute numbers were not reported)
Eating psychopathology
Cognitive restraint
Six studies included in Jacob (2018) reported on cognitive restraint/restraint eating. The pooled effect estimate on cognitive restraint was SMD=0.71; (95% CI 0.33 to 1.09), with a high level of heterogeneity (I2=81%), showing that CBT was associated with a significant and clinical relevant increase in cognitive restraint (Figure 5.4).
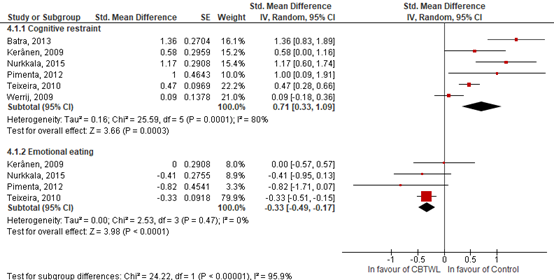
Figure 5.4 Forrest plot showing the effect of cognitive behavioural treatment on cognitive restraint and emotional eating compared to standard behavioural treatment. Standardized mean differences, random effects model (Jacob, 2018).
Five studies included in Lawlor (2020) reported on the effect of 3wCBT on dietary restraint. Pooled arm-specific showed no evidence of a significant and clinical relevant difference in dietary restraint (SMD=0.33; 95%CI -0.18 to 0.85; I2= 74%) (Figure 5.5).
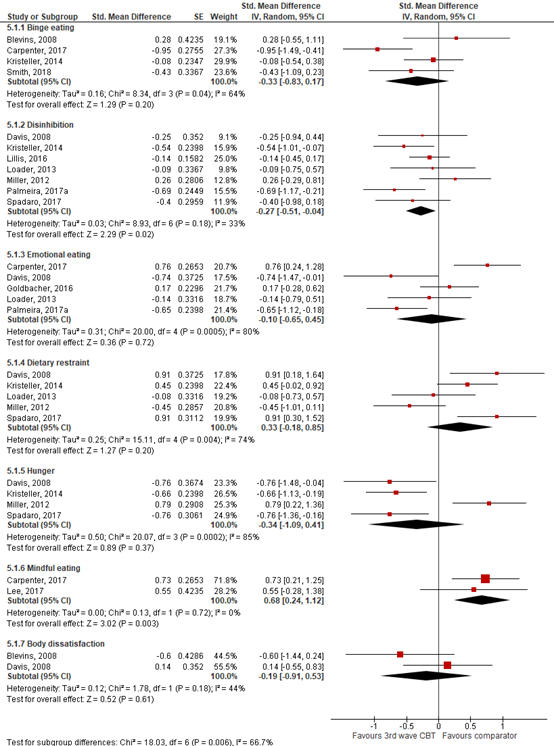
Figure 5.5 Forrest plot showing the effect of cognitive behavioural treatment on eating psychopathology compared to standard behavioural treatment. Standardized mean differences, random effects model
(Lawlor, 2020).
Emotional eating
Four studies included in Jacob (2018) reported on emotional eating. The pooled effect on emotional eating was SMD=-0.33; (95% CI -0.49 to -0.17); I2=0%), showing that CBT was associated with a significant but not a clinical relevant decrease in emotional eating
(Figure 5.6).
Five studies included in Lawlor (2020) reported on the effect of 3wCBT on emotional eating. Pooled arm-specific estimates showed no evidence of a difference compared to SBT in emotional eating (SMD=-0.10; 95% CI -0.65 to 0.44; I2=80%) (Figure 5).
Binge eating
Jacob (2018) could not conduct a meta-analysis for binge eating because of heterogeneity in the nature of the outcomes and the limited number of studies that included each type of outcome.
Four studies included in Lawlor (2020) reported on the effect of 3wCBT on dietary binge eating. Pooled arm-specific showed no evidence of a significant or clinical relevant difference between the groups in binge eating (SMD=-0.33; 95% CI -0.83 to 0.17; I2=64%), compared to SBT (Figure 5).
Disinhibition
Seven studies included in Lawlor (2020) reported on the effect of 3wCBT on disinhibition. Pooled arm-specific showed a significant but not a clinical relevant decrease in disinhibition when compared to SBT (SMD=-0.27; 95% CI -0.51 to -0.04; I2=33%) (Figure 5).
Mindful eating
Two studies included in Lawlor (2020) reported on the effect of 3wCBT on mindful eating. Pooled arm-specific estimates showed no significant increase in mindful eating for 3wCBT when compared to SBT (SMD=0.68; 95% CI 0.24 to 1.12; I2=0%) (Figure 5). This difference was however clinical relevant.
Hunger
Four studies included in Lawlor (2020) reported on the effect of 3wCBT on hunger. Pooled arm-specific estimates showed no significant or clinical relevant decrease in hunger for 3wCBT when compared to SBT (SMD=-0.34; 95% CI -1.09 to 0.41; I2=85%) (Figure 5).
Body dissatisfaction
Two studies included in Lawlor (2020) reported on the effect of 3wCBT on body dissatisfaction. Pooled estimates by showed no evidence of a significant or clinical relevant change in body dissatisfaction (SMD=-0.19; 95% CI -0.91 to 0.53; I2=44%) compared to SBT (Figure 5).
Quality of life
Depressive symptoms
Six studies included in Jacob (2018) reported on depressive symptoms. The pooled effect estimate for depressive symptoms was SMD=-0.10 (95% CI: -0.22 to 0.02) with a moderate level of heterogeneity (I2=37%), showing that CBT was not associated with a significant or clinical relevant effect in depressive symptoms (Figure 5.6).
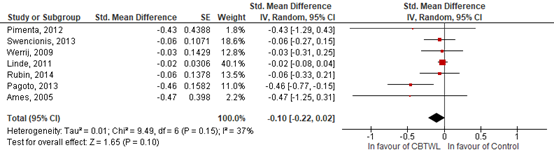
Figure 5.6 Standardized mean differences showing the effect of cognitive behavioural treatment on depressive symptoms compared to standard behavioural treatment (Jacob, 2018).
Six studies included in Lawlor (2020) reported on the effect of 3wCBT on depression. Pooled estimates showed no evidence of significant or clinical relevant differences in depression (SMD=0.02; 95% CI -0.19 to 0.23; I2=0%) (Figure 5.7).
Raman (2019) showed that participants in the CRT group reported a significant decrease in depression scores over time compared to the control group. On average, participants in the CRT-group had a depression score (on the DASS) of 19.1 (SD=11.2) at baseline, but at 3 month follow-up this had reduced to an average score of 5.8 (SD= 8.6; Cohen's d=-1.332; 95% CI -2.044; -0.62). This is a significant and clinical relevant difference. In contrast, the control condition had a depression score (on the DASS) of 13.3 (SD=12.2) on average at baseline decreasing to 11.9 (SD: 12.1) at 3-month follow-up (Cohen's d=-0.12; 95% CI -0.635 to 0.654). This is not a significant or clinical relevant difference
Stress
Four studies included in Lawlor (2020) reported on the effect of 3wCBT on stress. Pooled estimates showed no evidence of significant or clinical relevant differences in stress (SMD=-0.13; 95% CI -0.54 to -0.29; I2=58%) (Figure 5.7).
Anxiety
Jacob (2018) did not conduct meta-analyses for anxiety since there were only 2 studies. Both studies however did not found a significant or clinical relevant effect of CBT on reducing anxiety symptoms.
Five studies included in Lawlor (2020) reported on the effect of 3wCBT on anxiety. Pairwise estimates showed no evidence of significant or clinical relevant differences in anxiety (SMD=-0.12; 95% CI -0.45 to 0.21; I2=45%) compared to SBT (Figure 5.7)
Mental health related quality of life
Seven studies included in Lawlor (2020) reported on mindfulness. Pairwise estimates did not show significant or clinical relevant greater increase in mindfulness in (SMD=0.15; 95% CI -0.06 to 0.35; I2=0%), compared to SBT (Figure 7).This was measured by MAAS (Mindful Attention Awereness Scale), FFMQ (Five Facet Mindfulness Questionnaire) and TMS (Toronto Mindfulness Scale)
Lawlor (2020) included one study which reported 3wCBT resulted in a significant and clinical relevant greater increase in quality of life compared to SBT (SMD=0.69; 95% CI 0.22 to 1.16)
( Figure 5.7).
Raman (2019) showed that on average participants in the CRT-group had a mental Health quality of life score of 46.9 (part of HRQol = Health related Quality of Life) (SD=8.35) at baseline, but at 3 month follow-up this had increased to an average of 50.5 (SD= 10.7) (Cohen's d=-0.375; 95% CI -0.275 to 1.025). This is not a significant or clinical relevant difference. In contrast, the control condition had a mental health quality of life score of 45.7 (SD=9.4) on average at baseline increasing to 48.3 (SD=12.1) at 3-month follow-up (Cohen's d=0.24; 95% CI -0.635 to 0.654). This is not a significant or clinical relevant difference.
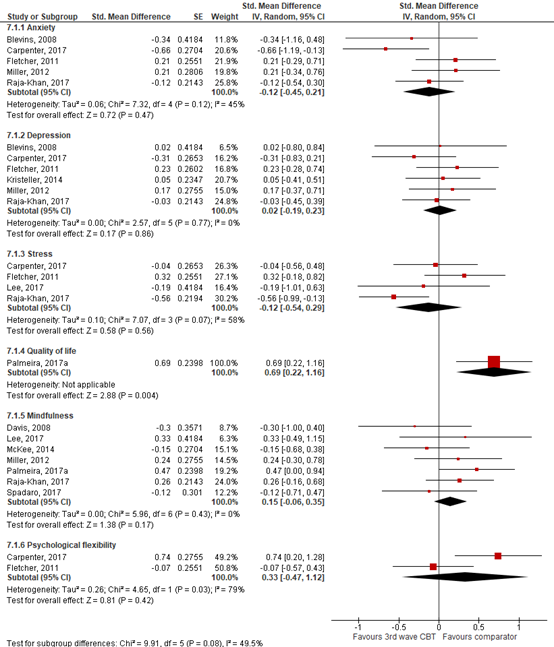
Figure 5.7 Forrest plot showing the effect of cognitive behavioural treatment on psychological outcomes and quality of live compared to no/minimum treatment and compared to standard behavioural treatment. Standardized mean differences, random effects model (Lawlor, 2020).
Level of evidence of the literature
The level of evidence of RCTs starts high. The level of evidence regarding the outcome measure weight loss was downgraded to low because of risk of bias and serious imprecision. There was high risk of bias since blinding of the trials was unclear or not possible, and the results cross the line of clinical relevance
The level of evidence regarding the outcome measure weight maintenance and lifestyle changes were downgraded to very low because of risk of bias and serious imprecision. There was high risk of bias since blinding of the trials was unclear or not possible. Moreover, only one study reported results on weight maintenance and two studies reporting on intentions to physical activity reported different outcome measures (imprecision)
Eating psychopathology included cognitive restraint, emotional eating, binge eating, disinhibition, mindful eating, hunger and body dissatisfaction. Quality of life included depressive symptoms, stress, anxiety and mental health related QoL. The level of evidence regarding the outcome measures eating psychopathology and quality of life were downgraded to very low because of risk of bias, inconsistency and imprecision. There was high risk of bias since blinding of the trials was unclear or not possible. Secondly, the results cross the line of clinical relevance (inconsistency). Finally, due to wide confidence intervals of effect size (imprecision).
Zoeken en selecteren
A systematic review of the literature was performed to answer the following question:
What is the effectiveness of cognitive behavioural therapy added to a combined lifestyle intervention compared to a diet and/or exercise intervention alone in the treatment of adults with overweight and comorbidities or adults with obesity?
P: Adults with obesity (BMI >30 kg/m2) or overweight (BMI ≥25 kg/m2) with comorbidities.
I: Cognitive behavioural therapy: cue-exposure therapy, cognitive therapy, Eye Movement Desensitization Reprocessing (EMDR), schema focussed therapy, Acceptance and Commitment Therapy, mindfulness, stimulus-control therapy, self-control therapy.
C: Combined lifestyle intervention, diet, exercise.
O: Weight (loss), weight maintenance, quality of life (psychological domain if reported), lifestyle changes (nutrition or physical activity), eating psychopathology (binge eating or grazing).
Relevant outcome measures
The guideline development group considered weight loss as a critical outcome measure for decision making; and weight maintenance, lifestyle changes, eating psychopathology and quality of life as an important outcome measure for decision making.
The working group defined the following outcomes as a minimal clinically (patient) important difference.
- Weight loss: 5% weight loss
- Weight maintenance: ≥10% weight loss
- Life style changes, eating psychopathology and quality of life: SMD>0.5
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from the 1st of January 2000 until the 30th of June 2020. An additional systematic search was performed covering literature from 1st of January 2016 until the 6th of October 2020 to select randomized controlled trials (RCTs) published after the search date for SRs. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 311 hits. Studies were selected based on the following criteria: systematic reviews (with meta-analyses), investigating the effect of cognitive behavioural therapy for obesity on weight loss in obese and overweight adults compared to obese and overweight adults receiving placebo. The systematic literature was search was updated to include randomized controlled trials (RCT) published between from the 1st of January 2016 until the 6th of October 2020 resulting in a further 553 hits bringing the total to 864 hits. Of these, Thirty-two studies were initially selected based on title and abstract screening. After reading the full text, 25 studies were excluded (see the table with reasons for exclusion under the tab Methods), and 7 studies were included.
Results
Two systemic reviews were included in the analysis of literature and reported on the impact of cognitive behavioral interventions on weight loss and psychological outcomes in overweight adults or obesity (Jacob, 2018; Lawlor, 2020). Jacob (2018) included 12 randomized controlled trials identified by a systematic search. Lawlor (2020) included 22 randomized controlled trials and 15 studies that used a pre-intervention to post-intervention group design. Three RCTs were included in the analysis of literature of which one reported on the effects of cognitive behavioural interventions on weight loss, quality of life, and psychologic outcomes (Raman, 2018), one RCT reported on the effects of cognitive behavioural therapy (CBT) on weight maintenance after successful weight loss (Madjd, 2020), and one RCT reported on the effect of CBT on intentions for physical activity (Godfrey, 2019).
Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
Referenties
- Cassin, S. E., Sockalingam, S., Du, C., Wnuk, S., Hawa, R., & Parikh, S. V. (2016). A pilot randomized controlled trial of telephone-based cognitive behavioural therapy for preoperative bariatric surgery patients. Behaviour research and therapy, 80, 1722.
- de Graaf, R., Ten Have, M., van Gool, C., & van Dorsselaer, S. (2012). Prevalence of mental disorders and trends from 1996 to 2009. Results from the Netherlands Mental Health Survey and Incidence Study-2. Social psychiatry and psychiatric epidemiology, 47(2), 203-213.
- Godfrey, K. M., Schumacher, L. M., Butryn, M. L., & Forman, E. M. (2019). Physical activity intentions and behavior mediate treatment response in an acceptance-based weight loss intervention. Annals of Behavioral Medicine, 53(12), 1009-1019.
- Jacob, A., Moullec, G., Lavoie, K. L., Laurin, C., Cowan, T., Tisshaw, C., ... & Bacon, S. L. (2018). Impact of cognitive-behavioral interventions on weight loss and psychological outcomes: A meta-analysis. Health Psychology, 37(5), 417.
- Keijsers, G. V., Van Minnen, A., Verbraak, M., Hoogduin, K., & Emmelkamp, P. (2017). Protocollaire behandelingen voor volwassenen met psychische klachten.
- Korrelboom, K. (2011). COMET voor negatief Zelfbeeld: Competitive memory training bij lage zelfwaardering en negatief zelfbeeld Bohn Stafleu van Loghum
- Kwaliteitsstandaard Psychosociale zorg bij somatische ziekte. (2019).
- Lawlor, E. R., Islam, N., Bates, S., Griffin, S. J., Hill, A. J., Hughes, C. A., ... & Ahern, A. L. (2020). Third?wave cognitive behaviour therapies for weight management: A systematic review and network meta?analysis. Obesity Reviews.
- Madjd, A., Taylor, M. A., Delavari, A., Malekzadeh, R., Macdonald, I. A., & Farshchi, H. R. (2019). Effects of cognitive behavioral therapy on weight maintenance after successful weight loss in women; a randomized clinical trial. European Journal of Clinical Nutrition, 1-9.
- Manzoni, G. M., Cesa, G. L., Bacchetta, M., Castelnuovo, G., Conti, S., Gaggioli, A., Mantovani, F., Molinari, E., Cárdenas-López, G., & Riva, G. (2016). Virtual Reality-Enhanced Cognitive-Behavioral Therapy for Morbid Obesity: A Randomized Controlled Study with 1 Year Follow-Up. Cyberpsychology, behavior and social networking, 19(2), 134140.
- Raman, J., Hay, P., Tchanturia, K., & Smith, E. (2018). A randomised controlled trial of manualized cognitive remediation therapy in adult obesity. Appetite, 123, 269-279.
- Zorginstituut (2020). Literatuuronderzoek naar werkzame elementen van een gecombineerde leefstijlinterventie voor personen met een extreem verhoogd gewichtsgerelateerde gezondheidsrisico. Geraadpleegd 1 september 2021, van https://www.zorginstituutnederland.nl/Verzekerde+zorg/gecombineerde-leefstijlinterventie-gli-zvw/documenten/publicatie/2020/03/31/literatuuronderzoek-naar-werkzame-elementen-van-gli-plus
Evidence tabellen
Evidence table for systematic review of RCTs and observational studies (intervention studies)
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Jacob, 2018
|
SR and meta-analysis of RCTs
Literature search up to May 2016
A: Ames, 2005 B: Werrij, 2009 C: Keranen, 2009 D: Cooper, 2010 E: Teixeira, 2010 F: Linde, 2011 G: Pimenta 2012 H: Batra, 2013 I: Pagota,2013 J: Rubin 2014 K: Swencionis, 2013 L: Nurkkala, 2015
Study design: RCT parallel group design (A, B, C, D, E, F, G, H, I, J, K L)
Setting and Country: A: United States B: Netherlands C: Finland D: United Kingdom E: Portugal F: United States G: Portugal H: United States I: United States J: United States K: United States L: Finland
Source of funding and conflicts of interest: Not reported for the individual studies
|
Inclusion criteria SR: RCTs comparing at least one active treatment including a CBT component to either another non-CBT active treatment and/or a waiting list/usual care comparison group in overweight adults without amajor comorbid chronic disease.
Exclusion criteria SR: Observational studies , reviews, editorials, in-progress studies, gray/ unpublished literature, or studies published in a language other than English or French
12 studies included
Important patient characteristics at baseline: N=6.805; median age 46 years (range of average age, 11–59 years); follow-up periods ranged from 4 to 162 months; duration of the interventions ranged from 4 weeks to 48 months (median=26 weeks); the mean number of sessions was 27
N, mean age A: 26 patients, 22 yrs B: 200 patients, 44 yrs C: 49 patients, 50 yrs D: 150 patients, 41 yrs E: 225 patients, 38 yrs F: 203 patients, 52 yrs G: 18 patients, 51 yrs H: 95 patients, 49 yrs I: 161 patients, 46 yrs J: 5.145 patients, 57 yrs K: 474 patients, 52 yrs L: 76 patients, 46 yrs
Sex: A: 100% female B: 84% female C: 74% female D: 100% female E: 100% female F: 100% female G: 100% female H: 73% female I: 100% female J: 59% female K: 82% female L: 71% female
Groups comparable at baseline? Yes |
Describe intervention A: CBT B: CBT C: CBT D: CBT E: CBT F: CBT G: CBT H: CBT I: CBT J: CBT K: CBT L: CBT
|
Describe control A: No CBT B: No CBT C: No CBT D: No CBT E: No CBT F: No CBT G: No CBT H: No CBT I: No CBT J: No CBT K: No CBT L: No CBT
|
End-point of follow-up A: 26 weeks B: 10 weeks C: 20 weeks D: 44 weeks E: 52 weeks F: 26 weeks G: 8 weeks H: 26 weeks I: 26 weeks J: 192 weeks K: 52 weeks L: 36 weeks
For how many participants were no complete outcome data available? (intervention/control) A: 41/67 (61%) B: 4/204 (2%) C: 33/82 (40%) D: 0/150 (0%) E: 0/225 (0%) F: 0/203 (0%) G: 3/21 (14%) H: 38/133 (29%) I: 0/161 (0%) J: 0/5145 (0%) K: 114/588 (19%) L: 44/120 (37%)
|
Outcome weight loss Effect CBT on weight loss; standard mean difference [95% CI: A: SMD=-0.05; (95% CI -0.82, 0.72) B: SMD=-0.01; (95% CI -0.29, 0.26) C: SMD=-0.59; (95% CI -1.17, -0.01) D: SMD=-0.26; (95% CI -0.66, 0.13) E: SMD=-0.89; (95% CI -1.09, -0.70) F: SMD=-0.15; (95% CI -0.43, 0.12) G: SMD=-0.09; (95% CI -0.94, 0.77) H: SMD=-0.45; (95% CI -0.94, 0.04) I: SMD=-0.12; (95% CI -0.43, -0.19) J: SMD=-0.06; (95% CI -0.11, -0.00) K: SMD=-0.27; (95% CI -0.49, -0.04) L: SMD=-0.62; (95% CI -1.17, -0.07)
Pooled effect (random effects model): SMD=-0.30; (95% CI -0.51, -0.09) favouring CBT
Heterogeneity (I2): 86%
Effect CBT on weight loss; raw mean difference kg [95% CI: A: MD=-0.70; (95% CI -10.78, 9.38) B: MD=-0.21; (95% CI -4.40, 3.98) C: MD=-2.60; (95% CI -4.94, -0.26) D: MD=-3.18; (95% CI -7.55, 1.19) E: NA F: MD=-1.00; (95% CI -2.82, 0.82) G: MD=-0.50; (95% CI -5.67, 4.67) H: MD=-9.53; (95% CI -20.15, 1.09) I: MD=-0.70; (95% CI -2.50, 1.10) J: MD=-3.80; (95% CI -7.37, -0.23) K: MD=-1.80; (95% CI -3.31, -0.28) L: MD=-8.40; (95% CI -15.74, -1.06)
Pooled effect (random effects model): SMD=-1.69; (95% CI -2.52, -0.86) favouring CBT
Heterogeneity (I2): 86%
Outcome cognitive restraint Effect CBT on cognitive restraint; standard mean difference [95% CI: A: NA B: SMD=0.09; (95% CI -0.18, 0.37) C: SMD=0.58; (95% CI 0.00, 1.16) D: NA E: SMD=0.47; (95% CI 0.28, -0.66) F: NA G: SMD=1.00; (95% CI 0.09, 1.91) H: SMD=1.36; (95% CI 0.83, 1.88) I: NA J: NA K: NA L: SMD=1.17; (95% CI 0.60, 1.74)
Pooled effect (Random effects model): SMD=0.71; (95% CI 0.33, 1.09) favouring CBT
Heterogeneity (I2): 81%
Outcome emotional eating Effect CBT on emotional eating; standard mean difference [95% CI: A: NA B: NA C: SMD=0.00; (95% CI -0.57, -0.57) D: NA E: SMD=-0.33; (95% CI -0.51, -0.14) F: NA G: SMD=-0.82; (95% CI -1.71, 0.07) H: NA I: NA J: NA K: NA L: SMD=-0.41; (95% CI -0.95, 0.14)
Pooled effect (Random effects model): SMD=-0.32; (95% CI -0.49, 1.09) favouring CBT
Heterogeneity (I2): 0%
Outcome weight depressive symptoms Effect CBT on depressive symptoms; standard mean difference [95% CI: A: SMD=-0.47; (95% CI -1.25, 0.31) B: SMD=-0.03; (95% CI -0.31, 0.25) C: NA D: NA E: NA F: SMD=-0.06; (95% CI -0.33, 0.22) G: SMD=-0.43; (95% CI -1.29, 0.44) H: NA I: SMD=-0.46; (95% CI -0.77, -0.15) J: SMD=-0.02; (95% CI -0.08, -0.03) K: SMD=-0.06; (95% CI -0.27, 0.16) L: NA
Pooled effect (Random effects model): SMD=-0.10; (95% CI -0.21, 0.03) favouring CBT
Heterogeneity (I2): 36%
|
Facultative: The authors conclude that CBTWL may be an efficient intervention for not only weight reduction, but also for psychologically related eating behaviors (i.e., cognitive restraint and emotional eating)
|
|
Lawlor, 2020 |
SR and meta-analysis of RCTs
Literature search up to September 2019
Study design: RCT design (all included studies)
Setting and country: See Table 1; Lawlor (2020) for setting and country of the individual RCTs
Source of funding and conflicts of interest: Not reported for the individual studies
|
Inclusion criteria SR: Adults (≥18 years) with overweight or obesity (BMI ≥25 kg/m2). Studies had to include a 3wCBT intervention for the purpose of weight management. Multi-component interventions were acceptable. Interventions could be of any duration.
Exclusion criteria SR: Not meeting the above inclusion criteria
36 studies included
Important patient characteristics at baseline:
See Table 1; Lawlor (2020) for baseline characteristics of the individual RCTs
|
Describe intervention: - MBCT - ACT - DBT
|
Describe control - SBT - No/minimal
|
End-point of follow-up 2,5 to 24 months. See Table 1; Lawlor (2020) for follow-up duration of the individual RCTs
For how many participants were no complete outcome data available? See Table 1; Lawlor (2020) for the number of participants included in individual RCTs |
Outcome weight loss See Figure 2, Lawlor (2020) for the outcome for each individual RCT
Pooled effect 3wCBT vs no/minimal post-intervention (random effects model): SMD=-0.21; (95% CI -0.44, -0.01).
Heterogeneity (I2): 0%
Pooled effect 3wCBT vs no/minimal 3-months (random effects model): SMD=-0.17; (95% CI -0.75, 0.40).
Heterogeneity (I2): 0%
Pooled effect 3wCBT vs no/minimal 6-months (random effects model): SMD=-0.01; (95% CI -0.46, 0.44).
Heterogeneity (I2): 0%
Pooled effect 3wCBT vs no/minimal 9-months (random effects model): SMD=-0.21; (95% CI -0.46, -0.03).
Heterogeneity (I2): 0%
Pooled effect 3wCBT vs SBT post-intervention (random effects model): SMD=-0.09; (95% CI -0.22, 0.04).
Heterogeneity (I2): 32.4%
Pooled effect 3wCBT vs SBT 3-months (random effects model): SMD=-0.04; (95% CI -0.24, 0.17).
Heterogeneity (I2): 34.1%
Pooled effect 3wCBT vs SBT 6-months (random effects model): SMD=-0.06; (95% CI -0.20, 0.08).
Heterogeneity (I2): 19.1%
Pooled effect 3wCBT vs SBT 9-months (random effects model): SMD=0.11; (95% CI -0.29, 0.51).
Heterogeneity (I2): 40.4%
Pooled effect 3wCBT vs SBT 12-months (random effects model): SMD=-0.17; (95% CI -0.36, 0.02).
Heterogeneity (I2): 33.3%
Pooled effect 3wCBT vs SBT 18-months (random effects model): SMD=-0.12; (95% CI -0.32, 0.08).
Heterogeneity (I2): 0%
Pooled effect 3wCBT vs SBT 24-months (random effects model): SMD=-0.21; (95% CI -0.42, 0.00).
Heterogeneity (I2): 0%
Pooled effect 3wCBT vs SBT 36-months (random effects model): SMD=-0.15; (95% CI -0.44, 0.13).
Heterogeneity (I2): 0%
|
Facultative: The authors conclude that 3wCBT (especially ACT) is an efficient intervention for weight reduction.
|
Evidence table for intervention studies (randomized controlled trials and non-randomized observational studies [cohort studies, case-control studies, case series])1
This table is also suitable for diagnostic studies (screening studies) that compare the effectiveness of two or more tests. This only applies if the test is included as part of a test-and-treat strategy – otherwise the evidence table for studies of diagnostic test accuracy should be used.
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Raman, 2018 |
Type of study: Randomized control trial
Setting and country: Australia
Funding and conflicts of interest: Non-commercial; Diabetes Australia Research Trust; NSW Institute of Psychiatry Fellowship.
One author received royalties from publishers |
Inclusion criteria: Inclusion BMI ≥30 kg/m2, age 18-55 years, current weight <180 kg, ability to provide informed consent and having completed 10 years of education in English.
Participants were recruited from 15th January 2013 to 25th March 2014
Exclusion criteria: history of psychosis, head injury, neurological disorder, diagnosed attention deficit hyperactivity disorder, epilepsy, developmental or intellectual disability; unable to complete the ; were on regular sedative or stimulant medication; and/or report regular substance use or abuse
N total at baseline: Treatment: n=38 Control: n=42
Important prognostic factors2:
Treatment/control age ± SD: 40.6±7.0/42.2±8.8
BMI ± SD 40.3±7.8/39.2±7.4
Weight ± SD 111.7±21.5/108.1±18.)
Depression ± SD 19.1±11.2/13.3±12.2
Mental health related QoL ± SD 46.9±8.4/45.7±9.4
Binge Eating Frequency ± SD 9.3±8.7/9.3±10.6
Groups comparable at baseline? Yes, except for the depression scores, which were higher in the treatment group (p=0.03). |
Describe intervention:
Participants received three weekly sessions of group Behavioural Weight Loss and then were randomised to 8 sessions of individual cognitive remediation therapy n=38)
|
Describe control:
Participants received three weekly sessions of group Behavioural Weight Loss and then were randomised to a no-treatment control group and were instructed to continue their weight loss efforts, but were not instructed how to do this (n=42)
|
Length of follow-up: 3 months
Loss-to-follow-up; n (%): Post therapy Treatment group n=7 (18)
Control: n=1 (2)
3-month follow-up Treatment group n=12 (32)
Control: n=5 (12)
No reason for loss of follow-up described described
Incomplete outcome data: No incomplete data
|
Outcome measures and effect size (include 95%CI and p-value if available):
Post treatment (Treatment/control)
Weight ± SD 108.1± 21.3/111.3± 20.7
Weight change percentage ± SD 0.04± 0.03)/-0.02± 0.04
BMI ± SD 38.9± 7.6/39.7± 8.4)
Depression ± SD 4.5± 5.1/15.4± 12.2
Mental health related QoL ± SD 53.1± 7.6)/ 45.2± 13.4
Binge eating frequency ± SD 3.2± 5.7/11.6±11.9
3 month follow-up (Treatment/control)
Weight ± SD 105.5± 20.7/109.3± 18.9
Weight change percentage ± SD 6.6± 4.0/-1.2± 7.5
BMI ± SD 38.3± 7.6/38.8±8.4
Depression ± SD 5.8± 8.6/11.9± 12.1
Mental health related QoL ± SD 50.5± 10.7/48.3± 12.0
Binge eating frequency ± SD 3.4 ± 6.0/9.2± 10.6 |
The authors conclude that CRT is an efficacious treatment to enhance weight loss, improve cognitive flexibility and reduce binge eating behaviour in individuals with obesity.
Power calculation: Determined based on power estimates using Cohen's tables for an estimated medium effect size of 0.6, power of 0.8, one-tailed test, P < .05 and attrition of 20%. The effect size of 0.6 was considered by the pilot data. One tailed was chosen because expected difference to be only in one direction.
RoB Randomisation and allocation concealment were conducted using an online randomizer. |
|
Forman, 2019 |
Type of study: Randomized control trial
Setting and country: USA
Funding and conflicts of interest: Non-commercial funding, but authors reported receiving royalties from Oxford Press for books on ABT |
Inclusion criteria: Inclusion BMI 27-50 kg/m2; age 18-70 years,
Exclusion criteria: Severe medical or psychiatric conditions; conditions that precluded adherence to the exercise prescription of the program; recent change in dosage of weight-influencing medications; pregnancy; recent weight loss of greater than 5% body weight; binge eating disorder diagnosis
N total at baseline: ABT: n=100 SBT: n=90
Important prognostic factors2: Sex (%) 82.1% female;
Ethnicity (%) Caucasian70.5% ; African American 24.7% ; Hispanic 3.7%; Asian 1.1%;
Age ± SD 51.64±0.73
Groups comparable at baseline? Yes
|
Describe intervention:
Participants were randomly assigned (stratified by gender and ethnicity) to two yearlong ABT (n = 100).
|
Describe control:
Participants were randomly assigned (stratified by gender and ethnicity) to two yearlong SBT (n = 90)
|
Length of follow-up:
Assessments were completed at months 0 (baseline), 6 (midpoint), 12 (posttreatment), 24 (1-year follow-up), and 36 (2-year follow-up).
Loss-to-follow-up; n (%): 12 months (posttreatment) ABT=20 (22) SBT=21 (21)
24 months (1-year follow-up) ABT=5(6) SBT=1 (1)
36 months (2-year follow-up) ABT=4 (4) SBT=4 (4)
Incomplete outcome data: No incomplete data
|
Outcome measures and effect size:
24-months (1 year follow-up) Weight loss (%±SD) ACT=7.5% ± 9.0% SBT=5.6% ± 8.2% (P = 0.15)
Proportion 10% weight loss (%) ACT=34.0 SBT=31.1 (P=0.67; OR = 1.14)
Quality of life (mean ± SD) ACT = 3.70 ± 2.89 SBT = 2.82 ± 3.06 (P<0.01)
Depression (mean ± SD) ABT = 6.85 ± 6.66 SBT = 8.19 ± 7.62 (P=0.32)
36-months (1 year follow-up) Weight loss (%±SD) ABT=7.5% ± 9.0% SBT=4.7% ± 10.1% (P = 0.31)
Proportion 10% weight loss (%) ACT=25.0 SBT=14.4 (P=0.07; OR = 1.97)
Quality of life (mean ± SD) ABT = 3.61 ± 3.05 SBT = 2.76 ± 2.95 (P=0.02)
Depression (mean ± SD) ABT = 6.85 ± 7.18 ± 6.25 SBT = 8.78 ± 7.60 (P=0.15)
|
The authors conclude that SBT for weight loss with acceptance-based strategies enhances weight loss initially, but effects fade in the years following the withdrawal of treatment. Participants receiving ABT were about twice as likely to maintain 10% weight loss at 36 months, and reported higher quality of life.
|
|
Godfrey, 2019 |
Type of study: Randomized control trial
Setting and country: USA
Funding and conflicts of interest: National Institute of Diabetes and Digestive and Kidney Diseases
Authors receive royalties from editing and authoring books on acceptance-based treatment |
Inclusion criteria: Inclusion BMI 27-50 kg/m2; age 18-70 years,
Exclusion criteria: medical/psychiatric conditions that could interfere with intervention engagement or the safety of weight loss, current or planned pregnancy, changes to medications related to weight or appetite in the past 3 months, a weight loss of more than 5% in the 6 months prior to recruitment, prior bariatric surgery, or meeting diagnostic criteria for binge eating disorder
N total at baseline: ABT: n=99 SBT: n=90
Important prognostic factors2:
Female n (%) ABT = 81 (81.8) SBT = 74 (82.2) (P=0.94)
African American n (%) ABT = 22 (22.2) SBT = 23 (25.6) (P=0.29)
White n (%) ABT = 67 (67.7) SBT = 64 (71.1)
Hispanic n (%) ABT = 5 (5.1) SBT = 2 (2.2)
Age M (SD) ABT = 52.0 (9.42) SBT = 51.7 (10.2) (P=0.84)
Baseline BMI Mean (SD) ABT = 36.5 (5.4) SBT = 37.4 (6.2) (P=0.30)
Baseline weight Mean (SD) ABT = 100.0 (18.6) SBT = 101.5 (19.3) (P=0.60)
Groups comparable at baseline? Yes
|
Describe intervention:
Participants (n=90) were assigned to ABT using randomization stratified by gender and ethnicity. Twenty-five 75 min manualized treatment groups were held during the 12 month intervention period with weekly meetings for the first 16 weeks, then tapering to biweekly for five sessions, two monthly sessions, and the remaining two sessions bimonthly.
|
Describe control:
Participants (n=99) were assigned to SBT using randomization stratified by gender and ethnicity.
|
Length of follow-up: 12 months
Loss-to-follow-up; n (%): Physical activity data; n(%) Baseline = 3 (2%)/ Mid treatment = 32(19) End of treatment = 49(26)
Incomplete outcome data: No incomplete data
|
Outcome measures and effect size:
PA = Physical activity MVPA = moderate-to-vigorous physical activity
Mid-treatment PA intention min/week; Mean (SD) ABT = 306.10 (56.03) SBT = 283.26 (62.45)
MVPA min/week; Mean (SD) ABT = 135.34 (107.19) SBT = 124.05 (129.05)
MVPA days/week; Mean (SD) ABT = 3.23 (2.00) SBT = 3.06 (2.12)
MVPA bouts; Mean (SD) ABT = 0.75 (0.60) SBT = 0.81 (0.84)
MVPA min/bout; Mean (SD) ABT = 24.22 (12.04) SBT = 28.68 (12.62)
End of treatment PA intention min/week; Mean (SD) ABT = 274.13 (86.70) SBT = 226.79 (83.36)
MVPA min/week; Mean (SD) ABT = 103.08 (109.08) SBT = 106.88 (135.94))
MVPA days/week; Mean (SD) ABT = 2.69 (2.07) SBT = 2.63 (2.38))
MVPA bouts; Mean (SD) ABT = 0.64 (0.65) SBT = 0.69 (0.80)
MVPA min/bout; Mean (SD) ABT = 24.61 (15.33)) SBT = 24.93 (12.31)
|
The authors conclude that the effect of ABT on weight loss throughout treatment resulted, in part, from participants increasing intentions for PA |
|
Madjd, 2020 |
Type of study: Randomized control trial
Setting and country: Iran
Funding and conflicts of interest: Non-commercial; The School of Life Sciences, The University of Nottingham, UK and The Digestive Disease Research Institute |
Inclusion criteria: BMI 23-30 kg/m2; age 18-45 years; weight loss of at least 10% of body weight within the 6 months before enrollment; premenopausal status.
Inclusion period: March 2015 and October 2015
Exclusion criteria: using medications for blood glucose or lipid control; pregnancy; cancer or chemotherapy/radiotherapy; participation in a competitive sport; abnormal thyroid hormone concentration; intake of medications that could affect body weight and/or energy expenditure; depression; immune-compromised conditions; smoking; cardiovascular disease.
N total at baseline: CBT: n=56 Control: n=57
Important prognostic factors2: W= waist circumference, TC=total cholesterol, TG=triglyceride, FPG=fasting plasma glucose, 2hppG=2 h postprandial glucose, Hb A1C=glycated hemoglobin, HOMA-IR=homeostasis model assessment of insulin resistance
Age; y (SD) CBT = 72.14 (4.39) Control = 71.32 (5.52)
Body weight; kg (SD) CBT = 71.32 (5.52) Control = 72.14 (4.39))
BMI; kg/m² (SD) CBT = 27.56 (1.83) Control =27.68 (1.78)
WC; cm (SD) CBT = 87 (7.35) Control = 88 (6.07)
TC; mmol/l (SD) CBT = 4.26 (0.61) Control = 4.24 (0.63)
HDL-C; mmol/l (SD) CBT = 1.36 (0.21) Control = 1.34 (0.23)
LDL-C; mmol/l (SD) CBT = 2.37 (0.68) Control = 2.34 (0.72)
TG; mmol/l (SD) CBT = 1.48 (0.20) Control = 1.48 (0.16)
FPG; mmol/l (SD) CBT = 4.56 (0.41) Control = 4.70 (0.47)
2hpp; mmol/l (SD) CBT = 6.56 (0.60) Control = 6.55 (0.56)
HA1C; % (SD) CBT = 4.76 (0.40) Control = 4.88 (0.38)
Insulin, m U/l (SD) CBT = 13.64 (2.84) Control = 13.18 (3.31)
HOMA (SD) CBT = 2.85 (0.78) Control = 2.77 (0.83
|
Describe intervention: Participants were randomly assigned after baseline to a CBT group. Participants received CBT classes plus instructions to follow the weight-maintenance diet |
Describe control: Participants were randomly assigned after baseline to a control group. Participants were asked to continue the weight maintenance diet only |
Length of follow-up: 6 months
Loss-to-follow-up; n (%): CBT = 5 (9) 1 participant = relocated 2 participants = time constraint 1 participant = no reason 1 participant = pregnancy
Control = 8(14) 3 participant = dissatisfied with program 2 participants = relocation 1 participant = dissatisfied with diet 1 participant = time constraint
Incomplete outcome data: No incomplete data
|
Outcome measures and effect size:
24 week follow-up Body weight; kg (SD) CBT = 70.05 (4.63) Control = 72.76 (4.30)
BMI; kg/m² (SD) CBT = 27.07 (1.49) Control = 27.91 (1.75)
WC; cm (SD) CBT = 85.13 (5.87) Control = 88.26 (5.83)
Difference between groups; Mean, (95%CI)
Body weight; kg −2.22 (−3.50; −0.94)
BMI; kg/m² −0.77 (−1.25; −0.28)
WC; cm −2.08 (−3.31; −0.84)
|
The authors conclude that cognitive behavioral therapy is an effective tool for weight maintenance over a 24-week period in successful weight losers, with corresponding maintenance of a reduced energy intake and doing more physical activity
Power calculation: The power calculation was based on prior data [α = 0.05, power (1 − β) = 0.85], and was performed on the basis of expected differences in weight loss maintenance between the intervention groups of 1.9 and an SD of 3.2 kg to determine the targeted final sample size (n = 102). When considering a dropout rate of 10%, the sample size required was 113.
RoB: randomized, single-blind, controlled trial. Participants were randomly assigned after baseline measures by using a computer-generated random numbers method by the project coordinator with allocation concealed from the participants and dietitians until the randomization was revealed to the study participants at the initial intervention clinic appointment |
Notes:
- Prognostic balance between treatment groups is usually guaranteed in randomized studies, but non-randomized (observational) studies require matching of patients between treatment groups (case-control studies) or multivariate adjustment for prognostic factors (confounders) (cohort studies); the evidence table should contain sufficient details on these procedures
- Provide data per treatment group on the most important prognostic factors [(potential) confounders]
- For case-control studies, provide sufficient detail on the procedure used to match cases and controls
- For cohort studies, provide sufficient detail on the (multivariate) analyses used to adjust for (potential) confounders
Risk of bias table for systematic reviews of RCTs and observational studies.
|
Study
First author, year |
Appropriate and clearly focused question?1
Yes/no/unclear |
Comprehensive and systematic literature search?2
Yes/no/unclear |
Description of included and excluded studies?3
Yes/no/unclear |
Description of relevant characteristics of included studies?4
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?5
Yes/no/unclear/notapplicable |
Assessment of scientific quality of included studies?6
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?7
Yes/no/unclear |
Potential risk of publication bias taken into account?8
Yes/no/unclear |
Potential conflicts of interest reported?9
Yes/no/unclear |
|
Jacob, 2018 |
Yes |
Yes |
Yes |
Yes |
Not applicable |
Yes |
Yes |
Yes |
Yes |
|
Lawlor, 2020 |
Yes |
Yes |
Yes |
Yes |
Not applicable |
Yes |
Yes |
Yes |
Yes |
- Research question (PICO) and inclusion criteria should be appropriate and predefined
- Search period and strategy should be described; at least Medline searched; for pharmacological questions at least Medline + EMBASE searched
- Potentially relevant studies that are excluded at final selection (after reading the full text) should be referenced with reasons
- Characteristics of individual studies relevant to research question (PICO), including potential confounders, should be reported
- Results should be adequately controlled for potential confounders by multivariate analysis (not applicable for RCTs)
- Quality of individual studies should be assessed using a quality scoring tool or checklist (Jadad score, Newcastle-Ottawa scale, risk of bias table etc.)
- Clinical and statistical heterogeneity should be assessed; clinical: enough similarities in patient characteristics, intervention and definition of outcome measure to allow pooling? For pooled data: assessment of statistical heterogeneity using appropriate statistical tests (e.g. Chi-square, I2)?
- An assessment of publication bias should include a combination of graphical aids (e.g., funnel plot, other available tests) and/or statistical tests (e.g., Egger regression test, Hedges-Olken). Note: If no test values or funnel plot included, score “no”. Score “yes” if mentions that publication bias could not be assessed because there were fewer than 10 included studies.
- Sources of support (including commercial co-authorship) should be reported in both the systematic review and the included studies. Note: To get a “yes,” source of funding or support must be indicated for the systematic review AND for each of the included studies.
Risk of bias table for intervention studies (randomized controlled trials)
|
Study reference
(first author, publication year) |
Describe method of randomisation1 |
Bias due to inadequate concealment of allocation?2
(unlikely/likely/unclear) |
Bias due to inadequate blinding of participants to treatment allocation?3
(unlikely/likely/unclear) |
Bias due to inadequate blinding of care providers to treatment allocation?3
(unlikely/likely/unclear) |
Bias due to inadequate blinding of outcome assessors to treatment allocation?3
(unlikely/likely/unclear) |
Bias due to selective outcome reporting on basis of the results?4
(unlikely/likely/unclear) |
Bias due to loss to follow-up?5
(unlikely/likely/unclear) |
Bias due to violation of intention to treat analysis?6
(unlikely/likely/unclear) |
|
Raman, 2018 |
Randomisation using a random number generator to assign patients to treatment or placebo arms. |
Unlikely Randomisation and allocation concealment were conducted using an online randomizer. |
Likely Lack of blinding of participants and assessor |
Likely Lack of blinding of care providers |
Likely Lack of blinding of participants and assessor |
Unlikely Protocol has been published (Raman, Hay, & Smith, 2014) |
Unlikely Limited loss to follow-up is mentioned
|
Unclear Not mentioned |
|
Godfrey, 2019 |
Randomisation using computer-based random allocation to assign patients to treatment or placebo arms. |
Unclear Not reported |
Unclear Not reported |
Unclear Not reported |
Unclear Not reported |
Unclear Not reported |
Unlikely Limited loss to follow-up is mentioned |
Unclear Not mentioned |
|
Madjd, 2020 |
Randomly assigned after baseline measures by using a computer-generated random numbers method |
Unlikely randomly assigned after baseline measures by using a computer-generated random numbers method by the project coordinator with allocation concealed from the participants and |
Likely Randomization was revealed to the study participants at the initial intervention clinic appointment. |
Likely Randomization was revealed to the study participants at the initial intervention clinic appointment. |
Likely Randomization was revealed after the randomization process |
Unikely Trial conducted as registered on clinicaltrials.gov (NCT02398253) |
Unlikely Limited loss to follow-up is mentioned |
Unlikely All participants who were randomly assigned and completed an initial assessment were included in the final results by using an intention-to-treat analysis.
|
- Randomisation: generation of allocation sequences have to be unpredictable, for example computer generated random-numbers or drawing lots or envelopes. Examples of inadequate procedures are generation of allocation sequences by alternation, according to case record number, date of birth or date of admission.
- Allocation concealment: refers to the protection (blinding) of the randomisation process. Concealment of allocation sequences is adequate if patients and enrolling investigators cannot foresee assignment, for example central randomisation (performed at a site remote from trial location) or sequentially numbered, sealed, opaque envelopes. Inadequate procedures are all procedures based on inadequate randomisation procedures or open allocation schedules.
- Blinding: neither the patient nor the care provider (attending physician) knows which patient is getting the special treatment. Blinding is sometimes impossible, for example when comparing surgical with non-surgical treatments. The outcome assessor records the study results. Blinding of those assessing outcomes prevents that the knowledge of patient assignment influences the process of outcome assessment (detection or information bias). If a study has hard (objective) outcome measures, like death, blinding of outcome assessment is not necessary. If a study has “soft” (subjective) outcome measures, like the assessment of an X-ray, blinding of outcome assessment is necessary.
- Results of all predefined outcome measures should be reported; if the protocol is available, then outcomes in the protocol and published report can be compared; if not, then outcomes listed in the methods section of an article can be compared with those whose results are reported.
- If the percentage of patients lost to follow-up is large, or differs between treatment groups, or the reasons for los to follow-up differ between treatment groups, bias is likely. If the number of patients lost to follow-up, or the reasons why, are not reported, the risk of bias is unclear
- Participants included in the analysis are exactly those who were randomized into the trial. If the numbers randomized into each intervention group are not clearly reported, the risk of bias is unclear; an ITT analysis implies that (a) participants are kept in the intervention groups to which they were randomized, regardless of the intervention they actually received, (b) outcome data are measured on all participants, and (c) all randomized participants are included in the analysis.
Verantwoording
Beoordelingsdatum en geldigheid
Publicatiedatum : 10-07-2023
Beoordeeld op geldigheid : 07-07-2023
Voor het beoordelen van de actualiteit van deze richtlijn is de werkgroep niet in stand gehouden. Uiterlijk in 2027 bepalen Partnerschap Overgewicht Nederland (PON) en Care for Obesity/de Vrije Universiteit Amsterdam, of de modules van deze richtlijn nog actueel zijn. Bij het opstellen van de richtlijn heeft de werkgroep per module een inschatting gemaakt over de maximale termijn waarop herbeoordeling moet plaatsvinden. De geldigheid van de richtlijnmodules komt eerder te vervallen indien nieuwe ontwikkelingen aanleiding zijn om een herzieningstraject te starten.
Het Partnerschap Overgewicht Nederland (PON) en Care for Obesity/de Vrije Universiteit Amsterdam (C4O/VU) zijn respectievelijk regiehouder van het volwassenendeel en het kinderdeel en van de richtlijn. Daarnaast zijn ze eerstverantwoordelijke op het gebied van de actualiteitsbeoordeling van hun deel van de richtlijn. De andere aan deze richtlijn deelnemende wetenschappelijke verenigingen of gebruikers van de richtlijn delen de verantwoordelijkheid en informeren de regiehouder over relevante ontwikkelingen binnen hun vakgebied.
Algemene gegevens
De richtlijnontwikkeling werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten en werd gefinancierd door de Vrije Universiteit Amsterdam en het Ministerie van Volksgezondheid, Welzijn en Sport. De financiers hebben geen enkele invloed gehad op de inhoud van de richtlijn.
Doel en doelgroep
Doel
Het doel van deze richtlijn is bij te dragen aan de verbetering van de ondersteuning en zorg voor volwassenen en kinderen met obesitas of overgewicht in combinatie met risicofactoren en/of comorbiditeit. Deze richtlijn is volgens Medische Specialistische Richtlijnen 2.0 tot stand gekomen, waarin de huidige stand van wetenschappelijke kennis en praktijkervaring aangaande het onderwerp is meegenomen.
De obesitasrichtlijn is ontwikkeld in samenwerking met veel partijen (zie samenstelling werkgroepen en klankbordgroepen) en is bedoeld voor de verschillende bij de ondersteuning en zorg voor obesitas of overgewicht in combinatie met risicofactoren en/of comorbiditeit betrokken beroepsgroepen.
Deze richtlijn gaat over de diagnostiek en behandeling van volwassenen en kinderen met obesitas of overgewicht in combinatie met risicofactoren en/of comorbiditeit. Het betreft hier zorggerelateerde preventie (VWS, 2021).
Deze richtlijn richt zich op de beste diagnostiek, ondersteuning en zorg voor volwassene en kinderen met obesitas, gebaseerd op de meest recente literatuur en expert-/practice-based adviezen. Daarnaast is deze richtlijn relevant voor de geïndiceerde preventie (VWS, 2021) van obesitas bij volwassenen en kinderen. Dit betreft volwassenen en kinderen met overgewicht zonder risicofactoren en/of comorbiditeit.
Hierbij moet worden opgemerkt dat het gezondheidsrisico van overgewicht en obesitas wordt bepaald aan de hand van de BMI in combinatie met wel of geen aanwezigheid van risicofactoren en/of comorbiditeit. De BMI is ingedeeld in categorieën. Echter, de afkappunten van die categorieën zijn niet voor alle groepen precies hetzelfde. De mate van vervetting van het lichaam bij een bepaalde BMI is afhankelijk van het geslacht (vrouwen hebben een hoger vetpercentage dan mannen), de leeftijd (oudere mensen hebben een hoger vetpercentage dan jongere) en de etniciteit (mensen uit Azië hebben een hoger vetpercentage dan Europeanen). Daarnaast kunnen mensen met een grote spiermassa zoals sporters en mensen die zwaar lichamelijk werk doen een lager gezondheidsrisico hebben dan van hun BMI afgeleid kan worden met de bestaande afkappunten. Dit is de reden dat naast de BMI ook de buikomvang van groot belang is bij de bepaling van het gezondheidsrisico bij volwassenen met overgewicht of obesitas (Wharton, 2020).
Doelgroep
Deze richtlijn is primair bedoeld voor de beroepsgroepen die betrokken zijn bij de diagnostiek, ondersteuning en zorg voor volwassenen en kinderen met obesitas of overgewicht in combinatie met risicofactoren en/of comorbiditeit.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijn is in 2019 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van relevante specialismen die betrokken zijn bij de ondersteuning en zorg voor kinderen en volwassenen met obesitas of overgewicht in combinatie met risicofactoren en/of comorbiditeit.
De werkgroepleden zijn door hun beroepsverenigingen gemandateerd voor deelname. De werkgroep is verantwoordelijk voor de integrale tekst van deze richtlijn.
Werkgroep
- Prof. dr. E.F.C. (Liesbeth) Van Rossum, PON, voorzitter
- W. (Wytse) Brongers, KNGF
- S.A. (Sione) Brugman, BLCN – tot februari 2023
- I. (Inge) Out, BLCN – vanaf februari 2023
- B. (Bernadette) Deenen, NVD
- K. (Karen) De Leest, KNMP
- Dr. K. (Karen) Freijer, PON
- E. (Ellen) Govers, NVD
- M. (Marc) Huls, NHG
- F. (Francoise) Langens, huisarts – tot februari 2021
- R.S.L. (Ronald) Liem, NVvH
- Dr. M. (Mattijs) Out, NIV
- E.M.J.N. (Evelyn) Sloots-Jongen, NIP
- N. (Nicolette) Slot, VvOCM
- I. (Inez) van den Anker, Stichting Over Gewicht (patiëntenorganisatie)
- J. (Jacqui) van Kemenade – van Vught, NHG
Klankbordgroep
- I.R.M. (Jurriaan) Blekemolen, NVAB
- Dr. G.J. (Gert-Jan) Braunstahl, NVALT
- D.O.A. (Darie) Daemers, KNOV
- D. (Dorenda) Dijken, NVOG
- S. (Sander) Galjaard, NVOG
- Prof. dr. A. (Annemieke) Hoek, NVOG
- M.M. (Maarten) Hoogbergen, NVPC
- Y.F.C. (Yvo) Kortmann, NVMDL
- P. (Patricia) Lottman, BLCN
- N. (Nienke) van der Putten, Hartstichting
- Dr. G.A.H. (Edgar) van Mil, NVK
- Dr. T.M. (Tessa) van Elten, Voedingscentrum
- Dr. M.E. (Janneke) Wittekoek, NVvC
Met ondersteuning van
- Dr. A.N. (Anh Nhi) Nguyen, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. B. (Bart) Versteeg, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
Overzicht van de belangen van werkgroepleden
|
Achternaam werkgroeplid |
Hoofdfunctie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Van Rossum (voorzitter) |
Internist-endocrinoloog/ hoogleraar Gezond Gewicht en biologisch stressonderzoek in het Erasmus MC |
-Voorzitter Partnerschap Overgewicht Nederland – onbetaald (met in dat kader extra werkzaamheden zoals: *vertegenwoordiger PON bij de tafel Overgewicht voor het Nationaal Preventie Akkoord (onbetaald ) *adviseur keten/netwerkaanpak overgewicht bij volwassenen (tijdelijk betaald) en *lid commissie onderwijs leefstijl en overgewicht in de basiscurricula van zorgprofessionals (onbetaald) -Voorzitter Nationaal Obesitas Symposium – betaald -Bestuurslid stichting STRESS-NL (platform Nederlandse stress onderzoekers)– onbetaald -Lid Koninklijke Hollandsche Maatschappij der Wetenschappen – onbetaald -Lid OPEN Policy working group European Association of the Study of Obesity (sinds Dec 2022) – onbetaald -Lid Voedingsbeleidadviesteam Erasmus MC – onbetaald -Lid Hogeschoolraad – onbetaald -Deelnemer netwerk NL2025 – onbetaald - Jurylid Heineken Award commissie - betaald - Lid voedingsbeleidcommissie Erasmus MC – onbetaald -Spreker /dagvoorzitter bij multipele (inter)nationale en regionale (wetenschappelijke) congressen, webinars, podcasts, media, en nascholingen voor zorgprofessionals. beleidsmakers of algemeen publiek : oa voor Langerhans symposia, Dutch Obesity Academy, Dutch Diabetes Academy, NVE Academy, E-wise, KOEL, SCEM, ASCEND, European Association of the Study of Obesity, International Medical Press, Food First Network, Obesitas Platform, overgewicht.tv, Breedenburg, Het Grote Obesitas Debat, POLITICO Health Care summit EU, European Commission, Diabetes Genootschap Zuid Nederland, Vereniging Arts en Leefstijl, Internistendagen – deels onbetaald en deels betaald (zonder belangenverstrengeling of bemoeienis over wetenschappelijke inhoud door commerciele partijen in geval van betaling).
Afgeronde nevenfuncties: Lid van diverse commissies en wetenschappelijke besturen (onbetaald) |
- In 2019 boek gepubliceerd met co-auteur Mariëtte Boon ""VET belangrijk: feiten en fabels over voeding, vetverbranding en verborgen dikmakers"". Inkomsten naar uitgever Ambo Anthos en boekwinkels en een klein deel naar de auteurs (Mariette Boon en Obesity Science). In 2020 is het boek internationaal gepubliceerd. - Elisabeth Fonds (ondergebracht bij Erasmus MC Trustfonds) financiert de ontwikkeling van de online diagnostische ObesEcare tool om oorzaken overgewicht op te sporen. Het Elisabeth Fonds is een maatschappelijk / charitatief fonds en heeft geen winstoogmerk. - Firma Rhythm financiert een internationale multicenter trial voor een nieuw geneesmiddel (setmelanotide) voor patiënten met een zeldzame vorm van genetische obesitas. - Bezoek aan internationale Masterclass: ''leading the change in the management of Obesity & T2D'', gesponsord door Johnson & Johnson, 2017 (geen honorarium ontvangen) - Actieve bijdrage aan de ontwikkeling van een gespecialiseerde leefstijlinterventie in het Erasmus MC en bij de ontwikkeling van een diagnostische (online) ondersteuningstool voor mensen met overgewicht of obesitas (ook in het Erasmus MC).
|
Geen |
|
Brongers |
Manager fysiotherapie, fysiotherapeut en leefstijlcoach (GLI aantekening). Werkgever: Leidsche Rijn Julius Gezondheidscentra |
Geen |
Geen |
Geen |
|
Brugman |
Zelfstandig Leefstijlcoach |
Bestuurslid BLCN, deel betaald |
Geen |
Geen |
|
De Leest |
Apotheker GHC de Roerdomp Nieuwegein 24 uur Apotheker Geneesmiddel Informatie Centrum KNMP 10 uur |
onbetaald redactie Vascazine/vrijwilliger Vasculitis Vereniging |
Geen |
Geen |
|
Freijer |
Algemeen manager Partnerschap Overgewicht Nederland (PON) ondergebracht bij Erasmus MC te Rotterdam |
- Voorzitter van ISPOR Special Interest Group (SIG) Nutrition Economics. Werkzaamheden: het nieuw opgezette gebied binnen het bestaande gebied van gezondheidseconomie en daarbuiten vergroten.
- Eigenaar van eenmanszaak met naam Freijer4Food & Health Care Activiteitenomschrijving: Geven van lezingen op gebied van voeding; ontwikkelen van kennis/kunde omtrent voedingseconomie (Nutrition Economics); Schrijver/publicist van (wetenschappelijke) artikelen; geven van workshops op bovengenoemd gebied; projectmatig begeleiden van (commerciële) onderzoeken; consultancy op gebied van voeding. |
Geen |
Geen |
|
Govers |
Voorzitter van het NVD netwerk Obesitas (Kenniscentrum Diëtisten Overgewicht en Obesitas; www.KDOO.nl) Dit is een niet betaalde functie |
Vice-voorzitter van de ESDN Obesity van the European Federation of Associations of Dietitians. Een niet betaalde functie |
Geen |
Geen |
|
Langens |
Huisarts |
Ontwikkelen e-learnings/ webinar ( CME-online/accredidact/medonline): betaald Preventieconsult: medische begeleiding bij overgewicht/leefstijl : betaald Huisartsen Eemland: bevorderen wijkgericht werken: betaald Fieldlab obesitas Amersfoort: onbetaald |
Geen |
Geen |
|
Liem |
Gastro-intestinaal en traumachirurg
Groene Hart Ziekenhuis (GHZ) in Gouda (60%) Alrijne Ziekenhuis in Leiderdorp/Alphen ad Rijn (10%) Nederlandse Obesitas Kliniek West in Den Haag (20%) Keizer Kliniek in Voorschoten (10%) |
- Hoofd afdeling chirurgie in GHZ - Voormalig voorzitter Dutch Society for Metabolic and Bariatric Surgery - Lid Auditcommissie (Ned Ver v Heelkunde) - Lid Landelijke Commissie Chirurgische Complicatie Registratie (Ned Ver v Heelkunde) - Clinical Audit Board Audit voor de Behandeling van Obesitas van DICA - Lid Registry Committee of the Internationale Federation for the Surgery of Obesity and Metabolic Disorders - Lid Multi-National Advisory Group of IFSO-European Chapter
Al deze nevenfuncties zijn onbetaald |
Nederlandse Obesitas Kliniek. De chirurgische behandeling van obesitas en obesitas gerelateerde metabole ziekten maakt onderdeel uit van het behandel spectrum. Als ervaren bariatrisch en metabool chirurg maak ik derhalve ondereel uit van deze commissie. De uiteindelijke richtlijn heeft invloed op de positionering van deze behandeling in het behandel spectrum. Voor de chirurgische behandeling zelf, is in 2020 een herziene richtlijn gepubliceerd door de NVVH en het Kennisinstituut. Hiernaar zal worden verwezen in deze Zorgstandaard. Ik heb een beperkt belang in NOK West in Den Haag.
Ik ben daarnaast regelmatig een gevraagde spreker op (internationale) bijeenkomsten en congressen, soms gefaciliteerd door Johnson & Johnson Institute, Medtronic, Gore en Olympus. Daar staat soms een tijdvergoeding tegenover, conform Europese regelgeving. |
Geen |
|
Out |
Internist-vasculair geneeskunde (MST Enschede, fulltime) |
Klinisch Netwerk Obesitas (commissie NVE, lid) |
Van januari t/m juni 2020 heb ik één dag per week onbetaald verlof om de mogelijkheden te exploreren van het opzetten van een leefstijicentrum (bijvoorbeeld als anderhalvelijns centrum, al dan niet in naam van/in samenwerking met het MST). - Deelname aan deze richtlijncommissie kan mijn naam/reputatie als leefstijlarts versterken |
Geen |
|
Out-Hoiting |
Eigenaar Mijn leefstijl op recept
Vice-voorzitter BLCN (deel betaald, deel vrijwillig) |
Geen |
In mijn bedrijf maak ik oa producten voor GLI coaches. Deze coaches hebben belang bij een goed obesitasbeleid waarbij de GLI blijft bestaan. ik ben zelf geen GLI coach meer. |
Geen |
|
Sloots-Jongen |
Klinisch psycholoog bij Maasstad Ziekenhuis |
Geen |
Geen |
Geen |
|
Slot |
VvOCM Nicolette Slot eigen praktijk voor oefentherapie, wandeltrainer en leefstijlcoach |
Oefentherapeut Mensendieck - betaald leefstijlcoach - betaald wandeltrainer - betaald voorzitter Drunens Wandelfestival - niet betaald voorzitter Avond4daagse Drunen - niet betaald |
Geen |
Geen |
|
Van den Anker |
Freelance opdracht HR bij WijzijnMeo (bedrijfsnaam Blue Wolf) Bestuurslid NSOG (Nederlandse stichtijng over gewicht) - Patiëntenorganisatie (onbezoldigd) |
Bestuurslid Pon (onbezoldigd) |
Als bestuurslid van de patiëntenorganisatie voor mensen die leven met obesitas kan de richtlijn ter uitleg en informatie gebruikt worden voor de patiënten |
Geen |
|
Van Kemenade |
Waarnemend huisarts (huisartspraktijk Biesbosch Made) |
Auteur Consult HZG (huisartszorggroep Breda) betaald per uur bij werkzaamheden Creeeren scholingen/presentaties op het gebied Diabetes/leefstijl. Betaald per scholing/presentatie |
Geen |
Geen |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door afgevaardigden van de patiëntenverenigingen in de werkgroepen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan de Nederlandse Stichting Over Gewicht.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Module |
Uitkomst raming |
Toelichting |
|
Cognitieve gedragstherapie |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (>40.000 patiënten), volgt uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse
Tijdens de voorbereidende fase inventariseerden de voorzitters van de werkgroep en de adviseurs knelpunten in de zorg voor kinderen en volwassenen met obesitas of overgewicht in combinatie met risicofactoren en/of comorbiditeit. Tevens zijn er knelpunten aangedragen door AJN Jeugdartsen Nederland, Beroepsvereniging Gewichtsconsulenten Nederland, Beroepsvereniging Leefstijl Coaches Nederland, Care for Obesity (VU Amsterdam), Inspectie voor de Gezondheidszorg en Jeugd, Jongeren op Gezond Gewicht, GGD Har voor Brabant, Amsterdamse Aanpak Gezond Gewicht (GGD Amsterdam), Koninklijk Nederlands Genootschap voor Fysiotherapie, Koninklijke Nederlandse Maatschappij ter bevordering der Pharmacie, Koninklijke Nederlandse Maatschappij ter bevordering van de Tandheelkunde, Landelijke Verenging Medische Psychologie, Landelijke Huisartsen Vereniging, Nederlandse Associatie Physician Assistants, Nederlands Centrum Jeugdgezondheid, Nederlandse Diabetes Federatie, Nederlands Huisartsen Genootschap, Nederlandse Internisten Vereniging, Nederlands Jeugdinstituut, Nederlandse Vereniging van Artsen voor Longziekten en Tuberculose, Nederlandse Vereniging van Diëtisten, Nederlandse Vereniging voor Kindergeneeskunde, Nederlandse Vereniging van Maag-Darm-Leverartsen, Nederlandse Vereniging voor Obstetrie & Gynaecologie, Nederlandse Vereniging voor Cardiologie, Nederlandse Vereniging voor Heelkunde, Nederlandse Vereniging voor Plastische Chirurgie, Partnerschap Overgewicht Nederland, Pharos, Stichting over gewicht, Vereniging Gehandicaptenzorg Nederland, Voedingscentrum, Vereniging Vertrouwensartsen Kindermishandeling, Vereniging van Oefentherapeuten Cesar en Mensendieck, Zorginstituut Nederland en Zelfstandige Klinieken Nederland via een Invitational conference. Een verslag van de Invitational conference is opgenomen in de bijlagen.
Uitgangsvragen en uitkomstmaten
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de voorzitters en de adviseur concept-uitgangsvragen opgesteld. Deze zijn met de werkgroepen besproken waarna de werkgroepen de definitieve uitgangsvragen hebben vastgesteld. Vervolgens inventariseerden de werkgroepen per uitgangsvraag welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. De werkgroepen waardeerden deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerden de werkgroepen ten minste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Strategie voor zoeken en selecteren van literatuur
Er werd voor de afzonderlijke uitgangsvragen aan de hand van specifieke zoektermen gezocht naar gepubliceerde wetenschappelijke studies in (verschillende) elektronische databases. Tevens werd aanvullend gezocht naar studies aan de hand van de literatuurlijsten van de geselecteerde artikelen. In eerste instantie werd gezocht naar studies met de hoogste mate van bewijs. De werkgroepleden selecteerden de via de zoekactie gevonden artikelen op basis van vooraf opgestelde selectiecriteria. De geselecteerde artikelen werden gebruikt om de uitgangsvraag te beantwoorden. De databases waarin is gezocht, de zoekstrategie en de gehanteerde selectiecriteria zijn te vinden in de module met desbetreffende uitgangsvraag.
Gezien de hoge mate van uitval en terugval en daarmee het teruglopen van het percentage succesvolle resultaten na verloop van tijd zijn korte-termijn leefstijlinterventies weinig informatief voor de klinische praktijk. Vanwege het belang van een duurzaam effect zijn bij de selectie van de literatuur daarom alleen studies met een minimale duur van 2 jaar geïncludeerd bij de kinderrichtlijn (Reinehr, 2009).
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur en de beoordeling van de risk-of-bias van de individuele studies is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Samenvatten van de literatuur
De relevante onderzoeksgegevens van alle geselecteerde artikelen werden overzichtelijk weergegeven in evidencetabellen. De belangrijkste bevindingen uit de literatuur werden beschreven in de samenvatting van de literatuur. Bij een voldoende aantal studies en overeenkomstigheid (homogeniteit) tussen de studies werden de gegevens ook kwantitatief samengevat (meta-analyse) met behulp van Review Manager 5.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Formuleren van de conclusies
Voor elke relevante uitkomstmaat werd het wetenschappelijk bewijs samengevat in een of meerdere literatuurconclusies waarbij het niveau van bewijs werd bepaald volgens de GRADE-methodiek. De werkgroepleden maakten de balans op van elke interventie (overall conclusie). Bij het opmaken van de balans werden de gunstige en ongunstige effecten voor de patiënt afgewogen. De overall bewijskracht wordt bepaald door de laagste bewijskracht gevonden bij een van de cruciale uitkomstmaten. Bij complexe besluitvorming waarin naast de conclusies uit de systematische literatuuranalyse vele aanvullende argumenten (overwegingen) een rol spelen, werd afgezien van een overall conclusie. In dat geval werden de gunstige en ongunstige effecten van de interventies samen met alle aanvullende argumenten gewogen onder het kopje 'Overwegingen'.
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk die meegewogen dienen te worden, zoals de expertise van de werkgroepleden, de waarden en voorkeuren van de patiënt (patient values and preferences), kosten, beschikbaarheid van voorzieningen en organisatorische zaken. Deze aspecten worden, voor zover geen onderdeel van de literatuursamenvatting, vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello, 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE-methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module ‘Organisatie van zorg’.
Kennislacunes
Tijdens de ontwikkeling van deze richtlijn is systematisch gezocht naar onderzoek waarvan de resultaten bijdragen aan een antwoord op de uitgangsvragen. Bij elke uitgangsvraag is door de werkgroep nagegaan of er (aanvullend) wetenschappelijk onderzoek gewenst is om de uitgangsvraag te kunnen beantwoorden. Een overzicht van de onderwerpen waarvoor (aanvullend) wetenschappelijk onderzoek van belang wordt geacht, is als aanbeveling in de Kennislacunes beschreven (onder aanverwante producten).
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Brouwers, M. C., Kho, M. E., Browman, G. P., Burgers, J. S., Cluzeau, F., Feder, G., et al. (2010). AGREE II: advancing guideline development, reporting and evaluation in health care. Canadian Medical Association Journal, 182(18), E839-E842.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit.https://richtlijnendatabase.nl/over_deze_site/richtlijnontwikkeling.htMl Ontwikkeling van Medisch Specialistische Richtlijnen: stappenplan. Kennisinstituut van Medisch Specialisten.
Schünemann H., Brożek J., Guyatt G., et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013.
Schünemann, H. J., Oxman, A. D., Brozek, J., Glasziou, P., Jaeschke, R., Vist, G. E., et al. (2008). Rating Quality of Evidence and Strength of Recommendations: GRADE: Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ: British Medical Journal, 336(7653), 1106.
Reinehr, T., Widhalm, K., l'Allemand, D., Wiegand, S., Wabitsch, M., Holl, R. W., & APV‐Wiss Study Group and German Competence Net Obesity. (2009). Two‐year follow‐up in 21,784 overweight children and adolescents with lifestyle intervention. Obesity, 17(6), 1196-1199.
Wessels, M., Hielkema, L., & van der Weijden, T. (2016). How to identify existing literature on patients' knowledge, views, and values: the development of a validated search filter. Journal of the Medical Library Association: JMLA, 104(4), 320.
Wharton, S., Lau, D. C., Vallis, M., Sharma, A. M., Biertho, L., Campbell-Scherer, D., ... & Boyling, E. (2020). Obesity in adults: a clinical practice guideline. CMAJ, 192(31), E875-E891.
Zoekverantwoording
Literature search strategy
|
Clinical question: What is the effectiveness of psychological interventions compared to a diet or exercise intervention alone in the treatment of overweight adults with comorbidities or obese adults? |
|
|
Database(s): Medline, Embase |
Date: 6 October 2020 |
|
Period: 2005 - October 2020 |
Language: English |
|
Database |
Search terms |
|||||||||||||||||||||
|
Embase
|
|
|||||||||||||||||||||
|
Medline (OVID)
|
1 exp overweight/ or obese*.ti,ab,kf. or obesit*.ti,ab,kf. or overweight*.ti,ab,kf. or 'over weight*'.ti,ab,kf. (375531) 2 exp *psychotherapy/ or ((cogniti* or 'cue exposure' or exposure or 'stimulus control' or 'self control' or 'schema focused' or "acceptance and commitment") adj3 (therap* or psychotherap*)).ti,ab,kf. or emdr.ti,ab,kf. or 'eye movement desensiti*ation reprocessing'.ti,ab,kf. or mindfulness.ti,ab,kf. or cbt.ti,ab,kf. (162431) 3 1 and 2 (3051) 4 limit 3 to (english language and yr="2016 -Current") (877) 5 (meta-analysis/ or meta-analysis as topic/ or (meta adj analy$).tw. or ((systematic* or literature) adj2 review$1).tw. or (systematic adj overview$1).tw. or exp "Review Literature as Topic"/ or cochrane.ab. or cochrane.jw. or embase.ab. or medline.ab. or (psychlit or psyclit).ab. or (cinahl or cinhal).ab. or cancerlit.ab. or ((selection criteria or data extraction).ab. and "review"/)) not (Comment/ or Editorial/ or Letter/ or (animals/ not humans/)) (474642) 6 (exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw.) not (animals/ not humans/) (2049459) 7 4 and 5 (100) 8 (4 and 6) not 7 (408) |
|||||||||||||||||||||
|
PsychInfo (OVID) |
1 exp overweight/ or obese*.ti,ab. or obesit*.ti,ab. or overweight*.ti,ab. or 'over weight*'.ti,ab. (44890) 2 exp *psychotherapy/ or ((cogniti* or 'cue exposure' or exposure or 'stimulus control' or 'self control' or 'schema focused' or "acceptance and commitment") adj3 (therap* or psychotherap*)).ti,ab. or emdr.ti,ab. or 'eye movement desensiti*ation reprocessing'.ti,ab. or mindfulness.ti,ab. or cbt.ti,ab. (225423) 3 1 and 2 (1253) 4 limit 3 to (english language and yr="2016 -Current") (275) 5 ((literature review or systematic review or meta analysis).md. or "literature review"/ or meta analysis/ or (((meta adj2 analy*) or metaanaly* or (synthes* adj2 (literature* or research* or studies or data)) or (pooled and analys*) or ((data adj1 pool*) and studies) or cochrane).mp. or (review* or overview).ti. or (bibliograph* or relevant journals or ((review* or overview*) adj9 (systematic* or methodologic* or quantitativ* or research* or literature* or studies or trial* or effective*))).ab.)) not (((retrospective* or record* or case* or patient*) adj1 review*) or ((patient* or review*) adj1 chart*)).ti,ab,id. [mp=title, abstract, heading word, table of contents, key concepts, original title, tests & measures, mesh] (417128) 6 exp randomized controlled trial/ or random*.ti,ab. or ((pragmatic or practical) adj clinical trial*).ti,ab. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab. (204026) 7 4 and 5 (26) 8 (4 and 6) not 7 (88) |