Zuigdrainage na een anatomische longresectie
Uitgangsvraag
Wat is de plaats van zuigdrainage via de thoraxdrain in relatie tot de duur van luchtlekkage na een anatomische longresectie?
Aanbeveling
Gebruik low suction/waterslot (≤ -8 cmH2O) als standaardbenadering voor postoperatief drainbeleid bij anatomische longresecties.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is een literatuuronderzoek verricht naar de vergelijking tussen zuigen aan de drain met lage druk (≤ -8 cmH2O) “low suction” ofwel waterslot, versus zuigen aan de drain met hoge druk, “high suction”, bij volwassen patiënten die een anatomische longresectie ondergaan. Er is één systematische review en er zijn drie RCT’s geïncludeerd die deze vergelijking hebben onderzocht. Voor de cruciale uitkomstmaat thoraxdrainduur werd de grens voor klinische relevantie (1 dag) niet bereikt: er werd wel een verschil van 0.92 dag in de review en 20 respectievelijk 3 uur in de 2 RCT’s gevonden in het voordeel van low suction/waterslot.
Hoewel er dus geen klinisch relevant verschil is bereikt, is het verschil in het voordeel van low suction/waterslot wel significant. Voor het effect op opnameduur geldt dat weliswaar een dag kortere opname wordt gevonden in gepoolde data, maar dat dit niet statistisch significant verschillend is. Opvallend genoeg zijn de criteria waarop thoraxdrains verwijderd worden slecht beschreven in de literatuur.
Voor de cruciale uitkomstmaat re-interventie werd een klinisch relevant verschil gevonden voor patiënten die low suction/waterslot ontvingen ten opzichte van patiënten die hoge druk ontvingen. Voor de belangrijke uitkomstmaten werd gevonden dat een lager aantal patiënten dat low suction/waterslot ontving overleed. Daarnaast lieten studies conflicterende resultaten zien voor opnameduur in het ziekenhuis en complicaties. De complicatie verlengde luchtlek kwam vaker voor bij patiënten die high suction ontvingen ten opzichte van patiënten die lage druk ontvingen, terwijl de complicatie pneumothorax vaker voor kwam bij patiënten die lage druk ontvingen ten opzichte van patiënten die hoge druk ontvingen. Voor zowel de cruciale als de belangrijke uitkomstmaten was de bewijskracht laag tot zeer laag, hier ligt dus een kennislacune. De lage bewijskracht werd met name veroorzaakt door resultaten van lage precisie en beperkingen van de studies.
Door de zeer lage bewijskracht zal de keuze voor het low suction/waterslot of high suction aan de drain dus afhangen van andere factoren.
De bevindingen halen de van tevoren vastgestelde klinische grenzen niet altijd, of halen ze wel zonder dat statistische significantie wordt bereikt. De bevindingen zijn echter vrijwel consistent in het voordeel van low suction/waterslot; alleen bij reïnterventies is er een niet significant voordeel voor high suction.
Vanuit de redenatie dat een negatief drukverschil over een defect in longparenchym zorgt voor luchtstroom door dit defect en daarmee sluiten tegengaat, is het voordeel van low suction/waterslot te verklaren. In gevallen waarbij sprake is van stijf longparenchym, bijvoorbeeld na inductiebehandeling, of bij fors luchtlek, waarbij de long niet goed ontplooit of invaliderend subcutaan emfyseem optreedt, kan gekozen worden om alsnog zuigdrainage toe te passen in plaats van low suction/waterslot. Hierbij wordt ervanuit gegaan dat het tegen elkaar brengen van de long en thoraxwand het sluiten van de parenchymlekkage bevordert, en dat zuigdrainage de morbiditeit van eventueel subcutaan emfyseem beperkt.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Belang van een zo kort mogelijke thoraxdrainage, gecombineerd met een lage kans op reïnterventies en complicaties, is gelijk voor patiënten en zorgverleners. De trend is in het voordeel van de low suction/waterslot benadering. Veranderingen in drainbeleid dienen vanzelfsprekend consistent te worden gecommuniceerd met patiënt, en binnen het behandelteam. Gezien het wijdverspreide gebruik van digitale drainsystemen is de impact op de mogelijkheid te mobiliseren bij verschillende zuigdrainage zeer beperkt. Analoge systemen op zuigdrainage vergen echter verbinding met een vacuüm slang aan de muur en beperken mobilisatie wel.
Kosten (middelenbeslag)
De weerslag op de kosten bestaat voornamelijk uit de kosten die voortkomen uit duur van opname en de kans op complicaties. De tendens lijkt in het voordeel van low suction/waterslot.
Aanvaardbaarheid, haalbaarheid en implementatie
Beide benaderingen (high en low suction) zijn breed aanvaarde strategieën. Hoewel de gestelde grenzen voor klinische relevantie niet worden gehaald, is de tendens consistent in het voordeel van low suction/waterslot met betrekking tot drainage duur en opname duur; effect op gepoolde complicaties is onduidelijk. In lijn met het ERAS® principe van marginal gains, tellen alle kleine effecten van perioperatieve maatregelen op tot een gezamenlijk groter positief effect op postoperatief herstel; low suction/waterslot als uitgangspunt voor drainbeleid lijkt vanuit die gedachte goed te rechtvaardigen. Eerdere argumenten voor het inzetten van zuigdrainage (stijf longparenchym, bijvoorbeeld na inductiebehandeling, of bij fors luchtlek) kunnen dan argumenten zijn voor afwijking van de standaard benadering (low suction/waterslot).
De meerwaarde van een eenduidige keuze voor benadering van drainbeleid is ook duidelijkheid voor behandelteam; dit komt de consistente communicatie met patiënt ten goede. De wijdverspreide beschikbaarheid van digitale drainagesystemen zorgt dat beide strategieën zonder beperkingen voor de patiënt uitvoerbaar zijn. Zuigdrainage gaat bij analoge systemen gepaard met een beperking van de mobiliteit van de patiënt. Bij gebruik van analoge systemen is dit een extra argument tegen zuigdrainage.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Hoewel de gestelde grenzen voor klinische relevantie niet worden gehaald, is de tendens consistent in het voordeel van low suction/waterslot met betrekking tot drainage duur en opname duur. In lijn met het ERAS® principe van marginal gains, tellen alle kleine effecten van perioperatieve maatregelen, zoals low suction/waterslot, op tot een gezamenlijk groter positief effect op postoperatief herstel; low suction als uitgangspunt voor drainbeleid lijkt vanuit die gedachte goed te rechtvaardigen.
Onderbouwing
Een van de belangrijkste barrières in herstel na anatomische longresecties is de aanwezigheid van een thoraxdrain. Aangezien langere drainageduur geassocieerd is met pijn, verminderde longfunctie, verminderd mobiliseren van patiënten en geassocieerd is met langere opnameduur, is het van groot belang een zo kort mogelijke drainageduur na te streven (Refai, 2012). In een enquête van von Meyenfeldt (2020) blijkt een aanzienlijke praktijkvariatie ten aanzien van drainbeleid rondom anatomische longresecties. In deze module kijken we naar welke strategie ten aanzien van luchtlekkage ertoe leidt dat de thoraxdrain veilig en zo snel mogelijk verwijderd kan worden. De hoofdvraag hierbij is: zorgt zuigdrainage ervoor dat een drain eerder verwijderd kan worden in vergelijking met alleen waterslot.
|
Low GRADE |
Low suction (water seal, ≤ -8 cmH2O) may reduce the length of chest drain duration when compared to high suction (> -8 cmH2O) in adult patients undergoing curative lung resection. Sources: Zhou, 2019; Holbek, 2019; Lijkendijk, 2019 |
|
Very low GRADE |
The evidence is very uncertain about the effect low suction (water seal, ≤ -8 cmH2O on reinterventions when compared with high suction (> -8 cmH2O) in adult patients undergoing curative lung resection. Source: Holbek, 2019 |
|
Very low GRADE |
The evidence is very uncertain about the effect low suction (water seal, ≤ -8 cmH2O on complications when compared with high suction (> -8 cmH2O) in adult patients undergoing curative lung resection. Source: Holbek, 2019; Lijkendijk, 2019; Zhou, 2019 |
|
Low GRADE |
Low suction (water seal, ≤ -8 cmH2O) may reduce the length of stay when compared with high suction (> -8 cmH2O) in adult patients undergoing curative lung resection. Source: Zhou, 2019; Cui, 2019; Holbek, 2019; Lijkendijk, 2019 |
|
Very low GRADE |
The evidence is very uncertain about the effect low suction (water seal, ≤ -8 cmH2O) on readmission rate when compared with high suction (> -8 cmH2O) in adult patients undergoing curative lung resection. Source: Holbek, 2019 |
|
No GRADE |
No evidence was found regarding the effect of low suction (water seal, ≤ -8 cmH2O) on quality of life when compared with high suction (> -8 cmH2O) in adult patients undergoing curative lung resection. Source: - |
|
No GRADE |
No evidence was found regarding the effect of low suction (water seal, ≤ -8 cmH2O) on functional recovery when compared with high suction (> -8 cmH2O) in adult patients undergoing curative lung resection. Source: - |
Description of studies
The systematic review by Zhou (2019) investigated the effect of suction added to simple water-seal drainage following pulmonary surgery on different postoperative outcomes. Randomized controlled trials studying patients who had undergone pulmonary surgery, comparing the addition of suction drainage and simple water-seal were eligible for inclusion. If essential information was incomplete, if the article was a conference abstract, letter, review, case report, or animal experiment, or if the article was written in another language than English, it was excluded. Electronic searches were performed in PubMed, EMBASE, and Web of Science from the date of their inception to 30 August 2017. Data of 10 published randomized controlled trials, including a total of 1568 patients were included. The included studies were RCTs performed in Italy (n=3), USA (n=2), UK (n=1), Kuwait (n=1), Poland (n=1), Iran (n=1), and Greece (n=1). Meta-analyses were performed in the systematic review. Subgroup analyses were performed for ethnicity, drainage volume for removal, and the definition of prolonged air leak. Important limitations of the current review were the heterogeneity among the included studies, high risk of bias in three of the included studies, lack of standard procedure for chest tube management, and insufficient sample size for some of the data items. The study reported the following relevant outcome measures: chest drain duration and length of stay.
Cui (2019) performed a single-center randomized trial to compare the use of a commonly used chest tube with water-sealed bottle without negative pressure suction with the use of a drainage ball with low negative pressure suction (about 10 kpa, which will decrease when the drainage ball is filled). Patients undergoing lobectomy by video-assisted thoracic surgery (VATS), with age between 30 and 70 years, and a diagnosis of invasive carcinoma by frozen section were eligible for trial participation. In total, 60 patients were eligible and were randomized into two groups. The intervention group (n=30) received a drainage ball with the function of negative pressure suction at the end of the lobectomy procedure. The control group (n=30) received a commonly used chest tube without negative pressure suction at the end of the lobectomy procedure. The duration of the follow-up was not reported. The study reported the following relevant outcome measures: chest drain duration, length of stay, and complications.
Holbek (2019) performed a single-center, parallel-arm, randomized controlled trial to assess the potential benefits of low chest drain suction of -2 cm H2O compared to high chest drain suction of -10 cm H2O, with the use of a digital draining device. Patients 18 years or older, able to speak and understand Danish, able to give informed consent, and scheduled to undergo video-assisted thoracic surgery (VATS) lobectomy for suspected or confirmed primary lung cancer were eligible for trial participation. In total, 230 patients were eligible and were randomized into two groups. The intervention group (n=115) received low chest drain suction of -2 cm H2O. The control group (n=115) received high chest drain suction of -10 cm H2O. The duration of the follow-up was until postoperative day 30. The study reported the following relevant outcome measures: chest drain duration, length of stay, complications, reoperation, overnight readmission, and mortality.
Lijkendijk (2019) performed a single-center, open-labelled, randomized trial to compare low suction to chest drains with high suction to chest drains in patients undergoing lobectomy. Patients admitted for standard lobectomy, older than 18 years of age, and able to give informed consent were eligible for trial participation. In total, 106 patients were eligible and were randomized into two groups. The intervention group (n=53) received low variable suction of -5 cm H2O on a digital drainage device. The control group (n=53) received high variable suction of -20 cm H2O on a digital drainage device. The duration of the follow-up was not reported. The study reported the following relevant outcome measures: chest drain duration and length of stay.
Results
Chest drain duration (critical)
Three studies reported the outcome measure chest drain duration (Holbek 2019, Lijkendijk 2019, Zhou 2019). As Holbek (2019) and Lijkendijk (2019) used a different measurement unit, the results were not pooled with the results from Zhou (2019).
Zhou (2019) reported the duration of chest tube drainage in days. In total 401 patients received low suction or no suction and 397 patients received high suction. Pooled data from these results showed a pooled mean difference of 0.92 days (95% CI 0.04 to 1.81), in favour of the patients who received low suction or no suction (Figure 1). This difference is not considered clinically relevant.
Holbek (2019) reported the drainage duration in hours. The patients who received low suction (n=111) had a median drainage duration of 27.4 hours (IQR 23.3-71.2), and the patients who received high suction (n=111) had a median drainage duration of 47.5 hours (IQR 24.5-117.8). The difference in medians was -20.1 hours, in favour of the patients who received low suction. This difference is not considered clinically relevant.
Lijkendijk (2019) also reported the chest drain duration in hours. The patients who received low suction (n=53) had a median chest drain duration of 25 hours (IQR 21-55), and the patients who received high suction (n=53) had a median chest drain duration of 28 hours (23-77). The difference in medians was -3 hours, in favour of the patients who received low suction. This difference is not considered clinically relevant.
Figure 1. Chest drain duration
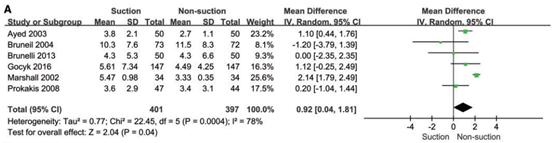
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval, from Zhou 2019.
Re-intervention (critical)
One study reported the outcome measure re-intervention (Holbek 2019). Holbek (2019) reported the number of patients that underwent a reoperation. In total, 2 of the 111 patients (1.8%) who received low suction, underwent a reoperation, versus 7 of the 111 patients (6.3%) who received high suction. The risk ratio (RR) was 0.29 (95% CI 0.06 to 1.35), in favour of the patients who received low suction. This difference is considered clinically relevant.
Complications (important)
Prolonged air leak
Three studies reported the outcome measure prolonged air leak (>5 days) (Holbek, 2019; Lijkendijk, 2019; Zhou, 2019).
Zhou (2019) reported prolonged air leak >5 to >8 days. Holbek (2019) and Lijkendijk (2019) reported prolonged air leak >5 days. In total, 110 of the 970 patients who received low suction had a prolonged air leak, versus 131 of the 959 patients who received high suction had a prolonged air leak. Pooled data from these results showed a pooled risk ratio of 0.77 (95% CI 0.53 to 1.11), in favour of the patients who received low suction (Figure 2). This difference is considered clinically relevant.
Figure 2. Prolonged air leak
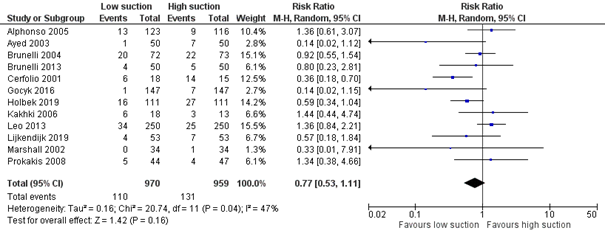
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval.
Cardiopulmonary complications
One study reported the outcome measure cardiopulmonary complications, including pneumonia, empyema, atelectasis, arrhythmia, and bleeding (Zhou, 2019). Pooled data from the results from three studies, including 745 patients, showed a pooled risk ratio of 0.65 (95% CI 0.48 to 0.89), in favour of the patients who received low suction or no suction. This difference is considered clinically relevant.
Holbek (2019) reported the outcome measure pneumonia. In total, 11 of the 111 patients (9.9%) who received low suction had pneumonia, and 10 of the 111 patients (9.0%) who received high suction had pneumonia. The risk ratio was 1.10 (95% CI 0.49 to 2.48), in favour of the patients who received high suction. This difference is not considered clinically relevant.
Holbek (2019) reported the outcome measure empyema. In total, 2 of the 111 patients (1.8%) who received low suction had empyema, and 0 of the 111 patients (0%) who received high suction had empyema. The risk ratio was 5.00 (95% CI 0.24 to 102.97), in favour of the patients who received high suction. This difference is considered clinically relevant.
Pneumothorax requiring drain re-insertion
One study reported the outcome measure pneumothorax requiring drain re-insertion (Holbek, 2019).
Holbek (2019) reported pneumothorax/subcutaneous emphysema requiring drain reinsertion. In total, 10 of the 111 (9.0%) patients who received low suction had pneumothorax or subcutaneous emphysema requiring drain reinsertion, and 6 of the 111 (5.4%) patients who received high suction had pneumothorax or subcutaneous emphysema requiring drain reinsertion. The risk ratio was 1.67 (95% CI 0.63 to 4.43), in favour of the patients who received high suction. This difference is considered clinically relevant.
Length of stay (important)
Four studies reported the outcome measure length of stay (Cui 2019, Holbek 2019, Lijkendijk 2019, Zhou 2019).
Zhou (2019) and Cui (2019) reported length of stay in days. In total, 280 patients received low suction and 284 patients received high suction. Pooled data from these results showed a pooled mean difference of -1.12 days (95% CI -3.13 to 0.88), in favour of the patients who received low suction (Figure 3). This difference is considered clinically relevant.
Figure 3. Length of stay
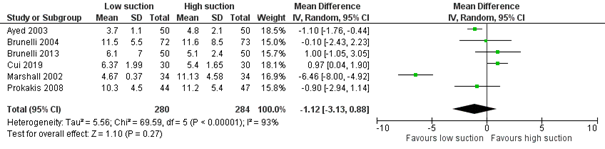
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval.
Holbek (2019) reported length of in-hospital stay in days. The patients who received low suction (n=111) had a median length of in-hospital stay of 2.0 days (IQR 2.0-5.8), and the patients who received high suction (n=111) had a median length of in-hospital stay of 3.0 days (IQR 2.0-9.0). The difference in medians was -1.0 days, in favour of the patients who received low suction. This difference is considered clinically relevant.
Lijkendijk (2019) reported length of stay in days. The patients who received low suction (n=53) had a median length of stay of 5 days (IQR 3-6), and the patients who received high suction (n=53) had a median length of stay of 5 days (IQR 3-7). This means there was no difference between the group that received low suction and the group that received high suction.
Readmission (important)
One study reported the outcome measure readmission (Holbek 2019). Holbek (2019) reported the number of patients that were readmitted overnight. In total, 17 of the 111 patients (15.3%) who received low suction were readmitted overnight, and 16 of the 111 patients (14.4%) who received high suction were readmitted overnight. The RR was 1.06 (95% CI 0.57 to 1.99), in favour of the patients who received high suction. This difference is not considered clinically relevant.
Quality of life (important)
None of the studies reported the outcome measure quality of life.
Functional recovery (important)
None of the studies reported the outcome measure recovery.
Level of evidence of the literature
The level of evidence regarding the outcome measure chest drain duration was based on RCTs and therefore starts high. The level of evidence was downgraded by 2 levels because of study limitations (risk of bias, -1), and because the confidence interval exceeds the levels for clinical relevance (imprecision, -1). The level of evidence is therefore low.
The level of evidence regarding the outcome measure re-intervention was based on an RCT and therefore starts high. The level of evidence was downgraded by 3 levels because of study limitations (risk of bias, -1), and because the confidence interval exceeds both levels for clinical relevance (imprecision, -2). The level of evidence is therefore very low.
The level of evidence regarding the outcome measure complications was based on RCTs and therefore starts high. The level of evidence was downgraded by 4 levels because of study limitations (risk of bias, -1), because the confidence interval exceeds the levels for clinical relevance (imprecision, -2), and because of conflicting results (inconsistency, -1). The level of evidence is therefore very low.
The level of evidence regarding the outcome measure length of stay was based on RCTs and therefore starts high. The level of evidence was downgraded by 2 levels because of study limitations (risk of bias, -1), and because the confidence interval exceeds the levels for clinical relevance (imprecision, -1). The level of evidence is therefore low.
The level of evidence regarding the outcome measure readmission was based on an RCT and therefore starts high. The level of evidence was downgraded by 3 levels because of study limitations (risk of bias, -1), and because the confidence interval exceeds both levels for clinical relevance (imprecision, -2). The level of evidence is therefore very low.
The level of evidence regarding the outcome measure quality of life could not be graded, as the included studies did not report this outcome measure.
The level of evidence regarding the outcome measure functional recovery could not be graded, as the included studies did not report this outcome measure.
A systematic review of the literature was performed to answer the following question:
What are the (un)favorable effects of drain suction compared to low suction in patients who have undergone an anatomical lung resection in the context of a curative treatment for lung cancer?
P: patients patients (>18 years) who have undergone an anatomical lung
resection in the context of a curative treatment for lung cancer
I: intervention low suction (water seal) (≤ -8 cmH2O)
C: control high suction (> -8 cmH20)
O: outcome measure chest drain duration, complications, re-interventions, length of
stay, readmissions, quality of life, functional recovery
Relevant outcome measures
The guideline development group considered chest drain duration and re-interventions as a critical outcome measure for decision making; and complications, length of stay, quality of life and functional recovery as an important outcome measure for decision making.
A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
The working group defined the following differences as minimal clinically (patient) important differences:
- Complications: 10% (RR < 0.90 or > 1.10)
- Number of re-interventions: 10% (RR < 0.90 OR > 1.10)
- Length of hospital stay: 1 day
- Chest drain duration: 1 day
- Readmissions: 10% (RR < 0.90 or > 1.10)
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 01-11-2022. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 306 hits. Studies were selected based on the following criteria: systematic reviews or RCTs comparing low suction versus high suction in patients who have undergone an anatomical lung resection in the context of a curative treatment. 17 studies were initially selected based on title and abstract screening. After reading the full text, 13 studies were excluded (see the table with reasons for exclusion under the tab Methods), and four studies were included.
Results
Four studies were included in the analysis of the literature. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Cui Z, Zhang Y, Xu C, Ding C, Chen J, Li C, Zhao J. Comparison of the results of two chest tube managements during an enhanced recovery program after video-assisted thoracoscopic lobectomy: A randomized trial. Thorac Cancer. 2019 Oct;10(10):1993-1999. doi: 10.1111/1759-7714.13183. Epub 2019 Sep 2. PMID: 31475791; PMCID: PMC6775025.
- Holbek BL, Christensen M, Hansen HJ, Kehlet H, Petersen RH. The effects of low suction on digital drainage devices after lobectomy using video-assisted thoracoscopic surgery: a randomized controlled trial. Eur J Cardiothorac Surg. 2019 Apr 1;55(4):673-681. doi: 10.1093/ejcts/ezy361. PMID: 30445572.
- Lijkendijk M, Licht PB, Neckelmann K. The Influence of Suction on Chest Drain Duration After Lobectomy Using Electronic Chest Drainage. Ann Thorac Surg. 2019 Jun;107(6):1621- 1625. doi: 10.1016/j.athoracsur.2018.12.059. Epub 2019 Feb 8. PMID: 30742815.
- Refai M, Brunelli A, Salati M, Xiumè F, Pompili C, Sabbatini A. The impact of chest tube removal on pain and pulmonary function after pulmonary resection. Eur J Cardiothorac Surg. 2012 Apr;41(4):820-2; discussion 823. doi: 10.1093/ejcts/ezr126. Epub 2011 Dec 21. PMID: 22219425.
- von Meyenfeldt EM, de Betue CTI, van den Berg R, van Thiel ERE, Schreurs WH, Marres GMH. Wide Variation in Perioperative Care in Anatomical Lung Resections in the Netherlands: A National Survey. Semin Thorac Cardiovasc Surg. 2020 Winter;32(4):1101-1110. doi: 10.1053/j.semtcvs.2020.05.015. Epub 2020 May 23. PMID: 32454091.
- Zhou J, Chen N, Hai Y, Lyu M, Wang Z, Gao Y, Pang L, Liao H, Liu L. External suction versus simple water-seal on chest drainage following pulmonary surgery: an updated meta- analysis. Interact Cardiovasc Thorac Surg. 2019 Jan 1;28(1):29-36. doi: 10.1093/icvts/ivy216. PMID: 30052997.
Evidence tables
Systematic review:
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Zhou, 2019
[Individual study characteristics deduced from Zhou, 2019]
|
SR and meta-analysis of 10 randomized controlled trials
Literature search up to 30 August 2017
A: Alphonso, 2005 B: Ayed, 2003 C: Brunelli, 2004 D: Brunelli, 2013 E: Cerfolio, 2001 F: Gocyk, 2016 G: Kakhki, 2006 H: Leo, 2013 I: Marshall, 2002 J: Prokakis, 2008
Study design: SR of 10 RCTS
Setting and country: (Retrieved from individual studies) A: UK B: Kuwait C: Italy D: Italy E: USA F: Poland G: Iran H: Italy I: USA J: Greece
Source of funding: The study was supported by the National Natural Science Foundation of China and the Key Science and Technology Program of Sichuan Province, China.
Conflicts of interest: None declared. |
Inclusion criteria SR: Randomized controlled trials, focussing on patients who had undergone pulmonary surgery, comparing the addition of suction drainage and simple water-seal.
Exclusion criteria SR: Essential information being incomplete, the article being conference abstracts, letters, reviews, case reports, and animal experiments, the article written in another language than English.
10 studies included
Important patient characteristics at baseline:
Sample size (n): A: 239 B: 100 C: 145 D: 100 E: 33 F: 294 G: 31 H: 500 I: 68 J: 91
Type of surgery: A: Lung surgery B: VATS C: Lobectomy D: Lobectomy E: Lung surgery F: Lung surgery G: Lung surgery H: Lung resection I: Lung resection J: Lobectomy
Initial suction: A: No B: No C: Yes D: NA E: NA F: Yes G: Yes H: Yes I: Yes J: No |
Intervention: Simple water-seal with additional suction on chest drains.
Suction pressure (cmH2O): A: -20 B: -20 C: -20 D: -11 to -20 E: -20 F: -20 G: -10 to -18 H: -15 I: -20 J: -15 to -20 |
Control: simple water-seal on chest drains without additional suction.
|
End-point of follow-up:
Not reported.
For how many participants were no complete outcome data available?
Not reported. |
Prolonged air leak occurrence: Defined as: from more than 5 to more than 8 days.
RR [95% CI] A: 0.73 [95% CI 0.33 to 1.65] B: 7.00 [95% CI 0.89 to 54.83] C: 1.08 [95% CI 0.65 to 1.81] D: 1.25 [95% CI 0.36 to 4.38] E: 2.80 [95% CI 1.44 to 5.46] F: 7.00 [95% CI 0.87 to 56.19] G: 0.69 [95% CI 0.21 to 2.27] H: 0.74 [95% CI 0.45 to 1.20] I: 3.00 [95% CI 0.13 to 71.15] J: 0.75 [95% CI 0.21 to 2.61]
Pooled effect (random effects model): RR 1.23 [95% CI 0.79 to 1.92] favoring non-suction. Heterogeneity (I2): 52%
Postoperative pneumothorax: RR [95% CI] A: 0.71 [95% CI 0.12 to 4.15] B: 0.06 [95% CI 0.00 to 0.99] E: 0.11 [95% CI 0.01 to 1.81] I: 0.11 [95% CI 0.01 to 1.99] J: 0.62 [95% CI 0.24 to 1.61]
RR 0.35 [95% CI 0.13 to 0.93] favoring suction. Heterogeneity (I2): 24%
Duration of chest tube drainage: Mean Difference [95% CI] B: 1.10 [95% CI 0.44 to 1.76] C: -1.20 [95% CI -3.79 to 1.39] D: 0.00 [95% CI -2.35 to 2.35] F: 1.12 [95% CI -0.25 to 2.49] I: 2.14 [95% CI 1.79 to 2.49] J: 0.20 [95% CI -1.04 to .44]
Pooled effect (random effects model): MD 0.92 [95% CI 0.04 to 1.81] favoring non-suction. Heterogeneity (I2): 78%
Air leak duration: Mean Difference [95% CI] C: -0.20 [95% CI -2.59 to 2.19] D: 0.26 [95% CI -0.65 to 1.17] F: 0.59 [95% CI -0.37 to 1.55] I: 1.77 [95% CI 1.48 to 2.06]
Pooled effect (random effects model): MD 0.81 [95% CI -0.21 to 1.82] favoring non-suction. Heterogeneity (I2): 81%
Hospital stay (days): Mean Difference [95% CI] B: 1.10 [95% CI 0.44 to 1.76] C: 0.10 [95% CI -2.23 to 2.43] D: -1.00 [95% CI -3.05 to 1.05] I: 6.46 [95% CI 4.92 to 8.00] J: 0.90 [95% CI -1.14 to 2.94]
Pooled effect (random effects model): MD 1.57 [95% CI -0.83 to 3.98] favoring non-suction. Heterogeneity (I2): 92%
Cardiopulmonary complications: Pooled effect (random effects model): RR 0.65 [95% CI 0.48 to 0.89] favoring non-suction. Heterogeneity (I2): 0% |
The authors concluded that additional suction to water-seal on chest drains made no difference for the outcome measures prolonged air leak duration and hospital stay. In patients with postoperative pneumothorax additional suction was favoured, and for hospital stay non-suction was favoured.
Incomplete outcome data addressed: low risk of bias in all RCTs.
No GRADE performed.
Sensitivity analysis: No significant discoveries were identified in the sensitivity analyses.
Subgroup analysis: subgroup analyses were performed ethnicity, drainage volume threshold for removal, and the definition of prolonged air leak. No significant difference was identified in subgroup analyses. |
RCTs:
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Cui, 2019 |
Single center randomized trial
Setting and country: The First Affiliated Hospital of Soochow University, Suzhou, China
Source of funding: Funded by the National Natural Science Foundation of China.
Conflicts of interest: None declared. |
Inclusion criteria: Lobectomy by video-assisted thoracic surgery (VATS), age range from 30 to 70 years, and a diagnosis of invasive carcinoma by frozen section.
Exclusion criteria: Previous history of pulmonary surgery, severe pulmonary or cardiac disease, metastasis, and serious pleural adhesions.
N total at baseline: Intervention: 30 Control: 30
Important prognostic factors2: Age ± SD: Intervention: 57.03 ± 9.74 Control: 55.53 ± 8.79
Sex (male): Intervention: 13 Control: 12
FEV 1 (%): Intervention: 81.03 ± 11.30
Blood loss (mL): Intervention: 51.33 ± 23.15 Control: 47.33 ± 23.81
Lobes removed (left upper lobe/left lower lobe/right upper lobe/right lower lobe): Intervention: 9/5/10/6 Control: 8/2/12/8
Groups were comparable at baseline. |
Intervention: At the end of the lobectomy procedure, a drainage ball with the function of negative pressure suction was placed. The actual value of negative pressure will decrease when the drainage ball gets filled. |
Control: At the end of the lobectomy procedure, a commonly used chest tube was placed in the basal position without negative pressure suction. |
Length of follow-up: Not reported.
Loss-to-follow-up: Not reported.
Incomplete outcome data: Not reported.
|
Drainage volume (mL): Intervention: 1017.67 ± 373.76 Control: 1100.67 ± 661.62 P=0.552
Drainage time (days): - Upper tube: Intervention: 3.89 ± 1.63 Control: 5.10 ± 2.02 P=0.048 - Upper lobe: Intervention: 4.84 ± 1.61 Control: 5.90 ± 1.52 P=0.041 - Lower lobe: Intervention: 3.82 ± 1.08 Control: 5.70 ± 2.63 P=0.042
Length of stay (days): Intervention: 5.4 ± 1.65 Control: 6.37 ± 1.99 P=0.045
Complications: - Air leakage: Intervention: 0 Control: 2 P=0.155 - Infection: Intervention: 0 Control: 1 P=0.321 - Cerebral infarction: Intervention: 1 Control: 0 P=0.321 |
. |
|
Holbek, 2019 |
Single-centre, parallel-arm, randomized controlled trial
Setting and country: Department of Cardiothoracic Surgery (in corporation with the Section for Surgical Pathophysiology) Rigshospitalet, Denmark
Source of funding: Funded by the Rigshospitalet’s Research Foundation; the Department of Cardiothoracic Surgery (Rigshospitalet), Section of Surgical Pathophysiology’s Global Excellence Foundation (Rigshospitalet); and Medela AG (Switzerland).
Conflicts of interest: Holbek received a research grant from Medela AG during the study period, Hansen and Petersen report personal fees from Medtronic outside the submitted work, Christensen is an investigator on the Medtronic Navigate Post Market study. Kehlet reported no conflicts of interest. |
Inclusion criteria: 18 years or older, able to speak and understand Danish, able to give informed consent, and scheduled to undergo VATS lobectomy for suspected or confirmed primary lung cancer.
Exclusion criteria: Scheduled for additional resection other than lobectomy (wedge, segment, lobe and chest wall). Patients were not excluded if an intra-operative decision led to additional resection.
N total at baseline: Intervention: 115 Control: 115
Important prognostic factors2: Age ± SD: Intervention: 67.9 ± 8.5 Control: 66.4 ± 10.4
Sex (female, %): Intervention: 71 (64.0) Control: 65 (58.6)
FEV1 (% of expected): Intervention: 87.1 ± 19.2 Control: 87.4 ± 19.8
Cardiovascular disease (%): Intervention: 61 (55) Control: 61 (55)
Diabetes mellitus (%): Intervention: 9 (8.1) Control: 14 (12.6)
Blood loss (mL): Control: 50.0 (10.0-100.0)
Groups comparable at baseline: not reported. |
Intervention: Low chest drain suction of -2 cm H2O. |
Control: High chest drain suction of -10 cm H2O. |
Length of follow-up: Until postoperative day 30.
Loss-to-follow-up: Intervention: N=3 (2.6%) Reasons: thoracotomy (n=1), two drains (n=2)
Control: N=5 (4.3%) Reasons: pneumonectomy (n=2), thoracotomy (n=1), two drains (n=2)
Incomplete outcome data: No incomplete outcome data.
|
Drainage duration (h): Intervention: 27.4 (23.3-71.2) Control: 47.5 (24.5-117.8) P=0.047
Prolonged air leak >5 days: Intervention: 16 (14.4) Control: 27 (24.3) P=0.089
Pneumothorax after drain removal: Intervention: 46 (41.8) P=0.31
Total drain fluid (mL): Intervention: 566.0 (329.0-1155.0) Control: 795.0 (454.2-1605.0) P=0.007
Length of in-hospital stay: Intervention: 2.0 (2.0-5.8) Control: 3.0 (2.0-9.0) P=0.18
Any complications: Intervention: 37 (33.3) Control: 51 (45.9) P= 0.074
Myocardial infarction: Intervention: 1 (0.9) Control: 0 (0.0)
Sepsis: Intervention: 4 (3.6) Control: 0 (0.0) P=0.13
Reoperation: - Due to bleeding: Intervention: 1 (0.9) Control: 3 (2.7) - Due to air leak: Intervention: 1 (0.9) Control: 3 (2.7) - Due to atelectasis: Intervention: 0 (0.0) Control: 1 (0.9) P=0.37
Overnight readmission: Intervention: 17 (15.3) Control: 16 (14.4) P=1.00
Duration of readmission: Intervention: 5.0 (3.0-8.0) Control: 4.0 (2.0-7.0) P=0.50
30-day mortality: Intervention: 1 (0.9) Control: 3 (2.7) P=0.61 |
|
|
Lijkendijk, 2019 |
Single-center, open-labelled, randomized trial
Setting and country: Department of Cardiothoracic Surgery, Odense University Hospital, Odense, Denmark
Source of funding: Not reported.
Conflicts of interest: Not reported. |
Inclusion criteria: Admitted for standard lobectomy, older than 18 years of age, able to give informed consent.
Exclusion criteria: Previous history of pulmonary or cardiac operations, expected difficulties with postoperative mobilization, participation in concomitant research studies (in the same department) where a different chest drainage protocol could influence results, expected postoperative mechanical ventilation, insertion of more than one chest drain, and bilobectomy or middle lobectomy.
N total at baseline: Intervention: 53 Control: 53
Important prognostic factors2: Age (median, range): Intervention: 69 (42-81) Control: 69 (46-88)
Sex (male): Intervention: 23
Type of surgery (VATS/thoracotomy /upper lobectomy/lower lobectomy): Intervention: 34/19/25/28 Control: 25/28/25/28
FEV1, mean ± SD: Intervention: 88.4 ± 20.6 Control: 83.6 ± 19.7
Incomplete fissure or adhesions: Intervention: 36 Control: 47
Groups comparable at baseline: not reported. |
Intervention: Low variable suction of -5 cm H2O on a digital drainage device. |
Control: High variable suction of -20 cm H2O on a digital drainage device. |
Length of follow-up: Not reported.
Loss-to-follow-up: No loss-to-follow-up.
Incomplete outcome data: No incomplete outcome data.
|
Chest drain duration (hours) Intervention: 25 (21-55) Control: 28 (23-77) P=0.97
Length of stay (days): Intervention: 5 (3-6) Control: 5 (3-7) P=0.75
Air leak: - Perioperative: Intervention: 38 (71.7) Control: 27 (50.9) - Postoperative recovery: - No air flow: Intervention: 22 (41.5) Control: 16 (30.2) - <100 mL/min: Intervention: 23 (43.4) Control: 28 (52.8) - 100-1000 mL/min: Intervention: 7 (13.2) Control: 4 (7.5) - >1000 mL/min: Intervention: 1 (1.9) Control: 5 (9.4)
Prolonged air leak >5 days: Intervention:4 P=0.34
|
|
Risk of bias systematic review:
Risk of bias RCTs:
|
Study
First author, year |
Appropriate and clearly focused question?1
Yes/no/unclear |
Comprehensive and systematic literature search?2
Yes/no/unclear |
Description of included and excluded studies?3
Yes/no/unclear |
Description of relevant characteristics of included studies?4
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?5
Yes/no/unclear/notapplicable |
Assessment of scientific quality of included studies?6
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?7
Yes/no/unclear |
Potential risk of publication bias taken into account?8
Yes/no/unclear |
Potential conflicts of interest reported?9
Yes/no/unclear |
|
Zhou, 2019 |
Yes
Reason: PICO and research question match, inclusion criteria were predefined. |
No
Reason: Search period and strategy are described, but Medline was not searched. |
Yes
Reason: Reasons for exclusion were provided in the flow diagram. |
Yes
Reason: Main characteristics of included RCTs are provided. |
Not applicable
Reason: 10 RCTs in SR. |
Yes
Reason: Risk of bias assessment was performed and table and graphs were provided. |
No
Reason: High statistical heterogeneity for multiple outcome measures. No information about clinical heterogeneity. |
Yes
Reason: No significant publication bias were found by visual inspection of funnel plot and Begg’s test. Funnel plot was not included in the SR. |
No
Reason: Potential conflicts of interest reported for SR but not for individual studies. |
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Cui, 2019 |
Probably yes
Reason: Patients were randomly assigned by sequentially numbered envelopes. |
Definitely yes
Reason: Opaque, sealed envelopes were used. |
Probably no
Reason: Not reported. |
Probably yes
Reason: Loss-to-follow-up and missing outcome data not reported, but 60 patients were randomized and 60 patients were analysed. |
Definitely yes
Reason: All relevant outcomes were reported. |
Definitely yes
Reason: No other problems noted. |
Some concerns
Reason: Blinding not reported.
|
|
Holbek, 2019 |
Definitely yes
Reason: The allocation sequence was created from a web-based computer-generated random number table. |
Definitely yes
Reason: Identical, sealed, opaque envelopes written in grey tone by an independent administrator were used. |
Probably yes
Reason: Surgical staff, patients, and research group individuals during surgery were blinded. Thereafter the trial was open label. |
Definitely yes
Reason: Loss-to-follow-up was approximately 7%. |
Definitely yes
Reason: All relevant outcomes were reported. |
Probably no
Reason: Possible bias because there was no central randomization, variability in the treatment, no power calculations for secondary outcomes with the potential of type II errors. |
Some concerns |
|
Lijkendijk, 2019 |
Probably yes
Reason: Patients were randomly assigned by sequentially numbered envelopes. |
Definitely yes
Reason: Sequentially numbered, opaque, and sealed envelopes were used. |
Definitely no
Reason: Blinding was not possible because it was necessary to view the digital display to determine when the chest drain could be removed. |
Definitely yes
Reason: There was no loss-to-follow-up in the intervention and control group. |
Definitely yes
Reason: All relevant outcomes were reported. |
Probably yes
Reason: No other problems noted. |
Some concerns
Reason: Blinding not possible. |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Alphonso N, Tan C, Utley M, Cameron R, Dussek J, Lang-Lazdunski L, Treasure T. A prospective randomized controlled trial of suction versus non-suction to the under-water seal drains following lung resection. Eur J Cardiothorac Surg. 2005 Mar;27(3):391-4. doi: 10.1016/j.ejcts.2004.12.004. Epub 2005 Jan 13. PMID: 15740944. |
This study is included in the SR from Zhou (2019). |
|
Brunelli A, Monteverde M, Borri A, Salati M, Marasco RD, Al Refai M, Fianchini A. Comparison of water seal and suction after pulmonary lobectomy: a prospective, randomized trial. Ann Thorac Surg. 2004 Jun;77(6):1932-7; discussion 1937. doi: 10.1016/j.athoracsur.2003.12.022. PMID: 15172239. |
This study is included in the SR from Zhou (2019). |
|
Brunelli A, Salati M, Pompili C, Refai M, Sabbatini A. Regulated tailored suction vs regulated seal: a prospective randomized trial on air leak duration. Eur J Cardiothorac Surg. 2013 May;43(5):899-904. doi: 10.1093/ejcts/ezs518. Epub 2012 Sep 28. PMID: 23024236. |
This study is included in the SR from Zhou (2019). |
|
Chang PC, Chen KH, Jhou HJ, Lee CH, Chou SH, Chen PH, Chang TW. Promising Effects of Digital Chest Tube Drainage System for Pulmonary Resection: A Systematic Review and Network Meta-Analysis. J Pers Med. 2022 Mar 22;12(4):512. doi: 10.3390/jpm12040512. PMID: 35455628; PMCID: PMC9029690. |
Network meta-analysis with multiple comparisons, not all relevant for this PICO. |
|
Cerfolio RJ, Bass C, Katholi CR. Prospective randomized trial compares suction versus water seal for air leaks. Ann Thorac Surg. 2001 May;71(5):1613-7. doi: 10.1016/s0003-4975(01)02474-2. PMID: 11383809. |
This study is included in the SR from Zhou (2019). |
|
Daneshvar Kakhki, A. and Pooya, M. and Pejhan, S. and Javaherzadeh, M. and Arab, M. and Shadmehr, M. B. and Abbasi, A. Effect of chest tube suction on air-leak following lung resection. Tanaffos. 2006 1(5): 37-43. |
This study is included in the SR from Zhou (2019). |
|
Gao S, Zhang Z, Aragón J, Brunelli A, Cassivi S, Chai Y, Chen C, Chen C, Chen G, Chen H, Chen JS, Cooke DT, Downs JB, Falcoz PE, Fang W, Filosso PL, Fu X, Force SD, Garutti MI, Gonzalez-Rivas D, Gossot D, Hansen HJ, He J, He J, Holbek BL, Hu J, Huang Y, Ibrahim M, Imperatori A, Ismail M, Jiang G, Jiang H, Jiang Z, Kim HK, Li D, Li G, Li H, Li Q, Li X, Li Y, Li Z, Lim E, Liu CC, Liu D, Liu L, Liu Y, Lobdell KW, Ma H, Mao W, Mao Y, Mou J, Ng CSH, Novoa NM, Petersen RH, Oizumi H, Papagiannopoulos K, Pompili C, Qiao G, Refai M, Rocco G, Ruffini E, Salati M, Seguin-Givelet A, Sihoe ADL, Tan L, Tan Q, Tong T, Tsakiridis K, Venuta F, Veronesi G, Villamizar N, Wang H, Wang Q, Wang R, Wang S, Wright GM, Xie D, Xue Q, Xue T, Xu L, Xu S, Xu S, Yan T, Yu F, Yu Z, Zhang C, Zhang L, Zhang T, Zhang X, Zhao X, Zhao X, Zhi X, Zhou Q. The Society for Translational Medicine: clinical practice guidelines for the postoperative management of chest tube for patients undergoing lobectomy. J Thorac Dis. 2017 Sep;9(9):3255-3264. doi: 10.21037/jtd.2017.08.165. PMID: 29221303; PMCID: PMC5708414. |
International guideline. The guideline does not comprise a systematic review including risk of bias assessment of included studies, meta-analysis and evidence tables. |
|
Gocyk W, Kużdżał J, Włodarczyk J, Grochowski Z, Gil T, Warmus J, Kocoń P, Talar P, Obarski P, Trybalski Ł. Comparison of Suction Versus Nonsuction Drainage After Lung Resections: A Prospective Randomized Trial. Ann Thorac Surg. 2016 Oct;102(4):1119-24. doi: 10.1016/j.athoracsur.2016.04.066. Epub 2016 Aug 23. PMID: 27526655. |
This study is included in the SR from Zhou (2019). |
|
Leo F, Duranti L, Girelli L, Furia S, Billè A, Garofalo G, Scanagatta P, Giovannetti R, Pastorino U. Does external pleural suction reduce prolonged air leak after lung resection? Results from the AirINTrial after 500 randomized cases. Ann Thorac Surg. 2013 Oct;96(4):1234-1239. doi: 10.1016/j.athoracsur.2013.04.079. Epub 2013 Jul 16. PMID: 23866802. |
This study is included in the SR from Zhou (2019). |
|
Lijkendijk M, Neckelmann K, Licht PB. External Suction and Fluid Output in Chest Drains After Lobectomy: A Randomized Clinical Trial. Ann Thorac Surg. 2018 Feb;105(2):393-398. doi: 10.1016/j.athoracsur.2017.08.048. Epub 2017 Nov 27. PMID: 29174779. |
Wrong outcomes. |
|
Marshall MB, Deeb ME, Bleier JI, Kucharczuk JC, Friedberg JS, Kaiser LR, Shrager JB. Suction vs water seal after pulmonary resection: a randomized prospective study. Chest. 2002 Mar;121(3):831-5. doi: 10.1378/chest.121.3.831. PMID: 11888968. |
This study is included in the SR from Zhou (2019). |
|
Prokakis C, Koletsis EN, Apostolakis E, Panagopoulos N, Kouki HS, Sakellaropoulos GC, Filos K, Dougenis DV. Routine suction of intercostal drains is not necessary after lobectomy: a prospective randomized trial. World J Surg. 2008 Nov;32(11):2336-42. doi: 10.1007/s00268-008-9741-3. PMID: 18787890. |
This study is included in the SR from Zhou (2019). |
|
Vuorisalo S, Aarnio P, Hannukainen J. Comparison between flutter valve drainage bag and underwater seal device for pleural drainage after lung surgery. Scand J Surg. 2005;94(1):56-8. doi: 10.1177/145749690509400114. PMID: 15865119. |
Different comparison: Heimlich valve versus water seal. |
Beoordelingsdatum en geldigheid
Publicatiedatum : 21-11-2023
Beoordeeld op geldigheid : 07-11-2023
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS) en/of andere bron. De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten die longresectie ondergaan.
Samenstelling van de werkgroep
Werkgroep
- Drs. E. (Erik) von Meyenfeldt, longchirurg, NVvH (voorzitter)
- Dr. C. (Chris) Dickhoff, longchirurg, NVvH
- Dr. N.J. (Nick) Koning, anesthesioloog, NVA
- Dr. T.J. (Thomas) van Brakel, cardio-thoracaal chirurg, NVT
- Dr. I. (Idris) Bahce, longarts, NVALT
- Drs. L.A. (Lidia) Barberio, directeur, Longkanker Nederland
- Dr. E. (Erik) Hulzebos, fysiotherapeut, KNGF
Meelezers:
- Dr. R. (Richard) van Valen, verpleegkundig specialist cardio-thoracale chirurgie, V&VN
Met ondersteuning van:
- Dr. R. (Romy) Zwarts - van de Putte, adviseur, Kennisinstituut van Medisch Specialisten
- Drs. E.R.L. (Evie) Verweg, junior adviseur, Kennisinstituut van Medisch Specialisten
- Drs. D.W. (Diederik) van Oyen, AOIS, NVvH
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Von Meyenfeldt |
Longchirurg |
Penningmeester Stichting Wetenschappelijk Onderzoek & Nascholing Heelkunde ASz (onbetaald), buitenpromovendus Vrije Universiteit/AmsterdamUMC (onbetaald) |
Bezig met ERATS Trial en Prehabilitatie-pilot bij longresecties. |
Geen |
|
Bahce |
Longarts |
Commissielid |
Honorering op naam van afdeling voor adviesraden bij diverse farmaceutische bedrijven. |
Geen |
|
Koning |
Anesthesioloog |
Lid Beroepsbelangencommissie NVA, deelname multidisciplinaire werkgroep PACU |
Geen |
Geen |
|
Barberio |
Directeur Longkanker Nederland |
Lid RvT Agora (tot eind 2022), leven tot het einde, bestuur Dutch Lung Cancer Audit (DLCA), vanaf 1 mei 2023 lid van IMAGIO project. |
Longkanker Nederland wordt gefinancierd door KWF en VWS, samenwerking met diverse bedrijven. |
Geen |
|
Dickhoff |
Longchirurg |
Complicatie commissie van de NVVL |
Honorering op naam van afdeling voor adviesraden bij diverse farmaceutische bedrijven. |
Geen |
|
Van Brakel |
Cardiothoracaal chirurg |
Niet van toepassing |
Geen |
Geen |
|
Hulzebos |
Fysiotherapeut |
Secretaris Vereniging voor Hart-, Vaat-, en Longfysiotherapie (VHVL) |
Geen |
Geen |
Inbreng patiëntenperspectief
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door de afgevaardigde patiëntenvereniging in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan de patiëntenvereniging Longkanker Nederland en de Patientenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijn is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling zijn richtlijnmodules op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
Module |
Uitkomst raming |
Toelichting |
|
Module [ERAS] |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling niet breed toepasbaar zijn (<5.000 patiënten) en daarom naar verwachting geen substantiële financiële gevolgen zal hebben voor de collectieve uitgaven. |
|
Module [Mobilisatie] |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling niet breed toepasbaar zijn (<5.000 patiënten) en daarom naar verwachting geen substantiële financiële gevolgen zal hebben voor de collectieve uitgaven. |
|
Module [Drainbeleid verwijdercriteria] |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling niet breed toepasbaar zijn (<5.000 patiënten) en daarom naar verwachting geen substantiële financiële gevolgen zal hebben voor de collectieve uitgaven. |
|
Module [Drainbeleid - Zuigdrainage] |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling niet breed toepasbaar zijn (<5.000 patiënten) en daarom naar verwachting geen substantiële financiële gevolgen zal hebben voor de collectieve uitgaven. |
|
Module organisatie van zorg |
Geen substantiële financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling niet breed toepasbaar zijn (<5.000 patiënten) en daarom naar verwachting geen substantiële financiële gevolgen zal hebben voor de collectieve uitgaven. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten die longresectie ondergaan. Tevens zijn er knelpunten aangedragen door de Nederlandse Vereniging voor Heelkunde, Nederlandse Vereniging voor Anesthesiologie, Longkanker Nederland, Inspectie Gezondheidszorg en Jeugd, Samenwerkende Topklinische opleidings Ziekenhuizen, Koninklijk Nederlands Genootschap voor Fysiotherapie, Nederlandse vereniging van Diëtisten, en Nederlandse Vereniging voor Geriatrie via een schriftelijke knelpuntenanalyse. Een verslag hiervan is opgenomen onder aanverwante producten.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit.
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Literature search strategy
Zoekverantwoording
Algemene informatie
|
Richtlijn: Optimalisatie van zorg rondom longresecties |
|
|
Uitgangsvraag: Wat is het optimale drainbeleid na een anatomische longresectie mbt luchtlekkage |
|
|
Database(s): Ovid/Medline, Embase |
Datum:1-11-2022 |
|
Periode: nvt |
Talen: nvt |
|
Literatuurspecialist: Ingeborg van Dusseldorp |
|
|
BMI zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht met de volgende concepten: Longresectie AND drainbeleid In de interventie en de comparison wordt gevraagd om low level versus high level. Omdat er geen specifieke trefwoorden zijn voor deze vergelijking wordt gezocht naar pressure of drainage or suction. Alhoewel aan deze woorden nog wel terminologie is toegevoegd waardoor het iets specifieker wordt, (((suction OR drainage OR pressure) NEAR/10 (low OR level OR tube* OR drain OR drains)):ti,ab,kw), ontstaat wel de nodige ruis. Als vergelijking is ook een zeer specifieke search uitgevoerd in Embase waarin alleen in title, abstract, keyword is gezocht naar low level (#18 Embase search). Uiteindelijk worden dan 19 referenties gevonden. Vraag is welke referenties uiteindelijk geïncludeerd worden en of die overeenkomen met deze set. NB. Er is niet gezocht naar luchtlekkage en ook niet naar digital drainage systems in zijn algemeenheid. De focus ligt op drainage, suction, pressure. De beide sleutelartikelen worden gevonden. |
|
|
Te gebruiken voor richtlijnen tekst: In de databases Embase en Ovid/Medline is op 1-11-2022 met relevante zoektermen gezocht naar systematische reviews en RCTs over drainbeleid bij longresectie. De literatuurzoekactie leverde unieke treffers op. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
61 |
43 |
72* |
|
RCTs |
198 |
150 |
234* |
|
Observationele studies |
931 |
490 |
|
|
Overig |
|
|
|
|
Totaal |
|
|
306* |
*in Rayyan
Zoekstrategie
Embase
|
No. |
Query |
Results |
|
#21 |
#9 AND #19 |
18 |
|
#20 |
#8 AND #19 |
1 |
|
#19 |
#7 AND #18 |
62 |
|
#18 |
(((low OR level) NEAR/4 (pressure OR suction OR drainage)):ti,ab,kw) OR '8 cm h2*':ti,ab,kw Specifieke strategie |
51641 |
|
#17 |
#3 AND #16 |
2 |
|
#16 |
#12 OR #13 |
270 |
|
#15 |
#13 NOT #12 RCT |
198 |
|
#14 |
#7 AND (#10 OR #11) |
931 |
|
#13 |
#7 AND #9 |
206 |
|
#12 |
#7 AND #8 SR |
61 |
|
#11 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
13571461 |
|
#10 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
7328041 |
|
#9 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
1976406 |
|
#8 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
871244 |
|
#7 |
#6 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
2054 |
|
#6 |
#4 AND #5 |
2603 |
|
#5 |
'suction'/exp OR 'surgical drainage'/exp OR 'pressure'/exp OR '8 cm h2*':ti,ab,kw OR (((suction OR drainage OR pressure) NEAR/10 (low OR level OR tube* OR drain OR drains)):ti,ab,kw) |
317794 |
|
#4 |
'lobectomy'/exp AND ('lung'/exp OR 'lung cancer'/exp) OR 'lung lobectomy'/exp OR 'lung resection'/exp OR 'lung resection':ti,ab,kw OR 'lung volume reduction surgery':ti,ab,kw OR 'pneumectomy':ti,ab,kw OR 'pneumonectomy':ti,ab,kw OR 'pneumonic resection':ti,ab,kw OR 'pneumoresection':ti,ab,kw OR 'pulmonary resection':ti,ab,kw OR 'pulmonectomy':ti,ab,kw OR 'resected lung':ti,ab,kw OR 'lung lobe resection':ti,ab,kw OR 'lung lobectomy':ti,ab,kw OR 'pneumolobectomy':ti,ab,kw OR 'pulmonary lobectomy':ti,ab,kw |
62094 |
|
#3 |
#1 OR #2 sleutelartikelen |
2 |
|
#2 |
the AND effects AND of AND low AND suction AND on AND digital AND drainage AND devices AND after AND lobectomy AND using AND 'video assisted' AND thoracoscopic AND surgery |
1 |
|
#1 |
what AND is AND the AND optimal AND level AND of AND suction AND on AND digital AND chest AND drainage AND devices AND following AND pulmonary AND lobectomy |
1 |
Ovid/Medline
|
# |
Searches |
Results |
|
12 |
10 not 9 RCT |
393 |
|
11 |
4 and (8 or 9) |
490 |
|
10 |
4 and 6 |
453 |
|
9 |
4 and 5 SR |
86 |
|
8 |
Case-control Studies/ or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or comparative study/ or control groups/ or controlled before-after studies/ or controlled clinical trial/ or double-blind method/ or historically controlled study/ or matched-pair analysis/ or single-blind method/ or (((control or controlled) adj6 (study or studies or trial)) or (compar* adj (study or studies)) or ((control or controlled) adj1 active) or "open label*" or ((double or two or three or multi or trial) adj (arm or arms)) or (allocat* adj10 (arm or arms)) or placebo* or "sham-control*" or ((single or double or triple or assessor) adj1 (blind* or masked)) or nonrandom* or "non-random*" or "quasi-experiment*" or "parallel group*" or "factorial trial" or "pretest posttest" or (phase adj5 (study or trial)) or (case* adj6 (matched or control*)) or (match* adj6 (pair or pairs or cohort* or control* or group* or healthy or age or sex or gender or patient* or subject* or participant*)) or (propensity adj6 (scor* or match*))).ti,ab,kf. or (confounding adj6 adjust*).ti,ab. or (versus or vs or compar*).ti. or ((exp cohort studies/ or epidemiologic studies/ or multicenter study/ or observational study/ or seroepidemiologic studies/ or (cohort* or 'follow up' or followup or longitudinal* or prospective* or retrospective* or observational* or multicent* or 'multi-cent*' or consecutive*).ti,ab,kf.) and ((group or groups or subgroup* or versus or vs or compar*).ti,ab,kf. or ('odds ratio*' or 'relative odds' or 'risk ratio*' or 'relative risk*' or aor or arr or rrr).ab. or (("OR" or "RR") adj6 CI).ab.)) |
5153100 |
|
7 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] |
4144134 |
|
6 |
(exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf.) not (animals/ not humans/) |
1371219 |
|
5 |
(meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf.) not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) |
568731 |
|
4 |
3 not ((exp animals/ or exp models, animal/) not humans/) not (letter/ or comment/ or editorial/) |
1602 |
|
3 |
1 and 2 |
1707 |
|
2 |
exp Drainage/ or exp Pressure/ or ((tube* or drain*or low or level) adj10 (pressure or suction or drainage)).ti,ab,kf. or "8 cm h2*".ti,ab,kf. |
214402 |
|
1 |
Pneumonectomy/ or (exp Thoracoscopy/ and Lung/) or exp Lung Neoplasms/su or lung resection.ti,ab,kf. or lung volume reduction surgery.ti,ab,kf. or pneumectomy.ti,ab,kf. or pneumonectomy.ti,ab,kf. or pneumonic resection.ti,ab,kf. or pneumoresection.ti,ab,kf. or pulmonary resection.ti,ab,kf. or pulmonectomy.ti,ab,kf. or resected lung.ti,ab,kf. or lung lobe resection.ti,ab,kf. or lung lobectomy.ti,ab,kf. or pneumolobectomy.ti,ab,kf. or pulmonary lobectomy.ti,ab,kf. or ((lung or pulmonary) adj3 (surger* or segmentectomy)).ti,ab,kf. |
64298 |