Tepelsteeltechniek
Uitgangsvraag
Wat is de meest optimale tepelsteeltechniek bij mammareductie?
Aanbeveling
- Kies een tepelsteeltechniek op basis van ervaring, expertise en voorkeur van de plastisch chirurg.
- Weeg in het besluit de volgende aspecten mee: eigenschappen van de te reduceren borst, wensen van de patiënt met betrekking tot het huidpatroon/littekens en bestaande littekens/eerdere operaties in de borst.
- Bij de keuze voor een tepelsteeltechniek, overweeg de mediocraniale techniek.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is een systematische literatuuranalyse uitgevoerd waarbij verschillende tepelsteeltechnieken voor mammareductie met elkaar zijn vergeleken. Dertien vergelijkende studies zijn meegenomen, waarbij de superior, superomediale en mediocraniale pedicle technieken vergeleken zijn met de inferior pedicle techniek.
Het waren allen relatief kleine observationele (veelal retrospectieve) studies, met beperkingen in het studiedesign, waardoor de bewijskracht voor zowel de cruciale als belangrijke uitkomstmaten uitkomt op GRADE zeer laag. Dit betekent dat er een zeer grote onzekerheid is over het ware effect. En hierdoor konden er voor geen van de uitkomstmaten eenduidige conclusies worden getrokken. Voor een deel van de uitkomstmaten werd überhaupt geen data gevonden.
Op basis van het gebrek aan bewijs in de beschikbare literatuur hebben we de conclusie moeten trekken dat er niet een type tepelsteel techniek de voorkeur heeft bij het uitvoeren van een mammareductie.
In de Nederlandse praktijk
Bij het verrichten van een mammareductie wordt in Nederland voornamelijk gekozen voor de mediocraniale steel. Dit in tegenstelling tot de Verenigde Staten, waar meestal een inferior pedicle techniek wordt toegepast. Hoogstwaarschijnlijk heeft dit verschil vooral een historische reden. In Nederland wordt in de praktijk de meeste ervaring opgedaan met de mediocraniale techniek. Dit leidt vanzelfsprekend tot meer verfijning van deze techniek, perioperatieve ervaring en beter management van complicaties in vergelijking met de inferior pedicle techniek.
De expertise die met de mediocraniale steel techniek is opgebouwd maakt dat Nederlandse plastisch chirurgen zich vooral met deze techniek comfortabel voelen. In de literatuur vinden we geen bewijs die het gebruik van deze specifieke tepelsteeltechniek ontmoedigt, er lijkt zelfs op enkele uitkomstmaten een tendens te zijn in het voordeel van de mediocraniale steel techniek. Klinisch relevante data die deze tendens onderbouwen kunnen in de literatuuranalyse echter niet worden gevonden, waardoor dit in de GRADE conclusies niet zo wordt gesteld.
De inferior pedicle techniek lijkt ook zeker een techniek die goed bruikbaar is. Bovengenoemde literatuuranalyse heeft immers geen bewijs gevonden voor specifieke nadelen van deze techniek. In de praktijk kan een inferior pedicle techniek soms juist wenselijk zijn, bijvoorbeeld in het geval van mammasparende oncologische borstchirurgie, waar veel gebruik wordt gemaakt van mammareductie technieken of bij een zeer lange tepel-jugulum afstand (TJD), waarbij er een verhoogd risico bestaat op doorbloedingsproblemen van het mammaweefsel en/of de tepel.
Het is belangrijk een techniek te kiezen waar de plastisch chirurg de meeste ervaring in heeft, zich het meest comfortabel bij voelt en waarmee het beoogde doel het beste behaald kan worden. De TJD is een belangrijke maat die kan bijdragen tot de keuze voor een van de tepelsteeltechnieken: zo is een relatief korte TJD meestal minder toegankelijk voor een zuiver laterale/mediale of mediocraniale steel, maar juist meer voor een zuiver craniale steel. Indien er sprake is van een relatief lange TJD en er derhalve een lange afstand overbrugd dient te worden tot de nieuwe tepelpositie, kan juist een inferior pedicle techniek superieur zijn om te kiezen om de kans op vetnecrose en doorbloedingsproblemen te verlagen. Dit heeft alles te maken met de draaiing die nodig is bij bijvoorbeeld een mediocraniale steel. Uiteraard wordt de beslissing tot het eventueel nemen van een vrij tepeltransplantaat in deze afweging ook meegenomen.
De omvang van de borst kan ook een rol spelen in de afweging voor welke tepelsteeltechniek te kiezen; bij een grote tot zeer grote cupmaat dient de tepel meer verplaatst te worden en is een ruimer huidpatroon met resectie geïndiceerd. Bij een relatief kleine cupmaat zal een beperkte tepelverplaatsing (lifting) van toepassing zijn en is een craniale tepelsteel vaak de meest logische keus, waarvoor de minste dissectie van het omliggende gebied nodig is, wat minder vasculaire risico’s geeft.
Waarden en voorkeuren van patiënten
Het type tepelsteeltechniek lijkt voor de patiënt zelf minder relevant. Het is immers een technisch onderdeel van de operatie, waar de patiënt zelf geen directe notie van heeft. Echter, van de gevolgen die kunnen resulteren uit de gemaakte keuze voor een tepelsteeltechniek, merkt de patiënt uiteraard wel wat. Daarom is bovengenoemde literatuuranalyse van de verschillende uitkomstmaten, nadelen en complicatierisico’s wel degelijk van belang.
Wat voor de patiënt een factor is die van belang is, is de hoeveelheid littekens en de vorm en positie daarvan. Er bestaan verschillende typen huidpatronen; Inverted-T (ook wel ‘Wise’ genoemd), short horizontal scar, vertical scar, J/L-vormig, zuiver peri-areolair, danwel afgeleiden daarvan.
In deze richtlijn is een literatuuranalyse over huidpatroon niet opgenomen. In de praktijk heeft de patiënt over het algemeen wel de wens voor zo min mogelijk littekens, vooral indien de patiënt bekend is met ongunstige en/of ontsierende littekenvorming (in voorgeschiedenis of gerelateerd aan het Fitzpatrick huidtype). Deze wens mag niet leiden tot het doen van concessies, waardoor de operatierisico’s omhooggaan, het esthetisch resultaat en/of mate van reductie worden beïnvloed. Daar waar mogelijk zal een optimale combinatie van deze factoren besproken en gekozen dienen te worden. En ook hier speelt ervaring en technische expertise een rol, alsmede de grootte en vorm van de borst. Dit in dialoog met de patiënt, die wensen qua littekens kenbaar maakt.
Bij de keuze voor het huidpatroon, is er soms wel, soms niet een relatie met de te gebruiken tepelsteeltechniek. Zo zal er in geval van een grote tot zeer grote cupmaat vaker gekozen worden voor een uitgebreid inverted-T huidpatroon. Hiermee kan immers een ruime huidreductie worden gedaan en is er de keus uit meerdere tepelsteeltechnieken. Bij de relatief kleine borst kan men veelal uit met een minder uitgebreid huidpatroon wat leidt tot een fraaier cosmetisch resultaat. Anderzijds geeft een kleine borst vaak minder mogelijkheden voor het gebruik van verschillende tepelsteeltechnieken. Zo zal bijvoorbeeld een vertical scar huidpatroon meestal niet worden gecombineerd met een inferior pedicle, maar juist wel met een craniale verplaatsing middels een craniale of mediale steel.
Tenslotte kan ook de keuze voor aanvullende liposuctie een rol spelen in het type huidpatroon dat gebruikt kan worden. Indien gekozen wordt voor aanvullende liposuctie, kan over het algemeen worden volstaan met minder huidreductie en derhalve minder uitgebreide littekens.
Een belangrijke factor die altijd moet worden meegewogen in de keuze voor de tepelsteeltechniek is de aanwezigheid van reeds bestaande littekens ten gevolge van eerdere operaties in de borst. De locatie en uitgebreidheid van deze littekens kunnen een belangrijke en zelfs doorslaggevende rol spelen in de keuze voor de juiste tepelsteeltechniek. Dit om een optimale vascularisatie van het weefsel te waarborgen en risico’s op doorbloedingsproblemen tot een minimum te beperken.
Kosten (middelenbeslag)
De verschillende tepelsteeltechnieken brengen onderling niet meer of minder kosten met zich mee voor patiënt, maatschappij, afdeling of ziekenhuis Het betreft puur een verschil in technisch handelen tijdens een operatie.
Aanvaardbaarheid, haalbaarheid en implementatie
In Nederland wordt in de praktijk voortdurend een variatie aan tepelsteeltechnieken toegepast, gebaseerd op historisch gebruik, ervaring, expertise, voorkeur van de plastisch chirurg, specifieke wensen van de patiënt, eigenschappen van de te reduceren borst en bijvoorbeeld reeds aanwezige littekens. Iedere plastisch chirurg neemt bovendien in zijn planning bij de verplaatsing van weefsels het belang van een optimale vascularisatie mee en baseert hierop zijn/haar keuze voor de tepelsteeltechniek.
De werkgroep voorziet daarom geen problemen op het gebied van aanvaardbaarheid, haalbaarheid en implementatie.
Voor een patiënt zien wij deze problemen evenmin, aangezien dit een operatie-technisch item is, waar een patiënt na de operatie geen notie van heeft.
Iedere tepelsteeltechniek is voor iedere patiënt toegankelijk in opzet. Wel zullen er verschillen zijn op basis van voorkeur plastisch chirurg, ervaring, kenmerken van de borst en eventuele littekens.
De werkgroep heeft op basis van de literatuuranalyse geen factoren kunnen vinden die het gebruik van alle mogelijke tepelsteeltechnieken in de weg staat. Noch zijn extra kosten, personeel, apparatuur, afstemming met andere stakeholders van toepassing.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Verschillende tepelsteeltechnieken leiden volgens de beschikbare literatuur niet, dan wel in zeer beperkte mate tot klinisch relevante verschillen in cruciale uitkomstmaten: bottoming out, patiënttevredenheid en belangrijke uitkomstmaten: verminderde sensibiliteit tepel, verlies NAC, vetnecrose en wonddehiscentie. De bewijskracht hiervoor is zeer laag.
Aangezien voor het slagen van een operatie de technische expertise en ervaring een cruciale rol spelen, vooral daar waar de doorbloeding van weefsels een belangrijk onderdeel is, ziet de werkgroep deze factoren als essentieel bij het maken van de keuze voor een bepaalde tepelsteeltechniek.
Het belangrijkst is dus om een techniek te kiezen waar de plastisch chirurg de meeste ervaring in heeft en zich het meest comfortabel bij voelt en waarmee de kans op het behalen van het beoogde doel het grootst is. Uitkomstmaten die kunnen worden meegenomen in de besluitvorming zijn: grootte en vorm van de borst, eventuele voorkeuren van de patiënt en reeds bestaande littekens.
Gezien de van oudsher ruime ervaring in Nederland met de mediocraniale tepelsteeltechniek geeft de werkgroep er de voorkeur aan om deze techniek als eerste keus te overwegen in de meerderheid van de borstreductiepatiënten.
Onderbouwing
In de huidige Nederlandse praktijk wordt met name de mediocraniale tepelsteeltechniek gebruikt, ook wel bekend als craniomediale techniek. In mindere mate wordt ook de mediale en inferior pedicle techniek gebruikt. Laatstgenoemde techniek wordt overigens met name in de Verenigde Staten gebruikt.
Knelpunten voor dit onderwerp zijn zowel praktijkvariaties als ook technische variaties. Dit heeft mogelijk een effect op factoren als vasculaire complicatierisico’s, sensibiliteit van de tepel en duurzaamheid van de vorm van de borst.
|
Very low GRADE |
1. Superior versus inferior pedicle technique
It is unclear whether there is a difference in bottoming out, patient satisfaction and adverse outcomes between patients that underwent reduction mammaplasty with superior pedicle compared to those with inferior pedicle.
Sources: de Biasio 2017, Chiummariello 2013, Toplu 2021, Schlenz 2005, Hamdi 2001, Mizgala 2000, Chiummariello 2008. |
|
No GRADE |
1. Superior versus inferior pedicle technique
No studies were found that could answer the question what the effect is of superior compared to inferior pedicle technique in reduction mammaplasty in ptosis and patient satisfaction.
Sources: - |
|
Very low GRADE |
2. Superomedial versus inferior pedicle technique
It is unclear whether there is a difference in bottoming out, patient satisfaction and adverse outcomes between patients that underwent reduction mammaplasty with superomedial pedicle compared to those with inferior pedicle.
Sources: Sapino 2021, Kemaloglu 2018, Makboul 2017, Jorgensen 2021, Antony 2013, Toplu 2021, Ogunleye 2017. |
|
Very low GRADE |
3. Medial versus inferior pedicle technique
It is unclear whether there is a difference in bottoming out, patient satisfaction and adverse outcomes between patients that underwent reduction mammaplasty with medial pedicle compared to those with inferior pedicle.
Sources: de Biasio 2017, Chiummariello 2008, Jorgensen 2021, Toplu 2021. |
|
No GRADE |
3. Medial versus inferior pedicle technique
No studies were found that could answer the question what the effect is of medial compared to inferior pedicle technique in reduction mammaplasty in ptosis and several adverse outcomes.
Sources: - |
Description of studies
As shown in table 1, all observational studies compared at least one superior, superomedial or medial pedicle technique to an inferior pedicle technique.
Table 1. Characteristics of included studies
|
Author, year |
Intervention |
Control |
N |
|
Mizgala 2000 |
Superior |
Inferior |
Superior: 9 Inferior: 65 |
|
Chiummariello 2008 |
Superior, medial, lateral |
Inferior |
Superior: 28 Medial: 25 Inferior: 23 |
|
Schlenz 2005 |
Lassus (superior) Lejour (superior) Würinger (inferocentral) McKissock (bipedicle) |
Georgiade (inferior) |
Lassus: 10 Lejour: 13 Würinger: 20 McKissock: 18 Georgiade: 19 |
|
Antony 2013 |
Superomedial |
Inferior |
Superomedial: 50 Inferior: 50 |
|
de Biasio 2017 |
Superior, medial |
Inferior |
Superior: 98 Medial: 84 Inferior: 76 |
|
Hamdi 2001 |
Superior |
Inferior |
Superior: 18 Inferior: 20 |
|
Ogunleye 2017 |
Superomedial |
Inferior |
Superomedial: 90 Inferior: 39 |
|
Sapino 2021 |
Superomedial |
Inferior |
Superomedial: 36 Inferior: 22 |
|
Toplu 2021 |
Superomedial, superior |
Inferior |
Superior: 55 Superomedial: 99 Inferior: 32 |
|
Chiummariello 2013 |
Superior |
Inferior |
Superior: 28 Inferior: 36 |
|
Makboul 2017 |
Superomedial |
Inferior |
Superomedial: 20 Inferior: 40 |
|
Jorgensen 2021 |
Orlando (superomedial) Hall-Findlay (medial) McKissock (bipedicle) |
Robbins (inferior) |
Orlando: 323 Hall-Findlay: 16 McKissock: 10 Robbins: 34 |
|
Kemaloglu 2018 |
Superomedial |
Inferior |
Superomedial: 25 Inferior: 50 |
Results
1. Superior versus inferior pedicle technique
1.1 Bottoming out
1.1.1 Nipple to inframammary fold area
One study reported the nipple to inframammary fold area comparing the superior and inferior pedicle technique. De Biasio (2017) reported the change in nipple to inframammary fold area (24th - 1st month) in cm. The superior pedicle technique resulted in 1.60 (SD 0.14) cm and the inferior pedicle technique in 3.28 (SD 0.53) cm (mean difference (MD) -1.68; 95% confidence interval (CI) -1.80, -1.56).
1.1.2 Ptosis
None of the included studies reported ptosis as an outcome measure.
1.2 Patient satisfaction
None of the included studies reported patient satisfaction as an outcome measure.
1.3. Adverse outcomes
1.3.1 Nipple and areola sensitivity
Four studies reported nipple sensitivity as outcome measure. Since the studies reported different measures and units, results were not pooled.
Chiummariello (2008) measured mean nipple-areola complex (NAC) sensitivity thresholds 30 days post-operatively. Higher thresholds indicate lower sensitivity. They found in the superior pedicle group threshold of 15.12 (SD 2.1) g/mm2 and in the inferior pedicle group 14.13 (SD 2.15) g/mm2 (MD 0.99; 95% CI -0.18, 2.16).
Hamdi (2001) measured nipple and areola sensitivity as mean thresholds pre-operatively, at 3 months and at 6 months post-operatively. In the superior pedicle group, the nipple sensitivity threshold changed from 26 (SEM 4) to 81 (SEM 29) to 52 (SEM 9) pre-operatively, at 3 months and at 6 months, respectively. In the inferior pedicle group, the nipple sensitivity was 23 (SEM 2), 75 (SEM 19) and 39 (SEM 4). Only at 3 months post-surgery a significant difference between the groups was found. The areolar sensitivity thresholds were also lower in the inferior pedicle group.
Toplu (2021) reported the percentage of patients that experienced nipple sensory loss. None of the 52 superior pedicle patients reported nipple sensory loss. In the inferior pedicle group, 1 out of 32 (3.1%) had nipple sensory loss.
Schlenz (2005) measured areola sensitivity at 3 weeks, 3 months, 6 months and 12 months post-operatively. No absolute data was presented, only figures. The sensitivity of the areola was decreased in all patients 3 weeks after surgery. Patients who underwent operation with an inferior pedicle technique reached preoperative values between 6 and 12 months postoperatively. A complete loss of sensitivity of the areola was found only in the superior pedicle groups, all cases being temporary.
Chiummariello (2013) measured nipple sensitivity at 3 weeks, 3 months, 6 months and 12 months post-operatively. The sensitivity was lower in patients treated with the superior pedicle at all time points. In the inferior pedicle group, the sensitivity was restored within 6 months, as opposed to the superior pedicle group that failed full recovery.
1.3.2 NAC loss
One study reported total areolar necrosis. Toplu (2021) reported total areolar necrosis in 1 patient in the inferior pedicle group (3.1%). Whether this led to NAC loss was not reported.
1.3.3 Fat necrosis
Two studies reported fat necrosis as outcome measure. Mizgala (2000) found fat necrosis in 2 out of 9 superior pedicle patients and 2 out of 65 inferior pedicle patients.
Toplu 2021 reported one superior pedicle patient (1.8%) and 0 inferior pedicle patients that developed fat necrosis.
1.3.4 Wound dehiscence
Two studies reported the number of patients with wound dehiscence. Mizgala (2000) and Toplu (2021) reported the number of patients developing wound dehiscence after surgery. Mizgala (2000) found 0 out 9 patients with wound dehiscence after the superior pedicle surgery and 1 out of 65 (1.5%) after the inferior pedicle surgery.
In Toplu (2021), no patients who underwent a superior pedicle procedure developed wound dehiscence. One out of 32 patients (3.1%) from the inferior pedicle procedure reported wound dehiscence.
1. Level of evidence of the literature
The level of evidence regarding the outcome measure bottoming out started as low, because the study was observational. The level of evidence was downgraded by 1 level because of the number of included patients (imprecision). The level of evidence for bottoming out is very low.
The level of evidence regarding the outcome measure nipple and areola sensitivity started as low, because all studies were observational. The level of evidence was downgraded by 1 level because of study limitations (heterogeneity, risk of bias) and conflicting results (inconsistency). The level of evidence for bottoming out is very low.
The level of evidence regarding the outcome measure NAC loss, fat necrosis and wound dehiscence started low, because the studies were observational. The level of evidence was downgraded by 1 level because of study limitations (risk of bias) the number of and included patients (imprecision). The level of evidence for bottoming out is very low.
2. Superomedial versus inferior pedicle technique
2.1 Bottoming out
2.1.1 Nipple to inframammary fold area
Two studies reported nipple to inframammary fold regarding bottoming out. Sapino (2021) reported mean (SD) area of infra-mammary fold to inferior border of NAC preoperatively, 2 weeks, 6 months and 24 months postoperatively. The outcomes are reported in table 2.
Table 2. infra-mammary fold to inferior border of NAC, superomedial versus inferior pedicle mean (SD)
|
|
Superomedial |
Inferior |
P |
MD (95% CI) |
|
Pre-operative |
12.9 (3.2) |
12.5 (3.9) |
0.1278 |
0.40 (-1.54, 2.34) |
|
2 weeks post-operative |
6.8 (1.1) |
7.0 (1.0) |
0.5219 |
-0.20 (-0.75, 0.35) |
|
6 months post-operative |
8.4 (1.4)
|
8.5 (1.2) |
0.8928 |
-0.10 (-0.78, 0.58) |
|
24 months post-operative |
8.8 (1.8) |
9.7 (1.1) |
<0.0001 |
-0.90 (-1.65, -0.15) |
Kemaloglu (2018) reported the elongation of NAC-inframammary fold distance at 1 year follow-up. They reported mean (SD) for left and right breast separately. The right pedicle was 2.15 (0.63) cm for superomedial compared for to 1.97 (0.60) for inferior pedicle technique (MD 0.18; 0.95% CI -0.12, 0.48). The left pedicle was 2.26 (0.66) for superomedial compared to 2.19 (0.61) for inferior pedicle technique (MD 0.07; 95% CI -0.24, 0.38).
2.1.2 Ptosis
Two studies reported ptosis as an outcome measure. Makboul (2017) found recurrence of breast ptosis in 1 out of 20 cases in the superomedial pedicle group (5.0%) and 15 out of 40 cases in the inferior pedicle group (37.5%) (RR 0.13; 95% CI 0.02, 0.94). This was considered clinically different in favor of the superomedial pedicle technique.
Sapino (2021) reported ptosis as a continuous outcome measure, quantified as cm of breast drooping under the infra-mammary fold. In the superomedial pedicle group, mean ptosis was 8.5 cm (SD 2.8) and in the inferior pedicle group 9.5 cm (SD 5.4)(MD -1.00; 95% CI -2.72, 0.72).
2.2 Patient satisfaction
Three studies reported patient satisfaction. All outcomes were continuous and reported as or converted to a score from 0 to 10. A MD of 1.17 (95% CI 0.84, 1.49) was found in favor of the inferior pedicle technique. Figure 1 shows the pooled data.

Figure 1: Patient satisfaction after reduction mammaplasty, superomedial versus inferior pedicle technique.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
2.3. Adverse outcomes
2.3.1 Nipple and areola sensitivity
Two studies reported nipple sensitivity as outcome measure. Antony (2013) reported decreased nipple sensation in 11 out of 100 reductions in the superomedial pedicle group and 13 out of 100 reductions in the inferior pedicle group.
Toplu (2021) reported nipple sensory loss in 0 out of 99 superomedial pedicle patients and 1 out of 32 (3.1%) inferior pedicle patients.
2.3.2 NAC loss
Three studies reported NAC loss or total NAC necrosis. As shown in figure 2, a risk difference (RD) of -0.01 (95% CI -0.04, 0.01) was found in favor of the superomedial pedicle technique. This difference was not considered clinically relevant.
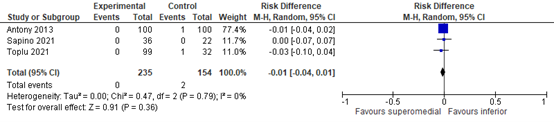
Figure 2: Incidence of NAC loss or necrosis after reduction mammaplasty, superomedial versus inferior pedicle technique.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
2.3.3 Fat necrosis
Three studies reported the incidence of fat necrosis. As shown in figure 3, a RD of -0.01 (95% CI -0.5, 0.02) was found in favor of the superomedial pedicle technique. This difference was not considered clinically relevant.
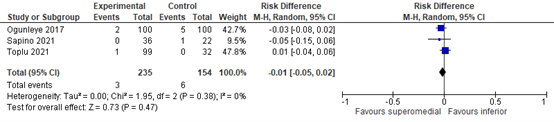
Figure 3: Incidence of fat necrosis after reduction mammaplasty, superomedial versus inferior pedicle technique.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
2.3.4 Wound dehiscence
Three studies reported the incidence of wound dehiscence. As shown in figure 4, a RR of 0.92 (95% CI: 0.34, 2.49) was found in favor of the superomedial pedicle technique. This difference was not considered clinically relevant.
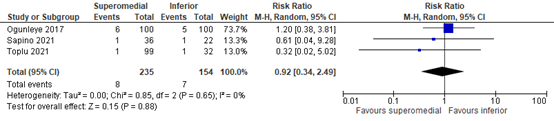
Figure 4: Incidence of wound dehiscence after reduction mammaplasty, superomedial versus inferior pedicle technique.
Z: p-value of the pooled effect; df: degrees of freedom; I2: statistic heterogeneity; CI: Confidence Interval
2. Level of evidence of the literature
The level of evidence regarding the outcome measure bottoming out started as low, because the study was observational. The level of evidence was downgraded by 1 level because of heterogeneity, the number of included patients (imprecision) and conflicting results (inconsistency). The level of evidence for bottoming out is very low.
The level of evidence regarding the outcome measure patient satisfaction started as low, because the studies were observational. The level of evidence was downgraded by 1 level because of number of included patients (imprecision). The level of evidence for patient satisfaction is very low.
The level of evidence for nipple and areola sensitivity and wound dehiscence started as low, because the studies were observational. The level of evidence was downgraded by 1 level because of number of included patients (imprecision) and conflicting results (inconsistency). The level of evidence for nipple and areola sensitivity, incidence of infection, hematoma and wound dehiscence is very low.
The level of evidence for incidence of NAC loss and fat necrosis started as low, because the studies were observational. The level of evidence was downgraded by 1 level because of number of included patients (imprecision). The level of evidence for NAC loss and fat necrosis is very low.
3. Medial versus inferior pedicle technique
3.1. Bottoming out
3.1.1 Nipple to inframammary fold area
One study reported the nipple to inframammary fold area comparing the medial and inferior pedicle technique. De Biasio (2021) reported the change in nipple to inframammary fold area (24th - 1st month) in cm. The medial pedicle technique resulted in 2.39 (SD 0.45) cm and the inferior pedicle technique in 3.28 (SD 0.53) cm (MD -0.89, 95% CI: -1.04, -0.74).
3.1.2 Ptosis
None of the included studies reported ptosis as an outcome measure.
3.2 Patient satisfaction
One study reported patient satisfaction scores. In Jorgensen (2021), ‘satisfaction with the outcome’ was scored on a scale from 0 to 100, with higher scores representing higher satisfaction. The medial pedicle technique scored 89.06 (SD 13.02) versus 74.87 (SD 22.48) for the inferior pedicle technique (MD 14.19, 95% CI: 4.30, 24.08).
3.3 Adverse outcomes
3.3.1 Nipple and areola sensitivity
One study reported NAC sensitivity. Chiummariello (2008) measured mean sensitivity at 30 days post-operatively. Patients that underwent the medial pedicle procedure had a sensitivity threshold of 14.9 (SD 3.26) and those with an inferior pedicle 14.13 (SD 2.15) g/mm2 (MD 0.77, 95% CI: -0.78, 2.32).
3.3.2 NAC loss
None of the included studies reported the incidence of NAC loss as an outcome measure.
3.3.3 Fat necrosis
None of the included studies reported the incidence of fat necrosis as an outcome measure.
3.3.4 Wound dehiscence
None of the included studies reported the incidence of wound dehiscence as an outcome measure.
3. Level of evidence of the literature
The level of evidence regarding the outcome measure bottoming out, patient satisfaction and nipple and areola sensitivity started low, because the studies were observational. The level of evidence was downgraded by 1 level because of number of included patients (imprecision). The level of evidence for bottoming out, patient satisfaction, nipple and areola sensitivity and infection is very low.
No studies were included reporting NAC loss, fat necrosis and wound dehiscence.
A systematic review of the literature was performed to answer the following question:
What are the effects of the superior, superomedial and medial pedicle technique compared to the inferior pedicle technique in mamma reduction patients on bottoming out, patient satisfaction and adverse outcomes?
P (patients): Mamma reduction patients
I (intervention): 1. Superior, 2. superomedial and 3. medial pedicle
C (control): Inferior pedicle
O (outcome measure): Bottoming out (Area nipple to inframammary fold, ptosis)
Patient satisfaction
Adverse outcomes (decrease in nipple sensitivity, nipple-areola complex (NAC) loss, fat necrosis, wound dehiscence)
Relevant outcome measures
The guideline development group considered bottoming out and patient satisfaction as critical outcome measures for decision making; and the adverse outcomes as an important outcome measure for decision making.
The working group defined minimal clinically (patient) important differences for the continuous outcome patient satisfaction a mean difference (MD) of < -1 or > 1 on a 10-point scale or MD < -10 or > 10 on a 100-point scale. For dichotomous outcomes, a difference of 10% was considered clinically relevant (relative risk: 0.91≤RR≥1.10 or -0.10≤RD≥0.10).
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until 14-9-2021. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 169 hits. Studies were selected based on the following criteria:
- Published ≥ 2000
- Patients ≥ 18 years
- Conform PICO
Thirty-one studies were initially selected based on title and abstract screening. After reading the full text, 18 studies were excluded (see the table with reasons for exclusion under the tab Methods), and 13 studies were included.
Results
Thirteen observational studies were included in the analysis of the literature. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Antony AK, Yegiyants SS, Danielson KK, Wisel S, Morris D, Dolezal RF, Cohen MN. A matched cohort study of superomedial pedicle vertical scar breast reduction (100 breasts) and traditional inferior pedicle Wise-pattern reduction (100 breasts): an outcomes study over 3 years. Plast Reconstr Surg. 2013 Nov;132(5):1068-1076. doi: 10.1097/PRS.0b013e3182a48b2d. PMID: 24165588; PMCID: PMC3923626.
- De Biasio F, Zingaretti N, De Lorenzi F, Riccio M, Vaienti L, Parodi PC. Reduction Mammaplasty for Breast Symmetrisation in Implant-Based Reconstructions. Aesthetic Plast Surg. 2017 Aug;41(4):773-781. doi: 10.1007/s00266-017-0867-2. Epub 2017 Apr 3. PMID: 28374302.
- Chiummariello S, Cigna E, Buccheri EM, Dessy LA, Alfano C, Scuderi N. Breastfeeding after reduction mammaplasty using different techniques. Aesthetic Plast Surg. 2008 Mar;32(2):294-7. doi: 10.1007/s00266-007-9023-8. Epub 2007 Sep 5. PMID: 17805921.
- Chiummariello S, Angelisanti M, Arleo S, Alfano C. Evaluation of the sensitivity after reduction mammoplasty. Our experience and review of the literature. Ann Ital Chir. 2013 Jul-Aug;84(4):385-8. PMID: 23916996.
- Hamdi M, Greuse M, De Mey A, Webster MH. A prospective quantitative comparison of breast sensation after superior and inferior pedicle mammaplasty. Br J Plast Surg. 2001 Jan;54(1):39-42. doi: 10.1054/bjps.2000.3456. PMID: 11121316.
- Jørgensen MG, Albertsdottir E, Dalaei F, Hesselfeldt-Nielsen J, Schmidt VJ, Sørensen JA, Toyserkani NM. Age and Body Mass Index Affect Patient Satisfaction Following Reduction Mammoplasty: A Multicenter Study Using BREAST-Q. Aesthet Surg J. 2021 May 18;41(6):NP336-NP345. doi: 10.1093/asj/sjaa395. PMID: 33561191.
- Kemalo?lu CA, Özocak H. Comparative Outcomes of Inferior Pedicle and Superomedial Pedicle Technique With Wise Pattern Reduction in Gigantomastic Patients. Ann Plast Surg. 2018 Mar;80(3):217-222. doi: 10.1097/SAP.0000000000001231. PMID: 28984653.
- Makboul M, Abdelhamid MS, Al-Attar GS. Long-term follow-up and patient satisfaction after reduction mammoplasty: Superomedial versus inferior pedicle. Indian J Plast Surg. 2016 May-Aug;49(2):214-219. doi: 10.4103/0970-0358.191299. PMID: 27833284; PMCID: PMC5052994.
- Mizgala CL, MacKenzie KM. Breast reduction outcome study. Ann Plast Surg. 2000 Feb;44(2):125-33; discussion 133-4. doi: 10.1097/00000637-200044020-00001. PMID: 10696037.
- Ogunleye AA, Leroux O, Morrison N, Preminger AB. Complications After Reduction Mammaplasty: A Comparison of Wise Pattern/Inferior Pedicle and Vertical Scar/Superomedial Pedicle. Ann Plast Surg. 2017 Jul;79(1):13-16. doi: 10.1097/SAP.0000000000001059. PMID: 28328638.
- Sapino G, Haselbach D, Watfa W, Baudoin J, Martineau J, Guillier D, di Summa PG. Evaluation of long-term breast shape in inferior versus superomedial pedicle reduction mammoplasty: a comparative study. Gland Surg. 2021 Mar;10(3):1018-1028. doi: 10.21037/gs-20-440. Erratum in: Gland Surg. 2021 May;10(5):1840. PMID: 33842246; PMCID: PMC8033061.
- Schlenz I, Rigel S, Schemper M, Kuzbari R. Alteration of nipple and areola sensitivity by reduction mammaplasty: a prospective comparison of five techniques. Plast Reconstr Surg. 2005 Mar;115(3):743-51; discussion 752-4. doi: 10.1097/01.prs.0000152435.03538.43. PMID: 15731673.
- Toplu G, Alt?nel D, Serin M. Evaluation of Factors Related to Postoperative Complications in Patients Who Underwent Reduction Mammoplasty. Eur J Breast Health. 2021 Mar 31;17(2):157-164. doi: 10.4274/ejbh.galenos.2021.6336. PMID: 33870116; PMCID: PMC8025730.
Evidence tables
Risk of bias table for intervention studies (observational: non-randomized clinical trials, cohort and case-control studies)
|
Study reference
(first author, year of publication) |
Bias due to a non-representative or ill-defined sample of patients?1
(unlikely/likely/unclear) |
Bias due to insufficiently long, or incomplete follow-up, or differences in follow-up between treatment groups?2
(unlikely/likely/unclear)
|
Bias due to ill-defined or inadequately measured outcome ?3
(unlikely/likely/unclear) |
Bias due to inadequate adjustment for all important prognostic factors?4
(unlikely/likely/unclear) |
|
Mizgala 2000 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Likely Note: follow-up varied between 4 and 67 months. |
Unclear Note: outcome measures were not defined |
Likely Note: small, inequal groups in combination with lots of prognostic factors |
|
Chiummariello 2008 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Unlikely Note: follow-up was 3 years for all groups |
Unlikely Note: outcome measures were well-defined |
Likely Note: small groups in combination with lots of prognostic factors |
|
Schlenz 2005 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Unlikely Note: follow-up was equal for all groups |
Unlikely Note: outcome measures were well-defined |
Likely Note: small groups in combination with lots of prognostic factors |
|
Antony 2013 |
Unlikely: Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient. Out of 382 patients, 100 were matched based on age and reduction weight. |
Unclear Note: Follow-up varied between 3 and 6 months, unclear if this differed between groups. |
Likely Note: aesthetic outcomes were measured ‘ad hoc’. |
Unlikely Note: Unlikely due to matching based on prognostic factors |
|
De Biasio 2017 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Unlikely Note: follow-up was equal for all groups |
Unlikely Note: outcome measures were well-defined |
Likely Note: small groups in combination with lots of prognostic factors |
|
Hamdi 2001 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient. Groups were matched. |
Likely Note: Follow-up was short and often incomplete. |
Unlikely Note: outcome measures were well-defined |
Likely Note: small groups in combination with lots of prognostic factors |
|
Ogunleye 2017 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Likely Note: follow-up varied |
Likely Note: Outcome measures were not assessed uniformly |
Unlikely Prognostic factors were adequately adjusted for. |
|
Sapino 2021 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Unlikely Note: follow-up was equal for all groups |
Unlikely Note: outcome measures were well-defined |
Likely Note: small groups in combination with lots of prognostic factors. |
|
Toplu 2021 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Unclear Note: Follow-up varied between 2 and 7 years, unclear if this differed between groups. |
Unlikely Note: outcome measures were well-defined |
Likely Note: Not adjusted for prognostic factors |
|
Chiummariello 2013 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Unlikely Note: follow-up was equal for all groups |
Unlikely Note: outcome measures were well-defined |
Likely Note: Not adjusted for prognostic factors |
|
Makboul 2017 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Likely Note: Length of follow-up was at least 1 year for each patient. No additional details provided. |
Unclear Note: not all outcome measures were defined |
Likely Note: small groups in combination with lots of prognostic factors, no adjustments. |
|
Jorgensen 2021 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Unclear Note: only mean length of follow-up reported. Range is unknown. |
Unlikely Note: outcome measures were well-defined |
Unlikely Prognostic factors were adequately adjusted for. |
|
Kemaloglu 2018 |
Unclear Note: patients were assigned to the groups according to the surgeon’s decision appropriate for the patient |
Unlikely Note: follow-up was equal for all groups |
Unclear Note: outcome measures were not defined |
Likely Note: small groups in combination with lots of prognostic factors, no adjustments. |
Table of excluded studies
|
Author and year |
Reason for exclusion |
|
McCulley 2009a |
A priori defined outcomes were not reported |
|
Beer 2004 |
No comparison |
|
Kakagia 2005 |
A priori defined outcomes were not reported |
|
Brownlee 2017 |
Wrong intervention |
|
Blondeel 2003 |
Wrong intervention |
|
Ghareeb 2017 |
A priori defined outcomes were not reported |
|
Spear 2003a |
No comparison |
|
Spear 2003b |
No comparison |
|
Villani 2009 |
No comparison |
|
Anzarut 2008 |
No comparison |
|
Hamdi 2001 |
Duplicate |
|
Kalkarni 2019 |
Wrong intervention |
|
Manahan 2015 |
No comparison |
|
Fernandez 2016 |
Wrong intervention |
|
Derby 2016 |
Wrong intervention |
|
Davison 2007 |
A priori defined outcomes were not reported |
|
McCulley 2009b |
Wrong intervention |
|
Bauermeister 2019 |
A priori defined outcomes were not reported |
Beoordelingsdatum en geldigheid
Publicatiedatum : 09-10-2023
Beoordeeld op geldigheid : 01-10-2023
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten die een mammareductie ondergaan.
Werkgroep
Drs. E.M.J. (Esther) Mesters, (voorzitter), plastisch chirurg, NVPC
Drs. M.F. (Mirjam) Hoefkens, plastisch chirurg, NVPC
Dr. C. (Corinne) Schouten, plastisch chirurg, NVPC
Dr. C.P.H. (Celien) Vreuls, patholoog, NVVP
Drs. K.M. (Katya) Duvivier, radioloog, NVvR
Drs. L.J. (Laura) Schijf, radioloog, NVvR
Drs. K. (Klaartje) Spijkers, senior adviseur patiëntbelang, Patiëntenfederatie Nederland
Met ondersteuning van
Dr. F. Willeboordse, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
I. van Dijk, junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
* Voorzitter |
Plastisch Chirurg
Mesters kliniek te Oisterwijk 01-12-2022 en Eyevolve-clinic te Schilde 01-12-2022 |
Geen |
Geen |
Geen actie |
|
Hoefkens |
Plastisch Chirurg - Alexander Monro Ziekenhuis (0,74 fte) |
Geen |
Geen |
Geen actie |
|
Schouten |
Plastisch chirurg in het Rijnstate Ziekenhuis in Arnhem. |
Geen |
Geen |
Geen actie |
|
Duvivier |
Radioloog AmsterdamUMC 0,8FTE |
Geen |
Geen |
Geen actie |
|
Schijf |
Radioloog AmsterdamUMC 0,7 FTE |
Geen |
Geen |
Geen actie |
|
Vreuls |
Patholoog (UMCU 0,8 FTE) |
voorzitter expert commissie mamma van de NVVP (onbetaald) |
Geen |
Geen actie |
|
Spijkers |
Senior adviseur bij MSZ Patiëntfederatie Nederland |
Geen |
Geen |
Geen actie |
|
Willeboordse |
Senior adviseur, Kennisinstituut Federatie Medisch specialisten |
Geen |
Geen |
Geen actie |
|
Van Dijk |
Junior adviseur, Kennisinstituut Federatie Medisch specialisten |
Geen |
Geen |
Geen actie |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland voor de schriftelijke knelpunteninventarisatie en afvaardiging in de werkgroep. Het verslag van de knelpunteninventarisatie (zie aanverwante producten) is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Wkkgz & Kwalitatieve raming van mogelijke substantiële financiële gevolgen
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijn is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling zijn richtlijnmodules op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
Module |
Uitkomst raming |
Toelichting |
|
Module Preoperatieve beeldvorming |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet OF het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Tepelsteeltechniek |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet OF het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Drainbeleid |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet OF het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Tranexaminezuur |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet OF het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Postoperatief pathologisch onderzoek |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet OF het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
|
Module Organisatie van zorg |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbeveling(en) breed toepasbaar zijn (5.000-40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet OF het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening betreft. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten die een mammareductie ondergaan. Tevens zijn er knelpunten aangedragen door relevante partijen via een schriftelijke knelpunteninventarisatie. Een verslag hiervan is opgenomen onder aanverwante producten.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Literature search strategy
|
Database |
Zoektermen |
||||||||||||||||||||||||||||||||||||
|
Embase
|
|
||||||||||||||||||||||||||||||||||||
|
Medline (OVID)
|
1 (((mammoplast* or mammaplast*or mastoplast*) adj3 (reduction or reductive)) or 'breast reduction*').ti,ab,kf. (2354) 2 ((craniomedi* or superomedi* or superior or cranial or lateral or laterocrani*) adj3 pedicle).ti,ab,kf. (999) 3 1 and 2 (154) 4 limit 3 to ((english or dutch) and yr="2000-Current") (132) 5 4 not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) (125) 6 (meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf.) not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) (518201) 7 (exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw.) not (animals/ not humans/) (2163730) 8 Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ [Onder exp cohort studies vallen ook longitudinale, prospectieve en retrospectieve studies] (3936155) 9 5 and 6 (3) – SRs 10 (5 and 7) not 9 (11) - RCTs 11 (5 and 8) not (9 or 10) (75) - observationeel 12 9 or 10 or 11 (89) 13 5 not 12 (36) – overige studiedesigns
|