Hoofdstuk 15: V-notes
Uitgangsvraag
Is V-NOTES (Vaginal Natural Orifice Transluminal Endoscopic Surgery) beter dan vaginale, laparoscopische of abdominale hysterectomie bij vrouwen die een hysterectomie ondergaan voor een benigne indicatie?
Aanbeveling
Verkies een vaginale hysterectomie (VH) boven een V-NOTES hysterectomie bij vrouwen die een hysterectomie voor benigne indicatie ondergaan.
Overweeg een V-NOTES hysterectomie in plaats van een laparoscopische hysterectomie (LH) bij vrouwen die een hysterectomie voor benigne indicatie ondergaan, en geen verklevingen hebben in Douglas.
Implementeer de nieuwe V-NOTES operatie volgens de richtlijnen van een introductie van een nieuwe techniek in het ziekenhuis met een gesuperviseerde leercurve van de operateur.
Voer bij vrouwen die een hysterectomie voor een benigne indicatie ondergaan alleen een abdominale hysterectomie (AH) uit wanneer vaginale (VH), laparoscopische (LH) en V-NOTES hysterectomie gecontraïndiceerd zijn.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
De resultaten van de literatuuranalyse zijn opgesplitst voor V-NOTES (Vaginal Natural Orifice Transluminal Endoscopic Surgery) vergeleken met vaginale hysterectomie (VH), laparoscopische hysterectomie (LH) en abdominale hysterectomie (AH).
1. V-NOTES vergeleken met een vaginale hysterectomie.
Er werd 1 studie geïncludeerd (Lee, 2019) waarin V-NOTES werd vergeleken met een vaginale hysterectomie. De bewijskracht voor de uitkomstmaten is in alle gevallen gegradeerd als GRADE ‘zeer laag’, vanwege imprecisie (er was een kleine sample size van 14 versus 42 vrouwen), risk of bias (mogelijke selectie bias) en indirectheid (sterk verminderde extrapoleerbaarheid van de resultaten omdat in deze studie werd gekeken naar transmannen bij wie gelijktijdig met V-NOTES of VH frequent ook een vaginectomie werd uitgevoerd. Deze ingreep is geassocieerd met operatieve risico’s en vermindert daarmee de mate waarin deze resultaten kunnen worden overgenomen). De overall bewijskracht is gelijk aan de laagst gevonden bewijskracht voor de cruciale uitkomstmaat en is daarmee voor de vergelijking met VH gegradeerd als ‘zeer laag’.
Een theoretisch voordeel van de V-NOTES techniek ten opzichte van de VH zou het verwijderen van de tubae tijdens een hysterectomie kunnen zijn. Veel gynaecologen counselen vrouwen over het verwijderen van de tubae tijdens een hysterectomie om de kans op toekomstig ovariumcarcinoom te verkleinen. Het is echter nog niet onderzocht of een tubectomie tijdens V-NOTES gemakkelijker is en/of minder complicaties geeft dan tijdens een VH.
Een ander nog niet door onderzoek gestaafd gegeven zijn de kosten van de V-NOTES ten opzichte van de VH. Het lijkt echter aannemelijk dat in de Nederlandse situatie V-NOTES duurder is dan een VH omdat er extra disposables (gelpad, trocars en hemostase instrument) en re-usables (laparoscoop met toebehoren, laparoscopisch instrumentarium) moeten worden gebruikt tijdens de V-NOTES.
2. V-NOTES vergeleken met een laparoscopische hysterectomie
De resultaten van de literatuuranalyse laten zien dat V-NOTES vergeleken met een laparoscopische hysterectomie mogelijk leidt tot minder postoperatieve complicaties, kortere operatieduur en een korter ziekenhuisverblijf. Deze uitkomsten werden beoordeeld met een GRADE ‘laag’, wegens risk of bias. Het is onzeker wat het effect van V-NOTES is op de uitkomstmaten intra-operatieve complicaties, bloedverlies en postoperatieve pijn. Deze uitkomstmaten werden beoordeeld met een GRADE ‘zeer laag’, wegens risk of bias en imprecisie (gevonden effect bevatte de waarde van geen (klinisch relevant) effect) dan wel inconsistentie (heterogeniteit in de richting van het effect tussen studies) in het gevonden bewijs. Het was niet mogelijk om de bewijskracht voor de uitkomstmaten operatieve kosten en tijd tot hervatten dagelijkse activiteiten of werk te onderzoeken. Operatieve kosten uit de gevonden studies zijn onvoldoende vergelijkbaar met de Nederlandse gezondheidszorg. Er werden geen studies gevonden waarin was gekeken naar de tijd tot hervatten van dagelijkse activiteiten of het werk.
De overall bewijskracht is gelijk aan de laagst gevonden bewijskracht voor de cruciale uitkomstaat en die is gegradeerd als ‘laag’.
V-NOTES hysterectomie lijkt veelbelovend als er inderdaad minder postoperatieve complicaties zijn dan na LH. Enige voorzichtigheid met de interpretatie van de huidige literatuur lijkt echter op zijn plaats omdat publicaties van V-NOTES nu nog afkomstig zijn van early adopters. Een multicenter studie met grote aantallen gaat waarschijnlijk al een reëler beeld weergeven van het optreden van postoperatieve complicaties.
Een belangrijk punt dat niet goed naar voren komt in de huidige literatuur is het morcelleren van de sterk vergrote uterus. De V-NOTES is een techniek die vooral zijn voordeel lijkt te hebben in het vaginaal verwijderen van grotere uteri, omdat kleinere uteri ook via een vaginale hysterectomie zouden kunnen worden uitgevoerd. Echter, juist bij grotere uteri bestaat alleen de mogelijkheid om transvaginaal te morcelleren, terwijl er tijdens een LH zowel transabdominaal (papierrolmethode en met een ‘morcellator’) als transvaginaal gemorcelleerd (papierrol methode) kan worden. Met name transvaginale morcellatie volgens de papierrol methode is technisch moeilijker omdat het incisievlak vaak beperkt is, moeilijk a vue te krijgen kan zijn, en de longitudinale as van het mesheft zich in een beperkte ruimte kan bevinden. Deze beperkingen spelen extra bij nulli para of vrouwen een anderszins nauwe vaginale toegang.
Mochten er aanwijzingen zijn voor verklevingen in Douglas bijvoorbeeld als gevolg van diepe endometriose ter plaatse of na rectumchirurgie, dan is een LH te verkiezen boven V-NOTES. Een operatie van bovenaf tijdens LH geeft meer overzicht op het dissectievlak, de omliggende structuren, en het te verwijderen weefsel (in geval van endometriose) dan tijdens de benadering van onderaf via V-NOTES.
3. V-NOTES vergeleken met een abdominale hysterectomie.
Er zijn geen studies gevonden in de literatuursearch waarin is gekeken naar de vergelijking tussen V-NOTES en een abdominale hysterectomie. Er kon daarom geen GRADE-beoordeling worden uitgevoerd. De overall bewijskracht voor deze uitkomstmaat is gegradeerd als ‘zeer laag’, omdat het effect onbekend is. Gezien de impact van de ingreep wordt een AH alleen geadviseerd als VH, LH en V-NOTES om wat voor reden dan ook gecontraïndiceerd zijn
Waarden en voorkeuren van patiënten (en eventueel hun verzorgers)
Voor de patiënte belangrijke potentiele voordelen van de V-NOTES, zoals minder postoperatieve complicaties, lijken nog in een grote multicenter studie bevestigd te moeten worden, waarbij ook beter gekeken kan worden of een significant kortere opnameduur ook leidt tot een relevant korter herstel en hervatting van dagelijkse activiteiten. Een kortere operatietijd is voordeliger voor patiënten omdat zij dan minder lang geëxposeerd zijn aan de risico’s van anesthesie en peroperatieve complicaties.
Een veel gehoord voordeel van de V-NOTES ten opzichte van de LH is het ontbreken van zichtbare abdominale littekens. Het is nog niet onderzocht welke waarde de (Nederlandse) patiënte hier aan hecht. Het lijkt voor de hand te liggen dat vrouwen het ontbreken van littekens, ook de kleine littekens van een laparoscopie, op prijs zouden stellen. Er zouden echter wel eens internationale subjectieve verschillen in deze waardering kunnen zijn. Zo is de single port hysterectomie/ adnexchirurgie via de navel (ook geen zichtbare littekens) erg populair in Zuid-Korea, omdat deze vrouwen abdominale littekens als een groot cosmetisch bezwaar zouden ervaren. In Nederland hebben cosmetische bezwaren niet geleid tot brede implementatie van de single port chirurgie.
Kosten (middelenbeslag)
Er zijn nog geen kostenvergelijkende studies gedaan tussen V-NOTES, LH en VH die van toepassing zouden kunnen zijn op de Nederlandse situatie. Voor de V-NOTES is onder andere een disposabel customized gelpad met 3 trocars nodig en dit kost in Nederland rond de €450,-. De benodigde vessel seal/energy devices variëren in kosten van €250,- tot €600,-.
De enige data die bekend zijn over de kosten gaan over de Belgische studie van Baekelandt (2018) en de Taiwanese studie van Wang (2014). Hieronder een korte beschrijving.
In de Belgische studie van Baekelandt (2018) werd geen verschil gerapporteerd in directe gezondheid gerelateerde kosten tussen total LH (€4,103 (standaard deviatie (SD) 1,348)) en V-NOTES (€3,599 (SD 914)) (gemiddeld verschil €-504 (€-1,044 tot €36)). De kosten waren berekend op basis van het verschil in ziekenhuisrekening 6 weken post-operatief. Omdat de Belgische overheid de kosten van disposables tot 550 euro vergoed zijn de totale kosten eigenlijk niet helemaal compleet voor wat betreft de kosten van de disposables.
In de Taiwanese studie van Wang (2014) werden significant hogere kosten voor V-NOTES gerapporteerd, vergeleken met LAVH (New Taiwan Dollar (NTD) 22,573.3 (SD 5528.8) versus 17,744.6 (SD 8939.2) P<0.001). Deze hoge kosten werden verklaard door de hogere kosten van de disposable devices (wound retractor en vessel sealing device) ondanks de kortere verblijfsduur in het ziekenhuis in de V-NOTES groep. Ook hier werd een gedeelte van de kosten door het nationale verzekeringsplan vergoed, maar hier is niet gespecificeerd om welk bedrag of welke producten werden vergoed.
Het is dus onduidelijk wat de kosten van V-NOTES vergeleken met VH, LH en AH zijn voor de Nederlandse gezondheidszorg.
Aanvaardbaarheid, haalbaarheid en implementatie
V-NOTES is een nieuwe techniek om de uterus te verwijderen en is tijdens het schrijven van deze richtlijn nog niet geïmplementeerd in de meeste ziekenhuizen. Het wordt geadviseerd om een vooraf bepaald implementatietraject te volgen waarbij rekening wordt gehouden met het feit dat deze operatie als een nieuwe techniek moet worden ingevoerd, en een gesuperviseerde leercurve van de operateur wordt nagestreefd. De implementatie van deze techniek lijkt op voorwaarde van het voorafgaande, en het feit dat met al bestaand instrumentarium dat innovatief wordt ingezet op een voor veel gynaecologen vertrouwde wijze van opereren (vaginale route) aanvaardbaar en haalbaar.
Rationale van aanbeveling 1: weging van argumenten voor en tegen de interventies
De overall bewijskracht voor de vergelijking V-NOTES versus VH is gegradeerd met een GRADE ‘zeer laag’. Het is aannemelijk dat de kosten van de ingreep met V-NOTES vergeleken met VH hoger zijn. Op basis van het gebrek aan bewijs en de kosten wordt aanbevolen om VH boven V-NOTES uit te voeren.
Rationale van aanbeveling 2: weging van argumenten voor en tegen de interventie
De overall bewijskracht voor de vergelijking V-NOTES versus LH is gegradeerd met een GRADE ‘laag’. V-NOTES hysterectomie lijkt veelbelovend als er inderdaad minder postoperatieve complicaties, een kortere operatietijd en eerder ontslag uit het ziekenhuis zijn dan na LH. Enige voorzichtigheid met de interpretatie van de huidige literatuur lijkt echter op zijn plaats omdat publicaties van V-NOTES nu nog afkomstig zijn van early adopters die vaak technisch vaardiger zijn, meer ingrepen doen, en daardoor minder complicaties hebben dan de gemiddelde gynaecoloog. Een multicenter studie met grote aantallen gaat waarschijnlijk al een reëler beeld weergeven van het optreden van postoperatieve complicaties. Let wel, bij verklevingen in het cavum Douglasi heeft een LH de voorkeur boven V-NOTES omdat de complexe dissectie van bovenaf bij een LH meer overzicht geeft dan van onderaf via V-NOTES. Het wordt geadviseerd om een vooraf bepaald implementatietraject te volgen waarbij rekening wordt gehouden met het feit dat deze operatie als een nieuwe techniek moet worden ingevoerd, en een gesuperviseerde leercurve van de operateur wordt nagestreefd.
Rationale van aanbeveling 3: weging van argumenten voor en tegen de interventies
Er zijn geen studies gevonden in de literatuursearch waarin is gekeken naar de vergelijking tussen V-NOTES en een abdominale hysterectomie. Er kon daarom geen GRADE-beoordeling worden uitgevoerd. De overall bewijskracht voor deze uitkomstmaat is gegradeerd als ‘zeer laag’, omdat het effect onbekend is. Gezien de impact van de ingreep wordt een AH alleen geadviseerd als VH, LH en V-NOTES om wat voor reden dan ook gecontraïndiceerd zijn.
Onderbouwing
Sinds een aantal jaren wordt een nieuwe techniek toegepast om de uterus te verwijderen; naast de inmiddels bekende abdominale hysterectomie (AH), vaginale hysterectomie (VH), laparoscopische hysterectomie (LH) en laparoscopisch robot-geassisteerde hysterectomie is de V-NOTES (Vaginal Natural Orifice Transluminal Endoscopic Surgery) in opkomst; een vaginale hysterectomie die grotendeels wordt verricht met laparoscopisch instrumentarium. Deze richtlijnmodule moet antwoord geven of de V-NOTES een veilige techniek is en of het beter is dan de conventionele methoden. Hierbij wordt gekeken naar complicaties, bloedverlies, operatieduur, operatiekosten, postoperatieve pijn, postoperatief gebruik pijnstilling, aantal dagen in het ziekenhuis, postoperatief hervatten dagelijkse activiteiten en postoperatief hervatten werk.
1. V-NOTES compared to vaginal hysterectomy (VH)
|
Very low GRADE |
It is uncertain what the effect of V-NOTES compared to vaginal hysterectomy is on the following outcome measures in women with benign gynecological disease: intra-operative complications, post-operative complications, blood loss, operative time, post-operative pain at 2, 24, 48 and 72 hours, post-operative use of pain medication, and length of hospital stay.
Sources: Lee, 2019 |
|
- GRADE |
It is unknown what the effect of V-NOTES compared to vaginal hysterectomy is on the following outcome measures in women with benign gynecological disease: operative costs, time-to resuming daily activities post-operatively and time-to resuming work post-operatively. None of the included studies reported the outcome measures.
Sources: Lee,2019 |
2. V-NOTES compared to laparoscopic hysterectomy (LH)
|
Very low GRADE |
It is uncertain what the effect of V-NOTES compared to laparoscopic hysterectomy is on intra-operative complications in women with benign gynecological disease.
Sources: Badiglian-Filho, 2020; Baeklandt, 2018; Kaya, 2020; Kim, 2017; Puisungnoen, 2020; Wang, 2014; Yang, 2014 |
|
Low GRADE |
V-NOTES compared to laparoscopic hysterectomy might lead to a lower number of post-operative complications in women undergoing hysterectomy for benign gynecological disease.
Sources: Baeklandt, 2018; Kaya, 2020; Kim, 2017; Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020 |
|
Very low GRADE |
It is uncertain what the effect of V-NOTES compared to laparoscopic hysterectomy is on blood loss in women with benign gynecological disease.
Sources: Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020 |
|
Low GRADE |
V-NOTES compared to laparoscopic hysterectomy might lead to a lower operative time in women undergoing hysterectomy for benign gynecological disease.
Sources: Badiglian-Filho, 2020; Baeklandt, 2018; Kaya, 2020; Kim, 2017; Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020 |
|
- GRADE |
It is unclear what the effect of V-NOTES compared to laparoscopic hysterectomy is on the operative costs in women undergoing hysterectomy for benign gynecological disease.
Sources: Baeklandt, 2018; Wang, 2014 |
|
Very low GRADE |
It is uncertain what the effect of V-NOTES compared to laparoscopic hysterectomy is on post-operative pain at 6 hours in women with benign gynecological disease.
Sources: Kaya, 2017; Puisungnoen, 2020 |
|
Very low GRADE |
It is uncertain what the effect of V-NOTES compared to laparoscopic hysterectomy is on post-operative pain at 12 hours in women with benign gynecological disease.
Sources: Yang, 2014 |
|
Very low GRADE |
It is uncertain what the effect of V-NOTES compared to laparoscopic hysterectomy is on post-operative pain at 24 hours in women with benign gynecological disease.
Sources: Baeklandt, 2018; Kaya, 2020; Puisungnoen, 2020; Yang, 2014 |
|
- GRADE |
It is unclear what the effect of V-NOTES compared to laparoscopic hysterectomy is on the post-operative pain in the studies by Badiglian-Filho, (2020) and Yang (2020), as moment of measurement was unknown.
Sources: Badiglian-Filho,2020; Yang, 2020 |
|
Very low GRADE |
It is uncertain what the effect of V-NOTES compared to laparoscopic hysterectomy is on post-operative use of pain medication in women with benign gynecological disease.
Sources: Puisungnoen, 2020 |
|
Low GRADE |
V-NOTES compared to laparoscopic hysterectomy might lead to a lower length of hospital stay in women undergoing hysterectomy for benign gynecological disease.
Sources: Badiglian-Filho, 2020; Baeklandt, 2018; Kaya, 2020; Kim, 2017; Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020 |
|
- GRADE |
It is unknown what the effect of V-NOTES compared to laparoscopic hysterectomy is on the outcome measures time-to resuming daily activities post-operatively and time-to resuming work post-operatively. None of the included studies reported the outcome measures. |
3. V-NOTES compared to abdominal hysterectomy (AH)
|
- GRADE |
It is unknown what the effect of V-NOTES compared to abdominal hysterectomy is on the outcome measures complications, blood loss, operative time, operative costs, post-operative pain, post-operative use of pain medication, length of hospital stay, time-to resuming daily activities post-operatively and time-to resuming work post-operatively. None of the included studies reported the outcome measures. |
Description of studies
In total, four studies were included in the analysis of the literature, one systematic review and meta-analysis (Housemans, 2020) and three retrospective cohort studies (Badiglian-Filho, 2020; Lee, 2019; Puisungnoen, 2020).
Housemans (2020) performed a systematic review and meta-analysis of the literature to study the effectiveness of V-NOTES compared to laparoscopic hysterectomy in women with benign indications for hysterectomy. The following databases were searched until 8 October 2020: MEDLINE (PubMed interface), EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL) and additional sources (see for complete list p. 3 of Housmans, 2020). Inclusion criteria were randomised controlled trials (RCTs), controlled clinical trials (CCTs) and prospective/retrospective cohort studies in human subjects that allowed direct comparison of V-NOTES to laparoscopy. Hence, studies comparing V-NOTES with abdominal and vaginal hysterectomy were excluded. In addition, studies on interventions for genital prolapse or gynecological malignancy were excluded. In total 6 studies were included, 1 RCT (Baeklandt, 2019) and 5 observational cohort studies (Kaya, 2020; Kim, 2018; Wang, 2014; Yang, 2014; Yang, 2020). Table 15.1 Description of intervention group and control group, per study as included by Housemans (2020) shows the specific intervention per study.
Table 15.1 Description of intervention group and control group, per study as included by Housemans (2020)
|
Author |
Intervention group |
Control group |
|
Baekland, 2019 |
vNOTES hysterectomy (VANH) plus 4 superficial non-therapeutic skin incisions identical to those in the control group. |
TLH (total laparoscopic hysterectomy) |
|
Kaya, 2020 |
vNOTES |
TLH (total laparoscopic hysterectomy) |
|
Kim, 2018 |
NAVH (NOTES-assisted vaginal hysterectomy) |
LAVH (laparoscopy-assisted vaginal hysterectomy) |
|
Wang, 2014 |
tVNOTHEH (transvaginal natural orifice transluminal endoscopic hysterectomy) |
LAVH (laparoscopy-assisted vaginal hysterectomy) |
|
Yang, 2014 |
NAVH (NOTES-assisted vaginal hysterectomy) |
SP-LAVH (single port laparoscopy assisted vaginal hysterectomy) |
|
Yang, 2020 |
vNOTES |
TLH (total laparoscopic hysterectomy) |
Badiglian-Filho (2020) performed a retrospective cohort study to compare V-NOTES hysterectomy with salpingectomy/salpingo-oophorectomy with standard laparoscopic access in women undergoing hysterectomy with adnexectomy for benign disease indication. Exclusion criteria were endometriosis, previous pelvic radiotherapy, history of inflammatory pelvic disease, any other concurrent surgery, robotic surgery, traditional vaginal hysterectomy, exenterations and cytoreductions. The number of patients that were excluded because of incomplete data or follow-up was unclear. In total 86 patients were included, 21 women underwent V-NOTES (mean age 47.19 years (standard deviation (SD) 11.11)) and 65 underwent hysterectomy via standard laparoscopic access (mean age 46.69 years (SD 9.11)). Patients did not differ at baseline based on mean age, body mass index, arterial hypertension/ diabetes, smoking, menopausal status, obstetric history, number of abdominal surgeries, uterine volume or preoperative haemoglobin level.
Lee (2019) performed a retrospective cohort study to compare V-NOTES vaginal hysterectomy with bilateral salpingo-oophorectomy with conventional vaginal hysterectomy with bilateral salpingo-oophorectomy in female-to-male transgender men. All patients had persistent gender dysphoria and had taken testosterone therapy continuously for at least 1 year before surgical intervention. Exclusion criteria were not defined. The number of patients that were excluded due to incomplete data or follow-up was unclear. In total 56 transgender men were included, 14 transgender men underwent V-NOTES (mean age 28.8 years (SD 7.3)) and 42 underwent conventional vaginal hysterectomy (mean age 29.3 years (SD 6.4)). Patients were comparable at baseline with regard to important patient characteristics, except for the number of vaginectomies: there was a higher number of simultaneous vaginectomies in the V-NOTES group compared to the control group (N=9 (64%) versus N=10 (24%; P=0.009)).
Puisungnoen (2020) performed a retrospective cohort study to compare V-NOTES vaginal hysterectomy with total laparoscopic hysterectomy in women with a non-prolapsed uterus and benign gynaecological disease. There were no exclusion criteria defined. The number of patients that were excluded because of incomplete data or follow-up was unclear. In total 228 patients were included, 50 women underwent V-NOTES vaginal hysterectomy and 178 underwent total laparoscopic hysterectomy. Women undergoing TLH were more likely to be diagnosed with endometriosis and to have a larger uterus than those who underwent V-NOTES. Patients were then matched using propensity analysis, resulting in the definitive sample for analysis, consisting of 50 women undergoing V-NOTES (mean age 47.3 years (SD 6.7)) and 50 women undergoing total laparoscopic hysterectomy (mean age 48.2 years (SD 5.8)). These patients did not differ at baseline.
Results
Meta-analyses were performed where possible. Odds ratios (ORs) are reported for dichotomous outcomes as the majority of included studies were retrospective observational studies. Risk ratios (RRs) were comparable (data not reported). The results are presented separately for:
1. V-NOTES compared to a vaginal hysterectomy (VH).
2. V-NOTES compared to a laparoscopic hysterectomy (LH).
3. V-NOTES compared to an abdominal hysterectomy (AH).
1. V-NOTES compared to vaginal hysterectomy (VH)
One study (Lee, 2019), in 56 transgender female-to-male transgender men, investigated the comparison v-notes to vaginal hysterectomy.
1. Complications
The outcome measure was reported as intra-operative and post-operative complications.
1.1. Intra-operative complications
One study reported intra-operative complications (Lee, 2019). The outcome was defined as conversion to abdominal hysterectomy.
Lee (2019) reported no cases of conversion to abdominal hysterectomy in either group (14 women who underwent V-NOTES compared to 42 women who underwent vaginal hysterectomy) (OR not estimable).
1.2. Post-operative complications
One study reported post-operative complications (Lee, 2019). The outcome was defined as conversion to abdominal hysterectomy. Lee (2019) did not define the outcome on forehand, but reported the following post-operative complications. It was unclear whether there were 5 or 7 post-operative complications reported, as Lee (2019) reported 5 in analysis and 7 in text. Results are reported descriptively.
Lee (2019) reported that 1 of 14 women (7.1%) who underwent V-NOTES reported a post-operative bleeding. 5 of 42 women (11.9%) who underwent vaginal hysterectomy reported post-operative internal bleeding (n=2); post-operative vaginal bleeding (n=2); pelvic abscess (n=2); bacteremia (n=1).
2. Blood loss
One study reported the outcome measure blood loss (Lee, 2019). The outcome was defined as estimated blood loss in mL.
Lee (2019) reported that the estimated blood loss did not differ between V-NOTES and vaginal hysterectomy (median 200 mL (interquartile range (IQR) 100 to 388) versus median 150 mL (IQR 100 to 350); P=0.757).
3. Operative time
One study reported the outcome measure operative time (Lee, 2019). The outcome was defined as operative time in minutes.
The mean difference in operative time was -4.90 minutes (95% confidence interval (CI) -35.50 to 25.70) between women in the V-NOTES group compared to women in the vaginal hysterectomy group. Standardized mean difference was -0.10 (95%CI -0.71 to 0.51).
4. Operative costs
The outcome was not reported.
5. Post-operative pain
One study reported the outcome measure post-operative pain (Lee, 2019) at 2, 24, 48 and 72 hours post-operative.
5.1. Post-operative pain at 2 hours
Lee (2019) reported that the mean difference in pain score 2 hours post-operatively between V-NOTES and vaginal hysterectomy was -2.20 (95%CI -3.83 to -0.57). Standardized mean difference was -1.13 (95%CI -1.78 to -0.49).
5.2. Post-operative pain at 24 hours
Lee (2019) reported that the mean difference in pain score 24 hours post-operatively between V-NOTES and vaginal hysterectomy was -0.50 (95%CI -2.08 to 1.08). Standardized mean difference was -0.21 (95%CI-0.81 to 0.40).
5.3. Post-operative pain at 48 hours
Lee (2019) reported that the mean difference in pain score 48 hours post-operatively between V-NOTES and vaginal hysterectomy was -1.50 (95%CI -2.32 to -0.68). Standardized mean difference was -0.93 (95%CI -1.57 to -0.29).
5.6. Post-operative pain at 72 hours
Lee (2019) reported that the mean difference in pain score 72 hours post-operatively between V-NOTES and vaginal hysterectomy was -1.00 (95%CI -1.68 to -0.32). Standardized mean difference was -0.91 (95%CI -1.60 to -0.23),
6. Post-operative use of pain medication
One study reported the outcome measure post-operative use of pain medication (Lee, 2019).
Lee (2019) reported that the mean difference in post-operative intravenous opioid (meperidine) cumulative dose (mg) was -49.90 (95%CI -85.73 to -14.07) between women in the V-NOTES group compared to women in the vaginal hysterectomy group. Standardized mean difference was -0.65 (95%CI -1.27 to -0.03).
Post-operative oral NSAID (naproxen) use was reported by Lee (2019) in 5 of 14 women (35.7%) who underwent hysterectomy by V-NOTES, compared to 11 of 42 women (26.2%) who underwent vaginal hysterectomy (OR 1.57 (95%CI 0.43 to 5.70)).
Take-home oral NSAID (naproxen) use was reported by Lee (2019) in 1 of 14 women (7.1%) who underwent hysterectomy by V-NOTES, compared to 9 of 42 women (21.4%) who underwent vaginal hysterectomy (OR 0.28 (95%CI 0.03 to 2.45)).
7. Length of hospital stay
One study reported the outcome measure length of hospital stay (Lee, 2019). It was reported as hospital stay in days.
Lee (2019) reported that the mean difference length of hospital stay between V-NOTES and vaginal hysterectomy was 0.60 days (95%CI -0.97 to 2.17). Standardized mean difference was 0.20 (95%CI -0.41 to 0.81).
8. Time-to resuming daily activities post-operatively
The outcome measure time to resuming daily activities post-operatively was not reported in the included studies.
9. Time-to resuming work post-operatively.
The outcome measure time to resuming work post-operatively was not reported in the included studies.
2. V-NOTES compared to laparoscopic hysterectomy (LH)
Eight studies, including one RCT by (Baeklandt, 2018) and seven observational studies (Badiglian-Filho, 2020; Kaya, 2020; Kim, 2017; Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020).
1. Complications
The outcome measure was reported as intra-operative and post-operative complications.
1.1. Intra-operative complications
Seven studies reported the outcome measure intra-operative complications, one RCT (Baeklandt, 2018) and six observational studies (Badiglian-Filho, 2020; Kaya, 2020; Kim, 2017;Puisungnoen, 2020; Wang, 2014; Yang, 2014). The outcome was not specifically defined on forehand in all studies, definitions are reported in the footnote of Figure 23.2.
Intra-operative complications were reported in 4 of 339 women (1.2%) who underwent hysterectomy by V-NOTES, compared to 10 of 697 women (1.4%) who underwent laparoscopic hysterectomy (OR 0.80 (95%CI 0.25 to 2.53)) (Figure 15.1.1 Intra-operative complications, comparison hysterectomy by VNOTES versus laparoscopic hysterectomy).
Figure 15.1.1 Intra-operative complications, comparison hysterectomy by VNOTES versus laparoscopic hysterectomy
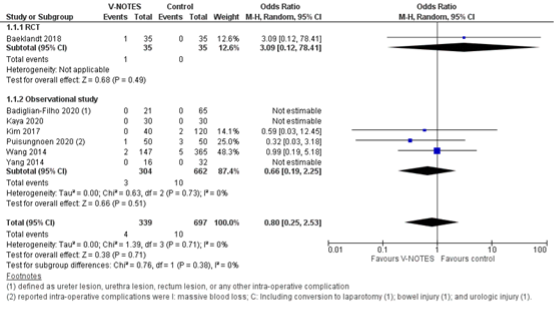
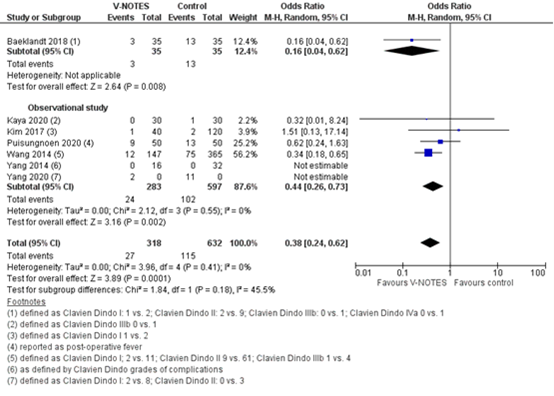
1.2. Post-operative complications
Seven studies reported the outcome measure post-operative complications, one RCT (Baeklandt, 2018) and six observational studies (Kaya, 2020; Kim, 2017; Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020). The studies included in the review by Housemans (2020) reported the outcome as defined by the Clavien Dindo classification. Clavien–Dindo grade I contains cases of fever (without mentioning treatment with antibiotics), pain and hematoma. Grade II contains cases of wound infections, pelvic inflammatory disease (PID) and blood transfusion. Grade IIIb contained one case of vesicovaginal fistula repair and cases of reintervention for bleeding. The case in Grade IVa was a case of pulmonary embolism with intensive-care unit (ICU) admission. The definitions by the other studies are reported in the footnote of Figure 23.3.
Post-operative complications were reported in 27 of 318 women (8.5%) who underwent hysterectomy by V-NOTES, compared to 115 of 632 women (18.2%) who underwent laparoscopic hysterectomy (OR 0.38 (95%CI 0.24 to 0.62)) (Figure 15.1.2 Post-operative complications, comparison hysterectomy by VNOTES versus laparoscopic hysterectomy).
Figure 15.1.2 Post-operative complications, comparison hysterectomy by VNOTES versus laparoscopic hysterectomy
2. Blood loss
Four studies reported the outcome measure blood loss (Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020). The outcome was defined as estimated blood loss in mL in all studies. One study could not be pooled in the meta-analysis as the authors only reported the median (interquartile range (IQR)) (Puisungnoen, 2020), the results are reported descriptively.
The mean difference in estimated blood loss was -94.6 mL (95%CI -141.15 to -48.05) between women in the V-NOTES group compared to women in the laparoscopic hysterectomy group (Figure 15.2 Blood loss, comparison hysterectomy by VNOTES versus conventional hysterectomy). The standardized mean difference was -0.74 (95%CI -1.35 to -0.12).
Puisungnoen (2020) reported an estimated blood loss of median 300 mL (IQR 450) in the V-NOTES group, compared to median 100 mL (IQR 212.5) in the laparoscopic hysterectomy group. Not tested for differences.
Figure 15.2 Blood loss, comparison hysterectomy by VNOTES versus conventional hysterectomy

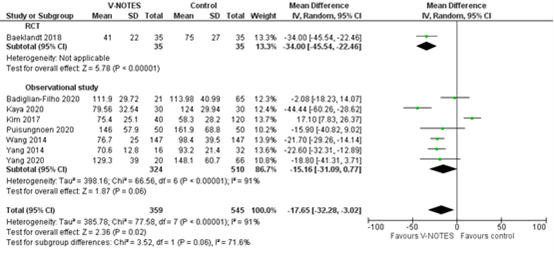
3. Operative time
Eight studies reported the outcome measure operative time, one RCT (Baeklandt, 2018) and seven observational studies (Badiglian-Filho, 2020; Kaya, 2020; Kim, 2017; Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020). The outcome was defined as operative time in minutes in all studies.
The mean difference in operative time was -17.65minutes (95%CI -32.28 to -3.02) between women in the V-NOTES group compared to women in the laparoscopic hysterectomy group (Figure 15.3 Operative time, comparison hysterectomy by VNOTES versus laparoscopic hysterectomy). Standardized mean difference was -0.55 (95%CI -1.02 to -0.08).
A sensitivity analysis was performed to explore the high heterogeneity. The study by Kim (2017) was considered by Housemans (2020) to be an outlier as they reported a significantly shorter operative time for the control group. Housemans (2020) reported that this was to be attributed to the technique of LAVH by Kim (2017), where the dissection of the ovarian ligaments, round ligaments and broad ligaments was performed by a 45 mm EndoGia® (Covidien, Ireland). The pooled mean difference without Kim (2017) in the analysis was -23.68 (95%CI -32.41 to -14.95), I2 was 66%.
Figure 15.3 Operative time, comparison hysterectomy by VNOTES versus laparoscopic hysterectomy
4. Operative costs
Two studies reported operative costs, one RCT (Baeklandt, 2018) and one retrospective cohort study (Wang, 2014). The results are reported descriptively.
Baekelandt (2018) reported no difference in direct health-related cost by measuring the difference in hospital bill up to 6 weeks postoperative. The direct hospital charge for disposable devices is not reflected entirely in the hospital bill described in the latter report, as the Belgian national health insurance automatically covers the cost of disposable devices up to approximately 550 EUR.
Wang (2014) reported a significantly higher hospital charge for V-NOTES compared to LAVH in New Taiwan Dollar (NTD) (22,573.3 (SD 5528.8) versus 17,744.6 (SD 8939.2)). Wang (2014) reported that this was driven by the higher cost of disposable devices (wound retractor and vessel sealing device) in spite of a shorter hospital stay for V-NOTES.
5. Post-operative pain
All studies reported post-operative pain. Where possible mean pain scores were pooled in a meta-analysis. Results are presented for moment of measurement, respectively at 6, 12, 24hours, and unknown moment of measurement.
5.2. Post-operative pain at 6 hours
Two studies reported pain at 6 hours post-operatively. Data could not be pooled as means and medians were reported.
Puisungnoen (2020) reported that the mean difference in pain score 6 hours post-operatively between V-NOTES and laparoscopic hysterectomy was -1,5 (95%CI -2.15 to -0.85). Standardized mean difference was -0.90 (95%CI -1.31 to -0.49).
Kaya (2020) reported that the VAS pain score at 6 hours was median 6 (range 4 to 7) for V-NOTES and median 6 (range 3 to 7) for TLH; P>0.05.
5.3. Post-operative pain at 12 hours
Yang (2014) reported pain scores at 12 hours as median 2 (range 0 to 6) for V-NOTES and median 2 (range 0 to 6) for LAVH; P>0.05.
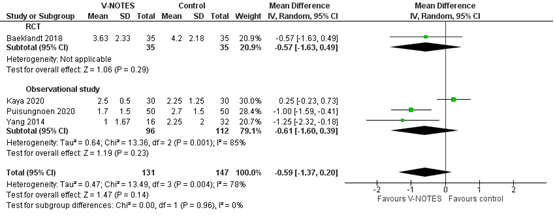
5.4. Post-operative pain at 24 hours
Four studies reported the outcome measure pain at 24 hours post-operative, one RCT (Baeklandt, 2018) and four observational studies (Kaya, 2020; Puisungnoen, 2020; Yang, 2014). The outcome was defined as pain by VAS-scale in all studies. Baeklandt (2018) reported a range of 0 to 10, the range of the VAS-scale was not reported by the other studies.
The mean difference in pain score by VAS at 24 hours post-operatively was -0.59 (95%CI -1.37 to 0.20) between women in the V-NOTES group compared to women in the laparoscopic hysterectomy group (Figure 15.4 Post-operative pain at 24 hours, comparison hysterectomy by VNOTES versus laparoscopic hysterectomy). Standardized mean difference was -0.33 (95%CI -0.75 to 0.10).
Figure 15.4 Post-operative pain at 24 hours, comparison hysterectomy by VNOTES versus laparoscopic hysterectomy
5.7. Post-operative pain at unknown moment of measurement
Two studies reported post-operative pain at an unknown moment of measurement (Badiglian-Filho, 2020; Yang, 2020), and it was therefore not possible to pool the results.
Badiglian-Filho (2020) did not report the outcome specifically, but it was reported that there was one case of shoulder pain (not further defined in text) in the group receiving laparoscopic hysterectomy (0 versus 1 (1.5%); P=1.00).
Yang 2020 reported significantly lower postoperative pain scores comparing V-NOTES to TLH. However, data from Yang (2020) could not be used for the pooled analysis for this outcome as Housemans (2020) was unable to retrieve information on the timepoint of this score after surgery.
6. Post-operative use of pain medication
One study reported the outcome measure post-operative use of pain medication (Puisungnoen, 2020).
Puisungnoen (2020) reported that the post-operative consumption of morphine (mg) between groups was median 0.0 (IQR 3.0) for women in V-NOTES group, compared to women in the laparoscopic hysterectomy group median 0.0 (IQR 3.0). Not tested for differences.
7. Length of hospital stay
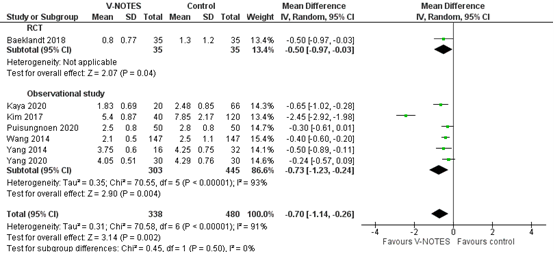
Eight studies reported the outcome measure length of hospital stay, one RCT (Baeklandt, 2018) and eight studies (Badiglian-Filho, 2020; Kaya, 2020; Kim, 2017; Puisungnoen, 2020; Wang, 2014; Yang, 2014; Yang, 2020). The outcome was defined as length of hospital stay in days in all studies. One study could not be pooled in the meta-analysis as they reported the median (interquartile range (IQR)) (Badiglian-Filho, 2020), the results are reported descriptively.
The mean difference in length of hospital stay was -0.70 days (95%CI -1.14 to -0.26) between women in the V-NOTES group compared to women in the laparoscopic hysterectomy group (Figure 15.7 Length of hospital stay (days), comparison hysterectomy by VNOTES versus laparoscopic hysterectomy). The standardized mean difference was -0.63 (95%CI -0.89 to -0.38).
Badiglian-Filho (2020) reported no difference in length of hospital stay between women in the V-NOTES group and laparoscopic hysterectomy group (P=0.491). Most women stayed 1 day (n=21 (100%) versus n=59 (90.8%)).
Figure 15.7 Length of hospital stay (days), comparison hysterectomy by VNOTES versus laparoscopic hysterectomy
8. Time-to resuming daily activities post-operatively
The outcome measure time to resuming daily activities post-operatively was not reported in the included studies.
9. Time-to resuming work post-operatively.
The outcome measure time to resuming work post-operatively was not reported in the included studies.
3. V-NOTES compared to abdominal hysterectomy.
None of the studies identified in the literature search compared to V-NOTES to abdominal hysterectomy. The following outcome measures were not studied: complications, blood loss, operative time, operative costs, post-operative pain, post-operative use of pain medication, length of hospital stay, time-to resuming daily activities post-operatively, time-to resuming work post-operatively.
Level of evidence of the literature
Analyses including RCTs start at a GRADE high; analyses with solely observational cohort studies start at a GRADE low and if so, is indicated below.
1. V-NOTES compared to vaginal hysterectomy (VH)
The level of evidence regarding the outcome measure intra-operative complications was downgraded with one level to a very low GRADE due to imprecision (no events; small sample size), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measure post-operative complications was downgraded with one level to a very low GRADE due to imprecision (impossible to estimate OR due to unknown definite number of complications), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measure blood loss was downgraded with one level to a very low GRADE due to risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measure operative time was downgraded with one level to a very low GRADE due to imprecision (optimal information size was not obtained), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measure operative costs could not be assessed with GRADE. None of the included studies reported the outcome measure for V-NOTES compared to VH.
The level of evidence regarding the outcome measure post-operative pain at 2 hours was downgraded with one level to a very low GRADE due to imprecision (optimal information size was not obtained), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measure post-operative pain at 24 hours was downgraded with one level to a very low GRADE due to imprecision (confidence interval of pooled effect includes no significant effect (mean difference=0) and no clinically relevant effect (SMD<0.5), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measure post-operative pain at 48 hours was downgraded with one level to a very low GRADE due to imprecision (optimal information size was not obtained), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measure post-operative pain at 72 hours was downgraded with one level to a very low GRADE due to imprecision (optimal information size was not obtained), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The outcome measure post-operative use of pain medication was reported as post-operative intravenous opioid (meperidine), post-operative oral NSAID (naproxen) use and take-home oral NSAID (naproxen use).
The level of evidence regarding the outcome measures post-operative intravenous opioid (meperidine), post-operative oral NSAID (naproxen) use and take-home oral NSAID (naproxen use) was downgraded with one level to a very low GRADE due to imprecision (optimal information size was not obtained), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measure length of hospital stay was downgraded with one level to a very low GRADE due to imprecision (confidence interval of pooled effect includes no significant effect (mean difference=0) and no clinically relevant effect (SMD<0.5), risk of bias (possible selection bias) and indirectness of evidence (high number of vaginectomies because of transgender surgery are associated with increased operative risks).
The level of evidence regarding the outcome measures time-to resuming daily activities post-operatively and time-to resuming work post-operatively could not be assessed with GRADE. None of the included studies reported these outcome measures.
2. V-NOTES compared to laparoscopic hysterectomy (LH)
The level of evidence regarding the outcome measure intra-operative complications was downgraded with three levels to a very low GRADE due to imprecision (confidence interval of pooled effect includes no significant effect (OR=1) and no clinically relevant effect (OR≤0.8)), inconsistency (heterogeneity in the direction of the effect between the RCT by Baeklandt (2018) and the included observational studies) and risk of bias (possible selection bias and bias in outcome measurement).
The level of evidence regarding the outcome measure post-operative complications was downgraded with two levels to a low GRADE due to risk of bias (possible selection bias and bias in outcome measurement).
The level of evidence regarding the outcome measure blood loss pertains solely observational studies and therefore starts at a GRADE low. The level of evidence regarding the outcome measure blood loss was downgraded with three levels to a very low GRADE due to inconsistency (heterogeneity in the direction of the effect between studies; Puisungnoen (2020 reported an effect in the opposite direction of the pooled effect) and risk of bias (possible selection bias and bias in outcome measurement).
The level of evidence regarding the outcome measure operative time was downgraded with two levels to a low GRADE due to risk of bias (possible selection bias and bias in outcome measurement). The outcome was not downgraded for inconsistency based on the results of the sensitivity analysis excluding Kim (2017).
The level of evidence regarding the outcome measure operative costs could not be assessed, due to limited comparability between the included studies and the Dutch health care system.
The level of evidence regarding the outcome measure post-operative pain at 6 hours solely pertains observational studies and therefore starts at a GRADE low. The level of evidence was downgraded with three levels to a very low GRADE due to inconsistency (heterogeneity in the direction of the effect between studies) and risk of bias (possible selection bias and bias in outcome measurement).
The level of evidence regarding the outcome measure post-operative pain at 12 hours solely pertains an observational study and therefore starts at a GRADE low. The level of evidence was downgraded with two levels to a very low GRADE due to risk of bias (possible selection bias and bias in outcome measurement).
The level of evidence regarding the outcome measure post-operative pain at 24 hours was downgraded with three levels to a very low GRADE due to imprecision (confidence interval of pooled effect includes no significant effect (mean difference=0) and no clinically relevant effect (SMD<0.5) and risk of bias (possible selection bias and bias in outcome measurement).
The level of evidence regarding the outcome measure post-operative pain at unknown moment of measurement could not be assessed as it was unclear when post-operative pain measurements were taken.
The level of evidence regarding the outcome measure post-operative use of pain medication could not be assessed as the outcome was only reported as median (IQR) and not tested for differences.
The level of evidence regarding the outcome measure length of hospital stay was downgraded with two levels to a low GRADE due to risk of bias (possible selection bias and bias in outcome measurement).
The level of evidence regarding the outcome measures time-to resuming daily activities post-operatively and time-to resuming work post-operatively could not be assessed with GRADE. None of the included studies reported these outcome measures.
A systematic review of the literature was performed to answer the following question:
What is the effectiveness of V-NOTES (Vaginal Natural Orifice Transluminal Endoscopic Surgery) compared to a vaginal hysterectomy (VH), laparoscopic hysterectomy (LH) or abdominal hysterectomy (AH) in women with benign indications?
P: Women undergoing a hysterectomy for benign indications.
I: Hysterectomy by V-NOTES.
C: VH, LH or AH.
O: Complications, blood loss, operative time, operative costs, post-operative pain, post-operative use of pain medication, length of hospital stay, time-to resuming daily activities post-operatively, time-to resuming work post-operatively.
Relevant outcome measures
The guideline development group considered complications as a critical outcome measure for decision making; and blood loss, operative time, operative costs, post-operative pain, post-operative use of pain medication, length of hospital stay, time-to resuming daily activities post-operative, time-to resuming work post-operative as an important outcome measure for decision making.
A priori, the working group did not define the outcome measures listed above but used the definitions used in the studies.
The GRADE default - a difference of 25% in the relative risk for dichotomous outcomes (Schünemann, 2013) and 0.5 standard deviation (reported as SMD) for continuous outcomes - was taken as a minimal clinically important difference.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from January 1st, 2010 until March 2nd, 2021. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 150 hits. Studies were selected based on the following criteria: 1) study reported women undergoing V-NOTES for benign indications; 2) V-NOTES was compared to at least one of the following techniques: VH, LH or AH; 3) one or more of the outcome measures as defined in the PICO was reported. 58 studies were initially selected based on title and abstract screening. After reading the full text, 54 studies were excluded (see the table with reasons for exclusion under the tab Methods) and 4 studies were included.
Results
In total, four studies were included in the analysis of the literature, one systematic review and meta-analysis (Housemans, 2020) and three retrospective cohort studies (Badiglian-Filho, 2020; Lee, 2019; Puisungnoen, 2020). Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Badiglian-Filho L, Chaves Faloppa C, Narciso de Oliveira Menezes A, Mantoan H, Kumagai LY, Baiocchi G. Vaginally assisted NOTES hysterectomy with adnexectomy (vNOTES) compared with conventional laparoscopy. A retrospective observational cohort study. Int J Gynaecol Obstet. 2021 May;153(2):351-356.
- Housmans S, Noori N, Kapurubandara S, Bosteels JJA, Cattani L, Alkatout I, Deprest J, Baekelandt J. Systematic Review and Meta-Analysis on Hysterectomy by Vaginal Natural Orifice Transluminal Endoscopic Surgery (vNOTES) Compared to Laparoscopic Hysterectomy for Benign Indications. J Clin Med. 2020 Dec 7;9(12):3959.
- Lee YL, Hsu TF, Jiang LY, Chao HT, Wang PH, Chen YJ. Transvaginal Natural Orifice Transluminal Endoscopic Surgery for Female-to-Male Transgender Men. J Minim Invasive Gynecol. 2019 Jan;26(1):135-142.
- Puisungnoen N, Yantapant A, Yanaranop M. Natural Orifice Transluminal Endoscopic Surgery-assisted Vaginal Hysterectomy versus Total Laparoscopic Hysterectomy: A Single-center Retrospective Study Using Propensity Score Analysis. Gynecol Minim Invasive Ther. 2020 Oct 15;9(4):227-230.
Evidence tables
Research question: What is the effectiveness of V-NOTES* compared to a vaginal hysterectomy (VH), laparoscopic hysterectomy (LH) or abdominal hysterectomy (AH) in women with benign indications?
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C) |
Follow-up |
Outcome measures and effect size |
Comments |
|
Housemans, 2020
PS., study characteristics and results are extracted from the SR (unless stated otherwise) |
SR and meta-analysis of (RCTs and cohort studies)
Literature search up to 8 October 2020.
A: Wang, 2014 B: Y S Yang, 2014 C: Kim, 2018 D: Baekelandt, 2019 E: Kaya, 2020 F: C-Y Yang, 2020
Study design: RCT (parallel / cross-over), cohort (prospective / retrospective), case-control
A: Retrospective chart analysis B: Retrospective chart analysis C: Retrospective chart analysis D: RCT, non-inferiority trial, single blind E: Cross-sectional study F: Retrospective chart analysis
Setting and Country:
A: Single centre tertiary, Taiwan. referral hospital B: single centre university, South Korea. affiliated hospital C: single centre university, South Korea. affiliated hospital D: Single centre, teaching hospital, Belgium. E: Single centre university, Turkey. F: Single centre university, China.
Source of funding and conflicts of interest: Not reported for the included studies. The authors of the review report: This systematic review is not funded by a pharmaceutical company or any other third party. SH is supported by a research grant of the Department of Obstetrics and Gynaecology, University Hospitals Leuven, 3000 Leuven, Belgium. Conflicts of Interest: J.B. (Jan Baekelandt) discloses consultancy for Applied Medical, but this did not interfere with this report.
|
Inclusion criteria SR: adult female population, undergoing removal of the uterus for benign gynecological disease w direct comparison of vNOTES to laparoscopy (laparoscopy assisted vaginal hysterectomy (LAVH), total laparoscopic hysterectomy (TLH) using single port (SILS) or multiple port (MP) access).
Exclusion criteria SR: Studies on interventions for genital prolapse or gynaecological malignancy were excluded. Studies comparing VNOTES with abdominal and vaginal hysterectomy were excluded.
6 studies included
Important patient characteristics at baseline:
N, mean age A: I:147; C: 147; aged 38-69 years B: I: 16; C: 32; age not reported. C: I: 40; C: 120; age not reported. D: I: 35; C:35; aged 18-70 years. E: I: 30; C: 69; age not reported; F: I: 31; C: 152; aged 38-56 years.
Sex: 100% female.
Groups comparable at baseline? Not reported. |
Describe intervention:
A: tVNOTHEH (transvaginal natural orifice transluminal endoscopic hysterectomy) B: NAVH (NOTES-assisted vaginal hysterectomy) C: NAVH D: vNOTES hysterectomy (VANH) plus 4 superficial non-therapeutic skin incisions identical to those in the control group E: vNOTES F: vNOTES
|
Describe control:
A: LAVH (laparoscopy-assisted vaginal hysterectomy) B: SP-LAVH (single port laparoscopy assisted vaginal hysterectomy) C: LAVH D: TLH (total laparoscopic hysterectomy) E: TLH F: TLH
|
End-point of follow-up:
Not reported.
For how many participants were no complete outcome data available? Not reported.
|
Outcome measure-1: Complications Defined as 1) intra-operative; and 2) postoperative complications using the Clavien-Dindo classification, and 3) post-operative infection defined by lower abdominal pain with fever >38 degrees Celsius and suggestive clinical signs or laboratory findings.
Effect measure: reported complications (Clavien-Dindo score): see Table 3 by Housemans 2020.
1.1. Intra-operative complications: Pooled effect (fixed effects model): OR 1.10 (95% CI 0.31 to 3.87) in favour of V-NOTES Heterogeneity (I2): 0%.
1.2. Post-operative complications: Pooled effect (fixed effects model): OR of 0.38 (95% CI 0.23 to 0.62) in favour of V-NOTES. Heterogeneity (I2): 0%
1.3. Postoperative infection (reported as fever or PID) Pooled effect (fixed effects model): OR 0.41 (95% CI 0.17 to 0.99), Z = 1.98 (p = 0.05) in favour of V-NOTES. Heterogeneity (I2): 0%.
Outcome measure-2: Blood loss Defined as estimated blood los (mL).
Effect measure: mean (+/- SD): A: I: 191.8 +/− 201.3 C: 324.6 +/− 242.4 B: I: 201.8 +/− 127 C: 228.1 +/− 172 C: not reported. D: not reported E: not reported F: I: 53.5 +/− 74.9 C: 43.8 +/− 83.7
Pooled effect (fixed effects model): MD −98.87 mL (95% CI −126.67 to −71.07), Z = 6.97 (p < 0.05) in favour of V-NOTES. Heterogeneity (I2): 55%.
Outcome measure-3: Operative time Defined as operative time in minutes.
Effect measure: mean (+/- SD): A: I: 76.7 +/− 25.0 C: 98.4 +/− 39.5 B: I: 70.6 +/− 12.8 C: 93.2 +/- 21.4 C: I: 75.4 +/− 25.1 C: 58.3 +/− 28.2 D: I: 41 +/− 22 C: 75 +/− 27 E: I: 79.56 +/− 32.54 C: 124 +/− 29.94 F: I: 129.3 +/− 39.0 C: 148.1 +/− 60.7
Pooled effect (fixed effects model): mean difference in operation time (OT) of 16.73 min, in favour of vNOTES (MD −16.73 (95% CI −21.04 to −12.40), Z = 7.57 (p < 0.05)) Heterogeneity (I2): 93%.
Outcome measure-4: Operative costs Defined as reported by study.
Effect measure: A: reported significantly higher hospital charges for vNOTES compared to LAVH: 22,573.3 +/− 5528.8 versus 17,744.6 +/− 8939.2 New Taiwan Dollar (NTD). They mention that this was driven by the higher cost of disposable devices (wound retractor and vessel sealing device) in spite of a shorter hospital stay for vNOTES. B: not reported. C: not reported. D: reported no difference in direct health-related cost by measuring the difference in hospital bill up to 6 weeks postoperative. The direct hospital charge for disposable devices is not reflected entirely in the hospital bill described in the latter report, as the Belgian national health insurance automatically covers the cost of disposable devices up to approximately 550 EUR. F: not reported.
Pooled effect (fixed effects model): data could not be pooled, too heterogenous.
Outcome measure-5: post-operative pain Defined as pain reported on VAS-scale on day 1.
Effect measure: see meta-analysis for data per individual study.
Pooled effect (fixed effects model): MD −0.09 (95% CI −0.49 to 0.32)) in favour of V-NOTES. Heterogeneity: 72%.
Outcome measure-6: post-operative use of pain medication Not reported.
Outcome measure-7: length of hospital stay Defined as length of hospital stay in days.
Effect measure: see meta-analysis for data per individual study.
Pooled effect (fixed effects model): mean difference (MD) of 0.58 days (95% CI −0.71 to −0.45) in favour of vNOTES. Z = 8.73 (p < 0.05). Heterogeneity (I2): 93%.
Outcome measure-8: time to resume daily activities post-operatively Not reported.
Outcome measure-8: time to resume work post-operatively Not reported. |
Facultative:
Brief description of author’s conclusion: “Pooled analysis of two subgroups showed that, compared to conventional laparoscopy, vNOTES is equally effective to successfully remove the uterus in individuals meeting the inclusion criteria. vNOTES had significantly lower values for operation time, length of stay and estimated blood loss. There was no significant difference in intra- and postoperative complications, readmission, pain scores at 24 h postoperative and change in hemoglobin (Hb) on day 1 postoperative.”
Personal remarks on study quality, conclusions, and other issues (potentially) relevant to the research question
Level of evidence: GRADE (per comparison and outcome measure) including reasons for down/upgrading
Sensitivity analyses (excluding small studies; excluding studies with short follow-up; excluding low quality studies; relevant subgroup-analyses); mention only analyses which are of potential importance to the research question:
1. Sensitivity analysis of outcome measure 3: operative time “We performed a sensitivity analysis on the outlier, the study by Kim et al. (18), which is responsible for the high heterogeneity in this subgroup. They reported a significantly shorter OT for the control group. We believe this to be attributed to the technique of LAVH described in the paper, where the dissection of the ovarian ligaments, round ligaments and broad ligaments was performed by a 45 mm EndoGia® (Covidien, Ireland).
2. Sensitivity analysis of outcome measure 7: length of hospital stay. “We performed a sensitivity analysis for the outlier, the study by Kim et al. (18), which is responsible for the high heterogeneity in this subgroup. They report a range of 4–17 days in length of stay for their control group, leading to a higher MD, which was calculated from the reported median (Figure 5).”
Heterogeneity: clinical and statistical heterogeneity; explained versus unexplained (subgroupanalysis) |
Evidence table
Research question: What is the effectiveness of V-NOTES* compared to a vaginal hysterectomy (VH), laparoscopic hysterectomy (LH) or abdominal hysterectomy (AH) in women with benign indications?
Table of quality assessment
|
Study
First author, year |
Appropriate and clearly focused question?
Yes/no/unclear |
Comprehensive and systematic literature search?
Yes/no/unclear |
Description of included and excluded studies?
Yes/no/unclear |
Description of relevant characteristics of included studies?
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?
Yes/no/unclear/notapplicable |
Assessment of scientific quality of included studies?
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?
Yes/no/unclear |
Potential risk of publication bias taken into account?
Yes/no/unclear |
Potential conflicts of interest reported?
Yes/no/unclear |
|
Housemans (2020) |
Yes |
Yes |
Yes |
Yes |
Unclear, it was not reported whether patients differed at baseline in the observational cohort studies and whether the authors corrected the results for important confounders or baseline differences. |
Yes |
Yes |
Yes, RoB2 tool to assess the risk of bias in randomised trials and the ROBINS-I tool for non-randomised trials |
No, it was not reported per individual study. It was reported for the authors of the review. |
Table of excluded studies
|
Author and year |
Reason for exclusion |
|
Baekelandt, 2019 |
Letter to the editor |
|
Baekelandt, 2019 |
Individual study already included in Houseman 2020 |
|
Baekelandt, 2019 |
Does not comply to PICO (not the right comparison) |
|
Baekelandt, 2021 |
Does not comply to PICO (not the right comparison) |
|
Chen, 2012 |
Does not comply to PICO (not the right comparison) |
|
Chen, 2020 |
Article in Chinese |
|
Ding, 2017 |
Does not comply to PICO (not the right comparison) |
|
Giacchino, 2019 |
Does not comply to PICO (not the right comparison) |
|
Kale, 2017 |
Does not comply to PICO (not the right comparison) |
|
Karkia, 2019 |
Does not comply to PICO (not the right comparison) |
|
Kaya, 2018 |
Does not comply to PICO (not the right comparison) |
|
Kaya, 2020 |
Individual study already included in Houseman 2020 |
|
Kaya, 2020 |
Does not comply to PICO (not the right comparison) |
|
Kim, 2013 |
Letter to the editor |
|
Kim, 2018 |
Individual study already included in Houseman 2020 |
|
Kim, 2019 |
Does not comply to PICO (not the right comparison) |
|
Lauterbach, 2020 |
Does not comply to PICO (not the right comparison) |
|
Lee, 2013 |
Does not comply to PICO (not the right comparison) |
|
Lee, 2014 |
Does not comply to PICO (not the right comparison) |
|
Lee, 2017 |
Does not comply to PICO (not the right comparison) |
|
Lee, 2019 |
Does not comply to PICO (all patients received V-NOTES) |
|
Li, 2020 |
Systematic review of low quality and shorter search than Houseman 2020 |
|
Lowenstein, 2020 |
Does not comply to PICO (not the right comparison) |
|
Lowenstein, 2020 |
Does not comply to PICO (not the right comparison) |
|
Lowenstein, 2021 |
Does not comply to PICO (not the right comparison) |
|
Matanes, 2019 |
Does not comply to PICO (not the right comparison) |
|
Matanes, 2019 |
Does not comply to PICO (not the right comparison) |
|
Michener, 2021 |
Systematic review about LESS and V-NOTES versus MPL hysterectomy. Does not add anything to Houseman 2020 and did not include all relevant studies. |
|
Mohan, 2013 |
narrative review |
|
Nulens, 2020 |
Does not comply to PICO (not the right comparison) |
|
Nulens, 2021 |
Does not comply to PICO (not the right comparison) |
|
Su, 2012 |
Does not comply to PICO (not the right comparison) |
|
Su, 2012 |
Does not comply to PICO (not the right comparison) |
|
Su, 2018 |
Does not comply to PICO (not the right comparison) |
|
Temtanakitpaisan, 2018 |
Does not comply to PICO (all patients received V-NOTES) |
|
Wang, 2015 |
Does not comply to PICO (not the right comparison) |
|
Wang, 2019 |
Does not comply to PICO (not the right comparison) |
|
Wang, 2019 |
Does not comply to PICO (not the right comparison, patients with endometrial cancer |
|
Wang, 2020 |
Does not comply to PICO (not the right comparison) |
|
Wang, 2021 |
Does not comply to PICO (not the right comparison), women with endometrial cancer, V-NOTES with lymphnode mapping. |
|
Weyl, 2021 |
Cadaver study |
|
Wright, 2019 |
Letter to the editor |
|
Yang, 2014 |
Individual study already included in Houseman 2020 |
|
Yang, 2020 |
Individual study already included in Houseman 2020 |
|
Yang, 2020 |
Does not comply to PICO (not the right comparison) |
|
Yantapant, 2019 |
Does not comply to PICO (not the right comparison) |
|
Zapico, 2018 |
Does not comply to PICO (not the right comparison, patients with gynaecological cancer |
Beoordelingsdatum en geldigheid
Publicatiedatum : 14-07-2023
Beoordeeld op geldigheid : 30-06-2023
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodules.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodules zijn in 2020 per module schrijvers en meelezers benoemd. Deze personen werden aangewezen als vertegenwoordigers door de relevante beroepsgroepen die betrokken zijn bij de in de module beschreven zorg (zie hiervoor de Samenstelling van de werkgroep). Alle schrijvers van modules vallend onder één richtlijn vormden samen een schrijfgroep. Alle meelezers van modules vallend onder één richtlijn vormden samen een clusterwerkgroep. In totaal resulteerde dit dus in zes werkgroep en zes clusterwerkgroepen.
Voorzitter project (technisch voorzitter)
Timmermans A. (Anne), gynaecoloog, AmsterdamUMC, NVOG
Werkgroep Laparoscopische Hysterectomie
Engberts M.K. (Marian), urogynaecoloog, Isala Ziekenhuis te Zwolle, NVOG
Kok H.S. (Helen), gynaecoloog, Alrijne Ziekenhuis te Leiden, NVOG
van Kesteren P.J.M. (Paul), gynaecoloog, OLVG te Amsterdam, NVOG
van Rijn C.A.L. (Karin), gynaecoloog, Haaglanden Medisch Centrum te Den Haag, NVOG
Clusterwerkgroep Laparoscopische Hysterectomie
Bosch M. (Marlies), patiëntvertegenwoordiger, Bekkenbodem4all
Ondersteuning project
Abdollahi M. (Mohammadreza), adviseur Kennisinstituut van de Federatie van Medisch Specialisten
Labeur Y.J. (Yvonne), junior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Olthuis-van Essen H. (Hanneke), adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Sussenbach A.E. (Annelotte), junior adviseur Kennisinstituut van de Federatie van Medisch Specialisten
Verhoeven M. (Maxime), adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
Projectleiding
Augustus 2022- nu Mostovaya I.M. (Irina) (projectleider), senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
April 2020 tot augustus 2021: Bijlsma-Rutte A. (Anne), adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
September 2021 tot januari 2022: Venhorst K. (Kristie), adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
Februari 2022 tot juni 2022: Göthlin M. (Mattias), adviseur, Kennisinstituut van de Federatie van Medisch Specialisten
Voor het ontwikkelen van de richtlijnmodules zijn in 2020 per module schrijvers en meelezers benoemd. Deze personen werden aangewezen als vertegenwoordigers door de relevante beroepsgroepen die betrokken zijn bij de in de module beschreven zorg (zie hiervoor de Samenstelling van de werkgroep). Alle schrijvers van modules vallend onder één richtlijn vormden samen een schrijfgroep. Alle meelezers van modules vallend onder één richtlijn vormden samen een clusterwerkgroep. In totaal resulteerde dit dus in zes werkgroep en zes clusterwerkgroepen.
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoek financiering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Timmermans (technisch voorzitter van het project) |
Gynaecoloog, Amsterdam UMC (0.5 fte) |
Commissie kwaliteitsdocumenten NVOG (onbetaald); projectgroep Gynae Goes Green NVOG (onbetaald) |
Geen |
Geen actie |
|
Laparoscopische hysterectomie - werkgroep |
||||
|
Engberts |
Urogynaecoloog ISALA |
Trainer Altis ® Sling voor Coloplast, betaald |
Geen |
Niet betrokken bij de besluitvorming rondom (fasci)slings. |
|
Kok |
Gynaecoloog; Alrijne Ziekenhuis; 0,53fte |
Geen |
Geen |
Geen actie |
|
Van Kesteren |
Gynaecoloog OLVG Oost Amsterdam |
Geen |
Geen |
Geen actie |
|
Van Rijn |
Gynaecoloog/ chef de clinique Haaglanden Medisch Centrum |
Richtlijnondersteuner NVOG |
Geen |
Geen actie |
|
Laparoscopische hysterectomie - clusterwerkgroep |
||||
|
Bosch |
Stichting Bekkenbodem4All. PR | Belangenbehartiging |
Fotograaf Bisdom Groningen-Leeuwarden. Deels betaald, deels vrijwilligerswerk |
Functie Belangenbehartiging Patiënten organisatie |
Geen |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van Patiëntenfederatie Nederland en Stichting Bekkenbodem4All voor de schriftelijke knelpunteninventarisatie en voor deelname aan de clusterwerkgroepen. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is voor commentaar voorgelegd aan Patiëntenfederatie Nederland en Stichting Bekkenbodem4All en de eventueel aangeleverde commentaren worden bekeken en verwerkt.
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld volgens de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerden de werkgroep de knelpunten in de zorg en de actualiteit van de aanbevelingen beschreven in de te reviseren modules. Tevens zijn er knelpunten aangedragen door de Nederlandse Vereniging voor Obstetrie en Gynaecologie (NVOG), de Nederlandse Vereniging van Maag-Darm-Leverartsen (NVMDL), Vereniging Klinische Genetica Nederland (VKGN), Inspectie Gezondheidszorg en Jeugd (IGJ), Koninklijke Nederlandse Organisatie van Verloskundigen (KNOV), Nederlands Huisartsen Genootschap (NHG), Nederlandse Vereniging voor Bekkenfysiotherapie en Pré- en Postpartum Gezondheidszorg, Nederlandse Vereniging van Ziekenhuizen (NVZ), Patiëntenfederatie Nederland, Zorginstituut Nederland (ZiNL), Zelfstandige Klinieken Nederland (ZKN) en Zorgverzekeraars Nederland (ZN) via een schriftelijke knelpunteninventarisatie.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Ook definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur en de beoordeling van de risk-of-bias van de individuele studies is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Hultcrantz, 2017; Schünemann, 2013).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nul effect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE-methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Volgens de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren worden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren wordt de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule wordt aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en akkoord.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwaliteit.
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013.
Schünemann HJ, Oxman AD, Brozek J, Glasziou P, Jaeschke R, Vist GE, Williams JW Jr, Kunz R, Craig J, Montori VM, Bossuyt P, Guyatt GH; GRADE Working Group. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ. 2008 May 17;336(7653):1106-10. Erratum in: BMJ. 2008 May 24;336(7654).
Wessels M, Hielkema L, van der Weijden T. How to identify existing literature on patients' knowledge, views, and values: the development of a validated search filter. J Med Libr Assoc. 2016 Oct;104(4):320-324.
Zoekverantwoording
Literature search strategy
Zoekverantwoording
Algemene informatie
|
Richtlijn: Laparoscopische Hysterectomie voor benigne indicaties, onderdeel van het 24-modules project (Actualisatie en revisie gynaecologische richtlijnmodules) |
|
|
Uitgangsvraag: Is V-Notes beter dan VH, LH of AH? |
|
|
Database(s): Ovid/Medline, Embase |
Datum: 02-03-2021 |
|
Periode: 2010 - heden |
Talen: Engels, Nederlands |
|
Literatuurspecialist: Miriam van der Maten |
|
|
BMI zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting en opmerkingen:
|
|
|
Te gebruiken voor richtlijnen tekst: In de databases Embase.com en Ovid/Medline is op 2 maart 2021 met relevante zoektermen gezocht naar systematische reviews, randomized controlled trials en observationele studies over hysterectomie middels V-Notes. De literatuurzoekactie leverde 150 unieke treffers op. |
|
Zoekopbrengst
|
|
Embase |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
10 |
5 |
10 |
|
RCT |
24 |
13 |
26 |
|
Observationeel |
114 |
47 |
114 |
|
Totaal |
148 |
65 |
150 |
Zoekstrategie
Embase
|
No. |
Query |
Results |
|
#10 |
#7 OR #8 OR #9 |
148 |
|
#9 |
#3 AND #6 NOT (#7 OR #8) = observationeel |
114 |
|
#8 |
#3 AND #5 NOT #7 = RCT |
24 |
|
#7 |
#3 AND #4 = SR |
10 |
|
#6 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
6387238 |
|
#5 |
('clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti) NOT 'conference abstract':it |
2500470 |
|
#4 |
('meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT ('conference abstract'/it OR 'conference review'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) |
533576 |
|
#3 |
#1 AND #2 AND (2010-2021)/py |
354 |
|
#2 |
'natural orifice transluminal endoscopic surgery'/exp OR ((notes:ti,ab,kw OR 'natural orifice') AND (vaginal:ti,ab,kw OR transvaginal:ti,ab,kw OR hybrid:ti,ab,kw)) OR (('v' NEAR/1 (notes OR 'natural orifice')):ti,ab,kw) OR vnotes:ti,ab,kw |
4385 |
|
#1 |
'hysterectomy'/exp OR hysterectom*:ti,ab,kw |
89341 |
Ovid/Medline
|
# |
Searches |
Results |
|
11 |
8 or 9 or 10 |
65 |
|
10 |
(4 and 7) not (8 or 9) = observationeel |
47 |
|
9 |
(4 and 6) not 8 = RCT |
13 |
|
8 |
4 and 5 = SR |
5 |
|
7 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort*.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ |
3793452 |
|
6 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2268310 |
|
5 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
504477 |
|
4 |
limit 3 to yr="2010 -Current" |
114 |
|
3 |
1 and 2 |
148 |
|
2 |
exp Natural Orifice Endoscopic Surgery/ or ((notes or 'natural orifice') and (vaginal or transvaginal or hybrid)).ti,ab,kf. or ('v' adj1 (notes or 'natural orifice')).ti,ab,kf. or vnotes.ti,ab,kf. |
4338 |
|
1 |
exp Hysterectomy/ or hysterectom*.ti,ab,kf. |
49804 |