Materiaalkeuze voor perifeer veneuze katheters
Uitgangsvraag
Aan welke materiaaleisen moet een perifeer veneuze katheter voldoen?
Deelvraag 1
Wat is de optimale diameter van een perifeer veneuze katheter om katheter-gerelateerde infecties te voorkomen?
Deelvraag 2
Aan welke overige materiaaleisen moet een perifeer veneuze katheter voldoen?
Aanbeveling
Aanbeveling 1 - Katheter diameter
- Baseer de keuze voor een perifeer veneuze katheter met een bepaalde diameter niet op infectiepreventieoverwegingen.
- Baseer de keuze voor een perifeer veneuze katheter met een bepaalde diameter op de indicatie voor katheterplaatsing en individuele patiëntkarakteristieken, zoals de benodigde lengte van de katheter, succes en complicaties van eerdere katheterplaatsing, en beschikbare informatie uit echografie.
- Houd bij de keuze voor een perifeer veneuze katheter met een bepaalde diameter rekening met het voorschrift van de fabrikant.
Aanbeveling 2 - Overige materiaaleisen
Kies een perifeer veneuze katheter die voldoet aan Europese wetgeving op het gebied van medische hulpmiddelen, waaronder de Verordening (EU) 2017/745, de REACH-verordening (EG) 1907/2006, en de geharmoniseerde Europese normen:
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Deelvraag 1 – Katheter diameter
Er is literatuuronderzoek verricht naar het effect van de diameter van perifeer veneuze katheters op katheter-gerelateerde infecties bij volwassen patiënten en kinderen (geen neonaten) in de medisch-specialistische zorg. ‘Katheter-gerelateerde bloedbaaninfectie (KRBBI) en katheter-geassocieerde bloedbaaninfectie (KABBI) werden als cruciale uitkomstmaten gedefinieerd. Infecties van de insteekplaats, (trombo)flebitis, mortaliteit door alle oorzaken, KRBBI/KABBI-gerelateerde mortaliteit, falen van eerste inbrengpoging, en katheterfalen door alle oorzaken werden als belangrijke uitkomstmaten gedefinieerd. Een relatief risico (RR) kleiner dan 0.8 of groter dan 1.25 werd als klinisch relevant beschouwd voor alle uitkomstmaten, met uitzondering van mortaliteit. Voor mortaliteit werd een relatief risico kleiner dan 0.95 of groter dan 1.05 als klinisch relevant beschouwd. Katheter diameter wordt uitgedrukt in Gauge (G). Hoe groter de diameter, hoe lager het aantal G.
De resultaten worden afzonderlijk gepresenteerd voor volwassenen en kinderen, omdat de optimale diameter van perifeer veneuze katheters naar verwachting anders is voor volwassenen patiënten en kinderen.
A. Volwassenen
Er werden één gerandomiseerde klinische studie en 23 observationele studies geïncludeerd die perifeer veneuze katheters van verschillende diameter vergeleken bij volwassen patiënten in het ziekenhuis. Bij de analyse werden katheters met een diameter <=18G (grotere diameter) vergeleken met katheters met een diameter >=20G (kleinere diameter). ‘Midline’ katheters werden niet onderzocht.
- In de gerandomiseerde klinische studie werd de cruciale uitkomstmaat KRBBI/KABBI niet gerapporteerd. In observationele studies was er een niet klinisch relevant verschil voor de cruciale uitkomstmaat KABBI (1 studie; bewijskracht zeer laag).
- In de gerandomiseerde klinische studie werd de belangrijke uitkomstmaat (trombo)flebitis gerapporteerd, maar het effect van katheter diameter kon niet worden geschat (1 studie; bewijskracht zeer laag). In observationele studies was er een niet klinisch relevant verschil voor deze uitkomstmaat (14 studies; bewijskracht zeer laag).
- In de gerandomiseerde klinische studie was er een niet klinisch relevant verschil voor de belangrijke uitkomstmaat falen van eerste inbrengpoging (1 studie; bewijskracht zeer laag). In observationele studies was er een klinisch relevant verschil voor deze uitkomstmaat in het voordeel van een grotere diameter (<=18G) (RR 0.42; 95% CI 0.32 tot 0.56; 1 studie; bewijskracht zeer laag).
- In de gerandomiseerde klinische studie was er een klinisch relevant verschil voor de belangrijke uitkomstmaat katheterfalen door alle oorzaken in het voordeel van een kleinere diameter (>=20G) (RR 2.00; 95% CI 0.72 tot 5.61; 1 studie; bewijskracht zeer laag). In observationele studies was er een niet klinische relevant verschil voor deze uitkomstmaat (2 studies; bewijskracht zeer laag).
- De andere belangrijke uitkomstmaten werden niet gerapporteerd.
Bij het bepalen van de bewijskracht is, naast imprecisie, voor de observationele studies rekening gehouden met mogelijke ‘confounding by indication’. De overall bewijskracht, gebaseerd op de cruciale uitkomstmaat KABBI, was zeer laag.
We concluderen dat voor volwassen patiënten in het ziekenhuis met een (korte of lange) perifeer veneuze katheter het bewijs voor een effect van katheter diameter op KABBI zeer onzeker is; dat het bewijs voor een effect van katheter diameter op (trombo)flebitis, falen van eerste inbrengpoging, en katheterfalen door alle oorzaken zeer onzeker is; en dat er geen bewijs is gevonden voor een effect van katheter diameter op de andere uitkomstmaten.
Er zijn geen studies gevonden naar het effect van de diameter van ‘midline’ katheters op katheter-gerelateerde infecties bij volwassen patiënten in het ziekenhuis.
B. Kinderen
Er werden drie observationele studies geïncludeerd die perifeer veneuze katheters van verschillende diameter vergeleken bij pediatrische patiënten in het ziekenhuis (Ben Abdelaziz, 2017; Gómez-Neva, 2022; Petroski, 2015). Bij de analyse werden katheters met een diameter <=22G (grotere diameter) vergeleken met katheters met een diameter >=24G (kleinere diameter). ‘Midline’ katheters werden niet onderzocht.
- De cruciale uitkomstmaat KRBBI/KABBI werd niet gerapporteerd.
- Er was een klinisch relevant verschil voor de belangrijke uitkomstmaat falen van eerste inbrengpoging in het voordeel van een grotere diameter (<=22G) (RR 0.51; 95% CI 0.23 tot 1.12; 1 studie; bewijskracht zeer laag).
- In twee observationele studies was er een tegengesteld klinisch relevant verschil voor de belangrijke uitkomstmaat katheterfalen door alle oorzaken (2 studies; bewijskracht zeer laag).
- De andere belangrijke uitkomstmaten werden niet gerapporteerd.
Bij het bepalen van de bewijskracht is, naast imprecisie, voor de observationele studies rekening gehouden met mogelijke ‘confounding by indication’. De overall bewijskracht, gebaseerd op de cruciale uitkomstmaten, kon niet worden bepaald.
We concluderen dat er voor pediatrische patiënten in het ziekenhuis met een perifeer veneuze katheter geen bewijs is gevonden voor een effect van katheter diameter op KRBBI/KABBI; dat het bewijs voor een effect van katheter diameter op falen van eerste inbrengpoging en katheterfalen door alle oorzaken zeer onzeker is; en dat er geen bewijs is gevonden voor een effect van katheter diameter op de andere uitkomstmaten.
Er zijn geen studies gevonden naar het effect van de diameter van ‘midline’ katheters op katheter-gerelateerde infecties bij pediatrische patiënten in het ziekenhuis.
Deelvraag 2 – Overige materiaaleisen
Er is geen systematisch literatuuronderzoek verricht naar de plaats van overige materiaaleisen voor perifeer veneuze katheters bij de preventie van katheter-gerelateerde infecties bij volwassen patiënten en kinderen (geen neonaten) in de medisch-specialistische zorg.
Voor aanbevelingen baseert de werkgroep zich op de eerdere WIP-richtlijn Flebitis en bloedbaaninfecties door intraveneuze infuuskatheters, internationale richtlijnen, wettelijke kaders, ondersteunende literatuur, en expert opinie.
Overige overwegingen bij de diameterkeuze
Naast infectiepreventieoverwegingen zijn andere factoren, zoals de indicatie voor katheterplaatsing en individuele patiëntkarakteristieken, van belang bij de keuze voor een perifeer veneuze katheter met een bepaalde diameter (zie Tabel 1). Deze aspecten kunnen een grotere impact hebben op de gezondheid van de patiënt dan eventuele infectiepreventie overwegingen.
Tabel 1. Factoren die van belang zijn bij de keuze voor een perifeer veneuze katheter met een bepaalde diameter
|
Indicatie voor katheterplaatsing (afname van bloed of noodzaak tot toedienen van grote volumina vocht in korte tijd vragen om een grotere diameter) |
|
Benodigde lengte van de katheter (een grotere lengte gaat vaak gepaard met een grotere diameter) |
|
Succes en complicaties van eerdere katheterplaatsing |
|
Beschikbare informatie uit echografie: diameter en traject van de vene waarin de katheter geplaatst wordt |
Bij de keuze voor een perifeer veneuze katheter met een bepaalde diameter dient rekening te worden gehouden met het voorschrift van de fabrikant.
Internationale richtlijnen
De richtlijnen van Centers for Disease Prevention and Control (CDC) (O’Grady, 2017), International Nursing Society (INS) (No authors listed, 2021), en World Health Organization (WHO) (No authors listed, 2024) zijn geraadpleegd (Tabel 2).
CDC en WHO doen geen aanbeveling over de optimale diameter en materiaaleisen voor perifeer veneuze katheters. INS beveelt aan om een perifeer veneuze katheter te kiezen met de kleinst mogelijke diameter die nodig is voor de voorgeschreven behandeling.
Tabel 2. Internationale richtlijnen voor de preventie van katheter-gerelateerde infecties
|
Richtlijn |
Aanbeveling(en) |
|
CDC (O’Grady, 2017) |
|
|
INS (No authors listed, 2021)1,2 |
|
|
WHO (No authors listed, 2024) |
|
CDC = Centers for Disease Prevention and Control; INS = International Nursing Society; WHO = World Health Organization
1 De INS-richtlijn is ontwikkeld met financiële ondersteuning van de industrie; ook waren auteurs niet vrij van persoonlijke financiële belangen.
2 Er wordt niet verwezen naar de in 2024 verschenen update van de INS-richtlijn, omdat deze niet publiek beschikbaar is.
Wettelijke kaders
Perifeer veneuze katheters zijn medische hulpmiddelen en moeten als zodanig voldoen aan Europese wetgeving op het gebied van medische hulpmiddelen, waaronder de Verordening (EU) 2017/745, de REACH-verordening (EG) 1907/2006, en de geharmoniseerde Europese normen:
- NEN-EN-ISO 10555-1 - Intravasculaire katheters - Steriele katheters voor eenmalig gebruik - Deel 1. Algemene eisen.
- NEN-EN-ISO 10555-5 - Intravasculaire katheters - Steriele katheters voor eenmalig gebruik - Deel 5. Perifere katheters met inbrengnaald.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Er is geen systematisch literatuuronderzoek verricht naar de waarden en voorkeuren van patiënten met betrekking tot de materiaalkeuze voor perifeer veneuze katheters.
In het algemeen kan gezegd worden dat de preventie van katheter-gerelateerde infecties past binnen de huidige maatstaven voor passende zorg. Standaardisatie en naleving van aanbevelingen over materiaalkeuze voor perifeer veneuze katheters is voor patiënten belangrijk omdat dit de kans op infecties niet wegneemt, maar wel vermindert.
Voor katheter diameter laten incidentele studies wisselende resultaten zien als het gaat om pijnbeleving bij de patiënt, waarbij katheters met een kleinere diamter soms wel en soms niet als minder pijnlijk worden ervaren (Kaplan, 2023; Kearney, 2021; van Loon, 2018). Hier ligt een kennisvraag.
Bij de materiaalkeuze voor perifeer veneuze katheters is het belangrijk rekening te houden met eventuele allergieën voor gebruikte materialen, zoals bijvoorbeeld polyurethaan overgevoeligheid (McCleskey, 2011; Milanesi, 2018; Pastor-Nieto, 2015).
Kosten (middelenbeslag)
Er is geen systematisch literatuuronderzoek verricht naar de kosteneffectiviteit van materiaalkeuze voor perifeer veneuze katheters.
In het algemeen kan gezegd worden dat katheter-gerelateerde infecties gepaard gaan met meer zorgkosten (Drugeon, 2023). Het voorkómen van deze complicaties door standaardisatie en naleving van aanbevelingen over materiaalkeuze voor perifeer veneuze katheters resulteert naar verwachting in een vermindering van zorgkosten.
Gelijkheid ((health) equity)
De werkgroep voorziet voor aanbevelingen over katheter diameter en materiaaleisen voor perifeer veneuze katheters geen effect op de gezondheidsgelijkheid.
Aanvaardbaarheid
Ethische aanvaardbaarheid
De werkgroep voorziet voor aanbevelingen over katheter diameter en materiaaleisen voor perifeer veneuze katheters geen ethische bezwaren.
Duurzaamheid
Er is geen systematisch literatuuronderzoek verricht naar duurzaamheid van materiaalkeuze voor perifeer veneuze katheters.
Het is belangrijk een afweging te maken tussen de noodzaak van het gebruik van verschillende materialen voor perifeer veneuze katheters enerzijds en duurzaamheid anderzijds. Deze afweging moet vanuit infectiepreventieoogpunt verantwoord gebeuren en kan verschillen per zorgsetting. Uitgangspunt hierbij is dat duurzaamheid niet ten koste mag gaan van patiëntveiligheid.
In het algemeen kan gezegd worden dat de preventie van katheter-gerelateerde infecties leidt tot minder gebruik van medische hulpmiddelen, minder gebruik van antibiotica en de daarmee gepaard gaande ontwikkeling van antibioticaresistentie.
Haalbaarheid
De werkgroep voorziet voor aanbevelingen over katheter diameter en materiaaleisen voor perifeer veneuze katheters geen belemmeringen voor de uitvoerbaarheid.
Rationale van aanbeveling 1 – Katheter diameter : weging van argumenten voor en tegen de interventies
De aanbevelingen over de optimale katheter diameter voor perifeer veneuze katheters bij volwassen patiënten en kinderen (geen neonaten) in de medisch-specialistische zorg zijn gebaseerd op het systematisch literatuuronderzoek, internationale richtlijnen, ondersteunende literatuur, en expert opinie.
Voor volwassen patiënten met een perifeer veneuze katheter is er onvoldoende bewijs gevonden voor een belangrijk effect van katheter diameter op katheter-gerelateerde infecties. Er zijn geen studies gevonden die het effect van katheter diameter hebben onderzocht voor ‘midline’ katheters. Er zijn geen studies gevonden die het effect van katheter diameter op katheter-gerelateerde infecties hebben onderzocht bij kinderen met een perifeer veneuze katheter.
Voor volwassen patiënten en kinderen met een perifeer veneuze katheter is er onvoldoende bewijs gevonden voor een belangrijk effect van katheter diameter op falen van de eerste inbrengpoging en katheterfalen door alle oorzaken.
Naast infectiepreventieoverwegingen zijn de indicatie voor katheterplaatsing en individuele patiëntkarakteristieken, zoals de benodigde lengte van de katheter, succes en complicaties van eerdere katheterplaatsing en beschikbare informatie uit echografie, van belang bij de keuze voor een perifeer veneuze katheter met een bepaalde diameter.
Alhoewel een katheter met een kleine diameter naar verwachting prettiger is voor de patiënt, is het effect van katheter diameter op de pijnbeleving in incidentele studies niet eenduidig. Hier ligt een kennisvraag.
Bij de keuze voor een perifeer veneuze katheter met een bepaalde diameter dient rekening te worden gehouden met het voorschrift van de fabrikant.
Gezien de onzekerheid van het bewijs voor een effect van katheter diameter op katheter-gerelateerde infecties is de werkgroep van mening dat er geen infectiepreventieoverwegingen zijn voor of tegen een bepaalde katheter diameter en adviseert daarom om de keuze voor een perifeer veneuze katheter met een bepaalde diameter niet op infectiepreventieoverwegingen te baseren. De werkgroep is van mening dat, rekening houdend met het voorschrift van de fabrikant, de indicatie voor katheterplaatsing en individuele patiëntkarakteristieken bepalend moeten zijn voor de keuze voor een perifeer veneuze katheter met een bepaalde diameter. De werkgroep maakt hierbij geen onderscheid tussen volwassen patiënten en kinderen.
Rationale van aanbeveling 2 – Overige materiaaleisen: weging van argumenten voor en tegen de interventies
Er is geen systematisch literatuuronderzoek verricht naar de plaats van overige materiaaleisen voor perifeer veneuze katheters bij de preventie van katheter-gerelateerde infecties bij volwassen patiënten en kinderen (geen neonaten) in de medisch-specialistische zorg.
De aanbevelingen over materiaaleisen voor perifeer veneuze katheters zijn gebaseerd op vigerende wet- en regelgeving.
Perifeer veneuze katheters zijn medische hulpmiddelen en moeten als zodanig voldoen aan Europese wetgeving op het gebied van medische hulpmiddelen, waaronder de Verordening (EU) 2017/745, de REACH-verordening (EG) 1907/2006, en de geharmoniseerde Europese normen:
Onderbouwing
Een perifeer veneuze katheter wordt ingebracht in een perifere vene en reikt niet verder dan de perifere venen.
Een perifeer veneuze katheter wordt gebruikt om (kortdurend) toegang te verkrijgen tot de bloedbaan voor het toedienen van medicatie, vloeistoffen en bloedproducten, en in uitzonderlijk gevallen voor het afnemen van bloed en het toedienen van parenterale voeding.
Er zijn verschillende typen perifeer veneuze katheters: 1) een korte perifeer veneuze katheter (tot 5 cm), die meestal wordt ingebracht in een vene in de hand, onderarm of elleboogplooi, ook wel bekend als ‘perifeer infuus’; 2) een lange perifeer veneuze katheter (6 tot 10 cm), die wordt ingebracht in een vene in de onderarm, elleboogplooi of bovenarm; en 3) een ‘midline’ katheter (vanaf 10 cm), die wordt ingebracht in een grote vene in de bovenarm.
Het gebruik van een perifeer veneuze katheter kan gepaard gaan met infectieuze en niet-infectieuze complicaties, zoals een bloedbaaninfectie en trombose. Deze complicaties kunnen belastend zijn voor de patiënt en kunnen resulteren in een afname van de kwaliteit van leven en een toename in zorgkosten.
Deze module beschrijft de materiaaleisen (waaronder de keuze voor een bepaalde diameter) voor perifeer veneuze katheters die van belang zijn bij de preventie van katheter-gerelateerde infecties voor volwassen patiënten en kinderen (geen neonaten) in de medisch-specialistische zorg.
Het is onduidelijk wat het effect is van de diameter van een perifeer veneuze katheter op katheter-gerelateerde infecties; het literatuuronderzoek richt zich op dit aspect. Indien er een effect is van diameter op katheter-gerelateerde infecties is de vraag wat de optimale diameter is en waar dit van afhankelijk is.
Table 1a. Summary of findings - adults
P: Adult patients requiring a peripheral venous catheter
I: Catheter diameter size <=18G
C: Catheter diameter size >=20G
S: Hospital
|
Outcome |
Number of patients (studies) |
Relative effect (95% CI) |
Absolute effect estimate (95% CI)* |
Certainty of the evidence** |
Conclusions |
|
CABSI (critical)1 |
RCTs -
|
RCTs -
|
RCTs -
|
RCTs No GRADE
|
No evidence was found regarding the effect of catheter diameter size <=18G (larger size) on CABSI compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter. |
|
Observational studies 93,233 (1 study)
|
Observational studies RR 0.87 (95% CI 0.45 to 1.69)
Not clinically relevant |
Observational studies <=18G: 35 per 100,000 >=20G: 40 per 100,000
RD 5 fewer (95% CI 22 fewer to 28 more) |
Observational studies Very low2 |
Observational studies The evidence is very uncertain about the effect of catheter diameter size <=18G (larger size) on CABSI compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter.
(Faltoni, 2023) |
|
|
Insertion site infection (important) |
- |
- |
- |
No GRADE |
No evidence was found regarding the effect of catheter diameter size <=18G (larger size) on insertion site infection compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter. |
|
(Thrombo)phlebitis (important) |
RCTs 178 (1 study) |
RCTs RR not estimable
|
RCTs 18G: not estimable 20G: 11 per 1,000
RD not estimable |
RCTs Very low3
|
RCTs The evidence is very uncertain about the effect of catheter diameter size <=18G (larger size) on (thrombo)phlebitis compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter.
(Mitra, 2024) |
|
Observational studies 5,920 (14 studies) |
Observational studies RR 1.03 (95% CI 0.88 to 1.22)
Not clinically relevant |
Observational studies <=18G: 400 per 1,000 >=20G: 388 per 1,000
RD 12 more (95% CI 47 fewer to 85 more) |
Observational studies Very low4 |
Observational studies The evidence is very uncertain about the effect of catheter diameter size <=18G (larger size) on (thrombo)phlebitis compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter.
Abbas, 2007; Buzatto, 2016; Cicolini, 2009; Cicolini, 2014; Gupta, 2022; Hasselberg, 2010; Kaur, 2011; Nassaji-Zavareh, 2007; Neopane, 2013; Rego Furtado, 2011; Saji, 2015; Simin, 2019; Singh, 2008; Uslusoy, 2008) |
|
|
All-cause mortality (important) |
- |
- |
- |
No GRADE |
No evidence was found regarding the effect of catheter diameter size <=18G (larger size) on all-cause mortality compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter. |
|
CABSI-related mortality (important)1 |
- |
- |
- |
No GRADE |
No evidence was found regarding the effect of catheter diameter size <=18G (larger size) on CABSI-related mortality compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter. |
|
First-attempt insertion failure (important) |
RCT 178 (1 study) |
RCT RR 0.88 95% CI 0.45 to 1.68)
Not clinically relevant |
RCT 18G: 158 per 1,000 20G: 180 per 1,000
RD 22 fewer (95% CI 99 fewer to 122 more) |
RCTs Very low5
|
RCTs The evidence is very uncertain about the effect of catheter diameter size <=18G (larger size) on first-attempt insertion failure compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter.
(Mitra, 2024) |
|
Observational study 1,063 (1 study) |
Observational studies RR 0.42 (95% CI 0.32 to 0.56)
Clinically relevant In favor of <=18G |
Observational studies <=18G: 106 per 1,000 >=20G: 252 per 1,000
RD 146 fewer (95% CI 171 fewer to 111 fewer) |
Observational studies Very low6 |
Observational studies The evidence is very uncertain about the effect of catheter diameter size <=18G (larger size) on first-attempt insertion failure compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter.
(van Loon, 2016) |
|
|
Catheter failure for any reason (important) |
RCT 178 (1 study)
|
RCT RR 2.00 95% CI 0.72 to 5.61)
Clinically relevant In favor of >=20G |
RCT 18G: 112 per 1,000 20G: 56 per 1,000
RD 56 more (95% CI 16 fewer to 259 more)
|
RCTs Very low5
|
RCTs The evidence is very uncertain about the effect of catheter diameter size <=18G (larger size) on catheter failure for any reason compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter.
(Mitra, 2024) |
|
Observational studies 4,527 (2 studies) |
Observational studies RR 0.99 (95% CI 0.61 to 1.16)
Not clinically relevant
|
Observational studies <=18G: 429 per 1,000 >=20G: 433 per 1,000
RD 4 fewer (95% CI 169 fewer to 69 more) |
Observational studies Very low7 |
Observational studies The evidence is very uncertain about the effect of catheter diameter size <=18G (larger size) on catheter failure for any reason compared with catheter diameter size >=20G (smaller size) in adult in-hospital patients requiring a peripheral venous catheter.
(DeVries, 2022; Leroux, 2023) |
CABSI = catheter-associated bloodstream infection; CI = confidence interval; CRBSI = catheter-related bloodstream infection; G = Gauge; RCT = randomized clinical trial; RD = risk difference; RR = risk ratio
* The risk in the <=18G group was based on the assumed risk in the >=20G group and the relative effect of the intervention.
** The level of evidence started at high for RCTs and low for observational studies.
1 None of the studies reported CRBSI as an outcome.
2 Downgraded by one level due to potential confounding by indication (risk of bias; -1), and the 95% confidence interval of the risk ratio crossing both thresholds for clinical relevance (imprecision; -2).
3 Downgraded by three levels due to lack of blinding and inadequate (too short) follow-up (risk of bias; -1), and zero events in one study group with a total sample size <4,000 (imprecision; -2).
4 Downgraded by one level due to the use of catheters as the unit of analysis and potential confounding by indication (risk of bias; -1), and inconsistent results (inconsistency; -1).
5 Downgraded by three levels due to lack of blinding and inadequate (too short) follow-up (risk of bias; -1), and the 95% confidence interval of the risk ratio crossing both thresholds for clinical relevance (imprecision; -2).
6 Downgraded by one level due to potential confounding by indication (risk of bias; -1).
7 Downgraded by one level due to the use of catheters as the unit of analysis and potential confounding by indication (risk of bias-1), and the 95% confidence interval of the risk ratio crossing the lower threshold for clinical relevance (imprecision;-1).
Table 1b. Summary of findings - children
P: Pediatric patients requiring a peripheral venous catheter
I: Catheter diameter size <=22G
C: Catheter diameter size >=24G
S: Hospital
|
Outcome |
Number of patients (studies) |
Relative effect (95% CI) |
Absolute effect estimate (95% CI)* |
Certainty of the evidence** |
Conclusions |
|
CRBSI/CABSI (critical) |
- |
- |
- |
No GRADE |
No evidence was found regarding the effect of catheter diameter size <=22G (larger size) on CRBSI/CABSI compared with catheter diameter size >=24G (smaller size) in pediatric in-hospital patients requiring a peripheral venous catheter. |
|
Insertion site infection (important) |
- |
- |
- |
No GRADE |
No evidence was found regarding the effect of catheter diameter size <=22G (larger size) on insertion site infection compared with catheter diameter size >=24G (smaller size) in pediatric in-hospital patients requiring a peripheral venous catheter. |
|
(Thrombo)phlebitis (important) |
- |
- |
- |
No GRADE |
No evidence was found regarding the effect of catheter diameter size <=22G (larger size) on (thrombo)phlebitis compared with catheter diameter size >=24G (smaller size) in pediatric in-hospital patients requiring a peripheral venous catheter. |
|
All-cause mortality (important) |
- |
- |
- |
No GRADE |
No evidence was found regarding the effect of catheter diameter size <=22G (larger size) on all-cause mortality compared with catheter diameter size >=24G (smaller size) in pediatric in-hospital patients requiring a peripheral venous catheter. |
|
CRBSI/CABSI-related mortality (important) |
- |
- |
- |
No GRADE |
No evidence was found regarding the effect of catheter diameter size <=22G (larger size) on CRBSI/CABSI-related mortality compared with catheter diameter size >=24G (smaller size) in pediatric in-hospital patients requiring a peripheral venous catheter. |
|
First-attempt insertion failure (important) |
425 (1 observational study) |
RR 0.51 (95% CI 0.23 to 1.12)
Clinically relevant In favor of <=22G |
<=22G: 46 1,000 >=24G: 91 per 1,000
RD 45 fewer (95% CI 70 fewer to 11 more) |
Very low1 |
The evidence is very uncertain about the effect of catheter diameter size <=22G (larger size) on first-attempt insertion failure compared with catheter diameter size >=24G (smaller size) in pediatric in-hospital patients requiring a peripheral venous catheter.
(Petroski, 2015) |
|
Catheter failure for any reason (important) |
4,38 (2 observational studies) |
Ben Abdelaziz, 2017 RR 1.36 (95% CI 1.04 to 1.77) |
Ben Abdelaziz, 2017 <=22G: 591 1,000 >=24G: 435 per 1,000
RD 157 more (95% CI 17 more to 335 more) |
Very low2 |
The evidence is very uncertain about the effect of catheter diameter size <=22G (larger size) on catheter failure for any reason compared with catheter diameter size >=24G (smaller size) in pediatric in-hospital patients requiring a peripheral venous catheter.
(Ben Abdelaziz, 2017; Gomez-Neva, 2022) |
|
Gomez-Neva, 2022 RR 0.71 (95% CI 0.44 to 1.15)
|
Gomez-Neva, 2022 <=22G: 258 1,000 >=24G: 364 per 1,000
RD 105 fewer (95% CI 204 fewer to 55 more) |
CABSI = catheter-associated bloodstream infection; CI = confidence interval; CRBSI = catheter-related bloodstream infection; G = Gauge; RD = risk difference; RR = risk ratio
* The risk in the <=18G group was based on the assumed risk in the >=20G group and the relative effect of the intervention.
** The level of evidence for observational studies started at low.
1 Downgraded by one level due to potential confounding by indication (risk of bias; -1) and the 95% confidence interval of the risk ratio crossing the lower threshold for clinical relevance (imprecision; -1).
2 Downgraded by one level due to potential confounding by indication (risk of bias; -1) and inconsistent results (inconsistency; -1).
Description of studies
Subquestion 1 – Catheter diameter
The literature summary is presented separately for adults and children because the working group expects the optimal peripheral venous catheter diameter size to differ between adults and children.
Adults
One RCT (Mitra, 2024) and 23 observational studies (Abbas, 2007; Abdul-Hak, 2014; Arias-Férnandez, 2017; Buzatto, 2016; Cicolini, 2009; Cicolini, 2014; DeVries, 2022; Erdogan, 2016; Faltoni, 2023; Gupta, 2022; Hasselberg, 2010; Kaur, 2011; Leroux, 2023; Nassaji-Zavareh, 2007; Neopane, 2013; Rego Furtado, 2011; Saji, 2015; Simin, 2019; Singh, 2008; Urbanetto, 2016; Uslusoy, 2008; Van Loon, 2016; Wallis, 2014) comparing different catheter diameter sizes in adult in-hospital patients requiring a peripheral venous catheter were included in the literature summary. Although an RCT was available, observational studies were included as well. The RCT reported only one (important) outcome of interest and optimal information size was not met. One observational study included both adults and children, but data were not presented by age (Faltoni, 2023). Midline catheters were not described.
Children
Three observational studies (Ben Abdelaziz, 2017; Gómez-Neva, 2022; Petroski, 2015) comparing different catheter diameter sizes in pediatric in-hospital patients requiring a peripheral venous catheter were included in the literature summary. Midline catheters were not described.
Important study characteristics of the included studies are summarized in the Characteristics of included studies table. The assessment of the risk of bias for the included studies is summarized in the Risk of bias table.
Subquestion 2 – Other material requirements
Not applicable.
Results
Subquestion 1 – Catheter diameter
Peripheral venous catheter diameter is expressed in Gauge (G). Catheter diameter and Gauge are inversely related; a lower Gauge indicates a larger diameter.
Adults
1. CABSI (critical)
One observational study reported CABSI as an outcome (Faltoni, 2023). The incidence of CABSI was 17/48,453 (0.04%) in the <=18G (larger size) group, compared to 18/44,780 (0.04%) in the >=20G (smaller size) group. This resulted in a 13% relative risk reduction in favor of <=18G (larger size) (RR 0.87; 95% CI 0.45 to 1.69). The relative risk reduction was considered not clinically relevant.
It should be noted that the authors reported an increased CABSI risk for catheters with a diameter size <=16G. The incidence of CABSI was 5/5,624 (0.09%) in the <=16G (larger size) group, compared to 30/87,609 (0.03%) in the >=18G (smaller size) group. The question is whether the choice for insertion of a <=16G catheter was (partially) driven by factors associated with a higher risk for infection (confounding by indication).
2. Insertion site infection (important)
None of the studies reported insertion site infection as an outcome.
3. (Thrombo)phlebitis (important)
One RCT reported (thrombo)phlebitis as an outcome (Mitra, 2024). The incidence of (thrombo)phlebitis was 0/89 (not estimable) in the 18G (larger size) group, compared to 1/89 (1.1%) in the 20G (smaller size) group. The risk ratio could not be estimated.
Nineteen observational studies reported (thrombo)phlebitis as an outcome. For fourteen studies, the results were pooled in a meta-analysis comparing catheter diameter size <=18G to >=20G (Abbas, 2007; Buzatto, 2016; Cicolini, 2009; Cicolini, 2014; Gupta, 2022; Hasselberg, 2010; Kaur, 2011; Nassaji-Zavareh, 2007; Neopane, 2013; Rego Furtado, 2011; Saji, 2015; Simin, 2019; Singh, 2008; Uslusoy, 2008) (Figure 1a.3a). The pooled incidence of (thrombo)phlebitis was 637/1,961 (32.5%) in the <=18G (larger size) group, compared to 1,537/3,959 (38.8%) in the >=20G (smaller size) group. This resulted in a pooled 3% relative risk increase in favor of >=20G (smaller size) (RRpooled 1.03; 95% CI 0.88 to 1.22). The relative risk increase was considered not clinically relevant. A funnel plot was not drawn because of inconsistent results.
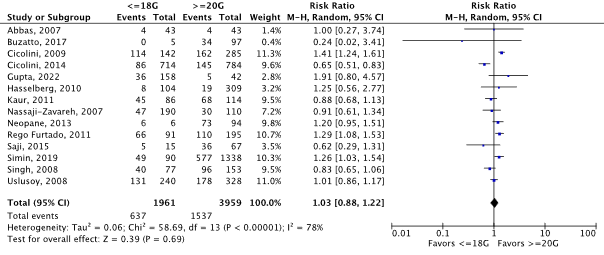
Figure 1a.3a Forest plot of (thrombo)phlebitis for catheter diameter size <=18G versus >=20G in adult in-hospital patients requiring a peripheral venous catheter. Pooled risk ratio, random effects model.
One observational study that compared catheter diameter size <=18G to >=20G did not report the absolute numbers of events and patients (or catheter days) per catheter diameter size group (Wallis, 2014). Therefore, the results could not be included in the meta-analysis. However, the reported 22% relative rate increase in favor of >=20G (smaller size) (RR 1.22; 95% CI 0.88 to 1.68) is consistent with the meta-analysis’s results.
Sensitivity analyses
The remaining four observational studies (Abdul-Hak, 2014; Arias-Fernandez, 2017; Erdogan, 2016; Urbanetto, 2016) were excluded from the primary meta-analysis, as the reporting of data did not allow a comparison between catheter diameter size <=18G and >=20G. As a sensitivity analysis, the results of these four studies were pooled in a meta-analysis comparing catheter diameter size <=20G to >=22G (Figure 1a.3b). The pooled incidence of (thrombo)phlebitis was 97/334 (29.0%) in the <=20G (larger size) group, compared to 155/661 (23.4%) in the >=22G (smaller size) group. This resulted in a pooled 19% relative risk increase in favor of >=22G (smaller size) (RRpooled 1.19; 95% CI 0.79 to 1.78), confirming the results of the primary meta-analysis.
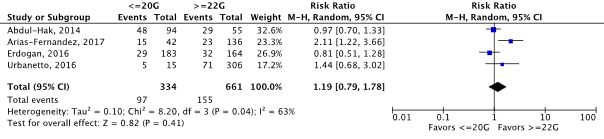
Figure 1a.3b Forest plot of (thrombo)phlebitis for catheter diameter size <=20G versus >=22G in adult in-hospital patients requiring a peripheral venous catheter (sensitivity analysis including studies that were excluded for the primary comparison only). Pooled risk ratio, random effects model.
4. All-cause mortality (important)
None of the studies reported all-cause mortality as an outcome.
5. CABSI-related mortality (important)
None of the studies reported CABSI-related mortality as an outcome.
6. First-attempt insertion failure (important)
One RCT reported first-attempt insertion failure as an outcome (Mitra, 2024). The incidence of first-attempt insertion failure was 14/89 (15.7%) in the 18G (larger size) group, compared to 16/89 (18.0%) in the 20G (smaller size) group. This resulted in a 12% relative risk reduction in favor of 18G (larger size) (RR 0.88; 95% CI 0.45 to 1.68). The relative risk reduction was considered not clinically relevant.
One observational study reported first-attempt insertion failure as an outcome (van Loon, 2016). The incidence of first-attempt insertion failure was 62/587 (10.6%) in the <=18G (larger size) group, compared to 120/476 (25.2%) in the >=20G (smaller size) group. This resulted in a 58% relative risk reduction in favor of <=18G (larger size) (RR 0.42; 95% CI 0.32 to 0.56). The relative risk reduction was considered clinically relevant.
7. Catheter failure for any reason (important)
One RCT reported catheter failure for any reason as an outcome (Mitra, 2024). The incidence of catheter failure for any reason was 10/89 (11.2%) in the 18G (larger size) group, compared to 5/89 (5.6%) in the 20G (smaller size) group. This resulted in a 100% relative risk increase in favor of 20G (smaller size) (RR 2.00; 95% CI 0.72 to 5.61). The relative risk increase was considered clinically relevant.
Two observational studies reported catheter failure for any reason as an outcome (DeVries, 2022; Leroux, 2023). The results were pooled in a meta-analysis (Figure 1a.7). The pooled incidence of catheter failure for any reason was 156/429 (36.4%) in the <=18G (larger size) group, compared to 1,775/4,098 (43.3%) in the >=20G (smaller size) group. This resulted in a pooled 1% relative risk reduction in favor of <=18G (larger size) (RRpooled 0.99; 95% CI 0.61 to 1.16). The relative risk reduction was considered not clinically relevant.

Figure 1a.7 Forest plot of catheter failure for any reason for catheter diameter size <=18G versus >=20G in adult in-hospital patients requiring a peripheral venous catheter. Pooled risk ratio, random effects model.
Children
1. CRBSI/CABSI (critical)
None of the studies reported CRBSI/CABSI as an outcome.
2. Insertion site infection (important)
None of the studies reported insertion site infection as an outcome.
3. (Thrombo)phlebitis (important)
None of the studies reported (thrombo)phlebitis as an outcome.
4. All-cause mortality (important)
None of the studies reported all-cause mortality as an outcome.
5. CRBSI/CABSI-related mortality (important)
None of the studies reported CRBSI/CABSI-related mortality as an outcome.
6. First-attempt insertion failure (important)
One observational study reported first-attempt insertion failure as an outcome (Petroski, 2015). The incidence of first-attempt insertion failure was 15/326 (4.6%) in the <=22G (larger size) group, compared to 9/99 (9.1%) in the >=24G (smaller size) group. This resulted in a 49% relative risk reduction (RR 0.51; 95% CI 0.23 to 1.12) in favor of <=22G (larger size). The relative risk reduction was considered clinically relevant.
7. Catheter failure for any reason (important)
Two observational studies reported catheter failure for any reason as an outcome with inconsistent results (Ben Abdelaziz, 2017; Gomez-Neva, 2022). The results were not pooled in a meta-analysis. In the study by Ben Abdelaziz (2017), the incidence of catheter failure for any reason was 59/100 (59.0%) in the <=22G (larger size) group, compared to 50/115 (43.5%) in the >=24G (smaller size) group. This resulted in a 36% relative risk increase in favor of >=24G (smaller size) (RR 1.36; 95% CI 1.04 to 1.77). In the study by Gomez-Neva (2022), the incidence of catheter failure for any reason was 15/58 (25.9%) in the <=22G (larger size) group, compared to 60/165 (36.4%) in the >=24G (smaller size) group. This resulted in a 29% relative risk reduction in favor of <=22G (larger size) (RR 0.71; 95% CI 0.44 to 1.15).
Subquestion 2 - Other material requirements
Not applicable.
Subquestion 1 – Catheter diameter
A systematic review of the literature was performed to answer the following (search)question:
What is the effect of peripheral venous catheter diameter size on catheter-related infections for in-hospital patients requiring a peripheral venous catheter?
Table PICOS
|
Patients |
Patients (non-neonates) requiring a peripheral venous catheter |
|
Intervention |
Peripheral venous catheters of different diameter size (<=16G, 18G, 20G, and >=22G) |
|
Control |
- |
|
Outcomes* |
CRBSI CABSI** Insertion site infection (Thrombo)phlebitis All-cause mortality CRBSI/CABSI-related mortality Insertion failure Catheter failure for any reason (e.g., phlebitis, infiltration, accidental removal, occlusion) |
|
Setting |
Hospital |
|
Other selection criteria |
Study design: systematic review, randomized controlled trial, or comparative observational study |
CABSI = catheter-associated bloodstream infection; CRBSI = catheter-related bloodstream infection; G = Gauge
* Per patient and, if reported, per 1,000 catheter days
**If CRBSI is not reported in any of the included studies
Relevant outcome measures
The guideline panel considered catheter-related bloodstream infection (CRBSI) and catheter-associated bloodstream infection (CABSI)* as critical outcome measures for decision-making; and insertion site infection, (thrombo)phlebitis, all-cause mortality, CRBSI (CABSI)-related mortality, insertion failure, and catheter failure for any reason as important outcome measures for decision-making.
* If CRBSI is not reported in any of the included studies
For CRBSI and CABSI, the guideline panel decided to use the definitions as described previously (Maki, 2006; Mermel, 2009; O’Grady, 2011). CRBSI was defined as a primary bloodstream infection with laboratory confirmation of the catheter as the source of the infection. CABSI was defined as a laboratory-confirmed primary bloodstream infection with the catheter in situ or within 48 hours of removal. For all other outcome measures, the guideline panel decided to use the definitions used by the authors of the individual studies.
The guideline panel defined the following thresholds for clinical relevance:
- Mortality: risk ratios of 0.95 and 1.05 (RR<0.95 or RR>1.05)
- Other dichotomous outcomes: risk ratios of 0.8 and 1.25 (RR<0.8 or RR>1.25)
Methods
Embase.com and Ovid/Medline databases were systematically searched with relevant search terms from 2000 until April 15, 2024. See Verantwoording for the detailed search strategy. The systematic literature search resulted in 272 unique hits.
Studies were selected based on the following eligibility criteria:
- Systematic review (SR) of randomized controlled trials (RCT) (at least two databases searched, detailed search strategy with search date, in- and exclusion criteria, description of individual study results, risk of bias assessment per study), or RCT; if an SR of RCTs or RCTs were not available, comparative observational studies were selected.
- SR describes at least one RCT that is not described in another selected SR.
- The research question includes all elements of the PICOS.
- The study population is not limited to hemodialysis patients.
- Full paper (i.e., no conference abstract, editorial, letter, or note).
- Full text is available.
- Full text is written in English or Dutch.
The reference lists of excluded systematic reviews were checked for studies that fulfilled the eligibility criteria and were not retrieved in the systematic literature search.
Based on title and abstract screening, 44 studies were initially selected. After reading the full text, 27 studies were excluded (Table of excluded studies), and seventeen were included. Reference checking of excluded systematic reviews resulted in ten additional eligible studies that were not retrieved in the literature search. Six studies were not indexed in Pubmed/Embase (Abdul-Hak, 2014; Buzatto, 2010; Erdogan, 2016; Kaur, 2011; Neopane, 2013; Saji, 2015); one study did not pass the design filter (Uslusoy, 2008); and three studies did not include I/C in title or abstract (Cicolini, 2014; Rego Furtado, 2011; Urbanetto, 2016).
Subquestion 2 – Other material requirements
For other material requirements for peripheral venous catheters, no systematic literature search was performed.
The recommendations were based on the previous WIP-guideline Flebitis en bloedbaaninfecties door intraveneuze infuuskatheters, international guidelines, legal regulations, supporting literature, and expert opinion.
- •Randomized controlled trials
- Mitra TP, Coulter-Nile S, Jegathees T, Luong J, Shetty A, Lai K. Spiced RCT: Success and Pain Associated with Intravenous Cannulation in the Emergency Department Randomized Controlled Trial. J Emerg Med. 2024 Feb;66(2):57-63. doi: 10.1016/j.jemermed.2023.10.008. Epub 2023 Oct 16. PMID: 38278677.
- •Observational studies
- Abbas SZ, de Vries TK, Shaw S, Abbas SQ. Use and complications of peripheral vascular catheters: a prospective study. Br J Nurs. 2007 Jun 14-27;16(11):648, 650, 652. doi: 10.12968/bjon.2007.16.11.23675. PMID: 17577181.
- Abdul-Hak CK, Barros AF. The incidence of phlebitis in a medical clinical unit. Texto Contexto Enferm. 2014 Jul Sept;23(3). doi: 10.1590/0104-07072014000900013.
- Arias-Fernández L, Suérez-Mier B, Martínez-Ortega MD, Lana A. Incidence and risk factors of phlebitis associated to peripheral intravenous catheters. Enferm Clin. 2017 Mar-Apr;27(2):79-86. English, Spanish. doi: 10.1016/j.enfcli.2016.07.008. Epub 2016 Sep 16. PMID: 27640931.
- Ben Abdelaziz R, Hafsi H, Hajji H, Boudabous H, Ben Chehida A, Mrabet A, Boussetta K, Barsaoui S, Sammoud A, Hamzaoui M, Azzouz H, Tebib N. Peripheral venous catheter complications in children: predisposing factors in a multicenter prospective cohort study. BMC Pediatr. 2017 Dec 19;17(1):208. doi: 10.1186/s12887-017-0965-y. Erratum in: BMC Pediatr. 2018 Sep 24;18(1):307. PMID: 29258474; PMCID: PMC5735659.
- Buzatto LL, Massa GP, Peterlini MAS, Whitaker IY. Factors associated with phlebitis in elderly patients with amiodarone intravenous infusion. Acta Paulista Enferm. 2016;29:260-266. doi:10.1590/1982-0194201600037.
- Cicolini G, Bonghi AP, Di Labio L, Di Mascio R. Position of peripheral venous cannulae and the incidence of thrombophlebitis: an observational study. J Adv Nurs. 2009 Jun;65(6):1268-73. doi: 10.1111/j.1365-2648.2009.04980.x. Epub 2009 Apr 3. PMID: 19374679.
- Cicolini G, Manzoli L, Simonetti V, Flacco ME, Comparcini D, Capasso L, Di Baldassarre A, Eltaji Elfarouki G. Phlebitis risk varies by peripheral venous catheter site and increases after 96 hours: a large multi-centre prospective study. J Adv Nurs. 2014 Nov;70(11):2539-49. doi: 10.1111/jan.12403. Epub 2014 Mar 31. PMID: 24684163.
- DeVries M, Scott N. Keeping Patients Safer: Reviewing Predictors of Success and Failure of Short Peripheral Intravenous Catheters. J Infus Nurs. 2022 Jul-Aug 01;45(4):210-219. doi: 10.1097/NAN.0000000000000468. PMID: 35820126.
- Erdogan BC, Denat Y. The development of phlebitis and infiltration in patients with peripheral intravenous catheters in the neurosurgery clinic and affecting factors. Int J Caring Sci. 2016;9(2):619-629.
- Faltoni M, Catho G, Pianca E, Minka-Obama B, Zanella MC, Chraiti MN, Fortchantre L, Harbarth S, Buetti N. Catheter size and risk of short-term peripheral venous catheter-associated bloodstream infections: an observational study. Clin Microbiol Infect. 2023 Dec 22:S1198-743X(23)00626-2. doi: 10.1016/j.cmi.2023.12.018. Epub ahead of print. PMID: 38142893.
- Gómez-Neva ME, Rondon Sepulveda MA, Buitrago-Lopez A. Lifespan of peripheral intravenous short catheters in hospitalized children: A prospective study. J Vasc Access. 2022 Sep;23(5):730-737. doi: 10.1177/11297298211005299. Epub 2021 Apr 12. PMID: 33845674.
- Gupta A, Nair R, Singh S, Khanna H, Bal A, Patrikar S. Compare the efficacy of recommended peripheral intravascular cannula insertion practices with a standard protocol: A randomized control trial. Med J Armed Forces India. 2022 Sep;78(Suppl 1):S111-S115. doi: 10.1016/j.mjafi.2022.01.004. Epub 2022 Apr 2. PMID: 36147434; PMCID: PMC9485856.
- Hasselberg D, Ivarsson B, Andersson R, Tingstedt B. The handling of peripheral venous catheters--from non-compliance to evidence-based needs. J Clin Nurs. 2010 Dec;19(23-24):3358-63. doi: 10.1111/j.1365-2702.2010.03410.x. Epub 2010 Oct 22. PMID: 20964751.
- Kaur P, Thakur R, Kaur S, Bhalla A. Assessment of risk factors of phlebitis amongst intravenous cannulated patients. Nursing Midwifery Res J. 2011;7:106-114. doi:10.1177/0974150X20110302.
- Leroux S, Deaner T, Wasser T, Huey C, Carr B, Howard A, Anspach C, Conner J, Sigal A. The Impact of Peripheral Intravenous Catheter Insertion Technique and Catheter-to-Vein Ratio on Postinsertion Failure. J Emerg Med. 2023 May;64(5):564-573. doi: 10.1016/j.jemermed.2023.02.011. Epub 2023 Mar 5. PMID: 37037760.
- Nassaji-Zavareh M, Ghorbani R. Peripheral intravenous catheter-related phlebitis and related risk factors. Singapore Med J. 2007 Aug;48(8):733-6. PMID: 17657380.
- Neopane A. Peripheral venous thrombophlebitis risk and the role of hand washing. Nepal J Med Sci. 2013;2(1):26-29. doi.org/10.3126/njms.v2i1.7647.
- Petroski A, Frisch A, Joseph N, Carlson JN. Predictors of difficult pediatric intravenous access in a community Emergency Department. J Vasc Access. 2015 Nov-Dec;16(6):521-6. doi: 10.5301/jva.5000411. Epub 2015 Jun 20. PMID: 26109542.
- Rego Furtado LC. Incidence and predisposing factors of phlebitis in a surgery department. Br J Nurs. 2011 Jul 28-Aug 4;20(14):S16-8, S20, S22 passim. doi: 10.12968/bjon.2011.20.sup7.s16. PMID: 21841668.
- Saji J, Korula SV, Mathew A, Mohan L. The incidence of thrombophlebitis following the use of peripheral intravenous cannula in post-operative patients a prospective observational study. IOSR J Dent Med Sci. 2015;14(6):1-4. doi:10.9790/0853-14610104.
- Simin D, Milutinović D, Turkulov V, Brkić S. Incidence, severity and risk factors of peripheral intravenous cannula-induced complications: An observational prospective study. J Clin Nurs. 2019 May;28(9-10):1585-1599. doi: 10.1111/jocn.14760. Epub 2019 Jan 17. PMID: 30589945.
- Singh R, Bhandary S, Pun KD. Peripheral intravenous catheter related phlebitis and its contributing factors among adult population at KU Teaching Hospital. Kathmandu Univ Med J (KUMJ). 2008 Oct-Dec;6(24):443-7. doi: 10.3126/kumj.v6i4.1732. PMID: 19483423.
- Urbanetto Jde S, Peixoto CG, May TA. Incidence of phlebitis associated with the use of peripheral IV catheter and following catheter removal. Rev Lat Am Enfermagem. 2016 Aug 8;24:e2746. doi: 10.1590/1518-8345.0604.2746. PMID: 27508916; PMCID: PMC4990043.
- Uslusoy E, Mete S. Predisposing factors to phlebitis in patients with peripheral intravenous catheters: a descriptive study. J Am Acad Nurse Pract. 2008 Apr;20(4):172-80. doi: 10.1111/j.1745-7599.2008.00305.x. PMID: 18387013.
- van Loon FHJ, Puijn LAPM, Houterman S, Bouwman ARA. Development of the A-DIVA Scale: A Clinical Predictive Scale to Identify Difficult Intravenous Access in Adult Patients Based on Clinical Observations. Medicine (Baltimore). 2016 Apr;95(16):e3428. doi: 10.1097/MD.0000000000003428. PMID: 27100437; PMCID: PMC4845841.
- Wallis MC, McGrail M, Webster J, Marsh N, Gowardman J, Playford EG, Rickard CM. Risk factors for peripheral intravenous catheter failure: a multivariate analysis of data from a randomized controlled trial. Infect Control Hosp Epidemiol. 2014 Jan;35(1):63-8. doi: 10.1086/674398. Epub 2013 Dec 2. PMID: 24334800.
- •Other
- Drugeon B, Guenezan J, Pichon M, Devos A, Fouassin X, Neveu A, Boinot L, Pratt V, Mimoz O. Incidence, complications, and costs of peripheral venous catheter-related bacteraemia: a retrospective, single-centre study. J Hosp Infect. 2023 May;135:67-73. doi: 10.1016/j.jhin.2023.02.012. Epub 2023 Mar 12. PMID: 36918069.
- Kaplan A, Korkut S, Avsarogullari OL. Comparison of procedure-related pain and patient satisfaction according to catheter size and insertion site in peripheral intravenous catheterization. J Vasc Access. 2023 Aug 3:11297298231190250. doi: 10.1177/11297298231190250. Epub ahead of print. PMID: 37537996.
- Kearney L, Craswell A, Massey D, Marsh N, Nugent R, Alexander C, Smitheram C, McLoughlin A, Ullman A. Peripheral intravenous catheter management in childbirth (PICMIC): A multi-centre, prospective cohort study. J Adv Nurs. 2021 Nov;77(11):4451-4458. doi: 10.1111/jan.14933. Epub 2021 Jun 12. PMID: 34118163.
- Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc. 2006 Sep;81(9):1159-71. doi: 10.4065/81.9.1159. PMID: 16970212.
- McCleskey P, Clark S. Contact dermatitis from a polyurethane dialysis catheter. Dermatitis. 2011 Mar-Apr;22(2):123-4. PMID: 21504702.
- Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O'Grady NP, Raad II, Rijnders BJ, Sherertz RJ, Warren DK. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2009 Jul 1;49(1):1-45. doi: 10.1086/599376. Erratum in: Clin Infect Dis. 2010 Apr 1;50(7):1079. Dosage error in article text. Erratum in: Clin Infect Dis. 2010 Feb 1;50(3):457. PMID: 19489710; PMCID: PMC4039170.
- Milanesi N, Gola M, Francalanci S. Allergic contact dermatitis caused by a polyurethane catheter. Contact Dermatitis. 2018 Nov;79(5):313-314. doi: 10.1111/cod.13050. Epub 2018 Jun 20. PMID: 29923607.
- O'Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, Lipsett PA, Masur H, Mermel LA, Pearson ML, Raad II, Randolph AG, Rupp ME, Saint S; Healthcare Infection Control Practices Advisory Committee (HICPAC). Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011 May;52(9):e162-93. doi: 10.1093/cid/cir257. Epub 2011 Apr 1. PMID: 21460264; PMCID: PMC3106269.
- O'Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, Lipsett PA, Masur H, Mermel LA, Pearson ML, Raad II, Randolph AG, Rupp ME, Saint S; Healthcare Infection Control Practices Advisory Committee (HICPAC). Guidelines for the prevention of intravascular catheter-related infections, 2011. Update 2017. 2017. ( https://www.cdc.gov/infection-control/media/pdfs/Guideline-BSI-H.pdf, accessed November 1, 2024).
- Pastor-Nieto MA, Alcántara F, Ballano A, Vergara A, Belmar P, Sánchez-Herreros C, Martín-Fuentes A, Jiménez E, De Eusebio E. Allergic contact dermatitis resulting from a poly(carbonate urethane) chronic haemodialysis central venous catheter. Contact Dermatitis. 2015 Feb;72(2):124-6. doi: 10.1111/cod.12325. Epub 2014 Dec 18. PMID: 25524294.
- van Loon FH, Puijn LA, van Aarle WH, Dierick-van Daele AT, Bouwman AR. Pain upon inserting a peripheral intravenous catheter: Size does not matter. J Vasc Access. 2018 May;19(3):258-265. doi: 10.1177/1129729817747531. Epub 2018 Mar 4. PMID: 29772984.
- No authors listed. 2021 Infusion Therapy Standards of Practice Updates. J Infus Nurs. 2021 Jul-Aug 01;44(4):189-190. doi: 10.1097/NAN.0000000000000436. PMID: 34197345.
- No authors listed. Guidelines for the prevention of bloodstream infections and other infections associated with the use of intravascular catheters: Part 1: peripheral catheters [Internet]. Geneva: World Health Organization; 2024. PMID: 38810002.
Characteristics of included studies table
|
Author, year Country Single- or multicenter
|
Catheter material Catheter insertion site Catheter size range |
N patients (baseline); catheters; catheter days Population Ward / procedure Follow-up |
Outcomes |
Remarks
|
|
|
Randomized controlled trials |
|||||
|
Mitra, 2024
Australia
Single-center |
FEP (Smiths Medical’s Jelco)
Hand Forearm Cubital fossa
18G to 20G |
T: 181*; 178; NR
Adults
ED
Until discharge from ED
* Incomplete outcome data: 3 |
Thrombophlebitis1 Insertion failure Catheter failure |
- |
|
|
Observational studies |
|||||
|
Abbas, 2007
United Kingdom
Single-center |
PTFE (Teflon)
NR
16G to 22G |
T: 86; 86; NR
Adults
ED
14 days (until removal) |
Thrombophlebitis2
|
- |
|
|
Abdul-Hak, 2014
Brazil
Single-center |
NR
Upper limb
18/20G – 22/24G |
T: 100; 234*
Adults
Pulmonology ward Cardiology ward
Until removal
* Catheter size unknown: 85 |
Phlebitis6 |
Unit of analysis: catheter |
|
|
Arias-Férnandez, 2017
Spain
Single-center |
NR
Hand Forearm Cubital fossa (‘flexure’) Arm
18G to 24G |
T: 105; 178; NR
Adults
Internal medicine Medical oncology Neurosurgery Hematology
Until removal
|
Phlebitis8 |
- |
|
|
Ben Abdelaziz, 2017
Tunesia
Multicenter |
FEP (B-CAT IV cannula)
Hand Wrist Forearm Antecubital fossa Foot Head
22G to 24G |
T: 98; 215; NR
Children (<18 years)
Pediatric ward Pediatric surgical ward
Until removal |
Catheter failure |
- |
|
|
Buzatto, 2016
Brazil
Single-center |
Vialon PU (Intima or Insyte)
Dorsal metacarpal Forearm Arm
16G-24G |
T: 102; 102; NR
Adults
CCU / receiving amiodarone MCU / receiving amiodarone
NR |
Phlebitis6 |
- |
|
|
Cicolini, 2009
Italy
Single-center |
NR
Hand Forearm Cubital fossa
16G-22G |
T: 427; 427; NR
Adults
Medical ward Surgical ward
12-96 hours (until removal) |
Thrombophlebitis4 |
- |
|
|
Cicolini, 2014
Italy
Multicenter |
Teflon Polyurethane Polyvinyl Polyethylene
Hand Forearm Antecubital fossa
14G-24G |
T: 1,498; 1,498. NR
Adults
Medical ward Surgical ward
Until 96 hours after insertion |
Phlebitis6 |
Multivariable analysis not considered (catheter size analyzed as continuous variable) |
|
|
DeVries, 2022
Australia
Single-center
|
Vialon PU (Nexiva / Insyte Autoguard)
Hand Forearm Antecubital fossa
14G to 24G |
T: NR; 4,305; 23,423
Adults
All wards
Until removal |
Catheter failure |
Unit of analysis: catheters |
|
|
Erdogan, 2016
Turkey
Single-center |
NR
Hand Wrist Forearm Antecubital fossa
20G-22G |
T: 325; 347; NR
Adults
Neurosurgery ward
Until 24 hours after catheter removal |
Phlebitis6 |
Unit of analysis: catheters |
|
|
Faltoni, 2023
Switzerland
Single-center
|
NR
Hand Wrist Forearm Antecubital fossa Other
≤16G to ≥22G |
T: 93,233; 206,804*; NR
Adults and children
Non-ICU wards
Until removal
* Catheter size NR: 5,391 |
CABSI |
Unit of analysis: catheters / analysis adjusted for clustering within patients |
|
|
Gómez-Neva, 2022
Colombia
Single-center |
Silicon, PTFE-coated
NR
18G to 24G |
T: 223; 223; NR
Children (<= 15 years)
Pediatric ward Pediatric ED
Until removal |
Phlebitis3 Catheter failure
|
- |
|
|
Gupta, 2022
India
Single-center |
PVC
Hand Wrist Forearm
16G-22G |
T: 200; 200; NR
Adults
Elective surgery
Until 72 hours or removal (if earlier) |
Thrombophlebitis5 |
Post-hoc analysis of RCT |
|
|
Hasselberg, 2010
Sweden
Single-center
|
PTFE (BD Venflon Pro)
NR
16G-22G |
T: 213*; 413; NR
Adults
Surgical ward
Until removal
* Incomplete outcome data: 17 |
Thrombophlebitis1 Occlusion |
Unit of analysis: catheters |
|
|
Kaur, 2011
India
Single-center |
NR
Hand Wrist Forearm
16G-22G
|
T: 349*; 200; NR
Adults
ED
Until removal
* Excluded for early removal: 149 |
Phlebitis8 |
- |
|
|
Leroux, 2023
United States
Single-center |
NR
Hand Forearm Antecubital fossa
16G-24G |
T: 222; 222; NR
Adults
ED
Until removal |
Catheter failure |
Post-hoc analysis of RCT
Ultrasound guidance more frequent for small catheter size groups |
|
|
Nassaji-Zavareh, 2007
Iran
Multicenter |
NR
Upper extremity Lower extremity
18G-20G |
T: 300; 300; NR
Adults
Medical ward Surgical ward
Until removal or discharge |
Phlebitis7 |
- |
|
|
Neopane, 2013
Nepal
Single-center |
NR
At and above elbow Below elbow
18G-22G |
T: 100; NR; NR
Adults
Medical ward
NR |
Thrombophlebitis10 |
Cannula and adhesive dressing brought by patient party |
|
|
Petroski, 2015
United States
Single-center |
NR
Hand Wrist Forearm Antecubital fossa Lower extremity
16G-24G |
T: 652*; 652; NR
Children (<18 years)
ED
NA
* Exposure data not available: no insertion failure: 206; insertion failure: 21 |
Insertion failure
|
-
|
|
|
Rego Furtado, 2011
Portugal (Azores)
Single-center |
NR
Back of hand Wrist Forearm Antecubital fossa Arm
18G-22G |
T: 171; 286; NR
Adults
General surgery ward
Until removal |
Phlebitis8 |
Unit of analysis: catheter |
|
|
Saji, 2015
India
Single-center |
NR
NR
18G-22G |
T: 82; NR; NR
Adults
Surgery ward
72 hours after insertion |
Phlebitis8 |
- |
|
|
Simin, 2019
Serbia
Single-center |
PTFE (Teflon) Vialon PU
Hand Wrist Lower forearm Antecubital fossa Lower limb
18G-24G |
T: 368; 1,428; NR
Adults
Infectious disease wards
Until removal
|
Phlebitis3 |
Unit of analysis: catheter |
|
|
Singh, 2008
Nepal
Single-center |
NR
Dorsum hand Forearm Joint
18G-20G |
T: 230; 230; NR
Adults
ICU Medical ward Surgical ward Obstetrics/gynecology ward
Until discharge or 2 days after removal |
Phlebitis8 |
- |
|
|
Urbanetto, 2016
Brazil
Single-center |
NR
Hand Wrist/arm Forearm Elbow pit
18G-24G |
T: 171; 361*; NR
Adults
All hospital wards
Until 96 hours after removal
* Lost to follow-up: 18G/20G: 5; 22G/24G: 35 |
Phlebitis1 |
Unit of analysis: catheter |
|
|
Uslusoy, 2008
Turkey
Single-center |
PTFE (Teflon)
Hand Wrist Forearm Antecubital fossa
16G-22G |
T: 355; 568; NR
Adults
General surgery ward
Until 48 hours after removal |
Phlebitis6 |
Unit of analysis: catheter |
|
|
Van Loon, 2016
The Netherlands
Single-center |
Vialon (Venflon Pro Safety BD)
Hand Forearm Antecubital Upper arm
14G-22G |
T: 1,104*; 1,104; NR
Adults
Scheduled for surgical procedure
NA
*Lost to follow-up: 41 |
Insertion failure |
- |
|
|
Wallis, 2014
Australia
Multicenter |
Vialon PU (Insyte Autoguard)
Hand Wrist Forearm Antecubital fossa Upper arm
≤18G-≥22 |
T: 3,283; 5,907; NR
Adults
Medical ward Surgical ward
NR |
Phlebitis9 |
Unit of analysis: catheters |
|
CABSI = catheter-associated bloodstream infection; CCU = coronary care unit; ED = emergency department; FEP = fluorinated ethylene propylene; G = Gauge; MCU = medium care unit; NA = not applicable; NR = not reported; PTFE = polytetrafluoroethylene; PVC = polyvinylchloride; PU = polyurethane; RCT = randomized controlled trial; T = total number
1 Criteria not reported
2 At least two of: pain, erythema, swelling, palpable venous cord
3 Visual infusion phlebitis scale (Jackson/Gallant, 2006)
4 Lundgren checklist
5 At least two of: local warmth, tenderness, redness, swelling
6 Infusion Nurses Society (INS) phlebitis scale
7 At least four of: erythema, pain, tenderness, warmth, induration, palpable cord, swelling
8 Jackson standard visual phlebitis scale (1998)
9 At least two of: pain and/or tenderness, erythema, swelling, purulent discharge, palpable venous cord
10 Redness, pain, and tenderness, with or without swelling, with or without fever, and blockage of the vein
intravenous flow
Risk of bias tables
Based on Cochrane risk of bias tool and suggestions by the CLARITY Group at McMaster University)
Randomized controlled trials
|
Author, year |
Random sequence generation |
Allocation concealment |
Blinding |
Incomplete outcome data |
Selective outcome reporting |
Other bias |
Overall risk of bias |
|
Was the allocation sequence adequately generated? |
Was the allocation adequately concealed? |
Was knowledge of the allocated interventions adequately prevented?
Were patients, healthcare providers, data collectors, outcome assessors, data analysts blinded? |
Was loss to follow-up (missing outcome data) infrequent? |
Are reports of the study free of selective outcome reporting? |
Was the study apparently free of other problems that could put it at a risk of bias? |
||
|
Mitra, 2024 |
Definitely yesA1 |
Definitely yesB1 |
Definitely noC1 |
Probably yesD1 |
Probably yesE1 |
Probably noF1, F2 |
High (all outcomes) |
A1 Central randomization using computer-generated random numbers
B1 Central randomization using opaque sealed envelopes
C1 Blinding of patients; no blinding of clinicians; blinding of outcome assessors and data analysts was not reported
D1 Missing outcome data were infrequent (<5%) and non-differential
E1 All outcomes described in the Methods section were reported
F1 No funding by industry or conflict of interest was reported
F2 Inadequate (too short) follow-up
Observational studies
|
Author, year |
Selection of participants |
Exposure |
Outcome of interest |
Confounding-assessment |
Confounding-analysis |
Assessment of outcome |
Follow-up |
Co-interventions |
Other bias |
Overall risk of bias |
|
Was selection of exposed and non-exposed cohorts drawn from the same population? |
Can we be confident in the assessment of exposure? |
Can we be confident that the outcome of interest was not present at start of study? |
Can we be confident in the assessment of confounding factors? |
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables? |
Can we be confident in the assessment of outcome? |
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed? |
Were co-interventions similar between groups? |
Was the study apparently free of other problems that could put it at a risk of bias? |
||
|
Abbas, 2007 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Probably yesD2 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI2,5 |
High (all outcomes) |
|
Abdul-Hak, 2014 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely noG6 |
Probably yesH1 |
Definitely noI2,4,5 |
High (all outcomes) |
|
Arias-Férnandez, 2017 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely yesE1 |
Probably noF2 |
Probably noG4 |
Probably yesH1 |
Definitely noI1,5 |
High (all outcomes) |
|
Ben Abdelaziz, 2017 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Probably noG5 |
Probably yesH1 |
Definitely noI2,5 |
High (all outcomes) |
|
Buzatto, 2016 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Probably noG5 |
Probably yesH1 |
Definitely noI2,5 |
High (all outcomes) |
|
Cicolini, 2009 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely yesE1 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,5 |
High (all outcomes) |
|
Cicolini, 2014 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,5 |
High (all outcomes) |
|
DeVries, 2022 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Probably yesD2 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI3,4,5 |
High (all outcomes) |
|
Erdogan, 2016 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,4,5 |
High (all outcomes) |
|
Faltoni, 2023 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Probably yesD2 |
Definitely yesE1 |
Definitely yesF1 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,5 |
High (all outcomes) |
|
Gómez-Neva, 2022 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,5 |
High (all outcomes) |
|
Gupta, 2022 |
Definitely yesA1 |
Definitely yesB1 |
Definitely yesC1 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,5 |
High (all outcomes) |
|
Hasselberg, 2010 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,4,5 |
High (all outcomes) |
|
Kaur, 2011 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely noG2,6 |
Probably yesH1 |
Definitely noI2,5 |
High (all outcomes) |
|
Leroux, 2023 |
Definitely yesA1 |
Definitely yesB1 |
Definitely yesC1 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Definitely noH2 |
Definitely noI2,5 |
High (all outcomes) |
|
Nassaji-Zavareh, 2007 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI2,5 |
High (all outcomes) |
|
Neopane, 2013 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Probably yesG1,3 |
Probably yesH1 |
Definitely noI2,5 |
High (all outcomes) |
|
Petroski, 2015 |
Definitely yesA1 |
Definitely noB2 |
Probably yesC2 |
Definitely noD3 |
Definitely noE2 |
Definitely noF3 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,5 |
High (all outcomes) |
|
Rego Furtado, 2011 |
Definitely yesA1 |
Definitely yesB1 |
Definitely yesC1 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,4,5 |
High (all outcomes) |
|
Saji, 2015 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI2,5 |
High (all outcomes) |
|
Simin, 2019 |
Definitely yesA1 |
Definitely yesB1 |
Definitely yesC1 |
Definitely yesD1 |
Definitely yesE1 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,4,5 |
High (all outcomes) |
|
Singh, 2008 |
Definitely yesA1 |
Definitely yesB1 |
Definitely yesC1 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI2,5 |
High (all outcomes) |
|
Urbanetto, 2016 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely noG2,6 |
Probably yesH1 |
Definitely noI2,4,5 |
High (all outcomes) |
|
Uslusoy, 2008 |
Definitely yesA1 |
Definitely yesB1 |
Probably yesC2 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI2,4,5 |
High (all outcomes) |
|
Van Loon, 2016 |
Definitely yesA1 |
Definitely yesB1 |
Definitely yesC1 |
Definitely yesD1 |
Definitely noE2 |
Probably noF2 |
Definitely yesG1,2 |
Probably yesH1 |
Definitely noI1,5 |
High (all outcomes) |
|
Wallis, 2014 |
Definitely yesA1 |
Definitely yesB1 |
Definitely noC3 |
Definitely yesD1 |
Definitely yesE1 |
Probably noF2 |
Probably yesG1,3 |
Probably yesH1 |
Definitely noI3,4,5 |
High (all outcomes) |
A1 Patients were selected from the same population within the same time frame
B1 Manufacturer-defined catheter size
B2 Exposure data were not available for a substantial part of the cohort
C1 Presence of the outcome at PVC insertion was excluded
C2 Patients enrolled required a (new) peripheral venous catheter, but the presence of the outcome at PVC insertion was not reported as an exclusion criterium
C3 Patients could be enrolled more than once
D1 Structured data collection
D2 Review of medical and nursing notes (reproducibility was not reported)
D3 Missing data on confounding variables reported
E1 Results were adjusted for confounding variables
E2 No adjustment for confounding variables
F1 Outcome data were extracted from a hospital-wide surveillance database
F2 Blinding of outcome assessment was not reported
F3 Outcome assessment was not blinded
G1 No or infrequent (<5%) missing outcome data were reported
G2 Follow-up was adequate
G3 Follow-up was not reported
G4 An unknown number of catheters was removed before the assessment of outcome
G5 No event was assumed for patients transferred to another ward
G6 Frequent (>=5%) missing outcome data
H1 No co-interventions were reported
H2 Co-intervention was not similar between groups
I1 No funding by industry or conflict of interest
I2 Funding by industry and conflict of interest were not reported
I3 Funding by industry, no bias was expected
I4 Catheters were used as the unit of analysis
I5 Potential confounding by indication
Tables of excluded studies
Systematic search – full text assessment
|
Reference |
Reason for exclusion |
|
Calleja R, Mielke N, Lee R, Johnson S, Bahl A. Hemolyzed Laboratory Specimens in the Emergency Department: An Underappreciated, but Frequent Problem. J Emerg Nurs. 2023 Sep;49(5):744-754. doi: 10.1016/j.jen.2023.06.001. Epub 2023 Jun 27. PMID: 37389514. |
O didn’t meet PICOS |
|
Chang WP, Peng YX. Occurrence of Phlebitis: A Systematic Review and Meta-analysis. Nurs Res. 2018 May/Jun;67(3):252-260. doi: 10.1097/NNR.0000000000000279. PMID: 29698331. |
Selection criteria for systematic reviews were not fulfilled |
|
Dugan L, Leech L, Speroni KG, Corriher J. Factors affecting hemolysis rates in blood samples drawn from newly placed IV sites in the emergency department. J Emerg Nurs. 2005 Aug;31(4):338-45. doi: 10.1016/j.jen.2005.05.004. PMID: 16126097. |
O didn’t meet PICOS |
|
Häske D, Dorau W, Eppler F, Heinemann N, Hochgreve B, Schempf B. Learning Success and Influencing Factors in Out-of-Hospital Placement of Intravenous Catheters. Prehosp Disaster Med. 2022 Dec;37(6):788-793. doi: 10.1017/S1049023X22001327. Epub 2022 Sep 26. PMID: 36156192. |
O didn’t meet PICOS |
|
Kaplan A, Korkut S, Avsarogullari OL. Comparison of procedure-related pain and patient satisfaction according to catheter size and insertion site in peripheral intravenous catheterization. J Vasc Access. 2023 Aug 3:11297298231190250. doi: 10.1177/11297298231190250. Epub ahead of print. PMID: 37537996. |
O didn’t meet PICOS |
|
Karaoğlan N, Sarı HY, Devrim İ. Complications of peripheral intravenous catheters and risk factors for infiltration and phlebitis in children. Br J Nurs. 2022 Apr 21;31(8):S14-S23. doi: 10.12968/bjon.2022.31.8.S14. PMID: 35439080. |
Relevant outcome data were not reported per catheter size |
|
Kashiura M, Yasuda H, Oishi T, Kishihara Y, Moriya T, Kotani Y, Kondo N, Sekine K, Shime N, Morikane K. Risk factors for peripheral venous catheter-related phlebitis stratified by body mass index in critically ill patients: A post-hoc analysis of the AMOR-VENUS study. Front Med (Lausanne). 2022 Nov 28;9:1037274. doi: 10.3389/fmed.2022.1037274. PMID: 36518742; PMCID: PMC9742461. |
Relevant outcome data were not reported for the overall population |
|
Kearney L, Craswell A, Massey D, Marsh N, Nugent R, Alexander C, Smitheram C, McLoughlin A, Ullman A. Peripheral intravenous catheter management in childbirth (PICMIC): A multi-centre, prospective cohort study. J Adv Nurs. 2021 Nov;77(11):4451-4458. doi: 10.1111/jan.14933. Epub 2021 Jun 12. PMID: 34118163. |
O didn’t meet PICOS |
|
Khan A, Laing E, Beaumont A, Wong J, Warrier S, Heriot A. Peripheral parenteral nutrition in surgery - a systematic review and meta-analysis. Clin Nutr ESPEN. 2023 Apr;54:337-348. doi: 10.1016/j.clnesp.2023.02.004. Epub 2023 Feb 10. PMID: 36963880. |
Selection criteria for systematic reviews were not fulfilled
I/C didn’t meet PICOS |
|
Lapostolle F, Catineau J, Garrigue B, Monmarteau V, Houssaye T, Vecci I, Tréoux V, Hospital B, Crocheton N, Adnet F. Prospective evaluation of peripheral venous access difficulty in emergency care. Intensive Care Med. 2007 Aug;33(8):1452-7. doi: 10.1007/s00134-007-0634-y. Epub 2007 Jun 7. PMID: 17554524. |
S didn’t meet PICOS |
|
Lee SU, Jung JY, Ham EM, Wang SW, Park JW, Hwang S, Kim DK, Kwak YH. Factors associated with difficult intravenous access in the pediatric emergency department. J Vasc Access. 2020 Mar;21(2):180-185. doi: 10.1177/1129729819865709. Epub 2019 Aug 3. PMID: 31379251. |
Reported outcome data were not suitable for data extraction |
|
Liu C, Chen L, Kong D, Lyu F, Luan L, Yang L. Incidence, risk factors and medical cost of peripheral intravenous catheter-related complications in hospitalised adult patients. J Vasc Access. 2022 Jan;23(1):57-66. doi: 10.1177/1129729820978124. Epub 2020 Dec 10. PMID: 33302797. |
I/C didn’t meet PICOS |
|
Matthews R, Gavin NC, Marsh N, Marquart-Wilson L, Keogh S. Peripheral intravenous catheter material and design to reduce device failure: A systematic review and meta-analysis. Infect Dis Health. 2023 Nov;28(4):298-307. doi: 10.1016/j.idh.2023.05.005. Epub 2023 Jul 5. PMID: 37419781. |
I/C didn’t meet PICOS
|
|
Naik VM, Mantha SSP, Rayani BK. Vascular access in children. Indian J Anaesth. 2019 Sep;63(9):737-745. doi: 10.4103/ija.IJA_489_19. PMID: 31571687; PMCID: PMC6761776. |
Selection criteria for systematic reviews were not fulfilled
I/C didn’t meet PICOS |
|
Paterson RS, Chopra V, Brown E, Kleidon TM, Cooke M, Rickard CM, Bernstein SJ, Ullman AJ. Selection and Insertion of Vascular Access Devices in Pediatrics: A Systematic Review. Pediatrics. 2020 Jun;145(Suppl 3):S243-S268. doi: 10.1542/peds.2019-3474H. PMID: 32482738. |
Selection criteria for systematic reviews were not fulfilled |
|
Resnick O, Abu Ahmad W, Bancovsky D, Rogachev S, Ashash A, Ohana Sarna Cahan L, Rekhtman D, Hashavya S, Gross I. Predicting factors for complications in peripheral intravenous catheters in the pediatric population. Acta Paediatr. 2021 May;110(5):1639-1644. doi: 10.1111/apa.15687. Epub 2020 Dec 2. PMID: 33226669. |
Reported outcome data were not suitable for data extraction |
|
Roggenland D, Peters SA, Lemburg SP, Holland-Letz T, Nicolas V, Heyer CM. CT angiography in suspected pulmonary embolism: impact of patient characteristics and different venous lines on vessel enhancement and image quality. AJR Am J Roentgenol. 2008 Jun;190(6):W351-9. doi: 10.2214/AJR.07.3402. PMID: 18492877. |
O didn’t meet PICOS |
|
Sabri A, Szalas J, Holmes KS, Labib L, Mussivand T. Failed attempts and improvement strategies in peripheral intravenous catheterization. Biomed Mater Eng. 2013;23(1-2):93-108. doi: 10.3233/BME-120735. PMID: 23442240. |
Selection criteria for systematic reviews were not fulfilled |
|
Shenoy S, Karunakar BP. Factors influencing the peripheral venous catheter survival in critically ill children in a pediatric intensive care unit. Indian J Pediatr. 2014 Dec;81(12):1293-6. doi: 10.1007/s12098-014-1430-7. Epub 2014 May 6. PMID: 24796410. |
I/C didn’t meet PICOS
|
|
Stroeder J, Fries P, Raczeck P, Buecker A, Jagoda P. Prospective safety evaluation of automated iomeprol 400 injections for CT through peripheral venous cannulas. Clin Radiol. 2020 May;75(5):396.e1-396.e6. doi: 10.1016/j.crad.2019.12.013. Epub 2020 Jan 20. PMID: 31969250. |
O didn’t meet PICOS |
|
Sweeny A, Archer-Jones A, Watkins S, Johnson L, Gunter A, Rickard C. The experience of patients at high risk of difficult peripheral intravenous cannulation: An Australian prospective observational study. Australas Emerg Care. 2022 Jun;25(2):140-146. doi: 10.1016/j.auec.2021.07.003. Epub 2021 Aug 27. PMID: 34456181. |
O didn’t meet PICOS |
|
Tagalakis V, Kahn SR, Libman M, Blostein M. The epidemiology of peripheral vein infusion thrombophlebitis: a critical review. Am J Med. 2002 Aug 1;113(2):146-51. doi: 10.1016/s0002-9343(02)01163-4. PMID: 12133753. |
Selection criteria for systematic reviews were not fulfilled |
|
Tripathi S, Kaushik V, Singh V. Peripheral IVs: factors affecting complications and patency--a randomized controlled trial. J Infus Nurs. 2008 May-Jun;31(3):182-8. doi: 10.1097/01.NAN.0000317704.03415.b9. PMID: 18496062. |
Reported outcome data were not suitable for data extraction |
|
Tripi PA, Thomas S, Clebone A, Goldfinger MM, Tobias JD. Peripheral intravenous catheter problems in infants and children presenting for anesthesia and surgery. Middle East J Anaesthesiol. 2016 Feb;23(4):411-4. PMID: 27382809. |
Relevant outcome data were not reported per catheter size |
|
Ullman AJ, Takashima M, Kleidon T, Ray-Barruel G, Alexandrou E, Rickard CM. Global Pediatric Peripheral Intravenous Catheter Practice and Performance: A Secondary Analysis of 4206 Catheters. J Pediatr Nurs. 2020 Jan-Feb;50:e18-e25. doi: 10.1016/j.pedn.2019.09.023. Epub 2019 Oct 21. PMID: 31648879. |
I/C didn’t meet PICOS O didn’t meet PICOS |
|
van Loon FH, Puijn LA, van Aarle WH, Dierick-van Daele AT, Bouwman AR. Pain upon inserting a peripheral intravenous catheter: Size does not matter. J Vasc Access. 2018 May;19(3):258-265. doi: 10.1177/1129729817747531. Epub 2018 Mar 4. PMID: 29772984. |
O didn’t meet PICOS |
|
Zarate L, Mandleco B, Wilshaw R, Ravert P. Peripheral intravenous catheters started in prehospital and emergency department settings. J Trauma Nurs. 2008 Apr-Jun;15(2):47-52. doi: 10.1097/01.JTN.0000327326.83276.ce. PMID: 18690133. |
Reported outcome data were not suitable for data extraction |
C = comparator; I = intervention; O = outcome; P = population; S = setting
In- and excluded systematic reviews – reference lists
|
Reference |
Reason for exclusion |
|
Bodenham Chair A, Babu S, Bennett J, Binks R, Fee P, Fox B, Johnston AJ, Klein AA, Langton JA, Mclure H, Tighe SQ. Association of Anaesthetists of Great Britain and Ireland: Safe vascular access 2016. Anaesthesia. 2016 May;71(5):573-85. doi: 10.1111/anae.13360. Epub 2016 Feb 17. Erratum in: Anaesthesia. 2016 Dec;71(12):1503. doi: 10.1111/anae.13691. PMID: 26888253; PMCID: PMC5067617. |
Clinical practice guideline |
|
Crocoli A, Tornesello A, Pittiruti M, Barone A, Muggeo P, Inserra A, Molinari AC, Grillenzoni V, Durante V, Cicalese MP, Zanazzo GA, Cesaro S. Central venous access devices in pediatric malignancies: a position paper of Italian Association of Pediatric Hematology and Oncology. J Vasc Access. 2015 Mar-Apr;16(2):130-6. doi: 10.5301/jva.5000314. Epub 2014 Oct 14. PMID: 25362978. |
Clinical practice guideline |
|
Doellman D, Buckner JK, Garrett JH, Catudal JP, Frey AM, Lamagna P, Whitehead M. Best practice guidelines in the care and maintenance of pediatric central venous catheters. 2015. Association for Vascular Access. |
Clinical practice guideline |
|
Gorski LA, Hadaway L, Hagle ME, Broadhurst D, Clare S, Kleidon T, Alexander M. Infusion therapy standards of practice. Journal of infusion nursing. 2021;44(1S);S1-S224. |
Clinical practice guideline |
|
Intravenous Nursing New Zealand Incorporated Society. Provisional Infusion Therapy Standards of Practice. Auckland, New Zealand: Intravenous Nursing New Zealand Incorporated Society. 2012. |
Clinical practice guideline |
|
Jacobson AF, Winslow EH. Variables influencing intravenous catheter insertion difficulty and failure: an analysis of 339 intravenous catheter insertions. Heart Lung. 2005 Sep-Oct;34(5):345-59. doi: 10.1016/j.hrtlng.2005.04.002. PMID: 16157191. |
Reported outcome data were not suitable for data extraction |
|
Khawaja HT, Campbell MJ, Weaver PC. Effect of transdermal glyceryl trinitrate on the survival of peripheral intravenous infusions: a double-blind prospective clinical study. Br J Surg. 1988 Dec;75(12):1212-5. doi: 10.1002/bjs.1800751223. PMID: 3148355. |
Reported outcome data were not suitable for data extraction |
|
Menéndez JJ, Verdú C, Calderón B, Gómez-Zamora A, Schüffelmann C, de la Cruz JJ, de la Oliva P. Incidence and risk factors of superficial and deep vein thrombosis associated with peripherally inserted central catheters in children. J Thromb Haemost. 2016 Nov;14(11):2158-2168. doi: 10.1111/jth.13478. Epub 2016 Oct 12. PMID: 27558946. |
P didn’t meet PICOS |
|
Nifong TP, McDevitt TJ. The effect of catheter to vein ratio on blood flow rates in a simulated model of peripherally inserted central venous catheters. Chest. 2011 Jul;140(1):48-53. doi: 10.1378/chest.10-2637. Epub 2011 Feb 24. PMID: 21349931. |
Laboratory study |
|
Sharp R, Cummings M, Fielder A, Mikocka-Walus A, Grech C, Esterman A. The catheter to vein ratio and rates of symptomatic venous thromboembolism in patients with a peripherally inserted central catheter (PICC): a prospective cohort study. Int J Nurs Stud. 2015 Mar;52(3):677-85. doi: 10.1016/j.ijnurstu.2014.12.002. Epub 2014 Dec 19. PMID: 25593110. |
P didn’t meet PICOS |
|
Wyckoff MM, Sharpe EL. Peripherally Inserted Central Catheters: Guideline for Practice, 3rd ed. Chicago, IL: National Association of Neonatal Nurses. 2015. |
Clinical practice guideline |
C = comparator; I = intervention; O = outcome; P = population; S = setting
Beoordelingsdatum en geldigheid
Publicatiedatum : 12-02-2026
Beoordeeld op geldigheid : 12-02-2026
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd door het ministerie van VWS. De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Werkgroep
- S. (Selma) Bons, Nederlandse Vereniging voor Anesthesiologie (NVA), voorzitter
- Dr. M. (Michelle) Gompelman, Nederlandse Internisten Vereniging (NIV), Nederlandse Vereniging van Internist-Infectiologen (NVII)
- R. (Renze) Jongstra, Verpleegkundigen & Verzorgenden Nederland (V&VN)
- H. (Heidy) Koene, Vereniging voor Hygiëne & Infectiepreventie in de Gezondheidszorg (VHIG)
- M.H.H. (Marc) Königs, Nederlandse Vereniging voor Intensive Care (NVIC)
- Dr. B.J. (Bart) Laan (AIOS), Nederlandse Internisten Vereniging (NIV), Nederlandse Vereniging van Internist-Infectiologen (NVII)
- K. (Kelly) Niggebrugge-Mentink, Nederlandse Vereniging van Ziekenhuisapothekers (NVZA)
- Dr. J.H. (Jan) van Zeijl, Nederlandse Vereniging voor Medische Microbiologie (NVMM)
Klankbordgroep
- Dr. J.R.A. (Jeetindra) Balak, Nederlandse Internisten Vereniging (NIV), Nederlandse Federatie voor Nefrologie (NFN)
- Werkgroep richtlijn Centraal veneuze toegang (NVvH)
- Werkgroep leidraad Infusietechnologie (NVKF)
Met ondersteuning van
- Mw. A. (Alies) Oost, informatiespecialist, Kennisinstituut van Federatie Medisch Specialisten
- Dr. H. (Haitske) Graveland, senior adviseur, Kennisinstituut van Federatie Medisch Specialisten
- Dr. M.F.Q. (Marjolein) Kluijtmans-van den Bergh, senior adviseur, Kennisinstituut van Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
S. (Selma) Bons |
Anesthesioloog, Prinses Maxima Centrum voor kinderoncologie, Utrecht |
Lid werkgroep SRI richtlijnen
Lid bestuur sectie kinderanesthesiologie NVA
Lid SRI |
Geen |
Geen restrictie |
|
Dr. M. (Michelle) Gompelman |
Internist-infectioloog, Elkerliek Ziekenhuis, Helmond |
Lid werkgroep FMS-richtlijn Centraal veneuze toegang
|
Geen |
Geen restrictie |
|
A. (Renze) Jongstra |
Intensive care verpleegkundige |
Vicevoorzitter V&VN afdeling IC (onbetaald)
|
Geen |
Geen restrictie |
|
H. (Heidy) Koene |
Deskundige infectiepreventie, Erasmus MC, Rotterdam |
Geen |
Geen |
Geen restrictie |
|
M.H.H. (Marc) Königs |
Intensivist, Maxima Medisch Centrum. Eindhoven/Veldhoven (100%) |
Duikerarts / duikclubarts
Waarnemer intensivist Aruba en via IC (max. 200 uur/jaar) In het verleden voordrachten op congressen voor 3M en BD (betaald) - ESAIC ( Milaan / München) - WOCOVA ( Athene) - Nordic congres for vasculary acces |
Geen |
Geen restrictie (adviseurschap 3M onbetaald) |
|
Dr. B.J. (Bart) Laan |
AIOS Interne Geneeskunde, Amsterdam UMC, Amsterdam |
Geen |
Geen |
Geen restrictie |
|
K. (Kelly) Niggebrugge-Mentink |
Ziekenhuisapotheker, Hagaziekenhuis, Den Haag |
Gastdocent Fontys Hogeschool (verpleegkundig specialistenopleiding); betaald Gastspreker congres Stichting Vascular Infusion Technology; onbetaald |
Geen |
Geen restrictie |
|
Dr. J.H. (Jan) van Zeijl |
Arts-microbioloog, Certe Medische Diagnostiek & Advies, afdeling Medische Microbiologie (tot april 2024)
Waarnemend arts-microbioloog, Certe Medische Diagnostiek & Advies, afdeling Medische Microbiologie (september t/m december 2025) |
Bestuurslid (sinds januari 2024 voorzitter) Vasculitis Stichting met portefeuille vrijwilligersbeleid en Zorg, Research en Belangenbehartiging; onbetaald |
Geen |
Geen restrictie |
|
Klankbordgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Dr. J.R.A. (Jeetindra) Balak |
Internist, Leids UMC, Leiden |
Geen |
Geen |
Geen restrictie |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van Patiëntenfederatie Nederland (PFNL) voor de schriftelijke knelpunteninventarisatie. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan PFNL en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijn is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling zijn richtlijnmodules op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Uit de kwalitatieve raming blijkt dat er geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
|
Module |
Uitkomst raming |
Toelichting |
|
Materiaalkeuze voor perifeer veneuze katheters |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn (>40.000 patiënten), volgt ook uit de toetsing dat het overgrote deel (±90%) van de zorgaanbieders en zorgverleners al aan de norm voldoet. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 3.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II-instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten met betrekking tot infectiepreventiemaatregelen rondom intravasculaire katheters. De werkgroep beoordeelde de aanbeveling(en) uit de eerdere WIP-richtlijn Arteriële katheters en de WIP-richtlijn Flebitis en bloedbaaninfecties door intraveneuze infuuskatheters. Tevens zijn er in de schriftelijke knelpunteninventarisatie knelpunten aangedragen door Inspectie Gezondheidszorg en Jeugd (IGJ), Landelijke Vereniging van Operatieassistenten (LVO), Nederlandse Vereniging van Anesthesiemedewerkers (NVAM), Nederlandse Vereniging van Revalidatieartsen (VRA), Nederlandse Vereniging van Ziekenhuizen (NVZ), Nederlandse Vereniging voor Heelkunde (NVvH), Nederlandse Vereniging voor Medische Microbiologie (NVMM), Rijksinstituut voor Volksgezondheid en Milieu (RIVM), Stichting Kind en Ziekenhuis, Vereniging voor Hygiëne & Infectiepreventie in de Gezondheidszorg (VHIG), Verpleegkundigen & Verzorgenden Nederland (V&VN). Een verslag hiervan is opgenomen onder Verslag schriftelijke knelpunteninventarisatie.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvragen behorende bij de uitgangsvragen inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Ook definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder Zoekverantwoording. Indien mogelijk werden de gegevens uit verschillende studies gepoold in een random-effects-model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de wetenschappelijke bewijskracht wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie https://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nul effect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), duurzaamheid, aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje Overwegingen en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016A; Alonso-Coello 2016B). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE-methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling is gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417. A
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494. B
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 3.0 (2023). Adviescommissie Richtlijnen van de Raad Kwaliteit. Available from: https://richtlijnendatabase.nl/uploaded/docs/FMS_MedSpecRicht_2023__v04.pdf?u=1bULOR
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from: https://gdt.gradepro.org/app/handbook/handbook.html.
Zoekverantwoording
Algemene informatie
|
Richtlijn Intravasculaire katheters |
|
|
Uitgangsvraag: Wat is de optimale diameter van een perifeer veneuze katheter om katheter-gerelateerde infecties te voorkomen? Zoekvraag: What is the effect of peripheral venous catheter size on catheter-related infectious complications in patients requiring a peripheral venous catheter? |
|
|
Database(s): Embase.com, Ovid/Medline |
Datum: 15 april 2024 |
|
Periode: vanaf 2000 |
Talen: geen restrictie |
|
Literatuurspecialist: Alies Oost |
Rayyan review: https://rayyan.ai/reviews/937502 |
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Deduplication: voor het ontdubbelen is gebruik gemaakt van http://dedupendnote.nl:9777/ |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen:
|
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SR |
19 |
17 |
19 |
|
RCT |
129 |
67 |
133 |
|
Observationele studies |
100 |
120 |
120 |
|
Totaal |
248 |
204 |
272* |
*in Rayyan
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#1 |
'peripheral venous catheter'/exp OR 'peripheral intravenous catheter*':ti,ab,kw OR 'peripheral intra venous catheter*':ti,ab,kw OR 'peripheral venous catheter*':ti,ab,kw OR 'peripheral vascular catheter*':ti,ab,kw OR 'peripheral intravascular catheter*':ti,ab,kw OR 'peripheral intra vascular catheter*':ti,ab,kw OR 'peripheral catheter*':ti,ab,kw OR 'peripheral intravenous cannula*':ti,ab,kw OR 'peripheral intra venous cannula*':ti,ab,kw OR 'peripheral venous cannula*':ti,ab,kw OR 'peripheral vascular cannula*':ti,ab,kw OR 'peripheral intravascular cannula*':ti,ab,kw OR 'peripheral intra vascular cannula*':ti,ab,kw OR 'peripheral cannula*':ti,ab,kw OR 'peripheral intravenous line*':ti,ab,kw OR 'peripheral intra venous line*':ti,ab,kw OR 'peripheral venous line*':ti,ab,kw OR 'peripheral vascular line*':ti,ab,kw OR 'peripheral intravascular line*':ti,ab,kw OR 'peripheral intra vascular line*':ti,ab,kw OR 'peripheral line*':ti,ab,kw OR 'peripheral intravenous access*':ti,ab,kw OR 'peripheral intra venous access*':ti,ab,kw OR 'peripheral venous access*':ti,ab,kw OR 'peripheral vascular access*':ti,ab,kw OR 'peripheral intravascular access*':ti,ab,kw OR 'peripheral intra vascular access*':ti,ab,kw OR ((peripheral* NEAR/2 (iv OR ivs)):ti,ab,kw) OR ((midline NEAR/2 catheter*):ti,ab,kw) OR pivc:ti,ab,kw OR pivcs:ti,ab,kw |
8159 |
|
#2 |
'vein diameter'/exp OR (((catheter* OR pvc OR pivc OR cannul* OR vein* OR venous) NEAR/4 (size* OR diameter OR caliber OR gauge OR ratio*)):ti,ab,kw) OR (((catheter* OR pvc OR pivc OR pivcs OR cannul*) NEAR/4 material):ti,ab,kw) OR cvr:ti,ab,kw |
30231 |
|
#3 |
#1 AND #2 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) AND [2000-2024]/py |
309 |
|
#4 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
1018893 |
|
#5 |
'clinical trial'/exp OR 'randomization'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp OR 'placebo'/exp OR 'prospective study'/exp OR rct:ab,ti OR random*:ab,ti OR 'single blind':ab,ti OR 'randomised controlled trial':ab,ti OR 'randomized controlled trial'/exp OR placebo*:ab,ti |
4010868 |
|
#6 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
8172045 |
|
#7 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
14991452 |
|
#8 |
#3 AND #4 - SR |
19 |
|
#9 |
#3 AND #5 NOT #8 - RCT |
129 |
|
#10 |
#3 AND (#6 OR #7) NOT (#8 OR #9) - observationeel |
100 |
|
#11 |
#8 OR #9 OR #10 |
248 |
Ovid/Medline
|
# |
Searches |
Results |
|
1 |
('Peripheral intravenous catheter*' or 'Peripheral intra venous catheter*' or 'Peripheral venous catheter*' or 'peripheral vascular catheter*' or 'peripheral intravascular catheter*' or 'peripheral intra vascular catheter*' or 'Peripheral catheter*' or 'Peripheral intravenous cannula*' or 'Peripheral intra venous cannula*' or 'peripheral venous cannula*' or 'peripheral vascular cannula*' or 'peripheral intravascular cannula*' or 'peripheral intra vascular cannula*' or 'Peripheral cannula*' or 'Peripheral intravenous line*' or 'Peripheral intra venous line*' or 'Peripheral venous line*' or 'Peripheral vascular line*' or 'peripheral intravascular line*' or 'peripheral intra vascular line*' or 'peripheral line*' or 'Peripheral intravenous access*' or 'Peripheral intra venous access*' or 'Peripheral venous access*' or 'Peripheral vascular access*' or 'peripheral intravascular access*' or 'peripheral intra vascular access*' or (peripheral* adj2 (iv or ivs)) or (midline adj2 catheter*) or pivc or pivcs).ti,ab,kf. |
4246 |
|
2 |
(((catheter* or pvc or pivc or cannul* or vein* or venous) adj4 (size* or diameter or caliber or gauge or ratio*)) or ((catheter* or pvc or pivc or pivcs or cannul*) adj4 material) or cvr).ti,ab,kf. |
17785 |
|
3 |
(1 and 2) not (comment/ or editorial/ or letter/) not ((exp animals/ or exp models, animal/) not humans/) |
297 |
|
4 |
limit 3 to yr="2000 -Current" |
262 |
|
5 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
739031 |
|
6 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2712861 |