Katheterslot
Uitgangsvraag
Wat is de waarde van een antimicrobieel katheterslot bij een centraal veneuze toegang (alle lijntypen) bij volwassen patiënten?
Aanbeveling
Gebruik geen antibiotisch katheterslot in de preventie van katheter-gerelateerde infecties.
Overweeg het gebruik van een Taurolidine gebaseerd katheterslot in het geval van:
- Een hogere lokale incidentie van katheter-gerelateerde infectieuze complicaties dan op basis van eerdere surveillancegegevens verwacht werd, ondanks optimale naleving van de aanbevelingen in deze richtlijn.
- Patiënten bekend met recidiverende katheterinfecties.
- Patiënten die immuun-gecompromitteerd zijn, zoals hematologische en oncologische patiënten.
- Frequent en/of thuisgebruik zoals bij Totale Parenterale Voeding (TPV).
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is literatuuronderzoek gedaan naar de gunstige en ongunstige effecten van het gebruik van een antimicrobieel katheterslot vergeleken met een katheterslot met heparine of fysiologisch zout bij patiënten met een centraal veneuze katheter. Op basis van elf gerandomiseerde studies lijkt de cruciale uitkomstmaat katheter-gerelateerde infectie lager bij patiënten met een antimicrobieel katheterslot. De Grade bewijskracht voor deze uitkomstmaat en daarmee ook de totale bewijskracht is laag, door beperkingen in de onderzoeksopzet en/of rapportage, en vanwege tegenstrijdige resultaten. De belangrijke uitkomstmaat complicaties kan geen richting geven aan de besluitvorming door de zeer lage bewijskracht. De belangrijke uitkomstmaten kwaliteit van leven, patiënttevredenheid en aantal katheter gerelateerde interventies per jaar werden niet beschreven in de geïncludeerde literatuur. Op basis van de directe literatuur zou de voorkeur uitgaan naar het gebruik van een antimicrobieel katheterslot ten opzichte van een katheterslot met heparine/fysiologisch zout bij patiënten met een centraal veneuze katheter.
Belangrijk bij het voorkomen van infecties zijn de infectiepreventiemaatregelen rondom inbrengen en verzorging. Bij de juiste infectiepreventiemaatregelen bij het inbrengen en verzorgen is de kans op een infectie lager. De rol van deze maatregelen is in de studies niet bekend. Daarom dient eerst deze preventie geoptimaliseerd te zijn alvorens naar een antimicrobieel katheterslot over te gaan. De complicaties bij katheter gebruik dienen jaarlijks geëvalueerd te worden. Interventie wordt alleen aanbevolen wanneer de lokale incidentie van katheter-gerelateerde infectieuze complicaties hoger is dan op basis van eerdere surveillancegegevens verwacht, ondanks optimale naleving van de aanbevelingen in deze richtlijn.
Bij het preventief gebruik van antibiotica is ook altijd het risico van het induceren van resistentie. Daarom wordt het gebruik van antibiotica die ook in de systemische behandeling van patiënten gebruikt worden, ontraden. De werkgroep ziet alleen plaats voor een antibiotisch katheterslot als behandeling van katheter gerelateerde infectie bij een bekend gevoelig micro-organisme.
Taurolidine en ethanol hebben geen systemische toepassing en zijn daarom de middelen van keuze voor een preventief katheterslot. Waarbij de sterkste evidentie voor taurolidine is (figuur 1).
Taurolidine is goed verenigbaar met andere medicatie, echter speelt het in dit geval geen rol, omdat taurolidine in het katheterslot zit en niet wordt ingespoten. De effectiviteit van ethanol is niet overtuigend. Daarnaast bestaat bij ethanol ook het risico op beschadiging van de katheter, daarom wordt dit niet aangeraden (ESPEN richtlijn, Pironi, 2016).
Bekende risicofactoren voor katheter-gerelateerde infecties zijn o.a. de duur dat de katheter aanwezig is, frequent aanprikken, multi-lumen katheters, gebruik voor TPV of chemotherapie en patiënten met immuun suppressie. Voor bepaalde groepen patiënten geldt dus een hoger risico voor katheter-gerelateerde infecties (Cabrero, 2023; Huang, 2024).
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Voor de patiënt zit er weinig risico aan het gebruik van een antimicrobieel katheterslot ten opzichte van een katheterslot met heparine of fysiologisch zout. De meerwaarde is het voorkomen van infecties. Als voor de betreffende katheter bij de specifieke patiëntengroep op voorhand al een lage infectiekans is, is de meerwaarde beperkt. Dat zal in individuele gevallen met meer risicofactoren afgewogen moeten worden.
Kosten (middelenbeslag)
De kosten van een ethanol katheterslot zijn verwaarloosbaar, van taurolidine zijn de kosten beperkt (op moment van schrijven van deze module €9,- per ampul). Dit is daarom niet van invloed op de besluitvorming.
Aanvaardbaarheid, haalbaarheid en implementatie
Het katheterslot wordt in de praktijk al gebruikt. De procedure van het omgaan met katheters verandert niet wezenlijk door het toevoegen van een antimicrobieel middel. Dus het heeft nauwelijks impact.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventie
De studies over het gebruik van antibiotica in het katheterslot zijn zeer divers in middel, gebruiksduur en populatie. Ook is het vaak niet duidelijk of er op een specifiek micro-organisme gericht wordt. Een middel als vancomycine komt er in studies soms beter uit dan een katheterslot met alleen heparine. Vancomycine is ook het eerste keus middel bij verdenking op CRBSI, dat is een belangrijke reden om vancomycine niet te gebruiken in de preventie. Daarnaast speelt er het risico op resistentievorming. Bij het goed toepassen van de procedure inclusief de daarbij horende infectiepreventiemaatregelen voor inbrengen en onderhouden van een CVL is de kans op infectie van de lijn zeer laag. De toegevoegde waarde van een antimicrobieel middel aan een katheterslot is beperkt. De sterkste argumenten om een katheterslot te gebruiken is voor specifieke patiëntenpopulatie (bijvoorbeeld oncologie), langdurig gebruik en frequent aanprikken (bijvoorbeeld TPV, ESPEN). In die gevallen lijkt er voor Taurolidine een toegevoegde waarde te zijn.
Onderbouwing
Achtergrond
Eén van de risico’s die het hebben van een centraal veneuze lijn (CVL) met zich meebrengt zijn katheter-gerelateerde infecties. Dit infectierisico hangt met name samen met de frequentie waarin de CVL gebruikt wordt. Daarom is er naast de juiste handhygiëne en steriel werken (zie modules infectiepreventie [in ontwikkeling]) mogelijk ook plaats voor regelmatige en lokaal toegediende antimicrobiële therapie (katheterslot) ter infectiepreventie.
Voor patiënten op de intensive care wordt verwezen naar de Richtlijn Centraal veneuze lijn van de NVIC. De aanleg van een vaattoegang voor hemodialyse valt buiten de afbakening van deze richtlijn en wordt beschreven in de richtlijn ‘Vaattoegang voor hemodialyse’.
Conclusies / Summary of Findings
Critical outcome
|
Low GRADE |
The use of antimicrobial catheter locks may reduce catheter-related bloodstream infection rate, when compared with the use of heparin or saline locks in patients with a central venous catheter.
Sources: Van den Bosch, 2022; Zhang, 2019; Carratala, 1999 |
Important outcomes
|
Very low GRADE |
The evidence is very uncertain about the effect of antimicrobial catheter locks on adverse events, when compared with heparin or saline locks in patients with a central venous catheter.
Sources: Van den Bosch, 2022; Zhang, 2019 |
|
No GRADE |
No evidence was found regarding the effect of antimicrobial catheter locks on quality of life, when compared with heparin or saline locks in patients with a central venous catheter. |
|
No GRADE |
No evidence was found regarding the effect of antimicrobial catheter locks on patient satisfaction when compared with heparin or saline locks in patients with a central venous catheter. |
|
No GRADE |
No evidence was found regarding the effect of antimicrobial catheter locks on number of catheter-related interventions per year, when compared with heparin or saline locks in patients with a central venous catheter. |
Samenvatting literatuur
Description of studies
Table 1 outlines the characteristics of the included studies.
The systematic review and meta-analysis by Van den Bosch (2022) included RCTs comparing the efficacy of taurolidine containing lock solutions (TL) to other lock solutions for the prevention of CVC-related bloodstream infections in all patient populations. Primary outcome was the pooled incidence rate ratio (IRR) comparing the efficacy of TLs to non-antibiotic lock solutions in terms of the incidence rates (IRs) of CVC-related bloodstream infections per 1000 CVC-days. Secondary outcomes were the incidence of adverse events (i.e. side-effects reported during lock replacement) and malfunction events (i.e. inability to flush and/or aspirate, thrombosis, administration of thrombolytics). A total of nine articles were included in the quantitative analysis, six of which were used in the current analysis.
The systematic review and meta-analysis by Zhang (2019) reported randomized controlled trials (RCTs) comparing ethanol lock solutions with other solutions in adults and children with a tunneled or non-tunneled central venous catheter (CVC) as vascular access, regardless of the type of disease. Solutions were allowed to dwell rather than simply being flushed through the catheter. The primary outcome was catheter related blood stream infection (CRBSI, as defined by the study author). The secondary outcomes were exit site infection (defined as the development of purulent exudates or redness around the site not resulting from residual stitches), catheter dysfunction (defined as catheter blockage or persistent inadequate flow rate), removal of the catheter (defined as removal of the catheter for any reason before the end of prophylactic treatment), catheter thrombosis (defined as thrombosis or the need for thrombolytic therapy or removal of the catheter because of thrombosis), and all-cause mortality and adverse events as reported by the study author. Incidence was presented as the number of episodes per catheter-day. Nine RCTs were included in the meta-analysis, four of which were used in the current analysis.
The systematic review by Norris focused on antimicrobial lock therapy for prevention of central-line-associated bloodstream infections in adult and pediatric cancer patients. Only one publication was in line with the PICO for the current analysis. Therefore, the original publication by Carratala (1999) was included in the analysis. This randomized, double-blind trial investigated an antibiotic-lock technique for prevention of Gram-positive central venous catheter-related infection in neutropenic patients with cancer. The trial randomized 120 hospitalized patients with a non-tunneled CVC who were to receive chemotherapy, to either a lock solution containing vancomycin and heparin or a lock solution containing heparin. The primary and secondary end points of the trial were significant colonization of the catheter hub and catheter-related bacteremia, respectively.
Table 1. Main study characteristics
|
Study |
Population |
Comparison |
N (I/C) |
Type of catheter |
No. of catheter days (I/C) |
|
Meta-analysis Van den Bosch, 2022 - taurolidine |
|||||
|
Gudiol, 2020 |
Oncology, hospitalized adults |
Taurolidine citrate heparin lock vs heparin lock |
72/69 |
Non-tunneled |
8982/6708 |
|
Longo, 2017 |
Oncology, in and outpatients |
Taurolidine citrate lock vs saline lock |
84/76 |
vascular access port |
10,000 (estimated) |
|
Wouters, 2018 |
Total parenteral nutrition, outpatients |
Taurolidine lock vs saline lock |
53/52 |
(Non)-tunneled, vascular access port |
15,318/12,493 |
|
Tribler, 2017 |
Total parenteral nutrition, outpatients |
Taurolidine citrate heparin lock vs heparin lock |
20/21 |
Tunneled |
9622/6956 |
|
Klek, 2015 |
Total parenteral nutrition, outpatients |
Taurolidine citrate lock, taurolidine lock vs saline lock |
10/10 |
Tunneled |
3658, 3650 / 3660 |
|
Bisseling, 2010 |
Total parenteral nutrition, outpatients |
Taurolidine lock vs heparin lock |
16/14 |
Tunneled, vascular access port |
5370/4939 |
|
Meta-analysis Zhang, 2019 - ethanol |
|||||
|
Sanders, 2008 |
Hematology, New Zealand |
70% ethanol lock vs heparin lock |
34/30 |
Tunneled |
5000/3537 |
|
Slobbe, 2010 |
Hematology, the Netherlands |
70% ethanol lock vs 0.9% NaCl lock |
376 |
Tunneled |
14262/13483 |
|
Worth, 2014 |
Hematology, Australia |
70% ethanol lock vs heparin lock |
42/43 |
Tunneled |
2216/2657 |
|
Salonen 2017 |
Parenteral nutrition, USA |
70% ethanol lock vs heparin lock |
18/20 |
Not reported |
2597/ 3125 |
|
Additional RCTs - antibiotic |
|||||
|
Carratala, 1999 |
Neutropenic cancer, 88% leukemia, Spain |
Vancomycin plus heparin lock vs heparin lock |
60/57 |
Non-tunneled |
Not reported |
Results
Infection rate
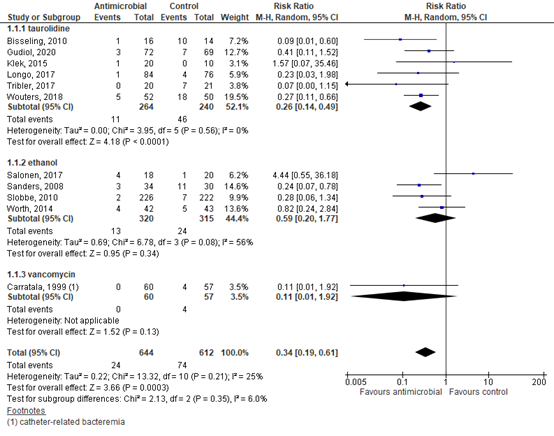
Both systematic reviews (Van den Bosch, 2022 and Zhang, 2019) considered catheter-related bloodstream infection (CRBSI) per 1000 catheter days as the primary outcome. In the current analysis, CRBSI is expressed per patient. As outlined in figure 1, CRBSI occurred in 5/264 (1.9%) patients receiving a taurolidine lock versus 18/240 (7.5%) in patients with a heparin or saline lock. This resulted in a pooled relative risk (RR) of 0.26 in favour of the antimicrobial lock, with a 95% confidence interval (CI) from 0.14 to 0.49.
In the comparison between ethanol locks and heparin or saline locks, 4/320 (1.3%) patients in the ethanol group developed CRBSI versus 5/315 (1.6%) in the control group. The pooled RR was 0.59 with a 95% CI from 0.20 to 1.77.
Carratala (1999) reported 0/60 (0%) cases of catheter-related bacteremia in patients with a vancomycin catheter lock, versus 4/57 (7%) in the control group. Taken together, the overall occurrence of CRBSI was 24/644 (3.7%) in patients with an antimicrobial catheter lock versus 74/612 (12.1%) in patients with a control lock solution, with a RR of 0.34 (95% CI 0.19 to 0.61). The difference was considered clinically relevant.
Figure 1. Catheter-related bloodstream infection
Random effects model; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval; Z: p-value of pooled effect
Adverse events
In the comparison between taurolidine and control locks, Bisseling, Gudiol and Klek reported no adverse events in either group. Wouters reported adverse events in 32/60 patients (53%) in the taurolidine group versus 39/75 (52%) in the saline group. Salonen reported no adverse events in either group in the comparison between ethanol and control locks. Other studies did not report the incidence of adverse effect on the patient level.
Quality of life
The outcome was not reported in the included literature.
Patient satisfaction
The outcome was not reported in the included literature.
Number of catheter-related interventions per year
The outcome was not reported in the included literature.
Level of evidence of the literature
The level of evidence for all outcome measures was based on randomized controlled trials and therefore started at high. The level of evidence regarding the outcome measure infection rate was downgraded by two levels to LOW because of study limitations (risk of bias because previous CVC-related bloodstream infections or not newly inserted CVCs were included, the comparator lock was not described, and/or the CVC-related infection definition was inappropriate, -1) and conflicting results (inconsistency, -1).
The level of evidence regarding the outcome measure adverse events was downgraded to VERY LOW because of study limitations (risk of bias because previous CVC-related bloodstream infections or not newly inserted CVCs were included, the comparator lock was not described, and/or the CVC-related infection definition was inappropriate, -1) and the very low number of events (imprecision, -2).
For the outcome measures quality of life, patient satisfaction and number of catheter-related interventions per year, the level of evidence could not be determined due to a lack of data.
Zoeken en selecteren
A systematic review of the literature was performed to answer the following question:
What are the benefits and harms of antimicrobial catheter locks compared to catheter locks without antimicrobial properties for patients with a central venous access?
| P: |
Adult patients receiving or having a central venous line for longer than 14 days |
| I: |
Antimicrobial catheter lock |
| C: |
Non-antimicrobial catheter lock |
| O: |
Catheter-related infection rate, quality of life, patient satisfaction, number of catheter-related interventions per year, antibiotic resistance, adverse events |
Relevant outcome measures
The guideline development group considered catheter-related infection rate (catheter-related bloodstream infection (CRBSI), central line-associated bloodstream infections (CLABSI), catheter-related exit-site infection, tunnel infection) as a critical outcome measure for decision making; and quality of life, patient satisfaction, number of catheter-related interventions per year, antibiotic resistance and adverse events as an important outcome measure for decision making.
The working group did not define the outcome measures listed above a priori, but followed the definitions used in the studies.
The working group defined 25% as a minimal clinically (patient) important difference for risk ratios (RR<0.8 or >1.25) and 10% of the maximum score for quality of life and patient satisfaction.
Search and select (Methods)
On the 6th of September 2022, relevant search terms were used to search for systematic reviews and RCTs about the value of antibiotic prophylaxis for patients receiving a central venous line in the databases Embase.com and Ovid/Medline. The detailed search strategy is depicted under the Methods tab. The search resulted in 456 unique hits. Studies were selected based on the following criteria: randomized controlled trials or a meta-analysis thereof comparing any antimicrobial catheter lock versus another type of catheter lock in adult patients with a central venous catheter. Pediatric populations and hemodialysis catheter studies were excluded. Based on title and abstract screening, 15 studies were initially included. After reading the full text, 12 studies were excluded (see the table with reasons for exclusion under the tab Methods), and 3 studies were included.
Results
Three systematic reviews were included in the analysis of the literature. One systematic review only reported one RCT in line with the PICO, so the original publication was used. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
Referenties
- Lafuente Cabrero E, Terradas Robledo R, Civit Cuñado A, García Sardelli D, Hidalgo López C, Giro Formatger D, Lacueva Perez L, Esquinas López C, Tortosa Moreno A. Risk factors of catheter- associated bloodstream infection: Systematic review and meta-analysis. PLoS One. 2023 Mar 23;18(3):e0282290. doi: 10.1371/journal.pone.0282290. PMID: 36952393; PMCID: PMC10035840.
- Carratalà J, Niubó J, Fernández-Sevilla A, Juvé E, Castellsagué X, Berlanga J, Liñares J, Gudiol F. Randomized, double-blind trial of an antibiotic-lock technique for prevention of gram-positive central venous catheter-related infection in neutropenic patients with cancer. Antimicrob Agents Chemother. 1999 Sep;43(9):2200-4. doi: 10.1128/AAC.43.9.2200. PMID: 10471564; PMCID: PMC89446.
- Huang H, Chang Q, Zhou Y, Liao L. Risk factors of central catheter bloodstream infections in intensive care units: A systematic review and meta-analysis. PLoS One. 2024 Apr 23;19(4):e0296723. doi: 10.1371/journal.pone.0296723. PMID: 38652718; PMCID: PMC11037535.
- Pironi L, Arends J, Bozzetti F, Cuerda C, Gillanders L, Jeppesen PB, Joly F, Kelly D, Lal S, Staun M, Szczepanek K, Van Gossum A, Wanten G, Schneider SM; Home Artificial Nutrition & Chronic Intestinal Failure Special Interest Group of ESPEN. ESPEN guidelines on chronic intestinal failure in adults. Clin Nutr. 2016 Apr;35(2):247-307. doi: 10.1016/j.clnu.2016.01.020. Epub 2016 Feb 8. Erratum in: Clin Nutr. 2017 Apr;36(2):619. PMID: 26944585.
- RIVM. PREventie van ZIEkenhuisinfectie door Surveillance (PREZIES). https://www.rivm.nl/prezies. Geraadpleegd december 2022.
- van den Bosch CH, Jeremiasse B, van der Bruggen JT, Frakking FNJ, Loeffen YGT, van de Ven CP, van der Steeg AFW, Fiocco MF, van de Wetering MD, Wijnen MHWA. The efficacy of taurolidine containing lock solutions for the prevention of central-venous-catheter-related bloodstream infections: a systematic review and meta-analysis. J Hosp Infect. 2022 May;123:143-155. doi: 10.1016/j.jhin.2021.10.022. Epub 2021 Nov 9. PMID: 34767871.
- Zhang J, Wang B, Wang J, Yang Q. Ethanol locks for the prevention of catheter-related infection in patients with central venous catheter: A systematic review and meta-analysis of randomized controlled trials. PLoS One. 2019 Sep 12;14(9):e0222408. doi: 10.1371/journal.pone.0222408. PMID: 31513652; PMCID: PMC6742384.
Evidence tabellen
Systematic review(s)
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Van den Bosch, 2022
Study characteristics and results are extracted from the SR, unless stated otherwise |
SR and meta-analysis of RCTs
Literature search up to 15 February 2021
A: Gudiol, 2020 B: Longo, 2017 C: Wouters, 2018 D: Tribler, 2017 E: Klek, 2015 F: Bisseling, 2010
Study design: RCT, double blind or open, parallel groups.
Setting and Country: Not specified per study
Source of funding and conflicts of interest: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Conflict of interest statement: None. |
Inclusion criteria SR: original RCTs comparing the efficacy of TLs with any other lock solution for the prevention of CVC-related bloodstream infections in all patient populations were included.
Exclusion criteria SR: non-RCTs, studies describing <10 patients and studies using TLs as treatment instead of prevention.
9 studies included, 6 of which in current analysis
Important patient characteristics at baseline:
N, mean age (I/C) A: 141, 56/57 B: 160, 62/61 C: 105, 59-47/55-47 D: 41, 56/58 E: 30, 44/46 F: 30, 55/49
Sex: Not reported
CVC type: A: Non-tunnelled B: VAP C: (Non)-tunnelled, VAP D: Tunnelled E: Tunnelled F: Tunnelled, VAP
Population: A: Oncology B: Oncology C: Total parenteral nutrition D: Total parenteral nutrition E: Total parenteral nutrition F: Total parenteral nutrition
Groups were comparable at baseline |
Taurolidine containing lock
A: Taurolidine 1.35%, Citrate 4% Heparin 100 IU/mL 2.5 mL 3x/week B: Taurolidine 1.35% Citrate 4%; 3.0 mL after use C: Taurolidine 2%; 5.0 mL 2-7x/week D: Taurolidine 1.35% Citrate 4% Heparin 100 IU/mL; 2.0-4.0 mL 2-7x/week E: Taurolidine 2% and Taurolidine 1.35%, Citrate 4%; dose and frequency not specified F: Taurolidine 2%; 5.0 mL, frequency not specified
|
Citrate/heparin/saline lock
A: Heparin 100 IU/mL B: Saline 0.9% C: Saline 0.9% D: Heparin 100 IU/mL E: Saline 0.9% F: Heparin 150 IU/mL
|
End-point of follow-up: Not specified
For how many participants were no complete outcome data available? (intervention/control) Not specified
|
Infection events (primary outcome) A: I 2/719; C 1/690 IRR 1.92 (0.18, 20.66), p=1.00 B: 1/10000; C 4/10000 IRR 0.23 (0.03, 2.06), p=0.21 C: I 5/15318; C 18/12493 IRR 0.23 (0.07, 0.63), P<0.01 D: I 0/9622; C 7/6956 IRR N/A E: I1 0/3658, I2 1/3650; C 0/3660 IRR N/A F: I 1/5370; C 10/4939
Infection per patient (data from original publications) A: I 3/72 (4.1%); C 7/69 (10.1%) B: TIVAP-BSI: I 1/84 (1%); C 4/76 (5%) C: I 5/52; C 18/50 D: I 0/20; C 7/21 E: tauro: 0/10; tauro+citr 1/10 (10%); C 0/10 F: I 1/16 (6%); C 10/14 (71%)
Quality of life Not reported
Patient satisfaction Not reported
Number of catheter-related interventions per year Not reported
Antibiotic resistance Not reported
Adverse events Number of patients when reported, otherwise number of events A: I 0/72; C 0/69 B: I Local paresthesia (9), body warm sensation (4), unpleasant taste (1), pain (1); C not specified C: I Unpleasant taste (1), dizziness (1), erhythema exit-site (1); C Flushing (1) D: I Unpleasant taste (8), paresthesia (3), nausea/ vomiting (2); C Heartburn/acid reflux (1), paresthesia (1), dizziness (1) E: I 0/10; C 0/10 F: I 0/16; C 0/14 |
Authors’ conclusions The use of TLs might be promising for the prevention of CVC-related bloodstream infections. Large-scale RCTs are needed to draw firm conclusions on the efficacy of TLs.
VAP: vascular access port |
|
Zhang, 2019
PROSPERO registration number CRD42015027833
Study characteristics and results are extracted from the SR, unless stated otherwise |
SR and meta-analysis of RCTs
Literature search up to March, 2018
A: Salonen, 2017 B: Sanders, 2008 C: Slobbe, 2010 D: Worth, 2014
Study design: A: prospective double blind randomized controlled study B: prospective double-blind randomized trial C: randomized, placebo-controlled trial D: randomized trial
Setting and country: A: USA B: New Zealand C: the Netherlands D: Australia
Setting was not reported in SR
Source of funding and conflicts of interest: The authors received no specific funding for this work. There was no additional external funding received for this study.
The authors have declared that no competing interests exist. |
Inclusion criteria SR: Adults and children with a tunneled or nontunneled CVC as vascular access, regardless of the type of disease; Ethanol lock solutions were used in the intervention group. Solutions were allowed to dwell rather than simply being flushed through the catheter. A control condition (e.g., heparin locks) was used in the control group.
Exclusion criteria SR: Overlapping study populations, non-RCTs, unavailable full-text.
9 studies included in meta-analysis, 4 of which relevant for current analysis.
Important patient characteristics at baseline:
N, population A: 38, parenteral nutrition B: 64, hematology C: 376, hematology D: 85, hematology Sex and age not reported in SR
Catheter type: A: not reported B: tunneled C: tunneled D: tunneled
Insertion site A: not reported B: Subclavian veins C: Internal jugular vein, subclavian vein, femoral vein D: Subclavian, internal jugular veins
Groups were comparable at baseline. |
Ethanol lock
A: Ethanol 70% Patients flushed their catheters with 10 ml 0.9% NaCl after completion of their parenteral nutrition and then locked the catheter with 3 ml 70% ethanol. Prior to administration of the next bag of parenteral nutrition, they again flushed their catheters with 10 mL 0.9% NaCl. B: Ethanol 70% Three milliliters of 70% ethanol was injected into each lumen of the catheter daily and left for 2 hours before being entirely removed and replaced with heparinized saline. C: Ethanol 70% During hospitalization, every lumen of the CVC was locked with 3 ml 70% ethanol for 15 minutes per day, following which the solution was flushed through with 10 ml 0.9% NaCl. During outpatient settings, ethanol locks were administered once weekly before the replacement of the regular heparin solution. D: Ethanol 70% After flushing CVC lumens with 10 ml 0.9% NaCl, 2 ml 70% ethanol was instilled into each CVC lumen daily for inpatients and left in situ for 2 hours. A 5- to 10-ml aliquot was then aspirated from each lumen before locking under positive pressure with 10 mL 0.9% NaCl. Self-caring outpatients were instructed to administer the ethanol lock three times weekly, with 2 hours dwell time.
|
Control lock
A: heparin B: heparin C: 0.9% NaCl D: heparin
|
End-point of follow-up: Not specified in SR
For how many participants were no complete outcome data available? Not specified in SR
|
Catheter-related bloodstream infection (primary outcome) CRBSI (as defined by the study author) per 1000 catheter days heparin A: I 4/2597; C 1/3125 OR 4.82 (0.54, 43.14) B: I 3/5000; C 11/3537 OR 0.19 (0.05, 0.69) D: I 4/2216; C 5/2657 OR 0.96 (0.26, 3.58)
NaCl C: I 10/14262; C 16/13483 OR 0.59 (0.27, 1.30)
CRBSI (as defined by the study author) per patient heparin A: I 4/18; C 1/20 OR 5.43 (0.55, 54.01) B: I 3/34; 11/30 OR 0.17 (0.04, 0.68) D: I 4/42; C 5/43 OR 0.80 (0.20, 3.21)
NaCl C*: I 2/226; C 7/222 *retrieved from original publication
Exit site infection per 1000 catheter days heparin A: not reported B: I 2/5000; C 1/3537 C: not reported D: I 2/2216; C 3/2657
Quality of life Not reported
Patient satisfaction Not reported
Number of catheter-related interventions per year Not reported
Antibiotic resistance Not applicable for this intervention
Adverse events Not reported at patient level A: No adverse events in either group B: I: Dyspnea immediately after the first treatment (n = 1); C Unusual taste sensation and anxiety (n = 1) C: I: Facial flushing (n = 39); nausea/vomiting (n = 20); altered taste (n = 31); dizziness/ drowsiness (n = 41); syncope shortly after the first treatment (n = 1); C: Facial flushing (n = 17); nausea/vomiting (n = 17); altered taste (n = 19); dizziness/ drowsiness (n = 10) D: I: Chest discomfort (3); nausea (n = 1); C: No adverse events. |
Authors’ conclusions
The present data indicate that ethanol lock prophylaxis is a potential candidate for the prevention of CRBSI in patients with CVC. However, more attention should be paid to the uniform ethanol lock procedure and toxic effects after long-term ethanol lock exposure. |
Randomized controlled trial(s)
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Carratala, 1999 |
Type of study: RCT
Setting and country: Single center, Spain
Funding and conflicts of interest: This study was supported in part by grant 93/1081 from Fondo de Investigacio´n Sanitaria, Madrid, Spain. No conflict of interest statement. |
Inclusion criteria: Hospitalized patients with a nontunneled, multilumen, polyurethane CVC in place and who were to receive chemotherapy designed to produce severe neutropenia were eligible for participation in the trial
Exclusion criteria: Patients were excluded if they had clinical or microbiologic evidence of infection or had a known allergy to vancomycin. Patients already receiving antibiotics or parenteral nutrition were also excluded.
N total at baseline: Intervention: 60 Control: 60
Important prognostic factors2: Age, mean ± SD: I: 42 C: 44
Sex: I: 51.7% M C: 68.4% M
Type of catheter Double lumen I: 66.7% C: 61.4& Triple lumen I: 33.3% C: 38.6%
Duration of catheterization prior to randomization (days) I: 25 C: 24
Groups were comparable at baseline. |
Lock solution containing heparin at 10 U/ml and vancomycin at 25 mg/ml.
|
Lock solution containing heparin at 10 U/ml
Catheters were inserted into the subclavian vein by physicians who wore masks, caps, sterile gloves, and surgical gowns and who used large sterile drapes. Study catheters were not exchanged over guidewires. At the time of catheter insertion, the skin insertion site was disinfected with 4% chlorhexidine gluconate (Hibiscrub; ICI Farma, Pontevedra, Spain), which was applied by scrubbing for at least 30 s. The insertion sites were covered with sterile gauze. |
Length of follow-up: 28 days
Loss-to-follow-up: Intervention: 0/60 (0%)
Control: 0/57 (0%)
Incomplete outcome data: Not specified.
|
Catheter infection Significant colonization of catheter hub (primary outcome) I: 0/60 (0%) C: 9/57 (15.8%) P=0.001
Catheter-related bacteremia I: 0/60 (0%) C: 4/57 (7.0%) P=0.05
Quality of life Not reported
Patient satisfaction Not reported
Number of catheter-related interventions per year Not reported
Antibiotic resistance No vancomycin-resistant organism was isolated from any source during the study period
Adverse events Not reported
|
Authors’ conclusions:
Our study shows that a solution containing heparin and vancomycin administered by using an antibiotic-lock technique effectively prevents catheter hub colonization with gram-positive bacteria and subsequent bacteremia during chemotherapy-induced neutropenia in patients with hematologic malignancy. |
Risk of bias table
Systematic review(s)
|
Study
First author, year |
Appropriate and clearly focused question?1
Yes/no/unclear |
Comprehensive and systematic literature search?2
Yes/no/unclear |
Description of included and excluded studies?3
Yes/no/unclear |
Description of relevant characteristics of included studies?4
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?5
Yes/no/unclear/not applicable |
Assessment of scientific quality of included studies?6
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?7
Yes/no/unclear |
Potential risk of publication bias taken into account?8
Yes/no/unclear |
Potential conflicts of interest reported?9
Yes/no/unclear |
|
Zhang, 2019 |
Yes |
Yes |
No Excluded studies were not.described. |
Yes |
N/A |
Yes |
Yes |
No |
Unclear Not specified for included studies |
|
Van den Bosch, 2022 |
Yes |
Yes |
No Excluded studies were not.described. |
Yes |
N/A |
Yes |
Yes |
Yes |
Unclear Not specified for included studies |
Randomized controlled trial(s)
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Were patients blinded?
Were healthcare providers blinded?
Were data collectors blinded?
Were outcome assessors blinded?
Were data analysts blinded?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Carratala, 1999 |
Definitely yes;
Reason: For study solution allocation a computer-generated list of random numbers, which was available only to the pharmacist, was used. |
Definitely yes;
Reason: The two solutions were indistinguishable to medical personnel and were dispensed in 20-ml vials that were numerically coded and that were kept refrigerated. The code list was kept in the hospital pharmacy and was opened only after the study was completed. |
Definitely yes;
Reason: The patients’ physicians and nurses, the clinical investigators, and the research microbiologists who processed all cultures were blinded to each study group. |
Probably yes;
Reason: Loss to follow-up was infrequent. |
Probably yes;
Reason: All relevant outcomes were reported. |
Probably yes;
Reason: No other problems noted. |
LOW |
Exclusie tabel
|
Reference |
Reason for exclusion |
|
Dang FP, Li HJ, Wang RJ, Wu Q, Chen H, Ren JJ, Tian JH. Comparative efficacy of various antimicrobial lock solutions for preventing catheter-related bloodstream infections: A network meta-analysis of 9099 patients from 52 randomized controlled trials. Int J Infect Dis. 2019 Oct;87:154-165. doi: 10.1016/j.ijid.2019.08.017. Epub 2019 Aug 20. PMID: 31442627. |
wrong P: includes hemodialysis |
|
Gudiol C, Arnan M, Aguilar-Guisado M, Royo-Cebrecos C, Sánchez-Ortega I, Montero I, Martín-Gandul C, Laporte-Amargós J, Albasanz-Puig A, Nicolae S, Perayre M, Berbel D, Tebe C, Riera J, Sureda A, Cisneros JM, Carratalà J. A Randomized, Double-Blind, Placebo-Controlled Trial (TAURCAT Study) of Citrate Lock Solution for Prevention of Endoluminal Central Venous Catheter Infection in Neutropenic Hematological Patients. Antimicrob Agents Chemother. 2020 Jan 27;64(2):e01521-19. doi: 10.1128/AAC.01521-19. PMID: 31712211; PMCID: PMC6985755. |
Reported in systematic review |
|
Gudiol C, Nicolae S, Royo-Cebrecos C, Aguilar-Guisado M, Montero I, Martín-Gandul C, Perayre M, Berbel D, Encuentra M, Arnan M, Cisneros-Herreros JM, Carratalà J. Administration of taurolidine-citrate lock solution for prevention of central venous catheter infection in adult neutropenic haematological patients: a randomised, double-blinded, placebo-controlled trial (TAURCAT). Trials. 2018 May 2;19(1):264. doi: 10.1186/s13063-018-2647-y. PMID: 29720244; PMCID: PMC5932813. |
Wrong study design: protocol |
|
Longo R, Llorens M, Goetz C, Platini C, Eid N, Sellies J, Ouamara N, Quétin P. Taurolidine/Citrate Lock Therapy for Primary Prevention of Catheter-Related Infections in Cancer Patients: Results of a Prospective, Randomized, Phase IV Trial (ATAPAC). Oncology. 2017;93(2):99-105. doi: 10.1159/000470911. Epub 2017 May 3. PMID: 28463827. |
Reported in systematic review |
|
Norris LB, Kablaoui F, Brilhart MK, Bookstaver PB. Systematic review of antimicrobial lock therapy for prevention of central-line-associated bloodstream infections in adult and pediatric cancer patients. Int J Antimicrob Agents. 2017 Sep;50(3):308-317. doi: 10.1016/j.ijantimicag.2017.06.013. Epub 2017 Jul 6. PMID: 28689878. |
Original publication used |
|
Reitzel RA, Rosenblatt J, Chaftari AM, Raad II. Epidemiology of Infectious and Noninfectious Catheter Complications in Patients Receiving Home Parenteral Nutrition: A Systematic Review and Meta-Analysis. JPEN J Parenter Enteral Nutr. 2019 Sep;43(7):832-851. doi: 10.1002/jpen.1609. Epub 2019 Jun 6. PMID: 31172542. |
wrong study design, only observational data |
|
Salonen BR, Bonnes SL, Vallumsetla N, Varayil JE, Mundi MS, Hurt RT. A prospective double blind randomized controlled study on the use of ethanol locks in HPN patients. Clin Nutr. 2018 Aug;37(4):1181-1185. doi: 10.1016/j.clnu.2017.05.009. Epub 2017 May 17. PMID: 28576557. |
Reported in systematic review |
|
Taşdelen Öğülmen D, Ateş S. Use of alcohol containing caps for preventing bloodstream infections: A randomized controlled trial. J Vasc Access. 2021 Nov;22(6):920-925. doi: 10.1177/1129729820952961. Epub 2020 Aug 27. PMID: 32854563. |
Wrong intervention |
|
van de Wetering MD, van Woensel JB, Lawrie TA. Prophylactic antibiotics for preventing Gram positive infections associated with long-term central venous catheters in oncology patients. Cochrane Database Syst Rev. 2013 Nov 25;2013(11):CD003295. doi: 10.1002/14651858.CD003295.pub3. Update in: Cochrane Database Syst Rev. 2021 Oct 7;10:CD003295. PMID: 24277633; PMCID: PMC6457614. |
more recent systematic review used |
|
Vassallo M, Dunais B, Roger PM. Antimicrobial lock therapy in central-line associated bloodstream infections: a systematic review. Infection. 2015 Aug;43(4):389-98. doi: 10.1007/s15010-015-0738-1. Epub 2015 Feb 6. PMID: 25657033. |
no usable data in article |
|
Vernon-Roberts A, Lopez RN, Frampton CM, Day AS. Meta-analysis of the efficacy of taurolidine in reducing catheter-related bloodstream infections for patients receiving parenteral nutrition. JPEN J Parenter Enteral Nutr. 2022 Sep;46(7):1535-1552. doi: 10.1002/jpen.2363. Epub 2022 Mar 25. PMID: 35233792. |
more complete systematic review used |
|
Worth LJ, Slavin MA, Heath S, Szer J, Grigg AP. Ethanol versus heparin locks for the prevention of central venous catheter-associated bloodstream infections: a randomized trial in adult haematology patients with Hickman devices. J Hosp Infect. 2014 Sep;88(1):48-51. doi: 10.1016/j.jhin.2014.06.007. Epub 2014 Jul 2. PMID: 25063013. |
Reported in systematic review |
|
Zacharioudakis IM, Zervou FN, Arvanitis M, Ziakas PD, Mermel LA, Mylonakis E. Antimicrobial lock solutions as a method to prevent central line-associated bloodstream infections: a meta-analysis of randomized controlled trials. Clin Infect Dis. 2014 Dec 15;59(12):1741-9. doi: 10.1093/cid/ciu671. Epub 2014 Aug 25. PMID: 25156111. |
more complete systematic review used |
Verantwoording
Beoordelingsdatum en geldigheid
Publicatiedatum : 25-06-2025
Beoordeeld op geldigheid : 25-06-2025
Nog in afwachting autorisatie van de volgende partijen:
- Vereniging voor Hygiëne en Infectiepreventie in de Gezondheidszorg
- Patiëntenfederatie Nederland
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg rondom vaattoegangswegchirurgie.
Werkgroep
- dr. C.G. (Niels) Vos (voorzitter), Nederlandse Vereniging voor Heelkunde
- dr. M.E. (Marianne) Sitsen (vice-voorzitter), Nederlandse Vereniging voor Anesthesiologie
- dr. M.J. (Marijke) Molegraaf, Nederlandse Vereniging voor Heelkunde
- dr. M.G.J. (Maarten) Snoeijs, Nederlandse Vereniging voor Heelkunde
- dr. M. (Mahir) Uslu, Nederlandse Vereniging voor Anesthesiologie
- dr. M. (Michelle) Gompelman, Nederlandse Internisten Vereniging
- dr. E.R. (Eric) van der Vorm, Nederlandse Vereniging voor Medische Microbiologie / Samenwerkingsverband Richtlijnen Infectiepreventie
- drs. Ir. P.A.A. (Pum) Le Haen, Nederlandse Vereniging voor Radiologie
Klankbordgroep
- dr. H. (Hanneke) Buter, Nederlandse Vereniging voor Intensive Care
- Werkgroep SRI-richtlijn Veneuze en arteriële katheters
Met ondersteuning van
- dr. M.S. (Matthijs) Ruiter, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- M. (Mitchel) Griekspoor, MSc, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Hoofdfunctie |
Project Tekstveld |
Nevenwerkzaamheden |
Persoonlijke Financiële belangen |
Persoonlijke relaties |
Extern gefinancierd onderzoek |
Intell. Belangen en reputatie |
Overige belangen |
Ondernomen actie |
|
Niels Vos (vz.) |
Vaatchirurg |
Richtlijn Centraal Veneuze Toegang |
Voorzitter huidige richtlijncommissie. |
Geen. |
Geen. |
1. Studie naar functioneren van Artivion (Jotec) EVAR prothese. Gefinancierd door Artivion. Multicenter, ik ben lokale (martini ziekenhuis) hoofdonderzoeker. Het ziekenhuis krijgt een onkosten vergoeding van een paar 100 euro. Persoonlijk krijg ik er niets voor. Het is een reguliere verkrijgbare stent waar de leverancier wilde kijken hoe deze presteert (technisch/klinisch en QoL).
2.Door ZonMW gefinancierde multicenter trial naar antistolling na pta (CLEARPATH trial, RCT, clopidogrel / placebo vs clopidogrel / ascal na dotter). Hier is een onkostenvergoeding per patiënt voor die naar het ziekenhuis (wetenschappelijk instituut) gaat. Ik ben ook hier lokale hoofdonderzoeker.
|
Geen. |
Geen. |
Geen restricties. Extern gefinancierd onderzoek valt buiten bestek van de richtlijn. |
|
Eric van der Vorm |
Arts-microbioloog |
Richtlijn Centraal Veneuze Toegang |
Geen. |
Geen. |
Geen. |
Geen. |
Geen. |
Geen. |
Geen restricties. |
|
Maarten Snoeijs |
Vaatchirurg |
Centraal Veneuze Toegang & Cluster expertisegroep Arteriële en Veneuze Pathologie. |
Geen. |
Geen. |
Geen. |
1. OASIS Zorgevaluatie (Zorgevaluatie Nederland) 2. FLOW Zorgevaluatie (ZonMw) 3. Personalised hemodynamic modeling of arteriovenous grafts for prediction of vascular access stenosis and thrombosis (Vascular Access Society research grant) 4. ShuntSimulationStudy (Nierstichting).
|
Leider expertisecentrum met topreferente zorgfunctie voor vaattoegangchirurgie in MUMC+ |
Geen. |
Geen restricties. Extern gefinancierd onderzoek valt buiten bestek van de richtlijn. |
|
Mahir Uslu |
Anesthesioloog |
Richtlijn Centraal Veneuze Toegang
|
Geen. |
Geen. |
Geen. |
Geen. |
Geen. |
Geen. |
Geen restricties. |
|
Marianne Elisabeth Sitsen |
Anesthesioloog en medisch manager OK centrum |
Richtlijn Centraal Veneuze Toegang |
Geen. |
Geen. |
Geen. |
Geen. |
Geen. |
Geen. |
Geen restricties. |
|
Marijke Molegraaf |
Vaatchirurg |
Richtlijn Centraal Veneuze Toegang
|
Geen. |
Geen. |
Geen. |
Geen. |
Geen. |
Geen. |
Geen restricties. |
|
Michelle Gompelman |
Internist-infectioloog, Arts-onderzoeker |
Richtlijn Centraal Veneuze Toegang |
Hoofdredactieraad lid Tijdschrift voor Infectieziekten – onbetaald. |
Geen. |
Geen. |
CARRIER-trial (ZonMW), Staphylococcus aureus decolonization in patients on home parenteral nutrition, geen PI. |
Geen. |
Geen. |
Geen restricties. Extern gefinancierd onderzoek valt buiten bestek van de richtlijn.
|
|
Pum le Haen |
Interventieradioloog |
Richtlijn Centraal Veneuze Toegang |
Geen. |
Geen. |
Geen. |
Lokale P.I. voor onderzoek naar de verbeterde/snellere toegang tot de AFS bij antegrade punctie van de AFC met de Speedwire. Multi center internationale studie onder P.I-schap van D. van den Heuvel, interventieradioloog St Antonius Ziekenhuis in Nieuwegein. Voor de inclusie van een patiënt in het bovengenoemde onderzoek wordt een onkostenvergoeding van 100 euro betaald. Deze vergoeding loopt via het ziekenhuis en de specialisten coöperatie en wordt betaald door Speedwire. Gaat om in totaal 20-25 patiënten in de looptijd van het onderzoek. |
Geen. |
Geen. |
Geen restricties. Extern gefinancierd onderzoek valt buiten bestek van de richtlijn. |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door uitnodigen van de Patiëntenfederatie Nederland voor de invitational conference. Het verslag hiervan is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan de deelnemers van de invitational conference en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz (Volgt na de commentaarfase)
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Module |
Uitkomst raming |
Toelichting |
|
Katheterslot |
Geen substantiële financiële gevolgen |
Hoewel uit de toetsing volgt dat de aanbevelingen breed toepasbaar zijn, betreft het geen nieuwe manier van zorgverlening of andere organisatie van zorgverlening. Er worden daarom geen substantiële financiële gevolgen verwacht. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met die een centraal veneuze lijn krijgen. Tevens zijn er knelpunten aangedragen via een invitational conference. Een verslag hiervan is opgenomen onder aanverwante producten. Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. [Review Manager 5.4] werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Algemene informatie
|
Cluster/richtlijn: Centraal Veneuze Toegang |
|
|
Uitgangsvraag/modules: Wat is de waarde van antibioticaprofylaxe bij een centraal veneuze toegang? |
|
|
Database(s): Ovid/Medline, Embase.com |
Datum: 6-9-2022 |
|
Periode: 2012-heden |
Talen: Engels, Nederlands |
|
Literatuurspecialist: Miriam van der Maten |
|
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen:
→ De opgegeven sleutelartikelen worden gevonden. → MeSH termen zijn veelal op major/focus gezet gezien de grote aantallen; de sleutelartikelen worden hiermee gevonden en relevante hits lijken de zoektermen goed, duidelijk en redelijk eenduidig te benoemen. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
188 |
170 |
251 |
|
RCT |
193 |
220 |
205 |
|
Totaal |
381 |
390 |
456 |
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#12 |
#10 OR #11 |
381 |
|
#11 |
#7 AND #9 NOT #10 = RCT |
193 |
|
#10 |
#7 AND #8 = SR |
188 |
|
#9 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
1954759 |
|
#8 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
855669 |
|
#7 |
#5 AND #6 AND ([english]/lim OR [dutch]/lim) AND [2012-2022]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
2137 |
|
#6 |
'antibiotic agent'/exp/mj OR 'antibiotic prophylaxis'/exp/mj OR antibiotic*:ti,ab,kw OR antimicrobial:ti,ab,kw OR 'vancomycin'/exp/mj OR 'taurolidine'/exp/mj OR 'heparin'/exp/mj OR taurolidin*:ti,ab,kw OR heparin*:ti,ab,kw OR 'vancomycin*':ti,ab,kw OR 'alcohol'/exp/mj OR 'alcohol':ti,ab,kw OR ethanol:ti,ab,kw OR 'citric acid'/exp/mj OR 'citric acid':ti,ab,kw OR citrate:ti,ab,kw OR ((catheter* NEAR/2 lock*):ti,ab,kw) |
1954141 |
|
#5 |
'central venous catheter'/exp/mj OR 'central venous catheterization'/exp OR ((central* NEAR/3 (venous OR vein OR intravenous) NEAR/3 (catheter* OR 'access' OR line* OR device*)):ti,ab,kw) OR 'peripherally inserted central venous catheter'/exp/mj OR ((peripheral* NEAR/3 (insert* OR catheter*)):ti,ab,kw) OR picc*:ti,ab,kw OR 'port a cath':ti,ab,kw OR 'implant* port*':ti,ab,kw OR 'implantable port system'/exp/mj OR 'total* implant*':ti,ab,kw OR tivad*:ti,ab,kw OR tivap*:ti,ab,kw OR 'tunneled central venous catheter'/exp/mj OR 'hickman catheter'/exp/mj OR hickman*:ti,ab,kw OR 'tunnel* central':ti,ab,kw OR 'nontunneled central venous catheter'/exp OR nontunnel*:ti,ab,kw OR 'non-tunnel*':ti,ab,kw OR 'subclavian vein catheter'/exp OR ((central NEAR/3 cath*):ti,ab,kw) |
47992 |
Ovid/Medline
|
# |
Searches |
Results |
|
14 |
12 or 13 |
390 |
|
13 |
(9 and 11) not 12 = RCT |
220 |
|
12 |
9 and 10 = SR |
170 |
|
11 |
exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf. |
1542846 |
|
10 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
615739 |
|
9 |
limit 8 to ((english language or dutch) and yr="2012 -Current") |
2091 |
|
8 |
7 not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) |
5100 |
|
7 |
5 and 6 |
5439 |
|
6 |
exp *Anti-Bacterial Agents/ or exp *Antibiotic Prophylaxis/ or antibiotic*.ti,ab,kf. or antimicrobial.ti,ab,kf. or exp Vancomycin/ or exp Heparin/ or exp Thiadiazines/ or taurolidin*.ti,ab,kf. or heparin*.ti,ab,kf. or 'vancomycin*'.ti,ab,kf. or exp Ethanol/ or 'alcohol'.ti,ab,kf. or ethanol.ti,ab,kf. or exp Citric Acid/ or 'citric acid'.ti,ab,kf. or citrate.ti,ab,kf. or (catheter* adj2 lock*).ti,ab,kf. |
1434059 |
|
5 |
exp *Catheterization, Central Venous/ or exp *Central Venous Catheters/ or (central* adj3 (venous or vein or intravenous) adj3 (catheter* or 'access' or line* or device*)).ti,ab,kf. or exp Catheterization, Peripheral/ or (peripheral* adj3 (insert* or catheter*)).ti,ab,kf. or PICC*.ti,ab,kf. or 'port a cath'.ti,ab,kf. or ('total* implant*' or tivad* or tivap* or hickman* or (tunnel* adj 3 central) or nontunnel* or 'non-tunnel*').ti,ab,kf. |
40914 |