Open chirurgische technieken bij hallux valgus
Uitgangsvraag
Welke chirurgische ingreep heeft de voorkeur als behandeling van patiënten met een hallux valgus?
Aanbeveling
Chirurgische correctie
Kies voor een techniek waarmee een adequate chirurgische correctie kan worden bereikt en waar voldoende ervaring mee is opgedaan.
Volg het stroomschema ‘chirurgische behandeling van hallux valgus’.
Voorkeurstechnieken
Verricht bij een milde hallux valgus bij voorkeur een chevron zonder DSTP.
Verricht bij een matige hallux valgus bij voorkeur een lange chevron of scarf.
Verricht bij een ernstige hallux valgus met sterk vergrote IMA bij voorkeur een proximale osteotomie of Lapidus.
Verricht geen proximale osteotomie of Lapidus bij een metatarsus adductus.
Verwijs patiënten met een metatarsus adductus naar een gespecialiseerde voetchirurg. Er is waarschijnlijk een grotere kans op complicaties en re-operaties.
Aanvullende technieken
Overweeg bij een toegenomen DMAA een biplane chevron of scarf met correctie van de DMAA.
Overweeg bij een hallux valgus interphalangeus een Akin osteotomie.
Verricht alleen een DSTP bij een matige of ernstige hallux valgus en een incongruent gewricht.
Zorg voor voldoende plantarisatie van het kopje en voorkom overmatig verkorten.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is literatuuronderzoek verricht naar de effectiviteit van de verschillende chirurgische technieken om hallux valgus te behandelen. Om te bepalen welke techniek voor welke situatie de voorkeur heeft, werden drie vergelijkingen gemaakt: distale versus proximale osteotomie, chevron osteotomie versus andere osteotomie en ten slotte de Lapidus techniek versus andere chirurgische behandelingen. Pijn, voetfunctie en recidive of heroperatie werden beschouwd als cruciale uitkomstmaten; complicaties, hallux valgus correctie en patiënttevredenheid werden als belangrijke uitkomstmaten beschouwd.
Bij de vergelijking tussen proximale en distale osteotomie, waar studies zijn beschreven met patiënten met matige tot ernstige hallux valgus, leek er op basis van twee gerandomiseerde studies geen verschil te zijn in pijn na de operatie. De ernst van de hallux valgus is in de verschillende studies onvoldoende duidelijk. De preoperatieve IMA varieert in de studies van 10 to 20 en van 12 to 15. Voetfunctie, bepaald met de AOFAS-score, leek niet verschillend. Recidive en heroperatie werden niet beschreven. Van de belangrijke uitkomstmaten leek patiënttevredenheid niet verschillend tussen de beide technieken. Het is onduidelijk of er een verschil is in complicaties tussen de technieken door de zeer lage bewijskracht. Het wel of niet bereiken van hallux valgus correctie werd niet beschreven in de geïncludeerde literatuur. De overall bewijskracht, de laagste bewijskracht voor de cruciale uitkomstmaten, is voor de vergelijking proximale versus. distale osteotomie zeer laag, door het ontbreken van data over recidive en heroperatie. Het is dus onduidelijk welke techniek de voorkeur heeft. Hier ligt een kennislacune.
De chevron techniek werd in de literatuur vergeleken met de scarf osteotomie, maar ook met andere technieken. Bij patiënten met matige hallux valgus, leek pijn hetzelfde na scarf en na chevron osteotomie, en bij patiënten met matige tot ernstige hallux valgus, leek de AOFAS-score ook niet verschillend tussen deze twee technieken. Recidive leek niet verschillend wanneer scarf osteotomie werd vergeleken met een “lange” chevron osteotomie bij patiënten met matige hallux valgus. Heroperatie werd voor deze vergelijking niet beschreven. Bij patiënten met matige tot ernstige hallux valgus leken pijn en AOFAS-score na proximale open wig osteotomie niet beter dan na de chevron techniek. Heroperatie binnen een jaar kwam minder vaak voor na proximale open wig osteotomie in deze studie. Recidive werd voor deze vergelijking niet beschreven. Op basis van de cruciale uitkomstmaten lijkt er dus geen duidelijke voorkeur voor chevron osteotomie ten opzichte van andere osteotomieën. De belangrijke uitkomstmaten konden verder geen richting geven aan de besluitvorming: door de zeer lage bewijskracht was het onduidelijk of er een verschil was in complicaties tussen de technieken, en valguscorrectie en patiënttevredenheid werden niet beschreven. De overall bewijskracht voor deze vergelijking is laag.
Er zijn geen studies gevonden die de Lapidus procedure vergeleken met andere technieken. Op basis van de literatuur kan er daarom geen conclusie worden getrokken. Hier ligt een kennislacune.
Er is geen sterke ondersteuning in de literatuur welke chirurgische techniek bij welke ernst van de hallux valgus verricht moet worden. De aanbevelingen zullen daarom gebaseerd worden op aanvullende argumenten waaronder expert opinion, waar mogelijk onderbouwd met (indirecte) literatuur.
De werkgroep heeft de indeling van eerdere hallux valgus richtlijn welke de ernst van de hallux valgus definieert overgenomen (Robinson, 2005). Deze indeling is gemaakt op basis van de afwijkingen op een belaste röntgenfoto. De preoperatieve intermetatarsale hoek (IMA) en hallux valgus hoek (HVA) worden gebruikt om de ernst van de hallux valgus te definiëren. Ondanks dat deze indeling in de literatuur niet op deze manier gebruikt wordt, geeft dit wel een handvat wanneer welke techniek overwogen kan worden.
- Een milde hallux valgus heeft een IMA van ≤ 13 en een HVA van ≤ 19 graden.
- Een matige hallux valgus heeft een IMA van 14 tot 20 en een HVA van 20 tot 40 graden.
- Een ernstige hallux valgus heeft een IMA van > 20 en een HVA van > 40 graden.
Een adequate vermindering van de IMA lijkt biomechanisch een logisch doel van de chirurgische correctie, met een verbetering van de deformerende krachten. Een uitzondering hierop is de metatarsus adductus, die zich kenmerkt door een kleine IMA bij een grote HVA.
Op welke wijze een adequate vermindering van de IMA wordt bereikt (chevron, scarf, Lapidus, proximale/ andere osteotomie) wordt vanuit de literatuur niet duidelijk.
De laatste jaren is door nieuwe beeldvormende technieken veel aandacht ontstaan over de rotatie van de eerste straal. Dit lijkt een belangrijke factor te zijn bij een groot deel van de hallux valgus deformiteiten. Het al dan niet corrigeren van deze rotatieafwijking bij de hallux valgus operatie lijkt een belangrijke rol te spelen bij de kans op een recidief. Er is echter onvoldoende over bekend. De werkgroep beschouwt dit als een belangrijke kennislacune. Rotatieafwijkingen van MT I kunnen niet representatief gemeten worden op de conventionele röntgenfoto’s. Een gestandaardiseerde meetmethode hiervoor is nog niet voorhanden. De klinische beoordeling speelt hierin een belangrijke rol. Ervaring van de chirurg is daarbij essentieel.
Milde hallux valgus
Bij een milde hallux valgus kan volstaan worden met een milde correctie en hiervoor lijkt de chevron techniek de meest aangewezen techniek. De meeste behandelaars hebben ervaring met deze techniek en deze techniek geeft een stabiele postoperatieve situatie met 1 schroef, welke direct belastbaar kan worden na behandeld en minder ingrijpend is voor de patiënt.
Matige hallux valgus
Bij een matige hallux valgus moet er een grotere correctie worden uitgevoerd. Hierbij zal er een osteotomie moeten worden uitgevoerd welke de metatarsaal sterker kan corrigeren. Hierbij is de lange chevron of scarf aan te bevelen, aangezien deze beide een stabiele osteotomie zijn, welke direct belastbaar kunnen worden na behandeld. Technisch is er bij de scarf de mogelijkheid het kopje iets verder op de schuiven dan bij de chevron en zou bij iets grotere IMA mogelijk een lichte voorkeur hebben, alhoewel er geen verschil tussen een lange chevron versus scarf in de literatuur kon worden aangetoond.
Indien de operateur ruime ervaring heeft met de proximale osteotomie, kan bij de grotere IMA binnen de matige hallux valgus ook gekozen worden voor deze techniek. Het nadeel van deze techniek is dat er veelal een onbelaste nabehandeling moet worden voorgeschreven. Bij een open wig osteotomie kan er bovendien een verlenging van de metatarsaal optreden, welke een stijfheid in het gewricht tot gevolg kan hebben. Daarnaast kan er door de grotere hevel bij een proximale osteotomie gemakkelijker een malunion ontstaan. Er kan bijvoorbeeld dorsiflexie in de osteotomie is ontstaan, die een transfer metatarsalgie tot gevolg kan hebben. Ook moet rekening worden gehouden met de onmogelijkheid met een proximale osteotomie de DMAA te corrigeren. Deze wordt zelfs iets negatief beïnvloed. Er zal dan ook laagdrempelig een dubbel osteotomie (dus ook een chevron met DMAA correctie) verricht moeten worden om de DMAA mede te kunnen corrigeren.
Ernstige hallux valgus
Het is aan te bevelen bij een ernstige hallux valgus met een grote IMA een techniek uit te voeren waarbij een sterke chirurgische correctie kan worden uitgevoerd (proximale osteotomie/ Lapidus/ MTP artrodese). Hierbij is het wel van belang de metatarsaal niet te verkorten of naar dorsaal te verplaatsen om postoperatieve metatarsalgie te voorkomen. Bij de Lapidus procedure en de proximale osteotomie moet ook hier rekening gehouden worden met een grote DMAA. Deze dient gecorrigeerd te worden indien vergroot door middel van een aanvullende chevron met DMAA correctie. Een MTP artrodese moet weinig dorsiflexie in de artrodese krijgen om pijn op het IP gewricht en op het kopje van MT1/ sesambeentjes te voorkomen. Aangezien de voorkeur uitgaat naar een techniek waarbij de mobiliteit van het MTP-I bewaard blijft, is de MTP artrodese met name geschikt bij hallux valgus met een MTP-I artrose of bij reuma patiënten.
Aanvullende chirurgische technieken
Aanvullend aan de basistechniek kunnen er afhankelijk van de stand van de hallux aanvullende chirurgische technieken worden gebruikt. Dit is belangrijk wanneer er sprake is van rotatie van de eerste straal of wanneer is sprake is van een toegenomen distal metatarsal articular angle (DMAA).
Indien er een toegenomen DMAA bestaat, is het raadzaam het gewricht te variseren middels een mediaal gesloten wig in de chevron (biplane chevron) of scarf, of bij de scarf het proximale deel meer naar lateraal te schuiven zodat het gewricht loodrecht op de metatarsaal komt te staan. Indien de DMAA niet gecorrigeerd wordt, zal de phalanx het naar lateraal gerichte gewricht volgen en zo kan er een vroeg recidief van de hallux valgus hoek bestaan.
Bij een hallux valgus interphalangeus kan een Akin osteotomie worden verricht. Ook kan de Akin mogelijk gebruikt worden om de correctie van de HVA van de hallux nog te versterken. Waarschijnlijk neemt de kans op recidief hiermee niet af. Mogelijk komt de flexor hallucis longus wel iets voordeliger onder het kopje van de MT1 te liggen.
Indien er een duidelijke subluxatie van het MTP-I gewricht bestaat kan een distal soft tissue procedure (DSTP) worden overwogen. Hierbij wordt de abductor van het sesambeen losgemaakt. Dit betekent dat bij een milde hallux valgus het verrichten van een DSTP wordt afgeraden. Dit laatste is belangrijk, mede gezien de klachten die patiënten ervaren na een DSTP. Om goed te kunnen schuiven kan de laterale metatarsaal goed vrij worden gemaakt zonder een laterale release te verrichten. Bedacht moet worden dat een DSTP meerdere nadelige uitkomsten kan hebben. Stijfheid van het gewricht, letsel van de nervus peroneus profundus en kopnecrose door letsel aan de vascularisatie zijn risico’s van de DSTP die voorkomen kunnen worden door niet onnodig een DSTP te verrichten.
Rotatie
De afgelopen jaren is door de belaste 3D beeldvorming veel meer inzicht gekomen in de driedimensionale deformiteit van de hallux valgus. Alhoewel op een belaste röntgenfoto de mate van rotatie van de eerste straal over het algemeen minder goed is te beoordelen, zijn er vaak een aantal aanwijzingen voor te vinden. Het zogenaamd ‘round sign’ (een ronde projectie van de laterale hoek van het MTP-I gewricht) zou een betere voorspeller zijn voor een recidief kans dan de positie van de sesamoidea (Okuda, 2007).
De mate van rotatie van het MT1 lijkt een belangrijke rol te spelen in de uitkomst van de operatie. Indien op de staande röntgenfoto een volledig ronde kop gezien wordt van het MT1 kopje (round sign), dan is er waarschijnlijk sprake van een significante rotatie van de metatarsaal (Yamaguchi, 2015). Er is een verhoogd risico op recidief bij een sterk geroteerde metatarsaal. Bij de chirurgische correctie zal er waarschijnlijk met een iets andere techniek gecorrigeerd moeten worden dan volgens de richtlijnen wordt geadviseerd vanuit IMA en HVA. Er zijn al verschillende methoden beschreven waarin een techniek voor correctie van de rotatie van de metatarsaal bij hallux valgus wordt voorgesteld. Hier kan bijvoorbeeld gedacht worden aan de proximale Dome osteotomie of een roterende Lapidus procedure. De resultaten van deze technieken zijn nog onvoldoende onderzocht, maar kunnen wellicht in de toekomst zorgen voor een reductie van de recidief kans in de geselecteerde groepen waarbij rotatie een belangrijke rol speelt (Mashima, 2009; Wagner, 2017).

Normale rotatie van de MT 1 Round sign: toegenomen rotatie van de MT 1
Subgroepen
Er worden in de literatuur geen subgroepen adequaat met elkaar vergeleken. Wel lijkt de kans op recidief bij ernstigere hallux valgus groter te zijn. Dit zou te maken kunnen hebben met een onvermogen een goede operatieve correctie te bereiken. Het is dus aan te bevelen bij patiënten met een ernstige hallux valgus peroperatief sterk te letten op een adequate correctie, onafhankelijk van de gebruikte techniek. Bij een ernstige hallux valgus is het niet aan te bevelen een chevron te verrichten, vanwege het onvermogen met deze techniek een adequate correctie uit te voeren.
Platvoet: Mogelijk is de recidief kans groter bij de groep patiënten met een pes planus en pronatie van de hallux. Mogelijk dat in de toekomst hier andere technieken voor worden ontwikkeld zoals een roterende osteotomie. Deze groep patiënten wordt vooralsnog volgens de normale indeling behandeld. Deze groep moet goed voorgelicht worden op de eventuele risico’s op recidief.
Juveniele hallux valgus: Bij een juveniele hallux valgus is er na uitvoering van een correctie waarschijnlijk een voortgaande progressie van het variseren van de metatarsaal. De werkgroep meent dat er in deze groep een verhoogde kans op een vroeg recidief aanwezig is.
Reumatoïde artritis: Bij reumatoïde artritis kan een correctie middels scarf of chevron worden overwogen. Echter bij ernstigere hallux valgus zou sneller tot een MTP artrodese moeten worden besloten om een stabiele eerste straal en een verminderd risico op recidief te bewerkstelligen.
Metatarsus Adductus: Een specifieke groep patiënten is die met een metatarsus adductus. Deze groep heeft een kleine IMA met een zeer grote HVA en heeft vaak lateralisatie van alle tenen, waarbij er na operatieve correctie een sterk verhoogde recidief kans is. Alhoewel er klinisch vaak een ernstige hallux valgus zichtbaar is, kan door de kleine IMA geen betere correctie door middel van een proximale osteotomie of een Lapidus worden verkregen dan door een distale osteotomie techniek. Het wordt in deze groep dus afgeraden een proximale osteotomie of Lapidus uit te voeren. Het is aan te bevelen deze groep patiënten naar een gespecialiseerd voetchirurg door te verwijzen vanwege de verhoogde kans op complicaties en re-operaties.
Waarden en voorkeuren van patiënten (en eventuele hun verzorgers)
Het doel van de operatieve behandeling van een hallux valgus voor de patiënt is het verminderen van de pijnklachten en het herstel van een normale functie van de eerste straal. De patiënt vindt het aanvullend van belang dat er ook een acceptabel cosmetisch resultaat is, ook al is dit primair minder belangrijk. Hierbij lijken de afwezigheid van pijn en recidief en een goede functie van het MTP-I gewricht de belangrijkste parameters. Uit de literatuur kan helaas geen goed advies gegeven worden over operatie techniek. Zowel voor pijn, recidief, voet functie scores en complicaties worden er geen duidelijk verschillen gevonden. De distale osteotomieën (chevron, scarf) zijn intrinsiek stabiel en kunnen zonder gips worden nabehandeld. Ze zijn meestal snel belastbaar. Om deze redenen zijn deze technieken in het vroege postoperatieve beloop voor de patiënt minder invaliderend en hebben ook om die reden de voorkeur bij milde tot matige hallux valgus.
Kosten (middelenbeslag)
Het kostenaspect is in de hallux valgus chirurgie van laag belang. De werkgroep meent dat de keuze van de chirurgie gebaseerd moet zijn op een adequate correctie, en niet zozeer op de kosten, welke voor de verschillende technieken niet ver uiteen liggen.
Buiten Nederland wordt ook gebruik gemaakt van niet schroefgefixeerde osteotomieën. Hoewel een niet gefixeerde osteotomie in kosten opzicht mogelijk de voorkeur heeft, wordt sterk afgeraden K-draad gefixeerde of niet gefixeerde osteotomieën te verrichten. De werkgroep meent dat er voldoende bewijs is dat een goed gefixeerde osteotomie al langere tijd de voorkeur heeft boven niet gefixeerde of met K-draad gefixeerde osteotomieën. Malunion/ verkorting van MT1 met transfermetatarsalgie komen minder voor sinds de stabiele osteotomieën met schroeffixatie hun intrede hebben gedaan.
Aanvaardbaarheid, haalbaarheid en implementatie
Alleen technieken die al routinematig in Nederland worden verricht zijn met elkaar vergeleken. Er zijn derhalve geen belemmerende factoren voor het toepassen van de technieken.
De mate van adequate chirurgische correctie is sterk afhankelijk van de ervaring van de chirurg. De chirurg zou in ieder geval voldoende ervaring moeten hebben in de hallux valgus chirurgie in het algemeen. Daarnaast is het aan te bevelen een techniek te gebruiken waarin hij/zij bedreven is en waarbij hij/zij in staat is de hallux valgus adequaat te corrigeren. De eigen ervaring met een bepaalde techniek lijkt hierin dus leidend. Bij voorkeur wordt elke hallux valgus correctie uitgevoerd door een chirurg, die ervaring heeft in de voet- en enkelchirurgie en bij voorkeur de voet-enkel chirurgie als aandachtsgebied heeft. Het lidmaatschap van de DFAS zou tot de aanbevelingen kunnen horen.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventie
Aanbeveling 1
De kans op recidief is met name afhankelijk van mate waarin een goede chirurgische correctie kan worden bereikt en dus van de ervaring van de chirurg met een bepaalde techniek. De keuze van de techniek is hier dus sterk afhankelijk van.
Aanbeveling 2
Er is in Nederland ruime ervaring met de chevron osteotomie. Deze techniek heeft de voorkeur bij milde hallux valgus. Een DSTP wordt bij een milde hallux valgus afgeraden. De DSTP heeft meerdere complicaties en is niet nodig bij een milde hallux valgus.
Bij een matige hallux valgus kan het beste gekozen voor een lange chevron of scarf. Vanwege de belaste nabehandeling en goede correctie, hebben deze technieken de voorkeur boven de proximale osteotomie. Indien met de laatste techniek ruime ervaring is, kan deze ook verricht worden bij de hogere IMA binnen deze groep.
Bij een ernstige hallux valgus moet een grote correctie worden uitgevoerd. Dit kan goed gedaan worden met een proximale osteotomie of Lapidus procedure. Een uitzondering hierop is de metatarsus adductus.
Patiënten met een platvoet of met een rotatie in de hallux hebben waarschijnlijk een hogere recidief kans. Mogelijk dat in de toekomst door beter inzicht in de bijkomende rotatie afwijking voor deze groep een betere chirurgische optie beschikbaar komt met een lager recidief percentage.
Bij een metatarsus adductus is er een grote HVA met een kleine IMA. Klinisch is er een ernstige hallux valgus met valgisatie van alle tenen. Omdat de IMA klein is, kan volstaan worden met een distale osteotomie en moet geen Lapidus of proximale osteotomie worden uitgevoerd. Voor een goede correctie wordt door de experts correctie van de overige stralen aangeraden. Wel is er een hoog risico op recidief en een hogere kans op complicaties en re-operaties. Deze groep patiënten kan beter naar een gespecialiseerd voetchirurg worden verwezen.
Aanbeveling 3
Indien er een gevalgiseerd gewricht is (vergrote DMAA) kan een biplane chevron osteotomie met varisatie van het gewricht overwogen worden. Bij een scarf osteotomie kan het proximale deel naar lateraal verplaatst worden om dit te bereiken. Hierbij moet vaak de plantaire proximale poot van de osteotomie iets worden verkort, omdat deze anders tegen de tweede straal aanligt waardoor de verplaatsing niet mogelijk is.
Bij een hallux valgus interphalangeus kan een Akin overwogen worden. De recidief kans neemt waarschijnlijk niet af. Wel ligt de pees van de flexor hallucis longus gunstiger onder het kopje.
Een DSTP heeft meerdere complicaties en zou alleen uitgevoerd moeten worden bij matige of ernstige hallux valgus indien er een incongruent gewricht bestaat.
Indien er dorsiflexie of overmatige verkorting ontstaat door de osteotomie, is er kans op transfer metatarsalgie. Plantariseren van de osteotomie en beperken van de verkorting kan dit waarschijnlijk voorkomen.
Onderbouwing
Er zijn vele operatietechnieken beschreven voor de behandeling van symptomatische hallux valgus. Het is onduidelijk wat de effectiviteit van de verschillende operatietechnieken is. Er is daarom behoefte aan een overzicht van de effectiviteit van de verschillende technieken om een indicatie te geven voor de keuze van een bepaalde operatietechniek voor een bepaalde patiënt.
1. Proximal versus distal osteotomy
|
Low GRADE |
Pain does not seem to differ after distal osteotomy compared to proximal osteotomy in patients with moderate to severe hallux valgus.
Sources: (Tsikopoulos, 2018) |
|
Low GRADE |
Foot function as determined by the AOFAS-score does not seem to differ after distal osteotomy compared to proximal osteotomy in patients with moderate to severe hallux valgus.
Sources: (Tsikopoulos, 2018) |
|
- GRADE |
It was not possible to draw conclusions or grade the level of evidence for the outcome recurrence for the comparison between proximal and distal osteotomy, due to lack of studies describing the outcome |
|
- GRADE |
It was not possible to draw conclusions or grade the level of evidence for the outcome reoperation for the comparison between proximal and distal osteotomy, due to lack of studies describing the outcome |
|
Very low GRADE |
It is unclear whether complication rate is different after proximal osteotomy compared to distal osteotomy in patients with moderate to severe hallux valgus
Sources: (Tsikopoulos, 2018) |
|
- GRADE |
It was not possible to draw conclusions or grade the level of evidence for the outcome valgus deformity correction for the comparison between proximal and distal osteotomy, due to lack of data. |
|
Low GRADE |
Patient satisfaction does not seem to differ after distal osteotomy compared to proximal osteotomy in patients with moderate to severe hallux valgus.
Sources: (Tsikopoulos, 2018) |
2. Chevron versus other osteotomy
|
Low GRADE |
Pain does not seem to be different after Scarf osteotomy compared to Chevron osteotomy in patients with mild to moderate hallux valgus.
Sources: (Klugarova, 2017) |
|
Low GRADE |
Pain does not seem to be different after proximal opening wedge osteotomy compared to Chevron osteotomy in patients with moderate to severe hallux valgus.
Sources: (Glazebrook, 2014) |
|
Low GRADE |
Foot function as determined by the AOFAS-score does not seem to be different after Scarf osteotomy compared to Chevron osteotomy in patients with moderate hallux valgus.
Sources: (Ma, 2018) |
|
Low GRADE |
Foot function as determined by the AOFAS-score does not seem to be different after proximal opening wedge osteotomy compared to Chevron osteotomy in patients with moderate to severe hallux valgus.
Sources: (Glazebrook, 2014) |
|
Low GRADE |
Recurrence does not seem to be different after Scarf osteotomy compared to a long Chevron osteotomy in patients with moderate hallux valgus.
Sources: (Elshazly, 2018) |
|
Low GRADE |
Reoperation within 1 year may be lower after proximal opening wedge osteotomy compared to Chevron osteotomy in patients with moderate to severe hallux valgus.
Sources: (Glazebrook, 2014) |
|
Very low GRADE |
It is unclear whether complication rate is different after Scarf osteotomy compared to Chevron osteotomy in patients with moderate hallux valgus.
Sources: (Elshazly, 2018; Ma, 2018) |
|
- GRADE |
It was not possible to draw conclusions or grade the level of evidence for the outcome valgus deformity correction for the comparison between Chevron and other osteotomies due to insufficient data. |
|
- GRADE |
It was not possible to draw conclusions or grade the level of evidence for the outcome patient satisfaction for the comparison between Chevron and other osteotomies due to insufficient data. |
3. Lapidus versus other technique
|
- GRADE |
It was not possible to draw conclusions or grade the level of evidence for any outcome for the comparison between Lapidus and other procedures due to lack of data. |
Description of studies
1. Proximal versus distal osteotomy
Tsikopoulos (2018) performed a systematic review and meta-analysis of clinical and radiological outcomes between proximal (PMO) versus distal metatarsal osteotomies (DMO) for moderate to severe hallux valgus deformity in adults. The review included studies that compared any type of PMO with any type of DMO. The Scarf osteotomy was not included in this systematic review as this is considered a mid-shaft rather a proximal or distal metatarsal osteotomy. In addition, the Lapidus procedure was not considered, since this is classified as an arthrodesis of the tarsometatarsal joint. Three of the 9 included studies met the PICO and were considered for the current analysis (Lee, 2015; Park, 2013; Resch, 1993).
2. Chevron versus other osteotomy
The systematic review by Ma (2018) described studies comparing Chevron osteotomy with Scarf osteotomy for hallux valgus correction. Hallux valgus angle was the main outcome. Inclusion criteria were 1) English language studies on the curative effect of Scarf osteotomy and Chevron osteotomy on patients with HV; 2) using Chevron osteotomy and Scarf osteotomy as the main treatment approach in Chevron and Scarf groups, respectively; and 3) posttreatment HVA and IMA data and AOFAS-scores as the main outcome variables in each study. The review included 4 studies with an unclear risk of bias. The 3 RCTs in this review were used for the present analysis (Deenik, 2007; Jeuken, 2016; Mahadevan, 2015). The review did not specify preoperative deformity severity. The mean preoperative HVA of study groups in the 3 studies was between 28.9 and 32.3 degrees, and preoperative IMA between 12.6 and 15.2 degrees, and are therefore considered of moderate severity.
The RCT by Elshazly (2018) compared Scarf and long ‘extended plantar limb’ Chevron osteotomies for the treatment of hallux valgus, describing power of deformity, correction, radiological results, ACFAS-score and complication rate with a follow up of 2 years. 48 consecutive patients with painful hallux valgus after failed conservative treatment for 6 months with inter-metatarsal angle (IMAs) between 10 up to 20 degrees aged 18 to 80 were included between January 2013 and January 2015. Patients with MTP arthrosis, rheumatoid arthritis, paralytic hallux valgus, patients not fit for surgery, or patients with lost follow ups were excluded. Patients with hallux interphalangeus invariably required an additional Akin osteotomy in both intervention groups. The study had an unclear risk of bias.
The systematic review by Klugarova (2017) included studies describing any type of hallux valgus surgery compared to no surgery, conservative treatment or different types of hallux valgus surgeries in adult patients, excluding adults with neurological problems causing foot deformities, for example, cerebral palsy, neuropathy, stroke, multiple sclerosis. The primary outcome was gait measurement, and secondary outcomes included quality of life, patient satisfaction, pain assessed using any validated assessment tool and adverse events. 25 studies of medium-to-poor quality were included in the review. Six of the studies were in line with the PICO and were used in the current analysis (Chuckpaiwong, 2012; Deenik, 2007; Easley, 1996; Lechler, 2012; Park, 2013; Resch, 1993). Hallux valgus severity ranged from mild to severe in the included studies.
Glazebrook (2014) compared proximal opening wedge osteotomy (with wedge-plate fixation) with proximal Chevron osteotomy and randomized 75 patients with an age of at least eighteen years; a hallux valgus angle of > 20° and an intermetatarsal angle of > 10°; and persistent, incapacitating symptoms despite nonoperative treatment (shoe-wear modification, orthotics, non-steroidal anti-inflammatory medications, and restricted activity). Patients were excluded from the study for the following reasons: degenerative arthritis of the first metatarsophalangeal joint, neuropathy, diabetes mellitus, peripheral vascular disease, previous surgery on the ipsilateral first metatarsal, hallux, or metatarsophalangeal joint, active or recent infection involving the foot, current participation in another clinical trial, a Workers’ Compensation claim, and tarsometatarsal instability diagnosed by clinical examination. The distal soft-tissue procedure was the same for both groups. Outcomes included AOFAS, patient satisfaction and pain scores, as well as HVA and IMA, with a 12-month follow up. The study had an unclear risk of bias.
3. Lapidus versus other technique
No publications were identified that compared the Lapidus procedure to another technique routinely applied in the Netherlands.
Results
1. Proximal versus distal osteotomy
Pain (critical)
When comparing proximal and distal osteotomies, Tsikopoulos (2018) described two studies that reported postoperative pain: the study of Chuckpaiwong (2012) found a difference in VAS (0 to 10) of 2.20 (95% CI from 1.76 to 2.64; N=131), and the study of Park (2013) found a difference in VAS (0 to 100) of 0.60 (95% CI from -1.12 to 2.32), both in favour of distal osteotomy. The SMD of these 2 studies is 0.87 (95% CI from -0.59 to 2.33), a large effect which is clinically relevant.
Foot function (critical)
Two studies compared function after proximal versus. distal osteotomies, as reviewed by Tsikopoulos (2018): Lee (2015) reported a difference of -0.40 (95% CI -5.21 to 4.41 in favour of proximal intervention, whereas Park (2013) reported a difference of 1.16 (95% CI -2.73 to 5.05) in favour of distal osteotomy. These differences were not clinically relevant.
Recurrence and reoperation (critical)
Recurrence and reoperation were not reported for proximal versus distal osteotomy.
Complications
The systematic review by Tsikopoulos (2018) reported the study by Park (2013) 6/54 (11%) complications for proximal, and 5/56 (9%) for distal osteotomy. The study by Resch (1993) on the other hand, found 1/43 (2%) and 11/37 (30%), respectively. Taken together, the pooled RR was 0.35 with a 95% CI from 0.02 to 6.15 with N=190 in favour of proximal osteotomy.
Valgus deformity correction
In the included literature, the ratio of patients that achieved valgus deformity correction was not described. However, postoperative HVA after proximal versus distal osteotomy was reported in 3 studies. The SMD was -0.32 in favour of proximal intervention, with a 95% CI from -0.64 to 0.01 (figure 1).
Figure 1 Postoperative HVA (degrees) after proximal versus distal osteotomy

Standardized mean difference; Mantel-Haenszel method; random effects model; CI: confidence interval; df: degrees of freedom; I2: statistical heterogeneity; Z: p-value of pooled effect. Source: Tsikopoulos, 2018
Three studies reported postoperative IMA comparing proximal and distal osteotomy. Taken together (figure 2), a moderate SMD of -0.43 (95% CI -0.70 to -0.15; N=282) was found.
Figure 2 Postoperative IMA (degrees) after proximal versus distal osteotomy

Standardized mean difference; Mantel-Haenszel method; random effects model; CI: confidence interval; df: degrees of freedom; I2: statistical heterogeneity; Z: p-value of pooled effect. Source: Tsikopoulos, 2018
Patient satisfaction
Tsikopoulos (2018) reported patient satisfaction (yes/no) in 3 studies comparing proximal and distal osteotomies, as shown in figure 3. The pooled RR was 1.01 with a 95% CI from 0.96 to 1.07 and N=283. This difference was not clinically relevant.
Figure 3 Patient satisfaction after proximal versus distal osteotomy
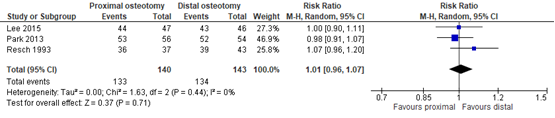
Risk ratio; Mantel-Haenszel method; random effects model; CI: confidence interval; df: degrees of freedom; I2: statistical heterogeneity; Z: p-value of pooled effect. Source: Tsikopoulos, 2018
Level of evidence of the literature
For the comparison proximal versus distal osteotomy, the level of evidence regarding all outcomes was based on randomized trials and therefore started high. For the outcomes pain, foot function, and patient satisfaction, the level of evidence was downgraded with 2 levels to low due to the limited number of included patients and because the CI crossed the clinical decision threshold (both imprecision).
For the outcome complications, level of evidence was downgraded with 3 levels to very low due to conflicting results (inconsistency), due to the limited number of events and because the CI crossed the clinical decision threshold (both imprecision).
For recurrence, reoperation and valgus deformity correction, the level of evidence could not be determined due to lack of data.
2. Chevron versus other osteotomy
Pain (critical)
Klugarova (2017) reported one RCT reporting pain (VAS 0 to 10) after Chevron versus Scarf osteotomy: the study of Lechler found a mean difference (MD) of -0.10 in favour of Chevron, with a 95% confidence interval (CI) from -0.38 to 0.18 (N=72). The study of Glazebrook (2014) reported a MD in VAS (0 to 10) of -0.90 (95% CI from -2.17 to 0.37) in Chevron compared to proximal opening wedge osteotomy (N=68). These differences were not clinically relevant.
Foot function (critical)
Foot function was reported in studies using the American Orthopedic Foot & Ankle Society (AOFAS) score. The review of Ma (2018) reported 2 studies comparing function after Chevron and Scarf osteotomies: Deenik (2007) reported a difference of -2.20 (95% CI from -7.06 to 2.66; N=96) in favour of Scarf, whereas Jeuken (2016) found a difference in favour of Chevron: 0.60 (95% CI -6.29 to 7.49; N=73). Taken together, the SMD was -0.08 (95% CI -0.39 to 0.22) in favour of Chevron, not a clinically relevant difference. Glazebrook (2014) found a higher AOFAS-score after proximal opening wedge osteotomy compared to Chevron (5.05; -3.26 to 13.36; N=68). This difference was not clinically relevant.
Recurrence and reoperation (critical)
Recurrence was described by Elshazly (2018) with a follow up of 2 years. After Scarf osteotomy, recurrence was 1/21 (4.8%) versus 1/22 (4.5%) after the long Chevron technique. The risk ratio (RR) was 0.95 (95% CI 0.06, 14.30), not a clinically relevant difference.
Reoperation within 1 year was described in 2 studies. Glazebrook (2014) reported reoperation for proximal opening wedge osteotomy 3/35 (9%) and Chevron 7/34 (21%), a clinically relevant RR of 2.40 (95% CI 0.68 to 8.53).
Complications
Complication rates for Chevron versus Scarf were described by Ma (2018) and Elshazly (2018). Based on 3 RCTs, a RR of 1.34 was found, with a 95% CI from 0.43 to 4.13 in 248 patients (figure 4).
Figure 4 Complication rate after Chevron versus Scarf
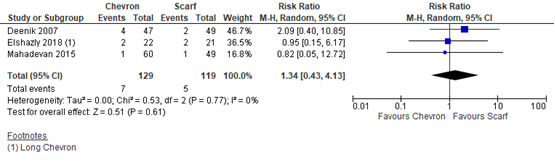
Mantel-Haenszel method; random effects model; CI: confidence interval; df: degrees of freedom; I2: statistical heterogeneity; Z: p-value of pooled effect. Sources: Elshazly, 2018; Ma, 2018
Chevron was also compared to other techniques by Klugarova (2017). One RCT (Lechler, 2012) compared distal Chevron and Chevron-akin double osteotomy. With Chevron, complication rate was 3/46 (7%), whereas with Chevron-akin no complications were reported (N=26), which gave a RR of 4.02 (95% CI 0.22 to 74.94). In the same review, the study of Easley (1996) was described, which compared proximal Chevron with proximal crescentic osteotomy, reporting a complication rate of 9/43 (21%) and 7/41 (17%), respectively (RR 1.23; 95% CI 0.50 to 2.99).
Valgus deformity correction
In the included literature, the ratio of patients that achieved valgus deformity correction was not described. However, postoperative HVA and IMA were reported in several studies. Four studies described postoperative HVA comparing Chevron and Scarf osteotomy. As depicted in figure 5, the SMD was with -0.16 with a 95% CI from -0.45 to 0.13 in favour of Chevron (N=321). This is considered a small effect. Glazebrook (2014) found a SMD of -0.19 (95% CI -0.66 to 0.28) in favour of Chevron, when compared to proximal opening wedge osteotomy.
Figure 5 Postoperative HVA (degrees) after Chevron versus Scarf
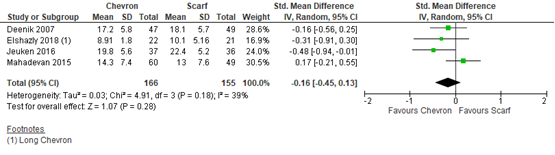
Standardized mean difference; Mantel-Haenszel method; random effects model; CI: confidence interval; df: degrees of freedom; I2: statistical heterogeneity; Z: p-value of pooled effect. Sources: Elshazly, 2018; Ma, 2018
Postoperative IMA was described in Chevron versus Scarf in 4 studies (figure 6), with a SMD of -0.13 (95% CI -0.42 to 0.16; N=321) in favour of Chevron.
Figure 6 Postoperative IMA (degrees) after Chevron versus Scarf
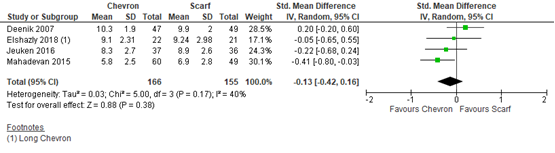
Standardized mean difference; Mantel-Haenszel method; random effects model; CI: confidence interval; df: degrees of freedom; I2: statistical heterogeneity; Z: p-value of pooled effect. Sources: Elshazly, 2018; Ma, 2018
Glazebrook (2014) found a SMD of 0.62 (0.15, 1.10) for postoperative IMA in favour of proximal opening wedge osteotomy, when compared to Chevron. Three studies reported postoperative IMA comparing proximal and distal osteotomy. Taken together (figure 7), a moderate SMD of -0.43 (95% CI -0.70 to -0.15; N=282) was found.
Figure 7 Postoperative IMA (degrees) after proximal versus distal osteotomy

Standardized mean difference; Mantel-Haenszel method; random effects model; CI: confidence interval; df: degrees of freedom; I2: statistical heterogeneity; Z: p-value of pooled effect. Source: Tsikopoulos, 2018
Patient satisfaction
One study reported the American College of Foot and Ankle Surgeons Scoring Scaling (ACFAS), a 100-point scale used to grade patient satisfaction two years after the surgery. The average ACFAS-score change in percentage was 69.1% for the long Chevron group compared to 57.5% for the Scarf group (Elshazly, 2018). There was no information provided about the distribution of the data, therefore it was not possible to grade the evidence.
Level of evidence of the literature
For the comparison Chevron versus other techniques, the level of evidence regarding all outcomes was based on randomized trials and therefore started high. For the outcomes pain, foot function, recurrence/reoperation, the level of evidence was downgraded with 2 levels to low due to the limited number of included patients and because the CI crossed the clinical decision threshold (both imprecision).
For the outcome complications, level of evidence was downgraded with 3 levels to very low due to conflicting results (inconsistency), due to the limited number of events and because the CI crossed the clinical decision threshold (both imprecision).
For patient satisfaction and valgus deformity correction, the level of evidence could not be determined due to lack of data.
3. Lapidus versus other technique
No data was found for the comparison between Lapidus technique and other procedures.
A systematic review of the literature was performed to answer the following question:
What are the (dis)advantages of the different surgical techniques to treat hallux valgus?
To make clinically meaningful comparisons, the question was split up into the following questions. Only techniques routinely used in the Netherlands were considered for analysis.
1. Proximal versus distal osteotomy
P: patients with hallux valgus;
I: distal osteotomy;
C: proximal osteotomy;
O: pain, foot function, recurrence/reoperation, complications (infection, delayed union), valgus deformity correction, patient satisfaction.
2. Chevron versus other osteotomy
P: patients with hallux valgus;
I: scarf osteotomy, proximal osteotomy, distal osteotomy, Lapidus procedure;
C: chevron osteotomy;
O: pain, foot function, recurrence/reoperation, complications (infection, delayed union), valgus deformity correction, patient satisfaction.
3. Lapidus versus other technique
P: patients with hallux valgus;
I: lapidus procedure;
C: other technique;
O: pain, foot function, recurrence/reoperation, complications (infection, delayed union), valgus deformity correction, patient satisfaction.
Relevant outcome measures
The guideline development group considered pain, foot function and recurrence/reoperation as critical outcomes for decision making; and complications (infection, delayed union), valgus deformity correction and patient satisfaction as important outcomes for decision making.
A priori, the working group defined valgus deformity correction as a dichotomous outcome, whether or not postoperative HVA < 15° and IMA < 9° were obtained. The working group did not define the other outcomes listed above but used the definitions used in the studies. The working group defined 25% as a minimal clinically (patient) important difference for dichotomous outcomes, 0.5 SD for standardized mean differences (SMD) and 10% for continuous scales (AOFAS, VAS, ACFAS).
Search and select (Methods)
The databases Medline (via OVID), Embase (via Embase.com) and Cochrane were searched for systematic reviews, randomized controlled trials (RCTs) and comparative observational research comparing any two (or more) surgical techniques for the treatment of hallux valgus until 2015. Fourteen studies were initially included. The search was updated in February 12, 2020, limiting the results to systematic reviews and RCTs comparing surgical techniques routinely applied in the Netherlands. The detailed search strategy is depicted under the tab Methods.
The first systematic literature search resulted in 254 hits. 48 studies were initially selected based on title and abstract screening. After reading the full text, 32 studies were excluded and 14 studies were analyzed. The updated systematic literature search resulted in 191 hits. 17 new studies were initially selected based on title and abstract screening. After reading the full text, 12 studies were excluded (see the table with reasons for exclusion under the tab Methods), and 5 studies were included. The new selection replaced the first selection completely.
Results
Three systematic reviews and four RCTs were included in the analysis of the literature. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Elshazly O, Abdel Rahman AF, Fahmy H, Sobhy MH, Abdelhadi W. Scarf versus long chevron osteotomies for the treatment of hallux valgus: A prospective randomized controlled study. Foot Ankle Surg. 2019;25(4):469-477. doi: 10.1016/j.fas.2018.02.017.
- Faber FW, van Kampen PM, Bloembergen MW. Long-term results of the Hohmann and Lapidus procedure for the correction of hallux valgus: a prospective, randomised trial with eight- to 11-year follow-up involving 101 feet. Bone Joint J. 2013;95-B(9):1222-1226. doi:10.1302/0301-620X.95B9.31560.
- Glazebrook M, Copithorne P, Boyd G, et al. Proximal opening wedge osteotomy with wedge-plate fixation compared with proximal chevron osteotomy for the treatment of hallux valgus: a prospective, randomized study. J Bone Joint Surg Am. 2014;96(19):1585-1592. doi:10.2106/JBJS.M.00231.
- Klugarova J, Hood V, Bath-Hextall F, Klugar M, Mareckova J, Kelnarova Z. Effectiveness of surgery for adults with hallux valgus deformity: a systematic review. JBI Database System Rev Implement Rep. 2017;15(6):1671-1710. doi:10.11124/JBISRIR-2017-003422.
- Ma Q, Liang X, Lu J. Chevron osteotomy versus scarf osteotomy for hallux valgus correction: A meta-analysis. Foot Ankle Surg. 2019;25(6):755-760. doi:10.1016/j.fas.2018.09.003.
- Mashima N, Yamamoto H, Tsuboi I, Tsuchiya H, Tanaka Y, Watanabe S. Correction of hallux valgus deformity using the center of rotation of angulation method. J Orthop Sci. 2009 Jul;14(4):377-84. doi: 10.1007/s00776-009-1345-8. Epub 2009 Aug 7. PMID: 19662470.
- Okuda R, Kinoshita M, Yasuda T, Jotoku T, Kitano N, Shima H. The shape of the lateral edge of the first metatarsal head as a risk factor for recurrence of hallux valgus. J Bone Joint Surg Am. 2007 Oct;89(10):2163-72. doi: 10.2106/JBJS.F.01455. PMID: 17908892.
- Tsikopoulos K, Papaioannou P, Kitridis D, Mavridis D, Georgiannos D. Proximal versus distal metatarsal osteotomies for moderate to severe hallux valgus deformity: a systematic review and meta-analysis of clinical and radiological outcomes. Int Orthop. 2018;42(8):1853-1863. doi:10.1007/s00264-018-3782-5.
- Wagner P, Ortiz C, Wagner E. Rotational Osteotomy for Hallux Valgus. A New Technique for Primary and Revision Cases. Tech Foot Ankle Surg. 2017 Mar;16(1):3-10. doi: 10.1097/BTF.0000000000000142. Epub 2016 Nov 17. PMID: 28286430; PMCID: PMC5335916.
- Yamaguchi S, Sasho T, Endo J, Yamamoto Y, Akagi R, Sato Y, Takahashi K. Shape of the lateral edge of the first metatarsal head changes depending on the rotation and inclination of the first metatarsal: a study using digitally reconstructed radiographs. J Orthop Sci. 2015 Sep;20(5):868-74. doi: 10.1007/s00776-015-0749-x. Epub 2015 Jul 16. PMID: 26179881.
Evidence table for systematic review of RCTs and observational studies (intervention studies)
Research question: What are the (dis)advantages of the different surgical techniques compared with each other to treat hallux valgus?
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C) |
Follow-up |
Outcome measures and effect size |
Comments |
|
PICO 1: Proximal versus distal osteotomy |
|||||||
|
Study characteristics and results are extracted from the SR (unless stated otherwise) |
SR and meta-analysis of RCTs
Literature search up to July 2017
A: Chuckpaiwong, 2012 B: Lee, 2015 C: Park, 2013 D: Resch, 1993
Study design: RCT (parallel)
Setting and Country: Army General Training Hospital, Thessaloniki, Greece
Source of funding and conflicts of interest: No funding reported. The authors declare no conflict of interest. |
Inclusion criteria SR: studies that compared the results of proximal and distal metatarsal osteotomies in adults with moderate to severe hallux valgus deformity. This review included studies that compared any type of PMO with any type of DMO.
Exclusion criteria SR: We excluded patients treated with scarf osteotomy as this is considered a mid-shaft rather a proximal or distal metatarsal osteotomy (9, 10). We also did not consider studies assessing the efficacy of Lapidus procedure, since this is classified as an arthrodesis of the tarsometatarsal (TMT) joint.
9 studies were included, 4 of which were RCTs reporting comparisons relevant to the PICO.
Important patient characteristics at baseline: N, mean age A: 125 patients, 131 feet B: 46 patients, 92 feet C: 110 patients D: 68 patients, 80 feet
Age A: PMO 57, DMO 60 years B: 53.8 years C: 54 years D: 49 years
Sex: A: 90% female B: 100% female C: 81% female D: 90% female
Groups comparable at baseline for IMA and HVA. |
A: Proximal metatarsal osteotomy B: PCO C: PCO D: Proximal closing wedge osteotomy
|
A: Distal metatarsal osteotomy B: DCO C: DCO D: DCO
|
End-point of follow-up: A: 12 months B: 40 months C: 38 months D: 42 months
For how many participants were no complete outcome data available? Not specified
|
IMA In degrees, medium term (> 1 and < 10 years). B: prox -9.5±2.4 (n=46) dist -8.6±2.4 (n=46) C: prox -10.5±3.5 (n=56) dist -9.7±2.8 (n=54) D: prox -6±4.7 (n=37) dist -2.4±5 (n=43)
Pooled effect (random effects model): SMD (95% CI):-0.43 (-0.70, -0.15) favouring PMO. Heterogeneity (I2): 25%
AOFAS Score (0-100), higher is better, medium term B: prox -36.5±11.7 Dist -36.1±11.84 C: prox -33.67±10.56 Dist -34.83±10.28 Pooled effect (random effects model): SMD 0.04 (95% CI -0.23 to 0.32) favoring DMO. Heterogeneity (I2): 0%
HVA In degrees, medium term B: prox -23.7±6.9 Dist -23±6.8 C: prox -28.3±6.8 Dist -26.9±5.7 D: prox -13±8.3 dist -8±6.4 Pooled effect (random effects model): SMD 0.04 (95% CI -0.23 to 0.32) favoring DMO. Heterogeneity (I2): 0%
Patient satisfaction Dichotomous, medium term B: prox 44/47 (94%) dist 43/46 (93%) C: prox 53/56 (95%) dist 52/54 (96%) D: prox 36/37 (97%) dist 39/43 (91%) Pooled effect (random effects model): RR 1.01 (0.96, 1.07) favouring DMO. Heterogeneity (I2): 0% |
Author’s conclusion: for the management of moderate to severe HV deformity, we found no significant clinical and radiographic differences between patients treated with proximal and distal metatarsal osteotomies.
Individual studies were of high risk of bias for blinding of participants and unclear risk of bias for selective outcome reporting..
|
|
PICO 2: Chevron versus other osteotomy |
|||||||
|
Klugarova 2017
Study characteristics and results are extracted from the SR (unless stated otherwise) |
SR and meta-analysis of RCTs
Literature search up to July 2014
A: Chuckpaiwong, 2012 B: Deenik, 2007 C: Easley, 1996 D: Lechler, 2012 E: Park, 2013 F: Resch, 1993
Study design: RCT (parallel)
Setting and Country: The Czech Republic (Middle European) Centre for Evidence-Based Healthcare: a Joanna Briggs Institute Centre of Excellence
Source of funding and conflicts of interest: Supported by a grant from European Social Funds ‘‘Support of Human Resources in Science and Research in Non-medical Healthcare at the Faculty of Health Sciences at Palacky´ University Olomouc’’ (CZ.1.07/2.3.00/20.0163) and RVO (61989592). There is no conflict of interest in this project. |
Inclusion criteria SR: RCTs studying adults (18 years or over) with HV deformity, with any type of HV surgery compared to no surgery, conservative management (e.g. physical therapy, kinesio taping, orthosis, etc.) and or different types of surgery.
Exclusion criteria SR: neurological problems causing foot deformities, for example, cerebral palsy, neuropathy, stroke, multiple sclerosis.
25 studies included, 6 of which reported comparisons relevant to the PICO.
Important patient characteristics at baseline:
N at baseline A: 125 patients with moderate to severe HV B: 120 patients, 141 feet C: 75 patients, 97 feet D: 72 patients with mild-to moderate HV E: 120 patients F: 79 patients
Age range (years) A: 30-79 B: not reported C: 25-73 D: mean 52.3 E: 24-71 F: 16-78
Sex: A: 90% female B: not reported C: not reported D: 82% female E: 100% female F: not reported |
A: Distal metatarsal osteotomy B: Scarf osteotomy C: Proximal Chevron osteotomy (PCO) D: Distal Chevron osteotomy (DCO) E: Proximal Chevron osteotomy F: Proximal osteotomy
|
A: Proximal metatarsal osteotomy B: Chevron osteotomy C: Proximal crescentic osteotomy D: Chevron-Akin double osteotomy E: Distal Chevron osteotomy
F: Distal Chevron osteotomy
|
End-point of follow-up: Not reported
For how many participants were no complete outcome data available? A: No loss to follow up B: 5 lost to follow up C: 9 lost to follow up D: unclear E: 10 lost to follow up F: 11 lost to follow up
|
Pain VAS, long term. Mean difference (95% CI): Distal versus proximal A: Distal OT 1.02±1.09 (n=52) Prox OT 3.22±1.5 (n=79) E: DCO -37.4±4.8 (n=54) PCO -36..8±4.4 (n=56) Pooled effect (random effects model) SMD: 0.87 (-0.59, 2.33) favouring distal osteotomy
Distal chevron versus other D: DCO 1.7±0.7 (n=46) Chevron-Akin 1.8±0.5 (n=26)
No trial assessed level of pain using a validated tool at short-term and medium-term follow-up.
Adverse events B: Chevron 9/70 (13%) Scarf 14/66 (21%) RR 0.61 (0.28, 1.31) Prox crescentic 7/41 (17%) RR 1.23 (0.50, 2.99) D: DCO 3/46 (7%) Chevron-Akin 0/26 (0%) RR 4.02 (0.22, 74.94) DCO 5/56 (9%) RR 1.24 (0.40, 3.84) F: prox OT 1/43 (2%) DCO 11/37 (30%) RR 0.08 (0.01, 0.58)
Patient satisfaction No trial assessed patient satisfaction using a validated tool. |
Author’s conclusions: This systematic review has identified that there is a lack of high-quality studies comparing similar types of HV treatment. Selection of outcome measures is inconsistent, and few trials have compared the same two surgical procedures. It is therefore not possible to recommend one type of treatment over another.
Primary outcome was gait performance.
Individual studies were of medium to low quality.
|
|
Ma, 2018
Study characteristics and results are extracted from the SR (unless stated otherwise) |
SR and meta-analysis of RCTs
Literature search up to October 2017
A: Deenik, 2007 B: Jeuken, 2016 C: Mahadevan, 2015
Study design: RCT (parallel)
Setting and Country: Department of Foot and Ankle Surgery, Xi'an Honghui Hospital, China
Source of funding and conflicts of interest: No funding. The authors declare no conflict of interest.
|
Inclusion criteria SR: 1) English language studies on the curative effect of scarf osteotomy and chevron osteotomy on patients with HV; 2) using chevron osteotomy and scarf osteotomy as the main treatment approach in chevron and scarf groups, respectively; and 3) posttreatment HVA and IMA data and AOFAS scores as the main outcome variables in each study.
Exclusion criteria SR: Non-treatise literature including reviews, letters, and comments.
4 studies included in the SR, 3 of which were RCTs
Important patient characteristics at baseline: N, mean age A: 96 feet, 44 yrs B: 73 feet, 57 yrs C: 109 feet, 51 yrs
Sex: Not reported
Deformity: HVA and IMA at baseline comparable between groups. |
A: Scarf osteotomy B: Scarf osteotomy C: Scarf osteotomy
|
A: Chevron osteotomy B: Chevron osteotomy C: Chevron osteotomy
|
End-point of follow-up: A: 2 years B: 13.8 ± 1.2 y C: 1 year
For how many participants were no complete outcome data available? Not reported
|
Function AOFAS Score (0-100), higher is better A: Chevron 89.0±12.2 (n=47) Scarf 91.2±12.1 (n=49) B: Chevron 80.1±15.9 (n=37) Scarf 79.5±14.1 (n=36)
Pooled effect (random effects model) mean difference (95% CI): -0.08 (-0.39, 0.22) favouring chevron. Heterogeneity (I2): 0%
HVA degrees A: Chevron 17.2±5.8 (n=47) Scarf 18.1±5.7 (n=49) B: Chevron 19.8±5.6 (n=37) Scarf 22.4±5.2 (n=36) C: Chevron 14.3±7.4 (n=60) Scarf 13.0±7.6 (n=49) Pooled effect (random effects model) mean difference (95% CI): -0.13 (-0.49, 0.23) favouring chevron Heterogeneity (I2): 56%
IMA degrees A: Chevron 10.3±1.9 (n=47) Scarf 9.9±2.0 (n=49) B: Chevron 8.3±2.7 (n=37) Scarf 8.9±2.6 (n=36) C: Chevron 5.8±2.5 (n=60) Scarf 6.9±2.8 (n=49) Pooled effect (random effects model) mean difference (95% CI): -0.15 (-0.52, 0.23) favouring chevron Heterogeneity (I2): 59%
Adverse events A: Chevron 4/47 (8.5%) Scarf 2/49 (4%) C: Chevron 1/60 (1.6%) Scarf 1/49 (2.0%) Pooled effect (random effects model) mean difference (95% CI): 1.63 (0.40, 6.69) favouring Scarf. Heterogeneity (I2): 0% |
Author’s conclusions: No significant difference was observed between chevron and scarf osteotomy for the treatment of HV patients with respect to HVA, IMA, AOFAS score, and complication rate.
Individual studies were of unclear risk of bias.
|
|
PICO 3: Lapidus versus. other technique |
|||||||
|
- |
|
|
|
|
|
|
|
Evidence table for intervention studies
Research question: What are the (dis)advantages of the different surgical techniques compared with each other to treat hallux valgus?
Table of quality assessment for systematic reviews of RCTs and observational studies
|
Study
First author, year |
Appropriate and clearly focused question?
Yes/no/unclear |
Comprehensive and systematic literature search?
Yes/no/unclear |
Description of included and excluded studies?
Yes/no/unclear |
Description of relevant characteristics of included studies?
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?
Yes/no/unclear/notapplicable |
Assessment of scientific quality of included studies?
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?
Yes/no/unclear |
Potential risk of publication bias taken into account?
Yes/no/unclear |
Potential conflicts of interest reported?
Yes/no/unclear |
|
Klugarove, 2017 |
Yes |
Yes |
Yes Reasons for exclusion are indicated, but not with exclusion table |
Yes |
N/A |
Yes |
Yes |
No |
Unclear . No conflict for SR, individual studies not reported. |
|
Ma, 2018 |
Yes |
Yes |
Yes Reasons for exclusion are indicated, but not with exclusion table |
Yes |
N/A |
Yes |
Yes |
Yes, Egger’s test |
Unclear . No conflict for SR, individual studies not reported. |
|
Tsikopoulos, 2018 |
Yes |
Yes |
Yes Reasons for exclusion are indicated, but not with exclusion table |
Yes |
N/A |
Yes |
Yes |
Yes |
Unclear . No conflict for SR, individual studies not reported. |
Based on AMSTAR checklist (Shea, 2007; BMC Methodol 7: 10; doi:10.1186/1471-2288-7-10) and PRISMA checklist (Moher, 2009, PLoS Med 6: e1000097; doi:10.1371/journal.pmed1000097)
Risk of bias table for intervention studies (randomized controlled trials)
|
Study reference
(first author, publication year) |
Describe method of randomisation |
Bias due to inadequate concealment of allocation?
(unlikely/likely/unclear) |
Bias due to inadequate blinding of participants to treatment allocati on?
(unlikely/likely/unclear) |
Bias due to inadequate blinding of care providers to treatment allocation?
(unlikely/likely/unclear) |
Bias due to inadequate blinding of outcome accessors to treatment allocation?
(unlikely/likely/unclear) |
Bias due to selective outcome reporting on basis of the results?
(unlikely/likely/unclear) |
Bias due to loss to follow-up?
(unlikely/likely/unclear) |
Bias due to violation of intention to treat analysis?
(unlikely/likely/unclear) |
|
Elshazly, 2018 |
Unclear: computer generated randomization by Random Allocation Software. |
Unclear, not described |
Likely, not blinded
|
Unclear |
Unclear |
Likely
|
unclear |
unclear |
|
Glazebrook, 2014 |
patients were prospectively randomized into one of two cohorts with use of sealed envelopes. |
Unclear |
Likely, not blinded
|
Unclear |
Unclear |
Unlikely, registered at clinicaltrials.gov |
unlikely |
unclear |
Table of excluded studies
|
Author and year |
Reason for exclusion |
|
Barg, 2018 |
No comparative data |
|
Faber, 2013 |
No comparison of the techniques in the PICO |
|
Fournier, 2019 |
Review, no comparative studies included |
|
Giannini, 2013 |
No comparison of the techniques in the PICO |
|
Harb, 2015 |
Review, no comparative studies included |
|
Jeuken, 2016 |
Described in included meta-analysis |
|
Lai, 2018 |
No randomized study |
|
Lee, 2015 |
Described in included meta-analysis |
|
Mahadevan, 2016 |
Described in included meta-analysis |
|
Matar, 2019 |
Review, no comparative studies included |
|
Park, 2013 |
Described in included meta-analysis |
|
Schuh, 2013 |
Review, no comparative studies included |
|
Uygur, 2016 |
No comparison of the techniques in the PICO |
|
Waizy, 2019 |
Review, no meta-analysis |
Beoordelingsdatum en geldigheid
Publicatiedatum : 08-10-2021
Beoordeeld op geldigheid : 29-07-2021
Algemene gegevens
De herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten en werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
De richtlijn is ontwikkeld in samenwerking met:
- Koninklijk Nederlands Genootschap voor Fysiotherapie
- Stichting Landelijk Overkoepelend Orgaan voor de Podologie
- Nederlandse Vereniging van Podotherapeuten
- NVOS-Orthobanda
- Nederlandse Vereniging voor Anesthesiologie
- Nederlandse Vereniging voor Radiologie
- ReumaNederland
- Patiëntenfederatie Nederland
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2019 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen die betrokken zijn bij de zorg voor patiënten met een hallux valgus.
Werkgroep
- Drs. W.P. Metsaars, orthopedisch chirurg bij Annatommie MC (voorzitter), NOV
- Dr. I.V. van Dalen, orthopedisch chirurg in de Bergman Kliniek, NOV
- Dr. M.A. Witlox, orthopedisch chirurg in MUMC, NOV
- Drs. S.B. Keizer, orthopedisch chirurg in Haaglanden MC, NOV
- C.J.C.M. Hoogeveen, podoposturaal therapeut bij Praktijk voor Podoposturale Therapie, KNGF en Stichting LOOP
- A.P. van Dam, orthopedisch schoentechnoloog bij Graas Company, NVOS-Orthobanda
- S.C.C. Scheepens, podotherapeut bij Scheepens en Klijsen Podotherapie, NVvP
- N. Lopuhaä, beleidsmedewerker Patiëntbelangen, ReumaNederland
Met ondersteuning van
- Dr. S. Persoon, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. M.S. Ruiter, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Metsaars (voorzitter) |
Orthopedisch chirurg, voet en enkel, Annatommie MC |
Penningmeester Dutch Foot & Ankle Society: onbetaald, verrichten expertises, DC expertise centrum: betaald. |
Geen |
Geen actie |
|
Scheepens |
Podotherapeut/eigenaar 30-40u/wk Scheepens en Vijsen Podotherapie |
Externe beoordelaar Fontys Hogeschool opleiding podotherapie betaald 2 x halve dag per jaar; |
Geen |
Geen actie |
|
Van Dalen |
Orthopedisch chirurg, voet en enkel, Bergmanclinics te Naarden fulltime |
Geen |
Geen |
Geen actie |
|
Lopuhaä |
Beleidsmedewerker Patientenbelangen ReumaNederland |
Geen |
Geen |
Geen actie |
|
Hoogeveen |
Werkzaam als podoposturaal therapeut in eigen praktijk - de Praktijk voor Podoposturale Therapie- in Nieuwegein (1,5 dag per week) met als achtergrond fysiotherapeut, manueel therapeut (Niet praktiserend)
Mede eigenaar van Kennis- en Opleidingsinstituut voor Voet, Houding en Beweging (3 dagen per week) - functie ontwikkelaar van oefenprotocollen voor de voet en opleiding voetentrainer voor fysio- en oefentherapeuten. |
Geen |
Geen |
Geen actie |
|
Keizer |
Orthopedisch Chirurg, Haaglanden MC. |
Geen |
Geen |
Geen actie |
|
Van Dam |
Orthopedisch Schoentechnoloog en directeur/eigenaar bij Graas Orthopedische Schoentechniek voor 38 uur per week |
Vicevoorzitter van NVOS-Orthobanda, branchevereniging voor zorgondernemers in orthopedische hulpmiddelen, onbetaalde functie. Voorzitter van Stichting Thuishuis Woerden, zet zich in tegen eenzaamheid onder ouderen in Woerden, onbetaalde functie. |
Geen |
Geen actie |
|
Witlox |
Orthopedisch Chirurg, MUMC+ |
Bestuur WKO, niet betaald Penningmeester oudervereniging OBS Maastricht, niet betaald |
Geen |
Geen actie |
|
Persoon |
Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Geen |
Geen actie |
|
Ruiter |
Kennisinstituut van de Federatie Medisch Specialisten |
Geen |
Geen |
Geen actie |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntperspectief door Patiëntenfederatie Nederland en andere relevante patiëntenorganisaties uit te nodigen voor de Invitational conference. Het verslag hiervan (zie bijlage) is besproken in de werkgroep. Bovendien is in 2013 een focusgroepbijeenkomst gehouden met patiënten. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen.
Bij het herzien van de (sub)modules ‘conservatieve behandeling’, ‘(contra-)indicaties voor chirurgische behandeling’, ‘open chirurgische technieken’ en ‘minimaal invasieve technieken’ werd het patiëntperspectief vertegenwoordigd door afvaardiging van patiëntenorganisatie ReumaNederland in de werkgroep. Tot slot werden de herziene modules voor commentaar voorgelegd aan de relevante patiëntenorganisaties en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Methode ontwikkeling
Evidence based
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met een hallux valgus. De werkgroep beoordeelde de aanbeveling(en) uit de eerdere richtlijnmodule (NOV, 2015) op noodzaak tot revisie. Tevens zijn er knelpunten aangedragen door een Invitational conference. Een verslag hiervan is opgenomen in de bijlagen. Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur en de beoordeling van de risk-of-bias van de individuele studies is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello, 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE-methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt)organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. https://richtlijnendatabase.nl/over_deze_site.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Schünemann HJ, Oxman AD, Brozek J, Glasziou P, Jaeschke R, Vist GE, Williams JW Jr, Kunz R, Craig J, Montori VM, Bossuyt P, Guyatt GH; GRADE Working Group. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ. 2008 May 17;336(7653):1106-10. doi: 10.1136/bmj.39500.677199.AE. Erratum in: BMJ. 2008 May 24;336(7654). doi: 10.1136/bmj.a139.
Schünemann, A Holger J (corrected to Schünemann, Holger J). PubMed PMID: 18483053; PubMed Central PMCID: PMC2386626.
Wessels M, Hielkema L, van der Weijden T. How to identify existing literature on patients' knowledge, views, and values: the development of a validated search filter. J Med Libr Assoc. 2016 Oct;104(4):320-324. PubMed PMID: 27822157; PubMed Central PMCID: PMC5079497.
Zoekverantwoording
|
Richtlijn: Hallux valgus |
|
|
Uitgangsvraag: Welke chirurgische ingreep heeft de voorkeur voor de behandeling van patiënten met een hallux valgus? |
|
|
Database(s): Medline, Embase |
Datum: 26-2-2020 |
|
Periode: 2013- feb 2020 |
Talen: Engels |
|
Literatuurspecialist: Miriam van der Maten |
|
|
Database |
Zoektermen |
|||||||||||||||||||||
|
Embase
|
|
|||||||||||||||||||||
|
Medline (OVID)
|
1 Hallux Valgus/ (3293) 2 ((("Great Toe*" or hallux) adj3 (Deform* or Valgus or Deviat* or abduct*)) or Bunion* or abductovalgus or "metatarsus primus varus").ti,ab. (3745) 3 1 or 2 (4368) 4 "Orthopedic Procedures"/ (25151) 5 (surgery or surgeon or surgical or operati*).ti. (709480) 6 Osteotomy/ or Osteotom*.ti,ab. (43055) 7 Bone Screws/ or lapidus.ti,ab. (22889) 8 Arthrodesis/ or Arthrodes*.ti,ab. (14920) 9 (scarf or chevron).ti,ab. (1314) 10 or/4-9 (789873) 11 3 and 10 (2580) 12 Hallux Valgus/su (2423) 13 11 or 12 (2989) 14 limit 13 to (yr="2013 -Current" and (dutch or english)) (789) 15 (meta-analysis/ or meta-analysis as topic/ or (meta adj analy$).tw. or ((systematic* or literature) adj2 review$1).tw. or (systematic adj overview$1).tw. or exp "Review Literature as Topic"/ or cochrane.ab. or cochrane.jw. or embase.ab. or medline.ab. or (psychlit or psyclit).ab. or (cinahl or cinhal).ab. or cancerlit.ab. or ((selection criteria or data extraction).ab. and "review"/)) not (Comment/ or Editorial/ or Letter/ or (animals/ not humans/)) (432821) 16 14 and 15 (30) 17 (exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw.) not (animals/ not humans/) (1949809) 18 (14 and 17) not 16 (90) 19 16 or 18 (120) |