Prokinetica bij GORZ
Uitgangsvraag
Welke farmacologische interventies (Prokinetica) zijn effectief en veilig voor de behandeling van GORZ bij kinderen van 0 – 18 jaar?
Aanbeveling
Erythromycine
Erythromycine wordt niet aangeraden voor de behandeling van GORZ bij kinderen (expert opinie).
Baclofen
Baclofen wordt niet aangeraden voor de behandeling van GORZ bij kinderen (expert opinie).
Metoclopramide en domperidon
Domperidon wordt niet aangeraden als eerste keus therapie voor GORZ bij kinderen (expert opinie).
Metoclopramide wordt niet aangeraden als eerste keus therapie voor GORZ bij kinderen (expert opinie).
Overwegingen
Metoclopramide en domperidon
Metoclopramide passeert de bloed-hersenbarrière en kan daardoor extrapyramidale bijwerkingen geven.104 Deze treden vooral op bij kinderen en jongvolwassenen, met name bij gebruik van een hoge dosering. De noodzaak tot gebruik van metoclopramide en domperidon bij kinderen dient zorgvuldig te worden afgewogen tegen het risico op bijwerkingen, alsmede de beschikbaarheid van alternatieve middelen. De European Medicines Agency (EMA) adviseert om metoclopramide en domperidon niet meer toe te passen bij deze indicaties, omdat in de meeste gevallen een langdurig gebruik vereist is, wat het risico op bijwerkingen verhoogt. Hoewel domperidon de bloed-hersenbarrière niet passeert, worden er naast extrapiramidale bijwerkingen nog andere (ernstige) bijwerkingen beschreven. Zo zou domperidon een verlengend effect op het QTc interval hebben waardoor cardiale bijwerkingen op kunnen treden (in het bijzonder ventriculaire aritmie en acute hartdood). Zie het Kinderformularium voor meest gerapporteerde bijwerkingen van metoclopramide en domperidon.
Onderbouwing
Achtergrond
Wanneer niet-farmacologische interventies onvoldoende effectief zijn en/of wanneer er sprake is van gecompliceerde GORZ, wordt farmacologische behandeling overwogen. Een overzicht van de meest gangbare medicatie, dosering en bijwerkingen is opgenomen in de aanverwante producten.
Conclusies / Summary of Findings
Erythromycine
Er is geen bewijs voor het gebruik van erythromycine voor de behandeling van GORZ bij kinderen.
Baclofen
Het is onzeker of baclofen leidt tot een vermindering van GOR-symptomen bij kinderen. Bijwerkingen van baclofen bij kinderen zijn niet goed onderzocht. Studies bij volwassenen laten echter significante bijwerkingen zien. Daarom wordt baclofen niet als eerste keus therapie voor GORZ bij kinderen geadviseerd.
Metoclopramide en domperidon
Het is onzeker of behandeling met metoclopramide of domperidon leidt tot een vermindering van GOR-symptomen bij kinderen. Bijwerkingen van deze middelen bij kinderen zijn niet goed onderzocht. Studies bij volwassenen laten echter significante (extrapyramidale) bijwerkingen zien. Daarom worden deze middelen niet als eerste keustherapie voor GORZ bij kinderen geadviseerd.
Samenvatting literatuur
In theorie zouden prokinetica een goede behandeling kunnen zijn voor GORZ door hun stimulerende werking op de motiliteit van het maagdarmkanaal wat tot een versnelde maaglediging en een verbeterde klaring van refluxaat in de slokdarm zou leiden. Er zijn een aantal geneesmiddelen met prokinetische eigenschappen beschikbaar voor de behandeling van GORZ, waaronder metoclopramide, domperidon, cisapride en erythromycine.
Erythromycine
Erythromycine is een macrolide antibioticum dat werkt als een motiline agonist door zijn interactie met motiline receptoren in de maag en het bovenste deel van het maagdarmkanaal. Buiten zijn prokinetische werking, versterkt erythromycine ook de antireflux barrière door verhoging van de tonus van de onderste slokdarmsfincter. Er werden door Rosen et al. geen studies naar het gebruik van erythromycine geïncludeerd. Na Rosen et al. zijn geen nieuwe studies gepubliceerd die voldoen aan de inclusiecriteria, echter recent verscheen één studie die het effect van enteraal toegediende erythromycine op pH-impedantieparameters bij premature neonaten met GOR symptomen onderzocht.98 In deze studie werd geen vermindering van het aantal zuurepisodes op pH-impedantiemetrie gezien, noch was er een verschil in proximale reflux, reflux-index, klaring of symptoomassociatie met apneu. Hoewel de rol van erythromycine in de behandeling van GORZ bij kinderen dus niet goed is onderzocht, wordt dit middel op grote schaal gebruikt in het Verenigd Koninkrijk en de Verenigde Staten.6 Beschreven bijwerkingen van erythromycine zijn onder andere misselijkheid, braken, diarree, maagpijn of –krampen en verminderde eetlust (zie verder Kinderformularium).
Baclofen
Net als bij volwassenen zijn bij kinderen transiënte onderste slokdarmsfincterrelaxaties het dominante mechanisme onderliggend aan een refluxepisode. Deze via de nervus vagus verlopende reflex kan farmacologisch worden geremd, onder andere met de GABA-b-receptor-agonist baclofen. Het effect van baclofen op GOR-symptomen bij kinderen is echter niet onderzocht. Rosen et al vonden één dubbelblinde gerandomiseerde studie die het effect van baclofen op manometrie, pH-metrie en de maaglediging onderzocht bij 30 kinderen met GORZ. Baclofen verminderde zowel de frequentie van het aantal transiënte onderste slokdarmsfincterrelaxaties als het aantal (zure) refluxepisoden en versnelde tevens de maaglediging.99 Er werden geen significante bijwerkingen van baclofen gevonden in deze studie. Studies bij volwassenen rapporteren bijwerkingen als misselijkheid, vermoeidheid, duizeligheid en verlaging van de convulsiedrempel en optreden van convulsies (in het bijzonder bij patiënten bekend met epilepsie). Zie voor meer informatie over bijwerkingen het Kinderformularium.
Metoclopramide en domperidon
Metoclopramide en domperidon zijn dopamine-antagonisten en werkzaam als anti-emeticum en gastroprokineticum. Ze verhogen de tonus van de onderste slokdarmsfincter en versnellen de peristaltiek van de darmen en maag. Rosen et al. includeerde in totaal vier studies die de (bij)werking(en) van domperidon of metoclopramide vs. placebo voor de behandeling van GORZ bij kinderen onderzochten. Er werden na Rosen et al. geen nieuwe studies gepubliceerd die voldoen aan de inclusiecriteria. Van de vier geïncludeerde studies waren er twee die naar het klinische effect (symptoomreductie) van de behandeling keken.100, 101 Alle studies rapporteerden over bijwerkingen en in geen van de studies was sprake van significante bijwerkingen gedurende de studieperiode.100-103 De Loore et al. vergeleken de werking van zowel domperidon als metoclopramide met placebo in een tweeweekse dubbelblinde studie onder 47 kinderen met een klinische GORZ diagnose.101 In deze studie werd een significante vermindering in het aantal patiënten dat regurgiteerde/spuugde na behandeling met domperidon vs. metoclopramide en placebo (p < 0.05 en p < 0.001 respectievelijk) en metoclopramide vs. placebo (p < 0.001) gevonden. Er werden in deze studie echter geen exacte aantallen genoemd en de kwaliteit werd als erg laag beoordeeld. In de studie door Carroccio et al. werd domperidon toegediend in combinatie met antacida en vergeleken met placebo.100 Er werd een significante verlaging van GOR symptomen en aantal refluxepisodes bij pH-metrie gevonden.
Cisapride
Cisapride is ruim 10 jaar geleden van de markt gehaald vanwege mogelijke cardiovasculaire bijwerkingen. De werkgroep heeft daarom besloten om cisapride niet in overweging te nemen als behandeloptie voor GORZ bij kinderen.
Zoeken en selecteren
Bij de selectie en beoordeling van richtlijnen, kwam de internationale richtlijn van Rosen et al. uit 2018 als beste naar voren.1, 6 De kwaliteit van deze richtlijn bleek voldoende om deze als uitgangspunt van de huidige richtlijn te gebruiken. De richtlijn van Rosen et al. is ontwikkeld door een internationale werkgroep van 10 kinderartsen MDL, één epidemioloog en één arts-onderzoeker. Er werd een systematische literatuursearch gedaan (zie de zoekstrategie, flowcharts en studiekarakteristieken) en de werkgroep kwam drie keer bijeen. Artikelen werden geëvalueerd met behulp van Quality Assessment of Studies of Diagnostic Accuracy in het geval van diagnostische studies (QUADAS) of GRADE in het geval van therapeutische studies (zie de evidence tabellen). Aanbevelingen werden gedaan op basis van evidence uit de literatuur. Bij gebrek aan evidence (van voldoende kwaliteit) werden aanbevelingen gedaan op basis van “expert opinion”. Om consensus te bereiken werden nominale groepstechnieken gebruikt.
In deze modules worden per PICO de beschikbare literatuur, conclusies, overige overwegingen en aanbevelingen besproken. We zijn uitgegaan van de NVK-richtlijn uit 2012 en de bevindingen van Rosen et al. en hebben deze waar nodig geüpdatet.
In de tabellen 1 t/m 3 (van het aanverwant product Symptomen bij GORZ) zijn symptomen en bevindingen die passen bij GORZ, alarmsymptomen en aandoeningen in de differentiaaldiagnose van GORZ bij kinderen van 0 – 18 jaar weergegeven. De tabellen zijn gebaseerd op Rosen et al.1 In de aanverwante producten is informatie over medicatie opgenomen (zie het Overzicht geneesmiddelen voor GORZ). De zoekverantwoording bevat informatie over de geïncludeerde studies en de in deze module beschreven literatuur weergegeven in evidence tabellen.
Referenties
- 1 - Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F, et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. Journal of pediatric gastroenterology and nutrition. 2018;66:516-54.
- 2 - Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. Journal of clinical epidemiology. 2011;64:383-94.
- 3 - Singendonk M, Goudswaard E, Langendam M, van Wijk M, van Etten-Jamaludin F, Benninga M, et al. Prevalence of Gastroesophageal Reflux Disease Symptoms in Infants and Children: A Systematic Review. Journal of pediatric gastroenterology and nutrition. 2019;
- 4 - Singendonk MM, Goudswaard E, Langendam M., Van Wijk MP, Van Etten F, Benninga MA, et al. Epidemiology of gastroesophageal reflux disease (GERD) in children: a systematic review [Submitted for publication]. 0000;
- 5 - Singendonk MMJ, Tabbers MM, Benninga MA, Langendam MW. Pediatric Gastroesophageal Reflux Disease: Systematic Review on Prognosis and Prognostic Factors. Journal of pediatric gastroenterology and nutrition. 2018;66:239-43.
- 6 - Davies I, Burman-Roy S, Murphy MS. Gastro-oesophageal reflux disease in children: NICE guidance. BMJ. 2015;350:g7703.
- 7 - Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. The American journal of gastroenterology. 2006;101:1900-20.
- 8 - Arasu TS, Wyllie R, Fitzgerald JF, Franken EA, Siddiqui AR, Lehman GA, et al. Gastroesophageal reflux in infants and children comparative accuracy of diagnostic methods. The Journal of pediatrics. 1980;96:798-803.
- 9 - Cucchiara S, Minella R, D'Armiento F, Franco MT, lervolino C, Campanozzi A, et al. Histologic grading of reflux oesophagitis and its relationship with intra-oesophageal and intragastric pH variables. European Journal of Gastroenterology & Hepatology. 1993;5:621-6.
- 10 - Ravelli AM, Villanacci V, Ruzzenenti N, Grigolato P, Tobanelli P, Klersy C, et al. Dilated intercellular spaces: a major morphological feature of esophagitis. Journal of pediatric gastroenterology and nutrition. 2006;42:510-5.
- 11 - Boix-Ochoa J, Lafuenta JM, Gil-Vernet JM. Twenty-four hour exophageal pH monitoring in gastroesophageal reflux. Journal of pediatric surgery. 1980;15:74-8.
- 12 - Da Dalt L, Mazzoleni S, Montini G, Donzelli F, Zacchello F. Diagnostic accuracy of pH monitoring in gastro-oesophageal reflux. Archives of disease in childhood. 1989;64:1421-6.
- 13 - Cucchiara S, Staiano A, Gobio Casali L, Boccieri A, Paone FM. Value of the 24 hour intraoesophageal pH monitoring in children. Gut. 1990;31:129-33.
- 14 - Cucchiara S, Minella R, Iervolino C, Franco MT, Campanozzi A, Franceschi M, et al. Omeprazole and high dose ranitidine in the treatment of refractory reflux oesophagitis. Archives of disease in childhood. 1993;69:655-9.
- 15 - Kahn A, Rebuffat E, Sottiaux M, Blum D, Yasik EA. Sleep apneas and acid esophageal reflux in control infants and in infants with an apparent life-threatening event. Biology of the neonate. 1990;57:144-9.
- 16 - Patra S, Singh V, Chandra J, Kumar P, Tripathi M. Diagnostic modalities for gastro-esophageal reflux in infantile wheezers. Journal of tropical pediatrics. 2011;57:99-103.
- 17 - Giacchino M, Savarino V, Savarino E. Distinction between patients with non-erosive reflux disease and functional heartburn. Annals of gastroenterology : quarterly publication of the Hellenic Society of Gastroenterology. 2013;26:283-9.
- 18 - Loots CM, van Wijk MP, Blondeau K, Dalby K, Peeters L, Rosen R, et al. Interobserver and intraobserver variability in pH-impedance analysis between 10 experts and automated analysis. The Journal of pediatrics. 2012;160:441-6.e1.
- 19 - Pilic D, Höfs C, Weitmann S. Inter- and intraobserver agreement in 24-hour combined multiple intraluminal impedance and pH measurement in children - a quality assessment from the German Pediatric Impedance Group (G-PIG). Journal of pediatric gastroenterology and nutrition. 2011;53:255-9.
- 20 - Wenzl TG, Benninga MA, Loots CM, Salvatore S, Vandenplas Y. Indications, methodology, and interpretation of combined esophageal impedance-pH monitoring in children: ESPGHAN EURO-PIG standard protocol. Journal of pediatric gastroenterology and nutrition. 2012;55:230-4.
- 21 - Ravi K, DeVault KR, Murray JA, Bouras EP, Francis DL. Inter-observer agreement for multichannel intraluminal impedance-pH testing. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus / ISDE. 2010;23:540-4.
- 22 - Hemmink GJ, Bredenoord AJ, Weusten BL, Monkelbaan JF, Timmer R, Smout AJ. Esophageal pH-impedance monitoring in patients with therapy-resistant reflux symptoms: 'on' or 'off' proton pump inhibitor? Am J Gastroenterol. 2008;103:2446-53.
- 23 - Zerbib F, des Varannes SB, Roman S, Pouderoux P, Artigue F, Chaput U, et al. Normal values and day-to-day variability of 24-h ambulatory oesophageal impedance-pH monitoring in a Belgian-French cohort of healthy subjects. Aliment Pharmacol Ther. 2005;22:1011-21.
- 24 - Loots C, van Herwaarden MY, Benninga MA, VanderZee DC, van Wijk MP, Omari TI. Gastroesophageal reflux, esophageal function, gastric emptying, and the relationship to dysphagia before and after antireflux surgery in children. The Journal of pediatrics. 2013;162:566-73.e2.
- 25 - Smits MJ, Loots CM, Benninga MA, Omari TI, van Wijk MP. New insights in gastroesophageal reflux, esophageal function and gastric emptying in relation to dysphagia before and after anti-reflux surgery in children. Current gastroenterology reports. 2013;15:351.
- 26 - Tucker E, Knowles K, Wright J, Fox MR. Rumination variations: aetiology and classification of abnormal behavioural responses to digestive symptoms based on high-resolution manometry studies. Alimentary pharmacology & therapeutics. 2013;37:263-74.
- 27 - Kessing BF, Bredenoord AJ, Smout AJ. Objective manometric criteria for the rumination syndrome. The American journal of gastroenterology. 2014;109:52-9.
- 28 - Rosen R, Rodriguez L, Nurko S. Pediatric rumination subtypes: A study using high-resolution esophageal manometry with impedance. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society. 2017;29.
- 29 - Singendonk MMJ, Oors JM, Bredenoord AJ, Omari TI, van der Pol RJ, Smits MJ, et al. Objectively diagnosing rumination syndrome in children using esophageal pH-impedance and manometry. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2017;29.
- 30 - Farhath S, He Z, Saslow J, Soundar S, Amendolia B, Bhat V, et al. Detection of pepsin in mouth swab: correlation with clinical gastroesophageal reflux in preterm infants. The journal of maternal-fetal & neonatal medicine: the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstet. 2013;26:819-24.
- 31 - Dy F, Amirault J, Mitchell PD, Rosen R. Salivary Pepsin Lacks Sensitivity as a Diagnostic Tool to Evaluate Extraesophageal Reflux Disease. The Journal of pediatrics. 2016;177:53-8.
- 32 - Fortunato JE, D'Agostino RB, Jr., Lively MO. Pepsin in saliva as a biomarker for oropharyngeal reflux compared with 24-hour esophageal impedance/pH monitoring in pediatric patients. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2016;
- 33 - van der Pol RJ, Smits MJ, van Wijk MP, Omari TI, Tabbers MM, Benninga MA. Efficacy of proton-pump inhibitors in children with gastroesophageal reflux disease: a systematic review. Pediatrics. 2011;127:925-35.
- 34 - Haddad I, Kierkus J, Tron E, Ulmer A, Hu P, Sloan S, et al. Efficacy and safety of rabeprazole in children (1-11 years) with gastroesophageal reflux disease. Journal of pediatric gastroenterology and nutrition. 2013;57:798-807.
- 35 - Fiedorek S, Tolia V, Gold BD, Huang B, Stolle J, Lee C, et al. Efficacy and safety of lansoprazole in adolescents with symptomatic erosive and non-erosive gastroesophageal reflux disease. Journal of pediatric gastroenterology and nutrition. 2005;40:319-27.
- 36 - Baker R, Tsou VM, Tung J, Baker SS, Li H, Wang W, et al. Clinical results from a randomized, double-blind, dose-ranging study of pantoprazole in children aged 1 through 5 years with symptomatic histologic or erosive esophagitis. Clinical pediatrics. 2010;49:852-65.
- 37 - Tolia V, Ferry G, Gunasekaran T, Huang B, Keith R, Book L. Efficacy of lansoprazole in the treatment of gastroesophageal reflux disease in children. Journal of pediatric gastroenterology and nutrition. 2002;35 Suppl 4:S308-18.
- 38 - Bautista J, Fullerton H, Briseno M, Cui H, Fass R. The effect of an empirical trial of high-dose lansoprazole on symptom response of patients with non-cardiac chest pain--a randomized, double-blind, placebo-controlled, crossover trial. Alimentary pharmacology & therapeutics. 2004;19:1123-30.
- 39 - Fass R, Fennerty MB, Ofman JJ, Gralnek IM, Johnson C, Camargo E, et al. The clinical and economic value of a short course of omeprazole in patients with noncardiac chest pain. Gastroenterology. 1998;115:42-9.
- 40 - Fass R, Murthy U, Hayden CW, Malagon IB, Pulliam G, Wendel C, et al. Omeprazole 40 mg once a day is equally effective as lansoprazole 30 mg twice a day in symptom control of patients with gastro-oesophageal reflux disease (GERD) who are resistant to conventional-dose lansoprazole therapy-a prospective, randomized, multi-centre study. Alimentary pharmacology & therapeutics. 2000;14:1595-603.
- 41 - Savarino E, Zentilin P, Savarino V. NERD: an umbrella term including heterogeneous subpopulations. Nat Rev Gastroenterol Hepatol. 2013;10:371-80.
- 42 - Cheng FK, Albert DM, Maydonovitch CL, Wong RK, Moawad FJ. Categorization of patients with reflux symptoms referred for pH and impedance testing while off therapy. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2015;13:867-73.
- 43 - Singendonk MMJ, Rexwinkel R, Steutel NF, Gottrand F, McCall L, Orsagh-Yentis DK, et al. Development of A Core Outcome Set For Infant Gastroesophageal Reflux Disease. Journal of pediatric gastroenterology and nutrition. 2018;
- 44 - Loots C, Kritas S, van Wijk M, McCall L, Peeters L, Lewindon P, et al. Body positioning and medical therapy for infantile gastroesophageal reflux symptoms. Journal of pediatric gastroenterology and nutrition. 2014;59:237-43.
- 45 - Corvaglia L, Rotatori R, Ferlini M, Aceti A, Ancora G, Faldella G. The effect of body positioning on gastroesophageal reflux in premature infants: evaluation by combined impedance and pH monitoring. The Journal of pediatrics. 2007;151:591-6, 6.e1.
- 46 - Omari TI, Rommel N, Staunton E, Lontis R, Goodchild L, Haslam RR, et al. Paradoxical impact of body positioning on gastroesophageal reflux and gastric emptying in the premature neonate. The Journal of pediatrics. 2004;145:194-200.
- 47 - Vandenplas Y, De Schepper J, Verheyden S, Devreker T, Franckx J, Peelman M, et al. A preliminary report on the efficacy of the Multicare AR-Bed in 3-week-3-month-old infants on regurgitation, associated symptoms and acid reflux. Archives of disease in childhood. 2010;95:26-30.
- 48 - Moon RY, SIDS and other sleep-related infant deaths: expansion of recommendations for a safe infant sleeping environment. Pediatrics. 2011;128:1030-9.
- 49 - Loots C, Smits M, Omari T, Bennink R, Benninga M, van Wijk M. Effect of lateral positioning on gastroesophageal reflux (GER) and underlying mechanisms in GER disease (GERD) patients and healthy controls. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society. 2013;25:222-9, e161-2.
- 50 - Ness-Jensen E, Hveem K, El-Serag H, Lagergren J. Lifestyle Intervention in Gastroesophageal Reflux Disease. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2016;14:175-82.e3.
- 51 - Vandenplas Y, Hachimi-Idrissi S, Casteels A, Mahler T, Loeb H. A clinical trial with an "anti-regurgitation" formula. European journal of pediatrics. 1994;153:419-23.
- 52 - Iacono G, Vetrano S, Cataldo F, Ziino O, Russo A, Lorello D, et al. Clinical trial with thickened feeding for treatment of regurgitation in infants. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2002;34:532-3.
- 53 - Chao HC, Vandenplas Y. Comparison of the effect of a cornstarch thickened formula and strengthened regular formula on regurgitation, gastric emptying and weight gain in infantile regurgitation. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus / ISDE. 2007;20:155-60.
- 54 - Xinias I, Mouane N, Le Luyer B, Spiroglou K, Demertzidou V, Hauser B, et al. Cornstarch thickened formula reduces oesophageal acid exposure time in infants. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2005;37:23-7.
- 55 - Ostrom KM, Jacobs JR, Merritt RJ, Murray RD. Decreased regurgitation with a soy formula containing added soy fiber. Clinical pediatrics. 2006;45:29-36.
- 56 - Chao HC, Vandenplas Y. Effect of cereal-thickened formula and upright positioning on regurgitation, gastric emptying, and weight gain in infants with regurgitation. Nutrition (Burbank, Los Angeles County, Calif). 2007;23:23-8.
- 57 - Miyazawa R, Tomomasa T, Kaneko H, Morikawa A. Effect of formula thickened with locust bean gum on gastric emptying in infants. Journal of paediatrics and child health. 2006;42:808-12.
- 58 - Miyazawa R, Tomomasa T, Kaneko H, Arakawa H, Morikawa A. Effect of formula thickened with reduced concentration of locust bean gum on gastroesophageal reflux. Acta paediatrica (Oslo, Norway : 1992). 2007;96:910-4.
- 59 - Miyazawa R, Tomomasa T, Kaneko H, Morikawa A. Effect of locust bean gum in anti-regurgitant milk on the regurgitation in uncomplicated gastroesophageal reflux. Journal of pediatric gastroenterology and nutrition. 2004;38:479-83.
- 60 - Moukarzel AA, Abdelnour H, Akatcherian C. Effects of a prethickened formula on esophageal pH and gastric emptying of infants with GER. J Clin Gastroenterol. 2007;41:823-9.
- 61 - Vanderhoof JA, Moran JR, Harris CL, Merkel KL, Orenstein SR. Efficacy of a pre-thickened infant formula: a multicenter, double-blind, randomized, placebo-controlled parallel group trial in 104 infants with symptomatic gastroesophageal reflux. Clinical pediatrics. 2003;42:483-95.
- 62 - Hegar B, Rantos R, Firmansyah A, De Schepper J, Vandenplas Y. Natural evolution of infantile regurgitation versus the efficacy of thickened formula. Journal of pediatric gastroenterology and nutrition. 2008;47:26-30.
- 63 - Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). Journal of pediatric gastroenterology and nutrition. 2009;49:498-547.
- 64 - Orenstein SR, Magill HL, Brooks P. Thickening of infant feedings for therapy of gastroesophageal reflux. The Journal of pediatrics. 1987;110:181-6.
- 65 - Ummarino D, Miele E, Martinelli M, Scarpato E, Crocetto F, Sciorio E, et al. Effect of magnesium alginate plus simethicone on gastroesophageal reflux in infants. Journal of pediatric gastroenterology and nutrition. 2015;60:230-5.
- 66 - Vandenplas Y, Benninga M, Broekaert I, Falconer J, Gottrand F, Guarino A, et al. Functional gastro-intestinal disorder algorithms focus on early recognition, parental reassurance and nutritional strategies. Acta paediatrica (Oslo, Norway : 1992). 2016;105:244-52.
- 67 - Khoshoo V, Dhume P. Clinical response to 2 dosing regimens of lansoprazole in infants with gastroesophageal reflux. Journal of pediatric gastroenterology and nutrition. 2008;46:352-4.
- 68 - Famouri F, Zibanejad N, Kabiri P, Kelishadi R. Comparison of Hypoallergenic Diet vs. Ranitidine in Treatment of Gastroesophageal Reflux Disease of Infants: A Randomized Clinical Trial. 2017;27:e5343.
- 69 - Koletzko S, Niggemann B, Arato A, Dias JA, Heuschkel R, Husby S, et al. Diagnostic approach and management of cow's-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. Journal of pediatric gastroenterology and nutrition. 2012;55:221-9.
- 70 - Alsalamah M, Makhajia M, Somers G, Marcon M, Hummel D, Upton J. Anaphylaxis to Milk After Elimination Diet for Eosinophilic Gastrointestinal Disease. Am J Gastroenterol. 2016;111:752-3.
- 71 - Maslin K, Grundy J, Glasbey G, Dean T, Arshad SH, Grimshaw K, et al. Cows' milk exclusion diet during infancy: Is there a long-term effect on children's eating behaviour and food preferences? Pediatric allergy and immunology : official publication of the European Society of Pediatric Allergy and Immunology. 2016;27:141-6.
- 72 - Miller S, Comparison of the efficacy and safety of a new aluminium-free paediatric alginate preparation and placebo in infants with recurrent gastro-oesophageal reflux. Current medical research and opinion. 1999;15:160-8.
- 73 - Oderda G, Dell'Olio D, Forni M, Farina L, Tavassoli K, Ansaldi N. Treatment of childhood peptic oesophagitis with famotidine or alginate-antacid. The Italian journal of gastroenterology. 1990;22:346-9.
- 74 - Cucchiara S, Staiano A, Romaniello G, Capobianco S, Auricchio S. Antacids and cimetidine treatment for gastro-oesophageal reflux and peptic oesophagitis. Archives of disease in childhood. 1984;59:842-7.
- 75 - Woodard-Knight L, Fudge A, Teubner J, Simmer K. Aluminium absorption and antacid therapy in infancy. Journal of paediatrics and child health. 1992;28:257-9.
- 76 - Tsou VM, Young RM, Hart MH, Vanderhoof JA. Elevated plasma aluminum levels in normal infants receiving antacids containing aluminum. Pediatrics. 1991;87:148-51.
- 77 - Davies I, Burman-Roy S, Murphy MS. Gastro-oesophageal reflux disease in children: NICE guidance. BMJ (Clinical research ed). 2015;350.
- 78 - Excellence NIfHaC. Dyspepsia and Gastro-Oesophageal Reflux Disease: Investigation and Management of Dyspepsia, Symptoms Suggestive of Gastro-Oesophageal Reflux Disease, or Both. 2014;
- 79 - Simeone D, Caria MC, Miele E, Staiano A. Treatment of childhood peptic esophagitis: a double-blind placebo-controlled trial of nizatidine. Journal of pediatric gastroenterology and nutrition. 1997;25:51-5.
- 80 - Cucchiara S, Gobio-Casali L, Balli F, Magazzu G, Staiano A, Astolfi R, et al. Cimetidine treatment of reflux esophagitis in children: an Italian multicentric study. Journal of pediatric gastroenterology and nutrition. 1989;8:150-6.
- 81 - Orenstein SR, Blumer JL, Faessel HM, McGuire JA, Fung K, Li BU, et al. Ranitidine, 75 mg, over-the-counter dose: pharmacokinetic and pharmacodynamic effects in children with symptoms of gastro-oesophageal reflux. Alimentary pharmacology & therapeutics. 2002;16:899-907.
- 82 - Arguelles-Martin F, Gonzalez-Fernandez F, Gentles MG. Sucralfate versus cimetidine in the treatment of reflux esophagitis in children. The American journal of medicine. 1989;86:73-6.
- 83 - Hussain S, Kierkus J, Hu P, Hoffman D, Lekich R, Sloan S, et al. Safety and efficacy of delayed release rabeprazole in 1- to 11-month-old infants with symptomatic GERD. Journal of pediatric gastroenterology and nutrition. 2014;58:226-36.
- 84 - Moore DJ, Tao BS, Lines DR, Hirte C, Heddle ML, Davidson GP. Double-blind placebo-controlled trial of omeprazole in irritable infants with gastroesophageal reflux. The Journal of pediatrics. 2003;143:219-23.
- 85 - Orenstein SR, Hassall E, Furmaga-Jablonska W, Atkinson S, Raanan M. Multicenter, double-blind, randomized, placebo-controlled trial assessing the efficacy and safety of proton pump inhibitor lansoprazole in infants with symptoms of gastroesophageal reflux disease. The Journal of pediatrics. 2009;154:514-20.e4.
- 86 - Winter H, Kum-Nji P, Mahomedy SH, Kierkus J, Hinz M, Li H, et al. Efficacy and safety of pantoprazole delayed-release granules for oral suspension in a placebo-controlled treatment-withdrawal study in infants 1-11 months old with symptomatic GERD. Journal of pediatric gastroenterology and nutrition. 2010;50:609-18.
- 87 - Davidson G, Wenzl TG, Thomson M, Omari T, Barker P, Lundborg P, et al. Efficacy and safety of once-daily esomeprazole for the treatment of gastroesophageal reflux disease in neonatal patients. The Journal of pediatrics. 2013;163:692-8.e1-2.
- 88 - Winter H, Gunasekaran T, Tolia V, Gottrand F, Barker PN, Illueca M. Esomeprazole for the treatment of GERD in infants ages 1-11 months. Journal of pediatric gastroenterology and nutrition. 2012;55:14-20.
- 89 - Cohen S, Bueno de Mesquita M, Mimouni FB. Adverse effects reported in the use of gastroesophageal reflux disease treatments in children: a 10 years literature review. British journal of clinical pharmacology. 2015;80:200-8.
- 90 - Zohalinezhad ME, Imanieh MH, Samani SM, Mohagheghzadeh A, Dehghani SM, Haghighat M, et al. Effects of Quince syrup on clinical symptoms of children with symptomatic gastroesophageal reflux disease: A double-blind randomized controlled clinical trial. Complementary therapies in clinical practice. 2015;21:268-76.
- 91 - Ummarino D, Miele E, Masi P, Tramontano A, Staiano A, Vandenplas Y. Impact of antisecretory treatment on respiratory symptoms of gastroesophageal reflux disease in children. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus. 2012;25:671-7.
- 92 - Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. The American journal of gastroenterology. 2013;108:308-28; quiz 29.
- 93 - Cremonini F, Ziogas DC, Chang HY, Kokkotou E, Kelley JM, Conboy L, et al. Meta-analysis: the effects of placebo treatment on gastro-oesophageal reflux disease. Alimentary pharmacology & therapeutics. 2010;32:29-42.
- 94 - Chiba N, De Gara CJ, Wilkinson JM, Hunt RH. Speed of healing and symptom relief in grade II to IV gastroesophageal reflux disease: a meta-analysis. Gastroenterology. 1997;112:1798-810.
- 95 - Labenz J, Malfertheiner P. Treatment of uncomplicated reflux disease. World journal of gastroenterology. 2005;11:4291-9.
- 96 - Rosen R, Amirault J, Liu H, Mitchell P, Hu L, Khatwa U, et al. Changes in gastric and lung microflora with acid suppression: acid suppression and bacterial growth. JAMA pediatrics. 2014;168:932-7.
- 97 - Trikha A, Baillargeon JG, Kuo YF, Tan A, Pierson K, Sharma G, et al. Development of food allergies in patients with gastroesophageal reflux disease treated with gastric acid suppressive medications. Pediatric allergy and immunology : official publication of the European Society of Pediatric Allergy and Immunology. 2013;24:582-8.
- 98 - Ballengee CR, Davalian F, Conaway MR, Sauer CG, Kaufman DA. Erythromycin and Reflux Events in Premature Neonates: A Randomized Clinical Trial. Journal of pediatric gastroenterology and nutrition. 2018;67:720-5.
- 99 - Omari TI, Benninga MA, Sansom L, Butler RN, Dent J, Davidson GP. Effect of baclofen on esophagogastric motility and gastroesophageal reflux in children with gastroesophageal reflux disease: a randomized controlled trial. The Journal of pediatrics. 2006;149:468-74.
- 100 - Carroccio A, Iacono G, Montalto G, Cavataio F, Soresi M, Notarbartolo A. Domperidone plus magnesium hydroxide and aluminum hydroxide: a valid therapy in children with gastroesophageal reflux. A double-blind randomized study versus placebo. Scandinavian journal of gastroenterology. 1994;29:300-4.
- 101 - De Loore I, Van Ravensteyn H, Ameryckx L. Domperidone drops in the symptomatic treatment of chronic paediatric vomiting and regurgitation. A comparison with metoclopramide. Postgraduate medical journal. 1979;55 Suppl 1:40-2.
- 102 - Tolia V, Calhoun J, Kuhns L, Kauffman RE. Randomized, prospective double-blind trial of metoclopramide and placebo for gastroesophageal reflux in infants. The Journal of pediatrics. 1989;115:141-5.
- 103 - Bellissant E, Duhamel JF, Guillot M, Pariente-Khayat A, Olive G, Pons G. The triangular test to assess the efficacy of metoclopramide in gastroesophageal reflux. Clinical pharmacology and therapeutics. 1997;61:377-84.
- 104 - Lau Moon Lin M, Robinson PD, Flank J, Sung L, Dupuis LL. The Safety of Metoclopramide in Children: A Systematic Review and Meta-Analysis. Drug safety. 2016;39:675-87.
- 105 - Stefanidis D, Hope WW, Kohn GP, Reardon PR, Richardson WS, Fanelli RD. Guidelines for surgical treatment of gastroesophageal reflux disease. Surgical endoscopy. 2010;24:2647-69.
- 106 - Moore M, Afaneh C, Benhuri D, Antonacci C, Abelson J, Zarnegar R. Gastroesophageal reflux disease: A review of surgical decision making. World journal of gastrointestinal surgery. 2016;8:77-83.
- 107 - Kubiak R, Andrews J, Grant HW. Long-term outcome of laparoscopic nissen fundoplication compared with laparoscopic thal fundoplication in children: a prospective, randomized study. Annals of surgery. 2011;253:44-9.
- 108 - Rothenberg SS. Two decades of experience with laparoscopic nissen fundoplication in infants and children: a critical evaluation of indications, technique, and results. Journal of laparoendoscopic & advanced surgical techniques Part A. 2013;23:791-4.
- 109 - Smith CD, McClusky DA, Rajad MA, Lederman AB, Hunter JG. When fundoplication fails: redo? Annals of surgery. 2005;241:861-9; discussion 9-71.
- 110 - Kellokumpu I, Voutilainen M, Haglund C, Farkkila M, Roberts PJ, Kautiainen H. Quality of life following laparoscopic Nissen fundoplication: assessing short-term and long-term outcomes. World journal of gastroenterology. 2013;19:3810-8.
- 111 - Davis CS, Baldea A, Johns JR, Joehl RJ, Fisichella PM. The evolution and long-term results of laparoscopic antireflux surgery for the treatment of gastroesophageal reflux disease. JSLS : Journal of the Society of Laparoendoscopic Surgeons / Society of Laparoendoscopic Surgeons. 2010;14:332-41.
- 112 - Wakeman DS, Wilson NA, Warner BW. Current status of surgical management of gastroesophageal reflux in children. Current opinion in pediatrics. 2016;28:356-62.
- 113 - Baerg J, Thorpe D, Bultron G, Vannix R, Knott EM, Gasior AC, et al. A multicenter study of the incidence and factors associated with redo Nissen fundoplication in children. Journal of pediatric surgery. 2013;48:1306-11.
- 114 - Mauritz FA, van Herwaarden-Lindeboom MY, Zwaveling S, Houwen RH, Siersema PD, van der Zee DC. Laparoscopic Thal fundoplication in children: a prospective 10- to 15-year follow-up study. Annals of surgery. 2014;259:388-93.
- 115 - Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). Journal of pediatric gastroenterology and nutrition. 2009;49:498-547.
- 116 - Bohmer CJ, Klinkenberg-Knol EC, Niezen-de Boer MC, Meuwissen SG. Gastroesophageal reflux disease in intellectually disabled individuals: how often, how serious, how manageable? The American journal of gastroenterology. 2000;95:1868-72.
- 117 - Del Giudice E, Staiano A, Capano G, Romano A, Florimonte L, Miele E, et al. Gastrointestinal manifestations in children with cerebral palsy. Brain & development. 1999;21:307-11.
- 118 - de Veer AJ, Bos JT, Niezen-de Boer RC, Bohmer CJ, Francke AL. Symptoms of gastroesophageal reflux disease in severely mentally retarded people: a systematic review. BMC gastroenterology. 2008;8:23.
- 119 - Kline AD, Moss JF, Selicorni A, Bisgaard AM, Deardorff MA, Gillett PM, et al. Diagnosis and management of Cornelia de Lange syndrome: first international consensus statement. Nature reviews Genetics. 2018;19:649-66.
- 120 - Singendonk MMJ, Brink AJ, Steutel NF, van Etten-Jamaludin FS, van Wijk MP, Benninga MA, et al. Variations in Definitions and Outcome Measures in Gastroesophageal Reflux Disease: A Systematic Review. Pediatrics. 2017; Jul 27 [Epub ahead of print].
Evidence tabellen
|
Quality assessment |
Summary of findings |
Importance |
||||||||||
|
No of patients |
Effect |
Quality |
||||||||||
|
No of studies |
Study design |
Risk of bias |
Inconsistency |
Indirectness |
Imprecision |
Baclofen |
Placebo |
|||||
|
BACLOFEN vs PLACEBO |
||||||||||||
|
Side-effects: AEs (number of adverse events) |
||||||||||||
|
1 |
RCT; parallel |
Serious1 |
N/A |
Serious2 |
Very serious3 |
15 |
15 |
Intervention vs placebo, total number of AEs: 5 vs 4.(35)a, 4,5 |
Very low |
Critical |
||
RCT = randomized controlled trial; N/A = not applicable, AE = adverse event.
- Reported events were: breathlessness , tiredness, nausea, sore nostril/throat.
- Allocation concealment and/or randomization process unclear. Not clear if personnel and participants were blinded. Measurement of symptoms up to 48h after each visit (in total n = 2 visits), but total duration of study not clear and not clear from what time-point the 48h were measured.
- Patients: Study in children only. Children with severe GERD were included, children were referred for further investigation who failed to improve after routine therapeutic measures (ie, parental reassurance, postural advice, feed thickeners, antacids, H2-antagonists, and proton pump inhibitors [PPIs]). Inclusion criteria not further specified.Intervention: One test dose of baclofen was given to assess toleration, second session performed > 72h after safety session. Study assesses only 2 doses of Baclofen. Outcome: methods and definitions of measurement of adverse events not predefined in methods section.
- Limited number of patients and events.
- Measured during and up to 48 hours after second visit. Symptoms after first visit not split out for intervention or placebo.
- Only total number of AEs reported, no data on number of AEs per patient.
|
Quality assessment |
Summary of findings |
Importance |
|||||||||
|
No of patients |
Effect |
Quality |
|||||||||
|
No of studies |
Study design |
Risk of bias |
Inconsistency |
Indirectness |
Imprecision |
Domperidone |
Placebo |
||||
|
DOMPERIDONE VS PLACEBO |
|||||||||||
|
Visible regurgitation/vomiting: % of patients vomiting at end of treatment |
|||||||||||
|
1 |
RCT; parallel |
Very serious1 |
N/A |
Not serious2 |
Very serious3 |
15 |
15 |
Data only provided in figure, no raw data provided. Authors report significant improvement of %patients vomiting in the domperidone vs placebo group (p<0.001). (36)* |
Very low |
Critical |
|
|
Side-effects: number of patients with AEs |
|||||||||||
|
2 |
RCT; parallel |
Very serious1,4 |
No |
Not serious5 |
Very serious3 |
0/35 |
0/35 |
RR = not estimable.(36)6(34) |
Very low |
Critical |
|
RCT = randomized controlled trial; RR = relative risk.
*As reported by study
- Allocation concealment and/or randomization process unclear. Not clear if personnel and participants were blinded. High chance of bias due to selective reporting. Groups not comparable at baseline.
- Patients: Study conducted in infants and children, no subanalysis performed according to age.
- Limited number of patients and events.
- In one study stratified and successive block randomization of patients. Therefore constrained randomization.
- Patients: Study conducted in infants and children, no subanalysis performed according to age. Intervention: All infants received additional treatments: fractionated feeding, thickened milk formulas for unweaned infants and positional management. All infants were treated with another dose of placebo administered 1 and 3 h after meals alongside domperidone and first dose of placebo. No downgrading was performed.
- RR not estimable as there were no events in both treatment arms.
|
Quality assessment |
Summary of findings |
Importance |
||||||||||
|
No of patients |
Effect |
Quality |
||||||||||
|
No of studies |
Study design |
Risk of bias |
Inconsistency |
Indirectness |
Imprecision |
Metoclopramide |
Placebo |
|||||
|
METOCLOPRAMIDE VS PLACEBO |
||||||||||||
|
Visible regurgitation/vomiting: % of patients vomiting at end of treatment |
||||||||||||
|
1 |
RCT; parallel |
Very serious1 |
N/A |
Not serious2 |
Very serious3 |
17 |
15 |
Data only provided in figure, no raw data provided. Authors report significant improvement of %patients vomiting in the metoclopramide vs placebo group (p<0.001).(36)* |
Very low |
Critical |
||
|
Side-effects: number of patients with AEs |
||||||||||||
|
2 |
RCT; cross-over |
Very serious4 |
N/A |
Not serious5 |
Very serious3 |
0/15 |
0/15 |
RR = not estimable.(37)6 |
Very low |
Critical |
||
|
1 |
RCT; parallel |
Very serious1 |
N/A |
Not serious2 |
Very serious3 |
0/17 |
0/15 |
RR = not estimable.(36)6 |
Very low |
Critical |
||
|
Side-effects: any AE leading to discontinuation |
||||||||||||
|
1 |
RCT; parallel |
Very serious1 |
N/A |
Not serious8 |
Very serious3 |
3/19 |
1/20 |
RR = 3.16 (95%CI = 0.36 - 27.78) (38) |
Very low |
Critical |
||
RCT = randomized controlled trial; SD = standard deviation; RR = relative risk; 95% CI = 95% confidence interval; N/A = not applicable.
*As reported by study
- Allocation concealment and/or randomization process unclear. Not clear if personnel and participants were blinded. High chance of bias due to selective reporting.
- Patients: Study conducted in infants and children, no subanalysis performed according to age.
- Limited number of patients and events.
- Allocation concealment and/or randomization process unclear. Not clear if personnel was blinded for outcome of investigations. High chance of bias due to selective reporting.
- No washout period between cross-over. Individual periods not reported so reanalysis could not be undertaken. No complete overview of baseline characteristics provided.
- Patients: Study conducted in infants and children, no subanalysis performed according to age. Intervention. Positioning or thickening of feeding, were kept constant during the pretreatment and both feeding periods. Not clear how many infants received conservative treatment. No downgrading was performed.
- RR not estimable as there were no events in both treatment arms.
- Patients: Study conducted in infants and children, no subanalysis performed according to age. Intervention. All patients received positional therapy. No other treatments for GERD allowed. No downgrading was performed. Outcome: ‘Triangular test’ (statistical approach) used on main endpoint, but no further specification provided on what authors define as the main endpoint.
|
Quality assessment |
Summary of findings |
Importance |
||||||||||
|
No of patients |
Effect |
Quality |
||||||||||
|
No of studies |
Study design |
Risk of bias |
Inconsistency |
Indirectness |
Imprecision |
Domperidone |
Metoclopramide |
|||||
|
DOMPERIDONE VS METOCLOPRAMIDE |
||||||||||||
|
Visible regurgitation/vomiting: % of patients vomiting at end of treatment |
||||||||||||
|
1 |
RCT; parallel |
Very serious1 |
N/A |
Not serious2 |
Very serious3 |
15 |
17 |
Data only provided in figure, no raw data provided. Authors report significant improvement of %patients vomiting in the domperidone vs metoclopramide group (p<0.05).(36)* |
Very low |
Critical |
||
|
Side-effects: number of patients with AEs |
||||||||||||
|
1 |
RCT; parallel |
Very serious1 |
N/A |
Not serious2 |
Very serious3 |
0/15 |
0/17 |
RR = not estimable.(36)4 |
Very low |
Critical |
||
RCT = randomized controlled trial; RR = relative risk.
*As reported by study
- Allocation concealment and/or randomization process unclear. Not clear if personnel and participants were blinded. High chance of bias due to selective reporting.
- Patients: Study conducted in infants and children, no subanalysis performed according to age.
- Limited number of patients and events.
- RR not estimable as there were no events in both treatment arms.
|
Farmacologische therapie |
||||||||||||||||||||||||||
|
Author |
Design |
Population |
Cochrane Risk of Bias Tool |
Dure |
Intervention |
Control |
Outcome of interest |
Outcome measures |
||||||||||||||||||
|
|
|
N |
Age |
Inclusion |
Random sequence generation |
Allocation concealment |
Blinding intervention |
Blinding outcome |
Selective reporting |
Follow-up |
|
|
|
|
|
|||||||||||
|
ANTACID VS PLACEBO |
||||||||||||||||||||||||||
|
Miller (1999) (25) |
RCT; parallel |
90 |
4 ± 0.28 mo (3.9 ± 0.40 vs 4.1 ± 0.39) |
Persistent , unmanageable vomiting/regurgitation or vomiting/regurgitation >2x day for 2 days prior to the start of the study |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
68/90 |
14 d |
Sodium alginate (225mg sodium alginate and magnesium alginate 87.5mg) in a total 0.65g. One sachet/day (<4.54kg) or two sachet/day (>4.54kg) (n=42) |
Matching placebo (n=48) |
Visible regurgitation/vomiting: Number of vomiting/regurgitation episodes in 24 hours, intervention vs control (medians): Baseline; 8.5 (2-50) vs 7.0 (2-36) 14 days: 3.0 (0-22) vs 5.0 (0-37)
Mean number of episodes, SD not reported (intervention vs control group) Baseline: 10.2 vs 10.6 Wk 2: 10.6 vs 6.2, p = 0.056
Side effects - AEs AE: 57% of patients >1 AE (55% vs 59%) . Withdrawal from study because of AE: 4/42 vs 7/46. SAE: 2/42 vs 2/46 (not related to treatment). No statistically significant differences in the incidence of these adverse events were observed between treatment groups (p>0.1 in all cases).
|
Frequency/cessation of regurgitation, patient reported improvement, safety analysis |
|||||||||||
|
ANTACID + SIMETHICONE VS NON-PHARMACOLOGICAL INTERVENTION (Feed thickeners/conservative treatment) |
||||||||||||||||||||||||||
|
Ummarino (2015) (18) |
RCT; parallel |
75 |
1-12 mo |
Infant regurgitation according to ROME III |
Yes |
Not clear |
Not clear |
Yes |
Yes |
67/75 |
8 wk |
Magnesium alginate aluminum-free formulation plus simethicone, 2.5mL 3x/day (weight <5kg) or 5mL 3x/day (weight >5 kg), 10 minutes after feeding + conservative therapy (A, n=25) |
Rice starch thickened (14.3g/100ml or 14.2g100ml for infants < 6 mo) + conservative therapy (A, n=25) Conservative therapy (=life style changes + reassurance) (A, n=25) |
I-GERQ-R scores Symptom scores, A vs B vs C Baseline: 15 (8-24) vs 13 (8-19) vs 13 (7-10), p = 02 Wk 4: 7 (1-20) vs 10 (5-16) vs 12 (7-14), p = 0.2 Wk 8: 1 (0-19) vs 5 (0-15) vs 8 (2-14), p =0.01
Median I-GERQ-R scores significantly lower in all groups (A p<0.002, B p<0.038, C p<0.03) at week 8 compared to baseline. No comparison between groups at week 8. Median I-GERQ-R scores more significantly reduced in intervention group vs control group (A vs B p<0.002, A vs C p<0.0001). (no subscores provided)
Visible regurgitation/vomiting Number of infants with regurgitation and vomiting, intervention vs thickened formula vs conservative treatment: Baseline = 25/25 vs 25/25 vs 25/25 4 wk = 21/25 vs 25/25 vs 17/17 8 wk = 6/24 vs 13/23 vs 15/17
Side effects (reported in diary) No SAEs reported. AEs: 1/25 patients in group A presented with constipation |
I-GERQ-R scores, <7 no clinical symptoms Side effects reported in diary |
|||||||||||
|
AE = adverse event; CI = confidence interval; GER = gastroesophageal reflux; GERD = GER disease; I-GERQ-R = infant gastroesophageal reflux questionnaire revised; MD = mean difference; MDchange = change in mean difference; NS = not significant; PPI = proton pump inhibitor; RCT = randomized controlled trial; RI = reflux index; RR = relative risk; SAE = serious adverse event. |
||||||||||||||||||||||||||
Author |
Design |
Population |
Cochrane Risk of Bias Tool |
Dure |
Intervention |
Control |
Outcome of interest |
Outcome measures |
|
||||||||||||||||||||||
|
|
|
N |
Age |
Inclusion |
Random sequence generation |
Allocation concealment |
Blinding intervention |
Blinding outcome |
Selective reporting |
Follow-up |
|
|
|
|
|
|
|||||||||||||||
|
LANSOPRAZOLE |
|
||||||||||||||||||||||||||||||
|
Orenstein (2009) (26) |
RCT; parallel |
162 |
16, 4-51 wks |
Infants with symptomatic GERD who remained symptomatic with crying, fussing or irritability during/within 1 hour after feeding despite at least 1 wk conservative non-pharmacologic management (1-2 wks before randomization) |
Yes |
Yes |
Yes |
Not clear |
Yes |
96/162 |
4 wks |
Lansoprazole 0.2-0.3mg/kg day for infants ≤10 wks and 1.0-1.5mg/kg/day for infants >10 wks (n=49) |
Placebo formulated identically dosed comparably (n=47) |
Side effects – (S)AEs Intervention vs control AE: 50 (62%); (46%); p = 0.058 SAE: 10 (12%); 2 (2%); p = 0.032
Crying/distress Intervention vs control - Percentage of feeds Baseline: 51.0 ± 20.39 vs 52.4 ± 20.46 4 wk: 31.0 ± 25.41 vs 32.4 ± 28.13 Change: -19.9 ± 23.10 vs -19.9 ± 23.83 (p=0.794)
- Mins postfeed Baseline: 7.9 ± 6.05 vs 9.0 ± 7.25 4 wk: 4.3 ± 5.52 vs 4.9 ± 6.20 Change: -3.6 ± 5.4 vs -4.1 ± 6.63 (p=0.830)
Mins/ day Baseline: 47.0 ± 37.30 vs 55.4 ± 46.11 4 wk: 22.1 ± 29.96 vs 27.6 ± 36.57 Change: -25.0 ± 31.86 vs -27.8 ± 41.41 (p=0.963)
Visible regurgitation/vomiting: % of feeds with regurgitation per wk Mean (ie, averaged across infants) change from pretreatment baseline, intervention vs control group: -14% vs -10% (NS) |
Primary endpoint: efficacy scores (not assessed by I-GERQ-R), total scores and individual domains |
|
|||||||||||||||
|
ESOMEPRAZOLE |
|
||||||||||||||||||||||||||||||
|
Loots (2014) (27) |
RCT; parallel |
57 |
13.6 (2-26) wks |
GERD symptoms > 5 days or increasing in frequency or severity for 3 days |
Yes |
Not clear |
No |
Not clear |
Yes |
51/57 |
2 wks |
Esomeprazole 1mg/kg/day 1x/day 2 hrs postprandially (all infants received positioning therapy, ie LLP or head of cot elevation to 20 degrees; (HE)n=12 in LLP, n=14 in HE) |
Antacid Mylanta, 1.5 (0-2mo), 3 (2-4 mo) or 6mL (4-6mo) once daily (all infants received positioning therapy, ie LLP or head of cot elevation to 20 degrees; n=13 in LLP, n=12 in HE) |
Crying/distress - In infants in LLP, PPI vs AA 1. Total crying time (mins) Baseline: 92 ±24.2 vs 106 ± 68.5 2 wk: 92 ± 34.6 vs 88 ± 36.1 (difference: -1 ± 24.2 vs -17 ± 64.9) 2. No of cry Baseline: 48 ± 31.2 vs 60 ± 43.3 2 wk: 48 ± 27.7 vs 54 ± 32.4 (difference: 5 ± 17.3 vs -7 ± 46.9)
- In infants in HE, PPI vs AA 1. Total crying time (mins) Baseline: 71 ± 41.2 vs 74 ± 69.4 2 wk: 81 ± 37.4 vs 66 ± 45.0 (difference: 9 ± 37.7 vs -8 ± 45.0) 2. No of cry Baseline: 30 ± 26.2 vs 38 ± 34.6 2 wk: 49 ± 26.2 vs 35 ± 24.2 (difference: 17 ± 37.4 vs -5 ± 34.6)
Side effects – AEs 5 AEs (not specified what treatment arm) 2 SAEs in PPI + HE group: 1 hospital admission for rota virus 1 hospital admission for reduced oral intake + weight loss |
I-GERQ-R GER monitoring (pH-MII) Gastric emptying Physiological monitoring |
|
|||||||||||||||
|
Davidson (2013) (28) |
RCT; parallel |
52 |
48.1 ± 29.8 vs 46.5 ± 31.2 days |
Suspected of having any two of (after 8h video monitoring): apnea with or without bradycardia and with or without oxygen desaturations, vomiting or gagging, and irritability or pain >1x every second feed or >2x in 8 hours |
Yes |
Yes |
Not clear |
Not clear |
No |
51/52 |
2 wks |
Esomeprazole 0.5mg/kg in 2ml/kg of sodium bicarbonate solution (n=25) |
Placebo, not further specified, 0.5mg/kg in 2ml/kg of sodium bicarbonate solution (n=26) |
Crying/irritability No of events, intervention vs control Baseline: 88.87 ± 24.71 vs 89.46 ± 22.71 2 wk: 88.83 ± 19.84 vs 88.85 ± 20.18 Change from baseline: -0.05 ± 17.27vs -0.61 ± 22.85
Side effects – AEs Intervention group: 6 patients experienced 10 AEs, no SAEs Placebo group: 9 patients experienced 14 AEs, 4 SAEs
Visible regurgitation/vomiting: Number of vomiting, Mean ± SD, intervention vs control group: Baseline: 5.79 ± 7.14 vs 4.17 ± 4.31 2 wk: 5.21 ± 6.75 vs 4.87 ± 5.93
Mean difference at 2 wks: MD: 0.34 (95%CI -3.15 - 3.83) MDchange: -1.28 (95%CI -4.42 - 1.86) |
Change from baseline in total GERD symptoms (video recording) and GERD-related signs (cardiorespiratory monitoring. Secondary: mean difference in change of signs and symptoms, pH-metry, adverse events, laboratory assessment |
|
|||||||||||||||
|
Winter (2012) (29) |
RCT; parallel |
80 |
4.9 ± 2.6 vs 4.9 ± 3.2 mo |
GERD suspected based on symptoms or endoscopically proven. >1 of symptoms of (extra-esophageal) GERD (vomiting/regurgitation, irritability, [cough, wheezing and/or stridor, labored breathing], respiratory symptoms triggered by feeding, feeding difficulties [food refusal, gagging/ choking, hiccups for >1 hour/day]) > 2x/wk in 4-wks |
Yes |
Not clear |
Yes |
Not clear |
Yes |
77/80 |
4 wks |
Esomeprazole 2.5mg (weight 3-5kg), 5mg (weight 5-7.5kg), 10mg (weight 7.5-12kg) once a day (n= 39) |
Placebo, sachets containing inactive granulate dissolved into water (n=41) |
Crying/irritability Mean (SD) change from baseline in symptom score. Esomeprazole vs placebo: 0.06 ± 0.58 vs 0.19 ± 0.59 (no mean scores provided)
Visible regurgitation/vomiting: Severity score (0-3, 3 = most severe). Mean ± SD, change from baseline in symptom score, intervention vs control group: 0.04 ± 0.56 vs 0.09 ± 0.61.
Change in mean difference at 4 wks: MDchange: = -0.13 (95%CI -0.39 – 0.13)
Side effects – (S)AEs Esomeprazol vs placebo: AE: 23/39 vs 27/41 patients, NS SAE: 4/39 vs 1/41 |
Time from randomization to discontinuation Treatment success Daily symptoms PGA symptom severity Safety and tolerability |
|
|||||||||||||||
|
RABEPRAZOLE |
|
||||||||||||||||||||||||||||||
|
Hussain (2014) (30) |
RCT; parallel |
268 |
4.7 ± 2.54 vs 4.7 ± 2.65 mo |
GERD: recurrent vomiting or regurgitation in infants unresponsive to conservative interventions, and >1 of: poor weight gain as defined by failure to thrive; irritability, excessive crying, or disturbed sleep, or refusal to eat even if hungry, or arching back at meals. During screening, score >16 on I-GERQ-R within 6 days of the first dose |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
231/268 |
5 wks |
Rabeprazole 5mg/day (A, n=90) or 10mg/day (B, n=88) |
Placebo (C, n=178) |
I-GERQ-R score Data only displayed in figure, insufficient information to calculate manually. No data on subscores.
Side effects – AEs Intervention vs control AE: no infants > 1 TEAE reported: 47% vs 47% SAE: 4.5% vs 2.2% infants SAE
Visible regurgitation/vomiting: |
- Frequency of regurgitation - Weight for age z-score - I-GERQ-R weekly score - I-GERQ-R daily score - Adverse events |
||||||||||||||||
|
OMEPRAZOL |
|
||||||||||||||||||||||||||||||
|
Zohalinezhad (2015)(25) |
RCT; parallel |
89 |
0-18 yrs
67.66 (7-216) mo. |
At least two of the following symptoms at least for one month, without improvement with routine treatments:
Also, patients with endoscopic results that proved GERD |
Yes |
Yes |
Yes |
Yes |
Yes |
79/89 |
7 wks |
Omeprazole (syrup) 1 ml/kg/day |
Quince syrup 0,6 ml/kg/day |
Composed clinical score (by authors).
Questionnaires to assess frequency and severity of symptoms: 1-11 mo. GSQ-I 1-4 yr. GSQ-YC 5-18 yr. GASP-Q
Parents indicated the frequency of the symptoms and rate them from 1 (not too severe) – 7 (very severe)
Safety via AEs and physical examination, laboratory determinations and vital sign measurements
|
Infants and young children (<60 months)
Visible vomiting/regurgitation Omeprazole vs Quince, individual symptom scores ± (SD) Baseline: 18.87 ± (49.50) vs 18.33 ± (34.92) 4 wks: 6.50 ± (24.43) vs 5.14 ± (12.81) 7 wks: 6.38 ± (24.44) vs 2.36 ± (6.70)
Irritability Omeprazole vs Quince, individual symptom scores ± (SD) Baseline: 14.12 ± (19.80) vs 18.09 ± (41.10) 4 wks: 12.93 ± (24.95) vs 10.21 ± (25.70) 7 wks: 16.33 ± (38.08) vs 2.97 ± (9.59)
Older children and adolescences (60-216 mo.)
Visible vomiting/regurgitation Omeprazole vs Quince, individual symptom scores ± (SD) Baseline: 1.95 ± (3.90) vs 1.77 ± (3.20) 4 wks: 0.67 ± (1.71) vs 3.06 (11.48) 7 wks: 2.04 ± (10.00) vs 0.02 ± (0.09)
Irritability Omeprazole vs Quince, individual symptom scores ± (SD) Baseline: 27.04 ± (59.20) vs 10.05 ± (26.20) 4 wks: 9.36 ± (25.26) vs 1.04 ± (1.94) 7 wks: 0.00 vs 0.17 ± (0.53)
Chest pain/heartburn Omeprazole vs Quince, individual symptom scores ± (SD) Baseline: 4.30 ± (6.96) vs 21.94 ± (35.92) 4 wks: 1.81 ± (7.08) vs 3.15 ± (8.25) 7 wks: 5.87 ± (22.80) vs 3.49 ± (7.07) |
|
|||||||||||||||
|
Moore (2003) (31) |
RCT; cross-over |
34 |
5.4 ± 2.1 mo |
Significant GER, RI>5% or esophagitis |
Not clear |
Not clear |
Yes |
Not clear |
Yes |
30/34 |
4 wks |
Omeprazole 10mg 1x/day (5-10kg) or 10mg 2x/day (>10kg) |
Placebo identical appearance to omeprazole |
Crying/distress Intervention vs control, Period 1 after 2 wks, period 2 after 4 wks (no wash-out period between treatments)
1. Cry/fuss mins per 24 hours - Baseline: 246 ±105 vs 287 ± 132 (p=0.481) - Period 1: 203 ± 113 vs 204 ± 87 (p=0.604) - Period 2: 179 ± 129 vs 198 ± 115 (p=0.534)
Independent from treatment, baseline vs period 1, p=0.040 and vs period 2, p=0.008
2. VAS for irritability - Baseline: 7.1 ± 1.4 vs 6.6 1.7 (p=0.262) - Period 1: 5.9 ± 2.6 vs 6.0 ± 2.1 (p=0.724) - Period 2: 4.0 ± 3.3 vs 5.7 ± 2.2 (p=0.105)
Independent from treatment, baseline vs period 2, p=0.008, vs period 1 p=NS)
Side effects – AEs No AEs encountered |
Infant behavior monitored by Barr diary and VAS |
|
|||||||||||||||
|
PANTOPRAZOL |
|
||||||||||||||||||||||||||||||
|
Winter (2010) (32) |
RCT; parallel |
106 |
5.15 ± 2.81 vs 5.04 ± 2.81 mo |
I-GERQ-R > 16 at screening and baseline and a clinical diagnosis of suspected, symptomatic or endoscopically proven GERD |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
86/106 |
4 wks |
Pantoprazole 1.2mg/kg/day (5 mg/day for infants 2.5-7 kg, or 10 mg/day for infants 7-15 kg) |
Placebo, not further specified |
Crying/distress Mean (SD) change from base line vs wk 4 Intervention group vs control group -0.39 ± 0.58 (p<0.001 vs baseline) vs -0.55 ± 0.55 (p<0.001 vs baseline)
Mean (SD) change from base line vs wk 8 Intervention group vs control group -0.49 ± 0.57 (p<0.001 vs baseline) vs -0.64 ± 0.72 (p<0.001 vs baseline) (no baseline and end of treatment scores provided)
Visible regurgitation/vomiting: Number of vomiting, Mean ± SD, change from base line vs wk 4, intervention vs control group: -0.45 ± 0.68 (p<0.001 vs baseline) vs -0.41 ± 0.52 (p<0.001 vs baseline. Mean ± SD, change from base line vs wk 8 intervention vs control group: -0.62 ± 0.72 (p<0.001 vs baseline) vs -0.48 ± 0.87 (p<0.001 vs baseline)
Change in mean difference at 4 wks: MDchange : -0.04 (95% CI -0.27 - 0.19)
Change in mean difference at 8 wks: MDchange : -0.14 (95% CI -0.44 - 0.16)
Side effects – (S)AEs Data on AEs not sufficient, only AEs described reported in >3% of patients, so no total numbers provided
SAE: 8 patients had 1 or 2 serious AEs during the study, of which 5 occurred during treatment with pantoprazole (all considered treatment unrelated) |
Withdrawal rate due to lack of efficacy, frequency of GERD symptoms, safety via AEs |
|
|||||||||||||||
|
OMEPRAZOL VS RANITIDINE |
|
||||||||||||||||||||||||||||||
|
Azizollahi (2016) (28) |
RCT; parallel |
76 |
2-12 mo. |
Infants with a GSQ of more than 16 at screening and baseline, and remain symptomatic after receiving 2 weeks of standard treatment of GERD |
Yes |
Yes |
Not clear |
Not clear |
Yes |
60/76 |
2 wks |
Omeprazole capsule 0,5 mg/kg/day (n=30) |
Ranitidine syrup 2-4 mg/kg/day (n=30) |
Daily form with questions completed bij parents, assessing the frequency of five key GERD symptoms:
Physical examinations at study visits
Safety via AE reported by parents |
Visible vomiting/regurgitation Omeprazole vs Ranitidine, change from baseline. 1 wk: 21.74-32.21 vs 17.25-24.53 2 wks: 5.01-11.15 vs 7.5-13.6 (P=0.019) No baseline scores provided.
Crying/irritability Omeprazole vs Ranitidine, change from baseline. 1 wk: 7.8-12.8 vs 8.20-14.32 2 wks: 1.8-6.5 vs 2.5-6.8 No baseline scores provided
AE No AEs were reported |
|
|||||||||||||||
|
Ummarino, 2012 |
RCT; parallel |
35 |
40.6 ± 36.4 mo |
GERD based on impact of symptoms on general well-being of the children and pH-MII results (SI>50% and SAP>95%); infants with manifestations of extra-esophageal GERD |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
35/35 |
1 yr |
Omeprazole 1.4mg/kg/day (n=19) |
Ranitidine 15mg/kg/day (n=16) |
Crying/distress Symptom score irritability (score 0-3, 3 = most severe) Intervention vs control Baseline: 0.84 ± 2.19 vs 0.81 ± 1.77 3 mo: 0.16 ± 0.69 vs 0.25 ± 1 (p=0.6 between groups after therapy)
Chest pain Symptom score (score 0-3, 3 = most severe) Mean ± SD, intervention vs control group: Baseline: 0.68 ± 20.06 vs 0.56 ± 2.25 3 mo: 0.05 ± 0.23 vs 0.56 ± 2.25 (p=0.01 between groups after therapy)
Mean difference at 3 mo: MD: -0.51 (95%CI -1.62 – 0.60)
Side effects – AEs No adverse events of treatment were reported |
Remission of symptoms, not further specified in methods |
|
|||||||||||||||
|
Cucchiara, 1993 |
RCT; parallel |
32 |
6 mo – 13.4 yrs |
GOR based on 24h pH monitoring and endoscopy with histology, unresponsive to an antireflux treatment |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
25/32 |
8 wks |
Omeprazole 40mg/day (n=13) |
Ranitidine 20mg/kg/day (n=12) |
Endoscopy/histology: Healing of esophagitis (score A – E; E = most severe; healing is return to score A or B) intervention vs control: 9/13 vs 9/12 |
Clinical score for GERD, pH-metry, endoscopy with histology |
|
|||||||||||||||
|
ESOMEPRAZOLE VS ANTACID |
|
||||||||||||||||||||||||||||||
|
Loots, 2014 |
RCT; parallel |
57 |
13.6 (2-26) wks |
GERD symptoms > 5 days or increasing in frequency or severity for 3 days |
Yes |
Not clear |
No |
Not clear |
Yes |
51/57 |
2 wks |
Esomeprazole 1mg/kg/day 1x/day 2 hrs postprandially (n=12 in LLP, n=14 in HE) |
Antacid, 1.5 (0-2mo), 3 (2-4 mo) or 6mL (4-6mo) once daily (n=13 in LLP, n=12 in HE) |
Crying/distress - In infants in LLP, PPI vs AA 1. Total crying time (mins) Baseline: 92 ±24.2 vs 106 ± 68.5 2 wk: 92 ± 34.6 vs 88 ± 36.1 (difference: -1 ± 24.2 vs -17 ± 64.9) 2. No of cry Baseline: 48 ± 31.2 vs 60 ± 43.3 2 wk: 48 ± 27.7 vs 54 ± 32.4 (difference: 5 ± 17.3 vs -7 ± 46.9)
- In infants in HE, PPI vs AA 1. Total crying time (mins) Baseline: 71 ± 41.2 vs 74 ± 69.4 2 wk: 81 ± 37.4 vs 66 ± 45.0 (difference: 9 ± 37.7 vs -8 ± 45.0) 2. No of cry Baseline: 30 ± 26.2 vs 38 ± 34.6 2 wk: 49 ± 26.2 vs 35 ± 24.2 (difference: 17 ± 37.4 vs -5 ± 34.6)
Side effects – AEs 5 AEs (not specified what treatment arm) 2 SAEs in PPI + HE group: 1 hospital admission for rota virus 1 hospital admission for reduced oral intake + weight loss |
I-GERQ-R GER monitoring (pH-MII) Gastric emptying Physiological monitoring |
|
|||||||||||||||
|
LANSOPRAZOLE VS FEED INTERVENTION |
|
||||||||||||||||||||||||||||||
|
Khoshoo, 2007 |
RCT; parallel |
45 |
4.8 ± 1.18 vs 4.3 ± 1.01 vs 4.6 ± 0.99 mo (A vs B vs C) |
Patients referred to pediatric gastroenterology clinic for evaluation and treatment of GERD, I-GERQ-R scores > 16 for 1 wk |
Not clear |
Not clear |
No |
No |
Yes |
45/45 |
2 wks |
Lansoprazole 15mg once a day (A, n=15) or 7.5mg twice a day (B, n=15) |
Extensively hydrolyzed formula (C, n=15), no placebo provided |
I-GERQ-R scores Mean ± SD, Group A vs Group C Baseline: 26.6 ± 2.8 vs 25.9 ± 3.3 2 wks: 20.6 ± 4.2 vs 25.8 ± 3.2 (no subscores provided)
Mean ± SD, Group B vs Group C 2 wks: 20.0 ± 3.3 vs 25.8 ± 3.2
Side effects – AEs - No clinical adverse reactions, no drop=outs |
No other outcome measures assessed |
|
|||||||||||||||
|
AE = adverse event; CI = confidence interval; GER = gastroesophageal reflux; GERD = GER disease; HE = head elevation; I-GERQ-R = infant gastroesophageal reflux questionnaire revised; LLP = left lateral position; MD = mean difference; MDchange = change in mean difference; NS = not significant; PPI = proton pump inhibitor; RCT = randomized controlled trial; RI = reflux index; RR = relative risk; SAE = serious adverse event; SI = symptom index; SAP = symptom association probability; VA =visual analogue |
|
||||||||||||||||||||||||||||||
|
Author |
Design |
Population |
Cochrane Risk of Bias Tool |
Dure |
Intervention |
Control |
Outcome of interest |
Outcome measures |
|
||||||||||||||||||||||||||||||
|
|
|
N |
Age |
Inclusion |
Random sequence generation |
Allocation concealment |
Blinding intervention |
Blinding outcome |
Selective reporting |
Follow-up |
|
|
|
|
|||||||||||||||||||||||||
|
RANITIDINE |
|
||||||||||||||||||||||||||||||||||||||
|
Orenstein (2002) (33) |
RCT; parallel |
29 |
9.0 (4-11) (8.0 (4-11) vs 9.0 (7-11)) mo |
Infants with a history of acid reflux symptoms over the previous 3 mo |
Not clear |
Not clear |
Not clear |
Not clear |
No |
29/29 |
6h |
Ranitidine 75 mg, single dose (n=19) |
Placebo, not further specified, single dose (n=10) |
Side effects – AEs 12 patients experienced a total of 15 AEs. Ranitidine vs control: AEs: 12/19 patients vs 0/10 patients (timepoint not clear) |
Pharmacokinetics and dynamics, Safety analysis |
|
|||||||||||||||||||||||
|
CIMETIDINE |
|
||||||||||||||||||||||||||||||||||||||
|
Cucchiara (1989) (34) |
RCT; parallel |
37 |
21.7 ± 37.65 vs 29.03 ± 39.73 mo |
Established peptic reflux esophagitis, 18-24h intraesophageal pH monitoring, a drop of the distal esophageal pH <4.00 for >20 seconds |
Not clear |
Not clear |
Yes |
Not clear |
Yes |
32/37 |
12 wks |
Cimetidine - 30 to 40 mg/kg/day three time a day after meals for 12 wks (n=17) |
Placebo - 30 to 40 mg/kg/day three time a day after meals for 12 wks (n=15) |
Histologic/endoscopic healing Cimetidine vs placebo
Histological score (score 0-9; 9 = most severe) Baseline: 6.35 +/- 2.78 vs 6.80 +/- 2.88 (p<0.01) 12 wks: 1.6 +/- 2.43 vs 5.43 +/- 3.81 (NS)
Esophagitis (score mild-severe) Mild or moderate esophagitis: improved or healed: 9/9 vs 4/7(unchanged 3/7)
Severe esophagitis: improved or healed: 7/8 vs 2/8 (unchanged or worsened 1/8 vs 6/8)
Side effects – AEs No adverse events were reported
|
Clinical score, histological score, endoscopic healing |
|
|||||||||||||||||||||||
|
NIZATIDINE |
|
||||||||||||||||||||||||||||||||||||||
|
Simeone (1997) (35) |
RCT; parallel |
26 |
2.08 (0.5- 12) vs 1.16 (0.5- 9.5) yrs
|
Patients with reflux esophagitis |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
24/26 |
8 wks |
Nizatidine 1 0mg/kg in a tablet of 150mg (n=13) |
Matching placebo (n=13) |
Histologic/endoscopic healing Esophagitis score (score 0-5; 5 = most severe) Nizatidine vs Placebo: Patients ‘cured’ based on endoscopy: 9/12 vs 2/13
Histologic improvement: 2/12 vs 3/13 Histologic unchanged: 1/12 vs 6/13 Histologic worsened: 0/12 vs 1/13.
Heartburn Chest pain, pyrosis symptom score (score 0-3; 3 = most severe) intervention vs control Baseline: 2.3 ± 1.2 vs 2.2 ± 0.8 4 wks: 1.7 ± 1.1 vs 1.8 ± 0.8 (p<0.01 in intervention group compared to baseline, placebo NS) 8 wks 1.0 ± 1.7 vs1.6 ±0.9 (p<0.01 in intervention group compared to baseline, placebo NS))
Visible regurgitation/vomiting: Frequency score (score 0-3; 3 = most severe)severity of regurgitation, Mean ± SD, intervention vs control group: Baseline: 2.4 ± 1.0 vs 2.5 ± 0.8 4 wks: 1.3 ± 1.1 vs 2.2 ± 1.3 (NS compared to baseline for placebo and intervention group) 8 wks: 0.3 ± 1.7 vs 1.7 ± 1.4 (p<0.01 in intervention group compared to baseline, placebo NS))
Mean difference at 4 and 8 wks: MD 4 wks : -0.90 (95%CI -1.86 - 0.06) MD 8 wks : -1.40 (95%CI -2.29 - -0.51)
Severity of vomiting (score 0-3; 3 = most severe) Mean ± SD, intervention vs control group: Baseline: 2.4 ± 0.7 vs 2.6 ± 0.5 4 wks: 0.8 ± 0.9 vs 2.1 ± 1.1 (p<0.01 in intervention group compared to baseline, placebo NS) 8 wks: 0.4 ± 0.7 vs1.6 ± 1.9 (p<0.01 in intervention and placebo group compared to baseline)
Mean difference at 4 and 8 wks: MD 4 wks : -1.30 (95%CI -2.10 - -0.50) MD 8 wks : -1.20 (95%CI -2.24 - -0.16)
Crying/distress Abdominal colic (for infants) Mean ± SD, intervention vs control group: Baseline: 2.7 ± 0.5 vs 2.7 ± 0.5 4 wks: 1.4 ± 1.1 vs 2.2 ± 1.0 (p<0.01 in intervention group compared to baseline, placebo NS) 8 wks: 0.7 ± 1.2 vs 1.6 ± 1.1 (p<0.01 in intervention group compared to baseline, placebo NS)) MD 4 wks : -0.80 (95%CI -1.64 – 0.04) MD 8 wks : -0.90 (95% CI -1.82 – 0.02) |
pH-metry, parental daily diary, endoscopy |
|
|||||||||||||||||||||||
|
H2RA vs Alginate-antacid |
|
||||||||||||||||||||||||||||||||||||||
|
Oderda (1990) (36) |
RCT; parallel |
49 |
10 (2-15.5) vs 7.9 (2-15.8) yrs |
Children with peptic esophagitis, > grade III or when grade I or II was seen esophagitis had to be histologically confirmed |
Not clear |
Not clear |
Not clear |
Not clear |
No |
47/49 |
6 mo |
Famotidine 1mg/kg before supper at 7 or 8 pm (n= 25) |
Alginate-antacid mixture, 30min after each meal and at bedtime (0.5gr alginic acid, 0.1gr allumium hydroxide, 0.025gr magnesium trisilicate and 0.17gr sodium bicarbonate)(n=24) |
Histologic/endoscopic healing Famotidine vs alginate-antacid
Endoscopy (score 1-3; 3 = most severe): Healed: 10/24 vs 10/23 Improved: 8/24 vs 3/23 Unchanged: 5/24 vs 10/23 Worsened: 1/14 vs 0/23
Histology (mild – severe): Healed: 17/24 vs 12/23 (p<0.001 between groups) Improved: 2/24 vs 6/23 Unchanged: 3/24 vs 3/23 Worsened: 2/24 vs 2/23 |
Histologic/endoscopic healing, no other outcome measures |
|
|||||||||||||||||||||||
|
Cucchiara (1984) (37) |
RCT; parallel |
33 |
8.9 (2-34) vs 9.4 (2-42) mo |
History suggesting GER, shown by radiology (positive if >2 episodes of reflux at fluoroscopy) and acid reflux test (Tuttle test, pH drop <4 for >20 sec). GERD confirmed by endoscopy (esophagitis) |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
29/33 |
12 wks |
Cimetidine syrup (20 mg/kg/day ) (n=17) |
liquid magnesium hydroxide and aluminum hydroxide in a dose of 700 mmol (mEq)/1 -73 ml/day, one and three hours after meals, and at bedtime. (n=16) |
Endoscopic/histologic healing Symptom scores (score mild – severe), Cimetidine vs antacid Baseline: 8.14 ± 2.17 vs 8.2 ± 2.39 12 wks: 3.21 ± 3.80 vs 3.4 ± 3.18 (wk 12 vs baseline in both groups p<0.01) (no data on |
Clinical, pH-metry and endoscopic assessment |
|
|||||||||||||||||||||||
|
H2RA vs Sucralfate |
|
||||||||||||||||||||||||||||||||||||||
|
Martin (1989) (38) |
RCT; parallel |
75 |
6.1 ± 3.6 yrs |
Gastroesophageal reflux symptoms and radiological diagnosis of reflux according to Cleveland criteria, and/or esophageal scintiscanning with a reflux index of >2.5% and endoscopic diagnosis of reflux esophagitis |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
75/75 |
8 wks |
Cimetidine dissolved in water in two doses, daily dose 20mg/kg |
1. Sucralfate tablets (<6 yrs: 0.5g 4x day, >6 yrs 1.0g 4x day) one half hour before meals and at bedtime 2. Sucralfate suspension (same dose and scheme) |
Endoscopic/histologic healing: Cimetidine vs sucralfate tablets vs sucralfate suspension: Healed: 14/25 vs 14/25 vs 15/25 Improved: 7/25 vs 7/25 vs 7/25 Without change/worsened: 4/25 vs 4/25 vs 3/25. (no baseline scores provided; criteria for healing/improving not further specified)
Adverse events: No adverse events reported by any of subjects. |
Symptoms during the treatment, symptoms not further specified, no baseline data provided on symptom breakdown, no validated scoring tool used. |
|
|||||||||||||||||||||||
|
H2RA vs Feed intervention |
|
||||||||||||||||||||||||||||||||||||||
|
Famouri (2017) (34) |
RCT |
50 |
< 1 yr
(2.8 ± 2.5 vs. 3.4 ± 1.8 mo.) |
Infants and children with suspected GERD
I-GERQ-R score of >7 |
Not clear |
Not clear |
Not clear |
Not clear
|
Yes |
50/50 |
2 wk |
Ranitidine 6 mg/kg daily in two divided doses |
Hypoallergenic diet: a diet free oof milk and dairy products, cow’s meat, penut, fish and soy |
Symptoms were evaluated and recorded by a pediatrician at baseline and after intervention to determine the outcome of intervention.
Symptoms were:
|
Vomiting Ranitidine vs. Hypoallergenic Diet. Baseline: 25/25 vs. 25/25 2 wks: 19/25 vs. 19/25 (p=0.01)
Irritability Ranitidine vs Hypoallergenic Diet. Baseline: 23/25 vs 18/25 2 wks: 21/25 vs 15/25 (P<0.05)
|
|
|||||||||||||||||||||||
|
AE = adverse event; CI = confidence interval; GER = gastroesophageal reflux; GERD = GER disease; I-GERQ-R = infant gastroesophageal reflux questionnaire revised; MD = mean difference; MDchange = change in mean difference; NS = not significant; PPI = proton pump inhibitor; RCT = randomized controlled trial; RI = reflux index; RR = relative risk; SAE = serious adverse event |
|
||||||||||||||||||||||||||||||||||||||
|
Author |
Design |
Population |
Cochrane Risk of Bias Tool |
Dure |
Intervention |
Control |
Outcome of interest |
Outcome measures |
|||||||||||||||||||||||||||||||
|
|
|
N |
Age |
Inclusion |
Random sequence generation |
Allocation concealment |
Blinding intervention |
Blinding outcome |
Selective reporting |
Follow-up |
|
|
|
|
|
||||||||||||||||||||||||
|
BACLOFEN |
|||||||||||||||||||||||||||||||||||||||
|
Omari (2006) (39) |
RCT; parallel |
30 |
11.0 ± 1.0 vs 9.1 ± 1.1 yrs |
Severe GERD, infants referred for further investigation who failed to improve after routine therapeutic measures (ie, parental reassurance, postural advice, feed thickeners, antacids, H2RAs, PPIs) |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
30/30 |
? |
Baclofen 0.5 mg/kg (up to a maximum of 40 mg) |
Placebo consisting of an equivalent volume of isotonic saline |
Side effects – AEs Baclofen vs placebo Total AEs 9, 5 vs 4 breathlessness (n = 2; 1 vs 1); tiredness (n = 2; 1 vs 1), nausea (n = 1; baclofen group), sore nostril/throat (n = 4; 2 vs 2). |
Gastric emptying, esophageal motility and reflux |
||||||||||||||||||||||||
|
DOMPERIDONE |
|||||||||||||||||||||||||||||||||||||||
|
DeLoore (1997) (40) |
RCT; parallel |
30 |
Domperidone 9 mo (3wks – 4 yr); Placebo: 6 mo (1mth – 5 yr) |
Clinical diagnosis of GER: pronounced vomiting after meals. |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
30/30 |
2 wks |
Domperidone 0.3 mg kg−1 three times a day |
Placebo three times a day |
Side effects No AEs reported
Visible vomiting/regurgitation Data only provided in figure and descriptively. No raw data provided. Authors report significant improvement of %patients vomiting in the domperidone vs placebo group (p<0.001). |
Symptoms of nausea and vomiting rated by investigator. Evaluation of treatment success (excellent, good, moderate or poor; based on symptom improvement |
||||||||||||||||||||||||
|
Carroccio (1994) (41) |
RCT; parallel |
40 |
Domperidone: Age median 5 mo (range 1 - 16 mo), Placebo: Age median 4 mo (range 1 - 16 mo)
|
GER confirmed by presence of at least 2 reflux episodes during fluoroscopy and 24-hour pH monitoring (RI >5.2%)
|
No |
Not clear |
Not clear |
Not clear |
No |
40/40 |
8 wks |
Domperidone (0.3 mg/kg/dose 15 minutes before meal) and placebo, administered 1 and 3 hours after meals (n=20) |
two different preparations of placebo administered 1 and 3 hours after meals (n=20)
|
Side effects No AEs reported
|
- 24-hour pH monitoring at baseline and 8 weeks (most of the children spent the monitoring period at home) - Reflux time - Number of reflux episodes - Duration of longest reflux (minutes) - Number of reflux episode > 5 minutes - Jolley score |
||||||||||||||||||||||||
|
METOCLOPRAMIDE |
|||||||||||||||||||||||||||||||||||||||
|
Bellissant (1997) (42) |
RCT; parallel |
44 |
105 ± 74 (87 ± 67 vs 122 ± 79) days |
24hour esoph- ageal pH recording when the percentage of time at pH <4 was at least equal to 5% of the analyzable duration of the recording.” GER determined by 24h pHmetry by percentage of time pH<4 >5% measurement |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
39/44 |
14 d |
Metoclopramide 2.6mg/ml solution (0.1mg/drop), 2 drops 3x/day before a meal (n=20) |
Placebo, not further specified (n=19) |
Side effects Treatment discontinued due to side effect Metoclopramide vs placebo: 1/20 vs 3/19 |
pH-metry, weight, four-class qualitative evaluation of treatment efficacy by parents |
||||||||||||||||||||||||
|
DeLoore (1997) (40) |
RCT; parallel |
32 |
Metoclopramide: 6 mo (3wks – 8yr); Placebo: 6 mo (1mth – 5 yr) |
Clinical diagnosis of GER: pronounced vomiting after meals. |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
32/32 |
2 wks |
Metoclopramide 0.3 mg kg−1 three times a day |
Placebo three times a day |
Side effects No AEs reported
Visible vomiting/regurgitation Data only provided in figure and descriptively. No raw data provided. Authors report significant improvement of %patients vomiting in the metcolopramide vs placebo group (p<0.001) |
Symptoms of nausea and vomiting rated by investigator. Evaluation of treatment success (excellent, good, moderate or poor; based on symptom improvement) |
||||||||||||||||||||||||
|
Tolia (1989) (43) |
RCT; cross-over |
30 |
Median age 2 mo (range 1 – 9 mo) |
pH probe confirmed GER, patients were only included if the pH result was abnormal during the initial 8 hours |
Not clear |
Not clear |
Yes |
Not clear |
Yes |
30/30 |
2 wks |
Metoclopramide 0.1 mg/kg x4 per day 30 minutes before feeding for 1 week (n=15)
|
Identical vehicle to metoclopramide and prescribed in a volume equal to 0.1mg/kg/dose of active metoclopramide (n=15)
|
Side effects No side effects observed during either study period
|
RI, number of reflux episodes < 4, number of episodes > 5 minutes, daily report of all symptoms, gastric emptying rates |
||||||||||||||||||||||||
|
DOMPERIDONE VS METOCLOPRAMIDE |
|||||||||||||||||||||||||||||||||||||||
|
DeLoore (1997) (40) |
RCT; parallel |
32 |
Domperidone 9 mo (3wks – 4 yr); Metoclopramide: 6 mo (3wks – 8yr) |
Clinical diagnosis of GER: pronounced vomiting after meals. |
Not clear |
Not clear |
Not clear |
Not clear |
Yes |
32/32 |
2 wks |
Domperidone 0.3 mg kg−1 three times a day |
Metoclopramide 0.3 mg kg−1 three times a day |
Side effects No AEs reported
Visible vomiting/regurgitation Data only provided in figure and descriptively. No raw data provided. Authors report significant improvement of %patients vomiting in the domperidone vs metoclopramide group (p<0.05) |
Symptoms of nausea and vomiting rated by investigator. . Evaluation of treatment success (excellent, good, moderate or poor; based on symptom improvement |
||||||||||||||||||||||||
|
AE = adverse event; CI = confidence interval; GER = gastroesophageal reflux; GERD = GER disease; I-GERQ-R = infant gastroesophageal reflux questionnaire revised; MD = mean difference; MDchange = change in mean difference; NS = not significant; PPI = proton pump inhibitor; RCT = randomized controlled trial; RI = reflux index; RR = relative risk; SAE = serious adverse event |
|||||||||||||||||||||||||||||||||||||||
Verantwoording
Beoordelingsdatum en geldigheid
Publicatiedatum : 01-06-2014
Beoordeeld op geldigheid : 01-07-2019
De richtlijn dient elke 5 jaar gereviseerd te worden.
Algemene gegevens
De ontwikkeling van de richtlijn gastro-oesofageale reflux ziekte bij kinderen is gefinancierd door Stichting Kwaliteitsgelden Medisch Specialisten (SKMS).
Doel en doelgroep
De richtlijn is geschreven voor alle behandelaren die te maken hebben met deze groep kinderen van de nulde tot de derdelijns gezondheidszorg. Het doel van deze richtlijn is te komen tot een betere herkenning, optimalisering van de diagnostiek en behandeling van GORZ bij kinderen van 0 tot 18 jaar. Om hierover gefundeerde aanbevelingen te kunnen doen, wordt een samenvatting gegeven van de wetenschappelijke stand van zaken en kennis uit de praktijk betreffende GOR en GORZ bij kinderen volgens de methode van evidence-based richtlijnontwikkeling.1, 2 Specifieke patiëntenpopulaties en hoog risicogroepen worden in een afzonderlijke paragraaf besproken. Er wordt in deze richtlijn onderscheid gemaakt tussen zuigelingen (0 tot 12 maanden) en oudere (12 maanden tot 18 jaar) kinderen en er wordt een een grens van 12 maanden aangehouden volgens de definitie van de World Health Organization. Wanneer geen leeftijdsspecificatie vermeld wordt, gelden uitspraken en aanbevelingen voor gehele populatie kinderen 0 – 18 jaar.
De richtlijn kan dienen als ondersteuning in het besluitvormingsproces, moet leiden tot een verbetering van de kwaliteit en doelmatigheid van het medisch handelen en moet meer uniformiteit in de praktijkvoering teweegbrengen. Deze richtlijn tracht duidelijke handvatten te bieden over wanneer en hoe ouders en patiënten op passende wijze kunnen worden gerustgesteld en biedt links naar downloadbare informatie. Er worden aanbevelingen gedaan over het op het juiste moment inzetten van diagnostiek en behandeling, met als doel doorverwijzing voor onnodige tests of het gebruik van medicatie zonder bevestigd effect te beperken. Echter, bij ernstige of evoluerende symptomen (met name potentiële rode vlag signalen), geeft de richtlijn aanbevelingen met betrekking tot acties die duidelijk noodzakelijk zijn bij onderzoek, behandeling en verwijzing.
De aanbevelingen in de richtlijn zijn te vertalen naar lokale protocollen die zijn toegespitst op de plaatselijke situatie. De behandelaar heeft de autonomie om, wanneer hij/zij dat nodig acht, beargumenteerd van de geformuleerde richtlijn af te wijken. Verwijzing naar een kinderarts MDL voor de diagnose en de behandeling van gecompliceerde pediatrische patiënten is ideaal; in situaties waarin dit niet mogelijk is, wordt in deze richtlijn rekening gehouden met mogelijke alternatieve opties.
Samenstelling werkgroep
De werkgroep is multidisciplinair samengesteld: zoveel mogelijk beoefenaars uit uiteenlopende disciplines, betrokken bij diagnostiek en behandeling van gastro-oesofageale refluxziekte bij kinderen in de eerste, tweede en derde lijn, zijn verzocht te participeren, als ook vertegenwoordigers vanuit patiëntenverenigingen. Leden van de werkgroep werden via de betreffende (wetenschappelijke) verenigingen verzocht zitting te nemen in de werkgroep op grond van hun persoonlijke expertise en/of affiniteit met het onderwerp. Zij ontvingen voor hun aanwezigheid bij werkgroepvergaderingen vacatiegelden en een reiskostenvergoeding.
AJN: mw. E. Vlaanderen
NVZA: mw. B. Witjes
NVMDL: dhr. prof. dr. A.J. Bredenoord
NVKC: mw. dr. M. Lindeboom
NHG: dhr. dr. G. Elshout
NVKMDL: dhr. prof. dr. M.A. Benninga
NVAVG: mw. M. Walinga (meelezer)
Kind en Ziekenhuis: mw. R. de Jonge (meelezer)
Samenstelling kernwerkgroep (2018)
Mw. Dr. M.M. Tabbers, projectleider
Mw. Dr. M.M.J. Singendonk
Belangenverklaringen
De werkgroepleden hebben een belangenverklaring ingevuld waarin ze hun eventuele banden met de farmaceutische industrie hebben aangegeven. De verklaringen liggen ter inzage bij de NVK.
Inbreng patiëntenperspectief
Het perspectief van patiënten wat betreft de zorg rondom GORZ vormt een waardevolle aanvulling bij de totstandkoming van een richtlijn over GORZ bij kinderen. Er is geen patiëntenvereniging specifiek voor kinderen met GORZ.
Methode ontwikkeling
Evidence based
Implementatie
De richtlijn is onder de verenigingen verspreid en via de websites van de verenigingen elektronisch beschikbaar gesteld. Op wetenschappelijke bijeenkomsten van de betrokken wetenschappelijke verenigingen zijn de aanbevelingen van de richtlijn gepresenteerd. Verder is er patiëntenvoorlichtingsmateriaal ontwikkeld ter ondersteuning van de richtlijn. Daarnaast zijn indicatoren ontwikkeld om te meten of de implementatie van de richtlijn daadwerkelijk effectief is geweest.
Werkwijze
Allereerst werd door middel van het versturen van vragenlijsten een knelpuntanalyse uitgevoerd om de huidige werkwijze ten aanzien van de diagnostiek en behandeling van kinderen met GORZ in de nulde t/m de derdelijns gezondheidszorg in Nederland in kaart te brengen. Op basis van de resultaten van de knelpuntenanalyse werden met de werkgroep de uitgangsvragen opgesteld. Vervolgens werd samen met een adviseur van het Kwaliteitsinstituut voor de Gezondheidszorg CBO volgens de methode van Evidence-based Richtlijn Ontwikkeling per vraag een uitgebreid literatuuronderzoek verricht. In eerste instantie werd gezocht naar Evidence based richtlijnen. De gevonden richtlijnen werden op kwaliteit beoordeeld door de kernwerkgroepleden met behulp van het Appraisal of Guidelines for Research & Evaluation (AGREE)-instrument. Wanneer er een valide richtlijn werd gevonden, werd de evidence uit de richtlijn gebruikt om de vragen te beantwoorden. Wanneer er geen geschikte richtlijn werd gevonden, werd vervolgens gezocht naar systematische literatuuroverzichten. Ook deze werden op inhoudelijke en methodologische kwaliteit beoordeeld door de kernwerkgroepleden. Bij het vinden van een valide systematic review voor beantwoording van één van de vragen, werden zowel de review als ook de afzonderlijke studies besproken in de betreffende modules. Vervolgens werd naar aanvullende studies gezocht vanaf het moment waar de zoekactie in de review eindigde.
Voor GOR en GORZ werden de volgende zoektermen gebruikt: “gastro(o)esophageal reflux” en afkortingen, “gastric acid reflux” en “(o)esophagitis” waarbij rekening werd gehouden met verschillen in de Britse en Amerikaanse spelling. Details over de zoekstrategie zijn weergegeven in Appendix 1. Er werd geen taalbeperking opgelegd.
Inclusiecriteria waren als volgt (er moest voldaan worden aan alle inclusiecriteria relevant voor de onderzoeksvraag):
- Studiepopulatie bestaande uit kinderen met GORZ in de leeftijd van 0 tot 18 jaar.
- Voor diagnostische studies (vraag 1) werden systematische reviews en originele onderzoeken met betrekking tot de diagnostische nauwkeurigheid van de specifieke diagnostische tests geïncludeerd. De referentiestandaard voor GORZ moest door auteurs worden gedefinieerd aan de hand van anamnese en lichamelijk onderzoek.
- Therapeutische randomized controlled trials (uitgangsvragen 2 en 3) werden alleen geïncludeerd wanneer zij minstens 10 personen per onderzoeksarm bevatten.
In 2018 – 2019 vond een update plaats van NVK richtlijn uit 2012 (zoekactie tot juni 2018) die gefinancierd werd door Stichting Kwaliteitsgelden Medisch Specialisten.
Bij deze update werd weer een knelpuntanalyse eerst uitgevoerd onder de werkgroepleden. Vervolgens werd er voor de therapeutische vragen nu gebruik gemaakt van The Grading of Recommendations Assessment, Development and Evaluation (GRADE). De GRADE-methode heeft als doel om de kwaliteit van evidence transparant weer te geven. Aan het begin van het richtlijntraject werden uitkomstmaten gedefinieerd. In overeenstemming met de meest recente pediatrische richtlijn, werd gebruik gemaakt van de volgende acht uitkomstmaten: oesofagitis (endoscopisch/histologisch), GOR-gerelateerde complicaties (Barrett metaplasie, stenose, en andere zoals gespecificeerd door auteurs), GOR-gerelateerde klachten en symptomen (gemeten met de infant gastroesophageal reflux questionnaire revised, I-GERQ-R), kwaliteit van leven (zowel van de ouder als de patiënt), huilen en onrust (rapportage door de ouder), spugen en/of regurgiteren (rapportage door de ouder en/of patiënt), zuurbranden (rapportage door de ouder en/of patiënt), en bijwerkingen van de behandeling.
Resultaten werden per uitkomstmaat samengevat, waarbij tevens de ‘overall’ kwaliteit van de onderliggende bewijslast (evidence) werd aangegeven. Bij de beoordeling werd gebruik gemaakt van de software “GRADE-pro”. Met behulp van dit programma werd bij elke uitgangsvraag een tabel met de beoordeling van het bewijs (“GRADE evidence profile”) gemaakt. Deze tabellen zijn bij elk uitgangsvraag te vinden.
GRADE kent vier niveaus: ‘high’ (hoog), ‘moderate’ (matig), ‘low’ (laag) en ‘very low’ (zeer laag). Per uitkomstmaat werd voor de kwaliteit van het bewijs met behulp van GRADE-pro een GRADE niveau toegekend.
‘Hoog’: Wanneer de kwaliteit van bewijs voor een uitkomst als ‘high’ ofwel ‘hoog’ geclassificeerd werd, wil dit zeggen dat het onwaarschijnlijk is dat toekomstig onderzoek de schatting van de uitkomst zal veranderen. Met andere woorden, er is veel vertrouwen in de juistheid van de schatting van de uitkomst.
‘Matig’: Wanneer de kwaliteit van bewijs voor een uitkomst als ‘moderate’ ofwel ‘matig’ geclassificeerd werd, wil dit zeggen dat het waarschijnlijk is dat toekomstig onderzoek effect heeft op het vertrouwen in de schatting van de uitkomst en zou de schatting van de uitkomst kunnen veranderen. Met andere woorden, er is matig vertrouwen in de juistheid van de schatting van de uitkomst.
‘Laag’: Wanneer de kwaliteit van bewijs voor een uitkomst als ‘low’ ofwel ‘laag’ geclassificeerd werd, wil dit zeggen dat het heel waarschijnlijk is dat toekomstig onderzoek effect heeft op het vertrouwen in de schatting van de uitkomst en zal deze schatting waarschijnlijk veranderen. Met andere woorden, er is beperkt vertrouwen in de juistheid van de schatting van de uitkomst.
‘Zeer laag’: Een ‘very low’ ofwel ‘zeer lage’ classificatie wil zeggen dat er veel onzekerheid is over de juistheid van de uitkomst.
De onderzoeksopzet is een belangrijke factor binnen GRADE. Gerandomiseerde en
gecontroleerde studies krijgen daarom in beginsel de kwalificatie ‘hoog’. Er zijn vijf factoren
die kunnen zorgen voor een lagere kwalificatie:
- Beperkingen in de onderzoeksopzet.
- Inconsistentie: onverklaarde heterogeniteit van de resultaten.
- Indirectheid: PICO waarop de evidence gebaseerd is wijkt op een of meer punten af van de PICO die men wil onderzoeken. Ook het gebruik van surrogaatmarkers valt onder indirectheid.
- Imprecisie: wijde betrouwbaarheidsintervallen rond een geschat effect duiden op onzekerheid in de grootte van het effect. Er is sprake van imprecisie bij een te kleine steekproef (lage statistische power), weinig gebeurtenissen (events) en een betrouwbaarheidsinterval dat wel statistisch significant is maar, zowel in het gebied van klinische relevantie als in het gebied van een verwaarloosbaar effect ligt.
- Publicatiebias.
Er zijn drie factoren die kunnen zorgen voor een hogere kwalificatie:
- Groot effect.
- Aanwezigheid van dosisresponsrelatie.
- Confounding die het werkelijke effect onderschat of een in werkelijkheid niet bestaand effect overschat.
Iedere beperkende (of bevorderende) factor kan leiden tot het verlagen (of verhogen) van de classificatie met een of twee niveaus. Indien de resultaten niet gepoold konden worden, werd volstaan met een globale inschatting van de kwaliteit van de onderliggende bewijslast. Voor een uitgebreidere beschrijving van GRADE verwijzen we naar www.gradeworkinggroup.org.
Uitgangsvragen
Uitgangsvraag 1:
Wat is, ten opzichte van de anamnese en lichamelijk onderzoek, de aanvullende diagnostische waarde van onderstaande onderzoeken bij het stellen van de diagnose GORZ bij kinderen van 0 – 18 jaar van:
- Endoscopie met biopten
- pH-metrie
- pH-impedantiemetrie
- Scintigrafie
- Röntgenonderzoek (barium slikfoto)
- Manometrie
- Biomarkers
- Proefbehandeling met PPI
Uitgangsvraag 2:
Welke niet-farmacologische interventies zijn effectief en veilig voor de behandeling van GORZ bij kinderen van 0 – 18 jaar?
- Ondersteuning en educatie van patiënt en ouders
- Leefstijladviezen
- Houdingsadviezen
- Verdikken van de voeding
- Vermindering voedingsvolume of -frequentie
- Eliminatie van koemelkeiwit
Uitgangsvraag 3:
Welke farmacologische interventies zijn effectief en veilig voor de behandeling van GORZ bij kinderen van 0 – 18 jaar?
- Antacida en alginaten
- Zuurremming (histamine-2-receptor antagonist (H2-antagonist) en protonpompremmers (proton pump inhibitors, PPIs))
- Prokinetica
Uitgangsvraag 4:
Bij welke kinderen met GORZ is chirurgie geïndiceerd boven (niet-)farmacologische behandeling?
Uitgangsvraag 5:
Wanneer dient de nulde of eerste lijn naar de tweede lijn te verwijzen en wanneer dient de tweede lijn naar de derde lijn te verwijzen bij kinderen van 0 – 18 jaar met klachten die wijzen op GORZ?
Totstandkoming van de aanbevelingen
Voor het komen tot een aanbeveling zijn er naast het wetenschappelijk bewijs ook andere aspecten van belang, bijvoorbeeld: patiëntenvoorkeuren, beschikbaarheid van speciale technieken of expertise, organisatorische aspecten, maatschappelijke consequenties en kosten. Deze aspecten worden besproken na de ‘Conclusie’. Hierin wordt de conclusie op basis van de literatuur geplaatst in de context van de dagelijkse praktijk en vindt een afweging plaats van de voor- en nadelen van de verschillende beleidsopties. De uiteindelijk geformuleerde aanbeveling is het resultaat van het beschikbare bewijs in combinatie met deze overwegingen. Het volgen van deze procedure en het opstellen van de richtlijn in dit ‘format’ heeft als doel de transparantie van de richtlijn te vergroten. Het biedt ruimte voor een efficiënte discussie tijdens de werkgroepvergaderingen en vergroot bovendien de helderheid voor de gebruiker van de richtlijn.
Juridische betekenis van richtlijnen
Richtlijnen zijn geen wettelijke voorschriften maar wetenschappelijk onderbouwde en breed gedragen inzichten en aanbevelingen. Hieraan moeten zorgverleners voldoen om kwalitatief goede zorg te verlenen. Zorgverleners kunnen op basis van hun professionele autonomie afwijken van de richtlijn. De aanbevelingen zijn immers hoofdzakelijk gebaseerd op de ‘gemiddelde patiënt’. Afwijken van richtlijnen is, als de situatie van de patiënt dat vereist, soms zelfs noodzakelijk. Wanneer van de richtlijn wordt afgeweken moet dit echter beargumenteerd, gedocumenteerd en, waar nodig, in overleg met de patiënt worden gedaan.
Zoekverantwoording
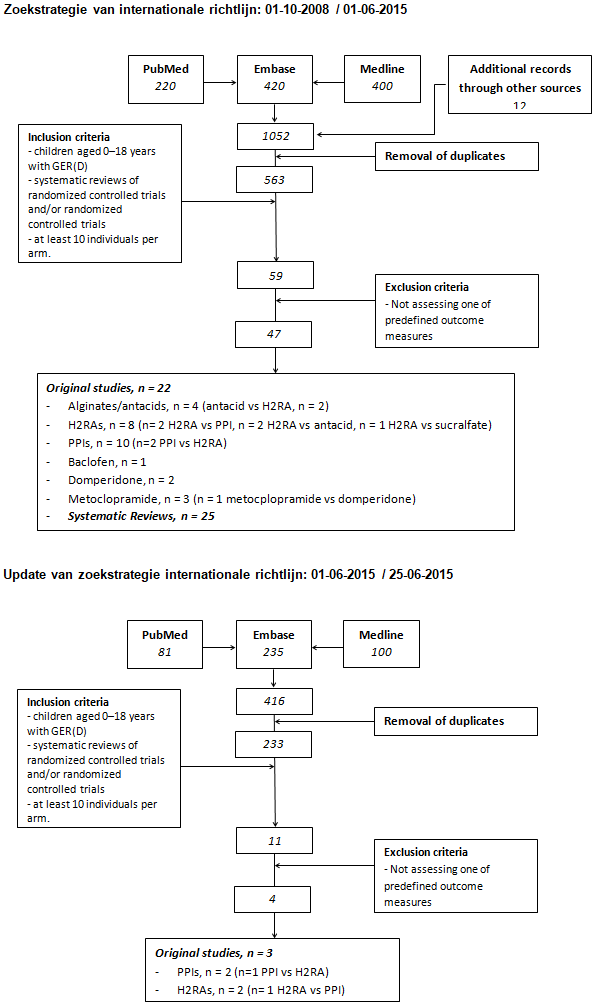
Database(s): Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations and Ovid MEDLINE(R) 1946 to Present
Search Strategy:
|
# |
Searches |
Results |
|
1 |
exp Gastroesophageal Reflux/ or esophagitis/ or esophagitis, peptic/ or (gastroesophageal adj reflux).ti,ab. or (gastrooesophageal adj reflux).ti,ab. or (gastro esophageal adj reflux).ti,ab. or (gastro oesophageal adj reflux).ti,ab. or (GORD or GOR or GERD or GER).ti,ab. or (esophagitis or oesophagitis).ti,ab,kw. or (gastric adj3 (acid or reflux)).ti,ab. or (reflux adj (oesophagitis or esophagitis)).ti,ab. or (erosive adj3 (oesophag* or esophag*)).ti,ab. |
50185 |
|
2 |
adolescent/ or child/ or child, preschool/ or infant/ or infant, newborn/ or infant, low birth weight/ or infant, postmature/ or infant, premature/ or exp Pediatrics/ or (child* or infant* or infancy or newborn* or neonat* or baby or babies or preschool or pre school or pubescen* or teen* or adolescen* or puber* or prepubert* or juvenil* or p?ediatric* or youth* or schoolchild* or school age* or schoolage* or preschool or pre-school or elementary school or high school* or highschool* or kindergar* or boy or boys or girl* or minor* or underag* or under ag* or kid or kids or toddler*).ti,ab. |
3666035 |
|
3 |
Antacids/ or Alginates/ or exp Proton Pump Inhibitors/ or Ranitidine/ or Nizatidine/ or Cimetidine/ or Famotidine/ or lansoprazole/ or omeprazole/ or esomeprazole/ or rabeprazole/ or cisapride/ or domperidone/ or Metoclopramide/ or erythromycin/ or azithromycin/ or clarithromycin/ or exp Histamine H2 Antagonists/ or Aluminum Hydroxide/ or sodium bicarbonate/ or calcium carbonate/ or (alginate* or gaviscon or almagate or almax or tisacid or magnesium hydroxide or brucite or magnesium hydrate or milk of magnesia or aluminum hydroxide or aldrox or algeldrate or alhydrogel or aloh-gel or alternagel or alu-cap or alu-tab or alugel or amphojel or andursil or brasivil or dialume or hydrated alumina or rocgel or maalox* or co-magaldrox or alucol or (alumina and magnesia) or aluminum hydroxide-magnesium hydroxide or aluminum magnesium hydroxide or co-magaldrox or magnesium aluminum hydroxide or maldroxal or mintox or novalucol or supralox or H2 antagonist* or ranitidin* or biotidin or pylorid or raniberl or ranisen or rantec or sostril or tritec or zantac or cimetidine or altramet or biomet or histodil or tagamet or zita or famotidine or pepcid or ym 11170 or PPI or PPIs or proton pump inhibitor* or lansoprazol* or dexlansoprazole or agopton or lanzoprazol* or lanzor or prevacid or takepron or zoton or pantoprazole or protonix or pantozol or pantoloc or controloc or omeprazole or losec or nexium or prilosec or rapinex or zegerid or OMEZ or antra or mopral or rabeprazole or aciphex or dexrabeprazole or pariet or esomeprazol* or nexium or nexiam or metoclopramide or cerucal or degan or gastrobid continus or gastromax or maxolon or maxeran or metaclopramide or octamide or primperan or reglan or rimetin or domperidon* or motilium or kw 5338 or erythromycin or aknemycin or T stat or e-base or emycin or emgel or eryc or eryderm or erythro or erythroped or gallimycin or ilosone or ilotycin or monomycin or romycin or staticin or stiemycin or theramycin or wyamycin or bethanechol or bethanecol or myotonine or urecholine or sucralfate or aluminum sucrose sulfate or antepsin or carafate or sutra or sulcrate or ulcogant or ulsanic or nizatidine or cisapride or azithromycin or clarithromycin or prokinetic agent* or prokinetic* or hydrotalcite or asilone or gastrocote or topal or sodium alginate* or altacite or sodium bicarbonate).ti,ab,kw. or (sodium adj alginate*).ti,ab,kw. |
125965 |
|
4 |
exp clinical trial/ or exp randomized controlled trial/ or controlled clinical trial/ or exp clinical trials as topic/ or exp randomized controlled trials as topic/ or Random Allocation/ or double-blind method/ or single-blind method/ or multicenter study/ or (random* or placebo).ti,ab,kw. or trial.ti. |
1517636 |
|
5 |
Animals/ not Humans/ |
3961836 |
|
6 |
exp Animals, Laboratory/ or exp Animal Experimentation/ or exp Models, Animal/ or exp Rodentia/ or (rat or rats or mouse or mice).ti. or editorial/ or letter/ or news/ or Comment/ or exp historical article/ or Anecdotes as Topic/ or Case Reports/ or (letter* or comment* or abstracts).ti. |
6409431 |
|
7 |
(1 and 2 and 3 and 4) not 5 not 6 |
669 |
|
8 |
limit 7 to yr="2008 -Current" |
202 |
Database(s): Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations and Ovid MEDLINE(R) 1946 to Present
Search Strategy:
|
# |
Searches |
Results |
|
1 |
exp Gastroesophageal Reflux/ or esophagitis/ or esophagitis, peptic/ or (gastroesophageal adj reflux).ti,ab. or (gastrooesophageal adj reflux).ti,ab. or (gastro esophageal adj reflux).ti,ab. or (gastro oesophageal adj reflux).ti,ab. or (GORD or GOR or GERD or GER).ti,ab. or (esophagitis or oesophagitis).ti,ab,kw. or (gastric adj3 (acid or reflux)).ti,ab. or (reflux adj (oesophagitis or esophagitis)).ti,ab. or (erosive adj3 (oesophag* or esophag*)).ti,ab. |
50185 |
|
2 |
adolescent/ or child/ or child, preschool/ or infant/ or infant, newborn/ or infant, low birth weight/ or infant, postmature/ or infant, premature/ or exp Pediatrics/ or (child* or infant* or infancy or newborn* or neonat* or baby or babies or preschool or pre school or pubescen* or teen* or adolescen* or puber* or prepubert* or juvenil* or p?ediatric* or youth* or schoolchild* or school age* or schoolage* or preschool or pre-school or elementary school or high school* or highschool* or kindergar* or boy or boys or girl* or minor* or underag* or under ag* or kid or kids or toddler*).ti,ab. |
3666035 |
|
3 |
Antacids/ or Alginates/ or exp Proton Pump Inhibitors/ or Ranitidine/ or Nizatidine/ or Cimetidine/ or Famotidine/ or lansoprazole/ or omeprazole/ or esomeprazole/ or rabeprazole/ or cisapride/ or domperidone/ or Metoclopramide/ or erythromycin/ or azithromycin/ or clarithromycin/ or exp Histamine H2 Antagonists/ or Aluminum Hydroxide/ or sodium bicarbonate/ or calcium carbonate/ or (alginate* or gaviscon or almagate or almax or tisacid or magnesium hydroxide or brucite or magnesium hydrate or milk of magnesia or aluminum hydroxide or aldrox or algeldrate or alhydrogel or aloh-gel or alternagel or alu-cap or alu-tab or alugel or amphojel or andursil or brasivil or dialume or hydrated alumina or rocgel or maalox* or co-magaldrox or alucol or (alumina and magnesia) or aluminum hydroxide-magnesium hydroxide or aluminum magnesium hydroxide or co-magaldrox or magnesium aluminum hydroxide or maldroxal or mintox or novalucol or supralox or H2 antagonist* or ranitidin* or biotidin or pylorid or raniberl or ranisen or rantec or sostril or tritec or zantac or cimetidine or altramet or biomet or histodil or tagamet or zita or famotidine or pepcid or ym 11170 or PPI or PPIs or proton pump inhibitor* or lansoprazol* or dexlansoprazole or agopton or lanzoprazol* or lanzor or prevacid or takepron or zoton or pantoprazole or protonix or pantozol or pantoloc or controloc or omeprazole or losec or nexium or prilosec or rapinex or zegerid or OMEZ or antra or mopral or rabeprazole or aciphex or dexrabeprazole or pariet or esomeprazol* or nexium or nexiam or metoclopramide or cerucal or degan or gastrobid continus or gastromax or maxolon or maxeran or metaclopramide or octamide or primperan or reglan or rimetin or domperidon* or motilium or kw 5338 or erythromycin or aknemycin or T stat or e-base or emycin or emgel or eryc or eryderm or erythro or erythroped or gallimycin or ilosone or ilotycin or monomycin or romycin or staticin or stiemycin or theramycin or wyamycin or bethanechol or bethanecol or myotonine or urecholine or sucralfate or aluminum sucrose sulfate or antepsin or carafate or sutra or sulcrate or ulcogant or ulsanic or nizatidine or cisapride or azithromycin or clarithromycin or prokinetic agent* or prokinetic* or hydrotalcite or asilone or gastrocote or topal or sodium alginate* or altacite or sodium bicarbonate).ti,ab,kw. or (sodium adj alginate*).ti,ab,kw. |
125965 |
|
4 |
meta-analysis as topic/ or Meta-Analysis/ or meta analy$.tw. or metaanaly$.tw. or (systematic adj (review$1 or overview$1)).tw. or exp Review Literature as Topic/ or cochrane.ab. or embase.ab. or (psychlit or psyclit).ab. or (psychinfo or psycinfo).ab. or (cinahl or cinhal).ab. or science citation index.ab. or bids.ab. or cancerlit.ab. or reference list$.ab. or bibliograph$.ab. or hand-search$.ab. or relevant journals.ab. or manual search$.ab. or ((selection criteria or data extraction).ab. and Review/) |
175717 |
|
5 |
Animals/ not Humans/ |
3961836 |
|
6 |
exp Animals, Laboratory/ or exp Animal Experimentation/ or exp Models, Animal/ or exp Rodentia/ or (rat or rats or mouse or mice).ti. or editorial/ or letter/ or news/ or Comment/ or exp historical article/ or Anecdotes as Topic/ or Case Reports/ or (letter* or comment* or abstracts).ti. |
6409431 |
|
7 |
(1 and 2 and 3 and 4) not 5 not 6 |
64 |
|
8 |
(1 and 2 and 3) not 5 not 6 |
1624 |
|
9 |
limit 8 to systematic reviews |
88 |
|
10 |
7 or 9 |
100 |
|
11 |
limit 10 to yr="2008 -Current" |
48 |