pH-impedantiemetrie bij GORZ
Uitgangsvraag
Wat is, ten opzichte van de anamnese en lichamelijk onderzoek, de aanvullende diagnostische waarde van onderstaande onderzoeken bij het stellen van de diagnose GORZ bij kinderen van 0 – 18 jaar van: pH-impedantiemetrie?
Aanbeveling
Een pH-impedantiemetrie heeft de voorkeur boven een pH-metrie en kan overwogen worden om:
- persisterende GOR-symptomen te correleren met zure en niet-zure GOR-episodes op pH-impedantiemetrie (advies: meting zonder zuurremmende medicatie) (expert opinie).
- de rol van zure en niet-zure reflux in de etiologie van oesofagitis en andere GOR gerelateerde symptomen en complicaties te onderzoeken (expert opinie).
- de effectiviteit van zuurremmende medicatie te evalueren, i.e. bepalen van oesofageale zuurexpositie (advies: meting met zuurremmende medicatie) (expert opinie).
- om het onderscheid te maken tussen niet-erosieve GORZ, hypersensitiviteit en functioneel zuurbranden bij patiënten met normale endoscopie (expert opinie).
Onderbouwing
Achtergrond
Veel diagnostische onderzoeken die bij volwassenen gebruikt worden om de diagnose GORZ te stellen, zoals een pH-impedantiemetrie, zijn invasief van aard. Omdat het verrichten van dit soort onderzoeken bij gezonde kinderen ethische bezwaren met zich meebrengt, kunnen geen normaalwaarden specifiek voor kinderen opgesteld worden. Deze onderzoeken kunnen hierdoor dus ook niet als goede diagnostische tests gebruikt worden voor het stellen van de diagnose GORZ bij kinderen. De resultaten hieronder moeten dus in het licht van deze beperkingen worden geïnterpreteerd.
Conclusies / Summary of Findings
Er is geen bewijs om het routinematig gebruik van pH-impedantiemetrie voor het stellen van de diagnose GORZ bij kinderen te ondersteunen.
Samenvatting literatuur
Een 24uurs pH-impedantiemetrie is een gecombineerde meting van de pH (zuurgraad) en impedantie (elektrische weerstand) in de slokdarm. Door meting van het impedantiesignaal op verschillende plekken in de slokdarm kunnen op- en neerwaartse bewegingen van lucht- en vloeistofstromen door slokdarm gemeten worden. Tegelijkertijd wordt ook de zuurgraad gemeten. In combinatie met de bevindingen tijdens endoscopie, kan met een pH-impedantiemetrie een onderscheid gemaakt worden tussen patiënten met GORZ en patiënten met niet-erosieve GORZ, een hypersensitieve slokdarm of functioneel zuurbranden.17
De beperkingen met betrekking tot symptoomassociatie van de pH-metrie gelden ook voor de pH-impedantiemetrie. Overige nadelen van beide metingen zijn verder het gebrek aan normaalwaardes voor deze metingen bij kinderen, waardoor de resultaten moeilijk klinisch te interpreteren zijn. Daarnaast is de analyse van deze metingen ingewikkeld en dient deze uitgevoerd te worden door een expert. Echter zelfs dan blijken de betrouwbaarheid en reproduceerbaarheid van resultaten beperkt.18-21
Vaak wordt de vraag gesteld of een pH-(impedantie)metrie het best mét of zonder zuurremmende medicatie verricht moet worden. Er zijn tot op heden geen studies bij kinderen verricht die dit onderzocht hebben. Algemeen wordt geadviseerd om dit af te laten hangen van het doel van de meting. Als het doel is om de zuurremmende effectiviteit van medicatie te onderzoeken, vindt de meting het best plaats mét medicatie. Als het doel is om symptomen te correleren met GOR episodes op de pH-(impedantie)metrie, vindt de meting het best zonder medicatie plaats.22, 23.
Er werden geen studies gevonden die het gebruik van pH-impedantiemetrie voor de diagnose van GORZ bij kinderen onderzochten die voldeden aan de inclusiecriteria. Bij volwassenen is een pH-impedantiemetrie de gouden standaard voor het stellen van de diagnose refluxziekte en om een onderscheid te maken tussen patiënten met niet-erosieve GORZ, een hypersensitieve slokdarm of functioneel zuurbranden.
Zoeken en selecteren
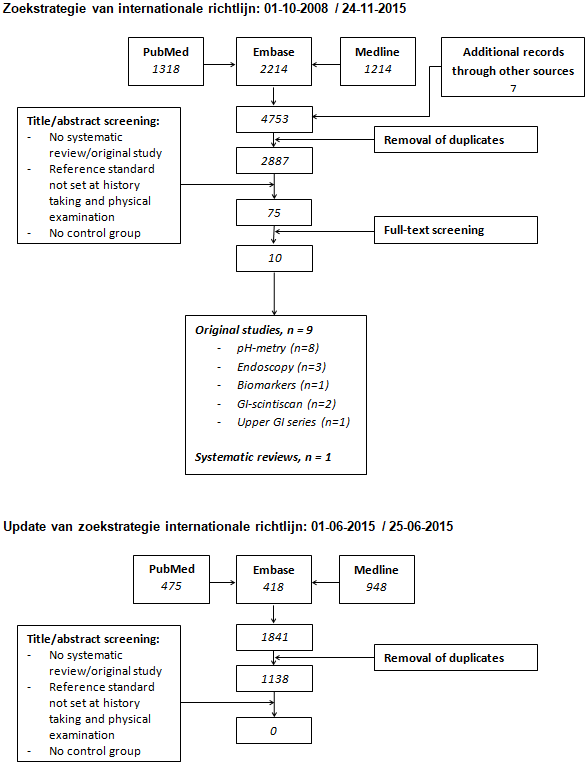
Bij de selectie en beoordeling van richtlijnen, kwam de internationale richtlijn van Rosen et al. uit 2018 als beste naar voren.1, 6 De kwaliteit van deze richtlijn bleek voldoende om deze als uitgangspunt van de huidige richtlijn te gebruiken. De richtlijn van Rosen et al. is ontwikkeld door een internationale werkgroep van 10 kinderartsen MDL, één epidemioloog en één arts-onderzoeker. Er werd een systematische literatuursearch gedaan (zie de zoekstrategie, flowcharts en studiekarakteristieken) en de werkgroep kwam drie keer bijeen. Artikelen werden geëvalueerd met behulp van Quality Assessment of Studies of Diagnostic Accuracy in het geval van diagnostische studies (QUADAS) of GRADE in het geval van therapeutische studies (zie de evidence tabellen). Aanbevelingen werden gedaan op basis van evidence uit de literatuur. Bij gebrek aan evidence (van voldoende kwaliteit) werden aanbevelingen gedaan op basis van “expert opinion”. Om consensus te bereiken werden nominale groepstechnieken gebruikt.
In deze modules worden per PICO de beschikbare literatuur, conclusies, overige overwegingen en aanbevelingen besproken. We zijn uitgegaan van de NVK-richtlijn uit 2012 en de bevindingen van Rosen et al. en hebben deze waar nodig geüpdatet.
In de tabellen 1 t/m 3 (van het aanverwant product Symptomen bij GORZ) zijn symptomen en bevindingen die passen bij GORZ, alarmsymptomen en aandoeningen in de differentiaaldiagnose van GORZ bij kinderen van 0 – 18 jaar weergegeven. De tabellen zijn gebaseerd op Rosen et al.1 In de aanverwante producten is informatie over medicatie opgenomen (zie het Overzicht geneesmiddelen voor GORZ). De zoekverantwoording bevat informatie over de geïncludeerde studies en de in deze module beschreven literatuur weergegeven in evidence tabellen.
Referenties
- 1 - Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F, et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. Journal of pediatric gastroenterology and nutrition. 2018;66:516-54.
- 2 - Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. Journal of clinical epidemiology. 2011;64:383-94.
- 3 - Singendonk M, Goudswaard E, Langendam M, van Wijk M, van Etten-Jamaludin F, Benninga M, et al. Prevalence of Gastroesophageal Reflux Disease Symptoms in Infants and Children: A Systematic Review. Journal of pediatric gastroenterology and nutrition. 2019;
- 4 - Singendonk MM, Goudswaard E, Langendam M., Van Wijk MP, Van Etten F, Benninga MA, et al. Epidemiology of gastroesophageal reflux disease (GERD) in children: a systematic review [Submitted for publication]. 0000;
- 5 - Singendonk MMJ, Tabbers MM, Benninga MA, Langendam MW. Pediatric Gastroesophageal Reflux Disease: Systematic Review on Prognosis and Prognostic Factors. Journal of pediatric gastroenterology and nutrition. 2018;66:239-43.
- 6 - Davies I, Burman-Roy S, Murphy MS. Gastro-oesophageal reflux disease in children: NICE guidance. BMJ. 2015;350:g7703.
- 7 - Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. The American journal of gastroenterology. 2006;101:1900-20.
- 8 - Arasu TS, Wyllie R, Fitzgerald JF, Franken EA, Siddiqui AR, Lehman GA, et al. Gastroesophageal reflux in infants and children comparative accuracy of diagnostic methods. The Journal of pediatrics. 1980;96:798-803.
- 9 - Cucchiara S, Minella R, D'Armiento F, Franco MT, lervolino C, Campanozzi A, et al. Histologic grading of reflux oesophagitis and its relationship with intra-oesophageal and intragastric pH variables. European Journal of Gastroenterology & Hepatology. 1993;5:621-6.
- 10 - Ravelli AM, Villanacci V, Ruzzenenti N, Grigolato P, Tobanelli P, Klersy C, et al. Dilated intercellular spaces: a major morphological feature of esophagitis. Journal of pediatric gastroenterology and nutrition. 2006;42:510-5.
- 11 - Boix-Ochoa J, Lafuenta JM, Gil-Vernet JM. Twenty-four hour exophageal pH monitoring in gastroesophageal reflux. Journal of pediatric surgery. 1980;15:74-8.
- 12 - Da Dalt L, Mazzoleni S, Montini G, Donzelli F, Zacchello F. Diagnostic accuracy of pH monitoring in gastro-oesophageal reflux. Archives of disease in childhood. 1989;64:1421-6.
- 13 - Cucchiara S, Staiano A, Gobio Casali L, Boccieri A, Paone FM. Value of the 24 hour intraoesophageal pH monitoring in children. Gut. 1990;31:129-33.
- 14 - Cucchiara S, Minella R, Iervolino C, Franco MT, Campanozzi A, Franceschi M, et al. Omeprazole and high dose ranitidine in the treatment of refractory reflux oesophagitis. Archives of disease in childhood. 1993;69:655-9.
- 15 - Kahn A, Rebuffat E, Sottiaux M, Blum D, Yasik EA. Sleep apneas and acid esophageal reflux in control infants and in infants with an apparent life-threatening event. Biology of the neonate. 1990;57:144-9.
- 16 - Patra S, Singh V, Chandra J, Kumar P, Tripathi M. Diagnostic modalities for gastro-esophageal reflux in infantile wheezers. Journal of tropical pediatrics. 2011;57:99-103.
- 17 - Giacchino M, Savarino V, Savarino E. Distinction between patients with non-erosive reflux disease and functional heartburn. Annals of gastroenterology : quarterly publication of the Hellenic Society of Gastroenterology. 2013;26:283-9.
- 18 - Loots CM, van Wijk MP, Blondeau K, Dalby K, Peeters L, Rosen R, et al. Interobserver and intraobserver variability in pH-impedance analysis between 10 experts and automated analysis. The Journal of pediatrics. 2012;160:441-6.e1.
- 19 - Pilic D, Höfs C, Weitmann S. Inter- and intraobserver agreement in 24-hour combined multiple intraluminal impedance and pH measurement in children - a quality assessment from the German Pediatric Impedance Group (G-PIG). Journal of pediatric gastroenterology and nutrition. 2011;53:255-9.
- 20 - Wenzl TG, Benninga MA, Loots CM, Salvatore S, Vandenplas Y. Indications, methodology, and interpretation of combined esophageal impedance-pH monitoring in children: ESPGHAN EURO-PIG standard protocol. Journal of pediatric gastroenterology and nutrition. 2012;55:230-4.
- 21 - Ravi K, DeVault KR, Murray JA, Bouras EP, Francis DL. Inter-observer agreement for multichannel intraluminal impedance-pH testing. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus / ISDE. 2010;23:540-4.
- 22 - Hemmink GJ, Bredenoord AJ, Weusten BL, Monkelbaan JF, Timmer R, Smout AJ. Esophageal pH-impedance monitoring in patients with therapy-resistant reflux symptoms: 'on' or 'off' proton pump inhibitor? Am J Gastroenterol. 2008;103:2446-53.
- 23 - Zerbib F, des Varannes SB, Roman S, Pouderoux P, Artigue F, Chaput U, et al. Normal values and day-to-day variability of 24-h ambulatory oesophageal impedance-pH monitoring in a Belgian-French cohort of healthy subjects. Aliment Pharmacol Ther. 2005;22:1011-21.
- 24 - Loots C, van Herwaarden MY, Benninga MA, VanderZee DC, van Wijk MP, Omari TI. Gastroesophageal reflux, esophageal function, gastric emptying, and the relationship to dysphagia before and after antireflux surgery in children. The Journal of pediatrics. 2013;162:566-73.e2.
- 25 - Smits MJ, Loots CM, Benninga MA, Omari TI, van Wijk MP. New insights in gastroesophageal reflux, esophageal function and gastric emptying in relation to dysphagia before and after anti-reflux surgery in children. Current gastroenterology reports. 2013;15:351.
- 26 - Tucker E, Knowles K, Wright J, Fox MR. Rumination variations: aetiology and classification of abnormal behavioural responses to digestive symptoms based on high-resolution manometry studies. Alimentary pharmacology & therapeutics. 2013;37:263-74.
- 27 - Kessing BF, Bredenoord AJ, Smout AJ. Objective manometric criteria for the rumination syndrome. The American journal of gastroenterology. 2014;109:52-9.
- 28 - Rosen R, Rodriguez L, Nurko S. Pediatric rumination subtypes: A study using high-resolution esophageal manometry with impedance. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society. 2017;29.
- 29 - Singendonk MMJ, Oors JM, Bredenoord AJ, Omari TI, van der Pol RJ, Smits MJ, et al. Objectively diagnosing rumination syndrome in children using esophageal pH-impedance and manometry. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2017;29.
- 30 - Farhath S, He Z, Saslow J, Soundar S, Amendolia B, Bhat V, et al. Detection of pepsin in mouth swab: correlation with clinical gastroesophageal reflux in preterm infants. The journal of maternal-fetal & neonatal medicine: the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstet. 2013;26:819-24.
- 31 - Dy F, Amirault J, Mitchell PD, Rosen R. Salivary Pepsin Lacks Sensitivity as a Diagnostic Tool to Evaluate Extraesophageal Reflux Disease. The Journal of pediatrics. 2016;177:53-8.
- 32 - Fortunato JE, D'Agostino RB, Jr., Lively MO. Pepsin in saliva as a biomarker for oropharyngeal reflux compared with 24-hour esophageal impedance/pH monitoring in pediatric patients. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2016;
- 33 - van der Pol RJ, Smits MJ, van Wijk MP, Omari TI, Tabbers MM, Benninga MA. Efficacy of proton-pump inhibitors in children with gastroesophageal reflux disease: a systematic review. Pediatrics. 2011;127:925-35.
- 34 - Haddad I, Kierkus J, Tron E, Ulmer A, Hu P, Sloan S, et al. Efficacy and safety of rabeprazole in children (1-11 years) with gastroesophageal reflux disease. Journal of pediatric gastroenterology and nutrition. 2013;57:798-807.
- 35 - Fiedorek S, Tolia V, Gold BD, Huang B, Stolle J, Lee C, et al. Efficacy and safety of lansoprazole in adolescents with symptomatic erosive and non-erosive gastroesophageal reflux disease. Journal of pediatric gastroenterology and nutrition. 2005;40:319-27.
- 36 - Baker R, Tsou VM, Tung J, Baker SS, Li H, Wang W, et al. Clinical results from a randomized, double-blind, dose-ranging study of pantoprazole in children aged 1 through 5 years with symptomatic histologic or erosive esophagitis. Clinical pediatrics. 2010;49:852-65.
- 37 - Tolia V, Ferry G, Gunasekaran T, Huang B, Keith R, Book L. Efficacy of lansoprazole in the treatment of gastroesophageal reflux disease in children. Journal of pediatric gastroenterology and nutrition. 2002;35 Suppl 4:S308-18.
- 38 - Bautista J, Fullerton H, Briseno M, Cui H, Fass R. The effect of an empirical trial of high-dose lansoprazole on symptom response of patients with non-cardiac chest pain--a randomized, double-blind, placebo-controlled, crossover trial. Alimentary pharmacology & therapeutics. 2004;19:1123-30.
- 39 - Fass R, Fennerty MB, Ofman JJ, Gralnek IM, Johnson C, Camargo E, et al. The clinical and economic value of a short course of omeprazole in patients with noncardiac chest pain. Gastroenterology. 1998;115:42-9.
- 40 - Fass R, Murthy U, Hayden CW, Malagon IB, Pulliam G, Wendel C, et al. Omeprazole 40 mg once a day is equally effective as lansoprazole 30 mg twice a day in symptom control of patients with gastro-oesophageal reflux disease (GERD) who are resistant to conventional-dose lansoprazole therapy-a prospective, randomized, multi-centre study. Alimentary pharmacology & therapeutics. 2000;14:1595-603.
- 41 - Savarino E, Zentilin P, Savarino V. NERD: an umbrella term including heterogeneous subpopulations. Nat Rev Gastroenterol Hepatol. 2013;10:371-80.
- 42 - Cheng FK, Albert DM, Maydonovitch CL, Wong RK, Moawad FJ. Categorization of patients with reflux symptoms referred for pH and impedance testing while off therapy. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2015;13:867-73.
- 43 - Singendonk MMJ, Rexwinkel R, Steutel NF, Gottrand F, McCall L, Orsagh-Yentis DK, et al. Development of A Core Outcome Set For Infant Gastroesophageal Reflux Disease. Journal of pediatric gastroenterology and nutrition. 2018;
- 44 - Loots C, Kritas S, van Wijk M, McCall L, Peeters L, Lewindon P, et al. Body positioning and medical therapy for infantile gastroesophageal reflux symptoms. Journal of pediatric gastroenterology and nutrition. 2014;59:237-43.
- 45 - Corvaglia L, Rotatori R, Ferlini M, Aceti A, Ancora G, Faldella G. The effect of body positioning on gastroesophageal reflux in premature infants: evaluation by combined impedance and pH monitoring. The Journal of pediatrics. 2007;151:591-6, 6.e1.
- 46 - Omari TI, Rommel N, Staunton E, Lontis R, Goodchild L, Haslam RR, et al. Paradoxical impact of body positioning on gastroesophageal reflux and gastric emptying in the premature neonate. The Journal of pediatrics. 2004;145:194-200.
- 47 - Vandenplas Y, De Schepper J, Verheyden S, Devreker T, Franckx J, Peelman M, et al. A preliminary report on the efficacy of the Multicare AR-Bed in 3-week-3-month-old infants on regurgitation, associated symptoms and acid reflux. Archives of disease in childhood. 2010;95:26-30.
- 48 - Moon RY, SIDS and other sleep-related infant deaths: expansion of recommendations for a safe infant sleeping environment. Pediatrics. 2011;128:1030-9.
- 49 - Loots C, Smits M, Omari T, Bennink R, Benninga M, van Wijk M. Effect of lateral positioning on gastroesophageal reflux (GER) and underlying mechanisms in GER disease (GERD) patients and healthy controls. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society. 2013;25:222-9, e161-2.
- 50 - Ness-Jensen E, Hveem K, El-Serag H, Lagergren J. Lifestyle Intervention in Gastroesophageal Reflux Disease. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2016;14:175-82.e3.
- 51 - Vandenplas Y, Hachimi-Idrissi S, Casteels A, Mahler T, Loeb H. A clinical trial with an "anti-regurgitation" formula. European journal of pediatrics. 1994;153:419-23.
- 52 - Iacono G, Vetrano S, Cataldo F, Ziino O, Russo A, Lorello D, et al. Clinical trial with thickened feeding for treatment of regurgitation in infants. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2002;34:532-3.
- 53 - Chao HC, Vandenplas Y. Comparison of the effect of a cornstarch thickened formula and strengthened regular formula on regurgitation, gastric emptying and weight gain in infantile regurgitation. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus / ISDE. 2007;20:155-60.
- 54 - Xinias I, Mouane N, Le Luyer B, Spiroglou K, Demertzidou V, Hauser B, et al. Cornstarch thickened formula reduces oesophageal acid exposure time in infants. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2005;37:23-7.
- 55 - Ostrom KM, Jacobs JR, Merritt RJ, Murray RD. Decreased regurgitation with a soy formula containing added soy fiber. Clinical pediatrics. 2006;45:29-36.
- 56 - Chao HC, Vandenplas Y. Effect of cereal-thickened formula and upright positioning on regurgitation, gastric emptying, and weight gain in infants with regurgitation. Nutrition (Burbank, Los Angeles County, Calif). 2007;23:23-8.
- 57 - Miyazawa R, Tomomasa T, Kaneko H, Morikawa A. Effect of formula thickened with locust bean gum on gastric emptying in infants. Journal of paediatrics and child health. 2006;42:808-12.
- 58 - Miyazawa R, Tomomasa T, Kaneko H, Arakawa H, Morikawa A. Effect of formula thickened with reduced concentration of locust bean gum on gastroesophageal reflux. Acta paediatrica (Oslo, Norway : 1992). 2007;96:910-4.
- 59 - Miyazawa R, Tomomasa T, Kaneko H, Morikawa A. Effect of locust bean gum in anti-regurgitant milk on the regurgitation in uncomplicated gastroesophageal reflux. Journal of pediatric gastroenterology and nutrition. 2004;38:479-83.
- 60 - Moukarzel AA, Abdelnour H, Akatcherian C. Effects of a prethickened formula on esophageal pH and gastric emptying of infants with GER. J Clin Gastroenterol. 2007;41:823-9.
- 61 - Vanderhoof JA, Moran JR, Harris CL, Merkel KL, Orenstein SR. Efficacy of a pre-thickened infant formula: a multicenter, double-blind, randomized, placebo-controlled parallel group trial in 104 infants with symptomatic gastroesophageal reflux. Clinical pediatrics. 2003;42:483-95.
- 62 - Hegar B, Rantos R, Firmansyah A, De Schepper J, Vandenplas Y. Natural evolution of infantile regurgitation versus the efficacy of thickened formula. Journal of pediatric gastroenterology and nutrition. 2008;47:26-30.
- 63 - Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). Journal of pediatric gastroenterology and nutrition. 2009;49:498-547.
- 64 - Orenstein SR, Magill HL, Brooks P. Thickening of infant feedings for therapy of gastroesophageal reflux. The Journal of pediatrics. 1987;110:181-6.
- 65 - Ummarino D, Miele E, Martinelli M, Scarpato E, Crocetto F, Sciorio E, et al. Effect of magnesium alginate plus simethicone on gastroesophageal reflux in infants. Journal of pediatric gastroenterology and nutrition. 2015;60:230-5.
- 66 - Vandenplas Y, Benninga M, Broekaert I, Falconer J, Gottrand F, Guarino A, et al. Functional gastro-intestinal disorder algorithms focus on early recognition, parental reassurance and nutritional strategies. Acta paediatrica (Oslo, Norway : 1992). 2016;105:244-52.
- 67 - Khoshoo V, Dhume P. Clinical response to 2 dosing regimens of lansoprazole in infants with gastroesophageal reflux. Journal of pediatric gastroenterology and nutrition. 2008;46:352-4.
- 68 - Famouri F, Zibanejad N, Kabiri P, Kelishadi R. Comparison of Hypoallergenic Diet vs. Ranitidine in Treatment of Gastroesophageal Reflux Disease of Infants: A Randomized Clinical Trial. 2017;27:e5343.
- 69 - Koletzko S, Niggemann B, Arato A, Dias JA, Heuschkel R, Husby S, et al. Diagnostic approach and management of cow's-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. Journal of pediatric gastroenterology and nutrition. 2012;55:221-9.
- 70 - Alsalamah M, Makhajia M, Somers G, Marcon M, Hummel D, Upton J. Anaphylaxis to Milk After Elimination Diet for Eosinophilic Gastrointestinal Disease. Am J Gastroenterol. 2016;111:752-3.
- 71 - Maslin K, Grundy J, Glasbey G, Dean T, Arshad SH, Grimshaw K, et al. Cows' milk exclusion diet during infancy: Is there a long-term effect on children's eating behaviour and food preferences? Pediatric allergy and immunology : official publication of the European Society of Pediatric Allergy and Immunology. 2016;27:141-6.
- 72 - Miller S, Comparison of the efficacy and safety of a new aluminium-free paediatric alginate preparation and placebo in infants with recurrent gastro-oesophageal reflux. Current medical research and opinion. 1999;15:160-8.
- 73 - Oderda G, Dell'Olio D, Forni M, Farina L, Tavassoli K, Ansaldi N. Treatment of childhood peptic oesophagitis with famotidine or alginate-antacid. The Italian journal of gastroenterology. 1990;22:346-9.
- 74 - Cucchiara S, Staiano A, Romaniello G, Capobianco S, Auricchio S. Antacids and cimetidine treatment for gastro-oesophageal reflux and peptic oesophagitis. Archives of disease in childhood. 1984;59:842-7.
- 75 - Woodard-Knight L, Fudge A, Teubner J, Simmer K. Aluminium absorption and antacid therapy in infancy. Journal of paediatrics and child health. 1992;28:257-9.
- 76 - Tsou VM, Young RM, Hart MH, Vanderhoof JA. Elevated plasma aluminum levels in normal infants receiving antacids containing aluminum. Pediatrics. 1991;87:148-51.
- 77 - Davies I, Burman-Roy S, Murphy MS. Gastro-oesophageal reflux disease in children: NICE guidance. BMJ (Clinical research ed). 2015;350.
- 78 - Excellence NIfHaC. Dyspepsia and Gastro-Oesophageal Reflux Disease: Investigation and Management of Dyspepsia, Symptoms Suggestive of Gastro-Oesophageal Reflux Disease, or Both. 2014;
- 79 - Simeone D, Caria MC, Miele E, Staiano A. Treatment of childhood peptic esophagitis: a double-blind placebo-controlled trial of nizatidine. Journal of pediatric gastroenterology and nutrition. 1997;25:51-5.
- 80 - Cucchiara S, Gobio-Casali L, Balli F, Magazzu G, Staiano A, Astolfi R, et al. Cimetidine treatment of reflux esophagitis in children: an Italian multicentric study. Journal of pediatric gastroenterology and nutrition. 1989;8:150-6.
- 81 - Orenstein SR, Blumer JL, Faessel HM, McGuire JA, Fung K, Li BU, et al. Ranitidine, 75 mg, over-the-counter dose: pharmacokinetic and pharmacodynamic effects in children with symptoms of gastro-oesophageal reflux. Alimentary pharmacology & therapeutics. 2002;16:899-907.
- 82 - Arguelles-Martin F, Gonzalez-Fernandez F, Gentles MG. Sucralfate versus cimetidine in the treatment of reflux esophagitis in children. The American journal of medicine. 1989;86:73-6.
- 83 - Hussain S, Kierkus J, Hu P, Hoffman D, Lekich R, Sloan S, et al. Safety and efficacy of delayed release rabeprazole in 1- to 11-month-old infants with symptomatic GERD. Journal of pediatric gastroenterology and nutrition. 2014;58:226-36.
- 84 - Moore DJ, Tao BS, Lines DR, Hirte C, Heddle ML, Davidson GP. Double-blind placebo-controlled trial of omeprazole in irritable infants with gastroesophageal reflux. The Journal of pediatrics. 2003;143:219-23.
- 85 - Orenstein SR, Hassall E, Furmaga-Jablonska W, Atkinson S, Raanan M. Multicenter, double-blind, randomized, placebo-controlled trial assessing the efficacy and safety of proton pump inhibitor lansoprazole in infants with symptoms of gastroesophageal reflux disease. The Journal of pediatrics. 2009;154:514-20.e4.
- 86 - Winter H, Kum-Nji P, Mahomedy SH, Kierkus J, Hinz M, Li H, et al. Efficacy and safety of pantoprazole delayed-release granules for oral suspension in a placebo-controlled treatment-withdrawal study in infants 1-11 months old with symptomatic GERD. Journal of pediatric gastroenterology and nutrition. 2010;50:609-18.
- 87 - Davidson G, Wenzl TG, Thomson M, Omari T, Barker P, Lundborg P, et al. Efficacy and safety of once-daily esomeprazole for the treatment of gastroesophageal reflux disease in neonatal patients. The Journal of pediatrics. 2013;163:692-8.e1-2.
- 88 - Winter H, Gunasekaran T, Tolia V, Gottrand F, Barker PN, Illueca M. Esomeprazole for the treatment of GERD in infants ages 1-11 months. Journal of pediatric gastroenterology and nutrition. 2012;55:14-20.
- 89 - Cohen S, Bueno de Mesquita M, Mimouni FB. Adverse effects reported in the use of gastroesophageal reflux disease treatments in children: a 10 years literature review. British journal of clinical pharmacology. 2015;80:200-8.
- 90 - Zohalinezhad ME, Imanieh MH, Samani SM, Mohagheghzadeh A, Dehghani SM, Haghighat M, et al. Effects of Quince syrup on clinical symptoms of children with symptomatic gastroesophageal reflux disease: A double-blind randomized controlled clinical trial. Complementary therapies in clinical practice. 2015;21:268-76.
- 91 - Ummarino D, Miele E, Masi P, Tramontano A, Staiano A, Vandenplas Y. Impact of antisecretory treatment on respiratory symptoms of gastroesophageal reflux disease in children. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus. 2012;25:671-7.
- 92 - Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. The American journal of gastroenterology. 2013;108:308-28; quiz 29.
- 93 - Cremonini F, Ziogas DC, Chang HY, Kokkotou E, Kelley JM, Conboy L, et al. Meta-analysis: the effects of placebo treatment on gastro-oesophageal reflux disease. Alimentary pharmacology & therapeutics. 2010;32:29-42.
- 94 - Chiba N, De Gara CJ, Wilkinson JM, Hunt RH. Speed of healing and symptom relief in grade II to IV gastroesophageal reflux disease: a meta-analysis. Gastroenterology. 1997;112:1798-810.
- 95 - Labenz J, Malfertheiner P. Treatment of uncomplicated reflux disease. World journal of gastroenterology. 2005;11:4291-9.
- 96 - Rosen R, Amirault J, Liu H, Mitchell P, Hu L, Khatwa U, et al. Changes in gastric and lung microflora with acid suppression: acid suppression and bacterial growth. JAMA pediatrics. 2014;168:932-7.
- 97 - Trikha A, Baillargeon JG, Kuo YF, Tan A, Pierson K, Sharma G, et al. Development of food allergies in patients with gastroesophageal reflux disease treated with gastric acid suppressive medications. Pediatric allergy and immunology : official publication of the European Society of Pediatric Allergy and Immunology. 2013;24:582-8.
- 98 - Ballengee CR, Davalian F, Conaway MR, Sauer CG, Kaufman DA. Erythromycin and Reflux Events in Premature Neonates: A Randomized Clinical Trial. Journal of pediatric gastroenterology and nutrition. 2018;67:720-5.
- 99 - Omari TI, Benninga MA, Sansom L, Butler RN, Dent J, Davidson GP. Effect of baclofen on esophagogastric motility and gastroesophageal reflux in children with gastroesophageal reflux disease: a randomized controlled trial. The Journal of pediatrics. 2006;149:468-74.
- 100 - Carroccio A, Iacono G, Montalto G, Cavataio F, Soresi M, Notarbartolo A. Domperidone plus magnesium hydroxide and aluminum hydroxide: a valid therapy in children with gastroesophageal reflux. A double-blind randomized study versus placebo. Scandinavian journal of gastroenterology. 1994;29:300-4.
- 101 - De Loore I, Van Ravensteyn H, Ameryckx L. Domperidone drops in the symptomatic treatment of chronic paediatric vomiting and regurgitation. A comparison with metoclopramide. Postgraduate medical journal. 1979;55 Suppl 1:40-2.
- 102 - Tolia V, Calhoun J, Kuhns L, Kauffman RE. Randomized, prospective double-blind trial of metoclopramide and placebo for gastroesophageal reflux in infants. The Journal of pediatrics. 1989;115:141-5.
- 103 - Bellissant E, Duhamel JF, Guillot M, Pariente-Khayat A, Olive G, Pons G. The triangular test to assess the efficacy of metoclopramide in gastroesophageal reflux. Clinical pharmacology and therapeutics. 1997;61:377-84.
- 104 - Lau Moon Lin M, Robinson PD, Flank J, Sung L, Dupuis LL. The Safety of Metoclopramide in Children: A Systematic Review and Meta-Analysis. Drug safety. 2016;39:675-87.
- 105 - Stefanidis D, Hope WW, Kohn GP, Reardon PR, Richardson WS, Fanelli RD. Guidelines for surgical treatment of gastroesophageal reflux disease. Surgical endoscopy. 2010;24:2647-69.
- 106 - Moore M, Afaneh C, Benhuri D, Antonacci C, Abelson J, Zarnegar R. Gastroesophageal reflux disease: A review of surgical decision making. World journal of gastrointestinal surgery. 2016;8:77-83.
- 107 - Kubiak R, Andrews J, Grant HW. Long-term outcome of laparoscopic nissen fundoplication compared with laparoscopic thal fundoplication in children: a prospective, randomized study. Annals of surgery. 2011;253:44-9.
- 108 - Rothenberg SS. Two decades of experience with laparoscopic nissen fundoplication in infants and children: a critical evaluation of indications, technique, and results. Journal of laparoendoscopic & advanced surgical techniques Part A. 2013;23:791-4.
- 109 - Smith CD, McClusky DA, Rajad MA, Lederman AB, Hunter JG. When fundoplication fails: redo? Annals of surgery. 2005;241:861-9; discussion 9-71.
- 110 - Kellokumpu I, Voutilainen M, Haglund C, Farkkila M, Roberts PJ, Kautiainen H. Quality of life following laparoscopic Nissen fundoplication: assessing short-term and long-term outcomes. World journal of gastroenterology. 2013;19:3810-8.
- 111 - Davis CS, Baldea A, Johns JR, Joehl RJ, Fisichella PM. The evolution and long-term results of laparoscopic antireflux surgery for the treatment of gastroesophageal reflux disease. JSLS : Journal of the Society of Laparoendoscopic Surgeons / Society of Laparoendoscopic Surgeons. 2010;14:332-41.
- 112 - Wakeman DS, Wilson NA, Warner BW. Current status of surgical management of gastroesophageal reflux in children. Current opinion in pediatrics. 2016;28:356-62.
- 113 - Baerg J, Thorpe D, Bultron G, Vannix R, Knott EM, Gasior AC, et al. A multicenter study of the incidence and factors associated with redo Nissen fundoplication in children. Journal of pediatric surgery. 2013;48:1306-11.
- 114 - Mauritz FA, van Herwaarden-Lindeboom MY, Zwaveling S, Houwen RH, Siersema PD, van der Zee DC. Laparoscopic Thal fundoplication in children: a prospective 10- to 15-year follow-up study. Annals of surgery. 2014;259:388-93.
- 115 - Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). Journal of pediatric gastroenterology and nutrition. 2009;49:498-547.
- 116 - Bohmer CJ, Klinkenberg-Knol EC, Niezen-de Boer MC, Meuwissen SG. Gastroesophageal reflux disease in intellectually disabled individuals: how often, how serious, how manageable? The American journal of gastroenterology. 2000;95:1868-72.
- 117 - Del Giudice E, Staiano A, Capano G, Romano A, Florimonte L, Miele E, et al. Gastrointestinal manifestations in children with cerebral palsy. Brain & development. 1999;21:307-11.
- 118 - de Veer AJ, Bos JT, Niezen-de Boer RC, Bohmer CJ, Francke AL. Symptoms of gastroesophageal reflux disease in severely mentally retarded people: a systematic review. BMC gastroenterology. 2008;8:23.
- 119 - Kline AD, Moss JF, Selicorni A, Bisgaard AM, Deardorff MA, Gillett PM, et al. Diagnosis and management of Cornelia de Lange syndrome: first international consensus statement. Nature reviews Genetics. 2018;19:649-66.
- 120 - Singendonk MMJ, Brink AJ, Steutel NF, van Etten-Jamaludin FS, van Wijk MP, Benninga MA, et al. Variations in Definitions and Outcome Measures in Gastroesophageal Reflux Disease: A Systematic Review. Pediatrics. 2017; Jul 27 [Epub ahead of print].
Evidence tabellen
|
Diagnostiek |
|||||||||||
|
Study |
Population |
Index test |
Index test cut-off/positivity |
Sensitivity (%) |
Specificity (%) |
PPV |
NPV |
Remarks |
|||
|
Subjects |
Age |
N |
Patients/controls (reference standard) |
|
|
|
|
|
|
|
|
|
pH-METRY |
|
||||||||||
|
Boix-Ochoa (1980)(1) |
Patients |
2 – 18 mo |
44 |
History of recurrent GER, and/or failure to thrive, and/or weight loss and/or feeding difficulties (not further specified) |
8h pH-metry – glass probe, position manometrically determined (electrode 2.5cm above LES), supine, prone and semi-seated position, symptoms recorded. |
pH in distal esophagus <4. Overall score computed from seven components, 1SD from score of each component in controls used as 1 scoring unit, final score total of all single score components: 1) the percent time pH<4 in 24h (RI, for each position); 2) total number of single refluxes pH <4; 3) number of refluxes longer than 5 minutes; 4) duration of longest episode. |
Not calculable: no p-values or cut-off values for test-positivity provided. Final score calculated based on data of controls.* Final score was highest in patient group (27,4 ± 9,2 vs 7,39 ± 4,6). |
|
|
|
Definition of GER(D) not further specified. Older children included in control group compared to patient group. No maximal value nor unit of measurement provided for the final score |
|
Controls |
2 mo – 3 yrs |
20 |
No history of GER (not further specified) |
||||||||
|
Da Dalt (1989)(2) |
Patients |
9.3 mo (1 mo – 13.5 yrs) |
111 |
Admitted patients with signs and symptoms typical of GER (vomiting (n=69), failure to thrive (n=29), feeding difficulties (n=20), hematemesis (n=15), recurrent wheezing (n=12) chronic cough (n=11), apnea (n=11), iron deficiency anemia (n=10), epigastric pain (n=10), irritability (n=7) |
24h pH-metry – glass probe, position determined by formula of Strobel (tip of catheter 87% of the distance from nares to upper limit of LES. Normal feeding and daily activities were remained. |
Drop in esophageal pH <4 for >8 seconds. Percent time pH<4 in 24h (RI), total number of reflux in 24h, number of refluxes longer than 5 minutes, duration of longest episode, mean duration of all reflux episode. Upper limit of normal based on 2SD from score of each component in controls. Measurement abnormal if percentage of reflux time and two other measurements abnormal. |
Reflux time and two other measurements abnormal: 41 (45/111) |
Not calculable: values of controls used as normal values. |
|
|
For this population, nu cut-off values have been established nor validated for pH-metry. Cut-off value for test-positivity therefore arbitrarily.
This study includes children with recurrent or persistent wheezing (>3 attacks requiring hospital visit or almost daily wheezing for >4 wks). Within this specific patient group, a division between children with and without a history suggestive or reflux is made. Therefore this study was included, but results should be interpreted in the light of the patient group (wheezers and not the general pediatric population) the study focuses on. |
|
Controls |
12.5 mo (3 – 68 mo) |
14 |
No history or symptoms suggestive of GER |
||||||||
|
Cucchiara (1990)(3) |
Patients |
GERD: 26.6 mo (2 mo – 10 yrs). GERD and esophagitis: 41.3 mo (1 mo – 12 yrs) |
114 |
Infants and children referred for symptoms suggestive of GE, all with well-documented history of vomiting/regurgitation, some with additional complications (weight failure (n=45), hematemesis (n=17), chronic respiratory symptoms (n=19). Based on endoscopy with biopsy: n=45 GERD only and n=69 GERD and esophagitis. |
24h pH-metry – glass probe, position determined by manometry or formula of Strobel (tip of catheter 87% of the distance from nares to upper limit of LES. Position confirmed by fluoroscopy. Normal feeding and daily activities were remained. Variables evaluated for entire period, wakefulness, sleep and postprandial. |
Distal esophageal pH <4 for >20 seconds, or additional decrease of >1 pH unit during period of pH <4. Percent time pH<4 in 24h (RI), total number of reflux in 24h, number of refluxes longer than 5 minutes, duration of longest episode, mean duration of all reflux episode. Normal acid exposure time/clearance time defined as <2SD from control means. |
RI: 81 (92/114) Number of refluxes > 5 min: 70 (80/114) (data on other parameters not provided) |
Not calculable: values of controls used as normal values. |
|
|
Definition of GER(D) not further specified. In this study, infants presenting with apnea and upper respiratory infection are considered as controls, despite that these symptoms can be regarded as reflux-related. It remains that these control children were not admitted/referred and did not have a clinical history suggesting GERD based on the information provided in the paper. |
|
Controls |
24.02 mo (2 mo – 12 yrs) |
63 |
Absence of typical GER symptoms, but presenting with functional abdominal pain (n=5), functional constipation (n=9), IBS (n=11), feeding problems due to maternal inexperience/anxiety (n=19), apnea (n=10), upper respiratory infections (n=9) |
||||||||
|
Kahn (1990)(4) |
Patients |
9 wks (4 – 25 wks) |
10 |
(Full-term) infants that had been found apneic, pale or cyanotic, loss of tone and consciousness and had received vigorous resuscitation, with no cause of apparent life treathening event ( ALTE) after diagnostic work-up. |
8.5h pH-metry – glass probe, position radiologically confirmed (3cm above cardia). |
Reflux episode if pH < 4. Total number of reflux in 8.5h, number of refluxes longer than 5 minutes, acid duration time (time spent with pH < 4). |
Not calculable: no p-values or cut-off values provided. |
|
|
|
Definition of GER(D) not further specified. This study includes children with ALTE. This study was included because ALTE was regarded by the authors as a possible presentation of GERD. |
|
Controls |
7 (4 – 16 wks) |
10 |
Infants with no history related to apnea or ALTE. |
||||||||
|
pH-METRY & ENDOSCOPY |
|
||||||||||
|
Cucchiara (1993) (5) |
Patients |
32.9 mo (2 – 141 mo) |
81 |
Children referred for evaluation of GERD, symptoms and signs including recurrent emesis/regurgitation (n=63), hematemesis (n=5), asthma (n=4), pneumonia (n=10), poor weight gain (n=23), apnea (n=2), irritability (n=13), anorexia (n=12), dysphagia (n=6), chest pain (n=5), heartburn (n=3), epigastric pain (n=17) |
24h pH-metry – glass probe, position determined by formula of Strobel (patients < 1 yr, tip of catheter 87% of the distance from nares to upper limit of LES) or position confirmed by fluoroscopy (patients >1 yr or >1meter height). Patients provided with standardized meals.
Endoscopy – Olympus panendoscope (2.8mm diameter bioptic channel), >2 biopies taken from distal esophagus (avoiding lower 20%) performed under general anesthesia. |
Distal esophageal pH <4 for >20 seconds. Percent time pH<4 in 24h (RI), total number of reflux in 24h, number of refluxes longer than 5 minutes. Normal acid exposure time/clearance time defined as <2SD from control means.
Aberrant macroscopy: friability, granularity, erosions, ulcerations. Aberrant histology: basal zone hyperplasia, papillar elongation, increased number of eosinophils and/or neutrophils, mucosal erosions. |
Not calculable: no p-values or cut-off values provided. No data on number of patients with abnormal test provided.
Macroscopy: 33 (27/81) Histology: 88 (71/81) |
Macroscopy: no data on controls provided. Histology: 100 (16/16) |
Macroscopy: no data on controls provided. Histology: 100 (71/71) |
Macroscopy: no data on controls provided. Histology: 62 (16/26) |
In all controls, histology as defined by the authors was normal . |
|
Controls |
7 mo (3 – 154 mo) |
16 |
Children selected for absence of symptoms of GERD, including feeding problems due to maternal inexperience/anxiety (n=5), functional abdominal pain (n=4), previous respiratory complaints (n=4), transient decreased food intake (n=3) |
||||||||
|
Ravelli (2006) (6) |
Patients |
3.95 yrs (2 mo – 11.9 yrs) |
48 |
Patients referred for diagnostic upper gastrointestinal endoscopy for symptoms suggestive of GERD: vomiting, regurgitation, epigastric pain, heartburn and/or dysphagia (n=26), crying, fussiness, back arching at meals (n=5), nocturnal cough, wheezing, recurrent pneumonia or apnea (n=17). |
24h pH-metry – antimony probe, positioned confirmed between 9th and 10th dorsal vertebra by fluoroscopy. Method not further specified.
Endoscopy – Standard videoendoscopes (outer diameters 5.3, 7.4 and 9 mm), performed under general anesthesia. 2-4 biopsies from distal esophagus 3-5cm above Z-line. |
Percent time pH<4 in 24h (RI), total number of reflux in 24h, number of refluxes longer than 5 minutes, duration of longest episode.
Aberrant macroscopy: erosive lesions. Aberrant histology: basal zone hyperplasia, papillar elongation, mucosal erosions, dilatation of interpapillary vascular spaces, increased number of neutrophils, eosinophils and lymphocytes, erosions or ulcerations and granulation tissue. |
RI: 52 (15/29)
Macroscopy: 15 (7/48) Histology: 83 (40/48) |
No controls underwent pH-metry
Macroscopy: no data on controls provided. Histology: 100 (22/22) |
Macroscopy: no data on controls provided. Histology: 100 (40/40) |
Macroscopy: no data on controls provided. Histology: 73 (22/30) |
Definition of GER(D) not further specified.
Control group includes patients with potential abnormal macroscopy and/or histology. In all controls, histology as defined by the authors was normal. No information on other possible detected macroscopic and/or histologic abnormalities provided by the authors. |
|
Controls |
5.58 yrs (1 - 16.9 yrs) |
22 |
Other manifestations, not compatible with GERD: food sensitive enterophaty (n=11), H. pylori infection with positive stool antigen or breath test (n=6), IBD (n=4), nonsteroidal anti-inflammatory drug gastropathy (n=1) |
||||||||
|
pH-METRY & GE SCINTIGRAPHY |
|
||||||||||
|
Patra (2011)(7) |
Patients |
10.4 mo (3 -24 mo, ± 5.24) |
16 |
Children 0-2 yrs with recurrent or persistent wheezing (>3 attacks requiring hospital visit or almost daily wheezing for >4 wks) with a history suggestive or reflux (not further specified) |
GE scintigraphy – dose of Tc-99m by nasogastric tube, infant placed supine, low-energy high sensitivity collimator anteriorly and posteriorly
24h pH-metry – glass probe, position radiologically confirmed, position, feeding and medication recorded (reflux medication prohibited) |
Refluxing into the esophagus on both cine images and on the time activity curve, on at least two or three consecutive frames.
RI > 10% in infants <1 yr and RI > 5% in children > 1 yr |
69 (11/16)
RI: 50 (8/16) |
78 (28/36)
RI: 82 (29/36) |
58 (11/19)
RI: 53 (8/15) |
85 (28/33)
|
Standards of interpretation of scintigraphy are poorly established.
Criteria for pathologic GER defined based on studies of Patwari et al. (2002) and VandenPlas et al. (1992). For this population, nu cut-off values have been established nor validated for pH-metry. The two studies referred to do not support the cut-off values used by the authors as a clinical diagnostic tool.Cut-off therefore arbitrary. |
|
Controls |
36 |
Children 0-2 yrs with recurrent or persistent wheezing (>3 attacks requiring hospital visit or almost daily wheezing for >4 wks) without a history suggestive or reflux (not further specified) |
|||||||||
|
pH-METRY & UPPER GI SERIES & GE SCINTIGRAPHY & ENDOSCOPY |
|
||||||||||
|
Arasu (1980)(8) |
Patients |
5.3 yrs (3 mo - 17 yrs) |
30 |
Infants/children referred with symptoms and signs suggestive of GER (not further specified) |
pH-metry – probe not specified, position based on manometry (tip of catheter 85% of the distance from nares to upper limit of LES), 5-10 minutes in supine, left lateral and right lateral decubitus positions. Total time of measurement not clear. If no spontaneous reflux observed, manual abdominal compression was performed. Total time of measurement not clear.
Upper GI series Fluoroscopy after barium swallow (volume of normal feeding), EGJ evaluated with intermittent fluoroscopy while rolling the patient from side to side, encountering maximum extent of reflux.
GE scintigraphy - dose of Tc-99m by nasogastric tube, infant upright and supine position, one minute camera pictures in both positions.
Endoscopy – Olympus panendoscope (outer diameter of 7.2mm < 4 yrs and 10 mm > 4 yrs), performed under general anesthesia. |
Intra-esophageal pH < 4 for >2 occasions (duration of event not specified)
Test positivity not further specified
Esophageal activity (not further specified)
Friability, erosion, ulceration or thickened mucosa with fine nodularity. |
97 (29/30)
Not calculable: no cut-off values for test-positivity provided.
Not calculable: no cut-off values for test-positivity provided.
71 (15/21) |
100 (15/15)
100 (3/3) |
100 (29/29)
100 (15/15) |
94 (15/16)
33 (3/9) |
Definition of GER(D) not further specified.
Positivity of pH-metry not based on any evidence. For this population, nu cut-off values have been established nor validated for pH-metry. Cut-off therefore arbitrary.
Test positivity not further specified.
Test positivity not further specified
|
|
Controls |
3.8 yrs (4 mo – 14 yrs) |
15 |
Infants/children with failure to thrive (n=6), choking with feeding (n=2), pulmonary disease (n=2), vomiting from identifiable causes apart from GER (n=5), high intestinal obstructions (n=2) |
||||||||
|
SALIVARY PEPSIN |
|
||||||||||
|
Farhath (2013)(9) |
Patients |
GA 29 wks (24 - 35) |
36 |
Premature infants, BW <2000g. Diagnosed with clinical GER if: (1) attending the neonatologist involved in clinical care and infants were on medication for GER at the time of sample collection or (2) presence of signs and symptoms of GER at the time of sample collection (persistent vomiting, apnea, bradycardia and desaturation attributed to GER, infant on prolonged or thickened feeding) |
Salivary pepsin Mouth swab samples were collected from the cheek and below the tongue at one, two and three hours after feeding. Pepsin detected by an enzymatic assay and Western blot analysis for pepsin A and C. (29/36 infants were on anti-reflux medication at time of sampling) |
Enzymatic assay positive for pepsin if concentration <12.5ng/ml. Test considered positive in case of >1 positive mouth swab sample. |
72 (26/36) |
71 (46/65) |
58 (26/45) |
82 (46/56) |
|
|
Controls |
GA 30 wks (23 - 35) |
65 |
Premature infants, BW <2000g, not fulfilling the above criteria for clinical GER. |
||||||||
|
IBS = irritable bowel syndrome; IBD = inflammatory bowel disease; GER = gastroesophageal reflux; GERD = GER disease; LES = lower esophageal sphincter; EGJ = esophageal gastric junction; GE = gastro-esophageal; GI = gastrointestinal; ALTE = apparent life-threatening event; GA = gestational age, BW = birth weight; RI = reflux index, percentage of time that the esophageal pH <4; PPV = positive predictive value; NPV = negative predictive value. *As values of controls are used as normal values, specificity will always be 100%. |
|||||||||||
|
Diagnostiek |
|||||||||||||||
|
QUADAS items |
Salivary pepsin |
pH-metry |
Endoscopy |
GI scintiscan |
Upper GI series |
||||||||||
|
|
Farhath (2013) (1) |
Boix-Ocha (1980) (2) |
Arasu (1980) (3) |
Da Dalt (1989) (4) |
Kahn (1990)1 (5) |
Cucchiara (1990) (6) |
Cucchiara (1993) (7) |
Ravelli (2006) (8) |
Patra (2011)2 (9) |
Cucchiara (1993) (7) |
Ravelli (2006) (8) |
Arasu (1980) (3) |
Arasu (1980) (3) |
Patra (2011) (9) |
Arasu (1980) (3) |
|
Was the spectrum of patients representative of the patients who will receive the test in practice? |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
|
Is the reference standard likely to correctly classify the target condition? (yes if reference test was a clinical definition of GERD)2 |
No* |
No |
No |
No* |
No |
No |
No* |
No |
No |
No* |
No |
No |
No |
No |
No |
|
Was the execution of the index test described in sufficient detail? |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
|
Were the index test results interpreted without knowledge of the results of the reference test? |
Unclear |
No |
Unclear |
No |
Yes |
Yes |
Unclear |
Yes |
Unclear |
Histology: unclear Macroscopy: yes |
Histology: unclear Macroscopy: yes |
Unclear |
Unclear |
Unclear |
Unclear |
|
Were the reference test results interpreted without knowledge of the results of the index test? |
Yes |
No |
Unclear |
No |
Yes |
Yes |
Unclear |
Yes |
Unclear |
Histology: unclear Macroscopy: yes |
Histology: unclear Macroscopy: yes |
Unclear |
Unclear |
Unclear |
Unclear |
|
Were withdrawals from the study explained? |
No |
No |
No |
No |
No |
No |
Yes |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
No |
|
Quality of evidence (Oxford Centre level of Evidence)4 |
C |
C |
C |
C |
C |
C |
C |
C |
C |
C |
C |
C |
C |
C |
C |
- This study includes children with ALTE. This study was included because ALTE was regarded as a possible presentation of GERD.
- This study includes children with recurrent or persistent wheezing (>3 attacks requiring hospital visit or almost daily wheezing for >4 weeks). Within this specific patient group, a division between children with and without a history suggestive or reflux is made. Therefore this study was included, but results should be interpreted in the light of the patient group (wheezers and not the general pediatric population) the study focuses on.
- Since GERD signs and symptoms are not distinctive, and therefore, difficult to diagnose, it is not clear if the reference standard (signs and symptoms) used in the included studies was correctly classifying the target condition. Studies marked with an (*) however did provide a clear definition/description of GERD.
- All studies are case-control study, poor or non-independent reference standard and thus level 4 studies: grade of recommendation C.
Verantwoording
Beoordelingsdatum en geldigheid
Publicatiedatum : 01-06-2014
Beoordeeld op geldigheid : 01-07-2019
De richtlijn dient elke 5 jaar gereviseerd te worden.
Algemene gegevens
De ontwikkeling van de richtlijn gastro-oesofageale reflux ziekte bij kinderen is gefinancierd door Stichting Kwaliteitsgelden Medisch Specialisten (SKMS).
Doel en doelgroep
De richtlijn is geschreven voor alle behandelaren die te maken hebben met deze groep kinderen van de nulde tot de derdelijns gezondheidszorg. Het doel van deze richtlijn is te komen tot een betere herkenning, optimalisering van de diagnostiek en behandeling van GORZ bij kinderen van 0 tot 18 jaar. Om hierover gefundeerde aanbevelingen te kunnen doen, wordt een samenvatting gegeven van de wetenschappelijke stand van zaken en kennis uit de praktijk betreffende GOR en GORZ bij kinderen volgens de methode van evidence-based richtlijnontwikkeling.1, 2 Specifieke patiëntenpopulaties en hoog risicogroepen worden in een afzonderlijke paragraaf besproken. Er wordt in deze richtlijn onderscheid gemaakt tussen zuigelingen (0 tot 12 maanden) en oudere (12 maanden tot 18 jaar) kinderen en er wordt een een grens van 12 maanden aangehouden volgens de definitie van de World Health Organization. Wanneer geen leeftijdsspecificatie vermeld wordt, gelden uitspraken en aanbevelingen voor gehele populatie kinderen 0 – 18 jaar.
De richtlijn kan dienen als ondersteuning in het besluitvormingsproces, moet leiden tot een verbetering van de kwaliteit en doelmatigheid van het medisch handelen en moet meer uniformiteit in de praktijkvoering teweegbrengen. Deze richtlijn tracht duidelijke handvatten te bieden over wanneer en hoe ouders en patiënten op passende wijze kunnen worden gerustgesteld en biedt links naar downloadbare informatie. Er worden aanbevelingen gedaan over het op het juiste moment inzetten van diagnostiek en behandeling, met als doel doorverwijzing voor onnodige tests of het gebruik van medicatie zonder bevestigd effect te beperken. Echter, bij ernstige of evoluerende symptomen (met name potentiële rode vlag signalen), geeft de richtlijn aanbevelingen met betrekking tot acties die duidelijk noodzakelijk zijn bij onderzoek, behandeling en verwijzing.
De aanbevelingen in de richtlijn zijn te vertalen naar lokale protocollen die zijn toegespitst op de plaatselijke situatie. De behandelaar heeft de autonomie om, wanneer hij/zij dat nodig acht, beargumenteerd van de geformuleerde richtlijn af te wijken. Verwijzing naar een kinderarts MDL voor de diagnose en de behandeling van gecompliceerde pediatrische patiënten is ideaal; in situaties waarin dit niet mogelijk is, wordt in deze richtlijn rekening gehouden met mogelijke alternatieve opties.
Samenstelling werkgroep
De werkgroep is multidisciplinair samengesteld: zoveel mogelijk beoefenaars uit uiteenlopende disciplines, betrokken bij diagnostiek en behandeling van gastro-oesofageale refluxziekte bij kinderen in de eerste, tweede en derde lijn, zijn verzocht te participeren, als ook vertegenwoordigers vanuit patiëntenverenigingen. Leden van de werkgroep werden via de betreffende (wetenschappelijke) verenigingen verzocht zitting te nemen in de werkgroep op grond van hun persoonlijke expertise en/of affiniteit met het onderwerp. Zij ontvingen voor hun aanwezigheid bij werkgroepvergaderingen vacatiegelden en een reiskostenvergoeding.
AJN: mw. E. Vlaanderen
NVZA: mw. B. Witjes
NVMDL: dhr. prof. dr. A.J. Bredenoord
NVKC: mw. dr. M. Lindeboom
NHG: dhr. dr. G. Elshout
NVKMDL: dhr. prof. dr. M.A. Benninga
NVAVG: mw. M. Walinga (meelezer)
Kind en Ziekenhuis: mw. R. de Jonge (meelezer)
Samenstelling kernwerkgroep (2018)
Mw. Dr. M.M. Tabbers, projectleider
Mw. Dr. M.M.J. Singendonk
Belangenverklaringen
De werkgroepleden hebben een belangenverklaring ingevuld waarin ze hun eventuele banden met de farmaceutische industrie hebben aangegeven. De verklaringen liggen ter inzage bij de NVK.
Inbreng patiëntenperspectief
Het perspectief van patiënten wat betreft de zorg rondom GORZ vormt een waardevolle aanvulling bij de totstandkoming van een richtlijn over GORZ bij kinderen. Er is geen patiëntenvereniging specifiek voor kinderen met GORZ.
Methode ontwikkeling
Evidence based
Implementatie
De richtlijn is onder de verenigingen verspreid en via de websites van de verenigingen elektronisch beschikbaar gesteld. Op wetenschappelijke bijeenkomsten van de betrokken wetenschappelijke verenigingen zijn de aanbevelingen van de richtlijn gepresenteerd. Verder is er patiëntenvoorlichtingsmateriaal ontwikkeld ter ondersteuning van de richtlijn. Daarnaast zijn indicatoren ontwikkeld om te meten of de implementatie van de richtlijn daadwerkelijk effectief is geweest.
Werkwijze
Allereerst werd door middel van het versturen van vragenlijsten een knelpuntanalyse uitgevoerd om de huidige werkwijze ten aanzien van de diagnostiek en behandeling van kinderen met GORZ in de nulde t/m de derdelijns gezondheidszorg in Nederland in kaart te brengen. Op basis van de resultaten van de knelpuntenanalyse werden met de werkgroep de uitgangsvragen opgesteld. Vervolgens werd samen met een adviseur van het Kwaliteitsinstituut voor de Gezondheidszorg CBO volgens de methode van Evidence-based Richtlijn Ontwikkeling per vraag een uitgebreid literatuuronderzoek verricht. In eerste instantie werd gezocht naar Evidence based richtlijnen. De gevonden richtlijnen werden op kwaliteit beoordeeld door de kernwerkgroepleden met behulp van het Appraisal of Guidelines for Research & Evaluation (AGREE)-instrument. Wanneer er een valide richtlijn werd gevonden, werd de evidence uit de richtlijn gebruikt om de vragen te beantwoorden. Wanneer er geen geschikte richtlijn werd gevonden, werd vervolgens gezocht naar systematische literatuuroverzichten. Ook deze werden op inhoudelijke en methodologische kwaliteit beoordeeld door de kernwerkgroepleden. Bij het vinden van een valide systematic review voor beantwoording van één van de vragen, werden zowel de review als ook de afzonderlijke studies besproken in de betreffende modules. Vervolgens werd naar aanvullende studies gezocht vanaf het moment waar de zoekactie in de review eindigde.
Voor GOR en GORZ werden de volgende zoektermen gebruikt: “gastro(o)esophageal reflux” en afkortingen, “gastric acid reflux” en “(o)esophagitis” waarbij rekening werd gehouden met verschillen in de Britse en Amerikaanse spelling. Details over de zoekstrategie zijn weergegeven in Appendix 1. Er werd geen taalbeperking opgelegd.
Inclusiecriteria waren als volgt (er moest voldaan worden aan alle inclusiecriteria relevant voor de onderzoeksvraag):
- Studiepopulatie bestaande uit kinderen met GORZ in de leeftijd van 0 tot 18 jaar.
- Voor diagnostische studies (vraag 1) werden systematische reviews en originele onderzoeken met betrekking tot de diagnostische nauwkeurigheid van de specifieke diagnostische tests geïncludeerd. De referentiestandaard voor GORZ moest door auteurs worden gedefinieerd aan de hand van anamnese en lichamelijk onderzoek.
- Therapeutische randomized controlled trials (uitgangsvragen 2 en 3) werden alleen geïncludeerd wanneer zij minstens 10 personen per onderzoeksarm bevatten.
In 2018 – 2019 vond een update plaats van NVK richtlijn uit 2012 (zoekactie tot juni 2018) die gefinancierd werd door Stichting Kwaliteitsgelden Medisch Specialisten.
Bij deze update werd weer een knelpuntanalyse eerst uitgevoerd onder de werkgroepleden. Vervolgens werd er voor de therapeutische vragen nu gebruik gemaakt van The Grading of Recommendations Assessment, Development and Evaluation (GRADE). De GRADE-methode heeft als doel om de kwaliteit van evidence transparant weer te geven. Aan het begin van het richtlijntraject werden uitkomstmaten gedefinieerd. In overeenstemming met de meest recente pediatrische richtlijn, werd gebruik gemaakt van de volgende acht uitkomstmaten: oesofagitis (endoscopisch/histologisch), GOR-gerelateerde complicaties (Barrett metaplasie, stenose, en andere zoals gespecificeerd door auteurs), GOR-gerelateerde klachten en symptomen (gemeten met de infant gastroesophageal reflux questionnaire revised, I-GERQ-R), kwaliteit van leven (zowel van de ouder als de patiënt), huilen en onrust (rapportage door de ouder), spugen en/of regurgiteren (rapportage door de ouder en/of patiënt), zuurbranden (rapportage door de ouder en/of patiënt), en bijwerkingen van de behandeling.
Resultaten werden per uitkomstmaat samengevat, waarbij tevens de ‘overall’ kwaliteit van de onderliggende bewijslast (evidence) werd aangegeven. Bij de beoordeling werd gebruik gemaakt van de software “GRADE-pro”. Met behulp van dit programma werd bij elke uitgangsvraag een tabel met de beoordeling van het bewijs (“GRADE evidence profile”) gemaakt. Deze tabellen zijn bij elk uitgangsvraag te vinden.
GRADE kent vier niveaus: ‘high’ (hoog), ‘moderate’ (matig), ‘low’ (laag) en ‘very low’ (zeer laag). Per uitkomstmaat werd voor de kwaliteit van het bewijs met behulp van GRADE-pro een GRADE niveau toegekend.
‘Hoog’: Wanneer de kwaliteit van bewijs voor een uitkomst als ‘high’ ofwel ‘hoog’ geclassificeerd werd, wil dit zeggen dat het onwaarschijnlijk is dat toekomstig onderzoek de schatting van de uitkomst zal veranderen. Met andere woorden, er is veel vertrouwen in de juistheid van de schatting van de uitkomst.
‘Matig’: Wanneer de kwaliteit van bewijs voor een uitkomst als ‘moderate’ ofwel ‘matig’ geclassificeerd werd, wil dit zeggen dat het waarschijnlijk is dat toekomstig onderzoek effect heeft op het vertrouwen in de schatting van de uitkomst en zou de schatting van de uitkomst kunnen veranderen. Met andere woorden, er is matig vertrouwen in de juistheid van de schatting van de uitkomst.
‘Laag’: Wanneer de kwaliteit van bewijs voor een uitkomst als ‘low’ ofwel ‘laag’ geclassificeerd werd, wil dit zeggen dat het heel waarschijnlijk is dat toekomstig onderzoek effect heeft op het vertrouwen in de schatting van de uitkomst en zal deze schatting waarschijnlijk veranderen. Met andere woorden, er is beperkt vertrouwen in de juistheid van de schatting van de uitkomst.
‘Zeer laag’: Een ‘very low’ ofwel ‘zeer lage’ classificatie wil zeggen dat er veel onzekerheid is over de juistheid van de uitkomst.
De onderzoeksopzet is een belangrijke factor binnen GRADE. Gerandomiseerde en
gecontroleerde studies krijgen daarom in beginsel de kwalificatie ‘hoog’. Er zijn vijf factoren
die kunnen zorgen voor een lagere kwalificatie:
- Beperkingen in de onderzoeksopzet.
- Inconsistentie: onverklaarde heterogeniteit van de resultaten.
- Indirectheid: PICO waarop de evidence gebaseerd is wijkt op een of meer punten af van de PICO die men wil onderzoeken. Ook het gebruik van surrogaatmarkers valt onder indirectheid.
- Imprecisie: wijde betrouwbaarheidsintervallen rond een geschat effect duiden op onzekerheid in de grootte van het effect. Er is sprake van imprecisie bij een te kleine steekproef (lage statistische power), weinig gebeurtenissen (events) en een betrouwbaarheidsinterval dat wel statistisch significant is maar, zowel in het gebied van klinische relevantie als in het gebied van een verwaarloosbaar effect ligt.
- Publicatiebias.
Er zijn drie factoren die kunnen zorgen voor een hogere kwalificatie:
- Groot effect.
- Aanwezigheid van dosisresponsrelatie.
- Confounding die het werkelijke effect onderschat of een in werkelijkheid niet bestaand effect overschat.
Iedere beperkende (of bevorderende) factor kan leiden tot het verlagen (of verhogen) van de classificatie met een of twee niveaus. Indien de resultaten niet gepoold konden worden, werd volstaan met een globale inschatting van de kwaliteit van de onderliggende bewijslast. Voor een uitgebreidere beschrijving van GRADE verwijzen we naar www.gradeworkinggroup.org.
Uitgangsvragen
Uitgangsvraag 1:
Wat is, ten opzichte van de anamnese en lichamelijk onderzoek, de aanvullende diagnostische waarde van onderstaande onderzoeken bij het stellen van de diagnose GORZ bij kinderen van 0 – 18 jaar van:
- Endoscopie met biopten
- pH-metrie
- pH-impedantiemetrie
- Scintigrafie
- Röntgenonderzoek (barium slikfoto)
- Manometrie
- Biomarkers
- Proefbehandeling met PPI
Uitgangsvraag 2:
Welke niet-farmacologische interventies zijn effectief en veilig voor de behandeling van GORZ bij kinderen van 0 – 18 jaar?
- Ondersteuning en educatie van patiënt en ouders
- Leefstijladviezen
- Houdingsadviezen
- Verdikken van de voeding
- Vermindering voedingsvolume of -frequentie
- Eliminatie van koemelkeiwit
Uitgangsvraag 3:
Welke farmacologische interventies zijn effectief en veilig voor de behandeling van GORZ bij kinderen van 0 – 18 jaar?
- Antacida en alginaten
- Zuurremming (histamine-2-receptor antagonist (H2-antagonist) en protonpompremmers (proton pump inhibitors, PPIs))
- Prokinetica
Uitgangsvraag 4:
Bij welke kinderen met GORZ is chirurgie geïndiceerd boven (niet-)farmacologische behandeling?
Uitgangsvraag 5:
Wanneer dient de nulde of eerste lijn naar de tweede lijn te verwijzen en wanneer dient de tweede lijn naar de derde lijn te verwijzen bij kinderen van 0 – 18 jaar met klachten die wijzen op GORZ?
Totstandkoming van de aanbevelingen
Voor het komen tot een aanbeveling zijn er naast het wetenschappelijk bewijs ook andere aspecten van belang, bijvoorbeeld: patiëntenvoorkeuren, beschikbaarheid van speciale technieken of expertise, organisatorische aspecten, maatschappelijke consequenties en kosten. Deze aspecten worden besproken na de ‘Conclusie’. Hierin wordt de conclusie op basis van de literatuur geplaatst in de context van de dagelijkse praktijk en vindt een afweging plaats van de voor- en nadelen van de verschillende beleidsopties. De uiteindelijk geformuleerde aanbeveling is het resultaat van het beschikbare bewijs in combinatie met deze overwegingen. Het volgen van deze procedure en het opstellen van de richtlijn in dit ‘format’ heeft als doel de transparantie van de richtlijn te vergroten. Het biedt ruimte voor een efficiënte discussie tijdens de werkgroepvergaderingen en vergroot bovendien de helderheid voor de gebruiker van de richtlijn.
Juridische betekenis van richtlijnen
Richtlijnen zijn geen wettelijke voorschriften maar wetenschappelijk onderbouwde en breed gedragen inzichten en aanbevelingen. Hieraan moeten zorgverleners voldoen om kwalitatief goede zorg te verlenen. Zorgverleners kunnen op basis van hun professionele autonomie afwijken van de richtlijn. De aanbevelingen zijn immers hoofdzakelijk gebaseerd op de ‘gemiddelde patiënt’. Afwijken van richtlijnen is, als de situatie van de patiënt dat vereist, soms zelfs noodzakelijk. Wanneer van de richtlijn wordt afgeweken moet dit echter beargumenteerd, gedocumenteerd en, waar nodig, in overleg met de patiënt worden gedaan.
Zoekverantwoording
Database(s): Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations and Ovid MEDLINE(R) 1946 to Present
Search Strategy:
|
# |
Searches |
Results |
|
1 |
exp Gastroesophageal Reflux/ or esophagitis/ or esophagitis, peptic/ or (gastroesophageal adj reflux).ti,ab. or (gastrooesophageal adj reflux).ti,ab. or (gastro esophageal adj reflux).ti,ab. or (gastro oesophageal adj reflux).ti,ab. or (GORD or GOR or GERD or GER).ti,ab. or (esophagitis or oesophagitis).ti,ab,kw. or (gastric adj3 (acid or reflux)).ti,ab. or (reflux adj (oesophagitis or esophagitis)).ti,ab. or (erosive adj3 (oesophag* or esophag*)).ti,ab. |
50237 |
|
2 |
adolescent/ or child/ or child, preschool/ or infant/ or infant, newborn/ or infant, low birth weight/ or infant, postmature/ or infant, premature/ or exp Pediatrics/ or (child* or infant* or infancy or newborn* or neonat* or baby or babies or preschool or pre school or pubescen* or teen* or adolescen* or puber* or prepubert* or juvenil* or p?ediatric* or youth* or schoolchild* or school age* or schoolage* or preschool or pre-school or elementary school or high school* or highschool* or kindergar* or boy or boys or girl* or minor* or underag* or under ag* or kid or kids or toddler*).ti,ab. |
3669364 |
|
3 |
*diagnostic techniques, digestive system/ or *Gastroesophageal Reflux/di or *Gastroesophageal Reflux/ra or esophageal ph monitoring/ or Barium Sulfate/ or esophagoscopy/ or gastroscopy/ or exp Biopsy/ or exp Proton Pump Inhibitors/du or Electric Impedance/ or exp Ultrasonography/ or Manometry/ or exp Radionuclide Imaging/ or endoscopy, digestive system/ or exp endoscopy, gastrointestinal/ or (barium or proton pump inhibitor* or PPI or PPIs or oesophagogastroduodenoscop* or esophagogastroduodenoscop*or esophagogastroscop* or oesophagogastroscop* or oesophago-gastroduodenoscop* or esophago-gastroduodenoscop* or esophago-gastroscop* or oesophago-gastroscop* or oesophago-gastro-duodenoscop* or esophago-gastro-duodenoscop* or gastroscop* or esophagoscop* or oesophagoscop* or biops* or pH-metry or pH-MII or impedance or manometr* or motility or HRM or HRIM or scintigraph* or ultraso*).ti,ab. or ((oesophag* or esophagi* or PH) adj1 (monitoring* or recording* or measure*)).ti,ab,kw. |
1179018 |
|
4 |
"Sensitivity and Specificity"/ or *diagnosis/ or diagnosis, differential/ or *Diagnostic Techniques, Digestive System/ or Gastric Acidity Determination/ or *Gastroesophageal Reflux/di or Gastrointestinal Motility/ or Reproducibility of Results/ or (sensitiv* or specific* or value* or diagnos* or accura*).ti,ab. |
6078599 |
|
5 |
Animals/ not Humans/ |
3963496 |
|
6 |
exp Animals, Laboratory/ or exp Animal Experimentation/ or exp Models, Animal/ or exp Rodentia/ or (rat or rats or mouse or mice).ti. or editorial/ or letter/ or news/ or Comment/ or exp historical article/ or Anecdotes as Topic/ or Case Reports/ or (letter* or comment* or abstracts).ti. |
6414567 |
|
7 |
(1 and 2 and 3 and 4) not 5 not 6 |
2703 |
|
8 |
limit 7 to yr="2008 -Current" |
856 |
Database(s): Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations and Ovid MEDLINE(R) 1946 to Present
Search Strategy:
|
# |
Searches |
Results |
|
1 |
exp Gastroesophageal Reflux/ or esophagitis/ or esophagitis, peptic/ or (gastroesophageal adj reflux).ti,ab. or (gastrooesophageal adj reflux).ti,ab. or (gastro esophageal adj reflux).ti,ab. or (gastro oesophageal adj reflux).ti,ab. or (GORD or GOR or GERD or GER).ti,ab. or (esophagitis or oesophagitis).ti,ab,kw. or (gastric adj3 (acid or reflux)).ti,ab. or (reflux adj (oesophagitis or esophagitis)).ti,ab. or (erosive adj3 (oesophag* or esophag*)).ti,ab. |
50237 |
|
2 |
adolescent/ or child/ or child, preschool/ or infant/ or infant, newborn/ or infant, low birth weight/ or infant, postmature/ or infant, premature/ or exp Pediatrics/ or (child* or infant* or infancy or newborn* or neonat* or baby or babies or preschool or pre school or pubescen* or teen* or adolescen* or puber* or prepubert* or juvenil* or p?ediatric* or youth* or schoolchild* or school age* or schoolage* or preschool or pre-school or elementary school or high school* or highschool* or kindergar* or boy or boys or girl* or minor* or underag* or under ag* or kid or kids or toddler*).ti,ab. |
3669364 |
|
3 |
exp Biological Markers/ or (biomarker* or biological marker* or transpyloric feed* or transpyloric food* or pyloric feed* or pyloric food*).ti,ab. or saliva/ or sputum/ or (saliva* or sputum).ti,ab,kw. or ((esophag* or oesophag* or ear or trachea* or gastr* or pulmon*) and (fluid* or juice* or effusion)).ti,ab,kw. |
882966 |
|
4 |
"Sensitivity and Specificity"/ or *diagnosis/ or diagnosis, differential/ or *Diagnostic Techniques, Digestive System/ or Gastric Acidity Determination/ or *Gastroesophageal Reflux/di or Gastrointestinal Motility/ or Reproducibility of Results/ or (sensitiv* or specific* or value* or diagnos* or accura*).ti,ab. |
6078599 |
|
5 |
Animals/ not Humans/ |
3963496 |
|
6 |
exp Animals, Laboratory/ or exp Animal Experimentation/ or exp Models, Animal/ or exp Rodentia/ or (rat or rats or mouse or mice).ti. or editorial/ or letter/ or news/ or Comment/ or exp historical article/ or Anecdotes as Topic/ or Case Reports/ or (letter* or comment* or abstracts).ti. |
6414567 |
|
7 |
(1 and 2 and 3 and 4) not 5 not 6 |
270 |