Plaat osteosynthese versus K-draad bij distale radiusfractuur
Uitgangsvraag
Welke operatietechniek heeft de voorkeur bij patiënten die zich presenteren met een gedisloceerde distale radius fractuur: gesloten repositie met K-draad fixatie of open repositie met plaat osteosynthese?
Aanbeveling
Verricht bij voorkeur open repositie en interne fixatie middels plaat-schroef osteosynthese bij volwassen patiënten met een distale radius fractuur en een gestelde operatie-indicatie.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Op basis van de beschikbare literatuur is er geen duidelijke voorkeur voor gesloten repositie en K-draad fixatie of open reductie en plaat osteosynthese voor de chirurgische behandeling van distale radius fracturen bij volwassenen, wanneer er wordt gekeken naar de uitkomst na een jaar. Er lijkt geen verschil in DASH- en PRWE-scores na een follow up van minimaal een jaar. Echter het aantal infecties is mogelijk wel hoger in de K-draad groep (gebaseerd op een lage bewijskracht). Voor range of motion, pees- en zenuwletsel, re-interventies en radiologische uitkomsten is het onduidelijk wat het effect van K-draden of plaat fixatie is op deze uitkomstmaten.
De geïncludeerde studies bevatten kleine patiënten aantallen en hadden een aantal beperkingen. Geen van de studies was geblindeerd. Daarnaast werden alleen in de studies van Chung (2019), Costa (2014), Costa (2019) en Goehre (2014) deelnemers exact geanalyseerd in de groepen waarin ze gerandomiseerd waren (intention to treat analyse). De overall bewijskracht voor de cruciale uitkomstmaat PRWE- en DASH score kwam daardoor uit op laag, range of motion op zeer laag en de bewijskracht voor de belangrijke uitkomstmaten was met uitzondering van de complicatie infecties, zeer laag. Verder werd er niet geclassificeerd naar fractuurtype en type A, B en C fracturen werden alle geïncludeerd. De studie van Costa (2014) randomiseerde 461 patiënten. Echter, 178 potentiële kandidaten weigerden mee te doen dit kan geleid hebben tot een selectie. Wat verder opvalt is dat 75 % van de plaatosteosynthese patiënten werden nabehandeld in een gips. Hoelang deze immobilisatie duurde werd echter niet vermeld. Opvallend is dat er tussen beide groepen na 6 weken geen verschil in PROM’s meetbaar is, terwijl in de meeste studies er na 6 weken een voordeel voor de plaat groep is, wat wordt toegerekend aan het vroege oefenen.
Waarden en voorkeuren van patiënten (en eventueel hun verzorgers)
Het doel van de operatie is een pijnvrije pols met een volledige functie. Echter, het tijdsinterval waarin dat bereikt wordt kan ook van invloed zijn. Het voordeel van plaatosteosynthese boven K-draden lijkt met name te liggen in het postoperatieve traject, de betere mogelijkheden een anatomische repositie te verkrijgen en de kortere tijd naar volledig herstel alsmede de mogelijk lagere kans op een infectie. Na K-draad fixatie worden patiënten nabehandeld met 5 tot 6 weken gips immobilisatie. Echter, na plaatfixatie kunnen de patiënten onbelast oefenen. Dit onbelast oefenen heeft een positief effect op hun ADL en snelheid van herstel. De studie van Rozental (2009) lijkt dan ook een klinisch relevant verschil in DASH scores te laten zien na 3 maanden. (DASH score (points) 11 ± 13 versus 26 ± 23.) Het voordeel van K-draden is dat de ingreep goedkoper is door het gebruikte materiaal en er hoeft ook later niet te worden overgegaan tot meer invasieve verwijdering van het osteosynthese materiaal. Echter, dit gaat dan mogelijk wel gepaard met meer infecties.
Kosten (middelenbeslag)
Een kosteneffectiviteitsanalyse gebaseerd op de data van de studie van Costa (Tubeuf, 2015) liet het volgende zien: De gemiddelde QALY’s (quality adjusted life years) gedurende 12 maanden waren iets hoger in de locking plate groep (0,742; standard deviation (SD) 0,156) dan in de K-draden groep (0,734; SD 0,167) maar het verschil was niet significant (0,013; SD 0,005; p-value 0,649, t-test).
De gemiddelde totale kosten voor het gebruik van NHS-middelen bedroegen respectievelijk £ 3385 (SD 2097,09) voor K-draad en £ 4288 (SD 2244,30) voor een plaat en waren significant hoger in de plaatgroep (£ 903, SD 260,43; p-waarde < 0,001, t-toets).
Inkomensverlies en productiviteitsverlies als gevolg van ziekteverzuim waren hoger in de K-draad-groep, maar het verschil was niet significant (- £ 120,44; SD 203,16; p-waarde 0,405, t-test). De totale maatschappelijke kosten, exclusief ziekenhuiskosten, waren gemiddeld £ 48 (SD 360,04) hoger in de K-draad groep.
De resultaten laten zien dat behandeling met platen duurder is dan met K-draden met een gemiddelde meerprijs van £ 726,46 (95% betrouwbaarheidsinterval (CI) 558,44 tot 864,48) per patiënt en een grotere, zij het kleine, winst in QALY’s. Het verschil in QALY-winst was 0,008 QALY's (wat overeenkomt met drie extra dagen perfecte gezondheid per jaar) tussen beide groepen.
In de steekproef van patiënten ouder dan 50 suggereerde de evaluatie dat patiënten die werden behandeld middels volaire plaatfixatie 0,018 QALY's meer behaalden dan degenen die werden behandeld middels K-draadfixatie, tegen een hogere kostprijs van £ 629 per patiënt, wat een ICER oplevert van £ 35.323 per QALY.
Aanvaardbaarheid, haalbaarheid en implementatie
De grootste belemmerende factor voor implementatie van standaard volaire plaatfixatie in plaat van K-draad fixatie zijn de kosten. De gemiddelde primaire kosten zijn ongeveer 700 euro hoger voor de plaat groep. Echter, hierbij kan de patiënt gelijk bewegen, heeft een lager inkomensverlies en een lagere kans op een infectie en betere PROMs de eerste maanden. Dit in ogenschouw nemend ziet de commissie weinig belemmerende factoren voor implementatie van open repositie en interne fixatie.
De werkgroep voorziet geen problemen, gezien van alle operateurs verwacht wordt alle bijbehorende operatieve technieken te beheersen.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Plaatfixatie van een distale radiusfractuur heeft voordelen ten opzichte van gesloten repositie en K-draad fixatie. Het is aannemelijk dat de PROMs de eerste maanden beter zijn. Dit heeft waarschijnlijk te maken met het vroegtijdig kunnen mobiliseren van de geopereerde pols van patiënten. Verder zijn er aanwijzingen in de literatuur dat plaatfixatie leidt tot minder infecties dan K-draad fixatie. De studie van Costa (2014) toont aan dat de kosten voor plaatfixatie hoger zijn dan K-draad fixatie, echter het productiviteitsverlies was hoger in de K-draad groep. De werkgroep is van mening dat vroegtijdig mobiliseren een voordeel heeft voor de patiënt en de snelheid van de revalidatie ten goede komt. Dit argument heeft de werkgroep zwaar laten meewegen in de aanbeveling. Echter, na een follow-up van minimaal een jaar is het verschil in PROMs verwaarloosbaar, dus lijkt er met name een korte-termijn voordeel te zijn voor deze functionele uitkomstmaat.
Onderbouwing
Er bestaan verschillende operatieve technieken voor gedisloceerde distale radiusfracturen. Twee bekende en veel gebruikte technieken zijn gesloten repositie met K-draad fixatie (in de tekst ook wel afgekort als K-draden) en open reductie met plaat osteosynthese. De vraag is nu welke techniek leidt tot de beste resultaten. De primaire uitkomst maat betreft gevalideerde patient reported outcome measures (PROM’s). Secundaire uitkomsten betreffen range of motion (ROM), radiologische parameters, complicaties zoals infecties, pees- en zenuw letsels en re-operaties.
|
Low GRADE |
The patient reported outcome measure scores (PROMs) after 12 months of follow up are possibly comparable between patients treated with closed reduction and Kirschner wire fixation and open reduction and plate fixation for the treatment of distal radial fractures in adult patients.
Sources: (Costa, 2019; Goehre, 2014; Youlden, 2019) |
|
Very low GRADE |
It is uncertain whether treatment with closed reduction and Kirschner wire fixation results in less range of motion compared to open reduction and plate fixation for the treatment of distal radial fractures in adult patients.
Sources: (Costa, 2019; Goehre, 2014; Youlden, 2019) |
|
- GRADE |
Because of a lack of data, it was not possible to compare pain following closed reduction and Kirschner wire fixation to open reduction and plate fixation in patients with a displaced distal radius fracture. |
|
Very low GRADE |
It is uncertain whether the treatment with closed reduction and Kirschner wire fixation results in inferior radiographic parameters compared to open reduction and plate fixation for the treatment of distal radial fractures.
Sources: (Goehre, 2014; Youlden, 2019) |
|
Low GRADE |
Patients treated with closed reduction and Kirschner wire fixation possibly have more infections compared to patients treated with open reduction and plate fixation for the treatment of distal radial fractures.
Sources: (Chung, 2019; Youlden, 2019) |
|
Very low GRADE |
It is uncertain whether treatment with closed reduction and Kirschner wire fixation results in less nerve- and tendon injuries compared to open reduction and plate fixation for the treatment of distal radial fractures in adult patients.
Sources: (Chung, 2019; Goehre, 2014; Youlden, 2019) |
|
Very low GRADE |
It is uncertain whether treatment with closed reduction and Kirschner wire fixation results in less reinterventions compared to open reduction and plate fixation for the treatment of distal radial fractures in adult patients.
Sources: (Chung, 2019; Goehre, 2014; Youlden, 2019) |
Description of studies
A total of 1 systematic review (Youlden, 2019), 1 study reporting the five-year follow-up of an RCT (Costa, 2014) included in the review of Youlden (2019) and 2 additional RCTs were included in this literature summary.
Chung (2019) performed a multicenter Wrist and Radius Injury Surgical Trial (WRIST) (RCT) among adults 60 years or older with isolated unstable distal radius fractures at 24 health sites in the United States, Canada, and Singapore. Participants opting for surgery were randomized to receive VLPs (volar locking plates) (n = 65), K-wires (n = 58), or bridging external fixation with or without supplemental pinning (n = 64). Patients who chose not to have surgery (n = 117) were not randomized and were enrolled for casting. Only data of percutaneous pinning, VLPs were extracted for this literature summary. The RCT was not double blind because of the nature of the intervention. Intention-to-treat analyses were performed. No participants randomized to the VLPs arm crossed over to another treatment. Of the participants randomized to pinning, 9 did not receive pinning. Only complications and reinterventions were reported.
Costa (2019) reported the 5-year follow-up of the RCT described in Costa (2014) (RCT included in systematic review Youlden, 2019). At year 5 data was available for 93 (43%) of the 217 in the K-wire group versus 105 (45%) of the 231, 48 in the plate fixation group.
In addition, the RCT of Goehre (2014) was included in this literature summary. It was excluded in the review of Youlden (2019) because 40 patients aged over 65 years were included of whom 19 received K-wires and 21 plate fixations. The follow-up was 1 year. The RCT was not double blind because of the nature of the intervention.
Youlden (2019) included randomized controlled trials (RCTs) and comparative studies with a follow-up of at least 1 year that compared K-wires with volar locking plates (VLP) in adult patients with distal radius fractures. Adjunctive external fixation for the K-wires group was accepted, as long as the intent was to use only K-wires. Studies were excluded if studies; had less than 20 patients, included patients with open fractures, vascular injuries, multiple fractures or bilateral fractures, evaluated isolated external fixation methods or evaluated elderly patients (>65). Electronic databases up to November 2017 were searched. A total of 14 studies (five randomized controlled trials and nine comparative studies) were included. Only results of the 5 RCTs (Costa, 2014; Bahari-Kashani, 2013; Hollevoet, 2011; Karantana, 2013; Rozental, 2009) were extracted for this literature summary. The 5 RCTs included a total of 790 patients, 393 patients underwent K-wires and in 397 patients volar locking plates were used. Four RCTs had a follow-up of 1 year and 1 RCT had a mean follow-up of 19 months. Risk of bias was assessed with the Cochrane Risk of Bias Tool. There was a lack of concealment in one RCT (Hollevoet, 2011). No trials were double blind because of the nature of the intervention. Three studies (Hollevoet, 2011; Karantana, 2013; Rozental, 2009) did not perform intention-to-treat analyses. In was unclear whether Hollevoet (2011) used intention-to-treat analyses. The use of intention-to-treat analyses was not assessed with the Cochrane Risk of Bias Tool in the systematic review.
Results
PROMs
DASH
The 5 RCTs included in the review of Youlden (2019) reported outcomes on the Disabilities of the Arm, Shoulder, and Hand (DASH scores) questionnaire. The DASH questionnaire comprises 30 items and focuses on two components, disability and symptoms of the upper extremity. It is scored from zero (good status) to 100 (poor status).
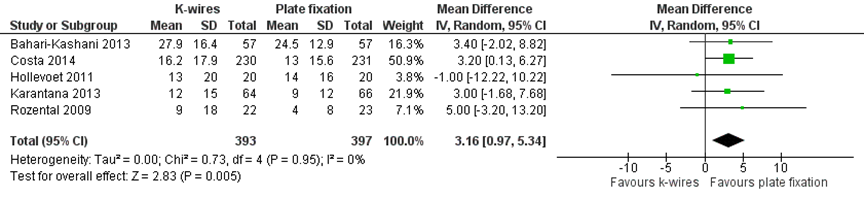
One RCT (Karantana, 2013) reported the Quick DASH scores and the other RCTs reported the DASH scores. Given that normative data for these scoring instruments are sufficiently similar. The MDs of these scores were pooled across the relevant studies. The pooled mean difference in DASH score at final follow-up was 3.16 (95% CI 0.97 to 5.34) favoring plate fixation (figure 1). This difference is not clinically relevant.
Goehre (2014) reported the median DASH score after one year of follow up. The median DASH score was 3 in both groups, the IQR was 0 to 4.8 in the K-wire versus 0 to 10.6 in the plate fixation group.
Figure 1 (Quick) DASH scores of K-wires versus plate fixation for the treatment of displaced distal radial fractures (source: Youlden, 2019)
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
PRWE
The PRWE was reported in two studies (Costa, 2014; Goehre, 2014). It is a 15-item questionnaire that focuses on measurement of wrist pain and disability in activities of daily living. It is scored from zero (minimum pain and disability) to 100 (maximum pain and disability).
Costa (2014) reported a mean PRWE score of 15.3 (SD 15.8) in the K-wire group versus 13.9 (SD 17.1) in the plate fixation group at 1 year follow-up. The mean difference in PRWE score at final follow-up was 1.40 (95% CI -1.61 to 4.41) favoring plate fixation. At 5-year follow-up the PRWE score was 8.3 (SD 12.5) in de K-wire group versus 11.3 (SD 15.6) in the plate fixation group. The mean difference in PRWE score at final follow-up was -3.00 (95% CI -5.58 to -0.42) favoring K-wires. The differences were not clinically relevant. Noteworthy is that all plate patients had plaster treatment postoperatively.
Goehre (2014) reported the median PRWE-score after one year of follow up. The median PRWE-score was 3.5 in both groups, the IQR was 0 to 12.5 in the K-wire versus 0 to 8.2 in the plate fixation group.
Level of evidence of the literature
The level of evidence regarding the outcome measure DASH- and PRWE-score was downgraded by two levels from high to low, because of study limitations such as lack of blinding of patients and outcome assessors and intention-to-treat analysis (risk of bias) and small number of included patients with wide confidence intervals (imprecision). Moreover, most studies included patients with Type A and C DRFs which makes it difficult to differentiate per fracture.
Range of motion
Goehre (2014) and four RCTs included in the review of Youlden (2019) reported the range of motion. However, the outcome was expressed in different ways.
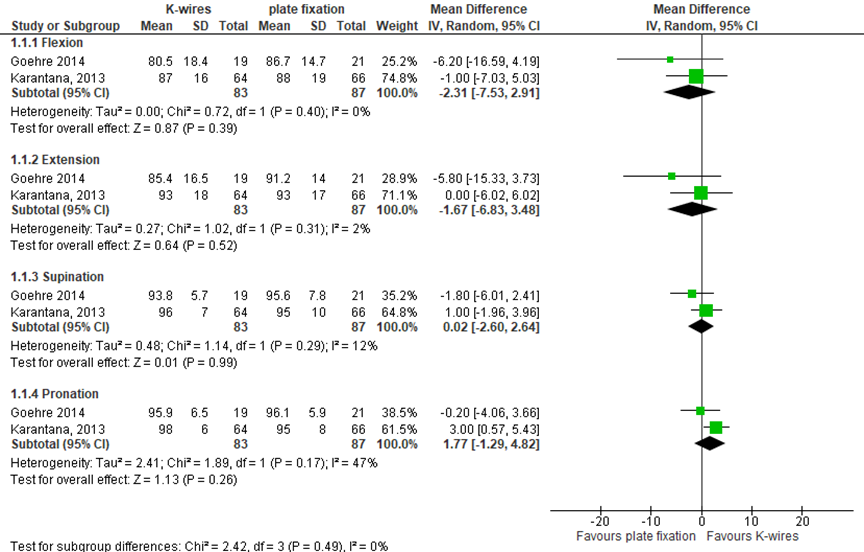
Goehre (2014) and Karantana (2013) reported the range of motion at respectively 12 and 19 months. This was expressed as a percentage of the uninjured contralateral side. The pooled differences between the groups are shown in figure 2). These differences are not clinically relevant. Goehre (2014) also reported the mean ulnar- and radial deviation. The ulnar deviation was 86.7 (SD 17.5) in the K-wires group and 88.0 (SD 15.2) in the plate fixation group. This difference is not clinically relevant. The radial deviation was 86.2 (SD 21.1) in the K-wires group and 81.5 (24.2) in the plate fixation group. This difference is not clinically relevant.
Figure 2 Range of motion (% of the uninjured contralateral side) of the use K-wire versus plate fixation for the treatment of distal radial fractures
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
In addition, Bahari-Kashani (2013) reported range of motion at 12 months (table 1). The study did not report how the range of motion was expressed. Hollevoet (2011) reported range of motion at 19 months. This was expressed as a percentage of the uninjured contralateral side (see table 2). These differences are not clinically relevant. Rozental (2009) reported range of motion at 12 months. This was expressed as degrees (see table 3). Because of this heterogeneity the results could not be pooled.
Table 1 Range of motion. Source: Bahari-Kashani (2013)
|
Range of motion |
K-wire, mean (SD) |
Plate fixation, mean (SD) |
Mean difference (95% CI) |
|
Flexion - extension |
87.1 (6.1) |
87.8 (8.5) |
-0.7 (-3.42 to 2.02) |
|
Supination - pronation |
76.5 (7.7) |
91.8 (7.1) |
-15.3 (-18.02 to -12.58) |
Table 2 Range of motion (% of the uninjured contralateral side). Source: Hollevoet (2011)
|
Range of motion (%) |
K-wire, mean (SD) |
Plate fixation, mean (SD) |
Mean difference (95% CI) |
|
Flexion – extension range |
86% (15) |
90% (8) |
-4 (-11.45 to 3.45) |
|
Pronation – supination range |
98% (6) |
97% (8) |
1 (-3.38 to 5.38) |
|
Radioulnar deviation range |
89% (18) |
90% (17) |
-1 (-11.85 to 9.85) |
Table 3 Range of motion (degrees). Source: Rozental (2009)
|
Range of motion (◦) |
K-wire, mean (SD) |
Plate fixation, mean (SD) |
Mean difference (95% CI) |
|
Flexion |
72 (15) |
68 (14) |
4 (-4.49 to 12.49) |
|
Extension |
66 (20) |
64 (17) |
2 (-8.87 to 12.87) |
|
Supination |
87 (9) |
88 (5) |
-1 (-5.28 to 3.28) |
|
Pronation |
88 (4) |
88 (4) |
0 (-2.34 to 2.34) |
|
Ulnar deviation |
32 (7) |
40 (11) |
-8 (-13.36 to -2.64) |
|
Radial deviation |
22 (10) |
28 (15) |
-6 (-13.42 to 1.42) |
Level of evidence of the literature
The level of evidence regarding the outcome measure range of motion was downgraded by three levels from high to very low because of study limitations such as lack of blinding of patients and outcome assessors and intention-to-treat analysis (risk of bias), heterogeneity between studies (inconsistency) and small number of included patients with wide confidence intervals (imprecision).
Radiographic parameters
The RCT of Goehre (2014) and four studies included in the review of Youlden (2019) reported radiographic parameters at 12 months and Hollevoet (2011) (RCT included in Youlden (2019)) at 5 weeks postoperative.
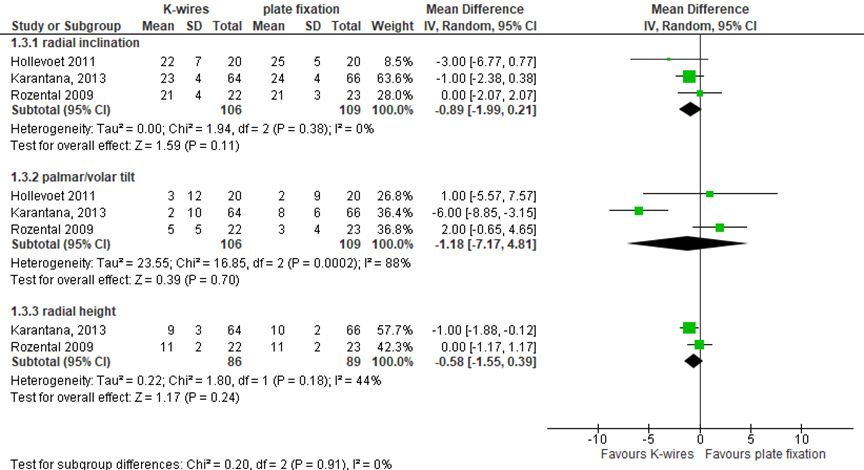
Hollevoet (2011), Karantana (2013) and Rozental (2009) reported the mean radial inclination, palmar/volar tilt and radial height. This was expressed in degrees or millimeters. The pooled differences between the groups are shown in figure 3. The mean difference of radial inclination was -0.89 (95% CI -1.99 to 0.21). The mean difference of palmar/volar tilt was -1.18 (95% CI -7.17 to 4.81). The mean difference for radial hight was -0.58 (95% CI -1.55 to 0.39). Hollevoet (2011) also reported the mean increase in ulnar variance (mm). The ulnar variance was 2 (SD 2) in the K-wires group and 1 (SD 2) in the plate fixation group. The differences were in favor of the K-wires. These are not clinically relevant differences.
Figure 3 Radiographic parameters (radial inclination, palmar/volar tilt and radial height) in degrees or mm of the K-wires versus plate fixation for the treatment of distal radial fractures
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
In addition, Bahari-Kashani (2013) reported inclination, tilt and ulnar variance at 12 months. The authors defined volar tilt and radial inclination as acceptable cases or not. However, the definition of acceptable wasn’t reported. Ulnar variance was divided in < 5mm or > 5mm. The cut-off values used by this study, are not in line with the cut-off values the working group would use and were therefore not included in this literature analysis.
Level of evidence of the literature
The level of evidence regarding the outcome measure radiographic parameters was downgraded by three levels from high to very low because of study limitations such as lack of blinding of patients and outcome assessors and intention-to-treat analysis (risk of bias), heterogeneity between studies (inconsistency) and small number of included patients with wide confidence intervals (imprecision).
Pain
None of the included studies comparing K-wires with plate fixation reported on pain.
Level of evidence of the literature
As none of the included studies reported data on the quality of life, it was not possible to assess the level of evidence.
Complications
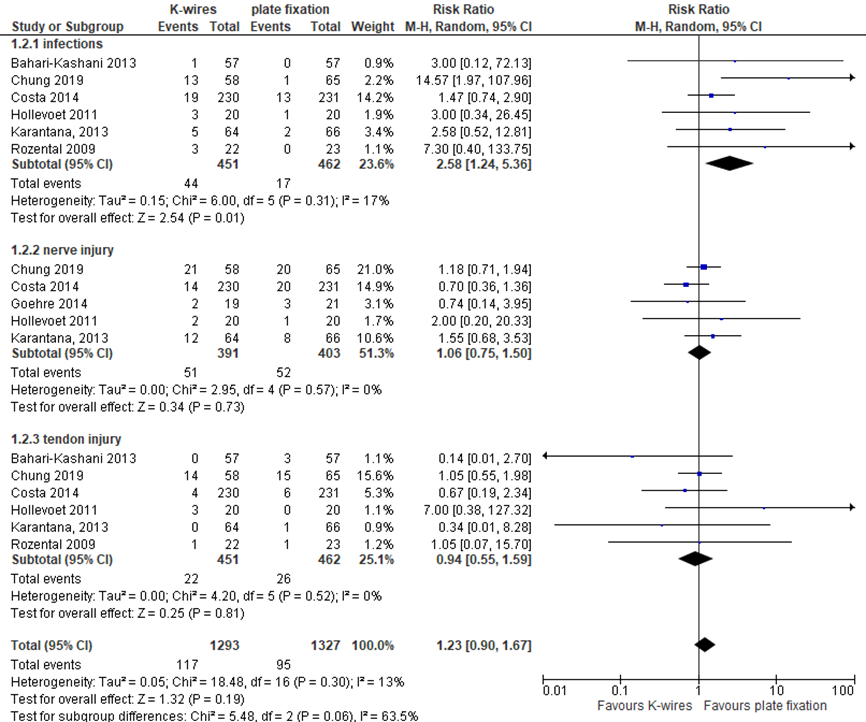
Chung (2019), Goehre (2014) and the 5 RCTs included in the review of Youlden (2019), reported complications after 12 months of follow up, except for one RCT included in Youlden (2019), Hollevoet (2011) reported complications after 19 months follow up. In 117 (9.0%) patients, complications were reported in the K-wires group versus 95 (7.2%) complications in patients with plate fixation (RR 1.23; 95% CI 0.90 to 1.67) favoring plate fixation (figure 4). This is not a clinically relevant difference. Complications were grouped in infections, nerve- and tendon injuries. See the evidence table for the exact definitions of these complications.
Infections
In 44 (9.80%) patients, infections were reported in the K-wires group versus 17 (3.7%) in patients with plate fixation (RR 2.58; 95% CI 1.24 to 5.36) favoring plate fixation (figure 4). This is a clinically relevant difference.
Nerve injury
In 51 (13.0%) patients, nerve injuries were reported in the K-wires group versus 52 (12.9%) in patients with a plate fixation (RR 1.06; 95% CI 0.75 to 1.50) (figure 4). This is not a clinically relevant difference. The included studies defined nerve injuries as neurological injury, carpal tunnel syndrome, transient nerve palsy, median nerve compression, radial nerve compression/neuropathy or ulnar nerve compression neuropathy.
Tendon injury
In 22 (4.9%) patients, tendon injuries were reported in the K-wires group versus 26 (5.6%) in patients with a plate fixation (RR 0.94; 95% CI 0.55 to 1.59) (figure 4). This is not a clinically relevant difference. The included studies defined tendon injuries as tendon injury,
trigger finger, extensor pollicis longus rupture, De Quervain tenosynovitis, extensor carpi ulnaris tendinitis, extensor tendon irritation, Dupuytren contracture, tendon adhesion/scarring, tendon rupture/tear, tendinitis/tenosynovitis and trigger finger.
Figure 4 Complication of the K-wires versus plate fixation for the treatment of distal radial fractures
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Level of evidence of the literature
The level of evidence regarding the outcome measure complications (infections) was downgraded by two levels from high to low, one level because of study limitations such as lack of blinding of patients and outcome assessors and intention-to-treat analysis (risk of bias) and one level because of small number of included patients and events and wide confidence intervals (imprecision).
The level of evidence regarding the outcome measure complications (nerve injury and tendon injury) was downgraded by three levels from high to very low, one level because of study limitations such as lack of blinding of patients and outcome assessors and intention-to-treat analysis (risk of bias) and two levels because of small number of included patients and events and wide confidence intervals consisting of both no effect as well as clinical relevant effects in favour of both groups (imprecision).
Reinterventions
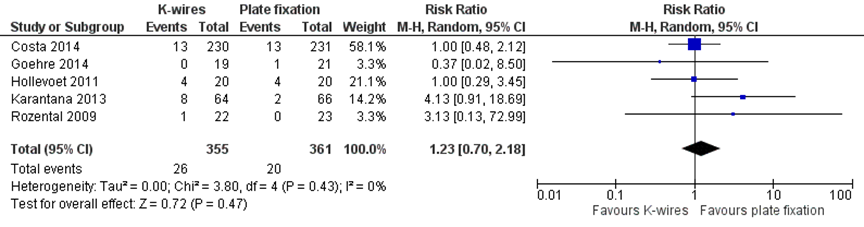
The RCT of Goehre (2014) and four studies included in the review of Youlden (2019) reported the number of reinterventions after 12 months and Hollevoet (2011) (study included in Youlden (2019)) after 19 months. This was defined as hardware removal or revision surgery. 26 patients (7.3%) in the K-wire group versus 20 patients (5.5%) in the plate fixation group had a reintervention (RR 1.23; 95% CI 0.70 to 2.18, see figure 5). This is not a clinically relevant difference.
In addition, Chung (2019) reported that 5 K-wire patients were treated with pin removal and/or topical antibiotics due to pin tract infections, but did not differentiate how many of these patients had actual pin removal or antibiotics. One patient in the plate fixation group experienced an extensor pollicis longus tendon rupture and had surgical repair. Three additional plate fixation (cross-overs) participants had hardware removed due to tendon irritation.
Figure 5 Reintervention of the K-wires versus plate fixation for the treatment of distal radial fractures
Z: p-value of overall effect; df: degrees of freedom; I2: statistical heterogeneity; CI: confidence interval
Level of evidence of the literature
The level of evidence regarding the outcome measure reinterventions was downgraded by three levels from high to very low, one level because of study limitations such as lack of blinding of patients and outcome assessors and intention-to-treat analysis (risk of bias) and two levels because of small number of included patients and events and wide confidence intervals, consisting of both no effect as well as clinically relevant effects in favour of both groups (imprecision).
A systematic review of the literature was performed to answer the following question:
What is the (non)-effectiveness of closed reduction and Kirschner wire fixation/closed reduction and percutaneous pinning (CRPP) versus open reduction and plate fixation for displaced distal radius fractures (DRFs) in adult patients?
P: patients with an intra- or extra-articular distal radius fracture;
I: closed reduction and Kirschner wire fixation;
C: open reduction and plate fixation;
O: PROMS, range of motion, radiographic parameters, pain, complications such as infections, tendon- and nerve injuries and reinterventions.
Relevant outcome measures
The guideline development group considered validated PROMs as critical outcome measures for decision making; and ROM, radiographic parameters, pain, complications and reinterventions as important outcome measures for future decision making.
The working group defined PROMs (Patient Reported Outcome Measures) as follows: Michigan Hand Outcomes Questionnaire (MHOQ), Patient Rated Wrist Evaluation (PRWE) and (Quick) Disability of the Arm, Shoulder and Hand (DASH) score. Other outcome measures were not defined a priori, but used the definitions used in the studies.
Regarding the PROMS, the working group defined 10.8 points for the DASH and 11.5 for the PRWE-score (Walenkamp, 2015) as a clinically meaningful difference. Regarding the range of motion (ROM), the threshold for clinical relevance was set at 20 degrees for extension and flexion, 7 degrees for ulnar deviation, 5 degrees for radial deviation and 20 degrees for supination and pronation. For VAS-scales, the threshold for clinically meaningful differences was set at 20mm or 2 points. For dichotomous outcomes a number needed to treat (NNT) was defined: secondary treatment: NNT ≤ 40; complications including infection: NNT ≤ 20, tendon pathology: NNT ≤ 40 and nerve pathology, NNT ≤ 20.
Search and select (Methods)
Only randomized trials (RCTs) or systematic reviews (SRs) evaluating closed reduction and Kirschner wire fixation and open reduction and plate fixation of displaced distal radius fractures in adults were included. The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms from 1990 until December 18, 2019. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 449 hits. Studies were selected based on the following criteria: RCTs with at least 1 year follow-up, comparing closed reduction and Kirschner wire fixation with open reduction and plate fixation in the treatment of patients with an intra- and extra-articular radius fracture. Studies were initially selected based on title and abstract screening. Full texts of 30 papers were evaluated for inclusion. After reading the full text, 26 articles were excluded (see the table with reasons for exclusion under the tab Methods) and 4 articles were included.
Results
One systematic review with meta-analysis (Youlden, 2019) including 5 RCTs, 1 article (Costa, 2019) reporting the five-year follow-up of an RCT (Costa, 2014) included in the review of Youlden (2019) and 2 additional RCTs (Chung, 2019; Goehre, 2014) were included in the analysis. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Chung KC, Malay S, Shauver MJ, Kim HM; WRIST Group. Assessment of Distal Radius Fracture Complications Among Adults 60 Years or Older: A Secondary Analysis of the WRIST Randomized Clinical Trial. JAMA Netw Open. 2019;2(1):e187053. Published 2019 Jan 4. doi:10.1001/jamanetworkopen.2018.7053.
- Costa ML, Achten J, Rangan A, Lamb SE, Parsons NR. Percutaneous fixation with Kirschner wires versus volar locking-plate fixation in adults with dorsally displaced fracture of distal radius: five-year follow-up of a randomized controlled trial. Bone Joint J. 2019;101-B(8):978-983. doi:10.1302/0301-620X.101B8.BJJ-2018-1285.R1.
- Goehre F, Otto W, Schwan S, Mendel T, Vergroesen PP, Lindemann-Sperfeld L. Comparison of palmar fixed-angle plate fixation with K-wire fixation of distal radius fractures (AO A2, A3, C1) in elderly patients. J Hand Surg Eur Vol. 2014;39(3):249-257. doi:10.1177/1753193413489057.
- Rozental, T. D., Blazar, P. E., Franko, O. I., Chacko, A. T., Earp, B. E., & Day, C. S. (2009). Functional outcomes for unstable distal radial fractures treated with open reduction and internal fixation or closed reduction and percutaneous fixation. A prospective randomized trial. The Journal of bone and joint surgery. American volume, 91(8), 1837–1846. https://doi-org.saz.idm.oclc.org/10.2106/JBJS.H.01478.
- Tubeuf S, Yu G, Achten J, et al. Cost effectiveness of treatment with percutaneous Kirschner wires versus volar locking plate for adult patients with a dorsally displaced fracture of the distal radius: analysis from the DRAFFT trial. Bone Joint J. 2015;97-B(8):1082-1089. doi:10.1302/0301-620X.97B8.35234.
- Walenkamp MM, de Muinck Keizer RJ, Goslings JC, Vos LM, Rosenwasser MP, Schep NW. The Minimum Clinically Important Difference of the Patient-rated Wrist Evaluation Score for Patients With Distal Radius Fractures. Clin Orthop Relat Res. 2015 Oct;473(10):3235-41. doi: 10.1007/s11999-015-4376-9. Epub 2015 Jun 4. Erratum in: Clin Orthop Relat Res. 2015 Sep;473(9):3063. PubMed PMID: 26040969; PubMed Central PMCID: PMC4562929.
- Youlden DJ, Sundaraj K, Smithers C. Volar locking plating versus percutaneous Kirschner wires for distal radius fractures in an adult population: a meta-analysis. ANZ J Surg. 2019;89(7-8):821-826. doi:10.1111/ans.14903.
Evidence table for systematic review of RCTs and observational studies (intervention studies)
Evidence table for intervention studies (randomized controlled trials and non-randomized observational studies (cohort studies, case-control studies, case series))1
Risk of bias table for intervention studies (randomized controlled trials)
|
Study reference
(first author, publication year) |
Describe method of randomisation |
Bias due to inadequate concealment of allocation?
(unlikely/likely/unclear) |
Bias due to inadequate blinding of participants to treatment allocation?
(unlikely/likely/unclear) |
Bias due to inadequate blinding of care providers to treatment allocation?
(unlikely/likely/unclear) |
Bias due to inadequate blinding of outcome assessors to treatment allocation?
(unlikely/likely/unclear) |
Bias due to selective outcome reporting on basis of the results?
(unlikely/likely/unclear) |
Bias due to loss to follow-up?
(unlikely/likely/unclear) |
Bias due to violation of intention to treat analysis?
(unlikely/likely/unclear) |
|
Goehre 2014 |
A modified randomization method was used. With a random number generator, two permuted single blocks (K-wire fixation and plate fixation) of variable length were created. The total length of both blocks was set to 40 events. Each of the 40 events was placed in a sealed non-translucent envelope and stored in a box. After recruitment of a patient to the study, an envelope was taken from storage by a resident in order to assign a treatment method to each patient. |
Unlikely |
Likely |
Likely |
Likely |
Unlikely |
Unlikely |
Unlikely |
|
Chung, 2019 |
Prior to commencing enrollment, the study statistician devised a randomization list stratified by study site using random block sizes of 3, 6, and 9. Randomization was executed by study coordinators through a secure website, Treatment Assignment Tool–University of Michigan. |
Unlikely |
Likely |
Likely |
Likely |
Likely |
Unlikely |
Unlikely |
|
Costa, 2019 |
See quality assessment Youlden (2019) |
See quality assessment Youlden (2019) |
See quality assessment Youlden (2019) |
See quality assessment Youlden (2019) |
See quality assessment Youlden (2019) |
Unlikely |
Likely |
Unlikely |
Table of quality assessment for systematic reviews of RCTs and observational studies
Based on AMSTAR checklist (Shea, 2007; BMC Methodol 7: 10; doi:10.1186/1471-2288-7-10) and PRISMA checklist (Moher, 2009; PLoS Med 6: e1000097; doi:10.1371/journal.pmed1000097)
|
Study
First author, year |
Appropriate and clearly focused question?
Yes/no/unclear |
Comprehensive and systematic literature search?
Yes/no/unclear |
Description of included and excluded studies?
Yes/no/unclear |
Description of relevant characteristics of included studies?
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?
Yes/no/unclear/notapplicable |
Assessment of scientific quality of included studies?
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?
Yes/no/unclear |
Potential risk of publication bias taken into account?
Yes/no/unclear |
Potential conflicts of interest reported?
Yes/no/unclear |
|
Youlden, 2019 |
Yes |
Yes |
No |
Yes |
Not applicable |
Yes |
Yes |
No |
No |
Table of excluded studies
|
Author and year |
Reason for exclusion |
|
Vannabouathong, 2019 |
Netwerk meta-analyse met bredere PICO dan deze uitgangsvraag. Review Youlden voldoet en is als uitgangspunt meegenomen. |
|
Peng, 2018 |
Recentere review Youlden is als uitgangspunt genomen |
|
Anderson, 2017 |
Recentere review Youlden is als uitgangspunt genomen |
|
Wang, 2017 |
Recentere review Youlden is als uitgangspunt genomen |
|
Xu, 2016 |
Recentere review Youlden is als uitgangspunt genomen |
|
Shen, 2016 |
Recentere review Youlden is als uitgangspunt genomen |
|
Shao, 2016 |
Recentere review Youlden is als uitgangspunt genomen |
|
Zao, 2015 |
Recentere review Youlden is als uitgangspunt genomen |
|
Zong, 2015 |
Recentere review Youlden is als uitgangspunt genomen |
|
Franceschi, 2015 |
Recentere review Youlden is als uitgangspunt genomen |
|
Chaudhry, 2015 |
Recentere review Youlden is als uitgangspunt genomen |
|
Kvernmo, 2013 |
Recentere review Youlden is als uitgangspunt genomen |
|
Costa, 2019 |
Meegenomen in review van Youlden |
|
Zyluk, Skala, Szlosser, 2018 |
Geen RCT |
|
Zyluk, Janowski, Szlosser, Puchalski, 2018 |
Geen RCT |
|
Costa, 2016 |
Geen RCT |
|
Costa, 2015 |
HTA rapport van de trial |
|
Costa, 2014 |
Meegenomen in review van Youlden |
|
Karantana, 2013 |
Meegenomen in review van Youlden |
|
Bahari-Kashan, 2013 |
Meegenomen in review van Youlden |
|
Costa, 2011 |
Studieprotocol |
|
Hollevoet, 2011 |
Meegenomen in review van Youlden |
|
Rozental, 2009 |
Meegenomen in review van Youlden |
|
Leung, 2008 |
Voldoet niet aan PICO: External fixator+percutaneous pin versus plate fixation |
|
Kreder, 2005 |
Voldoet niet aan PICO: Indirect reduction and percutaneous fixation versus open reduction and internal fixation |
|
Grewal, 2005 |
Voldoet niet aan PICO: open reduction and internal fixation and dorsal plating or external fixation and K-wires and mini-open reduction |
Beoordelingsdatum en geldigheid
Publicatiedatum : 18-08-2021
Beoordeeld op geldigheid : 02-08-2021
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten en werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS).
De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
De richtlijn is ontwikkeld in samenwerking met:
- Nederlandse Orthopaedische Vereniging
- Nederlandse Vereniging voor Plastische Chirurgie
- Nederlandse Vereniging voor Radiologie
- Nederlandse Vereniging van Spoedeisende Hulp Artsen
- Nederlandse Vereniging van Revalidatieartsen
- Koninklijk Nederlands Genootschap voor Fysiotherapie
- Nederlandse Vereniging voor Handtherapie
- Osteoporose Vereniging
Doel en doelgroep
Doel
Deze multidisciplinaire richtlijn bevat aanbevelingen ter ondersteuning van de dagelijkse praktijk voor hulpverleners die zich bezighouden met diagnostiek en behandeling van patiënten met een distale radius fractuur. De aanbevelingen zijn opgesteld op basis van de huidige wetenschappelijke inzichten. De knelpunten die behandelaars ervaren in de dagelijkse zorgpraktijk bij patiënten met een distale radius fractuur dienen als uitgangspunt bij de ontwikkeling van deze richtlijn.
Ter bevordering van de implementatie wordt geadviseerd om deze richtlijn aanknopingspunt te laten zijn voor lokale behandelprotocollen voor patiënten met een distale radius fractuur. Daarnaast kan de richtlijn gebruikt worden bij het geven van voorlichting aan patiënten met een distale radius fractuur.
Doelgroep
Deze richtlijn is bedoeld voor alle zorgverleners die betrokken zijn bij de zorg voor volwassen patiënten met een intra- of extra-articulaire distale radiusfractuur.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2019 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen die betrokken zijn bij de zorg voor patiënten met een distale radius fractuur.
Werkgroep
- Dr. P.F.W. Hannemann, chirurg, werkzaam in het Maastricht UMC te Maastricht, (voorzitter), NVvH
- Dr. N.W.L. Schep, chirurg, werkzaam in het Maasstad Ziekenhuis te Rotterdam, NVvH
- Dr. D.I. Vos, chirurg, werkzaam in het Amphia ziekenhuis te Breda, NVvH
- Dr. R.L.M. Deijkers, orthopaedisch chirurg, werkzaam in het HagaZiekenhuis te Den Haag, NOV
- Dr. J.W. Colaris, orthopaedisch chirurg, werkzaam in het Erasmus UMC te Rotterdam, NOV
- Drs. J. van Loon, plastisch chirurg, werkzaam bij Blooming plastisch chirurgie te Haarlem, NVPC
- Drs. S. Bollen, radioloog, werkzaam in Het Groene Hart Ziekenhuis te Gouda,NVvR
- Drs. G.J.P. Smits, SEH-arts, werkzaam in het Catharina Ziekenhuis te Eindhoven, NVSHA
- Drs. K.S. van Wonderen, AIOS SEH, werkzaam in het St. Antonius ziekenhuis te Nieuwegein, NVSHA
- Dr. G. Zemack, revalidatiearts, werkzaam bij Libra revalidatie audiologie te Eindhoven, NVR
- Dr. F.J.B. Lötters, fysiotherapeut en docent fysiotherapie, werkzaam bij het Hand & Pols Centrum te Dordrecht en Hogeschool Leiden, KNGF, NVvHandtherapie
- H.J.G. van den Broek, voorzitter Osteoporose Vereniging te Haarlem.
Met ondersteuning van
- Drs. T. Geltink, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
- Dr. S.N. Hofstede, senior adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Hannemann |
Traumachirurg/hand- en polschirurg (FESSH) Maastricht Universitair Medisch Centrum Maastricht |
Plaatsvervangend opleider heelkunde regio VIII (onbetaald); Course director CASH 3 cursus hand- en polschirurgie (onbetaald); Faculty lid AO (betaald); Faculty lid IBRA (betaald); Course director IBRA hand and wrist courses (betaald); Fellowship director IBRA upper limb training center MUMC Maastricht (betaald); Ontwikkeling course modules upper extremity IBRA (betaald); Faculty lid Esser Master class (onbetaald); ATLS instructor (betaald) Opleider HAIO’s (onbetaald) |
Begunstigde ZonMW subsidie aangaande onderzoek naar correctie osteotomie van de distale radius
Begunstigde Inscite subsidie (extern gefinancierd) voor onderzoek naar artrose van het polsgewricht |
Geen actie. De onderwerpen van de gesubsidieerde studies vallen buiten de afbakening van de richtlijn. |
|
Bollen |
Radioloog Groene Hart Ziekenhuis Gouda |
Geen |
Geen |
Geen actie. |
|
Deijkers |
Orthopedisch Chirurg HagaZiekenhuis Den Haag. |
Voorzitter Hand en Pols Werkgroep van de NOV (onbetaald); Organisator A&A Hand and Wrist Course Utrecht (onbetaald); Instructeur Dutch Wrist Arthroscopy Course (DWAC) (onbetaald); Voorzitter Commissie Certificering Subspecialisatie Handchirurgie van de Nederlandse Vereniging voor Handchirurgie (onbetaald) |
Geen |
Geen actie. |
|
van de Broek |
Voorzitter Osteoporose Vereniging (onbezoldigd)
|
Bestuurslid Energiek Heusden (energie coöperatie,(onbetaald); DGA eigen holding BV (pensioenrechten, betaald) |
Geen |
Geen actie. |
|
Van Loon |
Plastisch chirurg RKZ Beverwijk |
CFO Beverwijk Skin and Scar Company, Haarlem (betaald) |
Geen |
Geen actie. |
|
Colaris |
Orthopedisch chirurg - traumatoloog /hand- en polschirurg (FESSH) |
NOV bestuurslid (onkostenvergoeding); Bestuurslid Orthopedische Traumatologie Portefeuillehouder CCOC (onbetaald); Bestuurslid werkgroep hand-pols NOV (onbetaald); Bestuurslid werkgroep AI NOV (onbetaald); Bestuurslid Zuid West Overleg Traumatologie (onbetaald); Bestuurslid en co-founder BIG hand event (onbetaald); Faculty AO (betaald); Faculty OTC (betaald); Faculty Dutch wrist course (onbetaald); Faculty Esser Master Class (onbetaald) |
ZonMw subsidie voor uitwerking CAST-studie waarbij gereponeerde distale radiusfracturen ofwel in circulair gips ofwel in een gipsspalk worden geïmmobiliseerd. |
Geen actie. |
|
Zemack |
Revalidatiearts, Libra Revalidatie & Audiologie, Eindhoven, Tilburg en Weert. |
Voorzitter van de geaccrediteerde Werkgroep Trauma Revalidatie (WTR) van de VRA (Nederlandse Vereniging van Revalidatieartsen) (onbetaald) |
Geen |
Geen actie. |
|
Smits |
SEH-arts KNMG, Catharinaziekenhuis Eindhoven. |
PhD candidate, TU/e (onbetaald); Docent spoedzorg, Schola Medica Utrecht (betaald) |
Geen |
Geen actie. |
|
Lötters |
Hand-/fysiotherapeut, Bewegingswetenschapper bij Hand en Pols Revalidatie Nederland, locaties Den Haag en Dordrecht |
Docent bij de opleiding fysiotherapie bij de Hogeschool Leiden. |
Geen |
Geen actie. |
|
Schep |
Traumachirurg/hand- en polschirurg (FESSH), Maasstad Ziekenhuis Rotterdam, tevens werkzaam in het Spijkenisse Medisch Centrum |
Bestuurslid Ned. Ver. Handchirurgie (onbetaald); Bestuurslid Big Hand Event (onbetaald); Instructeur Dutch Wrist Ascopie course (onbetaald); Consultant Synthes, Arthrex: betrokken bij cursussen (betaald); Chairman diverse AO cursussen (onkosten vergoeding); Instructeur IBRA course (onkosten vergoeding); Instructeur CASH cursus handfracturen (onkosten vergoeding); Editor boek Leidraad chirurgie co- assistent revenuen; Consultant KLS Martin (betaald) |
Echtgenote heeft een medisch congres bureau. Geen relatie met deze richtlijn; Begunstigde diverse Zonmw subsidies voor onderzoek naar handfracturen, geen relatie met deze richtlijn; Meerdere publicaties aangaande de distale radius die ook in deze richtlijn aan bod komen.
|
Geen actie. |
|
Vos |
Traumachirurg Amphia Ziekenhuis Breda |
Lid klachten-commissie, Jeroen Bosch ziekenhuis den Bosch, (betaald); Lid kwaliteitsvisitatie commissie NVvH (onkostenvergoeding); ATLS instructor (betaald); AO faculty (betaald); consultant Operace Johnson & Johnson (betaald) |
Geen |
Geen trekker of meelezer bij uitgangsvragen over platen. |
|
Van Wonderen |
AIOS SEH bij st. Antoniusziekenhuis te Nieuwegein/Utrecht |
geen |
Geen |
Geen actie. |
Inbreng patiëntenperspectief
Voor de totstandkoming van deze richtlijn is aandacht besteed aan het patiëntenperspectief door uitnodigen van Patiëntenfederatie Nederland en patiëntenvereniging Osteoporose Vereniging voor de invitational conference en door middel van het aanstellen van een afgevaardigde van patiëntenvereniging Osteoporose Vereniging als lid van de werkgroep. Aanvullend zijn er door de Patiëntenfederatie Nederland patiëntervaringen verzameld door een vragenlijst uit te sturen onder het Zorgpanel van de Patiëntenfederatie. Het verslag hiervan (zie de bijlagen) is besproken in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan de Osteoporose Vereniging en de Patiëntenfederatie en de daarbij aangeleverde commentaren zijn bekeken en verwerkt.
Methode ontwikkeling
Evidence based
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met een distale radius fractuur. De werkgroep beoordeelde de aanbeveling(en) uit de eerdere richtlijnmodules (Nederlandse Vereniging voor Heelkunde, 2010) op noodzaak tot revisie. Tevens zijn er knelpunten aangedragen door de Beroepsvereniging Verzorgenden Verpleegkundigen (V&VN), de Nederlandse Vereniging van Revalidatieartsen (VRA), het Koninklijk Nederlands Genootschap voor Fysiotherapie (KNGF), de Nederlandse Vereniging voor Handtherapie (NVHT) en de Nederlandse Vereniging voor Heelkunde (NVvH) via een schriftelijke invitational conference. Daarnaast is er een enquête uitgezet onder het Zorgpanel van de Patiëntenfederatie. Het rapport hiervan is opgenomen in de bijlagen.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvragen behorende bij de uitgangsvragen inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt gerelateerd) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur en de beoordeling van de risk-of-bias van de individuele studies is te vinden onder ‘Zoeken en selecteren’ onder ‘Onderbouwing’. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello, 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE-methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE-gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module 'Organisatie van zorg'.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. https://richtlijnendatabase.nl/over_deze_site/richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
|
Database |
Zoektermen |
Totaal |
|
Medline (OVID) 2000-dec. 2019 Engels |
1 Radius Fractures/ (8942) 2 (((distal adj3 (radius or radial)) or wrist or colles or smith*) adj3 fracture*).ti,ab,kf. (6996) 3 1 or 2 (11988) 4 orthopedic fixation devices/ or internal fixators/ or bone plates/ or bone screws/ or fracture fixation/ (58849) 5 (osteosynthesis or plate* or "internal fixat*" or screw*).ti,ab,kf. (470504) 6 4 or 5 (497324) 7 3 and 6 (4629) 8 limit 7 to (english language and yr="2000 -Current") (2620) 18 (meta-analysis/ or meta-analysis as topic/ or (metaanaly* or metanaly* or meta-analy*).ti,ab,kf. or ((systematic* or scoping or evidence based) adj3 (review* or overview*)).ti,kf. or ((evidence or research) adj3 synthesis).ti,kf. or systematic review.pt. or (prisma or (("structured literature" or comprehensive or "quantitative literature" or evidence-based) adj2 (search or review)) or "systematic search" or ((systemic or systematized) adj3 review) or "systematic research synthesis" or (review* adj3 independent*)).ti,ab,kf. or (((quantitative or rapid or short or critical* or structured or comparative or comparitive or evidence or comprehensive) adj3 (review* or overview*)).ti. and search.ab.) or "Review Literature as Topic"/ or cochrane.jw. or (cochrane or embase or medline or cinahl or cinhal or cancerlit).ab. or (("selection criteria" or "data extraction").ab. and "review"/)) not (Comment/ or Editorial/ or Letter/ or (animals/ not humans/)) (347797) 19 8 and 18 (104) > 99 uniek 20 (exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf.) not (animals/ not humans/) (1159716) 21 8 and 20 (334) 22 21 not 19 (260) > 255 uniek |
449 |
|
Embase (Elsevier) |
((('distal radius fracture'/exp/mj OR ((distal NEAR/3 (radius OR radial) NEAR/3 fracture*):ti,ab) OR (((wrist OR colles OR smith*) NEAR/3 fracture*):ti,ab)) NOT 'conference abstract':it AND (english)/lim AND ((embase)/lim OR (pubmed-not-medline)/lim) AND (2000-2020)/py) AND ('orthopedic fixation device'/mj OR 'internal fixator'/mj OR 'bone plate'/exp OR 'bone screw'/exp OR 'fracture fixation'/exp/mj OR 'fracture fixation'/exp OR 'compression osteosynthesis'/exp OR 'fracture immobilization'/exp OR 'osteosynthesis'/exp OR 'plate fixation'/exp OR 'volar plate fixation'/exp OR osteosynthesis:ti,ab OR plate*:ti,ab OR 'internal fixat*':ti,ab OR screw*:ti,ab)) AND (('meta analysis'/exp OR 'meta analysis (topic)'/exp OR 'systematic review (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review):ti) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab) NOT (('animal'/de OR 'animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT ('conference abstract':it OR 'conference review'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it)) (89) >34 uniek ('randomized controlled trial'/exp OR 'randomized controlled trial (topic)'/exp OR random*:ti,ab OR rct*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab)) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) NOT ('conference abstract':it OR 'conference review'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) (211) > 61 uniek |
|