Pre-eclampsie en zwangerschapshypertensie
Uitgangsvraag
Uitgangsvraag 1
Wat is het risico op een cardiovasculaire gebeurtenis voor vrouwen met pre-eclampsie of zwangerschapshypertensie in de voorgeschiedenis?
Uitgangsvraag 2
Wat zijn de risico’s op een ongunstig cardiovasculaire risicoprofiel voor vrouwen met pre-eclampsie of zwangerschapshypertensie in de voorgeschiedenis?
Aanbeveling
Gelet op het toegenomen relatieve risico op hart- en vaatziekten bij vrouwen met pre-eclampsie in de voorgeschiedenis is er reden om verdere diagnostiek en behandeling te adviseren met betrekking tot cardiovasculair risicomanagement.
Gelet op het beperkte toegenomen relatieve risico op hart- en vaatziekten bij vrouwen met zwangerschapshypertensie in de voorgeschiedenis is er geen reden om verdere diagnostiek en behandeling te adviseren met betrekking tot cardiovasculair risicomanagement.
Overwegingen
De studies laten consistent zien dat het hebben doorgemaakt van een pre-eclampsie gepaard gaat met een duidelijk verhoogde kans op een CV gebeurtenis in de toekomst; met een sterker verband voor IHZ dan voor beroerte. Vier onderzoeken geven aan dat de risico’s na een vroege pre-eclampsie veel hoger zijn dan na een late pre-eclampsie. De verbanden voor zwangerschapshypertensie zijn zwakker, maar wel aanwezig. Studies naar de kans op het ontwikkelen van een risicofactor zijn consistent positief voor hypertensie en diabetes mellitus type 2, terwijl er geen verband gevonden werd voor gestoorde lipidenstofwisseling.
Etniciteit
De gevonden studies rapporteerden niet systematisch resultaten voor etnische groepen. Daarom hebben wij dit niet gerapporteerd. Verder onderzoek moet uitwijzen of er verschillen zijn tussen etnische groepen.
Dyslipidemie
Op grond van de resultaten op het gebied van lipiden stoornissen kan geconcludeerd worden dat er geen verhoogde kans op dyslipidemie is. Wel moet opgemerkt worden dat in deze onderzoeken sprake was van grote verschillen in de definitie van dyslipidemie, er gemeten werd op verschillende tijdstippen na de zwangerschap en dat onderzoek overwegend plaats vond bij premenopauzale vrouwen bij wie het lipidenprofiel gunstig beïnvloed wordt door de endogene oestrogeenstatus. Er zou meer onderzoek gedaan moeten worden naar dyslipidemie bij postmenopauzale vrouwen met een pre-eclamapsie in de voorgeschiedenis.
Verstorende factoren
De bewijsvoering over de kans op CV gebeurtenissen of het ontwikkelen van een CV risicofactor is gebaseerd op niet experimenteel onderzoek. In dergelijk onderzoek kunnen verbanden worden over- of onderschat als gevolg van aanwezigheid van verstorende variabelen. In de regel wordt statistisch ‘gecorrigeerd’ voor deze verstorende variabelen om zo dicht mogelijk bij de waarheid te komen. De mate van correctie varieert tussen de studies. Dit is weergegeven in de evidencetabellen. Als onvoldoende rekening gehouden wordt met deze verstorende variabelen (gecorrigeerd) dan kan er een gerede kans zijn op residual confounding. Dit leidt er toe dat het RR in een bepaalde mate overschat of onderschat wordt.
Publicatiebias en heterogeniteit
Op basis van de visuele inspectie van de funnelplots leek er geen sprake te zijn van publicatiebias in de door ons onderzochte determinanten. Op het oog lieten de resultaten weinig klinische heterogeniteit zien tussen studies in de determinant, de patiënten, en de klinische uitkomsten. Wel waren er aanzienlijke verschillen tussen studies in follow-up duur en mate van correctie voor verstorende variabelen. Statistische heterogeniteit werd op twee manieren geëvalueerd. Ten eerste werd deze visueel beoordeeld aan de hand van het al dan niet ver uit elkaar liggen van de puntschatters en betrouwbaarheidsintervallen op de verschillende ‘forest plots’. In de meeste van de analyses lagen de schattingen van de verbanden redelijk dicht bij elkaar én was meestal sprake van voldoende overlap tussen de betrouwbaarheidsintervallen. Daarnaast werd de heterogeniteit beoordeeld met de I2-test. Een I2 van >60% is aanwezig in vrijwel alle analyses.
Een tweede manier om te kijken naar de kracht van de bewijsvoering is te schatten waar de echte waarde van het RR zou kunnen liggen in een nieuwe te starten onderzoek, het zogenaamde ‘prediction interval’. Deze berekening kan worden gemaakt op basis van de informatie afkomstig uit de gepoolde effect schattingen, waarbij de precisie van de gepoolde schatting én de variatie tussen studies (tau) worden meegenomen in de berekening. Dan komt naar voren dat de ‘echte’ waarde van het RR van pre-eclampsie op CV gebeurtenis in een nieuw onderzoek voor 95% ligt tussen 1.33 en 3.48. Voor IHZ ligt dat tussen 1.32 en 3.20 en voor CVA tussen 1.06 en de 2.20. Voor zwangerschapshypertensie zien we grenzen voor IHZ van 1.30 en 1.60 en voor CVA van 1.20 en 1.66. Dergelijke berekeningen geven aan dat de verbanden tussen pre-eclampsie en het krijgen van een CV gebeurtenis redelijk robuust zijn.
Hetzelfde kan berekend worden voor de andere verbanden, bijvoorbeeld voor het verband tussen pre-eclampsie en de kans op hypertensie. Het nieuwe relatieve risico ligt dan tussen 0.99 en 7.67. Voor pre-eclampsie en de kans op diabetes mellitus ligt de waarde tussen 0.87 en 5.60. Deze resultaten geven aan dat er veel meer variatie zit tussen de gepoolde studies. Zo ook voor zwangerschapshypertensie en de kans op hypertensie (grenzen van 1.60 tot 12.40).
Absolute kans op het ontwikkelen van een risicofactor of CV gebeurtenis
Het meest interessant voor de patiënt zijn de absolute kansen. Een terechte vraag is: ’hoeveel kans heb ik om hoge bloeddruk te ontwikkelen in de komende tien jaar’. We hebben geen onderzoeken kunnen vinden die daar een eenduidig antwoord op geven, alleen onderzoeken waarbij het verband als een RR is uitgedrukt. Daarbij moet een kanttekening worden geplaatst. Als er onderzoeken waren gevonden die een 10 jaar risico op een CV gebeurtenis hadden gerapporteerd dan kan men zich afvragen in hoeverre deze absolute kansen nog wel van toepassing zijn op de huidige vrouw die een PE heeft gehad. De absolute kansen op een myocard infarct zijn immers aanzienlijk gedaald in de afgelopen jaren. Daarnaast bleek de gemiddelde follow-up te variëren van 4 tot 27 jaar. Afhankelijk van de leeftijd bij de aanvang van het cohort en het type klinische eindpunt kan de absolute kans sterk variëren tussen studies. Tevens kan een korte follow-up leiden tot minder CV gebeurtenissen.
Een laag aantal gebeurtenissen leidt tot schattingen met weinig precisie en daarmee tot een laag onderscheidend vermogen.
Toevoegde waarde van pre-eclampsie of zwangerschapshypertensie in de cardiovasculaire risicoprofilering
Onderzoek waarin gekeken is of het nuttig is om informatie over het hebben gehad van pre-eclampsie of zwangerschapshypertensie te betrekken in de risicoprofilering van vrouwen kon de werkgroep niet vinden. Er is wel een recente aanbeveling van de American Heart Association (AHA) die aangeeft dat vrouwen met een pre-eclampsie gezien moeten worden als ‘high risk’ groep (Bushnell 2014). Deze aanbeveling is echter niet gebaseerd op individueel onderzoek maar komt voort uit de beschikbare bewijsvoering zoals wij die hierboven ook geschetst hebben.
Onderbouwing
Tijdens de laatste decennia is steeds duidelijker geworden dat vrouwen met hypertensieve problemen en complicaties tijdens de zwangerschap een verhoogd risico hebben op hart- en vaatziekten (HVZ) later in het leven. Een groeiend aantal onderzoeken laat zien dat bij vrouwen die zwangerschapshypertensie (PIH) of pre-eclampsie (PE) hebben gehad na de bevalling vaker sprake is van afwijkingen in klassieke cardiovasculaire (CV) risicofactoren (hypertensie, dyslipidemie, overgewicht, gestoorde glucosetolerantie, diabetes mellitus) dan bij vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt. Bovendien is in een aantal cohortonderzoeken vastgesteld dat een deel van deze nog relatief jonge vrouwen een verhoogd 10-jaars en/of ‘life-time’ risico heeft op het krijgen van een CV gebeurtenis of op het overlijden aan een CV aandoening. Kennis over de verhoogde risico’s is geen gemeengoed bij behandelaars en de vrouwen zelf en over de precieze hoogte van de risico’s na een PIH of een PE is nog onduidelijkheid.
Dit wordt mede veroorzaakt doordat er verschillende vormen van verhoogde bloeddruk in de zwangerschap zijn en er verschillende definities worden gebruikt. Ook zijn er tussen de studies verschillen in de tijdsperioden tussen de zwangerschap en de gemeten CV risico’s (follow-up). Zo kan sprake zijn van zwangerschapshypertensie (PIH) waarbij sprake is van een verhoogde bloeddruk ontstaan tijdens de zwangerschap óf van een reeds aanwezige hoge bloeddruk vóór de zwangerschap (pre-existent verhoogde bloeddruk). Pre-eclampsie is een ernstige vorm van zwangerschapshypertensie waarbij tevens sprake is van eiwitverlies in de urine. Bij PE kan sprake zijn van een vroege vorm (vroege PE), meestal gedefinieerd als PE die wordt vastgesteld of leidt tot een bevalling vóór een zwangerschapsduur van 34 complete weken, en van een vorm die later optreedt (late PE). Late PE komt vaker voor dan de vroege variant. Men neemt aan dat verschillende mechanismen een rol spelen in de ontwikkeling van vroege en late PE en PIH (Steegers, 2010). De risico’s op de ontwikkeling van ongunstige CV risicofactoren en CV gebeurtenissen variëren tussen deze uitingsvormen. Dit zou kunnen leiden tot verschillende verbanden met het toekomstige risico op HVZ. Daarom is hier gekozen voor een beschrijving van de afzonderlijke resultaten voor PIH en PE. Waar mogelijk wordt ook onderscheid gemaakt tussen vroege en late PE.
Pre-eclampsie
|
Kwaliteit van bewijs: A1 |
Vrouwen met een pre-eclampsie in de voorgeschiedenis hebben een verhoogd risico op een fatale of niet fatale cardiovasculaire gebeurtenis (RR 2.15, 95% BI 1.76-2.61) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Bhattacharya 2011; Funai 2005; Kestenbaum 2003; Lin 2011; Lykke 2010; Mongraw 2010; Ray 2005; Skjaerven 2012 |
|
Kwaliteit van bewijs: A1 |
Vrouwen met een pre-eclampsie in de voorgeschiedenis hebben een verhoogd risico op een fatale of niet fatale ischemische hartziekten (RR 2.06, 95% BI 1.68-2.52) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Bhattacharya 2011; Haukkamaa 2009; Irgens 2001; Lin 2011; Lykke 2009; Smith 2001; Wikstrom 2005 |
|
Kwaliteit van bewijs: A1 |
Vrouwen met een pre-eclampsie in de voorgeschiedenis hebben een verhoogd risico op een fatale of niet fatale beroerte (RR 1.53, 95% BI 1.21-1.92) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Bhattacharya 2011; Irgens 2001; Lin 2011; Lykke 2009 |
|
Kwaliteit van bewijs: A2 |
Vrouwen met een vroege pre-eclampsie in de voorgeschiedenis hebben een 3-9 x hoger hoger risico op een cardiovasculaire gebeurtenis in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Mongraw 2010; Skjaerven 2012 |
|
Kwaliteit van bewijs: A1 |
Vrouwen met een pre-eclampsie in de voorgeschiedenis hebben een verhoogd risico op het ontwikkelen van hypertensie op latere leeftijd (RR 2.76, 95% BI 1.63- 4.69) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Haukkamaa 2009; Lykke 2009; Magnussen 2009 |
|
Kwaliteit van bewijs: A1 |
Vrouwen met een pre-eclampsie in de voorgeschiedenis hebben een verhoogd risico op het ontwikkelen van diabetes mellitus type 2 (RR 2.27, 95% BI 1.55-3.32) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Callaway 2007; Carr 2009; England 2011; Libby 2006; Lykke 2009; Magnussen 2009 |
|
Kwaliteit van bewijs: B |
Vrouwen met een pre-eclampsie in de voorgeschiedenis hebben geen verhoogd risico op het ontwikkelen van dyslipidemie (RR 1.07, 95% BI 0.74-1.54) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Drost 2012; Edlow 2009; Marin 2000; Sattar 2003 |
Zwangerschapshypertensie
|
Kwaliteit van bewijs: A1 |
Vrouwen met een zwangerschapshypertensie in de voorgeschiedenis hebben een verhoogd risico op een fatale of niet fatale cardiovasculaire gebeurtenis (RR 1.89, 95% BI 1.31-2.72) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Bhattacharya 2011, Kestenbaum 2003, Lykke 2010, Ray 2005 |
|
Kwaliteit van bewijs: A1 |
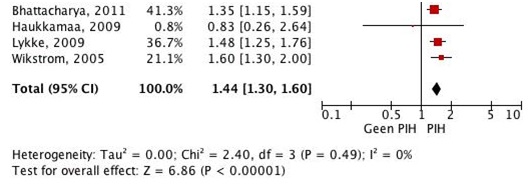
Vrouwen met een zwangerschapshypertensie in de voorgeschiedenis hebben een verhoogd risico op een fatale of niet fatale ischemische hartziekten (RR 1.44, 95% BI 1.30-1.60) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Bhattacharya 2011; Haukkamaa 2009; Lykke 2009; Wikstrom 2005 |
|
Kwaliteit van bewijs: A2 |
Vrouwen met een zwangerschapshypertensie in de voorgeschiedenis hebben een verhoogd risico op een fatale of niet fatale beroerte (RR 1.41, 95% BI 1.20-1.65) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Bhattacharya 2011; Lykke 2009 |
|
Kwaliteit van bewijs: B |
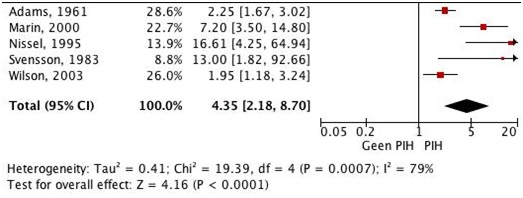
Vrouwen met een zwangerschapshypertensie in de voorgeschiedenis hebben een verhoogd risico op het ontwikkelen van hypertensie op latere leeftijd (RR 4.35, 95% BI 2.18-8.70) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Adams 1961; Marin 2000; Nissel 1995; Svensson 1983; Wilson 2003 |
|
Kwaliteit van bewijs: A1 |
Vrouwen met een zwangerschapshypertensie of pre-eclampsie in de voorgeschiedenis hebben een verhoogd risico op het ontwikkelen van diabetes mellitus type 2 (RR 2.10, 95% BI 1.45-3.04) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Gegevens over alleen zwangerschapshypertensie zijn niet beschikbaar. Callaway 2007, Carr 2009, Cassidy 2009, England 2011, Garovic 2010, Libby 2006, Lykke 2009, Magnussen 2009 |
|
Kwaliteit van bewijs: B |
Vrouwen met een zwangerschapshypertensie in de voorgeschiedenis hebben geen verhoogd risico op het ontwikkelen van dyslipidemie (RR 1.07, 95% BI 0.74-1.54) in vergelijking met vrouwen die een ongecompliceerde zwangerschap hebben gehad. Drost 2012; Edlow 2009; Marin 2000; Sattar 2003 |
Uitgangsvraag 1
Wat is het risico op een cardiovasculaire gebeurtenis voor vrouwen met pre-eclampsie of zwangerschapshypertensie in de voorgeschiedenis?
Uit de elders gedefinieerde zoekstrategie en na de beoordeling van de beoordelaars kwamen 23 onderzoeken naar voren die geschikt werden geacht voor het beantwoorden van deze uitgangsvraag (Arnadottir 2005, Ben-Ami 2010, Bhattacharya 2011, Freibert 2011, Funai 2005, Garovic 2010, Hannaford 1997, Haukkamaa 2009, Irgens 2001, Jonsdottir 1995, Kestenbaum 2003, Lin 2011, Lykke 2009, Lykke 2010, Marin 2000, Mongraw 2010, Ray 2005, Shalom 2013, Skjaerven 2012, Smith 2001, Spaan 2009, Wang 2011, Wikstrom 2005). De beschrijving van alle ruwe resultaten op basis waarvan de onderstaande figuren zijn gemaakt staat in bijlage 4. Voor de zoekverantwoording wordt verwezen naar bijlage 5 en voor de evidencetabel naar bijlage 6.
Het betrof 19 cohortonderzoeken en 4 onderzoeken op basis van patiënten series. In de onderzoeken werden verschillende definities gebruikt van PIH en PE; deze definities staan per onderzoek in de betreffende tabellen vermeld (bijlage 4). De tijdsperiode waarin deelnemers zijn gevolgd, de follow-up, varieerde aanzienlijk met een spreiding tussen de 5 en 20 jaar.
De figuren (4.1.1. t/m 4.1.6.) geven de kans weer op het krijgen van een CV gebeurtenis bij vrouwen die een PE of PIH hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben gehad. Resultaten worden per studie weergegeven als een relatief risico (RR) met bijbehorend 95% betrouwbaarheidsinterval (95% BI).
Pre-eclampsie - cardiovasculaire gebeurtenissen
In tabel 4.1.1. t/m 4.1.3. (bijlage 4) worden de studies beschreven met respectievelijk een CV gebeurtenis, IHZ en beroerte als uitkomstmaat.
Uit de cohortonderzoeken komt naar voren dat vrouwen die pre-eclampsie hebben gehad een 2.15 (95% BI 1.76-2.61) hogere kans hebben op het krijgen van een CV gebeurtenis dan vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt. (Figuur 4.1.1.).
Figuur 4.1.1. De kans op het krijgen van een CV gebeurtenis voor vrouwen die pre-eclampsie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
CV gebeurtenis |

In figuur 4.1.2. wordt voor IHZ een verhoogde kans van 2.06 (95% BI 1.68-2.02) weergegeven voor vrouwen die pre-eclampsie hebben gehad. In figuur 4.1.3. wordt voor beroerte een verhoogd risico van 1.53 (95% BI 1.21-1.92) weergegeven.
Figuur 4.1.2. De kans op het krijgen van ischemische hartziekte (IHZ) bij vrouwen die pre-eclampsie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
IHZ |

Figuur 4.1.3. De kans op het krijgen van een beroerte bij vrouwen die pre-eclampsie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
Beroerte |

Er werden twee onderzoeken gevonden waarbij onderscheid is gemaakt in vroege en late PE. De definitie van vroege PE werd in de ene studie gedefinieerd als het optreden van PE voor een zwangerschapsduur van 34 weken (Mongraw 2010) en in de andere studie als het optreden van PE voor 36 weken (Skjaerven 2012). Over het algemeen lieten beide studies zien dat het risico op een CV gebeurtenis hoger was voor vroege PE dan voor late PE ten opzichte van vrouwen met een ongecompliceerde zwangerschap. De gerapporteerde hazard ratio’s (HR) voor hart- en vaatziekten waren in de studie van Mongraw (2010) 9.5 (95% BI 3.5-20.3) en in de studie van Skjaerven (2012) 3.7 (95% BI 2.7-4.8) voor vroege PE. Voor late PE waren de HR’s respectievelijk 2.1 (95% BI 1.3-3.4) en 1.6 (95% BI 1.4-2.0). Voor beroerte (Irgens 2001 en Wang 2011) en IHZ (Irgens 2001) werden verbanden in dezelfde richting gezien (tabel 4.1.2. en 4.1.3.).
Zwangerschapshypertensie - cardiovasculaire gebeurtenissen
In tabel 4.1.1. t/m 4.1.3. (bijlage 4) worden de studies beschreven met respectievelijk een CV gebeurtenis, IHZ en beroerte als uitkomstmaat.
Uit de cohortonderzoeken komt naar voren dat vrouwen die zwangerschapshypertensie hebben gehad een 1.89 (95% BI 1.31-2.72) hogere kans hebben op het krijgen van een CV gebeurtenis dan vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt (Figuur 4.1.4.). Uit figuur 4.1.5. blijkt voor IHZ een verhoogde kans van 1.44 (95% BI 1.30-1.60). Uit figuur 4.1.6. blijkt voor beroerte (CVA) een verhoogd risico van 1.41 (95% BI 1.20-1.65).
Figuur 4.1.4. De kans op het krijgen van een CV gebeurtenis bij vrouwen die zwangerschapshypertensie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
CV gebeurtenis |

Figuur 4.1.5. De kans op het krijgen van IHZ bij vrouwen die zwangerschapshypertensie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
IHZ |
Figuur 4.1.6. De kans op het krijgen van een beroerte bij vrouwen die zwangerschapshypertensie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
Beroerte |

Uitgangsvraag 2
Wat zijn de risico’s op een ongunstig cardiovasculaire risicoprofiel voor vrouwen met pre-eclampsie of zwangerschapshypertensie in de voorgeschiedenis?
Uit de elders gedefinieerde zoekstrategie en na de beoordeling van de beoordelaars kwamen 33 onderzoeken naar voren die geschikt werden geacht voor het beantwoorden van deze uitgangsvraag (Adams 1961, Berends 2008, Bhattacharya 2011, Callaway 2007, Callaway 2011, Canti 2010, Carr 2009, Cassidy, 2009, Drost 2012, Edlow 2009, England 2011, Epstein 1964, Garovic 2010, Gaugler 2008, Hannaford 1997, Kharazmi 2007, Haukkamaa 2009, Lazdam 2012, Libby 2006, Lindeberg 1988, Lykke 2009, Magnussen 2009, Marin 2000, Nisell 1995, North 1996, Portelinha 2010, Sattar 2003, Shahbazian 2011, Shalom 2013, Sibai, 1986, Spaan 2009, Svensson 1983, Wilson 2003). De beschrijving van alle ruwe resultaten op basis waarvan de onderstaande figuren zijn gemaakt staat in bijlage 4. Voor de zoekverantwoording wordt verwezen naar bijlage 5 en voor de evidencetabel naar bijlage 6.
Het betrof 15 cohortonderzoeken en 18 onderzoeken op basis van patiënten series. In de onderzoeken werden verschillende definities gebruikt van PIH en PE; deze definities staan per onderzoek in de betreffende tabellen vermeld (bijlage 4). De tijdsperiode waarin deelnemers zijn gevolgd, de follow-up, varieerde aanzienlijk: tussen de 0.6 en 46 jaar na de index zwangerschap. Ook deze staat in de tabellen gespecificeerd.
De figuren (4.1.7. t/m 4.1.9.) geven de kans weer op een risicofactor van een genoemde CV gebeurtenis bij vrouwen die PE of PIH hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt. Resultaten worden per studie weergegeven als een RR met bijbehorend 95% BI.
Pre-eclampsie - hypertensie
In tabel 4.1.4. (bijlage 3) worden de studies beschreven met hypertensie als uitkomstmaat.
Uit de cohortonderzoeken komt naar voren dat vrouwen die pre-eclampsie hebben gehad een 2.76 (95% BI 1.63-4.69) hogere kans hebben op het ontwikkelen van hypertensie dan vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt (Figuur 4.1.7.). Uit figuur 4.1.8. blijkt dat deze kansen veel hoger liggen wanneer alleen naar de resultaten van onderzoeken uit patiënten series wordt gekeken, namelijk een verhoogde kans van 4.81 (95% BI 3.25-7.11); echter de patiënten series waren vaker veel kleinere studies.
Figuur 4.1.7. De kans op het ontwikkelen van hypertensie bij vrouwen die pre-eclampsie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben gehad op basis van cohortonderzoeken.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
Hypertensie |

De absolute kans om hypertensie te ontwikkelen na een zwangerschap die gecompliceerd werd door PE is moeilijk te schatten uit de gegevens van de cohortonderzoeken. Dit komt met name omdat de tijdsperiode dat de vrouwen gevolgd zijn sterk wisselde tussen de studies en dat de gegevens niet altijd uit de artikelen te extraheren zijn. Zo bleek uit het onderzoek van Lykke et al. (2009) dat bij een gemiddelde leeftijd van 41.6 jaar, 15 jaar na de index zwangerschap met pre-eclampsie sprake was van hypertensie bij 7.7% (1958/25184); bij de vrouwen met een ongecompliceerde zwangerschap had ongeveer 1.9% hypertensie (tabel 4.1.4.; bijlage 3).
Figuur 4.1.8. De kans op het ontwikkelen van hypertensie bij vrouwen die pre-eclampsie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt op basis van cohorten die bestaan uit patiënten series en op leeftijd gematchte controle groepen.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
Hypertensie |

Zwangerschapshypertensie - hypertensie
In tabel 4.1.4. (bijlage 4) worden de studies beschreven met hypertensie als uitkomstmaat.
De gegevens op dit gebied zijn veel beperkter dan voor pre-eclampsie. Slechts twee cohortstudies zijn beschikbaar die gegevens over hypertensie laten zien. De bevindingen variëren aanzienlijk tussen deze twee studies, zodat we de resultaten niet hebben samengevoegd. Het onderzoek van Lykke et al. (2009) liet een verhoogd risico zien op het ontwikkelen van hypertensie van 5.31 (95% BI 4.90-5.75), hetgeen gecorrigeerd was voor verschillende potentieel verstorende variabelen. Het onderzoek van Haukkamaa et al. (2009) liet ook een verhoogd risico zien maar deze was veel lager: 1.52 (95% BI 1.10-2.20), zonder correctie voor potentieel verstorende variabelen.
In figuur 4.1.9. zien we bevindingen uit de onderzoeken met patiënten series. Deze resultaten laten een verhoogde kans van 4.35 (95% BI 2.18-8.70) zien. Echter er zijn grote verschillen tussen de omvang van de populaties in de studies en precisie in de schatting van het relatieve risico.
Ook voor deze groep is de absolute kans om hypertensie te ontwikkelen na een zwangerschap die gecompliceerd werd door PIH moeilijk te schatten uit de gegevens van de onderzoeken.
Figuur 4.1.9. De kans op het ontwikkelen van hypertensie bij vrouwen die zwangerschapshypertensie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt op basis van cohorten die bestaan uit patiënten series en op leeftijd gematchte controle groepen.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
Hypertensie |
Pre-eclampsie en zwangerschapshypertensie - diabetes mellitus type 2
In tabel 4.1.5. (bijlage 3) worden de studies beschreven met diabetes mellitus type 2 (DM II) als uitkomstmaat. Op basis van de cohortonderzoeken komt naar voren dat vrouwen die pre-eclampsie hebben gehad een 2.27 (95% BI 1.55-3.32) hogere kans hebben op het ontwikkelen van diabetes mellitus dan vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt (figuur 4.1.7.). Uit figuur 4.1.8. blijkt dat deze kansen hetzelfde zijn wanneer de onderzoeken worden gebruikt waarbij geen onderscheid gemaakt is tussen pre-eclampsie en zwangerschapshypertensie, namelijk een verhoogde kans van 2.10 (95% BI 1.45-3.04). Er zijn geen studies beschikbaar voor zwangerschapshypertensie alleen.
Figuur 4.1.7. De kans op het ontwikkelen van diabetes mellitus type 2 (DM II) bij vrouwen die pre-eclampsie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben gehad op basis van cohort onderzoeken
|
Studie |
Gewicht |
Relatief risico (95% BI) |
DM II |

Figuur 4.1.8. De kans op het ontwikkelen van diabetes mellitus type 2 (DM II) bij vrouwen die pre-eclampsie of zwangerschapshypertensie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben gehad op basis van cohort onderzoek.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
DM II |

Pre-eclampsie en zwangerschapshypertensie - dyslipidemie
In tabel 4.1.6. (bijlage 4) worden de studies beschreven met dyslipidemie als uitkomstmaat.
Op basis van deze onderzoeken komt naar voren dat vrouwen die pre-eclampsie of zwangerschapshypertensie hebben gehad geen hogere kans hebben op het ontwikkelen van een ongunstig lipidenprofiel dan vrouwen die een ongecompliceerde zwangerschap hebben doorgemaakt (Figuur 4.1.9.).
Figuur 4.1.9. De kans op het ontwikkelen van dyslipidemie bij vrouwen die pre-eclampsie en of zwangerschapshypertensie hebben gehad ten opzichte van vrouwen die een ongecompliceerde zwangerschap hebben gehad op basis van cohortonderzoeken en op basis van cohorten die bestaan uit patiënten series en op leeftijd gematchte controle groepen.
|
Studie |
Gewicht |
Relatief risico (95% BI) |
Dyslipidemie |

- Adams, E.M., Macgillivray, I. (1961). Long-term effect of preeclampsia on blood-pressure. Lancet, 23, 1373-5.
- Arnadottir, G. A., Geirsson, R. T., Arngrimsson, R., Jonsdottir, L. S., & Olafsson, O. (2005). Cardiovascular death in women who had hypertension in pregnancy: a case-control study. BJOG: An International Journal of Obstetrics & Gynaecology, 112, 286-292.
- Ben-Ami, S., Oron, G., Ben-Haroush, A., Blickstein, D., Hod, M., & Bar, J. (2010). Primary atherothrombotic occlusive vascular events in premenopausal women with history of adverse pregnancy outcome. Thrombosis Research, 125, 124-127.
- Berends, A. L., de Groot, C. J., Sijbrands, E. J., Sie, M. P., Benneheij, S. H., Pal, R. et al. (2008). Shared constitutional risks for maternal vascular-related pregnancy complications and future cardiovascular disease. Hypertension, 51, 1034-1041.
- Bhattacharya, S., Prescott, G. J., Iversen, L., Campbell, D. M., Smith, W. C. S., & Hannaford, P. C. (2012). Hypertensive disorders of pregnancy and future health and mortality: A record linkage study. Pregnancy Hypertension, 2, 1-7.
- Bushnell, C., McCullough, L. D., Awad, I. A., Chireau, M. V., Fedder, W. N., Furie, K. L. et al. (2014). Guidelines for the Prevention of Stroke in Women: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke.
- Callaway, L. K., Lawlor, D. A., O'Callaghan, M., Williams, G. M., Najman, J. M., & MBIntyre, H. D. (2007). Diabetes mellitus in the 21 years after a pregnancy that was complicated by hypertension: findings from a prospective cohort study. American Journal of Obstetrics & Gynecology, 197, 492-497.
- Callaway, L. K., David, M. H., Williams, G. M., Najman, J. M., Lawlor, D. A., & Mamun, A. (2011). Diagnosis and treatment of hypertension 21 years after a hypertensive disorder of pregnancy. Australian & New Zealand Journal of Obstetrics & Gynaecology, 51, 437-440.
- Canti, I. C., Komlos, M., Martins-Costa, S. H., Ramos, J. G., Capp, E., & Corleta, H. (2010). Risk factors for cardiovascular disease ten years after preeclampsia. Sao Paulo Medical Journal = Revista Paulista de MediBIna, 128, 10-13.
- Carr, D. B., Newton, K. M., Utzschneider, K. M., Tong, J., Gerchman, F., Kahn, S. E. et al. (2009). Preeclampsia and risk of developing subsequent diabetes. Hypertension in Pregnancy, 28, 435-447.
- Cassidy, A., Chiuve, S.E., Manson, J.E., Rexrode, K.M., Girman, C.J., Rimm, E.B. (2009). Potential role for plasma placental growth factor in predicting coronary heart disease risk in women. Arterioscler Thromb Vasc Biol, 29, 134-9.
- Drost, J. T., ArpaBI, G., Ottervanger, J. P., de Boer, M. J., van, E. J., van der Schouw, Y. T. et al. (2012). Cardiovascular risk factors in women 10 years post early preeclampsia: the Preeclampsia Risk EValuation in FEMales study (PREVFEM). European Journal of Preventive Cardiology, 19, 1138-1144.
- Edlow, A. G., Srinivas, S. K., & Elovitz, M. A. (2009). Investigating the risk of hypertension shortly after pregnanBIes complicated by preeclampsia. American Journal of Obstetrics & Gynecology, 200, e60-e62.
- Engeland, A., Bjorge, T., Daltveit, A. K., Skurtveit, S., Vangen, S., Vollset, S. E. et al. (2011). Risk of diabetes after gestational diabetes and preeclampsia. A registry-based study of 230,000 women in Norway. European Journal of Epidemiology, 26, 157-163.
- Eptein, F.H. (1964) Late vascular effects of toxemia of pregnancy. N Engl J Med., 20, 391-5
- Freibert SM, Mannino DM, Bush H, Crofford LJ (2011). The assoBIation of adverse pregnancy events and cardiovascular disease in women 50 years of age and older. J Womens Health, 20, 287-93.
- Funai, E. F., Friedlander, Y., Paltiel, O., Tiram, E., Xue, X., Deutsch, L. et al. (2005). Long-term mortality after preeclampsia. Epidemiology, 16, 206-215.
- Garovic, V. D., Bailey, K. R., Boerwinkle, E., Hunt, S. C., Weder, A. B., Curb, D. et al. (2010). Hypertension in pregnancy as a risk factor for cardiovascular disease later in life. Journal of Hypertension, 28, 826-833.
- Gaugler-Senden, I. P., Berends, A. L., de Groot, C. J., & Steegers, E. A. (2008). Severe, very early onset preeclampsia: subsequent pregnanBIes and future parental cardiovascular health. European Journal of Obstetrics, Gynecology, & Reproductive Biology, 140, 171-177.
- Hannaford, P., Ferry, S., & Hirsch, S. (1997). Cardiovascular sequelae of toxaemia of pregnancy. Heart, 77, 154-158.
- Haukkamaa, L., Moilanen, L., Kattainen, A., Luoto, R., Kahonen, M., Leinonen, M. et al. (2009). Pre-eclampsia is a risk factor of carotid artery atherosclerosis. Cerebrovascular Diseases, 27, 599-607.
- Irgens, H. U., Reisaeter, L., Irgens, L. M., & Lie, R. T. (2001). Long term mortality of mothers and fathers after pre-eclampsia: Population based cohort study. British Medical Journal, 323, 1213-1216.
- Jonsdottir, L. S., Arngrimsson, R., Geirsson, R. T., Sigvaldason, H., & Sigfusson, N. (1995). Death rates from ischemic heart disease in women with a history of hypertension in pregnancy. Acta ObstetriBIa et Gynecologica Scandinavica, 74, 772-776.
- Kestenbaum, B., Seliger, S. L., Easterling, T. R., Gillen, D. L., Critchlow, C. W., Stehman-Breen, C. O. et al. (2003). Cardiovascular and thromboembolic events following hypertensive pregnancy. American Journal of Kidney Diseases, 42, 982-989.
- Kharazmi E, Kaaja R, Fallah M, Luoto R (2007). Pregnancy-related factors and the risk of isolated systolic hypertension. Blood Press., 16, 50-5.
- Lazdam, M., De La Horra, A., Diesch, J., Kenworthy, Y., Davis, E., Lewandowski, A. J. et al. (2012). Unique blood pressure characteristics in mother and offspring after early onset preeclampsia. Hypertension, 60, 1338-1345.
- Libby, G., Murphy, D. J., McEwan, N. F., Greene, S. A., Forsyth, J. S., Chien, P. W. et al. (2007). Pre-eclampsia and the later development of type 2 diabetes in mothers and their children: an intergenerational study from the Walker cohort. Diabetologia, 50, 523-530.
- Lin, Y. S., Tang, C. H., Yang, C. Y., Wu, L. S., Hung, S. T., Hwa, H. L. et al. (2011). Effect of pre-eclampsia-eclampsia on major cardiovascular events among peripartum women in Taiwan.[Erratum appears in Am J Cardiol. 2011 Apr 1;107(7):1104]. American Journal of Cardiology, 107, 325-330.
- Lindeberg, S., Axelsson, O., Jorner, U., Malmberg, L., & Sandstrom, B. (1988). A prospective controlled five-year follow-up study of primiparas with gestational hypertension. Acta ObstetriBIa et Gynecologica Scandinavica, 67, 605-609.
- Lykke, J. A., Langhoff-Roos, J., Sibai, B. M., Funai, E. F., Triche, E. W., & Paidas, M. J. (2009). Hypertensive pregnancy disorders and subsequent cardiovascular morbidity and type 2 diabetes mellitus in the mother. Hypertension, 53, 944-951.
- Lykke, J. A., Langhoff-Roos, J., Lockwood, C. J., Triche, E. W., & Paidas, M. J. (2010). Mortality of mothers from cardiovascular and non-cardiovascular causes following pregnancy complications in first delivery. Paediatric and Perinatal Epidemiology, 24, 323-330.
- Magnussen, E. B., Vatten, L. J., Smith, G. D., & Romundstad, P. R. (2009). Hypertensive disorders in pregnancy and subsequently measured cardiovascular risk factors. Obstetrics & Gynecology, 114, 961-970.
- Marin, R., Gorostidi, M., Portal, C. G., Sanchez, M., Sanchez, E., & Alvarez, J. (2000). Long-term prognosis of hypertension in pregnancy. Hypertension in Pregnancy, 19, 199-209.
- Mongraw-Chaffin, M. L., BIrillo, P. M., & Cohn, B. A. (2010). Preeclampsia and cardiovascular disease death: prospective evidence from the child health and development studies cohort. Hypertension, 56, 166-171.
- Nisell, H., Lintu, H., Lunell, N. O., Mollerstrom, G., & Pettersson, E. (1995). Blood pressure and renal function seven years after pregnancy complicated by hypertension. British Journal of Obstetrics & Gynaecology, 102, 876-881.
- North, R. A., Simmons, D., Barnfather, D., & Upjohn, M. (1996). What happens to women with preeclampsia? Microalbuminuria and hypertension following preeclampsia. Australian & New Zealand Journal of Obstetrics & Gynaecology, 36, 233-238.
- Opstelten, W., Scholten, R.J.P.M. (2014). Meta-analyse: prinBIpes en valkuilen. Ned Tijdschr Geneeskd., 158, A6882.
- Portelinha A, Belo L, Cerdeira AS, Braga J, Tejera E, Pinto F, Pinto A, Areias MJ, PatríBIo B, Rebelo I (2010). Lipid levels including oxidized LDL in women with history of preeclampsia. Hypertens Pregnancy, 29, 93-100
- Ray, J. G., Vermeulen, M. J., Schull, M. J., & Redelmeier, D. A. (2005). Cardiovascular health after maternal placental syndromes (CHAMPS): population-based retrospective cohort study. Lancet, 366, 1797-1803.
- Sattar, N., Ramsay, J., Crawford, L., Cheyne, H., & Greer, I. A. (2003). Classic and novel risk factor parameters in women with a history of preeclampsia. Hypertension, 42, 39-42.
- Shahbazian, N., Shahbazian, H., Ehsanpour, A., Aref, A., & Gharibzadeh, S. (2011). Hypertension and microalbuminuria 5 years after pregnanBIes complicated by pre-eclampsia.[Erratum appears in Iran J Kidney Dis. 2012 Jul;6(4):321]. Iranian journal of Kidney Diseases, 5, 324-327.
- Shalom, G., Shoham-Vardi, I., Sergienko, R., Wiznitzer, A., Sherf, M., & Sheiner, E. (2013). Is preeclampsia a significant risk factor for long-term hospitalizations and morbidity. Journal of Maternal-Fetal and Neonatal MediBIne, 26, 13-15.
- Sibai BM, el-Nazer A, Gonzalez-Ruiz A (1986). Severe preeclampsia-eclampsia in young primigravid women: subsequent pregnancy outcome and remote prognosis. Am J Obstet Gynecol., 155, 1011-6.
- Skjaerven, R., Wilcox, A. J., Klungsoyr, K., Irgens, L. M., Vikse, B. E., Vatten, L. J. et al. (2012). Cardiovascular mortality after pre-eclampsia in one child mothers: prospective, population based cohort study. BMJ, 345, e7677.
- Smith, G. C., Pell, J. P., & Walsh, D. (2001). Pregnancy complications and maternal risk of ischaemic heart disease: a retrospective cohort study of 129,290 births. Lancet, 357, 2002-2006.
- Spaan, J. J., Ekhart, T., Spaanderman, M. E., & Peeters, L. L. (2009). Remote hemodynamics and renal function in formerly preeclamptic women. Obstetrics & Gynecology, 113, 853-859.
- Steegers, E.A., von Dadelszen, P., Duvekot, J.J., Pijnenborg, R (2010). Pre-eclampsia. Lancet, 376, 631-644
- Svensson, A., Andersch, B., & Hansson, L. (1983). A clinical follow-up study of 260 women with hypertension in pregnancy. Clinical & Experimental Hypertension - Part B, Hypertension in Pregnancy, 2, 95-102.
- Wang, I. K., Chang, S. N., Liao, C. C., Liang, C. C., Chang, C. T., Lin, H. H. et al. (2011). Hypertensive disorders in pregnancy and preterm delivery and subsequent stroke in Asian women: A retrospective cohort study. Stroke, 42, 716-721.
- Wikstrom, A. K., Haglund, B., Olovsson, M., & Lindeberg, S. N. (2005). The risk of maternal ischaemic heart disease after gestational hypertensive disease. BJOG: An International Journal of Obstetrics & Gynaecology, 112, 1486-1491.
- Wilson, B. J., Watson, M. S., Prescott, G. J., Sunderland, S., Campbell, D. M., Hannaford, P. et al. (2003). Hypertensive diseases of pregnancy and risk of hypertension and stroke in later life: results from cohort study. BMJ, 326, 845.
|
Reference |
Study type |
Characteristics |
Determinant (I) |
Controls (C)
|
Outcome measures and follow-up time |
Results |
Quality assessment study |
|
Adams, 1961 |
Design Case-control study
N = 531
Country UK |
Aim of the study: whether blood-pressure in middle-aged parous women depends on whether or not they have had pre-eclampsia and to compare the blood-pressure of parous women with those of nulliparous women.
Inclusion criteria - women deliverd in the Aberdeen Maternity Hospital between 1938-43 and were primiparae and under 30 years of age
Exclusion criteria
|
Determinant
1) Severe PE in first pregnancy
N = 53
2) Mild PE in first pregnancy = PIH
N = 96 |
Controls
3) Normal BP in first pregnancy
N = 185
4) Nulliparae aged 35-50
N = 197 |
Primary outcomes: Blood-pressure
Secundary outcomes:
Follow up: 1) 16.9 yr 2) 17.6 yr 3) 17.8 yr |
Primary outcomes:
|
Clearly defined groups: Yes, severe pre-eclampsia was defined as a rise of the diastolic blood-pressure in the last trimester to 90 mmHg or more, on at least two occasions, together with definite proteinuria (0.25 g. per litre, or more). Mild pre-eclampsia was defined as a rise of diastolic pressure in the last trimester to 90 mmHg or more on at least two occasions, without proteinuria. The blood-pressure fell to normal during the puerperium. Controls had diastolic pressures below 90 mmHg throughout their first pregnancies and who had no proteinuria.
Selection bias: Possible, see selective loss to follow up
Method of assessing the outcome appropriately: Yes, all interviews and examinations were by one investigator (E. M. A.) except for 21 nulliparous factory workers who were seen by I. MacG.
Selective loss to follow up: Yes, suitable cases with an address in Aberdeen were written to participate in the study. By these means, about half the cases at risk were contacted. Very few refused to cooperate.
Identification confounders and correction in analysis: No
Funding: Not reported
|
|
Arnadottir, 2005 |
Design Case-control study
N = 629
Country Iceland |
Aim of the study: To determine whether an association exists between hypertension in pregnancy and later development of cardiovascular disease.
Inclusion criteria PE - women with hypertension in pregnancy in the years 1931-47 at the Landspitali University Hospital in Reykjavik Controls: - delivering before or after the case and matched for parity and age
Exclusion criteria - incomplete records - mortality as a result of the hypertensive disease during pregnancy - a history of underlying diabetes, renal disorders or other medical disease at the time of delivery and pre-existing hypertension |
Determinant Hypertensive disease in pregnancy
N = 325 |
Controls non-hypertensive, non-proteinuric control women, delivering just before or after the case woman, usually within two months and matched for parity and for age
N = 629 |
Primary outcomes: death due to to ischemic heart disease, stroke or cancer
Secundary outcomes:
Follow up: 31st December 1996
Cases: 50 yr Controls: 55 yr |
Primary outcomes: At the end of the follow up period, 194 (59.7%) of the cases and 331 (52.6%) of the controls had died.
Death with any evidence of ischaemic heart disease was significantly more common (n = 79/325, 24.3%) in the cases than among controls (n = 92/629, 14.6%) (RR 1.66; 95% CI 1.27–2.17) Cerebrovascular event deaths were 31 (9.5%) among cases and 41 (6.5%) in the controls (RR 1.46; 95% CI 0.94–2.28). Deaths from all cardiovascular causes were 110 (33.8%) of cases and 133 (21.1%) of controls (RR 1.60; 95% CI 1.29–1.98).
|
Clearly defined groups: Yes, eclampsia was defined as a seizure either antenatally, in labour or within 24 hours of delivery in a woman with raised blood pressure (BP) after 20 weeks of gestation, severe pre-eclampsia as a BP ≥ 160/110 mmHg with or without proteinuria or BP ≥ 160/100 with proteinuria (two assessments) after 20 weeks of gestation, mild preeclampsia as BP ≥ 140/90 with proteinuria and gestational hypertension as BP ≥ 140/90 without proteinuria after 20 weeks of gestation.
Selection bias: Not expected
Method of assessing the outcome appropriately: Information on whether the women were alive at 31st December 1996 was obtained from the national identity files of the Statistical Bureau of Iceland and the death certificate was inspected. ICD 9 410–414.9,
Selective loss to follow up: Yes, well described.
Identification confounders and correction in analysis: No information on smoking habits
Funding: Grant from the Landspitali University Hospital Research Fund
|
|
Ben-Ami, 2010 |
Design Case-control study
N = 202
Country Israel |
Aim of the study: To determine if adverse pregnancy outcomes are associated with atherothrombotic occlusive vascular disease (AOVD) in premenopausal women.
Inclusion criteria - women aged less than 50 years with documented AOVD whowere followed and treated (as inpatients or outpatients) at Rabin Medical Center between 1995 and 2004. - controls: Each patient in the study group was matched sequentially for age at the time of the thrombotic event (within less than 2 years) and body mass index (BMI) (within less than 2 kg/m2) with a healthy woman with no personal history of AOVD (1:1 ratio).
Exclusion criteria - Women who had died prior to the present analysis were excluded, as were women who had never been pregnant, were lost at follow up, or refused to participate, and women in whom the vascular event was known to be related to another cause, such as coronary spasm, emboli, cranial hemorrhage, tumor, arteritis, systemic lupus erythematosus, antiphospholipid antibodies, drug use, malignancy, or severe migraine. - diabetes type I |
Determinant Women with AOVD
N = 101
|
Controls Healthy woman with no history of AOVD
N = 101
|
Primary outcomes: Past pregnancy complications in premenopausal women with AOVD.
Secundary outcomes:
Follow up:
|
Primary outcomes: Of the 101 women with AOVD who met the study criteria, 53 had a Myocardial ischemic event, of them 36 (68%) had 1 vessel disease and 17 (32%) had≥2 vessel disease. Of the 33 women with a cerebrovascular event, 24 (73%) had transient ischemic attack and 9 (22%) had ischemic stroke.Of the 15with a peripheral ischemic event, 9 (60%) had aortoiliac and 6 (40%) had nonaortoiliac event. Thirty-two women had recurrent events. The mean age of the women at the time of the atherothrombotic occlusive vascular event was 43.3±5.7 years.
|
Clearly defined groups: Yes, following definitions were used: habitual abortions, as ≥3 consecutive abortions; preterm delivery, as delivery between 23 and 36 weeks of gestation. IUGR was defined as birth weight below the 10th percentile of Israeli growth curves, excluding growth restriction due to fetal malformations or aneuploidy. Preeclampsia and pregnancyinduced hypertension (PIH) were defined according to the International Society for the Study of Hypertension in Pregnancy [8]. Gestational diabetes mellitus (GDM) was defined according to the American College of Obstetricians and Gynecologists
Selection bias: Possible, case-control study
Method of assessing the outcome appropriately: The files were reviewed for classical risk factors for AOVD(ICD-9) and complications of pregnancy (abortions, pregnancy-induced hypertension, preeclampsia, gestational diabetes, intrauterine growth restriction (IUGR), fetal loss and preterm delivery). Findings were compared with healthy women matched for age and body mass index. Hypertension was defined as the use of antihypertensive drugs and/or systolic blood pressure ≥140 mmHg and/or diastolic ≥90 mmHg; dyslipidemia, as the use of statins or a low-density lipoprotein cholesterol (LDL-c) level of N160 mg/dL; type 2 diabetes mellitus, as the use of blood-glucose-lowering medication and/or a fasting glucose plasma level of N126 mg/dL and/or symptoms of diabetes plus a random blood glucose concentration of ≥200 mg/dL.
Selective loss to follow up: No
Identification confounders and correction in analysis: No
Funding: Not reported |
|
Berends, 2008 |
Design Case-control study
N = 212 |
Aim of the study: to provide biochemical and anthropometric evidence to substantiate the hypothesis that cardiovascular risk factors are constitutional in women with a history of pregnancies complicated by preeclampsia or IUGR.
Inclusion criteria - preeclampsia - IUGR - singletons
Exclusion criteria - pregnant - postmenopausal - DM - Lipid-lowering or antihypertensive medication use |
Determinant Preeclampsia
N = 50
|
Controls Uncomplicated pregnancies
N = 106
|
Primary outcomes: anthropometrics, lipids, glucose levels, blood pressure measurements, and IMT
Secundary outcomes:
Follow up: Time interval delivery – study, mean, y
Preeclampsia 7 (±5.6) IUGR 9.3 (±4.6) Controls 13.1 (±5.7) |
Primary outcomes: Diagnosis of hypertension was 5 times more common in formerly preeclamptic women compared with control subjects (46.7% versus 8.9%; P<0.001) and 3 times in women with IUGR-complicated pregnancies (26.9% versus 8.9%; P<0.01). Early Versus Late-Onset Preeclampsia Diastolic blood pressure was higher in women with early onset preeclampsia compared with those with late-onset disease (median, interquartile range: 88 mm Hg, 77 to 93 mm Hg for early onset; 81 mm Hg, 72 to 88 mm Hg for late onset; P=0.04). Diagnosis of hypertension was more common in the early onset than the late-onset group (66.7%) for early onset and 34.4% for late onset; P=0.04). No significant differences were found in the remaining risk factors. The prevalence of metabolic syndrome in the index generation was 3-fold higher in women with a history of preeclampsia compared with control subjects (Figure 2).
|
Clearly defined groups: Yes, Preeclampsia was defined as de novo hypertension (systolic: ≥ 140 mm Hg; diastolic: ≥90 mm Hg) and proteinuria as ≥300 mg/24 hours or ≥1+ on semiquantitative analysis. Preeclampsia was considered as “early onset” when it was diagnosed before 34 weeks of gestation and as “late-onset” when diagnosed after a gestational age of 34 weeks. Hypertension was defined as diastolic blood pressure ≥90 mm Hg, and/or a systolic blood pressure ≥140 mm Hg, and/or use of antihypertensive medication. Metabolic syndrome was retrospectively defined according to the consensus statement from the International Diabetes Federation. According to this definition, for a woman to be defined as having metabolic syndrome, she must have central obesity (waist circumference ≥80 cm) plus any 2 of 4 additional factors; raised triglycerides (≥1.7 mmol/L), reduced high-density lipoprotein cholesterol (<1.29mmol/L or treatment for lipid abnormalities), raised blood pressure (systolic blood pressure ≥130 or diastolic blood pressure ≥85 mm Hg or treatment of previously diagnosed hypertension), or raised fasting glucose (≥5.6 mmol/L or previously diagnosed type 2 diabetes).
Selection bias: Not expected
Method of assessing the outcome appropriately: Yes, women with a history of preeclampsia or a pregnancy complicated by IUGR were selected from the Genetic Research in Isolated Populations population. If preeclampsia and IUGR co-occurred (n=8), women were categorized in the preeclampsia Group. Diagnoses were confirmed by the research physician after reviewing the medical charts. Control subjects and their parents were recruited from participants of the Erasmus Rucphen Family
Selective loss to follow up: No
Identification confounders and correction in analysis: Yes
Funding: This study was sponsored by an Erasmus University Medical Center grant and the Center for Medical Systems Biology |
|
Bhattacharya, 2011 |
Design Cohort study
N = 34 854
Country UK |
Aim of the study: to examine the relationship between hypertensive disorders of pregnancy and future hospital discharges from specified causes including cardiovascular disease, incident cancer registrations and mortality.
Inclusion criteria - From the AMND all women were identified who were born before 1968 and who were living in Aberdeen City and District at the time of their first pregnancy. -
Exclusion criteria - chronic hypertension - twins or other multiple gestations |
Determinant PE
N = 2026
PIH
N = 8891 |
Controls Normal blood pressure
N = 23 937 |
Primary outcomes:
Secundary outcomes:
Follow up: Follow up for death was 1200910 woman years |
Primary outcomes:
Table 3 shows the counts of women in each group with at least one admission of the specific type as defined by the discharge diagnosis. A woman with at least one admission for hypertension and at least one admission for cerebrovascular disease would be counted in both of the appropriate discharge diagnosis rows, as well as once in the all circulatory row.
|
Clearly defined groups: Gestational hypertension was defined as diastolic pressure > 90 mm Hg on two occasions at least four hours apart or a single reading of >110 mm Hg; from 20 weeks gestation onwards in a previously normotensive woman. Pre-eclampsia was defined as gestational hypertension plus at least one episode of proteinuria of 0.3 g/24 h. Eclampsia was defined clinically as convulsions occurring in the presence of pre-eclampsia. Women with pre-eclampsia and those with eclampsia were considered together as one group.
Selection bias: Not expected
Method of assessing the outcome appropriately: The Aberdeen Maternity and Neonatal Databank (AMND) has recorded and stored information on all pregnancy related events occurring in Aberdeen from 1950 to the present day. The Information and Services Division (ISD) of the NHS (National Health Services), Scotland linked the AMND records with details of all subsequent hospital discharges (Scottish Morbidity Record, SMR01), cancer registrations (SMR06) and death registrations (General Register Office for Scotland, GRO-S) occurring in members of the cohort. Outcomes were categorised as: hypertension (ICD-9: 401-4; ICD-10: I10-4); ischaemic heart disease (410-4, 428; I20- 5, I50); cerebrovascular disease (430-8; I60-9); kidney disease (580-99; N00-39); other circulatory disease (390-8, 405, 415-27, 440-59; I00-9, I15, I26-8, I30-49, I51-2, I70- 99), all circulatory disease (390-459; I00-I99, G45). Since we did not have an accurate date of first diagnosis, incidence rate ratios could not be calculated for the hospital discharge data. Instead we used logistic regression to calculate odds ratios for the presence of specific hospital discharges, unadjusted and adjusted for potential confounding
Selective loss to follow up: Yes, 74.8% of the women were linked to one or more of SMR01, SMR06 and GRO-S.
Identification confounders and correction in analysis: Adjustments were made for: year of birth, smoking status and social class of the women at the time of their first pregnancy. For many women, smoking behaviour at time of booking was not recorded.
Funding: Not reported
|
|
Callaway, 2007 |
Design Cohort study
N = 3639
Country: Australia |
Aim of the study: to examine the relationship between hypertensive disorders of pregnancy (HDP) and self-reported diabetes mellitus 21 years after delivery.
Inclusion criteria - women who were part of The Mater-University of Queensland Study of Pregnancy (MUSP) cohort and for whom there were data regarding diabetes mellitus in the 21 years after the index pregnancy. - received antenatal care between 1981 and 1984 at a major public hospital (Mater Misericordiae Hospital) in South Brisbane. - women delivered a live singleton baby who neither died nor was adopted before leaving hospital.
Exclusion criteria - diabetes mellitus before the index pregnancy (n=16) and gestational diabetes mellitus or type 1 diabetes mellitus that was diagnosed during the index pregnancy (n=34) |
Determinant HDP (PE)
N = 333 |
Controls No HDP
N = 3306 |
Primary outcomes: self-reported diagnosis of diabetes mellitus
Secundary outcomes:
Follow up: 21 years |
Primary outcomes:
|
Clearly defined groups: Yes. HDP (termed preeclampsia at the time) were defined as a diastolic blood pressure of >90 mm Hg on at least 2 occasions beyond 20 weeks of gestation that were associated with proteinuria and/or excessive fluid retention (defined as generalized edema that included the face and hands and excessive weight gain).
Selection bias: Possible, women were asked to complete a questionnaire providing information regarding the diagnosis of diabetes mellitus 21 years after the delivery.
Method of assessing the outcome appropriately: Yes, women were followed prospectively and completed questionnaires regarding their own physical health at their first antenatal clinic visit, peripartum, and at 21 years after delivery. At the 21-year follow-up evaluation, height and weight were self-reported. Information on diabetes mellitus was collected with a self-administered questionnaire in which women were asked “Have you EVER been told by a doctor that you have diabetes mellitus (high blood sugars)?”
Selective loss to follow up: 7173 women were eligible for this study: 3708 women were found and completed either the questionnaire or the physical assessment at 21 years. 69 of these women did not provide any information regarding the diagnosis of diabetes mellitus at the 21 year follow-up period and were excluded.
Identification confounders and correction in analysis: Yes,
Funding: L.K.C. was supported by an Australian Government National Health and Medical Research Council Postgraduate Medical Scholarship at the commencement of this work. D.A.L. is funded by a UK Department of Health Career Scientist Award. The Mater–University of Queensland Study was funded by the National Health and Medical Research Council, Queensland Health, the Centre for Accident Research and Road Safety, Queensland, and the Australian Institute of Criminology. The views expressed in this study are those of the authors and not necessarily any funding body. The authors had full access to all data, and no funding bodies influenced the analysis or interpretation of results.
|
|
Callaway, 2011 |
Design Cohort study
N = 2112
Country Australia |
Aim of the study: to assess whether the long-term follow-up, diagnosis and treatment of hypertension in these women is adequate.
Inclusion criteria - Women who were part of the Mater University of Queensland Study of Pregnancy (MUSP). These women received antenatal care at a major public hospital in south Brisbane between 1981 and 1983 and delivered a live singleton child who was not adopted before leaving hospital
Exclusion criteria - women who had hypertension documented prior to pregnancy or prior to 20 weeks gestation in the index pregnancy (n = 2)
|
Determinant HDP
N = 191 |
Controls No HDPO
N = 1921 |
Primary outcomes: Bloodpressure
Secundary outcomes:
Follow up: 21 years |
Primary outcomes: At baseline, mothers were on average 25.67 (SD 4.95) years and at 21 years follow-up they were 46.41 (SD 4.97) years old. Of 2112 mothers, 191 (9.04%) had HDP. At 21 years follow-up, the mean (SD) SBP was 116.3 (15.60) mmHg and mean DBP was 73.6 (9.75) mmHg. Overall, 1189 (56.3%) were normotensive, 581 (27.5%) were prehypertensive, and 342 (16.2%) were hypertensive. Of the 191 women who had experienced HDP, 61 (31.94%) women were normotensive, 68 (35.60%) were prehypertensive and 62 (32.46%) were hypertensive. Of the 62 women with hypertension who had experienced HDP, 29 (46.8%) were on antihypertensive therapy with adequate blood pressure control at <140 ⁄ 90 mmHg and 33 (53.2%) women had inadequately identified or managed hypertension at the time of our evaluation. The women with inadequately identified or managed hypertension included those with a BP in excess of 140 ⁄ 90 mmHg despite antihypertensive therapy (n = 13) and those on no antihypertensive therapy despite a BP in excess of 140 ⁄ 90 mmHg (n = 20). For comparison, of the 1921 women without HDP, 1128 (58.72%) women were normotensive, 280 (14.58%) were hypertensive and 513 (26.70%) had pre-hypertension. Of the 280 with hypertension, 113 (40.4%) were adequately treated and 167 (59.6%) had inadequately identified or managed hypertension at the time of our evaluation. The women with inadequately identified or managed hypertension included those with a BP in excess of 140 ⁄ 90 mmHg despite antihypertensive therapy (n = 37) and those on no antihypertensive therapy despite a BP in excess of 140 ⁄ 90 mmHg (n = 130).
|
Clearly defined groups: Yes, hypertensive disorders of pregnancy (termed pre-eclampsia at the time) were defined as a DBP over 90 mmHg on at least two occasions with new onset beyond 20 weeks gestation, and associated with proteinuria and ⁄ or excessive fluid retention (defined as generalised oedema, including the face and hands and excessive weight gain). Proteinuria was diagnosed if there was at least 2+ of protein on dipstick testing (Albustix) on at least two occasions over at least several hours. Women were classified as normotensive (systolic blood pressure (SBP) <120 mmHg and diastolic blood pressure (DBP) <80 mmHg and no blood pressure medication), pre-hypertensive (measured SBP 120– 140 mmHg andDBP 80–90 mmHg and on no blood pressure medication) and hypertensive (SBP > 140 mmHg or DBP > 90 mmHg, or currently taking blood pressure medication).
Selection bias: Possible, only women who attended a clinical visit for blood pressure and other clinical measurens at the 21 years follow-up were included.
Method of assessing the outcome appropriately: Yes
Selective loss to follow up: Of 7223 women, 2114 women attended a clinical visit for blood pressure and other clinical measurens at the 21 years follow-up. Those lost to followup were more likely to be teenagers at their delivery, to be less educated, single or cohabitating, have three or more children, use tobacco and alcohol during pregnancy and to be anxious and depressed at their first antenatal visit.8–10 When we adjusted for these co-variables, the results presented here did not change substantively suggesting that these missing data have not importantly biased the findings.
Identification confounders and correction in analysis: No
Funding: The views expressed in this study are those of the authors and not necessarily any funding body. The authors had full access to all data and no funding bodies influenced the analysis or interpretation of results. |
|
Canti, 2010 |
Design Retrospective case-control study
N = 54
Country Brazil |
Aim of the study: The purpose of this study was to determine the risk factors for CVD among women with preeclampsia and/or eclampsia during pregnancies that occurred 10 or more years earlier.
Inclusion criteria - Patients who delivered at the Gynecology and Obstetrics service of the Hospital de Clínicas de Porto Alegre (HCPA) 10 or more years before the time of the present study were selected. Patients who previously presented preeclampsia and normal pregnant women (control group) were selected according to their medical records. - Controls were women who delivered on same day at same hospital
Exclusion criteria - patients who, at delivery (10 or more years earlier), had presented signs or a diagnosis of active or previous cardiovascular disease. |
Determinant Preeclampsia
N = 40 |
Controls Normotensive pregnancies
N = 14 |
Primary outcomes: Hypertension
Secundary outcomes:
Follow up: 14.6 ± 3.1 years in the control group and 15.9 ± 3.6 years in the preeclampsia group. |
Primary outcomes: The patients’ mean ages were similar at the time of drawing up this study: 37.2 ± 3.8 years in the control group and 39.2 ± 7.7 years in the preeclampsia group. In the preeclampsia group, 15.0 % of the patients presented hypertension 10 years later, while in the control group, only 7.1 % of the patients did so.
|
Clearly defined groups: No, preeclampsia was not defined
Selection bias: Possible, number of women who were invited was not reported.
Method of assessing the outcome appropriately: All of the patients underwent laboratory tests after 12 hours of fasting
Selective loss to follow up: Invitation letters were initially sent to the selected patients. Those who came to the hospital were instructed about the study objectives, and they signed an informed consent statement. Data were collected from charts.
Identification confounders and correction in analysis: No
Funding: This project was supported by the Fundo de Incentivo à Pesquisa of the Hospital de Clínicas de Porto Alegre (HCPA), GPPG 01-106, and the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), 305660/2006-3
|
|
Carr, 2009 |
Design Retrospective cohort study
N = 31 463
Country USA |
Aim of the study: Determine whether preeclampsia is associated with developing diabetes.
Inclusion criteria - women who received care at least one year prior to delivery, delivered between 1985 and 2002, and had at least 6 weeks of subsequent postpartum care, all at Group Health. - the first pregnancy -
Exclusion criteria - women who had not received care for ≥ 1 year prior to delivery (n = 23,954), had not received care at least 6 weeks postpartum (n = 936), and had pre-existing diabetes (n = 499) or chronic hypertension (n = 154) |
Determinant Pre-eclampsia
N = 2032 |
Controls No pre-eclampsia
N = 29 431 |
Primary outcomes: DM II
Secundary outcomes:
Follow up: 8.2 – 8.5 |
Primary outcomes:
During a median of 8.2 years (interquartile range, 4.8,13.2 years) of follow-up after delivery, subsequent diabetes was diagnosed in 342 women (33 women with preeclampsia and 309 women without preeclampsia) at a median age of 38 years (interquartile range 32, 43 years). The incidence rate for subsequent diabetes was 3.97/1,000 person-years in women with a history of preeclampsia compared to 2.21/1,000 person-years in women without prior preeclampsia (p = 0.003). The Cox model yielded an unadjustedHR of 1.98, 95%CI 1.38, 2.83 for the association between preeclampsia and subsequent diabetes. The risk of developing diabetes remained elevated after adjusting for age, primigravida status, and gestational diabetes (adjusted HR 1.82; 95%CI 1.26, 2.62).
|
Clearly defined groups: Yes, preeclampsia during the index pregnancy was classified as one occurrence of any of the following ICD-9 codes assigned during outpatient or inpatient visits associated with the pregnancy: ICD-9 642.4-642.5 (preeclampsia), 642.6 (eclampsia), or 646.8 (Hemolysis Elevated Liver enzymes Low Platelets, HELLP, syndrome).
Selection bias: Not expected
Method of assessing the outcome appropriately: Inpatient and outpatient automated data were reviewed for the following ICD-9 codes: 250.x0 and 250.x2 (type 2 diabetes) without or with complications (ICD-9 codes 250.2 – 250.9). Laboratory records were evaluated for plasma glucose levels that met the criteria for diabetes on two separate occasions: fasting plasma glucose ≥ 7.0 mmol/l (126 mg/dl) or random plasma glucose ≥ 11.1 mmol/l (200 mg/dl) Data were collected from pharmacy records of dispensed prescriptions for the following medications used to treat diabetes: metformin, sulfonylureas, hiazolidinediones, acarbose, miglitol, nateglinide, repaglinide, and insulin.
Selective loss to follow up: No
Identification confounders and correction in analysis: Yes, multivariate models included age at delivery as a continuous variable, primigravida status, and gestational diabetes.
Funding: This work was supported by the Washington State Obstetrical Association, the National Institutes of Health Grants K23RR16066 and K30RR022293 from the National Center for Research Resources, and the Department of Veterans Affairs.
|
|
Cassidy, 2009 |
Design Cohort study
N = 498
Country USA |
Aim of the study: whether a self-reported history of HDP, using a validated survey, is associated with the presence and extent of coronary artery calcification (CAC) in 498 non-Hispanic white women participating in the Epidemiology of Coronary Artery Calcification (ECAC) Study, a community-based study in Rochester, Minnesota.
Inclusion criteria - women participated in the the Rochester Family Heart Study (RFHS), conducted between 1984 and 1991, identified households where _2 children were enrolled in Rochester, Minnesota, schools. - The ECAC Study, conducted between 1991 and 1998, examined 533 women ≥20 years of age from the RFHS and 334 women ≥20 years of age living in the vicinity of Rochester, who were not pregnant or lactating and never had coronary or noncoronary heart surgery. - Questions on reproductive history pertaining to HDP were asked of the 574 (316 RFHS and 258 non-RFHS) women participating in the follow-up ECAC examination conducted between December 2000 and February 2005. The present study is limited to this follow-up examination.
Exclusion criteria Twenty-nine women with prevalent CHD (defined as self-reported history of myocardial infarction [MI], stroke, or a positive angiogram), 10 missing risk factor information, 1 who had kidney transplantation, and 25 without a pregnancy lasting >6 months |
Determinant HDP
N = 52 |
Controls No reported HDP
N = 446 |
Primary outcomes: CAC
Secundary outcomes:
Follow up: 27 years |
Primary outcomes:
|
Clearly defined groups: Self-reported history of preeclampsia, eclampsia, and toxemia was obtained. Women were considered hypertensive if they reported a prior diagnosis of hypertension and use of prescription BP-lowering medication or if average SBP or DBP was ≥140mm Hg or ≥90mm Hg. Participants were considered diabetic if they reported using insulin or oral hypoglycemic agents or if they reported a physician diagnosis of diabetes.
Selection bias: Not expected
Method of assessing the outcome appropriately: A total of 563 non-Hispanic white women with information on reproductive history had electron beam computed tomography (EBCT) examinations to measure the presence and extent of CAC.
Selective loss to follow up: Not reported
Identification confounders and correction in analysis: Yes, relation with CAC adjusted for age, bMI, waist/hip ratio, SBP, DBP, ln(SCr), ln(UACR), diabetes status, menopause status, and BP-lowering medication use
Funding: This research was supported by grant R01 HL46292 from the NIH, by a General Clinic Research Center grant from the NIH (M01RR00585) awarded to Mayo Clinic Rochester, and by grant K23 DK078229 from the NIH (A.D.R.).
|
|
Drost, 2012 E J Prev Cardiol |
Design Case-control study
N = 673
Country Netherlands |
Aim of the study: To investigate the prevalence of cardiovascular risk factors in women at 10 years post preeclampsia in comparison with a reference group.
Inclusion criteria - Pregnant women who have been registered in a database since 1991 at the Department of Obstetrics at the Isala Klinieken in Zwolle, The Netherlands - Period 1991-2007
Exclusion criteria - Pregnant or lactating Women (n=10) |
Determinant Early pre-eclampsia
N = 339 |
Controls Uncomplicated preganncy
N = 332 |
Primary outcomes: Cardiovascular risk factors
Secundary outcomes:
Follow up: 10 |
Primary outcomes:
|
Clearly defined groups: Early preeclampsia was defined (according to the ISSHP as an elevated diastolic blood pressure ≥90mmHg with proteinuria (≥0.3 g/24 h) between 20 and 32 weeks of gestation during index pregnancy.
Selection bias: Possible, not all women with early pre-eclampisa responded on invitation.
Method of assessing the outcome appropriately: Yes, they invited all women registered on the early preeclampsia database as well as an equal number of age-matched females without preeclampsia from the regular obstetric database in the same time period (1991–2007) to participate in the Preeclampsia Risk EValuation in FEMales (PREVFEM) study. Participants were asked to fill in a questionnaire, a physical examination was performed by trained vascular nurses and fasting blood and urine samples were collected. Cardiovascular risk factors were defined as follows: hypertension as a systolic blood pressure (SBP) ≥140 mmHg, a diastolic blood pressure (DBP) ≥90mmHg or use of antihypertensive medication. The presence of DM was defined as diagnosed DM with treatment (diet or medication) or fasting glucose ≥7.0 mmol/l and hypercholesterolaemia was defined as total cholesterol ≥5.0 mmol/l or current use of statins. The metabolic syndrome (MetS) is defined according to the ATP III criteria
Selective loss to follow up: A total of 339 out of 515 invited women (response rate 64%) were willing to participate and 332 of 810 non-exposed women (response rate 41%) served as a reference group
Identification confounders and correction in analysis: Yes, adjustment for age, years post index partus and current smoking
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. |
|
Edlow, 2009 |
Design prospective case-control study
N = 219
Country USA |
Aim of the study: whether a pregnancy complicated by preeclampsia is associated with an increased prevalence of maternal hypertension and other cardiovascular risk factors shortly after delivery.
Inclusion criteria - period March 2005 and August 2007 - women with PE and PIH
Exclusion criteria - Patients who had not received medical care after their postpartum visit to have their blood pressure measured |
Determinant PE/PIH ≤34 wks
N = 79 |
Controls No PE/PIH
N = 140 |
Primary outcomes: Hypertension, diabetes, dyslpidemia
Secundary outcomes:
Follow up:
|
Primary outcomes:
Of the 79 cases, 17 (21.5%) had preterm preeclampsia.
|
Clearly defined groups: Yes, preeclampsia was defined as blood pressure ≥ 140/90 mm Hg on 2 measurements ≥ 6 hours apart or ≥160/105 mm Hg, and proteinuria. Those women who met criteria for blood pressure but not proteinuria were also included
Selection bias: Not expected
Method of assessing the outcome appropriately: Yes, the presence of hypertension and other cardiovascular risk in cases and controls was assessed through telephone interviews 6-13 months after delivery. All telephone interviews were conducted by the primary author (A.G.E.) with a standardized script.
Selective loss to follow up: One hundred twenty-four cases and 279 controls were enrolled in the PMC study between January 2006 and October 2006. At the time of initial enrollment, 9% (11) of cases and 14% (40) of controls declined participation in this follow- up study. The total number of patients eligible for the follow-up assessment of cardiovascular risk included 113 cases and 239 controls. Of the patients eligible, 79 cases (70%) and 140 controls (59%) completed the follow-up study. The primary reasons that patients were not reached included: (1) disconnected or changed phone number (59% [20/34] of cases and 53% [52/99] of controls); (2) no answer or unreturned messages (41% [14/34] of cases and 43% [43/99] of controls); and (3) patients who declined participation at time of the follow-up phone interview (3% [3/99] of controls).
Identification confounders and correction in analysis: Yes, confounders including race (African American vs other), BMI, parity, and chronic hypertension
Funding: Support was provided through a FOCUS Medical Student Fellowship in Women’s Health supported by the Edna G. Kynett Memorial Foundation.
|
|
Epstein 1964 |
Design Case-control study
N = 162
Country USA |
Aim of the study: Long-term follow-up observation of toxemic pregnancies
Inclusion criteria - women delivered on the obstetric service of the Grace-New Haven Community Hospital from 1945-1948 - Diagnosis of toxaemia - Controls were selected from women of the same age and racial background living in teh same community, who had been pregnant at the same time and delivered in the same hospital but had not had hypertension, proteinuria or edema during the pregnancy
Exclusion criteria - episode of toxaemia did not conform to the criteria - records were inadequate - blood pressure before the midpoint of pregnancy was not known - negroes - hypertension was known or suspected before pregnancy
|
Determinant PE
N = 48 |
Controls No hypertension, proteinuria or edema
N = 114 |
Primary outcomes: Hypertension
Secundary outcomes:
Follow up: 15 years |
Primary outcomes:
|
Clearly defined groups: Toxemia was defined as hypertension, pronteinuria and edema in the last trimester
Selection bias: Not expected
Method of assessing the outcome appropriately: Women were re-examined an average of fifteen years after an episode of toxaemia. The blood pressure was taken several times in the sitting and reclining position. The lowest blood pressure recorded was considered to be the true blood pressure. Hypertension was defined as blood pressure >150/90 mmHg
Selective loss to follow up: No
Identification confounders and correction in analysis: No
Funding: Yes, well described
|
|
Engeland, 2011 |
Design Cohort study
N = 226 832
Country Norway |
Aim of the study: To use the population-based Norwegian Prescription Database (NorPD) to explore later development of diabetes in women registered with GDM and/or preeclampsia in Medical Birth Registry of Norway (MBRN) during 2004–8.
Inclusion criteria - women with pregnancies registered in MBRN during 2004–8, lasting more than 22 weeks - first pregnancy -
Exclusion criteria - abortions - diabetes, polycystic ovary syndrome (PCOS) or chronic hypertension before pregnancy - women received drugs used to treat diabetes |
Determinant PE
N = 8832 |
Controls No PE
N = 215 988 |
Primary outcomes: Prescription of anti-diabetics
Secundary outcomes:
Follow up: 3.7 years |
Primary outcomes:
Women with severe preeclampsia (33% of the preeclamptic pregnancies) had a higher risk of receiving prescription of drugs used to treat diabetes than other women with preeclampsia (RR 1.6, 95% CI 1.2–2.1). |
Clearly defined groups: The diagnostic criteria for preeclampsia in Norway have been blood pressure ≥ 140/90 after 20 weeks of gestation, combined with proteinuria ≥0.3 g/24 h) (≥+1 dipsticks) on at least two occasions
Selection bias: Not expected
Method of assessing the outcome appropriately: Maternal diseases, before and during pregnancy are coded by the staff at the MBRN using International Classification of Diseases (ICD) revision 10. Prescriptions of drugs used to treat diabetes (ATC code A10) were used as proxy for diabetes.
Selective loss to follow up: No
Identification confounders and correction in analysis: Adjustment for maternal age, and for parity
Funding: Not reported
|
|
Freibert, 2011 |
Design Cohort study
N = 3909
Country USA |
Aim of the study: To investigate the association between a prior history of pregnancy complications and cardiovascular disease (CVD) among Kentucky women aged ≥50 years.
Inclusion criteria - data from the 2006– 2008 Kentucky Women’s Health Registry (KWHR). - women aged ≥50
Exclusion criteria - inconsistent or incomplete data
|
Determinant HDP
N = 222
Preterm birth
N = 324
|
Controls Pregnancy without complications
N = 2558 |
Primary outcomes: self-reported prevalence of CVD, including angina, heart attack, heart failure, and arrhythmia.
Secundary outcomes:
Follow up: Not reported |
Primary outcomes:
|
Clearly defined groups: Definitions of the pregnancy complications in the survey were as follows: ‘‘preterm labor defined as contractions and changes in your cervix between your 20th and 36th week of pregnancy, may lead to preterm birth; preeclampsia defined as high blood pressure during pregnancy; gestational diabetes defined as high blood sugar during pregnancy.’’
Selection bias: Possible, only women with nonfatal CVD were included.
Method of assessing the outcome appropriately: To assess history of pregnancy complications, the survey asked: During your pregnancies, did you experience any of the following (CHOOSE ALL THAT APPLY): preterm labor, preeclampsia, gestational diabetes, bleeding during third trimester, none, and Choose not to answer. CVD was ascertained via self-report using the question: Have you ever had any of the following? CHOOSE ALL THAT APPLY: angina, heart attack, heart failure, irregular heart beat or arrhythmia, mitral valve prolapsed, rheumatic fever, heart murmur, aortic aneurysm, peripheral vascular disease or claudication, congenital (present at birth) heart disease, other.
Selective loss to follow up: No
Identification confounders and correction in analysis: No
Funding: Not reported
|
|
Funai, 2005 |
Design Cohort study
N = 37 061
Country Israel |
Aim of the study: to investigate the longterm risk of mortality in women with preeclampsia, focusing on those known to be subsequently normotensive.
Inclusion criteria - women participating in The Jerusalem Perinatal Study (a population-based research cohort derived from births in 1964–1976).
Exclusion criteria - Pre-existing hypertension and other rare diagnoses (such as renal or autoimmune disease) - missing data |
Determinant PE
N = 1070 |
Controls No PE
N = 35 991 |
Primary outcomes: Cause of dead
Secundary outcomes:
Follow up: 30 years (range, 24.5–36.5) |
Primary outcomes: There were 1070 women (2.9%) with preeclampsia. For 479 of these, we observed one or more subsequent births without preeclampsia; we classified these women as normotensive after preeclampsia. The remaining 591 women are classified as unknown with regard to subsequent normotensive status; this group is composed of women for whom we observed no further births in 1964–1976 (n = 538) and women whose subsequent pregnancies were also complicated by preeclampsia (n = 53).
|
Clearly defined groups: Yes, preeclampsia is defined as a systolic blood pressure ≥140 mmHg or a diastolic pressure ≥90 mmHg, or both, together with 1+ or more proteinuria and edema.
Selection bias: Not expected
Method of assessing the outcome appropriately: Causes of death, coded according to International Classification of Diseases-9,
Selective loss to follow up: Follow-up is complete through 30 June 2000, at which time we had successfully traced 92% of women.
Identification confounders and correction in analysis: Adjusted, where appropriate, for age, insulin-dependent diabetes, gestational diabetes, birth of infant(s) weighing <2500 g, education, social class and year of baseline birth
Funding: Supported by grants from the National Institutes of Health (1 K23 RR15536– 04) (to E.F.F.); 1R01 CA80197 (to S.H.)
|
|
Garovic, 2010 |
Design Cohort study
N = 4782
Country USA
|
Aim of the study: to assess the role of hypertension in pregnancy as an independent risk factor for hypertension, coronary heart disease (CHD), and stroke later in life.
Inclusion criteria - women participating in the Phase 2 (2000-2004) Family Blood Pressure Program study with at least one pregnancy that lasted more than 6 months
Exclusion criteria
|
Determinant HDP
N = 643 |
Controls Normotensive pregnancy
N = 3421 |
Primary outcomes: HT, CHD and stroke
Secundary outcomes:
Follow up: Not reported |
Primary outcomes: Women reporting hypertension in pregnancy compared with those with no history of hypertension in pregnancy had increased unadjusted risks for hypertension diagnosed after the age of 40 (50% hypertensive at the age 52 vs. 60, P <0.001), CHD (14% estimated event rate vs. 11% at 70 years, P = 0.049), and stroke (8% estimated event rate vs. 5% at 70 years, P = 0.009). Similarly, women reporting preeclampsia in pregnancy, compared with those with no history of hypertension in pregnancy, had increased unadjusted risks for hypertension diagnosed after the age of 40 (50% hypertensive at the age 54 vs. 60, P <0.001), CHD (14% estimated event rate vs. 11% at 70 years, P = 0.045), and stroke (24% estimated event rate vs. 5% at 70 years, P <0.001). Women with a history of hypertension in pregnancy and those with a history of preeclampsia, when grouped together and compared with women with a history of normotensive pregnancies, were at increased risks for the subsequent diagnoses of hypertension (50% hypertensive at the age 53 vs. 60, P <0.001), CHD (14% estimated event rate vs. 11%, P = 0.009), and stroke (12% estimated event rate vs. 5%, P <0.001).
|
Clearly defined groups: HDP was defined as whether or not they had developed hypertension during any of the pregnancies that have lasted more than 6 months.
Selection bias: Not expected
Method of assessing the outcome appropriately: Family Blood Pressure Program study (FBPP) was established in 1995 to investigate the genetics of hypertension in non-Hispanic blacks, Hispanic whites, Asians, and non-Hispanic whites. Questionnaires were administered in personal interviews by trained examiners. the diagnosis of hypertension was confirmed if a prior diagnosis of hypertension and use of prescription antihypertensive medication had been reported or if the average systolic or diastolic BPs were at least 140 or at least 90 mmHg, respectively. The diagnosis of CHD was established by self-reports of a previous history of myocardial infarction, coronary bypass surgery, coronary angioplasty, balloon dilatation or stent placement, whereas the diagnosis of cerebrovascular disease was based on self-reports of stroke and/or cerebral hemorrhage. Diabetes mellitus was self-reported. The diagnosis of dyslipidemia was confirmed if one or more of the following criteria were met: use of lipidlowering drugs or laboratory measurements at the Phase 2 examination revealing a total cholesterol 200 mg/dl or more, triglycerides 150 mg/dl or more, or high-density lipoprotein (HDL) 40 mg/dl or less. Blood was drawn by venipuncture after an overnight fast of at least 8 h.
Selective loss to follow up: No
Identification confounders and correction in analysis: Yes
Funding: The study was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (K08HD051714), and the National Heart, Lung, and Blood Institute, National Institutes of Health (U01HL054481, U01HL054471, U01HL054512, and U01HL054498).
|
|
Gaugler, 2008 |
Design Case-control study
N =40
Country Netherlands |
Aim of the study: To study subsequent pregnancy outcome in women with severe, very early onset preeclampsia (onset before 24 weeks’ gestation) and to analyze cardiovascular risk profiles of these women and their partners.
Inclusion criteria - women with preeclampsia with an onset before 24 weeks’ gestation, admitted between 1 January 1993 and 31 December 2002 at a tertiary university referral center - Healthy control patients after uncomplicated term pregnancies only, with healthy, appropriate for gestational age weight babies, matched for age, parity, race and year of delivery were selected by the computerized hospital database.
Exclusion criteria
|
Determinant Preeclampsia with an onset before 24 weeks
N = 20 |
Controls Uncomplicated pregnancies matched for age and parity
N = 20 |
Primary outcomes: Body weight, height, waist and hip circumference, blood pressure and intima media thickness (IMT)
Secundary outcomes:
Follow up: 5.5 years (range 4–10 years) after index pregnancy |
Primary outcomes:
|
Clearly defined groups: Severe preeclampsia was defined as an absolute diastolic blood pressure of ≥110 mmHgand proteinuria (≥2 + [1 g/L]) on a catheterized specimen on admission, or the occurrence of preeclampsia (blood pressure ≥140 mmHg systolic or ≥90 mmHg diastolic measured on at least two occasions in women normotensive before 20 weeks’ gestation and proteinuria ≥300 mg/24 h (or ≥2+ on dipstick of voided specimen) in combination with eclampsia or HELLP syndrome. Gestational hypertension was defined as a blood pressure of ≥140/90 mmHg after 20 weeks’ gestational age in formerly normotensive women, measured on two separate occasions with an interval of at least 4 h.
Selection bias: Not expected
Method of assessing the outcome appropriately: All participants were invited for examination at our hospital. Body weight, height, waist and hip circumference, blood pressure and intima media thickness (IMT) of the common carotid artery were measured. Fasted blood samples were drawn for detection of metabolic cardiovascular risk factors. Hypertension was defined as a systolic blood pressure ≥140 mm Hg and/or a diastolic blood pressure ≥90 mmHg and/or use of anti-hypertensive medication.
Selective loss to follow up: Twenty women (80%) consented to participation. Therewas 1 maternal death. Four women refrained from participation because of psycho-emotional distress due to traumatic memories of their hospital admission and poor perinatal outcomes, as all experienced intrauterine foetal death. One patient declined participation because of language difficulties.
Identification confounders and correction in analysis: No
Funding: This study was financially supported by a grant of the Dutch Society of Obstetrics and Gynaecology.
|
|
Hannaford, 1997 |
Design Prospective cohort study
N = 214 356 women-years of observation
Country UK |
Aim of the study: To determine whether the rate of cardiovascular disease is different among parous women with a general practitioner reported history of toxaemia of pregnancy than among those not reported to have experienced toxaemia, or among nuliparous women.
Inclusion criteria - Women who had never used oral contraceptives who were recruited to the Royal College of General Practitioners' oral contraception study - women who had never used oral contraceptives.
Exclusion criteria
|
Determinant Toxemia
N = 3000 (according to Brown)
28055 women-years |
Controls No toxemia
N = 18451 (according to Brown)
163 010 wome-years |
Primary outcomes: CVD, HT ICD codes
Secundary outcomes:
Follow up: 13 (0-25)
|
Primary outcomes:
|
Clearly defined groups: No, definition of toxaemia not clear
Selection bias: Not expected
Method of assessing the outcome appropriately: At regular intervals the general practitioners have supplied details of any hormonal preparations prescribed, all reported new episodes of illness, any operations, any pregnancies and their outcome, and when appropriate the date and cause of eath. First ever diagnosis rates of hypertensive disease (International Classification of Disease (ICD), 8th revision, codes 400 to 404), acute myocardial infarction (ICD code 410), other acute ischaemic heart disease (411), other chronic ischaemic heart disease (412), angina pectoris (413), total ischaemic heart disease (410-413), total cerebrovascular disease (430-438), total peripheral vascular disease (440-442, 4439), and total venous thromboembolic disease (450, 453) were calculated for each group.
Selective loss to follow up: Yes, described.
Identification confounders and correction in analysis: age at diagnosis, smoking, and social class at recruitment.
Funding: The oral contraception study currently receives financial support from the Royal College of General Practitioners, Schering AG, Schering Healthcare, and Wyeth-Ayerst International.
|
|
Haukkamaa, 2009 |
Design Cohort study
N = 767
Country Finland |
Aim of the study: To examine whether women with a history of pre-eclampsia more often show signs of atherosclerosis compared with 2 control groups.
Inclusion criteria - women from a large Finnish cross-sectional health examination survey (Health 2000 survey) carried out in 2000–2001.
Exclusion criteria - gestational diabetes - essential hypertension - proteinuria |
Determinant women with previous pre-eclampsia (n = 35) or pregnancy-induced hypertension (n = 61)
|
Controls healthy women who had had at least 1 childbirth (healthy parous controls, n = 489) and nulliparous controls (n = 182).
|
Primary outcomes: IMT, lipids, hypertension, CAD
Secundary outcomes:
Follow up: Not reported |
Primary outcomes:
|
Clearly defined groups: Yes, PE was defined as BP ≥ 140/90 mm Hg and proteinuria 1 stick + and/or ≥0.3 g/24 h specimen after 20 gestational weeks. Pregnancy-induced hypertension was defined as hypertension (BP ≥140/90 mm Hg) after 20 gestational weeks without proteinuria. (ICD-codes) Healthy parous controls were defined as women who had had at least 1 childbirth and no gestational diabetes, PE, hypertension or proteinuria before or during any of their pregnancies. Nulliparous controls were defined as women who had never been pregnant
Selection bias: Not expected
Method of assessing the outcome appropriately: Information on reproductive history, chronic diseases and smoking was obtained at the home health interview. Fasting blood samples were used. Hypertension and CAD diagnoses were obtained at the home health interview.
Selective loss to follow up: No
Identification confounders and correction in analysis: No
Funding: Not reported
|
|
Irgens, 2001 |
Design Cohort study
N = 626 272 births
Country Norway |
Aim of the study: To assess whether mothers and fathers have a higher long term risk of death, particularly from cardiovascular disease and cancer, after the mother has had preeclampsia.
Inclusion criteria - mothers' first deliveries, recorded in the Norwegian medical birth registry from 1967 to 1992.
Exclusion criteria
|
Determinant PE ≥ 37 weeks
N = 21 506
PE 16-36 weeks
N = 2649 |
Controls No PE ≥ 37 weeks
N = 576 099 |
Primary outcomes: Total mortality and mortality from cardiovascular causes, cancer, and stroke
Secundary outcomes:
Follow up: Median 13 years (0-25) |
Primary outcomes:
|
Clearly defined groups: Preeclampsia was defined as cases of pregnancies with a specified diagnosis of preeclampsia and all pregnancies in which both hypertension induced by pregnancy and proteinuria were recorded.
Selection bias: No
Method of assessing the outcome appropriately: Data on the cohorts were derived from the medical birth registry of Norway, which comprises all births in Norway since 1967 with more than 16 weeks of gestation and from the registry of causes of death. We defined cardiovascular mortality as all deaths in which the cause was registered as being related to the heart. This included codes 410 to 429 of ICD8 and ICD9 (international classification of diseases, 8th and 9th revisions).
Selective loss to follow up: No
Identification confounders and correction in analysis: Yes, adjustment for mother's age at delivery and year of birth of the baby.
Funding: Helse og Rehabilitering
|
|
Jonsdottir, 1995 |
Design Cohort study
N = ?
Country Iceland |
Aim of the study: To investigate the potential association between hypertension in pregnancy, preeclampsia and eclampsia with increased death rates from ischemic heart disease (IHD)
Inclusion criteria - women giving birth at the National Hospital in Reykjavik during 1931-1947
Exclusion criteria - women with pre-existing renal or hypertensive disease
|
Determinant HDP
N = 307 |
Controls General population
N = ? |
Primary outcomes: IHD (ICD)
Secundary outcomes:
Follow up: 41.9 years (1-60) |
Primary outcomes: During 1956-90 139 women died: a slightly higher proportion than expected (n=116.3) in the general population for the same period (RR 1.20; 95% CI 1.01-1.42). IHD was documented on death certificates in 39 women compared to 26.5 expected in the population (RR=1.47; 95% CI 1.05-2.02). The relative risk of dying from IHD was significantly higher among eclamptic women (RR=2.61; 95% CI 1.11-6.12) and those with eclampsia (RR=1.9; 95% CI 1.02-3.52) than among those who only had hypertension.
|
Clearly defined groups: Yes, hypertension in pregnancy was defined as blood pressure ≥140/90 mmHg after 20 weeks gestation. Preeclampsia was defined as hypertension and proteinuria ≥0.3 gr/L and eclampsia as seizure in hypertensive pregnancy.
Selection bias: Not expected
Method of assessing the outcome appropriately: The expected total mortality and IHD mortality in the study group was compared to corresponding population data from the Statistical Bureau, public health an census reports in Iceland for the years 1956-90.
Selective loss to follow up: Of 374 women, 67 were loss to follow-up: 2 couldn’t be traced, in 6 cases death certificates could not be obtained, 31 had died before 1956. Information on the health of those alive was obtained in all but 30 cases (refused participation = 22, not traceable=2, moved abroad but registered alive = 6.
Identification confounders and correction in analysis: No
Funding: This study was supported by the Icelandic Heart Association Research Fund an the National University Hospital Research Fund.
|
|
Kharazmi 2007 |
Design Cohort study
N = 3470
Country Finland |
Aim of the study: to identify associations between pregnancy-related factors and Isolated systolic hypertension (ISH).
Inclusion criteria - women participating in the Health 2000 Survey carried out in 2000–2001. - blood pressure data available
Exclusion criteria
|
Determinant ISH
N = 527 |
Controls No ISH
N = 2438 |
Primary outcomes: HT
Secundary outcomes:
Follow up:
|
Primary outcomes:
|
Clearly defined groups: Yes, however no definition of toxaemia.
Selection bias: Possible, recall bias.
Method of assessing the outcome appropriately: Pregnancy-related factors were assessed by questionnaire and the definition used for ISH was systolic blood pressure ≥140 mmHg and diastolic blood pressure >90 mmHg.
Selective loss to follow up: Of 3937 subjects, whose data were used for this study, 98.3% responded to the extensive primary home interviewer-administered questionnaire
Identification confounders and correction in analysis: Age
Funding: Not reported
|
|
Kestenbaum 2003 |
Design Cohort study
N = 124,141
Country USA |
Aim of the study: To estimate the risks for cardiovascular and thromboembolic events in women with pregnancy-related hypertension.
Inclusion criteria - birth records from BERD from 1987 to 1998 - controls: A sample of control mothers without hypertension during pregnancy was randomly selected from live singleton births in BERD. Approximately 4 control mothers were matched to each hypertensive mother by age, parity, and calendar year of delivery
Exclusion criteria - women with preexisting cardiac or renal disease established diabetes, or age older than 45 or younger than 15 Years - Cases in which ICD-9-CM hospital discharge codes did not link to the delivery, were missing, or coded for “unspecified hypertension” - preexisting hypertension |
Determinant PIH
N = 10,687
Mild PE
N = 15,508
Severe PE
N = 5044 |
Controls Nonhypertensive pregnancy
N = 92,902 |
Primary outcomes: CVD
Secundary outcomes:
Follow up: 7.8 years (intraquartile range, 4.8, 7.6, and 10.6 years |
Primary outcomes:
Mean maternal age at the time of a first cardiovascular event was 36.1 years (intraquartile range, 30.7, 36.8, and 42.0 years). Among women who developed cardiovascular events, mean time between the index pregnancy and first cardiovascular event was 5.1 years (intraquartile range, 2.0, 4.7, and 7.9 years).
|
Clearly defined groups: Potential cases of pregnancyrelated hypertension were screened on the basis of having an ICD-9-CM code for hypertension during pregnancy (ICD-9-CM codes 642.x) or a positive response on the birth certificate to the items “pregnancy induced hypertension,” “chronic hypertension,” or “eclampsia.”
Selection bias: Not expected
Method of assessing the outcome appropriately: Data were obtained from all live singleton births recorded in the Washington State Birth Events Record Database (BERD), which links birth hospitalization records with state birth certificate data. Maternal birth hospitalizations were linked to subsequent hospitalizations recorded in the Comprehensive Hospital Abstract Reporting System (CHARS) database. Cardiovascular events are defined as hospitalizations for acute myocardial infarction (ICD-9-CM code 410.x), acute stroke (ICD-9-CM codes 430.x, 431.x, 434.x, 436.x), or coronary artery revascularization procedure, including coronary artery bypass grafting (ICD-9 procedure codes 36.x).20-22 Because of their low sensitivity and specificity for predicting stroke, ICD-9-CM codes 432, 433, and 435 were not used. Thromboembolic events are defined as hospitalizations for deep venous thrombosis (ICD-9-CM code 451.1 or 453.x) or pulmonary embolism (ICD-9-CM code 415.1). For mothers with multiple outcomes, the first outcome was retained for analysis
Selective loss to follow up: No
Identification confounders and correction in analysis: Age, parity, race/ethnicity, gestational diabetes, smoking, cesarean section and type of insurance used for the index pregnancy
Funding: Not reported
|
|
Lazdam 2012 |
Design Case-control study
N = 140
Country UK |
Aim of the study: whether those who develop early onset disease have unique adverse blood pressure characteristics.
Inclusion criteria - all women discharged from the Oxford Maternity Unit between 1998 and 2003, with an ICD, 10th Revision, preeclampsia coding. - ISSHP criteria for preeclampsia - Controls: for every participant, potential controls were identified, with equivalent age and parity giving birth at the Oxford Maternity Unit in same year.
Exclusion criteria - women with hypertension, diabetes mellitus, renal impairment, polycystic ovary syndrome, or inflammatory disease at pregnancy |
Determinant Early onset PE
N = 45
Late onset PE
N = 45 |
Controls Uncomplicated pregnancy
N = 50 |
Primary outcomes: Hypertension
Secundary outcomes:
Follow up: 9.75 years (6–13 years) |
Primary outcomes: At 6 weeks postpartum, SBP and DBP were higher in the early onset preeclampsia group with DBPs unchanged to those at hospital discharge and significantly higher than those with late-onset preeclampsia (86.25 ± 13.46 versus 75.00 ± 5.00 mm Hg, p=0.04). In the late-onset group, by 6 weeks, both SBP and DBP had returned to levels seen at hospital discharge in those with a normotensive pregnancy (SBP 119.00 ± 10.25 versus 119.25 ± 13.27 mm Hg, P=0.97; DBP 75.00 ± 5.50 versus 74.70 ± 7.74 mm Hg, P=0.93). Six to 13 years postpartum women from both preeclampsia groups had higher SBP and DBP (Table S2). These differences remained significant after excluding women with diagnosed hypertension (P ≤0.05).
|
Clearly defined groups: Yes, preeclampsia according to ISSHP criteria. Controls women were not contacted if there was evidence of raised BP or proteinuria (>1+) during any pregnancy or delivery of a small-for-gestational-age infant during the index pregnancy (birthweight <10th centile).
Selection bias: Not expected
Method of assessing the outcome appropriately: Mothers attended a research clinic in the morning after a 12-hour fast and were assessed by investigators blinded to maternity data
Selective loss to follow up: Of 309 invited women, 90 agreed to participate
Identification confounders and correction in analysis: No
Funding: This study was funded by grants from the National Institute for Health Research Oxford Biomedical Research Centre and Oxford British Heart Foundation Centre of Research Excellence. Dr Lazdam was supported by the Oxford Health Services Research Committee, Dr Leeson by the British Heart Foundation, and A. Shore by the Peninsula National Institute for Health Research Clinical Research Facility.
|
|
Libby 2006 |
Design Cohort study
N = 7178
Country UK |
Aim of the study: whether there is a relationship between pre-eclampsia and the development of type 2 diabetes in mothers and their babies and how this is affected by infant birthweight.
Inclusion criteria - Mothers with at least one pregnancy recorded on Walker database 1952–1958 - Mothers resident in Tayside 2003 or died in Tayside 1993–2003
Exclusion criteria - Diabetic status not known - type 1 diabetes |
Determinant PE
N = 810 |
Controls No PE
N = 6377 |
Primary outcomes: DM II
Secundary outcomes:
Follow up: 46 year |
Primary outcomes:
|
Clearly defined groups: Pre-eclampsia was defined as a rise in diastolic blood pressure after the 26th week of pregnancy to ≥90 mmHg on two or more occasions separated by at least 1 day, together with confirmed albuminuria. The outcome of type 2 diabetes was defined according to WHO criteria and was confirmed by manual validation of case records of all diabetic patients in Tayside.
Selection bias: No
Method of assessing the outcome appropriately: data from the Walker database were linked to data from the Diabetes Audit and Research Tayside (DARTS) and Medicines Monitoring Unit (MEMO) collaboration, which includes a series of databases of health outcomes that are record-linked by the CHNo. Mothers who died between 1980 and 1993 were identified as diabetic if they had had more than one prescription for insulin or oral hypoglycaemic medication (British National Formulary Chapter 6.1.1 and 6.1.2) and/or had had at least one hospital admission for type 2 diabetes (International Classification of Diseases [ICD]9 Code 250 or ICD10 Codes E10 or E11).
Selective loss to follow up: No
Identification confounders and correction in analysis: Yes, adjustment for Quintiles of offspring birthweight, age and deprivation
Funding: The Walker project was funded by the medical charity, Tenovus Tayside.
|
|
Lin 2011 |
Design Cohort study
N = 1 132 064
Country Taiwan |
Aim of the study: The present study provides the incidence of major adverse cardiovascular events (MACE) in Taiwanese women for 1999 to 2003 based on birth certificate data linked with National Health Insurance (NHI) claims data to determine risk of MACEs in women from pregnancy to the third postpartum year.
Inclusion criteria - birth records for 1999 to 2003 for which the birth certificate dataset and delivery entries in the NHI hospital discharge data were successfully linked
Exclusion criteria - extreme values of maternal age (≤15 or ≥50 years old), infant’s birth weight (≤600 or ≥6,000 g), gestational weeks (≤19 or ≥45), and parity (≥11) |
Determinant PE/eclampsia
N =
|
Controls No PE/eclampsia
N = |
Primary outcomes: Cardiovascular events
Secundary outcomes:
Follow up: Third trimester of pregnancy till at least the third year postpartum |
Primary outcomes:
|
Clearly defined groups: pre-eclampsia/eclampsia, which was defined by ICD-9-CM codes 642.4 to 642.7 as the secondary diagnosis in the index discharge of delivery.
Selection bias: Not expected
Method of assessing the outcome appropriately: Data for this study were obtained from 3 main sources. The first source was birth registries from 1999 to 2003 provided by the ministry of the interior. This dataset contains comprehensive information about birth and parents’ data. The second source was the NHI hospital discharge data covering 1996 to 2004, a nationwide population-based data. including 21 million enrollees, representing about 97% of the Taiwanese population. It provided inpatient registries from all medical facilities contracted with the NHI and contained information on all admissions including newonset MACEs in peripartum women and all deliveries with 1 principal and 4 secondary International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes. The third source was death files from 1996 to 2004 that provide the incidence of death and cause of death. Cases of MACE were further classified as MI (ICD-9-CM code 410-410.9), heart failure (ICD-9-CM codes 428.0 to 428.10), percutaneous cardiac Determinant (ICD-9-CM codes 36.0 to 36.03, 36.05 to 36.09), coronary artery bypass grafting (ICD-9-CM codes 36.1 to 36.99, V45.81), erebrovascular accident (stroke; ICD-9-CM codes 430 to 432, 433 to 437), malignant dysrhythmia (ICD-9-CM codes 246.0, 426.12 to 426.13, 426.51 to 426.52, 426.54, 427.1, 427.4, 427.41 to 427.42, 427.5), cardiac shock (ICD-9-CM code 785.51), thrombolysis (ICD-9-CM codes 36.0 to 36.99), or implantable cardiac defibrillator (ICD-9-CM code V4502).
Selective loss to follow up: No
Identification confounders and correction in analysis: Yes, adjusted for age, years of education, marital status, multiple gestations, infant sex, birth weight, parity, long-term hypertension, pregnancy-related hypertension, anemia, diabetes, antepartum hemorrhage, postpartum hemorrhage, and systemic lupus erythematosus.
Funding: This work was supported by Grants NHRI-EX95-9108SC and NHRIEX969627SI from the National Health Research Institute, Taiwan; Grants NSC 96-2314-B182-026 and 97-2314-B-182-028-MY2 from the National Science Council, Taipei, Taiwan; Topnotch Stroke Research Center, Ministry of Education, Taipei, Taiwan; and Grant DOH-TD-B-111-002 from the Center of Excellence for Clinical Trial and Research in Neurology and Neurosurgery, Department of Health, Taipei, Taiwan.
|
|
Lindeberg 1988 |
Design Case-control study
N = 98
Country Sweden |
Aim of the study: To follow prospectively the development of blood pressure during a period of 5-6 years in primiparous women with gestational hypertension (GH) in an attempt to identify factors associated with increased risk of developing hypertension
Inclusion criteria - primparas without previously know hypertensive disease but with hypertension in pregnancy - Period: September 1978 till 31 August 1980 - lived in the town of Orebro
Exclusion criteria - hypertension only during labor and/or the puerperium -
|
Determinant PIH
N = 49 |
Controls Normotensive primiparas matched by age
N = 49 |
Primary outcomes: Hypertension
Secundary outcomes:
Follow up: 5 years |
Primary outcomes:
During the follow-up period, 7 women developed hypertension requiring therapy and 14 women were classified as having borderline hypertension, among the 49 women with hypertension in pregnancy. Only 2 women in the control group developed borderline hypertension. Fourteen women in the GH group had PE (hypertension + proteinuria) and 2 of these had severe PE.
|
Clearly defined groups: Hypertension was defined as a diastolic blood pressure ≥90 mmHg on at least 2 occasions more than 6 hours apart.
Selection bias: Not expected
Method of assessing the outcome appropriately: Blood pressure measurements and weight were registered at 2, 6 and 12 months after delivery and once a year thereafter. The diagnosis of hypertension was established if the criteria for drug therapy according the principles of the Hypertension clinic were fulfilled. Borderline hypertension was defined as a diastolic blood pressure of >90 mmHg or more than one occasion during follow-up
Selective loss to follow up: Fifty-four pairs of women initially agreed to take part in the study. Four subjects in the study group were lost to follow-up (refused, or had moved to distant place) and 2 in the control group (one refused, one moved abroad).
Identification confounders and correction in analysis: No
Funding: Not reported
|
|
Lykke 2009 |
Design Cohort study
N = 782 287
Country Denmark |
Aim of the study: the relationship between hypertensive pregnancy disorders and various subsequent cardiovascular events and the effect of type 2 diabetes mellitus on these
Inclusion criteria - women delivering in Denmark from 1978 to 2007 with a first singleton (n=782 287) and 2 first consecutive singleton deliveries (n=536 419).
Exclusion criteria - women with a Preceding cardiovascular diagnosis or type 1 and 2 diabetes mellitus and women who died or emigrated within 3 months of delivery |
Determinant PIH N = 7449
Mild PE N = 26 810
Severe PE N = 7016 |
Controls No hypertensive disorder
N = 741 012 |
Primary outcomes: the first diagnosis of hypertension, ischemic heart disease, congestive heart failure, thromboembolic event, stroke, and type 2 diabetes mellitus.
Secundary outcomes:
Follow up: 14.60 years (range: 0.25 to 30.20 Years) |
Primary outcomes:
|
Clearly defined groups: Hypertensive pregnancy disorders, placental abruption, stillbirth, and all of the end points were ascertained by the specific International Classification of Diseases 8 and 10 codes
Selection bias: Not expected
Method of assessing the outcome appropriately: They linked information in the National Patient Registry (NPR) with the Central Person Registry and Cause of Death Registry retrieving status on emigration and death on March 1, 2008.
Selective loss to follow up: In cohort 1 during the follow-up period, 15 902 (2.0%) emigrated and 8876 (1.1%) died. In cohort 2 during the follow-up period, 7109 (1.3%) women emigrated and 4888 (0.9%) died.
Identification confounders and correction in analysis: Yes
Funding: Not reported
|
|
Lykke, 2010
|
Design cohort study
N total = 782 287
Country Denmark
|
Aim of the study To elucidate the impact of preterm delivery, delivery of an SGA offspring, hypertensive disorders of pregnancy, placental abruption and stillbirth in a first delivery on subsequent rates of death from cardiovascular and noncardiovascular and all causes.
Inclusion criteria 1. Women delivering in Denmark from 1978 – 2007. 2. 15-50 years 3. First singelton delivery.
Exclusion criteria 1. any preceding cardiovascular diagnosis (e.g.hypertension or deep venous thromboembolism. 2. DM 3. Died or emigrate within 3 months of delivery.
|
Determinant PIH N = 7449
Mild PE N = 26 810
Severe PE N = 7016
Or
Pre-eclampsia N = 25 184 (= zonder vroeggeboorte, SGA etc) |
Controls Uncomplicated pregnancy
N = 643 935 |
Primary outcomes: Death from all causes, which was also subdivided into death from cardiovascular causes and non-cardiovascular causes.
Secundary outcomes:
Follow up: Median 14.63 years (-.25-30.1): |
Primary outcomes:
Secondary outcomes:
|
Clearly defined groups: Yes
Selection bias: Possible, no confounding for moking, obesity and socio-economic status and the questionable validity of the exposures and end points: the ICD codes of the hypertensive disorders of pregnancy have been assessed to be very specific, but only moderately sensitive, with PPVs ranging from 56% to 100%.
Method of assessing the outcome appropriately: Yes, they extract information from the National Patient Registry (NPR) and used ICD codes for the primary outcome. The NPR collects information on all discharge diagnoses from hospitals and deliveries in Denmark. Missing values occurred more frequently in the earlier years; these were analysed as separate groups. When investigating combinations of preterm delivery,SGA and pre-eclampsia, they dichotomised hypertensive disorders of pregnancy into two groups: pre-eclampsia and no-pre-eclampsia (the latter being the reference group, which included gestational hypertension). We restrictively defined a cardiovascular cause of death as either stated thus in the Cause of Death Registry, or a first cardiovascular diagnosis, e.g. de novo hypertension or ischaemic heart disease, reported within 1 week prior to the time of death.
Selective loss to follow up: They censored women who had emigrated at the time of departure: n=15 902 (2%)
Identification confounders and correction in analysis: Adjustment for maternal age at delivery and year of delivery.
Funding: Not reported
|
|
Magnussen 2009 |
Design Cohort study
N = 15,065
Country Norway |
Aim of the study: To study the association of hypertensive pregnancy disorders with modifiable risk factors for cardiovascular and metabolic diseases and to estimate the feasibility for early detection and prevention.
Inclusion criteria - women who participated in the HUNT Study with a birth that had occurred from 1967
Exclusion criteria - women who were pregnant at baseline of the HUNT Study, and women who were not primiparous when they were first registered in the Medical Birth Registry. - women with pregnancies of less than 22 weeks of gestation, - women with multiple births, with chronic hypertension, and women with known diabetes before pregnancy. |
Determinant HDP
N = 1433 |
Controls No HDP
N = 13 632 |
Primary outcomes: Blood pressure, lipids
Secundary outcomes:
Follow up: 16.5 years |
Primary outcomes:
In women with a history of preeclampsia, the adjusted odds ratio for diabetes was 3.8 (95% CI 2.1– 6.6) compared with other parous women, and after further adjustment for BMI, the odds ratio was attenuated to 2.8 (95% CI 1.6 –5.0). In relation to gestational hypertension, there was no clear association with later diabetes (adjusted odds ratio, 1.3, 95%C I 0.4–4.0), and after additional adjustment for BMI, the estimated odds ratio changed to 0.9 (95% CI 0.3–3.8). Women with a history of preeclampsia were three times (adjusted odds ratio 3.1, 95% CI 2.2 to 4.3) more likely to use blood pressure medication at follow-up compared with women with no history of preeclampsia.
|
Clearly defined groups: Yes, preeclampsia was defined as a sustained increase in blood pressure to at least 140/90 mm Hg after mid gestation, combined with proteinuria of at least 1+ or more on a semiquantitative dipstick. Gestational hypertension was defined as blood pressure of 140/90 mm Hg or more (one or both values exceeded) or increase in systolic blood pressure of 30 mm Hg or more and diastolic blood pressure of 15 mm Hg or more after mid gestation, without concomitant proteinuria.
Selection bias: Not expected
Method of assessing the outcome appropriately: Data from the Medical Birth Registry of Norway were linked to the Nord-Trøndelag Health (HUNT) Study; a population-based health survey conducted in Nord- Trøndelag County in Norway. All residents 20 years and older were invited to participate in the second wave of the HUNT Study (1995–1997),12 and a total of 34,882 women (75%) accepted the invitation and attended a clinical examination that included standardized measurements of height, weight, waist circumference, blood pressure, and nonfasting measurements of serum lipids and glucose.
Selective loss to follow up: No
Identification confounders and correction in analysis: Yes
Funding: No
|
|
Marin 2000 |
Design Case-control study
N =
Country Spain |
Aim of the study: To assess the prevalence of subsequent hypertension in women with hypertensive pregnancies and evaluate it according to the subclassifications of hypertension in pregnancy.
Inclusion criteria - The study group consisted of 634 patients obtained from a series of 864 pregnant women with hypertension evaluated between 1973 and 1996 (238 in a retrospective analysis from 1973 to 1980, and 626 in a prospective observation from 1981 to 1996), entered into the study up to 1991. - The control group consisted of 285 women that were the first 15 normotensive pregnancies with normal delivery and normotensive puerperium occurring each year from 1973 to 1991, and obtained from the birth register.
Exclusion criteria
|
Determinant HDP
N = 273
Or
Only GH, PE and eclampsia
N = 205 |
Controls No HDP
N = 86 |
Primary outcomes: prevalences of hypertension, diabetes, and hypercholesterolemia, together with cardiovascular morbidity.
Secundary outcomes:
Follow up: HDP: 13.6 years (range 6–24 years)
Controls: 16.2 years (range 6–24 years) |
Primary outcomes:
A further analysis was done after the exclusion of chronic hypertension (92% essential hypertension, 8% secondary hypertension) and unclassifiable hypertension cases. This group of pregnancy-induced hypertension cases consisted of 205 women. The remote hypertension prevalence continued to be higher within the cases (45% versus 14%; adjusted OR 5 5.1; 95% CI 5 2.4–9.8; p , 0.001) and these differences remained significant when multivariate analysis was used to adjust for body mass index and follow-up time (Table 4).
|
Clearly defined groups: The definition of hypertension in pregnancy was systolic BP ≥140 mm Hg or diastolic BP ≥90 mm Hg on at least two occasions in a 6-h period. Proteinuria was taken as significant when a dip-stick reading was 21 or more or when a 24-h sample showed ≥0.3 g. The term “pregnancy-induced hypertension” included preeclampsia, eclampsia, and gestational hypertension.
Selection bias: Possible, may non-responders
Method of assessing the outcome appropriately: Cases and controls were invited by mail to come to the hospital for an evaluation, which was performed by the same observer (C.G.P.) and included (1) a cardiovascular survey based on a standard questionnaire (15), (2) BP, weight, and height measurements, (3) laboratory tests: total cholesterol, HDL-cholesterol, triglyderides, glucose, uric acid, and creatinine in a 12-h-fast blood sample and (4) a dip-stick urine analysis. Hypertension was considered when previously diagnosed or when systolic BP was >140 mm Hg and/or diastolic BP was >90 mm Hg. Diabetes was considered when previously diagnosed or when the glucose level was ≥140 mg/dL (7.7 mmol/L) on two separate occasions. Hypercholesterolemia was defined as a total cholesterol level ≥240 mg/dL (6.2 mmol/L). The term “cardiovascular morbidity” included coronary heart disease (angina pectoris and/or myocardial infarction), congestive heart failure, cerebrovascular disease, and peripheral vascular disease.
Selective loss to follow up: The study group of 634 women was reduced to 476 cases (5 deaths and 153 inadequate addresses). Additional efforts to improve compliance (phone calls, death register consultation, and hospital record searches) were not successful. Two hundred seventy-three women (57%) agreed to revaluation. The control group was reduced to 226 women mainly because of inadequate addresses and 86 (38%) completed the evaluation.
Identification confounders and correction in analysis: Yes, but not described for which confounders
Funding: Not reported.
|
|
Mongraw 2010 |
Design Cohort study
N = 14 403
Country USA |
Aim of the study: This study prospectively investigates the contribution of pregnancy complications and other reproductive age risk factors on the risk of subsequent cardiovascular disease death.
Inclusion criteria - women partcipating in the Child Health and Development Studies pregnancy cohort drawn from the Kaiser Permanente Health Plan in California with nonmissing parity and no previously diagnosed heart conditions
Exclusion criteria - multiple birth pregnancies and pregnancies missing on parity. We also excluded all of the pregnancies that ended in abortion or fetal death before 20 weeks’ gestation and women with pre-existing heart conditions diagnosed before enrollment. |
Determinant PE
N = 481 |
Controls No PE
N = 13 922 |
Primary outcomes: CVD mortality
Secundary outcomes:
Follow up: 37 years |
Primary outcomes:
The increased risk of CVD death with PE remains even after adjusting for other known risk factors, including preexisting hypertension and delivering an IUGR infant. |
Clearly defined groups: Proteinuria is defined as a reading of +1 (0.5% or 300 mg/24 hours) on a urine dipstick. PE is defined as either of the following occurring after 20 weeks of gestation: ≥2 blood pressure readings ≥140/90 mm Hg and proteinuria or ≥2 systolic readings ≥140 mm Hg or ≥2 diastolic readings of ≥90 mm Hg and proteinuria. Preexisting hypertension was defined as ≥1 blood pressure reading of ≥140/90 mm Hg before 20 weeks of pregnancy or doctor-diagnosed hypertension from the medical chart. Gestational hypertension was defined as +1 blood pressure reading of ≥140/90 mm Hg that developed after the 20th week of pregnancy and not accompanied by proteinuria. Early onset PE was defined as onset of PE before 34 weeks of gestation. IUGR was defined as below the 10th percentile of z scores in birth weight by sex and gestational age for the CHDS distribution.
Selection bias: Not expected
Method of assessing the outcome appropriately: Cardiovascular disease death was determined by linkage with the California Department of Vital Statistics. CVD death, including the following: 420.1 for ICD-7; 410 and 412 for ICD-8; 410, 411, 414, and 429 for ICD-9, and I21 to I25 for ICD-10.
Selective loss to follow up: Not included in analysis
Identification confounders and correction in analysis: Yes, not well described (The full model was constructed using all of the variables of interest that were either independently significant and/or confounders to the 10% level after mutual adjustment)
Funding: This project was made possible by funding from the National Institutes of Health (grant N01 DK63422).
|
|
Nisell 1995 |
Design Case-control study
N = 138
Country Sweden |
Aim of the study: To assess the occurrence of chronic hypertension and renal disorder after gestations complicated by pregnancy induced hypertension or preeclampsia and to define background factors and laboratory analyses at follow up examination which discriminate between women who remain normotensive and those who develop hypertension
Inclusion criteria - women whose gestation were complicated by PIH and PE during 1986 and delivered at the Huddinge University Hospital - controls: women who experienced a normal pregnancy during 1986 à randomly selected from women delivered on the same day as those with PE an PIH
Exclusion criteria - chronic cardiovascular, renal or endocrinologic disease |
Determinant PIH
N = 49
PE
N = 45 |
Controls Normotensive pregnancy
N = 44 |
Primary outcomes: Hypertension
Secundary outcomes:
Follow up: 7 years |
Primary outcomes:
|
Clearly defined groups: Yes, mild PE was defined as blood pressure was 140/90-160/110 mmHg and urinary protein excretion measured 0.3-3 g/24 h after 20 weeks of pregnancy. Severe PE was defined as blood pressure above 160/110 mmHg and/or proteinuria exceeded 3g/24h. PIH was defined as blood pressure ≥ 140/90 mmHg in the absence of proteinuria after 20 weeks of gestation.
Selection bias: Not expected
Method of assessing the outcome appropriately: Women were considered to have chronic hypertension if they were on anti-hypertensive medication or if 2 diastolic readings with 15 min intervals ≥90 mmHg. Not clear if the blood samples were fasting.
Selective loss to follow up: Of 134 women invited to participate in the study, 94 agreed to participate and 40 declined because of social reasons.
Identification confounders and correction in analysis: No
Funding: Grants from the General Hospital Foundation, the Karlinska Institute and the Swedish Medical Research Council
|
|
North 1996 |
Design Case-control study
N = 100
Country Samoa |
Aim of the study: To compare the rate of microalbuminuria and hypertension in 50 Samoan women with past preeclampsia (cases) with 50 Samoan women who did not have past preeclampsia (controls).
Inclusion criteria - women with a history of preeclampsia in their first pregnancy in an Samoan hospital between 1980 and 1993 - contols: Samoan women aged between 20 and 35 years, who had their first baby in New Zealand. who did not have preeclampsia with their first pregnancy, and who were neither currently pregnant or known to have diabetes
Exclusion criteria
|
Determinant PE
N = 50 |
Controls No PE
N = 50 |
Primary outcomes: HT
Secundary outcomes:
Follow up: 5 years (range 1-25 years) |
Primary outcomes: only 1 (2%) of controls were currently hypertensive, 40% (20/50) of cases were hypertensive (P<o.O001), 6 of whom were receiving anti-hypertensive medication.
|
Clearly defined groups: Preeclampsia was defined as a blood pressure ≥140/90 mmHg after 20 weeks gestation. with an increase in diastolic blood pressure ≥15 mmHg, and proteinuria, 2+ or ≥0.3 g/24 hours.
Selection bias: Not expected
Method of assessing the outcome appropriately: Interviews with cases and controls were held by a medical research assistant and a Samoan link worker. Obstetric details were collated from the medical records. Hypertension at follow-up was diagnosed if the systolic blood pressure was greater than 140 mmHg and/or diastolic blood pressure greater than 90 mmHg.
Selective loss to follow up: Of the 181 Samoan women fitting the criteria for preeclampsia, 111 had moved from their original address and were not able to be traced. Fifty of the 70 (71%) women contactable were included in the study. The database identified I 0 9 women to serve as controls. However, after the first mailing and telephone contacts, only 8 women were able to be contacted, 7 of whom were included in the study. The door to door visits identified 52 women eligible to serve as controls. Forty three participated, 1 refused to participate, and 8 were unavailable in spite of repeated contact.
Identification confounders and correction in analysis: No
Funding: University of AuckIand Research Fund
|
|
Portelinha 2010 |
Design Case-control study
N = 150
Country Brasil and Portugal |
Aim of the study: the evaluation of lipid profile and oxLDL plasma concentration several years after pregnancy to see if these women have any alteration of these parameters that may be linked to the risk of CVD in the future.
Inclusion criteria - Women with a history of PE and women without medical complications (controls), at Hospital de São João, Hospital Geral de Santo António and Maternidade Júlio Dinis, Porto, Portugal - The control group consisted of women matched for age, who gave birth to the first child after an entirely normotensive pregnancy. - premenopausal state
Exclusion criteria - prior history of hypertension, heart disease, diabetes mellitus, renal disease, infections, recent surgery and current pregnancy |
Determinant PE
N = 90 |
Controls No PE
N = 60 |
Primary outcomes: Lipids, blood pressure
Secundary outcomes:
Follow up: 6 years postpartum |
Primary outcomes:
|
Clearly defined groups: PE was defined as an increase in blood pressure of at least 140/90 mmHg after the 20th week of gestation in previously normotensive women, combined with proteinuria (protein excretion at least 0.3 g per 24 hours, a spot urine protein/creatinine ratio 530 mg/mmol or at least 2+ protein by dipstick).
Selection bias: Not expected
Method of assessing the outcome appropriately: women were identified from medical records and were invited to the research centres after an overnight fast.
Selective loss to follow up: No
Identification confounders and correction in analysis: Adjustment of statistical differences for confounding factors was performed by analysis of covariance, after log transformation of variables (when necessary).
Funding: Not reported
|
|
Ray 2005 |
Design Cohort study
N = 1 026 265
Country Canada |
Aim of the study: to assess the risk of premature vascular disease in women who had had a pregnancy affected by maternal placental syndromes.
Inclusion criteria - all women admitted to hospital for the first obstetrical delivery of a liveborn or stillborn infant after 20 weeks’ gestation in the study period April 1, 1990, and March 31, 2004 - women free from cardiovascular disease before their first documented delivery
Exclusion criteria - people younger than age 14 years or older than age 50 years at the time of delivery, - those who had a diagnosis of cardiovascular disease up to 24 months before delivery, - those who were not residents of Ontario, - women without a valid OHIP health-card number. |
Determinant PE
N = 36 982
PIH
N = 20 942 |
Controls No maternal placental syndrome
N = 950 885 |
Primary outcomes: cardiovascular disease
Secundary outcomes:
Follow up: 8·7 years |
Primary outcomes: Of the remaining 1 026 265 women who had a first documented delivery during the study period, 75 380 (7%) were diagnosed with a maternal placental syndrome. The mean and maximum age at the time of first cardiovascular event was 38·3 years and 60·2 years, respectively.
|
Clearly defined groups: Pre-eclampsia is defined by the presence of hypertension in association with at least 2+ proteinuria on urinary dipstick or at least 300 mg of urinary protein per 24-h specimen collection. Poor fetal growth is typically based on an estimated fetal weight below the 10th percentile for gestational age (bases on ICD-codes)
Selection bias: No
Method of assessing the outcome appropriately: Yes, they uses linked health-care administrative databases. Our primary outcome was a composite of cardiovascular disease, defined as hospital admission for coronary, cerebrovascular, or peripheral artery disease, or revascularisation of the coronary, carotid, or a lower extremity arterial system. The diagnosis that most strongly affected the patient’s length of stay was used. We used ICD-9 codes to identify the study outcomes; after March 31, 2002, we used corresponding ICD-10-CA codes because hospitals in Ontario were mandated to use ICD-10-CA coding from April 1, 2002.
Selective loss to follow up: Yes, well described (exclusion criteria)
Identification confounders and correction in analysis: Yes, Adjusted for maternal age, multiple gestation, length of stay, income quintile, rural residence, drug dependence, and gestational diabetes mellitus in index delivery, and hypertension, any diabetes mellitus, obesity, dyslipidaemia, tobacco use, renal disease, migraine headache, and systemic lupus erythematosus up to 24 months before index delivery
Funding: There was no funding source for this study.
|
|
Sattar 2003 |
Design Case-control study
N = 80
Country UK |
Aim of the study: To explain the underlying mechanism of the relation between preeclampsia (PE) and an increased risk of maternal coronary heart disease (CHD) in later life.
Inclusion criteria - Primigravid women who delivered between 1975 and 1985 with proteinuric PE and controls, matched as a group for time of index pregnancy, smoking, and current body mass index,
Exclusion criteria
|
Determinant PE
N = 40 |
Controls No PE
N = 40 |
Primary outcomes: Riskprofile
Secundary outcomes:
Follow up: 20 years |
Primary outcomes:
|
Clearly defined groups: PE was defined as a diastolic blood pressure >90 mm Hg (but normal blood pressure at booking), and had >2+ of proteinuria on dipstick testing in the absence of renal disease or infection.
Selection bias: Not expected
Method of assessing the outcome appropriately: Cases and non-cases were identified from medical records. Venous blood was taken after an overnight fast.
Selective loss to follow up: Not applicable
Identification confounders and correction in analysis: No
Funding: Not reported
|
|
Shahbazian, 2011 |
Design Case-controls tudy
N = 70
Country Iran |
Aim of the study: whether Iranian women with a history of preeclampsia had higher rates of hypertension and microalbuminuria compared with women with uneventful pregnancy.
Inclusion criteria - primiparous women diagnosed with preeclampsia or eclampsia at Razi Hospital and Emam Khomeini Hospital, in Ahvaz, Iran between March 2001 and February 2003 - controls: women selected from the same database, matched for year of delivery and age, who had a pregnancy uncomplicated by hypertension during the same period.
Exclusion criteria - diagnosis of chronic hypertension. - no maternity data available |
Determinant PE
N = 35 |
Controls Uncomplicated pregnancy
N = 35 |
Primary outcomes: HT
Secundary outcomes:
Follow up: 5.7 years (range, 5.2 to 7.3 years). |
Primary outcomes:
1 woman (2.9%) from among the controls was currently hypertensive, 28.6% (n = 10) of formerly preeclamptic women were hypertensive (P = .003; relative risk, 10; 95% confidence interval, 1.35 to 74.00; attributable risk, 89.9%), 7 of whom were receiving antihypertensive medication at the time of recruitment. |
Clearly defined groups: Pre-eclampsia was defined as a blood pressure of 140/90 mm Hg and higher and urinary protein excretion of 300 mg/24 h and greater after 20 weeks of gestation.
Selection bias: Not expected
Method of assessing the outcome appropriately: Hypertension was diagnosed if the systolic blood pressure was equal or greater than 140 mm Hg and/or the diastolic blood pressure was equal or greater than 90 mm Hg or if the participant was taking antihypertensive medication.
Selective loss to follow up: 39 patients were invited to participate in historical cohort study and 35 provided consent (participation rate, 83%).
Identification confounders and correction in analysis: No
Funding: This project was funded by Diabetic Research Center of Ahvaz Jondi Shapour University of Medical Sciences.
|
|
Shalom 2013 |
Design Cohort study
N = 22 814
Country Israel |
Aim of the study: to evaluate long-term morbidity of patients with hypertensive disorders of pregnancy.
Inclusion criteria - women who gave birth at the Soroka University Medical Center between the years of 1988 to 1998, and with a follow-up until December 2009.
Exclusion criteria - women with chronic hypertension and pre-gestational diabetes before the index pregnancy. |
Determinant HDP
N = 2072 |
Controls No HDP
N = 20742 |
Primary outcomes: the first diagnosis of chronic HT or any relevant hospitalization during the follow-up years.
Secundary outcomes:
Follow up: at least 10 years |
Primary outcomes: Patients with hypertensive disorders had 15.8 fold (range 12.9–19.3) increased risk of chronic hypertension diagnosed after the pregnancy in which there had been a diagnosis of preeclampsia (the index pregnancy) as compared with patients without preeclampsia or any other hypertensive disorders.
|
Clearly defined groups: The cohort was divided into two groups: women who at one or more of their pregnancies were diagnosed with gestational hypertensive disorders: gestational hypertension (diagnosed empirically when appropriately taken blood pressure exceeded 140 mm Hg systolic or 90 mm Hg diastolic for the first time after midpregnancy), mild preeclampsia (blood pressure ≥ 140/90 mm Hg after 20 weeks’ gestation with proteinuria ≥ 300 mg/24 hours or ≥ 1+ dipstick), severe preeclampsia (mild preeclampsia accompanied by at least one of the following: blood pressure ≥ 160/110 mm Hg, proteinuria 2.0 g/24 hours or ≥ 2+ dipstick, serum creatinine >1.2 mg/dL unless known to be previously elevated, platelets < 100 000/μL, microangiopathic hemolysis: increased LDH, elevated serum transaminase levels: ALT or AST, persistent headache or other cerebral or visual disturbance, persistent epigastric pain), eclampsia (seizures that cannot be attributed to other causes in a woman with preeclampsia), that is, exposed group. The comparison group consisting of women who were not exposed to any of the obstetric hypertensive disorders, that is, non-exposed group
Selection bias:
Method of assessing the outcome appropriately: Data were extracted by linking a computerized database of hospitalizations with computerized database containing maternal records from the same regional medical center. All diagnoses are classified according to the International Classification of Diseases, 9th revision (ICD-9).
Selective loss to follow up:
Identification confounders and correction in analysis:
Funding:
|
|
Sibai 1986 |
Design Case-control study
N = 815
Country USA |
Aim of the study: To compare subsequent pregnancy outcome and incidence of chronic hypertension and diabetes on follow-up in women with a history of PE
Inclusion criteria - women delivered at the E.H. Crump Women’s Hospital and Perinatal Center, Memphis, Tennesse. - documented prenatal care with normal blood pressure before 20 weeks’gestation - normal blood pressure recording within 8 weeks after the first delivery - at least one subsequent pregnancy beyond 20 week’s gestation - adequate medical follow-up for a minimum of two completed years after the first delivery. - The control group consisted of women who remained normotensive throughout their first pregnancies and who had similar inclusion criteria. These patients were matched to the above group by age, race, gestational age at delivery and obstetric complications (excluding hypertension) and were delivered within 1 month of the study group
Exclusion criteria - associated medical complications before pregnancy |
Determinant Severe PE in first pregnancy
N = 406 |
Controls Normotensive during first pregnancy
N = 409 |
Primary outcomes: HT and DM
Secundary outcomes:
Follow up: PE: 6.6 yr C: 8.0 yr |
Primary outcomes: The incidence of diabetes was 1.7% in the PE group and 1.5% in the control group. The overall incidence of chronic hypertension was significantly higher in the PE group (14.8 % vs 5.6%). 90 patients in the PE group and 138 women in the control group were followed up ≥10 years. The average years of follow up within this subgroup were 13.8 ± 3.8 and 13.5 ± 3.1 years, respectively. In addition the mean maternal age on follow-up was 30.9 ± 4.2 years in the PE group versus 31.3 ± 4.2 years in the normotensive group. The incidence of subsequent chronic hypertension was 51% versus 14% in this follow up groups. The incidence of diabetes was 5.6% versus 3.6% among patients followed up ≥10 years.
|
Clearly defined groups: Yes, PE was defined as BP ≥160/110 mmHg, protein 3+, after 20 weeks gestation
Selection bias: Not expected
Method of assessing the outcome appropriately: Could be better, all patients’ records were carefully and extensively reviewed by the senior author. In the majority of cases the patients were seen and followed up by the senior author. In other cases hospital records and the records of other medical providers were accepted if they were determined to be adequate and reliable.
Selective loss to follow up: Yes, only women with subsequent pregnancies were included in this analysis
Identification confounders and correction in analysis: No
Funding: Not reported
|
|
Skjaerven, 2012 |
Design Cohort study
N = 836 147
Country Norway |
Aim of the study: To assess the association of pre-eclampsia with later cardiovascular death in mothers according to their lifetime number of pregnancies, and particularly after only one child.
Inclusion criteria - first singleton birth (from 22 weeks’ gestation) between 1967 and 2002,
Exclusion criteria
|
Determinant All PE
N = 34 824
Term PE
N = 26 708
Preterm PE
N = 5886 |
Controls All No PE
N = 801 323
Term no PE
N = 712 181 |
Primary outcomes: CVD mortality
Secundary outcomes:
Follow up: Not reported, but up to 40 years |
Primary outcomes:
We explored the possible role of diabetes by excluding 4322 (0.5%) women with recorded pre-gestational or gestational diabetes in their first pregnancy. After excluding these women, the adjusted hazard ratio of cardiovascular mortality with preterm pre-eclampsia fell from 9.4 (95% confidence interval 6.5 to 13.7; table 1) to 6.8 (4.3 to 11). A corresponding exclusion of women with pre-existing hypertension had little effect on the hazard ratios
|
Clearly defined groups: Yes, preeclampsia was defined as an increased blood pressure after 20 weeks’ gestation (defined as blood pressure 140/90 mm Hg or greater; or an increase in systolic blood pressure of ≥30 mm Hg or increase in diastolic blood pressure of ≥15 mm Hg, from measurements before 20 weeks of gestation), and proteinuria (≥0.3 g in 24 h urine specimen, or ≥1 point increase on urinary dipstick). Preterm birth is defined as a delivery occurring between 22 and 36 completed weeks of gestation.
Selection bias:
Method of assessing the outcome appropriately: Yes, using the national identification number, we linked each mother to her births for the period 1967-2009. Data for these women were linked to the national Cause of Death Registry through December 2009. We classified causes of maternal death according to ICD-10 for the years 1996-2009, ICD-9 for 1986-95, and ICD-8 for 1969-85).
Selective loss to follow up: Loss to follow-up owing to emigration from Norway was low (<1%).
Identification confounders and correction in analysis: Adjusted for maternal education (three categories), maternal age at first birth, and year of first birth. No adjustement for smoking and BMI!
Funding: The study has been supported by grants from the Norwegian Research Council and by the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institute of Health.
|
|
Smith, 2001 |
Design Cohort study
N total = 129 920
Country UK |
Aim of the study To investigate whether pregnancy complications associated with low birthweight are related to risk of subsequent IHD in the mother.
Inclusion criteria 1. SMR2 database: all singleton first births of a live baby between 1981 and 1985
Exclusion criteria 1. still births 2. birth < 24 wks 3. birthweight < 500 g 4. previous pregnancy other than induced abortion or miscarriage |
Determinant PE
N = 22 781 |
Controls No PE
N = 107 139 |
Primary outcomes: 1. death from any cause 2. death due to IHD 3. any IHD event
Secundary outcomes:
Follow up: 15-19 years |
Primary outcomes: There were 22 781 women with a hypertensive disease of pregnancy (17.5%)
Secundary outcomes:
|
Clearly defined groups: Yes, pre-eclampsia was defined as hypertension in pregnancy, childbirth, or the puerperium, not specified as pre-existing, with albuminuria, oedema, or both.
Selection bias: Not expected.
Method of assessing the outcome appropriately: The Scottish Morbidity Record (SMR) system collects routine discharge data on all patients admitted to Scottish National Health Service acute (SMR1) and maternity (SMR2) hospitals. The Information and Statistics Division of the Common Services Agency links all SMR records for an individual patient to each other and to the General Registrar’s Office death database. Birthweight was categorised by quintiles specific for sex and gestational age IHD was defined by an International Classification of Diseases (ICD) code of 410–414 (ninth revision) or I20–I25 (tenth revision) in the principal position.
Selective loss to follow up: Yes, complete data were available for 95.6% of women.
Identification confounders and correction in analysis: Yes, adjustment for socioeconomic deprivation, maternal height and age, and essential hypertension, lowest birthweight quintile, preterm delivery, and pre-eclampsia. No adjustment for smoking.
Funding: This project was funded by a grant from the Chief Scientist’s Office of the Scottish Executive Health Department (CZG/4/2/22). |
|
Spaan 2009 |
Design Case-control study
N = 51
Country Netherlands |
Aim of the study: To test whether preeclampsia predisposes to central hemodynamic and renal impairments 20 years after pregnancy.
Inclusion criteria - women who delivered after a preeclamptic pregnancy in the period between 1979 and 1987 at the Department of Obstetrics of the Academic Hospital of Maastricht in the Netherlands. - Controls: for every primiparous preeclamptic woman, we selected chronologically from the birth register the next two matching primiparous women with uncomplicated pregnancies and deliveries.
Exclusion criteria - no recent address - died - women with preexistent hypertension, diabetes mellitus, renal disease, current cancer therapy or chronic use of corticosteroid medication. |
Determinant PE
N = 22 |
Controls Uncomplicated pregnancy
N = 29 |
Primary outcomes: HT and stroke
Secundary outcomes:
Follow up: 23 year |
Primary outcomes:
|
Clearly defined groups: Preeclampsia was defined according to the criteria of the Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Early-onset preeclampsia was defined as preeclampsia resulting in birth before a gestational age of 34 weeks. An uncomplicated pregnancy was defined as a term singleton pregnancy without complications such as fetal growth restriction, pregnancy-induced hypertension, or gestational diabetes.
Selection bias: Not expected
Method of assessing the outcome appropriately: Yes, hypertension was defined as blood pressure above 140/90 mm Hg during the measurement session, using antihypertensive drugs, or both. Antihypertensive drugs were discontinued 2 weeks before the measurements. Participants did not drink caffeine- or alcohol-containing beverages and refrained from smoking and eating for at least 10 hours before the experiment.
Selective loss to follow up: 44 formerly preeclamptic women and 72 parous controls were invited to participate in this study. From these women, 22 formerly preeclamptic women (50%) and 29 controls (40%) gave informed consent to participate. Main reasons for refusal were lack of time (45%), psychological burden (25%), and invasiveness of measurements (10%).
Identification confounders and correction in analysis: No
Funding: Funded by Maastricht University Medical Centre, “profileringsfonds.”
|
|
Svensson 1983 |
Design Case-control study
N = 283
Country Sweden |
Aim of the study: To obtain reliable figures for late hypertension as well as to study factors possibly related to future hypertension.
Inclusion criteria - women giving birth between 1963-73 at the Ostra Hospital in Goteborg, Sweden - women with pre-eclampsia/hypertension in pregnancy -
Exclusion criteria
|
Determinant HDP
N = 237 |
Controls Normotensive pregnancy
N = 46 |
Primary outcomes: HT
Secundary outcomes:
Follow up: 7-12 yr |
Primary outcomes:
|
Clearly defined groups: HDP was defined as a blood pressure ≥140/90 mmHg after the 20th week of gestation. Mild PE ws defined as hypertension combined with proteinuria and edema. Severe PE was defined as BP 160 mmHg systolic or BP 110 mmHg diastolic or proteinuria at least 5 gr/24 hr or 24 hr urinary output <400 ml or cerebral or visual disturbances or pulmonary edema or cyanosis.
Selection bias: Possible, selection of control group was not well described
Method of assessing the outcome appropriately: Women with HDP were invited to a follow-up study. Women that had moved far out of town were instructed to get their blood pressure measured and return special forms with relevant information. Hospital record for 1969-73 were examined. Hypertension was defined as systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg on more than one occasion. Data from 262 normotensive pregnancies from 1969-73 were collected and 46 of these women were investigated in a manner identical to the procedure for women with a HDP
Selective loss to follow up: Out of 260 women with HDP, 237 were available for follow-up. No deaths were recorded.
Identification confounders and correction in analysis: No
Funding: This study was supported by a grant from the Gothenburg Medical Society
|
|
Wang, 2011 |
Design Case-control study
N = 5807
Country Taiwan |
Aim of the study: This study investigates whether preterm delivery further complicates the risk of stroke risk in women with hypertensive disorders in pregnancy (HDP) in Taiwan.
Inclusion criteria - women having their first pregnancies included in the database from January 1, 2000 through December 31, 2004;
Exclusion criteria - women with histories of stroke or hypertension diagnosed before the index date - or with missing information |
Determinant HDP
N = 1092 |
Controls No HDP
N = 4715 |
Primary outcomes: Stroke
Secundary outcomes:
Follow up: 6.64±1.57 years in the HDP cohort and 6.40±1.57 years in the non-HDP cohort |
Primary outcomes:
|
Clearly defined groups: Yes, ICD codes
Selection bias: Not expected
Method of assessing the outcome appropriately: This study used data from reimbursement claims of the universal National Health Insurance program, which was launched in March 1995 by incorporating 13 insurance programs in Taiwan. Patients with HDP (ICD-9-CM 642) were then identified from the group of women having their first pregnancies (primigravid) included in the database from January 1, 2000 through December 31, 2004; these women were designated as the HDP cohort. For each HDP case identified, 4 primigravid women without history of HDP were randomly selected, frequency-matched in the same year, and were designated as the non-HDP controls. The study subjects with and without HDP were linked to the registry for inpatient and outpatient claims data to identify those who had stroke develop (ICD-9-CM 430 to 437, 674.0, or A-code A290-294 and A299). Each subject either was followed-up from the index date until December 31, 2008 or was censored.
Selective loss to follow up: Not reported
Identification confounders and correction in analysis: adjusted for age and urbanization level
Funding: This study was supported in part by the Executive Yuan National Science Council (grant number NSC 98-2621-M-039-001), Clinical Trial and Research Center of Excellence of the Department of Health (grant number DOH99-TD-B-111-004), Taiwan Department of Health Cancer Research Center of Excellence (grant number DOH99-TD-C-111-005), and the China Medical University Hospital (grant number 1MS1)
|
|
Wikstrom 2005 |
Design Cohort study
N total = 403 550
Country Sweden
|
Aim of the study to investigate whether the risk of developing ischaemic heart disease (IHD) later in life increases with severity and recurrence of gestational hypertensive disease.
Inclusion criteria - Women giving birth to their first child in Sweden, 1973–1982
Exclusion criteria - Women with diabetes mellitus or essential hypertension |
Determinant Hypertensive disease
N = 20 469
PIH N = 7936
Mild Pe N = 9718
Severe PE N = 2815 |
Controls Uncomplicated pregnancy
N = 347 870 |
Primary outcomes: Fatal or non-fatal IHD
Secundary outcomes:
Follow up: follow up was restricted to the period 1987–2001. The first admission to hospital with IHD as the main diagnosis, or death with IHD as the underlying cause, was designated the event.
Mean follow-up for PIH: 14.7 yr
|
Primary outcomes:
Secundary outcomes:
|
Clearly defined groups: Yes, pre-eclampsia was defined as a rise in blood pressure (≥140/90) combined with proteinuria (≥300 mg/24 hours). Severe pre-eclampsia was defined as pre-eclampsia with either a diastolic blood pressure of at least 110 mmHg, or proteinuria of at least 5 g/24 hours, or both. Gestational hypertension was defined as a rise in blood pressure (≥140/90) occurring after 20 weeks of gestation without proteinuria. preterm delivery was defined as occurring before 37 weeks of gestation. SGA was defined as birthweight <2 SDs below the mean birthweight for gestational age.
Selection bias: Not expected
Method of assessing the outcome appropriately: Information from the Swedish Medical Birth Register, for the period 1973–1982, was used to define the study population. Complications during pregnancy and delivery are classified according to the Swedish version of the International Classification of Diseases (ICD)
Selective loss to follow up: Before 1987, 0.35% of the para-1 cohort had died and 2.8% had emigrated
Identification confounders and correction in analysis: They considered age, hospital at delivery and socioeconomic status to be possible confounders. BMI and smoking were no confounders
Funding: Not reported
|
|
Wilson, 2003 |
Design Case-cohort study
N = 3593
Country UK |
Aim of the study: To examine the association between hypertensive diseases of pregnancy (gestational hypertension and pre-eclampsia) and the development of circulatory diseases in later life.
Inclusion criteria - all women who had a diagnosis of pre-eclampsia or eclampsia during their first singleton pregnancy in the years 1951 to 1970 - an individually matched sample of women with a diagnosis of gestational hypertension during their first singleton pregnancy and matched for age to the nearest year and year of delivery with the previous group; - and an individually matched sample of women with no history of raised blood pressure during their first singleton pregnancy likewise matched with the first group.
Exclusion criteria - chronic hypertension |
Determinant PE
N = 1199
PIH
N = 1197 |
Controls Uncomplicated pregnancy
N = 1197 |
Primary outcomes: Current vital and cardiovascular health status, clinical examination, linkage to hospital discharge, and mortality data.
Secundary outcomes:
Follow up: Not reported |
Primary outcomes:
|
Clearly defined groups: Yes, gestational hypertension was defined as diastolic pressure ≥ 90 mm Hg on two occasions at least four hours apart or a single reading of ≥ 110 mm Hg from 20 weeks’ gestation onwards in a previously normotensive woman. Pre-eclampsia was defined as gestational hypertension plus proteinuria of ≥ 0.3 g/24 hours. Eclampsia was defined clinically as convulsions occurring in the presence of pre-eclampsia.
Selection bias: Not expected
Method of assessing the outcome appropriately: From the databank we identified a cohort of women who were living in Aberdeen city at the time of delivery. We carried out two tracing exercises for the cohort. The first, carried out in 1996, was at the local level using the Grampian community health index (a comprehensive regional primary care register24) to identify the current name and address of all cohort members still alive and resident in the Grampian area. From this exercise we were able us to contact the current general practitioners of women in the original cohort who were still living in the area. The second tracing exercise was at national level and was undertaken in 1999. The information and statistics division (ISD) of the NHS in Scotland, Edinburgh, used probability matching to identify any women from the cohort who were admitted to hospital from 1980 to 1999. In collaboration with the NHS central registry in Southport, the division also ascertained the vital status of women in the cohort and obtained death certificates for any who had died, including those who died in the United Kingdom but outside Scotland. For the mortality and hospital discharge outcomes, we used ICD codes.
Selective loss to follow up: Yes, well described
Identification confounders and correction in analysis: Hypertension: age at delivery, social class and smoking Events: age at delivery, social class
Funding: British Heart Foundation, grant number PG/95130. The guarantor accepts full responsibility for the conduct of the study, had access to the data, and controlled the decision to publish.
|
Risicotabellen
|
Tabel 4.1.1: risico’s op het krijgen van een fataal en/of niet-fataal cardiovasculaire gebeurtenis bij vrouwen met zwangerschapshypertensie en/of pre-eclampsie in de voorgeschiedenis vergeleken met vrouwen met een ongecompliceerde zwangerschap |
||||||||||||||||
|
Artikel |
Ziekte beeld |
N |
Gem FU (jr) |
Uitkomst |
CV gebeurtenis (N) |
Gecorrigeerde risico’s (95% BI) |
Gecorrigeerd voor |
|||||||||
|
A |
NA |
A |
NA |
|||||||||||||
|
Cohort onderzoeken waarin vrouwen met PIH/PE zijn vergeleken met vrouwen zonder PIH/PE |
||||||||||||||||
|
Bhattacharya, 2012 |
PIH (2/3) |
8891 |
23 937 |
34# |
F HVZ |
397 |
922 |
IRR 1.25 (1.11-1.41) |
Geboortejaar, socio-economische klasse, roken |
|||||||
|
PE (2/3 +4) |
2026 |
101 |
IRR 1.30 (1.06-1.60) |
|||||||||||||
|
PIH/PE |
10 917 |
498 |
IRR 1.26 (1.14-1.40) |
|||||||||||||
|
PIH (2/3) |
8891 |
NF HVZ |
2926 |
7273 |
OR 1.22 (1.15-1.29) |
|||||||||||
|
PE (2/3 +4) |
2026 |
662 |
OR 1.20 (1.08-1.33) |
|||||||||||||
|
Funai, 2005 |
PE (1/2 + 12 + 5) |
1070 |
35 991 |
30 |
F HVZ |
41 |
269 |
RR 3.07 (2.18-4.34) |
Lft, DM, GDM, geboortegewicht <2500 gr, opleidingsniveau, socio-economische klasse, jaar bevalling |
|||||||
|
Kestenbaum, 2003 |
PIH (7) |
10 687 |
92 902 |
7.8 |
F & NF HVZ |
19 |
64 |
HR 2.8 (1.6-4.8) |
Lft, pariteit, etniciteit, GDM, roken, sectio, soort verzekering |
|||||||
|
Milde PE(7) |
15 508 |
24 |
64 |
HR 2.2 (1.3-3.6) |
||||||||||||
|
Ernstige PE(7) |
5044 |
11 |
64 |
HR 3.3 (1.7-6.5) |
||||||||||||
|
PE all |
20 552 |
35 |
64 |
HR 2.54 (1.69-3.81) |
||||||||||||
|
PIH/PE |
31 239 |
54 |
64 |
HR 2.63 (1.90-3.64) |
||||||||||||
|
Lin, 2011 |
PE (7) |
nb |
nb |
Max 3 |
F & NF HVZ |
nb |
nb |
HR 12.6 (2.4-66.3) |
Lft, opleiding, huwelijkse status, gemelli, geslacht kind, geboortegewicht, pariteit, hypertensie, anemie, diabetes, fluxus postpartum, SLE |
|||||||
|
F HVZ |
nb |
nb |
HR 2.3 (1.6-3.1) |
|||||||||||||
|
Lykke, 2010 |
PIH (7) |
7449 |
643 935 |
14.6 |
F HVZ |
32 |
824 |
HR 2.47 (1.74-3.52) |
Lft, jaar bevalling,
|
|||||||
|
Milde PE (7) |
26 810 |
92 |
HR 1.99 (1.61-2.47) |
|||||||||||||
|
Ernstige PE (7) |
7016 |
24 |
HR 2.89 (1.93-4.33) |
|||||||||||||
|
PE (7) |
25 184 |
72 |
HR 2.08 (1.63-2.64) |
Vroeggeboorte, SGA, cases geexcludeerd |
||||||||||||
|
PIH/PE |
32 633 |
104 |
HR 2.20 (1.80-2.68) |
Lft, jaar bevalling
|
||||||||||||
|
Mongraw, 2010 |
PE (1, 2, 4) |
481 |
13 922 |
37 |
F HVZ |
24 |
242 |
HR 2.73 (1.78-4.18) |
Geen |
|||||||
|
PE ≤34 wk |
nb |
7 |
HR 9.54 (3.50-20.26) |
|||||||||||||
|
PE >34 wk |
nb |
17 |
HR 2.08 (1.26-3.44) |
|||||||||||||
|
Ray, 2005 |
PE (7) |
36 982 |
950 885 |
8.7 |
F & NF HVZ |
nb |
nb |
HR 2.1 (1.8-2.4) |
Lft, pariteit, socio-economische status, medicatie, GDM, HT, DM, obesitas, dyslipidemie, roken, nieraandoening, migraine, SLE |
|||||||
|
PIH (7) |
20 942 |
HR 1.8 (1.4-2.2) |
||||||||||||||
|
PE/PIH (7) |
57 924 |
HR 2.01 (1.79-2.26) |
||||||||||||||
|
Skjaerven, 2012 |
PE (1+2/ 11/12 en 4/12) |
34 824 |
801 323 |
nb |
F HVZ |
176 |
2380 |
HR 1.9 (1.6-2.2) |
Lft en jaar bevalling, opleidingsniveau |
|||||||
|
GA ≥36 |
26 708 |
712 181 |
115 |
2011 |
HR 1.6 (1.4-2.0) |
|||||||||||
|
GA 22-36 |
5886 |
712 181 |
45 |
2011 |
HR 3.7 (2.7-4.8) |
|||||||||||
|
Onderzoeken met patiënten series waarin vrouwen met PIH/PE zijn vergeleken met vrouwen zonder PIH/PE |
||||||||||||||||
|
Arnadottir 2005** |
PIH (1/2) & PE (1/2 + 9) |
325 |
629 |
50-55 |
F HVZ |
110 |
133 |
RR 1.60 (1.29-1.98) |
Geen |
|||||||
|
F HVZ ≤ 64 jaar |
28 |
15 |
RR 3.6 (1.98-6.61) |
|||||||||||||
|
F HVZ ≥ 65 jaar |
81 |
118 |
RR 1.3 (1.03-1.70) |
|||||||||||||
|
Marin, 2000** |
PE/PIH (1 /2 + 4) |
205 |
86 |
13.6-16.2 |
NF HVZ |
7 |
1 |
RR 2.94 (0.37-23.51) |
Geen |
|||||||
|
Onderzoeken met patiënten series waarin vrouwen met HVZ vergeleken zijn met vrouwen zonder HVZ |
||||||||||||||||
|
Studie |
Definitie PIH/PE |
HVZ (N) |
Gem. FU (jr) |
Uitkomst |
PIH/PE (N) |
Gecorrigeerde risico’s (95% BI) |
Gecorrigeerd voor |
|||||||||
|
Ja |
nee |
HVZ + |
HVZ - |
|||||||||||||
|
Ben-Ami, 2010 |
PIH (1/2) |
101 |
101 |
- |
NF HVZ |
23 |
5 |
RR 4.60 (1.82-11.62) |
Geen |
|||||||
|
|
PE (1/2 + 4) |
101 |
101 |
- |
NF HVZ |
20 |
3 |
RR 6.67 (2.04-21.73) |
||||||||
|
Akortingen: A = aangedaan door ziektebeeld; B = beroerte; BI = beroerte, ischemisch; BH = beroerte, hemorragisch; BMI = body mass index; DM = diabetes mellitus; DR = dysritmie; F = fataal; FU = follow-up; GDM = diabetes gravidarum; HT = hypertensie; HVZ = hart- en vaatziekten; IHZ = ischemische hartziekten; IUVD = intra-uteriene vruchtdood; MI = myocard infarct; NA = niet aangedaan door ziektebeeld; nb = niet bekend; NF = niet fataal; PE = pre-eclampsie; PIH = pregnancy induced hypertension/ zwangerschapshypertensie; SGA = small for gestational age; SLE = systemische lupus erythematodes; TE = thrombo-embolie; VG = voorgeschiedenis; VTE = veneuze thrombo-embolie
Definitie zwangerschapshypertensie en PE: 1. systolische bloeddruk ≥140 mmHg, twee x gemeten; 2. Diastolische bloeddruk ≥90 mmHg, twee x gemeten; 3. diastolische bloeddruk ≥110 mmHg, één x gemeten; 4. proteïnurie ≥0.3 gr/24 uur; 5. oedeem; 6. anamnestisch hypertensieve zwangerschap; 7. ICD code; 8. hypertensie niet nader gespecificeerd; 9. proteïnurie niet nader gespecificeerd; 10. systolische bloeddruk stijging ≥30 mmHg; 11. diastolische bloeddruk stijging ≥15 mmHg; 12. proteïnurie ≥1+dipstick; 13. Bloeddruk ≥160/110 mmHg met of zonder proteïnurie of bloeddruk ≥160/100 met proteïnurie; 14. Bloeddruk ≥160/105 mmHg eenmalig gemeten; 15. systolische bloeddruk ≥ 160 mmHg; 16. proteïnurie 3+ dipstick |
||||||||||||||||
|
Tabel 4.1.2: risico’s op het krijgen van fataal en/of niet-fataal ischemische hartziekte bij vrouwen met zwangerschapshypertensie en/of pre-eclampsie in de voorgeschiedenis vergeleken met vrouwen met een ongecompliceerde zwangerschap |
||||||||||
|
Artikel |
Ziekte beeld |
N |
Gem FU (jr) |
Uitkomst |
CV gebeurtenis (N) |
Gecorrigeerde risico’s (95% BI) |
Gecorrigeerd voor |
|||
|
A |
NA |
A |
NA |
|||||||
|
Cohort onderzoeken waarin vrouwen met PIH/PE zijn vergeleken met vrouwen zonder PIH/PE |
||||||||||
|
Bhattacharya, 2012 |
PIH (2/3) |
8891 |
23 937 |
34# |
F IHZ |
214 |
467 |
IRR 1.35 (1.15-1.59) |
Geboortejaar, socio-economische klasse, roken |
|
|
PE (2/3+4) |
2026 |
52 |
IRR 1.38 (1.03-1.84) |
|||||||
|
PIH en PE |
10917 |
266 |
IRR 1.36 (1.18-1.56) |
|||||||
|
PIH (2/3) |
8891 |
NF IHZ |
756 |
1882 |
OR 1.22 (1.11-1.34) |
|||||
|
PE (2/3+4) |
2026 |
172 |
OR 1.18 (0.99-1.41) |
|||||||
|
Freibert, 2011 |
PIH/ PE (6) |
222 |
2558 |
nb |
NF MI |
9 |
46 |
RR 2.25 (1.12-4.54) |
Geen |
|
|
AP |
21 |
113 |
RR 2.14 (1.37-3.34) |
|||||||
|
Garovic, 2010 |
PIH/ PE (6) |
4720 |
nb |
NF IHZ |
nb |
nb |
HR 1.14 (0.78-1.68) |
Ras, familieVG HVZ, roken, BMI, opleidingsniveau, DM, HT |
||
|
Hannaford, 1997 |
PIH/ PE (8) |
3000 |
18 451 |
13 |
F & NF IHZ |
69 |
216 |
RR 1.65 (1.26-2.16) |
Lft, roken en sociale klasse |
|
|
Haukkamaa, 2009 |
PE (1/2 + 4/12) |
35 |
489
|
nb |
NF IHZ |
2 |
29 |
RR 0.96 (0.24-3.87) |
Geen |
|
|
PIH (1/2) |
61 |
3 |
RR 0.83 (0.26-2.64) |
|||||||
|
PE en PIH |
96 |
5 |
RR 0.88 (0.36-2.14) |
|||||||
|
Irgens, 2001 |
PE ≥ 37 wk (8) |
21 506 |
576 099 |
13 |
F IHZ |
nb |
nb |
HR 1.65 (1.01-2.70) |
Lft en geboortejaar |
|
|
PE 16-36 wk (8) |
2649 |
HR 8.12 (4.31-15.33) |
||||||||
|
PE all |
24 155 |
HR 2.99 (2.02-4.42) |
||||||||
|
Jonsdottir, 1995 |
PIH/ PE (1/2 + 4) |
307 |
nb |
41.9 |
F IHZ |
39 |
26.5 |
RR 1.47 (1.05-2.02) |
Geen |
|
|
Lin, 2011 |
PE (7) |
nb |
nb |
Max 3 |
F & NF MI |
nb |
nb |
HR 13.0 (4.6-36.3) |
Lft, opleiding, gehuwd, gemelli, geslacht kind, geboortegewicht, pariteit, HT, anemie, DM, fluxus postpartum, SLE |
|
|
Lykke, 2009 |
PIH (7) |
7449 |
741 012
|
14.6
|
F/NF IHZ |
138 |
7727 |
HR 1.48 (1.25-1.76) |
Lft, jaar bevalling, vroeggeboorte, SGA, abruptio placentae, IUVD, DM II |
|
|
Milde PE (7) |
26 810 |
530 |
HR 1.57 (1.44-1.72) |
|||||||
|
Ernstige PE (7) |
7016 |
121 |
HR 1.61 (1.34-1.94) |
|||||||
|
PE (7) |
24 184 |
643 935 |
458 |
6086 |
HR 1.82 (1.65-2.00) |
Lft, jaar bevalling, abruptio placentae, IUVD |
||||
|
PIH en PE |
31 633 |
741 012 |
596 |
7727 |
HR 1.73 (1.59-1.88) |
Lft, jaar bevalling, vroeggeboorte, SGA, abruptio placentae, IUVD, DM II |
||||
|
Smith, 2001 |
PE (8) |
22781 |
107 139 |
15-19 |
F/NF IHZ |
nb |
nb |
HR 2.0 (1.5-2.5) |
Lft, lengte, socio-economische status, essentiële HT, laagste geboortegewicht quintiel, vroeggeboorte |
|
|
Wikstrom, 2005 |
PIH (7) |
7936 |
347 870 |
14.7 |
F/NF IHZ |
97 |
2306 |
RR 1.6 (1.3-2.0) |
Lft, socio-economische klasse |
|
|
Milde PE (7) |
9718 |
123 |
RR 1.9 (1.6-2.2) |
|||||||
|
Ernstige PE (7) |
2815 |
53 |
RR 2.8 (2.2-3.7) |
|||||||
|
PE |
12 533 |
176 |
RR 2.1 (1.8-2.4) |
|||||||
|
PE/PIH (7) |
20 469 |
273 |
RR (1.7 (1.5-2.0) |
|||||||
|
Onderzoeken met patiënten series waarin vrouwen met PIH/PE zijn vergeleken met vrouwen zonder PIH/PE |
||||||||||
|
Arnadottir 2005** |
PIH (1/2) & PE (1/2 + 9) |
325 |
629 |
50-55 |
F IHZ |
79 |
92 |
RR 1.66 (1.27-2.17) |
Geen |
|
|
≤ 64 jaar |
15 |
12 |
RR 2.4 (1.16-5.02 |
|||||||
|
≥ 65 jaar |
64 |
80 |
RR 1.5 (1.15-2.08) |
|||||||
|
E |
37 |
73 |
F IHZ |
13 |
4 |
RR 6.41 (2.25-18.30) |
||||
|
Ernstige PE (13) |
96 |
181 |
26 |
30 |
RR 1.63 (1.03-2.60) |
|||||
|
Milde PE (1/2 + 9) |
70 |
137 |
18 |
19 |
RR 1.85 (1.04-3.30) |
|||||
|
PIH (1/2) |
122 |
238 |
22 |
39 |
RR 1.10 (0.68-1.77) |
|||||
|
# berekend uit person-years Afkortingen: A = aangedaan door ziektebeeld; B = beroerte; BI = beroerte, ischemisch; BH = beroerte, hemorragisch; BMI = body mass index; DM = diabetes mellitus; DR = dysritmie; F = fataal; FU = follow-up; GDM = diabetes gravidarum; HT = hypertensie; HVZ = hart- en vaatziekten; IHZ = ischemische hartziekten; IUVD = intra-uteriene vruchtdood; MI = myocard infarct; NA = niet aangedaan door ziektebeeld; nb = niet bekend; NF = niet fataal; PE = pre-eclampsie; PIH = pregnancy induced hypertension/ zwangerschapshypertensie; SGA = small for gestational age; SLE = systemische lupus erythematodes; TE = thrombo-embolie; VG = voorgeschiedenis; VTE = veneuze thrombo-embolie
Definitie zwangerschapshypertensie en PE: 1. systolische bloeddruk ≥140 mmHg, twee x gemeten; 2. Diastolische bloeddruk ≥90 mmHg, twee x gemeten; 3. diastolische bloeddruk ≥110 mmHg, één x gemeten; 4. proteïnurie ≥0.3 gr/24 uur; 5. oedeem; 6. anamnestisch hypertensieve zwangerschap; 7. ICD code; 8. hypertensie niet nader gespecificeerd; 9. proteïnurie niet nader gespecificeerd; 10. systolische bloeddruk stijging ≥30 mmHg; 11. diastolische bloeddruk stijging ≥15 mmHg; 12. proteïnurie ≥1+dipstick; 13. Bloeddruk ≥160/110 mmHg met of zonder proteïnurie of bloeddruk ≥160/100 met proteïnurie; 14. Bloeddruk ≥160/105 mmHg eenmalig gemeten; 15. systolische bloeddruk ≥ 160 mmHg; 16. proteïnurie 3+ dipstick |
||||||||||
|
Tabel 4.1.3: risico’s op het krijgen van fatale en/of niet-fatale beroerte bij vrouwen met zwangerschapshypertensie en/of pre-eclampsie in de voorgeschiedenis vergeleken met vrouwen met een ongecompliceerde zwangerschap |
|||||||||
|
Artikel |
Ziekte beeld |
N |
Gem FU (jr) |
Uitkomst |
CV gebeurtenis (N) |
Gecorrigeerde risico’s (95% BI) |
Gecorrigeerd voor |
||
|
A |
NA |
A |
NA |
||||||
|
Cohort onderzoeken waarin vrouwen met PIH/PE zijn vergeleken met vrouwen zonder PIH/PE |
|||||||||
|
Bhattacharya, 2012 |
PIH (2/3) |
8891 |
23 937 |
34# |
F B |
117 |
266 |
IRR 1.28 (1.03-1.59) |
Geboortejaar, socio-economische klasse, roken |
|
PE (2/3+4) |
2026 |
29 |
IRR 1.27 (0.87-1.87) |
||||||
|
PIH/PE (2/3(+4) |
10 917 |
146 |
IRR 1.28 (1.06-1.55) |
||||||
|
PIH (2/3) |
8891 |
NF B |
361 |
1004 |
OR 1.04 (0.91-1.18) |
||||
|
PE (2/3+4) |
2026 |
94 |
OR 1.16 (0.93-1.45) |
||||||
|
Garovic, 2010 |
PIH/ PE (6) |
4720 |
nb |
NF B |
nb |
nb |
HR 1.86 (1.16-2.98) |
Ras, familieVG HVZ, roken, BMI, opleidingsniveau, DM, HT |
|
|
Hannaford, 1997 |
PIH/ PE (8) |
3000 |
18 451 |
13 |
F & NF B |
25 |
93 |
RR 1.39 (0.89-2.16) |
Leeftijd, roken en sociale klasse |
|
Irgens, 2001 |
PE ≥ 37 wk (8) |
21 506 |
576 099 |
13 |
F B |
nb |
nb |
HR 0.98 (0.50-1.91) |
Leeftijd en geboortejaar |
|
PE 16-36 wk (8) |
2649 |
nb |
HR 5.08 (2.09-12.35) |
||||||
|
PE all |
24 155 |
nb |
HR 1.77 (1.04-3.02) |
||||||
|
Lin, 2011 |
PE (7) |
nb |
nb |
Max 3 |
F & NF B |
nb |
nb |
HR 14.5 (1.3-165.1) |
Lft, opleiding, gehuwd, gemelli, geslacht kind, geboortegewicht, pariteit, HT, anemie, DM, fluxus postpartum, SLE |
|
Lykke, 2009 |
PIH (7) |
7449 |
741 012 |
14.6 |
F & NF B |
147 |
8240 |
HR 1.51 (1.26-1.81) |
Lft, jaar bevalling, vroeggeboorte, SGA, abruptio placentae, IUVD, DM II |
|
Milde PE (7) |
26 810 |
471 |
HR 1.43 (1.30-1.58) |
||||||
|
Ernstige PE (7) |
7016 |
129 |
HR 1.58 (1.23-2.03) |
||||||
|
PE (7) |
25 184 |
643 935 |
412 |
6555 |
HR 1.53 (1.38-1.69) |
Lft, jaar bevalling, abruptio placentae, IUVD |
|||
|
PE/PIH (7) |
32 633 |
741 012 |
560 |
8240 |
HR 1.46 (1.35-1.59) |
Lft, jaar bevalling, vroeggeboorte, SGA, abruptio placentae, IUVD, DM II |
|||
|
Wang, 2011 |
PIH/PE (7) ≥37 wk |
1092 |
4715 |
6.6 |
F & NF B |
Nb |
Nb |
HR 1.96 (0.98-3.91) |
Lft, woonomgeving, DM, dyslipidemie, IHZ, SLE, thrombofilie |
|
< 37 wk |
HR 3.22 (1.48-6.99) |
||||||||
|
PIH/PE all |
HR 2.44 (1.46-4.09) |
||||||||
|
Onderzoeken met patiënten series waarin vrouwen met PIH/PE zijn vergeleken met vrouwen zonder PIH/PE |
|||||||||
|
Arnadottir, 2005 |
PIH (1/2) & PE (1/2 + 9) |
325 |
629 |
50-55 |
F B |
31 |
41 |
RR 1.46 (0.94-2.28) |
Geen |
|
Nb |
Nb |
Nb |
F B ≤ 64 jaar |
13 |
3 |
RR 8.4 (2.58-27.28) |
|||
|
Nb |
Nb |
Nb |
F B ≥ 65 jaar |
18 |
38 |
RR 0.9 (0.53-1.57) |
|||
|
Spaan, 2009 |
PE (1/2 +4) |
22 |
29 |
23 |
NF B |
2 |
1 |
RR 2.64 (0.26-27.25) |
Geen |
|
Afkortingen: A = aangedaan door ziektebeeld; B = beroerte; BI = beroerte, ischemisch; BH = beroerte, hemorragisch; BMI = body mass index; DM = diabetes mellitus; DR = dysritmie; F = fataal; FU = follow-up; GDM = diabetes gravidarum; HT = hypertensie; HVZ = hart- en vaatziekten; IHZ = ischemische hartziekten; IUVD = intra-uteriene vruchtdood; MI = myocard infarct; NA = niet aangedaan door ziektebeeld; nb = niet bekend; NF = niet fataal; PE = pre-eclampsie; PIH = pregnancy induced hypertension/ zwangerschapshypertensie; SGA = small for gestational age; SLE = systemische lupus erythematodes; TE = thrombo-embolie; VG = voorgeschiedenis; VTE = veneuze thrombo-embolie
Definitie zwangerschapshypertensie en PE: 1. systolische bloeddruk ≥140 mmHg, twee x gemeten; 2. Diastolische bloeddruk ≥90 mmHg, twee x gemeten; 3. diastolische bloeddruk ≥110 mmHg, één x gemeten; 4. proteïnurie ≥0.3 gr/24 uur; 5. oedeem; 6. anamnestisch hypertensieve zwangerschap; 7. ICD code; 8. hypertensie niet nader gespecificeerd; 9. proteïnurie niet nader gespecificeerd; 10. systolische bloeddruk stijging ≥30 mmHg; 11. diastolische bloeddruk stijging ≥15 mmHg; 12. proteïnurie ≥1+dipstick; 13. Bloeddruk ≥160/110 mmHg met of zonder proteïnurie of Bloeddruk ≥160/100 met proteïnurie; 14. Bloeddruk ≥160/105 mmHg eenmalig gemeten |
|||||||||
|
Tabel 4.1.4a: risico’s op het ontwikkelen van hypertensie bij vrouwen met pre-eclampsie in de voorgeschiedenis vergeleken met vrouwen met een ongecompliceerde zwangerschap |
|||||||||||||
|
Studie |
Definitie PE
|
N |
Gem FU (jr) |
Gem. lft bij FU |
Definitie HT
|
Aantal vrouwen met HT (N) |
Gecorrigeerde risico (95% BI) |
Gecorrigeerd voor |
|||||
|
A |
NA |
A |
NA |
A |
NA |
||||||||
|
Cohort onderzoeken waarin vrouwen met PE zijn vergeleken met vrouwen zonder PE |
|||||||||||||
|
Bhattacharya, 2012 |
2/3 +4 |
2026 |
23 937 |
34# |
NA |
NA |
V |
290 |
2260 |
OR 1.79 (1.55-2.05) |
Geboortejaar, socio-economische klasse, roken |
||
|
Haukkamaa, 2009 |
7 |
35 |
489 |
nb |
57.2 |
57.2 |
nb |
15 |
137 |
RR 1.53 (1.02-2.30) |
Geen |
||
|
Lykke, 2009 |
Milde PE (7) |
26 810 |
741 012 |
14.6 |
41.6 |
V |
2126 |
14 762 |
HR 3.61 (3.43-3.80) |
Lft, jaar bevalling, vroeggeboorte, SGA, abruptio placentae, IUVD, DM II |
|||
|
Ernstige PE (7) |
7016 |
741 012 |
14.6 |
41.6 |
V |
793 |
14 762 |
HR 6.07 (5.45-6.77) |
Lft, jaar bevalling, vroeggeboorte, SGA, abruptio placentae, IUVD, DM II |
||||
|
PE (7) |
25 184 |
643 935 |
14.6 |
41.6 |
V |
1958 |
12 234 |
HR 4.07 (3.88-4.27) |
Lft, jaar bevalling, abruptio placentae, IUVD |
||||
|
Magnussen, 2009 |
1/ 2 + 4 |
661 |
14 404 |
16.5 |
40.1 |
39.9 |
II |
Nb |
Nb |
OR 3.1 (2.2-4.3) |
Lft, opleidingsniveau, roken, socio-economische status |
||
|
Onderzoeken met patiënten series waarin vrouwen met PE zijn vergeleken met vrouwen zonder PE |
|||||||||||||
|
Adams, 1961 |
2 + 4 |
53 |
185 |
16.9 |
41.6 |
42.0 |
III |
23 |
48 |
RR 1.67 (1.13-2.48) |
Geen |
||
|
Berends, 2008 |
1/2 + 4 |
50 |
106 |
7 |
36.2 |
39.2 |
II/III/ IV |
23 |
9 |
RR 5.42 (2.71-10.84) |
Geen |
||
|
Canti, 2010 |
8 + 9 |
40 |
14 |
15.9 |
39.2 |
37.2 |
nb |
6 |
1 |
RR 2.10 (0.28-15.95) |
Geen |
||
|
Drost, 2012 |
2 + 4 (AD 20-32) |
339 |
332 |
10 |
38.9 |
39.3 |
II/III /IV |
146 |
57 |
OR 3.59 (2.48-5.20) |
Lft, FU-duur en roken |
||
|
Epstein, 1964 |
5 + 8 + 9 |
48 |
114 |
15 |
45 |
45 |
BD >150/ 90 mmHg |
37 |
7 |
RR 12.55 (6.03-26.16) |
Geen |
||
|
Gaugler, 2008 |
(3/15) / (1/2+ 4) & E/HELLP ≤24 wk |
20 |
20 |
5.5 |
38.8 |
37.7 |
II/III /IV |
11 |
2 |
RR 5.50 (1.39-21.71) |
Geen |
||
|
Lazdam, 2012 |
1/2 + 4 |
90 |
50 |
9.75 |
40 |
40 |
nb |
8 |
0 |
RR 9.53 (0.56-161.69) |
Geen |
||
|
Marin, 2000 |
1/ 2 + 4 |
80 |
86 |
13.6-16.2 |
41.9 |
42.3 |
II/III/ IV |
38 |
14 |
OR 3.7 (1.7-7.9) |
Geen |
||
|
Nisell, 1995 |
1/ 2 + 4 |
45 |
44 |
7 |
36 |
37 |
II/IV |
20 |
2 |
RR 9.78 (2.43-39.37) |
Geen |
||
|
North, 1996 |
1/ 2 + 4 |
50 |
50 |
5 |
30 |
30 |
II/III/ IV |
20 |
1 |
RR 20.00 (2.79- 143.38)
|
Geen |
||
|
Portelinha, 2010 |
1/ 2 + 4 |
90 |
60 |
6 |
34 |
34 |
II |
28 |
2 |
RR 9.33 (2.31-37.73) |
Geen |
||
|
Sattar, 2003 |
2 +4 |
40 |
40 |
20 |
43 |
44 |
II |
7 |
2 |
RR 3.50 (0.77-15.83) |
Geen |
||
|
Shahbazian, 2011 |
1/ 2 + 4 |
35 |
35 |
5.7 |
32 |
31 |
II/III/ IV |
10 |
1 |
RR 10.0 (1.35-74.0) |
Geen |
||
|
Sibai, 1986 |
3/15 + 11 |
406 |
409 |
6.6-8.0 |
25 |
26 |
V |
60 |
23 |
RR 2.63 (1.66-4.17) |
Geen |
||
|
Spaan, 2009 |
1/2 +4 |
22 |
29 |
23 |
49.0 |
49.8 |
II/III/ IV |
12 |
2 |
RR 7.91 (1.97-31.77) |
Geen |
||
|
Svensson, 1983 |
1/2 +4 |
145 |
46 |
7-12 |
Nb |
Nb |
III/IV |
36 |
1 |
RR 11.42 (1.61-81.01) |
Geen |
||
|
Wilson, 2003 |
1/2 +4 |
443 |
206 |
nb |
60 |
60 |
II |
129 |
25 |
OR 2.77 (1.72-4.47) |
Leeftijd, BMI, sociale klasse, roken |
||
|
Afkortingen: A = aangedaan door ziektebeeld; B = beroerte; BI = beroerte, ischemisch; BH = beroerte, hemorragisch; BMI = body mass index; DM = diabetes mellitus; DR = dysritmie; F = fataal; FU = follow-up; GDM = diabetes gravidarum; HT = hypertensie; HVZ = hart- en vaatziekten; IHZ = ischemische hartziekten; IUVD = intra-uteriene vruchtdood; MI = myocard infarct; NA = niet aangedaan door ziektebeeld; nb = niet bekend; NF = niet fataal; PE = pre-eclampsie; PIH = pregnancy induced hypertension/ zwangerschapshypertensie; SGA = small for gestational age; SLE = systemische lupus erythematodes; TE = thrombo-embolie; VG = voorgeschiedenis; VTE = veneuze thrombo-embolie Definitie PE: 1. systolische bloeddruk ≥140 mmHg, twee x gemeten; 2. Diastolische bloeddruk ≥90 mmHg, twee x gemeten; 3. diastolische bloeddruk ≥110 mmHg, één x gemeten; 4. proteïnurie ≥0.3 gr/24 uur; 5. oedeem; 6. anamnestisch hypertensieve zwangerschap; 7. ICD code; 8. hypertensie niet nader gespecificeerd; 9. proteïnurie niet nader gespecificeerd; 10. systolische bloeddruk stijging ≥30 mmHg; 11. diastolische bloeddruk stijging ≥15 mmHg; 12. proteïnurie ≥1+dipstick; 13. Bloeddruk ≥160/110 mmHg met of zonder proteïnurie of bloeddruk ≥160/100 met proteïnurie; 14. Bloeddruk ≥160/105 mmHg eenmalig gemeten; 15. systolische bloeddruk ≥ 160 mmHg; 16. proteïnurie 3+ dipstick Definitie hypertensie: I zelfrapportage; II medicatie gebruik; III systolische bloeddruk ≥140 mmHg; IV diastolische bloeddruk ≥90 mmHg; V ICD code |
|
||||||||||||
|
Tabel 4.1.4b: risico’s op het ontwikkelen van hypertensie bij vrouwen met een zwangerschapshypertensie en/of pre-eclampsie in de voorgeschiedenis vergeleken met vrouwen met een ongecompliceerde zwangerschap |
|||||||||||
|
Studie |
Definitie A |
N |
Gem FU (jr) |
Gem lft FU |
Definitie HT
|
Aantal vrouwen met HT (N) |
Gecorrigeerde risico (95% BI) |
Gecorrigeerd voor |
|||
|
A |
NA |
A |
NA |
A |
NA |
||||||
|
Cohort onderzoeken waarin vrouwen met PE en/of PIH zijn vergeleken met vrouwen zonder PE/PIH |
|||||||||||
|
Callaway, 2011 |
2 (+ 5/9) |
191 |
1921 |
21 |
46.41 |
46.41 |
II/III/ IV |
62 |
280 |
OR 4.09 (2.76-6.07) |
Geen |
|
Cassidy, 2009 |
6 |
52 |
446 |
27 |
60.6 |
63.6 |
II/III/ IV |
29 |
201 |
RR 1.24 (0.95-1.61) |
Geen |
|
Garovic, 2010 |
6 |
643 |
3421 |
nb |
53.5 |
II/III/ IV |
370 |
1362 |
RR 1.45 (1.34-1.56) |
Geen |
|
|
Hannaford, 1997 |
8 |
3000 |
18 451 |
13 |
nb |
V |
377 |
922 |
RR 2.35 (2.08-2.65) |
Lft, roken en sociale klasse |
|
|
Kharazmi, 2007 |
6 |
131 |
2834 |
nb |
nb |
III/IV |
30 |
497 |
OR 1.80 (1.07-3.04) |
Leeftijd |
|
|
Magnussen, 2009 |
1/2 (+ 4) |
1433 |
13 632 |
16.5 |
40.1 |
39.9 |
II |
138 |
303 |
RR 4.33 (3.57-5.26)
|
Geen |
|
Shalom, 2013 |
1/2 (+4) |
2072 |
20 742 |
>10 |
Nb |
Nb |
V |
Nb |
Nb |
OR 15.8 (12.9-19.3) |
Geen |
|
Onderzoeken met patiënten series waarin vrouwen met PE en/of PIH zijn vergeleken met vrouwen zonder PIH |
|||||||||||
|
Edlow, 2009 |
1/2/14 |
79 |
140 |
0.6 |
26.6 |
28.3 |
I/II |
33 |
10 |
OR 13.92 (5.2-37.4) |
Ras, BMI, pariteit, chronische HT |
|
Lindeberg, 1988 |
2 |
49 |
49 |
5 |
30 |
30 |
II/IV |
21 |
2 |
RR 10.50 (2.60-42.38 |
Geen |
|
Marin, 2000 |
1/2 (+ 4) |
205 |
86 |
13.6-16.2 |
41.9 |
42.3 |
I/III/ IV |
92 |
12 |
OR 5.1 (2.4-9.8) |
Ja, alleen niet beschreven waarvoor |
|
Nissel, 1995 |
1/ 2 (+ 4 |
94 |
44 |
7 |
36 |
37 |
II/IV |
57 |
2 |
RR 13.34 (3.41-52.17) |
Geen |
|
Svensson, 1983 |
1/2 +4 |
237 |
46 |
7-12 |
Nb |
Nb |
III/IV |
62 |
1 |
RR 12.03 (1.71-84.61) |
Geen |
|
Afkortingen: A = aangedaan door ziektebeeld; B = beroerte; BI = beroerte, ischemisch; BH = beroerte, hemorragisch; BMI = body mass index; DM = diabetes mellitus; DR = dysritmie; F = fataal; FU = follow-up; GDM = diabetes gravidarum; HT = hypertensie; HVZ = hart- en vaatziekten; IHZ = ischemische hartziekten; IUVD = intra-uteriene vruchtdood; MI = myocard infarct; NA = niet aangedaan door ziektebeeld; nb = niet bekend; NF = niet fataal; PE = pre-eclampsie; PIH = pregnancy induced hypertension/ zwangerschapshypertensie; SGA = small for gestational age; SLE = systemische lupus erythematodes; TE = thrombo-embolie; VG = voorgeschiedenis; VTE = veneuze thrombo-embolie
Definitie zwangerschapshypertensie en PE: 1. systolische bloeddruk ≥140 mmHg, twee x gemeten; 2. Diastolische bloeddruk ≥90 mmHg, twee x gemeten; 3. diastolische bloeddruk ≥110 mmHg, één x gemeten; 4. proteïnurie ≥0.3 gr/24 uur; 5. oedeem; 6. anamnestisch hypertensieve zwangerschap; 7. ICD code; 8. hypertensie niet nader gespecificeerd; 9. proteïnurie niet nader gespecificeerd; 10. systolische bloeddruk stijging ≥30 mmHg; 11. diastolische bloeddruk stijging ≥15 mmHg; 12. proteïnurie ≥1+dipstick; 13. Bloeddruk ≥160/110 mmHg met of zonder proteïnurie of bloeddruk ≥160/100 met proteïnurie; 14. Bloeddruk ≥160/105 mmHg eenmalig gemeten; 15. systolische bloeddruk ≥ 160 mmHg; 16. proteïnurie 3+ dipstick
Definitie hypertensie: I zelfrapportage; II medicatie gebruik; III systolische bloeddruk ≥140 mmHg; IV diastolische bloeddruk ≥90 mmHg; V ICD code |
|||||||||||
|
Tabel 4.1.4c: risico’s op het ontwikkelen van hypertensie bij vrouwen met een zwangerschapshypertensie in de voorgeschiedenis vergeleken met vrouwen met een ongecompliceerde zwangerschap |
||||||||||||
|
Studie |
Definitie PIH |
N |
Gem FU (jr) |
Gem lft FU |
Definitie HT
|
Aantal vrouwen met HT (N) |
Gecorrigeerde risico (95% BI) |
Gecorrigeerd voor |
||||
|
A |
NA |
A |
NA |
A |
NA |
|||||||
|
Cohort onderzoeken waarin vrouwen met PIH zijn vergeleken met vrouwen zonder PIH |
||||||||||||
|
Bhattacharya, 2012 |
2/3 |
8891 |
23 937 |
34# |
NA |
NA |
V |
1201 |
2260 |
OR 1.68 (1.55-1.82) |
Geboortejaar, socio-economische klasse, roken |
|
|
Haukkamaa, 2009 |
7 |
61 |
489 |
nb |
55.0 |
57.2 |
nb |
26 |
137 |
RR 1.52 (1.10-2.10) |
Geen |
|
|
Lykke, 2009 |
7 |
7449 |
741 012 |
14.6 |
41.6 |
V |
870 |
14 762 |
HR 5.31 (4.90-5.75) |
Lft, jaar bevalling, vroeggeboorte, SGA, abruptio placentae, IUVD, DM II |
||
|
Onderzoeken met patiënten series waarin vrouwen met PIH zijn vergeleken met vrouwen zonder PIH |
||||||||||||
|
Adams, 1961 |
2 |
96 |
185 |
17.6 |
41.6 |
42.0 |
III |
56 |
48 |
RR 2.25 (1.67-3.02) |
Geen |
|
|
Marin, 2000 |
1/2 |
111 |
86 |
13.6-16.2 |
41.9 |
42.3 |
I/III/IV |
54 |
14 |
OR 7.2 (3.5-14.8) |
Geen |
|
|
Nissel, 1995 |
1/2/3 |
49 |
44 |
7 |
37 |
37 |
II/IV |
37 |
2 |
RR 16.61 (4.25-64.94) |
Geen |
|
|
Svensson, 1983 |
1/2 |
92 |
46 |
7-12 |
Nb |
Nb |
III/IV |
26 |
1 |
RR 13.00 (1.82-92.82) |
Geen |
|
|
Wilson, 2003 |
2/3 |
343 |
206 |
nb |
60 |
60 |
II |
80 |
25 |
OR 1.95 (1.18-3.24) |
Lft, BMI, sociale klasse, roken |
|
|
Afkortingen: A = aangedaan door ziektebeeld; B = beroerte; BI = beroerte, ischemisch; BH = beroerte, hemorragisch; BMI = body mass index; DM = diabetes mellitus; DR = dysritmie; F = fataal; FU = follow-up; GDM = diabetes gravidarum; HT = hypertensie; HVZ = hart- en vaatziekten; IHZ = ischemische hartziekten; IUVD = intra-uteriene vruchtdood; MI = myocard infarct; NA = niet aangedaan door ziektebeeld; nb = niet bekend; NF = niet fataal; PE = pre-eclampsie; PIH = pregnancy induced hypertension/ zwangerschapshypertensie; SGA = small for gestational age; SLE = systemische lupus erythematodes; TE = thrombo-embolie; VG = voorgeschiedenis; VTE = veneuze thrombo-embolie Definitie zwangerschapshypertensie en PE: 1. systolische bloeddruk ≥140 mmHg, twee x gemeten; 2. Diastolische bloeddruk ≥90 mmHg, twee x gemeten; 3. diastolische bloeddruk ≥110 mmHg, één x gemeten; 4. proteïnurie ≥0.3 gr/24 uur; 5. oedeem; 6. anamnestisch hypertensieve zwangerschap; 7. ICD code; 8. hypertensie niet nader gespecificeerd; 9. proteïnurie niet nader gespecificeerd; 10. systolische bloeddruk stijging ≥30 mmHg; 11. diastolische bloeddruk stijging ≥15 mmHg; 12. proteïnurie ≥1+dipstick; 13. Bloeddruk ≥160/110 mmHg met of zonder proteïnurie of bloeddruk ≥160/100 met proteïnurie; 14. Bloeddruk ≥160/105 mmHg eenmalig gemeten; 15. systolische bloeddruk ≥ 160 mmHg; 16. proteïnurie 3+ dipstick Definitie hypertensie: I zelfrapportage; II medicatie gebruik; III systolische bloeddruk ≥140 mmHg; IV diastolische bloeddruk ≥90 mmHg; V ICD code |
||||||||||||
|
Tabel 4.1.5: risico’s op het ontwikkelen van diabetes mellitus bij vrouwen met zwangerschapshypertensie en/of pre-eclampsie in de voorgeschiedenis vergeleken met vrouwen met een ongecompliceerde zwangerschap |
|||||||||||||||
|
Studie |
Definitie PIH/PE
|
N |
Gem FU (jr) |
Gem lft FU |
Definitie DM
|
Aantal vrouwen met DM (N) |
Gecorrigeerde risico (95% BI) |
Gecorrigeerd voor |
|||||||
|
A |
NA |
A |
NA |
A |
NA |
||||||||||
|
Cohort onderzoeken waarin vrouwen met PE/PIH zijn vergeleken met vrouwen zonder PE/PIH |
|||||||||||||||
|
Callaway, 2007 |
PE (2 + 4/5) |
333 |
3306 |
21 |
nb |
nb |
I |
51 |
244 |
OR 1.71 (1.19-2.47) |
Lft, pariteit, roken, inkomen, fysieke activiteit en BMI |
||||
|
Carr, 2009 |
PE (7) |
2032 |
29 431 |
8.2 |
nb |
nb |
III/IV/V |
33 |
309 |
HR 1.82 (1.38-2.83) |
Lft, primigravida, GDM |
||||
|
Cassidy, 2009 |
PE/PIH (6) |
52 |
446 |
27 |
60.6 |
63.6 |
I/II |
8 |
27 |
RR 2.54 (1.22-5.30) |
Geen |
||||
|
England, 2011 |
PE (1/2 + 4/12) |
8646 |
215 988 |
3.7 |
Nb |
Nb |
II |
Nb |
nb |
RR 3.0 (2.4-3.6) |
Geen |
||||
|
Garovic, 2010 |
PE/PIH (6) |
643 |
3421 |
nb |
53.5 |
I |
164 |
616 |
RR 1.42 (1.22-1.65) |
Geen |
|||||
|
Lazdam, 2012 |
PE (1/2 + 4) |
90 |
50 |
9.75 |
40 |
Nb |
2 |
0 |
RR 2.80 (0.14-57.25) |
Geen- |
|||||
|
Libby, 2006 |
PE (2/ 9) |
810 |
6377 |
46 |
71 |
71 |
VI |
107 |
638 |
OR 1.40 (1.12-1.75) |
Geboortegewicht, lft. en socio-economische status |
||||
|
Lykke, 2009 |
PIH (7) |
26 810 |
741 012 |
14.6 |
41.6
|
V |
197 |
5604 |
HR 3.12 (2.63-3.70) |
Lft, jaar bevalling, vroeggeboorte, SGA, abruptio placentae, IUVD Lft, jaar bevalling, abruptio placentae, IUVD |
|||||
|
Milde PE (7) |
26 810 |
742 |
HR 3.53 (3.23-3.85) |
||||||||||||
|
Ernstige PE (7) |
7016 |
177 |
HR 3.68 (3.04-4.46) |
||||||||||||
|
PE (7) |
25 184 |
643 935 |
670 |
4531 |
HR 3.63 (3.34-3.93) |
||||||||||
|
PE en PIH |
51 994 |
741 012 |
867 |
5604 |
HR 3.53 (3.29-3.80) |
||||||||||
|
Magnussen, 2009 |
PE (1/2 + 4) |
661 |
14 404 |
16.5 |
40.1 |
39.9 |
VII |
nb |
nb |
OR 2.8 (1.6-5.0) |
Lft, opleidingsniveau, roken, socio-economische status, BMI |
||||
|
PIH (1/2) |
321 |
14 404 |
OR 0.9 (0.2-3.8) |
||||||||||||
|
PE en PIH |
982 |
14 404 |
OR 2.38 (1.38-4.11) |
||||||||||||
|
Onderzoeken met patiënten series waarin vrouwen met PE/PIH zijn vergeleken met vrouwen zonder PE/PIH |
|||||||||||||||
|
Berends, 2008 |
PE (1/2 + 4) |
50 |
106 |
7 |
36.2 |
39.2 |
nb |
2 |
0 |
RR 10.49 (0.51-214.53) |
Geen |
||||
|
Drost, 2012 |
PE (2 + 3) (AD 20-32) |
339 |
332 |
10 |
38.9 |
39.3 |
II/III |
8 |
5 |
OR 1.72 (0.54-5.48) |
Lft, FU en roken |
||||
|
Edlow, 2009 |
PE/PIH (1/2 / 3 + 9) |
79 |
140 |
0.6 |
26.6 |
28.3 |
I/II |
6 |
5 |
OR 1.84 (0.5-6.5) |
Ras, BMI, pariteit |
||||
|
Lazdam, 2012 |
PE (1/2 + 4) |
90 |
50 |
9.75 |
40 |
Nb |
2 |
0 |
RR 2.80 (0.14-57.25) |
Geen- |
|||||
|
Marin, 2000 |
PE/PIH (1/2 + 3) |
205 |
86 |
13.6-16.2 |
41.9 |
42.3 |
I/III |
4 |
2 |
RR 0.84 (0.16-4.50) |
Geen |
||||
|
Sibai, 1986 |
PE (3+16) |
406 |
409 |
6.6-8.0 |
25 |
26 |
VII |
7 |
6 |
RR 1.18 (0.40-3.47) |
Geen |
||||
|
Afkortingen: A = aangedaan door ziektebeeld; B = beroerte; BI = beroerte, ischemisch; BH = beroerte, hemorragisch; BMI = body mass index; DM = diabetes mellitus; DR = dysritmie; F = fataal; FU = follow-up; GDM = diabetes gravidarum; HT = hypertensie; HVZ = hart- en vaatziekten; IHZ = ischemische hartziekten; IUVD = intra-uteriene vruchtdood; MI = myocard infarct; NA = niet aangedaan door ziektebeeld; nb = niet bekend; NF = niet fataal; PE = pre-eclampsie; PIH = pregnancy induced hypertension/ zwangerschapshypertensie; SGA = small for gestational age; SLE = systemische lupus erythematodes; TE = thrombo-embolie; VG = voorgeschiedenis; VTE = veneuze thrombo-embolie
Definitie zwangerschapshypertensie en PE: 1. systolische bloeddruk ≥140 mmHg, twee x gemeten; 2. Diastolische bloeddruk ≥90 mmHg, twee x gemeten; 3. diastolische bloeddruk ≥110 mmHg, één x gemeten; 4. proteïnurie ≥0.3 gr/24 uur; 5. oedeem; 6. anamnestisch hypertensieve zwangerschap; 7. ICD code; 8. hypertensie niet nader gespecificeerd; 9. proteïnurie niet nader gespecificeerd; 10. systolische bloeddruk stijging ≥30 mmHg; 11. diastolische bloeddruk stijging ≥15 mmHg; 12. proteïnurie ≥1+dipstick; 13. Bloeddruk ≥160/110 mmHg met of zonder proteïnurie of bloeddruk ≥160/100 met proteïnurie; 14. Bloeddruk ≥160/105 mmHg eenmalig gemeten; 15. systolische bloeddruk ≥ 160 mmHg; 16. proteïnurie 3+ dipstick
Definitie DM: I zelfrapportage; II medicatie gebruik; III nuchtere glucose ≥ 7.0 mmol/l; IV random glucose ≥ 11.1 mmol/l; V ICD-9 codes; VI WHO criteria; VII = onbekend; H medisch dossier
|
|||||||||||||||
|
Tabel 4.1.6: risico’s op het ontwikkelen van dyslipidemie bij vrouwen met zwangerschapshypertensie en/of pre-eclampsie in de voorgeschiedenis vergeleken met vrouwen met een ongecompliceerde zwangerschap |
|||||||||||
|
Studie |
Definitie PIH/PE
|
N |
Gem FU (jr) |
Gem lft FU |
Definitie dyslip |
Aantal met dyslipidemie (N) |
Gecorrigeerde risico (95% BI) |
Gecorrigeerd voor |
|||
|
A |
NA |
A |
NA |
A |
NA |
||||||
|
Cohort onderzoeken waarin vrouwen met PE/PIH zijn vergeleken met vrouwen zonder PE/PIH |
|||||||||||
|
Garovic, 2010 |
PE/PIH (6) |
643 |
3421 |
nb |
53.5 |
II/III/ IV/V |
463 |
2634 |
OR 0.77 (0.64-0.93) |
Geen |
|
|
Onderzoeken met patiënten series waarin vrouwen met PE/PIH zijn vergeleken met vrouwen zonder PE/PIH |
|||||||||||
|
Drost, 2012 |
PE (2 + 4) |
339 |
332 |
10 |
38.9 |
39.3 |
II/III |
131 |
141 |
OR 0.94 (0.68-1.30) |
Lft., FU-duur en roken |
|
Edlow, 2009 |
PE/PIH (1/2/3 + 9) |
79 |
140 |
0.6 |
26.6 |
28.3 |
I/II |
6 |
4 |
OR 3.12 (0.81-12.0) |
Ras, BMI, pariteit |
|
Marin, 2000 |
PE/PIH (1/2 + 4) |
205 |
86 |
13.6-16.2 |
41.9 |
42.3 |
VI |
45 |
19 |
RR 0.99 (0.62-1.60) |
Geen |
|
Sattar, 2003 |
PE (2 + 4) |
40 |
40 |
20 |
43 |
44 |
II |
2 |
0 |
RR 5.00 (0.25-100.97) |
Geen |
|
Afkortingen: A = aangedaan door ziektebeeld; B = beroerte; BI = beroerte, ischemisch; BH = beroerte, hemorragisch; BMI = body mass index; DM = diabetes mellitus; DR = dysritmie; F = fataal; FU = follow-up; GDM = diabetes gravidarum; HT = hypertensie; HVZ = hart- en vaatziekten; IHZ = ischemische hartziekten; IUVD = intra-uteriene vruchtdood; MI = myocard infarct; NA = niet aangedaan door ziektebeeld; nb = niet bekend; NF = niet fataal; PE = pre-eclampsie; PIH = pregnancy induced hypertension/ zwangerschapshypertensie; SGA = small for gestational age; SLE = systemische lupus erythematodes; TE = thrombo-embolie; VG = voorgeschiedenis; VTE = veneuze thrombo-embolie Definitie zwangerschapshypertensie en PE: 1. systolische bloeddruk ≥140 mmHg, twee x gemeten; 2. Diastolische bloeddruk ≥90 mmHg, twee x gemeten; 3. diastolische bloeddruk ≥110 mmHg, één x gemeten; 4. proteïnurie ≥0.3 gr/24 uur; 5. oedeem; 6. anamnestisch hypertensieve zwangerschap; 7. ICD code; 8. hypertensie niet nader gespecificeerd; 9. proteïnurie niet nader gespecificeerd; 10. systolische bloeddruk stijging ≥30 mmHg; 11. diastolische bloeddruk stijging ≥15 mmHg; 12. proteïnurie ≥1+dipstick; 13. Bloeddruk ≥160/110 mmHg met of zonder proteïnurie of bloeddruk ≥160/100 met proteïnurie; 14. Bloeddruk ≥160/105 mmHg eenmalig gemeten; 15. systolische bloeddruk ≥ 160 mmHg; 16. proteïnurie 3+ dipstick Definitie dyslipidemie: I zelfrapportage; II medicatie gebruik; III cholesterol ≥5.0 mmol/l ; IV triglyceriden ≥1.7 mmol/l; V HDL ≤1.0 mmol/l; VI Totaal cholesterol ≥6.2 mmol/l |
|||||||||||
Beoordelingsdatum en geldigheid
Publicatiedatum : 29-04-2015
Beoordeeld op geldigheid : 02-03-2023
Omdat deze richtlijn modulair is opgebouwd, kan herziening op onderdelen eenvoudig plaatsvinden.
De richtlijn zal waarschijnlijk in 2016 al voor de eerste keer worden herzien, als nieuwe gegevens van ten tijde van de richtlijnontwikkeling lopende studies beschikbaar komen. De geldigheid van de richtlijn komt eerder te vervallen indien nieuwe ontwikkelingen aanleiding zijn om een herzieningstraject te starten.
De Nederlandse Vereniging voor Obstetrie en Gynaecologie is als houder van deze richtlijn de eerstverantwoordelijke voor de actualiteit van deze richtlijn. De andere aan deze richtlijn deelnemende wetenschappelijk verenigingen of gebruikers van de richtlijn delen de verantwoordelijkheid en informeren de eerstverantwoordelijke over relevante ontwikkelingen binnen hun vakgebied.
Algemene gegevens
Deze richtlijn is tot stand gekomen met ondersteuning van de Afdeling Ondersteuning Professionele Kwaliteit van de Orde van Medisch Specialisten en met financiële steun van SKMS.
INITIATIEF
Nederlandse Vereniging voor Obstetrie en Gynaecologie
IN SAMENWERKING MET
Nederlands Huisartsen Genootschap
Nederlandse Vereniging voor Cardiologie
Nederlandse Internisten Vereniging
Nederlandse Vereniging voor Neurologie
Nederlandse Vereniging voor Radiologie
MET ONDERSTEUNING VAN
Orde van Medisch Specialisten
FINANCIERING
De richtlijnontwikkeling werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS)
Doel en doelgroep
Doelstelling
Het doel van deze richtlijn is (a) inventariseren van de beschikbare kennis over cardiovasculaire risicofactoren en het risico op cardiovasculaire morbiditeit en mortaliteit bij vrouwen met in het verleden opgetreden of vastgestelde reproductieve aandoeningen (zwangerschapshypertensie, pre-eclampsie, herhaald miskraam, vroeggeboorte, groeibeperkt kind, PCOS en/of POI); (b) opstellen van aanbevelingen voor multidisciplinair cardiovasculair risicomanagement (diagnostiek en therapie) op maat bij deze vrouwen, zoveel mogelijk aansluitend bij de bestaande NHG standaard CVRM; (c) ontwikkelen van consensus over de taakverdeling tussen de verschillende disciplines die betrokken zijn bij dit cardiovasculair risicomanagement, alsmede over indicaties voor doorverwijzing, aangezien dit buiten het traditionele kennisgebied van de gynaecoloog valt; en (d) identificeren van belangrijke hiaten in de huidige kennis op dit gebied.
Patiëntencategorie
De richtlijn geldt voor: (a) alle vrouwen die een zwangerschap hebben doorgemaakt die werd gecompliceerd door zwangerschapshypertensie, pre-eclampsie, vroeggeboorte of groeibeperkt kind; (b) vrouwen met een herhaalde miskraam, prematuur ovariële insufficiëntie of polycysteus ovarium syndroom.
Doelgroep en gebruikers
De richtlijn beoogt zorgverleners die betrokken zijn bij de zorg voor vrouwen met een doorgemaakte of aanwezige reproductieve aandoening (zwangerschapshypertensie, pre-eclampsie, vroeggeboorte, intra-uteriene groeivertraging, herhaald miskraam, prematuur ovariële insufficiëntie en polycysteus ovarium syndroom) zoals gynaecologen, huisartsen, (vasculair) internisten, cardiologen, radiologen en neurologen te voorzien van een landelijke, door alle betrokken beroepsverenigingen gedragen richtlijn. Deze richtlijn voldoet aan de eisen van een AGREE-instrument volgens de EBRO-methode en geeft inzicht in de huidige kennis over het cardiovasculaire risico van vrouwen met zwangerschapshypertensie, pre-eclampsie, vroeggeboorte, intra-uteriene groeivertraging, herhaald miskraam, prematuur ovariële insufficiëntie en polycysteus ovarium syndroom. Ook geeft de richtlijn aanbevelingen voor adequate diagnostiek van verhoogd risico en voor behandeling van deze vrouwen. De richtlijn voorziet in de meest recente 'evidencebased' informatie en beoogt de onduidelijkheid en onzekerheid te verminderen over cardiovasculair risicomanagement bij vrouwen met een reproductieve aandoening.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijn is in 2012 een multidisciplinaire werkgroep ingesteld bestaande uit vertegenwoordigers van de relevante beroepsgroepen die betrokken zijn bij het zorgproces in de eerste, tweede en derde lijn van vrouwen met zwangerschapshypertensie, pre-eclampsie, vroeggeboorte, groeibeperkt kind, herhaald miskraam, primair ovariële insufficiëntie en polycysteus ovarium syndroom. Deze beroepsgroepen zijn de Nederlandse Vereniging voor Obstetrie & Gynaecologie (NVOG), het Nederlands Huisartsen Genootschap (NHG), de Nederlandse Vereniging voor Radiologie (NVvR), de Nederlandse Internisten Vereniging (NIV) en de Nederlandse Vereniging voor Cardiologie (NVvC). De werkgroepleden (zie samenstelling van de werkgroep op pagina 3) waren door de bovengenoemde wetenschappelijke verenigingen gemandateerd voor deelname aan deze werkgroep. De werkgroepleden zijn gezamenlijk verantwoordelijk voor de integrale tekst van deze conceptrichtlijn. De Nederlandse Vereniging voor Neurologie (NVN) en patiëntenvereniging Stichting HELLP-syndroom hadden geen zitting in de werkgroep maar zijn wel geraadpleegd bij de ontwikkeling.
- Dhr. A. Franx, gynaecoloog, Universitair Medisch Centrum Utrecht, Utrecht (voorzitter)
- Dhr. M.L. Bots, arts-epidemioloog, Julius Centrum voor Gezondheidswetenschappen en Eerstelijns Geneeskunde, Utrecht
- Mw. M. Cohen, huisarts, Amsterdam
- Mw. F.M. van Dunné, gynaecoloog, Medisch Centrum Haaglanden, Den Haag
- Mw. C.J.M. de Groot, gynaecoloog, Vrije Universiteit Medisch Centrum, Amsterdam
- Mw. N.M. Hammoud, AIOS gynaecologie, Universitair Medisch Centrum Utrecht, Utrecht
- Mw. A. Hoek, gynaecoloog, Universitair Medisch Centrum Groningen, Groningen
- Dhr. J.S.E. Laven, gynaecoloog, Erasmus Medisch Centrum, Rotterdam
- Mw. A.H.E.M. Maas, cardioloog, Radboud Universitair Medisch Centrum, Nijmegen
- Mw. J. Roeters van Lennep, internist, Erasmus Medisch Centrum, Rotterdam
- Mw. B.K. Velthuis, radioloog, Universitair Medisch Centrum Utrecht, Utrecht
- Dhr. T.A. van Barneveld, klinisch epidemioloog, Orde van Medisch Specialisten, Utrecht
- Dhr. K.Y. Heida, richtlijnondersteuner Nederlandse Vereniging van Obstetrie en Gynaecologie, Utrecht
Extern advies:
- Dhr. Y. B.W.E.M. Roos, neuroloog, Academisch Medisch Centrum, Amsterdam
- Mw. M. Wessels, informatiespecialist, Orde van Medisch Specialisten, Utrecht
- Mw. C. De Groot, voorzitter Stichting HELLP-syndroom
Belangenverklaringen
De belangen van de werkgroepleden werden geïnventariseerd met het door KNAW, KNMG en OMS opgestelde belangenverklaringsformulier. De gemelde belangen zijn besproken in de werkgroep en met vertegenwoordigers van het bestuur van de NVOG. Geconcludeerd werd dat de werkgroep evenwichtig was samengesteld en dat er geen bezwaren waren tegen deelname aan de werkgroep en besluitvorming (proportionaliteitsbeginsel, zie Code KNMG, KNAW).
Inbreng patiëntenperspectief
Voor de ontwikkeling van een goede richtlijn is de input van patiënten nodig. Een behandeling moet immers voldoen aan de wensen en eisen van patiënten en zorgverleners. Patiënten kunnen zorgverleners die een richtlijn ontwikkelen helpen om te begrijpen hoe het is om met een ziekte of aandoening te leven of om er mee geconfronteerd te worden. Op deze manier kan bij het ontwikkelen van een richtlijn beter rekening gehouden worden met de betekenis van verschillende vormen van diagnostiek, behandeling en zorg voor patiënten. Het in kaart brengen van de behoeften, wensen en ervaringen van patiënten met de behandeling biedt tevens de gelegenheid om de knelpunten in kaart te brengen. Wat zou er volgens patiënten beter kunnen? Een patiënt doorloopt het hele zorgtraject, een behandelaar ziet vaak slechts het stukje behandeling waarin hij zich heeft gespecialiseerd. Het is dus heel zinvol om voor verbetering van de kwaliteit van de behandeling ook knelpunten vanuit patiëntenperspectief in kaart te brengen. Bij deze richtlijn is er in de beginfase van de ontwikkeling een knelpuntenanalyse uitgevoerd door middel van een drietal groepsinterviews met patiënten (focusgroepen). Uit de praktijken van leden van de werkgroep en via de Stichting HELLP-syndroom werden patiënten met een pre-eclampsie in de voorgeschiedenis, PCOS of POI uitgenodigd om deel te nemen aan een van deze focusgroep bijeenkomsten. De verslagen van de focusgroepen zijn besproken binnen de werkgroep en de belangrijkste knelpunten die uit de verslagen naar voren kwamen zijn geadresseerd in de richtlijn. Het concept van de richtlijn is voor commentaar voorgelegd aan deelnemers van de focusgroep. Zie hieronder voor de focusgroep verslagen.
Verslag patiëntenfocusgroep ‘pre-eclampsie’
In dit document worden de aandachtspunten die volgden uit het focusgroepsgesprek van 13 december 2012 uitgelicht.
Doel van het focusgroepsgesprek
Vanuit het patiëntenperspectief inzichtelijk maken hoe de nazorg aan vrouwen, die een hypertensieve aandoening tijdens de zwangerschap hebben gehad, patiënt gerichter kan.
Deelneemsters aan het focusgroepgesprek
In samenwerking met de Stichting HELLP-syndroom, een patiëntenvereniging specifiek voor deze doelgroep, en werkgroepleden, werden deelnemers benaderd en geselecteerd. Er namen in totaal 7 vrouwen deel, waarbij de periode na de doorgemaakte pre-eclampsie varieerde van anderhalf tot 35 jaar.
De gespreksstructuur
Het gesprek werd gestructureerd door chronologisch het zorgproces door te spreken volgens een vast stramien: periode in het ziekenhuis, nazorg in het eerste jaar en nazorg op lange termijn. De belangrijkste aandachtspunten worden in dit verslag uitgelicht, gegroepeerd naar bovenstaande zorgmomenten.
Algemene punten voor verbetering van het multidisciplinaire zorgproces
Periode in het ziekenhuis
- Informatievoorziening in de periode dat de deelneemsters opgenomen lagen in het ziekenhuis met een hypertensieve aandoening, inclusief kraambed.
a) De ervaringen in de verschillende ziekenhuizen wisselden sterk, sommige deelneemsters werden continu goed geïnformeerd over de stand van zaken, terwijl één deelneemster er pas bij de zes weekse controle achterkwam dat ze een ernstige pre-eclampsie had. Iedereen geeft aan dat eerlijkheid gewaardeerd wordt.
b) Een deelneemster geeft aan dat nazorg al begint tijdens de opname. Als men daar minder steken laat vallen, dan heb je een betere nazorg.
c) Er wordt echter ook aangegeven dat de informatie die gegeven wordt, vaak niet opgeslagen wordt, aangezien ze op dat moment voornamelijk zijn gefocust op hun kind en niet op hun eigen gezondheid. Dit komt pas in een later stadium, maar hier dient wel rekening mee gehouden te worden door de hulpverleners. - Een terugkomende klacht is dat zo snel de baby geboren is, er geen aandacht meer is voor de moeder, ongeacht haar ziektebeeld. Tevens wordt de man vaak vergeten, terwijl het voor hem ook heel heftig is. Het is erg belangrijk om hem er ook bij te betrekken.
- De opvang door de afdeling neonatologie werd door allen als prettig ervaren, aangezien er goed geluisterd werd en er naar oplossingen werd gezocht.
- Er wordt geopperd om de ontslag brief niet alleen naar de huisarts te sturen, maar ook naar het consultatiebureau en bedrijfsarts, zodat er meer awareness en begrip is voor klachten die samenhangen met een doorgemaakte hypertensieve aandoening in de zwangerschap. Over het consultatiebureau is overigens niet iedereen het eens.
- In de ontslagbrief moet meer aandacht komen voor de overdracht aan de huisarts, zodat de nazorg voor de vrouwen een stuk beter is.
Nazorg in het eerste jaar - De deelneemsters geven aan erg onzeker te zijn na een doorgemaakte pre-eclampsie. Niet alleen laat je eigen lichaam je in de steek en duurt het lang voordat je weer op de been bent. Ook staan op internet beangstigende ervaringsverhalen van andere vrouwen.
- Alles huisartsen hebben een brief ontvangen over het verloop van de zwangerschap en bevalling. Bij een enkeling kwam de huisarts langs in het kraambed. Het contact bestond verder uit nog eenmalig de bloeddruk meten, maar verder was er geen follow-up.
- Controle 6 weken postpartum bij gynaecoloog
a) Bij de meeste deelneemster is er onvoldoende informatie gegeven over de langdurige gevolgen van een ernstige pre-eclampsie. Wat kunnen de vrouwen zowel lichamelijk als geestelijk verwachten? Veel gehoorde klachten zijn concentratiestoornissen, geheugenverlies en vermoeidheid. Het merendeel geeft aan niet meer op het oude niveau terug te kunnen komen.
b) Naonderzoek (bijvoorbeeld Prius in Nijmegen en Maastricht) is niet aangeboden aan iedereen.
c) Naast de standaard controle, 6 weken postpartum, is er ook behoefte aan een gesprek op een later tijdstip. Dit initiatief moet ook van de zorgverlener komen, aangezien veel vrouwen het allemaal zelf willen oplossen en zichzelf niet op de eerste plaats zetten.
d) Men is unaniem over de toegevoegde waarden van de Stichting HELPP- syndroom, aangezien ze daar veel informatie vandaan halen, bijvoorbeeld over hart- en vaatziekten op latere leeftijd. Ze zouden hier graag bij ontslag of bij de controle 6 weken postpartum over geïnformeerd worden. Dit zou ook in een patiëntenfolder aan bod kunnen komen. - Er is een duidelijke behoefte aan een patiëntenfolder/naslagboekje over het traject na een doorgemaakte pre-eclampsie. Niet alleen over de klachten die kunnen voorkomen, maar ook tot wie je je kan wenden bij welk probleem. Deze patiëntenfolder kan eventueel ook gebruikt worden bij overleg met de bedrijfsarts. Zo’n patiëntenfolder kan zowel in boekvorm als op een website.
- De vraag is wie in de nazorg een centrale rol moeten spelen, hierover zijn de meningen verdeeld. Een enkeling vind de gynaecoloog de aangewezen persoon, aangezien diegene vaker te maken heeft met dit soort patiënten. Terwijl een ander juist de huisarts noemt, maar niet iedereen heeft een even goede band met haar huisarts. Ook wordt medisch maatschappelijk werk als mogelijkheid genoemd. Het was niet voor iedereen bekend dat het mogelijk is om na ontslag uit het ziekenhuis alsnog contact op te nemen met maatschappelijk werk. Zij kunnen mogelijk ook nazorg groepen organiseren, zodat lotgenoten met elkaar in contact komen. Hier is ook duidelijk behoefte aan. Tot slot wordt het consultatiebureau geopperd als belangrijke schakel tussen de verschillende disciplines, maar er komt ook naar voren dat daar minder expertise is betreft de gezondheid van moeders.
- Er wordt meer begrip verwacht van de huisarts en gynaecoloog voor de klachten waarmee de deelneemsters te kampen hebben. Ook zouden ze, indien noodzakelijk, een juiste doorverwijzing krijgen naar bijvoorbeeld een diëtiste, fysiotherapeut, oogarts, neuroloog etc. Op dit moment is er weinig begrip voor hun klachten, dit in tegenstelling tot oncologie patiënten. Voor hen is er een uitgebreid nazorgtraject.
- Eén deelneemster wordt regelmatig gezien op een gecombineerd spreekuur met een gynaecoloog en internist. Er is dan niet alleen aandacht voor lichamelijke klachten, maar ook op het emotionele vlak. Zij is hier erg over te spreken.
- Door meerdere deelneemster wordt aangegeven dat ze het erg fijn zouden vinden om nog eens een rondleiding te krijgen door het ziekenhuis en verloskunde centrum om hetgeen er gebeurd is beter te kunnen verwerken.
- Ervaren wordt dat er weinig begrip is in de omgeving t.a.v. aanhoudende klachten zoals vermoeidheid en concentratieproblemen. Ze lopen hier tegen aan in hun vrienden- en familiekring, maar ook op het werk. De ziekte heeft een erg lange nasleep. Meerder deelneemsters hebben een burn-out gekregen.
- Er komt met name naar voren dat de deelneemsters gehoord willen worden. En dat er een gestructureerde manier van nazorg georganiseerd moet worden, waarin duidelijke informatie gegeven wordt en er indien nodig doorverwezen wordt.
Nazorg lange termijn - De deelneemsters willen graag een duidelijk nazorg traject Wanneer dienen ze voor te komen, op welke klachten moeten ze letten, welke testen moeten uitgevoerd worden. Deze verantwoordelijkheid moet bij de huisarts komen te liggen en niet bij henzelf.
- Ze zouden graag een advies op maat krijgen. Bijvoorbeeld leefstijl- en sportadviezen/begeleiding of gespreksgroepen. Hier dient zo vroeg mogelijk mee begonnen te worden, zodat vrouwen sneller in het arbeidstraject komen.
- De meesten van de deelneemsters voelen zich best gezond. Hier moet in de richtlijn wel rekening mee gehouden worden, want het is iets heel anders als je gaat werken vanuit de motivatie dat je ziek bent dan wanneer je gezond ben. Het uitgangspunt moet gezondheidsbevordering zijn.
Verslag patiëntenfocusgroep PCOS
In dit document worden de aandachtspunten die volgden uit het focusgroepsgesprek van 1 juli 2013 uitgelicht.
Doel van het focusgroepsgesprek
Vanuit het patiëntenperspectief inzichtelijk maken hoe de zorg aan vrouwen met het polycysteus ovarium syndroom (PCOS) patiënt gerichter kan.
Deelneemsters aan het focusgroepgesprek
Er bestaat tot dusver geen patiëntenvereniging specifiek voor deze doelgroep. Voor het organiseren van de focusgroep werden deelnemers daarom benaderd en geselecteerd door werkgroepleden. Er namen in totaal 7 vrouwen deel.
De gespreksstructuur
Het gesprek werd gestructureerd door chronologisch het zorgproces door te spreken volgens een vast stramien: stellen van diagnose, behandeling, voorlichting, nazorg en toekomst. De belangrijkste aandachtspunten worden in dit verslag uitgelicht, gegroepeerd naar bovenstaande zorgmomenten.
Algemene punten voor verbetering van het multidisciplinaire zorgproces
Diagnose
- De diagnose PCOS werd niet altijd tijdig gesteld ondanks dat er sprake was van klachten.
- Klachten die met name genoemd werden, zijn: overberharing, acné, onregelmatig en/of weinig tot niet menstrueren en een onvervulde kinderwens.
- De diagnose werd meestal gesteld door een gynaecoloog, maar een enkele keer door bijvoorbeeld een dermatoloog die geconsulteerd werd in verband met overbeharing, waarna een verwijzing naar de gynaecoloog volgde.
- De ervaring van de meeste deelneemster was dat door de huisarts weinig gesproken wordt over de menstruatie, waardoor de diagnose PCOS pas laat gesteld werd. Sommige gynaecologen gaven ook niet veel uitleg over PCOS nadat ze de diagnose gesteld hadden.
- Ook al is de frequentie en regelmaat van de menstruatie te beschouwen als afwijkend, toch wordt dit vaak als normaal beschouwd. Dit kan komen doordat vrouwelijke familieleden hetzelfde menstruatiepatroon hebben (gehad) of dat men ervan uitgaat dat met het ouder worden de menstruatie vanzelf regelmatig wordt.
- Vrouwen met PCOS hebben vaker een eetstoornis en last van stemmingswisselingen.
- Voor de meeste deelneemsters was het een opluchting dat de klachten die zij hadden, verklaarbaar waren.
Behandeling - Alle deelneemsters kregen ‘de pil’ (orale anticonceptiva) voorgeschreven. Ook kregen zij leefstijladviezen: gezond eten en sporten om af te vallen.
- Een enkele deelneemster kreeg het advies van de huisarts of internist om te stoppen met ‘de pil’ aangezien ze last hadden van depressieve gevoelens. Bij deze hulpverleners was echter niet bekend dat ‘de pil’ niet als anticonceptiemiddel voorgeschreven werd, maar in verband met PCOS.
- Eén deelneemster is verwezen naar een diëtiste, maar aangezien zij een normale voedselintake had, kon de diëtiste weinig voor haar betekenen.
- De meeste deelneemsters zijn goed op gewicht, maar kennen vrouwen met PCOS die ondanks veel sporten en een dieet, toch aankomen in gewicht.
- Bij kinderwens werd meestal ovulatie inductie toegepast en werd vaak uitgelegd dat overgewicht de uitkomsten nadelig kon beinvloeden.
Voorlichting - Er zou meer bekendheid bij huisartsen en andere specialisten moeten komen over PCOS. De ervaring van enkele deelneemsters is dat hun huisarts onjuiste informatie geeft, zoals dat het helemaal niet erg is als je niet ongesteld wordt, dat scheelt alleen maar ‘gezeik’.
- De deelneemsters van deze focusgroep ervaren PCOS als verzamelbak van veel symptomen, waarin ze zichzelf niet altijd even goed herkennen, aangezien ze vaak maar één of twee symptomen hebben.
- De meningen wisselen over het zelf halen of aangeboden krijgen van informatie. Het liefst willen de deelneemsters zelf bepalen wanneer ze over een bepaald onderwerp meer willen weten afhankelijk van de fase in hun leven, zoals bij een kinderwens.
- Er is weinig Nederlandstalige informatie over dit onderwerp, ondanks dat er een NVOG patiëntenfolder is. Deze vinden de deelneemsters echter te beknopt.
- Informatie zouden ze het liefst aangeboden krijgen via internet. Ook zou een mail waarin staat dat er nieuwe informatie beschikbaar is, gewaardeerd worden.
- De meeste deelneemsters hebben geen behoefte aan lotgenotencontact, maar zouden het wel fijn vinden als er een patiëntenvereniging zou bestaan die zou dienen als informatiepunt. Je kan dan als patiënt zelf bepalen of je behoefte hebt aan lotgenoten contact of als je naar een informatieavond wilt gaan of lotgenotencontact waarin je kan delen als gewoon inhoudelijke informatieve avonden. Voorkeur om dit van het ziekenhuis uit te laten gaan.
- Een andere vorm van informatievoorziening, zou een soort van chatbox zijn, waarin de patiënt vragen kan stellen aan de hulpverlener. Dan is het niet noodzakelijk om een afspraak te hebben op de poli en kunnen ze sneller antwoord krijgen als ze een vraag hebben.
- Aan de meesten is wel verteld dat er een hogere kans bestaat op het ontwikkelen van hart- en vaatziekten, maar er is niet diep op in gegaan en het werd vaak tegelijk met de diagnose PCOS medegedeeld. Het zou beter zijn als hier op een later moment op terug gekomen wordt.
- Informatie moet veel meer uitgewisseld worden onder specialisten en huisartsen. Als een patiënt bijvoorbeeld al onder controle is bij een internist, dan hoeft diegene geen extra cardiovasculaire check meer te krijgen.
- Een terugkerend item is het onderwerp ‘zorg op maat’. De deelneemsters willen niet alleen informatie die op dat moment belangrijk voor hen is, ook moet de hulpverlener zich aanpassen aan het intelligentieniveau van de patiënt.
- De ervaring van de deelneemsters is dat het bij PCOS vooral over een eventuele kinderwens gaat, daar richt de gezondheidszorg zich nu met name op. Ze hebben het idee dat PCOS pas van belang is als je zwanger wilt worden. Voor hun is het ook belangrijk om informatie te krijgen over PCOS als er geen kinderwens is. Wat betekent de diagnose PCOS dan voor je.
- Ook informatie voor familie is belangrijk, zij maken zich vaak nog meer zorgen dan de patiënt zelf.
Nazorg - In principe hebben de deelneemsters eens in de 2 jaar een controle bij de gynaecoloog. In de tussenperiode hebben ze regelmatig vragen, maar hiermee gaan ze niet naar de huisarts, want de deelneemsters vinden dat die niet voldoende weten over PCOS. Een digitaal spreekuur zou een uitkomst zijn.
Toekomst - Alle deelneemsters zijn zich bewust van het belang van een gezonde leefstijl.
- Indien er bepaalde risicofactoren aanwezig zijn op het krijgen van hart- en vaatziekten, zoals een te hoog cholesterol, dan is er onder de deelneemsters een wisselende bereidheid om te starten met medicatie. Dit is ook afhankelijk van hoe hoog het risico is op hart- en vaatziekten.
- Risicocommunicatie is erg belangrijk, risico’s zijn namelijk moeilijk in te schatten en te begrijpen. Daarom is het belangrijk dat de patiënt de risico’s kan visualiseren door bijvoorbeeld kleuren toe te kennen aan de hoogte van een risico. Verder is het is belangrijk om gezamenlijk tot een beslissing te komen.
- De zorg rond hart- en vaatziekten risico moet bij voorkeur bij de internist komen te liggen. De gynaecoloog ziet deze vrouwen echter vroeg in hun leven en kan de regie over het verdere zorgpad voeren.
Verslag patiëntenfocusgroep POI
In dit document worden de aandachtspunten die volgden uit het focusgroepsgesprek van 2 juli 2013 uitgelicht.
Doel van het focusgroepsgesprek
Vanuit het patiëntenperspectief inzichtelijk maken hoe de zorg aan vrouwen met premature ovariële insufficiëntie (POI) patiënt gerichter kan.
Deelneemsters aan het focusgroepgesprek
Er bestaat tot dusver geen patiëntenvereniging specifiek voor deze doelgroep. Voor het organiseren van de focusgroep werden deelnemers daarom benaderd en geselecteerd door werkgroepleden. Er namen in totaal 7 vrouwen deel.
De gespreksstructuur
Het gesprek werd gestructureerd door chronologisch het zorgproces door te spreken volgens een vast stramien: stellen van diagnose, behandeling, voorlichting, nazorg en toekomst. De belangrijkste aandachtspunten worden in dit verslag uitgelicht, gegroepeerd naar bovenstaande zorgmomenten.
Algemene punten voor verbetering van het multidisciplinaire zorgproces
Diagnose
- De diagnose POI werd meestal gesteld nadat de deelneemsters zich meldden met de volgende klachten: ongewenste kinderloosheid of bij het opeens optreden van een onregelmatige menstruatie of nadat de menstruatie opeens gestopt was terwijl die voorheen normaal blek te zijn geweest (dit laatste ook na het gebruik van orale anticonceptiva).
- Ook waren er deelneemsters die POI hebben ontwikkeld na chemotherapie. Zij kregen de mogelijkheid om eitjes in te laten vriezen, maar op jonge leeftijd is het erg moeilijk om deze beslissing te nemen aangezien er dan nog geen kinderwens is.
- De diagnose werd meestal gesteld door een gynaecoloog in een 2e lijns centrum, maar ook een enkele keer door de huisarts. De diagnose werd vaak niet of slechts ten dele medegedeeld. Meestal werd patiënten verteld dat de gynaecoloog het zelf niet zo goed begreep. Soms werd gezegd dat de tot dan toe gedane bevindingen niet konden kloppen en om die reden werd patiënte verwezen naar de 3e lijn. De deelneemsters kregen het gevoel dat de arts zelf ook schrok van de uitslagen van het bloedonderzoek en ze kregen nauwelijks uitleg over oorzaken en de gevolgen van POI.
- Eén deelneemster kreeg de diagnose te horen tijdens een telefonisch consult, dit heeft zij als zeer lomp ervaren.
- Ze kregen allen een doorverwijzing naar een gynaecoloog in een 3e lijns centrum. Een enkele deelneemster vraagt zich af of het ook mogelijk is om meteen doorgestuurd te worden naar een 3e lijn centrum in plaats van eerst naar een 2e lijns ziekenhuis. De ervaring is dat er meer expertise is in een 3e lijns centrum.
- De deelneemster waarderen een directe en eerlijke manier van communiceren.
Behandeling - De deelneemsters gebruiken eventueel orale anticonceptiva gezien de kleine kans om toch zwanger te worden. Meestal echter gebruikte men een hormoonsubstitutie preparaat. Sommigen zijn nog wel behandeld voor hun kinderwens terwijl dat bij anderen niet zinvol werd geacht, zij hebben daarom die behandeling niet gehad. Er was een deelneemster die ondanks de slechte prognose toch behandeld werd en ook een kind kreeg, dat is echter wel de uitzondering op de regel. Hormoonsubstitutie werd ook gegeven om overgangsklachten te verminderen. Sommigen gebruikten ook homeopathische middelen. Een enkeling was gestopt of had geen medicatie. Daarnaast werd ook vaak leefstijladviezen gegeven.
Voorlichting - Met allen is er is over hart- en vaatziekten gesproken en over botontkalking. Vooral dat laatste is benadrukt.
- Over het algemeen staat het onderwerp hart- en vaatziekten ver van de deelneemsters af, er is hun vertelt dat pas na het 40e levensjaar verdere controle volgen.
- Wat betreft informatie over hart- en vaatziekten is het advies gegeven om te sporten. Door de bijkomende overgangsklachten kan het echter wel extra zwaar zijn. Er is behoefte aan meer begeleiding en informatie over hoe je dit het beste kan combineren.
- Een deelneemster heeft de bloeduitslagen mee naar huis gekregen. Dit heeft haar goed geholpen bij de acceptatie van de diagnose POI. Bij twijfel pakt ze de uitslagen erbij en realiseert ze zich dat de waarden afwijkend zijn.
- Er is geen patiëntenvereniging voor vrouwen met POI, deelneemsters zouden wel behoefte hebben aan meer informatie, zowel patiëntspecifieke uitslagen als algemene informatie. En ze zouden graag op de hoogte willen zijn van de laatste ontwikkelingen op het gebied van onderzoek. De meeste deelneemsters zouden het fijn vinden als er een patiëntenvereniging zou bestaan die zou dienen als informatiepunt. Als patiënt kan je dan zelf bepalen of je behoefte hebt aan lotgenoten contact of naar een informatieavond wilt gaan.
- Informatie zouden ze het liefst aangeboden krijgen via internet, maar dit zou ook in de vorm van een standaard informatiepakket kunnen. Deze informatie kan ook nuttig zijn voor mensen in de directe omgeving.
- De meningen wisselen over het zelf halen of aangeboden krijgen van informatie. Het liefst willen de deelneemsters zelf bepalen wanneer ze over een bepaald onderwerp meer willen weten afhankelijk van de fase in hun leven.
Nazorg - Eén deelneemsters heeft positieve ervaring met de Mammacare verpleegkundige in het omgaan met stress in relatie tot overgangsklachten.
- Niet aan iedereen is nazorg aangeboden bij een psycholoog of medisch maatschappelijk werk, maar deelneemsters geven aan dat ze er gebruik van willen maken wanneer zij daar zelf behoefte aan hebben. Ze staan er wel positief tegenover, want het kan prettig zijn om met een onafhankelijk persoon te praten, waarbij je geen rekening hoeft te houden met de gevoelens van diegene.
- Het wordt gewaardeerd als de polikliniek voor patiënten met POI gescheiden is van de zwangere poli.
Toekomst - De meeste deelneemsters blijven tegen beter weten in toch hopen dat er misschien nog ‘een verdwaald eitje’ zit.
- Als er iemand in de omgeving zwanger is of al kinderen heeft, kunnen de meeste deelneemsters hier mee omgaan, maar ze blijven het er wel moeilijk mee hebben. Ieder heeft zijn eigen manier om hier mee om te gaan.
- De mening over klachten die samenhangen met POI zijn wisselend. Sommigen hebben helemaal geen klachten, anderen noemen minder energie, concentratiestoornissen en verandering van het karakter als klachten die samenhangen met POI.
Deelneemsters kunnen er goed met de omgeving over praten, ze merken dat er begrip is voor hun situatie, maar echt begrijpen doen ze het niet.
Methode ontwikkeling
Evidence based
Implementatie
In de verschillende fasen van de richtlijnontwikkeling is geprobeerd rekening te houden met de implementatie van de richtlijn en de praktische uitvoerbaarheid van de aanbevelingen. Daarbij is uitdrukkelijk gelet op factoren die de invoering van de richtlijn in de praktijk kunnen bevorderen of belemmeren. De richtlijn wordt verspreid onder alle relevante beroepsgroepen en ziekenhuizen. Daarnaast wordt patiëntenvoorlichtingsmateriaal ontwikkeld. Ook is de richtlijn te downloaden via de websites van de Nederlandse Vereniging voor Obstetrie en Gynaecologie (www.nvog.nl), de Nederlandse Vereniging voor Cardiologie (www.nvvc.nl), de Nederlandse Internisten Vereniging (www.internisten.nl) en de algemen richtlijnendatabase (www.richtlijnendatabase.nl).
Werkwijze
Werkwijze werkgroep
De werkgroep werkte gedurende twee jaar aan de totstandkoming van de conceptrichtlijn. De werkgroepleden zochten systematisch naar de literatuur en beoordeelden de kwaliteit en inhoud ervan. De richtlijnondersteuner maakte, in samenspraak met de subwerkgroep die voor elk hoofdstuk was aangesteld, bewijs (evidence)tabellen. Een samenvatting van het bewijs met de conclusies werd teruggekoppeld aan de gehele werkgroep waarna gezamenlijk de overige overwegingen en aanbevelingen werden geformuleerd. Tijdens vergaderingen werden teksten toegelicht en werd door de werkgroepleden meegedacht en gediscussieerd. De uiteindelijke teksten vormen samen de hier voorliggende conceptrichtlijn.
Methode richtlijnontwikkeling
Deze richtlijn is opgesteld aan de hand van het “Appraisal of Guidelines for Research & Evaluation” (AGREE) instrument (www.agreecollaboration.org). Dit instrument is een breed (internationaal) geaccepteerd instrument voor de beoordeling van de kwaliteit van richtlijnen.
Knelpuntenanalyse /invitational conference
De werkgroep heeft een analyse gemaakt van knelpunten die aanknopingspunten bieden voor de verbetering van de zorg voor vrouwen die een zwangerschap hebben doorgemaakt die werd gecompliceerd door zwangerschapshypertensie, pre-eclampsie, vroeggeboorte of een groeibeperkt kind of vrouwen met een herhaalde miskraam, prematuur ovariële insufficiëntie of polycysteus ovarium syndroom. Op basis hiervan is een concept raamwerk van de in de richtlijn te bespreken onderwerpen opgesteld. Om de richtlijn zoveel mogelijk te laten aansluiten bij de dagelijkse praktijk is vervolgens een invitational conference georganiseerd. Hiervoor zijn diverse stakeholders, betrokken bij de zorg voor patiënten met een van deze reproductieve aandoeningen, uitgenodigd zoals: zorgverzekeraars, de Inspectie voor de Gezondheidszorg (IGZ) , patiëntenorganisaties, organisaties van zorginstellingen en het College voor Zorgverzekeringen (CVZ). Met deze partijen is het door de werkgroep opgestelde raamwerk besproken en nader geëxpliciteerd. Ook zijn stakeholders gevraagd aanvullingen te geven en zijn hun verwachtingen over de richtlijn en het richtlijnontwikkelingsproces geïnventariseerd. De werkgroep heeft vervolgens een prioritering aangebracht van in de richtlijn te behandelen onderwerpen en het raamwerk van de richtlijn definitief vastgesteld.
Strategie voor zoeken naar literatuur
Er werd eerst oriënterend gezocht naar bestaande richtlijnen (https://www.ahrq.gov/, http://www.nice.org.uk/, http://www.cbo.nl/thema/Richtlijnen/, SUMsearch: http://sumsearch.uthscsa.edu/ en http://www.sign.ac.uk/) en naar systematische reviews in de Cochrane Library en via SUMsearch. Vervolgens werd er voor de afzonderlijke uitgangsvragen aan de hand van specifieke zoektermen gezocht naar gepubliceerde wetenschappelijke studies in de elektronische databases Medline en Embase. Tevens werd aanvullend handmatig gezocht naar studies aan de hand van de literatuurlijsten van de opgevraagde artikelen. De gebruikte zoektermen staan in bijlage 5, zoekverantwoording.
Definiëren klinisch relevante uitkomstmaten en acceptabele meetinstrumenten hiervoor
Alvorens te starten met de literatuurselectie werden door de werkgroep klinisch relevante uitkomstmaten en acceptabele meetinstrumenten gedefinieerd. Ook definities voor andere relevante variabelen werden afgestemd. Zie voor de uitwerking hiervan verderop in dit hoofdstuk onder het kopje ‘Uitkomstmaten’ (blz 13) en hoofdstuk 3 ‘Definities’ (blz 21).
Literatuurselectie
Per uitgangsvraag werden ten minste twee werkgroepleden aangesteld om onafhankelijk van elkaar de literatuur te beoordelen op relevantie.
Bij deze selectie van titel en abstract werden de volgende exclusiecriteria gehanteerd:
- niet van toepassing op de vraagstelling;
- niet vergelijkbaar met de Nederlandse populatie;
- niet-gedefinieerde uitkomstmaat;
- minder dan 10 vrouwen in de onderzoekspopulatie (imprecisie);
- niet-primair onderzoek;
- case reports, case series, letters, abstracts.
Beoordeling van de kwaliteit van studies
Na selectie door de werkgroepleden bleven de artikelen over die als onderbouwing bij de verschillende conclusies staan vermeld. De geselecteerde artikelen zijn vervolgens door minimaal twee werkgroepleden op volledige tekstinhoud beoordeeld en daarna beoordeeld op kwaliteit van het onderzoek en gegradeerd naar mate van bewijs. Hierbij is de indeling gebruikt, zoals weergegeven in tabel 1.1.
De beoordeling van de verschillende artikelen vindt u in de verschillende teksten terug onder het kopje ‘Samenvatting van de literatuur’. De richtlijnondersteuner maakte in samenspraak met de subgroepen per uitgangsvraag evidencetabellen (zie bijlage 6) van de geselecteerde individuele studies als hulpmiddel bij het beoordelen en samenvatten van deze studies. Vervolgens werd de kwaliteit van de evidence op het niveau van de systematische review beoordeeld. Met de kwaliteit van de evidence wordt bedoeld in hoeverre er vertrouwen is dat de aanbevelingen gebaseerd kunnen worden op de (effectschatting van de) evidence. Het wetenschappelijk bewijs is vervolgens kort samengevat in de ‘conclusies uit de literatuur’. De belangrijkste literatuur waarop deze conclusies zijn gebaseerd staat bij de conclusies vermeld, inclusief de EBRO-gradering van bewijs. Voor deze richtlijn hebben we geen gebruik gemaakt van de GRADE-methode, omdat GRADE momenteel alleen geschikt is voor het beoordelen van vergelijkend interventieonderzoek. Voor het beoordelen van diagnostisch accuratesse onderzoek of onderzoeken met een etiologische of prognostische vraagstelling blijft de ‘reguliere’ EBRO-beoordelingsmethode van toepassing.
Bij de EBRO-methode worden studies individueel beoordeeld op methodologische kwaliteit (onderzoeksopzet/studiedesign). Naar aanleiding van deze beoordeling wordt elke studie ingedeeld naar mate van bewijs volgens de classificatie in tabel 1.1. Studies van niveau A1 hebben de hoogste mate van bewijs en niveau D staat voor de laagste bewijskracht.
Tabel 1.1: EBRO-indeling van methodologische kwaliteit van individuele studies
|
Bewijskrachtniveau |
Interventieonderzoek |
Onderzoek naar diagnostische accuratesse |
Schade of bijwerkingen, etiologie, prognose |
|
|
A1 |
systematische review/meta-analyse van ten minste 2 onafhankelijk van elkaar uitgevoerde onderzoeken van A2-niveau |
|||
|
A2
|
gerandomiseerd dubbelblind vergelijkend klinisch onderzoek van goede kwaliteit van voldoende omvang
|
onderzoek t.o.v. een referentietest (‘gouden standaard’) met tevoren gedefinieerde afkapwaarden en onafhankelijke beoordeling van resultaten, met voldoende grote serie van opeenvolgende patiënten die allen de index- en referentietest hebben gehad |
prospectief cohortonderzoek van voldoende omvang en follow-up, waarbij adequaat gecontroleerd is voor ‘confounding’ en selectieve follow-up voldoende is uitgesloten
|
|
|
B |
vergelijkend onderzoek, maar niet met alle kenmerken als genoemd onder A2 (ook patiënt-controleonderzoek, cohortonderzoek) |
onderzoek t.o.v. een referentietest, maar niet met alle kenmerken die onder A2 zijn genoemd |
prospectief cohortonderzoek, maar niet met alle kenmerken als genoemd onder A2 of retrospectief cohortonderzoek of patiënt-controleonderzoek |
|
|
C |
niet-vergelijkend onderzoek |
|||
|
D |
mening van deskundigen |
|||
Formuleren van aanbevelingen
Nadat de gegevens uit de evidencetabellen werden samengevat als tekst werden hieruit conclusies getrokken. Om vervolgens tot een gewogen aanbeveling te komen werden de overige overwegingen besproken en geformuleerd. Dit is van belang omdat voor een aanbeveling naast het wetenschappelijke bewijs ook nog andere aspecten in mee gewogen horen te worden zoals patiëntenvoorkeuren, frequentie en ernst van aandoening, kosten, beschikbaarheid van voorzieningen of organisatorische aspecten. Bij de overwegingen spelen de ervaring en opvattingen van de werkgroepleden een rol bij het ontbreken van wetenschappelijk bewijs. De ‘aanbevelingen’ geven een antwoord op de uitgangsvraag en zijn gebaseerd op zowel het beschikbare wetenschappelijke bewijs als op de belangrijkste overwegingen. De gebruikte methodiek voor richtlijnontwikkeling verhoogt de transparantie van de totstandkoming van de aanbevelingen in deze richtlijn.
Uitkomstmaten
Bij de beoordeling van de literatuur heeft de werkgroep vooral gekeken naar studies waarbij naar inzicht van de werkgroepleden klinisch relevante uitkomstmaten gebruikt werden.
Om pragmatische redenen zijn hierbij de definities uit de gevonden literatuur overgenomen.
Tabel 1.2 Uitkomstmaten en gebruikte definities
|
Uitkomstmaten |
Gekozen meetinstrumenten
|
|
Cardiovasculaire gebeurtenissen |
Sterfte aan een cardiovasculaire oorzaak, en niet fatale, myocardinfarct, coronaire hartziekte, beroerte (CVA), decompensatio cordis, nierfalen, perifeer vaatlijden, angina pectoris, aneurysma aortae. |
|
Risicofactoren |
Hypertensie, diabetes mellitus type 2, dyslipidemie |
Zoekverantwoording
|
Onderwerp:
|
Database |
Zoekstrategie |
Aantal ref. |
|
4.1 PE / zwangerschapshypertensie
4.1.1 Wat is het risico op een cardiovasculaire gebeurtenis voor vrouwen met pre-eclampsie of zwangerschapshypertensie in de voorgeschiedenis?
4.1.2 Wat zijn de risico’s op een ongunstig cardiovasculaire risicoprofiel voor vrouwen met pre-eclampsie of zwangerschapshypertensie in de voorgeschiedenis?
|
Medline (OVID), Tot jan 2013 Engels, Nederlands
Embase (Elsevier) |
5 exp Hypertension, Pregnancy-Induced/ (25741) 6 ((pregnancy-induced or gestational or maternal) adj3 hypertension*).ti. (1547) 7 ((transient adj3 hypertension) and pregnan*).ti. (10) 8 ("h?emolysis, elevated liver enzymes, and low platelet'*" or hellp or eclampsia or pre-eclampsia or preeclampsia or (pregnancy adj3 toxemia)).ti. (11855) 9 or/5-8 (27132) 10 exp Cardiovascular Diseases/ep, et [Epidemiology, Etiology] (439592) 11 (exp Renal Insufficiency/ or calcinosis/ or exp vascular calcification/ or Hypercholesterolemia/ or exp Obesity/ or exp Electrocardiography/ or exp Hypertension/ or exp Diabetes Mellitus/ or Metabolic Syndrome X/) and (epidemiology or etiology).fs. (276102) 12 (stroke or CVA or cerebrovascular or cardiovascul* or (myocard* adj2 infarct*) or atheroscleros* or "vascular calcification*" or ((renal or kidney) adj3 (insufficienc* or failure*)) or "ischaemic attack*" or TIA or "angina pectoris" or electrocardiogra* or ecg or hypercholesterolemia or hypertension or diabet* or ((endothelial or vascular) adj2 dysfunction*) or (("left ventricular" or myocardial) adj3 hypertroph*) or (metabol* adj2 syndrome*)).ti. (630214) 13 10 or 11 or 12 (1048086) 14 9 and 13 (5425) 15 limit 14 to english language (4061) - 16 (meta-analysis/ or meta-analysis as topic/ or (meta adj analy$).tw. or (systematic* adj review$1).tw. or (systematic adj overview$1).tw. or exp "Review Literature as Topic"/ or cochrane.ab. or cochrane.jw. or embase.ab. or medline.ab. or (psychlit or psyclit).ab. or (cinahl or cinhal).ab. or cancerlit.ab. or ((selection criteria or data extraction).ab. and "review"/)) not (Comment/ or Editorial/ or Letter/ or (animals/ not humans/)) (117463) 18 15 and 16 (57) – (SR) – keyword in reference manager: Medline-Cardio-Hypertensie-SR-23-01-2013 19 15 not 18 (3994)
'cardiovascular disease'/exp/mj OR 'kidney failure'/exp/mj OR 'diabetes mellitus'/exp/mj OR 'electrocardiography'/exp/mj OR 'hypercholesterolemia'/exp/mj OR 'hypertension'/exp/mj OR 'obesity'/exp/mj OR 'blood vessel calcification'/exp/mj OR 'metabolic syndrome x'/exp/mj OR stroke:ab,ti OR cva:ab,ti OR cerebrovascular:ab,ti OR cardiovascul*:ab,ti OR (myocard* NEAR/2 infarct*):ab,ti OR atheroscleros*:ab,ti OR (vascular NEAR/2 calcification):ab,ti OR ((renal OR kidney) NEAR/3 (insufficienc* OR failure*)):ab,ti OR (ischaemic NEAR/2 attack*):ab,ti OR tia:ab,ti OR 'angina pectoris':ab,ti OR electrocardiogra*:ab,ti OR ecg:ab,ti OR hypercholesterolemia:ab,ti OR obesity:ab,ti OR hypertension:ab,ti OR diabet*:ab,ti OR ((endothelial OR vascular) NEAR/2 dysfunction*):ab,ti OR (('left ventricular' OR myocardial) NEAR/3 hypertroph*):ab,ti OR (metabol* NEAR/2 syndrome*):ab,ti AND ('maternal hypertension'/exp/mj OR ((transient NEAR/3 hypertension):ti AND pregnan*:ab,ti) OR (('pregnancy induced' OR gestational OR maternal) NEAR/3 hypertension*):ti OR 'h?emolysis, elevated liver enzymes, and low platelet':ti OR 'h?emolysis, elevated liver enzymes, and low platelets':ti OR hellp:ti OR eclampsia:ti OR 'pre eclampsia':ti OR preeclampsia:ti OR (pregnancy NEAR/3 toxemia):ti) NOT 'conference abstract':it AND [english]/lim AND [embase]/lim,
|
7497 |
|
4.2 PCOS
4.2.1. Wat is het risico op een cardiovasculaire gebeurtenis bij een vrouw met PCOS? 4.2.2. Wat is het cardiovasculaire risicoprofiel van vrouwen met PCOS?
|
Medline (OVID), 2010- tot Dec 2012 Engels, Nederlands
Embase (Elsevier) |
1 Polycystic Ovary Syndrome/ (9485) 2 ((("stein-leventhal syndrome" or "Polycystic Ovar*") adj3 (Syndrome* or disease*)) or PCOS).ti,ab. (9318) 3 1 or 2 (11469) 9 exp Cardiovascular Diseases/ (1774139) 10 exp Renal Insufficiency/ or calcinosis/ or exp vascular calcification/ or Hypercholesterolemia/ or exp Obesity/ or exp Electrocardiography/ or exp Hypertension/ or exp Proteinuria/ or exp Diabetes Mellitus/ or Metabolic Syndrome X/ (904001) 11 (stroke or CVA or cerebrovascular or cardiovascul* or (myocard* adj2 infarct*) or atheroscleros* or "vascular calcification*" or ((renal or kidney) adj3 (insufficienc* or failure*)) or "ischaemic attack*" or TIA or "angina pectoris" or electrocardiogra* or ecg or hypercholesterolemia or hypertension or proteinuria or diabet* or ((endothelial or vascular) adj2 dysfunction*) or (("left ventricular" or myocardial) adj3 hypertroph*) or (metabol* adj2 syndrome*)).ti. (642987) 12 9 or 10 or 11 (2334775) 13 3 and 12 (2488) 14 limit 13 to english language (2213) 15 (meta-analysis/ or meta-analysis as topic/ or (meta adj analy$).tw. or (systematic* adj review$1).tw. or (systematic adj overview$1).tw. or exp "Review Literature as Topic"/ or cochrane.ab. or cochrane.jw. or embase.ab. or medline.ab. or (psychlit or psyclit).ab. or (cinahl or cinhal).ab. or cancerlit.ab. or ((selection criteria or data extraction).ab. and "review"/)) not (Comment/ or Editorial/ or Letter/ or (animals/ not humans/)) (120628) 16 14 and 15 (53)
'cardiovascular disease'/exp/mj OR 'kidney failure'/exp/mj OR 'diabetes mellitus'/exp/mj OR 'electrocardiography'/exp/mj OR 'hypercholesterolemia'/exp/mj OR 'hypertension'/exp/mj OR 'obesity'/exp/mj OR 'proteinuria'/exp/mj OR 'blood vessel calcification'/exp/mj OR 'metabolic syndrome x'/exp/mj OR stroke:ab,ti OR cva:ab,ti OR cerebrovascular:ab,ti OR cardiovascul*:ab,ti OR (myocard* NEAR/2 infarct*):ab,ti OR atheroscleros*:ab,ti OR (vascular NEAR/2 calcification):ab,ti OR ((renal OR kidney) NEAR/3 (insufficienc* OR failure*)):ab,ti OR (ischaemic NEAR/2 attack*):ab,ti OR tia:ab,ti OR 'angina pectoris':ab,ti OR electrocardiogra*:ab,ti OR ecg:ab,ti OR hypercholesterolemia:ab,ti OR hypertension:ab,ti OR proteinuria:ab,ti OR diabet*:ab,ti OR ((endothelial OR vascular) NEAR/2 dysfunction*):ab,ti OR (('left ventricular' OR myocardial) NEAR/3 hypertroph*):ab,ti OR (metabol* NEAR/2 syndrome*):ti AND ('ovary polycystic disease'/exp/mj OR 'stein-leventhal syndrome':ab,ti OR ('polycystic ovary' NEAR/3 (syndrome* OR disease*)):ab,ti OR pcos:ab,ti OR 'stein-leventhal syndromes':ab,ti OR ('polycystic ovarian' NEAR/3 (syndrome* OR disease*)):ab,ti) AND [english]/lim AND [embase]/lim NOT ('meta analysis'/de OR cochrane:ab OR embase:ab OR psychlit:ab OR cinahl:ab OR medline:ab OR (systematic NEAR/1 (review OR overview)):ab,ti OR (meta NEAR/1 analy*):ab,ti OR metaanalys*:ab,ti OR 'data extraction':ab OR cochrane:jt OR 'systematic review'/de) NOT (animal* NOT human*) |
820 |
|
4.3 POI
4.3.1. Wat is het risico op een cardiovasculaire gebeurtenis bij vrouwen met POI? 4.3.2. Wat is het cardiovasculaire risicoprofiel van vrouwen met POI? 4.3.3. Beïnvloedt het gebruik van hormoon suppletie therapie het risico op cardiovasculaire gebeurtenissen?
|
Medline (OVID), Tot dec 2012 Engels, Nederlands
Embase (Elsevier) |
1 Primary Ovarian Insufficiency/ or Menopause, Premature/ or ((premature or primary) adj2 ovarian adj2 (failure or insufficiency)).ti,ab. or ((premature or early) adj3 menopause).ti,ab. (3783) 2 exp Cardiovascular Diseases/ (1770679) 3 exp Renal Insufficiency/ or calcinosis/ or exp vascular calcification/ or Hypercholesterolemia/ or exp Obesity/ or exp Electrocardiography/ or exp Hypertension/ or exp Proteinuria/ or exp Diabetes Mellitus/ or Metabolic Syndrome X/ (901853) 4 (stroke or CVA or cerebrovascular or cardiovascul* or (myocard* adj2 infarct*) or atheroscleros* or "vascular calcification*" or ((renal or kidney) adj3 (insufficienc* or failure*)) or "ischaemic attack*" or TIA or "angina pectoris" or electrocardiogra* or ecg or hypercholesterolemia or obesity or hypertension or proteinuria or diabet* or ((endothelial or vascular) adj2 dysfunction*) or (("left ventricular" or myocardial) adj3 hypertroph*) or (metabol* adj2 syndrome*)).ti,ab. (1225080) 5 2 or 3 or 4 (2545477) 6 1 and 5 (505) 7 limit 6 to english language (437) 8 (meta-analysis/ or meta-analysis as topic/ or (meta adj analy$).tw. or (systematic* adj review$1).tw. or (systematic adj overview$1).tw. or exp "Review Literature as Topic"/ or cochrane.ab. or cochrane.jw. or embase.ab. or medline.ab. or (psychlit or psyclit).ab. or (cinahl or cinhal).ab. or cancerlit.ab. or ((selection criteria or data extraction).ab. and "review"/)) not (Comment/ or Editorial/ or Letter/ or (animals/ not humans/)) (109969) 9 7 and 8 (5) – risk - epi 10 exp epidemiologic studies/ (1485441) 11 7 and 10 (104) 12 (risk* or predict* or event*).ti,ab. (2087355) 13 7 and 12 (242) 14 11 or 13 (272) 15 14 not 9 (268) – risk-epi
('cardiovascular disease'/exp/mj OR 'kidney failure'/exp/mj OR 'diabetes mellitus'/exp/mj OR 'electrocardiography'/exp/mj OR 'hypercholesterolemia'/exp/mj OR 'hypertension'/exp/mj OR 'obesity'/exp/mj OR 'proteinuria'/exp/mj OR 'blood vessel calcification'/exp/mj OR 'metabolic syndrome x'/exp/mj OR stroke:ab,ti OR cva:ab,ti OR cerebrovascular:ab,ti OR cardiovascul*:ab,ti OR (myocard* NEAR/2 infarct*):ab,ti OR atheroscleros*:ab,ti OR (vascular NEAR/2 calcification):ab,ti OR ((renal OR kidney) NEAR/3 (insufficienc* OR failure*)):ab,ti OR (ischaemic NEAR/2 attack*):ab,ti OR tia:ab,ti OR 'angina pectoris':ab,ti OR electrocardiogra*:ab,ti OR ecg:ab,ti OR hypercholesterolemia:ab,ti OR obesity:ab,ti OR hypertension:ab,ti OR proteinuria:ab,ti OR diabet*:ab,ti OR ((endothelial OR vascular) NEAR/2 dysfunction*):ab,ti OR (('left ventricular' OR myocardial) NEAR/3 hypertroph*):ab,ti OR (metabol* NEAR/2 syndrome*):ab,ti AND ('early menopause'/exp/mj OR 'premature ovarian failure'/exp/mj OR ((premature OR primary) NEAR/2 ('ovarian failure' OR 'ovarian insufficiency')):ab,ti OR ((premature OR early) NEAR/3 menopause):ab,ti) AND [english]/lim AND [embase]/lim AND (risk*:ab,ti OR predict*:ab,ti OR event*:ab,ti)) or 'clinical study'/exp or SR |
679 |
|
4.4 Herhaalde miskraam
4.4.1 Wat is het risico op een cardiovasculaire gebeurtenis bij vrouwen met 2 of meer miskramen in de voorgeschiedenis? 4.4.2 Wat is het cardiovasculaire risicoprofiel van vrouwen met 2 of meer miskramen in de voorgeschiedenis?
|
Medline (OVID), Tot dec 2012 Engels, Nederlands
Embase (Elsevier) |
1 exp abortion, habitual/ (6296) 2 ((recurren* or habitual) adj3 (miscarriage* or abortion* or "pregnancy loss*")).ti,ab. (4616) 3 Abortion, Spontaneous/ (13738) 4 Recurrence/ (151907) 5 3 and 4 (204) 6 1 or 2 or 5 (7921) 7 exp Cardiovascular Diseases/ (1780857) 8 exp Renal Insufficiency/ or calcinosis/ or exp vascular calcification/ or Hypercholesterolemia/ or exp Obesity/ or exp Electrocardiography/ or exp Hypertension/ or exp Proteinuria/ or exp Diabetes Mellitus/ or Metabolic Syndrome X/ (907743) 9 (stroke or CVA or cerebrovascular or cardiovascul* or (myocard* adj2 infarct*) or atheroscleros* or "vascular calcification*" or ((renal or kidney) adj3 (insufficienc* or failure*)) or "ischaemic attack*" or TIA or "angina pectoris" or electrocardiogra* or ecg or hypercholesterolemia or obesity or hypertension or proteinuria or diabet* or ((endothelial or vascular) adj2 dysfunction*) or (("left ventricular" or myocardial) adj3 hypertroph*) or (metabol* adj2 syndrome*)).ti,ab. (1292223) 10 7 or 8 or 9 (2619398) 11 6 and 10 (846) 12 limit 11 to english language (674) 17 12 not (animals/ not humans/) (670) 18 (mouse or mice or cat? or rat? or dog? or cow or horse?).ti. (1325374) 19 17 not 18 (667) 20 (meta-analysis/ or meta-analysis as topic/ or (meta adj analy$).tw. or (systematic* adj review$1).tw. or (systematic adj overview$1).tw. or exp "Review Literature as Topic"/ or cochrane.ab. or cochrane.jw. or embase.ab. or medline.ab. or (psychlit or psyclit).ab. or (cinahl or cinhal).ab. or cancerlit.ab. or ((selection criteria or data extraction).ab. and "review"/)) not (Comment/ or Editorial/ or Letter/ or (animals/ not humans/)) (121431) 21 19 and 20 (14) 22 17 not 21 (656)
cardiovascular disease'/exp/mj OR 'kidney failure'/exp/mj OR 'diabetes mellitus'/exp/mj OR 'electrocardiography'/exp/mj OR 'hypercholesterolemia'/exp/mj OR 'hypertension'/exp/mj OR 'obesity'/exp/mj OR 'proteinuria'/exp/mj OR 'blood vessel calcification'/exp/mj OR 'metabolic syndrome x'/exp/mj OR stroke:ab,ti OR cva:ab,ti OR cerebrovascular:ab,ti OR cardiovascul*:ab,ti OR (myocard* NEAR/2 infarct*):ab,ti OR atheroscleros*:ab,ti OR (vascular NEAR/2 calcification):ab,ti OR ((renal OR kidney) NEAR/3 (insufficienc* OR failure*)):ab,ti OR (ischaemic NEAR/2 attack*):ab,ti OR tia:ab,ti OR 'angina pectoris':ab,ti OR electrocardiogra*:ab,ti OR ecg:ab,ti OR hypercholesterolemia:ab,ti OR obesity:ab,ti OR hypertension:ab,ti OR proteinuria:ab,ti OR diabet*:ab,ti OR ((endothelial OR vascular) NEAR/2 dysfunction*):ab,ti OR (('left ventricular' OR myocardial) NEAR/3 hypertroph*):ab,ti OR (metabol* NEAR/2 syndrome*):ab,ti AND ('recurrent abortion'/exp/mj OR ((recurren* OR habitual) NEAR/3 (miscarriage* OR abortion* OR 'pregnancy loss' OR 'pregnancy losses')):ab,ti OR ('spontaneous abortion'/exp/mj AND 'recurrent disease'/exp)) AND [english]/lim AND [embase]/lim ' not conference abstract':it
|
818 |
|
4.5 Vroeggeboorte
4.5.1. Wat is het risico op een cardiovasculaire gebeurtenis voor vrouwen met één vroeggeboorte (bevalling voor de 37 weken amenorroeduur) in de voorgeschiedenis? 4.5.2. Wat is het risico op een cardiovasculaire gebeurtenis voor vrouwen met meerdere vroeggeboortes in de voorgeschiedenis? 4.5.3. Wat is het cardiovasculaire risicoprofiel van vrouwen met een vroeggeboorte in de voorgeschiedenis?
|
Medline (OVID), Tot dec 2012 Engels, Nederlands
Embase (Elsevier) |
1 exp Obstetric Labor, Premature/ (16630) 2 ((preterm or premature) adj3 (birth* or deliver*)).ti,ab. (21419) 3 1 or 2 (29988) 4 exp Cardiovascular Diseases/ (1780857) 5 exp Renal Insufficiency/ or calcinosis/ or exp vascular calcification/ or Hypercholesterolemia/ or exp Obesity/ or exp Electrocardiography/ or exp Hypertension/ or exp Proteinuria/ or exp Diabetes Mellitus/ or Metabolic Syndrome X/ (907743) 6 (stroke or CVA or cerebrovascular or cardiovascul* or (myocard* adj2 infarct*) or atheroscleros* or "vascular calcification*" or ((renal or kidney) adj3 (insufficienc* or failure*)) or "ischaemic attack*" or TIA or "angina pectoris" or electrocardiogra* or ecg or hypercholesterolemia or obesity or hypertension or proteinuria or diabet* or ((endothelial or vascular) adj2 dysfunction*) or (("left ventricular" or myocardial) adj3 hypertroph*) or (metabol* adj2 syndrome*)).ti,ab. (1292223) 7 4 or 5 or 6 (2619398) 8 3 and 7 (4756) 13 limit 8 to english language (3950) 16 mothers/ or (maternal adj6 (cardiovascular or risk*)).ti,ab. (32037) 17 13 and 16 (312) 22 (preterm and cardiovascular).ti. (72) 23 8 and 22 (28) 24 17 or 23 (337)
('cardiovascular disease'/exp/mj OR 'kidney failure'/exp/mj OR 'diabetes mellitus'/exp/mj OR 'electrocardiography'/exp/mj OR 'hypercholesterolemia'/exp/mj OR 'hypertension'/exp/mj OR 'obesity'/exp/mj OR 'proteinuria'/exp/mj OR 'blood vessel calcification'/exp/mj OR 'metabolic syndrome x'/exp/mj OR stroke:ab,ti OR cva:ab,ti OR cerebrovascular:ab,ti OR cardiovascul*:ab,ti OR (myocard* NEAR/2 infarct*):ab,ti OR atheroscleros*:ab,ti OR (vascular NEAR/2 calcification):ab,ti OR ((renal OR kidney) NEAR/3 (insufficienc* OR failure*)):ab,ti OR (ischaemic NEAR/2 attack*):ab,ti OR tia:ab,ti OR 'angina pectoris':ab,ti OR electrocardiogra*:ab,ti OR ecg:ab,ti OR hypercholesterolemia:ab,ti OR obesity:ab,ti OR hypertension:ab,ti OR proteinuria:ab,ti OR diabet*:ab,ti OR ((endothelial OR vascular) NEAR/2 dysfunction*):ab,ti OR (('left ventricular' OR myocardial) NEAR/3 hypertroph*):ab,ti OR (metabol* NEAR/2 syndrome*):ab,ti) AND ('premature labor'/exp/mj OR ((preterm OR premature) NEAR/3 (birth* OR deliver*)):ab,ti) AND ((maternal NEAR/6 (cardiovascular OR risk*)):ab,ti OR 'mother'/exp) AND [english]/lim AND [embase]/lim NOT 'conference abstract':it
|
532 |
|
4.6 Groeibeperkt kind
4.6.1 Wat is het risico op een cardiovasculaire gebeurtenis bij vrouwen met een kind met een groeibeperkt kind (<p10) in de voorgeschiedenis? 4.6.2 Wat is het cardiovasculaire risicoprofiel van vrouwen met een kind met een groeibeperkt kind (<p10) in de voorgeschiedenis?
|
Medline (OVID), Tot dec 2012 Engels, Nederlands
Embase (Elsevier) |
1 ("small for gestational age" or SGA or ("intrauterine growth" adj3 (restriction or retardation)) or ("fetal growth" adj3 (restriction or retardation)) or IUGR).ti,ab. or Fetal Growth Retardation/ or infant, small for gestational age/ (23549) 2 exp Cardiovascular Diseases/ (1781176) 3 exp Renal Insufficiency/ or calcinosis/ or exp vascular calcification/ or Hypercholesterolemia/ or exp Obesity/ or exp Electrocardiography/ or exp Hypertension/ or exp Proteinuria/ or exp Diabetes Mellitus/ or Metabolic Syndrome X/ (908008) 4 (stroke or CVA or cerebrovascular or cardiovascul* or (myocard* adj2 infarct*) or atheroscleros* or "vascular calcification*" or ((renal or kidney) adj3 (insufficienc* or failure*)) or "ischaemic attack*" or TIA or "angina pectoris" or electrocardiogra* or ecg or hypercholesterolemia or obesity or hypertension or proteinuria or diabet* or ((endothelial or vascular) adj2 dysfunction*) or (("left ventricular" or myocardial) adj3 hypertroph*) or (metabol* adj2 syndrome*)).ti,ab. (1292793) 5 2 or 3 or 4 (2620184) 6 1 and 5 (6023) 7 (Birth characteristics and subsequent risks of maternal cardiovascular disease: effects of gestational age and fetal growth).m_titl. (1) 8 "Maternal cardiovascular disease risk in relation to the number of offspring born small for gestational age: national, multi-generational study of 2.7 million births".m_titl. (1) 9 7 or 8 (2) 10 6 and 9 (2) 11 limit 10 to english language (2) 12 limit 6 to english language (5277) 13 mothers/ or maternal.ti. or (maternal adj6 risk*).ti,ab. (74353) 14 12 and 13 (714) 17 mothers/ or (maternal adj6 (cardiovascular or risk*)).ti,ab. (32045) 18 12 and 17 (295)
'cardiovascular disease'/exp/mj OR 'kidney failure'/exp/mj OR 'diabetes mellitus'/exp/mj OR 'electrocardiography'/exp/mj OR 'hypercholesterolemia'/exp/mj OR 'hypertension'/exp/mj OR 'obesity'/exp/mj OR 'proteinuria'/exp/mj OR 'blood vessel calcification'/exp/mj OR 'metabolic syndrome x'/exp/mj OR stroke:ab,ti OR cva:ab,ti OR cerebrovascular:ab,ti OR cardiovascul*:ab,ti OR (myocard* NEAR/2 infarct*):ab,ti OR atheroscleros*:ab,ti OR (vascular NEAR/2 calcification):ab,ti OR ((renal OR kidney) NEAR/3 (insufficienc* OR failure*)):ab,ti OR (ischaemic NEAR/2 attack*):ab,ti OR tia:ab,ti OR 'angina pectoris':ab,ti OR electrocardiogra*:ab,ti OR ecg:ab,ti OR hypercholesterolemia:ab,ti OR obesity:ab,ti OR hypertension:ab,ti OR proteinuria:ab,ti OR diabet*:ab,ti OR ((endothelial OR vascular) NEAR/2 dysfunction*):ab,ti OR (('left ventricular' OR myocardial) NEAR/3 hypertroph*):ab,ti OR (metabol* NEAR/2 syndrome*):ab,ti AND ('intrauterine growth retardation'/exp/mj OR 'small for date infant'/exp/mj) AND ('small for gestational age':ab,ti OR sga:ab,ti OR ('intrauterine growth' NEAR/3 (restriction OR retardation)):ab,ti OR ('fetal growth' NEAR/3 (restriction OR retardation)):ab,ti OR iugr:ab,ti) AND ('mother'/exp OR (maternal NEAR/6 (cardiovascular OR risk*)):ab,ti) AND [english]/lim AND [embase]/lim, |
361 |