Contacteczeem organisatie van zorg
Uitgangsvraag
Op welke manier dient de zorg voor patiënten met contacteczeem (irritatief en/of allergisch) georganiseerd te worden als de verdenking bestaat dat werk een uitlokkende of onderhoudende factor is of het verrichten van werk door het eczeem belemmerd wordt?
Subvraag:
- Op welke manier kan de communicatie tussen het ARBO en curatieve zorgstelsels verbeterd worden?
Aanbeveling
- Vraag de patiënt naar werkzaamheden, blootstellingen en huidbelastende factoren. Denk hierbij ook aan aerogene blootstellingen en werkklimaat.
- Maak in de verslaglegging een onderscheid tussen irritatie, sensibilisatie en een klinisch relevante allergie voor de huidige klachten.
- Vraag in de voorgeschiedenis naar constitutioneel eczeem en co-morbiditeiten.
- Adviseer een patiënt met eczeem contact op te nemen met de bedrijfsarts als er een verdenking is op huidbelastende factoren op de werkplek.
- Overweeg voor advies en begeleiding en behandeling omtrent huidverzorging, met name bij ernstig irritatief eczeem en/of bij een combinatie met constitutioneel eczeem, doorverwijzing naar een zorgverlener zoals bijvoorbeeld de eczeem verpleegkundige, verpleegkundig specialist of de huidtherapeut.
- In overleg met de medisch specialist kan bij een allergisch contacteczeem ook een verpleegkundig specialist, eczeem verpleegkundige, physician assistant of arbo-deskundige betrokken worden ter ondersteuning bij de advisering over het vermijden van het allergeen en de huidverzorging.
Overwegingen
Kwaliteit van het bewijs
Deze module is niet gebaseerd op systematisch literatuuronderzoek omdat het een beleidsvraagstuk is. Bij het opstellen van deze module is gebruik gemaakt van reeds bestaande richtlijnen, zoals het zorgpad werkgerelateerde longziekten [LAN, 2022].
Professioneel perspectief
In deze module wordt expliciet gesteld dat allergologisch onderzoek door dermatologen én internist-allergoloog-immunologen verricht kan worden mits zij bekwaam zijn in het uitvoeren van epicutane allergologische diagnostiek en de interpretatie van de testuitslagen. Zo zal in deze module de overkoepelende term “dermato-allergologische specialist” gebruikt worden. Bij onvoldoende eigen kennis kan de patiënt naar een deskundige collega hiervoor verwezen worden. Een in contacteczeem gespecialiseerde verpleegkundig specialist kan ook ondersteunen in het uitvoeren van het allergologisch onderzoek.
Organisatie van de arbo-curatieve zorg
Netwerkzorg
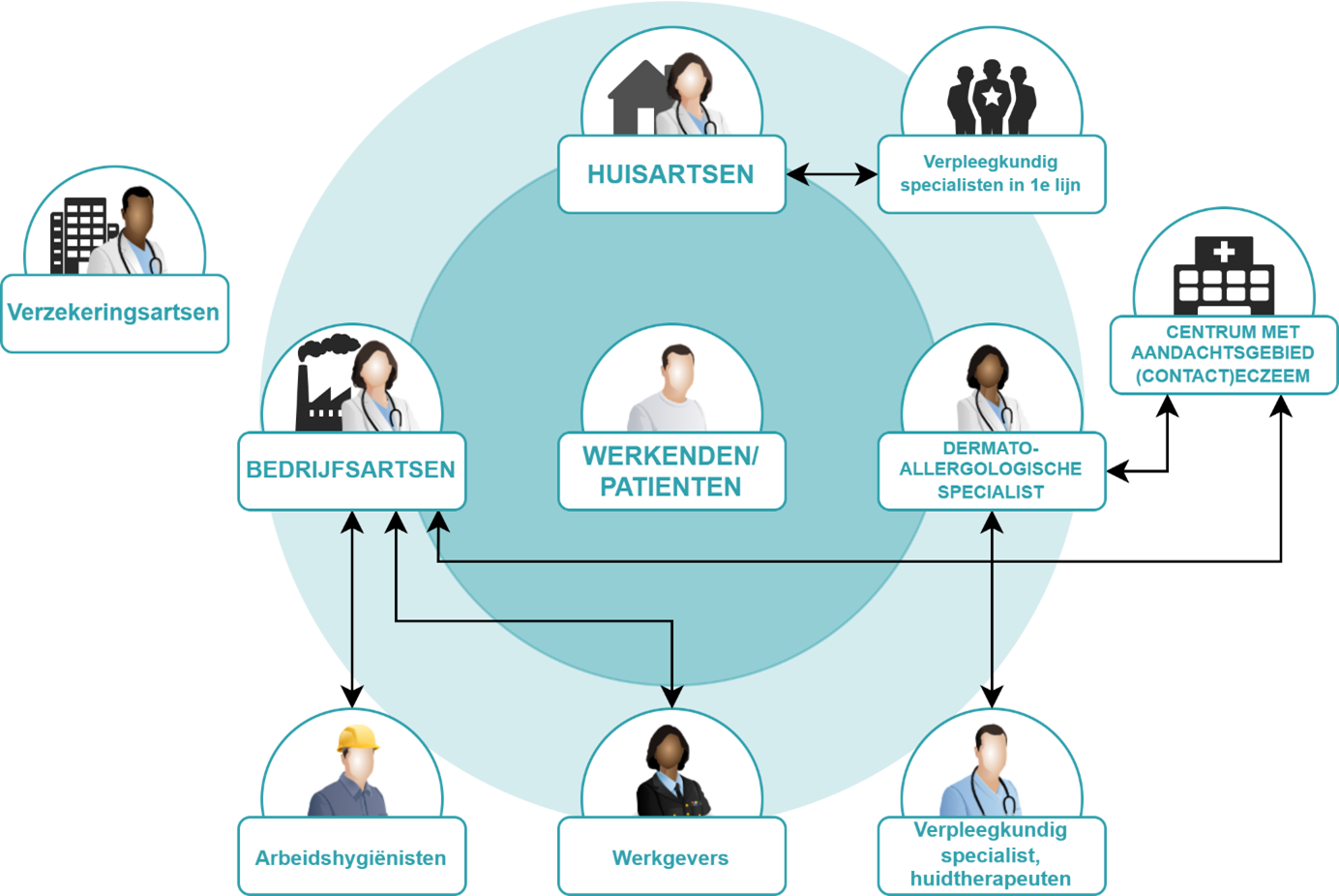
De werkgroep is van mening dat het organiseren van netwerkzorg belangrijk is om betere multidisciplinaire zorg te kunnen realiseren voor patiënten met contacteczeem en constitutioneel eczeem. Bij netwerkzorg werken de zorgverleners in de eerste en tweede lijn nauw samen om geïntegreerde en multidisciplinaire zorg te bieden. Door de communicatie en samenwerking te verbeteren kunnen diagnose, behandeling en follow-up beter worden afgestemd op de specifieke behoeften van de patiënt.
Een visualisatie van de zorgverleners die betrokken zijn bij de zorg rondom patiënten met werkgerelateerd contacteczeem is weergegeven in Figuur 1 ‘Overzicht organisatie van zorg bij (contact)eczeem’.
Figuur 1 Betrokkenen bij de zorg voor patiënten met (contact)eczeem (aangepast vanuit het Zorgpad werkgerelateerde longziekten. Bron: Long Alliantie Nederland. (2022). Zorgpad werkgerelateerde longziekten. Long Alliantie Nederland.
Diagnostiek
Contacteczeem kan worden veroorzaakt of verergerd door blootstelling aan irritantia en/of allergenen op het werk. Bij het diagnostisch onderzoek is het van belang dat zorgverleners aan patiënten vragen naar een mogelijke relatie tussen de klachten en het werk. Dit is tweeledig. Aan de ene kant gaat het om mogelijke huidbelastende factoren en blootstellingen op het werk die contacteczeem veroorzaken dan wel bestaand (constitutioneel) eczeem verergeren (zie voor meer informatie hierover de module ‘Contacteczeem diagnostiek’). Aan de andere kant gaat het om de gevolgen van het contacteczeem en constitutioneel eczeem op de mogelijkheid om het werk te kunnen blijven uitvoeren (zie voor meer informatie hierover de module ‘Kernboodschap: vraag naar werk’ binnen de richtlijn Arbeidsparticipatie voor medisch specialistische richtlijnen).
De huisarts verwijst patiënten met contacteczeem door naar een dermato-allergologisch specialist voor verdere diagnostiek en behandeling conform de NHG-standaard Eczeem [NHG-Standaard Eczeem, 2014].
Een verwijzing naar een dermato-allergologisch specialist kan ook worden gedaan door de bedrijfsarts.
Beleid en behandeling
De dermato-allergologische specialist heeft naast het diagnosticeren en eventuele allergologische onderzoek (epicutaan, intracutaan of sensibilisatie onderzoek in het bloed) en belangrijke rol in de voorlichting over de (medicamenteuze) behandeling van contacteczeem. Hierbij dienen ook atopische co-morbiditeiten in de anamnese meegenomen te worden.
Wanneer er samen met de patiënt is geconcludeerd dat de huidbelasting op de werkplek een rol speelt, wordt aangeraden om de patiënt te adviseren om contact op te nemen met een eigen bedrijfsarts. Geef de patiënt daarbij een brief met relevante informatie en de vraagstelling voor de bedrijfsarts mee. De bedrijfsarts of arbeidsgeneeskundige kan onderzoek naar huidbelastende factoren op de werkplek (laten) verrichten. Hierbij behoort ook de blootstelling aan aerogene allergenen, irritantia, persoonlijke beschermingsmiddelen en het werkklimaat. Indien de bedrijfsarts verwijzing naar een specialist in dermato-allergologie voor aanvullende diagnostiek of behandeling noodzakelijk acht, informeert hij of zij de huisarts hierover.
Het kan in de praktijk lastig zijn om contact te leggen met de bedrijfsarts van een patiënt. Mocht de medisch specialist terugkoppeling willen geven aan de bedrijfsarts, dan kan deze een brief meegeven aan de patiënt om aan de bedrijfsarts te geven. Leg uit dat de bedrijfsarts gebonden is aan geheimhoudingsplicht en de belangen van de werknemer behartigt. In sommige gevallen kan een telefonisch driegesprek tussen de medisch specialist, bedrijfsarts en patiënt nuttig zijn.
Niet alle patiënten hebben toegang tot een bedrijfsarts, vooral zelfstandigen en werknemers in kleinere bedrijven [NOV Richtlijn arbeidsparticipatie voor medisch specialistische richtlijnen, 2024]. Alleen werknemers hebben via hun werkgever toegang tot bedrijfsgeneeskundige zorg. Voor zelfstandigen is dat meestal niet het geval.
Het is de taak van een bedrijfsarts advies te geven aan zowel de werkgever als de patiënt over reductie van belasting aan huidirriterende en allergische factoren op het werk [NVAB Richtlijn Contacteczeem voor de bedrijfsarts 2020]. Hierbij kunnen arbeidshygiënisten ingeschakeld worden. Zie voor meer informatie over mogelijke werkplekinterventies de module ‘Contacteczeem arbeid’.
De verzekeringsarts komt in beeld als langdurig ziekteverzuim en uitval dreigt. In dat geval wordt de verzekeringsarts gecontacteerd door de werkgever.
Voor patiënten met contacteczeem en constitutioneel eczeem is het belangrijk om ondersteuning te bieden bij de niet-medicamenteuze behandeling en huidzorg. Daarnaast zijn begeleiding, educatie voor zelfmanagement, en advies over het omgaan met de aandoening van groot belang. De huidtherapeut of verpleegkundig specialist kan hierbij een waardevolle rol spelen. Patiënten kunnen zowel met als zonder verwijzing bij een huidtherapeut terecht (tot op heden onvergoede zorg).
Onvoldoende herstel of recidief
Als er geen oorzaak wordt gevonden, onvoldoende herstel optreedt of er sprake is van een recidief, ondanks adequate diagnostiek en behandeling, wordt aanbevolen om door te verwijzen naar een centrum dat werkgerelateerd (contact)eczeem als aandachtsgebied heeft, zoals het Amsterdam UMC, het UMCG in Groningen (beide verenigd in het NECOD), het Erasmus MC in Rotterdam of het Rijnstate ziekenhuis in Elst (GLD). In deze centra vindt multidisciplinaire samenwerking plaats tussen arbeidsdermatologen en gespecialiseerde bedrijfsartsen, die zijn aangesloten bij de Nederlandse Vereniging voor Klinische Arbeidsgeneeskunde [Bakker, 2020]. Op dit moment vallen deze onderzoeken niet onder de vergoede zorg, net zoals de diagnostiek bij elke beroepsziekte niet vergoed wordt.
Terugverwijzing
Het is de bedoeling dat bij een behandeling in de tweede en of derde lijn de patiënt uiteindelijk bij een stabiele situatie terugkeert naar de eerstelijnszorg. Na afronding van het diagnostisch proces bespreekt de dermato-allergologische specialist de resultaten en de betekenis van de testuitslagen met de patiënt en koppelt deze, in overleg met de patiënt, in een brief terug naar de verwijzer en stuurt een kopie naar de huisarts en de bedrijfsarts met een voorstel voor het beleid op lange termijn. Hierbij is het belangrijk om in ieder geval ook de volgende informatie te benoemen:
- Benoem de geteste reeksen en de positieve bevindingen van het contactallergologisch onderzoek.
- Maak een onderscheid tussen sensibilisatie en een klinisch relevante allergie
- Benoem de klinische relevantie van de positieve sensibilisaties.
- Benoem irriterende werkfactoren en factoren in de privésfeer
- Bespreek in de brief de implicaties van de positieve en negatieve resultaten voor de privé- en de werksituatie.
Apothekers
Voor het bereiken van optimale therapietrouw en behandeluitkomsten bij patiënten met contacteczeem is nauwe samenwerking tussen voorschrijvend arts en apotheker essentieel. De apotheker speelt een belangrijke rol in het herhalen en toelichten van de behandeladviezen zoals voorgeschreven door de arts. Om verwarring bij de patiënt te voorkomen is het cruciaal dat beide zorgverleners eenduidige informatie verstrekken.
Aangezien bij eczeem regelmatig sprake is van off-label gebruik van geneesmiddelen, is het van belang dat de apotheker op de hoogte is van de indicatie, het voorgeschreven gebruik en het verwachte verbruik. Deze informatie kan worden gedeeld via het recept of elektronische gegevensuitwisseling, met expliciete toestemming van de patiënt conform de richtlijn Overdracht van Medicatiegegevens in de keten (MDR, 2019).
De voorschrijvend arts dient voldoende hoeveelheid topicale middelen voor te schrijven op basis van de fingertip-unit (FTU)-methode om het aangedane huidoppervlak adequaat te kunnen behandelen. Onvoldoende aflevering kan bij de patiënt onbedoeld de indruk wekken dat spaarzaam gebruik gewenst is, wat de effectiviteit van de behandeling belemmert. De apotheker dient hierin een actieve rol te nemen door voldoende medicatie af te leveren en hierover uitleg te geven.
Het uitproberen van verschillende basiszalven via de apotheek kan helpen om een product te vinden dat goed aansluit bij de voorkeur van de patiënt. Dit verhoogt het gebruiksgemak en bevordert de therapietrouw. Wanneer patiënten zich comfortabel voelen bij een bepaalde zalf, zijn zij doorgaans gemotiveerder om het behandelplan te volgen, wat kan bijdragen aan het voorkomen of uitstellen van escalatie naar intensievere medicatie.
Het verdient aanbeveling om afspraken over de behandeling van eczeem en het gebruik van topicale middelen te bespreken tijdens regionaal farmacotherapeutisch overleg (FTO). Daarnaast is het wenselijk om apothekers te betrekken bij klinische besprekingen en onderwijsbijeenkomsten, bijvoorbeeld in ziekenhuizen of klinieken, om de samenwerking binnen de keten te versterken.
Onderbouwing
In deze module wordt de organisatie van de zorg bij patiënten met contacteczeem beschreven. Er zijn een aantal disciplines betrokken bij de zorg voor patiënten met (contact)eczeem. Enerzijds de specialisten (dermatologen, allergologen, immunologen), anderzijds de huisarts en overige disciplines (zoals de bedrijfsarts, verzekeringsarts, huidtherapeut of verpleegkundig specialist).
Binnen de huidige zorgstructuur is er een scheiding tussen de curatieve- en bedrijfsgeneeskundige gezondheidszorg. Dit kan leiden tot onduidelijkheden over de mogelijkheden tot doorverwijzing en samenwerking tussen de verschillende disciplines. Samenwerking is van belang met als doel het beleid van deze disciplines op elkaar af te stemmen en de patiëntenzorg te verbeteren.
Voor deze vraag is geen systematische literatuuranalyse verricht. Overwegingen en aanbevelingen zijn gebaseerd op basis van expert opinion.
- Bakker, J. G., & Wintzen, M. (2010). Handeczeem: een arbeidsgerelateerd probleem. TBV–Tijdschrift voor Bedrijfs-en Verzekeringsgeneeskunde, 18, 22-25. Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (NVAB). Richtlijn Preventie van contacteczeem, 2020.
- Dirven-Meijer, P. C., De Kock, C. A., Nonneman, M. M. G., Van Sleeuwen, D., De Witt-de Jong, A. W. F., Burgers, J. S., De Vries, C. J. H. (2014). NHG-standaard eczeem. Huisarts wet, 57(5), 240-52.
- LAN: Long Alliantie Nederland. (2022). Zorgpad werkgerelateerde longziekten. Long Alliantie Nederland.
- NHG Richtlijn informatie uitwisseling 2017: https://richtlijnendatabase.nl/richtlijn/informatie-uitwisseling_tussen_huisarts_en_specialist_hasp/richtlijn_informatieuitwisseling_tussen_huisarts_en_specialist.html Geraadpleegd juli 2024.
Risk of bias
De Risk of bias analyse is overgenomen uit het standpunt van het Zorginstituut Nederland, de volledige Risk of bias analyse is ook terug te vinden in dit standpunt (Zorginstituut Nederland 2023). Het Zorginstituut Nederland heeft de methodologische kwaliteit van de studie van Ragamin et al. beoordeeld aan de hand van de Cochrane Risk of Bias tool. Zij vonden een hoog risico op attrition bias vanwege uitval van patiënten. De uitval was het grootst in de chitosangroep (44% na 12 maanden) en het kleinst in de controlegroep (17% na 12 maanden).
Beoordelingsdatum en geldigheid
Publicatiedatum : 23-09-2025
Beoordeeld op geldigheid : 22-07-2025
Algemene gegevens
De ontwikkeling van deze richtlijnmodule werd ondersteund door Nederlandse Vereniging van Dermatologie en Venereologie (NVDV) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2024 een multidisciplinaire cluster ingesteld. Dit cluster bestaat uit vertegenwoordigers van alle relevante organisaties die betrekking hebben op de zorg voor patiënten met: eczeem.
Het cluster Eczeem bestaat uit meerdere richtlijnen, zie hier voor de actuele clusterindeling. De stuurgroep bewaakt het proces van modulair onderhoud binnen het cluster. De expertisegroepsleden worden indien nodig gevraagd om hun expertise in te zetten voor een specifieke richtlijnmodule. Het cluster Eczeem bestaat uit de volgende personen:
Clusterstuurgroepleden
- S. Stewart, Nederlandse Vereniging van Dermatologie en Venereologie (NVDV)
- M.L. Schuttelaar, NVDV
- M. de Bruin-Weller, NVDV
- I. Haeck, NVDV
- D.M.W. Gorissen, Nederlandse Vereniging voor Kindergeneeskunde (NVK)
Clusterexpertisegroepleden
- S. Stewart, NVDV
- T. Rustemeyer, NVDV
- M.L. Schuttelaar, NVDV
- M. de Bruin-Weller, NVDV
- L. Gerbens, NVDV
- S. G. M. A. Pasmans, NVDV
- I. Haeck, NVDV
- A.M. van Tuyll van Serooskerken, NVDV
- C.M. van Luijk, Nederlandse Oogheelkundig Gezelschap (NOG)
- L. Dam – Vervloet, Nederlandse Vereniging voor Klinische Fysica (NVKF)
- D.M.W. Gorissen, NVK
- R. Lakenman, Jeugdartsen Nederland
- R. Rösken, Nederlandse Internisten Vereniging (NIV) en Nederlandse Vereniging voor Allergologie en Klinische Immunologie (NVvAKI)
- W.P. Piebenga, Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (NVAB)
- M. van Dijk, Nederlandse Vereniging Voor Pathologie (NVVP)
- B. Breeuwsma, Nederlandse Maatschappij ter bevordering der Pharmacie (KNMP)
- K. Sterkenburg, Nederlandse Vereniging Huidtherapeuten (NVH)
- J. de Groot, Verpleegkundigen & Verzorgenden Nederland (V&VN)
- W. Kouwenhoven, Vereniging voor Mensen met Constitutioneel Eczeem (VMCE)
Ondersteuning werkgroep:
- Dr. W.A. van Enst, epidemioloog, NVDV
- Drs. A. Kersbergen, arts-onderzoeker mei 2024 t/m januari 2025
- Drs. M.R. Masselink, arts-onderzoeker vanaf februari 2025
Met ondersteuning van
- Nederlandse Vereniging van Dermatologie en Venereologie (NVDV)
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle clusterstuurgroepleden en actief betrokken expertisegroepsleden (fungerend als schrijver en/of meelezer bij tenminste één van de geprioriteerde richtlijnmodules) hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een richtlijnmodule worden wijzigingen in belangen aan de projectleider doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase. Een overzicht van de belangen van de clusterleden en betrokken expertisegroepsleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
Clusterstuurgroep
Tabel 1. Gemelde (neven)functies en belangen stuurgroep
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
S. Stewart
|
Voorzitter modulaire herziening richtlijn CE Dermatoloog Ijsselland Ziekenhuis |
Project Huid in de Klas – Huidpatiënten Nederland: 1 sessie betaald, de rest onbetaald |
IJsselland ziekenhuis neemt deel aan Bioday Registry |
Geen |
|
M.L. Schuttelaar |
Associate professor, dermatoloog UMC Groningen |
Advisor, consultant, speaker and/or investigator for AbbVie, Pfizer, LEO Pharma, Regeneron, Sanofi Genzyme, Eli Lilly, Galderma and Amgen. She has received grants from Regeneron, Sanofi Genzyme, Novartis and Pfizer. It involves paid work, for the department in the UMCG where I work or personally |
Geen |
Geen |
|
M. de Bruin-Weller |
Dermatoloog UMC Utrecht |
- Speakers Honoraria: (Betaald aan UMCU) - AbbVie, Almirall, Eli Lilly, Galderma, Leo Pharma, Novartis, Pfizer, Takeda, Regeneron, and Sanofi-Genzyme |
Extern gefinancieerd onderzoek:
|
Geen |
|
I. Haeck |
Dermatoloog UMC Utrecht |
Adviesraad/consultant voor: Lilly, Abbvie, Sonofi/Regeneron, LEO Pharma
M18-891 studie Abbvie |
Geen |
Geen |
|
D.M.W. Gorissen |
Kinderarts-allergoloog Deventer Ziekenhuis 0.7fte, Medisch Leider Innovatie en Zorgtransformatie Deventer Ziekenhuis 0.2fte |
Voorzitter Nationale Allergie Monitor, onbetaald. |
Expertcommissie rondom ernstig eczeem en rol van systemische medicatie daarbinnen, waarvoor honorering door de farmaceutische industrie. In de bijdrage aan het cluster eczeem niet bemoeid met het onderdeel systemische medicatie. |
Geen |
Clusterexpertisegroep
Tabel 2. Gemelde (neven)functies en belangen expertisegroep
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
S. Stewart |
Voorzitter modulaire herziening richtlijn CE Dermatoloog Ijsselland Ziekenhuis |
Project Huid in de Klas – Huidpatiënten Nederland: 1 sessie betaald, de rest onbetaald |
IJsselland ziekenhuis neemt deel aan Bioday Registry |
Geen |
|
T. Rustemeyer |
Leidinggevende van de subafdeling Dermato-Allergologie en Arbeidsdermatologie, dermatoloog Amsterdam UMC |
- Bestuurslid NVKA. Onbetaald. Voorzitter van verschillende ESCD en -EADV taskforce. Onbetaald. |
Adviesraden en Sanofi, LeoPharma, Janssen, Pfizer, Galderma, Vifor, L’Oreal. |
Geen |
|
M.L. Schuttelaar |
Professor, dermatoloog UMC Groningen |
Advisor, consultant, speaker and/or investigator for AbbVie, Pfizer, LEO Pharma, Regeneron, Sanofi Genzyme, Eli Lilly, Galderma and Amgen. She has received grants from Regeneron, Sanofi Genzyme, Novartis and Pfizer. It involves paid work, for the department in the UMCG where I work or personally |
Geen |
Geen |
|
M. de Bruin-Weller |
Dermatoloog UMC Utrecht |
- Speakers Honoraria: (Betaald aan UMCU) - AbbVie, Almirall, Eli Lilly, Galderma, Leo Pharma, Novartis, Pfizer, Takeda, Regeneron, and Sanofi-Genzyme |
Extern gefinancieerd onderzoek:
|
Geen |
|
L. Gerbens |
Dermatoloog Amsterdam UMC, Huid Medisch Centrum |
- Co-auteur European Dermatology Forum (EDF) EuroGuiDerm Atopic Dermatitis guideline, geleid doorprof. dr. A. Wollenberg en prof. dr. C. Flohr. Onbetaald. - Projectleider UPDATE trial, beurs ZonMw. Mijn functie is in-kind. - Data Monitoring Board (DMC) van A-STAR registry UK/Ireland. Onbetaald. - Lid Board of Directors C3: The CHORD COUSIN Collaboration for Dermatology Outcomes. Onbetaald. - Lid Scientific Committee Skin Inflammation & Psoriasis International Network (SPIN). Onbetaald. - Advisory journal editor of Dutch Amsterdam Medical Student journal (AMSj). Onbetaald. - Lid Executive Committee Harmonising Outcome Measurements for Eczema (HOME) initiative. Onbetaald. - Lid steering committee of the international TREatment of ATopic eczema (TREAT) Registry Taskforce and of the Dutch TREAT NL registry. Onbetaald. |
Geen. Wel projectleider UPDATE trial; NB-UVB bij atopisch eczeem. Geen systemische medicatie is hierbij betrokken. |
Geen |
|
S. G. M. A Pasmans |
Professor, (kinder)dermatoloog/immunoloog Erasmus Universiteit Rotterdam, Erasmus MC-Sophia Kinderziekenhuis/afdeling Dermatologie, Centrum Kinderdermatologie/ Centrum voor Zeldzame Huidziekten |
- Huidpatienten Nederland; bestuurslid en commissielid zeldzame huidaandoeningen - Board Member of the European Reference Network Skin+vice chair subthematic group Mosaicism; coordinator transversal groups registry, research; coordinator HPO in dermatology. Onkostenvergoeding. - Board member European Society of Pediatric Dematology; chair education for certificaat in pediatric dermatology. Onkostenvergoeding. - Lid Domeingroep Kinderdermatologie Nederlandse Vereniging voor Dermatologie en Venereologie (vacatiegelden). -Lid domeingroep Eczeem en Allergie NVDV (vacatiegelden). - Advisor, consultant, speaker and/or investigator for LEO Pharma, Regeneron Pharmaceuticals, Sanofi Genzyme, Novartis, Pierre Fabre. Boehringer, Quoin, Biocryst. Onkostenvergoeding/vergoeding werkzaamheden. - Unrestricted grant department of dermatology of Pierre Fabre, VWS/Zorginstituut/ZonMw, ZonMw, Novartis, BAP Medical, D&M B.V., and DeclaCare (part of BENU Netherlands), Micreos, Boehringer, Sophia foundation. Vergoeding werkzaamheden. - NFU-Rare disease program beoordelaar en ook deelnemer Onkostenvergoeding. - ZonMW commissie Paramedische zorg till Dec 2024 (onkostenvergoeding). - Lid medische adviesraad Patiëntenvereniging Hemangiomen en Vaatmalformaties (HEVAS). Onkostenvergoeding. - Lid medische adviesraad Patiëntenvereniging Alopecia Areata. Onkostenvergoeding. - Lid medische adviesraad Patiëntenvereniging Cutis Marmorata Teleangiectatica Congenita. Onkostenvergoeding. - Lid medische adviesraad Patiëntenvereniging Nevus Netwerk Nederland. Onkostenvergoeding. - Lid Raad van advies Stichting Under Your Skin Foundation. - Bestuurslid Stichting Huidhuis.nl. - Ontwikkelen van informatie voor patienten (en betrokken professionals) voor Nationaal Constitutioneel Eczeem Plan (NCEP), Huidhuis.nl, ERN-SKIN, centrum Kinderdermatologie/Zeldzame Huidziekten. - Initiator and organizer together with Netherton patients of the International Netherton Networkrk. - Voorzitter revisie richlijn Congenital Melanocytic Nevi. Vacatiegelden. - Lid werkgroep commissie revisie richtlijn Huid voor de Jeugdgezondheidszorg. Vacatiegelden. - Lid werkgroep modulaire revisie richtlijn Constitutioneel eczeem. Vacatiegelden. - Marathons and triathlons for fundraising for the Under Your Skin Foundation: NCEP, huishuis.nl, information for patients (and professionals). |
Verbandpakken studie-ABC studie heeft een “unrestricted grant” aan de afdeling dermatologie gegeven naast het ministerie van VWS voor het uitvoeren van de trial multicenter |
Geen |
|
I. Haeck |
Dermatoloog UMC Utrecht |
Adviesraad/consultant voor: Lilly, Abbvie, Sonofi/Regeneron, LEO Pharma
M18-891 studie Abbvie |
Geen |
Geen |
|
A.M. van Tuyll van Serooskerken |
Dermatoloog HagaZiekenhuis |
Adviesraden voor verschillende firma's echter hiervoor geen persoonlijke betaling aangezien vergoeding voor werkzaamheden gestort wordt op de Stichting Dermatologische Scholing en Communicatie ten behoeve van de kwaliteit van zorg t.b.v. het NCEP Projectleider Nationaal Constitutioneel Eczeem Project (NCEP): onbetaald. |
Deelname aan het pedistad onderzoek, maar dit heeft weer geen relatie met advies met t.b.v. de richtlijn |
Geen |
|
R. Lakenman |
Jeugdarts KNMG GGD Hollands Noorden |
Geen |
Geen |
Geen |
|
C.M. van Luijk |
Oogarts UMC Utrecht |
Eenmalig betaalde nascholing door Santen (4-2021)
Eenmalig deelname adviescommissie bijwerkingen dupilumab waarvoor vergoeding door Regeneron (12-2019)
Bijzondere en unieke expertise in atopische oogpathologie binnen multidisciplinair eczeem zorgteam in UMC Utrecht |
Beurs voor onderzoek te besteden aan ciclosporine door Santen. Onafhankelijkheid verklaard in overeenkomst. |
Geen |
|
D.M.W. Gorissen |
Kinderarts-allergoloog Deventer Ziekenhuis |
Geen |
Geen |
Geen |
|
R. Rösken |
Internist allergoloog-immunoloog Zaans Medisch Centrum |
Geen |
Geen |
Geen |
|
W.P. Piebenga |
Bedrijfsarts en klinisch arbeidsgeneeskundige Amsterdam UMC |
Geen |
Geen |
Geen |
|
M. van Dijk |
Professor, patholoog UMC Utrecht |
Spreker op symposia en congressen, deels betaald, deels onbetaald. |
Geen |
Geen |
|
B. Breeuwsma |
Apotheker, Apotheek pharmacor |
Geen |
Geen |
Geen |
|
W. Kouwenhoven |
Patiëntvertegenwoordiger VMCE |
Geen |
Geen |
Geen |
|
K. Sterkenburg |
Huidtherapeut, Beleidsmedewerker onderzoek & kwaliteit bij de Nederlandse Vereniging van Huidtherapeuten |
Projectlid 'Eczeemvriendelijk Veenendaal'. Betaald. |
Geen |
Geen |
|
J. de Groot |
Verpleegkundig specialist UMC Utrecht |
Geen |
Geen |
Geen |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door deelname van relevante patiëntenorganisaties aan de need-for-update en/of prioritering. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijnmodule is tevens ter commentaar voorgelegd aan alle relevante patiëntenorganisaties in de stuur- en expertisegroep (zie ‘Samenstelling cluster’ onder ‘Verantwoording’) en aan alle patiëntenorganisaties die niet deelnemen aan de stuur- en expertisegroep, maar wel hebben deelgenomen aan de need-for-update (zie ‘Need-for-update’ onder ‘Verantwoording’). De eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Module |
Uitkomst raming |
Toelichting |
|
Organisatie van zorg |
Geen financiële gevolgen |
Uitkomst 3 |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 3.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Need-for-update, prioritering en uitgangsvragen
Tijdens de need-for-update fase (oktober, 2023) inventariseerde het cluster de geldigheid van de richtlijnmodules binnen het cluster. Naast de partijen die deelnemen aan de stuur- en expertisegroep zijn hier ook andere stakeholders voor benaderd. Per richtlijnmodule is aangegeven of deze geldig is, herzien moet worden, kan vervallen of moet worden samengevoegd. Ook was er de mogelijkheid om nieuwe onderwerpen aan te dragen die aansluiten bij één (of meerdere) richtlijn(en) behorend tot het cluster. De richtlijnmodules waarbij door één of meerdere partijen werd aangegeven herzien te worden, werden doorgezet naar de prioriteringsronde. Ook suggesties voor nieuwe richtlijnmodules werden doorgezet naar de prioriteringsronde. Afgevaardigden vanuit de partijen in de stuur- en expertisegroep werden gevraagd om te prioriteren (zie ‘Samenstelling cluster’ onder ‘Verantwoording’). Hiervoor werd de RE-weighted Priority-Setting (REPS) – tool gebruikt. De uitkomsten (ranklijst) werd gebruikt als uitgangspunt voor de discussie. Voor de geprioriteerde richtlijnmodules zijn door de het cluster concept-uitgangsvragen herzien of opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde het cluster welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. Het cluster waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde het cluster tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’. Indien mogelijk werd de data uit verschillende studies gepoold in een [random-effects model]. [Review Manager 5.4] werd indien mogelijk gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding). GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
Tabel 6. Gradaties voor de kwaliteit van wetenschappelijk bewijs
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in een richtlijnmodule volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door het cluster wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. Het cluster heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
Tabel 7. Sterkte van de aanbevelingen
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
Bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de richtlijnmodule Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd voorgelegd aan alle partijen die benaderd zijn voor de need-for-update fase. De commentaren werden verzameld en besproken met het cluster. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door het cluster. De definitieve richtlijnmodule werd ter autorisatie of goedkeuring voorgelegd aan de partijen die beschreven staan bij ‘Initiatief en autorisatie’ onder ‘Verantwoording’.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Voor dit hoofdstuk geldt dat de zoekstrategie is uitgevoerd in de EMBASE database, Medline database en de Cochrane library. Enkel de keywords gebruikt in de Medline database zijn weergeven. Experts op het gebied van constitutioneel eczeem en contacteczeem werden geraadpleegd voor eventuele ontbrekende artikelen en / of casereports. De search is geüpdatet tot 24-4-2024.
De zoekactie is met behulp van de PICO-systematiek opgebouwd. De zoekvragen hebben de P als gemeenschappelijke onderdeel. De overige onderdelen van de PICO werden geformuleerd op basis van de uitgangsvraag.
De volgende afbakening is gebruikt:
Voor de P: baby’s, kinderen en volwassenen met matig tot ernstig constitutioneel eczeem (CE)
Voor de I: verbandkleding met antibacteriële toevoeging chitosan of zilver
Voor de C: verbandkleding zonder antibacteriële toevoeging
Voor de O: de relevante cruciale en belangrijke uitkomsten
Voor de T: relevante follow-up duur: minimaal 1 jaar (52 weken) voor beoordeling van effectiviteit en veiligheid
Inclusie- en exclusiecriteria
|
Inclusiecriteria |
Exclusiecriteria |
|
Gepubliceerd ná 23 april 2023 |
|
|
Vergelijkend onderzoek (RCT, CCT, SR (RCT/CCT) |
|
|
|
|
Uitgangsvragen
- Wat is de meerwaarde van antibacteriële verbandpakken ten opzichte van niet antibacteriële verbandpakken bij patiënten met matig tot ernstig constitutioneel eczeem?
EMBASE (datum 24-04-2024)
Zoektermen
('constitutional eczema'/exp OR 'atopic dermatitis'/exp OR 'neurodermatitis'/exp OR (neurodermatit* OR ((atopic*) NEAR/2 (eczema* OR dermatit*))):ab,ti) AND ('protective clothing'/de OR 'textile'/exp/mj OR 'bandages and dressings'/de/mj OR 'bandage'/exp/mj OR (garment* OR undergarment* OR cloth* OR fabric OR fabrics OR textile* OR ((fiber OR fibers) NOT (diet*)) OR bandage* OR dressing*):ab,ti) NOT ((animal/exp OR animal*:de OR nonhuman/de) NOT ('human'/exp)) NOT ([Conference Abstract]/lim) AND ('systematic review'/de OR 'randomized controlled trial'/exp OR (randomi* OR ((systematic*) NEAR/3 (review*)) OR meta-analys* OR metaanaly*):ab,ti OR 'Cochrane Database Syst Rev'/ta)
Resultaten = [5 publicaties]
MEDLINE (datum 24-04-2024)
Zoektermen
(exp "Dermatitis, Atopic"/ OR exp "Neurodermatitis"/ OR (neurodermatit* OR ((atopic*) ADJ2 (eczema* OR dermatit*))).ab,ti.) AND ("Protective Clothing"/ OR "Textiles"/ OR exp *"Bandages"/ OR (garment* OR undergarment* OR cloth* OR fabric OR fabrics OR textile* OR ((fiber OR fibers) NOT (diet*)) OR bandage* OR dressing*).ab,ti.) NOT (exp animals/ NOT humans/) NOT (news OR congres* OR abstract* OR book* OR chapter* OR dissertation abstract*).pt. AND ("Randomized Controlled Trial".pt. OR "Systematic Review".pt. OR (randomi* OR ((systematic*) ADJ3 (review*)) OR meta-analys* OR metaanaly*).ab,ti.)
Resultaten = [4 publicaties]
Cochrane (datum 24-04-2024)
Zoektermen
((neurodermatit* OR ((atopic*) NEAR/2 (eczema* OR dermatit*))):ab,ti) AND ((garment* OR undergarment* OR cloth* OR fabric OR fabrics OR textile* OR ((fiber OR fibers) NOT (diet*)) OR bandage* OR dressing*):ab,ti) AND ((randomi* OR ((systematic*) NEAR/3 (review*)) OR meta NEXT/1 analys* OR metaanaly*):ab,ti)
Resultaten = [5 publicaties, 2 uniek]
Cochrane Reviews (0)
All
Review
Protocol
Other Reviews (0)
Trials (5)
Methods Studies (0)
Technology Assessments (0)
Economic Evaluations (0)
Cochrane Groups (0)
Alle resultaten
|
Database |
Datum |
# hits |
|
EMBASE |
24-04-2024 |
5 |
|
MEDLINE |
24-04-2024 |
4 |
|
Cochrane |
24-04-2024 |
2 |
|
Totaal |
11 |
|
|
Duplicates |
5 |
|
|
Netto aantal |
6 |
|
In de systematische review door het Zorginstituut Nederland in 2023 naar de effecten van antibacteriële toevoeging van zilver of chitosan aan verbandmiddel bij matig tot ernstig CE werd een zoekactie uitgevoerd naar RCT’s en systematische reviews in Embase, Medline en Cochrane Central voor de periode tot april 2023. Er werd gebruik gemaakt van reference checking om aanvullende RCT’s te vinden. De zoekstrategie van het Zorginstituut identificeerde in totaal 140 publicaties, waarvan er 12 werden geselecteerd op basis van beoordeling van titel en abstract. Uiteindelijk werd geen van deze studies geïncludeerd na beoordeling van de volledige tekst. Het standpunt van het Zorginstituut wordt daarom volledig gebaseerd op de resultaten van de ABC-studie (Ragamin 2024).
In de aanvullende zoekactie vanaf april 2023 werden 6 studies geïdentificeerd waaronder het artikel van de ABC-studie van Ragamin et al (2024). Uiteindelijk werden er op basis van beoordeling van titel en abstract geen verdere studies geïncludeerd.